Council of GovernorsInformation, Advice and Support Service (SENDIASS). Mar 2013 Mar 2013 Mar 2014...
252
Agenda Welcome Declaration of Interest Apologies Minutes Matters Arising Chairman's Report Chief Executive's Report Integrated Quality Report Any Other Business Attendance Record Integrated Improvement Plan Dementia Strategy Presentation Governance and Governors' responsibili- ties Council of Governors 2 June 2015 4.00pm Village Hotel, The Green Business Park, Dog Kennel Lane, Shirley, Solihull
Transcript of Council of GovernorsInformation, Advice and Support Service (SENDIASS). Mar 2013 Mar 2013 Mar 2014...

Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Council ofGovernors
2 June 2015 4.00pm
Village Hotel,The Green Business Park, Dog Kennel Lane,
Shirley, Solihull

June 2015
Council of Governors
.2
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Notice is hereby given that a meeting of the Council of Governors
of Heart of England NHS Foundation Trust will be held at the Village Hotel, The Green Business Park, Dog Kennel Lane, Shirley, Solihull B90 4GW
on 2 June 2015 4.00 – 6.00pm
A G E N D A
Indicative Timings
(minutes) Presenter
1. Welcome
2 Chair
2. Apologies
1 Kevin Smith
3. Declarations of Interest - Governors - Directors
2 Chair (Enclosure)
Strategy
4. Chief Executive’s Report
10 Andrew Foster
(Enclosure)
Quality & Performance
5. Integrated Quality & Performance Report, including Finance
20 Jonathan Brotherton/ Darren Cattell/ Andrew Catto/ Sam Foster
(Enclosure)
6. Integrated Improvement Plan
10 Andrew Catto (Enclosure)
Matters for Report
7. Dementia Strategy Presentation
20 Niall Fergusson/ Phil Hall (Oral)
Governance & Administration
8. Minutes of previous meetings – 14 April & 5 May 2015
5 Chair (Enclosure)
9. Matters Arising/ Recommendations Tracker
5 Kevin Smith (Enclosure)
10. Governance and Governors’ responsibilities
5 Kevin Smith (Enclosure)
11. Attendance Record
2 Chair (Enclosure)
For Information
12. Chair’s Report
5 Chair
(To follow)
13. Any Other Business Previously Advised to the Chair
14. Date of Next Meeting
8 July 2015 – Harry Hollier Lecture Theatre, Good Hope Hospital, Sutton Coldfield Refreshments will be available from 3.30pm Kevin Smith Company Secretary 26 May 2015

June 2015
Council of Governors
.3
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Welcome

June 2015
Council of Governors
.4
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Apologies

June 2015
Council of Governors
.5
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declarations ofInterests

Council of GovernorsJune 2015
.6
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declaration of Interests - Governors
COUNCIL OF GOVERNORS
REGISTER OF INTERESTS NAME INTEREST DECLARED DATE
DECLARED DATECEASED
Cllr Mohammed Aikhlaq
Awaiting information
Arshad Begum Nothing to declare 21 Nov 2011
Kath Bell Company Secretary - Succeed Services Ltd 21 Nov 2011
Nicola Burgess Awaiting information
Elaine Coulthard Nothing to declare 21 Nov 2011
Dr Olivia Craig No declaration received
Carol Doyle Awaiting information
Helen Griffiths Awaiting information
Emma Hale Nothing to declare 27 May 2014
Ron Handsaker 1. Shareholder – Santander 2. Director – 24/7 Industrial Services UK Ltd
200020 Oct 2014
Albert Fletcher Director – Aquarius (unpaid). A charity that specialises in helping and treating those with drink and/or drug issues.
28 May 2013
Richard Hughes 1.Chairman – Homestart (Tamworth) 2.Chairman – Tamworth Credit Union Ltd 3.Director – The Pathway Project 4.Director – Tamworth Community Advice Network CIC 5.Chairman – Tamworth Talking Newspaper Ltd 6.TrusteeChairman – The Rawlett Trust
7.Vice Chairman – Standards Committee, Tamworth Borough Council 8.Divisional President – St John’s Ambulance 9.Member – Appeal Committee, St Giles Hospice 10.Retired CEO & President Secretary, Tamworth Cooperative Society 11.Mr Hughes’ son holds a very senior managerial position with Barclays Bank 12.Chairman – Tamworth Community Advice Network CIC 13. Independent Member – Tamworth Borough Council Nominations Committee 14. Member – Conservation Advisory Committee, Tamworth Borough Council 15. President – Tamworth Male Voice Choir 16. Treasurer – St Andrew’s Methodist Church, Tamworth 17. Shareholder – BP 18. Shareholder – Santander 19. Trustee – Spirit of Tamworth Trust
21 Nov 2011
Amended 1 Sep 2013
Amended 23 Oct 2012 16 Feb 2012
23 Oct 2012
23 Oct 2012
23 Oct 2012 23 Oct 2012 23 Oct 2012 23 Oct 2012
23 Oct 2012 23 Oct 2012 May 2014
23 Oct 2012 4 Mar 2014 23 Oct 2012
23 Oct 2012
23 Oct 2012

Council of GovernorsJune 2015
.7
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declaration of Interests - Governors
Michael Hutchby Nothing to declare 16 Aug 2013
Sue Hutchings Shareholder in Lloyds TSB 19 Sept 2013
Phillip Johnson Nothing to declare 21 Nov 2011
Michael Kelly Nothing to declare 21 Nov 2011
Attiqa Khan Nothing to declare 16 Aug 2013
Heidi Lane 1. Member of Church – Renewal Christian Centre 2. Husband is an Elder of the Church. 3. Trust uses Christian Renewal Centre for
conferences & meetings
21 Nov 2011
Andrew Lydon Nothing to declare 16 Aug 2013
Anne McGeever 1. Registered with Therapy Bank in Worcestershire to provide services to BMI Droitwich Spa Hospital. 2. Unite Professionals Limited (Occupational Therapists) – ad hoc employment.
12 Sep 2014
14 Apr 2015
Margaret Meixner Awaiting information
CatherineNeedham
Nothing to declare 13 May 2014
Barry Orriss Nothing to declare 21 Nov 2011
Mark Pearson Member of Green Party 21 Jan 2015
Cllr Jim Ryan Archway Academy Ltd – Owner/MD Archway Community College - Owner/MD Archway Brimstone Security – Owner/MD Archway Renaissance LLP – Owner/MD Robert Ryan Housing Investments - Owner /MD
15 July 2013
Liz Steventon Friends of Solihull Hospital 21 Nov 2011
David Treadwell 1. Shareholder - Lloyds TSB 2. Shareholder - STW 3. Shareholder - National Grid
21 Nov 2011
Matthew Trotter 1. HEFT Employee 2. Director - Specialist Health Partnership 3. Director - Specialist ENT Care Ltd
12 Sep 13
15 Dec 14

Council of GovernorsJune 2015
.8
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declaration of Interests - Voting Directors
REGISTER OF DIRECTORS and REGISTER OF DIRECTORS’ INTERESTS
VOTING DIRECTORS
NAME DATE OF APPOINTMENT INTEREST (if any) DATE OF
NOTIFICATION DATE OF
TERMINATION OF INTEREST
Mr Jonathan Brotherton
04.03.15 Nothing to declare
Dr Patrick Cadigan 01.07.13 1. Consultant cardiologist at Sandwell and West Birmingham Hospital Trust.
2. Registrar of the Royal College of Physicians of London.
3. Member of the clinical advisory group advising the Trust Special Administrators re the future of Mid Staffs NHS Trust.
4. Member of the clinical advisory group to NHS England on rare diseases.
5. Undertakes paid consultancy work for McKinsey & Co.
Mar 2014
04.07.14
31.12.13
Mar 2014
Mr Darren Cattell 19.01.15 Director & Shareholder - Mill Street Consultancy Limited.
Sept 2005
Dr Andrew Catto 01.03.14 (Interim CEO -
14.11.14 to 16.02.15)
Nothing to declare.
Mr Andrew Edwards
01.10.14 1. Couch Perry & Wilkes. In receipt of annuity following business sale until May 2019.
Mr Andrew Foster 16.02.15 Director of Wrightington Wigan & Leigh NHS Foundation Trust.
Mrs Sam Foster 01.09.13 Nothing to declare.
Ms Hazel Gunter 04.03.15
Nothing to declare.
Mrs Karen Kneller 01.10.14 1. CEO of Criminal Cases Review Commission
2. Part time judge Social Entitlement Chamber Fitness to Practise
3. Member for General Dental Council 4. Director (unremunerated) of BRAP, an
equalities think tank.

Council of GovernorsJune 2015
.9
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declaration of Interests - Voting Directors
NAME DATE OF APPOINTMENT INTEREST (if any) DATE OF
NOTIFICATION DATE OF
TERMINATION OF INTEREST
Mr Les Lawrence 01.04.12 (Chair –
01.06.14)
1. Trustee for the National Institute for Conductive Education.
2. Governor of City of Birmingham School.
3. Director of Lindridge Enterprises Limited.
4. Director (unremunerated) of Bordesley Birmingham Trust Limited (since 7 July 2011).
5. Chairman of the Birmingham Special Educational Needs & Disability Information, Advice and Support Service (SENDIASS).
Mar 2013
Mar 2013
Mar 2014
July 2014
Mar 2015
Mr David Lock 01.07.13 1. Practising barrister and a member of Landmark chambers. Providing legal advice and representation to a wide range of individuals, NHS organisations, local authorities, charities and commercial organisations mainly on public law issues. These frequently involve issues concerning the rights of patients to NHS treatment as well as structural and management issues involving NHS bodies.
2. Member of Amnesty International. 3. Member of the BMA Ethics Committee
(unremunerated). 4. Member of the Labour Party and
occasional legal advice to Labour Party and elected Members of Parliament on NHS policy issues.
5. Mr Lock’s wife, Dr Bernadette Gregory, is a medical doctor employed by Redditch and Bromsgrove Clinical Commissioning Group and is Clinical Lead for the Worcestershire Integrated Care Project.
6. Chairman of Innovation Birmingham Limited.
7. Representing NHS England in relation to specialised services.
8. Receives instructions from the CQC.
Updated Jan 14
05.11.13
06.01.14
04.07.14
Ms Alison Lord 01.05.13 1. CEO and Shareholder of Allegra Ltd. 2. Voluntary role as a business mentor
for the Prince's Trust. 3. In her professional capacity as a
'turnaround executive' Ms Lord has relationships from time to time with major accountancy firms, legal firms, banks and venture capital providers.
4. Company Secretary - Adente Limited (unremunerated).
22.01.14
13.05.14

Council of GovernorsJune 2015
.10
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Declaration of Interests - Voting Directors
NAME DATE OF APPOINTMENT INTEREST (if any) DATE OF
NOTIFICATION DATE OF
TERMINATION OF INTEREST
Dr Jammi Rao 01.07.13 1. Sole director of Gorway Global Ltd. a private company and owning 50% of its share capital. A consulting company offering management support, training and bespoke public health analytical support to public sector organisations involved in health, well-being and health care.
2. Board Director of Welcome CIC - a Community Interest Company supporting minority and disadvantaged communities by working with statutory and other agencies.
3. Trustee of the Faculty of Public Health as an elected General Board Member. Term of office from 2010 to July 2013.
4. Visiting Professorship in Public Health in the School of Health, Staffordshire University.
Jul 2013
Prof Laura Serrant 01.04.12 1. Director of Research & Enterprise at University of Wolverhampton
2. Non-executive director National Skills Academy for Health (unremunerated).
01.04.12
23.01.14
Mr Adrian Stokes 01.07.08 1. Director of Heartlands Education Centre Ltd.
2. Pfizer Virtual Customer programme.
01.07.08
20.06.11

Council of GovernorsJune 2015
.11
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report

Council of GovernorsJune 2015
.12
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
1
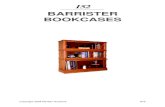
Chief Executive’s Report Introduction I have now been in post for just over three months and it has been quite a journey. There have been several ups and downs but for the most part I think we can see signs of small improvements in performance and more significant advances in our systems of governance. Monitor tell us that they feel more assured that the Executive team is performing cohesively and, through the Integrated Improvement Plan, can demonstrate that we are tackling all of the major challenges we face. I hope that we can move from a position of being constantly on the back foot, responding to concerns from our Regulators and others, onto the front foot when we can agree a suite of strategies and plans in September. By the time today’s HEFT Board meeting takes place, the WWL Board should have formally approved the extension of my interim period by a further 3 months, taking me through to mid-November 2015. This enables me to offer a little more stability and consistency of message which is very important to each of my three main priorities of Clarity, Staff Engagement and Quality Improvement. Clarity The two key areas of work are about how the Trust is managed and what are its plans for the future? We have extended the structure charts to a third level (Appendix A) and published them internally. This means that everyone can see the main responsibilities and reporting lines for Executive Directors, each of their direct reports, and each next in line direct report. The plan is to continue this process until we have a full line of sight from Ward to Board. The EMB has also held three discussions about the thorny issue of whether we manage by Site or by Service where currently we have an unhelpful hybrid of the two. The emerging view is that we should manage by Division. Thus the five Divisions include Heartlands and Good Hope as Sites, Solihull as a combined Site and Community, and Clinical Support and Women’s and Children’s as Cross-Site Divisions. The main principles of this should be that:
We will operate a clinically–led, devolved system of management where the Trust Board sits above the Executive Management Board (EMB)
The EMB comprises the Executive Directors, Associate Medical Directors and Heads of key departments
AMDs will have direct line management of all staff in their Division through Clinical Directors
The Clinical Support Division - stressing its role is indeed to support other Divisions and for CSS to reflect on possible future models of operation for example the equivalent of a Service Line Agreement
In so far as possible, every member of staff should have a single line manager There will also be discussion with Clinical Directors (CD) on developing CDs with a
Cross-Divisional responsibility. Their duty will not be to line manage other sites but to lead on collaboration between sites, professional standards and long term planning. There will also be work on the role of the clinical lead.
We will now consult with CDs and others to come up with a clear statement of how this will work in practice and the respective duties of a Divisional CD and a Cross-Divisional CD.

Council of GovernorsJune 2015
.13
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
2
Matthew Cooke continues to make good progress on the suite of strategies. Two large Listening Events were well attended and produced enthusiastic initial feedback. The next major draft will be discussed in the second part of this meeting. Staff Engagement Hazel Gunter is reporting on progress in Part 2 of the meeting so I will not comment further here other than to thank the many hundreds of staff who have now actively participated in various events and Alex Covey’s team who are enthusiastically managing this complex and ambitious programme. Quality Improvement We held a Quality Summit on 27th April to celebrate four examples of excellence that are already happening in the Trust:
Phil Hall, senior dementia nurse, gave a presentation on dementia care and we heard that the Trust has been selected as the acute pilot site for the Midlands to test a new Learning Needs Analysis (LNA) tool. This is part of the Skills for Health dementia innovation programme of work and its aim is to develop a national competency framework for staff working with people with dementia across healthcare organisations, social care, GP practices, care homes and voluntary organisations.
Michelle Davies, resuscitation officer gave a presentation on the excellent work they are doing at Good Hope on anaphylaxis, making sure that the lifesaving adrenalin injection is administered correctly.
Mr Haney Youssef talked us through the latest developments with peritoneal surgery and I had not previously known that HEFT is one of just three centres in England conducting this complex surgery. Mr Youssef is pioneering a new procedure called the “sugarbaker” which has spectacularly improved survival rates.
Dr Das Pillay and Caroline Maries-Tillott gave a presentation about antibiotic initiatives in the Trust. They have helped electronic prescribing wards to increase antibiotic stop date performance which has gone up by 28% compared to the same period last year. IV antibiotic administration within one hour has improved in the past 2 years from 56% to 71%. A ‘live’ antibiotic dashboard (unique in the NHS) is available for wards to maintain vigilance to avert delays in STAT antibiotic dose administration. This involved the introduction of a medication dashboard which is part of a wider quality and safety improvement project to advance the Trust’s performance of indicating stop/review dates and administration of antibiotic doses
A different kind of Quality Summit was held on 20 May when the CQC presented its findings following the unannounced inspection in December 2014. The final version of the report is due to be published on 1st June so we will arrange to have a full item about the report and our response at a future Trust Board meeting. In the meantime here are the headlines:
The Trust will receive an overall rating of “Requires Improvement”. There are two higher ratings (Outstanding and Good ) and one lower (Inadequate)
One department, Heartlands Emergency Services, was rated as Inadequate; Solihull Outpatients was rated as Good; all other departments were rated as Requires Improvement.
The report cites five examples of outstanding practice: Heartlands AMU complaints resolution, leadership on five wards at Heartlands, the Practice Placement Team, Sexual Health Information and widespread observation of compassionate care across the Trust.

