CT Findings in Superior Vena Cava Obstruction€¦ · SUPERIOR VENA CAVA OBSTRUCTION Fig 1. Massive...
7
CT Findings in Superior Vena Cava Obstruction By Joseph W. Yedlicka, Kurt Schultz, Rogelio Moncada, and Michael Flisak T HE CLINICAL manifestations of SVCS were first described by Hunter in 1757, secondary to a syphilitic aneurysm of the ascending aorta.’ SVCS usually has an insidious presentation and eventually leads to a collection of signs and symptoms that together are diagnos- tic of the disorder. Obstruction of the SVC may result from external compression or intrinsic thrombotic disorders, and leads to proximal venous hypertension of varying magnitude. Clin- ically, the syndrome is manifested by: (1) the progressive dilatation of the veins of the upper trunk, arms, neck, and head; (2) increasing edema and plethora of the face, neck, upper torso, and breasts (Fig 1); (3) CNS disturbances with visual symptoms, syncope, dizziness, head- aches, altered state of consciousness, and somno- lence; (4) cyanosis and conjunctival edema; and (5) edema of the trachea and esophagus with respiratory distress and dysphagia. The development of the SVCS relates to the nature of the blood vessel as well as to the surrounding mediastinal anatomy. The SVC is a thin-walled structure without valves that drains ABBREVIATIONS CNS, central nervous system IVC, inferior vena cava LIV, left innominate vein MRI, magnetic resonance imaging RUL, right upper lobe SVC, superior vena cava SVCS, superior vena cava syndrome From the Department of Radiology, University of Minne- sota, Minneapolis; and the Department of Radiology, Loyola University Medical Center, Loyola. IL. Joseph W. Yedlicka: Fellow, Department of Radiology. University of Minnesota; Kurt Schultz: Resident, Depart- ment of Radiology, Loyola University Medical Center; Rogelio Moncada: Professor and Chairman, Department of Radiology. Loyola University Medical Center; Michael Flis- ak: Professor, Department of Radiology, Loyola University Medical Center. Address reprint requests to Rogelio Moncada, MD, Department of Radiology, Loyola University Medical Cen- ter, 2160 S First Ave. Maywood, IL 60153. 0 1989 by W.B. Saunders Company. 0037- I98X/89/2402-0004$5.00/0 the returning blood flow of the head and upper half of the trunk. It measures approximately 7 cm in length and has a varied cross-sectional shape. The greatest diameter of the normal SVC is generally about 1.5 cm, but can be as much as 2.0 cm. The intravascular pressure of the SVC is low, a reflection of the normally low systemic venous pressure. The SVC is firmly bound in the right anterosuperior mediastinum and is in contact with the ascending aorta, right pulmonary arte- ry, left atrium, right pulmonary veins, and the right main stem bronchus. It is flanked by a network of lymph nodes and small lymphatic vessels. Lymph drainage from the right thoracic cavity and the lower part of the left cavity passes through these nodes. The azygos vein is the major tributary of the SVC and is formed by the lumbar veins at the level of the diaphragmatic crura, and ascends to enter the dorsal aspect of the mid-SVC. Small pericardial and mediastinal veins may drain into the intrapericardial portion of the SVC. The lower half of the SVC is covered by the parietal pericardium, and its wall is partially lined by the visceral pericardium. There is rela- tive fixation of the SVC due to its intrapericar- dial location, leaving little room for its displace- ment by a space-occupying lesion. The vessel is, however, susceptible to pericardial or cardiac abnormalities. Compression of this low-pressure, thin-walled vessel leads to compromise of its lumen (Figs 2 and 3). When the lumen is completely obliter- ated, the signs and symptoms of SVCS become evident, especially if the azygos vein orifice is also obstructed. However, partial obstruction occurring slowly may allow enough collateral circulation to develop so that the obstruction may not be clinically apparent. In the event of SVC obstruction, there are four main routes of collateral circulation between the SVC and IVC: azygos/hemiazygos, internal mammary, vertebral, and thoracoepigastric/lat- era1 thoracic veins. Superior intercostal and paraesophageal veins may also serve as part of the collateral circulation. Blood may be diverted to the periumbilical veins and subsequently to the 84 Seminars in Roentgenology, Vol XXIV, No 2 Mpril), 1989: pp 84-90
Transcript of CT Findings in Superior Vena Cava Obstruction€¦ · SUPERIOR VENA CAVA OBSTRUCTION Fig 1. Massive...

