Critical Care update - Physiotherapy Alberta · Respiratory physiotherapy in critical care...
25
1/24/2018 1 Critical Care update Shane Patman President, International Confederation of Cardiorespiratory Physical Therapists Associate Professor, School of Physiotherapy Session outline • The role of the physiotherapist in the ICU. • The evidence to support the interventions that physiotherapists implement with the ICU patient population. • The evidence regarding which patients benefit, and which patients may not benefit, from physiotherapy in this setting. • The evidence regarding the risks of physiotherapy interventions in ICU. • Best practices for mitigating these risks and safely intervening in this practice environment. 2
Transcript of Critical Care update - Physiotherapy Alberta · Respiratory physiotherapy in critical care...
1/24/2018
1
Critical Care update
Shane PatmanPresident, International Confederation of Cardiorespiratory Physical Therapists
Associate Professor, School of Physiotherapy
Session outline
• The role of the physiotherapist in the ICU.
• The evidence to support the interventions that physiotherapists implement with the ICU patient population.
• The evidence regarding which patients benefit, and which patients may not benefit, from physiotherapy in this setting.
• The evidence regarding the risks of physiotherapy interventions in ICU.
• Best practices for mitigating these risks and safely intervening in this practice environment.
2

1/24/2018
2
Critical care admission = Major life event
3Iwashyna T (2012). AJRCCM 186(4) https://doi.org/10.1164/rccm.201206-1138ED
Koo, Choong & Fan (2011) Prioritizing rehabilitation strategies in the care of the critically ill. Critical Care Rounds 8(4) http://www.canadiancriticalcare.org/resources/Pictures/ccroundsv8i4_11.pdf

1/24/2018
3
Truong A, et al. (2009). 13:216 Crit Care https://doi.org/10.1186/cc7885
Consequences of critical care
5
Critical care admission = Major life event
Iwashyna T (2012). AJRCCM 186(4) https://doi.org/10.1164/rccm.201206-1138ED 6

1/24/2018
4
Respiratory physiotherapy in critical care• Respiratory physiotherapy interventions are generally aimed to facilitate airway clearance, optimise lung volumes, enhance gas exchange, and reduce work of breathing.
• Techniques may include positioning, manual and ventilator hyperinflation (MHI & VHI), percussion, vibration, suctioning, respiratory muscle strengthening, breathing exercises and mobilisation, along with education, weaning from mechanical ventilation and non‐invasive ventilation.
• Multimodal respiratory physiotherapy treatment as practiced by physiotherapists is considered safe.
• Insufficient evidence‐based to date to support respiratory physiotherapy as a distinct part of respiratory care in MV patients
• published studies are all small‐sized, insufficiently powered, conducted in a variety of populations and utilising different treatments and various clinical endpoints
• not proven to influence relevant ICU outcome parameters
Berney S, Haines K, Denehy L (2012); Spapen HD, De Regt J, Honoré PM (2017)7
Evidence?• Gosselink, R., Bott, J., Johnson, M., Dean, E., Nava, S., Norrenberg, M., & ... Vincent, J. L. (2008). Physiotherapy for adult patients with critical illness: recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Medicine, 34(7), 1188‐1199. https://doi.org/10.1007/s00134‐008‐1026‐7
• Evidence from randomized controlled trials or meta‐analyses was limited and most of the recommendations were level C (evidence from uncontrolled or nonrandomized trials, or from observational studies) and D (expert opinion).
• Stiller, K. (2013). Physiotherapy in intensive care: an updated systematic review. Chest, 144(3), 825‐847. http://dx.doi.org/10.1378/chest.12‐2930
• The evidence from RCTs evaluating the effectiveness of routine multimodality respiratory physiotherapy is conflicting
8

