Digestion. Digestive System (Blank) Digestive System (Labeled)
https://doi.org/10.1530/ERC-20-0227https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.
27:10Endocrine-Related Cancer
L de Mestier et al. MGMT status in digestive NET R391–R405
-20-0227
REVIEW
Critical appraisal of MGMT in digestive NET treated with alkylating agents
Louis de Mestier 1,2, Anne Couvelard2,3, Anela Blazevic4, Olivia Hentic1, Wouter W de Herder 4, Vinciane Rebours1,2, Valérie Paradis2,3, Philippe Ruszniewski1,2, Leo J Hofland4 and Jérôme Cros 2,3
1Department of Gastroenterology-Pancreatology, ENETS Centre of Excellence, Beaujon University Hospital (APHP), and Université de Paris, Clichy, France2Centre of Research on Inflammation, INSERM U1149, Paris, France3Department of Pathology, ENETS Centre of Excellence, Bichat/Beaujon University Hospitals (APHP), and Université de Paris, Clichy/Paris, France4Division Endocrinology, Department of Internal Medicine, ENETS Centre of Excellence, Erasmus Medical Center, Rotterdam, The Netherlands
Correspondence should be addressed to L de Mestier: [email protected]
Abstract
The efficacy of alkylating agents (temozolomide, dacarbazine, streptozotocin) in patients with advanced neuroendocrine tumors (NETs) has been well documented, especially in pancreatic NETs. Alkylating agents transfer methyl adducts on DNA bases. Among them, O6-methylguanine accounts for many of their cytotoxic effects and can be repaired by the O6-methylguanine-methyltransferase (MGMT). However, whether the tumor MGMT status could be a reliable biomarker of efficacy of alkylating agents in NETs is still a matter of debate. Herein, we sought to provide a critical appraisal of the role of the MGMT status in NETs. After reviewing the molecular mechanisms of repair of DNA damage induced by alkylating agents, we aimed to comprehensively review the methods of determination of the MGMT status and its impact on prognosis, prediction of objective response and progression-free survival in patients with advanced digestive NETs treated by alkylating agents. About half of pancreatic NETs are MGMT-deficient, as determined by impaired tumor MGMT expression or by MGMT promoter methylation. Overall, while published studies are heterogeneous and mostly limited in size, they advocate that MGMT deficiency may be a relevant biomarker for increased objective response rate, prolonged progression-fee survival and overall survival in patients with advanced NETs treated by alkylating agents. While these data require confirmation in prospective controlled studies, future research should focus on the standardization of MGMT status assessment. Additional mechanisms of repair of DNA damages induced by alkylating agents should be explored in order to identify biomarkers complementary to MGMT and targets for potential antitumor synergy, such as PARP.
Introduction
Well-differentiated digestive neuroendocrine tumors (NETs) are associated with distant metastases in 60–80% of patients (Pavel et al. 2016). In these patients, therapeutic options include somatostatin analogs, cytotoxic or targeted agents, liver-directed therapies and
peptide-radionuclide receptor therapy (Frilling et al. 2014, Pavel et al. 2016). No clear recommendation exist regarding therapeutic sequences, given the lack of predictive biomarkers or trials comparing these treatments (Walter et al. 2012, Frilling et al. 2014, Pavel et al. 2016,
Endocrine-Related Cancer (2020) 27, R391–R405
10
Key Words
f neuroendocrine tumors
f DNA repair enzymes
f biomarkers
f antineoplastic agents/alkylating
f dacarbazine
f temozolomide
f streptozotocin
27
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R392L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
de Mestier et al. 2020a). Chemotherapy remains a therapeutic cornerstone as it can benefit to patients with aggressive tumors (i.e. progressive, with high tumor burden and/or high Ki67 index), or in a neoadjuvant setting aiming to obtain tumor shrinkage (Frilling et al. 2014, Pavel et al. 2016). Of note, chemotherapy is especially relevant in pancreatic NETs (PanNETs), which are more chemo-sensitive than intestinal NETs.
The most widely used chemotherapy regimens in PanNETs rely on alkylating agents, such as streptozotocin (STZ) (combined with 5-fluorouracil (5FU) or doxorubicin (Dilz et al. 2015, Clewemar Antonodimitrakis et al. 2016)), dacarbazine (DTIC) (alone or combined with 5FU (Walter et al. 2015, de Mestier et al. 2019)) and its oral prodrug temozolomide (TMZ) (alone or combined with capecitabine (CAP) (Koumarianou et al. 2015, de Mestier et al. 2020b). However, chemotherapy has been scarcely compared to other therapeutic options yet.
Although biomarkers predictive of the efficacy of alkylating agents would be of major interest in order to help selecting the best candidates, there is currently no such biomarker validated for clinical practice. Over the last decade, an increasing number of publications have explored whether the tumor expression of O6-methylguanine-DNA methyltransferase (MGMT) could influence the efficacy of alkylating agents (Koumarianou et al. 2015). However, the published studies were heterogeneous, with an inconstant association of low MGMT tumor expression with a better efficacy of TMZ (Kulke et al. 2009, Walter et al. 2015, Cros et al. 2016). Such discrepancies might be explained by methodological differences.
The objectives of this paper were to comprehensively review the evidence-based role of MGMT as a predictive biomarker of the efficacy of alkylating agents in digestive
well-differentiated NET and to draw perspective regarding its possible use in clinical practice. This review will mainly focus on PanNETs, which stand as the main indication of chemotherapy among digestive well-differentiated NET. To provide a comprehensive and up-to-date review, we searched PubMed, Web of Science and Google Scholar electronic databases for relevant articles published between 2000 and 2020, with no language restrictions, using the following keywords ‘neuroendocrine tumor’, ‘temozolomide’, ‘dacarbazine’, ‘streptozotocin’, ‘biomarker’, ‘O6-methylguanine-DNA methyltransferase’ and/or ‘MGMT’ and excluding case reports. Relevant studies were also identified through the bibliographic references of selected articles.
Reparation of DNA lesions induced by alkylating agents
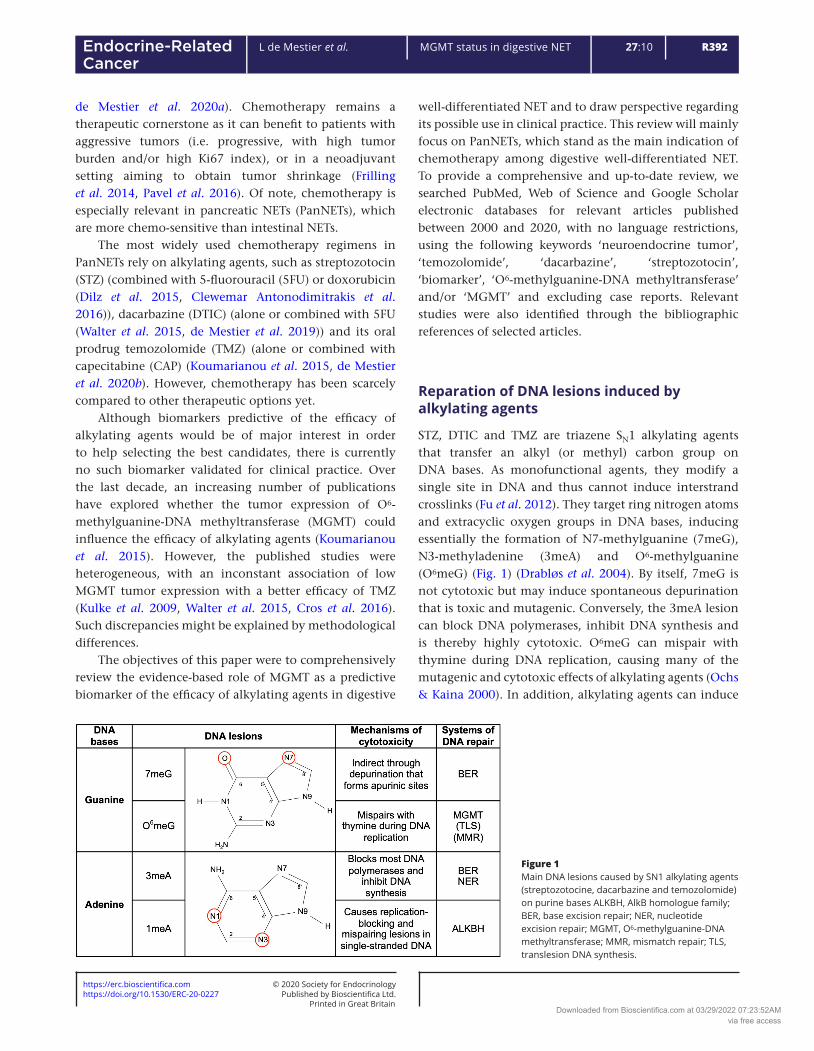
STZ, DTIC and TMZ are triazene SN1 alkylating agents that transfer an alkyl (or methyl) carbon group on DNA bases. As monofunctional agents, they modify a single site in DNA and thus cannot induce interstrand crosslinks (Fu et al. 2012). They target ring nitrogen atoms and extracyclic oxygen groups in DNA bases, inducing essentially the formation of N7-methylguanine (7meG), N3-methyladenine (3meA) and O6-methylguanine (O6meG) (Fig. 1) (Drabløs et al. 2004). By itself, 7meG is not cytotoxic but may induce spontaneous depurination that is toxic and mutagenic. Conversely, the 3meA lesion can block DNA polymerases, inhibit DNA synthesis and is thereby highly cytotoxic. O6meG can mispair with thymine during DNA replication, causing many of the mutagenic and cytotoxic effects of alkylating agents (Ochs & Kaina 2000). In addition, alkylating agents can induce
Figure 1Main DNA lesions caused by SN1 alkylating agents (streptozotocine, dacarbazine and temozolomide) on purine bases ALKBH, AlkB homologue family; BER, base excision repair; NER, nucleotide excision repair; MGMT, O6-methylguanine-DNA methyltransferase; MMR, mismatch repair; TLS, translesion DNA synthesis.
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access
https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R393L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
the methylation of N1-adenine (1meA) and N3-cytosine (3meC) in ssDNA (during replication, transcription or recombination), thereby causing replication-blocking and mispairing lesions (Fu et al. 2012).