Council of GovernorsJune 2015
.14
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
3
It also cites numerous areas for improvement and 26 must-dos, many of which have already been done. The number one outstanding issue is safety in ED.
We fully accepted the CQC report and recommendations and agreed to build them all into our Integrated Improvement Plan
Other Matters As at the last Board, my contention is that we should accord most priority to the challenges described above but there is still a long list of other major issues that need attention:
A&E performance and the controversial issue of what trajectory we can “commit” to 18 week performance (especially gastroenterology) Financial trading deficit last year and this Building and maintaining Monitor’s confidence Developing and mainstreaming the Integrated Improvement Plan The Deloitte Governance and IT reports The Kennedy report The Silverman report and excess mortality and harm Relationships with commissioners and the 15-16 contracts Staff shortages, especially nursing Surgical reconfiguration Solihull Urgent Care Centre Solihull Integration Plan Quality and capacity of senior and middle management
Andrew Foster 21 May 2015

Council of GovernorsJune 2015
.15
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Dep
uty
Dire
ctor
and
Chi
ef o
f Sta
ff (M
edic
al D
irect
or’s
Offi
ce)
Head
of R
evie
w a
nd
Reca
ll
Caro
line
Will
iam
s (In
terim
)
Head
of
Com
mun
icat
ions
Ka
te E
ccle
s
Med
ical
Illu
stra
tion
and
Mul
ti M
edia
Man
ager
Gl
enn
Man
nion
Med
ical
Dire
ctor
’s O
ffice
Ad
min
istr
atio
n
Clin
ical
Rev
iew
–
Spec
ialis
t cas
es
Reca
ll pl
anni
ng a
nd
deliv
ery
Med
ical
Illu
stra
tion
Gr
aphi
cs
Desig
n
Inte
rnal
Co
mm
unic
atio
ns
Exte
rnal
Co
mm
unic
atio
ns
Intr
anet
M
edia

Council of GovernorsJune 2015
.16
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Dep
uty
Med
ical
Dire
ctor
(Str
ateg
y an
d Tr
ansf
orm
atio
n)
Mat
thew
Coo
ke
Head
of C
linic
al
Serv
ices
Str
ateg
y
Joan
na H
odgk
iss
Dire
ctor
of R
esea
rch
Don
Mill
igan
Head
of I
nnov
atio
n
Beth
an B
isho
p
Stra
tegy
Dev
elop
men
t St
rate
gy D
eplo
ymen
t Pr
iorit
y pr
ogra
mm
es
Spec
ialis
ed S
ervi
ces
Prim
ary
Care
Inte
grat
ion
Inno
vatio
n Te
lehe
alth
Rese
arch
M
IDRU
Not
e ch
ange
s Ho
lier-
now
Phi
l Brig
ht
Med
Illu
stra
tion-
Ric
hard
Bro
wn
Emer
genc
y Pl
anni
ng- J
onat
han
Brot
hert
on
Med
Lea
ders
hip-
DM
D (E
lder
ly)
Chief Executive's Report

Council of GovernorsJune 2015
.17
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Dep
uty
Med
ical
Dire
ctor
– A
ppra
isal,
Perfo
rman
ce a
nd O
utco
mes
Cl
ive
Ryde
r
As
soci
ate
Med
ical
Di
rect
or R
eval
idat
ion
–Ad
edej
i Oku
bade
jo
Ope
ratio
ns M
anag
er
(TBC
)
Dire
ctor
of M
edic
al
Safe
ty /
Qua
lity
Impr
ovem
ent
Ann
Keog
h
Med
ical
Rev
alid
atio
n
Inve
stig
atio
ns
Cald
icot
t Gua
rdia
n
Qua
lity
Impr
ovem
ent
Mor
talit
y
Adm
inist
ratio
n Su
ppor
t Pr
ojec
t Sup
port
Chief Executive's Report

Council of GovernorsJune 2015
.18
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Ch
ief N
urse
Sa
m F
oste
r
Depu
ty C
hief
N
urse
Sue
Hyla
nd
Head
of P
MO
Nic
k Va
rney
(in
terim
unt
il en
d Ju
ne ‘1
5)
Head
N
urse
s Ch
ildre
n’s
Head
of
Mid
wife
ry
Depu
ty C
hief
N
urse
Julie
Tun
ney
De
puty
Dire
ctor
of
Pat
ient
Ex
perie
nce
Ri
char
d Br
own
Head
Nur
se
Safe
guar
ding
Mar
ia K
ilcoy
ne
Head
of
Gov
erna
nce
TB
C
Head
Nur
se
Infe
ctio
n Pr
even
tion
&
Con
trol
Gill
Abb
ott
Chief Executive's Report

Council of GovernorsJune 2015
.19
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Depu
ty C
hief
N
urse
Sue
Hyla
nd
Depu
ty C
hief
N
urse
Sue
Hyla
nd
Head
Nur
ses
Ch
ildre
n’s
BH
H GH
H So
lihul
l
Head
of M
idw
ifery
Head
Nur
se –
Pat
ient
Exp
erie
nce
Co
rpor
ate
Nur
sing
Tea
m
De
puty
Chi
ef N
urse
Sue
Hyla
nd
De
puty
Chi
ef N
urse
Julie
Tun
ney
Chief Executive's Report

Council of GovernorsJune 2015
.20
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
De
puty
Dire
ctor
of P
atie
nt
Expe
rienc
e
Rich
ard
Brow
n
Ja
mie
Em
ery
He
ad o
f Pat
ient
Ser
vice
s &
Enga
gem
ent
Chief Executive's Report

Council of GovernorsJune 2015
.21
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Head
Nur
se
Safe
guar
ding
Mar
ia K
ilcoy
ne
M
atro
n Ad
ult
Safe
guar
ding
Lorr
aine
Lon
gsta
ff
Le
ad M
idw
ife
Safe
guar
ding
Ca
rol O
wen
Chief Executive's Report

Council of GovernorsJune 2015
.22
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
De
puty
Dire
ctor
of
Gove
rnan
ce
TB
C
He
ad o
f Co
rpor
ate
Risk
&
Com
plia
nce
Ra
chae
l Bl
ackb
urn
He
ad o
f Hea
lth
& S
afet
y Go
vern
ance
Dian
e Au
cott
He
ad o
f Go
vern
ance
Loui
se R
udd
He
ad o
f Leg
al
and
Inve
stig
atio
ns
Sara
h C
arr-
Cave
Pa
tient
Saf
ety
Advi
sor
Caro
line
Mar
ies-
Tillo
tt
Chief Executive's Report

Council of GovernorsJune 2015
.23
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Head
Nur
se
Infe
ctio
n Pr
even
tion
&
Con
trol
Gill
Abbo
tt
Depu
ty H
ead
Nur
se
Infe
ctio
n Pr
even
tion
&
Cont
rol
Ja
ne C
odd
Chief Executive's Report

Council of GovernorsJune 2015
.24
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
D
irect
or o
f Fin
ance
and
Per
form
ance
(Int
erim
) D
arre
n C
atte
ll
Fina
nce
& P
erfo
rman
ce
Dep
uty
Fi
nanc
e D
irect
or
A
idan
Qui
nn
Hea
d of
P
erfo
rman
ce
(Inte
rim)
D
iane
Pov
ey
Dire
ctor
o
f Ass
et
Man
agem
ent
Jo
hn S
ella
rs
Dire
ctor
of
ICT
(Int
erim
)
Jon
Rex
Dire
ctor
of
Fina
nce
Ope
ratio
ns
Jo
nath
an G
ould
May
201
5
PM
O
TB
C
Chief Executive's Report

Council of GovernorsJune 2015
.25
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
D
irect
or o
f Fin
ance
Ope
ratio
ns
Jona
than
Gou
ld
Fina
nce
Ope
ratio
ns
Chi
ef F
inan
cial
C
ontro
ller
A
ngel
ine
Jone
s
H
ead
of In
com
e &
C
ontra
ctin
g
M
ike
Arc
her
P
rocu
rem
ent
Dire
ctor
Dav
e C
oley
Proj
ect
Sup
port
Mon
a Ta
ylor
May
201
5
Chief Executive's Report

Council of GovernorsJune 2015
.26
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
H
ead
of P
erfo
rman
ce (I
nter
im)
Dia
ne P
ovey
Perf
orm
ance
Ope
ratio
nal
Per
form
ance
&
Del
iver
y M
anag
er
C
laire
Rym
er
Hea
d of
Ser
vice
Im
prov
emen
ts
Va
canc
y
Cor
pora
te
Per
form
ance
&
Del
iver
y M
anag
er
D
awn
Car
ty
Pro
ject
Man
ager
Fi
nanc
e S
taff
Dev
elop
men
t
Sue
Lyd
don
Hea
d of
Clin
ical
C
odin
g
Ste
phen
Cro
ss
May
201
5
Chief Executive's Report

Council of GovernorsJune 2015
.27
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Faci
litie
s &
C
orpo
rate
Mal
colm
Cla
rk
D
eput
y Fi
nanc
e D
irect
or
Aida
n Q
uinn
Ope
ratio
nal B
usin
ess
Supp
ort
H
eartl
ands
H
ospi
tal
C
lair
Youn
g
Goo
d H
ope
Hos
pita
l
Ele
na E
dwar
ds
Sol
ihul
l Hos
pita
l
Ada
m W
inst
anle
y
Clin
ical
Sup
port
Ser
vice
s
Cla
ire P
ooni
Wom
en’s
&
Chi
ldre
n’s
Jo
-Ann
e Jo
hn
Ric
hard
Bar
ratt
Hea
d of
Pro
ject
s S
ue K
ing
May
201
5
Chief Executive's Report

Council of GovernorsJune 2015
.28
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
D
irect
or o
f IC
T (In
terim
) Jo
nath
an R
ex
D
eput
y D
irect
or o
f IC
T
Ann
e S
mal
lpag
e
Hea
d of
ICT
Bus
ines
s D
eliv
ery
Lee
Woo
tton
H
ead
of
Med
ical
R
ecor
ds
Ly
nn D
ugga
n
ICT
H
ead
of IC
T P
rogr
amm
e M
anag
emen
t an
d Tr
aini
ng
C
arol
ine
Sad
ler
H
ead
of IC
T
Sys
tem
s D
evel
opm
ent
D
ave
Hex
tell
H
ead
of IC
T Te
chni
cal
Ser
vice
s
D
idie
r Mee
rt M
ay 2
015
Chief Executive's Report

Council of GovernorsJune 2015
.29
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
D
irect
or o
f Ass
et M
anag
emen
t Jo
hn S
ella
rs
Ass
et M
anag
emen
t
H
ead
of E
stat
es
M
ike
Tayl
or
Hea
d of
Fac
ilitie
s
Chr
is D
avie
s
H
ead
of C
apita
l P
roje
cts
M
ark
Pig
gott
O
pera
tions
Lea
d fo
r Ass
et
Man
agem
ent
K
aren
Ton
gue
May
201
5
Chief Executive's Report

Council of GovernorsJune 2015
.30
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Rol
e
TBC
PMO
R
ole
Nam
e
Rol
e N
ame
Rol
e N
ame
Rol
e N
ame
May
201
5
Chief Executive's Report

Council of GovernorsJune 2015
.31
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Carl
Holla
nd
Head
of O
pera
tions
BH
H
Emer
gen
cy C
are
Gro
up
Gen
eral
M
anag
er
Ben
Rich
ards
Em
erge
ncy
Care
G
roup
G
ener
al
Man
ager
Be
n Ri
char
ds
Surg
ery
Gro
up G
ener
al
Man
ager
C
hery
l Hud
son
Ad
mis
sion
s &
Disc
harg
e
Govi
ndan
Ra
ghur
aman
AM
D, B
HH
Sara
h Q
uint
on
Head
Nur
se, B
HH
Em
erge
ncy
Care
As
soci
ate
Head
Nur
se
Sa
rah
Brow
n
Med
icin
e
G
roup
G
ener
al
Man
ager
M
ark
Houg
hton
Med
icin
e
As
soci
ate
Head
Nur
se
Ly
nn F
ishe
r
Surg
ery
G
roup
Cl
inic
al
Dire
ctor
TB
C
Surg
ery
As
soci
ate
Head
N
urse
Lo
uise
Ev
eret
t
Med
icin
e
G
roup
Cl
inic
al
Dire
ctor
Ra
hul
Muk
herje
e
Surg
ery
G
roup
G
ener
al
Man
ager
Ch
eryl
Hu
dson
Emer
genc
y Ca
re
Gro
up
Clin
ical
Di
rect
or
TBC
BHH
Site
Emer
genc
y De
part
men
t AM
U
Elde
rly C
are
Stro
ke
Card
iolo
gy
Gen
eral
M
edic
ine
Capa
city
M
anag
emen
t SA
U
Gen
eral
Su
rger
y
Thor
acic
Gas
tro
Uro
logy
Vasc
ular
Trau
ma
Neu
rolo
gy
CH
ON
C
Resp
irato
ry
Re
nal

Council of GovernorsJune 2015
.32
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Dr A
lan
Jone
s As
soci
ate
Med
ical
Dire
ctor
Eric
a Lo
ftus
He
ad o
f Ope
ratio
ns
Lab
Med
ID
/Sex
ual
Heal
th
OPD
& A
BC
Criti
cal C
are
&
Anae
sthe
tics
Thea
tres
, DS
U, P
re o
p,
SAL
Radi
olog
y Ph
arm
acy
Cl
inic
al
Com
plia
nce
Clin
ical
Di
rect
or
Dr R
eyno
lds
Clin
ical
Dire
ctor
Dr
O’B
rien
(CC)
&
Dr S
eeth
aram
a (A
naes
)
Clin
ical
Di
rect
or
Mr S
uper
Clin
ical
Di
rect
or
Dr S
mith
Stua
rt D
ale
Gene
ral M
anag
er
Clin
ical
Di
rect
or
Dr Jo
nes
Ther
esa
Pric
e Ge
nera
l Man
ager
Clin
ical
Di
rect
or
T Ca
rrut
hers
Stev
e W
alle
r Ge
nera
l Man
ager
Mar
ie P
eplo
w
Radi
olog
y
Rach
el
Ferr
eday
Th
eatr
es
Mar
ie N
olan
An
aes &
Crit
Ca
re
Hele
n Ev
ans
OPD
& A
BC
Trac
y Pe
arso
n ID
/Sex
ual
Heal
th
Jane
t Fre
el
Med
ical
De
vice
s
Balji
t Atw
al
Phar
mac
y
CLIN
ICAL
SU
PPO
RT
SERV
ICES

Council of GovernorsJune 2015
.33
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Andr
ew C
lem
ents
He
ad o
f Ope
ratio
ns
Plan
ned
Care
Ge
nera
l M
anag
er
Su
zann
e N
icho
lls
Pl
anne
d Ac
ute
and
Com
mun
.
Unp
lann
ed
Acut
e an
d Co
mm
un.
Ther
apie
s acr
oss
all a
cute
and
SO
L Co
mm
unity
Ge
nera
l M
anag
er
Unp
lann
ed
Care
Sally
Car
en
Vario
us
Child
rens
Co
mm
unity
Se
rvic
es
Gene
ral
Man
ager
Tr
ansf
orm
atio
n
Emm
a Ta
lla
N
urse
Lead
Ch
ildre
ns
Com
mun
ity
Ka
ty C
oate
s
Pr
ogra
mm
e M
anag
emen
t/De
liver
y St
rate
gies
Ther
apie
s M
ary
Ross
An
d ot
her
Clin
ical
Di
rect
ors
Rich
ard
Stey
n AM
D Va
ness
a W
ort
Head
Nur
se
SOLI
HULL
DIV
ISIO
N
Asso
c.
Head
N
urse
An
n Ed
gar
Nur
sing
Supe
rvis.
Nur
sing
Pr
ofes
s.
Advi
ce
Supe
rvis
ion

