COVER STORY Survey of Accommodating IOL...
19
OCTOBER 2010 CATARACT & REFRACTIVE SURGERY TODAY EUROPE 53 W ith the push toward refractive cataract surgery, presbyopia-correcting IOLs are steadily gaining popularity, both with surgeons who are implanting them and with patients who are asking for them. An abundance of multifocal and accommodating IOLs are currently available, and there are more models on the horizon. One area of intense focus is the search for a truly accommodative lens technology. For now, several pseudoaccom- modating lenses are either currently available or in the pipeline. The following questions were sent to a panel of anterior segment surgeons who have experience implanting accommodating IOLs. 1. Do you have any experience with this lens, either in practice or in clinical testing? If so, how many have you implanted? 2. Whether or not you have personal experience with this lens, what is your impression of its mechanism of accommodation? Why does it work, or what in its current design limits it from working? 3. What are the advantages of the lens design? The disadvantages? 4. Who is the ideal candidate for this lens? What tips do you have for implanting this lens or optimizing postoperative visual acuity? 5. What is your opinion on the future of this lens technology? This survey is intended to offer a sampling of thoughts on eight accommodating IOL technologies: the Akkommodative 1CU (HumanOptics AG, Erlangen, Germany), the Crystalens AO (Bausch + Lomb, Rochester, New York), the FluidVision (PowerVision, Inc., Belmont, California), the NuLens DynaCurve (NuLens, Ltd., Herzliya Pituach, Israel), the SmartIOL (Medennium, Inc., Irvine, California), the Synchrony (Abbott Medical Optics Inc., Santa Ana, California), the Tek-Clear (Tekia, Inc., Irvine, California), and the Tetraflex (Lenstec, St. Petersburg, Florida). Vision Solutions Technologies (Rockville, Maryland) asked that its LiquiLens not be featured in this survey. Some responses contain forward-looking thoughts and are not necessarily intended to provide clinical infor- mation. In some cases, the participant did not respond about a particular lens, and therefore that set of questions was left out. VICTOR BOHÓRQUEZ, MD I am currently the Chief of Ophthalmology at Saludcoop EPS – Servioftalmos, in Bogota, Colombia. I have been implanting accommodating IOLs for the past 6 years, and most of my experience has been in clinical research trials with the Synchrony dual-optic IOL (Visiogen Inc.; now Abbott Medical Optics Inc., Santa Ana, California). I have also started implanting the Crystalens HD (Bausch + Lomb, Rochester, New York) this past year. My experience is based on these two accommodating IOLs. Currently, I implant accommodating lenses in approxi- mately 10% of cataract patients. This percentage is increas- ing fairly quickly and will rapidly outgrow my percentage of Survey of Accommodating IOL Technologies A panel of anterior segment surgeons provides answers to five questions. BY VICTOR BOHÓRQUEZ, MD; SHERAZ M. DAYA, MD, FACP, FACS, FRCS(ED), FRCOPHTH; ROBERT K. MALONEY, MD; SAMUEL MASKET, MD; MARK PACKER, MD, FACS; MAGDA RAU, MD; AND SUNIL SHAH, FRCOPHTH, FRCS(E D), FBCLA COVER STORY
Transcript of COVER STORY Survey of Accommodating IOL...

OCTOBER 2010 CATARACT & REFRACTIVE SURGERY TODAY EUROPE 53
With the push toward refractive cataract surgery, presbyopia-correcting IOLs are steadily gaining popularity,
both with surgeons who are implanting them and with patients who are asking for them. An abundance of
multifocal and accommodating IOLs are currently available, and there are more models on the horizon. One
area of intense focus is the search for a truly accommodative lens technology. For now, several pseudoaccom-
modating lenses are either currently available or in the pipeline. The following questions were sent to a panel of anterior
segment surgeons who have experience implanting accommodating IOLs.
1. Do you have any experience with this lens, either in practice or in clinical testing? If so, how many have you
implanted?
2. Whether or not you have personal experience with this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current design limits it from working?
3. What are the advantages of the lens design? The disadvantages?
4. Who is the ideal candidate for this lens? What tips do you have for implanting this lens or optimizing
postoperative visual acuity?
5. What is your opinion on the future of this lens technology?
This survey is intended to offer a sampling of thoughts on eight accommodating IOL technologies: the Akkommodative 1CU
(HumanOptics AG, Erlangen, Germany), the Crystalens AO (Bausch + Lomb, Rochester, New York), the FluidVision (PowerVision,
Inc., Belmont, California), the NuLens DynaCurve (NuLens, Ltd., Herzliya Pituach, Israel), the SmartIOL (Medennium, Inc., Irvine,
California), the Synchrony (Abbott Medical Optics Inc., Santa Ana, California), the Tek-Clear (Tekia, Inc., Irvine, California), and the
Tetraflex (Lenstec, St. Petersburg, Florida). Vision Solutions Technologies (Rockville, Maryland) asked that its LiquiLens not be
featured in this survey. Some responses contain forward-looking thoughts and are not necessarily intended to provide clinical infor-
mation. In some cases, the participant did not respond about a particular lens, and therefore that set of questions was left out.
VICTOR BOHÓRQUEZ,MD
I am currently the Chief of Ophthalmology at
Saludcoop EPS – Servioftalmos, in Bogota,
Colombia. I have been implanting accommodating IOLs for
the past 6 years, and most of my experience has been in
clinical research trials with the Synchrony dual-optic IOL
(Visiogen Inc.; now Abbott Medical Optics Inc., Santa Ana,
California). I have also started implanting the Crystalens HD
(Bausch + Lomb, Rochester, New York) this past year. My
experience is based on these two accommodating IOLs.
Currently, I implant accommodating lenses in approxi-
mately 10% of cataract patients. This percentage is increas-
ing fairly quickly and will rapidly outgrow my percentage of
Survey ofAccommodating IOL
TechnologiesA panel of anterior segment surgeons provides answers to five questions.
BY VICTOR BOHÓRQUEZ, MD; SHERAZ M. DAYA, MD, FACP, FACS, FRCS(ED), FRCOPHTH;
ROBERT K. MALONEY, MD; SAMUEL MASKET, MD; MARK PACKER, MD, FACS;
MAGDA RAU, MD; AND SUNIL SHAH, FRCOPHTH, FRCS(ED), FBCLA
COVER STORY

