COVID-19 INFECTION IN PREGNANCY
48
COVID-19 INFECTION IN PREGNANCY PROTOCOL FOR HEALTH CARE PROFESSIONALS PALESTINE, JULY 2020 STATE OF PALESTINE MINISTRY OF HEALTH WOMEN’S HEALTH AND DEVELOPMENT UNIT
Transcript of COVID-19 INFECTION IN PREGNANCY

COVID-19 INFECTION IN PREGNANCYPROTOCOL FOR HEALTH CARE PROFESSIONALS
PALESTINE, JULY 2020
STATE OF PALESTINEMINISTRY OF HEALTHWOMEN’S HEALTH AND
DEVELOPMENT UNIT


COVID-19 INFECTION IN PREGNANCYPROTOCOL FOR HEALTHCARE PROFESSIONALS
PALESTINE, JULY 2020
STATE OF PALESTINEMINISTRY OF HEALTHWOMEN’S HEALTH AND
DEVELOPMENT UNIT
1

2
3

Members of the TechnicalCommittee of the protocol
• Mrs. Maha Awwad, Director of Women’s Health and Development.• Dr. Hadeel Yousif Al-Masri, Obstetrician and Gynecologist, MD, PhD, Director
of Women’s Health.• Dr. Emad Abed, Obstetrician and Gynecologist, MD, Head of Obstetrics and
Gynecology department, Palestine Medical Complex.• Dr.Rasha Al-Hamouz ,Obstetrician and Gynecologist, MD, Rafedia Surgical
hospital. • Dr. Bassam Al-Akhdar Obstetrician and Gynecologist, MD, Head of Obstetrics
and Gynecology Department, Al-Makassed Islamic Charitable Hospital.• Dr. Saeed Al Sarahneh, President of Obstetrics and Gynecology Association.• Dr. Sahar Hassan, PhD, Dean Faculty of Pharmacy, Nursing, and Health
Professions, Birzeit University.• Dr. Ruqaya Al-Faqeeh, Obstetrician and gynecologist, MD, Primary Healthcare
directorate.• Dr. Amir Atawneh, Neonatologist, MD, Al-Makassed Islamic Charitable
Hospital.• This document has been reviewed and appraved by the Reproductive and
Sexual Health National committee.
4
Table of contents1. Background and goals . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.1 Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
1.2 Goals of the protocol . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
2. Screening for COVID-19 infection and medical staff considerations . . . . . . . . . . . . . . . . . . . . 8
2.1 Screening for COVID-19 infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
2.2 Medical staff considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
3. Antenatal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.1 Women low risk or negative for COVID-19 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
3.2 Women with suspected or confirmed COVID-19 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
3.3 Remote antenatal care checklists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4. In-hospital management of COVID-19 disease during pregnancy . . . . . . . . . . . . . . . . . . . . . 22
4.1 Indication for admission due to COVID-19 disease during pregnancy . . . . . . . . . . . . . . . 23
4.2 Investigations for women admitted with COVID-19 disease during pregnancy . . . . 24
4.3 Treatment of COVID-19 disease during pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
5. Labor and delivery in women with COVID-19 infection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
5.1 Preterm labor in women with suspected or confirmed COVID-19 . . . . . . . . . . . . . . . . . . 33
5.2 Time of delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
5.3 Intrapartum management of women with suspected or confirmed COVID-19 . . . . 34
5.4 Immediate postpartum care for women with suspected or confirmed COVID-19. . . . . . . . . . . 35
6. Newborns and breast feeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
7. Postnatal care and family planning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
7.1 Remote postnatal checklist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
8. Thromboprophylaxis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
5
1. BACKGROUND AND GOALS
6
1.1 Background• Based on currently available evidence, otherwise healthy pregnant women seem
not to be at risk for more severe disease of COVID-19 infection than their non-pregnant peers. A study in the UK including 427 pregnant women with COVID-19, reported that 9% of women included in the study required critical care and 1.2% (five women) died. Whether these deaths are a direct result of COVID-19 infection is currently unclear, and these data are likely to be updated in the future.
• It is uncertain whether COVID-19 infection is associated with increased adverse maternal or neonatal outcomes. Evidence is limited to infection in the third trimester, with some cases of premature rupture of membranes, fetal distress and preterm birth reported.
• Possible vertical transmission has been reported in several cases of peripartum maternal infection in the third trimester, suggesting congenital infection is possible but uncommon.
• A review of 71 neonates delivered to women with COVID-19 in the third trimester reported that neonatal infection was diagnosed in 4 cases (5.6%) within 48 hours of delivery by PCR tests of cord and neonatal blood samples. Existing evidence has not identified major risks of complications in babies born to mothers with COVID-19.
• More research is awaited to determine if COVID-19 infection at earlier gestations would impose teratogenic threats to the fetus.
• It is estimated that there are more than 210,000 pregnant and lactating women in the West Bank and Gaza and more than 30 000 births are expected over the next three months.
• This document provides a guidance to maternal care providers for the management of pregnancy during the corona pandemics but also can be replicated in other emergency situations.
1.2 Goals of the protocol• Provide maternity and sexual and reproductive health care providers with a
summary of currently existing evidence on management of pregnant women during the corona pandemics.
• Ensure continuity of care for all women regardless of COVID-19 status.• Provide pathways to deliver sexual and reproductive health care for women with
COVID-19 without compromising the health of the rest of the population.• Screening and early detection of COVID-19 infection to allow rapid supportive
treatment.• Ensure protection of health care providers.
7

2. SCREENING FOR COVID-19 INFECTION AND MEDICAL STAFF CONSIDERATIONS
8

2.1 Screening for COVID-19 infection• Screening allows early detection of patients with COVID-19 to slow transmission
and provide timely appropriate care for COVID-19 patients.• Screening for symptoms of COVID-19 should be undertaken during remote
antenatal check-up (see section 3.3 Remote antenatal care checklists) and by phone before arrival wherever possible.
• Triage and risk screening for COVID-19 exposure and symptoms needs to be undertaken for all women presenting to the health facility, both the primary healthcare clinics and hospitals.
• At any face-to-face contact, all women need to be provided with a facemask.• Women with suspected symptoms of COVID-19 should be directed and treated in
a dedicated treatment area separate from other patients where possible.• Medical staff should be equipped with personal protective equipment (PPEs).
Table1: Clinical presentation of COVID-19 infectionClinical presentation Frequency of
presentationFever 83-99%
• Immunosuppressed patients (e.g. cancer or chronic disease) may present with atypical symptoms as fatigue reduced alertness, reduced mobility, diarrhea, etc. in the absence of fever.
• Symptoms due to physiologic adaptations in pregnant women such as dyspnea, fever, gastrointestinal symptoms and fatigue may overlap with symptoms of COVID - 19. Careful assessment is mandated.
Cough 59-82%Fatigue 44-70%Anorexia 40-84%Shortness of breath 31-40%Myalgia 11-35%Non - specific symptoms
• Sore throat• Nasal congestion• Headache• Diarrhea• Nausea and vomiting• Loss of smell• Loss of taste
• Women suspected for COVID-19 infection include those who have at least one of two:
1. Clinical presentation suggestive of COVID-19 infection.2. History of direct contact with confirmed COVID-19 patient.
• Women with confirmed COVID-19 infection include those who have a positive PCR test in the last 14 days.
• Both groups are combined and managed as one group in this protocol “women with suspected or confirmed COVID-19 infection”.
Preceding the onset of respiratory symptoms
9

2.2 Medical staff considerations• For contact with women with suspected or confirmed COVID-19, a team of
healthcare providers should be in charge based on a pre-set scheduled program, to minimize the number of healthcare providers in contact with COVID-19 patients and to ensure continuity of care.
• The medical team should be:1. Trained in infection control with the attention to infection prevention
practices to be higher during the corona pandemics (how to use PPEs, discard of medical waste, etc.).
2. Trained in screening for COVID-19 symptoms and high risk pregnancy signs.
3. Have sufficient supplies with PPEs.4. Provided with mobile/phone lines.5. Provided with transportation when necessary.
Immediate implementation of appropriate infection prevention measures is an integral part of clinical management of patients per se, and should include:
Instructions to patients
Medical staff should provide the patients with instructions to:
• Wear a facemask. • Keep at least one meter distance between other patients • Disposal of tissues immediately after use. • Perform hand hygiene after contact with respiratory secretions.
Standard infection prevention measures
• All surfaces should be cleaned thoroughly with spray and a clean cloth after any contact by patient or staff.
• Staff should follow regular hand hygiene practices – hand washing before and after examining each patient.
• Use of personal protective equipment (PPE) when in contact with patient’s blood, body fluids, secretions and non-intact skin.
10

