CRANA Inc - Services for Australian Rural and Remote...
48
-
Upload
nguyencong -
Category
Documents
-
view
214 -
download
1
Transcript of CRANA Inc - Services for Australian Rural and Remote...


Published by the Council of Remote Area Nurses of Australia Incwith the support of the Commonwealth Dept of Health and Ageing’sRural Health Support Education and Training (RHSET) Program
CRANA IncPMB 203Alice Springs N.T. 0872
Telephone (08) 8953 5244Facsimile (08) 8953 5245Internet address: www.crana.org.au
Copyright CRANA Inc. 2000ISBN 0-646-40231-5
Cover design, layout and printing by Asprint, Alice SpringsTelephone (08) 8952 8877
DISCLAIMER
The contents of this booklet are intendedonly as a guide to the issues discussed.
The author and CRANA expressly disclaimall and any liability to any person, in respectof anything, or the consequences ofanything, done or omitted to be done, byany person in reliance, whether wholly orpartially, upon the statements containedwithin this booklet.
C R A N ACouncil of Remote Area Nurses of Australia Incorporated
A Guide for Remote Health Practitioners

Avoiding Burn-out in Remote AreasSurviving the day-to-day hassles: a guide for remote
health practitioners
Written by Kerrie Kelly, Program Coordinator, CRANA Bush Crisis Line & Support Services
Acknowledgements
Sincere thanks to the CRANA Bush Crisis Line & Support Services Critical Reference Group fortheir comments and input into the development of this booklet.
Members include:Ree Dunne, remote area nurse, NTRon Archer, cross cultural facilitator, Qld.Damien Howard, psychologist, NTErnest Hunter, psychiatrist, QldCraig San Roque, psychologist, NTMandy Seal, remote GP, WARobert Williams, psychologist, QldJohn Wilson, remote manager, SAJames Woolridge, psychiatrist, Qld
Additional comments and feedback were also received from:Sue Lenthall, Centre for Remote Health (Alice Springs)Bernadette Ward, CRANA Board of ManagementAmanda Bigg, Bush Crisis Line & Support Services Administration Officer
This is the first edition of this booklet.
Suggestions about how it may be improved will be gratefully accepted. Send comments andsuggestions to CRANA Bush Crisis Line & Support Services, PMB 203, Alice Springs, NT 0872.
Additional copies can be ordered from the above address.
Funding for the publication of this booklet was provided by the Commonwealth Department ofHealth and Ageing Rural Health Support Education and Training (RHSET) Program.
August 2000Reprinted Dec. 2002
Council of Remote Area Nurses of Australia Incorporated
C R A N A
This booklet has been developedspecifically to support health
practitioners working in remotecommunities.
However health practitionersworking in small rural communities
may find some sections of thebooklet can be usefully applied to
their setting.
FREECALL:
1800 805 391
INTRODUCTION 6
Chapter One:REMOTE HEALTH SERVICES AND PRACTITIONERS: FEW AND FAR BETWEEN 7
Chapter Two:STRESS AND HOW IT AFFECTS YOU 13
Chapter Three:THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE 19
Chapter Four:PREVENTABLE SOURCES OF STRESS ASSOCIATED WITH REMOTE PRACTICE 35
Chapter Five:AVOIDINGTHE SLOW SIZZLE OF BURN OUT 41
Chapter Six:AVOIDING CRASH AND BURN: COPING WITH TRAUMATIC STRESS 57
Chapter Seven:WHEN ALL ELSE FAILS (IF THE HORSE HAS ALREADY BOLTED) 63
Chapter Eight:COPING STRATEGIES 69
REFERENCES 88
Page
PERSONAL SUPPORT FOR REMOTE HEALTHPRACTITIONERS
This booklet is one of a range of resources developedby the CRANA Bush Crisis Line & Support Services usingfunding provided by the Commonwealth Departmentof Health and Ageing through the Rural Health SupportEducation and Training (RHSET) Program.
The CRANA Bush Crisis Line & Support Services aimsto contribute to the well-being and retention of multi-disciplinary health practitioners by supporting them andtheir families to successfully manage the stress associatedwith remote and rural practice.
BUSH CRISIS LINE24 hour confidential telephone debriefingand support for multi-disciplinary remote &rural health practitioners and their families.
CONTENTS
76
Remote health practice can offer be a challeging and intensely rewarding expe- rience. It offers practitioners a unique opportunity to provide holistic care forindividuals, families and communities across the lifespan.
Yet, historically it has been extremely difficult to attract health practitioners to work outbush. Even when they do take up the challenge they tend not to stay. The turnover ofhealth practitioners in remote areas has always been extraordinarily high.
Anecdotal evidence suggests high levels of job related stress have been a major con-tributor to staff turnover. Burn-out rates are thought to be very high. Yet there is littleliterature which explicitly examines the stress associated with remote practice.
This booklet aims to identify some of the major sources of stress associated with remotehealth practice. It also attempts to offer some skills and strategies to assist practitioners tosuccessfully deal with some of these pressures.
It begins by describing the context of remote practice in chapter one.
Chapter two provides an overview of how stress can affect practitioners, what stressreactions feel like, and the impact prolonged stress responses can have on their well-being.
Chapter three identifies some of the unique sources of day-to-day stress out bush. Thisincludes the stress associated with adaptation to remote practice, and some of theunavoidable differences practitioners will need to adjust to.
Chapters 3 to 7 have suggested strategies sections whichg refer the reader to appropriatecoping strategies in Chapter 8.
Chapter four briefly examines some of the preventable sources of stress associatedwith remote practice.
Chapter five examines ways to maintain long-term well-being and to avoid burn-out inthe face of these challenges.
Chapter six briefly touches on job-related traumatic stress. This can occur as a result ofresponding to sudden accidents and emergencies. Some strategies to promote recoveryfollowing such events are offered.
Chapter seven looks at what can be done if, despite their best attempts to prevent it, thepractitioner burns out anyway.
Finally, a range of practical strategies to manage some of the day-to-day challengesand stresses are drawn together for remote practitioners to pick and choose from asthey wish in chapter eight.
INTRODUCTION
Chapter One
REMOTE HEALTH SERVICES ANDPRACTITIONERS: FEW AND FAR BETWEEN

98
Remote Employers
Remote health practitioners work in a variety of settings. These include Aboriginal andTorres Strait Islander communities, railway, tourism, pastoral, mining and offshore islandcommunities.
Employers might be state governments, mining companies, independent communitycontrolled organisations, the Royal Flying Doctor Service, local community boards,religious affiliated organisations, or bush nursing associations. Some doctors in remoteareas are wholly or partly self employed.
Most employing organisations are located hundreds of kilometres away from the remotecommunity itself.
Remote Health Practice
There is not a great deal of uniformity in remote practice. The roles of industry-basedstaff such as those working for mining companies, tourist islands or oil-rigs are usuallyfocused on providing accident and emergency responses and dealing with occupationalhealth and safety issues.
However, the most common form of health service delivery tends to be a communityclinic staffed by a multidisciplinary team of generalist health practitioners. The on-sitehealth team usually consists of remote area nurses and, if an indigenous community,indigenous Health Workers. In some situations, a doctor may be contracted to provideGP services as part of the on-site team. On-site health services are usually supplementedby visiting services by specialists based in regional centres.
Between them the on-site team provides a 24-hour primary care service (curative service).This includes accident and emergency, acute care, referral, follow-up and rehabilitativecare for members of the community. If hospitalisation is required, transfer to a regionalcentre is usually necessary.
While a few doctors live and work on-site in remote communities, more often than notthey are based in regional centres. From here they provide 24-hour clinical back up andsupport to several on-site teams, usually by telephone, and facilitate emergencyevacuations from remote communities to regional centres. Some travel to remotecommunities to provide regular visiting GP services on-site. These services are oftenprovided by or in conjunction with, the Royal Flying Doctor Service.
Services taken for granted in rural or urban settings such as on-site doctors, pharmacy, x-ray, pathology, ambulance service or a range of allied health services such as dentists,social workers and physiotherapists are usually not available in remote communities. Mostremote health practitioners, regardless of professional background, are required to workin extended roles to provide elements of these ‘missing’ health services. This is true forthose providing visiting services as well. This is commonly known as adopting an ‘extendedgeneralist role’. Some provide veterinary services as well.
Chapter OneREMOTE HEALTH SERVICES ANDPRACTITIONERS: FEW AND FAR BETWEEN
T he further the fewer describes the population distribution as onemoves from the major towns and cities situated on the coastal fringes of Australia.
Only about three percent of the population live in the more remote areas of Australia.Remote owns tend to be small, with populations of 5,000 or less.
The land itself tends to be characterised by very low or high rainfall and what is termed‘degraded or depleted soil, water or vegetation resources’ (Department of Primary Industries& Energy and Department Human Services & Health, 1994). Environmental conditionstend to be extreme - very high or low temperatures, lots of dust, wind and insects.
Transport, communications infrastructure, public utilities and commercial, financial andgovernment services tend to be very basic. Most goods and services cost more.
Some people live out bush because of their work - mining, broad acre farming, railway,or tourism.
However, the majority of people in remote areas tend to be Aboriginal and Torres StraitIslander people who have long-term associations with the land. Aboriginal and TorresStrait Islander communities tend not to have an economic infrastructure.
Health Resources - The Further The Fewer
As with most other things, the further one gets from the cities, the fewer the healthresources become. This is influenced by resource allocation at a federal, state andregional level as well as organisational, climatic, geographical, population and otherfactors.
There tends to be fewer health services and practitioners per head of population whencompared to urban settings.
As a result, remote practitioners provide a higher proportion of health care services tolarger pools of people than their urban counterparts.
Historically, it has been extremely difficult to attract medical practitioners to work inremote communities. Service delivery has been characterised by substitution of GPservices by nurses and Health Workers and telephone consultations. Specialist servicesare more likely to be provided by GPs than by specialists (McDermott, 1994).
The outcome of this for residents of remote communities has been restricted access tohealth services and resources when compared to those living in the cities.
Some see this inequity and disadvantage as a human rights issue.

1110
REMOTE HEALTH SERVICES AND PRACTITIONERS: FEW AND FAR BETWEEN
Why do they do it?
Why do health practitioners choose to provide their services to residents of remotecommunities?
The motivations are likely to be as many and varied as the practitioners themselves.
Some practitioners are motivated to work out bush because they enjoy providing healthservices in a small community where everybody knows everybody else - having animportant role can be a rewarding experience.
Some Indigenous Health Workers may have been nominated by the community to carrythe responsibility for the health of the community.
Some practitioners may be drawn by the remote lifestyle and landscape. Others may bemotivated to address the inequity reflected in the health statistics of remotecommunities. Some may be attracted by the increased remuneration.
Regardless of their motivation, all practitioners who choose to provide health services inremote settings will be challenged by the task set before them. It will be unlike anyother job they have done before.
Summary
Remote practice can be very rewarding work. It offers practitioners an opportunity toprovide holistic health care to individuals, families and communities in a way that cannotoccur in the cities. Care can be provided from birth to death with continuity andmeaningfulness within the context of the lives of the practitioner, their clients and thecommunity. The larger population base in urban areas requires the fragmentation ofthe various elements of health care in order for health services to function.
Successfully meeting the challenges posed by remote practice can offer practitionersintense satisfaction on both a personal and professional level.
However, in light of the current under-resourcing of remote health services, remotepractice also has the potential to overwhelm the coping resources of any practitioner.
While practitioners deal with the stress associated with health practice in general, theyalso carry a unique burden of stress that arises out of the context of remote practice.They therefore need to be particularly active in caring for themselves if they are not tobecome overwhelmed by their role(s).
CHAPTER 1
As well as providing curative services, the on-site health team is required to practicewithin a primary health care philosophy and framework - as per the World HealthOrganisation Alma-Ata Declaration of 1978. This includes taking on a communitydevelopment and consultation role in relation to health promotion and illness prevention,developing and implementing early intervention and harm minimisation strategies,developing responses to meet the expressed health needs of the community, andparticipating in population and public health programs.
Thus remote practice involves meeting a community’s health needs across the broadspectrum of possibilities. Providing continuous and coordinated acute and public healthcare for individuals, families and the community can be a challenging task for the smallteams of on-site practitioners.
In some instances, providing acute care services twenty four hours a day, seven days aweek can absorb the limited resources of the on-site team and leave them unable toattend to the broader primary health care role expected of them.
This is often cited as a particular source of frustration for those working in Aboriginal orTorres Strait Islander communities. High levels of preventable morbidity and mortality(ie the source of high demands for curative health services) often have their roots ininadequate housing, poor nutrition, lack of clean water and sanitation and lifestyle issues.Many practitioners report that the lack of funding and resources limits their ability toprovide more than a curative service. The frustration associated with being unable toaddress the underlying causes of ill health in a community can be a source of ongoingstress for many on-site health teams.
It’s a Multi-disciplinary Health Team, Right?
Historically, remote health service provision has relied on multi-disciplinary teams.However the functioning of these teams tends to be different from those in the cities.The notion that practitioners from a variety of disciplines cooperate to provide coordinatedcare doesn’t always hold true in the bush.
Geography, time constraints, and the expense associated with travel all contribute to asituation where the multi-disciplinary team rarely meets face to face as a group orparticipate in team activities usually associated with a ‘multi-disciplinary team approach’.
Visiting health services tend to be ‘staggered’ in time to allow access to on-site staff,facilities and clients. Visits tend to be busy, have a curative focus, and are mostly basedon client presentations for clinical services. Those providing visiting health servicesrarely have the time or opportunity to participate in the planning or coordination ofmulti-disciplinary care.
The on-site health team tends to be the only common point of contact between thecommunity, clients, and the various visiting health service providers. Health care tendsto be mediated and coordinated through them.
1312
Chapter Two
STRESS AND HOW IT AFFECTS YOU