multifocal IOL patients. I prefer implanting accommodating
lenses in younger patients because I believe it is a better way
to restore natural physiological accommodation and pro-
vide good quality of vision at all distances. Multifocal IOLs
split incoming light rays into two or more focal points, thus
producing uncomfortable photic phenomena.
It is important to mention that there is still no specific
IOL that fulfills all needs for all patients. It is ultimately up to
the surgeon to carefully select the correct IOL for the
patient’s individual lifestyle. The challenge for current and
future accommodating IOL technologies is to prevent fibro-
sis and maintain capsular clarity. A functioning capsule is
essential for the accommodative mechanism to work prop-
erly. As imaging technologies advance, so will IOL design.
When accurate capsular bag and ciliary muscle strength
measurements are finally possible, custom-designed IOLs
will become reality.
AKKOMMODATIVE 1CU 1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
Even though I do not have personal experience with this
lens, it has been on my radar for a while because it was one
of the first accommodating lenses available in the world.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
The lens has four flexible haptics, which should allow
back-and-forth movement; however, published data from
several nonrandomized and randomized controlled clinical
trials show limited objective accommodative effect.1-4
3. What are the advantages of the lens design? The dis-
advantages?
Capsular fibrosis seems to be a problem, with high
Nd:YAG rates. There are also reports of haptics bent inward,
toward the rhexis edge.
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
CRYSTALENS AO 1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I do not have experience with the new version of the
Crystalens, the AO, but I have implanted more than 60 eyes
with the Crystalens HD.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
I cannot speak for the Crystalens AO. In terms of the HD,
it incorporates a small magnitude of negative spherical aber-
ration within the central 1.5-mm diameter region of the 5.0-
mm optic. This negative spherical aberration is expected to
improve intermediate and near vision by increasing the
depth of focus. The mechanism of action of this lens
remains unproven.
3. What are the advantages of the lens design? The dis-
advantages?
[No answer provided.]
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
Most of my HD patients are satisfied, and the lens fulfills
most of their needs. These cataract patients accept the possi-
bilities of needing reading glasses for small print and of
decreases in contrast sensitivity. The HD lens is a good option
for patients who are worried about glare and halos and will
accept low-powered glasses for reading. I tend to target mini-
monovision with 0.25 D in the dominant eye and -0.25 D in
the fellow eye, as recommended by Bausch + Lomb.
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
FLUIDVISION1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no experience implanting this IOL.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
My understanding is that this IOL works by moving
fluid from the haptics into a bladder in the center of
the lens. This movement alters the anterior radius of
curvature and shifts the lens forward.
54 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY

The design could be limited by the development of cap-
sular fibrosis. In case of capsular fibrosis, more fluid would
be needed to produce a greater magnitude of accommoda-
tion, or, even worse, the lens could get stuck at a single focal
point, resulting in large refractive errors.
3. What are the advantages of the lens design? The dis-
advantages?
[No answer provided.]
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
NULENS DYNACURVE1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
I understand that the flexible polymer, located between
two rigid plates, moves posteriorly with accommodative
effort to decrease the power of the eye (contrary to human
accommodation, which increases the power of the eye to
see near objects clearly).
3. What are the advantages of the lens design? The dis-
advantages?
It may be awkward to ask patients to learn to see near
objects by disaccommodation and to do activities like driv-
ing or watching a movie by forcing accommodation.
Another issue with this lens is that it must be placed in the
ciliary sulcus; it is a big lens that may cause iris chafing with
resulting inflammation and/or pigmentary dispersion.
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
SYNCHRONY 1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have implanted the Synchrony in more than 300 eyes.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
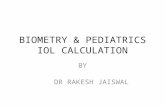
The rear optic of this one-piece, dual-optic accommodat-
ing IOL is a minus lens, with a power chosen to produce the
desired overall net IOL power in the patient’s eye. The front
optic, which is mobile, is always 32.00 D, which inherently
provides more accommodation per unit of movement
compared with single-optic designs (Figure 1). Also, the
Synchrony provides consistent accommodative amplitude
regardless of lens power.
Our group has been able to show, utilizing several objec-
tive techniques including ultrasound biomicroscopy and
iTrace wavefront aberrometry (Tracey Technologies, Corp.,
Houston), that the lens works according to the Helmholtz
theory of accommodation. With accommodation (near
stimulus), the ciliary body contracts, releasing zonular and
capsular bag tension and allowing forward movement of
the anterior optic of the IOL. This results in an increase in
the power of the eye (ie, myopization).
3. What are the advantages of the lens design? The dis-
advantages?
The only disadvantages I have observed are refractive sur-
prises in some patients and restricted movement of the
anterior optic in others. Extreme capsular bag sizes can
cause refractive errors or lack of anterior lens movement.
Currently, we do not have an accurate method of predicting
capsular bag volume; however, in the future, if we could
OCTOBER 2010 CATARACT & REFRACTIVE SURGERY TODAY EUROPE 55
COVER STORY
Figure 1. The difference in accommodative amplitude
between dual- and single-optic lenses, per millimeter of
movement.
Courtesy of Victor Bohórquez,MD

