Crystal Run Health Plan, LLC
56
Crystal Run Health Plan, LLC 2017 Individual Off Exchange Plans Rating Manual 2017 Premium Rates
Transcript of Crystal Run Health Plan, LLC

Crystal Run Health Plan, LLC
2017 Individual Off Exchange Plans Rating Manual
2017 Premium Rates

Crystal Run Health Plan, LLC2017 Individual Off Exchange Plans Rating Manual
Table of Contents Page
2017 Form Numbers for Region 3 1
2017 Premium Rates for Region 3 2
Composition of Rating Regions 3
Benefit Designs 4-19
Description of Revised Rating Classes, Factors, and Discounts 20 Examples of Rate Calculations 21 Commission Schedules 22 Census Tiers and Factors 23 Adjustment Factors for Major Variations 24 Expected Loss Ratios 25
Underwriting Guidelines 26
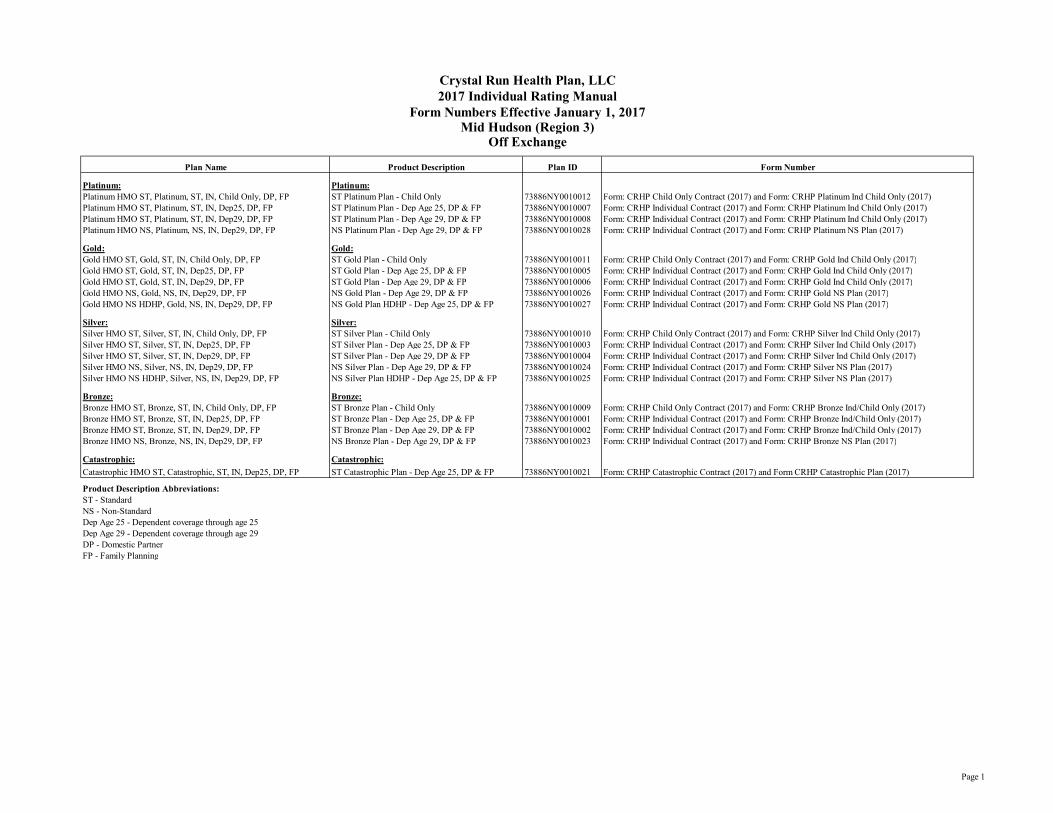
Plan Name Product Description Plan ID Form Number
Platinum: Platinum:Platinum HMO ST, Platinum, ST, IN, Child Only, DP, FP ST Platinum Plan - Child Only 73886NY0010012 Form: CRHP Child Only Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO ST, Platinum, ST, IN, Dep25, DP, FP ST Platinum Plan - Dep Age 25, DP & FP 73886NY0010007 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO ST, Platinum, ST, IN, Dep29, DP, FP ST Platinum Plan - Dep Age 29, DP & FP 73886NY0010008 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO NS, Platinum, NS, IN, Dep29, DP, FP NS Platinum Plan - Dep Age 29, DP & FP 73886NY0010028 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum NS Plan (2017)
Gold: Gold:Gold HMO ST, Gold, ST, IN, Child Only, DP, FP ST Gold Plan - Child Only 73886NY0010011 Form: CRHP Child Only Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO ST, Gold, ST, IN, Dep25, DP, FP ST Gold Plan - Dep Age 25, DP & FP 73886NY0010005 Form: CRHP Individual Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO ST, Gold, ST, IN, Dep29, DP, FP ST Gold Plan - Dep Age 29, DP & FP 73886NY0010006 Form: CRHP Individual Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO NS, Gold, NS, IN, Dep29, DP, FP NS Gold Plan - Dep Age 29, DP & FP 73886NY0010026 Form: CRHP Individual Contract (2017) and Form: CRHP Gold NS Plan (2017)Gold HMO NS HDHP, Gold, NS, IN, Dep29, DP, FP NS Gold Plan HDHP - Dep Age 25, DP & FP 73886NY0010027 Form: CRHP Individual Contract (2017) and Form: CRHP Gold NS Plan (2017)
Silver: Silver:Silver HMO ST, Silver, ST, IN, Child Only, DP, FP ST Silver Plan - Child Only 73886NY0010010 Form: CRHP Child Only Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO ST, Silver, ST, IN, Dep25, DP, FP ST Silver Plan - Dep Age 25, DP & FP 73886NY0010003 Form: CRHP Individual Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO ST, Silver, ST, IN, Dep29, DP, FP ST Silver Plan - Dep Age 29, DP & FP 73886NY0010004 Form: CRHP Individual Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO NS, Silver, NS, IN, Dep29, DP, FP NS Silver Plan - Dep Age 29, DP & FP 73886NY0010024 Form: CRHP Individual Contract (2017) and Form: CRHP Silver NS Plan (2017)Silver HMO NS HDHP, Silver, NS, IN, Dep29, DP, FP NS Silver Plan HDHP - Dep Age 25, DP & FP 73886NY0010025 Form: CRHP Individual Contract (2017) and Form: CRHP Silver NS Plan (2017)
Bronze: Bronze:Bronze HMO ST, Bronze, ST, IN, Child Only, DP, FP ST Bronze Plan - Child Only 73886NY0010009 Form: CRHP Child Only Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO ST, Bronze, ST, IN, Dep25, DP, FP ST Bronze Plan - Dep Age 25, DP & FP 73886NY0010001 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO ST, Bronze, ST, IN, Dep29, DP, FP ST Bronze Plan - Dep Age 29, DP & FP 73886NY0010002 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO NS, Bronze, NS, IN, Dep29, DP, FP NS Bronze Plan - Dep Age 29, DP & FP 73886NY0010023 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze NS Plan (2017)
Catastrophic: Catastrophic:Catastrophic HMO ST, Catastrophic, ST, IN, Dep25, DP, FP ST Catastrophic Plan - Dep Age 25, DP & FP 73886NY0010021 Form: CRHP Catastrophic Contract (2017) and Form CRHP Catastrophic Plan (2017)
Product Description Abbreviations:ST - StandardNS - Non-StandardDep Age 25 - Dependent coverage through age 25Dep Age 29 - Dependent coverage through age 29DP - Domestic PartnerFP - Family Planning
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Form Numbers Effective January 1, 2017Mid Hudson (Region 3)
Off Exchange
Page 1

Premium Per Contract
Plan Name Product Description Plan ID SingleSingle + Spouse
Single + Child(ren)
Single + Spouse +
Child(ren)
One Child Only
Two Children
Only*
Three or More
Children Only**
Platinum: Platinum:Platinum HMO ST, Platinum, ST, IN, Child Only, DP, FP ST Platinum Plan - Child Only 73886NY0010012 $331.18 $662.36 $993.54Platinum HMO ST, Platinum, ST, IN, Dep25, DP, FP ST Platinum Plan - Dep Age 25, DP & FP 73886NY0010007 $803.85 $1,607.69 $1,366.54 $2,290.96Platinum HMO ST, Platinum, ST, IN, Dep29, DP, FP ST Platinum Plan - Dep Age 29, DP & FP 73886NY0010008 $803.85 $1,607.69 $1,366.54 $2,290.96Platinum HMO NS, Platinum, NS, IN, Dep29, DP, FP NS Platinum Plan - Dep Age 29, DP & FP 73886NY0010028 $784.54 $1,569.08 $1,333.72 $2,235.94
Gold: Gold:Gold HMO ST, Gold, ST, IN, Child Only, DP, FP ST Gold Plan - Child Only 73886NY0010011 $290.86 $581.72 $872.58Gold HMO ST, Gold, ST, IN, Dep25, DP, FP ST Gold Plan - Dep Age 25, DP & FP 73886NY0010005 $705.96 $1,411.92 $1,200.13 $2,011.98Gold HMO ST, Gold, ST, IN, Dep29, DP, FP ST Gold Plan - Dep Age 29, DP & FP 73886NY0010006 $705.96 $1,411.92 $1,200.13 $2,011.98Gold HMO NS, Gold, NS, IN, Dep29, DP, FP NS Gold Plan - Dep Age 29, DP & FP 73886NY0010026 $686.92 $1,373.84 $1,167.76 $1,957.72Gold HMO NS HDHP, Gold, NS, IN, Dep29, DP, FP NS Gold Plan HDHP - Dep Age 25, DP & FP 73886NY0010027 $660.82 $1,321.64 $1,123.39 $1,883.33
Silver: Silver:Silver HMO ST, Silver, ST, IN, Child Only, DP, FP ST Silver Plan - Child Only 73886NY0010010 $254.32 $508.64 $762.96Silver HMO ST, Silver, ST, IN, Dep25, DP, FP ST Silver Plan - Dep Age 25, DP & FP 73886NY0010003 $617.29 $1,234.57 $1,049.39 $1,759.26Silver HMO ST, Silver, ST, IN, Dep29, DP, FP ST Silver Plan - Dep Age 29, DP & FP 73886NY0010004 $617.29 $1,234.57 $1,049.39 $1,759.26Silver HMO NS, Silver, NS, IN, Dep29, DP, FP NS Silver Plan - Dep Age 29, DP & FP 73886NY0010024 $563.44 $1,126.89 $957.85 $1,605.81Silver HMO NS HDHP, Silver, NS, IN, Dep29, DP, FP NS Silver Plan HDHP - Dep Age 25, DP & FP 73886NY0010025 $575.54 $1,151.07 $978.41 $1,640.28
Bronze: Bronze:Bronze HMO ST, Bronze, ST, IN, Child Only, DP, FP ST Bronze Plan - Child Only 73886NY0010009 $206.37 $412.74 $619.11Bronze HMO ST, Bronze, ST, IN, Dep25, DP, FP ST Bronze Plan - Dep Age 25, DP & FP 73886NY0010001 $500.90 $1,001.79 $851.52 $1,427.56Bronze HMO ST, Bronze, ST, IN, Dep29, DP, FP ST Bronze Plan - Dep Age 29, DP & FP 73886NY0010002 $500.90 $1,001.79 $851.52 $1,427.56Bronze HMO NS, Bronze, NS, IN, Dep29, DP, FP NS Bronze Plan - Dep Age 29, DP & FP 73886NY0010023 $496.41 $992.83 $843.90 $1,414.78
Catastrophic: Catastrophic:Catastrophic HMO ST, Catastrophic, ST, IN, Dep25, DP, FP ST Catastrophic Plan - Dep Age 25, DP & FP 73886NY0010021 $240.19 $480.39 $408.33 $684.55
Product Description Abbreviations:ST - StandardNS - Non-StandardDep Age 25 - Dependent coverage through age 25Dep Age 29 - Dependent coverage through age 29DP - Domestic PartnerFP - Family Planning
*For a child only plan that covers two children in a family**For a child only plan that covers three or more children in a family
Mid Hudson (Region 3)Off Exchange
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Premium Rates Effective January 1, 2017
Page 2