Council of GovernorsJune 2015
.34
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Phill
Lydd
on
Head
of O
pera
tions
Emer
gen
cy C
are
Grou
p Ge
nera
l M
anag
er
Ben
Rich
ards
Obs
tetr
ics
Ge
nera
l M
anag
er
Katy
Hog
an
Surg
ery
Grou
p Ge
nera
l M
anag
er
Che
ryl H
udso
n
Ad
mis
sion
s &
Disc
harg
e
Vaca
ncy
AMD
Bhav
na G
okan
i He
ad N
urse
O
bste
tric
s
Ope
ratio
nal
Depu
ty to
Ho
M
Trac
ey N
ash
M
atro
n M
idw
ifes
GHH
Asse
ssm
ent
& W
ards
M
aggi
e Co
lem
an
Deliv
ery
suite
Jo
selle
W
right
BH
H Lo
rna
Fost
er
ass/
war
ds
Carla
Ch
arle
s-Jo
nes
Deliv
ery
suite
Gyna
ecol
ogy
Ge
nera
l M
anag
er
Katy
Hog
an
Gyna
ecol
ogy
Mat
ron
Tr
acey
Nas
h
Paed
iatr
ics
Cl
inic
al
Dire
ctor
Ro
opa
Mul
ik
GH
H Cl
inic
al
Lead
An
jum
Ga
ndhi
Paed
iatr
ics
M
atro
n Am
ee
Deny
er
Gyna
ecol
ogy
Cl
inic
al
Dire
ctor
Ka
ther
ine
Barb
er
Clin
ical
Lea
d Pr
atim
a Gu
pta
Paed
iatr
ics
Ge
nera
l M
anag
er
Lynn
e Bo
wye
r
Obs
tetr
ics
Cl
inic
al
Dire
ctor
Ka
ther
ine
Barb
er
GHH
Site
Le
ad
Liz
How
land
Wom
en &
Chi
ldre
n's D
ivis
ion
Joy
Payn
e He
ad o
f Mid
wife
ry
Obs
tetr
ics
Head
of
Safe
guar
ding
Ca
rol O
wen
Lead
Mid
wife
Go
vern
ance
&
Safe
ty
Jane
t Pol
lard
MLU
& C
omm
unity
Kare
n M
cGui
gan

Council of GovernorsJune 2015
.35
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Dire
ctor
of W
orkf
orce
Ha
zel G
unte
r
Head
of T
rans
actio
nal
HR
Ray
Reyn
olds
- Rec
ruitm
ent
- Ban
k - E
mpl
oyee
Ser
vice
s - W
orkf
orce
Info
rmat
ion
Depu
ty D
irect
or o
f W
orkf
orce
/
Head
of O
pera
tiona
l HR
(inte
rim K
yria
cos K
yria
cou
6 m
onth
s)
(And
rew
McM
enem
y fr
om 2
9.06
.15)
- Ope
ratio
nal H
R - P
olic
y De
velo
pmen
t - O
ccup
atio
nal H
ealth
- S
ervi
ce T
rans
form
atio
n - W
orkf
orce
Pla
nnin
g
Head
of F
acul
ty
(Inte
rim)
Clai
re W
hitt
le
- Edu
catio
n - T
rain
ing
Head
of O
D Al
ex C
ovey
- Cul
ture
- E
ngag
emen
t - L
eade
rshi
p

Council of GovernorsJune 2015
.36
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Depu
ty D
irect
or o
f W
orkf
orce
/ He
ad o
f Ope
ratio
nal H
R (in
terim
Kyr
iaco
s Kyr
iaco
u 6
mon
ths)
(A
ndre
w M
cMen
emy
from
29.
06.1
5)
Al
ison
M
oney
Seni
or H
R Bu
sines
s Pa
rtne
r •B
HH S
ite
Mar
k Ti
pton
HR
Bu
sines
s Pa
rtne
r •G
ood
Hope
Si
te
Je
an
Deve
nney
HR
Busin
ess
Part
ner
•Cor
pora
te
& F
acili
ties
Hele
n Ba
rlow
HR
Bu
sines
s Pa
rtne
r •P
olic
ies
&
Proj
ects
Sara
Woo
d •W
ork
&
Wel
lbei
ng
Ju
lie
Stew
ard
•Wor
kfor
ce
Plan
ning
Fr
ieza
M
ahm
ood
HR
Busin
ess
Part
ner
•Sol
ihul
l Site
Leea
nne
Stok
es
HR B
usin
ess
Cons
ulta
nt
BHH
Nat
alie
Coo
ke
HR B
usin
ess
Cons
ulta
nt
W&
C
Laur
a G
raha
m
HR B
usin
ess
Cons
ulta
nt
CSS
OPE
RAT
ION
AL H
R M
ANAG
EMEN
T ST
RU
CTU
RE

Council of GovernorsJune 2015
.37
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
OD
TEAM
PRO
POSE
D ST
RUCT
URE
Alex
Cov
ey
Head
of O
D
Amy
Pass
ey
OD
Man
ager
St
aff E
ngag
emen
t
•En
gage
men
t Pr
ogra
mm
es
•St
aff S
urve
ys
tbc
OD
Man
ager
Cu
lture
& V
alue
s
•Va
lues
dev
elop
men
t •
Beha
viou
ral
fram
ewor
ks
•Su
ppor
t im
plem
enta
tion
of
Valu
es &
Beh
avio
urs
into
oth
er w
orki
ng
prac
tices
tb
c O
D M
anag
er
Tale
nt M
anag
emen
t
•Pr
ogra
mm
e le
ader
ship
•
Appr
aisa
l •
Tale
nt M
anag
emen
t •
Succ
essio
n Pl
anni
ng
Bi
ll N
utta
ll Le
ader
ship
Spe
cial
ist
(int
erim
12
mth
s)
•
Lead
ersh
ip
Deve
lopm
ent
Plan
s •
Appr
aisa
l •
Succ
essio
n Pl
anni
ng
Da
niel
le G
odda
rd
Cultu
re &
En
gage
men
t Pro
ject
M
anag
er
(inte
rim 6
mon
ths)
•Pr
ogra
mm
e m
anag
e Cu
lture
&
Enga
gem
ent
Wor
kstr
eam
s

Council of GovernorsJune 2015
.38
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Actin
g De
puty
Hea
d of
Ed
ucat
ion
Clai
re W
hitt
le
Asso
ciat
e De
an
Wor
kfor
ce
Deve
lopm
ent
Sa
ra Ja
skie
wic
z
•He
alth
care
Ca
reer
s De
velo
pmen
t Uni
t (H
CDU
) •
Prof
essio
nal
Educ
atio
n fo
r N
urse
s, M
idw
ives
&
AHP
s
Asso
ciat
e De
an
Lear
ning
, In
nova
tion
&
Desi
gn
Tr
acey
St
arke
y-M
oore
•Cl
inic
al S
kills
&
Sim
ulat
ion
•M
oodl
e •
Libr
arie
s
Actin
g De
puty
He
ad o
f Ed
ucat
ion
Acad
emic
Affa
irs
& B
usin
ess
Deve
lopm
ent
Cl
aire
Whi
ttle
•Ac
adem
ic C
ours
es
•Fa
culty
Bus
ines
s U
nit (
FBU
) ad
min
istra
tion
team
Asso
ciat
e De
an
Qua
lity
Assu
ranc
e &
Co
re C
ompl
ianc
e Ka
ren
Shar
p •
Man
dato
ry T
rain
ing
•Ed
ucat
ion
Qua
lity
Assu
ranc
e •
Pre
Reg
Non
-M
edic
al E
duca
tion
•Ac
cess
, Sys
tem
s &
Ev
ents
(Ed
Cent
re
Man
agem
ent)
FACU
LTY
TEAM
STR
UCT
URE

Council of GovernorsJune 2015
.39
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chief Executive's Report
Ray
Reyn
olds
He
ad o
f Tra
nsac
tiona
l W
orkf
orce
and
Wor
kfor
ce
Info
rmat
ion
Cl
aire
Whi
te
Divi
sion
al
Man
ager
•Rec
ruitm
ent
•Med
ical
Wor
kfor
ce
•Em
ploy
men
t Co
mpl
ianc
e •M
edic
al W
orkf
orce
Lo
cum
Ban
k Te
ams
John
Hoo
d Em
ploy
ee
Serv
ices
Man
ager
•Pay
roll
•Pen
sion
s •C
ontr
acts
•E
xpen
ses
Jean
ette
Bul
lock
W
orkf
orce
In
form
atio
n M
anag
er
•Wor
kfor
ce
Info
rmat
ion
•KPI
s
Sally
Law
son
•Ser
vice
Tr
ansf
orm
atio
n •S
peci
alis
t HR
TRAN
SAC
TIO
NA
L H
R A
ND
WO
RK
FOR
CE
MAN
AGEM
ENT
STR
UC
TUR
E

Council of GovernorsJune 2015
.40
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Quality and PerformanceReport, including Finance
Integrated Quality and PerformanceReport, includingFinance

