course andprognosis of ulcerative colitis Part III fileGut, 1964, 5, 1 Thecourse andprognosis...
15
Gut, 1964, 5, 1 The course and prognosis of ulcerative colitis FELICITY C. EDWARDS AND S. C. TRUELOVE From the Nuffield Department of Clinical Medicine, The Radcliffe Infirmary, Oxford Part III Complications One of the outstanding features of ulcerative colitis is the diversity of complications of the disease. They fall logically into two main groups: local complica- tions in and around the large bowel, and remote or systemic complications affecting distant parts of the body. Some of these complications are so dangerous that they make a substantial contribution to the con- siderable fatality due to this disease. Tables XXIV and XXV show the incidence of the main complications divided between 'first attack' cases and 'relapses', and further subdivided accord- ing to whether the complication occurred during the first referred attack or during the period of sub- sequent follow-up.' The right-hand column shows the overall incidence of these complications in our total series of 624 patients. This incidence must be regarded as an underestimate for two distinct reasons. First, in many cases we have had to rely purely on the case notes for our information, and some of the complications, especially minor ex- amples, may not have been recorded in all instances. Secondly, it can be seen from Tables XXIV and XXV that these complications are numerous during the course of follow-up and therefore some patients who have so far escaped complications are almost certain to have one or more in the future. LOCAL COMPLICATIONS ISCHIO-RECTAL OR PARARECTAL ABSCESS Ischio- rectal abscess is a common complication, about one in 25 of our whole series having had one so far. Such an abscess may form at any time, either in a first attack or in a relapse of long-established disease. Sometimes the abscess may appear when the colitis is clinically quiescent, although sigmoidoscopy will reveal that the rectum and lower colon are inflamed. An ischio-rectal abscess demands surgical drainage without delay. The abscess is often deep-seated so that formal surgery is required. It is one of the few 'The Tables are numbered consecutively in Parts I to IV inclusive. complications which are amenable to conservative surgery, leaving the colon intact. Illustrative case history Mr. W. L. was first seen at this hospital in 1955, when he presented in his first attack of ulcerative colitis, at the age of 34 years. There was evidence of disease affecting the bowel from the trans- verse colon onwards, but the attack was mild, and he responded well to treatment with local hydrocortisone. Three months later, after a recurrence of symptoms, he developed a very large ischio-rectal abscess. This was opened and drained without any complications, and he made a satisfactory recovery. Since then, there has been no recurrence of symptoms. FISTULA-IN-ANO This may present as an ischio- rectal abscess, but when the abscess bursts or is incised, persistent purulent discharge occurs. The internal openings into the rectum may be small or multiple, so that the surgeon must explore with a probe to find them. They seldom heal spontaneously. They can be treated by conservative surgery if not too severe and it is essential for the surgeon to open up all the tracks into the rectum. This usually means cutting through the sphincter muscles of the anus, but anal continence is nearly always recovered when the large exposed surface granulates and heals. Severe examples offer adequate justification for colectomy. Fistula-in-ano resembles ischio-rectal abscess in being liable to present at any stage of the disease, from first attacks to recurrences of long-established disease, and also during clinical remissions. Its occurrence during a period of clinical remission always implies that there is active disease in the bowel, even though diarrhoea and the passage of blood per rectum may both be absent. Ischio-rectal abscess and fistula-in-ano frequently occur in the same patient, 11 of our series having suffered from both. Illustrative case history Mr. E. W. developed ulcer- ative colitis in 1937 at the age of 26, and subsequently on 21 March 2019 by guest. Protected by copyright. http://gut.bmj.com/ Gut: first published as 10.1136/gut.5.1.1 on 1 February 1964. Downloaded from
Transcript of course andprognosis of ulcerative colitis Part III fileGut, 1964, 5, 1 Thecourse andprognosis...

Gut, 1964, 5, 1
The course and prognosis of ulcerative colitisFELICITY C. EDWARDS AND S. C. TRUELOVE
From the Nuffield Department of Clinical Medicine,The Radcliffe Infirmary, Oxford
Part III Complications
One of the outstanding features of ulcerative colitisis the diversity of complications of the disease. Theyfall logically into two main groups: local complica-tions in and around the large bowel, and remote orsystemic complications affecting distant parts of thebody. Some of these complications are so dangerousthat they make a substantial contribution to the con-siderable fatality due to this disease.
Tables XXIV and XXV show the incidence of themain complications divided between 'first attack'cases and 'relapses', and further subdivided accord-ing to whether the complication occurred during thefirst referred attack or during the period of sub-sequent follow-up.' The right-hand column showsthe overall incidence of these complications in ourtotal series of 624 patients. This incidence must beregarded as an underestimate for two distinctreasons. First, in many cases we have had to relypurely on the case notes for our information, andsome of the complications, especially minor ex-amples, may not have been recorded in all instances.Secondly, it can be seen from Tables XXIV and XXVthat these complications are numerous during thecourse of follow-up and therefore some patients whohave so far escaped complications are almost certainto have one or more in the future.
LOCAL COMPLICATIONS
ISCHIO-RECTAL OR PARARECTAL ABSCESS Ischio-rectal abscess is a common complication, about onein 25 of our whole series having had one so far.Such an abscess may form at any time, either in afirst attack or in a relapse of long-established disease.Sometimes the abscess may appear when the colitisis clinically quiescent, although sigmoidoscopy willreveal that the rectum and lower colon are inflamed.An ischio-rectal abscess demands surgical drainage
without delay. The abscess is often deep-seated sothat formal surgery is required. It is one of the few'The Tables are numbered consecutively in Parts I to IV inclusive.
complications which are amenable to conservativesurgery, leaving the colon intact.
Illustrative case history Mr. W. L. was first seen atthis hospital in 1955, when he presented in his first attackof ulcerative colitis, at the age of 34 years. There wasevidence of disease affecting the bowel from the trans-verse colon onwards, but the attack was mild, and heresponded well to treatment with local hydrocortisone.Three months later, after a recurrence of symptoms, hedeveloped a very large ischio-rectal abscess. This wasopened and drained without any complications, and hemade a satisfactory recovery. Since then, there has beenno recurrence of symptoms.
FISTULA-IN-ANO This may present as an ischio-rectal abscess, but when the abscess bursts or isincised, persistent purulent discharge occurs. Theinternal openings into the rectum may be small ormultiple, so that the surgeon must explore with aprobe to find them. They seldom heal spontaneously.They can be treated by conservative surgery if nottoo severe and it is essential for the surgeon to openup all the tracks into the rectum. This usually meanscutting through the sphincter muscles of the anus,but anal continence is nearly always recovered whenthe large exposed surface granulates and heals.Severe examples offer adequate justification forcolectomy.
Fistula-in-ano resembles ischio-rectal abscess inbeing liable to present at any stage of the disease,from first attacks to recurrences of long-establisheddisease, and also during clinical remissions. Itsoccurrence during a period of clinical remissionalways implies that there is active disease in thebowel, even though diarrhoea and the passage ofblood per rectum may both be absent.
Ischio-rectal abscess and fistula-in-ano frequentlyoccur in the same patient, 11 of our series havingsuffered from both.
Illustrative case history Mr. E. W. developed ulcer-ative colitis in 1937 at the age of 26, and subsequently
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

Felicity C. Edwards and S. C. Truelove
TABLE XXIV
First Attacks
Before First In FirstReferred ReferredAttack Attack
LOCAL COMPLICATIONS
Relapses
Ischio-rectal abscessFistula-in-anoRecto-vaginal fistulaRecto-vesical fistulaEntero-colic fistulaRectal prolapseHaemorrhoidsFibrous stricturePseudo-polyposisPerforationAcute dilatation of the colonMassive haemorrhageCarcinoma of the colon
'Of 373 women in the series.
First Attacks
Before First In FirstReferred ReferredAttack Attack
TABLE XXVSYSTEMIC COMPLICATIONS
Relapses
Erythema nodosumPyodermia gangrenosumOther skin eruptionsArthritisAnkylosing spondylitisEye lesionsTransient hepatitisChronic hepatitisRenal diseasePulmonary embolismVenous thrombosisOral aphthous ulcerationOral moniliasisExtensive moniliasisOsteoporosisAnaemia due to ulcerative colitisOther disorders of the blood
suffered from the chronic intermittent form of the disease.He was first seen at the Radcliffe Infirmary in 1959, aged48, in a mild relapse, the whole colon being affected.Treatment with local and systemic corticosteroids pro-duced an early remission. However in 1960 he relapsedand presented with a painful swelling to the left of theanus which later discharged pus, and a small submucousfistula-in-ano. Two months later two more fistuloustracks had appeared, and these were subsequently laidopen. They healed well, and no further fistulae developed.He has since had several mild recurrences of ulcerativecolitis which have been treated satisfactorily withoutadmission to hospital.