1514
released into the bloodstream, triggering a chain of reactions throughout the body.Every part of the body is affected. A large amount of energy is made available and thebody is prepared to either fight or run very quickly away from the danger (ie fight orflight). This response can literally save our lives.
• Breathing rate slows down
• Heart rate slows down
• Blood pressure reduces
• Muscles relax
• All organs adequately perfused
• Blood returns to usual clotting ability
• Thinking broadens and becomes less extreme
• Feelings are less extreme
The major emotions associated with a stress response tend to beanger (‘fight’) and fear (‘flight’).
A short-term stress response is useful and positive. It providesenergy and motivation to respond to challenges and threats.When the threat is over the parasympathetic (relaxation)nervous system kicks in and neutralises the effects of the stressresponse. No harm is done.
STRESS AND HOW IT AFFECTS YOU
Breathing rate increasesHeart beats faster and more stronglyBlood pressure increasesBlood clotting ability increases in case of injuryMuscles tense ready for actionSweating increases to cool the bodyBlood diverts to body’s emergency functionsNon emergency functions close down: digestion, skinperfusion, sexual activity.
Body: enables immediate, strong,powerful physical response todanger.
Mind: enables focused, decisive,immediate, and strong reactions.
Emotions: feelings are strong to give powerto responses.
Chapter Two
STRESS AND HOW IT AFFECTS YOU
Understanding stress
Before we look at some of the causes of stress associated with remote practice it may beuseful to refresh our knowledge of the impact that stress can have on the practitioner’smind, body, feelings and long-term wellbeing.
Stress reactions depend very much on the eye of the beholder. This is an important point.Stress responses are activated not by what happens in itself but by how the person interpretswhat is happening. What is stressful for one person may not be for someone else - what onemay see as dangerous and threatening, another may see as challenging or exciting.
Lazarus (1984) suggested stress is an outcome of the interaction of the person and thesituation. External events make unusual or extraordinary demands on the person.Depending on the person’s assessment of how well or poorly they will be able to copewith these demands, a milder or stronger stress response will result. Usually some stressor ‘strain’ results until some sort of a balance between the demand and the person’sability to respond is achieved.
Generally, if a big difference exists between the demand made on the person and how wellthey think they can cope with it, their stress reaction (ie the ‘strain’ to cope) will be stronger.
Indeed, many people don’t recognise they have a problem with stress until their abilityto cope is outweighed by stressful events.
How stress can affect you
Our bodies are continually changing in response to what is happening around us. Werelax when things are going well. We tense up and become more alert when newchallenges arise.
Usually, how alert someone feels is a product of the interplay of the two parts of theautonomic nervous system: the parasympathetic (relaxation) and the sympathetic (fightand flight) nervous systems. Although the two systems act in opposition to one another,they are usually both active at the same time. The relative dominance of one or theother will determine how stressed or relaxed they feel at any given time.
While going about one’s daily business these fluctuations in energy tend to be so mildthat they are hardly noticed. In fact, low level stress responses help to add interest andexcitement to life. They help us to feel really ‘alive’ - they keeps us on our toes, help usto think and move more quickly and to work more intensively - they give us an ‘edge’.
When faced with a big threat or danger, our ‘panic buttons’ go on and the sympatheticnervous system becomes dominant. The chemicals adrenaline and noradrenaline are
1716
STRESS AND HOW IT AFFECTS YOU
Prolonged stress responses can increase the risk of:
• Heart disease
• Hypertension
• Strokes - from clots or hypertension
• Infectious diseases - immune system becomes less effective over time
• Sleep deprivation
• Physical & emotional exhaustion
Effects of long-term stress responses on the mind
Over the long-term high levels of stress can impair performance. Those who are stressedhave a tendency to:
• remain focused on the stressor - seem tunnel visioned and distracted
• have difficulty in thinking broadly and well
• have difficulty in setting priorities and making decisions
• have difficulty concentrating
• have impaired ability to learn new information - poor short-term memory
Over time, psychological energy is drained, performance becomes impaired, and self-esteem starts to plummet.
Effect of long-term stress responses on emotions
Emotions come in response to thoughts. When stressed, one’s emotions tend to bestronger than usual. This can have a pendulum or a ‘roller coaster’ effect on thepractitioner’s emotional life. If they think positive thoughts, strongly positive emotionstend to follow. If they think negative thoughts, strongly negative emotions tend toresult. This swinging between strong emotions is usually what makes those who arevery stressed think they are going crazy or losing control.
Effect of prolonged stress on those around them
While it is unpleasant to live in a chronically stressed state, those who are stressed canalso be difficult to be around. They may seem tense, hostile, impatient and intolerant(expressing ‘fight’) or alternatively anxious, fearful and withdrawn (expressing ‘flight’).It is not surprising that conflict with others can increase and relationships start todeteriorate.
Isolation is a not an uncommon outcome of prolonged stress. This usually results frommutual withdrawal. If the practitioner seems hostile and difficult to deal with, othersstart to limit their interactions with them. At the same time the practitioner may find iteasier to be alone - particularly if they are feeling fearful or angry much of the time and/ or finding relationships difficult to manage.
CHAPTER 2
Effects of long-term stress
Short-term stress responses are positive, life enhancing reactions - problems only arisewhen stress responses are prolonged.
It may be helpful to think of a stress response as similar to low-range four-wheel drive.While it is very useful to get out of tough spots, it is not designed for long-range touring.If a vehicle becomes stuck in low range four-wheel-drive while on a long trip, is likely tobreak down eventually. Usually it will give out at its weakest point.
People are much the same. Stress reactions put enormous pressure on all body systems,and cannot be maintained for long before the person either becomes exhausted or theirbody gives out at the weakest point. This is often a genetic weak point - the risk isincreased that they will succumb to whatever illnesses run in the family.
Stress responses become a liability if they continue for weeks, months or years. Whatwas meant to be a protective mechanism can become a source of harm.
Effects of long-term stress on the body
Symptoms of prolonged stress responses may include:
• Insomnia
• Restlessness
• Digestive upsets (diarrhoea and / or constipation)
• Increased blood pressure
• Palpitations
• Tremors
• Nausea
• Heartburn
• Muscle aches
• Headaches
• Lack of interest in, or ability for sex
• Immune system less effective.
These are a direct result of having the sympathetic nervous system dominant for longperiods of time.
1918
Chapter Three
THE CHALLENGE OF ADAPTING TOREMOTE PRACTICE
CHAPTER 2
Those who are stressed have a tendency to give their energy and focus to what is stressingthem. Other activities and interests can fall by the wayside. In particular, fun, frivolity,humour and the ability to enjoy life often go out the door.
Prolonged stress usually leads to a decrease in the practitioner’s quality of life.
Burn-out
Eventually prolonged stress responses can lead to ‘burn out’.
Burn-out has several core characteristics: emotional and physical exhaustion, low self-esteem, poor job satisfaction and a negative and cynical attitude towards clients.
Often the practitioner starts to think their clients deserve their health problems.
Insomnia, increased use of alcohol and other drugs, and relationship and family problemsare commonly associated with burn out.
It is important to remember that burn-out rarely happens suddenly - it occurs over time.
Self care is both prevention and cure for burn-out.
Before we look at self-care it is necessary to look at some of the sources of stress thatconfront remote practitioners when they take up remote work. The next two chapterswill examine some of the unavoidable and some of the preventable challenges associatedwith remote practice.
Strategies to prevent burn-out will be offered in chapter five of this booklet.

2120
Suggested Coping Strategies
Adapting to Remote Practice
Maladjustment:• Failure to adjust.
• Becomes overwhelmed by the challenge.
• Uses inappropriate behaviours.
• Engages in behaviours that consistently produce more problems.
Those who use the extra energy in a positive way, that is, to be curious, ask questions,find out more information, and to learn new skills and ways of doing things are likely tobe rewarded by decreasing levels of stress and a corresponding increase in their sense ofmastery, job satisfaction and self-esteem.
The stress associated with adaptation can thus be seen as a force that stimulates growthin practitioners who have enough skills and resources available to respond to meet thisdemand. However, if the challenge (ie the demand made on them) is too great, if theycannot find ways to cope or grow, or use coping strategies which only makes the situationworse, then they are likely to become overwhelmed. Impairment rather than growth islikely to occur. Stress can then become distress.
Practitioners new to remote practice or experienced practitioners new to a remotecommunity would do well to use their newness as an excuse to ask what mightotherwise be seen as ‘dumb’ questions.
Critical reflection is crucial strategy to maximise adaptation in an isolated setting.See page 86Sometimes personal characteristics can hinder adaptation. See page 48
Chapter Three
THE CHALLENGE OF ADAPTING TOREMOTE PRACTICE
When health practitioners begin work in a situation they have not worked inbefore, a period of adaptation or adjustment is expected.
This will give rise to varying levels of stress (ie psychological ‘strain’) until they find theirfeet and become comfortable and effective in their new setting.
Adjusting to the unique demands of remote practice can be a major source of stress forpractitioners. This can impact on those new to remote work or experienced practitionerswho move into new roles, organisations or communities.
Two major forces are at work - the challenges posed by the workplace, and thepractitioner’s ability to respond effectively to meet these challenges.
There are a number of possible responses to this interface between the practitioner andthe workplace. While one can think of them as reactions to the workplace, it is importantto recognise that practitioners bring their own histories, skills, strengths and vulnerabilitiesto the situation as well. This will affect how they perceive and respond to the challengesbefore them.
Outcomes of adaptation are usually a result of the interaction between the practitionerand the workplace.
Successful adaptation can lead to a sense of mastery and job satisfaction, organisationalcommitment and positive self-esteem (Grasha & Kirschenbaum, 1986).
Maladjustment can result if the practitioner becomes overwhelmed or is unable to developthe skills and qualities they need to become effective in their practice. For example, theymay respond in ways that are inappropriate, or which only create more problems.
Most practitioners adapt by transferring their existing skills to the remote situation. Thisusually enables them to get by or to survive. However, essentially they are still using oldways to respond to new challenges.
Becoming effective or competent, ie thriving, means meeting challenges creatively andby responding with growth and change. For example, the practitioner uses their currentskills in new ways, or learns new skills.
The adaptation process and accompanying stress response makes extra energy availableto practitioners - it can be experienced as an exciting, challenging and adventuroustime.

2322
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
Any incongruence between health promotion activities and the lifestyle of the practitionerwill be apparent to all. For example a Quit Smoking campaign may lose its impact ifeveryone knows the practitioner is still smoking. Practitioners may feel some pressure to‘walk their talk’.
Sometimes knowing everyone and everyone knowing the practitioner can be a blessing- when things are going well the practitioner may be seen as some sort of a local hero.At other times it may seem like a curse. When things aren’t going so well, one’s lack ofanonymity may seem oppressive - there is no place to run and no place to hide.
The lack of anonymity can impact on the practitioner’s ability to maintain their privacyand personal space. Residents may believe the practitioner will be eager to meet theirhealth needs at any time of the day or night. Practitioners may find themselves doingconsultations while they are shopping, socialising and so on.
‘I feel quite alienated by having to be a doctor 24 hours a day in the supermarket andeverywhere else’. General Practitioner (Tolhurst, Bell, Baker, Talbot & Cleasby, 1997,p.36).
Accountability can take on new dimensions. Residents happy or unhappy with the healthservice have ample opportunities to express their satisfaction or dissatisfaction directly tothe practitioner.
Talking about work related issues is recognised as an important stress management strategy.Yet opportunities for practitioners to talk about their work can be restricted because ofpotential breaches of confidentiality in small communities. For example, a common ruleof thumb in relation to maintaining confidentiality has been that practitioners may talkabout work related issues with others, eg one’s partner, but only if this can be done in away which does not identify those involved now or in the future. This is difficult to achievewhen most people in small communities know what goes on and who was involved (orwill know eventually).
Practitioners may find themselves to be the keeper of community secrets. This can becomea burden. Knowing some of what goes on ‘behind the scenes’ can influence and complicatethe way in which practitioners see and relate to others socially and professionally.
Knowing everyone and everyone knowing the practitioner can be a positive or negativeexperience.
This will depend on whether the practitioner sees this level of trust and responsibility asenriching or as an intrusive burden, or perhaps as somewhere in between. However, it ispart and parcel of health practice in a small community and the practitioner will need tolearn to live with it.
If the practitioner has grown up in a small community, adjustment to lack of anonymitymay be easier than it will be for those who are accustomed to the anonymity and personalfreedom of urban environments.
CHAPTER 3
Survive:• Uses old ways to meet new challenges.
• Transfers existing skills to new situation - may ‘get by’.
• Still using old ways to meet new challenges.
• Isn’t developing new and more successful behaviours.
Thrive:• Challenges used as growth producing experiences.
• Meets challenges creatively.
• Uses existing skills in innovative ways.
• Learns new skills, knowledge and attitudes.
Some of the unavoidable challenges associated with remote practice
Working in a remote setting is very different to urban practice.
Some suggest remote practice is a lifestyle rather than just a job and the practitioner’swhole way of life will be affected.
Some sources of stress or difference are part and parcel of the remote workplace andcannot be avoided. Since they can’t be changed, it is up to the practitioner to adjust to,or learn to live with these factors.
The following section attempts to identify some of the major dimensions of differenceassociated with remote practice. These are likely to impact on all practitioners regardlessof their professional background or the type of community they work in.
Some of the unique dimensions of difference associated with remote practice can be positiveor negative experiences, depending on how the practitioner sees them at the time.
Lack of anonymity and personal privacy
In small communities, the practitioner is likely to know or know of everybody, andeverybody will know them. This lack of anonymity affects all areas of the practitioner’slife.
Living in small remote communities has often been described as ‘life in a fish bowl’. Allareas of a practitioner’s life may be subject to scrutiny and comment by local residents,not just their professional skills.
‘There’s no privacy, our behaviour is judged quite critically. The standard ofbehaviour that people expect us to maintain doesn’t necessarily apply to the restof the community’ Remote Area Nurse (Kreger, 1991, p. 25).
2524
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
For strategies to:• Identify common errors to avoid when treating friends and family, see page 85• Monitor long term well-being, see page 79• Manage time and set priorities, see page 72• Deal with conflicting demands, see page 74• Solve problems, see page 71• Relax, see page 82
If a remote practitioner wishes to maintain the essence of who they are, keep thespring in their step and the sparkle in their eye, then finding ways to have ‘time out’from their professional duties and responsibilities will be essential.
All remote practitioners should have their own GP, even if the GP is based in town.Telephone consultations may be better than no consultation or self prescribing andself treatment.
developed to suit the majority (ie urban practitioners) whose clients are usually strangersto them. For example, practitioners are usually discouraged from providing health servicesto friends and family, or from developing a relationship with anyone who has been a clientin the past. This is not so simple in small communities.
Sometimes it can be difficult for remote practitioners to access health services to meettheir own or their family’s needs. Other practitioners may not be available (there areplenty of stories about remote practitioners taking their own blood or even doing theirown pap smears!). In some instances practitioners may be reluctant to become theclient of a colleague they will be dealing with professionally in the future - particularly inrelation to sensitive or personal issues.
Those who live on-site may even find their home becomes part of the workplace whenthey are on call - people knock on their door to request assistance after hours.
It can be very difficult for remote practitioners to find the time and space to relax awayfrom their professional roles or just to be themselves.
Some practitioners report this to be personally impoverishing.
Others suggest it is not possible to split the person from the professional in small communities.Rather, it is necessary to combine the two and to become an ‘integrated practitioner’.
Yet some practitioners are uncomfortable with the notion that they must allow clients to knowthem personally as well as professionally – it may goes against the urban-based notion that tobe considered ‘professional’ a practitioner must maintain a ‘professional distance’.
Certainly, maintaining a strongly professional persona can undermine the practitioner’sability to build relationships based on trust with members of the community – somesuggest this is a pre-requisite to effective remote practice.
Suggested Coping Strategies
Lack of boundaries between work and home and blurred professional boundaries
The division between the person and the professional tend to be less clear cut in smallcommunities.
This is due to the lack of anonymity discussed in the previous section and is compoundedby the lack of natural circuit breakers between work and home and between personal andprofessional roles in small communities.
City workers and those who provide visiting health services to remote communities havethe luxury of being able to leave their professional role behind when they go home. Theirpersonal lives may be unconnected to their jobs. Friends and acquaintances may be drawnfrom outside the workplace. They may have a range of recreational activities to choosefrom, for example movies, restaurants, shopping, sporting activities. This helps thepractitioner to have some time to relax away from work and their professional role.
In remote communities, work and home life are not so easily separated. Home may bejust a stroll away from work. Movements may be restricted when the practitioner is oncall. There are likely to be few recreational choices available. Friends and acquaintancesmay be drawn from the workplace, or areas of common interest may be work related.
Professional and social relationships constantly overlap and become blurred in smallcommunities.
Knowing clients personally as well as professionally can make it difficult for practitioners tokeep their personal feelings separate from their professional role. It can also increase thepractitioner’s vulnerability to the impact of traumatic stress if they are required to respondto a clinical emergency that involves someone they know and care about.
Being the only, or one of only a few health care providers in town can create ethicaldilemmas for many practitioners. Professional and ethical guidelines have usually been
Suggested Coping Strategies
CHAPTER 3
Practitioners may need to think of ways they can talk about the challenges they facewithout breaching confidentiality. For example, they could talk to others in theteam who are also bound by confidentiality or talk to those outside the communitysuch as the confidential CRANA Bush Crisis Line 1800 805 391.
Assertive communication strategies can help set boundaries in relation to personalspace and privacy.
A degree of acceptance that remote practice is a lifestyle rather than just a job is probablynecessary if the practitioner wishes to avoid stewing endlessly over perceived intrusionsinto their personal life.
For strategies to:• Communicate assertively, see page 81• Change the way you think and feel, see page 74
2726
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
• Communicate assertively, see page 81• Manage frustration and anger, see page 76• Solve problems, see page 71• Identify sources of stress, see page 70• Change the way you think and feel, see page 74
Suggested Coping Strategies
For strategies to:
Unrelenting and unrealistic demands
Many remote practitioners report that employers and community residents often havequite unrealistic expectations of what they can achieve.
The human limitations of the practitioner can sometimes be overlooked. Their need forsleep, rest, or food may be unacknowledged or even resented by those with healthneeds.
‘You have to be everything to everybody, and it’s just impossible. I mean you’re humanand you’re constantly being asked to do more and more... something’s got to give andit’s usually the nurse that gives.’ (Howard and Ferguson, 1999, p. 29).
Those practitioners who have grown up in the community may find the demands oftheir position and their responsibilities to others overwhelming.
One female Health Worker in a remote community is the sole support for an extendedfamily of four children and three chronically ill old people. She is also herself a diabetic.She prepares the day for all in her household before attending the clinic for a day’s work.Her occasional lateness became an issue with the nursing staff, who increased the pressureon her for being ‘lazy’. (Tregenza & Abbott, 1995).
Those who are required to be on-call frequently may find the unrelenting nature ofremote work to be a particular issue. When on call their work-load is unpredictable - atany minute they may interrupted or required to deal with an emergency. They reportbeing unable to relax in the knowledge they have finished work for the day or the week- over time they can find themselves constantly on edge.
Sole practitioners may be on call 24 hours a day, seven days a week.
Demands for after-hours health services wax and wane over time. During times wherethe demand is high, the lack of anonymity of all involved combined with the lackof boundaries between work and home, can make it difficult for practitioners, particularlysole practitioners, to get adequate sleep or rest. Their ability to provide a safe level ofcare may be compromised as a result.
Housing Issues
Housing issues in remote areas have traditionally been long-standing sources of stressand conflict for many practitioners.
Practitioners often work in uncomfortable and difficult surroundings and live in extremeclimatic conditions. Their ability to control the impact of the climate on themselves andtheir family will depend on the standard of housing they enjoy.
Home may be one of the only places in which the practitioner can rest, relax andrejuvenate away from work.
Perceived inequalities in housing allocation and standard of housing can causeresentments which run deep and wide and can impact on relationships with others inthe community.
While practitioners recruited from outside the community are usually provided withhousing, health practitioners such as Indigenous Health Workers drawn from the localpopulation, are not. Yet many Health Workers are likely to share the same issues ofinadequate and overcrowded housing as others in Aboriginal and Torres Strait Islandercommunities.
If a practitioner’s housing is inadequate, unsafe, substandard or overcrowded, it canhave a major influence on the practitioner’s ability to recover from job related stress andto maintain their well-being over time.
In some instances the lack of guest accommodation in remote communities (eg motelsor guest houses) may mean practitioners are expected to provide accommodation forothers who visit the community.
‘I provide accommodation and meals to visitors, for example, the guy that comes to fixthe solar systems and the guy from the tax department. All these little added things...leaveno time to yourself. It wears you down a bit sometimes’. Remote area nurse (Kreger,1991, p. 55).
By the same token, some practitioners may enjoy the stimulation provided by thosevisiting the community.
Some remote practitioners are required to move out of their accommodation whenthey take their annual leave so their reliever can live in their house. Aside from privacyissues, and the hassles of preparing their accommodation for others while packing togo on leave, this can be difficult for practitioners who just want to relax at home duringtheir holidays.
Difficulties and delays in having houses repaired and maintained can be a source ofconflict between remote practitioners and their employers or managers. Employers havea duty of care to provide safe, if not comfortable housing for their employees.
The impact of housing issues on practitioners can be difficult to understand for thosewho have not lived in remote communities.
CHAPTER 3