Table 2 Recommended type of PPE to be used in the context of COVID-19 according to the setting, personnel and type of activity – WHO recommendation
Setting Target personnel or patients
Activity Type of PPE or procedure
Healthcare facilities
Inpatient facilities Patient room healthcare workers Providing direct care to
COVID 19 patients Medical mask Gown Gloves Eye protection (goggles or face shield)
Aerosol – generating procedures performed on COVID-19 patients
Respirator N95 or FFP2 standard, or equivalentGownGlovesEye protection Apron
Cleaners Entering the room of COVID-19 patients
Medical mask GrownHeavy duty glovesEye protection (if risk of splash from organic material or chemical).Boots or close work shoes
Visitors Entering the room of a COVID-19 patient
Medical mask GrownGloves
Other areas of patient transit (e.g.wards, corridors)
All staff, including healthcare workers
Any activity that does not involve contact with COVID-19 patients
*Medical mask
Triage Healthcare workers Preliminary screening not involving direct contact
Maintain spatial distance of at least 1 m.*Medical mask
Patients with respiratory symptoms
Any Maintain spatial distance of at least 1 m.Wear medical maskProvide medical mask if tolerated by patient
Patients without respiratory symptoms
Any *Medical mask
11
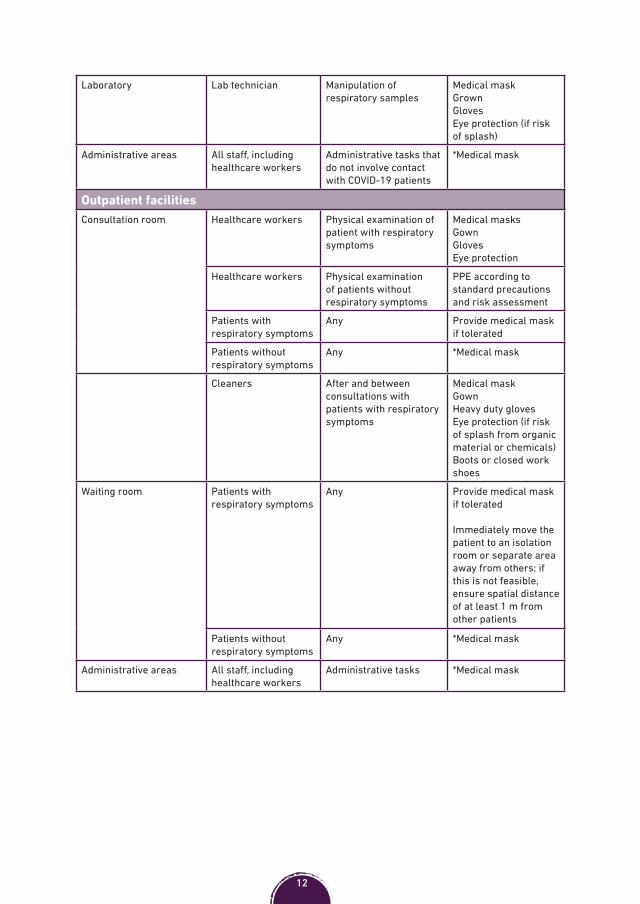
Laboratory Lab technician Manipulation of respiratory samples
Medical mask GrownGlovesEye protection (if risk of splash)
Administrative areas All staff, including healthcare workers
Administrative tasks that do not involve contact with COVID-19 patients
*Medical mask
Outpatient facilities Consultation room Healthcare workers Physical examination of
patient with respiratory symptoms
Medical masksGown Gloves Eye protection
Healthcare workers Physical examination of patients without respiratory symptoms
PPE according to standard precautions and risk assessment
Patients with respiratory symptoms
Any Provide medical mask if tolerated
Patients without respiratory symptoms
Any *Medical mask
Cleaners After and between consultations with patients with respiratory symptoms
Medical mask GownHeavy duty gloves Eye protection (if risk of splash from organic material or chemicals) Boots or closed work shoes
Waiting room Patients with respiratory symptoms
Any Provide medical mask if tolerated
Immediately move the patient to an isolation room or separate area away from others; if this is not feasible, ensure spatial distance of at least 1 m from other patients
Patients without respiratory symptoms
Any *Medical mask
Administrative areas All staff, including healthcare workers
Administrative tasks *Medical mask
12
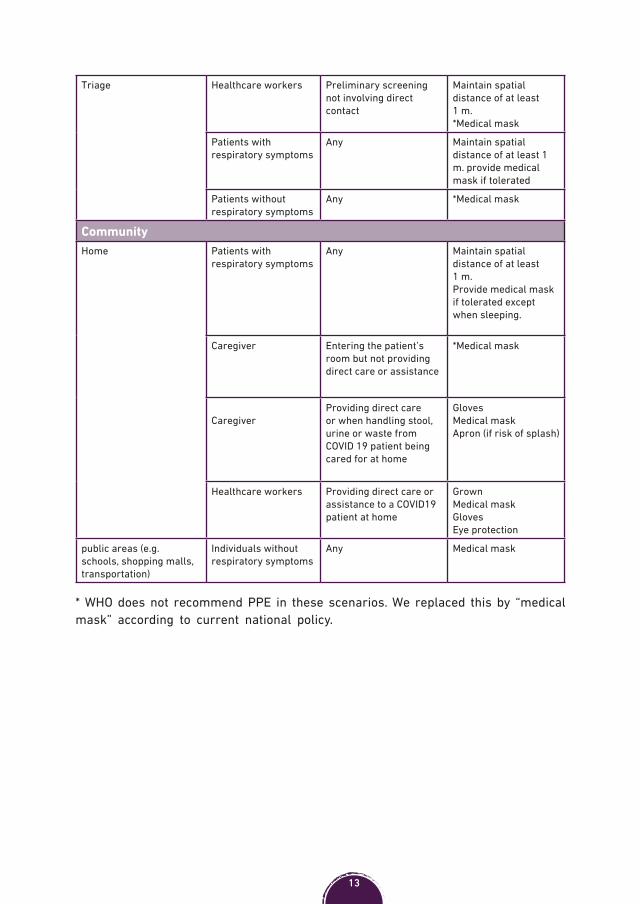
Triage Healthcare workers Preliminary screening not involving direct contact
Maintain spatial distance of at least 1 m. *Medical mask
Patients with respiratory symptoms
Any Maintain spatial distance of at least 1 m. provide medical mask if tolerated
Patients without respiratory symptoms
Any *Medical mask
CommunityHome Patients with
respiratory symptomsAny Maintain spatial
distance of at least 1 m. Provide medical mask if tolerated except when sleeping.
Caregiver Entering the patient’s room but not providing direct care or assistance
*Medical mask
Caregiver Providing direct care or when handling stool, urine or waste from COVID 19 patient being cared for at home
Gloves Medical mask Apron (if risk of splash)
Healthcare workers Providing direct care or assistance to a COVID19 patient at home
GrownMedical mask Gloves Eye protection
public areas (e.g. schools, shopping malls, transportation)
Individuals without respiratory symptoms
Any Medical mask
* WHO does not recommend PPE in these scenarios. We replaced this by “medical mask” according to current national policy.
13