1/24/2018
5
Respiratory physiotherapy in critical care
• There is reducing focus on the provision of respiratory treatment unless patients present with atelectasis and/or secretion retention
• May promote better “airway hygiene”
• May provide short term effects on oxygenation and ventilation
• Techniques should not be performed routinely but only if considered to be appropriate and useful in selected patients.
Berney S, Haines K, Denehy L (2012); Spapen HD, De Regt J, Honoré PM (2017)
9
Physiotherapy in Critical Care“Physiotherapy is an important intervention that prevents and mitigates adverse effects of
prolonged bed rest and mechanical ventilation during critical illness.
Rehabilitation delivered by the physiotherapist is tailored to patient needs and depends on
conscious state, psychological status and physical strength.
It incorporates any active and passive therapy that promotes movement and includes
mobilisation.
Early progressive physiotherapy, with a focus on mobility and walking whilst ventilated, is
essential in minimising functional decline.
If this process does not occur within the critical care environment, there are increased costs of
service provision to the health system, as these patients often require extensive periods of
rehabilitation and follow‐up to meet long‐term disability needs as a result of critical illness.”
http://www.csp.org.uk/publications/physiotherapy‐works‐critical‐care
10
1/24/2018
6
Benefits of early rehabilitation in ICU
• There is a growing body of evidence to support programmes of early mobilisation within ICU
• When utilised, early mobility is associated with reduced ICU and hospital length of stay and improved functional outcomes.
• evidence to show patients do show a response to exercise and can therefore be trained
• shorter duration of delirium
• improved weaning from MV, with more ventilator‐free days
• reduced muscle atrophy
• improved strength and independence with functional ADLs
• The exact definition of early mobility is still not defined, and actual ability to mobilise can be limited
11
Denehy, L., Lanphere, J. & Needham, D.M. Ten reasons why ICU patients should be mobilized early. Intensive Care Med (2017) 43: 86.
https://doi.org/10.1007/s00134‐016‐4513‐2
• Attenuates complications of bed rest
• Addresses sequelae of ICU‐acquired weakness
• Perceived barriers are modifiable
• Implementation is feasible
• Promotes reduction of sedation
• It is safe
• Promotes improved functional outcomes with early start
• May improve delirium
• New technologies expand opportunities
• May reduce overall resource utilization12

1/24/2018
7
What is early rehabilitation?Passive Techniques
• Passive movements / CPM
• Stretching
• Splinting
• Passive cycling
• NMES (electrical muscle stimulation)
• Tilt tabling / moveo
Active Techniques
• Exercise therapy
• Cycle ergometry
• Interactive video games
• IMT
• ADL training
• Out of bed / functional mobilisation
https://youtu.be/woofpnw‐u74
13
See: Sommers, J., Engelbert, R. H., Dettling‐Ihnenfeldt, D., Gosselink, R., Spronk, P. E., Nollet, F., & van der Schaaf, M. (2015). Physiotherapy in the intensive care unit: an evidence‐based, expert driven, practical statement and rehabilitation recommendations. Clinical Rehabilitation, 29(11), 1051‐1063. doi:10.1177/0269215514567156
Exercise Prescription for critically ill• Based on functional capability and ability to tolerate activity
• Progressive phases with guidelines:
• positioning
• exercise type
• transfers
• gait retraining
• education
• FITT, SMART considerations / framework
• MDT effort
14
Source: http://i.ytimg.com/vi/TasqmU4yK8w/maxresdefault.jpg
See also: https://youtu.be/rAEjjcjob‐Y

1/24/2018
8
Electrical Muscle Stimulation• very low to low quality evidence of the beneficial effects of EMS delivered in the ICU for improving muscle strength, muscle structure and critical illness polyneuropathy/myopathy
• Electrical muscle stimulation appears to preserve muscle mass and strength in long‐stay participants and in those with less acuity. No such benefits were observed when commenced prior to 7 days or in patients with high acuity.
• Minimal adverse events reported.
• Optimal training variables and safety of the intervention require further investigation.
Connolly, B., O'Neill, B., Salisbury, L., & Blackwood, B. (2016). Physical rehabilitation interventions for adult patients during critical illness: an overview of systematic reviews. Thorax, 71(10), 881‐890. https://doi.org/10.1136/THORAXJNL‐2015‐208273
Hermans, G., De Jonghe, B., Bruyninckx, F., & Van den Berghe, G. (2014). Interventions for preventing critical illness polyneuropathy and critical illness myopathy. The Cochrane Database Of Systematic Reviews, (1),
Edwards, J., McWilliams, D., Thomas, M., & Shah, S. (2014). Electrical Muscle Stimulation in the Intensive Care Unit: An Integrative Review. Journal of the Intensive Care Society, 15(2): 142‐9. https://doi.org/10.1177/175114371401500212
Parry, S. M., Berney, S., Granger, C. L., Koopman, R., El‐Ansary, D., & Denehy, L. (2013). Electrical muscle stimulation in the intensive care setting: a systematic review. Critical Care Medicine, 41(10), 2406‐2418. https://doi.org/10.1097/CCM.0b013e3182923642
Cycle ErgometryKho, M. E., Molloy, A. J., Clarke, F. J., Ajami, D., McCaughan, M., Obrovac, K., & ... Cook, D. J. (2016). TryCYCLE: A
Prospective Study of the Safety and Feasibility of Early In‐Bed Cycling in Mechanically Ventilated Patients. Plos One, 11(12). https://doi.org/10.1371/journal.pone.0167561
• 30 minutes of in‐bed supine cycling 6 days/week in the ICU
• Cycling termination was infrequent (2.0%, 95% CI: 0.8%‐4.9%) and no device dislodgements occurred.
• Early cycling within the first 4 days of MV among hemodynamically stable patients is safe and feasible. Research to evaluate the effect of early cycling on patient function is warranted.
Kho ME, Molloy AJ, Clarke F, et al. CYCLE pilot: a protocol for a pilot randomised study of early cycle ergometry versus routine physiotherapy in mechanically ventilated patients. BMJ Open 2016;6:e011659.
https://doi.org/10.1136/bmjopen‐2016‐011659
Nickels, M. R., Aitken, L. M., Walsham, J., Barnett, A. G., & McPhail, S. M. (2017). Critical Care Cycling Study (CYCLIST) trial protocol: a randomised controlled trial of usual care plus additional in‐bed cycling sessions
versus usual care in the critically ill. BMJ Open, 7(10), e017393. https://doi.org/10.1136/bmjopen‐2017‐017393