2928
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
Those who provide visiting health services will have little opportunity to learn how acommunity or its culture and social and political structures work. Their ability to achievesuccessful outcomes will be handicapped as a result.
It is not uncommon for practitioners drawn from the local population to bear the bruntof the community backlash which can result if the health service does not adapt itspractice to suit the community,
The most significant source of pressure comes from being forced to operate under non-Aboriginal rules in their Aboriginal community. Aboriginal Health Workers report ongoingstress, with resultant strain on their family and community relationships. (Tregenza &Abbott, 1991, p. 7).
Numerous national reports, commissions and conferences have recommended thatnon-indigenous people who provide services to Aboriginal or Torres Strait Islandercommunities should undertake cross-cultural education. This can certainly ease theirprocess of cultural adaptation. At the same time, Indigenous health practitioners mayneed support to understand and adapt to the organisational culture of the clinic andthe bureaucratic structure of their employing organisation.
As with any cultural learning experience, unwitting errors, embarrassments andhumiliations are likely to be part of the process of learning and adaptation.
The path of adjustment can be easier if the practitioner finds a cultural mentor fromwithin the local population. With a mentor, mistakes will become lessons, and repeatingthem over and over will become avoidable.
Some practitioners make the mistake of thinking they need to discard their own culturalvalues and replace them with those of the culture they are moving into. This is notnecessary.
Rather, an awareness of the differences in cultural values and a commitment to developingsufficient understanding of these in order to firstly, not offend or cause distress to clients,families and communities and secondly, to become an effective practitioner within thatparticular cultural context.
What is required is sufficient understanding to enable a culturally safe work space whichallows effective and culturally safe health care provision:
‘I’m doing seven out of fourteen nights on call… You get so exhausted towards the endthat you know you are not functioning well. I’ve done thirty six hours on my feet. Thisplaces you in a very dangerous situation’. Remote area nurse. (Fisher et al, 1995).
Without enough sleep, practitioners can have problems paying attention, and may missimportant information. In addition, those deprived of sleep tend to be more irritablethan usual.
Cultural adaptation
All remote communities have their own culture, whether mining, tourist, railway,Aboriginal or Torres Strait Islander communities.
A practitioner will need to undergo a period of cultural adaptation when they take upremote practice or when they move from one remote community or position to another.
The greater the difference between the practitioner’s cultural background and theculture(s) they are moving into, the greater the challenge will be for them to adapt.
This is particularly so for non-indigenous practitioners recruited to work in remoteAboriginal and Torres Strait Islander communities. And vice versa. While Indigenoushealth practitioners drawn from the local population are likely to be comfortable withinthe community culture, working in a mainstream bureaucratic organisation may seemstrange and uncomfortable at first.
Part of adapting to a community is learning about how it works - socially, culturally andpolitically. If health interventions and strategies are to work, they will need to be in linewith the cultural, social and political structures of the community. This is a deceptivelysimple point. Those who take it on board may be able to avoid some of the frustrationand powerlessness felt by many remote practitioners who work in cultures andcommunities other than their own.
Those who grew up in the community or who have lived there for several years are likelyto have a good sense of what will work, what won’t and why. Practitioners drawn fromthe local population have the advantage of already possessing the information requiredto implement successful interventions in their community.
Suggested Coping Strategies
For strategies to:• Communicate assertively, see page 81• Manage frustration and anger, see page 76• Solve problems, see page 71• Identify sources of stress, see page 70• Change the way you think and feel, see page 74• Manage time and set priorities, see page 72
CHAPTER 3

3130
Issues of isolation
Isolation in remote communities can occur at several levels: geographical, professionaland cultural.
Geographical isolation
Geographical isolation is by definition part and parcel of remote health work.
The distance between the remote community and the nearest regional centre can leadto frustrating delays and inconveniences. Time delays in having equipment repaired andmaintained or receiving drugs and stores orders can lead to high levels of stress.Breakdowns in communication between regional hospitals and clinics can be a barrier toco-ordinated care of clients.
The tyranny of distance usually means that travel is expensive. Having friends visit, beingable to upgrade skills, attend conferences and in-services can be costly exercises.
Fruit and vegetables may have reached their use-by date by the time they arrive in thecommunity. Most things cost more because of the cost of getting it there.
For some, particularly those who grew up in a remote community, geographic isolationmay be seen as a positive rather than a negative attribute.
Suggested Coping Strategies
Sense of geographical isolation may be relative - it may be reduced by roadsbeing upgraded, increased frequency of air services, owning one’s own vehicle,networking with outside organisations, or maintaining contact with othersinside and outside the community.
The practitioner may need to set up their own networks in order to accesspersonal goods, eg mail order shopping, freight account, book or CD clubs.
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
• Manage frustration and anger, see page 76
For strategies to:
Professional isolation
Working alone and without colleagues to discuss issues with can increase the stressassociated with remote practice.
Learning and adaptation can be inhibited since it can be difficult for a practitioner toobtain feedback on how they are going or whether they are on the right track.
Opportunities to get some reassurance or to comfort themselves with the knowledgethat colleagues are experiencing similar problems may also be limited.
By the same token, many practitioners value the independence and autonomy thatcomes from working in isolation from others.
Suggested Coping Strategies
Practitioners will be well served if they can establish a cultural mentoringrelationship which allows them to become more and more competent withinthe community’s culture(s).
Indigenous Health Workers contain the knowledge required to implement anyhealth strategy in their community. Practitioners from outside the communitycan save themselves much wasted time and energy if they heed the advice anddirection of Health Workers.
Keeping a journal can be a very effective strategy for practitioners to tracktheir progress and adaptation, and record their successes.
Critical reflection is an invaluable tool to promote cultural adaptation, seepage 86
CHAPTER 3
The degree of overlap is likely to increase over time as the practitioner becomes morecompetent within the cultural framework of the community.
However, at the same time it is probably wise for the practitioner to recognise that theremay be some ‘no go’ areas of the culture (of the individual or the community) intowhich they, as visitors, should not proceed without an invitation. Mutual respect and anawareness of one’s boundaries can reduce the risk of being seen as intrusive or offensive.
The ability to develop relationships based on trust is the key to effective remote practice.Flexibility, sensitivity, respect for difference, a non-judgemental approach, and optimismare good indicators of someone who has adapted successfully to the remote community.So are relationships with local residents based on mutual trust and respect.
As a practitioner adapts to the culture of a remote community over time, it is almostinevitable they will be changed in some ways. It can be somewhat disconcerting for apractitioner to find that a period of re-adaptation is required if they return to their ownculture. Many report feeling uncomfortable and strangely out of place until theyre-adapt and reintegrate into their own cultural milieu.
culturally safe work space

3332
THE CHALLENGE OF ADAPTING TO REMOTE PRACTICE
In the cities, this is increasingly experienced as roadrage, plane rage and so on. What might the strawand the accompanying reaction be called in remoteareas? ‘The missing discharge summary rage’? Orperhaps the ‘incomplete stores order rage’?
There are many straws lurking in remote areas,jockeying for position, intent on being the last one.Practitioners should be alert to this possibility andaim to deal with stress as it arises, rather thanallowing it to build up.
Suggested Coping Strategies
Cultural isolation
If the practitioner has not grown up in the cultural context of a particular community, beit mining, tourism, railway, or Aboriginal or Torres Strait Islander, then a sense of isolationmay arise, particularly until they become comfortable within the cultural context of thecommunity.
A sense of cultural isolation can arise from being a member of a minority culture withina larger cultural group. This can be felt not only when the practitioner is recruited fromoutside the community, but also when they are working in an organisational setting thatdoes not share their cultural values.
Living one’s own life according to one’s own cultural values is important in maintaininga sense of security, meaning and identity. It is a basic human right enjoyed by practitionersas well as consumers.
A sense of cultural isolation may be reduced and sense of security and identitymaintained if the practitioner maintains links with their own culture, particularlyduring the early stages of adaptation. Regular periods of time out in one’s ownculture can also be beneficial.
CHAPTER 3
Suggested Coping Strategies
Sense of professional isolation can be reduced by, for example, setting up a mentoringprogram, joining and participating in professional bodies that contain other remotepractitioners, networking with other remote practitioners, subscribing to professionaljournals or attending remote health conferences.
Some remote practitioners may even feel isolated within their own profession. Manyreport that urban-based colleagues and professional organisations have agendas andconcerns that differ from theirs.
The straws which lurk in remote areas
For many practitioners, the stress associated with adapting to remote practice and theday-to-day hassles associated with living and working in remote areas may be theirgreatest sources of stress. While not necessarily major issues on their own, they can addup and take a toll on well-being over time.
Sometimes these low-level stresses may build up to a surprisingly strong reaction to arelatively minor matter - otherwise known as the ‘straw that breaks camel’s back’.
The intensity of a stress reaction that has been building over time may take the practitionerand those around them by surprise.
Summary
Health practitioners are faced with many challenges when they take up remote practice.Nonetheless, they can anticipate some of the challenges they will be faced with. Ratherthan waiting until they feel overwhelmed, they can take a pro-active approach bydeveloping a personal plan to manage or soften the impact of some of these challenges.
In general, isolation is a major risk factor in relation to maintaining wellbeing.
Developing a personal plan to overcome or mitigate the effects of what are multiplelayers of isolation (geographic, cultural, social, professional) may help prevent thepractitioner from feeling vulnerable and alone.
Those practitioners who take a creative approach and plan to grow and change are likelyto be rewarded by becoming progressively more comfortable and effective in their role(s).
For health services and health professionals, remote area practice is... the best and worst ofworlds. The work is exciting, colleagues are motivated and there is innovative practice. Itis the worst of worlds because of... the inadequate preparation of staff to meet the challengesof the environment, their frustration, burnout and high staff turnover resulting in poorcontinuity of programs’. (Wakerman, 1999, p2)

3534
Chapter Four
PREVENTABLE SOURCES OF STRESSASSOCIATED WITH REMOTE PRACTICE
3736
Chapter Four
PREVENTABLE SOURCES OF STRESSASSOCIATED WITH REMOTE PRACTICE
For health services and health professionals, remote area practice is... the best and worst ofworlds. The work is exciting, colleagues are motivated and there is innovative practice. It is theworst of worlds because of... the inadequate preparation of staff to meet the challenges of theenvironment, their frustration, burnout and high staff turnover resulting in poor continuity ofprograms’. (Wakerman, 1999, p2)
Providing practitioners with the required skills, knowledge and attitudes they needbefore they take up remote practice can greatly enhance their ability to adapt
and to meet the demands of their job.
However, to date, there has been a lack of adequate preparation for remote practice.This has been an ongoing and multi-disciplinary problem.
This has been due largely to the lack of recognition of the extended generalist role thathas grown in response to the lack of health services and resources in remote areas.
Kelly (1998) in a review of the literature suggests the remote workplace is unregulated,uncontrolled, and professionally chaotic in comparison to urban workplaces. She identifiesthe following preventable sources of stress associated with remote practice:
• lack of recognition of extended generalist role.
• inappropriate legislation to support remote practice (which give rise toprofessional risk).
• inadequate orientation & preparation (including cross cultural education).
• lack of policies, procedures, protocols and guidelines.
• conflicting expectations (community, employers, team members).
These issues appear to be shared across the various professions providing health servicesto remote communities.
A great deal of confusion remains in relation to the roles, responsibilities and scope ofpractice of the various professions involved in remote health care provision. This canmake the adaptation process much harder than it needs to be. How can a practitioneradapt to a job that hasn’t been adequately defined, or where the expectations of the jobhave not been spelled out?
As a result of this lack of clarity, many practitioners are still not provided with the skillsand competencies they need before they take up their positions. Many are left to learnby trial and error on the job.
Learning primarily by making mistakes can make growth and adaptation painful and difficultfor all concerned. It takes longer before practitioners are able to function effectively, the riskof being overwhelmed is increased, and maladjustment is more likely to occur.
Role conflict and confusion
The unregulated nature of remote practice can also give rise to high levels of role conflictand role confusion.
Role conflict arises when two or more pressures occur together so that complying with onewould make doing the other more difficult. This is often cited as a major source of occupationalstress among the various professions providing health services in remote areas.
The most commonly cited source of role conflict is between the expectations of the employerand those of the community. Many suggest meeting their employer’s expectations canwork against them being able to meet expressed community needs.
This is particularly salient for small on-site teams who have limited resources (human andmaterial) at their disposal. All needs cannot be met, and practitioners may find they have tochoose between the two - an either / or choice, as opposed to being able to do both.
Role confusion refers to the difference between what others expect of the practitioner,and what they themselves feel they should be doing. This can cause uncertainty. Thepractitioner may not understand what is expected of them, may not know how tomeet expectations, or may think the job should be different from what it is.
Health Workers conveyed their feelings of frustration, confusion and stress created bythe lack of agreed definition of the Health Worker’s roles. The role of the Health Workeris varied, largely undefined, and complex. (Tregenza & Abbott, 1991, p.8).
Many remote practitioners have unrealistically high expectations of themselves. This canbe a major cause of excessive stress. If a practitioner constantly expects too much ofthemselves, they will tend to drive themselves too hard and take on too much.
Unclear role specifications can add to this process - if a practitioner is not clear what isexpected of them they will be unable to develop accurate criteria with which to measurethe success or otherwise of their efforts.
‘You’re always at logger heads with yourself trying to work out ‘What am I here for?What should I be doing? What should I do first?’ because of the unrealistic expectationson the part of yourself and the employer. That’s what really breaks a lot of nurses’.Remote area nurse. (Kreger, 1991, p. 29).
Role conflict and confusion can not only stymie adaptation, it can create an environmentwhich is fertile for disagreement and conflict. Conflict may arise between team members,or between teams and employers or communities. This is compounded by many on-siteteams being unable to meet other than the most pressing of priorities.
Practitioners working for community controlled organisations may have fewer problems tryingto meet conflicting community and employer expectations. In theory at least, communitymembers have had some input into the planning of health service provision, and practitionershave had an opportunity to negotiate the role and function of the health service.