Council of GovernorsJune 2015
.41
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Inte
grat
ed P
erfo
rman
ce R
epor
t
Mon
th 1
- Ap
ril 2
015
1
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.42
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Qua
lity
and
Risk
12 14 15 16 17 18 19 21Ap
prai
sals
Man
dato
ry T
rain
ing
20In
fect
ion
Cont
rol
Sick
ness
Volu
ntar
y Tu
rnov
er a
nd R
ecru
itmen
t
22 23 24 25 26 27
Heat
Map
- A&
EAc
cide
nt a
nd E
mer
genc
yHe
at M
ap -
18 w
eeks
, Dia
gnos
tics,
Ope
ratio
ns18
Wee
ks R
TT a
nd O
pen
Cloc
ksDi
agno
stic
sO
pera
tions
Heat
Map
- Ca
ncer
sCa
ncer
s 2 W
eek
wai
t, 31
and
62
day
Sum
mar
yHe
at M
ap -
Nur
sing
Per
form
ance
Nur
sing
- In
jurio
us F
alls
Nur
sing
- Pr
essu
re U
lcer
s
Heat
map
- In
fect
ion
Cont
rol,
VTE,
Mor
talit
y
Nur
sing
Wor
kfor
ceN
ursi
ng V
acan
cies
Sect
ion
Page
Num
ber
Perf
orm
ance
Indi
cato
r
Heat
Map
- W
orkf
orce
Per
form
ance
Wor
kfor
ce a
nd W
ell-b
eing
Patie
nt E
xper
ienc
eM
etric
sCo
mpl
aint
s
Exec
utiv
e Su
mm
ary
3 4 5 6 7
Cont
ents
9 10 11
Emer
genc
y Ca
re
Plan
ned
Care
2
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.43
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
rgra
ted
Perf
orm
ance
Rep
ort -
Apr
il
Inte
grat
ed P
erfo
rman
ce R
epor
t
Exec
utiv
e Su
mm
ary
Perf
orm
ance
Ana
lysi
s Th
e m
ain
area
s of c
once
rn fo
r the
Tru
st re
mai
n ur
gent
car
e, R
TT a
nd d
iagn
ostic
s in
part
icul
ar in
end
osco
py.
Perf
orm
ance
aga
inst
the
A&E
4 ho
ur ta
rget
for A
pril
was
86.
25%
. Des
pite
the
signi
fcan
t inc
reas
e in
att
enda
nces
at H
eart
land
s and
Goo
d Ho
pe H
ospi
tal f
rom
Apr
il 20
14 to
Apr
il 20
15, t
here
has
bee
n an
impr
ovem
ent i
n A&
E 4
hour
co
mpl
ianc
e. O
vera
ll em
erge
ncy
adm
issio
ns h
ave
redu
ced
over
the
sam
e tim
e pe
riod.
Th
e ur
gent
car
e pa
thw
ay c
ontin
ued
to e
xper
ienc
e fu
rthe
r inc
reas
e in
dem
and
durin
g Ap
ril. T
his p
lace
d bo
th th
e He
artla
nds a
nd G
ood
Hope
Hos
pita
ls un
der s
igni
fican
t str
ain
in te
rms o
f hig
h be
d oc
cupa
ncy,
ED
cong
estio
n an
d de
lays
for l
arge
num
bers
of p
atie
nts w
aitin
g fo
r a b
ed to
bec
ome
avai
labl
e.
All t
hree
of t
he ta
rget
s for
refe
rral
to tr
eatm
ent w
ere
not a
chie
ved
this
mon
th. H
owev
er, b
oth
the
adm
itted
and
non
-adm
itted
pat
hway
hav
e im
prov
ed fr
om M
arch
to A
pril
as sh
own
in th
e he
at m
ap.
Traj
ecto
ries f
or re
duci
ng th
e RT
T ad
mitt
ed b
ackl
ogs h
ave
been
revi
sed
for 2
015/
16 a
nd th
e ov
eral
l bac
klog
(1,2
71) i
s per
form
ing
wel
l aga
inst
the
in m
onth
targ
et (1
,322
). Fr
om th
e ca
paci
ty v
ersu
s dem
and
wor
k un
dert
aken
it w
as
foun
d th
at to
ach
ieve
the
RTT
targ
ets t
he T
rust
will
nee
d to
app
roxi
mat
ely
unde
rtak
e an
add
ition
al 5
100
case
s com
pare
d to
201
4/15
. The
incr
ease
in d
eman
d is
pred
omin
antly
due
to u
rgen
t ref
erra
ls, th
is is
unde
r disc
ussio
n w
ith
the
CCGs
. Ga
stro
ente
rolo
gy (a
nd m
ore
spec
ifica
lly th
e En
dosc
opy
Serv
ice)
con
tinue
s to
expe
rienc
e in
crea
sed
dem
and
whi
ch si
gnifi
cant
ly im
pact
s on
the
over
all a
dmitt
ed b
ackl
og a
nd d
iagn
ostic
s com
plia
nce.
Th
ere
has b
een
a sig
nific
ant r
educ
tion
in h
ospi
tal l
ed c
ance
llatio
ns o
f ele
ctiv
e su
rger
y fr
om th
e pe
ak in
Janu
ary
to M
arch
. Th
e va
lidat
ed c
ance
r per
form
ance
for t
wo
wee
k w
aits
and
for b
reas
t sym
ptom
atic
targ
ets h
ave
faile
d in
Mar
ch 2
015.
The
re c
ontin
ues t
o be
an
abov
e av
erag
e in
the
num
ber o
f ref
erra
ls to
two
wee
k w
ait c
linic
s (in
clud
ing
brea
st
sym
ptom
atic
). Pe
rfor
man
ce a
gain
st th
e 31
and
62
day
canc
er ta
rget
s wer
e m
et in
Mar
ch 2
015,
99.
41%
and
86.
24%
resp
ectiv
ely.
Th
ere
have
bee
n no
new
cas
es o
f pos
t 48
hour
MRS
A ba
cter
aem
ia in
Apr
il, th
ere
is a
zero
tole
ranc
e ta
rget
for M
RSA
Bact
erae
mia
s in
2015
/16.
Clo
strid
ium
diff
icile
(C.d
iff) t
arge
t was
met
in A
pril
with
onl
y 2
case
s aga
inst
a ta
rget
of
less
than
6. T
he n
ew C
.diff
traj
ecto
ry fo
r 201
5/16
is m
ore
chal
leng
ing
this
year
, the
yea
r end
targ
et is
less
than
64
case
s. T
he T
rust
con
tinue
s to
mai
ntai
n go
od p
erfo
rman
ce in
falls
and
pre
ssur
e ul
cers
des
pite
an
incr
ease
in fr
ail a
nd
elde
rly p
atie
nts.
Re
crui
tmen
t of s
taff
espe
cial
ly n
ursin
g an
d m
edic
al st
aff
cont
inue
s to
be c
halle
ngin
g w
ith tu
rnov
er c
ontin
uing
to b
e ab
ove
targ
et. S
taff
sickn
ess h
as im
prov
ed th
is m
onth
and
is b
elow
the
new
201
5/16
traj
ecto
ry. T
he 8
5% ta
rget
fo
r man
dato
ry tr
aini
ng w
as a
chie
ved
in M
arch
201
5 (d
ata
is on
e m
onth
in a
rrea
rs).
The
appr
aisa
ls ta
rget
was
not
met
this
mon
th, h
owev
er th
ere
is an
impr
oved
per
form
ance
on
2014
/15.
App
raisa
l com
plet
ion
from
Apr
il is
now
re
port
ed a
s a ro
lling
12
mon
th p
ositi
on a
gain
st a
con
stan
t tar
get o
f 85%
acr
oss t
he w
hole
Tru
st.
3
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.44
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Per
cent
age
of A
mbu
lanc
e Se
rvic
es
Han
dove
r ≥
60
min
utes
0.00
%
0.00
%
5.95
%3.
96%
Emer
genc
y Ca
re
Heat
Map
- A&
E
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RK
TARGET
In month trajectory
Last
Mon
th
Trus
t (M
ar-1
5)H
eart
land
s H
ospi
tal
Goo
d H
ope
Hos
pita
lSo
lihul
l H
ospi
tal
Clin
ical
Su
ppor
t Se
rvic
es
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Apr
-15
Perf
orm
ance
Im
prov
emen
t
80.2
3%97
.82% 0
86.2
5% 1
AOS5
A&
E: m
axim
um w
aiti
ng
tim
e of
fou
r ho
urs
from
arr
ival
to
adm
issi
on/t
rans
fer/
disc
harg
e>
95%
83.6
1%86
.45%
4.88
%
0.24
%0.
25%
0.27
%0.
48%
0.28
%
ANQ
R9Tr
olle
y w
aits
in A
&E
long
er t
han
12
hou
rs
Per
cent
age
of A
mbu
lanc
e Se
rvic
es
Han
dove
r ≥
30
min
utes
20
10
7.31
%1.
45%
4
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.45
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
ED A
tten
danc
e (B
HH &
GHH
)
Emer
genc
y Le
ngth
of S
pell
(BHH
& G
HH)*
86.4
5%-7
.95%
16,8
1317
,909
6.52
%
Emer
genc
y Ca
re
Acci
dent
& E
mer
genc
y
Key
Emer
genc
y In
dica
tors
YTD
com
paris
onAp
rilAp
r-14
Apr-
15%
Var
ianc
e
A&E
Atte
ndan
ces a
nd A
mbu
lanc
e Ar
rival
s at H
eart
land
s & G
ood
Hope
Hos
pita
ls
Ambu
lanc
e Ar
rival
s5,
726
5,87
12.
53%
* Ba
sed
on p
atie
nts d
isch
arge
d fr
om a
dult
acut
e w
ards
onl
y
ED 4
hou
r per
form
ance
by
site
, Apr
-14
vs A
pr-1
5 co
mpa
rison
Emer
genc
y Ad
mis
sion
s (BH
H &
GHH
)6,
531
5,79
5-1
1.27
%7.
008.
2217
.43%
4 Ho
ur P
erfo
rman
ce (H
EFT,
no
WIs
)94
.40%
Head
lines
Th
e pe
rfor
man
ce in
Apr
il 20
15 w
as 8
6.25
%.
The
indi
vidu
al si
te p
ositi
on in
Mar
ch:
•He
artla
nds E
D (B
HH) –
86.
45%
,
•Go
od H
ope
ED (G
HH) –
80.
23%
, •
Solih
ull E
D (n
ow M
IU) –
97.
82%
.
Perf
orm
ance
Ana
lysi
s 1)
Incr
ease
d De
man
d Th
ere
cont
inue
s to
be a
n in
crea
sing
dem
and
plac
ed o
n em
erge
ncy
depa
rtm
ents
(ED)
at H
eart
land
s and
Goo
d Ho
pe
Hosp
itals.
The
incr
ease
in a
tten
danc
es co
ntin
ued
in th
e fir
st w
eeks
of A
pril
2015
, rea
chin
g a
peak
of 4
,238
at
tend
ance
s dur
ing
wee
k en
ding
19/
04/2
015
(for B
HH a
nd G
HH).
Co
mpa
ring
April
201
4 to
Apr
il 20
15, B
HH a
nd G
HH h
ad 1
,096
mor
e at
tend
ance
s. T
his i
ncre
ase
equa
tes t
o an
ad
ditio
nal 2
0 an
d 17
att
enda
nces
per
day
to B
HH a
nd G
HH E
Ds re
spec
tivel
y.
2) B
reac
h &
Cap
acity
Th
e m
ajor
ity o
f bre
ache
s (52
.35%
) wer
e du
e to
aw
aitin
g a
bed
or n
o ro
om in
AM
U .
Capa
city
issu
es a
re a
lso im
pact
ed
by th
e in
crea
se in
the
aver
age
cycl
e tim
e of
pat
ient
s in
AMU
are
as w
ho a
re la
ter t
rans
ferr
ed to
bas
e w
ards
. Co
mpa
ring
April
-14
to A
pril-
15:
•BH
H AM
U -
incr
ease
from
14.
09 h
ours
in A
pril
2014
to 1
9.37
hou
rs in
Apr
il 20
15 (+
37.5
% v
aria
nce)
. •
GHH
AMU
- in
crea
se fr
om 1
0.05
hou
rs in
Apr
il 20
14 to
26.
97 h
ours
in A
pril
2015
(+16
8.4%
var
ianc
e).
Th
e m
edia
n tim
e fo
r pat
ient
s in
ED w
ho a
re la
ter a
dmitt
ed to
hos
pita
l has
also
rem
aine
d hi
gh. T
he in
crea
se h
as b
een
as fo
llow
s:
•W
hen
BHH
last
ach
ieve
d th
e 95
% 4
Hou
r tar
get (
Janu
ary
2014
) m
edia
n tim
e in
ED
was
190
min
utes
. In
cont
rast
, du
ring
April
201
5 th
e m
edia
n tim
e in
BHH
ED
is sig
nific
antly
incr
ease
d at
221
min
utes
. •
Med
ian
time
in G
HH E
D w
as 1
93 m
inut
es in
Janu
ary
2011
(the
last
tim
e GH
H ac
hiev
ed th
e 4
hour
targ
et).
Curr
ently
, m
edia
n tim
e in
GHH
ED
is 27
1 m
inut
es.
Apr-14, 94.40%
Apr-14, 93.46%
Apr-14, 93.40%
Apr-14, 98.63%
Apr-15, 86.25%
Apr-15, 86.45%
Apr-15, 80.23%
Apr-15, 97.82%
60.0
0%
65.0
0%
70.0
0%
75.0
0%
80.0
0%
85.0
0%
90.0
0%
95.0
0%
100.
00%
Trus
t (no
WIC
)H
eart
land
sG
ood
Hop
eSo
lihul
l
A&E
4 ho
urs P
erfo
rman
ce: A
pr-1
4 vs
Apr
-15
Actio
ns T
aken
•
Laun
ch o
f ‘Dr
ive
for D
ischa
rge’
. Thi
s is a
n in
itiat
ive
to e
nsur
e av
aila
bilit
y of
six
AMU
and
two
SAU
spac
es a
t key
po
ints
dur
ing
the
day
to im
prov
e flo
w to
the
asse
ssm
ent u
nits
. Thi
s has
bee
n im
plem
ente
d to
cre
ate
capa
city
and
ke
ep th
e ED
s saf
e by
redu
cing
the
num
ber o
f bre
ache
s due
to n
o sp
ace
in A
MU
. •
Plan
ned
esta
tes w
ork
to c
reat
e a
larg
er E
D m
ajor
s are
a ha
s beg
un. T
his w
ill se
e ED
min
ors t
akin
g ov
er fr
actu
re
clin
ic a
nd fr
actu
re cl
inic
mov
ing
into
the
ther
apie
s dep
artm
ent.
This
mea
ns E
D M
ajor
s to
doub
le in
size
allo
win
g be
tter
man
agem
ent o
f the
surg
es in
our
mos
t acu
tely
unw
ell p
atie
nts.
•11
hou
rs o
f priv
ate
ambu
lanc
es co
ver w
as p
rovi
ded
to b
oth
GHH
and
BHH
sites
Mon
day
to F
riday
to su
ppor
t pa
tient
disc
harg
e. T
wo
new
disc
harg
e lo
unge
s ope
ned
on e
ach
site
to c
reat
e ea
rly fl
ow in
the
hosp
ital.
5
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.46
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
89.6
1%
92.3
1%91
.22%
88.1
8%
AOS1
Adm
itte
d P
atie
nts
Trea
ted
wit
hin
18
Wee
ks
of R
efer
ral (
mia
)
AOS2
Non
-Adm
itte
d P
atie
nts
Trea
ted
wit
hin
18
W
eeks
of
Ref
erra
l (m
ia)
> 9
5%89
.83%
82.0
9%
93.1
0%
Heat
Map
- 18
Wee
ks, D
iagn
ostic
s, O
pera
tions
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RK
TARGET
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Apr
-15
Perf
orm
ance
Im
prov
emen
tH
eart
land
s H
ospi
tal
Goo
d H
ope
Hos
pita
lSo
lihul
l H
ospi
tal
Clin
ical
Su
ppor
t Se
rvic
es
Plan
ned
Care
In month trajectory
Last
Mon
th
Trus
t (M
ar-1
5)
No
urge
nt o
pera
tion
can
celle
d fo
r th
e 2
nd
tim
e
90.6
3%
> 9
0%78
.92%
83.6
9%83
.72%
78.6
6%
92.1
0%D
iagn
osti
cs w
aiti
ng
tim
es le
ss t
han
6 w
eeks
> 9
9%
Can
celle
d op
erat
ions
not
off
ered
ano
ther
da
te w
ithi
n 2
8 d
ays
AOS3
18
wee
k in
com
plet
e pa
thw
ays
(mia
)>
92%
90.2
6%88
.89%
90.9
1%88
.99%
6
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.47
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
18 W
eeks
- Re
ferr
al to
Tre
atm
ent (
RTT)
Plan
ned
Care
18 w
eeks
Bac
klog
Tabl
e: H
igh
risk
Spec
ialti
es a
gain
st th
e O
vera
ll RT
T Pe
rfor
man
ce (A
pril
2015
)
Lega
cy O
pen
Cloc
ks c
losu
re im
apct
on
path
way
s
Head
lines
•
April
Adm
itted
Per
form
ance
: 82
.09%
. •
April
Non
-Adm
itted
Per
form
ance
: 93
.10%
. •
April
Inco
mpl
ete
Perf
orm
ance
: 89.
61%
52
Wee
k Br
each
Pos
ition
: The
re a
re 8
pat
ient
s wai
ting
mor
e th
an 5
2 w
eeks
on
the
inco
mpl
ete
path
way
at t
he e
nd o
f Apr
il. T
here
wer
e 59
patie
nts b
reac
hed
the
52 w
eek
stan
dard
in A
pril,
all
of th
ese
patie
nts b
reac
hed
due
to c
losu
re o
f leg
acy
open
clo
ck
path
way
s.
Perf
orm
ance
Ana
lysi
s Ca
ncel
latio
n of
Sur
gery
(on
& b
efor
e th