measure or estimate the strength of the ciliary muscle and
capsular bag volume preoperatively, we could better choose
the appropriate technology and lens size that best fits the
patient’s anatomy.
When compared with other accommodating IOLs
and the multifocal IOLs currently available, the
Synchrony provides uninterrupted vision at all dis-
tances through physiologic accommodation.5-7 The
most powerful advantage of this lens is that the sub-
jective and objective evaluations of accommodative
amplitude correlate and show approximately 2.00 to
3.00 D, suggesting real and natural accommodation.
Additionally, the Synchrony is the only IOL that com-
pletely fills the capsular bag, keeping the anterior and
posterior capsules apart and thus limiting fibrosis
(Figure 2).
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
Our experience with this lens extends to 4 years’ follow-
up. Patients have excellent visual acuity at all distances, very
functional reading speed (comparable with multifocal IOLs
at newspaper print size), and lower incidence of glare and
halos than multifocal lenses.
As with other premium IOLs, a careful surgical tech-
nique is ideal. The Synchrony is provided in a preloaded
injector, and the lens is delivered into the capsular bag
in a consistently controlled fashion through a small inci-
sion. I attempt a perfect 5.0-mm continuous curvilinear
capsulorrhexis (CCC) by creating a guide before my inci-
sion with a 5.3-mm corneal marker.
With premium IOLs, I try to decrease the incidence of
capsular opacification by cleaning the capsular bag
completely, including polishing the undersurface of the
anterior capsule to remove lens epithelial cells. I prefer
bimanual I/A to achieve 360º polishing, including the
subincisional areas.
With any accommodating lens, I want to have a cap-
sule that remains clean and flexible to increase the
chances of success. The Synchrony has features that
help prevent anterior and posterior capsular opacifica-
tion. A system of fluid channels on the anterior optic
allows aqueous humor circulation between the bag
and the anterior chamber and keeps the CCC edge
raised, preventing rubbing between the optic and the
lens epithelial cells, thus inhibiting lens epithelial cell
fibrous metaplasia (a precursor of anterior capsular
opacification).
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
TETRAFLEX1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its current
design limits it from working?
The Tetraflex is another single-optic IOL that is much
like the Crystalens in its design and anticipated mode of
action.
3. What are the advantages of the lens design? The dis-
advantages?
Based on my experience with other accommodating
lenses, I am skeptical of this IOL’s ability to generate a
significant magnitude of accommodation with vitreous
displacement alone.
4. Who is the ideal candidate for this lens? What tips do
you have for implanting this lens or optimizing postoper-
ative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
56 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
Figure 2. Transillumination photo 1 year after surgery of an
eye implanted with the Synchrony.
Cour
tesy
of Vi
ctor B
ohór
quez
,MD

58 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
SHERAZ M. DAYA, MD,FACP, FACS, FRCS(ED),FRCOPHTHI work in both the government sector
(National Health Service; NHS) and run a private
organization that provides cornea, cataract, and
refractive surgery. I have been involved with accom-
modating lenses since 2002 and commenced with the
Crystalens AT-45. I have also used Crystalens’ later-gen-
eration lenses, the 5-0, the HD, and now the AO. In my
practice, I implant accommodating IOLs in 20% of
patients.
AKKOMMODATIVE 1CU 1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
I believe the lens works by moving forward as a result
of vitreous displacement from ciliary body contraction,
although this seems to be more dependent on capsule
malleability. I gather (anecdotally) that the lens ceases to
function once the capsule fibroses.
3. What are the advantages of the lens design? The
disadvantages?
Its advantages include four-point fixation and easy implan-
tation through a microincision with the correct injector.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
It will be surpassed by other technologies.
CRYSTALENS AO1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted more than 800 Crystalens IOLs since
2002 and have used the AT-45, the 5-0, the HD, and cur-
rently the AO.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
This lens works both by vaulting forward as a result
of vitreous movement and by arching; the silicone
lens is flexible, and the configuration of the haptics
and the hinge seems to permit this process. The limi-
tation is its inconsistency of action. Almost all recipi-
ents obtain good distance and intermediate vision,
but only 67% get good near vision. Myopes seem to
do better, which is a little counterintuitive in that the
lens power is low; however, it is easily explained by
the fact that eyes with longer axial lengths have a
greater depth of focus.
3. What are the advantages of the lens design? The
disadvantages?
The AO version has a monocular aberration-free optic,
which ensures good visual quality and is forgiving of mild
centration and tilt. To reduce the incidence of tilt and
refractive change, we now routinely follow a suggestion
made by my co-chief medical editor, Erik L. Mertens, MD,
FEBOphth, which is to implant a capsular tension ring
(Ophtec BV, Groningen, Netherlands) in conjunction
with lens implantation.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
Patients who absolutely must drive at night and can-
not risk the compromises associated with multifocal
lenses and night driving (eg, chauffeurs), those requir-
ing good unaided intermediate vision, and those in
whom a multifocal lens is a relative contraindication
Victor Bohórquez, MD, is with the Department of
Ophthalmology at Servioftalmos, Bogotá, Colombia. Dr.
Bohórquez states that he is a paid consultant to Visiogen (now
part of Abbott Medical Optics Inc.). He may be reached at
e-mail: [email protected].
1.Findl O, Leydolt C.Meta-analysis of accommodating intraocular lenses.J Cataract Refract Surg..2007; 33:522-527.2.Findl O, Kriechbaum K, Menapace R, et al. Laserinterferometric assessment of pilocarpine-induced movement of
an accommodating intraocular lens:a randomized trial.Ophthalmol.2004;111(8):1515-1521.3.Schneider H, Stachs O, Go¨bel K, Guthoff R.Changes of the accommodative amplitude and the anterior chamberdepth after implantation of an accommodative intraocular lens.Graefes Arch Clin Exp Ophthalmol. 2006; 244:322-329.4.Uthoff D, Gulati A, Hepper D and Holland D.Potentially Accommodating 1CU Intraocular Lens:1-year Results in 553Eyes and Literature Review.J Refract Surg. 2007;23(2).5.McLeod SD, Portney V,Ting A.A dual optic accommodating foldable intraocular lens.Br J Ophthalmol.2003;87:1083-1085.6.McLeod SD,Vargas LG, Portney V,Ting A.Synchrony dual-optic accommodating intraocular lens.Part 1:Optical andbiomechanical principles and design considerations.J Cataract Refract Surg.2007; 33:37-46.7.Ossma IL, Glavis A,Vargas LG,Trager MJ, et al.Synchrony dual-optic accommodating intraocular lens.Part 2:Pilotclinical evaluation.J Cataract Refract Surg.2007; 33:47-52.