Crystal Run Health Plan, LLC2017 Individual Rating ManualComposition of Rating Regions
Region 3 (Mid-Hudson)OrangeSullivan
Off Exchange
Page 3

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)BENEFIT Core Network Only Core Network OnlyFINANCIAL / DEDUCTIBLESDeductible (Single/Family) $0/$0 $600/$1200Max Out of Pocket (Single/Family) $2,000/$4,000 $4,000/$8,000HSA Qualified NA NADeductible Structure Embedded EmbeddedDeductible Applies to: NA All except RxPREVENTIVE CARE
Adult & Women's (USPSTF & HRSA required) See Section N SG 42 Implemention Guide Covered in Full Covered in Full
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implemenation Guide Covered in Full Covered in Full
Preventive Dental for Children (Up to age 19) Not Covered Not CoveredPediatric Vision Exam (Up to age 19; 1 per 12 month period) $15 copay $25 copay*Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period) 10% coinsurance 20% coinsurance*
OFFICE VISITS
PCP (includes any PCP allergy diag/treatment) $15 copay $25 copay*
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies) $35 copay $40 copay*
Lab Performed as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copayRadiology/Ultrasound as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copaySurgery Performed as Part of PCP/SCP Office Visit Covered by Office Visit copay Covered by Office Visit copayMedications Administered in PCP/SCP Office (preauth infusion) Covered by Office Visit copay Covered by Office Visit copay
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim)Lab - Outpatient Hospital Setting $35 copay $40 copay*Lab - Outpatient Hospital Setting, preadmission testing $0 copay $0 copay*Lab - Independent Laboratory $35 copay $40 copay*Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
$15 copay $25 copay*
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, sleep studies ) $35 copay $40 copay*
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting $35 copay $40 copay*X-ray/Ultrasound – Freestanding Facility $35 copay $40 copay*
Page 4

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital Setting $35 copay $40 copay*MRI, CT, Nuclear Medicine & PET – Freestanding Facility $35 copay $40 copay*
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility) $100 copay $100 copay*Outpatient Surgery – Freestanding Facility (facility) $100 copay $100 copay*Outpatient Surgery - Surgeon’s Services $100 copay $100 copay*
INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity) $500/admission $1,000/admission*Surgeon's Services Inpatient $100 copay $100 copay*Maternity Delivery (physician or midwife) $100 copay $100 copay*Anesthesiologist/Radiologist/Pathologist Covered in Full Covered in FullAll Other Physician Services/Visits $0 Copay $0 Copay*Inpatient Medical Visits $0 Copay $0 Copay*Observation Stays $100 copay $150 copay*Transplants (must be performed at desiginated facilities) $500/admission $1,000/admission*End of Life Care (In-network and OON) $500/admission $1,000/admission*Autologous Blood Banking 10% coinsurance 20% coinsurance*
EMERGENCY CAREEmergency Room Care (World Wide) (No physician copay) $100 copay $150 copay*Ambulance (Non-Emergency ambulance requires preauthorization) $100 copay $150 copay*Hospital ER for follow-up, routine or urgent care Not Covered Not CoveredUrgent Care Center (Covered outside Service Area in-network and OON . Not covered OON within Service Area.) Facility only. $55 copay $60 copay*
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregancy preauth ) Covered in Full Covered in Full*
Inpatient Hospital Charges for Mother and Child (other than preventive care) $500/admission $1,000/admission*
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions. Appropriate Cost Share Appropriate Cost Share
Page 5

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)SKILLED NURSING FACILITY200 days per Plan Year (Base plan) $500/admission $1,000/admission*
HOSPICE CAREInpatient Hospice Care $500/admission $1,000/admission*Home Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement. $15 copay $25 copay*
HOME HEALTH CAREHome Care Visits (40 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
$15 copay $25 copay*
Physician House Calls (where available) PCP/SCP OV cost share PCP/SCP OV cost share
MENTAL HEALTH &SUBSTANCE USE DISORDERSInpatient Mental Health (limited to facilities defined in NY Law 1.03 (10)) $500/admission $1,000/admission*Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services) $15 copay $25 copay*
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
$500/admission $1,000/admission*
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities) $500/admission $1,000/admission*
Outpatient Substance Use Services (OASAS-certifed or waivered SCP's under the Drug Addiction Treatment Act of 2000. Up to 20 visits per calendar year may be used for family counseling.)
$15 copay $25 copay*
MICELLANEOUS
Allergy Testing and Treatment (preauth IVIG only) PCP/SCP OV cost share PCP/SCP OV cost share
Podiatric Procedures $35 copay $40 copay*Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year. $35 copay $40 copay*
After full or partial mastectomy,breast reconstruction including implants. Appropriate Cost Share Appropriate Cost Share
Chiropractic Care - Unlimited Visits $35 copay $40 copay*Clinical Trials Appropriate Cost Share Appropriate Cost ShareSecond Opinions Cancer, Surgery, Required and Other $35 copay $40 copay*Referrals to Non-Network Providers Appropriate Cost Share Appropriate Cost Share
Page 6

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)SHORT TERM REHAB & HABILITATIVE SERVICES
Inpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime. $500/admission $1,000/admission*
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT. $25 copay $30 copay*
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment 10% coinsurance 20% coinsurance*Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.) 10% coinsurance 20% coinsurance*
MEDICAL SUPPLIESMedical Supplies When Medically Necessary 10% coinsurance 20% coinsurance*
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered. 10% coinsurance 20% coinsurance*
AUTISM SPECTRUM DISORDER (ASD)
Applied Behavior Analysis treatment for ASD under 11 NYCRR 440 $15 copay $25 copay*
Assistive Communication Devices for ASD $15 copay $25 copay*
DIABETIC SERVICES
Insulin and Oral Medication - 30/90 day supply $15 copay per 30 day supply $25 copay per 30 day supply*
Diabetic Supplies (needles and syringes) and Equipment - 30/90 day supply $15 copay per 30 day supply $25 copay per 30 day supply*Diabetic Education $15 copay $25 copay*
EXERCISE FACILITY
Subscriber (Reimbursement upon completion of 50 visits in six-month period.) $200 per 6 month period $200 per 6 month period
Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP. $100 per 6 month period $100 per 6 month period
Prescription Drug Deductible (If applicable) Not subject to deductible Not subject to deductiblePharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays) $10/$30/$60 $10/$35/$70Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays) 2.5 times Rx copay 2.5 times Rx copay
*Cost shares listed with an asterisk indicate subject to deductible.
Page 7

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMEBENEFITFINANCIAL / DEDUCTIBLESDeductible (Single/Family)Max Out of Pocket (Single/Family)HSA QualifiedDeductible StructureDeductible Applies to:PREVENTIVE CARE
Adult & Women's (USPSTF & HRSA required) See Section N SG 42 Implemention Guide
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implemenation GuidePreventive Dental for Children (Up to age 19)Pediatric Vision Exam (Up to age 19; 1 per 12 month period)Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period)
OFFICE VISITS
PCP (includes any PCP allergy diag/treatment)
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies)
Lab Performed as Part of Office VisitRadiology/Ultrasound as Part of Office VisitSurgery Performed as Part of PCP/SCP Office VisitMedications Administered in PCP/SCP Office (preauth infusion)
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim)Lab - Outpatient Hospital SettingLab - Outpatient Hospital Setting, preadmission testingLab - Independent LaboratoryOutpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, sleep studies )
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting X-ray/Ultrasound – Freestanding Facility
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)Core Network Only Core Network Only Core Network Only
$2,000/$4,000 $4,000/$8,000 $7,150/$14,300$6,750/$13,500 $7,150/$14,300 $7,150/$14,300
NA NA NAEmbedded Embedded Embedded
All except Rx All All
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
Not Covered Not Covered Not Covered$30 copay* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance* (3 PCP Visits w/o deductible with cost-share)
$50 copay* 50% coinsurance* 0% coinsurance*
Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*$0 copay* 50% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*$50 copay* 50% coinsurance* 0% coinsurance*
Page 8

