Country Presentations Mexico - Pugatch Consilium · 2014-03-01 · Pricing and Reimbursement ......
44
Country Presentations Mexico
Transcript of Country Presentations Mexico - Pugatch Consilium · 2014-03-01 · Pricing and Reimbursement ......

Country Presentations
Mexico

Mexico’s Pharmaceutical DNA and
Key Challenges and Opportunities
2

Mexico’s Pharmaceutical DNA Health system
– Population aged 65 and over predicted to reach 21% of total by 2050 – Public expenditure on health lowest in OECD (as of 2010) – Annual growth rates of health expenditure below OECD average
Pharmaceutical Environment – Pharmaceutical expenditure represents high percentage of total health expenditure – Private out-of-pocket (OOP) spending represents 95% of spending on pharmaceuticals
Pricing and Reimbursement (P&R) – Price caps on patented medicines based on international referencing – Reimbursement limited mainly to generic medicines, based on health technology assessment (HTA)
Intellectual Property (IP) – Biopharmaceutical IP protection fairly standard, except limitations in ability to enforce patents – Counterfeited medicines problematic, particularly in private pharmacies
3

Key Challenges and Opportunities
Challenges
• Below OECD average annual growth rates of health expenditure over last decade
• Fragmented health system and health policymaking
• Pharmaceutical provision by public health insurance schemes focused almost entirely on generics
• Challenging IP environment – ability to enforce patents, particularly in the approval of generics and in the judicial system
Opportunities
• Dependency population rapidly increasing to developed world proportions
• Relatively small public health care sector, compared to other OECD countries; room for growth in private health insurance sector
• Potential for expanding consumption of innovative pharmaceuticals, particularly in light of historically low consumption of pharmaceuticals, demographic opportunities, and the population’s propensity to purchase medicines from the private sector
• Increasingly strong regulation of quality and safety in the biopharmaceutical market, including phasing out of similares, leading to greater purchase and utilization of high quality products
4

Presentation Overview
5

Presentation Overview
• Demographic background
• Macro-economic background
• Health system overview
• Pharmaceutical overview
• Pricing and reimbursement policies
• Intellectual property environment
• Biopharmaceutical regulatory requirements
• Public procurement policies – pharmaceuticals
6

Demographic Background
7
Demographics
• Total population: 34 million
• Annual population growth rates: between 0.79% and 1.36% 2000-2010
• Dependency population 2010 – Youth population (aged less than 15): 28.1% – Elderly population (aged 65 and over): 5.9%
• Dependency population aged 65 and over growing rapidly:
predicted to reach 21.2% of total population by 2050
8

Dependency Population, Trend and Forecast, 2000-2050
Source: OECD Stat (2012) 0
5
10
15
20
25
30
35
2000 2005 2010 2020 2030 2040 2050
Youth Population (aged less than 15) % of total Population
Elderly population (aged 65 and over) % of total Population
9

Macroeconomic Background
10

Macroeconomic Background • GDP per head: USD 15,195 (2010)
• OECD average USD 33,976 (2010)
• Annual GDP growth 2011: 4.5%
• OECD average 2011: 1.8%
• Volatile economic growth rates over past decade – greater highs
and lows than US, EU27 and OECD averages
• Low national debt: 27% of GDP in 2010
• OECD central government debt average close to 80% 11

Real GDP % Growth 1997-2010
Source: OECD Stat (2012)
-8
-6
-4
-2
0
2
4
6
8
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Mexico
United States
EU27 total
OECD total
12

Health System Overview
13

General Health System Facts • Several vertically integrated public insurers/providers for different
parts of population (social security, low-income, unemployed/self-employed)
• Universal coverage (through expansion of public insurance schemes) targeted in 2012
• Outside social security system, financing mix of MoH and states • Actual coverage and medical services provided by social security
system and State Health Services • Out-of-pocket spending highest in the OECD (49% in 2010) • Health policy fragmented, divided between federal and state
governments • Large private sector (represents 50% of health spending)
14

Health Expenditure
• TEH 6.2% of GDP in 2010 (latest figures) – 3.3% lower than OECD average of 9.5% (2010)
• 47.3% of total health spending in 2010 public expenditure – OECD average 72% (2010)
• 3-4% increase in public expenditure as % of TEH since 2005 • Annual average growth rate (AAGR) total health expenditure 3.8%
per year 2000-2009 – OECD average 4.3%
• AAGR public sector 4.0% per year 2000-2009 – OECD average 4.5%
• Out of pocket spending as % of TEH 49% 2010 – OECD average 19.5 % (2010)
15