e da
y of
adm
issi
on)
18 p
atie
nts w
ere
canc
elle
d in
Apr
il, a
ll w
ere
due
to n
o be
ds a
vaila
ble
(BHH
- 15
, SO
L - 2
, GHH
- 1)
. Rel
ativ
e to
pre
viou
s m
onth
s, th
is is
a sm
all i
ncre
ase
on M
arch
whe
n 11
pat
ient
s wer
e ca
ncel
led.
O
ne o
f the
se p
atie
nts w
as o
n th
e ca
ncer
pat
hway
requ
iring
a c
ritic
al c
are
bed,
the
RCA
has b
een
com
plet
ed a
nd a
n ac
tion
plan
is in
pla
ce.
Ba
cklo
g Th
e nu
mbe
r of p
atie
nts i
n th
e ba
cklo
g at
the
end
of A
pril
was
1,2
71 v
ersu
s an
expe
cted
bac
klog
traj
ecto
ry p
ositi
on o
f 1,
322.
All
spec
ialti
es w
ith th
e ex
cept
ion
of U
rolo
gy a
nd G
astr
oent
erol
ogy
ache
ived
thei
r pre
dict
ed tr
ajec
tory
with
O
rtho
pead
ics o
ver a
chei
ving
by
76 p
atie
nts.
Th
e m
ain
spec
ialti
es co
ntnu
ing
to c
ontr
ibut
ing
to th
e ba
cklo
g ar
e as
follo
ws :
•
Gast
roen
tero
logy
= 3
87, 3
0.4%
of t
otal
bac
klog
. •
Ort
hopa
edic
= 2
51, 1
9.7%
of t
otal
bac
klog
. •
Gene
ral S
urge
ry =
167
, 13.
1% o
f tot
al b
ackl
og.
•U
rolo
gy =
135
, 10.
6% o
f tot
al b
ackl
og.
The
over
all b
ackl
og p
ositi
on fo
r May
is o
n ta
rget
for d
eliv
ery.
1198
1180
1182
1501
1285
1284
1231
1314
1253
1271 1322
1286
1314
1350
1337
1207
1079
928
809
741
701
589
0
200
400
600
800
1000
1200
1400
1600
Apr-14
May-14
Jun-14
Jul-14
Aug-14
Sep-14
Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
Apr-15
May-15
Jun-15
Jul-15
Aug-15
Sep-15
Oct-15
Nov-15
Dec-15
Jan-16
Feb-16
Mar-16
Back
log
Traj
ecto
ry
143
145
113
177
174
188
204
166
169
146
157
175
228
255
240
238
193
176
170
186
188
188
203
212
225
247
299
320
337
350
337
050100
150
200
250
300
350
400
Back
log
Traj
ecto
ry
7
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.48
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
0-17
1819
-25
26-3
738
-51
52+
Tota
l12
5159
231
209
3717
8710
0815
5135
81
1118
820
3297
107
1010
6660
434
130
105
303
906
548
1753
614
683
377
2158
6715
538
341
1572
718
507
274
626
4310
359
Ope
n Cl
ocks
- Pa
tient
s who
hav
e at
tend
ed b
ut h
ave
no fu
rthe
r app
oint
men
t boo
ked
18 W
eeks
- O
pen
Cloc
ks
Plan
ned
Care
Ope
n Cl
ocks
pro
file
@15
/05/
2015
Ope
n Cl
ocks
with
no
futu
re a
ppoi
ntm
ent b
ooke
d - T
op 8
Spe
cial
ties
% o
f tot
al o
pen
cloc
ks >
18
wks
Gra
nd T
otal
Wee
ks
5971
252
916
869
176
481
88
Spec
ialty
Gas
troe
nter
olog
yCa
rdio
logy
T&O
Uro
logy
Gyn
aeG
en S
urg
Derm
atol
ogy
Resp
Med
24.1
8%4.
96%
11.1
0%13
.62%
6.09
%7.
26%
7.49
%3.
83%
Perf
orm
ance
Ana
lysi
s Ei
ght p
atie
nts r
emai
n on
an
open
cloc
k pa
thw
ay w
aitin
g 52
wee
ks o
r mor
e. A
ll bu
t tw
o pa
tient
s are
exp
ecte
d to
ha
ve th
eir p
athw
ay c
lose
d in
May
. The
se tw
o pa
tient
s are
und
ergo
ing
furt
her d
iagn
ostic
inte
rven
tions
follo
win
g fa
ce to
face
con
sulta
tion.
Th
ere
is st
ill a
sign
ifica
nt p
eak
of p
atie
nts o
n an
ope
n cl
ock
path
way
bet
wee
n 19
and
25
wee
ks. T
he n
ew P
atie
nt-
targ
eted
list
(PTL
) pro
vide
s bet
ter v
isabl
ity fo
r tea
ms t
o m
anag
e th
eir p
atie
nts o
n an
ope
n cl
ock
path
way
. Ga
stro
entr
olog
y ac
coun
ts fo
r 24.
18%
of t
otal
pat
ient
s with
an
open
cloc
k of
mor
e th
an 1
8 w
eeks
and
no
plan
ned
futu
re a
ppoi
ntm
ent.
Oth
er sp
ecia
lties
that
acc
ount
for m
ore
than
10%
of t
his g
roup
are
: •
T&O
- 1
1.10
%
•U
rolo
gy -
13.6
2%
Furt
her A
ctio
ns
•RC
As w
ill b
e un
dert
aken
on
both
pat
ient
s wai
ting
long
er th
an 5
2wee
ks w
hen
thei
r tre
atm
ents
are
com
plet
ed,
this
will
incl
ude
a re
view
of h
arm
. •
PTL
wil
be m
onito
red
thro
ugh
the
18 w
eek
and
Canc
er m
eetin
g w
ith a
ll Di
visio
ns h
avin
g in
tern
al p
roce
dure
s in
plac
e to
ens
ure
impr
oved
pat
hway
s man
agem
ent o
f pat
ient
s.
59
15
32
34
17
21
15
6
231
51
97
130
53
58
72
26
209
35
107
105
61
67
71
43
37
8
10
30
4 15
8
10
0
100
200
300
400
500
600
Gas
tro
Card
iolo
gyT&
OU
rolo
gyG
ynae
Gen
Sur
gDe
rmat
olog
yRe
sp M
ed
1819
-25
26-3
738
-51
52+
8
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.49
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
No.
> 6
W
eeks
% w
ithin
6
wee
ksN
o. >
6
Wee
ks%
with
in
6 w
eeks
199
.96%
299
.87%
010
0.00
%0
-0
100.
00%
584
.38%
199
.79%
0-
0-
691
.78%
1278
.18%
274
57.1
2%17
857
.72%
2784
.39%
363
62.6
9%86
992
.10%
Neu
roph
ysio
logy
- pe
riphe
ral n
euro
phys
iolo
gy
Diag
nost
ics S
umm
ary
Diag
nost
ics t
ests
seen
with
in 6
wee
ks
Diag
nost
ics t
ests
seen
with
in 6
wee
ks
Mag
netic
Res
onan
ce Im
agin
gCo
mpu
ted
Tom
ogra
phy
Non
-obs
tetr
ic u
ltras
ound
Bariu
m E
nem
aDE
XA S
can
Uro
dyna
mic
s - p
ress
ures
& fl
ows
Cyst
osco
py
Audi
olog
y - A
udio
logy
Ass
essm
ents
Card
iolo
gy -
echo
card
iogr
aphy
Plan
ned
Care
Imag
ing
Phys
iolo
gica
l M
easu
rem
ent
Endo
scop
y
Tota
lGa
stro
scop
y
Mar
-15
Apr-
15Te
st
Resp
irato
ry p
hysio
logy
- sle
ep st
udie
s
Colo
nosc
opy
Flex
i sig
moi
dosc
opy
Card
iolo
gy -
elec
trop
hysio
logy
Head
lines
En
dosc
opy
and
the
rela
ted
Gast
roen
tero
logy
serv
ice
is co
nsid
ered
to b
e th
e sp
ecia
lty o
f hig
hest
risk
in S
ched
uled
Ca
re.
Chan
ge in
NIC
E gu
idlin
es a
re d
ue to
be
in e
ffect
from
the
end
of Ju
ne. T
hese
chan
ges w
ill fu
rthe
r inc
reas
e th
e de
man
d on
the
serv
ices
and
retu
rn to
com
plia
nce
will
not
be
met
unt
il la
ter i
n th
e ye
ar.
Perf
orm
ance
Ana
lysi
s Th
e nu
mbe
r of p
atie
nts o
n th
e En
dosc
opy
adm
itted
wai
ting
list h
as in
crea
sed
signi
fican
tly fr
om 5
78 in
Oct
ober
201
4 to
2,4
43 p
atie
nts a
t the
end
of A
pril
with
360
wai
ting
18 w
eeks
or m
ore.
Th
e Tr
ust h
as fa
iled
its 6
wee
k 99
% d
iagn
ostic
targ
et si
nce
Sept
embe
r 201
4 du
e to
the
dete
riora
tion
of p
erfo
rman
ce
with
in e
ndos
copy
. Ac
tions
Tak
en
•A
rem
edia
l act
ion
plan
(RAP
) for
the
serv
ice
was
subm
itted
to th
e CC
G de
taili
ng a
traj
ecto
ry to
retu
rn to
6 w
eek
com
plia
nce.
Acc
ordi
ng to
the
revi
sied
traj
ecto
ry, d
iagn
ostic
com
plia
nce
is ex
pect
ed to
retu
rn to
the
99%
targ
et in
Se
ptem
ber 2
015.
(Thi
s is d
epen
dant
on
addi
tiona
l cap
acity
)
99.51%
99.89%
99.74%
99.29%
98.53%
99.91%
99.79%
99.29%
99.75%
99.46%
99.57%
99.66%
99.17%
99.32%
99.22%
99.02%
98.44%
95.15%
98.03%
94.90%
93.48%
93.81%
92.10%
90.63%
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
% <
6wks
Targ
etM
ON
ITO
R tr
ajec
tory
Valid
ated
su
mm
ary
figur
es fo
r Ap
ril w
ill b
e up
date
d in
ne
xt m
onth
s re
port
9
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.50
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
Apr-
151
03
11
34
34
32
30
21
21
11
00
11
0
Plan
ned
Care
Canc
elle
d O
pera
tions
Brea
ches
of 2
8 da
y el
ectiv
e gu
aran
tee
Urg
ent O
pera
tions
Can
celle
d fo
r 2nd
Tim
e
Perc
enta
ge o
f Can
celle
d O
pera
tions
on
the
day
Urg
ent o
pera
tions
can
celle
d fo
r a se
cond
tim
e
Hosp
ital l
ed O
pera
tions
can
celle
d on
the
day
Head
lines
Th
ere
wer
e 75
hos
pita
l led
can
celle
d op
erat
ions
on
the
day
durin
g Ap
ril-1
5, a
slig
ht in
crea
se w
hen
com
pare
d w
ith th
e pr
evio
us m
onth
(72)
. 38
(51%
) of t
he ca
ncel
led
oper
atio
ns w
ere
at G
ood
Hope
, 21
(28%
) at H
eart
land
s and
16
(21%
) at S
olih
ull.
1
pate
int w
ith c
ance
r was
can
celle
d on
the
day
of th
eir s
urge
ry d
ue to
no
Criti
cal C
are
bed
In a
dditi
on tw
o pa
tient
s had
thei
r ‘ur
gent
’ ope
ratio
n ca
ncel
led
for a
seco
nd ti
me
at d
urin
g Ap
ril.
Perf
orm
ance
Ana
lysi
s Th
e fo
llow
ing
reas
ons a
ccou
nt fo
r 85%
of t
he H
ospi
tal l
ed c
ance
lled
oper
atio
ns o
n th
e da
y du
ring
April
201
5; R
an o
ut
of ti
me
(28)
, Sta
ff un
avai
labl
e (1
7),
Equi
pmen
t fai
lure
(11)
and
No
bed
(8).
•Th
ere
wer
e 28
(37%
) can
celle
d op
erat
ions
due
to a
lack
of t
ime,
11
at G
ood
Hope
, 10
at S
olih
ull a
nd 7
at
Hear
tland
s. T
he o
pera
tions
wer
e ca
ncel
led
by O
rtho
paed
ics (
8), G
ynae
colo
gy (7
), Ge
nera
l Sur
gery
(5),
Oph
thal
mol
ogy
(3),
Uro
logy
(3) a
nd T
hora
cic
Surg
ery
(2).
•17
ope
ratio
ns (2
3%) w
ere
canc
elle
d du
e to
staf
f mem
bers
bei
ng u
nava
ilabl
e, 1
4 of
thes
e w
ere
at G
ood
Hope
Ho
spita
l and
3 a
t Hea
rtla
nds H
ospi
tal.
10 o
f the
can
celle
d op
erat
ions
at G
ood
Hope
was
due
to n
o an
aest
hetis
t be
ing
avai
labl
e, th
is le
ad to
Oph
thal
mol
ogy
(9) a
nd C
ardi
olog
y (1
) can
celli
ng o
pera
tions
. •
11 o
pera
tions
(15%
) wer
e ca
ncel
led
due
to e
quip
men
t fai
lure
, 8 a
t Goo
d Ho
pe H
ospi
tal a
nd 3
at S
olih
ull H
ospi
tal.
•8
(11%
) ope
ratio
ns w
ere
canc
elle
d du
e to
no
bed,
7 w
ere
at H
eart
land
s and
1 a
t Sol
ihul
l. Ac
tions
take
n •
RCA
unde
rtak
en to
iden
tify
unde
rlyin
g ca
use
for p
atie
nt ca
ncel
led
with
can
cer.
Esca
latio
n pr
oces
s has
bee
n re
view
ed, r
eite
rate
d an
d en
hanc
ed a
s a re
sult.
•
Wee
kly
thea
tre
sche
dulin
g m
eetin
gs in
pla
ce to
faci
litat
e a
two
wee
k fo
rwar
d. T
his w
ill id
entif
y po
tent
ial i
ssue
s w
ith li
sts a
nd im
prov
e ef
ficie
ncy.
The
se m
eetin
gs h
ave
star
ted
to im
prov
e se
ssio
n ut
ilisa
tion
from
84.
79%
in M
arch
to
86.
16%
in A
pril
•
The
Thea
tre
Util
isatio
n Pr
ojec
t com
men
ced
in A
pril,
the
two
core
wor
kstr
eam
s are
pre
-ope
rativ
e pr
oces
s and
th
eatr
e sc
hedu
ling.
0.95%
0.77%
1.19%
1.36%
1.83%
1.33%
1.26%
0.93%
1.94%
1.95%
1.47%
0.87%
0.80
%
0.00
%
0.50
%
1.00
%
1.50
%
2.00
%
2.50
%
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
% C
ance
lled
Ops
201
4/15
% C
ance
lled
Ops
201
3/14
Targ
et
72
65
80
86
109
86
96
53
70
88
44
68
73
60
78
89
108
93
89
67
127
164
121
72
75
020406080100
120
140
160
180
Apr-13
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
Nov-13
Dec-13
Jan-14
Feb-14
Mar-14
Apr-14
May-14
Jun-14
Jul-14
Aug-14
Sep-14
Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
Apr-15
10
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.51
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Plan
ned
Care
Heat
Map
- Ca
ncer
s (m
ia)
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RKLa
st M
onth
Tr
ust
(Feb
-15)
Hea
rtla
nds
Hos
pita
lG
ood
Hop
e H
ospi
tal
Solih
ull
Hos
pita
l
Clin
ical
Su
ppor
t Se
rvic
es
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Mar
-15
Perf
orm
ance
Im
prov
emen
t
AOS6
Patie
nts
first
see
n by
a s
peci
alis
t w
ithin
tw
o w
eeks
w
hen
urge
ntly
ref
erre
d by
the
ir G
P or
den
tist
with
su
spec
ted
canc
er (
mia
)>
93%
89.6
2%(M
ar-1
5)
AOS1
2Pa
tient
s re
ceiv
ing
thei
r fir
st d
efin
itive
tre
atm
ent
for
canc
er w
ithin
tw
o m
onth
s (6
2 da
ys)
of G
P or
de
ntis
t ur
gent
ref
erra
l for
sus
pect
ed c
ance
r (m
ia)
> 8
5%
AOS9
Patie
nts
rece
ivin
g su
bseq
uent
tre
atm
ent
(sur
gery
an
d dr
ug t
reat
men
t on
ly)
with
in o
ne m
onth
(31
da
ys)
of a
dec
isio
n to
tre
at -
Sur
gery
Mod
ality
(m
ia)
> 9
4%
AOS1
0
Patie
nts
rece
ivin
g su
bseq
uent
tre
atm
ent
(sur
gery
an
d dr
ug t
reat
men
t on
ly)
with
in o
ne m
onth
(31
da
ys)
of a
dec
isio
n to
tre
at -
Ant
i Can
cer
Dru
g M
odal
ity (
mia
)
> 9
8%
AOS7
Patie
nts
first
see
n by
a s
peci
alis
t w
ithin
tw
o w
eeks
w
hen
urge
ntly
ref
erre
d by
the
ir G
P w
ith a
ny
brea
st s
ympt
om e
xcep
t su
spec
ted
canc
er (
mia
)>
93%
99.4
1%(M
ar-1
5)94
.29%
(Mar
-15)
96.3
3%(M
ar-1
5)93
.09%
(Mar
-15)
96.9
2%(M
ar-1
5)
100%
(Mar
-15)
100%
(Mar
-15)
AOS8
Patie
nts
rece
ivin
g th
eir
first
def
initi
ve t
reat
men
t w
ithin
one
mon
th (
31 d
ays)
of
a de
cisi
on t
o tr
eat
(as
a pr
oxy
for
diag
nosi
s) f
or c
ance
r (m
ia)
> 9
6%
N/A
94.7
2%(M
ar-1
5)
99.2
4%(M
ar-1
5)
82.9
5%(M
ar-1
5)
QS8
Patie
nts
rece
ivin
g th
eir
first
def
initi
ve t
reat
men
t fo
r ca
ncer
with
in 1
00 d
ays
of G
P or
den
tist
urge
nt
refe
rral
for
sus
pect
ed c
ance
r (m
ia)
100%
AOS1
3Pa