RECTO-VAGINAL FISTULA This is not infrequentamong the female patients, there being 3% of thepresent series so affected. This condition gives riseto a profuse, foul, vaginal discharge. Spontaneous
healing seldom occurs. Conservative surgery isusually ineffective. Severe examples demand colec-tomy, but in this series there are two patients whohave done well by being treated by a three-stageprocedure consisting of double-barrelled ileostomy,conservative surgery to repair the fistula, and sub-sequent restoration of the continuity of the intestine.
Illustrative case history Mrs. P. V. developed severeulcerative colitis involving the distal colon in 1957 at theage of 47 years. Treatment with local and systemiccorticosteroids had little effect, and a recto-vaginalfistula developed five weeks after the onset.
Shortly afterwards she developed an ischio-rectalabscess, and this was opened and drained. At the sametime a double-barrelled transverse colostomy was per-formed, and local hydrocortisone was applied to thediseased colon through the distal stoma. Two months
Local Complication
During Before First In FirstFollow-up Referred Referred
Attack Attack
Whole SeriesNo.
DuringFollow-up
17
434
32
191322
643
1311172
54
23
25
2
3
53
6131634
l678
8123
2
10213
410
26 (4-2 %)26 (4 2%)1 1 (3-0%)'
3 (05%)8 (1-3 %)
129 (20-7%)39 (6-3%)93 (14 9%)20 (3-2%)10 (1 6%)21 (3 4%)22 (3-5%)
Systemic Complication
During Before First In FirstFollow-up Referred Referred
Attack Attack
5
3
194
Whole SeriesNo.
DuringFollow-up
1 36 23 25 _
1 61 10
3
3- 36
2
2
173382
428102
135
4
108
151659l63
82
32
261035
2761410222
525
229215434
5173
3184
14 (2-2%)4 (0-6%)
99 (15.90%)35 (5 6%)1 1 (18%)47 (7-5%)30 (4-8%)16 (2-6%)29 (4-6%)10 (1-6%)40 (6-4%)51 (8-2%)1 1 (1.8%)3 (0 5%)9 (1-4%)
127 (20 4%)18 (2-9%)
2
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
later an extensive, recently developed, fistula-in-ano wasexcised and she became symptom-free.
She was readmitted in 1960, having been well for overa year, and the recto-vaginal fistula was repaired. Thecolostomy was closed a few weeks later, and since thenshe has been in good health and has had no recurreniceof the colitis.
RECTO-VESICAL FISTULA This must be rare inulcerative colitis because no cases occurred in thisseries.
ENTERO-ENTERIC FISTULA This is an uncommoncomplication of ulcerative colitis in contrast toCrohn's disease, in which entero-enteric fistula isfrequent. There were three patients with entero-colic fistula in the present series. One had a fistulousconnexion between the tip of the appendix and thesigmoid colon, which was discovered at operationfor carcinoma of the transverse colon complicatinglong-standing ulcerative colitis. The other twopatientseach had a fistula between the colon and a loop ofsmall intestine.An entero-enteric fistula demands surgical inter-
vention with excision of the fistulous tract in addi-tion to whatever other surgery appears necessary.
RECTAL PROLAPSE This is an occasional complica-tion which develops during the course of an actualattack of ulcerative colitis when there is muchdiarrhoea. It is interesting that in the present seriesthere was no example during the first attack of thedisease. There is the possibility that the rectalmusculature becomes altered as a result of repeatedattacks of severe diarrhoea so that prolapse is liableto occur.
It is well known that, apart from ulcerative colitis,rectal prolapse chiefly occurs in infancy and in oldage. In the present series, rectal prolapse occurredchiefly in patients aged 25 to 40 years, which furthersuggests that the disease itself creates the circum-stances which lead to the development of the pro-lapse.
HAEMORRHOIDS These occur frequently in ulcera-tive colitis and appear to be one of the complicationsof diarrhoea. They also bulk largely in the casehistories for the following additional reason. Apatient may complain of passing bright blood ondefaecation and be treated as a case of haemorrhoidsby injection or actual haemorrhoidectomy. If thesymptoms persist, it is not rare to find that thepatient has the distal form of ulcerative colitis, whichoften causes bleeding without diarrhoea. We haveseen many patients with ulcerative colitis who havegiven this type of history.
When severe prolapsed haemorrhoids occur duringan actual attack of ulcerative colitis, they representan unpleasant complication. It is best to treat themconservatively until the ulcerative colitis is quiescentand then to carry out haemorrhoidectomy as in anyother patient.
FIBROUS STRICTURE This occurs in a small propor-tion of patients and is essentially a manifestation ofchronic disease, as can be seen from Table XXIV.
It is not impossible for a fibrous stricture to formduring the course of a first attack, and there was onesuch case in the present series, confirmed at surgicaloperation. Once the disease has become chronic, astricture may become apparent at any time and one-third of the cases in the present series were diagnosedwithin five years of the onset of the ulcerative colitis.Patients with the chronic continuous form of thedisease are more liable to stricture than those with thechronic intermittent form: but caution is necessaryin the interpretation of this finding, because thepresence of a stricture will itself cause chronicdiarrhoea, and it is therefore difficult to distinguishbetween cause and effect unless repeated bariumenema examinations have been made throughout thecourse of the disease.Whenever a stricture is found, the possibility of
carcinoma must be considered, but many of thestrictures are fibrous with no evidence of malignancy.They are most frequent in the rectum and sigmoidcolon but may occur in any part of the colon; theyare occasionally multiple. A fibrous stricture isalmost always an indication for surgical treatment,if only because the possibility of carcinoma mustexist whenever a stricture is found and it is necessaryto resect the lesion and to carry out histologicalexamination before the distinction can be made withcertainty.
Illustrative case history Mrs. J. M. was first seen at theRadcliffe Infirmary in 1959, when she presented in herfirst attack of ulcerative colitis at the age of 37 years.The disease pursued an intermittent course over the nexttwo years and during this time she received treatment withlocal and systemic steroids. In April 1961 a stricture ofthe recto-sigmoid junction was diagnosed and the fol-lowing operations were then performed: double-barrelledileostomy (April 1961), resection of the sigmoid colonand upper rectum, with end-to-end anastomosis (May1961), and closure of the ileostomy (August 1961).Pathological examination confirmed the fibrous nature ofthe excised stricture.
While the bowel was uncoupled, the colon was irrigatednightly with local hydrocortisone solution. After the finaloperation her symptoms were much less severe and allsteroid therapy was stopped some weeks before discharge.Since then she has been seen regularly as an out-patient,and when last seen was in good health.
3
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

Felicity C. Edwards and S. C. Truelove
g.,
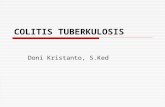
FIG. 13. Pseudo-polyposis affecting the left half of thecolon.
PSEUDO-POLYPOSIs This is a consequence of severeulcerative disease. The mucosa between the ulcera-tions becomes much swollen and raised above thegeneral surface. Alternatively, the ulcerations may bethe site of exuberant granulation tissue, which islater epithelialized. The condition can occur rapidlyand is not infrequent during the first attack of thedisease. It is most likely to occur in a severe attackof the disease, especially when the whole colon isinvolved, but the left half of the colon is the moreliable to show pseudo-polypoid change and some-times the process stops short at a particular point inthe colon (Fig. 13). Once developed, the conditionis likely to persist, but this is not invariable and com-plete regression to normality can occur over thecourse of time.
It is sometimes supposed that pseudo-polyposismay be a precancerous change. There appears to beno good evidence for this except that this complica-tion is a measure of severe disease and may thus bean indirect indication that cancer of the colon isspecially liable to occur. In the present series, onlyone patient with cancer of the colon complicatingulcerative colitis was known to have pseudo-poly-posis preceding it.The condition is not, in itself, a firm indication for
colectomy.
PERFORATION OF THE COLON This is the most danger-ous local complication of the disease. The colondoes not form adhesions in ulcerative colitis and theconsequence is that, if perforation does occur, itusually results in a generalized faecal peritonitiswhich is extremely dangerous. The complication isoften hard to recognize because. although there aresometimes the classical signs of a perforation, thecondition may produce few local signs and the onlyindication that some disaster has occurred is amarked deterioration in the general condition of thepatient. In any case of doubt, an immediate plainx-ray examination should be made. When the patientis gravely ill, he should be examined by portablex-ray machine on his own bed; it is best to use ahorizontal beam with the patient lying on his leftside. so that any free gas between the right lobe ofthe liver and the thoraco-abdominal wall can beseen. The same film will also show if there is dilata-tion of the colon (see acute dilatation of the colon,below).
