
Critical Neonate Rafat Mosalli MD. Objectives Describe the algorithm for neonatal resuscitation and...
39
Critical Neonate Critical Neonate Rafat Mosalli MD Rafat Mosalli MD
-
Upload
joel-reynolds -
Category
Documents
-
view
219 -
download
2
Transcript of Critical Neonate Rafat Mosalli MD. Objectives Describe the algorithm for neonatal resuscitation and...
Critical NeonateCritical Neonate
Rafat Mosalli MDRafat Mosalli MD
Objectives
Describe the algorithm for neonatal Describe the algorithm for neonatal resuscitation and Delivery room resuscitation and Delivery room managementmanagement
Approach to a infant with Respiratory Approach to a infant with Respiratory distressdistress
Describe the etiology and effect of birth Describe the etiology and effect of birth asphyxiaasphyxia
Describe common birth injuriesDescribe common birth injuries
Case 1 ScenarioCase 1 Scenario
You are called to attend the delivery of a You are called to attend the delivery of a baby who is not born yet.baby who is not born yet.
What should you do firstWhat should you do first
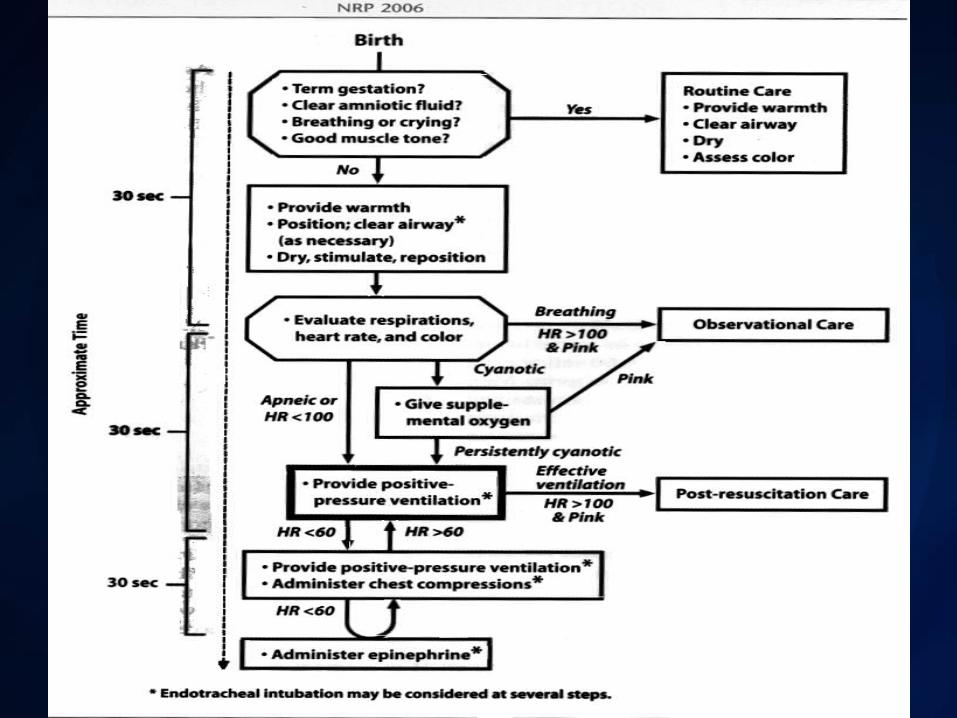
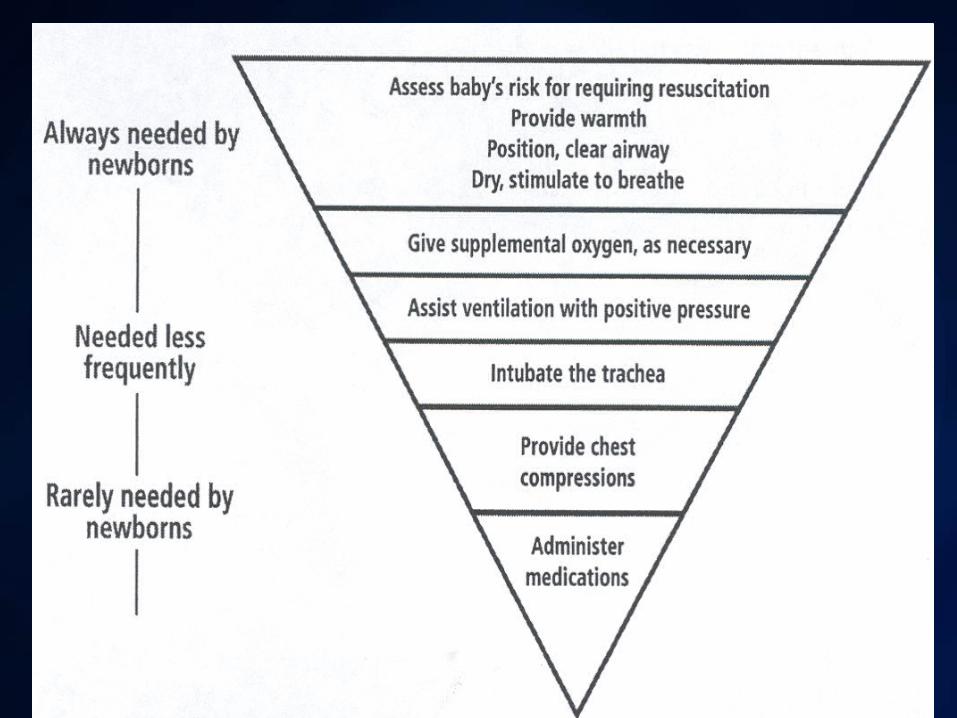
Delivery Room Care: ResuscitationDelivery Room Care: Resuscitation
Detailed maternal hx, GADetailed maternal hx, GA
Preparation ( equipments and personals)Preparation ( equipments and personals)