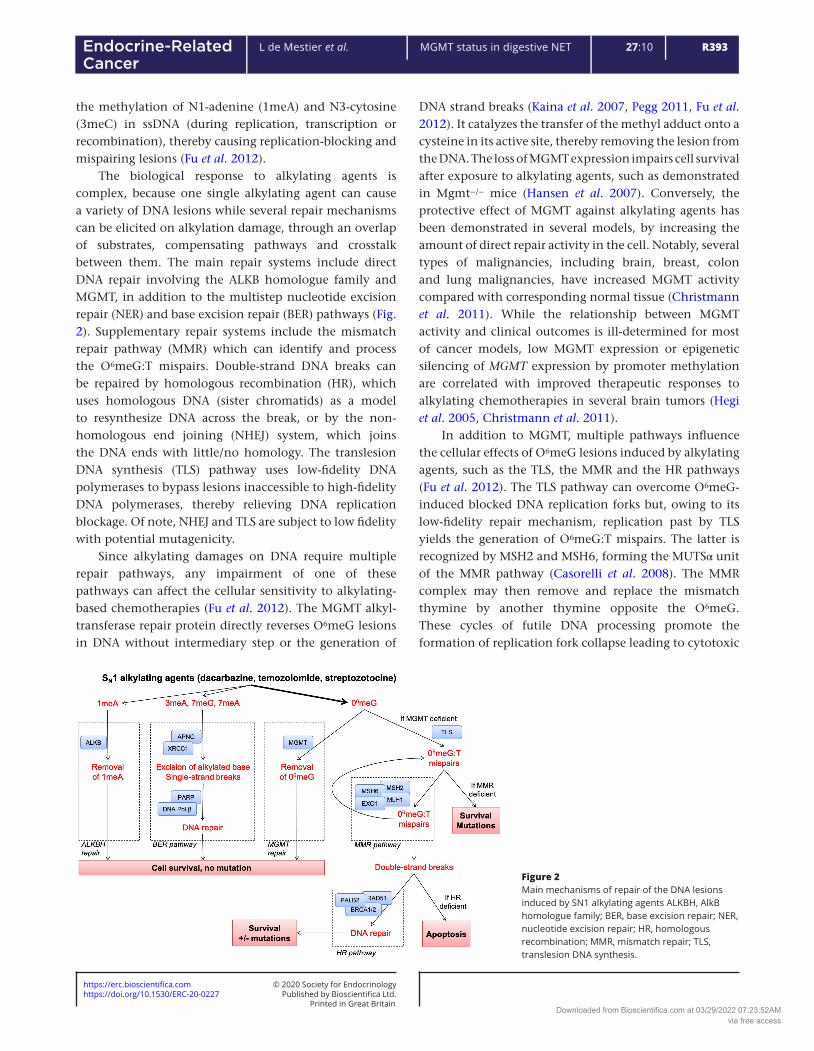
The biological response to alkylating agents is complex, because one single alkylating agent can cause a variety of DNA lesions while several repair mechanisms can be elicited on alkylation damage, through an overlap of substrates, compensating pathways and crosstalk between them. The main repair systems include direct DNA repair involving the ALKB homologue family and MGMT, in addition to the multistep nucleotide excision repair (NER) and base excision repair (BER) pathways (Fig. 2). Supplementary repair systems include the mismatch repair pathway (MMR) which can identify and process the O6meG:T mispairs. Double-strand DNA breaks can be repaired by homologous recombination (HR), which uses homologous DNA (sister chromatids) as a model to resynthesize DNA across the break, or by the non-homologous end joining (NHEJ) system, which joins the DNA ends with little/no homology. The translesion DNA synthesis (TLS) pathway uses low-fidelity DNA polymerases to bypass lesions inaccessible to high-fidelity DNA polymerases, thereby relieving DNA replication blockage. Of note, NHEJ and TLS are subject to low fidelity with potential mutagenicity.
Since alkylating damages on DNA require multiple repair pathways, any impairment of one of these pathways can affect the cellular sensitivity to alkylating-based chemotherapies (Fu et al. 2012). The MGMT alkyl-transferase repair protein directly reverses O6meG lesions in DNA without intermediary step or the generation of
DNA strand breaks (Kaina et al. 2007, Pegg 2011, Fu et al. 2012). It catalyzes the transfer of the methyl adduct onto a cysteine in its active site, thereby removing the lesion from the DNA. The loss of MGMT expression impairs cell survival after exposure to alkylating agents, such as demonstrated in Mgmt−/− mice (Hansen et al. 2007). Conversely, the protective effect of MGMT against alkylating agents has been demonstrated in several models, by increasing the amount of direct repair activity in the cell. Notably, several types of malignancies, including brain, breast, colon and lung malignancies, have increased MGMT activity compared with corresponding normal tissue (Christmann et al. 2011). While the relationship between MGMT activity and clinical outcomes is ill-determined for most of cancer models, low MGMT expression or epigenetic silencing of MGMT expression by promoter methylation are correlated with improved therapeutic responses to alkylating chemotherapies in several brain tumors (Hegi et al. 2005, Christmann et al. 2011).
In addition to MGMT, multiple pathways influence the cellular effects of O6meG lesions induced by alkylating agents, such as the TLS, the MMR and the HR pathways (Fu et al. 2012). The TLS pathway can overcome O6meG-induced blocked DNA replication forks but, owing to its low-fidelity repair mechanism, replication past by TLS yields the generation of O6meG:T mispairs. The latter is recognized by MSH2 and MSH6, forming the MUTSα unit of the MMR pathway (Casorelli et al. 2008). The MMR complex may then remove and replace the mismatch thymine by another thymine opposite the O6meG. These cycles of futile DNA processing promote the formation of replication fork collapse leading to cytotoxic
Figure 2Main mechanisms of repair of the DNA lesions induced by SN1 alkylating agents ALKBH, AlkB homologue family; BER, base excision repair; NER, nucleotide excision repair; HR, homologous recombination; MMR, mismatch repair; TLS, translesion DNA synthesis.
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R394L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
double-strand DNA breaks that trigger apoptosis (Mojas et al. 2007, Fu et al. 2012). Hence, alkylation-induced cell death relies on the MMR-dependent recognition of O6meG lesions, and MMR-deficient cells are resistant to the cytotoxic effects of SN1 alkylating agents (Hickman & Samson 2004, Klapacz et al. 2009, Fu et al. 2012). O6meG adducts that escape MMR processing are highly mutagenic, oncogenic and can lead to the chemo-induce selection of resistant cancer clones (Bugni et al. 2009).
The HR pathway can overcome MMR-induced double-strand DNA breaks, and thus stand as another cellular survival mechanism against the cytotoxic effects of O6meG (Roos et al. 2009). Consistently, cells that are deficient in the HR pathway display increased sensitivity to SN1 alkylating agents (Fu et al. 2012). Nevertheless, the HR pathway induces sister chromatid exchanges, resulting in additional mutagenicity and cellular damages.
Post-transcriptional regulation of MGMT and polymorphisms in MGMT
Understanding how the MGMT gene is regulated is crucial for two aspects: (1) it may open therapeutic avenues if a mechanism of MGMT expression can be targeted and/or if MGMT silencing can be achieved and (2) if there are important post-transcriptional mechanisms controlling the MGMT level, the methylation of MGMT promoter may not be a good surrogate for the amount of enzyme present in the tumor. Most of the mechanisms exposed below were described in glioblastoma cell lines or tumors and may not be completely applicable to NETs as their biology is radically different.
Ramakrishnan et al. (2011) demonstrated early in the TCGA dataset that, whereas MGMT promoter methylation is associated with low MGMT mRNA expression, there is a wide range of MGMT mRNA when the promoter is unmethylated and a low correlation between mRNA and protein levels, which suggests important post-transcriptional mechanisms. Since then, multiples factors were described to directly or indirectly control MGMT expression such as Wnt, STAT3, MEK, GSK3β and NFκB (Lavon et al. 2007, Sato et al. 2011, Kohsaka et al. 2012, Wickström et al. 2015). In addition, multiple miRNA were described to target MGMT mRNA such as miR-181d-5p, miR-409-3p, miR142-3p and miR-602, some of them being specific of an elongated form of the MGMT mRNA (Zhang et al. 2012, Kreth et al. 2013, Kushwaha et al. 2014, Khalil et al. 2016, Lee et al. 2018). It was also described that histone modifications (acetylation of
H3K9) could regulate MGMT expression, independently of promoter methylation (Kitange et al. 2012). This is of particular interest as multiple histone modifiers are under clinical development. Finally, multiple studies in several types of malignancies described the relationship between MGMT promoter methylation and a polymorphism present in the promoter (rs16906252), although the underlying mechanism remains unknown. Patients with homozygous TT genotype were more likely to have their MGMT promoter methylated than patients with TC/CC genotypes and had a longer survival when treated by alkylating agent (Candiloro & Dobrovic 2009, Hawkins et al. 2009, Kristensen et al. 2011, Leng et al. 2011, Rapkins et al. 2015). More recently, Hsu et al. (2017) reported a novel SNP (rs1625649) located in the promoter region and associated with its methylation and low MGMT protein level. Taken together, all these mechanisms highlight the complexity of MGMT regulation and may explain the discrepancies observed between promoter methylation and protein level.
Methodology of evaluation of the MGMT status
Many different techniques have been proposed to evaluate the MGMT status and there is no consensus yet on how to best determine this biomarker, impairing its wide use in clinical practice. Most of the studies that attempted to define the best evaluation method were performed in glioblastoma-derived cell lines or samples. The ideal method would be to measure MGMT enzymatic activity directly within the tumor but because it requires fresh or frozen tissues, it is only restricted to in vitro mechanistic studies (Robinson et al. 2010). In the glioblastoma field, the most used method is the evaluation of the MGMT promoter methylation as an inverse surrogate of the MGMT status while in the NET field, immunohistochemistry (IHC) has been proposed by several groups, alone or together with promoter methylation assessment. MGMT promoter methylation clearly depicts how much work is still needed to standardize this biomarker. First, there is still a debate regarding the regions and the CpGs that are indeed controlling MGMT expression (beyond the scope of this review, discussed in Yu et al. 2019). This is of major importance as several methods of evaluation are ‘targeted’, that is, they only assess the methylation status of a finite number of CpG. Second, several methods have been proposed to evaluate MGMT promoter methylation, such as methylation-specific PCR (MS-PCR),
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R395L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
methylation-specific multiplex ligation-dependent probe amplification (MS-MLPA) and pyrosequencing. It should be noted that in all studies that compared these techniques, the endpoint was not the ‘true methylation status’ (defined by methylation chips for instance) but patient survival. In all studies, pyrosequencing showed the best association with survival and is now the most widely used technique in neuro-oncology (Christians et al. 2012, Quillien et al. 2012). It is quantitative and can be performed in routine on formalin-fixed paraffin-embedded samples. The cut-off value usually reported in the studies is 8–10%. This cut-off gives the best rate of agreement with (q)MS-PCR, the technique that was used in most early clinical trials and also has a good predictive value in TMZ-treated patients with glioblastoma (Mikeska et al. 2007, Felsberg et al. 2011, Quillien et al. 2012). In NET, there is no study that attempted to define a ‘NET-specific cut-off’. Walter et al. (2015) and Cros et al. (2016) used the 7–8% threshold, while Raj et al. (2017) used a higher value (20%) although it is unclear why such cut-off was chosen. This technique requires a specific equipment and a significant technical ‘hand-on time’ for bisulfite conversion and pyrosequencing. A possible issue with this technique is when tumor cells are very scarce and/or when the samples highly contaminated by non-tumor cells. Targeted evaluation of DNA methylation by next-generation sequencing (NGS) following bisulfite conversion is not yet performed in clinical practice but because of the availability of NGS in oncology platforms, this approach could replace pyrosequencing, should its calibration be robustly achieved.