CT Findings in Superior Vena Cava Obstruction
By Joseph W. Yedlicka, Kurt Schultz, Rogelio Moncada, and Michael Flisak
T HE CLINICAL manifestations of SVCS were first described by Hunter in 1757,
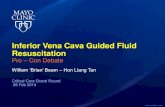
secondary to a syphilitic aneurysm of the ascending aorta.’ SVCS usually has an insidious presentation and eventually leads to a collection of signs and symptoms that together are diagnos- tic of the disorder. Obstruction of the SVC may result from external compression or intrinsic thrombotic disorders, and leads to proximal venous hypertension of varying magnitude. Clin- ically, the syndrome is manifested by: (1) the progressive dilatation of the veins of the upper trunk, arms, neck, and head; (2) increasing edema and plethora of the face, neck, upper torso, and breasts (Fig 1); (3) CNS disturbances with visual symptoms, syncope, dizziness, head- aches, altered state of consciousness, and somno- lence; (4) cyanosis and conjunctival edema; and (5) edema of the trachea and esophagus with respiratory distress and dysphagia.
The development of the SVCS relates to the nature of the blood vessel as well as to the surrounding mediastinal anatomy. The SVC is a thin-walled structure without valves that drains
ABBREVIATIONS
CNS, central nervous system
IVC, inferior vena cava LIV, left innominate vein MRI, magnetic resonance imaging RUL, right upper lobe SVC, superior vena cava SVCS, superior vena cava syndrome
From the Department of Radiology, University of Minne-
sota, Minneapolis; and the Department of Radiology, Loyola University Medical Center, Loyola. IL.
Joseph W. Yedlicka: Fellow, Department of Radiology. University of Minnesota; Kurt Schultz: Resident, Depart- ment of Radiology, Loyola University Medical Center; Rogelio Moncada: Professor and Chairman, Department of
Radiology. Loyola University Medical Center; Michael Flis- ak: Professor, Department of Radiology, Loyola University Medical Center.
Address reprint requests to Rogelio Moncada, MD, Department of Radiology, Loyola University Medical Cen- ter, 2160 S First Ave. Maywood, IL 60153.
0 1989 by W.B. Saunders Company. 0037- I98X/89/2402-0004$5.00/0
the returning blood flow of the head and upper half of the trunk. It measures approximately 7 cm in length and has a varied cross-sectional shape. The greatest diameter of the normal SVC is generally about 1.5 cm, but can be as much as 2.0 cm.
The intravascular pressure of the SVC is low, a reflection of the normally low systemic venous pressure. The SVC is firmly bound in the right anterosuperior mediastinum and is in contact with the ascending aorta, right pulmonary arte- ry, left atrium, right pulmonary veins, and the right main stem bronchus. It is flanked by a network of lymph nodes and small lymphatic vessels. Lymph drainage from the right thoracic cavity and the lower part of the left cavity passes through these nodes.
The azygos vein is the major tributary of the SVC and is formed by the lumbar veins at the level of the diaphragmatic crura, and ascends to enter the dorsal aspect of the mid-SVC. Small pericardial and mediastinal veins may drain into the intrapericardial portion of the SVC.
The lower half of the SVC is covered by the parietal pericardium, and its wall is partially lined by the visceral pericardium. There is rela- tive fixation of the SVC due to its intrapericar- dial location, leaving little room for its displace- ment by a space-occupying lesion. The vessel is, however, susceptible to pericardial or cardiac abnormalities.
Compression of this low-pressure, thin-walled vessel leads to compromise of its lumen (Figs 2 and 3). When the lumen is completely obliter- ated, the signs and symptoms of SVCS become evident, especially if the azygos vein orifice is also obstructed. However, partial obstruction occurring slowly may allow enough collateral circulation to develop so that the obstruction may not be clinically apparent.
In the event of SVC obstruction, there are four main routes of collateral circulation between the SVC and IVC: azygos/hemiazygos, internal mammary, vertebral, and thoracoepigastric/lat- era1 thoracic veins. Superior intercostal and paraesophageal veins may also serve as part of the collateral circulation. Blood may be diverted to the periumbilical veins and subsequently to the
84 Seminars in Roentgenology, Vol XXIV, No 2 Mpril), 1989: pp 84-90

SUPERIOR VENA CAVA OBSTRUCTION
Fig 1. Massive edema of the chest wall in a patient
with SVC obstruction. Pleural effusion8 IE) are present.
85
left portal vein along the ligamentum teres by superficial thoracoabdominal and epigastric veins, accounting for the “hot spot” projected over the liver on radionuclide scans in such cases.2 In cases of WC obstruction, Ishikawa et al3 described an abnormal area of enhancement in the liver on contrast-enhanced CT, repre- senting collateral flow.