Total Expenditure on Health % of GDP, 1990-2010
Source: OECD Stat (2012)
16
0
2
4
6
8
10
12
14
16
18
20
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Mexico
United States
France
Germany
Japan
United Kingdom
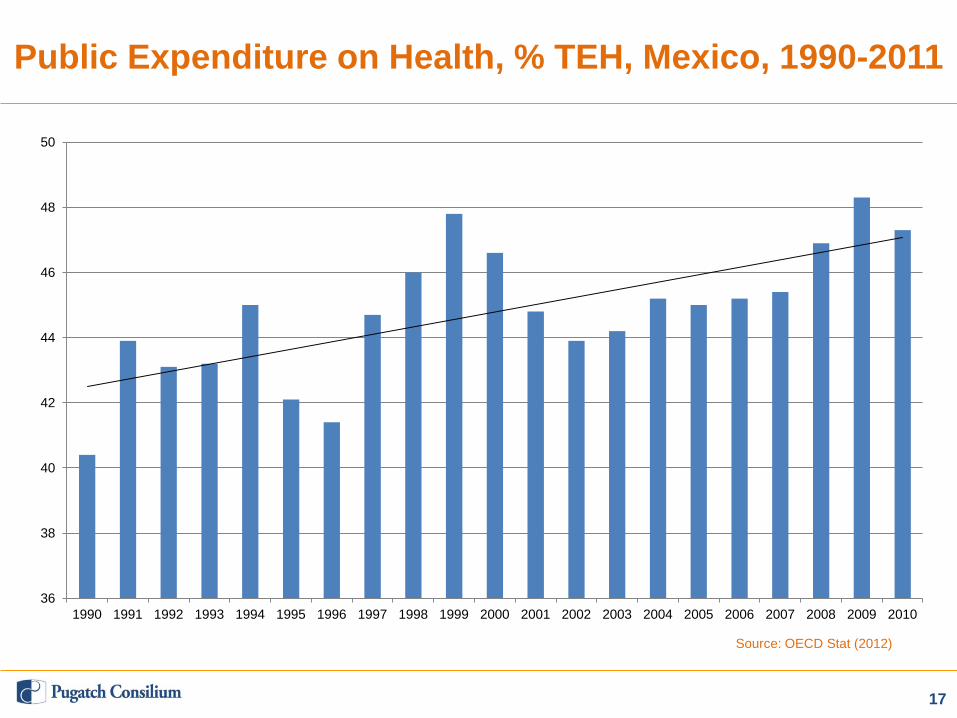
Public Expenditure on Health, % TEH, Mexico, 1990-2011
Source: OECD Stat (2012)
17
36
38
40
42
44
46
48
50
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
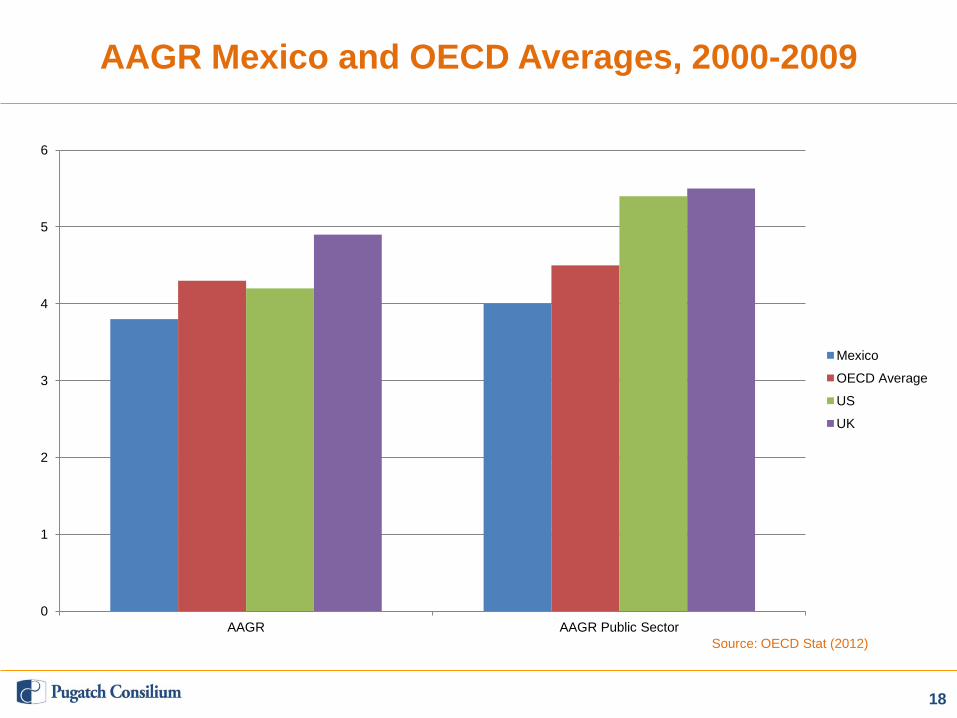
AAGR Mexico and OECD Averages, 2000-2009
Source: OECD Stat (2012)
18
0
1
2
3
4
5
6
AAGR AAGR Public Sector
Mexico
OECD Average
US
UK
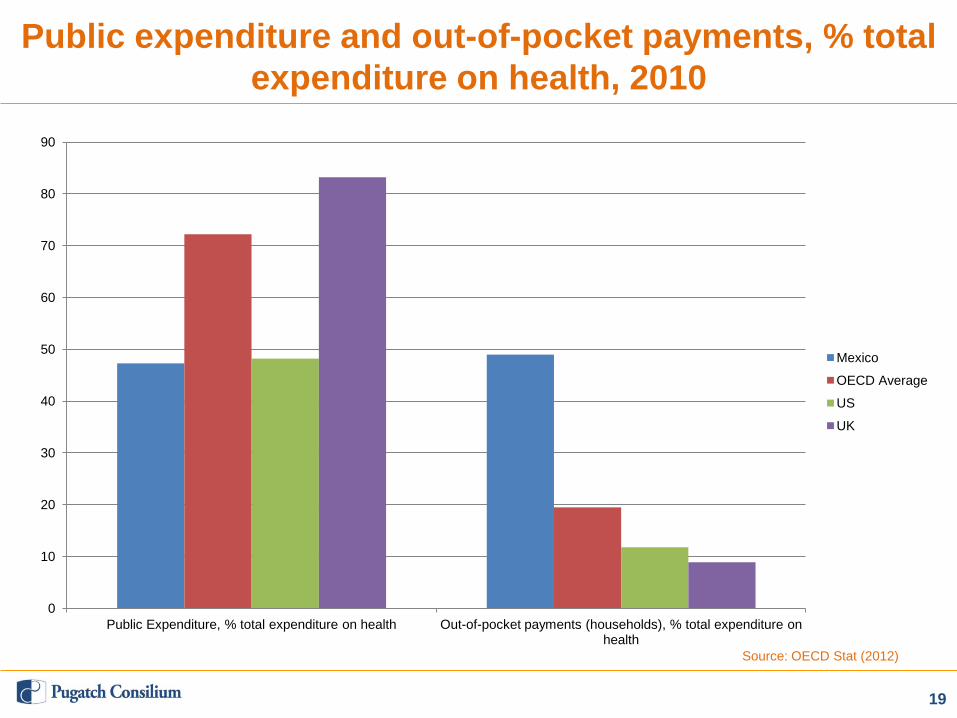
Public expenditure and out-of-pocket payments, % total
expenditure on health, 2010
Source: OECD Stat (2012)
19
0
10
20
30
40
50
60
70
80
90
Public Expenditure, % total expenditure on health Out-of-pocket payments (households), % total expenditure on health
Mexico
OECD Average
US
UK