tient
s re
ceiv
ing
thei
r fir
st d
efin
itive
tre
atm
ent
for
canc
er w
ithin
tw
o m
onth
s (6
2 da
ys)
of u
rgen
t re
ferr
al f
rom
the
nat
iona
l scr
eeni
ng s
ervi
ce (
mia
)>
90%
71.4
3% (
Feb-
15)
100%
(Mar
-15)
83.3
3%(M
ar-1
5)
92.7
4%(F
eb-1
5
92.3
3% (
Feb-
15)
98.8
4% (
Feb-
15)
100%
(Feb
-15)
100%
(Feb
-15)
81.9
8% (
Feb-
15)
91.3
8%(M
ar-1
5)
89.3
8%(M
ar-1
5)
85.9
0%(M
ar-1
5)
66.6
7%(M
ar-1
5)
97.9
9%(M
ar-1
5)
TARGET
11
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.52
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
81.0
4%77
.91%
70.0
4%80
.11%
79.1
2%78
.75%
89.3
8%90
.36%
88.9
5%91
.24%
92.7
4%91
.38%
--
--
--
-88
.90%
88.9
0%90
.50%
91.5
0%93
.00%
60.5
9%65
.38%
55.2
4%82
.69%
83.5
8%85
.23%
88.0
8%87
.50%
81.0
5%76
.61%
92.3
3%89
.38%
--
--
--
-88
.50%
89.5
0%90
.50%
92.6
0%93
.60%
SPC
of T
wo
wee
k w
ait r
efer
rals
Indi
cato
rTa
ble
1: T
wo
wee
k w
aits
/Bre
ast S
ympt
oms:
per
cent
age
of p
atie
nts s
een
in 2
wee
ks
2 W
eek
Wai
t (T
93%
)M
onito
r Pla
n2
Wee
k W
ait -
(T93
%) B
reas
t Sym
ptom
sM
onito
r Pla
n
Plan
ned
Care
Canc
ers -
Tw
o w
eek
wai
t Per
form
ance
Conv
ersi
on ra
te fo
r Dia
gnos
is o
f Can
cer a
fter
2-w
eek
wai
t clin
ics
Two
Wee
k W
ait B
reac
hes (
inc
Brea
st)
Head
lines
Tw
o w
eek
wai
t per
form
ance
(Tar
get 9
3%),
Mar
ch 9
1.4%
(bel
ow tr
ajec
tory
).
Brea
st S
ympt
omat
ic tw
o w
eek
wai
t per
form
ance
Mar
ch 8
9.38
% (s
light
dec
reas
e fr
om 9
2.33
% in
Feb
ruar
y).
Perf
orm
ance
Ana
lysi
s Th
e vo
lum
e of
two
wee
k w
aits
refe
rral
s con
tinue
s to
be a
bove
ave
rage
. Add
ition
al ca
paci
ty is
bei
ng p
ut in
to p
lace
bu
t the
rate
of g
row
th is
exc
eedi
ng w
hat h
as b
een
plan
ned.
Thi
s is l
ikel
y to
be
exac
erba
ted
by th
e N
ICE
guid
ance
pu
ttin
g ac
hiev
emen
t of t
wo
wee
k w
aits
per
form
ance
at r
isk.
The
num
ber o
f pat
ient
s pos
itive
ly d
iagn
osed
with
can
cer r
educ
ed b
y 40
pat
ient
s (20
01 in
13/
14 v
196
1 in
14/
15).
Derm
atol
ogy,
Gyn
aeco
logy
, Upp
er a
nd Lo
wer
GI s
aw th
e m
ost s
igni
fican
t inc
reas
e in
refe
rral
rate
and
redu
ctio
n in
co
nver
sion
rate
. Tw
o w
eek
wai
t bre
ache
s (in
clud
ing
Brea
st) h
ave
mos
tly b
een
due
to p
atie
nt ch
oice
. The
pro
port
ion
of b
reac
hes d
ue
to p
atie
nt ch
oice
has
bee
n sig
nific
antly
hig
her t
han
capa
city
sinc
e O
ctob
er 2
014.
Ac
tions
Tak
en
•HE
FT re
pres
enta
tives
met
San
dwel
l and
City
cou
terp
arts
in A
pril
to d
iscus
s how
they
impr
oved
thei
r per
form
ance
, sp
ecifi
cally
in su
spec
ted
and
exhi
bite
d tw
o w
eek
wai
t Bre
ast r
efer
rals.
A si
gnifi
cant
fact
or w
as tr
ansf
er o
f ser
vice
s to
one
site
. A m
ulti-
disc
iplin
ary
grou
p w
ill d
iscus
s bre
ast p
erfo
rman
ce a
nd a
gree
furt
her s
hort
and
long
term
ac
tions
that
will
pro
vide
an
impr
ovem
ent i
n th
e st
anda
rd.
•Th
e Tr
ust i
s con
tinui
ng to
wor
k w
ith C
CG o
n th
e ap
prop
riate
ness
of t
wo
wee
k w
ait r
efer
rals.
Thi
s inc
lude
s up
datin
g of
refe
rral
form
s in
Derm
atol
ogy
neop
lasm
s (in
Mar
ch) a
nd G
ynae
colo
gy n
eopl
asm
s (in
June
). Fu
rthe
r w
ork
to u
pdat
e re
ferr
als f
orm
s for
Lung
and
Uro
logy
is u
nder
way
. An
aud
it w
ill c
omm
ence
in Ju
ly 2
015
to a
sses
s th
e im
pact
of t
his c
hang
e.
•Da
ta a
nd p
atie
nt e
xper
ienc
es re
gard
ing
inap
prop
riate
refe
rral
s are
bei
ng sh
ared
with
CCG
s and
GPs
.
142
239
205
158
176
185
108
132
158
00.2
0.4
0.6
0.8
11.2
050100
150
200
250
300
350
400
450
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
No. Breaches
Capa
city
Patie
nt C
hoic
e%
Due
to P
atie
nt C
hoic
e
12
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.53
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
96.1
0%95
.20%
98.9
0%97
.09%
97.9
8%98
.51%
99.4
3%99
.03%
97.7
0%98
.12%
98.8
4%99
.41%
80.5
7%78
.75%
83.4
1%86
.85%
87.5
0%87
.01%
85.4
1%88
.75%
87.5
8%86
.22%
81.9
8%86
.24%
100.
00%
100.
00%
92.3
1%10
0.00
%10
0.00
%94
.29%
100.
00%
100.
00%
88.8
9%50
.00%
71.4
3%66
.67%
405
87.6
%
Tota
lW
ithin
62
Days
% 6
2 Da
ys48
539
280
.8%
Plan
ned
Care
925
875
94.6
%91
991
599
.6%
Uni
vers
ity H
ospi
tals
of L
eice
iste
r NHS
FT
Glo
uces
ters
hire
Hos
pita
ls N
HS F
T91
887
2
% 3
1 Da
ysW
ithin
31
Days
Tota
l
397
82.2
%
955
98.9
%94
791
696
.7%
1,06
7
354
74.9
%
1,30
21,
280
98.3
%1,
296
1,28
098
.8%
1,03
597
.0%
985
951
96.5
%
95.0
%69
,131
67,5
9997
.8%
27,5
8183
.9%
438
328
74.9
%43
034
881
.0%
Uni
ted
Linc
olns
hire
Hos
pita
ls N
HS F
TO
xfor
d U
nive
rsity
Hos
pita
ls N
HS F
T
449
363
80.9
%44
334
8
458
399
87.0
%
78.6
%N
ottin
gham
Uni
vers
ity H
ospi
tals
NHS
FT
Glo
uces
ters
hire
Hos
pita
ls N
HS F
T
Canc
ers -
31
and
62 D
ays
Tabl
e: H
EFT
31 D
ay P
erfo
rman
ce v
Pee
r Tru
sts –
Qua
rter
3 2
014/
15
Tabl
e: H
EFT
62 D
ay P
erfo
rman
ce v
Pee
r Tru
sts –
Qua
rter
3 2
014/
15
31 D
ay P
athw
aySh
effie
ld T
each
ing
Hosp
itals
NHS
FT
All E
nglis
h Pr
ovid
ers
Tabl
e 1
: Tw
o w
eek
wai
ts/B
reas
t Sym
ptom
s: p
erce
ntag
e of
pat
ient
s see
n in
2 w
eeks
Indi
cato
r31
Day
Tar
get (
96%
targ
et)
62 D
ay T
arge
t (85
% ta
rget
)62
Day
Nat
iona
l Scr
eeni
ng P
rogr
amm
e
Uni
vers
ity H
ospi
tals
of L
eice
ter N
HS F
TEa
st K
ent H
ospi
tals
Uni
vers
ity N
HS F
TLe
eds T
each
ing
Hosp
itals
NHS
FT
Hear
t of E
ngla
nd N
HS F
T
32,9
11
462
966
The
New
cast
le u
pon
Tyne
Hos
pita
ls N
HS F
TN
ottin
gham
Uni
vers
ity H
ospi
tals
NHS
FT
Nor
folk
and
Nor
wic
h U
nive
rsity
Hos
pita
ls N
HS F
THe
art o
f Eng
land
NHS
FT
Oxf
ord
Uni
vers
ity H
ospi
tals
NHS
FT
62 D
ay P
athw
ay
The
New
cast
le u
pon
Tyne
Hos
pita
ls N
HS F
T
483
Guy
's an
d St
Tho
mas
' NHS
FT
All E
nglis
h Pr
ovid
ers
473
Head
lines
Pe
rfor
man
ce in
62
day
stan
dard
in M
arch
201
5 (T
arge
t 85%
): 86
.24%
Pe
rfor
man
ce in
62
day
scre
enin
g in
Mar
ch 2
015
(Tar
get 9
0%):
66.6
7%
Perf
orm
ance
Ana
lysi
s Q
uart
erly
per
form
ance
of a
ll 31
and
62
day
stan
dard
s was
ach
eive
d w
ith th
e ex
cept
ion
of th
e 62
day
nat
iona
l sc
reen
ing
prog
ram
me.
The
num
ber o
f pat
ient
s on
a 62
day
scre
enin
g pa
thw
ay w
ere
low
er in
Q4
com
pare
d to
pr
evio
us q
uart
ers
due
to th
e re
lativ
e re
duct
ion
in p
atie
nts u
nder
goin
g br
east
scre
enin
g lo
cally
. Th
e nu
mbe
r of p
atie
nts w
ho h
ave
wai
ted
mor
e th
an 1
00 d
ays f
or th
eir c
are
to b
e co
mpl
eted
redu
ced
to 4
in A
pril,
th
e lo
wes
t for
ove
r 12
mon
ths
Actio
ns T
aken
•
Wor
ksho
ps to
furt
her i
mpr
ove
patie
nt p
athw
ays i
n Lu
ng a
nd U
rolo
gy w
ill ta
ke p
lace
in M
ay
•Fo
cus i
s bei
ng a
pplie
d at
the
wee
kly
canc
er P
atie
nt-t
arge
ted
List
(PTL
) mee
ting
to e
nsur
e al
l pat
ient
s are
dat
ed a
nd
issue
s esc
alat
ed
•M
eetin
g w
ith C
CG w
ill ta
ke p
lace
in M
ay re
gard
ing
'pan
-Birm
ingh
am' m
anag
emen
t of p
atie
nts r
efer
red
late
into
th
eir p
athw
ay a
nd th
e im
pact
this
has o
n ou
tcom
es a
nd p
erfo
rman
ce
13
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.54
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
ALQ
R26
ALQ
R24c
ALQ
R24b
89.5
1%10
0.00
%10
0.00
%94
.19%
Har
m F
ree
Care
95%
94.8
9%94
.04%
93.7
3%
00
00
00
12
11
10
02
93
61
2
zero
tole
ranc
e
Pres
sure
Ulc
er R
educ
tion
for
avoi
dabl
e gr
ade
2 pr
essu
re u
lcer
s
Pres
sure
Ulc
er R
educ
tion
for
avoi
dabl
e gr
ade
3 pr
essu
re u
lcer
s
Pres
sure
Ulc
er R
educ
tion
for
avoi
dabl
e gr
ade
4 pr
essu
re u
lcer
sze
ro to
lera
nce
5.17
81
54
No.
of I
njur
ious
Fal
ls
Redu
ctio
n in
ove
rall
falls
rate
(per
100
,000
be
d da
ys)
N/A
7.71
6.70
8.62
N/A TB
C
Qua
lity
& R
isk
Heat
Map
- N
ursi
ng P
erfo
rman
ce
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RK
TARGET
In month trajectory
Last
Mon
th
Trus
t (M
ar-1
5)H
eart
land
s H
ospi
tal
Goo
d H
ope
Hos
pita
lSo
lihul
l H
ospi
tal
Clin
ical
Su
ppor
t Se
rvic
es
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Mar
-15
Perf
orm
ance
Im
prov
emen
t
6.5010
14
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.55
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Gra
ph: I
njur
ious
Fal
ls
Gra
ph: F
alls
rate
per
1,0
00 o
ccup
ied
bed
days
(OBD
)
Qua
lity
& R
isk
Falls
Tabl
e: N
ursi
ng M
etric
s - F
alls
Ass
essm
ent
Head
lines
Th
e Fa
lls a
sses
smen
t ele
men
t of t
he n
ursin
g m
etric
s ach
ieve
d a
scor
e of
95%
for A
pr-1
5, th
e hi
ghes
t sco
re si
nce
the
Falls
Bun
dle
was
firs
t int
rodu
ced
in Ju
l-14.
The
re is
a y
ear e
nd ta
rget
ove
rall
for 2
015-
16 o
f 95%
, with
eac
h el
emen
t of
the
falls
bun
dle
to a
chie
ve 9
0% b
y ye
ar e
nd.
Ther
e w
ere
no in
dica
tors
scor
ing
less
than
90%
for A
pr-1
5.
The
Trus
t fal
ls ra
te p
er 1
,000
occ
upie
d be
d da
ys h
as fa
llen
to 6
.50
in A
pr-1
5, it
s low
est r
ate
since
Jun-
13. T
here
is n
o of
ficia
l tar
get f
or 2
015/
16 b
ut th
e in
tern
al ta
rget
is n
ot to
per
form
abo
ve th
e up
per c
ontr
ol li
mit
(i.e.
less
than
8.8
0).
Perf
orm
ance
Ana
lysi
s Th
ere
wer
e te
n in
jurio
us fa
lls in
Apr
-15:
•
One
on
the
Hear
tland
s site
(War
d 29
) •
Five
at G
ood
Hope
(War
ds 1
1, 1
7, 1
8, 2
3 an
d Ce
darw
ood)
•
Four
on
the
Solih
ull s
ite (W
ards
19,
20A
, 20B
and
AM
U S
hort
Sta
y).
The
them
es fr
om R
CAs w
ill b
e pu
blish
ed o
n a
quar
terly
bas
is.
The
falls
rate
per
1,0
00 o
ccup
ied
beds
day
s wer
e sp
lit a
cros
s the
site
s as f
ollo
ws:
•
Hear
tland
s, 2
014/
15 =
7.4
1, A
pril
2015
= 6
.70
•Go
od H
ope,
201
4/15
= 9
.34,
Apr
il 20
15 =
8.6
2 •
Solih
ull,
2014
/15
= 7.
26, A
pril
2015
= 5
.17
Ac
tions
take
n •
Nur
sing
Care
indi
cato
rs h
ave
been
revi
sed,
ther
efor
e w
orki
ng to
new
met
rics i
n 20
15/1
6 •
The
new
met
ric q
uest
ions
are
now
live
•
Peer
revi
ews/
aud
its to
be
carr
ied
out b
y w
ard
man
ager
s or s
enio
r sist
ers.
Thi
s may
hav
e an
initi
al n
egat
ive
impa
ct
on p
erfo
rman
ce d
ue to
inte
rpre
tatio
n of
the
new
que
stio
ns.
Actio
ns fo
r Inj
urio
us F
alls
•RC
As to
be
com
plet
ed fo
r rec
urre
nt fa
llers
in M
ar 2
015.
•
Them
es to
be
iden
tifie
d an
d m
onito
red
over
the
next
12
mon
ths.
Thi
s inf
orm
atio
n w
ill b
e us
ed w
hen
deve
lopi
ng
targ
ets i
n 20
16/1
7.
7
0
5 7
8
2
6 5
5
8
4
8 10
024681012
Num
ber o
f Inj
urio
us F
alls
HEFT
Ave
rage
Upp
er C
ontr
ol L
imit
Low
er C
ontr
ol L
imit
6.70
6.73
6.50
6.91
8.15
7.15
7.13
7.01
8.05
7.26
6.96
7.71
6.50
5.00
6.00
7.00
8.00
9.00
10.0
0
HEFT
Fal
ls Ra
te p
er 1
,000
OBD
HEFT
Ave
rage
Upp
er C
ontr
ol L
imit
Low
er C
ontr
ol L
imit
15
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.56
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Qua
lity
& R
isk
Avoi
dabl
e Gr
ade
2Av
oida
ble
Grad
e 3
Apr-
1512
2
Pres
sure
Ulc
ers
Tabl
e: N
ursi
ng M
etric
s - T
issue
Via
bilit
y
Tabl
e: N
umbe
r of
avoi
dabl
e Ho
spita
l acq
uire
d Pr
essu
re U
lcer
s (in
Mon
th a
nd Y
TD)
Grap
h 2:
Saf
ety
Ther
mom
eter
Poi
nt p
reva
lenc
e of
all
pres
sure
ulc
ers
2014
/15
(YTD
)21
466
Head
lines
The
Tiss
ue V
iabi
lity
Asse
ssm
ent i
ndic
ator
of t
he n
ursin
g m
etric
s ach
ieve
d a
scor
e of
94%
for A
pr-1
5. A
95%
yea
r en
d ta
rget
has
bee
n ag
reed
for t
he th
ree
elem
ents
of t
he ti
ssue
via
bilit
y m
etric
s tha
t wer
e un
der-p
erfo
rmin
g du
ring
2014
-15
(dai
ly sk
in in
spec
tions
, rep
ositi
onin
g fr
eque
ncy
com
plet
ed, a
nd re
posit
ioni
ng fr
eque
ncy
adhe
red
to).
The
se th
ree
elem
ents
wer
e al
so th
e m
ost c
omm
only
occ
urrin
g th
emes
from
the
RCAs
resu
lting
in p
ress
ure
ulce
rs b
eing
clas
sed
as a
void
able
. Th
e Tr
ust p
ress
ure
ulce
r poi
nt p
reva
lenc
e ha
s rem
aine
d be
low
the
aver
age
line
for t
he p
ast 1
4 co
nsec
utiv
e m
onth
s de
spite
the
smal
l inc
reas
e in
mon
th (f
rom
3.5
1 to
3.7
7).
The
Trus
t also
con
tinue