3. ANTENATAL CARE (ANC)
14
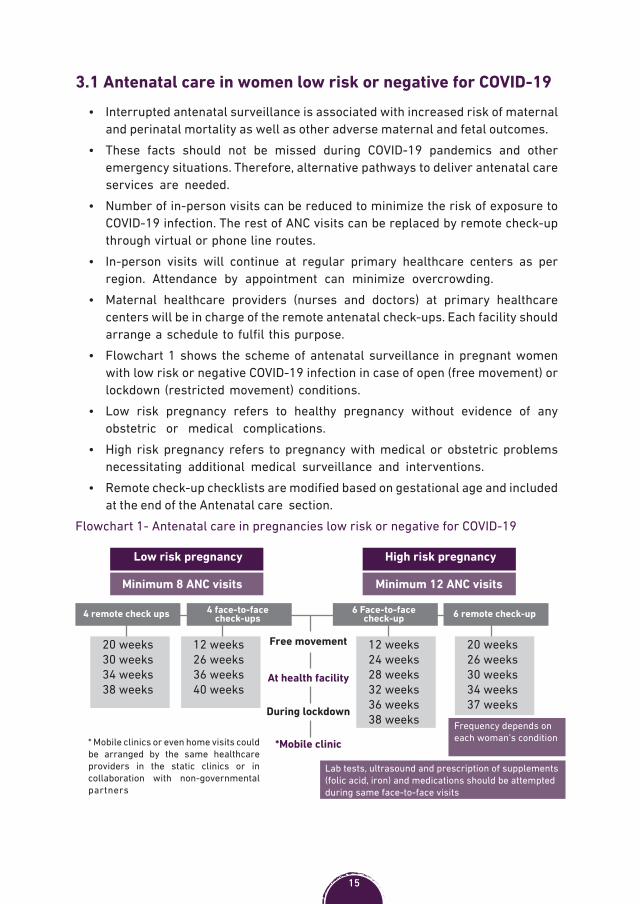
3.1 Antenatal care in women low risk or negative for COVID-19• Interrupted antenatal surveillance is associated with increased risk of maternal
and perinatal mortality as well as other adverse maternal and fetal outcomes. • These facts should not be missed during COVID-19 pandemics and other
emergency situations. Therefore, alternative pathways to deliver antenatal care services are needed.
• Number of in-person visits can be reduced to minimize the risk of exposure to COVID-19 infection. The rest of ANC visits can be replaced by remote check-up through virtual or phone line routes.
• In-person visits will continue at regular primary healthcare centers as per region. Attendance by appointment can minimize overcrowding.
• Maternal healthcare providers (nurses and doctors) at primary healthcare centers will be in charge of the remote antenatal check-ups. Each facility should arrange a schedule to fulfil this purpose.
• Flowchart 1 shows the scheme of antenatal surveillance in pregnant women with low risk or negative COVID-19 infection in case of open (free movement) or lockdown (restricted movement) conditions.
• Low risk pregnancy refers to healthy pregnancy without evidence of any obstetric or medical complications.
• High risk pregnancy refers to pregnancy with medical or obstetric problems necessitating additional medical surveillance and interventions.
• Remote check-up checklists are modified based on gestational age and included at the end of the Antenatal care section.
Flowchart 1- Antenatal care in pregnancies low risk or negative for COVID-19
Low risk pregnancy High risk pregnancy
Minimum 8 ANC visits Minimum 12 ANC visits
4 remote check ups 6 remote check-up4 face-to-face check-ups
6 Face-to-face check-up
20 weeks30 weeks34 weeks38 weeks
12 weeks26 weeks36 weeks40 weeks
20 weeks26 weeks30 weeks34 weeks37 weeks
12 weeks24 weeks28 weeks32 weeks36 weeks38 weeks
* Mobile clinics or even home visits could be arranged by the same healthcare providers in the static clinics or in collaboration with non-governmental partners
Lab tests, ultrasound and prescription of supplements (folic acid, iron) and medications should be attempted during same face-to-face visits
Frequency depends on each woman’s condition
Free movement
At health facility
During lockdown
*Mobile clinic
15

3.2 Antenatal care in women with suspected or confirmed COVID-19
• Pregnant women with suspected or confirmed COVID-19 should continue to receive ANC as appropriate.
• Remote antenatal care surveillance of pregnant women with suspected or confirmed COVID-19 infection through virtual/online or hotline route is recommended to monitor signs of progression of the disease.
• Women with confirmed COVID-19 are excepted to have full recovery of the virus within 4 weeks. Face-to-face/in-person antenatal surveillance is preferably delayed until full recovery or after end of home-quarantine. However, this may be modified based on the condition of each woman.
• For women who have recovered from COVID-19 with no or mild symptoms, without requiring admission to hospital, standard antenatal care should remain unchanged.
• Flowchart 2 shows the scheme of antenatal surveillance in pregnant women with suspected or confirmed COVID-19 infection.
• 10% of pregnancies with moderate-severe disease of COVID-19 might be associated with IUGR due to maternal hypoxia or coagulopathy. Serial ultrasound assessment of fetal growth and amniotic fluid volume should be undertaken after full recovery or after end of home-quarantine
• For women with first- or early second-trimester infection, a detailed fetal morphology scan at 18 to 23 weeks of gestation is indicated
Flowchart 2- Antenatal care in pregnancies with suspected or confirmed COVID-19
Mobile clinic preferable• Restrict movement of COVID-19 patient
to minimize risk of infection spread• Need of transportation• Limited access to appropriate place
• Means of transfer• Coordination with recipient facility
* At least once per week** including labor pain
Low risk pregnancy High risk pregnancy
*Remote regular check-up Remote risk assessment
Handling & transfer of lab tests if indicated Delivery of medications
needed; LMWH, antihypertensives, etc.
Assess need for face-to-face check-up Face-to-face check-
up needed*Remote regular check-up until recovery from COVID-19**Assess need for transfer
16

3.3 Remote antenatal care checklists• Standard antenatal care should continue the same way during face-to-face visits.• Checklists for remote antenatal surveillance are included in this document. The
contents of checklists are modified based on gestational age and can be used for both women with negative or suspected and conformed COVID-19.
• Additional modification to the content of the checklists maybe required according to the condition of each woman. During remote surveillance, women should be provided with the education and information she needs to know about her pregnancy.
Remote Antenatal checklist for women pregnant <20 weeks
<20 weeks
Ask the woman about her general condition How are you feeling today?
Calculate and confirm gestational age with womanAsk how is her pregnancy going on:• Discuss any problems identified in
previous ANC• Discuss any problems in a previous
pregnancy• Review lab. tests if available ( ABO,
Rh, Hb )
• If hypertensive assess BP readings taken by the woman
• If diabetic assess blood sugar measurements taken by the woman
Are you taking any medications (folic acid, iron, others) Does she have enough amount?
Are you having trouble going to the toilet?
Possible UTIConstipation
Assess for possible symptoms of COVID-19 infection Assess for:• Severe abdominal pain• Vaginal bleeding• Severe vomiting
Other danger signs like difficult breathing, dizziness, syncope
Provide emotional/psychological supportExplain when to seek medical helpInclude who and where to seek help?
Confirm she has phone number to contact
Assess if hospital transfer is necessary• Arrange transfer if indicated• Coordinate with recipient hospital
Allow time for questions and answers
Make next appointment
17

Remote Antenatal checklist for women pregnant 20-27 weeks
20-27 weeks
Ask the woman about her general condition How are you feeling today?
Calculate and confirm gestational age with woman
Ask how is her pregnancy going on:• Discuss any problems identified in
previous ANC• Discuss any problems in a previous
pregnancy
• If hypertensive assess BP readings taken by the woman
• If diabetic assess blood sugar measurements taken by the woman
Are you taking any medications (folic acid, iron, others) Does she have enough amount?
Are you having trouble going to the toilet?
Possible UTIConstipation
Ask about fetal movement
Assess for possible symptoms of COVID-19 infection
Assess for danger signs:• Severe abdominal pain• Epigastric pain• Vaginal bleeding• Vomiting• Convulsions• Severe headache• Fast or difficult breathing • Face and Lower limbs edema
Provide emotional/psychological support
Explain when to seek medical helpInclude who and where to seek help?
Confirm she has phone number to contact
Assess if hospital transfer is necessary• Arrange transfer if indicated• Coordinate with recipient hospital
Allow time for questions and answers
Make next appointment
18
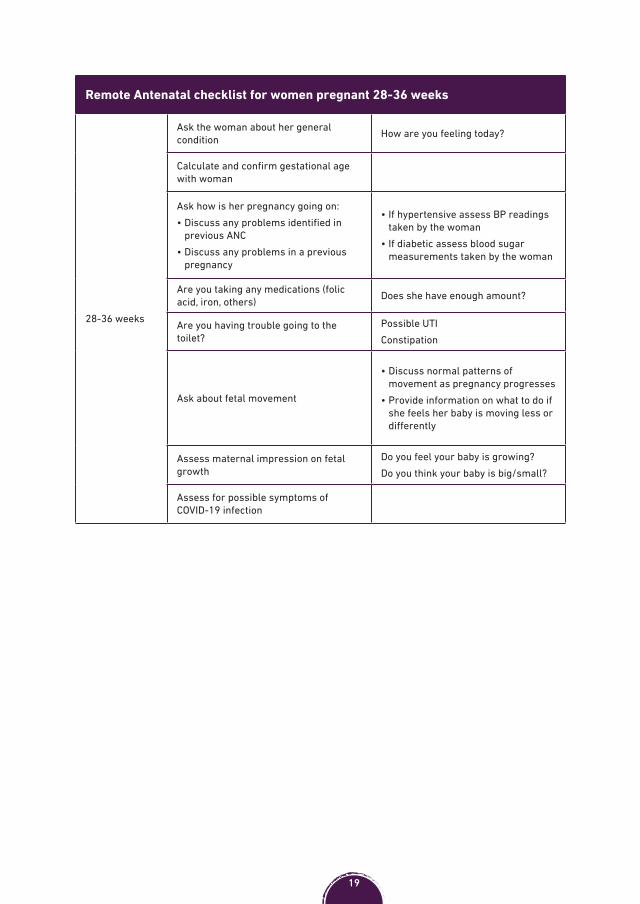
Remote Antenatal checklist for women pregnant 28-36 weeks
28-36 weeks
Ask the woman about her general condition How are you feeling today?
Calculate and confirm gestational age with woman
Ask how is her pregnancy going on:• Discuss any problems identified in
previous ANC• Discuss any problems in a previous
pregnancy
• If hypertensive assess BP readings taken by the woman
• If diabetic assess blood sugar measurements taken by the woman
Are you taking any medications (folic acid, iron, others) Does she have enough amount?
Are you having trouble going to the toilet?
Possible UTIConstipation
Ask about fetal movement
• Discuss normal patterns of movement as pregnancy progresses
• Provide information on what to do if she feels her baby is moving less or differently
Assess maternal impression on fetal growth
Do you feel your baby is growing?Do you think your baby is big/small?
Assess for possible symptoms of COVID-19 infection
19