Pharmaceutical Overview
20

Pharmaceutical Overview (1)
• Pharmaceuticals partially covered through various health
insurance schemes • Public insurance provision dominated by generics • Traditionally, three main classes of medicines in the market:
- Innovative (patented); - “Interchangeable generics” (approved and registered by MoH based on
bioequivalence tests); and - “Similar generics” or similares (generics approved and registered without
bioequivalence tests)
• Public insurance provision of similares phased out 2005-present
21

Pharmaceutical Overview (2)
• High volume of medicines sold through private pharmacies due
to insufficient public health insurance coverage of pharmaceuticals
• Private financing of medicines far outweighs public financing: 80% vs. 20%
• Majority of private spending on medicines is OOP (over 95%) • Still, overall, lowest consumption of pharmaceutical products per
capita in OECD
22

Snapshot of Pharmaceutical Spending
23
• Pharmaceutical spending as % TEH 2nd highest in OECD (27.1% in 2009)
• Per capita spending 2nd lowest in OECD (2009) • Medium growth in per capita pharmaceutical spending in 2000s,
from very low rates at beginning of decade • Between 1999-2009 per capita spending almost tripled from
USD 87.3 to USD 249.9 (PPP) • Incremental growth expected: pharmaceutical sales projected to
rise from US$13 billion (MXN161 billion) in 2011 to US$18 billion in 2015