ETIOLOGY
The overwhelming majority of cases of SVC obstruction are due to malignant disease. Iatro- genie manipulation has recently become increas- ingly frequent.4-7 The pulmonary artery catheter, peritoneovenous shunt, hyperalimentation line,
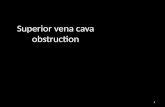
Fig 2. Mediistinal lymph-
adenopathy causing narrowing of the SVC in a patient with
lymphoma.

86
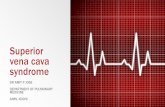
central venous pressure monitor, and transvenous pacemaker have all been associated with WCS. The wall of the SVC may be compressed or directly invaded by tumor. Tumor thrombus may occlude the vessel (Fig 4) or the lumen may be narrowed and encased by nodal metastases.
Mclntire and Sykeq8 in a review of cases of SVCS before 1949, showed that only one third were caused by primary intrathoracic malignan- cy. One third were secondary to aortic aneurysm (now a rare cause). Compression by scar tissue (chronic mediastinitis) accounted for 15% and metastatic disease for 3%.
Recent reviews have shown the percentage of
YEDLICKA ET AL
cases of SVCS from malignant tumor has been steadily increasing. Today SVCS has become virtually synonymous with malignant obstruc- tion. Reviews indicate a primary malignant etiol- ogy for SVCS in 65% to 97% of the patientsg-13 Lochridge et al reported that 82% of the patients with malignant etiology had bronchogenic carci- noma, 12% lymphoma, and 6% metastatic dis- ease.13 Ooizumi et alI4 reported an incidence of SVCS of 4% among all patients with lung cancer and 8% of patients with small cell type. Shimm et all5 stated that 5% to 15% of lung cancers, 5% of lymphomas, and 1% of pulmonary metastases result in SVCS. The most common metastatic
Fig 4. Metastatic renal cell carcinoma. Filling defect representing a thrombus (T) in right subclavian vein. Collateral vessels rows). (B) Filling defects in the SVC re senting tumor thrombus. Note the enhan sternal metastasis (MI.
(A) / the (ar-
pre- cing
SUPERIOR VENA CAVA OBSTRUCTION
neoplasm to cause SVCS has been reported to be breast carcinoma.”
SVC obstruction is uncommon in childhood and adolescence, and is usually iatrogenic. The predominant primary cause of SVCS in these age groups are mediastinal tumors, the most common offender being the lymphoproliferative neoplasms.‘6
Of the minority of cases of SVCS with a benign etiology, about 75% are secondary to mediastinal granulomatous disease, and the remainder are caused by such disorders as retro- sternal goiter and aortic aneurysms (Fig 5).”
DIAGNOSIS
In recent years there has been controversy over the diagnosis and management of SVC obstruc- tion. Selection of an appropriate diagnostic pro- cedure should be based on whether the following critical information is required: (1) definition of the site and extent of obstruction; (2) routes of collateral circulation; and (3) acquisition of tis- sue for a histopathologic diagnosis.
Plain chest radiographs are of limited diagnos- tic value. Mediastinal widening is reported to be the most common abnormality on the chest radiograph in SVC obstruction.” Other abnor- malities that may be seen include pleural effu- sion, right hilar mass, bilateral diffuse infiltrates, cardiomegaly, RUL collapse, and anterior
87
mediastinal mass. SVC obstruction may also result in rib notching. It is important to remem- ber that a normal chest radiograph is not incon- sistent with the diagnosis of SVC obstruc- tion.‘0*‘8
Esophagography may demonstrate filling defects compatible with esophageal varices. Classically, the varices are “downhill,” repre- senting collateral circulation through enlarged upper esophageal veins, bypassing the obstructed SVC to reach the IVC.
SVC phlebography has been the standard pro- cedure for the diagnosis of SVC obstruction and provides useful information. The route and extent of collateral circulation is well demon- strated, and. may be of prognostic importance in predicting clinical response. Opacification of the innominate veins by phlebography is useful for planning a venous bypass and for designing radiation portals. Collateral vessels are clearly demonstrated with contrast-enhanced CT, and
can better demonstrate the location and extent of both tumor and thrombus, thus offering more information to the radiotherapist.