On the contrary, IHC is a fast and cheap technique, available in all pathology laboratories, which allows to measure MGMT expression only in tumor cells. This approach is seducing as it truly reflects the amount of enzyme (but not its activity) regardless of all the possible mechanisms of regulation of its expression. MGMT staining is classically nuclear but additional cytoplasmic staining may also be seen. It should be noted that in most studies, only the nuclear staining was quantified and recorded. In addition, because most non-tumor cells (e.g. hepatocytes, acinar cells or inflammatory cells) express MGMT, they can be used as internal control for IHC in cases of complete loss of MGMT within tumor cells. Yet, it also suffers from a complete lack of consensus regarding the clone that should be used and how the enzyme should be quantified (Table 1). Similarly, the level of expression in non-tumor cells could be used to standardize the IHC between laboratories. Neto et al. compared several clones with the amount of MGMT mRNA defined by RT-PCR in
a series of breast tumors (Neto et al. 2011). The authors concluded that the SPM287 clone (Santa Cruz) was the most sensitive and specific. Yet, in the NET field, the MT3.1 clone has been the most widely reported in studies, while the different clones have never been compared (Kulke et al. 2009, Schmitt et al. 2014, Cros et al. 2016, Girot et al. 2017, Krug et al. 2017, Hijioka et al. 2019) (Table 1). While there is a consensus on the cut-off for CpG methylation levels, there is none on IHC. Most studies dichotomized NETs in MGMT-deficient and MGMT-proficient with a very stringent cut-off (MGMT-deficient: no expression at all or in less than 10% of the cells). An alternative is to use a continuous scoring system to better reflect all the possibilities of MGMT expression, such as the H-score (% of positive cells (0–100) × intensity (0–3), score (0–300) (Cros et al. 2016)), the immunoreactive score (% of positive cells (0–4) × intensity (1–3), score (0–12) (Yang et al. 2014)) or the Allred score which is similar (Allred et al. 1993, Cives et al. 2016).
Yet, in the last two studies, while MGMT staining was recorded as a continuous value, the authors used a single stringent cut-off (Yang et al. 2014, Cives et al. 2016). In a previous publication, we used the H-score and reported that only a stringent cut-off (H-score <50) was associated with radiological objective response, but that a higher value (H-score <100) could be used to define MGMT-deficient NET and still selected patients with prolonged progression-free survival (PFS) (Cros et al. 2016). The use of a continuous scoring system, while more adaptative to the expected clinical benefit, would require the choice of the clone and methods of immunohistochemistry and scoring to be standardized. Current trials on the predictive value of MGMT promoter methylation and immunohistochemistry should help to clarify the best method to assess the MGMT status (Lemelin et al. 2019).
Which method is best to assess the MGMT status has yet to be determined. Overall, IHC is well correlated to the promoter methylation in pancreatic and lung NETs, although the number of samples tested was often small (Schmitt et al. 2014, Walter et al. 2015, Cros et al. 2016, Vatrano et al. 2020). Several studies highlighted below used promoter methylation and/or IHC and demonstrated inconsistently the prognostic or predictive value of either, both or none. More than one technique on the same samples were performed in seven studies but comparative results were only presented in five (Schmitt et al. 2014, Walter et al. 2015, Cros et al. 2016, Girot et al. 2017, Raj et al. 2017). MS-PCR and pyrosequencing were only compared in one study and showed a good correlation (88% of concordant cases, κ = 0.6)
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R396L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
(Walter et al. 2015). Regarding promoter methylation and IHC, Schmidt et al. reported a 66% concordance (6/9 samples but correlation not significant P = 0.5), a result similar to that of Walter et al. (89% concordance pyrosequencing/IHC, κ = 0.7; 84% MS-PCR/IHC κ = 0.6) and higher than Girot et al. (50% concordance; 10/20 samples) and Raj et al. (54% concordance; 15/28). Taken together, these results highlight the importance of involvement of post-transcriptional regulations and the need for a standardized method to assess MGMT status.
MGMT status in digestive NETs
We identified 14 studies that studied the association between the MGMT status and response to alkylating
agents and/or survival in digestive NET (Table 1) (Ekeblad et al. 2007, Kulke et al. 2009, Schmitt et al. 2014, Yang et al. 2014, Dussol et al. 2015, Walter et al. 2015, Cives et al. 2016, Cros et al. 2016, Girot et al. 2017, Krug et al. 2017, Owen et al. 2017, Raj et al. 2017, Campana et al. 2018, Hijioka et al. 2019). All of them were retrospective and only three were multicentric (Yang et al. 2014, Girot et al. 2017, Campana et al. 2018). The techniques used to determine MGMT status were highly heterogeneous. One study measured MGMT promoter methylation only, seven studies measured MGMT IHC expression only and six studies assessed both. The origin of the samples (primary tumor or metastases) was clearly reported in only two studies (Cros et al. 2016, Krug et al. 2017). This may have its importance in the interpretation of data since MGMT expression may be different between primary tumors and metastases (Yang et al. 2014).
Table 1 Studies that explored the role of MGMT status in pancreatic neuroendocrine tumors.
Study Organ of origin TechniqueDefinition for MGMT deficient (low expression or promoter methylation) MGMT deficiency
Ekeblad et al. (2007) Pancreas 35%Lung 39%
IHC (MAB16200, 1:500) <10% cells 43%
Kulke et al. (2009) Pancreas 38% IHC (MT3.1, 1:25) No staining 24%Schmitt et al. (2014) Pancreas (resected) IHC (MT3.1, 1:160) ≤5% cells 66%
MS-PCR Detection+ 56%Pancreas (metastatic) MS-PCR + MSqPCR Detection+, Threshold ≥ 10% 30%
IHC (MT3.1, 1:160) ≤5% cells 44%Yang et al. (2014) Pancreas 48%
Intestine 48%IHC (NR, 1:50) Immunoreactive score ≤ 2 31.6%
Walter et al. (2015) Pancreas 58%Intestine 31%
Pyrosequencing Threshold >8% 24%(pancreas 27%)
MS-PCR Detection+ 12%(pancreas 7%)
IHC (MT23.2, 1:200) <10% cells 33%(pancreas 36%)
Dussol et al. (2015) Pancreas 43%Intestine 33%Lung 14%
Pyrosequencing Threshold >8% 38%(pancreas 54%)
IHC (MT23.2, 1:200) <10% cells 42%Cros et al. (2016) Pancreas Pyrosequencing Threshold ≥7% 52%
IHC (MT3.1, 1:25) H-score ≤50 70%Cives et al. (2016) Pancreas IHC (MS-470-P1, 1:20) No staining 29%
<10% cells 38%Allred score <4 36%
Owen et al. (2017) Pancreas 61% IHC (MS-470-B, dilution NR)
<10% cells 57%
Girot et al. (2017) Pancreas IHC (MT3.1, 1:200) ≤10% cells 59%MS-PCR NR 15%
Raj et al. (2017) Pancreas IHC (NR) No staining 55%Pyrosequencing Threshold ≥20% 14%
Krug et al. (2017) Pancreas 83% IHC (MT3.1, 1:25) No staining 63%(pancreas 55%)
Hijioka et al. (2019) Pancreas IHC (MT3.1, 1:25) <10% cells 46%Campana et al. (2018) Pancreas 45%
Lung 22%MS-PCR Detection+ Pancreas 30% Pyrosequencing Threshold >7%
IHC, immunohistochemistry; MS-PCR, methylation-specific PCR; NR, not reported.
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R397L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
Among the seven studies that analyzed MGMT promoter methylation (Schmitt et al. 2014, Dussol et al. 2015, Walter et al. 2015, Cros et al. 2016, Girot et al. 2017, Raj et al. 2017, Campana et al. 2018), five studies used pyrosequencing. Four of them used a threshold of CpG islands methylated between 6 and 8% and described rates of MGMT promoter methylation between 23 and 52% (Dussol et al. 2015, Walter et al. 2015, Cros et al. 2016, Campana et al. 2018). This rate was 14% in the fifth study, which used more stringent criteria (at least 4/5 CpG island methylated at 20% or greater (Raj et al. 2017)). Three studies used MS-PCR (including one that also performed primer extension-based quantitative PCR) and found rates of MGMT promoter methylation between 12 and 56% (Schmitt et al. 2014, Walter et al. 2015, Girot et al. 2017). Finally, one study found a 30% rate of MGMT promoter methylation mixing both MS-PCR and pyrosequencing (with a >7% threshold) (Campana et al. 2018).
Among the 13 studies assessing MGMT IHC, at least five different antibodies were used, including MT3.1 (n = 6), MT23.2 (n = 2), MS-470-P1, MS-470-B and MAB16200 (n = 1 each), and two studies did not specify the antibody used (Table 1). Additionally, dilution of the antibody was not systematically reported, or variable. For instance, the MT3.1 antibody could be used at very different dilutions, from 1:25 to 1:200. The scoring system used was also heterogeneous. Some authors reported a rate of MGMT-deficient tumors of 24–63% when defined by complete absence of staining (Kulke et al. 2009, Girot et al. 2017, Krug et al. 2017, Raj et al. 2017) and 33–57% when defined by ≤10% of positive cells (Ekeblad et al. 2007, Dussol et al. 2015, Walter et al. 2015, Owen et al. 2017, Hijioka et al. 2019). The studies reporting on more complex scores combining nuclear staining intensity and the percentage of stained cells reported higher rates (70–82%) of MGMT-deficient NETs (Yang et al. 2014, Cros et al. 2016).
Overall, among the five studies that assessed the MGMT status based on MGMT promoter methylation specifically in PanNET patients, representing 219 patients (without the study by Raj et al. (2017) due to too important methodological heterogeneity), the rate of patients with MGMT-deficient tumors ranged from 15 to 70% (pooled mean, 48%) (Schmitt et al. 2014, Dussol et al. 2015, Walter et al. 2015, Cros et al. 2016, Girot et al. 2017, Campana et al. 2018). MGMT status based on protein expression was available specifically for 415 patients with PanNET included in nine studies (Kulke et al. 2009, Schmitt et al. 2014, Dussol et al. 2015, Cives et al. 2016, Cros et al. 2016, Girot et al. 2017, Krug et al. 2017, Raj et al. 2017, Hijioka et al. 2019). Although significant heterogeneity existed as
mentioned above, the rate of MGMT deficiency ranged from 29 to 70% (pooled mean, 52%). Overall, about 50% of PanNET are MGMT-deficient.