Perforation of the colon is specially liable to occurin the first attack of the disease. In the present series,among the 20 patients who suffered from perfora-tion, there were 13 who developed this complicationin the first attack. From our own data, perforationappears to be the only local complication with such amarked tendency to occur in the first attack.The risk of perforation varies greatly according to
the clinical severity of the attack of ulcerative colitis.In the present series the majority of perforations(16 cases) occurred in severe attacks, a few occurredin attacks classed as moderately severe (four cases),and none in attacks which were mild.The common site of perforation was the sigmoid
colon. The sites of perforation were as follows:Sigmoid colon 12Descending colon 4Caecum 2Terminal ileum IMultiple sites (caecum, splenic flexure and descending colon) I
One of the supposed dangers of corticosteroidtherapy is that it may increase the risk of perforationof the colon. It is therefore important to record thefact that there has been no increase in the frequencyof colonic perforation in the present series since theintroduction of cortisone in 1952. If we confine our-selves to first attacks, when the population at risk isprecisely known, and if we also exclude all mildattacks, none of which proceeded to perforation,we are left with the following data for severe andmoderately severe attacks in relation to pre-cortisoneand post-cortisone eras:
No. ofPatients in First Attack with Severeor Moderately Severe Disease
1938-521953-62
ANo. withPerforation
59 8 (13-6%)55 5 (9 1%)
4
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
Perforation of the colon may be preceded bydilatation of the colon although often perforationoccurs without any such premonitory manifestation.In fact, in the present series, only one patient de-veloped perforation in association with severe
dilatation of the colon.Three-quarters of the patients who developed
colonic perforation died. On studying our data, twosalient facts emerge. First, there is the difficulty ofrecognizing the condition in life, because in half thepatients with perforation in the present series, thecomplication was diagnosed only at post-mortemexamination, and the possibility of colonic perfora-tion had not been entertained by the physician duringlife. This emphasizes that plain x-ray examinationwith the patient in his own bed is an importantdiagnostic tool in any patient admitted in a severe
attack of ulcerative colitis. Secondly, if emergencycolectomy is to be performed, it must be carried outwithout delay, because death occurs quickly after a
colonic perforation. Only five patients were treatedby emergency surgery but three of them survived, incontrast to only two survivals among 15 patientstreated conservatively. Even though an emergency
colectomy is a hazardous operation in a patientwho is already gravely ill, it offers the best chance ofsurvival.
Illustrative case history Mr. W. H., aged 64, was
admitted to the Radcliffe Infirmary on 9 October 1962 inhis third attack of ulcerative colitis, having had symptomsfor the previous six weeks. The attack was severe andthere was evidence that the disease affected the bowelfrom the transverse colon onwards. He was treated withlocal and systemic corticosteroids in addition to generalmeasures and blood transfusion, and showed some im-provement over the next three weeks. On 30 October hecomplained, on waking, of feeling particularly unwell,but the possibility of perforation was not considered owingto the absence of more specific symptoms. Later in themorning his condition deteriorated and he complainedof pain in the left iliac fossa. Localized tenderness andguarding were found, bowel sounds were absent, and a
plain radiograph showed the presence of free gas in theabdomen. It was decided that laparotomy should be doneat once, and operation revealed a perforation in the regionof the splenic flexure. A subtotal colectomy with terminalileostomy was performed. He recovered steadily withoutcomplication and, after his general health had improvedsubstantially, the rectum and remaining sigmoid colonwere removed by combined abdomino-perineal excision.
ACUTE DILATATION OF THE COLON Ten patients hadevidence of marked dilatation of the colon, a com-
plication which has sometimes been termed 'toxicmegacolon' (Roth, Valdes-Dapena, Stein, andBockus, 1959). The attack of ulcerative colitis inwhich this occurred was usually severe. Acute dilata-
tion of the colon may occur in either a first attack ora relapse of the colitis and is regarded as a dangerouscomplication, because it is thought to be a sign ofimpending perforation. In the present series only onepatient was treated surgically; of the remaining ninepatients, three died, but in one case death occurredshortly after admission to hospital. Of the threedeaths, post-mortem examination in two patientsshowed that there was no perforation, and in thethird, in whom there was no necropsy, there was noclinical evidence of perforation.During recent years the importance of potassium
deficiency has been appreciated as a cause of intes-tinal dilatation and paralysis, but some of our casesdate from before this era and potassium studies werenot made in them. Another known factor in theaetiology of the condition is the excessive use ofanticholinergic drugs. Some authorities regard theoccurrence of acute dilatation of the colon as anindication for immediate emergency colectomy;however, the present series shows that some casescan be managed conservatively with success. If aconservative approach to treatment is contemplated,it is first essential to take plain radiographs to excludethe presence of free gas as a sign of perforation of thecolon, which usually calls for emergency colectomy.Blood electrolytes should be estimated, and anytreatment with anticholinergic drugs stopped atonce. Neither food nor drink should be given bymouth, and intubation of the gastrointestinal tractshould be performed to enable gastrointestinal suc-tion to be carried out. Control of water and electro-lyte balance is achieved by intravenous therapy, andglucose and other suitable foods should also be givenparenterally.
Illustrative case history Miss A. F. developed ulcera-tive colitis in 1952 at the age of 18, and subsequently hadseveral attacks. She was admitted to this hospital in 1960in a severe relapse. Diarrhoea had begun two weeks pre-viously and for the week immediately before admissionshe had, in addition, abdominal pain, anorexia, andvomiting. On examination she was feverish and ill andthe abdomen was very tense with slight tenderness in theleft iliac fossa. A plain radiograph showed a greatlydilated colon with mucosal changes consistent with wide-spread colitis. There was no evidence, either on admissionor subsequently, of free gas in the peritoneal cavity. Shehad not been treated with anticholinergic drugs and herserum potassium level was not lowered. It was decidedto treat her conservatively and she slowly improved underthe regime outlined above. Local and systemic corti-costeroids were given to supplement the general measures.Blood electrolyte estimations and radiographs were re-peated at frequent intervals throughout her illness and,although one month after admission a plain radiographshowed that there was still considerable colonic dilata-tion, her general condition continued to improve and she
5
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

Felicity C. Fdwards and S. C. Truelove
was discharged a few weeks later. She has since beenseen regularly as an out-patient; there have been no re-currences and she is at present in very good health.
MASSIVE HAEMORRHAGE We define as a massivehaemorrhage in this disease a sudden bleed demand-ing urgent blood transfusion or continued heavybleeding demanding massive transfusion. When sodefined, massive haemorrhage is not a frequent com-plication (21 cases). It can usually be treated success-fully by blood transfusion but exceptionally it is anindication for emergency colectomy.
Illustrative case history Mrs. R. W. was admitted tothe Radcliffe Infirmary in 1957 in her first attack ofulcerative colitis. She was 34 years of age and was severelyill. The disease affected the whole colon and sigmoidoscopyshowed a markedly inflamed and haemorrhagic mucosa.Her stay in hospital was notable for numerous episodesof exsanguinating haemorrhage from the bowel, all ofwhich required immediate massive transfusion. Six weeksafter admission, following one of these episodes, she com-plained of pain in the left iliac fossa. Local tendernesswas present, but there was no evidence of free gas in theperitoneal cavity. Her general condition remained fairlygood and it was considered that, as this might be a per-foration resulting in a localized pelvic abscess, she shouldbe treated conservatively with parenteral antibiotics inaddition to the other treatment she was then receiving.She improved steadily after this further setback, butshortly afterwards had another very severe haemorrhagefor which she received further urgent and repeated trans-fusions over the next few days. During her admission,which lasted for five months, she received a total of 64pints of whole blood. Her treatment otherwise consistedof general measures, A.C.T.H., and both systemic andlocal corticosteroids. Aftei discharge, she had one furtherrectal haemorrhage which responded rapidly to bloodtransfusion and corticosteroid therapy. Apart from this,she has remained in uninterrupted good health.
CANCER OF THE COLON This complication hasoccurred in 22 patients (3 5 %) of the present series,with death in 17 of them. The complication is soimportant that it is dealt with separately in Part IV.
REMOTE OR SYSTEMIC COMPLICATIONS
ERYTHEMA NODOSUM This is well recognized as acomplication of ulcerative colitis and fairly oftenoccurs in association with arthritis. There were 14patients in the present series who developed ery-thema nodosum, and all but one of them werewomen, a sex difference which is statistically signi-ficant. However, erythema nodosum is known to bemore frequent in women than in men when it occursapart from ulcerative colitis, so the marked sexdifference in this disease may not have any specialsignificance. Three patients in the present series had
an attack of erythema nodosum before the onset ofthe ulcerative colitis. In all but one of the remainder,the erythema nodosum coincided with a frank attackof ulcerative colitis, either the first attack or a re-lapse, while the one exception had the erythemanodosum two weeks before a relapse. Sometimesthere are repeated attacks of erythema nodosum,and there were three such patients in the presentseries; in these patients, the erythema nodosum co-incided with frank attacks of colitis.
Illustrative case history Miss M. S. was first seen at theRadcliffe Infirmary in 1940, when she presented in herfirst attack of ulcerative colitis at the age of 17 years.This attack was severe and the distal colon was affected.She was treated with general measures and transfusionbut showed little improvement. She was still in hospitalfive months after admission when she developed erythemanodosum of both shins and, a few days later, an acutearthritis affecting the right elbow and wrist. These mani-festations eventually subsided but she continued to havesymptoms of colitis and two months later a second cropof lesions typical of erythema nodosum appeared.Throughout the whole of this admission she was veryill, with high fever and a much raised sedimentation rate.Her condition slowly improved and she was dischargedsome months later, although she had not gone into fullclinical remission.