s to
sit w
ell b
elow
the
Nat
iona
l av
erag
e fig
ure
of 4
.48%
. Th
e nu
mbe
r of a
void
able
pre
ssur
e ul
cers
con
firm
ed fo
r Apr
-15
wer
e tw
elve
gra
de 2
, on
e gr
ade
3, a
nd o
ne
necr
otic
. Ho
wev
er, t
here
are
still
48
pres
sure
ulc
ers f
or A
pr-1
5 st
ill a
wai
ting
an o
utco
me
follo
win
g RC
A. F
inal
fig
ures
for 2
014-
15 sh
ow th
e Tr
ust h
as re
cord
ed 2
14 g
rade
2 a
void
able
pre
ssur
e ul
cers
whi
ch is
a 2
1% re
duct
ion
on
2013
-14
(271
). Co
mm
issio
ners
hav
e se
t a fu
rthe
r 20%
redu
ctio
n fo
r 201
5-16
in a
void
able
gra
de 2
pre
ssur
e ul
cers
w
hich
wou
ld m
ean
no m
ore
than
171
inci
denc
es a
cros
s the
Tru
st.
Poin
t pre
vale
nce
is no
long
er a
CQ
UIN
or K
PI b
ut is
requ
ired
as a
n in
form
atio
n re
quire
men
t (w
ith n
o se
t tar
get)
. Fu
rthe
r Act
ions
•
Disc
ussio
ns w
ith C
CG re
gard
ing
avoi
dabl
e pr
essu
re u
lcer
s and
targ
ets c
ontin
ues.
A p
oten
tial T
rust
targ
et o
f 10%
re
duct
ion
is st
ill to
be
agre
ed.
•In
tern
al ta
rget
set a
t 20%
redu
ctio
n ac
ross
all
sites
(inc
CSS
) to
be p
rese
nted
in M
ay 2
015.
•
Site
bas
ed tr
ajec
torie
s set
inte
rnal
ly fo
r the
redu
ctio
n of
pre
ssur
e ul
cers
to co
me
into
effe
ct fr
om M
ay 2
015.
3.82
3.62
3.20
3.78
3.93
3.62
3.34
3.86
3.36
3.99
3.92
3.51
3.77
1.00
2.00
3.00
4.00
5.00
6.00
CQU
IN T
arge
tPr
essu
re U
lcer
Pre
vale
nce
Nat
iona
l Ave
rage
16
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.57
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Divi
sion
BHH
GHH SO
LO
&G
HEFT
Qua
lifie
d Co
mpl
ianc
eHC
A Co
mpl
ianc
e97
%10
5%10
9%12
1%99
%10
8%
96%
105%
101%
99%
4.00
%
3.08
%
4.87
%
4.40
%
5.70
%
8.59
%
7.62
%
5.17
%
6.18
%
Qua
lity
& R
isk
Nur
sing
Wor
kfor
ce
Gra
ph: %
Sic
knes
s in
Nur
sing
at H
EFT
Tabl
e by
site
sick
ness
in A
pril
2015
UN
IFY
Staf
fing
Retu
rn
Divi
sion
BHH
GHH SO
L
CSS
W&
C
Qua
lifie
d N
ursi
ngN
on-q
ualif
ied
Nur
sing
4.87
%
Wor
kfor
ce H
eadl
ines
:
Ove
rall
ther
e ha
s bee
n a
redu
ctio
n in
Nur
sing
sickn
ess.
Th
ere
is a
signi
fican
t diff
eren
ce b
etw
een
sickn
ess i
n qu
alifi
ed n
ursin
g an
d no
n-qu
alifi
ed n
ursin
g. Q
ualif
ied
nurs
ing
sickn
ess a
lone
is b
elow
the
4.65
% ta
rget
in A
pril
2015
. Ac
tions
•
Raisi
ng h
igh
leve
l of s
ickn
ess o
f non
-qua
lifie
d nu
rsin
g at
site
mee
tings
, esp
ecia
lly G
HH a
nd S
OL
•Th
e sp
lit b
etw
een
qual
ified
and
non
-qua
lifie
d nu
rsin
g sic
knes
s in
2014
/15
to b
e de
taile
d in
May
201
5 re
port
. N
atio
nal S
taffi
ng R
etur
n:
The
UN
IFY
natio
nal s
taffi
ng re
turn
show
ed th
at a
ll sit
es a
nd W
omen
s ser
vice
s acr
oss A
pril
2015
wer
e co
mpl
iant
w
ith st
affin
g to
thei
r fun
ded
esta
blish
men
ts (9
5% o
r ove
r). T
his i
nclu
ded
the
flex
area
s on
each
site
. How
ever
ther
e ar
e a
num
ber o
f war
ds a
t BHH
that
hav
e sig
nific
ant n
umbe
rs o
f qua
lifie
d va
canc
ies (
War
ds 2
,3,8
,9 a
nd 2
4). T
hese
ar
eas a
re h
eavi
ly re
liant
on
tem
pora
ry st
affin
g w
hich
is a
ffect
ing
the
skill
mix
and
con
tinui
ty o
f car
e.
Actio
ns
•Sp
ecifi
c w
ork
is be
ing
unde
rtak
en to
mea
sure
qua
lity
of c
are
war
ds w
ith a
sign
ifica
nt n
umbe
r of q
ualif
ied
vaca
ncie
s.
•Di
ffere
ntia
ting
betw
een
bank
and
trus
t sta
ff in
term
s of H
CAs,
to b
e av
aila
ble
in M
ay 2
015.
Thi
s is t
o de
term
ine
whe
ther
th
ere
is an
y im
pact
on
war
d sa
fety
.
4.10%
5.23%
5.55%
5.69%
5.55%
5.80%
6.11%
6.15%
5.95%
5.81%
5.25%
4.86%
4.98%
3.00
%
3.50
%
4.00
%
4.50
%
5.00
%
5.50
%
6.00
%
6.50
%
% S
ickn
ess i
n N
ursin
g &
Mid
wife
ryTr
ust S
ickn
ess T
arge
t
17
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.58
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Nur
sing
Vaca
ncie
s
Gra
ph: Q
ualif
ied
Nur
sing
Vac
ancy
Pos
ition
Apr
il 20
15
Gra
ph: Q
ualif
ied
Nur
sing
Vac
ancy
Pos
ition
Apr
il 20
15 (A
&E,
CSS
and
W&
C on
ly)
Qua
lity
& R
isk
Head
lines
Th
e ke
y iss
ue re
mai
ns th
e sh
orta
ge o
f reg
ister
ed n
urse
s ava
ilabl
e to
recr
uit a
nd a
lso th
e cu
rren
t tur
nove
r of s
taff.
Th
e in
trod
uctio
n of
new
serv
ices
and
the
prov
ision
al p
lan
to su
bsta
ntiv
ely
esta
blish
som
e of
the
flexi
ble
capa
city
be
ds is
like
ly to
hav
e ha
d a
nega
tive
impa
ct o
n th
e va
canc
y po
sitio
n.
Actio
ns ta
ken
•86
pos
ts h
ave
been
offe
red
over
the
last
thre
e m
onth
s to
nurs
es w
ho q
ualif
y in
Sep
tem
ber 2
015.
•
Loca
l rec
ruitm
ent e
vent
s hav
e be
en h
eld
to ta
rget
vac
anci
es in
spec
ialis
t are
as. T
his h
as b
een
very
succ
essf
ul in
th
e Ac
ute
Med
ical
Uni
ts o
n al
l thr
ee si
tes.
•
Busin
ess c
ase
bein
g pr
epar
ed fo
r the
recr
uitm
ent o
f nur
ses i
nter
natio
nally
as a
resu
lt of
the
Recr
uitm
ent a
nd
Rete
ntio
n pa
per p
rese
nted
to E
MB.
•
The
Trus
t has
inve
sted
in N
ursin
g Ti
mes
Gro
up A
cces
s for
eve
ry re
gist
ered
nur
se a
cros
s the
Tru
st. T
his i
s aim
ed
at sl
owin
g do
wn
attr
ition
and
enc
oura
ging
new
recr
uitm
ent i
nter
est p
artic
ular
ly fr
om n
urse
s with
pos
t re
gist
ratio
n ex
perie
nce.
Fu
rthe
r Act
ion
•HR
and
Nur
sing
are
wor
king
toge
ther
to p
rodu
ce p
erso
nal d
evel
opm
ent a
nd p
asto
ral c
are
ince
ntiv
es to
mak
e th
e Tr
ust a
n em
ploy
er o
f cho
ice
•Pr
ogra
mm
e of
loca
l and
nat
iona
l rec
ruitm
ent e
vent
s pla
nned
thro
ugho
ut 2
015.
Data
not
ava
ilabl
e at
this
tim
e, d
ue to
be
avai
labl
e fo
r May
201
5 Re
port
Data
not
ava
ilabl
e at
this
tim
e, d
ue to
be
avai
labl
e fo
r May
201
5 Re
port
18
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.59
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
ANQ
R2<
646
ANQ
R3
ANQ
R1
QS6
QS7
ANQ
R11
95.0
0%
N/A
Mor
talit
y -
HSM
R
Mor
talit
y -
SHM
I
93.5
3%95
.82%
97.4
3%
N/A
N/A
N/A
N/A
N/A
10
00
8
N/A
2
N/A 0
N/A
1M
inim
ise
rate
s of
Clo
stri
dium
dif
fici
le
VTE
ris
k as
sess
men
t: a
ll in
pati
ent
Serv
ice
Use
rs u
nder
goin
g ri
sk
asse
ssm
ent
for
VTE
, as
defi
ned
in
Con
trac
t Te
chni
cal G
uida
nce
93.1
7%N
/A
0 0
> 9
0%
> 9
0%
00
0
92.7
1%81
.60%
82.9
8%78
.94%
86.5
5%77
.43%
> 9
5%
0
N/A
N/A
N/A
N/A
95.0
6%
The
num
ber
of a
void
able
Clo
stri
dium
D
iffi
cile
Qua
lity
& R
isk
Heat
Map
- In
fect
ion
Cont
rol,
VTE,
Mor
talit
y
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RK
TARGET
In month trajectory
Last
Mon
th
Trus
t (M
ar-1
5)H
eart
land
s H
ospi
tal
Goo
d H
ope
Hos
pita
lSo
lihul
l H
ospi
tal
Clin
ical
Su
ppor
t Se
rvic
es
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Apr
-15
Perf
orm
ance
Im
prov
emen
t
2 00
Zero
tol
eran
ce M
RSA
MR
SA E
lect
ive
Scre
enin
g R
ates
(%
pa
tien
ts s
cree
ned)
MR
SA E
mer
genc
y Sc
reen
ing
Rat
es
(% p
atie
nts
scre
ened
)
19
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.60
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Emer
genc
y Sc
reen
ing
Apr
-15
81.6
%YT
D81
.6%
Qua
lity
& R
isk
Infe
ctio
n Co
ntro
l
Trus
t wid
e
Elec
tive
Scre
enin
gA
pr-1
5YT
D
Tabl
e: T
rust
Wid
e Av
oida
ble/
Una
void
able
Tox
in P
ositi
ve P
ost 4
8 hr
C.D
iff c
ases
Gra
ph: T
rust
Wid
e Av
oida
ble/
Una
void
able
Tox
in P
ositi
ve P
ost 4
8 hr
C.D
iff c
ases
Post
-48h
r Cas
esA
pr-1
50
YTD
0D
ays
Bet
wee
n M
RSA
Bac
tere
amia
Cas
es10
5
Pre-
48hr
Cas
esA
pr-1
50
YTD
0
Head
lines
Th
ere
wer
e no
cas
es o
f pos
t 48
hour
MRS
A ba
cter
aem
ia re
port
ed in
Apr
il. T
here
is st
ill a
zero
tole
ranc
e ta
rget
for
MRS
A po
st 4
8 ho
ur b
acte
raem
ias.
Th
ere
have
bee
n tw
o ca
ses o
f pos
t 48
hour
toxi
n po
sitiv
e Cl
ostr
idiu
m D
iffic
ile (C
.diff
) in
April
aga
inst
the
mon
th
targ
et o
f 6 o
r les
s. T
he 2
015/
16 y
ear t
arge
t is ≤
64
case
s (16
per
qua
rter
).
Ther
e w
as o
ne n
ew c
ase
of C
PE id
entif
ied
in A
pril.
Thi
s was
from
a c
linic
al sp
ecim
en (s
putu
m) f
rom
a c
hild
who
has
re
ceiv
ed h
ealth
care
in In
dia.
Th
ere
wer
e tw
o ca
ses o
f sus
pect
ed e
bola
in A
pril.
Bot
h pa
tient
s wer
e re
turn
ing
heal
thca
re w
orke
rs w
ho w
ere
low
ris
k an
d lo
w p
roba
bilit
y of
ebo
la. I
n ea
ch c
ase
the
patie
nt w
as n
egat
ive
for e
bola
and
was
disc
harg
ed w
ithin
24
hour
s.
Perf
orm
ance
Ana
lysi
s •
Four
war
ds w
ere
clos
ed d
urin
g Ap
ril d
ue to
out
brea
ks o
f dia
rrho
ea a
nd v
omiti
ng co
nfirm
ed a
s Nor
oviru
s. T
hese
w
ere
BHH
war
d 6,
GHH
war
d 14
, GHH
war
d 16
and
GHH
war
d 9.
•Th
ere
was
an
outb
reak
dec
lare
d of
CPE
on
BHH
war
d 12
in A
pril
(all
the
patie
nts w
ere
in h
ospi
tal d
urin
g M
arch
). Th
e in
dex
patie
nt h
ad th
e or
gans
im id
entif
ied
from
a c
linic
al sp
ecim
en o
f urin
e an
d tw
o pa
tient
cont
acts
wer
e fo
und
to b
e po
sitiv
e on
scre
enin
g. T
ypin
g of
the
spec
imen
s ide
ntifi
ed th
at th
ey w
ere
indi
stin
guish
able
. All
thre
e pa
tient
s had
bee
n di
scha
rged
and
scre
enin
g of
the
rem
aini
ng p
atie
nts o
n th
e w
ard
was
neg
ativ
e.
Actio
ns ta
ken
•De
ep cl
eani
ng w
as c
arrie
d ou
t on
all n
orov
irus o
utbr
eak
war
ds p
rior t
o re
-ope
ning
.
•An
RCA
was
car
ried
out f
or th
e CP
E ou
tbre
ak o
n BH
H w
ard
12 a
nd a
ctio
ns in
clud
ed d
eep
clea
ning
of t
he e
ntire
w
ard
, aud
it of
pra
ctic
e, h
and
hygi
ene
educ
atio
n an
d re
-ass
essm
ent o
f clin
ical
staf
f for
AN
TT (a
sept
ic n
on-t
ouch
te
chni
que)
.
•Th
e eb
ola
actio
n gr
oup
mee
ts m
onth
ly a
nd a
deb
rief i
s car
ried
out f
or a
ll su
spec
ted
case
s.
•
CPE
scre
enin
g ha
s bee
n im
plem
ente
d in
adu
lt in
patie
nt a
nd a
dmiss
ion
area
s w
ith th
e sc
reen
ing
ques
tion
bein
g as
ked
of a
ll pa
tient
s and
incl
uded
in e
lect
roni
c and
pap
er d
ocum
enta
tion.
2 6
11
16
22
27
32
38
43
48
54
59
64
4
13
21
28
32
39
45
46
56
64
67
75
01020304050607080
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Trus
t wid
e Av
oida
ble/
Una
void
able
Toxi
n Po
sitiv
e Po
st 4
8hr
C.Di
ff Ca
ses
Avoi
dabl
eUn
avoi
dabl
eAw
aitin
g Ty
ping
2015
/16
Targ
et20
14/1
5
20
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.61
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
W5
W6
8.5%
by
Mar
-16
9.00
%
W7
4.25
%
by M
ar-
164.
65%
W12
W13
85.8
6%83
.62%
86.1
0%85
.50%
86.0
7%84
.77%
86.4
2%
3.93
%5.
85%
3.71
%4.
07%
4.18
%4.
32%
73.8
2%62
.72%
60.0
9%74
.71%
80.9
2%66
.05%
73.2
9%
Vaca
ncie
s
Staf
f FFT
N/A
14.4
11.4
15.5
14.7
Volu
ntar
y Tu
rnov
er
Sick
ness
- in
mon
th p
ositi
on (Y
TD fi
gure
=
MAA
) mia
Aver
age
Tim
e to
Rec
ruit
from
vac
ancy
ap
prov
al to
star
t dat
e - A
ll St
aff G
roup
s<
11 w
eeks
85%
rolli
ng y
ear
No
targ
et se
t
Num
ber o
f App
raisa
ls Co
mpl
eted
Trus
twid
e Ag
ency
Spe
nd
Man
dato
ry T
rain
ing
85%
rolli
ng y
ear
9.01
%10
.34%
11.9
5%8.
58%
4.33
%
14.6
14N
/A
8.90
%Wor
kfor
ce &
Wel
l-bei
ng
Heat
Map
CC
G /
H
EFT
Ref.
MO
NIT
OR
CO
MP
LIA
NC
E -
RISK
ASS
ESSM
ENT
FRAM
EWO
RK
TARGET
In month trajectory
Last
Mon
th
Trus
t (M
ar-1
5)H
eart
land
s H
ospi
tal
Goo
d H
ope
Hos
pita
lSo
lihul
l H
ospi
tal
Clin
ical
Su
ppor
t Se
rvic
es
Wom
ens
&
Chi
ldre
n
Trus
t P
erfo
rman
ce
Apr
-15
Perf
orm
ance
Im
prov
emen
t
8.30
%9.
01%
21
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.62
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Wor
kfor
ce &
Wel
l-bei
ng
Appr
aisa
ls
Appr
aisa
ls tr
ajec
tory
% A
ppra
isal
s com
plet
ed b
y Di
visi
on
CSS
Divi
sion
BHH
GHH SO
L
WC
CORP
FAC
HEFT
Mar
-15
Apr-
15
0.00
%0.
00%
0.00
%0.
00%
2014
/15
61.1
7%61
.08%
73.0
9%82
.53%
0.00
%0.
00%
0.00
%0.
00%
62.7
2%60
.09%
74.7
1%80
.92%
67.3
6%
73.8
2%
90.1
7%92
.57%
73.2
9%
66.0
5%86
.67%
89.0
2%
73.29% 58.76%
0%10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
% A
ppra
isals
Com
plet
ed 2
015/
16%
App
raisa
ls Co
mpl
eted
201
4/15
Targ
et 2
015/
16
Head
lines
Th
ere
has b
een
a ch
ange
in th
e w
ay a
ppra
isal c
ompl
eted
dat