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMEMRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital SettingMRI, CT, Nuclear Medicine & PET – Freestanding Facility
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility)Outpatient Surgery – Freestanding Facility (facility)Outpatient Surgery - Surgeon’s Services
INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity)Surgeon's Services InpatientMaternity Delivery (physician or midwife)Anesthesiologist/Radiologist/PathologistAll Other Physician Services/VisitsInpatient Medical VisitsObservation StaysTransplants (must be performed at desiginated facilities)End of Life Care (In-network and OON)Autologous Blood Banking
EMERGENCY CAREEmergency Room Care (World Wide) (No physician copay)Ambulance (Non-Emergency ambulance requires preauthorization)Hospital ER for follow-up, routine or urgent careUrgent Care Center (Covered outside Service Area in-network and OON . Not covered OON within Service Area.) Facility only.
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregancy preauth )
Inpatient Hospital Charges for Mother and Child (other than preventive care)
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions.
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$50 copay* 50% coinsurance* 0% coinsurance*$50 copay* 50% coinsurance* 0% coinsurance*
$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*
Covered in Full 50% coinsurance* 0% coinsurance*$0 Copay* 50% coinsurance* 0% coinsurance*$0 Copay* 50% coinsurance* 0% coinsurance*
$250 copay* 50% coinsurance* 0% coinsurance*$1,500/admission* 50% coinsurance* 0% coinsurance*$1,500/admission* 50% coinsurance* 0% coinsurance*30% coinsurance* 50% coinsurance* 0% coinsurance*
$250 copay* 50% coinsurance* 0% coinsurance*$150 copay* 50% coinsurance* 0% coinsurance*Not Covered Not Covered Not Covered
$70 copay* 50% coinsurance* 0% coinsurance*
Covered in Full* Covered in Full Covered in Full
$1,500/admission* 50% coinsurance* 0% coinsurance*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
Page 9

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMESKILLED NURSING FACILITY200 days per Plan Year (Base plan)
HOSPICE CAREInpatient Hospice CareHome Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement.
HOME HEALTH CAREHome Care Visits (40 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.Physician House Calls (where available)
MENTAL HEALTH &SUBSTANCE USE DISORDERSInpatient Mental Health (limited to facilities defined in NY Law 1.03 (10))Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services)
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities)
Outpatient Substance Use Services (OASAS-certifed or waivered SCP's under the Drug Addiction Treatment Act of 2000. Up to 20 visits per calendar year may be used for family counseling.)
MICELLANEOUS
Allergy Testing and Treatment (preauth IVIG only)
Podiatric ProceduresInterruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year.
After full or partial mastectomy,breast reconstruction including implants.
Chiropractic Care - Unlimited VisitsClinical TrialsSecond Opinions Cancer, Surgery, Required and OtherReferrals to Non-Network Providers
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$1,500/admission* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
PCP/SCP OV cost share 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
PCP/SCP OV cost share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
Appropriate Cost Share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*Appropriate Cost Share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*Appropriate Cost Share 50% coinsurance* 0% coinsurance*
Page 10

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMESHORT TERM REHAB & HABILITATIVE SERVICES
Inpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime.
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT.
DURABLE MEDICAL EQUIPMENTDurable Medical EquipmentProsthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.)
MEDICAL SUPPLIESMedical Supplies When Medically Necessary
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered.
AUTISM SPECTRUM DISORDER (ASD)
Applied Behavior Analysis treatment for ASD under 11 NYCRR 440
Assistive Communication Devices for ASD
DIABETIC SERVICES
Insulin and Oral Medication - 30/90 day supply
Diabetic Supplies (needles and syringes) and Equipment - 30/90 day supplyDiabetic Education
EXERCISE FACILITY
Subscriber (Reimbursement upon completion of 50 visits in six-month period.)
Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP.
Prescription Drug Deductible (If applicable)Pharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays)Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays)
*Cost shares listed with an asterisk indicate subject to deductible.
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay per 30 day supply* 50% coinsurance* 0% coinsurance*
$30 copay per 30 day supply* 50% coinsurance* 0% coinsurance*$30 copay* 50% coinsurance* 0% coinsurance*
$200 per 6 month period $200 per 6 month period $200 per 6 month period
$100 per 6 month period $100 per 6 month period $100 per 6 month period
Not subject to deductible Integrated with Medical Integrated with Medical$10/$35/$70 $10*/$35*/$70* 0% coinsurance*
2.5 times Rx copay 2.5 times Rx copay 0% coinsurance
Page 11

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)BENEFIT Core Network Only Core Network Only Core Network OnlyFINANCIAL / DEDUCTIBLESDeductible (Single/Family) $0/$0 $0/$0 $1,500/$3,000Max Out of Pocket (Single/Family) $2,100/$4,200 $4,400/$8,800 $6,550/$13,100HSA Qualified NA NA YesDeductible Structure Embedded Embedded AggregateDeductible Applies to: NA NA All Except Preventive RxPREVENTIVE CAREAdult & Women's (USPSTF & HRSA required) See Section N SG 42 Implementation Guide Covered in Full Covered in Full Covered in Full
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implementation Guide Covered in Full Covered in Full Covered in Full
Preventive Dental for Children (Up to age 19) Not Covered Not Covered Not CoveredPediatric Vision Exam (Up to age 19; 1 per 12 month period) $50 copay $50 copay $25 copay*Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period) 50% coinsurance 50% coinsurance 50% coinsurance*
OFFICE VISITSPCP (includes any PCP allergy diag/treatment) $0 copay $0 copay $0 copay*
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies) $50 copay $50 copay $25 copay*
Lab Performed as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Radiology/Ultrasound as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Surgery Performed as Part of PCP/SCP Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Medications Administered in PCP/SCP Office (preauth infusion) Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim.)Lab - Outpatient Hospital Setting, including preadmission tests $50 copay $50 copay $25 copay*Lab - Independent Laboratory $0 copay $0 copay $0 copay*
Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
$50 copay $50 copay $25 copay*
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, neuro psych testing , sleep studies ) $50 copay $50 copay $25 copay*
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting $50 copay $75 copay $75 copay*X-ray/Ultrasound – Freestanding Facility $25 copay $50 copay $50 copay*
MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital Setting $200 copay $200 copay $200 copay*MRI, CT, Nuclear Medicine & PET – Freestanding Facility $150 copay $150 copay $150 copay*
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility) 20% coinsurance 50% coinsurance 20% coinsuranceOutpatient Surgery – Freestanding Facility (facility) 20% coinsurance 50% coinsurance 20% coinsuranceOutpatient Surgery - Surgeon's/Physician's Services (Same incision highest amount; different incision highest plus 50% others) Covered in Full 30% coinsurance Covered In Full*
Outpatient Surgery - Anesthesiologist/Radiologist/Pathologist Covered in Full 30% coinsurance Covered In Full*
Page 12

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity) 20% coinsurance 50% coinsurance $500 copay*Surgeon's Services Inpatient $100 copay $100 copay $100 copay*Maternity Delivery (physician or midwife) $100 copay $100 copay $100 copay*Anesthesiologist/Radiologist/Pathologist 20% coinsurance 50% coinsurance Covered in Full*All Other Physician Services/Visits 20% coinsurance 50% coinsurance Covered in Full*Inpatient Medical Visits 20% coinsurance 50% coinsurance Covered in Full*Observation Stays 20% coinsurance 50% coinsurance $500 copay*Transplants (must be performed at designated facilities) 20% coinsurance 50% coinsurance $500 copay*End of Life Care (In-network and OON) See COC. 20% coinsurance 50% coinsurance $500 copay*Autologous Blood Banking 20% coinsurance 50% coinsurance $25 copay*
EMERGENCY CARE AND URGENT CARE
Hospital Emergency Room for Emergency Condition - Professional & Facility (U.S., Canada, Mexico) (Covered as Inpatient Hospital Charges if admitted) 20% coinsurance 50% coinsurance $200 copay*
Ambulance (Non-Emergency ambulance requires preauthorization) 20% coinsurance 50% coinsurance $100 copay*
Hospital ER for follow-up, routine or urgent care Not Covered Not Covered Not Covered
Urgent Care (Covered OON out-of-area. Not covered OON within Service Area.) $0 copay $0 copay $0 copay*
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregnancy preauth ) Covered in Full Covered in Full Covered in Full
Elective Sterilizations Covered in Full Covered in Full Covered in Full
Inpatient Hospital Charges for Mother and Child (other than preventive care) 20% coinsurance 50% coinsurance $500 copay*
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions. Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
SKILLED NURSING FACILITY365 days per Plan Year (Base plan) 20% coinsurance 50% coinsurance $500 copay*
HOSPICE CAREInpatient Hospice Care 20% coinsurance 50% coinsurance $500 copay*Home Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement. $50 copay $50 copay $25 copay*
HOME HEALTH CARE
Home Care Visits (60 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
$50 copay $50 copay $25 copay*
Physician House Calls (where available) PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share
MENTAL HEALTH & SUBSTANCE USE DISORDERS (Non-emergency coverage limited to Beacon providers)Inpatient Mental Health (limited to facilities defined in NY Law 1.03 (10)) 20% coinsurance 50% coinsurance $500 copay*
Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services) $50 copay $50 copay $25 copay*
Page 13