Remote Antenatal checklist for women pregnant 28-36 weeks (cont.)
Assess for danger signs:• Severe abdominal pain• Gush of fluid from vagina• Epigastric pain• Vaginal bleeding• Vomiting• Convulsions• Severe headache• Fast or difficult breathing• Signs of preeclampsia , signs of
anemia
Provide emotional/psychological support
Explain when to seek medical helpInclude who and where to seek help?
Confirm she has phone number to contact
Assess if hospital transfer is necessary• Arrange transfer if indicated• Coordinate with recipient hospital
Allow time for questions and answersMake next appointment
Remote Antenatal checklist for women pregnant >36 weeks
>36 weeks
Ask the woman about her general condition How are you feeling today?
Calculate and confirm gestational age with womanAsk how is her pregnancy going on:• Discuss any problems identified in
previous ANC• Discuss any problems in a previous
pregnancy
• If hypertensive assess BP readings taken by the woman
• If diabetic assess blood sugar measurements taken by the woman
Are you taking any medications (folic acid, iron, others) Does she have enough amount?
Are you having trouble going to the toilet?
Possible UTIConstipation
Ask about fetal movement
• Discuss normal patterns of movement as pregnancy progresses
• Provide information on what to do if she feels her baby is moving less or differently
Assess maternal impression on fetal growth
Do you feel your baby is growing?Do you think your baby is big/small?
Assess for possible symptoms of COVID-19 infection
20
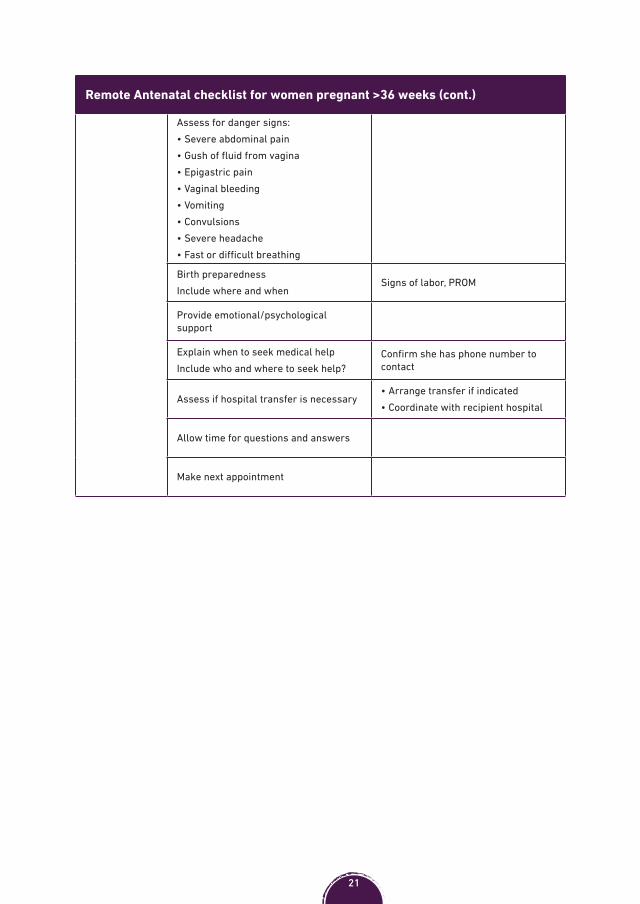
Remote Antenatal checklist for women pregnant >36 weeks (cont.)
Assess for danger signs:• Severe abdominal pain• Gush of fluid from vagina• Epigastric pain• Vaginal bleeding• Vomiting• Convulsions• Severe headache• Fast or difficult breathing
Birth preparednessInclude where and when
Signs of labor, PROM
Provide emotional/psychological support
Explain when to seek medical helpInclude who and where to seek help?
Confirm she has phone number to contact
Assess if hospital transfer is necessary• Arrange transfer if indicated• Coordinate with recipient hospital
Allow time for questions and answers
Make next appointment
21
4. IN-HOSPITAL MANAGEMENT OF COVID-19 DURING PREGNANCY
22

4.1 Indication for admission due to COVID-19 during pregnancy• At least 86 % pregnant patients with suspected or confirmed COVID-19 have mild
disease (no shortness of breath) that does not warrant in-hospital care in the absence of obstetric problems, concern for rapid deterioration, or an inability to promptly reach to the hospital.
• Risk factors that seem to be associated with hospital admission with COVID-19 disease during pregnancy include: 1. Black and Asian2. Obesity 3. Pre-existing comorbidity –particularly diabetes, …..4. Maternal age >35 years 5. Preeclampsia6. IVF7. Twins
• Pregnant women with COVID-19 should be transferred to in-hospital management if they have one of the following:
• Moderate and severe respiratory symptoms.• Mild COVID-19 disease with co-morbidities (e.g. diabetes).• Mild COVID-19 disease with signs of fetal compromise (e.g. decreased fetal
movement).• Women with suspected or confirmed COVID-19 should be admitted to isolated
rooms separate from other uninfected women.• They should wear medical masks during contact with medical staff
1. N95 in pregnancy- These filtering masks are associated with resistance to airflow and increased static dead space volumes, which may affect maternal cardiorespiratory function and fetal oxygenation when worn for prolonged periods. Surgical masks are preferable.
• Medical staff contact with this group should follow the recommended infection control measures (see section 2.2).
• In-hospital management of pregnant COVID-19 patients is multidisciplinary, where internists, pulmonologists, pediatrician and or adult ICU care should be involved.
23