1/24/2018
9
Cycle Ergometry
17Gosselink, R et al Neth J Crit Care 2011:15(2) pg69
18
Gosselink, R et al. Neth J Crit Care 2011:15(2) pg70
Ambrosino et al Rev Port Pneumol. 2011;17(6):283‐288
https://www.worldnewsmd.com/Video/Physical%20Therapy/7News‐‐‐Sleep‐cycle‐helping‐patients

1/24/2018
10
Inspiratory Muscle Training
• Inspiratory muscle training for selected patients in the ICU facilitates weaning, with potential reductions in length of stay and the duration of non‐invasive ventilatory support after extubation.
• The heterogeneity among the results suggests that the effects of IMT may vary; this perhaps depends on factors such as the components of usual care or the patient's characteristics.
Elkins, M., & Dentice, R. (2015). Inspiratory muscle training facilitates weaning from mechanical ventilation among patients in the intensive care unit: a systematic review. Journal
of Physiotherapy, 61(3), 125‐134 http://dx.doi.org/10.1016/j.jphys.2015.05.016
Rehabilitation activities – linking research to practice
Lai, Chih‐Cheng et al (2017). Early mobilization reduces duration of mechanical ventilation and intensive care unit stay in patients with acute respiratory
failure. Arch Phys Med Rehab 98(5): 931‐939. http://dx.doi.org/10.1016/j.apmr.2016.11.007
• MDT protocol, within 72 hrs of MV & CVS stable
• 4 levels of the protocol: level 1 ‐ passive extremities movement; level 2 ‐active extremities movement; level 3 ‐ a sitting position on the bed; and level 4 ‐ move from the bed to a chair beside the bed.
• twice daily, 5 days/wk during family visit, 30 minutes each
• shorter MV durations (4.7d vs 7.5d; P<.001)
• shorter ICU stays (6.9d vs 9.9d; P=.001)

1/24/2018
11
Lai et al (2017). Arch Phys Med Rehab. 98(5): 931–939
What is the latest evidence saying?Tipping C et al (2017) The effects of active mobilisation and rehabilitation in ICU
on mortality and function: a systematic review. Intensive Care Med 43:171–183 https://doi.org/10.1007/s00134‐016‐4612‐0
• Active mobilisation and rehabilitation in the ICU has no impact on short‐ and
long‐term mortality, but may improve mobility status, muscle strength and days
alive and out of hospital to 180 days.
• There were no consistent effects on function, QoL, ICU or hospital length of stay, duration of MV, or discharge destination
22

1/24/2018
12
Early Rehabilitation ‐ Safety
Hodgson, C. L., Stiller, K., Needham, D. M., Tipping, C. J., Harrold, M., Baldwin, C. E., ... & Green, M. (2014). Expert consensus and recommendations on safety
criteria for active mobilization of mechanically ventilated critically ill adults. Critical Care, 18(6), 658. https://doi.org/10.1186/s13054‐014‐0658‐y
http://ccforum.com/content/18/6/658