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
20% coinsurance 50% coinsurance $500 copay*
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities) 20% coinsurance 50% coinsurance $500 copay*
Outpatient Substance Use Services (OASAS-certified or waivered SCP's under the Drug Addiction Treatment Act of 2000.) Up to 20 visits per calendar year for family counseling provided family member is a covered person under member's family COC. Allowed Amount same irrespective of number of family members attending session.)
$50 copay $50 copay $25 copay*
MISCELLANEOUSAllergy Testing and Treatment PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost sharePodiatric Procedures $50 copay $50 copay $25 copay*
Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year. $50 copay $50 copay $25 copay*
After full or partial mastectomy, breast reconstruction including implants (preauth required to the extent inpt or outpt surg req'd) Appropriate Cost Share Appropriate Cost Share Appropriate Cost ShareChiropractic Care - Unlimited Visits $50 copay $50 copay $25 copay*Clinical Trials Appropriate Cost Share Appropriate Cost Share Appropriate Cost ShareSecond Opinions Cancer, Surgery, Required and Other $50 copay $50 copay $25 copay*Referrals to Non-Network Providers Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
SHORT TERM REHAB & HABILITATIVE SERVICESInpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime. 20% coinsurance 50% coinsurance $500 copay*
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT. $50 copay $50 copay $25 copay*
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment (greater than or equal to $500) 20% coinsurance 50% coinsurance $500 copay*Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.) 20% coinsurance 50% coinsurance $500 copay*
MEDICAL SUPPLIESMedical Supplies When Medically Necessary 20% coinsurance 50% coinsurance 50% coinsurance*
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered. 20% coinsurance 50% coinsurance 50% coinsurance*
AUTISM SPECTRUM DISORDER (ASD)Applied Behavior Analysis treatment for ASD under 11 NYCRR 440 $50 copay $50 copay $25 copay*Assistive Communication Devices for ASD $50 copay $50 copay $25 copay*
DIABETIC SERVICESInsulin and Oral Medication - 30/90 day supply See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingDiabetic Supplies (needles and syringes) and Equipment - 30/90 day supply See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingDiabetic Education $50 copay $50 copay $25 copay*
Page 14

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)EXERCISE FACILITYSubscriber (Reimbursement upon completion of 50 visits in six-month period.) $200 per 6 month period $200 per 6 month period $200 per 6 month periodSpouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP. $100 per 6 month period $100 per 6 month period $100 per 6 month period
PHARMACYPrescription Drug Deductible (If applicable) Not subject to deductible Not subject to deductible Integrated with MedicalPharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays) $10/$50/$80 $10/$50/$80 $0*/$30*/$60*Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays) 2.5 times Rx copay 2.5 times Rx copay 2.5 times Rx copay
*Cost shares listed with an asterisk indicate subject to deductible.
Page 15

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMEBENEFITFINANCIAL / DEDUCTIBLESDeductible (Single/Family)Max Out of Pocket (Single/Family)HSA QualifiedDeductible StructureDeductible Applies to:PREVENTIVE CAREAdult & Women's (USPSTF & HRSA required) See Section N SG 42 Implementation GuideInfant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implementation GuidePreventive Dental for Children (Up to age 19)Pediatric Vision Exam (Up to age 19; 1 per 12 month period)Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period)
OFFICE VISITSPCP (includes any PCP allergy diag/treatment)
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies)
Lab Performed as Part of Office VisitRadiology/Ultrasound as Part of Office VisitSurgery Performed as Part of PCP/SCP Office VisitMedications Administered in PCP/SCP Office (preauth infusion)
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim.)Lab - Outpatient Hospital Setting, including preadmission testsLab - Independent Laboratory
Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, neuro psych testing , sleep studies )
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting X-ray/Ultrasound – Freestanding Facility
MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital SettingMRI, CT, Nuclear Medicine & PET – Freestanding Facility
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility)Outpatient Surgery – Freestanding Facility (facility)Outpatient Surgery - Surgeon's/Physician's Services (Same incision highest amount; different incision highest plus 50% others)Outpatient Surgery - Anesthesiologist/Radiologist/Pathologist
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)Core Network Only Core Network Only Core Network Only
$2,000/$4,000 $2,000/$4,000 $6,000/$12,000$7,000/$14,000 $6,550/$13,100 $6,550/$13,100
NA Yes NAEmbedded Aggregate Embedded
All Except 2 PCP OVs & Rx Tier 1 All Except Preventive Rx All
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
Not Covered Not Covered Not Covered$75 copay* $75 copay* $75 copay*
50% coinsurance* 50% coinsurance 50% coinsurance*
$0 copay* $0 copay* $0 copay*
$75 copay* $75 copay* $75 copay*
Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*
$75 copay* $75 copay* $75 copay*$0 copay* $0 copay* $0 copay*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*$50 copay* $50 copay* $50 copay*
$250 copay* $250 copay* $300 copay*$200 copay* $200 copay* $200 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
Page 16

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMEINPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity)Surgeon's Services InpatientMaternity Delivery (physician or midwife)Anesthesiologist/Radiologist/PathologistAll Other Physician Services/VisitsInpatient Medical VisitsObservation StaysTransplants (must be performed at designated facilities)End of Life Care (In-network and OON) See COC.Autologous Blood Banking
EMERGENCY CARE AND URGENT CARE
Hospital Emergency Room for Emergency Condition - Professional & Facility (U.S., Canada, Mexico) (Covered as Inpatient Hospital Charges if admitted)
Ambulance (Non-Emergency ambulance requires preauthorization)
Hospital ER for follow-up, routine or urgent care
Urgent Care (Covered OON out-of-area. Not covered OON within Service Area.)
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregnancy preauth )Elective Sterilizations
Inpatient Hospital Charges for Mother and Child (other than preventive care)
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions.
SKILLED NURSING FACILITY365 days per Plan Year (Base plan)
HOSPICE CAREInpatient Hospice CareHome Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement.
HOME HEALTH CARE
Home Care Visits (60 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
Physician House Calls (where available)
MENTAL HEALTH & SUBSTANCE USE DISORDERS (Non-emergency coverage limited to Beacon providers)Inpatient Mental Health (limited to facilities defined in NY Law 1.03 (10))
Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services)
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
50% coinsurance* 25% coinsurance* 50% coinsurance*$100 copay* $100 copay* $100 copay*$100 copay* $100 copay* $100 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
Not Covered Not Covered Not Covered
$0 copay* $0 copay* $0 copay*
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
50% coinsurance* 25% coinsurance* 50% coinsurance*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
Page 17

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAME
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities)Outpatient Substance Use Services (OASAS-certified or waivered SCP's under the Drug Addiction Treatment Act of 2000.) Up to 20 visits per calendar year for family counseling provided family member is a covered person under member's family COC. Allowed Amount same irrespective of number of family members attending session.)MISCELLANEOUSAllergy Testing and TreatmentPodiatric Procedures
Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year.
After full or partial mastectomy, breast reconstruction including implants (preauth required to the extent inpt or outpt surg req'd)Chiropractic Care - Unlimited VisitsClinical TrialsSecond Opinions Cancer, Surgery, Required and OtherReferrals to Non-Network Providers
SHORT TERM REHAB & HABILITATIVE SERVICESInpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime.Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT.
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment (greater than or equal to $500)Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.)
MEDICAL SUPPLIESMedical Supplies When Medically Necessary
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered.
AUTISM SPECTRUM DISORDER (ASD)Applied Behavior Analysis treatment for ASD under 11 NYCRR 440Assistive Communication Devices for ASD
DIABETIC SERVICESInsulin and Oral Medication - 30/90 day supplyDiabetic Supplies (needles and syringes) and Equipment - 30/90 day supplyDiabetic Education
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*$75 copay* $75 copay* $75 copay*
See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingSee Rx Cost Sharing See Rx Cost Sharing See Rx Cost Sharing
$75 copay* $75 copay* $75 copay*
Page 18

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOff Exchange Plans
PLAN NAMEEXERCISE FACILITYSubscriber (Reimbursement upon completion of 50 visits in six-month period.)Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP.PHARMACYPrescription Drug Deductible (If applicable)Pharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays)Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays)
*Cost shares listed with an asterisk indicate subject to deductible.
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
$200 per 6 month period $200 per 6 month period $200 per 6 month period
$100 per 6 month period $100 per 6 month period $100 per 6 month period
Integrated with Medical, Tier 1 Waived Integrated with Medical Integrated with Medical$10/$50*/$80* $10*/$50*/$80* $10*/$50*/$80*
2.5 times Rx copay 2.5 times Rx copay 2.5 times Rx copay
Page 19

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Description of Revised Rating Classes, Factors, and Discounts
Not applicable for Individual products.
Off Exchange
Page 20

Crystal Run Health Plan, LLC2017 Individual Rating ManualExamples of Rate Calculations
Not applicable for Individual products. See page 2 for premium rates by tier.
Off Exchange
Page 21

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Commission Schedule
Broker 0% of premium
Off Exchange
Page 22

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Census Tiers and Factors
Single 1.000Employee & Spouse 2.000Employee & Child(ren) 1.700Family 2.850Child Only 0.412
Off Exchange
Page 23

With Through Age 29 Coverage 1.000Without Family Planning Coverage N/AWithout Domestic Partner Coverage N/AWith Pediatric Dental Coverage N/A
Off Exchange
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Adjustment Factors for Major Variations From Plan Base
Page 24

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Expected Loss Ratio
Standard Plans Expected Loss Ratio
Platinum 82%
Gold 82%
Silver 82%
Bronze 82%
Catastrophic 82%
Non-Standard Plans Expected Loss Ratio
Platinum 82%
Gold 82%
Silver 82%
Bronze 82%
Off Exchange
Page 25

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Underwriting Guidelines
Refer to separately provided Underwriting Guidelines.
Off Exchange
Page 26

Crystal Run Health Plan, LLC
2017 Individual On Exchange Plans Rating Manual
2017 Premium Rates

Crystal Run Health Plan, LLC2017 Individual On Exchange Plans Rating Manual
Table of Contents Page
2017 Form Numbers for Region 3 1
2017 Premium Rates for Region 3 2
Composition of Rating Regions 3
Benefit Designs 4-19
Description of Revised Rating Classes, Factors, and Discounts 20 Examples of Rate Calculations 21 Commission Schedules 22 Census Tiers and Factors 23 Adjustment Factors for Major Variations 24 Expected Loss Ratios 25
Underwriting Guidelines 26