4.2 Investigations for women admitted with COVID-19 during pregnancy
• Pregnant women admitted to hospital due to moderate to severe respiratory symptoms should undergo the following investigations:1. Chest x-ray and CT should be performed when indicated, and not delayed
because of concerns of possible fetal exposure to radiation, as maternal wellbeing is most important.
2. Complete blood count (CBC)- Consider bacterial infection if the white blood cell count is raised. Lymphocytes usually normal or low with COVID-19. Thrombocytopenia can be seen with COVID-19 infection too.
3. Liver function tests- 20-50% patients may demonstrate elevated liver enzymes.
4. Total, direct and indirect serum bilirubin.5. Serum lactate dehydrogenase (LDH).6. Coagulation profile, fibrinogen, D-dimer.7. Kidney function tests.8. Serum electrolytes. 9. Blood cultures/septic work up if secondary bacterial infection is suspected or
in severe and critical disease (see section 4.3).• Consider additional investigations to rule out differential diagnoses – e.g.
electrocardiogram (ECG), CT pulmonary angiogram, echocardiogram, Troponin tests, etc.
• The diagnoses of pulmonary embolism, acute coronary syndrome and heart failure should be ruled out in women with chest pain, worsening hypoxia or a respiratory rate >22 breaths/min (particularly if there is a sudden increase in oxygen requirements), or in women whose breathlessness persists or worsens after expected recovery from COVID-19.
Symptoms of COVID-19 overlap with symptoms of other etiologies. Pyrexia may suggest COVID-19 but other differential diagnosis should be ruled out, e.g. chorioamnionitis, pyelonephritis, etc.
Some COVID-19-related laboratory abnormalities (hemolysis, elevated liver enzyme levels, thrombocytopenia) are the same as those that occur in preeclampsia with severe features and HELLP syndrome. These diagnoses should also be considered and may coexist with COVID-19
24
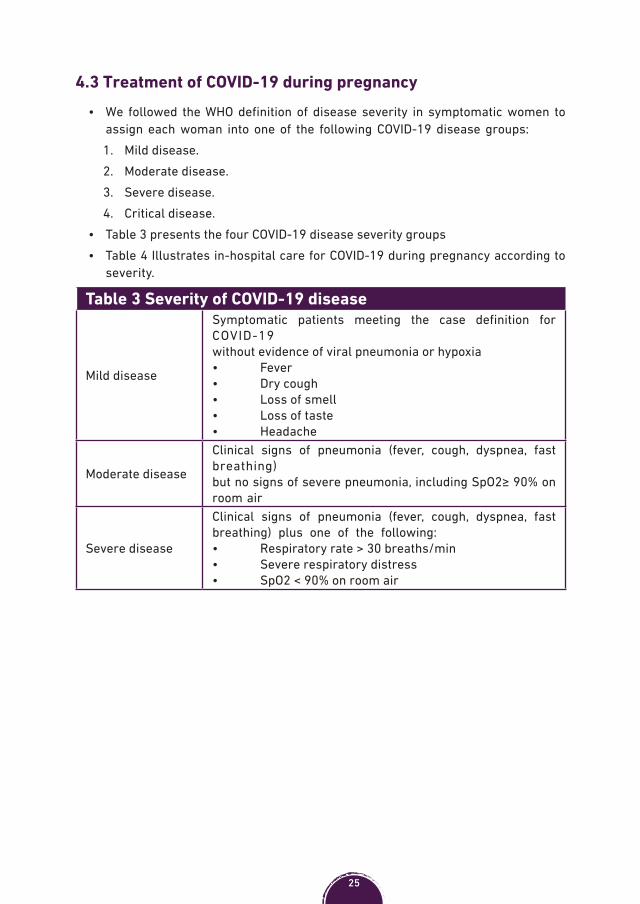
4.3 Treatment of COVID-19 during pregnancy• We followed the WHO definition of disease severity in symptomatic women to
assign each woman into one of the following COVID-19 disease groups:1. Mild disease.2. Moderate disease.3. Severe disease.4. Critical disease.
• Table 3 presents the four COVID-19 disease severity groups• Table 4 Illustrates in-hospital care for COVID-19 during pregnancy according to
severity.
Table 3 Severity of COVID-19 disease
Mild disease
Symptomatic patients meeting the case definition for COVID-19without evidence of viral pneumonia or hypoxia• Fever• Dry cough• Loss of smell• Loss of taste• Headache
Moderate disease
Clinical signs of pneumonia (fever, cough, dyspnea, fast breathing) but no signs of severe pneumonia, including SpO2≥ 90% on room air
Severe disease
Clinical signs of pneumonia (fever, cough, dyspnea, fast breathing) plus one of the following: • Respiratory rate > 30 breaths/min• Severe respiratory distress• SpO2 < 90% on room air
25
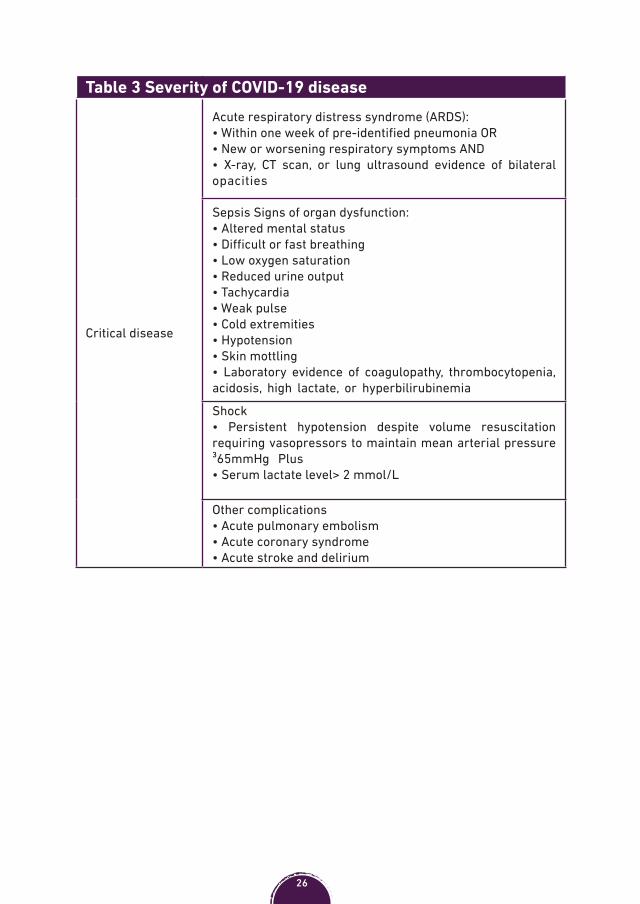
Table 3 Severity of COVID-19 disease
Critical disease
Acute respiratory distress syndrome (ARDS):• Within one week of pre-identified pneumonia OR• New or worsening respiratory symptoms AND• X-ray, CT scan, or lung ultrasound evidence of bilateral opacities
Sepsis Signs of organ dysfunction:• Altered mental status• Difficult or fast breathing • Low oxygen saturation• Reduced urine output • Tachycardia • Weak pulse• Cold extremities• Hypotension • Skin mottling• Laboratory evidence of coagulopathy, thrombocytopenia, acidosis, high lactate, or hyperbilirubinemia
Shock • Persistent hypotension despite volume resuscitation requiring vasopressors to maintain mean arterial pressure ³65mmHg Plus• Serum lactate level> 2 mmol/L
Other complications• Acute pulmonary embolism• Acute coronary syndrome• Acute stroke and delirium
26

Table 4 In-hospital care of COVID-19 disease during pregnancy
Mild disease
This group should be given symptomatic treatment:
• Antipyretics for fever and pain.• Adequate nutrition. • Appropriate rehydration.• Mobilization.• Thromboprophylaxis by low weight molecular heparin
should be initiated (see section 8; Thromboprophylaxis). • Fetal monitoring based on gestational age (e.g. CTG once
per day). • Observation for symptoms and signs of preterm labor.
This group includes women who are admitted due to co-morbidity, obstetric indication or those unable to promptly reach the hospital
Antibiotic therapy or prophylaxis is notrecommended in mild COVID-19 disease
Moderate disease(pneumonia)
• Close monitoring of patients for signs or symptoms of disease progression:
• Vital signs including respiratory rate.• O2 saturation.• Input/output fluid chart.• Symptomatic treatment: • Antipyretics for fever and pain.• Adequate nutrition. • Appropriate rehydration.• SpO2 should be maintained at levels ≥ 94% to avoid fetal
hypoxia. If SpO2<94%, administer supplemental oxygen therapy. Use O2 flow rate by nasal cannula up to 5 L/min; Venturi mask 6–10 L/min; and face mask with reservoir bag 10–15 L/min.
• Escalate urgently if any signs of decompensation develop: • Young, fit women can compensate for a deterioration in
respiratory function and are able to maintain normal oxygen saturations until sudden decompensation.
27