Besides using a heterogeneous methodology for MGMT status evaluation, six studies included only patients with PanNET (Schmitt et al. 2014, Cives et al. 2016, Cros et al. 2016, Girot et al. 2017, Raj et al. 2017, Hijioka et al. 2019), while the other studies included 15–65% of patients with NET from other origins (mainly gastrointestinal tract or lung). Another potentially important bias is the timing between the acquisition of the specimen used to determine the MGMT status and alkylating treatment. Indeed, it can be suspected that other DNA-damaging treatments, such as other types of chemotherapy, might influence the expression and activity of DNA repair pathways, including that of MGMT, although it was never demonstrated. For instance, we previously reported that pretreatment using chemotherapy (HR 1.79, P = 0.03) but not using somatostatin analogs (HR 1.39, P = 0.21) was independently associated with a higher risk of progression under TMZ (de Mestier et al. 2020b). Similarly, Campana et al. reported that previous chemotherapy independently increased the risk of progression (HR 1.92, P = 0.014) and death (HR 2.87, P = 0.003) in patients with PanNET treated with TMZ-based therapy (Campana et al. 2018). Hence, assessing the MGMT status might be relevant only if it is carried out on a sample taken just before initiating the alkylating agent. Among the reviewed literature, this information was never reported and only six studies reported pretreatment (17–39% of patients) with chemotherapy (Schmitt et al. 2014, Cives et al. 2016, Cros et al. 2016, Girot et al. 2017, Owen et al. 2017, Campana et al. 2018). In such patients, the MGMT status should be interpreted with caution, as it might have been altered by previous chemotherapy.
Prognostic role of MGMT expression in PanNETs
Eleven studies explored the prognostic impact of the MGMT status (assessed by IHC or MGMT promoter methylation analysis) in patients with NET from various origins treated with alkylating agents (Kulke et al. 2009, Schmitt et al. 2014, Yang et al. 2014, Dussol et al. 2015, Walter et al. 2015, Cives et al. 2016, Krug et al. 2017, Owen et al. 2017, Raj et al. 2017, Campana et al. 2018, Hijioka et al. 2019). Most of these studies suggested that MGMT deficiency might be associated with a prolonged OS in this setting (Kulke et al. 2009, Schmitt et al. 2014,
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R398L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
Yang et al. 2014, Walter et al. 2015, Owen et al. 2017, Campana et al. 2018, Hijioka et al. 2019), although in a number of them the statistical significance was not reached due to low statistical power in relation with the limited number of patients included (Table 2). Nevertheless, most of these studies included patients treated with alkylating agents. In the absence of control groups not treated with alkylating agents, the prognostic impact of the MGMT status, independently from the treatment received, is difficult to distinguish from its predictive value on survival.
In 130 patients with resected non-metastatic PanNET, Schmitt et al. (2014) reported that those with MGMT-deficient tumors had prolonged disease-free survival (P = 0.005) and disease-specific survival (P = 0.03), although none remained significant at multivariate analysis adjusted on stage, grade and CK19 expression.
Most studies have explored the prognostic impact of the MGMT status in the metastatic setting. Walter et al. (2015) reported that the MGMT status (whatever the method of evaluation) had no prognostic impact
Table 2 MGMT status in pancreatic neuroendocrine tumors treated by alkylating agents: prediction of response and prognostic impact.
Study
Treatment
Population evaluable for response (method for MGMT status)
Comparison of MGMT-deficient vs MGMT-proficient subgroups
Objective response rate Median PFS (months) Median OS (months)
Ekeblad et al. (2007) TMZ 23 (IHC) 40% vs 8% (P = 0.13)
NR NR
Kulke et al. (2009) TMZ-based 21 (IHC) 80% vs 0% (P < 0.001)
19.2 vs 9.3(P = 0.11)
>60 vs 19.1 (P = 0.14)
Schmitt et al. (2014) TMZ 8 (MS-PCR+ MSqPCR) Rate NR (P = 0.03) NR NR9 (IHC) Rate NR (P = 0.06) NR NR
Walter et al. (2015) TMZ-based 22%DTIC-based 49%STZ-based 29%
69 (PS) 50% vs 11% (P = 0.003)
26.4 vs 10.8(P = 0.002)
77 vs 43(P = 0.026)
69 (IHC) 62% vs 7% (P < 0.001)
20.2 vs 7.6(P < 0.001)
105 vs 34(P = 0.006)
Dussol et al. (2015) TMZ-based 25% 26 (PS) 40% vs 6% (P = 0.03)
23.8 vs 6.7(P = 0.04)
63.2 vs 68.7(P = 0.88)
DTIC-based 44% 19 (IHC) 38% vs 9% (P = 0.13)
15.7 vs 6.7 (P = 0.14)
58.4 vs 62.5(P = 0.86)
Cros et al. (2016) TMZ-based 29 (PS) NR (P = 0.1) >36 vs 20(P = 0.05)
NR
43 (IHC) 50% vs 15% (P = 0.04)
Median NR(P = 0.01)
NR
Cives et al. (2016) TMZ-based 52 (IHC, no staining) 40% vs 65% (P = 0.10)
14.5 vs 16.8 (P = 0.25)
81.1 vs >100 (P = 0.40)
52 (IHC, <10% cells) 50% vs 63% (P = 0.37)
16.6 vs 14.5 (P = 0.62)
81.1 vs 73.2 (P = 0.41)
52 (IHC, Allred <4) 47% vs 64% (P = 0.25)
16.6 vs 17.4 (P = 0.54)
81.1 vs 73.2 (P = 0.27)
Owen et al. (2017) TMZ-based 14 (IHC) 63% vs 17% (P = 0.18)
16.6 vs 9.5 (P = 0.19)
42.9 vs 18.1 (P = 0.16)
Girot et al. (2017) TMZ-based 22 (IHC) 15% vs 11% (P = 1)
18 vs 9 (P = 0.84)
NR
20 (MS-PCR) 0% vs 17% (P = 1)
18 vs 15(P = 0.85)
NR
Raj et al. (2017) TMZ 77% 36 (IHC) 50% vs 31% (P = 0.26)
NR Median NR(P = 0.47)
DTIC 23% 28 (PS) 25% vs 38% (P = 1)
NR NR
Krug et al. (2017) DTICSTZ-based
24 (IHC) 50% vs 25% (P = 0.24)
12 vs 13(P = 0.82)
NR
Hijioka et al. (2019) STZ 13 (IHC) 83.3% vs 14.3% (P = 0.013)
5.6 vs 4.6(P = 0.50)
27.1 vs 14.7(P = 0.339)
Campana et al. (2018) TMZ-based 95 (MS-PCR or PS) 51.8% vs 17.7%(P = 0.001)
21 vs 8(P = 0.017)
>70 vs 23(P = 0.057)
DTIC, dacarbazine; IHC, immunohistochemistry; MS-PCR, methylation-specific PCR; NR, not reported; PS, pyrosequencing; STZ, streptozotocin; TMZ, temozolomide.
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R399L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
among 107 patients with NET, 50% of them being treated by alkylating agents. However, in the subgroup of patients treated by alkylating agents, MGMT deficiency was associated with prolonged OS. The prognostic role of MGMT status was more discriminant if assessed by IHC (105 months vs 34 months, P = 0.006) than by pyrosequencing (77 months vs 43 months, P = 0.026). In addition, MGMT promoter methylation was associated with longer OS in patients with PanNET (87.8 months vs 33.3 months, P = 0.006) but not significantly in those with gastrointestinal NET (63.3 months vs 44.1 months, P = 0.45) (Walter et al. 2015). Only one large study provided a methodologically reliable multivariate analysis in the metastatic setting (Campana et al. 2018). In the latter, the authors reported that patients with MGMT-proficient PanNET (MGMT promoter not methylated) treated with TMZ-based therapy had a 2.91-fold increased risk of death (95% CI (1.24–6.86), P = 0.014) in comparison with the MGMT-deficient PanNET group.
Overall, although the prognostic role of MGMT status was not uniformly reported, possibly due to the uneven quality of studies and the generally limited number of included patients, patients with MGMT-deficient PanNET treated with alkylating agents might have prolonged OS in comparison to those with MGMT-proficient tumors.
Of note, PanNET harboring a ‘hypermethylator’ phenotype may be associated with shorter OS. For instance, Walter et al. (2015) reported, in a study of 47 patients (21 with PanNET and 26 with ileal NET), that OS was significantly shorter in those with NETs containing >3 methylated genes (of a panel of 12 frequently methylated genes) in comparison with those having ≤3 methylated genes. MGMT methylation was more frequent in hypermethylated NETs. Although in this population OS was not influenced by MGMT methylation, some patients received alkylating agents. This suggests that MGMT methylation could be part of a ‘hypermethylator’ phenotype, associated with a pejorative prognostic impact which may be reversed or at least counterbalanced by a better efficacy of alkylating agents.
MGMT status as a predictive biomarker of morphological response in advanced PanNETs treated with alkylating agents
The antitumor efficacy of alkylating agents in advanced NET in general and in PanNET, in particular, has been well documented. Overall, the most recent series demonstrated
an objective response rate of 30–50% with TMZ-, DTIC- or STZ-based chemotherapy (Dilz et al. 2015, Cives et al. 2016, Clewemar Antonodimitrakis et al. 2016, Krug et al. 2017, Campana et al. 2018, de Mestier et al. 2019, 2020b).
There are scarce preclinical data documenting the relationship between MGMT activity and sensitivity to alkylating agents in NETs. Using the BON1 PanNET MGMT-deficient cell line, Hijioka et al. (2019) performed MGMT lentiviral-transduced overexpression. After treatment with various doses of STZ, the MGMT-overexpressing cell line had a significantly increased viability in comparison with the parental BON1 cell line.
The influence of the MGMT status on the morphological response of advanced PanNET to alkylating agent was explored in the 13 studies reported in Table 2. As reported above, these studies were heterogeneous and most were limited in size. The alkylating agent reported was mostly TMZ, alone or combined (mostly with CAP). Among seven of them, the MGMT status was determined by promoter methylation, either by MS-PCR (Schmitt et al. 2014, Girot et al. 2017), pyrosequencing (Dussol et al. 2015, Walter et al. 2015, Cros et al. 2016, Raj et al. 2017) or both (Campana et al. 2018). Overall, four studies found that MGMT promoter methylation significantly predicted objective response to alkylating agents (Schmitt et al. 2014, Dussol et al. 2015, Walter et al. 2015, Campana et al. 2018) and one found a statistical tendency (Cros et al. 2016), while two studies reported no association (Girot et al. 2017, Raj et al. 2017). In the largest (n = 96) – and possibly most informative – of these studies, the objective response rates to were 51.8 and 17.7% in PanNET with and without MGMT promoter methylation, respectively (P = 0.001) (Campana et al. 2018). Interestingly, this difference remained significant at multivariable analysis (HR 6.53, 95% CI (2.23–19.10), P = 0.001).