Case 1
Baby is 35 weeks delivered now, breathing Baby is 35 weeks delivered now, breathing fast ,irregular, Nasal flaring,blue in color fast ,irregular, Nasal flaring,blue in color and intercostal Retractions?and intercostal Retractions?
how you would approach this newborn?how you would approach this newborn? What is your DD?What is your DD?

Case 1:ABCD first
APGAR SCOREAPGAR SCORE Resuscitation (NRP)Resuscitation (NRP) ABCDABCD Postnatal resuscitation.Postnatal resuscitation.

(Or 21%-100%)

Resuscitation Drugs
30 ml30 ml
20 ml20 ml
10 ml10 ml
Volume Expanders normal salinePacked red cells
6 ml4 ml2 mlGlucose D10WIV bolus200 mg/kgfor documentedhypoglycemia
0.75 ml0.5 ml0.25 mlNaloxone IV or IM0.4 mg/ml (0.1 mg/kg)
contraindicated in narcotic dependentmothers
12 ml8 ml4 mlSodium Bicarbonate IV4.2% (2 mmol/kg)0.5 mmol/ml for prolonged arrest
3 ml2 ml1 mlETT Route
(0.1 mg/kg)
0.3 ml0.2 ml0.1 mlIV Route
(Preferred route)
(0.01 mg/kg)
Epinephrine1:10,000 0.1 mg/mlq3-5 minutes
3 kg> 36 weeks
2 kg30-36 weeks
1 kg< 30 weeks
Differential Diagnosis
RDSRDS TTNTTN InfectionInfection MAMA

Respiratory Distress Syndrome (RDS)
Surfactant Production?Surfactant Production? ComplicationsComplications
Risk Factors
Premature babiesPremature babies Previous baby with RDSPrevious baby with RDS Maternal diabetesMaternal diabetes HypothermiaHypothermia Fetal Distress AsphyxiaFetal Distress Asphyxia Male sexMale sex Caucasian raceCaucasian race Second twinSecond twin C/S with out laborC/S with out labor