Plan Name Product Description Plan ID Form Number
Platinum: Platinum:Platinum HMO ST, Platinum, ST, IN, Child Only, DP, FP ST Platinum Plan - Child Only 73886NY0010012 Form: CRHP Child Only Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO ST, Platinum, ST, IN, Dep25, DP, FP ST Platinum Plan - Dep Age 25, DP & FP 73886NY0010007 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO ST, Platinum, ST, IN, Dep29, DP, FP ST Platinum Plan - Dep Age 29, DP & FP 73886NY0010008 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum Ind Child Only (2017)Platinum HMO NS, Platinum, NS, IN, Dep29, DP, FP NS Platinum Plan - Dep Age 29, DP & FP 73886NY0010028 Form: CRHP Individual Contract (2017) and Form: CRHP Platinum NS Plan (2017)
Gold: Gold:Gold HMO ST, Gold, ST, IN, Child Only, DP, FP ST Gold Plan - Child Only 73886NY0010011 Form: CRHP Child Only Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO ST, Gold, ST, IN, Dep25, DP, FP ST Gold Plan - Dep Age 25, DP & FP 73886NY0010005 Form: CRHP Individual Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO ST, Gold, ST, IN, Dep29, DP, FP ST Gold Plan - Dep Age 29, DP & FP 73886NY0010006 Form: CRHP Individual Contract (2017) and Form: CRHP Gold Ind Child Only (2017)Gold HMO NS, Gold, NS, IN, Dep29, DP, FP NS Gold Plan - Dep Age 29, DP & FP 73886NY0010026 Form: CRHP Individual Contract (2017) and Form: CRHP Gold NS Plan (2017)Gold HMO NS HDHP, Gold, NS, IN, Dep29, DP, FP NS Gold Plan HDHP - Dep Age 25, DP & FP 73886NY0010027 Form: CRHP Individual Contract (2017) and Form: CRHP Gold NS Plan (2017)
Silver: Silver:Silver HMO ST, Silver, ST, IN, Child Only, DP, FP ST Silver Plan - Child Only 73886NY0010010 Form: CRHP Child Only Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO ST, Silver, ST, IN, Dep25, DP, FP ST Silver Plan - Dep Age 25, DP & FP 73886NY0010003 Form: CRHP Individual Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO ST, Silver, ST, IN, Dep29, DP, FP ST Silver Plan - Dep Age 29, DP & FP 73886NY0010004 Form: CRHP Individual Contract (2017) and Form: CRHP Silver Ind Child Only (2017)Silver HMO NS, Silver, NS, IN, Dep29, DP, FP NS Silver Plan - Dep Age 29, DP & FP 73886NY0010024 Form: CRHP Individual Contract (2017) and Form: CRHP Silver NS Plan (2017)Silver HMO NS HDHP, Silver, NS, IN, Dep29, DP, FP NS Silver Plan HDHP - Dep Age 25, DP & FP 73886NY0010025 Form: CRHP Individual Contract (2017) and Form: CRHP Silver NS Plan (2017)
Bronze: Bronze:Bronze HMO ST, Bronze, ST, IN, Child Only, DP, FP ST Bronze Plan - Child Only 73886NY0010009 Form: CRHP Child Only Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO ST, Bronze, ST, IN, Dep25, DP, FP ST Bronze Plan - Dep Age 25, DP & FP 73886NY0010001 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO ST, Bronze, ST, IN, Dep29, DP, FP ST Bronze Plan - Dep Age 29, DP & FP 73886NY0010002 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze Ind/Child Only (2017)Bronze HMO NS, Bronze, NS, IN, Dep29, DP, FP NS Bronze Plan - Dep Age 29, DP & FP 73886NY0010023 Form: CRHP Individual Contract (2017) and Form: CRHP Bronze NS Plan (2017)
Catastrophic: Catastrophic:Catastrophic HMO ST, Catastrophic, ST, IN, Dep25, DP, FP ST Catastrophic Plan - Dep Age 25, DP & FP 73886NY0010021 Form: CRHP Catastrophic Contract (2017) and Form CRHP Catastrophic Plan (2017)
Product Description Abbreviations:ST - StandardNS - Non-StandardDep Age 25 - Dependent coverage through age 25Dep Age 29 - Dependent coverage through age 29DP - Domestic PartnerFP - Family Planning
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Form Numbers Effective January 1, 2017Mid Hudson (Region 3)
On Exchange
Page 1

Premium Per Contract
Plan Name Product Description Plan ID SingleSingle + Spouse
Single + Child(ren)
Single + Spouse +
Child(ren)
One Child Only
Two Children
Only*
Three or More
Children Only**
Platinum: Platinum:Platinum HMO ST, Platinum, ST, IN, Child Only, DP, FP ST Platinum Plan - Child Only 73886NY0010012 $331.18 $662.36 $993.54Platinum HMO ST, Platinum, ST, IN, Dep25, DP, FP ST Platinum Plan - Dep Age 25, DP & FP 73886NY0010007 $803.85 $1,607.69 $1,366.54 $2,290.96Platinum HMO ST, Platinum, ST, IN, Dep29, DP, FP ST Platinum Plan - Dep Age 29, DP & FP 73886NY0010008 $803.85 $1,607.69 $1,366.54 $2,290.96Platinum HMO NS, Platinum, NS, IN, Dep29, DP, FP NS Platinum Plan - Dep Age 29, DP & FP 73886NY0010028 $784.54 $1,569.08 $1,333.72 $2,235.94
Gold: Gold:Gold HMO ST, Gold, ST, IN, Child Only, DP, FP ST Gold Plan - Child Only 73886NY0010011 $290.86 $581.72 $872.58Gold HMO ST, Gold, ST, IN, Dep25, DP, FP ST Gold Plan - Dep Age 25, DP & FP 73886NY0010005 $705.96 $1,411.92 $1,200.13 $2,011.98Gold HMO ST, Gold, ST, IN, Dep29, DP, FP ST Gold Plan - Dep Age 29, DP & FP 73886NY0010006 $705.96 $1,411.92 $1,200.13 $2,011.98Gold HMO NS, Gold, NS, IN, Dep29, DP, FP NS Gold Plan - Dep Age 29, DP & FP 73886NY0010026 $686.92 $1,373.84 $1,167.76 $1,957.72Gold HMO NS HDHP, Gold, NS, IN, Dep29, DP, FP NS Gold Plan HDHP - Dep Age 25, DP & FP 73886NY0010027 $660.82 $1,321.64 $1,123.39 $1,883.33
Silver: Silver:Silver HMO ST, Silver, ST, IN, Child Only, DP, FP ST Silver Plan - Child Only 73886NY0010010 $254.32 $508.64 $762.96Silver HMO ST, Silver, ST, IN, Dep25, DP, FP ST Silver Plan - Dep Age 25, DP & FP 73886NY0010003 $617.29 $1,234.57 $1,049.39 $1,759.26Silver HMO ST, Silver, ST, IN, Dep29, DP, FP ST Silver Plan - Dep Age 29, DP & FP 73886NY0010004 $617.29 $1,234.57 $1,049.39 $1,759.26Silver HMO NS, Silver, NS, IN, Dep29, DP, FP NS Silver Plan - Dep Age 29, DP & FP 73886NY0010024 $563.44 $1,126.89 $957.85 $1,605.81Silver HMO NS HDHP, Silver, NS, IN, Dep29, DP, FP NS Silver Plan HDHP - Dep Age 25, DP & FP 73886NY0010025 $575.54 $1,151.07 $978.41 $1,640.28
Bronze: Bronze:Bronze HMO ST, Bronze, ST, IN, Child Only, DP, FP ST Bronze Plan - Child Only 73886NY0010009 $206.37 $412.74 $619.11Bronze HMO ST, Bronze, ST, IN, Dep25, DP, FP ST Bronze Plan - Dep Age 25, DP & FP 73886NY0010001 $500.90 $1,001.79 $851.52 $1,427.56Bronze HMO ST, Bronze, ST, IN, Dep29, DP, FP ST Bronze Plan - Dep Age 29, DP & FP 73886NY0010002 $500.90 $1,001.79 $851.52 $1,427.56Bronze HMO NS, Bronze, NS, IN, Dep29, DP, FP NS Bronze Plan - Dep Age 29, DP & FP 73886NY0010023 $496.41 $992.83 $843.90 $1,414.78
Catastrophic: Catastrophic:Catastrophic HMO ST, Catastrophic, ST, IN, Dep25, DP, FP ST Catastrophic Plan - Dep Age 25, DP & FP 73886NY0010021 $240.19 $480.39 $408.33 $684.55
Product Description Abbreviations:ST - StandardNS - Non-StandardDep Age 25 - Dependent coverage through age 25Dep Age 29 - Dependent coverage through age 29DP - Domestic PartnerFP - Family Planning
*For a child only plan that covers two children in a family**For a child only plan that covers three or more children in a family
Mid Hudson (Region 3)On Exchange
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Premium Rates Effective January 1, 2017
Page 2

Crystal Run Health Plan, LLC2017 Individual Rating ManualComposition of Rating Regions
Region 3 (Mid-Hudson)OrangeSullivan
On Exchange
Page 3

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)BENEFIT Core Network Only Core Network OnlyFINANCIAL / DEDUCTIBLESDeductible (Single/Family) $0/$0 $600/$1200Max Out of Pocket (Single/Family) $2,000/$4,000 $4,000/$8,000HSA Qualified NA NADeductible Structure Embedded EmbeddedDeductible Applies to: NA All except RxPREVENTIVE CARE
Adult & Women's (USPSTF & HRSA required) See Section N SG 42 Implemention Guide Covered in Full Covered in Full
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implemenation Guide Covered in Full Covered in Full
Preventive Dental for Children (Up to age 19) Not Covered Not CoveredPediatric Vision Exam (Up to age 19; 1 per 12 month period) $15 copay $25 copay*Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period) 10% coinsurance 20% coinsurance*
OFFICE VISITS
PCP (includes any PCP allergy diag/treatment) $15 copay $25 copay*
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies) $35 copay $40 copay*
Lab Performed as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copayRadiology/Ultrasound as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copaySurgery Performed as Part of PCP/SCP Office Visit Covered by Office Visit copay Covered by Office Visit copayMedications Administered in PCP/SCP Office (preauth infusion) Covered by Office Visit copay Covered by Office Visit copay
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim)Lab - Outpatient Hospital Setting $35 copay $40 copay*Lab - Outpatient Hospital Setting, preadmission testing $0 copay $0 copay*Lab - Independent Laboratory $35 copay $40 copay*Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
$15 copay $25 copay*
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, sleep studies ) $35 copay $40 copay*
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting $35 copay $40 copay*X-ray/Ultrasound – Freestanding Facility $35 copay $40 copay*
Page 4