Among the 12 studies assessing the MGMT status using IHC, four reported that MGMT deficiency predicted alkylating agents efficacy (Kulke et al. 2009, Walter et al. 2015, Cros et al. 2016, Hijioka et al. 2019), six studies reported a non-significant statistical trend (Ekeblad et al. 2007, Schmitt et al. 2014, Dussol et al. 2015, Krug et al. 2017, Owen et al. 2017, Raj et al. 2017) and two studies reported no association (Cives et al. 2016, Girot et al. 2017). Of note, in one of the two latter studies, the authors found no association of the MGMT expression and objective response to TMZ-based therapy, whatever the methodology used (no staining, <10% positive cells, or Alldred quantitative score) (Cives et al. 2016). However, in this study, the main usual prognostic factors (e.g. Ki67 index) had the opposite effect as expected, questioning
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R400L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
its external validity and therefore its relevance. None of these studies reported a multivariate analysis.
Interestingly, a recent meta-analysis of 11 of these studies (n = 382 patients included) reported that the proportion of patients achieving objective response was higher in those with MGMT-deficient NET (75/146, 51.4%) than in those without MGMT deficiency (40/236, 16.9%), whatever the method used (Qi & Tan 2020). This corresponded to a five-fold increase in the probability of objective response (95% CI (3.04–8.22), P < 0.001, I2 = 3%). Moreover, this difference remained statistically significant when focusing on the studies using IHC-based (OR 5.27, 95% CI (2.57–10.82), P < 0.001, I2 = 5%) or methylation-based (OR 4.73, 95% (2.38–9.42), P < 0.001, I2 = 3%) determination of the MGMT status.
The predictive impact of the MGMT status seems to be relevant in either SN1 alkylating agent. Walter et al. (2015) reported that MGMT promoter methylation was predictive of the efficacy of either TMZ (objective response, 100% vs 9%, P = 0.008), DTIC (44% vs 9%, P = 0.05) or STZ (25% vs 15%, P = 0.44), although the latter was not statistically significant. In another study, the same group similarly reported that MGMT promoter methylation could predict the efficacy of alkylating agents (40% vs 6%, P = 0.03) but not of that of the gemcitabine–oxaliplatin combination (27% vs 26%, P = 0.92) (Dussol et al. 2015). Hence, the MGMT status is not predictive of the efficacy of any DNA-toxic chemotherapy but is specific to that of alkylating agents.
MGMT status as a predictive biomarker of progression in advanced PanNETs treated with alkylating agents
Among the ten studies that have explored the influence of the MGMT status on the PFS of patients treated with alkylating agents for an advanced NET, nine assessed MGMT IHC. The two largest studies reported that low MGMT expression was associated with significantly prolonged PFS (Walter et al. 2015, Cros et al. 2016), four studies depicted only a statistical tendency (Kulke et al. 2009, Dussol et al. 2015, Girot et al. 2017, Owen et al. 2017) and the three last studies reported no impact (Cives et al. 2016, Krug et al. 2017, Hijioka et al. 2019). In the largest study (n = 69), patients with low MGMT expression had a prolonged PFS under alkylating agent in comparison with those with high MGMT expression (20.2 months vs 7.6 months, HR 0.19, 95% CI (0.08–0.48), P < 0.001) (Walter et al. 2015).
While all these studies used various thresholds to determine the MGMT status, the use of continuous scoring systems may reflect the wide range of expression seen in tumors. Interestingly, this allowed to describe that the impact of alkylating agents on PFS was correlated to the importance of MGMT expression. Indeed, in the study by Cros et al. (2016), the 2-year PFS rate was 65, 53 and 45% in case of H-score ≤50, ≤100 or ≤150, respectively. Similarly, more stringent thresholds could predict a higher probability of response.
In addition, four studies reported that MGMT promoter methylation was associated with prolonged PFS (Dussol et al. 2015, Walter et al. 2015, Cros et al. 2016, Campana et al. 2018), which was not confirmed by another – although smaller – study (Girot et al. 2017). Again, MGMT promoter methylation may predict prolonged PFS using either STZ (19.5 months vs 7.6 months, P = 0.04), DTIC (26.4 months vs 12.4 months, P = 0.004) or TMZ (16.3 months vs 7.2 months, P = 0.23), although not significantly for the latter (Walter et al. 2015). Moreover, this study provided a multivariable analysis, in which MGMT promoter methylation significantly decreased the risk of progression (HR 0.29, 95% CI (0.13–0.64), P = 0.002). This result was concordant with the study by Campana et al. (2018), in which MGMT-proficient tumors had a significantly higher risk of progression (HR 2.62, 95% CI (1.38–5.00), P = 0.003), independently from the Ki67 index and the previous use of chemotherapy.
Overall, despite aforementioned heterogeneity of the literature, the pooled analysis of available data advocate that MGMT may be a relevant biomarker predictive of sensitivity to alkylating agents in NETs. In order to further explore this hypothesis, the MGMT-NET randomized phase II study (NCT03217097) aims at evaluating the value of the MGMT status in the prediction of the objective response at 3 months in patients treated with alkylating agents (Lemelin et al. 2019).
Other biomarkers potentially complementary to MGMT for the evaluation of the sensitivity to alkylating agents
MGMT is the first enzyme to be involved in the repair of TMZ-induced DNA damages and probably one of the most important. Yet, other DNA repair systems can play an important role in the resistance to alkylating agents. For instance, the BER pathway is another mechanism involved in the repair of DNA lesions caused by alkylating
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R401L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
agents and especially N3 and N7 methyl adducts. Within the BER system, alkylpurine–DNA–N-glycosylase (APNG) removes the alkylated DNA bases carrying the 7meG, 3meA or 7meA lesions, creating apurinic sites. In glioblastoma, the APNG level correlated with resistance to TMZ (Agnihotri et al. 2012). However, there is no data in NETs regarding the predictive role of APNG.
Among the subsequent phases of the BER cascade, the limiting step is the activation of the poly-(ADP)-ribose polymerase (PARP). Alkylating agents are among the most potent activators of PARP and increasing interest has emerged in the development of PARP inhibitors as modulators of resistance to alkylating agents such as TMZ. Indeed, PARP inhibitors could potentiate the effect of TMZ by inhibiting the repair of the single-strand breaks generated by the excision of the TMZ-induced N-methylpurine (Curtin & Szabo 2013). Preclinical studies reported a synergistic enhanced sensitivity of the combination of TMZ to PARP inhibitors in various cancer models (Palma et al. 2009), including glioblastoma (Jue et al. 2017), small-cell lung cancer (Lok et al. 2017) and melanoma (Toshimitsu et al. 2010), which are models known to be relatively close to NET, and especially in MGMT-deficient, MMR proficient or BRCA-deficient models (Curtin & Szabo 2013, Erice et al. 2015). Interestingly, resistance to TMZ seems to be overcome by PARP inhibitors in MGMT-proficient and/or MMR deficient models (Higuchi et al. 2020). Several phase I and II studies have reported potential antitumor activity of PARP inhibitors combined to TMZ in patients with recurrent brain tumors (Su et al. 2014, Robins et al. 2016, Blakeley et al. 2019), small-cell lung cancer (Pietanza et al. 2018), melanoma (Plummer et al. 2013, Middleton et al. 2015), colorectal cancer (Pishvaian et al. 2018) and breast cancer (Han et al. 2018). Potentiated myelotoxicity was the most frequent adverse event described. To date, data specific to the combination of PARP inhibitors and alkylating agents in NET models are very scarce. In one study, veliparib dose-dependently enhanced the efficacy of DTIC in the H727 (lung NET) and BON (small-intestine NET) cell lines, with increased DNA damage, cytotoxicity, apoptosis and decreased chromogranin A expression (Somnay et al. 2016).
Among other potential biomarkers, it has been previously shown that a deficient MMR system is also a strong predictor of TMZ resistance (Perazzoli et al. 2015). However, dMMR phenotype was only described in a limited proportion of neuroendocrine carcinomas, but not in NETs (Sahnane et al. 2015, Liu et al. 2016). Hence, there is no rational to assess it in NETs as a predictive biomarker of TMZ resistance. An important finding on
MMR was discovered when comparing post-TMZ vs pre-TMZ glioblastoma samples. It was found that about 15% of patients with recurrence had an hypermutator phenotype mostly because of MSH6 loss (Barthel et al. 2019). Should a similar mechanism existed in NETs, these patients could be good candidates for immunotherapy while classical NET patients are not. However, this remains to be demonstrated in PanNETs. Indeed, in the series by Cros et al. (2016), seven patients progressive under TMZ had a microsatellite stable status.
The homologous recombination system is required for TMZ-induced double strand DNA breaks. Rare cases of PanNETs were reported in the context of germline BRCA2 mutation. However, such cases are very rare, and there is no evidence of any impact on sensitivity to alkylating agents (Scarpa et al. 2017). Finally, ALT activation and DAXX/ATRX loss have prognostic implication in PanNET. One study explored their impact (determined by telomeric FISH or IHC, respectively) on response to TMZ-CAP and found no association (Cives et al. 2016).
Conclusions
MGMT is the main enzyme responsible for the repair of O6meG lesions in DNA induced by alkylating agents in NETs. Increasing arguments advocate that MGMT deficiency could significantly predict increased objective response rate, prolonged PFS and prolonged OS in patients with NETs (and especially PanNETs) treated with alkylating agents. Nevertheless, many pitfalls are to be overcome in order to be able to generalize the evaluation of the MGMT status to clinical routine. While MGMT promoter methylation may be a reference technique, it may not reflect entirely the MGMT activity in tumor cells, which could be more appropriately assessed by IHC, which, however, requires standardization. Finally, the understanding of intermingled DNA repair pathways has led to identify PARP inhibitors as candidates to overcome resistance to alkylating agents in MGMT-proficient NETs.
Declaration of interestL M: Ipsen (consulting, research grant), Novartis (consulting, research grant), and Pfizer (consulting). A C: Ipsen and Novartis (research grant, consulting). W D H: Ipsen (advisory board, research grant), Novartis (advisory board), AAA (advisory board), and Pfizer (advisory board). O H: Ipsen, Novartis, and Pfizer (consulting). V R: Ipsen (research grant) and Novartis (research grant). P R: Ipsen, Novartis, AAA, Keocyt, and ITM (consulting). L H: Novartis and Ipsen (research grants). J C: Novartis (consulting). The other authors have nothing to disclose.