Signs of Respiratory Distress
Grunting Grunting Tachypnea (RR >60/m)Tachypnea (RR >60/m) Nasal flaring, chest indrawingNasal flaring, chest indrawing
Apnea
Obstructive Apnea:No air flow but the Obstructive Apnea:No air flow but the chest wall movements continuechest wall movements continue
Central Apnea:Central Apnea:
Complete cessation of airflow and Complete cessation of airflow and respiratory airflow and respiratory efforts respiratory airflow and respiratory efforts with no chest wall movementwith no chest wall movement
Mixed Apnea (Is the most frequent type)Mixed Apnea (Is the most frequent type)

CyanosisCyanosis
Deoxygenated hemoglobin is 5 g/dlDeoxygenated hemoglobin is 5 g/dl Types?Types? ACROCYANOSIS: blue color of the hands ACROCYANOSIS: blue color of the hands
and feet with pink color of the rest of the and feet with pink color of the rest of the body, common in delivery room and is body, common in delivery room and is usually NORMALusually NORMAL

Other Routine Delivery Room CareRoutine Delivery Room Care
Erythromycin eye drops?Erythromycin eye drops? Vitamin K IM?Vitamin K IM?
Case 2
You are called to attend a delivery for You are called to attend a delivery for baby with Meconuim liquor?baby with Meconuim liquor?
What you do first?What you do first?
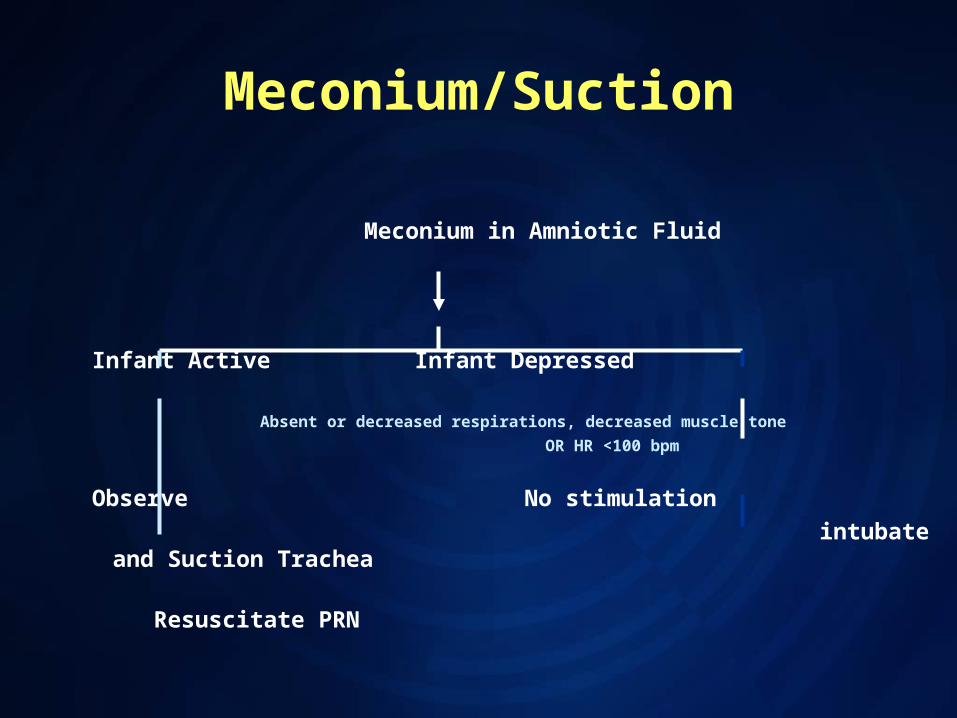
Meconium/Suction
Meconium in Amniotic Fluid
Infant Active Infant Depressed
Absent or decreased respirations, decreased muscle tone
OR HR <100 bpm
Observe No stimulation
intubate and Suction Trachea
Resuscitate PRN
Depressed Meconium baby

MAS

MAS
Radiological appearance:Radiological appearance:
1-overexpanded lungs.1-overexpanded lungs.
2-coarse air space infiltrates.2-coarse air space infiltrates.
3-Wide spread consolidation.3-Wide spread consolidation.
4-+/-airleakage.4-+/-airleakage.
MAS and HIE !
The baby is born now and he is flat with The baby is born now and he is flat with Apgar score of ZERO?Apgar score of ZERO?
How do you proceed?How do you proceed?