3938
Suggested Coping Strategies
Becoming a member of, and supporting the activities of the peak professional bodiesthat represent remote practitioners within each profession is an important step inaddressing the preventable sources of stress. These organisations have a role to lobbyand act at State and national levels to bring about the changes required to supportremote practice.
PREVENTABLE SOURCES OF STRESS ASSOCIATED WITH REMOTE PRACTICE
Until adequate preparation becomes available, it may be useful for practitionersthemselves to identify the skills they need for their role, identify any gaps in theirskills or knowledge, and then develop a professional development plan to gain skillsand competencies in the areas they identify as deficient.
It may be useful to clarify and negotiate roles, professional boundaries, and roleexpectations at a local level. To be sustainable, key stakeholders would need to beincluded in this process, ie community, team members.
On-site practitioners should seek to be included in planning activities in relation tohealth service provision in the community.
Practitioners need to make sure they are aware of any legislation that impacts ontheir practice.
• Resolve conflict, see page 80• Communicate assertively, see page 81• Manage frustration and anger, see page 76• Deal with conflicting demands, see page 74• Solve problems, see page 71• Identify sources of stress, see page 70
CHAPTER 4
Shouldn’t the preventable be prevented?
No amount of training practitioners to manage their own stress responses will impact onthe preventable sources of stress associated with remote practice.
Indeed, some would say it is unethical to train practitioners to better tolerate poorconditions, particularly if the causes of practitioners’ stress aren’t also being addressed.
It is very important that remote workplace conditions are changed so that it becomes astressful environment to work in.
Interventions should be two pronged. While practitioners must do what they can tomanage their own reactions and maintain their wellbeing, professional bodies, employersand others also have a responsibility to address the preventable sources of stress associatedwith remote practice.
However, if the health service is State controlled and, as often occurs, on-site staff andcommunity members have not been included in the planning of the community’s healthservice, then conflicting expectations and role confusion and conflict are likely to be amajor source of job related stress for practitioners.
Suggested Coping Strategies
For strategies to:
Employers have a responsibility to identify and eliminate or minimise potential stressfactors that can be impacted by improving work place practices. Examples might be:ensuring staff have the competencies required to fulfil the requirements of their job (ieorientation and in-service); providing clear job descriptions which reflect actual practice;and minimising uncertainty, conflicting expectations, role conflicts and excessive workloadpressures and fluctuations wherever possible.
However, many of the preventable sources of stress associated with remote practicecannot be addressed by practitioners or even employers acting alone.
The complexities involved in clarifying professional roles and scope of practice or issuesof legislative support need to be addressed by professional and funding bodies at stateand national levels. Long lasting solutions are only likely to come through the slowerand more difficult methods of lobbying for action and change at higher levels.
Summary
The challenges faced by practitioners taking up remote work are many and varied, occurat several different levels and include both professional and personal challenges. Manypractitioners do not manage to complete their adaptation process before they becomeoverwhelmed and leave their job.
So far, high levels of staff turnover in remote areas have largely prevented the developmentof an experienced workforce - the bulk of the remote workforce at any given time islikely to be at the beginning of their learning curve.
It is unfortunate that until and unless many of the preventable sources of stress areaddressed, the challenge to adapt to remote practice will remain too great for manyhealth practitioners. New staff will continue to become overwhelmed and leave.
It can be difficult to establish or maintain effective health services when staff are constantlybeing replaced.
If and when the preventable sources of stress are addressed, many practitioners mayfind they are able to more comfortably meet the challenges of adjustment to remotepractice. Their adaptation process will become limited to those factors which are partand parcel of remote work.
It is not intended to paint a pessimistic picture, or to deter practitioners from taking upremote practice.

4140
Chapter Five
AVOIDING THE SLOW SIZZLE OF BURN OUT
CHAPTER 4
However, if practitioners are forewarned about some of the sources of stress, they cananticipate and guard against their impact.
In addition practitioners will be less likely to blame themselves for what are essentiallyshortcomings of their workplace. For far too long, practitioners have blamed themselvesor been blamed by others if they felt out of their depth or were struggling to cope. Atthe same time little was being done to provide them with the skills or support theyneeded.
However, it is largely irrelevant whether the stressors confronting remote practitionersarise from unavoidable or preventable sources.
Whether inherent or preventable, these are the challenges practitioners are confrontedwith when they take up remote practice. They will need to develop some strategies tocope if they are to survive, to adapt to and to flourish.

4342
Indeed, many practitioners can push themselves for a short time and get away with it -the stress response actually provides extra energy to do this. Once the task is completedthe source of stress is controlled and the practitioner’s stress response is then deactivated.This is a healthy process.
However, it is almost always a mistake for a practitioner to work harder and harder in anattempt to get on top of a workload that has no bounds. Physical and emotionalexhaustion, ie burn-out, is almost inevitable.
If the practitioner is constantly overloaded then an ability to set realistic work goals, toprioritise, and to set boundaries which allow them to have a healthy lifestyle is essentialif they wish to last more than a few brief but exhausting months.
If a practitioner has a balanced and satisfying life which includes periods of relaxation theywill be better able to deal with whatever challenges confront them in the workplace.
A healthy lifestyle should include elements of the following:
Set realistic goals
There is no surer path to burn-out than setting unrealistic goals and then working flatout to meet them.
It can also lead to practitioners being unable to recognise their successes.
If they have set unachievable goals they are likely to only see what they haven’t beenable to do, rather than any successes they may have had. Therefore they rarely feelsatisfied with their performance, and will be prevented from being able to relax with thefeeling of a job well done.
Any hope of feeling some job satisfaction was hijacked at the planning stage.
For strategies to:• Deal with conflicting demands, see page 74• Monitor long-term well-being, see page 79• Manage time and set priorities, see page 72
Manage your time
Few people work best when under unrelenting pressure. Some practitioners may feel sooverwhelmed by the demands of the job they don’t know where to start or when to stop.
The ability to sort the sheep from the goats is an essential stress management strategy forremote practitioners. In practice this may mean avoiding taking on battles that cannotbe won, declining to participate or devote too much time to projects or programs whichare ill-timed, ill-conceived, not a community priority, are under resourced, or which usestrategies unlikely to be successful in a particular community.
Chapter Five
AVOIDING THE SLOW SIZZLE OF BURN OUT
Unfortunately, large pools of un-met needs, and under-resourcing to meet theseneeds is not uncommon in remote Australia. The needs of many remote com
munities are often greater than the abilities of the practitioners employed to meet them.
‘I found it enormously stressful that you couldn’t get it all done. So there was a sense ofsomehow failing constantly, because the workload was more than could ever be done.’(Howard and Ferguson, 1999, p. 29).
When high levels of demand are combined with the lack of natural circuit breakers betweenhome and work, the lack of anonymity of all involved, and the twenty-four hour nature ofthe job, it can be difficult for a practitioner to protect their well-being over time.
While adequate resourcing would go some way to redressing the balance, this has yet tooccur. Until this happens, practitioners will need to do the best they can in the givencircumstances.
Finding a balance between maintaining their own wellbeing and meeting the urgentneeds of others can be a difficult task. However, practitioners who overcommit to theirjob and fail to care for themselves in communities with high levels of illness and distresswill not be sustainable. They will merely add to the already high statistics relating tostaff turnover.
‘We don’t get a chance to reach our full potential because we burn out before we reachthat. But that’s the trap of the game you see’. Remote area nurse (Kreger, 1991).
The practitioner should aim to maintain their resilience. This refers to their ability tobounce back or to recover when difficulties arise.
If a practitioner’s resilience becomes eroded they will become more and more vulnerableto burn-out.
Avoiding burn-out is less about short term coping strategies and more about puttingboundaries and structures in place which allow the practitioner to sustain themselves overtime.
Self care is the key to avoiding burn-out - it is both prevention and cure.
Self Care - The Big Picture
It makes perfect sense for a practitioner to push themselves to work harder for a shorttime to get on top of a problem if it can be overcome by short-term effort.

4544
Exercise
Exercise is an important way to relieve stress which requiresno special skills. It is a surprisingly effective remedy forreducing the impact of stress in the short and long-term.
Regular exercise and a nutritious diet can contribute toa strong and healthy body which will be better able towithstand the wear and tear of short and long-term stressresponses.
Stress creates physical energy. When no action is allowedto take place the energy remains pent up in the body.Exercise ‘burns off’ that energy and thereby reduces stress.This can help prevent a slow drift toward existing in achronically stressed state.
Meditate
The benefits of regular meditation cannot be overstated - it can bring an enduring senseof calm and peace into a practitioner’s life. It is a personal investment in preventingstress, anxiety, worries, and negative emotional states in general.
Meditation helps the practitioner to deal with their thoughts and to become more calmand peaceful in everyday life.
Exercise and meditation are two of the most powerful interventions for practitioners todevelop the personal resources needed to counter all sorts of stress, anxiety, worry andnegative emotional states.
Have a life
Remote practitioners will need to be particularly vigilant about maintaining the non-work areas of their lives. This may include working to preserve some special blocks oftime that are all theirs and cannot be interfered with. This may be difficult for those whoare required to be on call frequently, however, making the effort to achieve this is asound investment in long-term sustainability.
Some seasoned practitioners ensure they have regular breaks away from the community.Some schedule some type of leave every few months, for example. study leave, annualleave, isolation leave etc.
• Relax, see page 82• Set boundaries between work and home, see page 79• Deal with conflicting demands, see page 74• Manage time and set priorities, see page 72
Doing things the practitioner finds relaxing is a natural way to calm oneself, for example,the simple pleasures such as lying down, reading, taking a bath, going for a walk orenjoying hobbies. These activities not only enhance one’s sense of self but will also bringthe relaxation response into play and deactivate the stress response for a time.
Taking regular breaks from work such as tea and lunch breaks, although sometimesdifficult to achieve, is part of effective time management. These breaks provideopportunities to draw breath, to reorientate thinking and to plan improved use of timebefore returning to the fray. It also acknowledges the human limitations of any workerand the need for them to rest and have some time out.
There are many simple exercises practitioners can use to deactivate their stress response.
Regular exercise can also be useful as a circuit breaker at the end of the day. It can helpto put a boundary between work and home.
The ability to manage time can be greatly assisted by the health service having a strategicplan. Practitioners can then invest time and energy selectively and strategically in waysthat further the health service’s goals.
For strategies to:
CHAPTER 5
For strategies to:
Strategies:
• Manage time and set priorities, see page 72• Comåmnicate assertively, see page 81• Solve problems, see page 71
For meditation techniques, see page 84
Sometimes it may be necessary to ‘burn off’ the stress chemicals with some form ofexercise before the practitioner can relax properly. Exercise followed by a simple relaxationexercise can be an effective way to maximise the practitioner’s ability to relax.
Sex and laughter can have a similar effect to exercise. The sympathetic nervous systemdischarge that occurs during orgasm can neutralise the effects of stress - laughter hasbeen shown to have similar benefits.
Rest & relax:
Practitioners should aim to recognise and addressstress symptoms as they arise, and not allowthemselves to exist in a chronically stressed state.
With stress, the mind and body are one. If thepractitioner can calm their body their mind will followand vice versa.
AVOIDING THE SLOW SIZZLE OF BURN OUT

4746
Suggested Coping Strategies
Deal effectively with conflict
Remote practice has traditionally been characterised by health care provision in thecontext of multi-disciplinary teams. Currently there are high levels of confusion aboutroles, functions and boundaries of the various members of the team. This can create anenvironment fertile for friction and conflict. There may be struggles for status, for powerand influence, to defend professional territory, or to expand or reduce responsibilities.
Conflict may arise between team members, between team members and employer, andbetween team members and the community.
This situation can become more volatile during period of high levels of demand thatleave team members feeling tired, stressed and, more often than not, traumatised.
The lack of natural circuit breakers or boundaries between work and home, and theclose nature of life in remote areas means the impact of job related conflict on theindividual can be intense and debilitating.
An ability to recognise conflict and a willingness to resolve it before it escalates toArmageddon are valuable attributes for all remote practitioners.
In some instances, conflict within a team can escalate to workplace bullying. Bullyingmay be defined as ‘aggressive behaviour arising from the deliberate intent to causephysical or psychological distress to others’ (Randall, 1997, p. 12 emphasis mine).
Bullying may be subtle or direct and usually involves attempts to dominate or humiliateanother person. Using aggression or bullying in the remote workplace to achieve one’sown ends is not acceptable.
Clarity of roles, expectations, scope of responsibility, lines of reporting,team purpose and vision can reduce conflict in the workplace. Regularteam meetings and good communication can bring clarity to a team.
Ability to recover when difficult things happen
Practitioners can maintain their resilience by:Balanced, healthy lifestyle (work, rest and play)Good social support networksActively manage stress responsesRegular periods of rest and relaxationSeek support when needed.
For strategies to:• Monitor long-term well-being, see page 79• Manage time and set priorities, see page 72
CHAPTER 5
Accept the support of others
Establishing and maintaining a good social support network is probably the bestinvestment a practitioner can make toward their long-term well-being.
Social support can come from local support systems or from outside the remotecommunity.
Those who have partners and family available to them on-site are fortunate indeed.Close relationships provide opportunities to confide painful feelings and help to bufferall types of stress.
Mind you, meeting the responsibilities associated with close relationships can sometimesbe a source of stress in themselves.
Admit vulnerability
At the risk of generalising, many remote practitioners tend to be extremely strong andindependent people. However, some practitioners can take this too far.
Some practitioners may find it difficult to admit to personal vulnerability or to seek thesupport of others when they need it. While this might give an impression of ‘strength’,it can be a liability in remote areas.
Sharing their experiences with others can enrich the practitioner’s life. It can promotelearning, adaptation and personal growth in response to the demands, challenges andtraumas associated with remote practice.
Isolation is risk. The wellbeing of the practitioner will almost certainly be jeopardised ifthey are aloof and alone.
A strong culture of ‘if you can’t stand the heat, get out of the kitchen’ exists in someremote areas and organisations. This can work against a practitioner feeling safe enoughto disclose their feelings of vulnerability to others.
It is important to remember that stress is a normal human response to any challenge. Ifmanaged well, it can lead to growth and change. It does not indicate weakness orinadequacy.
AVOIDING THE SLOW SIZZLE OF BURN OUT
Resilience:

4948
For strategies to:
Own Your Own ‘Stuff’
Practitioners need to be aware of the part they themselves play in how they experiencestress.
Sometimes the practitioner’s own perceptions and behaviours can cause or exacerbatejob-related stress.
Practitioners need to take responsibility for their own personality traits. Theyshould not expect others to share them, or become angry or disappointed ifothers decline to participate in them, for example, perfectionism.
If a personal characteristic is a liability, the practitioner can work to mitigateits effects.
For example, a practitioner could choose tasks that allow them to expressparticular parts of themselves. For example, those who like to be orderly andmeticulous could find certain tasks for which this is an advantage. At thesame time, they could work to increase their tolerance for ambiguity andloose ends in relation to other, less controllable tasks.
Practitioners going through stressful personal experiences need to be awarewhen they are becoming overloaded with stress, and implement additionalself care strategies or set firmer boundaries during periods of vulnerability.
Suggested Coping Strategies
The ability to communicate clearly and assertively has been recognised as anessential skill in the prevention or mitigation of all forms of conflict. It canalso stop aggressive, domineering or bullying behaviour in its tracks.
While assertive communication skills may require careful consideration beforeapplication in Aboriginal and Torres Strait Islander situations, they are usefulgeneric skills that can be useful in a variety of situations in the remoteworkplace.
• Communicate assertively, see page 81• Resolve conflict, see page 80• Solve problems, see page71
For strategies to:
CHAPTER 5 AVOIDING THE SLOW SIZZLE OF BURN OUT
DefinitionPersonality style: enduring patterns of self-perception,interpersonal relations, and approach to work tasks and otherinvolvements, which limits the individual’s adaptability andcapacity to cope with stress (Cotton, 1994, p. 94).
For example, the practitioner who is inclined to be orderly and meticulous may strugglewith high levels of stress in the remote setting where workload and demands tend to beunpredictable and job role boundaries ill-defined.
Practitioners with self pressuring and perfectionist traits, and a constricted (overly blackand white) cognitive style may experience high levels of stress. They usually like everythingto be cut and dried, precise and predictable. Few remote workplaces are able to meetthis criterion - particularly if the practitioner is working in a culture other than their own.
Those practitioners with a tendency to become over-involved in their work, emotionallyintense, and overly sensitive to the distress of others may be particularly vulnerable toburn-out. This is more so if their work involves high levels of contact with large numbersof distressed people.
Some remote practitioners may be very idealistic about their work and mistakenly believeif they work hard enough, they can single-handedly relieve the suffering of entirecommunities. Unless they also care for themselves, the will almost certainly burn out.
If a practitioner has a habit of interpreting things in a negative light and telling themselvesfrightening stories about what is happening around them, then continuously high levelsof a stress will result. On the other hand, if a practitioner tends to find the positives inany situation, they will tend to be more relaxed overall.
Those going through major life events such as divorce, bereavement, financial difficultiesetc may find it difficult to function well at work. Home related stressors can reduce thepractitioner’s threshold in relation to being able to tolerate additional stress.
Self Care - the smaller stuff
Once the practitioner has a structure in place which allows them to protect and sustain theirwell-being over time, that is, they have a healthy attitude and lifestyle in place, they can turntheir attention to dealing with some of the day-to-day hassles which confront them.
It can be easy for a practitioner to become so immersed in their stress that they feel theycan’t afford the time or space to stand back and re-appraise their situation. However,this is often the first step to effective management of stressful situations.
Theologian Reinhold Niebuhr neatly summed up the essence of good stress management:changing what can be changed, accepting what cannot be changed, and - the key toavoiding burn out - having the wisdom to know the difference.
* Change the way you think and feel, see page 74* Manage frustration and anger in self and others, see page 76
Suggested Coping Strategies

5150
The main methods of managing stress include:i) Try to change the situation if possible.ii) Try to alter the way a situation is perceived or reacted to if it can’t be
changed.iii) Try to reduce the wear and tear of prolonged stress reactions on the mind
and body.
Each of these approaches will be addressed in the following section.
Try to change the situation if possible
Once the practitioner recognises they are becoming stressed it is useful to locate thecause of their stress, ie identify the stressor, or define the problem.
Sometimes the very act of identifying and naming the precise sources of stress can behelpful. It can help to make the problem more tangible and help shift the focus from‘what is wrong with me?’ to ‘what can I do (or not do) about the situation?’.
Sometimes what one thinks is the problem may not be the main issue. The ‘problem’confronting the practitioner may just be a symptom of a greater underlying problem.
Say, for example, a practitioner is feeling stressed and exhausted by high levels of latenight call outs for non-emergency health care. The strategies the practitioner developsto change the situation will depend on how they define the problem. The best laidplans won’t work if the strategies don’t address the problem.
Using the above example, say the health service was previously provided by anorganisation that contained elements of paternalism in its service provision. Say foryears, community residents were encouraged to go to the clinic for all health mattersregardless of how big or small, or at what hour of the day or night.
If this was the case, attempting to change the expectations of particular individuals orfamilies at the time they present late at night is unlikely to be effective. Such an approachmay also be fraught with conflict since it may seem to community members that thepractitioner is just trying to avoid work.
Instead, it may be more effective if the practitioner undertook a broader strategy thataimed to change community expectations and to re-negotiate the role and function ofthe health service after hours.
The methods and the time frame required to change entrenched community attitudesto the role of the health service are likely to be different than trying to change thebehaviour of particular individuals.
It is important the practitioner clearly identifies the real issue of concern rather thanfocusing on what may be just a symptom of a larger underlying problem. Otherwise apractitioner can find themself industriously implementing a plan which may be irrelevantto the issue at hand.
CHAPTER 5 AVOIDING THE SLOW SIZZLE OF BURN OUT
If a practitioner recognises they are unable to influence or change a source of stress, thenthey should acknowledge this and stop trying. Working flat out trying to changesomething they can’t will just exhaust them. It is better for them to stop and to redirecttheir energy to something they can change.
Accept that which cannot be changed
Remote practice can contain a multitude of factors and events the practitioner is unableto control.
If a practitioner cannot change an upsetting or stressful situation then it is time to moveto plan B: changing the way they see the situation or the way they think about what ishappening.
Regardless of what is happening around them, the practitioner can control their ownactions, attitudes and perceptions.
A practitioner’s thoughts will influence how they feel. How they assess a potentiallystressful event is the mediating influence over whether a stress response will result ornot. The practitioner has to identify something as threatening or dangerous before theirstress response is triggered.
Trying to control that which is beyond their influence can leave the practitioner feelingconstantly frustrated, angry and disappointed.
Some even end up blaming themselves for not being able to somehow control eventsthat are not theirs to control.
Sometimes a surrender may be necessary - practitioners may need to give up the ideathat they can or must control everything. Attempting to control only that which can becontrolled can be a giant step toward long-term sustainability.
Some practitioners can forget their role is to serve the remote community. The practitioneris an instrument or tool of the community - not vice versa. The community has a rightand responsibility to control its own health. It is not the practitioner’s responsibility toattempt to wrest control from the community or to take charge of its health outcomes.
If the practitioner is feeling overly responsible for the actions of others it may be useful toidentify and acknowledge this. Sometimes it can be useful to ask, ‘whose problem is itanyway?’
For strategies to:• Identify sources of stress, see page 70• Solve problems, see page 71

5352
For strategies to:
CHAPTER 5 AVOIDING THE SLOW SIZZLE OF BURN OUT
For strategies to:
Practitioners can attempt to influence, but cannot control the behaviour of other adults(unless they are deemed to be either mad or bad - and this requires the intervention ofpolice or mental health legislation). Adults have a right to behave in ways they see fit.Whether the practitioner approves or disapproves is largely irrelevant – they cannotforce them to behave otherwise.
If an issue is beyond the practitioner’s control they can choose to ignore it, attempt toadapt to it, or to work toward not reacting to it in a way which leaves them feelingcontinually stressed.
Reduce the wear and tear of stress reactions
The key to maintaining long-term wellbeing is to ensure that the sympathetic (fight andflight) system does not remain dominant for days, weeks or months.
Remember, the stress and relaxation responses are actually equal and opposite to eachother. What one does, the other can undo.
Like a drug, the relaxation response has a strong effect on the body and the mind. Theheart rate slows down, blood pressure decreases, breathing slows, and the brain waveswhich facilitate mental calmness increase.
When the relaxation response is activated the ability to think broadly and well improves,fun can be had, sense of humour re-emerges, sex life can be maintained, emotionalintimacy becomes possible and relationships can be nurtured.
Periods of relaxation allow repair, rejuvenation and renewal of oneself. This should occurregularly if the practitioner wishes to maintain their quality of life and their ability tofunction well in their jobs.
Remote practitioners would do well to become proficient in developing skills and strategieswhich allow them to relax as much as possible while at home.
• Identify sources of stress, see page 70• Change the way you think and feel, see page 74• Engage in critical reflection, see page 86• Solve problems, see page 71• Manage anger in self and others, see page 76• Relax, see page 82• Meditate, see page 84
Suggested Coping Strategies
• Relax, see page 82• Meditate, see page 84
PATH TO SUSTAINABILITY IN REMOTE AREAS
(long-term wellbeing, job satisfaction, high self esteem)
Maintain resilience & wellbeing:
• Maintain balanced lifestyle (work, rest and play)• Maintain good social support networks• Regular periods of rest or time out• Maintain a healthy lifestyle
Act on the situation:
• Clarify your role and its boundaries• Clarify others’ expectations of you• Skill up: have sufficient skills to deal with likely occurrences• Identify sources of stress• Act to change stressors which can be changed• Learn to live with stressors which can’t be changed• Use good problem solving skills
Be active about managing your stress responses:
• Accept responsibility for your wellbeing• Actively manage stress responses as they arise• Realistic view of human capabilities - prioritise, set realistic goals,
and then set boundaries.• See challenges as growth producing experiences• Optimism: reframe, look for positives, reduce negative self talk.• Keep a journal.• Engage in critical reflection.• Exercise.• Meditate

5554
CONCLUSION
While this booklet has been developed to assist remote practitioners to identify andmanage some of the stress associated with remote practice, we are aware that there isa distinct danger that it may be taken to mean practitioners have to do all the adapting,all the coping.
Much work remains to be done to address some of the preventable sources of stressassociated with remote practice. This is the role of professional and other bodies at stateand national levels.
The employer also has a responsibility to provide a healthy and safe work environment.If potentially harmful stressors are known and predictable, then employers have a dutyof care to prevent them if they can. If they can’t prevent them, then the employer hasa duty of care to provide support to prevent the practitioner from sustaining long-termpsychological harm as a result of doing their job.
The employer, if made aware of potential dangers to practitioners or clients as a result ofhigh levels of stress, has a responsibility to support the worker and to remedy the situation.
At the same time practitioners need to accept responsibility to safeguard their wellbeing,their ability to provide a safe level of care and to maintain professional standards.Practitioners have a duty to not put themselves at risk of harm, and to seek support andassistance if they feel overwhelmed. This is particularly important if their ability to providea safe level of care is becoming impaired.
Thus, responsibility for maintaining a safe working environment is a mutual responsibility.
While we should not underestimate the impact of occupational stress in the remoteworkplace, we must also respect the ability of many practitioners to manage the mostdemanding of circumstances and emerge stronger as a result of their experience.Practitioners can be enormously resistant to stress.
However, they need to be alert to threats to their well-being, and take the initiative andtry to do something about them before they become overwhelmed.
Currently, working in a hectic, unpredictable, exciting, variable and at times chaoticworkplace is inseparable from remote practice. Good stress management skills can helppractitioners to maintain their resilience and their ability to provide a high quality of careto people in remote communities.
PATH TO BURN OUT IN REMOTE AREAS
(Physical and emotional exhaustion, cynicism, low job satisfaction,poor self esteem).
Erode your resilience:
• Give all of your energy and focus to the job• Isolate yourself from others• Don’t take regular breaks or time out.• Don’t have a social life• Adopt an unhealthy lifestyle
Fail to act on the situation:
• Remain confused about what it is exactly you’re supposed to be doing• Remain confused about what others expect you to do• Remain ill equipped to meet the demands of the job• Be unable or unwilling to respond to new challenges• Stubbornly persist with old skills which don’t work in new environment.• Fail to identify stressors• Fail to change the stressors which can be changed• Continue to stress out over stressors which can’t be changed• Don’t use problem solving skills
Fail to use effective coping strategies:
• See your comfort and wellbeing as someone else’s responsibility• Use coping strategies which create more problems• Allow stress responses to run unfettered for prolonged periods• Fail to acknowledge human limitations: attempt to meet excessive
demands and place all other’s needs before your own.• Set unrealistic goals and then work hard to achieve them• Be pessimistic, only see negatives, engage in negative self talk• Be a couch potato, don’t exercise - use substances to relax instead.• Fail to critically reflect on experiences - always blame others.
CHAPTER 5 AVOIDING THE SLOW SIZZLE OF BURN OUT