In 1946 she was readmitted in a sharp relapse and hadat that time effusions into both knee joints and erythemanodosum of the legs and forearms. Since then she has hadcontinuous bowel symptoms of varying severity, but hashad no further attacks oferythema nodosum. She has hadno medical supervision since 1946 and when seen by us in1962 refused investigation and treatment, but it is almostcertain, from her appearance and history, that she hasgradually developed a severe degree of ankylosingspondylitis over the last 15 years.
PYODERMIA GANGRENOSUM This rare and seriouscondition is virtually confined to ulcerative colitisand there were four such cases in the present series.The essential lesion is an intra-epidermal bulla
which is filled with a sterile milky fluid containinginflammatory cells. The surface of the bulla breaksdown and scabbing occurs, sometimes with second-ary infection. The bullae may be numerous andoften coalesce so that the final result is an extensivearea of scabbing, which may become gangrenous.The condition is usually a complication of a severe
attack of ulcerative colitis and is attended by markedconstitutional symptoms. although it is hard toseparate these from those of the colitis. The essentialin treatment is to control the ulcerative colitis, eitherby corticosteroids or by colectomy; successful treat-ment of the colitis by either of these methods resultsin healing of the skin.Although typically an acute complication, the
condition may exist in a chronic form for months or
6
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
years, even when the symptoms of colitis are absentor slight. One such case occurred in the series andwe have seen another recently.
Illustrative case history Mrs. E. W. developed ulcera-tive colitis in 1952 when she was 25 years old. Followingher first attack she had many relapses, which were oftenassociated with arthralgia and which responded to steroidtherapy. During her second pregnancy, in 1957, she hadanother relapse of the colitis, during the course of whichshe developed a deep vein thrombosis of the right leg.Superficial ulceration of the leg, which later progressedto pyodermia gangrenosum, subsequently occurred, butimmediately after delivery of her child both the colitisand the skin lesion improved greatly. However, a fewweeks later there was a recurrence of ulceration and, sometime afterwards, of the colitis. This relapse was treatedwith systemic corticosteroids in addition to generalmeasures and, as the colitis improved, the ulcerated areaon the leg healed. However a widespread crop of vesicles,particularly marked on the scalp, ears, and legs, then ap-peared. The vesicles coalesced and burst, to be replacedby extensive scabbing. All these lesions, which were typicalof pyodermia gangrenosum, rapidly progressed and hergeneral condition greatly deteriorated. Rectal hydrocorti-sone was added to the existing treatment, but no improve-ment occurred. Colectomy was seriously considered, butit was decided to try first the effect of very large doses ofsteroids. Accordingly, she was given 240 mg. of prednis-olone daily and she responded dramatically. The diarrhoeaquickly improved her general condition began to re-turn to normal, and the skin lesions began to epithelialize.She was kept on this high dose of prednisolone for fourweeks, and it was then reduced to a smaller maintenancedose for several more weeks. Healing of all the lesionscontinued steadily and there has been no recurrence ofthis complication. She was discharged in full clinical re-mission and she is at present in good health, although shehas had one relapse of the colitis in the intervening period.
OTHER SKIN LESIONS These are numerous anddiverse; 99 patients were affected, some with morethan one type of lesion. In 13 patients the skincondition preceded the colitis, while in 86 patients itoccured either at, or after, the onset of the colitis.In 24 of these 86 cases the two conditions were con-sidered to be unrelated, while in the remaining 62patients skin lesions developed in relation to attacksof colitis.A variety of skin reactions was noted in this latter
group. In eight patients generalized rashes, mainlyurticarial, were attributed to drugs (usually sulphon-amides) or to serum sickness. Some patients de-veloped mild forms of dermatitis, or macular andpapular rashes. The largest group (13) had wide-spread erythematous lesions of varying severity andan additional three patients had definite erythemamultiforme. Seven patients suffered from pustularrashes, four from superficial boils and abscesses,
while three had erysipelas. The remainder developedvesicular rashes, ulceration, eczema, abnormalities ofpigmentation, or affections of the hair and nails.
Eighteen patients developed arthritis, eye lesions,or aphthous ulceration of the mouth at the same timeas the skin condition.
ARTHRITIS This is a commoni complication of thedisease. The usual form is a polyarthritis, which mayaffect either large or small joints. Involvement of asingle large joint is fairly common. Sometimes thecondition closely resembles rheumatoid arthritis,but it is known that the Rose-Waaler test is usuallynegative in the arthritis of ulcerative colitis (By-waters and Ansell, 1958; Wright and Watkinson,1959). There is often an effusion into the affectedjoints, but aspiration shows this to be sterile. Thecondition usually complicates a frank attack ofulcerative colitis but occasionally may precede theonset of the disease, and also may occur duringperiods of clinical remission.When the colitis is treated effectively, the arthritis
subsides. Corticosteroids have transformed medicaltreatment for the better in this respect. It has beensaid that 'arthritis and iritis constitute urgent indica-tions for removal of the bowel' (Brooke, 1954) butthis can no longer be regarded as a valid assessment,although some patients with arthritis may be foundto require colectomy.
Thirty-five patients developed such an arthritis,which almost always coincided with either a firstattack or a relapse of the colitis; in slightly less thanhalf the cases the arthritis occurred simultaneouslywith erythema nodosum, aphthous ulceration, con-junctivitis, or a rash.
ANKYLOSING SPONDYLITIS This is less common thanarthritis but is nevertheless not rare. Our presentfigure of 180% is certainly an underestimate of thefrequency of the complication, because it covers onlysevere cases, and special study of patients with ulcera-tive colitis with this complication in mind revealsthat early and minor changes of ankylosing spondy-litis are fairly frequent. Whereas there is a heavypreponderance of male subjects when ankylosingspondylitis occurs in the absence of ulcerative colitis,the male: female ratio being about 10:1, in thisdisease the men are only about twice as frequentlyaffected as the women.
In some patients, the ankylosing spondylitis pre-cedes the symptoms of ulcerative colitis, as has beenpointed out by Acheson (1960). There were threesuch patients in the present series.
Illustrative case history Miss M. D. was 28 years oldwhen she had her first attack of ulcerative colitis in 1940
7
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

Felicity C. Edwards and S. C. Truelove
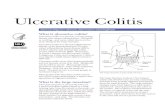
FIG. 14. Ankylosing
spondylitis in a woman
with chronic ulcerativecolitis.
a..s r...fl.e..c.... :Yr
;.H. .. .... ..l... .
* '.
.... ............;:.:.
*
;.
.... ::...--.:..... ...::'~.........
t:....... .x.
Shortly after she had recovered she had an attack ofiritis which was later followed by a recurrence of bowelsymptoms. Intermittent diarrhoea continued over thenext three years and in one relapse an appendicostomywas performed and the bowel irrigated. In 1943 she hadtwo more attacks of iritis and for the first timheI noticedpain and stiffness of her back. These symptoms worsenedand her back began to become fixed. In 1945 and 1946she had two courses of deep x-ray treatment to the back,with some symptomatic relief. The colitis was largely in-active at this time, but in 1948 a fourth attack of iritis oc-curreandextin 1950 she again experienced troublesomediarrhoea. She was referred to the Radcliffe Infirmaryfor the first time in 1951 and advanced ulcerative colitisinvolving the whole colon was found. A severnsieeane ofankylosing spondylitis was present and she experiencedalso, at that time, an attack of erythema nodosum andone of arthritis of the ankles. From 1952 onwards shehas had extensive medical treatment for the colitis butthis has continued to relapse, although less frequentlyand severely than during the first years of her illness.The spondylitis remained unchanged (Fig. 14) and thelast radiograph, taken in 1960, showed extensive ankylos-ing spondylitis of the cervical, dorsal and lumbar spine,with marked bony fusion of the lumbar vertebrae.
EYE LESIONS These are common complications ofulcerative colitis. They were slightly more commonin the women (8-9 %) than in the men (566%) of thisseries but this small difference is probably of littleaccount. Conjunctivitis is common, as are iritis andother forms of uveitis. Repeated attacks of the eyecomplication, usually coincident with frank attacks
of the colitis, are a special feature. These eye com-plications may also coincide with other remotecomplications of the disease, notably arthritis, skinlesions, and aphthous ulceration of the mouth.Once again, our figures for this group of complica-
tions are almost certainly an underestimate, and thisissue is being studied at present by our colleagues.The majority of patients with eye lesions had eitherconjunctivitis or iritis, two patients having both dis-orders. Conjunctivitis occurred in 20 patients, in allbut three of them in direct association with an attackof colitis. Thirteen patients had one or more attacksof iritis and in three cases the first attack of iritispreceded the onset of ulcerative colitis. The remainingeye lesions were few: corneal ulceration, keratitis,blepharitis, and Sjogren's syndrome were the chiefexamples.