Meconium Aspiration Syndrome
Complications:Complications: Severe Resp. failureSevere Resp. failure HIEHIE PPHN(persistent pulmonary hypertension)PPHN(persistent pulmonary hypertension) Pulmonary air leak Pulmonary air leak

Effect Of Asphyxia(HIE)Effect Of Asphyxia(HIE)
CNSCNS CVSCVS PulmonaryPulmonary RenalRenal AdrenalAdrenal GITGIT MetabolicMetabolic HematologyHematology

Treatment
ResuscitationResuscitation Post resuscitation:Post resuscitation:
Depend on severity(stage3 is the worst)Depend on severity(stage3 is the worst) Fluids restrictionsFluids restrictions O2 and ventilationO2 and ventilation InotropsInotrops Anti seizure medicationAnti seizure medication

Primary Pulmonary Hypertension of the Newborn (PPHN)
Severe hypoxemia, with out evidence of Severe hypoxemia, with out evidence of parenchymal lung or structural heart parenchymal lung or structural heart disease that also may cause right to left disease that also may cause right to left shunting.shunting.
Often seen in term or post-term infants Often seen in term or post-term infants who are asphyxiated or meconium stained who are asphyxiated or meconium stained fluidfluid

Case2
You are called to assess the same baby You are called to assess the same baby with MAS because of worsning respiartory with MAS because of worsning respiartory status and sudden status and sudden desaturation ,bradycardia and desaturation ,bradycardia and hypotension?hypotension?
What is your approach?What is your approach?