A recent review has found SVC venography to be of limited value compared to CT.” The veno- gram is seldom needed since it offers no informa- tion about histology and the diagnosis is often clinically apparent. Furthermore, elevated ve- nous pressure in the arms may lead to difficulty
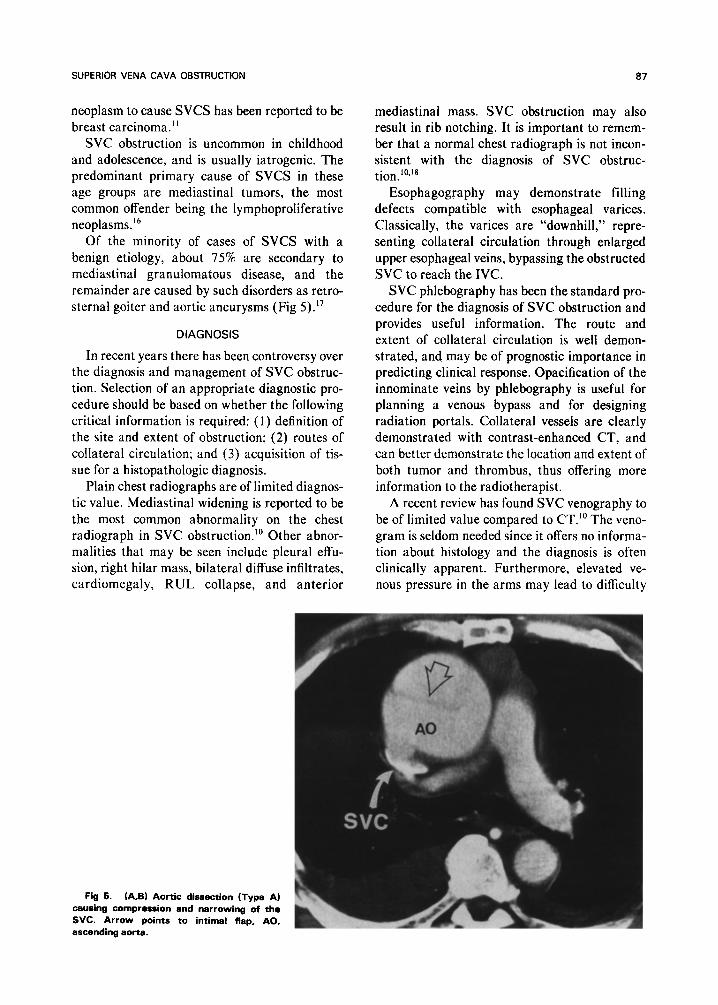
Fig 5. (A,B) Aortic dissection (Type A) causing compression and narrowing of the SVC. Arrow points to intimal flap, AO,
ascending aorta.

YEDLICKA ET AL
Fig 6. Metastatic bronchogenic carcinoma. Contrast-enhanced CT demonstrates a filling defect within the SVC. representing bland throm- bus. l , mediestinal lymphadenopathy.
in controlling bleeding at the puncture site. sels.18 However, the resolution of scintigraphy is Because of the ancillary benefits of the CT scan, lower than venography, and it also fails to dem- a previously performed venogram should not onstrate the pathologic anatomy of the obstruc- obviate the need for CT. tion.
Diagnosis of SVC obstruction may also be The diagnosis of SVC obstruction by contrast- suggested by scintigraphy, which also demon- enhanced CT requires that at least two criteria strates obstruction of flow and collateral ves- be met. First, there must be diminished or absent
Fig 7. Contrast-enhanced CT demonstrating the route and extent of collateral path- ways (arrows) in a patient with SVC obstruction.

SUPERIOR VENA CAVA OBSTFlUCTION 89
opacification of central venous structures such as the innominate vein or SVC inferior to the site of obstruction. Second, collateral venous routes must be opacified. The fulfillment of either crite- ria alone is not sufficient for an accurate CT diagnosis of venous obstruction. It is well known that dilution of the contrast medium by unopa-
cified blood and its displacement by laminar flow may simulate an intraluminal filling defect. The absence of opacification of collaterals helps to make the distinction.2q’9 Conversely, one may see opacification of collateral veins in the absence of mediastinal obstruction, ie, with normal opacifi- cation of the SVC and innominate veins.* Thus
Fig 8. Bronchogonic carcinoma. (Al Narrowing and stncwmmt of both the superior vena cave (SW.) and right main bronchus IBI by a hrge right upper lobe mnu with msdlsstlnal extension. (B) CT dig&al @k&qpwn conlirms tha prasanca of a tapsrsd narrw of tha ancasad BVC larrows). Ao, aorta; C. collatual vales. /Aaprm with garmisslon from Moncada R at al and tha Amarican Roantgan Ray SOCI-
atY.=)

90
the diagnosis of SVC obstruction requires the presence of intraluminal filling defects (Fig 6) or extrinsic compression or encasement of major thoracic venous channels, combined with collat- eral vessel opacification (Fig 7).