LIVER DISEASE The relationship between ulcerativecolitis and liver disease is complex.
Transient hepatitis is fairly frequently associatedwith ulcerative colitis. Some patients have a pasthistory of an attack of jaundice (presumably in-fective hepatitis from the available evidence) whenthey develop ulcerative colitis and there were 14such patients in the present series. Three otherpatients gave a history of an attack of jaundice, alsopresumed to be infective hepatitis, that was followedimmediately by the first symptoms of the colitis.The remaining 13 patients developed temporaryhepatitis at varying times after the onset of thecolitis.
There is often the possibility that such attacks ofhepatitis are examples of homologous serumjaundice following blood transfusion and no diag-nostic methods are yet available for establishing thishypothesis; two of the 13 cases developed jaundiceat an appropriate interval after blood transfusion.Two other patients developed jaundice during chlor-promazine therapy, and were judged on the basis ofinvestigations to be examples of drug-induced chole-static hepatitis. Finally, one other patient was work-ing with toxic chemicals in a factory and the jaun-dice was attributed to this.
In the remaining eight patients, no predisposingfactor other than the ulcerative colitis could be foundto account for the hepatitis. The precise reasons forthis association remain to be determined but severaldistinct possibilities exist. First, ulcerative colitis mayrender the subject unduly prone to infective hepatitis.Secondly, the temporary hepatitis may be directlydue to the ulcerative colitis, because liver biopsystudies have shown various abnormalities during acuteattacks of ulcerative colitis in the majority of subjects(Kleckner, Stauffer, Bargen, and Dockerty, 1952;Brooke, Dykes, and Walker, 1961), and Brooke and
8
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
Slaney (1958) have been able to culture bacteria fromthe portal blood of the patients undergoing colec-tomy for the disease. Finally, some workers haveconsidered both the hepatitis and the colitis to beseparate manifestations of an auto-immune disease,especially as the sera of ulcerative colitis patientsmay give auto-immune reactions against liver as wellas against colon (Broberger and Perlmann, 1959;Broberger, 1961).
In a similar way, there is a definite relationshipbetween ulcerative colitis and chronic liver disease(usually cirrhosis) but the underlying mechanismsare not yet understood. In the present series, therewere 16 cases of chronic liver disease, which is a fargreater number than would be expected by chance.Sometimes the liver disease develops after the onsetof the colitis but it appears to be equally common forulcerative colitis to develop as a complication ofchronic liver disease; in the present series, there wereeight patients in each of these two groups. The com-bination of ulcerative colitis and chronic liver diseaseis dangerous and 11 of these 16 patients are alreadydead. In effect, this small group has contributed 10%of the total deaths in the whole series of 624 patients.Case histories to illustrate the two distinct patterns
are given below:-
Illustrative case history 1 Mrs. M. C. had her firstattack of ulcerative colitis in 1939, when aged 30 years.She subsequently suffered from the chronic intermittentform of the disease. She was under medical supervisionfrom 1947 onwards, when a stricture of the rectum wasdiagnosed, but the colitis did not improve. She was firstreferred to this hospital in 1951 when, at the age of 42, shehad experienced for the first time a transitory episode ofjaundice associated with pain in the right hypochondrium.She was found on examination to have a grossly enlargedliver and spleen, and there was evidence of long-standingulcerative colitis involving the whole colon. Cholecyst-ectomy and terminal ileostomy were performed; thethickened contracted gall bladder contained purulentfluid and when examined microscopically showed chronicatrophic cholecystitis. Biopsy of the liver showed chroniccholangiohepatitis. She recovered from the operationsbut over the next three years had persistent jaundice withfrequent intestinal haemorrhages and a progressivetendency to bruise easily. A barium swallow done in 1955showed oesophageal varices and she had a well-markedcaput medusa around the ileostomy stoma. A liverbiopsy obtained in the same year showed severe post-necrotic scarring with extensive fibrosis. An attempt tolower the portal venous pressure was made in 1955, by thenow out-moded Talma-Morrison operation, but shedied a few months later after a particularly severe haemor-hage from the ileostomy.
Illustrative case history 2 Mrs. A. S. was perfectlywell until 1943, when, at the age of 20 and during thecourse of her first pregnancy, she developed jaundice.Thiscleared after a few weeks, only to recur in the weeks fol-.2
lowing premature delivery of a stillborn child. She wasthen well until 1944, when exactly the same sequence ofevents occurred during and after her second pregnancywhich terminated in a full-term normal live birth. By 1945the jaundice had faded and she remained well until 1946,when her third pregnancy was associated with severepruritus, pale stools, and bile in the urine. Liver functiontests showed some evidence of liver damage and the liverwas found to be enlarged. She was discharged after thebaby was born and was not seen again until her secondadmission in 1949. She had had pruritus continuallysince 1947 and jaundice had returned in 1949. She hadalso passed some blood per rectum but no cause wasfound for this. She had a high sedimentation rate andhepatosplenomegaly at this time.
She developed severe bloody diarrhoea and colic in1951, and also had piles and marked anaemia. The diar-rhoea lasted for five months during which time she be-came very oedematous, with a low serum albumin level,and had several small haematemeses. Throughout 1952she had mild episodic jaundice and was next seen in 1953with a recurrence of bloody diarrhoea, oedema andascites, associated with fever. She was severely anaemicand several spider naevi were noted. The hepatosplenome-galy remained unchanged. She was treated with bloodtransfusion, antibiotics, vitamins, and corticosteroids,but her condition steadily deteriorated. She died in 1954in hepatic coma associated with a marked exacerbationof intestinal bleeding.
Necropsy showed advanced cirrhosis of the liver withpost-necrotic scarring, oesophageal varices, and severeulcerative colitis involving the whole colon with theexception of the sigmoid colon and rectum. It was coii-sidered that the original illness was infective hepatitis andthat recurrent subacute hepatitis had progressed to cir-rhosis.
RENAL DISEASE There were 29 patients in the serieswith renal disease. In 12 patients this preceded theonset of the ulcerative colitis and there appeared tobe no relationship between the two conditions. Ofthe remaining 17 patients, the biggest group sufferedfrom renal infection, there being six cases of pyelitisand four of chronic pyelonephritis. All except two ofthese 10 patients were women. The only otherexamples worth noting were two cases of uretericobstruction with subsequent pyonephrosis, due tocarcinoma of the colon, and two cases of temporaryrenal failure after colectomy.
In effect, the association between ulcerative colitisand serious renal disease is not marked.
PULMONARY EMBOLISM Of the 10 patients withpulmonary embolism in the present series, nine werewomen, whereas in the hospital population as a wholethe condition affects both sexes equally (Morrell,Truelove, and Barr, 1963). It is of interest that nocases were recorded in this series before 1950, andthere is therefore the possibility that the use of cor-
9
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

10Felicity C. Edwards and S. C. Truelove
ticosteroids has increased the risk. Hmonary embolism has become increasirin the total experience of this hospital didecade and its increased occurrencecolitis may be no more than a reflection
In each case, the pulmonary embosociated with a frank attack of ulceratilatter being either severe (five cases) osevere (five cases); in one instance t]occurred two days after total colectomy.The range of ages affected was wide,
patient being 18 and the oldest 76, butpatients were under 45 years of age.Pulmonary embolism was the immed
death in five instances, and it is pernexpected that three of these patientsolder age group, their ages being 59, 69,
Clinical signs of peripheral venouspreceding the pulmonary embolism wparent in half the patients, althoulrevealed the presence of ante-morterthrombosis in an additional three cases.that some deaths could have been av4use of anticoagulant therapy. Anticoaused, in this small group of cases, in (
stance (a patient who recovered) and tthe management of venous thrombosiscolitis will be discussed in the next secti
VENOUS THROMBOSIS OF LEGS This iscomplication of ulcerative colitis, thepatients so affected in the present series.at any stage of the disease and there is 1that corticosteroid therapy has influeicidence. If we confine ourselves to first a
disease in order to define the populatioiprecision, we have the following datacortisone and post-cortisone eras:
No. of Patientsin First Attacks
1938-521953-62
108142
This is in contrast to the appareninumber of pulmonary embolisms durdecade, as mentioned in the preceding:.The question of employing anticoagu
arises whenever a leg vein thrombosis i:It is our personal experience that theulcerative colitis is not a contraindicaform of therapy, although it may increablood from the bowel. Pulmonary em
dangerous that this risk of increased blcthe bowel is worth accepting because jbe well established that anticoagulantleg vein thrombosis greatly diminishes
lowever, pul-ngly commonuring the pastin ulcerativeof this trend.lism was as-ve colitis, ther moderatelyhe embolism
the youngestseven of the
liate cause ofzaps not un-were of anand 76 years.i thrombosisrere only ap-gh necropsy
developing pulmonary embolism and renders it lessdangerous if it does occur (Barritt and Jordan, 1960).In the present series, anticoagulant therapy was usedin 10 patients with leg vein thrombosis and none ofthem sustained a pulmonary embolism. If we excludethree patients who died from pulmonary embolismwithout preceding clinical recognition of leg veinthrombosis, we have the following data:
No. ofPatients No. ofPatientswith Leg Vein with PulmonaryThrombosis Embolism
With anticoagulantsWithout anticoagulants
1027
05 (18 5 %)
No firm conclusion can be drawn from this in-formation in view of the small numbers but thefindings are in the direction which suggests that anti-coagulants should be used.