(eg, patients with glaucoma, age-related macular
degeneration, diabetes) are good candidates.
5. What is your opinion on the future of this lens
technology?
It is a useful lens to have in our surgical armamen-
tarium. Other technologies that function similarly and
do not reduce contrast sensitivity may well replace
this lens, unless a new iteration of the implant is
developed to provide increased reliability in terms of
lens movement.
FLUIDVISION 1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
2. Whether or not you have personal experience
with this lens, what is your impression of its mecha-
nism of accommodation? Why does it work, or what in
its current design limits it from working?
It has an interesting mechanism of action. The sustain-
ability of action might be an issue and may be reduced
as a result of capsular fibrosis. Further investigation is
required.
3. What are the advantages of the lens design? The
disadvantages?
One advantage is the potential for a large amplitude of
accommodation. In terms of disadvantages, there is pos-
sible decreased performance with time. I would be inter-
ested to know about visual performance and aberrations
at different levels of accommodation.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
Any patient could be a potential candidate, as long as the
device works and does not produce any optical aberrations.
5. What is your opinion on the future of this lens
technology?
Unsure, but the future looks good if it works long-term.
Sheraz M. Daya, MD, FACP, FACS, FRCS(Ed), FRCOphth,
is Director and Consultant of Centre for Sight and the
Corneoplastic Unit and Eyebank, Queen Victoria Hospital,
East Grinstead, United Kingdom. Dr. Daya is the Chief
Medical Editor of CRST Europe. He states that he is a con-
sultant to Bausch + Lomb. He may be reached at e-mail:

60 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
ROBERT K. MALONEY, MDI am in a group private practice in Los Angeles.
Our center has been implanting accommodat-
ing IOLs since 2006. Accommodating IOLs are
used in approximately 25% of our cataract sur-
gery patients currently.
AKKOMMODATIVE 1CU 1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The accommodative mechanism is similar to the
Crystalens; with soft flexible haptics, the optic will move
forward in response to vitreous pressure.
3. What are the advantages of the lens design? The
disadvantages?
The four-haptic design fills the capsular bag, dis-
tending it. This distension may improve the ability of
the ciliary body to generate the accommodative force
on the lens.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
I have no opinion.
5. What is your opinion on the future of this lens
technology?
Because the accommodative mechanism is similar to
the Crystalens, I expect the lens to have a future similar
to that lens.
CRYSTALENS AO1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I use either the Crystalens AO or the Crystalens HD in
approximately 25% of my premium IOL patients.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The lens accommodates when vitreous pressure
induces either forward movement of the lens or a distor-
tion of the lens, leading to an increase in spherical aber-
ration with increased depth of focus.
3. What are the advantages of the lens design? The
disadvantages?
The two-haptic design is easy to insert and requires
no significant changes in surgical technique from stan-
dard cataract surgery. Because the positioning loops at
the ends of the plate haptics become encased in the
capsular bag, the haptics cannot be explanted once the
bag fibroses, and the haptics must be amputated.
However, because of the good optical performance of
the lens, explantation is rarely necessary.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
The optimal candidate is a patient who requires excellent
distance and intermediate visual acuity, is willing to sacrifice
near visual acuity, and would be intolerant to the increased
night glare that accompanies multifocal lenses. Because the
lens is flexible, the refractive outcome is slightly less accurate
than with a standard monofocal lens, so the surgeon must
be prepared and able to perform a laser corneal surgical
refractive enhancement postoperatively.
5. What is your opinion on the future of this lens
technology?
The lens has a secure position in our armamentarium now
because it offers an alternative for patients who want a premi-
um IOL but who are intolerant of the night glare of multifocals.
FLUIDVISION1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
Figure 3. A Synchrony accommodating IOL in the eye 2 years
postoperatively.The capsule remains quite clear, possibly
because the IOL completely fills the capsular bag.
Courtesy of Robert K.Maloney,M
D

2. Whether or not you have personal experience
with this lens, what is your impression of its mecha-
nism of accommodation? Why does it work, or what in
its current design limits it from working?
Because the lens relies on the movement of fluid
behind the membrane, it potentially has a much greater
amplitude of accommodative power than a solid lens.
3. What are the advantages of the lens design? The
disadvantages?
[No answer provided.]
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
[No answer provided.]
SYNCHRONY 1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
2. Whether or not you have personal experience
with this lens, what is your impression of its mecha-
nism of accommodation? Why does it work, or what in
its current design limits it from working?
The Synchrony entirely fills the capsular bag (Figure 3),
maximizing ciliary action. The combination of its plus and
minus optics increases its accommodative response to cil-
iary movement.
3. What are the advantages of the lens design? The
disadvantages?
[No answer provided.]
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
I am looking forward to adding this lens to my practice
when it is available in the United States.
TETRAFLEX 1. Do you have any experience with this lens, either

62 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
SAMUEL MASKET, MDMy practice concerns mainly complex anterior
segment cases. As a result, I see a relatively small
number of routine cataract candidates, limiting
the number of patients who are eligible for either
multifocal or accommodating IOLs. With that
said, I have implanted accommodating IOLs for nearly 3
years and they represent between 5% and 10% of my cases.
All surgery is performed at Specialty Surgery Center, an out-
patient center dedicated to anterior segment eye surgery.
AKKOMMODATIVE 1CU1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no clinical experience with the Akkommodative1CU,
as it is not available in the United States.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Given low market interest where available and because it
has been on the market for several years, I doubt that it
achieves much accommodation.
3. What are the advantages of the lens design? The
disadvantages?
Today, focus-shift, single-optic IOLs are of limited value.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
In my opinion, the future of this technology is limited.
CRYSTALENS AO1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted approximately 100 of these lenses.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Its mechanism of accommodation is speculative; in
concept, it is a single-optic, focus-shift lens with little
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The accommodation of this lens may occur when ciliary
pressure causes the lens to flex, inducing a change in spheri-
cal aberration and increasing the depth of focus. The lens
has a four-haptic design and is vaulted anteriorly, which may
improve the response of the lens to ciliary movement.
3. What are the advantages of the lens design? The
disadvantages?
[No answer provided.]
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
[No answer provided.]
A FINAL COMMENTWe are moving into a generation of accommodating
lenses with accommodative amplitudes dramatically
increased over what has been previously available. An
unrecognized problem with these lenses is that they
will have less refractive accuracy than the lenses we are
used to. The reason for this is simple: these lenses are
designed to respond to small changes in the ciliary
force with large changes in refractive power.
Because of variations in the sizing of human eyes and
variations in capsular bag contraction, the resting force
on the lens with the ciliary muscle relaxed will vary sig-
nificantly from patient to patient. Therefore, many of
these lenses will be in a partially accommodated state
even with the ciliary muscle relaxed. We should expect
to see larger spherical refractive errors in these lenses
than we are accustomed to. To use these lenses, the
cataract surgeon will need to be an expert refractive
surgeon as well.
Robert K. Maloney, MD, is the Director of the Maloney
Vision Institute in Los Angeles. He states that he is a con-
sultant to Abbott Medical Optics Inc. and is a consultant to
and an owner or shareholder in Calhoun Vision, Inc. Dr.
Maloney may be reached at tel: +1 310 208 3937; e-mail:

64 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
true movement demonstrated. Some patients have an
improved accommodative range over monofocal lens
designs, but this is not predictable. The Crystalens HD
model improved near visual acuity but at the expense of
vision quality and IOL power predictability.
3. What are the advantages of the lens design? The
disadvantages?
The disadvantages include the size of the optic (5
mm), lack of a UV-absorbing chromophore, and its
flexible haptics, which, in combination with postopera-
tive capsular fibrosis, leads to mild to severe Z syn-
drome.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
This lens serves those who desire reduced spectacle
dependence and are willing to accept limited near
UCVA. Patients are best served with mini-monovision.
During implantation, it is imperative to clean anterior
subcapsular lens epithelial cells and to cover the hap-
tics with the anterior capsule to prevent Z syndrome. I
prefer an ovoid capsulorrhexis, placing the long axis of
the optic perpendicular to the short axis of the capsu-
lotomy. I offer this IOL to those who are not appropri-
ate candidates for multifocal IOLs.
5. What is your opinion on the future of this lens
technology?
It will be replaced by evolving IOLs.
FLUIDVISION1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
No personal experience; however, I am a member of
the medical advisory board.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Accommodation is accomplished by transfer of fluid
from the haptic reservoirs to a bladder within the optic
on accommodative demand (Figure 4). It has been
demonstrated to work in the laboratory and in a small
number of humans.
3. What are the advantages of the lens design? The
disadvantages?
The advantages include adequate range of accommo-
dation. Disadvantages include its novel technology, sizing
issues of the capsular bag, and the necessary incision size
of approximately 5 mm.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
Figure 4. A prototype of the FluidVision IOL.
Figure 5. Cadaver eye after SmartIOL implantation and
subsequent removal of the cornea for visibility.The SmartIOL
is designed to fill the capsular bag.
Figur
es 4
and 5
cour
tesy
of Sa
mue
l Mas
ket,M
D

OCTOBER 2010 CATARACT & REFRACTIVE SURGERY TODAY EUROPE 65
COVER STORY
5. What is your opinion on the future of this lens
technology?
This lens will soon enter clinical trials.
NULENS DYNACURVE1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted this IOL only in the wet lab setting.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Reverse accommodation is achieved by impaling the
haptics in the ciliary body, avoiding the need for capsular
bag shape change.
3. What are the advantages of the lens design? The
disadvantages?
The main advantage is the potential for sulcus place-
ment, which may also be disadvantageous. The major
disadvantage is its mechanism of reverse accommoda-
tion.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
Speculative.
SMARTIOL1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have done prior laboratory testing in a few cadaver
eyes (Figure 5).
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Its full-sized optic allows transmission of capsular
forces to induce IOL shape change.
3. What are the advantages of the lens design? The
disadvantages?
Advantages include its full-size hydrophobic acrylic
thermoplastic optic. The disadvantages include IOL sizing
and flexibility of material.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
No information at this time.
5. What is your opinion on the future of this lens
technology?
Speculative but hopeful.
SYNCHRONY1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
None implanted.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
This lens’ double-optic Galilean telescopic design pro-
vides the mechanism of accommodation, allowing true
accommodation.
3. What are the advantages of the lens design? The
disadvantages?
Advantages include its double optic, which fills the
capsular bag. The major disadvantages are the large
incision size required and the need for perfect sur-
gery.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
This lens will likely have favorable market position for
several years.
TETRAFLEX1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?

66 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
MARK PACKER, MD, FACSI practice in the beautiful valley town of
Eugene, Oregon, nestled between coastal hills
and the towering Cascade Mountain volcanic
peaks, home to the University of Oregon, the
birthplace of Nike footwear, and the last refuge
of the 1960s generation. Our private practice and surgery
center enjoy a reputation for superb, state-of-the-art
cataract and refractive surgery, built and maintained for
more than 40 years by offering the most advanced and
effective technologies and delivering them with genuine
care for each person who trusts his or her sight to us.
This year to date, 35% of my patients have opted for
presbyopia correction at the time of cataract surgery. Of
these patients, 20% have received an accommodating
lens (the Crystalens AO is the only accommodating IOL
currently available in the United States; however, I am an
investigator for the Synchrony and have implanted it
under an Investigational Device Exemption [IDE] in some
cases). The other 80% of patients have received multifo-
cal IOLs, predominately the Tecnis Multifocal (Abbott
Medical Optics Inc.). In general, currently available multi-
focal IOLs provide a higher level of spectacle independ-
ence than the Crystalens—albeit at the cost of some
reduction in quality of vision. However, for patients moti-
vated to live without glasses, multifocal lenses achieve a
high level of satisfaction. Future accommodating lenses
should achieve a higher level of spectacle independence
by providing a greater amplitude of accommodation or
pseudoaccommodation and preserve high-quality vision
with low overall optical aberrations.
AKKOMMODATIVE 1CU 1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no personal experience with this lens.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
I remember its launch with great fanfare at the European
Society of Ophthalmology (SOE) in Istanbul, Turkey, in
2001; however, to the best of my knowledge, it has not
demonstrated more than 1.00 D of accommodation.
3. What are the advantages of the lens design? The
disadvantages?
There have been reports of capsular contraction and
centripetal movement of the haptics.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
Unless improvements in its design are forthcoming, I
do not believe the 1CU will remain a viable entry.
CRYSTALENS AO 1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have extensive experience with the Crystalens, begin-
ning as an investigator in 2000 with the AT-45 and span-
ning the decade since.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Axial movement was the initial conceptual mechanism
The lens has a single optic and the haptics are flexible.
However, it is a focus-shift IOL.
3. What are the advantages of the lens design? The
disadvantages?
Advantages include simple insertion and acrylic mate-
rial. A disadvantage is limited accommodation due to the
single-optic, focus-shift design.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
Should it receive US Food and Drug Administration
(FDA) approval, it will have some impact on the mar-
ket, although its accommodative function is limited.
Samuel Masket, MD, is a Clinical Professor at the David
Geffen School of Medicine, UCLA, and is in private practice
in Los Angeles. Dr. Masket states that he has no financial
interest in the products or companies mentioned. He may
be reached at tel: +1 310 229 1220; e-mail:

68 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
of this lens, but it has not been demonstrated to move
significantly. Alternative explanations for its clinical effec-
tiveness include arching, bending, and high spherical
aberration. The FDA approval for the Crystalens
described 1.00 D of accommodation, and I believe this
accurately represents a mean minimum. Some patients
achieve higher levels of function, perhaps from
pseudoaccommodative mechanisms.
3. What are the advantages of the lens design? The
disadvantages?
I had minimal trouble with complaints of halo after
Crystalens HD implantation, but I have heard of this
phenomenon from other surgeons. The current AO
design provides optical quality similar to a monofocal
IOL.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
I continue to recognize that some patients do
extraordinarily well with this technology, and that these
patients tend to be axial myopes with minimal astigma-
tism and little to no residual refractive error. It is not
unusual to achieve 20/20 and J2 or better vision in this
group. On the other hand, the majority of patients
implanted bilaterally with any model of the Crystalens
should be counseled to expect to wear low-power read-
ing glasses postoperatively (usually 1.25 to 1.50 D). I
continue to offer the Crystalens AO, primarily for
patients who specifically request it and secondarily for
patients who wish to reduce their need for glasses but
are averse to halos or dysphotopsia. I discourage hyper-
opes and patients with higher degrees of keratometric
cylinder preoperatively unless they are comfortable
with the high likelihood (about 15%) of an excimer laser
enhancement procedure afterward.
5. What is your opinion on the future of this lens
technology?
The Crystalens is currently experiencing a declining
market share in the United States; however, it has been
reimagined and redesigned several times and may have
yet another rebirth in store.
FLUIDVISION1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have seen the design of the FluidVision lens and heard
some reports about it at meetings. I have no personal
experience.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
I believe the concept could be effective; however, I am
concerned about long-term safety.
3. What are the advantages of the lens design? The
disadvantages?
It may provide substantial accommodation.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
This design has some potential; however, there is a long
clinical row yet to hoe.
NULENS DYNACURVE1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no personal experience.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The NuLens represents a captivating and innovative
idea; however, its embodiment is complex and fraught.
3. What are the advantages of the lens design? The
disadvantages?
This design has the ability to provide high amounts of
accommodative amplitude through changes in the sur-
face curvature of the deformable piston. The device is
fairly complex and much different from anything we have
experienced before.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
This technology has developed a great deal since I first
became aware of it. With greater simplification, it may
yet prove itself.

SMARTIOL1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
I have no personal experience.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The SmartIOL has been off my radar screen for some time.
Several years ago it was a hot topic, with benchtop videos of its
expansion in warm water and its inherent flexibility.
3. What are the advantages of the lens design? The dis-
advantages?
Simple, straightforward and easy to implant, it seemed at
the time to be a winner design. Even the potential compli-
cation of posterior capsular opacification seemed manage-
able because Nd:YAG capsulotomy would not be con-
traindicated. At the moment, I am wondering what became
of the SmartIOL.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing post-
operative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens tech-
nology?
[No answer provided.]
SYNCHRONY1. Do you have any experience with this lens, either in
practice or in clinical testing? If so, how many have you
implanted?
As a US investigator for this lens, I have been able to
implant it under an IDE in some cases.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The Synchrony represents a unique combination of origi-
nal design, ingenuity, and functionality. I have been
extremely impressed by the demonstration of forward
movement of the anterior optic with ultrasound biomi-
croscopy under ciliary body contraction.
3. What are the advantages of the lens design? The dis-
advantages?
The resultant 2.00 to 3.00 D of accommodation provides
Visit us at AAO