1/24/2018
13
Nydahl P et al (2017). Safety of Patient Mobilization and Rehabilitation in the ICU: Systematic Review with Meta‐Analysis.
Annals ATS 14(5): 766‐777. https://doi.org/10.1513/AnnalsATS.201611‐843SR
• 48 studies of 7546 patients, with 583 potential safety events occurring in 22,351 mobilization/rehabilitation sessions.
• Total of 583 (2.6%) potential safety events, with heterogeneity in the definitions for these events
• pooled incidences per 1,000 mobilization/rehabilitation sessions (95% CI)
• hemodynamic changes, 3.8 (1.3–11.4)
• desaturation, 1.9 (0.9–4.3)
• Consequences (e.g. needing to increase dose of vasopressor due to mobility‐related hypotension):
• a frequency of 0.6% in 14,398 mobilization/rehabilitation sessions
• Patient mobilization and physical rehabilitation in the ICU appears safe with a low incidence of potential safety events, and only rare events having any consequences for patient management.
25
Boyd, J., Paratz, J., Tronstad, O., Caruana, L., McCormack, P., & Walsh, J. (2017). When is it safe to exercise mechanically ventilated patients in the intensive care unit? An evaluation of consensus recommendations in a cardiothoracic setting.
Heart & Lung: The Journal Of Critical Care, http://dx.doi.org/10.1016/j.hrtlng.2017.11.006
• 91 mechanically ventilated participants; 54 (59.3%) male; mean age of 56.52 (16.3) years; were studied with 809 occasions of service recorded.
• Ten (0.0182%) minor adverse events were recorded, with only one adverse event occurring when a patient was receiving moderate level of vasoactive support.
Conclusions: The consensus recommendations are a useful tool in guiding safe exercise rehabilitation of mechanically ventilated patients. Our findings suggest that there is further scope to safely commence exercise rehabilitation in patients receiving vasoactive support.
26

1/24/2018
14
Early mobilisation in ICU is far more than just exercise
• The critical care environment presents many challenges and opportunities in linking research to practice
• early mobilisation in the ICU is a complex intervention demanding interdisciplinary coordination and communication.
• much of the physiotherapists’ time goes into preparing patients for physiotherapy
• prevention’s goal is the modest retention of function, rather than ambitious rebuilding in patients who have already lost some functioning abilities.
But which patients to target? Which prescription? What is success?
Iwashyna, T. J., & Hodgson, C. L. (2016). Early mobilisation in ICU is far more than just exercise. Lancet (London, England), 388(10052), 1351‐1352. http://dx.doi.org/10.1016/S0140-6736(16)31745-7 27
Source: Hodgson C, Tipping C Physiotherapy management of intensive care unit‐acquired weakness Journal of Physiotherapy, Volume 63, Issue 1, 2017, 4–10 http://dx.doi.org/10.1016/j.jphys.2016.10.011
Interventions for management of ICU‐AW, with associated levels of evidence.
28

1/24/2018
15
Bakhru, R. N., McWilliams, D. J., Wiebe, D. J., Spuhler, V. J., & Schweickert, W. D. (2016). Intensive Care Unit Structure Variation and Implications for Early Mobilization Practices. An
International Survey. Annals Of The American Thoracic Society, 13(9), 1527‐1537. https://doi.org/10.1513/AnnalsATS.201601‐078OC
• International ICU structure and practice is quite heterogeneous, and several
factors (multidisciplinary rounds, setting daily goals for patients, presence of a
dedicated physiotherapist, country, and nurse/patient staffing ratio) are
significantly associated with the practice of early mobility.
• Practice and barriers may be far different based upon staffing structure.
• To achieve successful implementation, whether through trials or quality
improvement, ICU staffing and practice patterns must be taken into account.
29
Bear, D. E., Parry, S. M., & Puthucheary, Z. A. (2017). Can the critically ill patient generate sufficient energy to facilitate exercise in the ICU?. Current Opinion In
Clinical Nutrition And Metabolic Care, https://doi.org/10.1097/MCO.0000000000000446
• The metabolic demands of exercise are poorly understood in the ICU setting.
• Recent research has highlighted that there is significant heterogeneity in energy requirements between critically ill individuals undertaking the same functional activities, such as sit‐to‐stand.
• Nutrition in the critically ill is currently thought of in terms of carbohydrates, fat and protein. It may be that we need to consider nutrition in a more contextual manner such as energy generation or management of protein homeostasis.
• Current nutritional support practices in critically ill patients do not lead to improvements in physical and functional outcomes, and it may be that alternative methods of delivery or substrates are needed
30