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R402L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
FundingThis work did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
ReferencesAgnihotri S, Gajadhar AS, Ternamian C, Gorlia T, Diefes KL, Mischel PS,
Kelly J, McGown G, Thorncroft M, Carlson BL, et al. 2012 Alkylpurine-DNA-N-glycosylase confers resistance to temozolomide in xenograft models of glioblastoma multiforme and is associated with poor survival in patients. Journal of Clinical Investigation 122 253–266. (https://doi.org/10.1172/JCI59334)
Allred DC, Clark GM, Elledge R, Fuqua SA, Brown RW, Chamness GC, Osborne CK & McGuire WL 1993 Association of p53 protein expression with tumor cell proliferation rate and clinical outcome in node-negative breast cancer. Journal of the National Cancer Institute 85 200–206. (https://doi.org/10.1093/jnci/85.3.200)
Barthel FP, Johnson KC, Varn FS, Moskalik AD, Tanner G, Kocakavuk E, Anderson KJ, Abiola O, Aldape K, Alfaro KD, et al. 2019 Longitudinal molecular trajectories of diffuse glioma in adults. Nature 576 112–120. (https://doi.org/10.1038/s41586-019-1775-1)
Blakeley JO, Grossman SA, Chi AS, Mikkelsen T, Rosenfeld MR, Ahluwalia MS, Nabors LB, Eichler A, Ribas IG, Desideri S, et al. 2019 Phase II study of iniparib with concurrent chemoradiation in patients with newly diagnosed glioblastoma. Clinical Cancer Research 25 73–79. (https://doi.org/10.1158/1078-0432.CCR-18-0110)
Bugni JM, Meira LB & Samson LD 2009 Alkylation-induced colon tumorigenesis in mice deficient in the Mgmt and Msh6 proteins. Oncogene 28 734–741. (https://doi.org/10.1038/onc.2008.426)
Campana D, Walter T, Pusceddu S, Gelsomino F, Graillot E, Prinzi N, Spallanzani A, Fiorentino M, Barritault M, Dall’Olio F, et al. 2018 Correlation between MGMT promoter methylation and response to temozolomide-based therapy in neuroendocrine neoplasms: an observational retrospective multicenter study. Endocrine 60 490–498. (https://doi.org/10.1007/s12020-017-1474-3)
Candiloro ILM & Dobrovic A 2009 Detection of MGMT promoter methylation in normal individuals is strongly associated with the T allele of the rs16906252 MGMT promoter single nucleotide polymorphism. Cancer Prevention Research 2 862–867. (https://doi.org/10.1158/1940-6207.CAPR-09-0056)
Casorelli I, Russo MT & Bignami M 2008 Role of mismatch repair and MGMT in response to anticancer therapies. Anti-Cancer Agents in Medicinal Chemistry 8 368–380. (https://doi.org/10.2174/187152008784220276)
Christians A, Hartmann C, Benner A, Meyer J, von Deimling A, Weller M, Wick W & Weiler M 2012 Prognostic value of three different methods of MGMT promoter methylation analysis in a prospective trial on newly diagnosed glioblastoma. PLoS ONE 7 e33449. (https://doi.org/10.1371/journal.pone.0033449)
Christmann M, Verbeek B, Roos WP & Kaina B 2011 O(6)-methylguanine-DNA methyltransferase (MGMT) in normal tissues and tumors: enzyme activity, promoter methylation and immunohistochemistry. Biochimica et Biophysica Acta 1816 179–190. (https://doi.org/10.1016/j.bbcan.2011.06.002)
Cives M, Ghayouri M, Morse B, Brelsford M, Black M, Rizzo A, Meeker A & Strosberg J 2016 Analysis of potential response predictors to capecitabine/temozolomide in metastatic pancreatic neuroendocrine tumors. Endocrine-Related Cancer 23 759–767. (https://doi.org/10.1530/ERC-16-0147)
Clewemar Antonodimitrakis P, Sundin A, Wassberg C, Granberg D, Skogseid B & Eriksson B 2016 Streptozocin and 5-fluorouracil for the treatment of pancreatic neuroendocrine tumors: efficacy, prognostic
factors and toxicity. Neuroendocrinology 103 345–353. (https://doi.org/10.1159/000439086)
Cros J, Hentic O, Rebours V, Zappa M, Gille N, Theou-Anton N, Vernerey D, Maire F, Lévy P, Bedossa P, et al. 2016 MGMT expression predicts response to temozolomide in pancreatic neuroendocrine tumors. Endocrine-Related Cancer 23 625–633. (https://doi.org/10.1530/ERC-16-0117)
Curtin NJ & Szabo C 2013 Therapeutic applications of PARP inhibitors: anticancer therapy and beyond. Molecular Aspects of Medicine 34 1217–1256. (https://doi.org/10.1016/j.mam.2013.01.006)
de Mestier L, Walter T, Brixi H, Evrard C, Legoux JL, de Boissieu P, Hentic O, Cros J, Hammel P, Tougeron D, et al. 2019 Comparison of temozolomide-capecitabine to 5-fluorouracile-dacarbazine in 247 patients with advanced digestive neuroendocrine tumors using propensity score analyses. Neuroendocrinology 108 343–353. (https://doi.org/10.1159/000498887)
de Mestier L, Lepage C, Baudin E, Coriat R, Courbon F, Couvelard A, Do Cao C, Frampas E, Gaujoux S, Gincul R, et al. 2020a Digestive Neuroendocrine Neoplasms (NEN): French InterGroup clinical practice guidelines for diagnosis, treatment and follow-up (SNFGE, GTE, RENATEN, TENPATH, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, SFR). Digestive and Liver Disease 52 473–492. (https://doi.org/10.1016/j.dld.2020.02.011)
de Mestier L, Walter T, Evrard C, de Boissieu P, Hentic O, Cros J, Tougeron D, Lombard-Bohas C, Rebours V, Hammel P, et al. 2020b Temozolomide alone or combined with capecitabine for the treatment of advanced pancreatic neuroendocrine tumor. Neuroendocrinology 110 83–91. (https://doi.org/10.1159/000500862)
Dilz LM, Denecke T, Steffen IG, Prasad V, von Weikersthal LF, Pape UF, Wiedenmann B & Pavel M 2015 Streptozocin/5-fluorouracil chemotherapy is associated with durable response in patients with advanced pancreatic neuroendocrine tumours. European Journal of Cancer 51 1253–1262. (https://doi.org/10.1016/j.ejca.2015.04.005)
Drabløs F, Feyzi E, Aas PA, Vaagbø CB, Kavli B, Bratlie MS, Peña-Diaz J, Otterlei M, Slupphaug G & Krokan HE 2004 Alkylation damage in DNA and RNA – repair mechanisms and medical significance. DNA Repair 3 1389–1407. (https://doi.org/10.1016/j.dnarep.2004.05.004)
Dussol AS, Joly MO, Vercherat C, Forestier J, Hervieu V, Scoazec JY, Lombard-Bohas C & Walter T 2015 Gemcitabine and oxaliplatin or alkylating agents for neuroendocrine tumors: comparison of efficacy and search for predictive factors guiding treatment choice? Cancer 121 3428–3434. (https://doi.org/10.1002/cncr.29517)
Ekeblad S, Sundin A, Janson ET, Welin S, Granberg D, Kindmark H, Dunder K, Kozlovacki G, Orlefors H, Sigurd M, et al. 2007 Temozolomide as monotherapy is effective in treatment of advanced malignant neuroendocrine tumors. Clinical Cancer Research 13 2986–2991. (https://doi.org/10.1158/1078-0432.CCR-06-2053)
Erice O, Smith MP, White R, Goicoechea I, Barriuso J, Jones C, Margison GP, Acosta JC, Wellbrock C & Arozarena I 2015 MGMT expression predicts PARP-mediated resistance to temozolomide. Molecular Cancer Therapeutics 14 1236–1246. (https://doi.org/10.1158/1535-7163.MCT-14-0810)
Felsberg J, Thon N, Eigenbrod S, Hentschel B, Sabel MC, Westphal M, Schackert G, Kreth FW, Pietsch T, Löffler M, et al. 2011 Promoter methylation and expression of MGMT and the DNA mismatch repair genes MLH1, MSH2, MSH6 and PMS2 in paired primary and recurrent glioblastomas. International Journal of Cancer 129 659–670. (https://doi.org/10.1002/ijc.26083)
Frilling A, Modlin IM, Kidd M, Russell C, Breitenstein S, Salem R, Kwekkeboom D, Lau WY, Klersy C, Vilgrain V, et al. 2014 Recommendations for management of patients with neuroendocrine liver metastases. Lancet: Oncology 15 e8–e21. (https://doi.org/10.1016/S1470-2045(13)70362-0)
Fu D, Calvo JA & Samson LD 2012 Balancing repair and tolerance of DNA damage caused by alkylating agents. Nature Reviews: Cancer 12 104–120. (https://doi.org/10.1038/nrc3185)
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access
https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R403L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
Girot P, Dumars C, Mosnier JF, Muzellec L, Senellart H, Foubert F, Caroli-Bosc FX, Cauchin E, Regenet N, Matysiak-Budnik T, et al. 2017 Short article: Evaluation of O6-methylguanine-DNA methyltransferase as a predicting factor of response to temozolomide-based chemotherapy in well-differentiated metastatic pancreatic neuroendocrine tumors. European Journal of Gastroenterology and Hepatology 29 826–830. (https://doi.org/10.1097/MEG.0000000000000874)
Han HS, Diéras V, Robson M, Palácová M, Marcom PK, Jager A, Bondarenko I, Citrin D, Campone M, Telli ML, et al. 2018 Veliparib with temozolomide or carboplatin/paclitaxel versus placebo with carboplatin/paclitaxel in patients with BRCA1/2 locally recurrent/metastatic breast cancer: randomized phase II study. Annals of Oncology 29 154–161. (https://doi.org/10.1093/annonc/mdx505)