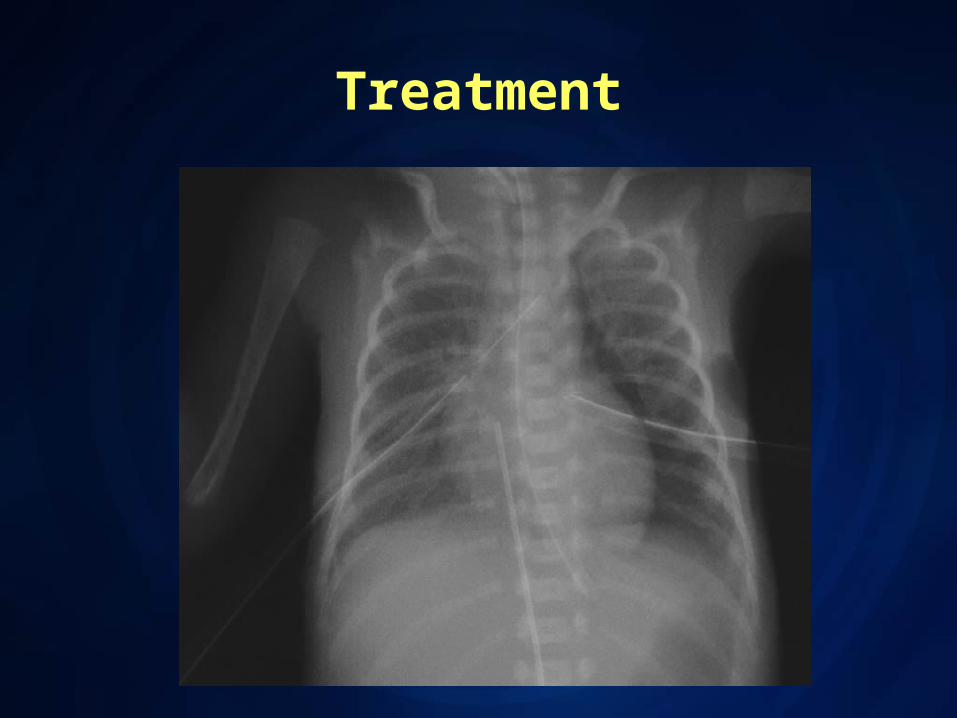
Treatment
Other Pulmonary Air Leaks
Pulmonary Interstitial Emphysema (PIE)Pulmonary Interstitial Emphysema (PIE) PneumomediastinumPneumomediastinum Subcutaneous EmphysemaSubcutaneous Emphysema PneumopericardiumPneumopericardium
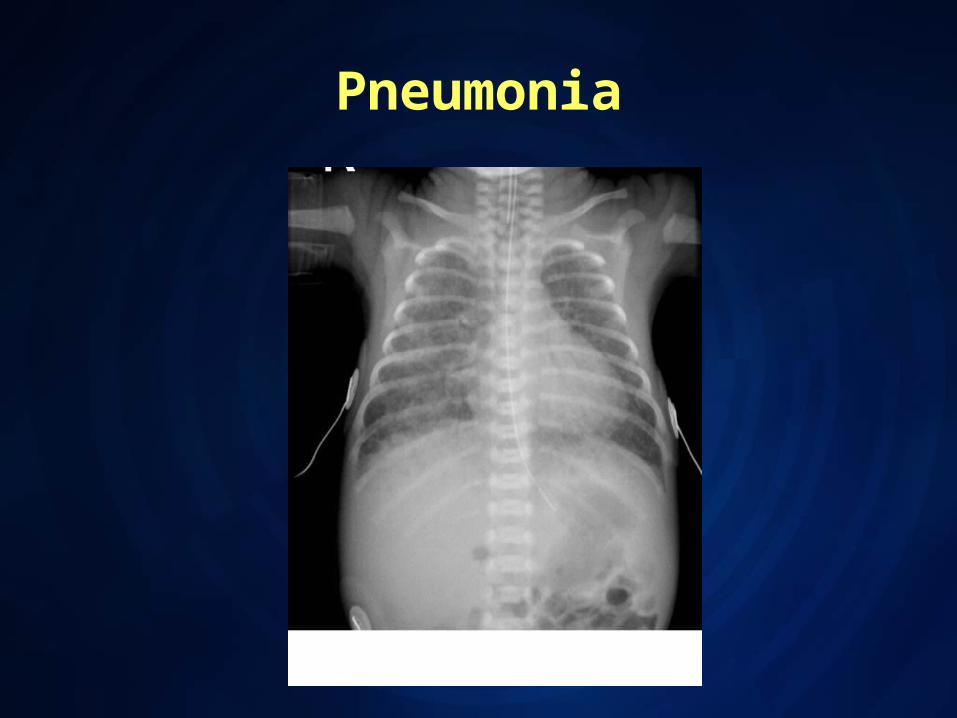
Pneumonia
Pneumonia
Early Vs Late.Early Vs Late. Diagnosis is impossible from XR alone.Diagnosis is impossible from XR alone. frank lobar consolidation as seen in adults frank lobar consolidation as seen in adults
and older children is rare and older children is rare More commonly, there is coarse opacity of More commonly, there is coarse opacity of
one or more regions of the lung one or more regions of the lung parenchyma parenchyma
Transient Tachypnoea of the Newborn
Typically, respiratory symptoms resolve Typically, respiratory symptoms resolve within the first 24-hours of life, but within the first 24-hours of life, but occasionally can persist longer. occasionally can persist longer.
Typical radiologic features:Typical radiologic features: Increased central vascular markings Increased central vascular markings
Hyperaeration Hyperaeration Evidence of interstitial and pleural fluid Evidence of interstitial and pleural fluid Prominent interlobar fissures Prominent interlobar fissures


We Talked about!
Algorithm for neonatal resuscitation and Algorithm for neonatal resuscitation and Delivery room managementDelivery room management
Approach & DD of an infant with Approach & DD of an infant with Respiratory distressRespiratory distress
Effect of MAS and birth asphyxiaEffect of MAS and birth asphyxia




![A Cone-Based Distributed Topology-Control Algorithm for Wireless Multi-Hop … · 2018-01-04 · Algorithm for Wireless Multi-Hop Networks Li (Erran) Li ... et al. [7] describe an](https://static.fdocuments.in/doc/165x107/5f37c43e4da5c84b564be69e/a-cone-based-distributed-topology-control-algorithm-for-wireless-multi-hop-2018-01-04.jpg)