1/24/2018
16
Roberson, A. R., Starkweather, A., Grossman, C., Acevedo, E., & Salyer, J. (2018). Influence of muscle strength on early mobility in critically ill adult
patients: Systematic literature review. Heart & Lung: The Journal Of Critical Care, 47(1), 1‐9. https://doi.org/10.1016/j.hrtlng.2017.10.003
• Immobility and muscle deconditioning impact early mobilization in the ICU setting.
• Muscle strength in critically ill patients can be measured as a clinical assessment.
• Integrating muscle strength tests, interprofessional engagement and patient assessment optimizes patient outcomes.
• Research is required on the influence of muscle strength on early mobility.
31
Physical Function Assessment Tools• ICU Mobility Scale (IMS)
• Chelsea Critical Care Physical Assessment tool (CPAx)
• Physical Function ICU Test (Scored) (PFIT‐s)
• Functional Status Score for the Intensive Care Unit (FSS‐ICU)
• de Morton Mobility Index (DEMMI)
• Perme ICU Mobility Score
• Surgical Intensive Care Unit Optimal Mobilization Score (SOMS)
• Acute Care Index of Function (ACIF)
• Short Physical Performance Battery (SPPB)
• Functional Capacity Scale (FCS)
• Early Functional Abilities Scale (EFA)
• Functional Independence Measure (FIM)
• Barthel Index 32
Summary information about many of these instruments (including how to access and use them) is available:
http://www.improvelto.com/
and/or Parry et al. Critical Care (2017) 21:249https://doi.org/10.1186/s13054‐017‐1827‐6

1/24/2018
17
• The evaluation of physical functioning is valuable in the ICU to help inform patient recovery after critical illness, to identify patients who may require rehabilitation interventions, and to monitor responsiveness to such interventions.
• This viewpoint article discusses:
1. the concept of physical functioning with reference to the WHO International Classification of Functioning, Disability and Health;
2. the importance of measuring physical functioning in the ICU; and
3. methods for evaluating physical functioning in the ICU.
• Recommendations for clinical practice and research are made, along with discussion of future directions.
Crit Care (2017); 21:249 http://dx.doi.org/10.1186/s13054‐017‐1827‐6
33
Recommendations
• Screening for mental capacity should commence from ICU admission and include assessments of pain, sedation, and delirium status.
• Regular screening for muscle weakness using the Medical Research Council sum‐score recommend .
• Identification of patients who need evaluation of physical functioning in the ICU is largely reliant on clinical judgment regarding many potential risk factors.
• Once the patient can follow commands, at a minimum, use of one of four physical functioning tools is recommended:
1. Physical Functional in ICU Test‐scored;
2. Chelsea Critical Care Physical Assessment Tool;
3. Functional Status Score for the ICU; and
4. ICU Mobility scale.
Parry, Huang & Needham 2017 34

1/24/2018
18
ICU Mobility Scale (IMS)
35
Classification Definition
0 Nothing (lying in bed) Passively rolled or passively exercised by staff, but not actively moving
1 Sitting in bed, exercises in bed Any activity in bed, including rolling, bridging, active exercises, cycle ergometry and active assisted exercises; not moving out of bed or over the edge of the bed
2 Passively moved to chair (no standing) Hoist, passive lift or slide transfer to the chair, with no standing or sitting on the edge of the bed
3 Sitting over edge of bed May be assisted by staff, but involves actively sitting over the side of the bed with some trunk control
4 Standing Weight bearing through the feet in the standing position, with or without assistance. This may include use of a standing lifter device or tilt table.
5 Transferring bed to chair
Able to step or shuffle through standing to the chair. This involves actively transferring weight from one leg to another to move to the chair. If the patient has been stood with the assistance of a medical device, they must step to the chair (not included if the patient is wheeled in a standing lifter device.)
6 Marching on spot (at bedside)Able to walk on the spot by lifting alternate feet (must be able to step at least 4 times, twice on each foot), with or without assistance
7 Walking with assistance of 2 or more people Walking away from the bed/chair by at least 5 metres (5 yards) assisted by 2 or more people
8 Walking with assistance of 1 person Walking away from the bed/chair by at least 5 metres (5 yards) assisted by 1 person
9 Walking independently with a gait aid Walking away from the bed/chair by at least 5 metres (5 yards) with a gait aid, but no assistance from another person. In a wheelchair bound person, this activity level includes wheeling the chair independently 5 metres (5 years) away from the bed/chair
10 Walking independently without a gait aidWalking away from the bed/chair by at least 5 metres (5 yards) without a gait aid or assistance from another person.
Heart & Lung 43 (2014) 19e24 https://doi.org/10.1016/j.hrtlng.2013.11.003
36
Corner E et al (2014) Critical Care. 18:R55https://doi.org/10.1186/cc13801