Hansen RJ, Nagasubramanian R, Delaney SM, Samson LD & Dolan ME 2007 Role of O6-methylguanine-DNA methyltransferase in protecting from alkylating agent-induced toxicity and mutations in mice. Carcinogenesis 28 1111–1116. (https://doi.org/10.1093/carcin/bgl218)
Hawkins NJ, Lee JH-F, Wong JJ-L, Kwok CT, Ward RL & Hitchins MP 2009 MGMT methylation is associated primarily with the germline C>T SNP (rs16906252) in colorectal cancer and normal colonic mucosa. Modern Pathology 22 1588–1599. (https://doi.org/10.1038/modpathol.2009.130)
Hegi ME, Diserens AC, Gorlia T, Hamou MF, de Tribolet N, Weller M, Kros JM, Hainfellner JA, Mason W, Mariani L, et al. 2005 MGMT gene silencing and benefit from temozolomide in glioblastoma. New England Journal of Medicine 352 997–1003. (https://doi.org/10.1056/NEJMoa043331)
Hickman MJ & Samson LD 2004 Apoptotic signaling in response to a single type of DNA lesion, O(6)-methylguanine. Molecular Cell 14 105–116. (https://doi.org/10.1016/s1097-2765(04)00162-5)
Higuchi F, Nagashima H, Ning J, Koerner MVA, Wakimoto H & Cahill DP 2020 Restoration of temozolomide sensitivity by PARP inhibitors in mismatch repair deficient glioblastoma is independent of base excision repair. Clinical Cancer Research 26 1690–1699. (https://doi.org/10.1158/1078-0432.CCR-19-2000)
Hijioka S, Sakuma K, Aoki M, Mizuno N, Kuwahara T, Okuno N, Hara K & Yatabe Y 2019 Clinical and in vitro studies of the correlation between MGMT and the effect of streptozocin in pancreatic NET. Cancer Chemotherapy and Pharmacology 83 43–52. (https://doi.org/10.1007/s00280-018-3700-y)
Hsu CY, Ho HL, Lin SC, Ho TD-H & Ho DM-T 2017 The MGMT promoter single-nucleotide polymorphism rs1625649 had prognostic impact on patients with MGMT methylated glioblastoma. PLoS ONE 12 e0186430. (https://doi.org/10.1371/journal.pone.0186430)
Jue TR, Nozue K, Lester AJ, Joshi S, Schroder LBW, Whittaker SP, Nixdorf S, Rapkins RW, Khasraw M & McDonald KL 2017 Veliparib in combination with radiotherapy for the treatment of MGMT unmethylated glioblastoma. Journal of Translational Medicine 15 61. (https://doi.org/10.1186/s12967-017-1164-1)
Kaina B, Christmann M, Naumann S & Roos WP 2007 MGMT: key node in the battle against genotoxicity, carcinogenicity and apoptosis induced by alkylating agents. DNA Repair 6 1079–1099. (https://doi.org/10.1016/j.dnarep.2007.03.008)
Khalil S, Fabbri E, Santangelo A, Bezzerri V, Cantù C, Di Gennaro G, Finotti A, Ghimenton C, Eccher A, Dechecchi M, et al. 2016 miRNA array screening reveals cooperative MGMT-regulation between miR-181d-5p and miR-409-3p in glioblastoma. Oncotarget 7 28195–28206. (https://doi.org/10.18632/oncotarget.8618)
Kitange GJ, Mladek AC, Carlson BL, Schroeder MA, Pokorny JL, Cen L, Decker PA, Wu W, Lomberk GA, Gupta SK, et al. 2012 Inhibition of histone deacetylation potentiates the evolution of acquired temozolomide resistance linked to MGMT upregulation in glioblastoma xenografts. Clinical Cancer Research 18 4070–4079. (https://doi.org/10.1158/1078-0432.CCR-12-0560)
Klapacz J, Meira LB, Luchetti DG, Calvo JA, Bronson RT, Edelmann W & Samson LD 2009 O6-methylguanine-induced cell death involves exonuclease 1 as well as DNA mismatch recognition in vivo. PNAS 106 576–581. (https://doi.org/10.1073/pnas.0811991106)
Kohsaka S, Wang L, Yachi K, Mahabir R, Narita T, Itoh T, Tanino M, Kimura T, Nishihara H & Tanaka S 2012 STAT3 inhibition overcomes temozolomide resistance in glioblastoma by downregulating MGMT expression. Molecular Cancer Therapeutics 11 1289–1299. (https://doi.org/10.1158/1535-7163.MCT-11-0801)
Koumarianou A, Kaltsas G, Kulke MH, Oberg K, Strosberg JR, Spada F, Galdy S, Barberis M, Fumagalli C, Berruti A, et al. 2015 Temozolomide in advanced neuroendocrine neoplasms: pharmacological and clinical aspects. Neuroendocrinology 101 274–288. (https://doi.org/10.1159/000430816)
Kreth S, Limbeck E, Hinske LC, Schütz SV, Thon N, Hoefig K, Egensperger R & Kreth FW 2013 In human glioblastomas transcript elongation by alternative polyadenylation and miRNA targeting is a potent mechanism of MGMT silencing. Acta Neuropathologica 125 671–681. (https://doi.org/10.1007/s00401-013-1081-1)
Kristensen LS, Nielsen HM, Hager H & Hansen LL 2011 Methylation of MGMT in malignant pleural mesothelioma occurs in a subset of patients and is associated with the T allele of the rs16906252 MGMT promoter SNP. Lung Cancer 71 130–136. (https://doi.org/10.1016/j.lungcan.2010.05.008)
Krug S, Boch M, Rexin P, Gress TM, Michl P & Rinke A 2017 Impact of therapy sequence with alkylating agents and MGMT status in patients with advanced neuroendocrine tumors. Anticancer Research 37 2491–2500. (https://doi.org/10.21873/anticanres.11590)
Kulke MH, Hornick JL, Frauenhoffer C, Hooshmand S, Ryan DP, Enzinger PC, Meyerhardt JA, Clark JW, Stuart K, Fuchs CS, et al. 2009 O6-methylguanine DNA methyltransferase deficiency and response to temozolomide-based therapy in patients with neuroendocrine tumors. Clinical Cancer Research 15 338–345. (https://doi.org/10.1158/1078-0432.CCR-08-1476)
Kushwaha D, Ramakrishnan V, Ng K, Steed T, Nguyen T, Futalan D, Akers JC, Sarkaria J, Jiang T, Chowdhury D, et al. 2014 A genome-wide miRNA screen revealed miR-603 as a MGMT-regulating miRNA in glioblastomas. Oncotarget 5 4026–4039. (https://doi.org/10.18632/oncotarget.1974)
Lavon I, Fuchs D, Zrihan D, Efroni G, Zelikovitch B, Fellig Y & Siegal T 2007 Novel mechanism whereby nuclear factor kappaB mediates DNA damage repair through regulation of O(6)-methylguanine-DNA-methyltransferase. Cancer Research 67 8952–8959. (https://doi.org/10.1158/0008-5472.CAN-06-3820)
Lee YY, Yarmishyn AA, Wang ML, Chen HY, Chiou SH, Yang YP, Lin CF, Huang PI, Chen YW, Ma HI, et al. 2018 MicroRNA-142-3p is involved in regulation of MGMT expression in glioblastoma cells. Cancer Management and Research 10 775–785. (https://doi.org/10.2147/CMAR.S157261)
Lemelin A, Barritault M, Hervieu V, Payen L, Péron J, Couvelard A, Cros J, Scoazec JY, Bin S, Villeneuve L, et al. 2019 O6-methylguanine-DNA methyltransferase (MGMT) status in neuroendocrine tumors: a randomized phase II study (MGMT-NET). Digestive and Liver Disease 51 595–599. (https://doi.org/10.1016/j.dld.2019.02.001)
Leng S, Bernauer AM, Hong C, Do KC, Yingling CM, Flores KG, Tessema M, Tellez CS, Willink RP, Burki EA, et al. 2011 The A/G allele of rs16906252 predicts for MGMT methylation and is selectively silenced in premalignant lesions from smokers and in lung adenocarcinomas. Clinical Cancer Research 17 2014–2023. (https://doi.org/10.1158/1078-0432.CCR-10-3026)
Liu IH, Ford JM & Kunz PL 2016 DNA-repair defects in pancreatic neuroendocrine tumors and potential clinical applications. Cancer Treatment Reviews 44 1–9. (https://doi.org/10.1016/j.ctrv.2015.11.006)
Lok BH, Gardner EE, Schneeberger VE, Ni A, Desmeules P, Rekhtman N, de Stanchina E, Teicher BA, Riaz N, Powell SN, et al. 2017 PARP
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
https://erc.bioscientifica.com © 2020 Society for Endocrinology
R404L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
inhibitor activity correlates with SLFN11 expression and demonstrates synergy with temozolomide in small cell lung cancer. Clinical Cancer Research 23 523–535. (https://doi.org/10.1158/1078-0432.CCR-16-1040)
Middleton MR, Friedlander P, Hamid O, Daud A, Plummer R, Falotico N, Chyla B, Jiang F, McKeegan E, Mostafa NM, et al. 2015 Randomized phase II study evaluating veliparib (ABT-888) with temozolomide in patients with metastatic melanoma. Annals of Oncology 26 2173–2179. (https://doi.org/10.1093/annonc/mdv308)
Mikeska T, Bock C, El-Maarri O, Hübner A, Ehrentraut D, Schramm J, Felsberg J, Kahl P, Büttner R, Pietsch T, et al. 2007 Optimization of quantitative MGMT promoter methylation analysis using pyrosequencing and combined bisulfite restriction analysis. Journal of Molecular Diagnostics 9 368–381. (https://doi.org/10.2353/jmoldx.2007.060167)
Mojas N, Lopes M & Jiricny J 2007 Mismatch repair-dependent processing of methylation damage gives rise to persistent single-stranded gaps in newly replicated DNA. Genes and Development 21 3342–3355. (https://doi.org/10.1101/gad.455407)
Neto JC, Carvalho K, Olivieri E, Carraro D, Cunha I, Vassallo J, Kagohara L, Soares F & Rocha R 2011 Evaluation of O6-methylguanine-DNA methyltransferase by immunohistochemistry: best clinical and research practices. Pathology, Research and Practice 207 492–497. (https://doi.org/10.1016/j.prp.2011.06.003)
Ochs K & Kaina B 2000 Apoptosis induced by DNA damage O6-methylguanine is Bcl-2 and caspase-9/3 regulated and Fas/caspase-8 independent. Cancer Research 60 5815–5824.