Total Expenditure on Pharmaceuticals and Other Medical Non-durables, % TEH, Mexico, 1999-2009
Source: OECD Stat (2012)
0
5
10
15
20
25
30
35
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
24
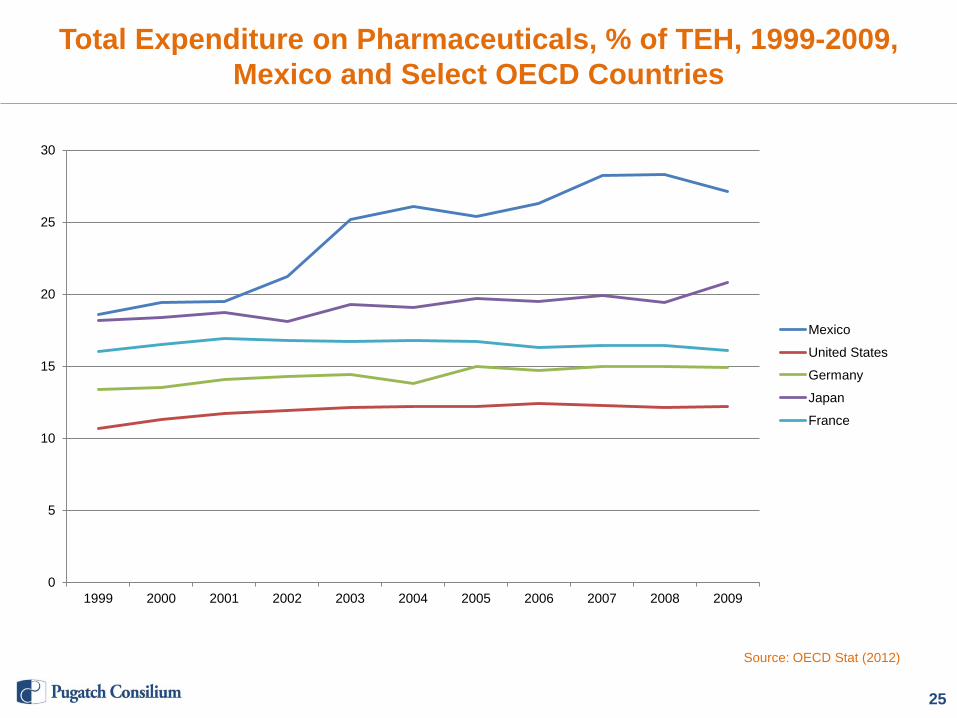
Total Expenditure on Pharmaceuticals, % of TEH, 1999-2009, Mexico and Select OECD Countries
Source: OECD Stat (2012)
0
5
10
15
20
25
30
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Mexico
United States
Germany
Japan
France
25

Total Per Capita Spending, Pharmaceuticals and Other Medical Non-durables, US$ PPP, Mexico, 1999-2009
Source: OECD Stat (2012)
0
50
100
150
200
250
300
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
26

Total Per Capita Spending, Pharmaceuticals and Other Medical non-durables, US$ PPP, 2010 or Closest Year, OECD
Source: OECD Stat (2012)
0
100
200
300
400
500
600
700
800
900
1000
27
Pricing and Reimbursement Policies
28

Pricing Policies Patented Medicines
• Maximum retail prices capped by Ministry of Economy (mainly
for private sector) • Use international reference pricing • Calculated on basis of the average ex-factory price of the
previous quarter in the six largest markets for a given product globally
• Governed by General Law on Health, Article 31 • Lack of across-the-board compliance by pharmacies, poorly
regulated • Little competition in public sector prices for patented medicines
(due to centralized purchasing price)
29

Generic Pricing Policies
Pricing • Public sector: no central price control, wide variation in prices by
state or insurance scheme • Private sector: generics/off-patent medicines no price control Policies Promoting the Use of Generics • Federal Commission for the Protection against Sanitary Risks
(COFEPRIS) creates Interchangeable Generics List • Listed by INN, includes both generic and original products • Public sector insurance schemes use list as well as National
Formulary to encourage (but not require) generic prescription • Generic consumption through public insurance coverage still
limited
30
Reimbursement Policies
• All public institutions and insurance schemes governed by
National Formulary (Cuadro Básico y Catálogo de Medicamientos)
• Set by National Formulary Committee (CICBISS) of the General Health Council (CSG)
• Dictates first, second and third lines of treatment • 4-5 months for review and decision • Listed by INN, each assigned a code • Limits medicines available to 932 INNs (2011) based on market
authorization and Economic Evaluation Study (EEE) • Large majority are off-patent • Published annually
31
HTA Policies
• Economic Evaluation Study (EEE) compares current standard
treatment with product proposed for inclusion in Cuadro Básico • Mandated by CICBISS Internal Regulation, Article 24 • Submitted by company, CICBISS reviews according to CSG
guidelines • Must include at least 1 of the following comparisons:
- Cost-minimization – cost savings compared to equally effective comparators
- Cost-effectiveness – incremental cost-effectiveness ratio relative to GDP per capita per additional years of life
- Cost-utility – same as above, using QALY as denominator - Cost-benefit – rate of return relative to public debt issued by Federal
Government
32
Intellectual Property Environment
33