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital Setting $35 copay $40 copay*MRI, CT, Nuclear Medicine & PET – Freestanding Facility $35 copay $40 copay*
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility) $100 copay $100 copay*Outpatient Surgery – Freestanding Facility (facility) $100 copay $100 copay*Outpatient Surgery - Surgeon’s Services $100 copay $100 copay*
INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity) $500/admission $1,000/admission*Surgeon's Services Inpatient $100 copay $100 copay*Maternity Delivery (physician or midwife) $100 copay $100 copay*Anesthesiologist/Radiologist/Pathologist Covered in Full Covered in FullAll Other Physician Services/Visits $0 Copay $0 Copay*Inpatient Medical Visits $0 Copay $0 Copay*Observation Stays $100 copay $150 copay*Transplants (must be performed at desiginated facilities) $500/admission $1,000/admission*End of Life Care (In-network and OON) $500/admission $1,000/admission*Autologous Blood Banking 10% coinsurance 20% coinsurance*
EMERGENCY CAREEmergency Room Care (World Wide) (No physician copay) $100 copay $150 copay*Ambulance (Non-Emergency ambulance requires preauthorization) $100 copay $150 copay*Hospital ER for follow-up, routine or urgent care Not Covered Not CoveredUrgent Care Center (Covered outside Service Area in-network and OON . Not covered OON within Service Area.) Facility only. $55 copay $60 copay*
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregancy preauth ) Covered in Full Covered in Full*
Inpatient Hospital Charges for Mother and Child (other than preventive care) $500/admission $1,000/admission*
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions. Appropriate Cost Share Appropriate Cost Share
Page 5

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)SKILLED NURSING FACILITY200 days per Plan Year (Base plan) $500/admission $1,000/admission*
HOSPICE CAREInpatient Hospice Care $500/admission $1,000/admission*Home Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement. $15 copay $25 copay*
HOME HEALTH CAREHome Care Visits (40 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
$15 copay $25 copay*
Physician House Calls (where available) PCP/SCP OV cost share PCP/SCP OV cost share
MENTAL HEALTH &SUBSTANCE USE DISORDERSInpatient Mental Health (limited to facilities defined in NY Law 1.03 (10)) $500/admission $1,000/admission*Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services) $15 copay $25 copay*
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
$500/admission $1,000/admission*
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities) $500/admission $1,000/admission*
Outpatient Substance Use Services (OASAS-certifed or waivered SCP's under the Drug Addiction Treatment Act of 2000. Up to 20 visits per calendar year may be used for family counseling.)
$15 copay $25 copay*
MICELLANEOUS
Allergy Testing and Treatment (preauth IVIG only) PCP/SCP OV cost share PCP/SCP OV cost share
Podiatric Procedures $35 copay $40 copay*Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year. $35 copay $40 copay*
After full or partial mastectomy,breast reconstruction including implants. Appropriate Cost Share Appropriate Cost Share
Chiropractic Care - Unlimited Visits $35 copay $40 copay*Clinical Trials Appropriate Cost Share Appropriate Cost ShareSecond Opinions Cancer, Surgery, Required and Other $35 copay $40 copay*Referrals to Non-Network Providers Appropriate Cost Share Appropriate Cost Share
Page 6

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO ST (2017) GOLD HMO ST (2017)SHORT TERM REHAB & HABILITATIVE SERVICES
Inpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime. $500/admission $1,000/admission*
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT. $25 copay $30 copay*
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment 10% coinsurance 20% coinsurance*Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.) 10% coinsurance 20% coinsurance*
MEDICAL SUPPLIESMedical Supplies When Medically Necessary 10% coinsurance 20% coinsurance*
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered. 10% coinsurance 20% coinsurance*
AUTISM SPECTRUM DISORDER (ASD)
Applied Behavior Analysis treatment for ASD under 11 NYCRR 440 $15 copay $25 copay*
Assistive Communication Devices for ASD $15 copay $25 copay*
DIABETIC SERVICES
Insulin and Oral Medication - 30/90 day supply $15 copay per 30 day supply $25 copay per 30 day supply*
Diabetic Supplies (needles and syringes) and Equipment - 30/90 day supply $15 copay per 30 day supply $25 copay per 30 day supply*Diabetic Education $15 copay $25 copay*
EXERCISE FACILITY
Subscriber (Reimbursement upon completion of 50 visits in six-month period.) $200 per 6 month period $200 per 6 month period
Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP. $100 per 6 month period $100 per 6 month period
Prescription Drug Deductible (If applicable) Not subject to deductible Not subject to deductiblePharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays) $10/$30/$60 $10/$35/$70Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays) 2.5 times Rx copay 2.5 times Rx copay
*Cost shares listed with an asterisk indicate subject to deductible.
Page 7

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMEBENEFITFINANCIAL / DEDUCTIBLESDeductible (Single/Family)Max Out of Pocket (Single/Family)HSA QualifiedDeductible StructureDeductible Applies to:PREVENTIVE CARE
Adult & Women's (USPSTF & HRSA required) See Section N SG 42 Implemention Guide
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implemenation GuidePreventive Dental for Children (Up to age 19)Pediatric Vision Exam (Up to age 19; 1 per 12 month period)Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period)
OFFICE VISITS
PCP (includes any PCP allergy diag/treatment)
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies)
Lab Performed as Part of Office VisitRadiology/Ultrasound as Part of Office VisitSurgery Performed as Part of PCP/SCP Office VisitMedications Administered in PCP/SCP Office (preauth infusion)
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim)Lab - Outpatient Hospital SettingLab - Outpatient Hospital Setting, preadmission testingLab - Independent LaboratoryOutpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, sleep studies )
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting X-ray/Ultrasound – Freestanding Facility
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)Core Network Only Core Network Only Core Network Only
$2,000/$4,000 $4,000/$8,000 $7,150/$14,300$6,750/$13,500 $7,150/$14,300 $7,150/$14,300
NA NA NAEmbedded Embedded Embedded
All except Rx All All
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
Not Covered Not Covered Not Covered$30 copay* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance* (3 PCP Visits w/o deductible with cost-share)
$50 copay* 50% coinsurance* 0% coinsurance*
Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*Covered by Office Visit copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*$0 copay* 50% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*$50 copay* 50% coinsurance* 0% coinsurance*
Page 8

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMEMRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital SettingMRI, CT, Nuclear Medicine & PET – Freestanding Facility
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility)Outpatient Surgery – Freestanding Facility (facility)Outpatient Surgery - Surgeon’s Services
INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity)Surgeon's Services InpatientMaternity Delivery (physician or midwife)Anesthesiologist/Radiologist/PathologistAll Other Physician Services/VisitsInpatient Medical VisitsObservation StaysTransplants (must be performed at desiginated facilities)End of Life Care (In-network and OON)Autologous Blood Banking
EMERGENCY CAREEmergency Room Care (World Wide) (No physician copay)Ambulance (Non-Emergency ambulance requires preauthorization)Hospital ER for follow-up, routine or urgent careUrgent Care Center (Covered outside Service Area in-network and OON . Not covered OON within Service Area.) Facility only.
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregancy preauth )
Inpatient Hospital Charges for Mother and Child (other than preventive care)
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions.
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$50 copay* 50% coinsurance* 0% coinsurance*$50 copay* 50% coinsurance* 0% coinsurance*
$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*$100 copay* 50% coinsurance* 0% coinsurance*
Covered in Full 50% coinsurance* 0% coinsurance*$0 Copay* 50% coinsurance* 0% coinsurance*$0 Copay* 50% coinsurance* 0% coinsurance*
$250 copay* 50% coinsurance* 0% coinsurance*$1,500/admission* 50% coinsurance* 0% coinsurance*$1,500/admission* 50% coinsurance* 0% coinsurance*30% coinsurance* 50% coinsurance* 0% coinsurance*
$250 copay* 50% coinsurance* 0% coinsurance*$150 copay* 50% coinsurance* 0% coinsurance*Not Covered Not Covered Not Covered
$70 copay* 50% coinsurance* 0% coinsurance*
Covered in Full* Covered in Full Covered in Full
$1,500/admission* 50% coinsurance* 0% coinsurance*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
Page 9

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMESKILLED NURSING FACILITY200 days per Plan Year (Base plan)
HOSPICE CAREInpatient Hospice CareHome Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement.
HOME HEALTH CAREHome Care Visits (40 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.Physician House Calls (where available)
MENTAL HEALTH &SUBSTANCE USE DISORDERSInpatient Mental Health (limited to facilities defined in NY Law 1.03 (10))Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services)
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities)
Outpatient Substance Use Services (OASAS-certifed or waivered SCP's under the Drug Addiction Treatment Act of 2000. Up to 20 visits per calendar year may be used for family counseling.)
MICELLANEOUS
Allergy Testing and Treatment (preauth IVIG only)
Podiatric ProceduresInterruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year.
After full or partial mastectomy,breast reconstruction including implants.
Chiropractic Care - Unlimited VisitsClinical TrialsSecond Opinions Cancer, Surgery, Required and OtherReferrals to Non-Network Providers
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$1,500/admission* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
PCP/SCP OV cost share 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
PCP/SCP OV cost share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*
Appropriate Cost Share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*Appropriate Cost Share 50% coinsurance* 0% coinsurance*
$50 copay* 50% coinsurance* 0% coinsurance*Appropriate Cost Share 50% coinsurance* 0% coinsurance*
Page 10