Owen DH, Alexander AJ, Konda B, Wei L, Hemminger JA, Schmidt CR, Abdel-Misih SRZ, Dillhoff ME, Sipos JA, Kirschner LS, et al. 2017 Combination therapy with capecitabine and temozolomide in patients with low and high grade neuroendocrine tumors, with an exploratory analysis of O6-methylguanine DNA methyltransferase as a biomarker for response. Oncotarget 8 104046–104056. (https://doi.org/10.18632/oncotarget.22001)
Palma JP, Wang YC, Rodriguez LE, Montgomery D, Ellis PA, Bukofzer G, Niquette A, Liu X, Shi Y, Lasko L, et al. 2009 ABT-888 confers broad in vivo activity in combination with temozolomide in diverse tumors. Clinical Cancer Research 15 7277–7290. (https://doi.org/10.1158/1078-0432.CCR-09-1245)
Pavel M, O’Toole D, Costa F, Capdevila J, Gross D, Kianmanesh R, Krenning E, Knigge U, Salazar R, Pape UF, et al. 2016 Enets consensus guidelines update for the management of distant metastatic disease of intestinal, pancreatic, bronchial neuroendocrine neoplasms (NEN) and NEN of unknown primary site. Neuroendocrinology 103 172–185. (https://doi.org/10.1159/000443167)
Pegg AE 2011 Multifaceted roles of alkyltransferase and related proteins in DNA repair, DNA damage, resistance to chemotherapy, and research tools. Chemical Research in Toxicology 24 618–639. (https://doi.org/10.1021/tx200031q)
Perazzoli G, Prados J, Ortiz R, Caba O, Cabeza L, Berdasco M, Gónzalez B & Melguizo C 2015 Temozolomide resistance in glioblastoma cell lines: implication of MGMT, MMR, P-glycoprotein and CD133 expression. PLoS ONE 10 e0140131. (https://doi.org/10.1371/journal.pone.0140131)
Pietanza MC, Waqar SN, Krug LM, Dowlati A, Hann CL, Chiappori A, Owonikoko TK, Woo KM, Cardnell RJ, Fujimoto J, et al. 2018 Randomized, double-blind, Phase II study of temozolomide in combination with either veliparib or placebo in patients with relapsed-sensitive or refractory small-cell lung cancer. Journal of Clinical Oncology 36 2386–2394. (https://doi.org/10.1200/JCO.2018.77.7672)
Pishvaian MJ, Slack RS, Jiang W, He AR, Hwang JJ, Hankin A, Dorsch-Vogel K, Kukadiya D, Weiner LM, Marshall JL, et al. 2018 A phase 2 study of the PARP inhibitor veliparib plus temozolomide in patients
with heavily pretreated metastatic colorectal cancer. Cancer 124 2337–2346. (https://doi.org/10.1002/cncr.31309)
Plummer R, Lorigan P, Steven N, Scott L, Middleton MR, Wilson RH, Mulligan E, Curtin N, Wang D, Dewji R, et al. 2013 A phase II study of the potent PARP inhibitor, Rucaparib (PF-01367338, AG014699), with temozolomide in patients with metastatic melanoma demonstrating evidence of chemopotentiation. Cancer Chemotherapy and Pharmacology 71 1191–1199. (https://doi.org/10.1007/s00280-013-2113-1)
Qi Z & Tan H 2020 Association between MGMT status and response to alkylating agents in patients with neuroendocrine neoplasms: a systematic review and meta-analysis. Bioscience Reports 40 BSR20194127. (https://doi.org/10.1042/BSR20194127)
Quillien V, Lavenu A, Karayan-Tapon L, Carpentier C, Labussière M, Lesimple T, Chinot O, Wager M, Honnorat J, Saikali S, et al. 2012 Comparative assessment of 5 methods (methylation-specific polymerase chain reaction, methylight, pyrosequencing, methylation-sensitive high-resolution melting, and immunohistochemistry) to analyze O6-methylguanine-DNA-methyltranferase in a series of 100 glioblastoma patients. Cancer 118 4201–4211. (https://doi.org/10.1002/cncr.27392)
Raj N, Klimstra DS, Horvat N, Zhang L, Chou JF, Capanu M, Basturk O, Do RKG, Allen PJ & Reidy-Lagunes D 2017 O6-Methylguanine DNA methyltransferase status does not predict response or resistance to alkylating agents in well-differentiated pancreatic neuroendocrine tumors. Pancreas 46 758–763. (https://doi.org/10.1097/MPA.0000000000000842)
Ramakrishnan V, Kushwaha D, Koay DC, Reddy H, Mao Y, Zhou L, Ng K, Zinn P, Carter B & Chen CC 2011 Post-transcriptional regulation of O(6)-methylguanine-DNA methyltransferase MGMT in glioblastomas. Cancer Biomakers: Section A of Disease Markers 10 185–193. (https://doi.org/10.3233/CBM-2012-0245)
Rapkins RW, Wang F, Nguyen HN, Cloughesy TF, Lai A, Ha W, Nowak AK, Hitchins MP & McDonald KL 2015 The MGMT promoter SNP rs16906252 is a risk factor for MGMT methylation in glioblastoma and is predictive of response to temozolomide. Neuro-Oncology 17 1589–1598. (https://doi.org/10.1093/neuonc/nov064)
Robins HI, Zhang P, Gilbert MR, Chakravarti A, de Groot JF, Grimm SA, Wang F, Lieberman FS, Krauze A, Trotti AM, et al. 2016 A randomized phase I/II study of ABT-888 in combination with temozolomide in recurrent temozolomide resistant glioblastoma: an NRG oncology RTOG group study. Journal of Neuro-Oncology 126 309–316. (https://doi.org/10.1007/s11060-015-1966-z)
Robinson C, Palomo J & Vogelbaum MA 2010 Thin layer chromatography-based assay of O6-methylguanine-DNA methyltransferase activity in tissue. Analytical Biochemistry 405 263–265. (https://doi.org/10.1016/j.ab.2010.06.019)
Roos WP, Nikolova T, Quiros S, Naumann SC, Kiedron O, Zdzienicka MZ & Kaina B 2009 BRCA2/Xrcc2 dependent HR, but not NHEJ, is required for protection against O(6)-methylguanine triggered apoptosis, DSBs and chromosomal aberrations by a process leading to SCEs. DNA Repair 8 72–86. (https://doi.org/10.1016/j.dnarep.2008.09.003)
Sahnane N, Furlan D, Monti M, Romualdi C, Vanoli A, Vicari E, Solcia E, Capella C, Sessa F & La Rosa S 2015 Microsatellite unstable gastrointestinal neuroendocrine carcinomas: a new clinicopathologic entity. Endocrine-Related Cancer 22 35–45. (https://doi.org/10.1530/ERC-14-0410)
Sato A, Sunayama J, Matsuda K, Seino S, Suzuki K, Watanabe E, Tachibana K, Tomiyama A, Kayama T & Kitanaka C 2011 MEK-ERK signaling dictates DNA-repair gene MGMT expression and temozolomide resistance of stem-like glioblastoma cells via the MDM2-p53 axis. Stem Cells 29 1942–1951. (https://doi.org/10.1002/stem.753)
Scarpa A, Chang DK, Nones K, Corbo V, Patch A-M, Bailey P, Lawlor RT, Johns AL, Miller DK, Mafficini A, et al. 2017 Whole-genome
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access

https://erc.bioscientifica.com © 2020 Society for Endocrinology
Printed in Great BritainPublished by Bioscientifica Ltd.https://doi.org/10.1530/ERC-20-0227
R405L de Mestier et al. MGMT status in digestive NET 27:10Endocrine-Related Cancer
landscape of pancreatic neuroendocrine tumours. Nature 543 64–71. (https://doi.org/10.1038/nature21063)
Schmitt AM, Pavel M, Rudolph T, Dawson H, Blank A, Komminoth P, Vassella E & Perren A 2014 Prognostic and predictive roles of MGMT protein expression and promoter methylation in sporadic pancreatic neuroendocrine neoplasms. Neuroendocrinology 100 35–44. (https://doi.org/10.1159/000365514)
Somnay Y, Lubner S, Gill H, Matsumura JB & Chen H 2016 The PARP inhibitor ABT-888 potentiates dacarbazine-induced cell death in carcinoids. Cancer Gene Therapy 23 348–354. (https://doi.org/10.1038/cgt.2016.39)
Su JM, Thompson P, Adesina A, Li XN, Kilburn L, Onar-Thomas A, Kocak M, Chyla B, McKeegan E, Warren KE, et al. 2014 A phase I trial of veliparib (ABT-888) and temozolomide in children with recurrent CNS tumors: a pediatric brain tumor consortium report. Neuro-Oncology 16 1661–1668. (https://doi.org/10.1093/neuonc/nou103)
Toshimitsu H, Yoshimoto Y, Augustine CK, Padussis JC, Yoo JS, Angelica Selim M, Pruitt SK, Friedman HS, Ali-Osman F & Tyler DS 2010 Inhibition of poly(ADP-ribose) polymerase enhances the effect of chemotherapy in an animal model of regional therapy for the treatment of advanced extremity malignant melanoma. Annals of Surgical Oncology 17 2247–2254. (https://doi.org/10.1245/s10434-010-0971-x)
Vatrano S, Giorcelli J, Votta A, Capone G, Izzo S, Gatti G, Righi L, Napoli F, Scagliotti G, Papotti M, et al. 2020 Multiple assays to determine methylguanine-methyltransferase status in lung carcinoids and correlation with clinical and pathological features. Neuroendocrinology 110 1–9. (https://doi.org/10.1159/000500158)
Walter T, Brixi-Benmansour H, Lombard-Bohas C & Cadiot G 2012 New treatment strategies in advanced neuroendocrine tumours. Digestive and Liver Disease 44 95–105. (https://doi.org/10.1016/j.dld.2011.08.022)
Walter T, van Brakel B, Vercherat C, Hervieu V, Forestier J, Chayvialle JA, Molin Y, Lombard-Bohas C, Joly MO & Scoazec JY 2015 O6-Methylguanine-DNA methyltransferase status in neuroendocrine tumours: prognostic relevance and association with response to alkylating agents. British Journal of Cancer 112 523–531. (https://doi.org/10.1038/bjc.2014.660)
Wickström M, Dyberg C, Milosevic J, Einvik C, Calero R, Sveinbjörnsson B, Sandén E, Darabi A, Siesjö P, Kool M, et al. 2015 Wnt/β-catenin pathway regulates MGMT gene expression in cancer and inhibition of Wnt signalling prevents chemoresistance. Nature Communications 6 8904. (https://doi.org/10.1038/ncomms9904)
Yang QC, Wang YH, Lin Y, Xue L, Chen YJ, Chen MH & Chen J 2014 Expression of O(6)-methylguanine DNA methyltransferase (MGMT) and its clinical significance in gastroenteropancreatic neuroendocrine neoplasm. International Journal of Clinical and Experimental Pathology 7 4204–4212.
Yu W, Zhang L, Wei Q & Shao A 2019 O6-methylguanine-DNA methyltransferase (MGMT): challenges and new opportunities in glioma chemotherapy. Frontiers in Oncology 9 1547. (https://doi.org/10.3389/fonc.2019.01547)
Zhang W, Zhang J, Hoadley K, Kushwaha D, Ramakrishnan V, Li S, Kang C, You Y, Jiang C, Song SW, et al. 2012 miR-181d: a predictive glioblastoma biomarker that downregulates MGMT expression. Neuro-Oncology 14 712–719. (https://doi.org/10.1093/neuonc/nos089)
Received in final form 9 July 2020Accepted 21 July 2020Accepted Manuscript published online 22 July 2020
Downloaded from Bioscientifica.com at 03/29/2022 07:23:52AMvia free access