5756
Chapter Six
AVOIDING CRASH AND BURN:COPING WITH TRAUMATIC STRESS

5958
After the event:
• Strong feelings of distress and anxiety
• Sleep disturbances such as not being able to get to sleep, or having nightmares
about the event or other catastrophes.
• Flashbacks, or unwanted thoughts about the event keep popping into one’s
mind, causing distress.
• Feeling emotionally numb or strangely empty.
• Wanting to avoid reminders of the event.
Most often, traumatic stress reactions tend to have a cyclical effect of intense memoriesand feelings followed by periods of numbness, then distress and so on.
Traumatic stress reactions are NORMAL human reactions to extremely difficult experiences.
Reactions can be mild or strong and may last for hours, days or weeks (although theyusually start to settle after the first week or so).
Because practitioners often put their feelings on hold in order to respond to the event,they increase the likelihood their reactions will be delayed. Reactions may not comeuntil they have achieved a safe environment, ie they are able to relax. Being hit withreactions some days or weeks down the track can be a bit off putting but is not uncommon.
If the practitioner experiences the event as traumatic then they should acknowledge thisfact and take appropriate action to recover and to ensure their long-term wellbeing.
The more deeply the practitioner has been affected, the more important it is that theyreceive psychological support / debriefing from a mental health professional.
If a practitioner’s safety is at risk or they feel unable to function at work or at home thenthey need to stop work and receive face to face psychological support from a mentalhealth practitioner.
Practitioners can access debriefing / psychological support from:
• Employee Assistance Services (contracted by your employer to provide
employees with psychological support)
• Bush Crisis Line (you may be anonymous if you wish) Toll free 1800 805 391
• Visiting mental health services
• Visiting medical officers
Note: Group debriefing is not recommended in small communities where everyoneknows everyone else.
Chapter Six
AVOIDING CRASH AND BURN:COPING WITH TRAUMATIC STRESS
Traumatic Events
Traumatic events are defined as those which involve the threatened or actualdeath or serious injury to the practitioner or others, perhaps under violent, shock
ing or horrific circumstances.
Job related events which contain the potential to traumatise practitioners include medicalemergencies, natural disasters, motor vehicle accidents, homicides, suicides, familyviolence, physical and sexual assaults, vehicle breakdown in remote areas, needle stickinjury, home invasion, stalking, and death threats or threats of violence.
Some events may be more difficult to deal with than others. For example, if it was sudden,with little time to prepare, involved exposure to grotesque images, was deliberate ratherthan accidental, involved children or people known to the practitioner, if they were aloneduring the event, or if they felt unsure about their chosen course of action.
The type of event is only half of the equation. The practitioner’s reactions during and afterthe event, particularly feelings of horror and helplessness, make up the other half.
Basically, if the practitioner experiences an event as traumatic and has strong emotionalreactions during or after the event, then it is defined as traumatic, rather than ordinarilystressful.
Traumatic events are likely to be more complex experiences for remote practitionersthan urban counterparts. The lack of anonymity of all involved, the public nature ofsuch events, the ripple effects throughout the community, and issues about maintainingconfidentiality in small places, all work to complicate the situation and inhibit thepractitioner’s ability to recover.
It is important to note that high levels of ongoing stress (home or work related) canincrease the vulnerability of a practitioner to the impact of job related traumatic events.
Traumatic Stress Reactions
Indicators of a traumatic, rather than an ordinary or garden variety stress reaction, mayinclude one or more of the following:
During the event:
• Intense feelings of fear, horror and / or helplessness.
• Feeling unreal, numb, in a daze, outside of self looking on.
• Time becomes distorted
• Disorientation to time and place
6160
Recovery After the Event
There is thought to be a natural recovery period of about a month following traumaticevents.
Recovery cannot begin until the event is over and the practitioner achieves an environmentwhich is safe enough to allow them to take stock of the event and its impact.
The aim of supportive interventions is to encourage (but not force) people to talk aboutwhat happened and how they felt, to stand and face their fears, use positive rather thannegative coping strategies, and work through their experience until they find some sortof a peace with what happened.
While it is important practitioners talk about the event and how it affected them, thelack of anonymity can make it difficult to do this without breaching confidentiality insmall communities. Talking about what happened and some of the gory details mightintensify the distress of others (eg family of victims). Bush Crisis Line is a useful 24-houroption in these circumstances Freecall 1800 805 391.
Practitioners may choose to talk to someone outside the community. Friends, family,peers, mentors or supervisors are all good choices. It is probably important that whomeverthe practitioner choose to talk to, cares about them.
If a practitioner doesn’t have someone to confide in, their recovery may be compromisedas a result.
Generally, the practitioner should return to usual strength and coping abilities within amonth. If he or she does not, or if their ability to function at work or at home appears tobe deteriorating then they should be referred to an employee assistance service forpsychological support.
AVOIDING CRASH AND BURN: COPING WITH TRAUMATIC STRESSCHAPTER 6
Recovery Takes Time
Debriefing interventions should not be seen as a one-off or ‘cure all’ intervention.Traumatic stress reactions are normal reactions that will unfold in their own time.Debriefing will not magically take away the practitioner’s reactions.
Support needs of practitioners are likely to be ongoing until their recovery is complete.This may take hours, days or weeks. The possibility of delayed reactions should also bekept in mind.
Practitioners may be particularly vulnerable to the impact of subsequent traumatic eventsif they occur before they have fully recovered from the initial event.
Support needs may increase during events related to the trauma eg funerals, courtappearances, investigations, anniversaries, or the return of the perpetrator to community.
Those who live and work in communities which experience repeated traumatic eventsmay find that everyone around them is also traumatised. Recovery in small communitiescan sometimes be a collective endeavour. It may be hard for a practitioner to recoverbefore everyone else does.
Many remote health practitioners may be repeatedly exposed to traumatic events, andrecovery can become more and more compromised with each event.
It is therefore important remote practitioners accept responsibility for their wellbeing,seek to maximise their recovery after each event and use the best available resources ifthey are to avoid paying a high psychological price for the type of work they do.
Suggested coping strategies:
The practitioner should try to arrange 24 hours off call as soon as possible afterthe event. There is usually no need to take time off work, just off call.
This will give the practitioner a chance to relax after hours and take stock of theevent, to feel the feelings as they come up, and perhaps to nurture themselvesa bit.
The practitioner should try to ensure they have regular periods of ‘time out’until they feel they have recovered (this may take hours days or weeks). Thismay be just taking regular meal breaks, perhaps having some time off call, timeoutside the community, or maybe getting away for weekends. Time off in lieu,annual leave, sick leave, or leave without pay are also options.
The needs of others in the health team need to be kept in mind. In arrangingtime out or time off, others should not be overloaded or pushed beyond theirown coping abilities.
Draw on all available sources of social support. Some practitioners may need touse the phone to access the support of those who care about them if they liveoutside the remote community.
Delays in official processes should be minimised wherever possible, eg, todetermine cause of death, justice system processes, investigations, statementsto police, funerals. These delays can also delay recovery.
Practitioners should aim to use positive rather than negative strategies to managetheir distress. Some people make the mistake of lashing out at others in their
CRANA Bush Crisis Line & Support Services has a booklet available for remoteand rural health practitioners and their families to help manage traumaticstress reactions. ‘Surviving Traumatic Stress’ is available through the CRANAoffice in Alice Springs:
Telephone: 08 9853 5244or the CRANA webpage www.crana.org.au
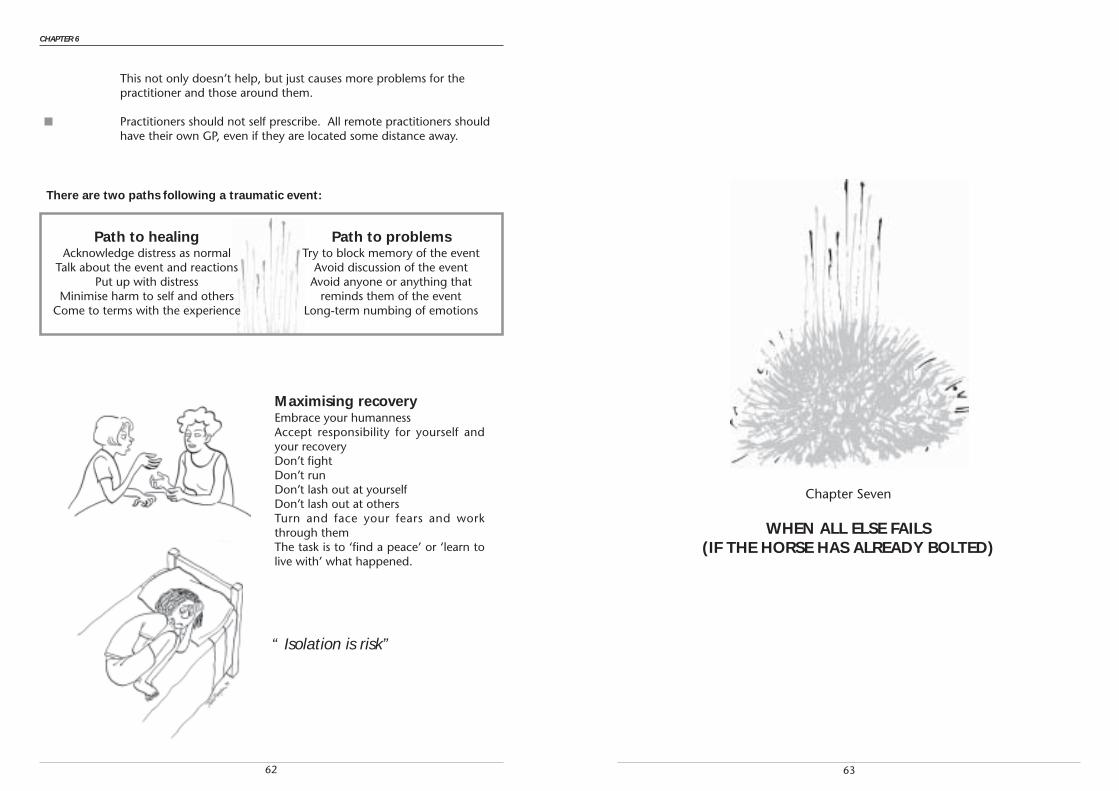
6362
This not only doesn’t help, but just causes more problems for thepractitioner and those around them.
Practitioners should not self prescribe. All remote practitioners shouldhave their own GP, even if they are located some distance away.
CHAPTER 6
Path to healingAcknowledge distress as normal
Talk about the event and reactionsPut up with distress
Minimise harm to self and othersCome to terms with the experience
Path to problemsTry to block memory of the event
Avoid discussion of the eventAvoid anyone or anything that
reminds them of the eventLong-term numbing of emotions
Maximising recoveryEmbrace your humannessAccept responsibility for yourself andyour recoveryDon’t fightDon’t runDon’t lash out at yourselfDon’t lash out at othersTurn and face your fears and workthrough themThe task is to ‘find a peace’ or ‘learn tolive with’ what happened.
“ Isolation is risk”
There are two paths following a traumatic event:
Chapter Seven
WHEN ALL ELSE FAILS(IF THE HORSE HAS ALREADY BOLTED)

6564
Chapter Seven
WHEN ALL ELSE FAILS(IF THE HORSE HAS ALREADY BOLTED)
If, despite the practitioner’s best efforts they still find themselves on the ‘slipperyslope’ toward burn out, it is important they take immediate steps to reverse the
process.
Practitioners have a finite store of energy, and when it is used up they may need sometime away from the job before it can be replenished.
It takes a fair amount of time to burn out. A similar amount of time may be required torepair the damage. The longer a practitioner leaves it before they try to reverse theprocess, the longer their recovery process is likely to take.
As mentioned, self-care is both prevention and cure for burn out.
Burn-out is usually identified by the core characteristics of physical and emotionalexhaustion, low self-esteem, poor job satisfaction, and a negative and cynical attitudetoward individuals, families or the community.
Sometimes it can be difficult to determine if a practitioner is burning out because ofday-to-day stress or traumatic stress. The former has a slow sizzle effect over time whilethe latter can have more of a crash and burn effect.
In remote areas, burn-out is more likely to result from a combination of both exhaustionand traumatisation. This can give rise to a high level of distress - even anguish.
If there are elements of trauma involved then the practitioner would do well to seek thesupport of a mental health practitioner.
If a practitioner thinks they are burning out, it is time to make a sober assessment oftheir situation.
They should assess their ability to recover on the job. If this is not possible, they shouldconsider taking whatever leave they have available to them as soon as they can arrangeit (ideally within weeks rather than months).
For those who see themselves as indispensable and unable to leave the position whichis burning them out, the cynicism often identified as a core component of burn outrarely makes it worthwhile to hang on. It is likely to ruin everything. The practitionermay end up despising everyone, and everyone may end up being none too keen on thepractitioner either.
While on leave the practitioner should aim to rest, recover and nurture themselves asindulgently as they can manage.
Once they have recovered sufficiently to think clearly, they should ask themselves thefollowing questions: Is it possible for any practitioner to sustain themselves in theirposition? Is the work environment safe for them to work in?
If the job demands more of them than it is humanly possible for any practitioner to give,then it will probably burn them out regardless of how well they try to care for themselves.
If they feel certain they will end up being damaged by their job then they should transfer,resign, whatever, but they should get out of there. Flee!
Many practitioners would agree that there are some communities / health services /employers which are toxic for any health practitioner - they will overwhelm anypractitioner’s abilities to cope and burn them out sooner or later. An extremely highturnover of staff can be a good indicator of such settings. Often it is best to avoid suchplaces, at least until the health service structure or provision is examined and improved.
By the same token, there are many remote communities or health services or employersthat offer good support to practitioners and allow them to sustain themselves. Highretention rates may indicate such places. A practitioner can always choose to work inanother, less stressful situation.
Alternatively, it may be necessary for the practitioner to reassess their goals. Are they inthe right job after all? Are they the right person to be doing remote work? Is remotepractice really what they want to do at this particular point in their lives?
If remote practice constantly leaves them feeling inadequate and overwhelmed then thepractitioner may need to take some time out. During this time they could, for example,skill themselves up before returning, take a year off and work somewhere else (preferablyless challenging), change their employer / organisation / community, or perhaps leaveremote practice altogether.
This should not be seen as a sign of failure, but as a courageous and positive move,informed by a realistic assessment of their situation and a perfectly proper concern fortheir own welfare.
In general sole practitioner positions demand a lot from practitioners, particularly if theyare required to be on call twenty four hours a day, seven days a week. It is probablyunwise for a practitioner new to remote practice to accept such a position.
Indeed, a question should be raised as to whether any sole practitioner position canallow even the most experienced practitioner to maintain their wellbeing for longerthan a year or two.
Sometimes moving to a team setting where on-call is shared can allow sole practitionersto recover.
6766
WHEN ALL ELSE FAILS (IF THE HORSE HAS ALREADY BOLTED)
What if someone else’s horse has already bolted?
A common issue raised by remote practitioners is what to do with those practitionerswho have already burnt out. This refers less to those practitioners who stay for only ashort time and burn out during the course of their adaptation process, and more tothose practitioners who have been around for a few years and who have burnt out onthe job.
The practitioner concerned is often a shell of their former fully functional self, and hasbecome full of hostility, negativity and cynicism.
It is commonly reported that everyone but the practitioner recognises that they arebadly burnt-out. They may be unaware of the negative impact they are having onteams, on communities and the ability to provide an effective health service.
There is often concern about the impact such practitioners can have on new staff.
In their mind, the burnt out practitioner is just calling like it is - to them there is nogravity, remote practice / remote health / the organisation / management sucks.
To others they may seem punch drunk, dodging shadows and slogging it out overimagined or unresolved grievances. Sometimes the practitioner may seem wild withpain and anguish. Their perceptions may seem flawed. They may seem depressed, orbe using substances to dampen their distress.
They may feel guilty and blame themselves for what happened, for how they feel, orview their distress as a personal failure.
Often this level of burn out is a result of prolonged and high levels of stress overlaid withrepeated traumatisation. High levels of distress are not uncommon in practitioners whowork in communities which experience repeated traumatic events. As the practitioner’sresilience becomes more and more eroded, each event takes an increasing toll. Like theresidents of the community, they may have been pushed beyond their boundaries by somany layers of loss, grief and pain.
So what can be done?
Unless the practitioner is prepared to acknowledge where they are at, personally andprofessionally, very little can really be done. Sometimes, particularly if the practitioner isno longer able to provide a safe level of care, it may even be necessary to take the issueout of their hands.
However, a punitive response which seeks to monitor and ‘improve’ their performance,is only likely to increase their stress levels and their sense of betrayal - ie make thingsworse. What is required is a supportive response which encourages them to admit tothemselves that they need a rest and time out to recover.
Raising the issue with a burnt out practitioner can be fraught with risk. They are likely
CHAPTER 7
to be very defensive and reactive. There is some risk that expressing concern about theirwellbeing will be misinterpreted as an attack or a criticism, or as blaming them for theircurrent state of mind.
If the issue of burn-out is to be raised with a practitioner it should be done carefully andsensitively and according to a plan (preferably by someone the practitioner trusts orknows such as a mentor or professional supervisor).
Expressing concern and a willingness to listen can be a beginning. The listener mayhave to hear an outpouring of many grievances before they get to the bottom of what iscausing them the most anguish. Sometimes guiding the practitioner to look back towhen things started to go wrong can help. It is not uncommon to find a job relatedtraumatic event has set the process of ‘burn out’ under-way. The distress associatedwith an unfettered traumatic stress reaction can bring any practitioner and their situationundone.
Lending resources such as this booklet may help a practitioner to recognise the signs ofburn-out. It may help them reach a point where they can admit that they need to takesome action to reverse the process (those readers now feeling paranoid because acolleague gave them this booklet to read, may need to reflect on their behaviour...!).Admitting they have been overwhelmed is often the first step toward the practitioner’srecovery.
Options for recovery or time out, or perhaps redeployment to a less demanding positionor community should be considered. Recovery on the job can be assisted by psychologicalsupport through employee assistance services.
Many practitioners will be able to recover using whatever leave they have available tothem. Some may be able to recover on the job if they are relocated to a less stressfulposition. However, some practitioners may be so badly burnt out they are unable tocontinue to work or to meet their financial commitments. If this if the case they are likelyto be disadvantaged financially as a result.
The issue of responsibility and duty of care must be raised here.
The practitioner did not burn out for fun or as a hobby. It is a job-related injury. As suchtheir current employer should offer whatever support they can to help them recover orto seek worker’s compensation.