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMESHORT TERM REHAB & HABILITATIVE SERVICES
Inpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime.
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT.
DURABLE MEDICAL EQUIPMENTDurable Medical EquipmentProsthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.)
MEDICAL SUPPLIESMedical Supplies When Medically Necessary
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered.
AUTISM SPECTRUM DISORDER (ASD)
Applied Behavior Analysis treatment for ASD under 11 NYCRR 440
Assistive Communication Devices for ASD
DIABETIC SERVICES
Insulin and Oral Medication - 30/90 day supply
Diabetic Supplies (needles and syringes) and Equipment - 30/90 day supplyDiabetic Education
EXERCISE FACILITY
Subscriber (Reimbursement upon completion of 50 visits in six-month period.)
Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP.
Prescription Drug Deductible (If applicable)Pharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays)Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays)
*Cost shares listed with an asterisk indicate subject to deductible.
SILVER HMO ST (2017) BRONZE HMO ST (2017) CATASTROPHIC ST (2017)
$1,500/admission* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
30% coinsurance* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay* 50% coinsurance* 0% coinsurance*
$30 copay per 30 day supply* 50% coinsurance* 0% coinsurance*
$30 copay per 30 day supply* 50% coinsurance* 0% coinsurance*$30 copay* 50% coinsurance* 0% coinsurance*
$200 per 6 month period $200 per 6 month period $200 per 6 month period
$100 per 6 month period $100 per 6 month period $100 per 6 month period
Not subject to deductible Integrated with Medical Integrated with Medical$10/$35/$70 $10*/$35*/$70* 0% coinsurance*
2.5 times Rx copay 2.5 times Rx copay 0% coinsurance
Page 11

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)BENEFIT Core Network Only Core Network Only Core Network OnlyFINANCIAL / DEDUCTIBLESDeductible (Single/Family) $0/$0 $0/$0 $1,500/$3,000Max Out of Pocket (Single/Family) $2,100/$4,200 $4,400/$8,800 $6,550/$13,100HSA Qualified NA NA YesDeductible Structure Embedded Embedded AggregateDeductible Applies to: NA NA All Except Preventive RxPREVENTIVE CAREAdult & Women's (USPSTF & HRSA required) See Section N SG 42 Implementation Guide Covered in Full Covered in Full Covered in Full
Infant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implementation Guide Covered in Full Covered in Full Covered in Full
Preventive Dental for Children (Up to age 19) Not Covered Not Covered Not CoveredPediatric Vision Exam (Up to age 19; 1 per 12 month period) $50 copay $50 copay $25 copay*Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period) 50% coinsurance 50% coinsurance 50% coinsurance*
OFFICE VISITSPCP (includes any PCP allergy diag/treatment) $0 copay $0 copay $0 copay*
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies) $50 copay $50 copay $25 copay*
Lab Performed as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Radiology/Ultrasound as Part of Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Surgery Performed as Part of PCP/SCP Office Visit Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*Medications Administered in PCP/SCP Office (preauth infusion) Covered by Office Visit copay Covered by Office Visit copay Covered by Office Visit copay*
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim.)Lab - Outpatient Hospital Setting, including preadmission tests $50 copay $50 copay $25 copay*Lab - Independent Laboratory $0 copay $0 copay $0 copay*
Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
$50 copay $50 copay $25 copay*
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, neuro psych testing , sleep studies ) $50 copay $50 copay $25 copay*
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting $50 copay $75 copay $75 copay*X-ray/Ultrasound – Freestanding Facility $25 copay $50 copay $50 copay*
MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital Setting $200 copay $200 copay $200 copay*MRI, CT, Nuclear Medicine & PET – Freestanding Facility $150 copay $150 copay $150 copay*
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility) 20% coinsurance 50% coinsurance 20% coinsuranceOutpatient Surgery – Freestanding Facility (facility) 20% coinsurance 50% coinsurance 20% coinsuranceOutpatient Surgery - Surgeon's/Physician's Services (Same incision highest amount; different incision highest plus 50% others) Covered in Full 30% coinsurance Covered In Full*
Outpatient Surgery - Anesthesiologist/Radiologist/Pathologist Covered in Full 30% coinsurance Covered In Full*
Page 12

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)INPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity) 20% coinsurance 50% coinsurance $500 copay*Surgeon's Services Inpatient $100 copay $100 copay $100 copay*Maternity Delivery (physician or midwife) $100 copay $100 copay $100 copay*Anesthesiologist/Radiologist/Pathologist 20% coinsurance 50% coinsurance Covered in Full*All Other Physician Services/Visits 20% coinsurance 50% coinsurance Covered in Full*Inpatient Medical Visits 20% coinsurance 50% coinsurance Covered in Full*Observation Stays 20% coinsurance 50% coinsurance $500 copay*Transplants (must be performed at designated facilities) 20% coinsurance 50% coinsurance $500 copay*End of Life Care (In-network and OON) See COC. 20% coinsurance 50% coinsurance $500 copay*Autologous Blood Banking 20% coinsurance 50% coinsurance $25 copay*
EMERGENCY CARE AND URGENT CARE
Hospital Emergency Room for Emergency Condition - Professional & Facility (U.S., Canada, Mexico) (Covered as Inpatient Hospital Charges if admitted) 20% coinsurance 50% coinsurance $200 copay*
Ambulance (Non-Emergency ambulance requires preauthorization) 20% coinsurance 50% coinsurance $100 copay*
Hospital ER for follow-up, routine or urgent care Not Covered Not Covered Not Covered
Urgent Care (Covered OON out-of-area. Not covered OON within Service Area.) $0 copay $0 copay $0 copay*
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregnancy preauth ) Covered in Full Covered in Full Covered in Full
Elective Sterilizations Covered in Full Covered in Full Covered in Full
Inpatient Hospital Charges for Mother and Child (other than preventive care) 20% coinsurance 50% coinsurance $500 copay*
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions. Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
SKILLED NURSING FACILITY365 days per Plan Year (Base plan) 20% coinsurance 50% coinsurance $500 copay*
HOSPICE CAREInpatient Hospice Care 20% coinsurance 50% coinsurance $500 copay*Home Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement. $50 copay $50 copay $25 copay*
HOME HEALTH CARE
Home Care Visits (60 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
$50 copay $50 copay $25 copay*
Physician House Calls (where available) PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share
MENTAL HEALTH & SUBSTANCE USE DISORDERS (Non-emergency coverage limited to Beacon providers)Inpatient Mental Health (limited to facilities defined in NY Law 1.03 (10)) 20% coinsurance 50% coinsurance $500 copay*
Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services) $50 copay $50 copay $25 copay*
Page 13

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
20% coinsurance 50% coinsurance $500 copay*
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities) 20% coinsurance 50% coinsurance $500 copay*
Outpatient Substance Use Services (OASAS-certified or waivered SCP's under the Drug Addiction Treatment Act of 2000.) Up to 20 visits per calendar year for family counseling provided family member is a covered person under member's family COC. Allowed Amount same irrespective of number of family members attending session.)
$50 copay $50 copay $25 copay*
MISCELLANEOUSAllergy Testing and Treatment PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost sharePodiatric Procedures $50 copay $50 copay $25 copay*
Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year. $50 copay $50 copay $25 copay*
After full or partial mastectomy, breast reconstruction including implants (preauth required to the extent inpt or outpt surg req'd) Appropriate Cost Share Appropriate Cost Share Appropriate Cost ShareChiropractic Care - Unlimited Visits $50 copay $50 copay $25 copay*Clinical Trials Appropriate Cost Share Appropriate Cost Share Appropriate Cost ShareSecond Opinions Cancer, Surgery, Required and Other $50 copay $50 copay $25 copay*Referrals to Non-Network Providers Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
SHORT TERM REHAB & HABILITATIVE SERVICESInpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime. 20% coinsurance 50% coinsurance $500 copay*
Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT. $50 copay $50 copay $25 copay*
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment (greater than or equal to $500) 20% coinsurance 50% coinsurance $500 copay*Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.) 20% coinsurance 50% coinsurance $500 copay*
MEDICAL SUPPLIESMedical Supplies When Medically Necessary 20% coinsurance 50% coinsurance 50% coinsurance*
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered. 20% coinsurance 50% coinsurance 50% coinsurance*
AUTISM SPECTRUM DISORDER (ASD)Applied Behavior Analysis treatment for ASD under 11 NYCRR 440 $50 copay $50 copay $25 copay*Assistive Communication Devices for ASD $50 copay $50 copay $25 copay*
DIABETIC SERVICESInsulin and Oral Medication - 30/90 day supply See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingDiabetic Supplies (needles and syringes) and Equipment - 30/90 day supply See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingDiabetic Education $50 copay $50 copay $25 copay*
Page 14

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME PLATINUM HMO NS (2017) GOLD HMO NS (2017) GOLD HMO NS HDHP (2017)EXERCISE FACILITYSubscriber (Reimbursement upon completion of 50 visits in six-month period.) $200 per 6 month period $200 per 6 month period $200 per 6 month periodSpouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP. $100 per 6 month period $100 per 6 month period $100 per 6 month period
PHARMACYPrescription Drug Deductible (If applicable) Not subject to deductible Not subject to deductible Integrated with MedicalPharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays) $10/$50/$80 $10/$50/$80 $0*/$30*/$60*Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays) 2.5 times Rx copay 2.5 times Rx copay 2.5 times Rx copay
*Cost shares listed with an asterisk indicate subject to deductible.
Page 15