n deep vein APHTHOUS ULCERATION OF THE MOUTH This is aIt is possible common complication of ulcerative colitis (51oided by the patients in the present series) and is frequently severevgulants were during an acute attack. The pain of severe aphthousonly one in- ulceration is often so extreme that it impedes eatingtheir place in and drinking and so may cause difficulties in thein ulcerative management of the colitis. Local hydrocortisone ap-on. plied to the mouth as a mouthwash is sometimes
beneficial in promoting rapid healing. Care must bea common taken not to miss an associated moniliasis if this
are being 40 treatment is being employed. Such attacks of severeIt may occur aphthous ulceration frequently recur whenever theittle evidence subject has an attack of the colitis.nced the in- Aphthous ulceration was more commonly asso-tttacks of the ciated with severe attacks of colitis (25 patients) thann at risk with with moderate (11 patients) or mild attacks (sevenfor the pre- patients). Five patients had ulceration while in re-
mission, and one patient developed aphthous ulcersafter colectomy. In five cases ulceration occurred
No. with Leg some time -before the onset of the colitis. Of the 51Vein Thrombosis patients, 11 were known to have recurrent bouts of
5 (4 6%) mouth ulcers. In only four cases was moniliasis7 (4.9 %) noted.
t rise in theing the past MONILIASIS Moniliasis of the mouth and throat issection. not very common. Its importance lies in the fact thatilants always in some patients extensive or generalized moniliasisvs recognized. may supervene and these forms of the disease arepresence of very dangerous. For this reason, moniliasis of the
ation to this mouth should immediately be treated with NystatinLse the loss of tablets to suck and these are usually effective.ibolism is so Generalized forms can also be treated with Nystatin,)od loss from either locally or systemically. If this is not rapidlyit appears to successful, Amphotericin B should be employedtreatment of parenterally.s the risk of Oral moniliasis was recorded in 11 patients, and in
10
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
three of these cases there was extensive spread. Mostcases occurred in the course of severe attacks ofcolitis. Of the three patients with generalized monilia-sis of the gastrointestinal tract, two recovered aftertreatment with the antifungal agent, Nystatin, whileone patient died (see below).
Illustrative case history Mrs. E. C. was in good healthuntil the age of 43 when she had a large bowel intussuscep-tion, which was treated with a permanent left iliaccolostomy. She remained in good health until 1953, when,at the age of 53 she had her first attack of ulcerativecolitis. During the following two years she had recurrentattacks of colitis, and was first seen at this hospital in 1955when she was admitted in a moderately severe relapse.There was evidence of widespread colitis with maximalchanges in the right half of the colon and the rectum.During this admission she received systemic corti-costeroids in addition to general medical measures andwas discharged after four weeks showing very littleimprovement. A few days later she developed an ex-tremely sore throat and mouth, with marked pain onswallowing and severe anorexia; she continued to havesix to eight actions of the colostomy daily, the materialconsisting mainly of blood and mucus, and she was re-admitted 12 days after discharge. On examination themouth and throat were affected with thrush, some oralulceration was present, and there was right-sided ab-dominal distension and tenderness. Swabs from the mouthgrew Candida albicans and B. aerogenes, while culture ofthe colostomy discharge yielded yeasts and C. albicans.She was unable to take food and oral drugs, and was givenintravenous saline to correct salt depletion and bloodtransfusions; these were supplemented by parenteralvitamins and Ferrivenin. She received A.C.T.H. dailythroughout this admission, but apart from gentian violetapplications to the mouth did not receive any treatmentfor the moniliasis. Although the oral moniliasis appearedto improve during the last few weeks of her admissionshe still could not take nourishment by mouth. She dis-charged herself, against medical advice, seven weeks aftershe had been readmitted and died two weeks later athome.Her general practitioner recorded that -the moniliasis
had continued and that she had died, in effect, frommalnutrition secondary to this.
OSTEOPOROSIS Osteoporosis was diagnosed in ninecases. This must be regarded as an underestimate ofits true frequency, which would only be determinedby systematic studies. Among these nine patients,the majority (seven) were women; and six of the ninewere over the age of 60 years when osteoporosis wasdiagnosed. There were only two patients under theage of 45 and it may be of significance that both ofthem had been treated with corticosteroids. Amongthe older patients, only two out of seven had pre-viously received corticosteroid therapy.
In six cases, the osteoporosis was purely a radio-logical diagnosis and there were no gross clinical
effects; but in the remaining three, obvious clinicalmanifestations were present, namely, fracture-collapse of a lumbar vertebra, collapse of cervicalvertebrae with neurological symptoms and signs,and generalized aches and pains.
DISORDERS OF THE BLOOD
We include under this heading both anaemia second-ary to ulcerative colitis and other miscellaneousblood disorders.
ANAEMIA SECONDARY TO LOSS OF BLOOD Ulcerativecolitis may produce, as one of its more frequentcomplications, an anaemia of very variable severity.Persistent or recurrent loss of blood from the bowel,which may be the chief feature of the diarrhoea, orwhich may be so mild as to escape attention, will inalmost all cases lead eventually to an iron-deficiencyanaemia unless corrective measures are taken. It isprobable that a far greater proportion of patientswith chronic ulcerative colitis are kept undermedical supervision at the present time than wasformerly the case and so the extremely low levels ofhaemoglobin that used to occur are nowadays rarelyseen. However, a severe degree of anaemia oftenarises in a surprisingly short time during the courseof an acute attack of colitis, even in the absence ofany frank episode of severe bleeding from the bowel.Various predisposing factors may also be present, ascomplications of the primary disease, and contributesubstantially to the development of anaemia. Bloodmay be lost from carcinoma of the colon or rectum,or from associated haemorrhoids; and, among moreremote complications, chronic hepatic or renallesions may be important contributory causes.We have defined anaemia as a haemoglobin level
of 60% (9 0 g.) or less, occurring at any time duringthe course of the illness. Even having adopted such astringent definition, we have found that 127, or 20-4%of the whole series of 624 patients, fulfilled thiscriterion. Haemoglobin levels between 60% and 80%were so common as to be almost universal.The majority of the patients with anaemia had a
hypochromic anaemia with evidence of moderate orsevere iron deficiency. In some cases, particularlythose occurring after isolated severe attacks of colitisinvolving heavy bleeding, the anaemia was normo-chromic at first. Studies employing red blood cellstagged with radioactive chromium have revealed thatthere is frequently a substantial loss of blood in thefaeces in ulcerative colitis even if the symptoms aremild and in some cases when the patient is entirelysymptom-free (Beal, Skyring, McRae, and Firkin,1961).Table XXVI shows the distribution of patients
11
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

Felicity C. Edwards and S. C. Truelove
TABLE XXVIDISTRIBUTION OF PATIENTS ACCORDING TO SEVERITY OF
* 1t I _ *1 >_w * -- - e%l
Blood Disorder
ANAEMIA SECONDAKY 10 LOSS OF BLOOI
Haemoglobin(%)
<2020-2930-3940-4950-60Total with valuesof 60% and below
No. ofPatients
M(251) F (373) Whole
3
1225
391360
L} Heinz body anaemiaIdiopathic thrombocytopenic purpuraNon-thrombocytopenic purpura
Series (624) Pernicious anaemia
I Christmas disease4 Acquired haemolytic anaemia (auto-immune type)
1t2 Anaemia associated with polyarteritis nodosa2585
42 (16-7%) 85 (22-8%) 127 (20-4%)
classified according to the lowest haemoglobin levelrecorded at any time during their colitis. It can beseen that 42 patients (25 women and 17 men) had a
severe degree of anaemia, with haemoglobin levelsbelow 50%, while, of these, 12 women and five menhad levels below 40%.
It is noteworthy that in 13 of these 17 patients theanaemia had arisen before 1946, and that severeanaemia has become unusual during the past decadein spite of the far greater number of patients seen.
It is also noteworthy that nine of these 17 cases ofsevere anaemia developed this state within the firstyear of the onset of the disease. Indeed the chanceof developing anaemia, as we have defined it with ahaemoglobin level of 60% or less, appears to bemaximal in the first year of the illness and to becomesteadily less likely to arise, although this may reflectmedical treatment more than the natural history ofthe disease (Table XXVII).
TABLE XXVIINUMBER OF PATIENTS DEVELOPING ANAEMIA SECONDARY TO
LOSS OF BLOOD IN RELATION TO THE LENGTH OF HISTORYOF ULCERATIVE COLITIS
Length of History of Ulcerative Colitisbejore Diagnosis o0 Anaemia (yr.)