Table 4 In-hospital care of COVID-19 disease during pregnancy
Moderate disease(pneumonia)
• Signs of decompensation include:• An increase in oxygen requirements• An increasing respiratory rate despite oxygen therapy• An acute kidney injury • Drowsiness even if the saturations are normal• SpO2 should be maintained at levels ≥ 94%• Dexamethasone for unwell patient or who need supplementary oxygen:• 24 to 33+6 weeks give the usual doses of dexamethasone (four doses of 6 mg given intramuscularly 12 hours apart) or betamethasone (two doses of 12 mg given intramuscularly 24 hours apart) to induce fetal pulmonary maturation followed by either prednisolone (40 mg orally daily) or hydrocortisone (80 mg intravenously twice daily) for 10 days.• ³ 34 weeks start with prednisolone (40 mg orally daily) or hydrocortisone (80 mg intravenously twice daily) for 10 days.This avoids exposing the fetus to a prolonged course of dexamethasone or betamethasone, which cross the placenta in an active form and may have adverse effects (e.g. preterm birth, long-term neurodevelopmental impairment) • Monitor symptoms and signs of preterm labor.• Fetal well-being should be assessed. The frequency of fetal heart rate observations should be individualized based on gestational age, maternal clinical status (e.g. hypoxia), other maternal co-morbidities and fetal conditions.• In patients with stable SpO2, CTG or fetal heart rate assessment is done once or twice per day.
A systematic review of patients hospitalized with COVID-19 has shown that only 8% were reported as developing bacterial or fungal co-infection during hospital admission. Therefore, antibiotic therapy or prophylaxis is not recommended in moderate COVID-19 disease unless there is clinical suspicion of secondary bacterial infection
28
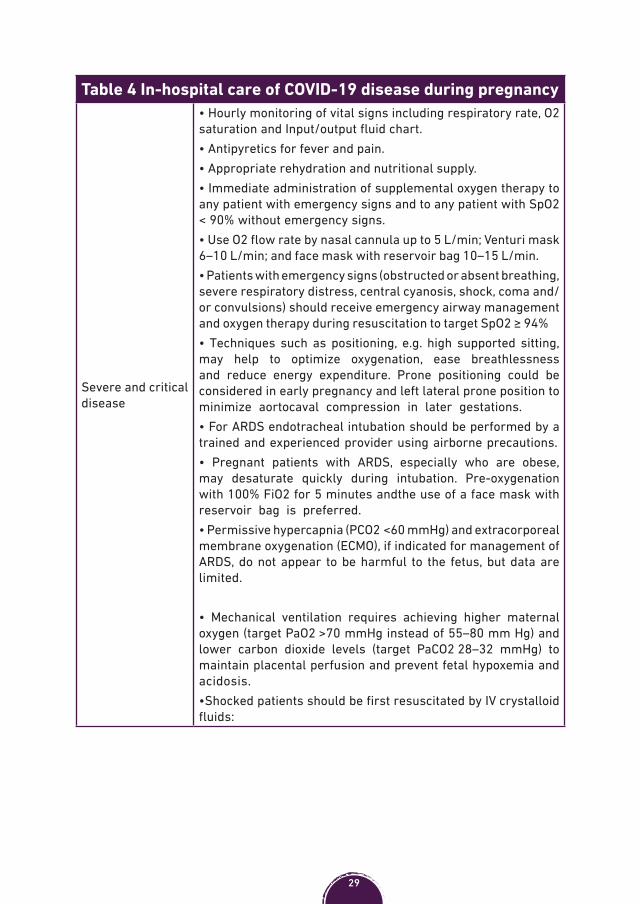
Table 4 In-hospital care of COVID-19 disease during pregnancy
Severe and critical disease
• Hourly monitoring of vital signs including respiratory rate, O2 saturation and Input/output fluid chart.• Antipyretics for fever and pain.• Appropriate rehydration and nutritional supply.• Immediate administration of supplemental oxygen therapy to any patient with emergency signs and to any patient with SpO2 < 90% without emergency signs.• Use O2 flow rate by nasal cannula up to 5 L/min; Venturi mask 6–10 L/min; and face mask with reservoir bag 10–15 L/min. • Patients with emergency signs (obstructed or absent breathing, severe respiratory distress, central cyanosis, shock, coma and/or convulsions) should receive emergency airway management and oxygen therapy during resuscitation to target SpO2 ≥ 94%• Techniques such as positioning, e.g. high supported sitting, may help to optimize oxygenation, ease breathlessness and reduce energy expenditure. Prone positioning could be considered in early pregnancy and left lateral prone position to minimize aortocaval compression in later gestations.• For ARDS endotracheal intubation should be performed by a trained and experienced provider using airborne precautions.• Pregnant patients with ARDS, especially who are obese, may desaturate quickly during intubation. Pre-oxygenation with 100% FiO2 for 5 minutes andthe use of a face mask with reservoir bag is preferred.• Permissive hypercapnia (PCO2 <60 mmHg) and extracorporeal membrane oxygenation (ECMO), if indicated for management of ARDS, do not appear to be harmful to the fetus, but data are limited.
• Mechanical ventilation requires achieving higher maternal oxygen (target PaO2 >70 mmHg instead of 55–80 mm Hg) and lower carbon dioxide levels (target PaCO2 28–32 mmHg) to maintain placental perfusion and prevent fetal hypoxemia and acidosis.•Shocked patients should be first resuscitated by IV crystalloid fluids:
29

Table 4 In-hospital care of COVID-19 disease during pregnancy• Starches are associated with an increased risk of death and acute kidney injury compared with crystalloids. • Hypotonic (vs. isotonic) solutions are less effective at increasing intravascular volume.• Administer vasopressors when shock persists during or after fluid resuscitation. The initial blood pressure target is MAP ≥ 65 mmHg in adults and improvement of markers of perfusion.• Thromboprophylaxis by low weight molecular heparin.• Dexamethasone for unwell patient or who need supplementary oxygen:• 24 to 33+6 weeks give the usual doses of dexamethasone (four doses of 6 mg given IM 12 hours apart) or betamethasone (two doses of 12 mg given IM 24 hours apart) to induce fetal pulmonary maturation followed by prednisolone (40 mg orally daily) if oral intake is possible or hydrocortisone (80 mg IV twice daily) for 10 days.• ³ 34 weeks start with hydrocortisone (80 mg IV twice daily) for 10 days or until discharge.• Administer empiric antibiotic treatment, after obtaining blood culture, for 5-7 days.• After resuscitation and stabilization of the woman, fetal well-being should be monitored. The frequency of fetal heart rate observations should be individualized based on gestational age, maternal clinical status and fetal conditions. Continuous CTG maybe considered if SpO2 is unstable.
30

Experimental pharmacological treatment for moderate and severe COVID-19 disease
Hydroxychloroquine or chloroquine
• Although earlier studies in China showed benefit, data from randomized trials suggest no benefit from administration of hydroxychloroquine or chloroquine. Adverse maternal effects include systolic hypotension, which may exacerbate the aortocaval compression effect and abnormal heart rhythms (QT interval prolongation and ventricular tachycardia), especially in patients taking other drugs associated with QTc prolongation.
• Hydroxychloroquine crosses the placenta but potential fetal risk has not been observed in humans. Available data are limited, however, and a risk to the fetus cannot be ruled out when used at different doses for other indications.
• Chloroquine is a drug with a large volume of distribution, and pharmacokinetic studies have shown significantly lower plasma drug concentrations in pregnancy, which suggests the need for a higher dose in COVID-19 (at least 500 mg twice daily).
Antiviral drugs
• Several agents are being evaluated for treatment of COVID-19 so their use for COVID-19 remains investigational.
• Antiproteases (Lopinavir/Ritonavir) were reported to be safe; however, therapeutic efficacy and safety of Remdesivir still lack evidence.
• Ribavirin and Favipiravir have teratogenic effects, but there are some debates on the use of ribavirin in severe cases.
31