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMEBENEFITFINANCIAL / DEDUCTIBLESDeductible (Single/Family)Max Out of Pocket (Single/Family)HSA QualifiedDeductible StructureDeductible Applies to:PREVENTIVE CAREAdult & Women's (USPSTF & HRSA required) See Section N SG 42 Implementation GuideInfant and Pediatric (USPSTF & HRSA required) See Section N, SG 42 Implementation GuidePreventive Dental for Children (Up to age 19)Pediatric Vision Exam (Up to age 19; 1 per 12 month period)Pediatric Vision Hardware (Up to age 19; 1 frame & pair of lenses or 1 pair of contact lenses per 12 month period)
OFFICE VISITSPCP (includes any PCP allergy diag/treatment)
SCP (includes allergist diag/treatment, podiatric, chiropractic & vasectomies)
Lab Performed as Part of Office VisitRadiology/Ultrasound as Part of Office VisitSurgery Performed as Part of PCP/SCP Office VisitMedications Administered in PCP/SCP Office (preauth infusion)
OUTPATIENT SERVICES (Where there is a facility and a professional component, any copayment is applied (once) to the facility component claim.)Lab - Outpatient Hospital Setting, including preadmission testsLab - Independent Laboratory
Outpatient Hospital/Freestanding - Therapeutic Services (Radiation/Infusion/Chemo/Dialysis/ Inhalation/Hyperbaric Oxygen/Cardio Rehab/Pulmonary Rehab , etc.) Up to 10 OON Dialysis visits covered/year - see COC.
Outpatient Hospital/Freestanding - (Non-Lab/Radiology) Diagnostic Testing (e.g., EKG, EEG, pulmonary, stress testing, neuro psych testing , sleep studies )
RADIOLOGY & ULTRA-SOUNDX-ray/Ultrasound – Hospital Setting X-ray/Ultrasound – Freestanding Facility
MRI, MRA, CT, NUCLEAR MED & PET SCANSMRI, CT, Nuclear Medicine & PET – Hospital SettingMRI, CT, Nuclear Medicine & PET – Freestanding Facility
OUTPATIENT SURGERYOutpatient Surgery – Hospital Setting (facility)Outpatient Surgery – Freestanding Facility (facility)Outpatient Surgery - Surgeon's/Physician's Services (Same incision highest amount; different incision highest plus 50% others)Outpatient Surgery - Anesthesiologist/Radiologist/Pathologist
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)Core Network Only Core Network Only Core Network Only
$2,000/$4,000 $2,000/$4,000 $6,000/$12,000$7,000/$14,000 $6,550/$13,100 $6,550/$13,100
NA Yes NAEmbedded Aggregate Embedded
All Except 2 PCP OVs & Rx Tier 1 All Except Preventive Rx All
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
Not Covered Not Covered Not Covered$75 copay* $75 copay* $75 copay*
50% coinsurance* 50% coinsurance 50% coinsurance*
$0 copay* $0 copay* $0 copay*
$75 copay* $75 copay* $75 copay*
Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*Covered by Office Visit copay* Covered by Office Visit copay* Covered by Office Visit copay*
$75 copay* $75 copay* $75 copay*$0 copay* $0 copay* $0 copay*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*$50 copay* $50 copay* $50 copay*
$250 copay* $250 copay* $300 copay*$200 copay* $200 copay* $200 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
Page 16

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMEINPATIENT CAREHospital Inpatient Charges (Medical/Surgical/Maternity)Surgeon's Services InpatientMaternity Delivery (physician or midwife)Anesthesiologist/Radiologist/PathologistAll Other Physician Services/VisitsInpatient Medical VisitsObservation StaysTransplants (must be performed at designated facilities)End of Life Care (In-network and OON) See COC.Autologous Blood Banking
EMERGENCY CARE AND URGENT CARE
Hospital Emergency Room for Emergency Condition - Professional & Facility (U.S., Canada, Mexico) (Covered as Inpatient Hospital Charges if admitted)
Ambulance (Non-Emergency ambulance requires preauthorization)
Hospital ER for follow-up, routine or urgent care
Urgent Care (Covered OON out-of-area. Not covered OON within Service Area.)
REPRODUCTIVE CAREPrenatal and Postpartum Care including breast pump rental for duration of breast feeding (>3 Ultrasounds/pregnancy preauth )Elective Sterilizations
Inpatient Hospital Charges for Mother and Child (other than preventive care)
Infertility Services (Ages 21 - 44, inclusive) See COC for exclusions.
SKILLED NURSING FACILITY365 days per Plan Year (Base plan)
HOSPICE CAREInpatient Hospice CareHome Hospice - 210 days combined (Inpatient & Home) per Plan Year. Plus 5 visits family bereavement.
HOME HEALTH CARE
Home Care Visits (60 visits per Plan Year) Up to 4 hours equals 1 visit. Home Rehab/Hab don't count against Rehab/Hab benefits. One visit w/o cost share if mother discharged < 48/96 hours which don't count against the 60.
Physician House Calls (where available)
MENTAL HEALTH & SUBSTANCE USE DISORDERS (Non-emergency coverage limited to Beacon providers)Inpatient Mental Health (limited to facilities defined in NY Law 1.03 (10))
Outpatient Mental Health Care (Including Partial Hospitalization and Intensive Outpatient Program Services)
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
50% coinsurance* 25% coinsurance* 50% coinsurance*$100 copay* $100 copay* $100 copay*$100 copay* $100 copay* $100 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
Not Covered Not Covered Not Covered
$0 copay* $0 copay* $0 copay*
Covered in Full Covered in Full Covered in Full
Covered in Full Covered in Full Covered in Full
50% coinsurance* 25% coinsurance* 50% coinsurance*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
Page 17

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAME
Residential Care in residential treatment facility for (a) children and youth under NY Law 1.03 (33) (admission age up to 21; discharge age up to 22) or (b) that are part of a comprehensive care center for eating disorders identified pursuant to Article 27-J.
Inpatient Substance Use Services (detox and rehabilitation in OASAS-certified facilities)Outpatient Substance Use Services (OASAS-certified or waivered SCP's under the Drug Addiction Treatment Act of 2000.) Up to 20 visits per calendar year for family counseling provided family member is a covered person under member's family COC. Allowed Amount same irrespective of number of family members attending session.)MISCELLANEOUSAllergy Testing and TreatmentPodiatric Procedures
Interruption of Pregnancy - Therapeutic & non- therapeutic in cases of rape, incest, fetal malformation plus, unless FP opt out, 1 elective per member per Plan Year.
After full or partial mastectomy, breast reconstruction including implants (preauth required to the extent inpt or outpt surg req'd)Chiropractic Care - Unlimited VisitsClinical TrialsSecond Opinions Cancer, Surgery, Required and OtherReferrals to Non-Network Providers
SHORT TERM REHAB & HABILITATIVE SERVICESInpatient rehab consisting of PT/ST/OT limited to one consecutive 60 day period per condition per lifetime.Outpatient rehab and habilitation limited to 60 visits of each per condition per lifetime, includes PT/ST/OT.
DURABLE MEDICAL EQUIPMENTDurable Medical Equipment (greater than or equal to $500)Prosthetic Devices (One External Device per limb per lifetime except for up to age 19 for growth. No limit on Internal Devices.)
MEDICAL SUPPLIESMedical Supplies When Medically Necessary
HEARING AIDSLimited to a single purchase (including repair & replacement) per hearing impaired ear every three years. One Cochlear implant per time covered.
AUTISM SPECTRUM DISORDER (ASD)Applied Behavior Analysis treatment for ASD under 11 NYCRR 440Assistive Communication Devices for ASD
DIABETIC SERVICESInsulin and Oral Medication - 30/90 day supplyDiabetic Supplies (needles and syringes) and Equipment - 30/90 day supplyDiabetic Education
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
PCP/SCP OV cost share PCP/SCP OV cost share PCP/SCP OV cost share$75 copay* $75 copay* $75 copay*
$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share$75 copay* $75 copay* $75 copay*
Appropriate Cost Share Appropriate Cost Share Appropriate Cost Share
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
50% coinsurance* 25% coinsurance* 50% coinsurance*
$75 copay* $75 copay* $75 copay*$75 copay* $75 copay* $75 copay*
See Rx Cost Sharing See Rx Cost Sharing See Rx Cost SharingSee Rx Cost Sharing See Rx Cost Sharing See Rx Cost Sharing
$75 copay* $75 copay* $75 copay*
Page 18

Crystal Run Health Plan, LLC2017 Individual Rating ManualBenefit Design Description GridOn Exchange Plans
PLAN NAMEEXERCISE FACILITYSubscriber (Reimbursement upon completion of 50 visits in six-month period.)Spouse (Reimbursement upon completion of 50 visits in six-month period.) Limited to Subscriber & Spouse/DP.PHARMACYPrescription Drug Deductible (If applicable)Pharmacy Retail (6) (Tier 1/Tier 2/Tier 3 copays)Pharmacy Mail Order (6) (Tier 1/Tier 2/Tier 3 copays)
*Cost shares listed with an asterisk indicate subject to deductible.
SILVER HMO NS (2017) SILVER HMO NS HDHP (2017) BRONZE HMO NS HDHP (2017)
$200 per 6 month period $200 per 6 month period $200 per 6 month period
$100 per 6 month period $100 per 6 month period $100 per 6 month period
Integrated with Medical, Tier 1 Waived Integrated with Medical Integrated with Medical$10/$50*/$80* $10*/$50*/$80* $10*/$50*/$80*
2.5 times Rx copay 2.5 times Rx copay 2.5 times Rx copay
Page 19

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Description of Revised Rating Classes, Factors, and Discounts
Not applicable for Individual products.
On Exchange
Page 20

Crystal Run Health Plan, LLC2017 Individual Rating ManualExamples of Rate Calculations
Not applicable for Individual products. See page 2 for premium rates by tier.
On Exchange
Page 21

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Commission Schedule
Broker 0% of premium
On Exchange
Page 22

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Census Tiers and Factors
Single 1.000Employee & Spouse 2.000Employee & Child(ren) 1.700Family 2.850Child Only 0.412
On Exchange
Page 23

With Through Age 29 Coverage 1.000Without Family Planning Coverage N/AWithout Domestic Partner Coverage N/AWith Pediatric Dental Coverage N/A
On Exchange
Crystal Run Health Plan, LLC2017 Individual Rating Manual
Adjustment Factors for Major Variations From Plan Base
Page 24

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Expected Loss Ratio
Standard Plans Expected Loss Ratio
Platinum 82%
Gold 82%
Silver 82%
Bronze 82%
Catastrophic 82%
Non-Standard Plans Expected Loss Ratio
Platinum 82%
Gold 82%
Silver 82%
Bronze 82%
On Exchange
Page 25

Crystal Run Health Plan, LLC2017 Individual Rating Manual
Underwriting Guidelines
Refer to separately provided Underwriting Guidelines.
On Exchange
Page 26