<I1-
2-3-4-5-9 (average annual number)10-19 (average annual number)20-29 (average annual number)
No. of PatientsDeveloping Anaemia
3418108
Severe anaemia due to blood loss demands bloodtransfusion. Less severe grades can be treated suc-cessfully with iron, which sometimes needs to begiven parenterally because oral iron is liable to beirritating to the bowel in patients with ulcerativecolitis. In the present series, the anaemic patientswere almost all treated along these lines.
OTHER DISORDERS OF THE BLOOD The other disordersof the blood were as follows:
7
3
I
3
Heinz body anaemia is a particular type of haemo-lytic anaemia brought about by the action of variousdrugs, of which sulphonamides are an example. Inthe present series, all the cases were due to the use ofsulphasalazine (salicylazosulphapyridine), and thefirst account of Heinz body anaemia occurring as a
complication of this form of therapy came from thishospital (Spriggs, Smith, Griffith, and Truelove,1958). Any patient who develops anaemia while ontreatment with sulphasalazine should have the bloodspecially examined for this, as the changes are notevident in a standard blood film preparation.
There were four cases of purpura, of which threewere thrombocytopenic and did not appear to berelated to the use of drugs. The fourth case was anexample of non-thrombocytopenic purpura whichwas attributed to either penicillin or sulphonamides,as the patient was on treatment with both, and thecondition subsided soon after these drugs were with-drawn.The three cases of pernicious anaemia appear to be
much above the rate to be expected among 624patients, especially as this includes a considerablenumber of young persons. With such a small numberof cases this might be due to a chance samplingeffect, but there exists the possibility that the twodiseases have some connexion, especially as the twoconditions have been described in the same patient(Perillie and Nagler, 1959). It is also of interest thatone of the patients with pernicious anaemia hadpreviously suffered from thyrotoxicosis, because theassociation between thyroid disease and perniciousanaemia is now well-established and they have closeimmunological similarities (Taylor, Roitt, Doniach,Couchman, and Shapland, 1962; Doniach, Roitt,and Taylor, 1963).There were two cases of coagulation defects. One
was an example of severe prothrombin deficiency dueto chronic liver disease. The second was a patient withChristmas disease, which must be regarded as un-related to the ulcerative colitis. The blood conditionhad a major effect upon the course of the illness, be-cause the patient had a severe first attack and sufferedfrom massive bleeding from the bowel. Medicalmanagement proved ineffective and he was treatedby emergency colectomy, but died two days later.
There was one patient with acquired haemolytic
No. of Cases
12
1
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis
anaemia of the auto-immune type, giving a positiveCoombs test. She also suffered from multiplesclerosis.
Finally, one patient suffered from severe anaemiain association with polyarteritis nodosa. This diseasecan itself affect any part of the gastrointestinal tract,and may exceptionally give rise to a bloody diarrhoeaand thus mimic ulcerative colitis. It is therefore im-portant to record that the ulcerative colitis developednine years before the onset of symptoms attributableto the polyarteritis nodosa. The colitis was in com-plete clinical remission but the patient had a carci-noma of the colon which was detected by the findingof a palpable mass on ordinary clinical examination.Presumably the carcinoma could have contributed tothe severe anaemia even though there was no obviousblood in the stools.
In considering this group of miscellaneous blooddisorders associated with ulcerative colitis, it is im-possible to avoid being struck by the fact that im-munological disturbances are known to occur inseveral of them, namely, in pernicious anaemia,idiopathic thrombocytopenic purpura, acquiredhaemolytic anaemia, and polyarteritis nodosa. Thisis of interest as there is evidence of abnormal im-munological reactions in ulcerative colitis, both inregard to auto-immune reactions and to dietaryantigens (Broberger and Perlmann, 1959; Taylor andTruelove, 1961).
ASSOCIATED DISEASES
We have noted the incidence of a number of diseases,some of which have been said to be associated withulcerative colitis. The main examples were asfollows:Pulmonary tuberculosis .. .. 15 (2 4%)Diabetes mellitus .. .. .. 10 (1-6%)Gastric ulcer .. .. .. .. 7 (11 %)Duodenal ulcer .. .. .. 16 (2-6 %)Cholecystitis and/or gall-stones .. 10 (1 6%)Mental illnesses .. .. .. 35 (5'6%)Allergic diseases (asthma, hay fever,
eczema) .. .. .. .. 16 (2.6%)Thyroid disease .. .. .. 15 (24%)Carcinoma other than of the colon
(stomach 4; biliary tract 3; oeso-phagus 1; pancreas 1; breast 5; lung1; prostate 1) .. .. .. 16 (2-6%)All these diseases are common and it is impossible
for us to say that the observed numbers exceed thoseto be expected in a random sample of the generalpopulation, especially when followed over the courseof a number of years.However, it may be of significance that, as far as
carcinoma other than of the colon is concerned, therewere nine cases involving other parts of the digestive
system, which raises the possibility that a widespreaddisturbance of the digestive system is present inulcerative colitis.
CROHN'S DISEASE
Fourteen of the patients suffered from Crohn'sdisease of the small intestine in addition to the ulcera-tive colitis. The relationship between the two diseasesis a strong one, and it is even conceivable that theyare brought about by the same aetiological mechan-isms. As primary Crohn's disease of the large bowelhas become increasingly recognized in recent years,it is important to record that we are not here describ-ing such cases. The question of combined Crohn'sdisease of the small intestine and ulcerative colitisis so confused that it will be discussed in a separatearticle.
DISCUSSION
The local complications have been briefly discussedin the body of the text and will not receive furtherattention here.The frequency with which complications remote
from the colon occur in this disease affords scopefor speculation. There are two main possibilities toaccount for their occurrence. First, ulcerative colitismay be a generalized disease in which the brunt fallson the colon but in which many other organs areaffected, to a greater or lesser extent, as an integralpart of the illness. Secondly, all these complicationsmay be secondary to the diseased colon, provided weexclude those due to malnutrition, those which mayarise in any illness (such as venous thrombosis andpulmonary embolism), and those due to the side-effects of drugs.A number of writers have suggested the possibility
that ulcerative colitis may be a generalized diseasemerely because arthritis, erythema nodosum, skinrashes, eye lesions, chronic hepatitis, aphthous ulcer-ation, and ankylosing spondylitis are frequentlyfound in association with the colitis. The possibilitygains some support from the finding that it is notunusual for one or more of these 'complications' toprecede, often by years, the onset of the colitis. Forexample, Acheson (1960) found an association be-tween ulcerative colitis and ankylosing spondylitis,and records the fact that in 19 patients the symptomsof ankylosing spondylitis preceded the symptoms ofcolitis and in 12 patients the diagnosis of ankylosingspondylitis was firmly established before the onset ofbowel symptoms. In our series, three patients sufferedfrom ankylosing spondylitis before the onset of anycolonic symptoms. Similarly, although chronichepatitis is well recognized as a complication ofulcerative colitis, in a number of patients theulcerative colitis appears to develop in the course of
13
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

4Felicity C. Edwards and S. C. Truelove
fully established chronic liver disease; in our ownseries, these two patterns were equally common,there being eight patients in each group. This isinteresting in relation to so-called 'lupoid' hepatitis,an active chronic hepatitis in which L.E. cells arefrequently found in the blood and which is consideredby some workers to be an auto-immune disease. Theparticular point of interest is that Mackay and Wood(1962) give the case histories of 22 such patients andit is striking that five of them suffered from ulcerativecolitis and in at least one of these patients the livercondition was fully established before the onset ofthe ulcerative colitis. Furthermore, circulating anti-bodies to liver have been demonstrated in the seraof some patients with ulcerative colitis (Brobergerand Perlmann, 1959; Broberger, 1961). Anotherpoint possibly in favour of ulcerative colitis being ageneralized disease, at any rate in some patients, isthe fact that some of the remote complications fre-quently occur in the same patient. The remote com-plications which are specially likely to occur in thesame subject, either concurrently or consecutively,are arthritis, ankylosing spondylitis, erythema nodo-sum, certain skin eruptions, aphthous ulceration ofthe mouth, and eye lesions. In brief, in these subjects,the skin and a variety of mucous and synovial mem-branes appear to share a common liability to be-come inflamed.
If we examine the evidence critically, it is ap-parent that none of the foregoing is sufficientlystrong to make us regard ulcerative colitis as ageneralized disease in its very nature. The fact thatsome 'complications' precede the colonic symptoms,often by years, is at first sight an unassailable pieceof evidence in favour of the generalized diseasetheory. However, the exact starting point of ulcera-tive colitis may be difficult to determine and it isestablished that the colon may be inflamed as judgedby sigmoidoscopic appearances and by the histo-logical picture of biopsy specimens even though thepatient is in perfect clinical remission. For example,in a systematic sigmoidoscopic and colonic biopsystudy of the disease, it was found that more than halfof the patients in clinical remission had obviouscolonic inflammation by both these criteria (True-love and Richards, 1956). Of course this refers topatients already known to have had an attack ofulcerative colitis, but many of these subjects, on closequestioning, give a history of minor bowel disturb-ances long before they develop the overt symptomsof the disease. There is therefore the possibility thatthe colon may be inflamed from time to time inpatients for a number of years before they comeunder close medical examination, and the fact thatarthritis, ankylosing spondylitis, etc., may precedethe classical bowel symptoms does not mean that
they were not secondary to an inflamed colonicmucosa. The difficulty that may exist in determiningthe exact time of onset of ulcerative colitis can beillustrated by a case in our recent personal experience.