MAGDA RAU, MD
In Germany, I practice in the hospital setting at
Augenklinik Cham and also am in private prac-
tice at Refractive Privatklinik-Dr.Rau, both in
Cham. I also practice at Eye Centre Prag in the
Czech Republic. I have been implanting accommodating
IOLs for the past 9 years. Currently, I use accommodative
technologies in 15% of my cataract patients.
AKKOMMODATIVE 1CU1. Do you have any experience with this lens, either
intermediate vision that outperforms multifocal IOLs and
near vision that matches them, without the induction of
aberrations. The persistent clarity of the capsule beyond
3-year follow-up is an unexpected benefit of this IOL.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
The surgical technique demands a precise capsulor-
rhexis and careful cortical clean-up; the injector provides
a simple and predictable method of implantation.
5. What is your opinion on the future of this lens
technology?
Acquired by Abbott Medical Optics Inc. last year, the
Synchrony is awaiting FDA approval. I believe it has the
potential to become a dominant market player in the
near-term.
TEK-CLEAR1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no personal experience.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The Tek-Clear is a lens within a ring; it is a bending,
accommodating IOL. It is not available in the United States.
3. What are the advantages of the lens design? The
disadvantages?
It is a simple design, but one that does not appear to
have the potential for greater accommodative amplitude
than the Tetraflex or the Crystalens.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
I do not see this IOL garnering a significant market share.
TETRAFLEX1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no personal experience.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The Tetraflex reportedly works through a bending-
and-flexing mechanism, with changes in surface curva-
ture and possibly some axial movement.
3. What are the advantages of the lens design? The
disadvantages?
The Tetraflex appears to provide a range of function
similar to the Crystalens.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
The Tetraflex may have some adherents, but is unlikely
to be a big winner in the market place.
Mark Packer, MD, FACS, is a Clinical Associate Professor
at the Casey Eye Institute, Department of Ophthalmology,
Oregon Health & Science University, and is in private prac-
tice at Drs. Fine, Hoffman & Packer, LLC, Eugene, Oregon.
He states that he is a paid consultant to Abbott Medical
Optics Inc., Advanced Vision Science, Bausch + Lomb, Carl
Zeiss Meditec Surgical, Inc., Celgene Corp., Corinthian
Ophthalmic Inc., GE Healthcare, Haag-Streit USA, Ista
Pharmaceuticals, Inc., and Rayner Intraocular Lenses, Inc.,
and holds stock options with LensAR, Inc., Surgiview LLC,
Corinthian Ophthalmic, Inc., Transcend Medical, Inc.,
TrueVision Systems, Inc., and WaveTec Vision Systems. Dr.
Packer may be reached at tel: +1 541 687 2110; e-mail:
COVER STORY
70 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010

in practice or in clinical testing? If so, how many have
you implanted?
I have used the 1CU regularly since 2001; I have
implanted approximately 500.
2. Whether or not you have personal experience
with this lens, what is your impression of its mecha-
nism of accommodation? Why does it work, or what
in its current design limits it from working?
The accommodative function is based on the focus-shift
principle; the flexible geometry and composition of the
four haptics allow the IOL to move forward in correspon-
dence with the ocular structures such as the ciliary muscle.
Successful performance of the lens depends on the healthy
physiology of the accommodating structures of the eye.
A forward lens movement of 0.64 to 1.10 mm achieves
0.50 to 1.80 D of accommodation. Higher lens powers (start-
ing at 23.00 D) increase the amount of pseudoaccommoda-
tion. Additionally, according to the principle of the conoid of
Sturm (astigmatmus inversus against-the-rule), astigmatism
of -0.50 to -1.25 D increases the amount of pseudoaccom-
modation achieved after the implantation of 1CU.
3. What are the advantages of the lens design? The
disadvantages?
Pseudoaccommodation is achieved through deforma-
tion of the haptics, so the monofocal nature of the lens
optic avoids the typical side effects (eg, glare and halos)
associated with multifocal IOLs. Patients do not have to
get used to two different foci, which for some is difficult.
In my opinion, the greatest advantage of this lens is that it
can be offered to patients who wish to be spectacle inde-
pendent but do not want to compromise distance vision;
who drive a lot at night; or who work in an illuminated
environment, such as under spotlights on the stage.
The disadvantage is that the achieved accommoda-
tion is usually only 1.00 to 2.00 D, contraindicating
patients who want 100% spectacle independence.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
The ideal candidate wants spectacle independence in
daily life; these are active people who work on the com-
puter, play sports and cards, go to the cinema, and drive
at night. Candidates who read often, work a lot at near,
and desire complete spectacle independence are not ideal
candidates for this IOL. I usually start with the dominant
eye and calculate the refraction target for plano. After 1
month, if the patient requires better near vision, I calcu-
late the lens for the nondominant eye for between -0.50
and -1.25 D. I implant the 1CU through an astigmatically
eyetube.net
b
The world’s
#1online source for
ophthalmic videos
Thousands of videoswith audio tracks
•High-Definition
video•
Links to articles•
watch + listen + learn
www.eyetube.net
Find us on
&

neutral clear corneal incision. It is important to perform a
well-centered rhexis, without any peripheral tears and not
exceeding 5 mm in diameter, to ensure that the capsule is
stable enough to withstand any IOL movement. As it
might hinder the shift of the IOL, no capsular tension ring
should be used. Patients with symptoms that might hinder
the accommodative mechanism, such as pseudoexfolia-
tion syndrome, synechia, phacodonesis, or damaged
zonules, should be fit with another IOL.
5. What is your opinion on the future of this lens
technology?
In my practice, I use the 1CU as a complement to multifocal
IOLs. This lens addresses the needs of patients who wish to
achieve spectacle independence. In the future, it may be possi-
ble to combine the flexible haptics with movement-induced
changes of the lens optic material. This could increase
pseudoaccommodation to 3.00 D. I think that there will con-
tinue to be further need for accommodating IOLs, because
although multifocal IOLs continue to emerge in the market,
not every patient is a good candidate for this lens design.
CRYSTALENS AO1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted approximately 10.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
[No answer provided.]
3. What are the advantages of the lens design? The
disadvantages?
In my opinion, results after implantation of the Crystalens
AO are comparable with results after implantation of the
Akkommodative 1CU. Therefore, the advantages and disad-
vantages of both IOLs are nearly the same.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
For patients to achieve more spectacle independence, I
correct the nondominant eye to -0.50 or -1.00 D. Women
seem to tolerate slight monovision better than men. In my
experience, 25% of women and 15% of men have been able
to adapt to monovision. For this reason, I usually target
higher monovision in women than in men. We examine the
tolerance of monovision preoperatively with test glasses or
contact lenses. Even after 10 minutes with test glasses,
patients can usually tell if they will tolerate monovision.
5. What is your opinion on the future of this lens
technology?
[No answer provided.]
TEK-CLEAR1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted three lenses thus far.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The Tek-Clear is a successful attempt to simulate the
human lens. Designed to take advantage of the natural
accommodating process of the human eye, the lens hap-
tics and optic incorporate a bending-beam approach
that fully optimizes IOL movement as the ciliary muscle
contracts and relaxes during accommodation.
3. What are the advantages of the lens design? The
disadvantages?
Unfortunately, even though the lens is very flexible, with
its large diameter it is difficult to implant. The accommoda-
tion achieved in our hands with this lens was 1.00 D.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
[No answer provided.]
Magda Rau, MD, is the Head of the Augenklinik Cham
and Refractive Privatklinik-Dr.Rau, Cham, Germany, and
Eye Centre Prag, Czech Republic. Dr. Rau states that she has
no financial interest in the products or companies men-
tioned. She may be reached at tel: +49 9971 861076; e-mail:
72 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY
Would you like to comment on an author’s article? Do you have an article topic to suggest?
Do you wish to tell us how valuable CRST Europe
is to your practice? Please e-mail us at [email protected] with any thoughts, feel-
ings, or questions you have regarding this publication.
SHARE YOUR FEEDBACK