The diagnosis of SVCS can be reliably made by chest CT, which provides detailed anatomic information of the entire mediastinum and is less invasive than other methods, especially bron- choscopy and mediastinoscopy. It may provide the information needed to plan a safe route for percutaneous fine needle biopsy and to direct bronchoscopy toward the area of interest for specimen retrieval. CT is useful in planning radiation portals and is the procedure of choice for follow-up after treatment. It may also be employed to evaluate the patency of a venous bypass.
The recent addition of MRI to the diagnostic armamentarium provides a potential alternative modality in selected cases. The ability of MRI to demonstrate vascular structures without the use
YEDLICKA ET AL
of intravenous contrast medium makes it an attractive alternative. However, unstable pa- tients may not be able to cooperate with this somewhat lengthy examination. Recent ad- vances in cardiac and respiratory gating as well as continued advances in fast scanning may make this the procedure of choice for the future, but at present more experience is needed before adopting this modality.
CT digital phlebography has been reported as a valuable adjunct to axial CT scanning in SVC obstruction (Fig 8).*’ It provides an AP bidimen- sional image of the thoracic veins as well as transverse axial images. Venography can usually be avoided when this combination technique is employed. The CT digital phlebogram can also reveal patency of a venous bypass of a SVC obstruction. We believe that the combination of CT digital phlebography and axial CT scanning is currently the most efficient, informative, and cost-effective technique available for the diag- nosis and management of SVC obstruction.
REFERENCES
1. Hunter W: The history of an aneurysm of the aorta with some remarks on aneurysms in general. Med Obstet Sot Phys
(Lond) 1757;1:323 2. Engel IA, Auh YH, Rubenstein WA, et al: CT diag-
nosis of mediastinal and thoracic inlet obstruction. AJR 1983;141:521-6
3. Ishikawa T, Clark RA, Tokuda M, et al: Focal enhancement on hepatic CT in superior vena caval and brachiocephalic vein obstruction. AJR 1983;140:337-8
4. Gore JM, Matsumoto AH, Layden JJ, et al: Superior vena cava syndrome: Its association with indwelling balloon- tipped pulmonary artery catheters. Arch Intern Med 1981;144:506-8
5. Bertrand M, Presant CA, Klein L, et al: Iatrogenic superior vena cava syndrome. Cancer 1984;54:376-8
6. Yakirevich V, Alagem D, Papo J, et al: Fibrotic stenosis of the superior vena cava with widespread thrombotic occlu- sion of its major tributaries: An unusual complication of transvenous cardiac pacing. J Thorac Cardiovasc Surg
1983;85:632-4 7. Katz PO, Hackshaw RT, Barish CF, et al: Venous
thromobosis as a cause of superior vena cava syndrome. Arch Intern Med 1983;143:1050-2
8. McIntire RT, Sykes EM Jr: Obstruction of the superior vena cava: A review of the literature and report of two personal cases. Ann Intern Med 1949;30:925-60
9. Banker VP, Maddison FE: Superior vena cava syn- drome secondary to aortic disease: Report of two cases and review of the literature. Dis Chest 1967;51:656-62
10. Parish JM, Marschke RF, Dines DE, et al: Etiologic considerations in superior vena cava syndrome. Mayo C/in Proc 198 1;56:407- 13
11. Lopez MJ, Sala JM: Malignant superior vena cava syndrome. MO Med 1982;79:8 10-5
12. Effler DB, Groves LK: Superior vena caval obstruc- tion. J Thorac Cardiovasc Surg 1962;43:574-84
13. Lochridge SK, Knibbe WP, Doty DB: Obstruction of the superior vena cava. Surgery 1979;85:14-24
14. Ooizumi K, Togashi H, Watanabe A, et al: Lung cancer abstracted (Haigah) (Suppl) 1977
15. Shimm DB, Logue CL, Rigsby LC: Evaluating the superior vena cava syndrome. JAMA 198 1;245:95 l-3
16. Janin Y, Becker J, Wise L, et al: Superior vena cava syndrome in childhood and adolescence: A review of the literature and report of three cases. J Pediatr Surg
1982;17:290-5 17. Mahajan V, Strimlan V, Van Ordstrand HS, et al:
Benign superior vena cava syndrome. Chest 1975;68:32-5 18. Bechtold RE, Solfman NT, Karstaedt N, et al:
Superior vena cava obstruction: Detection using CT. Radiol-
ogy 1985;157:485-7 19. Godwin JD, Webb WR: Contrast related flow phe-
nomena mimicking pathology on thoracic computed tomog- raphy. J Comput Assist Tomogr 1981;6:460-4
20. Moncada R, Cardella R, Demos TC, et al: Evaluation of superior vena cava syndrome by axial CT and CT phle- bography. AJR 1984;143:731-6