A young man aged 20 presented with a severe attack ofulcerative colitis involving the whole colon for which hehas since been treated with radical surgery. This wasjudged to be his first attack of the disease until it wasfound that there had been diarrhoea in his early child-hood, attributed to rectal polyps, which were removed.This had been done in our hospital and the pathologicalspecimens were still preserved. They showed changestypical of pseudo-polyps in active ulcerative colitis.
We therefore judge that there is no indisputableevidence in support of the generalized disease hypo-thesis. If we consider the other main alternative,namely, that the remote complications are a conse-quence of the colitis, it is plain that we do not knowthe mechanisms by which such complications couldbe brought about. One possibility is that the remotecomplications are brought about by immunologicalprocesses; for example, the ulcerative colitis mightset up auto-immune reactions which could affect avariety of organs or there might be serological re-actions to the bacterial flora of the large bowel or todietary antigens, perhaps because such antigens maybe absorbed readily through a damaged colonicmucosa. These are speculative possibilities whichdeserve experimental study but for which at presentthere is no conclusive evidence. On clinical grounds,the point most in favour of the remote complica-tions being secondary to the colitis is the fact thattotal colectomy usually prevents their occurrence or,if they are already present, exerts a favourable in-fluence upon their clinical course. Isolated exampleshave been published of complications of ulcerativecolitis developing after colectomy; for example,Margoles and Wenger (1961) have described theoccurrence of pyodermia gangrenosum in a patientsix months after colectomy. However, such occur-rences appear to have been so infrequent among thepatients treated by pan-proctocolectomy and per-manent ileostomy that we do not judge them to be aserious obstacle to accepting the theory that theremote complications are secondary to the diseasedcolon.
It is impossible at present to judge this major issueand the main value of a study such as the present oneis to focus attention on the importance of the prob-lem and the need for it to be studied, especially bylaboratory methods.
SUMMARY OF PART III
The complications of ulcerative colitis fall logicallyinto two main groups: local complications in and
14
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from

The course and prognosis of ulcerative colitis 15
around the large bowel and remote or systemiccomplications affecting distant parts of the body.The main local complications in the present series
of 624 patients were: ischio-rectal abscess, fistula-in-ano, recto-vaginal fistula, rectal prolapse, fibrousstricture, pseudo-polyposis, perforation of the colon,acute dilatation of the colon, massive haemorrhage,and carcinoma of the colon.
Perforation of the colon is worth special mention.It occurred only in attacks which were clinicallyeither severe or moderately severe and was speciallylikely to occur in the first attack of the disease. Itcarried a high fatality rate and was sometimes notdiagnosed until after death. Its incidence showed noincrease after the introduction of corticosteroidtherapy.The main systemic complications were: erythema
nodosum, pyodermia gangrenosum, various skinrashes, arthritis, ankylosing spondylitis, various eyelesions, liver disease, renal disease, peripheral venousthrombosis, pulmonary embolism, anaemia andother blood disorders, aphthous ulceration of themouth, moniliasis, and osteoporosis.The two systemic complications which made the
biggest contribution to the mortality of the diseasewere liver disease and pulmonary embolism.The incidence of some diseases which have been
considered to show an association with ulcerativecolitis is examined and discussed.The frequency with which certain systemic com-
plications occur in ulcerative colitis has suggestedto some writers that ulcerative colitis may be ageneralized disease, especially as these 'complica-tions' may precede all bowel symptoms. This con-cept is discussed.
REFERENCES
Acheson, E. D. (1960). An association between ulcerative colitis,regional enteritis, and ankylosing spondylitis. Quart. J. Med.,29, 489-499.
Barritt, D. W., and Jordan, S. C. (1960). Anticoagulant drugs in thetreatment of pulmonary embolism: a controlled trial. Lancet,1, 1309-1312.
Beal, R. W., Skyring, A. P., McRae, J., and Firkin, B. G. (1961).The mechanism of production of anaemia in ulcerative colitis.Med. Res., 1, 7-8.
Broberger, 0. (1961). Studies of the immunological relationshipbetween the antigens from different organs in human ulcerativecolitis. Acta paediat. (Uppsala), 50, 577-580.and Perlmann, P. (1959). Autoantibodies in human ulcerativecolitis. J. exp. Med., 110, 657-674.
Brooke, B. N. (1954). Ulcerative Colitis and its Surgical Treatment.Livingstone, Edinburgh & London.Dykes, P. W., and Walker, F. C. (1961). A study of liver dis-order in ulcerative colitis. Postgrad. med. J., 37, 245-251.and Slaney, G. (1958). Portal bacteraemia in ulcerative colitis.Lancet, 1, 1206-1207.
Bywaters, E. G. L., and Ansell, B. M. (1958). Arthritis associatedwith ulcerative colitis: a clinical and pathological study. Ann.rheum. Dis., 17, 169-183.
Doniach, D., Roitt, I. M., and Taylor, K. B. (1963). Autoimmunephenomena in pernicious anaemia: serological overlap withthyroiditis, thyrotoxicosis, and systemic lupus erythematosus.Brit. med. J., 1, 1374-1379.
Kleckner, M. S. Jr., Stauffer, M. H., Bargen, J. A., andDockerty, M. B. (1952). Hepatic lesions in the livingpatient with chronic ulcerative colitis as demonstrated byneedle biopsy. Gastroenterology, 22, 13-33.
Mackay, I. R., and Wood, I. J. (1962). Lupoid hepatitis: a comparisonof 22 cases with other types of chronic liver disease. Quart. J.Med., 31, 485-507.
Margoles, J. S., and Wenger, J. (1961). Stomal ulceration associatedwith pyoderma gangrenosum and chronic ulcerative colitis.Gastroenterology, 41, 594-598.
Morrell, M. T., Truelove, S. C., and Barr, A. (1963). Pulmonaryembolism. Brit. med. J., In the press.
Perillie, P. E., and Nagler, R. (1959). Development of perniciousanemia in a young patient with chronic ulcerative colitis:report of a case. New Engl. J. Med., 261, 1175-1177.
Roth, J. L. A., Valdes-Dapena, A., Stein, G. N., and Bockus, H. L.(1959). Toxic megacolon in ulcerative colitis. Gastroenterology,37, 239-255.
Spriggs, A. I., Smith, R. S., Griffith, H., and Truelove, S. C. (1958).Heinz-body anaemia due to salicylazosulphapyridine. Lancet,1, 1039-1042.
Taylor, K. B., Roitt, I. M., Doniach, D., Couchman, K. G., andShapland, C. (1962). Autoimmune phenomena in perniciousanaemia: gastric antibodies. Brit. med. J., 2, 1347-1352.and Truelove, S. C. (1961). Circulating antibodies to milkproteins in ulcerative colitis. Ibid., 2, 924-929.
Truelove, S. C., and Richards, W. C. D. (1956). Biopsy studies inulcerative colitis. Ibid., 1, 1315-1318.
Wright, V., and Watkinson, G. (1959). The arthritis of ulcerativecolitis. Medicine (Baltimore), 38, 243-262.
Part IV Carcinoma of the colonOver the last 35 years numerous papers relating tothe association between ulcerative colitis andcarcinoma of the colon have appeared (Bargen,1928; Bargen, Jackman, and Kerr, 1938; Sauer andBargen, 1944; Cattell and Boehme, 1947; Kasich,Weingarten, and Brown, 1949; Svartz and Ernberg,1949; Sauer and Bargen, 1949; Gleckler and Brown,1950; Sloan, Bargen. and Baggenstoss, 1950;Lyons and Garlock, 1951; Brown, Kasich, andWeingarten, 1951; Counsell and Dukes, 1952;
Dennis and Karlson, 1952; Weckesser and Chinn,1953; Bargen, Sauer, Sloan, and Gage, 1954;Bacon, Yang, Carroll, Cates, Villalba, andMcGregor, 1956; Goldgraber, Humphreys, Kirsner,and Palmer, 1958a and b; Rosenqvist, Ohrling,Lagercrantz, and Edling, 1959; Dawson and Pryse-Davies, 1959; Slaney and Brooke, 1959; Lindner,King, and Bolt, 1960; Bargen and Gage, 1960;Edling and Eklof, 1961; Bruce and Cole, 1962).The publication of so many series of cases with a
on 21 March 2019 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.5.1.1 on 1 F
ebruary 1964. Dow
nloaded from