1/24/2018
19
Chelsea Critical Care Physical Assessment tool (CPAx)
Chelsea Critical Care Physical Assessment tool (CPAx)
1/24/2018
20
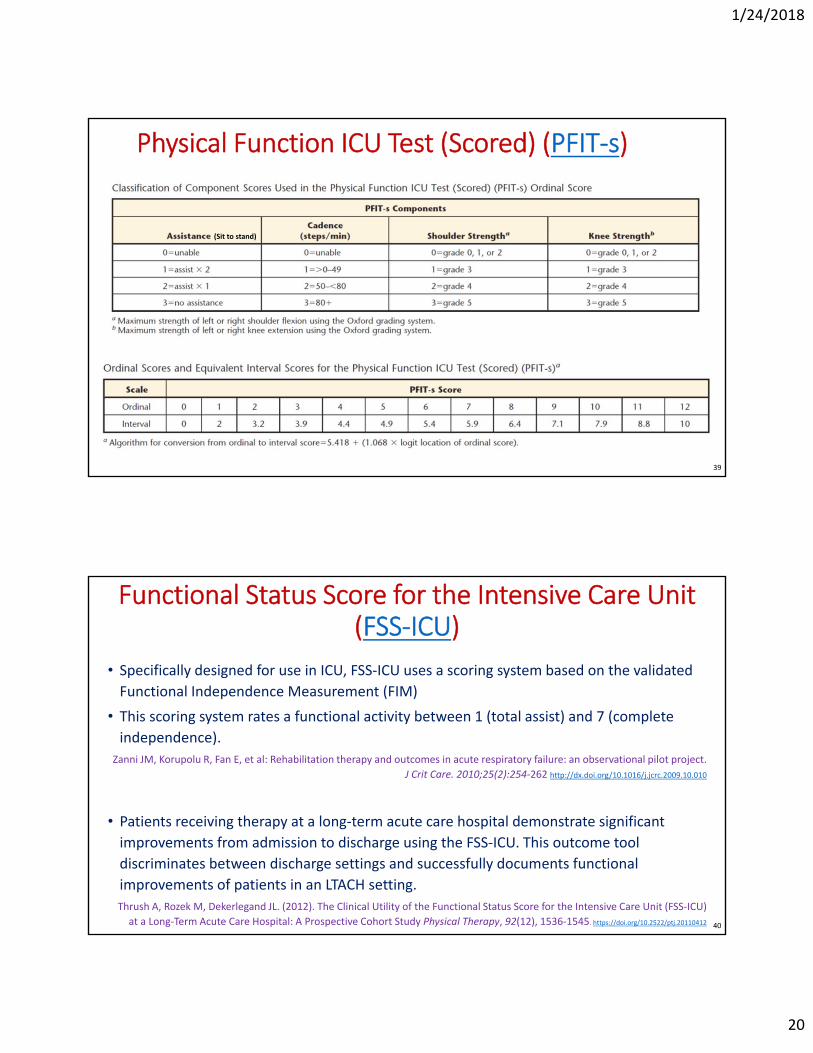
Physical Function ICU Test (Scored) (PFIT‐s)
39
(Sit to stand)
Functional Status Score for the Intensive Care Unit (FSS‐ICU)
• Specifically designed for use in ICU, FSS‐ICU uses a scoring system based on the validated
Functional Independence Measurement (FIM)
• This scoring system rates a functional activity between 1 (total assist) and 7 (complete
independence).
Zanni JM, Korupolu R, Fan E, et al: Rehabilitation therapy and outcomes in acute respiratory failure: an observational pilot project.
J Crit Care. 2010;25(2):254‐262 http://dx.doi.org/10.1016/j.jcrc.2009.10.010
• Patients receiving therapy at a long‐term acute care hospital demonstrate significant
improvements from admission to discharge using the FSS‐ICU. This outcome tool
discriminates between discharge settings and successfully documents functional
improvements of patients in an LTACH setting.
Thrush A, Rozek M, Dekerlegand JL. (2012). The Clinical Utility of the Functional Status Score for the Intensive Care Unit (FSS‐ICU)
at a Long‐Term Acute Care Hospital: A Prospective Cohort Study Physical Therapy, 92(12), 1536‐1545. https://doi.org/10.2522/ptj.20110412 40