Pharmaceutical IP Overview
• Biopharmaceutical IP protection fairly standard, but not fully in
line with international standards and bilateral commitments • Biotech inventions patentable, except in natural state or
processes of reproduction • Patent linkage system ineffective, lacks transparency • IP enforcement improving but insufficient
- Significant delays in prosecution common - Injunctions frequently ineffective - Sales of counterfeit medicines in pharmacies undeterred, although efforts
to contain are increasingly routine
34

Pharmaceutical ‘Patent Linkage’ Mechanism
• Basic linkage system exists based on Presidential Decree
(2003)
• Requires generic applicants to comment on the patent status of the reference product
• Potential infringement issues resolved by Mexican Patent Office (IMPI) and COFEPRIS and published by IMPI
• Significant weaknesses: – Does not involve notification or consultation of the patent holder – Only applies to substance patents; despite 2008 Supreme Court ruling
requiring inclusion of formulation and use patents, not consistently applied – Process often delayed and ineffective
35
PTE and RDP
• Mexico does not offer patent term extensions for pharmaceutical
products
• COFEPRIS introduced 5 year regulatory data protection term in 2012
• RDP only applies to NCEs thus far
• Implementation of RDP still uncertain
36

Biopharmaceutical Regulatory Requirements
37

Marketing Authorization for Chemical Entities
• MoH Federal Commission for the Protection against Health
Risks (COFEPRIS) responsible for drug testing and approval • New drug submissions required to undergo safety, efficacy and
quality testing • All generics now required to submit bioequivalence tests • Re-registration required every 5 years (elimination of similares) • COFEPRIS actively monitors availability of unapproved/sub-
standard drugs • Recent delays in approvals; 2011-12 new target maximum
approval time 180 days • COFEPRIS observes and has adopted guidelines of
International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH)
38

Removal of Similares from the Mexican Market
• Similares formalized in 1998 reform to General Law on Health • Reform identified three classes of drugs approved by MoH
(innovative, interchangeable generics and similar generics) • Similares did not undergo bioequivalence tests; not sanctioned
as interchangeable with the original drug • Accounted for 36% of medicines sold in private sector in 2002 • Quality and safety debate over non-bioequivalence tested
products in both public and private sectors 2002-2005 • Effort to phase out similares from the market, 2005-2010
- 2005 amendment to General Law on Health, Art.376 required all generics to undergo bioequivalence tests
- All generics registered prior to 2005 had to be re-registered using bioequivalence tests by 2010
• Not yet fully implemented; severe delays in re-registration (1,000 applications remaining in Oct 2012)
39

Marketing Authorization for Biologics and Biosimilars
• Biological drugs undergo the same procedure and testing
requirements as new chemical entities
• “Biocomparables” (biosimilars) pathway came into force in 2012 (Mexican Health Law, Art 222bis and COFEPRIS guidelines)
• Mexican biosimilar pathway de facto resembles that used by the European Medicines Agency
• Biologic similares (bio-similares) being phased out along with other similares
• RDP protection/periods do not exist for biologics and biosimilars
40

Public Procurement Policies – Pharmaceuticals
41

Public Procurement Policies – Pharmaceuticals (1)
General characteristics of the procurement system
• Relies on INN (as per the Cuadro Básico)
• Favors generics over innovative products
• Decisions based largely on price
• Value plays a role mainly to the extent it is a factor of a product’s inclusion in the Cuadro Básico
42
Public Procurement Policies – Pharmaceuticals (2)
Phase I: Setting of centralized procurement price • Coordinating Commission for Negotiating the Price of Medicines
and Other Health Inputs (CCNPMIS) annually secures single price for given product for all public institutions
• Composed of representatives of MoH, MoEcon, public health insurers
• Principle objective: uniform price reductions Phase II: Actual procurement by individual institutions • Based on centrally agreed price • Mandatory to tender for products included in Cuadro Básico
(generics where possible) • States handle purchasing of non-essential medicines for all
MoH-dependent schemes • Wide variation in average drug prices among states
43
Thank you!
44