6968

70 71
A smorgasborg of strategies to assist practitioners to cope with some of the stressassociated with remote practice is offered in the following section.
Practitioners are invited to select whatever strategies suit their own taste, and leave therest for others to choose from.
STRATEGIES FOR IDENTIFYING SOURCES OF STRESS
Try these simple exercises to differentiate what you can influence and what is beyondyour control.
Identifying sources of stress: strategy one.
Make a list of the things in your life which are causing you stress or problems.
Rank order them in their importance or impact on your life.
Categorise each one as either requiring ‘immediate action’, ‘future action’ or ‘ignore oradapt to’.
Immediate action refers to issues which need to be dealt with to day or within the nextfew days.
Future action refers to issues that require action, but you may be unsure about whataction is required, or it may be clear what is needed but nothing can be done until amore appropriate time.
Ignore or adapt to refers to those issues which are beyond your reach for the foreseeablefuture, and just have to be coped with as they are.
If your list is intimidatingly long, decide to address the easiest ones first, rather thangoing straight to the big issues.
Some issues may need to be put on the back burner to give yourself time to examine theproblem and decide the best course of action to deal with it.
(Adapted from Fontana, 1994)
Identifying sources of stress: strategy two.
Write the problem on a piece of paper.
Draw two circles around it. A large outer circle and a smaller inner circle.
The large outer circle is your circle of concern. Note down the elements of the problemthat are beyond your control. These are the elements that you will have to come toterms with, or learn to live with, without letting them erode your peace of mind.
The smaller circle is your circle of influence. Within the smaller circle note down theelements of the problem that you have some power to influence or change in some way.These are the elements that you can start to do something about.
During the process of starting to address the issues in the smaller circle you may findsome of the elements in the larger outer circle may come under your control. By thesame token you may find issues that you thought you could address are not really withinyour control.(Adapted from Covey, 1993)
STRATEGIES FOR SOLVING PROBLEMS
Solving problems: strategy one
Try this exercise:
Identify the problem. Condense it down to one word or sentence.Think up as many possible solutions as you can.Then weigh up the good and bad points about each option.
Ask what are the consequences of each option. What would be likely to happen if youdid what was listed - can the outcomes be predicted?
Decide which one is best and commit yourself to carrying out this solution.
Once you have decided on a course of action it may help to break it down into severalsmaller steps.
Then follow the plan through one step at a time.
If it works, great!
If it doesn’t work, it will still be a learning experience that can help you clarify the situation. Youcan feed the information about why it didn’t work back in. Then you try again - taking intoaccount the outcome of the first solution. Or perhaps you can explore alternative solutions.
1
Chapter Eight
COPING STRATEGIES 2
1
72 73
If nothing works, perhaps you need to accept you cannot change the situation.
If this is the case, it may be useful to think of strategies that might help you to live withthe situation as it is. This may mean implementing practical strategies to protect yourwellbeing in the face of the stressor, by changing your attitude to the situation, or byimplementing good self care strategies.
Solving problems: strategy two
Begin with the end in mind. Identify your desired outcome.
Imagine that your fairy godmother appeared and offered you a wish to sort a situationout.
What would the situation look like once the problem had been solved?
What changes can you make to bring that about?
Make a plan and implement it to bring your desired outcome into being.
STRATEGIES TO MANAGE TIME & SET PRIORITIES
Ask yourself these three questions:Are you completely satisfied with the way you use your time?If not, why not?What could be done to use your time more satisfactorily?
Probably one of the most important time management strategies is learning to say no.Sometimes, knowing what not to do is as important as knowing what to do.
Let others know your limitations. Over commitment is a sure road to exhaustion.
Time management: strategy one
List all the things you want to get done.
Separate this list into what MUST to be done and what you WANT to get done.
Then list what MUST to be done in order of priority.
Then work through this list one point at a time. This may mean saying no to otherthings.
Time management: strategy two
Identify activities you would like to spend more time doingIdentify activities you would like to spend less time doing.List some short but realistic steps you could take now to start seeing these goals comeabout.Long-term goals:Set some goals for yourself for the upcoming year. What obstacles might be in the wayof these? What can you start doing now toward these goals?
Time management: strategy three
Differentiating between what is urgent and what is important can be useful to managetime and set priorities.
Make a list of the things you need to do.
Identify those tasks which are both urgent and important. Do these tasks first.Identify those tasks which are urgent but not important.Identify those tasks which are not urgent but important.Identify those tasks which are not urgent and not important. Do these tasks last.
(Adapted from Covey, 1993)
Time management: strategy four
How the practitioner structures or manages their time may help reduce the impact ofday to day stress. Research with stress and coping among urban based occupationaltherapists (Sweeney, Nichols & Cormack, 1993) revealed coping strategies which maybe applicable across professions and perhaps in remote settings as well:
1. Taking time out during the day for coffee and lunch breaks.2. Programming some time each day as non-treatment time eg. for report
writing or program management.3. Having a cut off point at the end of each day to indicate the transition
from a work to a social role (e.g. some form of exercise)4. Spacing out rewarding and non-rewarding tasks.5. Using positive coping skills in the workplace, such as time management,
prioritising and limit setting.6. Cultivating personal awareness of stress as well as discussing stress issues
with colleagues.
2
1
2
3
4
74 75
Some suggested strategies to do this:
• Try to think positive thoughts. Look for and notice any positive attributes, nomatter how small, in any given situation.
• Imagine you are several years into the future. How much will it really matterthen?
• Confront your fear. Exaggerate the situation. Paint a worst case scenario - what’sthe worst thing that can happen? How likely is it?
• Eliminate ‘should’ statements from your thinking and replace these with ‘could’or ‘want to’ or ‘choose to’. Directing ‘shoulds’ at yourself means you are tryingto motivate yourself with guilt and punishment rather than moving toward positiveoutcomes. Directing ‘shoulds’ at others often leads to feelings of anger, frustrationand resentment if they don’t comply.
• Be as fair to yourself as you would be to others. Imagine a good friend is describinga situation similar to that you are experiencing and imagine what advice youwould give them. Follow your own advice.
• Don’t let negative thoughts run out of control. If you notice yourself constantlypainting worse case scenarios and interpreting situations in a negative mannersay to yourself ‘STOP’, pause, and then take a fresh and more balanced look atthe situation.
• Analyse the ‘self talk’ that may lead you to feel stressed about a situation. Changethe ‘self talk’ to a more positive interpretation. For example, instead of thinking‘this person drives me nuts’ try replacing it with ‘I can cope with this person’ andnotice the difference in the way you feel in response.
• If you have a particular worry that keeps popping unwanted into your mindmake a plan to allocate some ‘worry time’ to it each day. Schedule this, say forhalf an hour in the evening. Put off worrying about whatever it is until you sitdown to have your ‘worry time’. This will allow you to concentrate on the task athand and minimise the amount of worry in your day.
• Assess your strengths and weaknesses. Accept yourself as you are, warts and all.No one is perfect or without human frailties (in fact they would be scary to bearound if they were!).
• Keep a journal of gratitude. Note down pleasant moments or experiences inyour day. This might be as simple as the way the morning light falls in yourkitchen, or the smell of your bread maker at work. While a simple strategy, it canhave a powerful positive effect on your perception, how you feel, what you notice,and the amount of pleasure you experience during each day.
1
2
STRATEGIES TO DEAL WITH CONFLICTING DEMANDS
Decision making: strategy one
You have one or two choices and you can’t make up your mind which one is best?
This exercise may help you to clarify your choices.
Take a piece of paper and draw a line down the middle that divides the page into twocolumns.At the head of one column write ‘negatives’ and on the other write ‘positives’.Now list the positives and negatives associated with each choice.Weigh up the positives and negatives and select the best option.
Decision making: strategy two
Having difficulty in prioritising or meeting conflicting demands? Try the following exercise:
Imagine you are at your own funeral. How would you like others to remember you? Asa great parent? As someone who made an important contribution to your profession?As someone who was always willing to have fun? A great artist?
At a work level, you could imagine what you would like people to remember or say aboutyou as a practitioner. What contributions would you want to be remembered for? Is it assomeone who was fun to work with? Is it someone who worked to achieve change?Someone who embodied a primary health care philosophy? As a great clinician?
This exercise may help clarify what choices to make next time two important butcompeting demands come up.
For some reason, it is often easier to clarify what you want to achieve by looking backwards,ie to imagine you have ‘arrived’ and then identify the elements which make up thepicture of success. (Adapted from Covey, 1993)
STRATEGIES TO CHANGE THE WAY YOU THINK & FEEL
Be careful about the things you say to yourself. The stress response can be set off byactual events or by your thinking and imagination alone.
The way you think about a situation will influence how you feel and ultimately how youbehave in response to it. If you can change the way you think, you can change the levelof stress you feel about a situation.

76 77
• If your anger indicates a threat to your wellbeing, plan to address it in coolheaded way, rather than just by venting your emotions in the heat of the moment.
• Develop a few coping strategies to defuse your angry reactions before you lashout at others. For example, by counting to ten, taking a few deep breaths, byleaving the situation, by going off alone to cool down, by engaging in exercise,by using relaxation exercises, or by working out a resolution within yourself.
When you feel angry:
• Acknowledge but do not indulge the emotion.
• Use the coping strategies you have developed to defuse the anger and cool off a bit.
• Think about the situation – is there anything you need to do – is there a threat toyour wellbeing that needs to be addressed – or was your anger just a result ofyour overall stress?
• Try to achieve a calm state of mind before working out a plan to deal with theproblem.
• Do not allow your anger to build on itself. Challenge any negative thoughts thatmay be fuelling your anger. Distraction can help prevent a negative train of thoughtfrom escalating or maintaining your anger, eg, watching TV, reading.
• Plan to deal with the problem constructively. Begin with the desired outcome inmind, and use assertive communication skills to achieve what you want.
Managing anger in others
Clashes with clients or community members may be particularly upsetting. This may bemore so when clashes are unexpected or perceived to be unfair or unjustified. Sometimespractitioners are faced with blame which belongs more to the system rather than theindividual practitioner.
This can be distressing when the practitioner feels they are genuinely doing the bestthey can to help their client(s). They may have even been expecting appreciation.
It may leave unhappy feelings that persist for days or weeks after the event.
If the practitioner reacts to the anger of others by attacking or withdrawing, conflictmay be escalated.
• Don’t struggle to control situations which are beyond your control. Sometimesthe best thing to do is to ‘let go’, and accept what is rather than what you wouldlike it to be. Let go of your expectations. Go with the flow.
• Aim to be as happy as you can as often as you can. Laugh as much as possible.
STRATEGIES TO MANAGE FRUSTRATION AND ANGER
Remote practitioners often have to deal with high levels of frustration. Frustration ariseswhen you are blocked from achieving a goal or something you want to do. This can giverise to strong stress responses of high levels of anger.
In small team and community settings uncontrolled anger can destroy relationships anderode any good will the practitioner may have built up. Reacting angrily can be destructive– it only makes the situation worse. This is most likely to occur when you are feelinghighly stressed and under a lot of pressure. People who are highly stressed tend to bedefensive and reactive in response to new challenges. Try to avoid blowing up withanger at others, or by withdrawing and stewing over your anger.
Anger can be used constructively or destructively. If used well, it can provide energy andmotivation to respond to and overcome threats or challenges, ie it can be used to createa better situation.
Managing anger
Anger is a natural, healthy emotion that can help you recognise when you or your well-being are put at risk. As well as physical threat, this might include being blocked fromachieving an important goal, being insulted, demeaned or having one’s self esteem ordignity threatened.
Beware of anger which is unrecognised or unacknowledged and becomes turned in ononeself (one theory of depression is that it is anger turned inwards). At the same timeone needs to be aware that anger can build on itself. Ruminating on the things thatmake you angry will usually increase rather than decrease the anger. Avoid doing this ifyou can.
Before you get angry:
• Remember you are responsible for your own feelings (no-one can make you feelanything).
• Identify those events and behaviours that can trigger your anger.
• Avoid ‘setting yourself up’ to get angry

78 79
STRATEGY TO MONITOR LONG-TERM WELLBEING
Maintaining all the important elements of a practitoiner’s life may be a struggle in remoteareas.
The following strategy may help you to monitor where you are putting your time andenergy and how well the different parts of your life are going. This exercise can be usedto regularly appraise what is happening in your life, and what is good about it and whatcould be better.
Draw the spokes of a wheel.
Label each spoke with an important part of your life, eg one spoke for family, one forwork, one for hobbies, one for study etc. Each person’s wheel will reflect their uniqueinterests and will be different from other peoples.
Give each spoke a mark out of ten depending on how well that part of their life is going- ten being the most, one being the least.
Join the dots and then assess how round the wheel looks.
The aim is to have the wheel as round as possible. A round wheel will indicate a holisticand broad base to your wellbeing.
If you are allocating all of your energy to only one or two areas of your life then the circle(and your life) will be out of kilter. The exercise may show up areas of your life that arebeing neglected and need some attention.
STRATEGIES TO SET BOUNDARIES BETWEEN WORK AND HOME
The two main factors which can erode non-work areas of the practitioner’s life are thelack of natural circuit breakers between work and home and the lack of anonymity of thepractitioner.
Sole practitioners who are required to be on twenty-four hour call seven days a weekmay find it particularly difficult to relax beyond a certain level when they are on call.Indeed being totally relaxed while on call is perhaps not desirable. However, there is aneed to relax as much as possible if long-term wellbeing is to be maintained.
Avoid going home and rehashing the days events and letting your mind chew over theevents of the day in a repetitive and unproductive way or nursing your outrage atcolleagues, clients or whatever. Develop some routines that you build into each day.
Some suggested strategies to help reorient yourself from work to home:
• Have a shower and change into comfortable clothes when you get home. Lightsome incense, put some relaxing music on. Make a cup of tea.
If the practitioner chooses to respond respectfully instead, they may be able to de-escalate the conflict and bring emotions to a level where the issue can be dealt withmore constructively.
Suggested strategy to respond to the aggression of clients / consumers:
1. Remain calm and respectful.2. Listen and say nothing for the moment.3. Acknowledge their anger.4. Show empathy.5. Apologise without accepting blame.6. Ask questions if necessary in a polite, even handed manner.7. Agree with the person.8. Do not offer excuses or argue.9. Suggest a strategy to deal with the person’s concerns, including a time frame.
(Adapted from Bull & Coop, 1997).
Note: Sometimes a practitioner may catch the brunt of misplaced anger from a pastsituation that may be being projected into the current situation. Such anger may seemto be sudden and inexplicable.
In Aboriginal & Torres Strait Islander settings this anger may be related to the chronicand collective traumatisation by non-Indigenous colonisers over several generations.
Survivors of prolonged trauma, including Indigenous Australians, can be ‘triggered’ byevents which remind them of the original trauma, or perhaps by any event which leavesthem feeling powerless or victimised. Overwhelming emotional reactions can result inresponse to such triggers or reminders.
Non-Indigenous practitioners need to be aware of the history and how this impactson Indigenous people and health service delivery today. They also need to beespecially sensitive to perceptions of power and its misuse by non-indigenouspractitioners.
Practitioners unaware of the history of colonisation may remain oblivious to their role intriggering overwhelming reactions in Indigenous clients or colleagues.
Developing an understanding of the political and historical environment in which theywork may help the practitioner to avoid such incidents and increase their safety and thatof their clients.