SUNIL SHAH, FRCOPHTH,FRCS(ED), FBCLA
I work both in the Midland Eye Institute, a dedi-
cated private ophthalmic day hospital, and the
Birmingham and Midland Eye centre, an NHS
hospital, both in the United Kingdom. I have
been using accommodating lenses for more than
6 years, both for research trials and in routine practice. I use
accommodating IOLs for appropriate patients and feel that
they are a necessary part of my armamentarium to offer
patients a complete range of choices.
AKKOMMODATIVE 1CU1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted 50 lenses. Initially, this was part of a study.8
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Theoretically, it is the focus-shift principle that pro-
vides the mechanism of accommodation. In practice, it is
probably lens flexing.
3. What are the advantages of the lens design? The
disadvantages?
I found the lens to be slightly fiddly to insert.
Additionally, in my experience, it provided only limited
pseudoaccommodation and had a high early posterior
capsular opacification rate.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
I do not use this lens any longer.
5. What is your opinion on the future of this lens
technology?
Limited.
CRYSTALENS AO1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have no experience with this lens.
COVER STORY
66thth International Congress ofInternational Congress ofCorneal CrossCorneal Cross--LinkingLinking
January 21-22, 2011 - Milan/Italy
The CXL congress is an international forum for the most recent advancesin corneal cross-linking
For more information please contactFor more information please contact:CBS Congress & Business Services,
Technoparkstrasse 1, CH-8005 Zurich, SwitzerlandE-mail address: [email protected]
Registration form on: www.cxl-congress.org
www.cxl-congress.org

2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Like the Akkommodative 1CU, the mechanism is theo-
retically the focus-shift principle. However, in practice, it
is probably the lens flexing.
3. What are the advantages of the lens design? The
disadvantages?
There are few advantages other than the marketing by
the manufacturer.
4. Who is the ideal candidate for this lens? Do you
have any tips for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
Limited, given other lenses on the market now.
SYNCHRONY1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
My only knowledge of this lens comes from presenta-
tions made at conferences.
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
The focus-shift principle works better in a lens with a
dual-optic design, such as this one.
3. What are the advantages of the lens design? The
disadvantages?
The advantage is that more pseudoaccommodation is
possible. However, it is a large lens and more difficult to
manage. Additionally, it may induce myopia for a few
weeks after surgery.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
[No answer provided.]
5. What is your opinion on the future of this lens
technology?
This is an interesting technology. I look forward to see-
ing whether it lives up to its potential.
TETRAFLEX1. Do you have any experience with this lens, either
in practice or in clinical testing? If so, how many have
you implanted?
I have implanted approximately 1,000. Initially this was
through a research study.9 I have recently completed
another research study on this lens.10
2. Whether or not you have personal experience with
this lens, what is your impression of its mechanism of
accommodation? Why does it work, or what in its cur-
rent design limits it from working?
Theoretically, like the Akkommodative 1CU and the
Crystalens AO, the focus-shift principle is the mechanism of
accommodation, but in practice it is probably the lens flexing.
3. What are the advantages of the lens design? The
disadvantages?
The main advantage is that this lens is simple to use, as
it behaves just like a monofocal lens for insertion. It per-
forms very well on functional visual acuity testing even
though push-pull testing gives only a mean of approxi-
mately 1.60 D pseudoaccommodation. However, the pos-
terior capsular opacification rate is slightly high.
4. Who is the ideal candidate for this lens? What tips
do you have for implanting this lens or optimizing
postoperative visual acuity?
Anyone who desires good distance and intermediate
vision and some near vision, without the risk of dyspho-
topsias. This lens is ideal for micro-monovision or for
patients who are slightly myopic in both eyes.
5. What is your opinion on the future of this lens
technology?
This lens has good potential, and I understand it is due
to receive FDA approval soon. ■
Sunil Shah, FRCOphth, FRCS(Ed), FBCLA, is a Visiting
Professor at the School of Biomedical Sciences, University of
Ulster, Coleraine, Northern Ireland; Visiting Professor at the
School of Life & Health Sciences, Aston University, Birmingham,
UK; Medical Director, Midland Eye Institute, Solihull, UK; and
Consultant Ophthalmic Surgeon, Birmingham & Midland Eye
Centre, Birmingham, UK. Professor Shah states that he is a con-
sultant to Abbott Medical Optics Inc. and Lenstec Inc. He may
be reached at tel: +44 1217112020; fax: +44 1217114040; e-
mail: [email protected].
8.Wolffshon JS,Hunt OA,Naroo S,et al. Objective accommodative amplitude and dynamics with the 1CU accommoda-tive intraocular lens.Invest Ophthalmol Vis Sci. 2006;47:1230-1235.9.Wolffshon JS, Davies LN, Gupta N, et al.Mechanism of action of the Tetraflex accommodative intraocular lens. JRefract Surg.2010;28:1-5.10.Wolffsohn JS,Naroo SA,Motwani NK,et al.Subjective and objective performance of the Lenstec KH-3500 accommoda-tive intraocular lens.Br J Ophthalmol.2006;90(6):692-696.
74 CATARACT & REFRACTIVE SURGERY TODAY EUROPE OCTOBER 2010
COVER STORY