5. LABOR AND DELIVERY IN WOMEN WITH SUSPECTED OR CONFIRMED COVID-19
32
Clinical practice in labor and delivery of pregnant women who are low risk or negative for COVID-19 should remain the same and is determined by the usual obstetric guidelines (Available; Obstetric Guidelines and Labor Ward protocols, Fourth edition, 2016).
5.1 Preterm labor in women with suspected or confirmed COVID-19
• For most women with preterm labor at <34 weeks and non-severe COVID-19 disease who have no medical or obstetric indications for prompt delivery, tocolysis can be safely used to allow administration of corticosteroids for fetal lung maturity or in-utero transfer to a hospital with NICU. Nifedipine is currently the tocolytic agent of choice due to its minor side effects. Beta-sympathomimetics, should be avoided as they can further increase the maternal heart rate.
• For most women with PPROM and non-severe illness who have no medical or obstetric indications for prompt delivery, can be managed by usual protocols for PPROM.
• Women with severe- critical disease may need to be delivered prematurely. Please see section 5.2 “Timing of delivery”.
5.2 Timing of deliveryMild-moderate disease
• For most women <37 weeks and with non-severe COVID-19 disease who have no medical or obstetric indications for prompt delivery, delivery is not indicated and ideally will occur sometime after a negative testing result is obtained or isolation status is lifted, thereby minimizing the risk of postnatal transmission to the neonate.
• For most women <37 weeks and with non-severe COVID-19 disease who also have medical or obstetric complications (e.g. PPROM, preeclampsia), the timing of delivery is determined by usual protocols for the specific medical and obstetric complications.
• For women at term who are in home-isolation with COVID-19, individualized assessments to consider delaying elective birth (elective CS or IOL) taking into account the urgency of the birth and the risk of infectious transmission to other women, medical staff and, postnatally, to her baby. In general, good obstetric practice should continue the same, and urgent delivery should not be delayed.
Severe-critical disease
• For women with severe COVID-19 disease, timing of delivery needs to be individualized taking into account: 1. Whether the mother’s respiratory disease be improved or exacerbated by
delivery.
33
2. The risk of postnatal transmission in the delivery room when maternal symptoms are acute.
3. Increased oxygen consumption and reduced functional residual capacity, which are normal in pregnancy, may facilitate maternal deterioration in patients with pneumonia.
4. Excessive uterine distension from multiple gestation or severe polyhydramnios in the third trimester may further compromise pulmonary function.
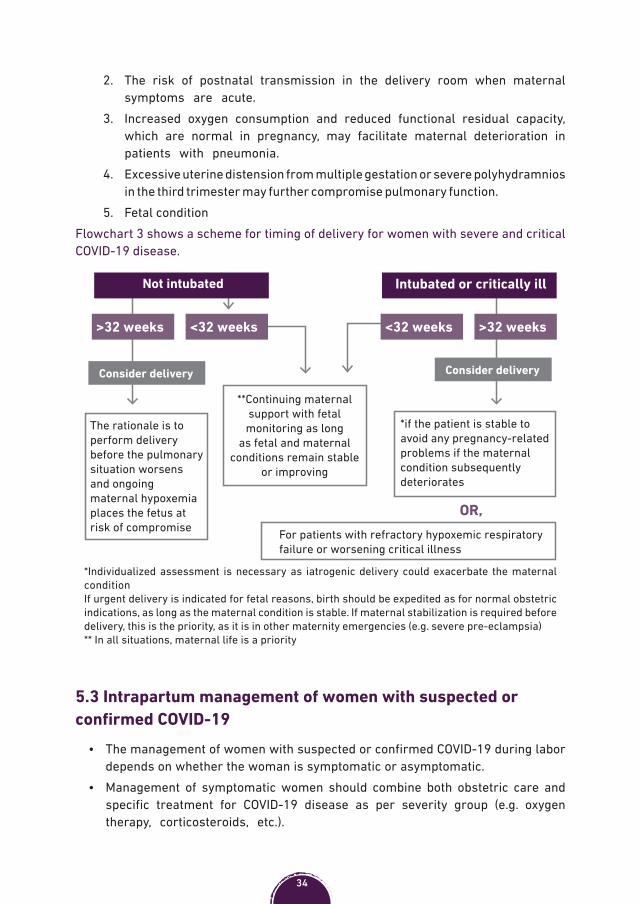
5. Fetal conditionFlowchart 3 shows a scheme for timing of delivery for women with severe and critical COVID-19 disease.
*Individualized assessment is necessary as iatrogenic delivery could exacerbate the maternal conditionIf urgent delivery is indicated for fetal reasons, birth should be expedited as for normal obstetric indications, as long as the maternal condition is stable. If maternal stabilization is required before delivery, this is the priority, as it is in other maternity emergencies (e.g. severe pre-eclampsia)** In all situations, maternal life is a priority
Not intubated Intubated or critically ill
>32 weeks<32 weeks <32 weeks>32 weeks
**Continuing maternal support with fetal monitoring as long
as fetal and maternal conditions remain stable
or improving
The rationale is to perform delivery before the pulmonary situation worsens and ongoing maternal hypoxemia places the fetus at risk of compromise
*if the patient is stable to avoid any pregnancy-related problems if the maternal condition subsequently deteriorates
For patients with refractory hypoxemic respiratory failure or worsening critical illness
Consider delivery Consider delivery
OR,
5.3 Intrapartum management of women with suspected or confirmed COVID-19
• The management of women with suspected or confirmed COVID-19 during labor depends on whether the woman is symptomatic or asymptomatic.
• Management of symptomatic women should combine both obstetric care and specific treatment for COVID-19 disease as per severity group (e.g. oxygen therapy, corticosteroids, etc.).
34

• Assessment of the severity of COVID-19 symptoms should be undertaken by the most senior available clinician.
• There is no evidence that delaying cord clamping increases the possibility of viral transmission from the mother to the newborn. The proven benefits of a 1–3 minute delay in clamping the cord outweigh the theoretical, and unproven, harms.
Flowchart 4 illustrates the management approach of women with suspected or confirmed COVID-19 during labor and delivery.
• **Maternal observations including temperature, respiratory rate, oxygen saturation and fluid input/output charts hourly.
• Aim at PsO2>94%• Continuous CTG• Efforts should be targeted towards
achieving neutral fluid balance in labor
• Try boluses in volumes of 250–500 ml and then assess for fluid overload before proceeding with further fluid resuscitation
• Cesarean delivery is performed only for obstetric indications unless symptoms are severe, the patient is hypoxic and exhausted and delivery is not soon expected
• If the patient is unwell and and delivery is soon expected, consider assisted vaginal delivery for shortening of second stage of labor
• Epidural and spinal analgesia are and accepted and preferable than general anesthesia
Ideally, there should be available consultant obstetrician, consultant anesthesiologist, midwife, consultant neonatologist and neonatal nurse
Asymptomatic Symptomatic
Management as per usual labor protocol
*Assess severity of COVID-19 disease and manage accordingly
(section 4.3; Treatment of COVID-19 during pregnancy)
Continuous CTG is not recommended, unless indicated for another reason
*Refer to WHO COVID-19 severity group (section 4.3 Treatment of COVID-19 during pregnancy ** This includes relevant investigations (see section 4.2 Investigations for COVID-19 during pregnancy
Efforts should be made to minimize the number of staff members entering the room
5.4 Immediate postpartum care for women with suspected or confirmed COVID-19
• will depend on maternal condition and severity of COVID-19 disease.• Patients should be monitored for progression of COVID-19 disease in the first 24
hours.• Adequate hydration, thromboprophylaxis and postpartum follow-up plan should
be provided.• Early discharge for women low risk or negative COVID-19 should be considered.• For women with moderate-severe COVID-19 disease, treatment plan should
be continued as per protocol (see section 4.3 “Treatment of COVID-19 during pregnancy”).
35

6. NEWBORNS AND BREAST FEEDING
36
• A designated senior member of the neonatal team should be assigned to attend suspected or confirmed COVID-19 deliveries. It is important that the most senior person likely to be required attends in the first instance, to minimize staff exposure. If it is anticipated that the baby will require respiratory support, the neonatal team members should be present at delivery and wearing PPE.
• Neonatal resuscitation/stabilization should proceed as per current guidance.• If necessary, neonates should be transferred in a closed incubator. Where possible, all
procedures and investigations should be carried out in the single room with a minimal number of staff present.
• In general, risks and benefits discussion with neonatologists and families is recommended to individualize care in babies who may be more susceptible to COVID-19 infection.
• All babies of suspected or confirmed COVID-19 positive mothers need to be tested for COVID- 19 and kept in isolation with the mother, where possible, until the test result is received. The newborn should be tested at day 0, if negative the PCR should be repeated within 72-120 hours.
• Women with COVID-19 and their healthy babies, who do not require maternal critical care or neonatal care, should be kept together in the immediate postpartum period.
• The risk of separating the mother and baby to reduce infection transmission, and potentially mild COVID-19 disease in the baby, may considerably outweigh the benefits of keeping mothers and babies together given the evidence supporting immediate skin to skin contact and early initiation of breastfeeding for thermal regulation, prevention of hypoglycemia and reduced sepsis and death in infants.
• The few neonatal infections that have been reported were acquired in the postnatal period and the infants were not significantly unwell. Fetal distress and early neonatal complications when present, were considered due to maternal illness or prematurity. Newborns born prematurely or sick may require additional medical support in the health facility. but they still have the right to access his or her mother or parent. No mother should be separated from her baby without her informed consent.
• Breast milk from mothers with COVID-19 infection has been shown to be negative for COVID-19 so breastfeeding is not contraindicated. Healthcare providers need to support the mother’s intention to breastfeed and where a woman is unwell, provide support for the woman to express breast milk and feed this to her baby and parents should be informed that infection with COVID-19 is not a contraindication to breastfeeding. If the mother wants to pump, use a personal pump rather than a hospital pump.
• The following precautions should be taken to limit viral spread to the baby:1. Wash hands before touching the baby, breast pump or bottles.2. Avoid coughing or sneezing on the baby while feeding.3. Wear face covering or fluid-resistant face mask while feeding or caring for the baby. 4. Considering asking someone who is well to feed the baby.
Babies should not wear masks or other face coverings, as they may risk suffocation
37
7. POSTNATAL CARE AND FAMILY PLANNING
38