80 81
The earlier the conflict is detected and dealt with, the easier it will be to settle.
Conflict can be resolved if disagreement is not seen as a situation where one wins andthe other loses.
One must first give up ideas of ‘getting even’ or punishing the other person. That is notresolving conflict - it is escalating it.
Those who seek a solution in which one party is humiliated or ‘loses’ may find theconflict is merely prolonged. Revenge may be exacted at a later date if one party perceivesunfairness or injustice in the outcome.
Therefore an attitude of respect and legitimacy for views other than one’s own is necessarybefore one begins.
Conflict can provide opportunities for changes that can lead to better outcomes for allinvolved.
Resolving conflict requires one to think along the lines of trying to find a solution thatmeets the needs of all parties concerned. This can be a challenge and may take somecreativity.
Begin by identifying what your needs are.
Identify what the needs of the other party are.
Is there a way that all parties can have their needs met?
Set goals which all parties can accept.
Work towards achieving those goals.
It is well worthwhile for remote practitioners to locate readings, resources or training inrelation to conflict resolution. It is a very useful skill for remote practitioners to have.
STRATEGIES TO COMMUNICATE ASSERTIVELY
Remember you are both a receptor and transmitter of stress.
You probably need to take some responsibility of the stress you may cause others. Becareful how you communicate when you are feeling stressed and under pressure.
The stress response pushes you to ‘fight’ or ‘flight’ your way out of problems. Usuallypeople express this by exploding with pent up aggression or by withdrawing and sulking.Try to avoid either ‘fight’ or ‘flight’ and aim for ‘flow’ instead.
It is best to be assertive in your relationships with work colleagues - don’t just give in, yet
• At the end of the work day take ten minutes to acknowledge what you haveachieved and give yourself credit for it. Don’t waste time feeling guilty aboutwhat you could not do. Try to discipline yourself to work during work time, andallow yourself to relax at the end of each day.
• Try a guided visualisation on the drive home or as you walk through your front gate:imagine you have a box in your hands or on the seat next to you. This is a box forwork related worries. Imagine you are taking the lid off and putting your workworries in the box and then putting the lid back on.
In the morning as you drive to work or walk out the front gate, take the lid off thebox, and take back your work related worries, ready to start the day’s work.
• Some practitioners put strong boundaries around their home. Visitors are byinvitation only.
• Some ensure their home is as comfortable as possible. Much loved objects canbe transported to the community. Some use aromatherapy products, candles,and relaxing music etc to create a relaxing ambience.
• Some ensure they take regular breaks (eg camping or fishing) away from thecommunity.
• Some use a bout of exercise to put a boundary between work time and hometime; for example: walking or jogging. This uses up the energy made availableby the stress response and enhances their ability to relax when they get home.
• For those who are undertaking further study the constant pressure to devote timeto study can lead to chronic stress. Good time management skills become essential.Some allocate relaxation time for themselves, say one or two hours in the eveningor one or two nights a week off for guilt free relaxation. This avoids the situationwhere, even if they are relaxing they are feeling guilty and beating on themselvesfor not studying.
• A Zen approach might be to give up ideas of trying to draw a line betweenpersonal and professional or between work and home. This approach acceptsthat remote health work is a lifestyle rather than a job.
STRATEGIES TO RESOLVE CONFLICT
Conflict arises from difference. Since everyone is different some conflict is an unavoidablepart of life.
Left un-managed, conflict can escalate from a feeling of discomfort through todisagreements, misunderstandings, tensions and crisis.
82 83
relaxed at the drop of a hat. The more you practice, the easier and the more automaticit will become.
Try to do at least one of the following relaxation exercises every day. You need certainthings to be able to relax:
• Somewhere quiet where you won’t be interrupted.• Comfortable position.• Right attitude: a willingness to allow yourself to relax.
Abdominal Breathing
When people are stressed they tend to breathe faster and higher in their chest thanwhen they are relaxed. Many people report that when they slow their breathing, feelingsof stress and tension decrease.
Learning to notice your breathing pattern and being able to change it to a relaxedpattern is a simple yet crucial skill to learn to relax.
Abdominal Breathing Technique
1. Place one hand over your navel.2. Take a deep breath in and blow it out completely through your mouth like a sigh.
Notice how your stomach flattens. Squeeze out every last bit of air.3. Allow the next breath to flow in by itself through your nose. Your hand on your
stomach will rise or move upward if you breathed in correctly.
Check your breathing several times a day, particularly when feeling tense. Slow anddeepen your breathing to abdominal breathing. You will find feelings of tension lessen.
Muscle Relaxation Exercise
1. Sit or recline comfortably with eyes closed.2. Really tense up one set of muscles - such as the arms or legs.3. Now let them go limp. If you do this properly, the contrast between tense and
relaxed should show you what relaxed really feels like. Dwell on that feeling.4. Now work on another set of muscles - such as the back, the stomach, the face.5. Now let them go limp. Dwell on the relaxed feeling. Try to hang onto it.6. Repeat through all the muscle groups.
Body Scanning
This is a useful exercise to practice during the day. Scanning can allow you to developan awareness of your body and to check whether you have built up tension in yourmuscles. It is quick and can be done anywhere.
at the same time don’t feel you have to be aggressive to achieve what you want. Youcan defend your rights and have your needs met without abusing or dominating others.
The aim of assertive communication is to communicate clearly and cleanly yourperceptions of and feelings about a problem without attacking, blaming or hurting theother person. It can also be used to open a discussion without eliciting defensivenessfrom the other person.
An assertive statement is usually made up of three parts. The first part of the sentencerelates to the action that you would like to be changed:
For example, ‘when you….leave without telling me,The next part of the sentence relates to how you feel about the action.For example, ‘when you leave without telling me, I feel…confused andcan’t make my own plans because I don’t know where you are’,
The last part of the sentence relates to what you would like to see happen instead in thefuture:
For example, ‘when you leave without telling me, I feel confused and can’t make myown plans because I don’t know where you are, and what I’d like tohappen is that you tell me when you are going, please’.
This basic structure can be used to build any manner of sentences to get your pointacross in a way which is clean and clear. You will be more likely to achieve what youwant if you are not aggressive or hurtful in your efforts.
(Adapted from Conflict Resolution Network material, 1998)
RELAXATION STRATEGIES
Mind and body are one. If you can calm your mind, your body will follow and viceversa.
Be aware that while stress chemicals are floating around your body, you will be gearedup to panic. Relaxing may therefore seem somewhat ‘unnatural’ to you. It may seemeasier to remain worried and restless.
However, relaxation exercises will help you to think more clearly, improve yourconcentration and reduce the strength of your stress symptoms. It is worth the effort.Prolonged stress reactions can, over time, not only exhaust you and put your health atrisk, but will almost certainly impact on your quality of life, erode your sense of humour,your sense of fun, your ability to find joy in life or to be vulnerable, warm and caring withothers.
As a remote practitioner, you will be well served if you aim to seize the moment andbecome deeply relaxed at short notice. Try to develop the skill of becoming deeply

84 85
Meditation can enhance your calmness, can ‘centre’ you andrelax you. It may enable you to be more aware of yourself,your needs and motivations and the needs and motivationof the needs of others. That is, it can bring increased clarityand calmness to your every day. It can also help your bodyto repair itself from the impact of stress and allow you torecharge your batteries, physically and mentally.
Meditation can be a natural state. If you have activities whichbring that about for you then ensure that they are includedin your regular routine.
The benefits of meditation may not be immediately apparent, and regular meditationmay be necessary before you reap the benefits.
A simple meditation technique is to sit comfortably in a quiet place. Close your eyes, orhave them slightly open while you become aware of your breathing - simply watch yourbreath go in and out. It may be helpful to count your ‘out’ breath up to ten. You willprobably be distracted by thoughts popping into your mind. Just return to your countingand let the distractions pass. When you meditate regularly the constant chatter in yourmind will decrease, and you will feel more calm and relaxed.
Repeat the exercise for ten minutes at a time, twice a day.
COMMON ERRORS WHEN TREATING FRIENDS AND FAMILY
Rourke and Rourke have examined common challenges posed by health practice insmall communities in Canada (1998). They suggest there are five common types ofhazards which can occur when treating friends as patients.
1. Risk of omission: Omissions may occur due to a reluctance to ask about or sharedifficult, painful or private problems with friends.
2. Breaches of Confidentiality: Confidentiality is difficult yet important to maintain.Ethical dilemmas can be heightened in situations when one knows all concerned.
3. Assumptions: Practitioners might assume they know how patients are feeling orreacting rather than asking directly. Familiarity can lead to closely identifying withpatients and adopting their problems as their own.
4. Loss of objectivity: This is a particular problem in critical situations or seriousillnesses. Judgement can become clouded and cause difficulties.
5. Blurred boundaries: Relationships in small communities may be complex andmultidimensional. Patients known in other roles may have increased access topractitioners after hours. Unclear or blurred professional boundaries can lead toabuse of patient by practitioner or practitioner by patient.
1. Breathe in while scanning one area of your body for tension.2. As you breath out relax that area.3. Progress through each area of your body.4. Move through your face and neck, shoulders and arms, chest, stomach, legs and feet.
Use scanning regularly through the day and when you first arrive home from work toensure you are fully relaxed.
Word Repetition Relaxation Exercise
1. Sit or recline comfortably with eyes closed.2. Deeply relax all your muscles, beginning with your feet and progressing up to your
face.3. Breathe through your nose. Become aware of your breathing.4. As you breathe out, say the word, ‘ONE’, silently to yourself. For example, breathe
in...out, ‘ONE’; ....in...out...’ONE’ etc. Breathe easily and naturally. The repetitionof ‘ONE’ helps break the train of distracting thoughts.
5. Continue for 10 - 20 minutes.6. When you finish, sit quietly for several minutes, at first with your eyes closed, and
later with your eyes open.
Visualisation Exercise
1. Sit or recline comfortably with eyes closed.2. Use an exercise to relax yourself.3. When you are relaxed, see yourself in your mind’s eye in a place where you feel
very relaxed, peaceful, safe and tranquil.4. Think of the sounds you can hear there, the fragrances you can smell there, what it
feels like to be there, the relaxed body sensations.5. For a couple of minutes just stay there in that peaceful place enjoying all these
sensations.6. Imagine how you look while you’re there, feeling peaceful and free.7. Allow your mind to come back to the room you’re in.8. Move and stretch a little.9. Open your eyes and feel alert and refreshed.
Adapted from Wilson (1997)
MEDITATION TECHNIQUES
The benefits of meditation can make you physically and mentally able to deal betterwith stress and help to develop a new perspective on problems.
It is difficult to describe exactly what meditation is, but most people have experienced ameditative state. This is the feeling one gets when totally absorbed in an activity, alosing of awareness of oneself, of time and place. A sense of being ‘at one’ with whatone is doing. This may occur while fishing, sitting by the water or a fire, or whilecreating something....

86 87
They suggest practitioners should set the same limits for all patients whether a specialfriend, colleague or not. Both practitioners and patients must be alert to the effect ofthe non-professional relationship on the professional one and vice-versa, and to adjusteither relationship accordingly.
This is an interesting article and is worth a read if you can access it.
USE OF CRITICAL REFLECTION TO PROMOTE ADAPTATION
This section was contributed by Bernie Ward, CRANA Board of Management.
As far back as 1933 Dewey documented that there is no true growth in learning by mereexperience alone, but only by reflecting on experience. Reflection helps giving meaningto our lives and the world in which we live.
Boud, Keogh and Walker (1985) described a three stage model of reflection that hasbeen used by many health science disciplines.
Stage 1: Returning to the experience
Recalling the event either by writing about it, telling someone about the experience orreplaying the experience in your mind. The recall should not include any judgementsbut instead should focus on what actually happened not what could have happened.
Stage 2: Attending to one’s feelings
Returning to an experience may be uncomfortable or distressing. Negative emotionssuch as anger and fear can block the reality of the situation and make it difficult to seeother ways of looking at the situation.. Try focusing on whatever positive feelings arethere and explore and enjoy them.
Stage 3: Re-evaluating the experience
Analyse the issues. Would you do anything different if a similar event occurred again?Are there any old practices or attitudes that need to be replaced with better ways ofdoing things in the future?
Keeping a journal to map the process of critical reflection can help to facilitate andenhance the adaptation process of remote practitioners.
88 89
McDermott, R. (1994) Redressing Urban Bias: A Needs-Based Approach to Health CareResource Allocation in Remote Australia, Proceedings of International Conference on IssuesAffecting Rural Communities Conference, Townsville, July.
Randall, P. (1997). Adult Bullying: Perpetrators and Victims. New York: Routlege.
Raphael, B. (1986). When Disaster Strikes. New York: Basic Books.
Rourke, L & Rourke, J (1998) Close Friends as Patients in Rural Practice. Canadian FamilyPhysician. Vol 44, June, pp1208 – 1210.
Sutherland, D. (1999) Profile. Bush Alert. Newsletter of the RACGP’s Rural Faculty andRural Training Stream. Vol 3, (1), March 1999.
Sweeney, Nichols & Cormack, (1993) Job stress in occupational therapy: copingstrategies, stress management techniques, and recommendations for change. BritishJournal of Occupational Therapy. Cited in S. Hardy, J. Carson, and B. Thomas (Eds)(1998) Occupational Stress: Personal and Professional Approaches. Cheltenham: StanleyThornes Ltd.
Tolhurst, H., Bell, P., Baker. L., Talbot, J. and Cleasby, L. (1997) Educational and SupportNeeds of Female Rural General Practitioners: Final Report. School of Nursing and HealthAdministration, Charles Sturt University, Bathurst.
Tregenza J. & Abbott, K. (1995) Rhetoric and Reality. Perceptions of the Roles of AboriginalHealth Workers in Central Australia. Central Australian Aboriginal Congress, Alice Springs.
Wakerman, J. (1999) Access to Health Care Services in Remote Areas. Conference paper,Rehabilitation Conference, Adelaide
Wilson, P. (1997) Calm at Work. Sydney: Penguin Books.
Bull, B. & Coop, C. (1997) Resources in Mental Health, Gordonvale Ph: (07) 40561570, Qld.
Conflict Resolution Network (1998) Conflict Resolution: Trainers’ Manual. Chatswood.
Cotton P (Ed) (1996) The Major Types of Psycholgical Dysfunction in Workplace Settings.In P. Cotton (Ed). Psychological Health in the Workplace: Understanding and ManagingOccupational Stress. Australian Psychological Society. Melbourne.
Covey, S (1994) The Seven Habits of Highly Effective People. The Business Library,Melbourne.
Department of Primary Industries and Energy and Department of Human Services andHealth (1994) Rural, Remote and Metropolitan Areas Classification 1991 Census Edition,Australian Government Publishing Service, Canberra.
Fisher, J., Bradshaw, J., Currie, B., Klotz, J., Robins, P., Searle, K., & Smith, J. (1996)Violence and Remote Area Nursing. Australian Journal of Rural Health. 4. 190 - 199.
Fontana D, (1989) Managing Stress. British Psychological Society & Routledge Ltd,London.
Grasha A, and Kirschenbaum, D (1986). Adjustment and Competence. West PublishingCompany. New York.
Howard, D. and Ferguson, A. (1999). More than Just a Nurse. Territory Health Services,Darwin.
Kelly, K (1999) Preventable Sources of Stress in the Remote Workplace CRANA OccasionalPaper Series: Paper One CRANA Secretariat Office, Alice Springs, NT.
Kelly, K. (1999) Preventing Posttraumatic Stress Disorder Among Remote HealthPractitioners: An Overview of the Evidence. CRANA Occasional Paper Series: Paper Two.CRANA Secretariat Office, Alice Springs, NT.
Kreger, A. (1991) Remote Area Nursing Practice: A Question of Education, Council ofRemote Area Nurses of Australia Report, Cairns.
Lazarus, R. & Folkman (1984) Stress, appraisal and coping. Springer: New York.
REFERENCES

90 91

92