1/24/2018
21
FSS‐ICU
The FSS‐ICU consists of five categories:
• rolling
• supine to sit transfers
• unsupported sitting
• sit to stand transfers
• ambulation
Each category was rated from zero to
seven with a maximum cumulative FSS‐
ICU score of 35.
0 = unable to perform
1 = total assistance
2 = maximum assistance
3 = moderate assistance
4 = minimal assistance
5 = supervision
6 = moderate independence
7 = complete independence
However,… Point prevalence data
Australia & New Zealand
• 18% of patients walked
• 23% of pts in ICU for ≥7 days ‐ not
SOEOB or walked
• 30% of patients with 02 therapy walked
Berney et al 2013
Germany
• 24% of patients mobilised out of bed
• 8% on MV were mobilised
• 4% stood, marched or walked
Nydahl et al 2014
USA (across 2 days; acute resp failure)
• 32% mobility (PT/OT provided)
• Non‐MV 48% vs MV 26%
• 16% on MV achieved out of bedJolley et al 2017
Switzerland (45% all ICUs)
• 33% on MV were actively mobilized
• 2% on MV walked
• 20% potential safety events (nsd passive vs. active)
Sibilla et al 2017
42

1/24/2018
22
Connolly, B. A., Mortimore, J. L., Douiri, A., Rose, J. W., Hart, N., & Berney, S. C. (2017). Low Levels of Physical Activity During Critical Illness and
Weaning: The Evidence‐Reality Gap. Journal Of Intensive Care Medicine, https://doi.org/10.1177/0885066617716377
• between 08:30am – 08:00pm, ICU patients spent a median (IQR) of 100% (96%‐100%) of the day (10.5 [10.0‐10.5] hours) located in bed, with minimal/no activity for 99% (96%‐100%) of the day.
• spent approximately two‐thirds of the day alone
• all physical activities occurred during physical rehabilitation sessions
• highlight the need for targeted strategies to improve levels beyond therapeutic rehabilitation and support for a culture shift toward providing patients with, and engaging them in, a multidisciplinary, multiprofessional environment that optimizes overall physical activity.
43
Parry, S. M., Knight, L. D., Connolly, B., Baldwin, C., Puthucheary, Z., Morris, P., & ... Granger, C. L. (2017). Factors influencing physical activity and
rehabilitation in survivors of critical illness: a systematic review of quantitative and qualitative studies. Intensive Care Medicine, 43(4), 531‐542.
• The main barriers identified were patient physical and psychological capability to perform physical activity, safety concerns, lack of leadership and ICU culture of mobility, lack of interprofessional communication, expertise and knowledge, and lack of staffing/equipment and funding to provide rehabilitation programs.
• Barriers and enablers are multidimensional and span diverse factors. The majority of these barriers are modifiable and can be targeted in future clinical practice.
44