7.1 Remote postnatal checklist• Postnatal follow up and family planning services should be continued for
all women, regardless of COVID-19 status, to minimize risk of postpartum complications and unintended pregnancies.
• Flowcharts 5 and 6 show postnatal pathway for women low risk or negative for COVID-19 during free movement and lockdown, respectively.
• Flowchart 7 shows postnatal pathway for women with suspected or confirmed COVID-19.
• Remote postnatal care checklists are included.Flowchart 5- Postnatal care in pregnancies low risk or negative for COVID-19 Free movement
Contraception • Women should be encouraged to seek family planning on time• Provide adequate amount (double the amount) of contraception
Post low risk pregnancy Post high risk pregnancy
*Risk assessment Risk assessment
Remote check upsFace-to-face
check-upsAt least one face-to-face check-up
Remote regular check-up
* Risk assessment for both postpartum complications and signs of progression of COVID-19 disease
Flowchart 6- Postnatal care in pregnancies low risk or negative for COVID-19 Lockdown
Contraception • Consider distribution of barrier- and/or progesterone-minipill contraceptive methods
at birth facility• Combined oral pills should be avoided in the immediate postpartum period due to the
risk of thromboembolism and effect on breast feeding• Deliver adequate amount of contraception through mobile clinic
Post low risk pregnancy Post high risk pregnancy
Risk assessment Risk assessment
Remote check upsFace-to-face
check-ups
Mobile Clinic
At least one face-to-face check-up
Remote regular check-up
* Risk assessment for both postpartum complications and signs of progression of COVID-19 disease
39

Flowchart 7- Postnatal care in pregnancies with suspected or confirmed COVID-19
Contraception• Consider distribution of barrier or progesterone-minipill contraception at birth facility• Combined oral pills should be avoided in the immediate postpartum period due to risk of
thromboembolism and effect on breast feeding• Deliver adequate amount of contraception through mobile clinic• Consider & inform women to seek contraception after recovery from COVID-19
Post high risk pregnancy
Remote assessment
Need face-to-face check-up?
• Means of transfer• Coordination with recipient facility
* At least once per week
*Remote regular check-up until recovery from COVID-19
Mobile clinic preferable• Limited access to appropriate place• Restrict movement of patients to minimize
risk of infection spread• Need of transportation
Post low risk pregnancy
Remote regular check-up until recovery from COVID-19
Assess need for face-to-face check-up
Assess need for transfer
YesYes No
Remote Postnatal care checklist
Ask the woman about her general condition• Amount of lochia• Emphasize adequate hydration, nutrition and
mobilization
How are you feeling today?
• Ask her on breast feeding• Handling of her baby if she has COVID-19• Does she wear a mask during caring for baby• Does she attend to hand washing
• Amount, frequency, any problems, pain, redness, fissured nipples, swelling, infection?
• Discuss any problems identified during pregnancy, labor and delivery
• If hypertensive assess BP readings taken by the woman
• If diabetic assess blood sugar measurements taken by the woman
Is she taking any medications• Dose adjustment if necessary
Does she have enough amount?
Are you having trouble going to the toilet?
Possible UTIConstipation
40
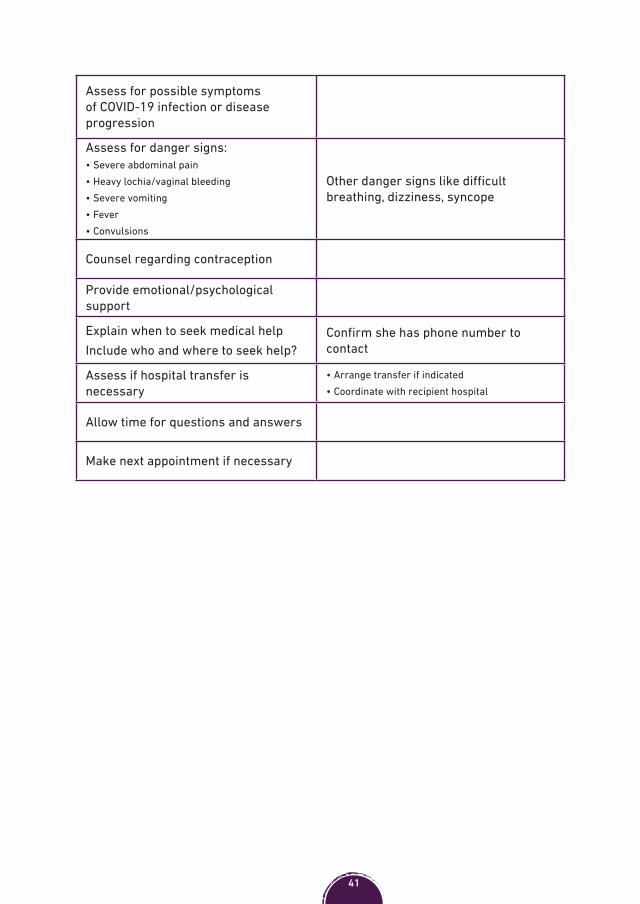
Assess for possible symptoms of COVID-19 infection or disease progression
Assess for danger signs:• Severe abdominal pain• Heavy lochia/vaginal bleeding• Severe vomiting• Fever• Convulsions
Other danger signs like difficult breathing, dizziness, syncope
Counsel regarding contraception
Provide emotional/psychological support
Explain when to seek medical helpInclude who and where to seek help?
Confirm she has phone number to contact
Assess if hospital transfer is necessary
• Arrange transfer if indicated• Coordinate with recipient hospital
Allow time for questions and answers
Make next appointment if necessary
41
8. THROMBOPROPHYLAXIS
42

8.1 Thromboprophylaxis• Direct data on thromboembolic risk with COVID-19 are limited but suggest an
increased risk.• Thromboprophylaxis by low molecular weight heparin (LMWH) should
be commenced for pregnant women who are self-isolating and should be continued until they have recovered from the acute illness (between 7 and 14 days).
• Similarly, hospitalized pregnant women with confirmed or suspected COVID-19 should receive thromboprophylaxis by LMWH for the duration of their admission unless there is a contraindication (e.g. bleeding, severe thrombocytopenia) or birth is expected within 12 hours.
• For antepartum prophylaxis in women who are not severely or critically ill and who may deliver within a few days, unfractionated heparin 5000 units subcutaneously every 12 hours maybe alternatively used.
• All pregnant women who have been hospitalized and have had confirmed COVID-19 should receive thromboprophylaxis for 10 days following hospital discharge. For women with persistent morbidity, consider a longer duration of thromboprophylaxis.
• If women are admitted with confirmed or suspected COVID-19 within 6 weeks postpartum, they should receive thromboprophylaxis for the duration of their admission and for at least 10 days post discharge. Consider extending this until 6 weeks postpartum for women with significant ongoing morbidity.
With the emerging evidence that COVID-10 patients are at increased risk of thromboembolism and as pregnancy is hypercoagulable state per se, justifies the administration of thromboprophylaxis for pregnant women with suspected or confirmed COVID-19
43

References• COVID-19 Technical Brief Package for Maternity Services. United Nations Population
Fund (UNFPA);2020 May. Available online at https://www.unfpa.org/resources/covid-19-technical-brief-maternity-services.
• Coronavirus (COVID-19) Infection in pregnancy. Royal College of Obstetricians & Gynaecologists and The Royal College Of Midwives; June 2020. Available online at https://www.rcog.org.uk/globalassets/documents/guidelines/2020-06-18-coronavirus-covid-19-infection-in-pregnancy.pdf.
• COVID-19 - guidance for paediatric services. Royal College of Peadiatrics and Child Health; March 2020. Available at https://www.rcpch.ac.uk/resources/covid-19-guidance-paediatric-services.pdf.
• Coronavirus Disease 2019 (COVID-19) Pandemic and Pregnancy. Dashraath P, Jeslyn Wong J, Karen Lim M, et al. Am J Obstet Gynecol. 2020 Jun;222(6):521-531. doi: 10.1016/j.ajog.2020.03.021.
• Romeo R, Penelop S, Margaret CS, et al. Severe Coronavirus Infection in Pregnancy. A systematic review. American College of Obstetricians and Gynecologists; 2020.
• Clinical management of COVID-19. Interim guidance. World Health Organization (WHO); 2020 May. Available online at https://www.who.int/publications/i/item/clinical-management-of-covid-19.
44