1/24/2018
23
Need for continuity of care throughout continuum
Journal of Critical Care (2015); 30:242‐9 http://dx.doi.org/10.1016/j.jcrc.2014.10.017
• Informational needs change at different time points: Be specific
• Fear and worry persists when families do not know what to expect: more work is needed
from Phase 3
• Care givers need support to facilitate patient transition from dependence to
independence: up to 2 years after survival. Continued follow up – structured rehab45
Azoulay, E., Vincent, J., Angus, D. C., Arabi, Y. M., Brochard, L., Brett, S. J., & ... Herridge, M. (2017). Recovery after critical illness: putting the puzzle together‐a consensus of 29. Critical Care (London, England), 21(1), 296.
https://doi.org/10.1186/s13054‐017‐1887‐7
• highlights how critical illness and critical care affect longer‐term outcomes,
• underlines the contribution of ICU delirium to cognitive dysfunction several months after ICU discharge,
• gives new insights into ICU acquired weakness,
• emphasizes the importance of value‐based healthcare, and
• delineates the elements of family‐centered care.
46
1/24/2018
24
Physiotherapy in Critical Care update
Take‐home messages:
• Routine or prophylactic respiratory physiotherapy unsupported by literature
• Rehabilitation must be commenced within 3 days of ICU admission
• early mobility in patients diagnosed with sepsis may be an exception to this
• IMT during MV has benefit
• Early mobilisation in ICU is far more than just exercise
• Choice of Physical Function Assessment Tool important
• need to consider psychometric properties, utility of measure across continuum of care, & feasibility throughout all phases of recovery (based on your casemix)
• Expertise, multidisciplinary teamwork, leadership and workplace culture are key considerations
• There are many unanswered questions and therefore opportunities for collaborative research efforts
47
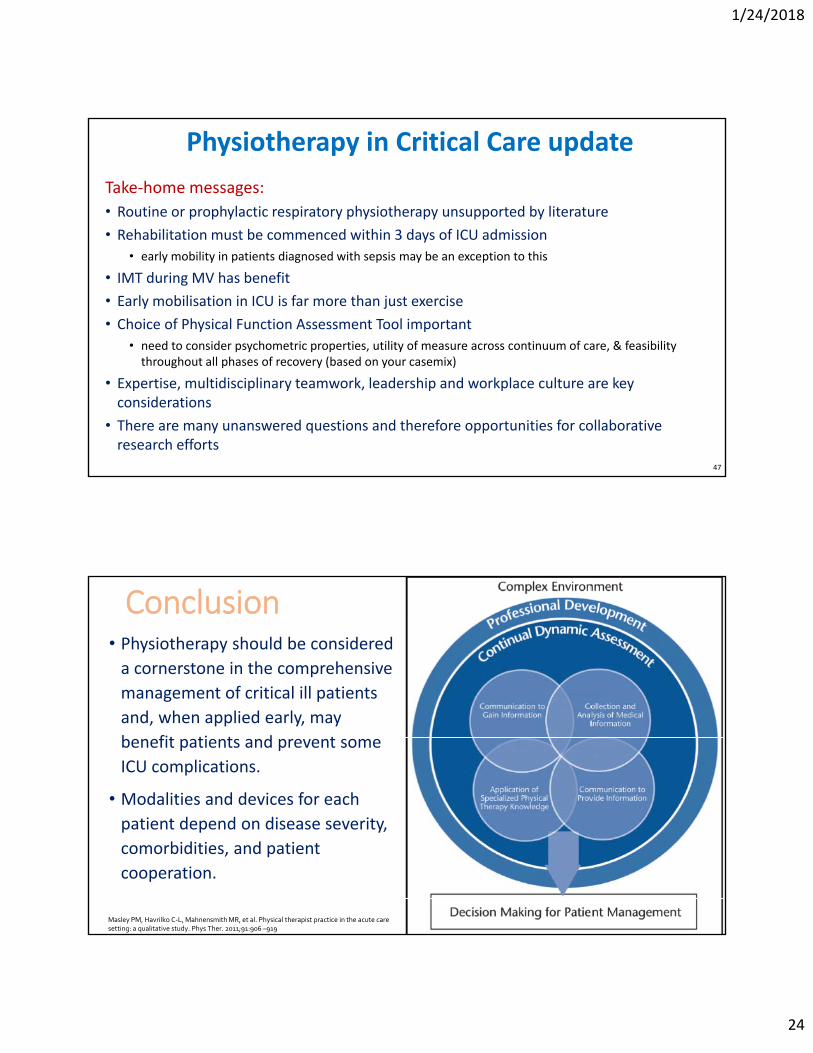
Conclusion• Physiotherapy should be considered a cornerstone in the comprehensive
management of critical ill patients
and, when applied early, may
benefit patients and prevent some
ICU complications.
• Modalities and devices for each
patient depend on disease severity,
comorbidities, and patient
cooperation.
Masley PM, Havrilko C‐L, MahnensmithMR, et al. Physical therapist practice in the acute care setting: a qualitative study. Phys Ther. 2011;91:906 –919

1/24/2018
25
Questions?
• Presenter contact details:
Shane Patman
Associate Professor, School of Physiotherapy
The University of Notre Dame Australia19 Mouat Street (PO Box 1225) Fremantle WA 6959 Australia
49