a is
publ
ished
in 2
015/
16. T
he 2
015/
16 ta
rget
is 8
5%
over
a ro
lling
12
mon
ths (
rath
er th
an th
e tr
ajec
tory
use
d in
201
4/15
). Th
e ro
lling
12
mon
ths i
n Ap
ril 2
015
is 73
.29%
. All
data
in th
is re
port
is b
ased
on
this
new
met
hod
of d
ata
colle
ctio
n.
HR A
naly
sis
Ther
e ha
s bee
n gr
adua
l im
prov
emen
t thr
ough
201
4/15
from
58.
76 %
at t
he st
art o
f 201
4/15
to 7
3.29
% b
y Ap
ril
2015
. Th
e Di
rect
orat
es w
ith st
aff n
umbe
rs m
ore
than
50
whi
ch a
re m
ost c
ontr
ibut
ing
to th
e pe
rfor
man
ce b
eing
bel
ow
targ
et
are:
Th
ere
wer
e no
maj
or is
sues
in C
orpo
rate
and
Fac
ilitie
s.
Actio
ns
•Th
ere
is fu
rthe
r tra
inin
g fo
r app
raise
rs b
eing
pro
vide
d ce
ntra
lly b
y HR
.
•Im
prov
ing
and
simpl
ifyin
g th
e ap
prai
sal p
roce
ss in
clud
ing
inve
stig
atin
g an
onl
ine
appr
aisa
l sys
tem
.
22
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.63
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Wor
kfor
ce &
Wel
l-bei
ng
Man
dato
ry T
rain
ing
(MIA
)
Man
dato
ry T
rain
ing
(MIA
)
Divi
sion
per
form
ance
(MIA
)
83.8
3%
Divi
sion
FAC
HEFT
Feb-
15
CORP
WC
BHH
GHH SO
LCS
S0.
00%
86.1
0%85
.50%
86.0
7%0.
00%
0.00
%0.
00%
0.00
%
Mar
-15
83.6
2%
84.7
7%76
.40%
83.0
3%85
.03%
85.5
9%84
.84%
2015
/16
0.00
%0.
00%
0.00
%
76.8
7%76
.87%
85.8
6%79
.02%
86.4
2%
0
60%
65%
70%
75%
80%
85%
90%
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Man
dato
ry T
rain
ing
% C
ompl
ianc
e 20
15/1
6M
anda
tory
Tra
inin
g %
Com
plia
nce
2014
/15
Targ
et 2
015/
16
Head
lines
Th
e to
tal f
igur
e fo
r the
yea
r to
Mar
ch 2
015
is 86
.42%
aga
inst
a ta
rget
of 8
5%.
HR A
naly
sis
Desp
ite a
chie
ving
the
over
all t
rain
ing
targ
et, t
here
are
still
are
as w
here
com
plia
nce
can
be im
prov
ed:
•Re
susc
itatio
n 61
.33%
•
Fire
Saf
ety
59.7
7%
•Bl
ood
Tran
sfus
ion
(adm
inist
erin
g) 5
9.7%
Th
e re
leas
e of
staf
f is s
till a
fact
or in
non
-del
iver
y in
the
abov
e ar
eas.
Thi
s is c
ompo
unde
d by
a n
umbe
r of
vaca
ncie
s in
the
resu
scita
tion
team
whi
ch im
pact
s on
thei
r abi
lity
to d
eliv
er th
e m
anda
tory
trai
ning
. Al
l div
ision
s hav
e se
en a
n in
crea
se fr
om la
st m
onth
with
the
exce
ptio
n of
Cor
pora
te D
ivisi
on (0
.47%
dec
reas
e).
The
Dire
ctor
ates
with
mor
e th
an 5
0 st
aff a
nd re
lativ
ely
low
com
plia
nce
incl
ude:
He
artla
nds
El
derly
Med
72
.26%
CS
S
Lab
Med
76
.16%
Ac
tions
Tak
en
•N
on re
leas
e of
staf
f has
bee
n es
cala
ted
to A
MDs
. •
Resu
scita
tion
staf
fing
leve
l rev
iew
is c
urre
ntly
in th
e pr
oces
s of b
eing
com
plet
ed. E
stim
ated
4 w
eeks
•
Addi
tiona
l adm
in su
ppor
t con
firm
ed fo
r LM
S.
•Th
e th
ree
area
s of c
once
rn w
erer
aise
d at
the
Risk
Com
mitt
ee in
Apr
il 20
15.
•DN
A an
d Ca
ncel
latio
n re
port
s hav
e be
en e
scal
ated
to d
ivisi
onal
leve
l. Fu
rthe
r Act
ions
•
New
Lea
rner
Man
agem
ent S
yste
m (L
MS)
bei
ng la
unch
ed 1
st Ju
ne, g
radu
ated
roll
out w
ill ta
ke 9
wee
ks.
Not
ava
ilabl
e at
this
time
23
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.64
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Divi
sion
per
form
ance
HEFT
Wor
kfor
ce &
Wel
l-bei
ng
Sick
ness
Trus
t Sic
knes
s
Divi
sion
BHH
GHH SO
LCS
SW
CCO
RPFA
C
Mar
-15
Apr-
15M
ovin
g An
nual
Ave
rage
4.57
%3.
93%
4.56
%5.
19%
4.00
%4.
93%
5.21
%3.
63%
6.50
%4.
71%
4.96
%4.
06%
4.97
%5.
27%
3.58
%6.
38%
4.71
%
5.85
%3.
71%
4.07
%4.
18%
3.34
%8.
02%
4.32
%
Head
lines
Si
ckne
ss fo
r Apr
il w
as 4
.32%
acr
oss t
he T
rust
, a v
ery
sligh
t red
uctio
n ag
ains
t the
Mar
ch fi
gure
of 4
.33%
. The
mov
ing
annu
al a
vera
ge fi
gure
has
stay
ed u
ncha
nged
com
pare
d w
ith la
st m
onth
so w
e ar
e ab
ove
targ
et w
hich
is f
orec
ast a
s a
mon
th b
y m
onth
redu
ctio
n ov
er th
e ye
ar.
HR
Ana
lysi
s Ar
eas w
ith si
gnifi
cant
staf
f num
bers
and
the
high
est s
ickn
ess l
evel
s for
the
mon
th o
f Apr
il 15
wer
e:
The
area
s with
the
high
est s
ickn
ess l
evel
s ove
r a ro
lling
-12
mon
th p
erio
d w
ere:
Ac
tions
•
HR c
ontin
ues t
o as
sist m
anag
ers w
ith th
e m
anag
emen
t of s
taff
sickn
ess.
Furt
her A
ctio
ns
•Th
ere
is re
view
of s
ickn
ess p
olic
y un
der c
onsu
ltatio
n w
ith st
aff s
ide
whi
ch sh
ould
hel
p to
impr
ove
proc
esse
s for
m
anag
ing
sickn
ess.
Thi
s is d
ue to
take
pla
ce a
t the
end
of M
ay.
•Co
ntin
ued
deve
lopm
ent o
f sta
ff en
gage
men
t pla
n as
par
t of o
vera
ll tr
ust p
lan.
A w
orki
ng g
roup
will
mee
t in
May
to
con
sider
ince
ntiv
es fo
r sta
ff ac
hiev
ing
low
sick
ness
.
4.32%
3.50
%
3.70
%
3.90
%
4.10
%
4.30
%
4.50
%
4.70
%
4.90
%
5.10
%
5.30
%
5.50
%
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Sick
ness
201
5/16
Sick
ness
201
4/15
Targ
et 2
015/
16
24
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.65
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Wor
kfor
ce &
Wel
l-bei
ng
Volu
ntar
y Tu
rnov
er &
Rec
ruitm
ent
Divi
sion
HEFT
GHH SO
LCS
S
Volu
ntar
y tu
rnov
er
Aver
age
time
to re
crui
t in
wee
ks
Aver
age
time
to re
crui
t
BHH
CORP
FAC
WC
Mar
-15
9.3
8.4
8.4
9.2
10.7
11.1
8.7
8.3
Apr-
1514
.411
.415
.514
.714
.611
.213
.514
.0
2015
/16
14.4
11.4
15.5
14.7
14.6
11.2
13.5
14.0
9.01%
0%1%2%3%4%5%6%7%8%9%10%
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
Volu
ntar
y Tu
rnov
er 2
015/
16Vo
lunt
ary
Turn
over
201
4/15
Targ
et 2
015/
16
14
0123456789101112131415
Apr
May
Jun
Jul
Aug
Sep
Oct
Nov
Dec
Jan
Feb
Mar
weeks
Aver
age
Tim
e to
Rec
ruit
2015
/16
Aver
age
Tim
e to
Rec
ruit
2014
/15
Targ
et 2
015/
16
N.B
. Tim
e to
recr
uit 2
014/
15 d
ata
only
incl
udes
Ope
ratio
nal m
anga
gem
ent
activ
ity d
urin
g re
crui
ting.
201
5/16
targ
et a
nd d
ata
incl
udes
bot
h op
erat
ion
man
agm
ent a
nd H
R ce
ntra
l rec
ruitm
ent a
ctiv
ity.
Head
lines
Vo
lunt
ary
Turn
over
Tu
rnov
er w
as v
ery
sligh
tly a
bove
the
9% ta
rget
in A
pril
2015
(9.0
1%).
This
has s
tabi
lised
ove
r the
last
few
mon
ths.
Turn
over
Ana
lysi
s De
spite
bei
ng a
bove
targ
et d
urin
g Ap
ril 2
015,
turn
over
is e
xpec
ted
to re
duce
to 8
.5%
by
the
year
end
. Di
rect
orat
es w
ith m
ore
than
50
staf
f and
the
high
est l
evel
s of T
urno
ver a
re:
Re
crui
tmen
t - ti
me
to h
ire
The
targ
et is
11
wee
ks c
onsis
ting
of 6
.25
wee
ks fo
r the
Ope
ratio
nal M
anag
emen
t par
t of t
he p
roce
ss a
nd 4
.75
wee
ks
for t
he ce
ntra
l rec
ruitm
ent s
ectio
n. T
he a
ctua
l pos
ition
for A
pril
2015
was
8.5
wee
ks a
nd 5
.5 w
eeks
resp
ectiv
ely,
gi
ving
a to
tal o
f 14
wee
ks.
Recr
uitm
ent A
naly
sis
The
mai
n re
ason
for d
elay
s is t
he ti
me
take
n to
shor
tlist
cand
idat
es a
nd re
turn
a su
cces
sful
can
dida
te fo
rm.
The
mai
n ar
eas w
ith lo
ng ti
mes
cale
s are
: Ac
tions
Tak
en
•A
repo
rt is
now
sent
mon
thly
to e
ach
of th
e ar
eas p
erfo
rmin
g po
orly
. Fu
rthe
r Act
ion
•An
alys
is in
to a
pot
entia
l lin
k be
twee
n th
e nu
mbe
r of v
acan
cies
and
long
are
as w
ith lo
nger
recr
uitm
ent t
imes
is
bein
g un
dert
aken
.
25
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.66
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Apr-
15M
ay-1
5Ju
n-15
Jul-1
5Au
g-15
Sep-
15O
ct-1
5N
ov-1
5De
c-15
Jan-
16Fe
b-16
Mar
-16
2014
/15
24.9
1%29
.09%
16.3
5%18
.19%
% R
espo
nses
Inpa
tient
sA&
E
YTD
24.9
1%16
.35%
Inpa
tient
s FFT
201
4/15
Per
form
ance
, Pos
itive
vs N
egat
ive
resp
onde
rs
A&E
FFT
2014
/15
Perf
orm
ance
, Pos
itive
vs N
egat
ive
resp
onde
rs
Tabl
e: T
rust
Inpa
tient
War
d Su
mm
ary
Mar
-15
Patie
nt E
xper
ienc
e
Met
rics
Frie
nds a
nd F
amily
Tes
t per
cent
age
of re
spon
ses
Head
lines
Fr
iend
s and
Fam
ily T
est (
FFT)
Th
is is
no lo
nger
a C
QU
IN re
quire
men
t but
it is
an
impo
rtan
t and
use
ful m
etric
. Cur
rent
ly, t
he ta
rget
s are
se
t at t
he Q
uart
er 4
201
4/15
pos
ition
. •
The
abso
lute
num
ber o
f res
pons
es to
the
FFT
cont
inue
s to
grow
. •
The
num
ber o
f pos
itive
resp
onse
s for
inpa
tient
s is b
elow
the
regi
onal
scor
e of
95%
how
ever
this
does
va
ry m
onth
on
mon
th.
In th
e A&
E da
ta th
e po
sitiv
e re
spon
se ra
te is
low
er th
an th
at o
f inp
atie
nts,
this
indi
cate
s a lo
wer
leve
l of
satis
fact
ion
with
our
A&
E se
rvic
e. T
here
is a
lso a
larg
er d
iffer
ence
bet
wee
n th
e A&
E sc
ore
for H
eart
of
Engl
and
and
the
regi
onal
scor
e (8
7% in
Mar
ch, f
or B
irmin
gham
and
Bla
ck C
ount
ry re
gion
). Th
ere
is no
regi
onal
ben
chm
arki
ng fo
r neg
ativ
e re
spon
ders
ther
efor
e w
e ar
e un
able
to d
raw
any
co
mpa
rison
s. C
ompa
rison
dat
a fo
r pos
itive
resp
onse
s was
not
ava
ilabl
e at
the
time
of w
ritin
g.
Dist
urbe
d by
Noi
se a
t Nig
ht
The
noise
at n
ight
que
stio
ns co
ntin
ues t
o be
the
poor
est p
erfo
rmin
g m
etric
. On
furt
her a
naly
sis it
is
diffi
cult
to ta
rget
war
d ar
eas w
here
ther
e m
ight
be
a pa
rtic
ular
issu
e du
e to
a w
ide
rang
e of
var
ianc
e in
the
num
ber o
f rep
onse
s per
war
d.
Furt
her A
ctio
ns
•Ag
reem
ent t
o be
reac
hed
on th
e th
resh
olds
for F
FT fo
r 201
5/16
•
Furt
her w
ork
to im
prov
e th
e va
lidity
and
com
para
bilit
y of
the
noise
at n
ight
dat
a is
ongo
ing
•Da
ta fr
om in
patie
nt q
uest
ionn
aire
s is b
eing
mad
e m
ore
read
ily a
vaila
ble
to n
ursin
g st
aff.
5060708090
Q1
14/1
5Q
2 14
/15
Q3
14/1
5Q
4 14
/15
Invo
lved
in T
reat
men
t Dec
ision
sCa
ll bu
zzer
resp
onse
Info
rmed
abo
ut g
oing
hom
eDi
stur
bed
by n
oise
at n
ight
Ove
rall
721
769
863
1769
18
48
1490
15
31
1784
1419
1864
1468
2145
89%
87
%
92%
91
%
94%
92
%
90%
88
%
93%
90
%
89%
93
%
6%
7%
5%
2%
1%
3%
3%
4%
2%
3%
3%
2%
0500
1000
1500
2000
2500
3000
0%20%
40%
60%
80%
100%
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
Tota
l Res
pons
esPe
rcen
tage
Pos
itive
resp
onse
sPe
rcen
tage
Neg
ativ
e re
spon
ses
2335
24
44
2291
23
04
2242
22
21
2293
20
10
2040
20
92
2376
24
87
75%
73
%
73%
74
%
75%
70
%
73%
76
%
73%
77
%
76%
75
%
14%
16
%
17%
16
%
16%
19
%
18%
17
%
19%
15
%
15%
11
%
0500
1000
1500
2000
2500
3000
0.00
%
15.0
0%
30.0
0%
45.0
0%
60.0
0%
75.0
0%
90.0
0%
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
Tota
l Res
pons
esPe
rcen
tage
Pos
itive
resp
onse
sPe
rcen
tage
Neg
ativ
e re
spon
ses
26
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.67
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Inte
grat
ed P
erfo
rman
ce R
epor
t - A
pril
Patie
nt E
xper
ienc
e
Com
plai
nts
New
Com
plai
nts
Re-o
pene
d Co
mpl
aint
s and
Com
plai
nts r
efer
red
to O
mbu
dsm
an
Gra
ph 2
: The
mes
of N
ew C
ompl
aint
s
230
218
179
119
151
123
92
120
88
46
72
92
47
67
44
050100
150
200
250
Qua
rter
120
14-1
5Q
uart
er 2
2014
-15
Qua
rter
320
14-1
5Q
uart
er 4
2014
-15
Dela
ys /
Canc
ella
tions
Attit
ude
/ Beh
avio
urAp
prop
riate
Tre
atm
ent
Poor
/ La
ck o
f Inf
orm
atio
nM
edic
atio
n
Head
lines
Th
e nu
mbe
r of n
ew c
ompl
aint
s in
April
(93)
incr
ease
d sli
ghtly
com
pare
d to
Mar
ch (8
9).
Valid
atio
n of
201
4/15
has
bee
n un
derw
ay.
The
num
ber o
f com
plai
nts c
lose
d in
yea
r has
impr
oved
from
the
prev
ious
yea
r as h
as th
e nu
mbe
r of
com
plai
nts w
hich
hav
e be
en re
open
ded:
N
B: T
hese
yea
r end
figu
res n
eed
to b
e va
lidat
ed.
Them
es A
naly
sis
The
mai
n th
emes
for c
ompl
aint
s sho
w a
sim
ilar p
ictu
re a
cros
s the
qua
rter
s of 2
014/
15. C
ompl
aint
s are
of
ten
com
plex
and
cove
r mor
e th
an o
ne is
sue.
The
big
gest
num
ber o
f com
plai
nts b
y fa
r in
each
qua
rter
re
late
to d
elay
s and
can
cella
tions
. Ac
tions
Tak
en
•In
form
atio
n on
del
ays a
nd c
ance
llatio
ns is
cur
rent
ly b
eing
repo
rted
as p
art o
f the
sche
dule
d ca
re
prog
ram
me.
Fu
rthe
r Act
ions
•
To c
ount
er th
e nu
mbe
r of a
ttitu
des a
nd b
ehav
iour
s com
plai
nts t
he T
rust
is c
urre
ntly
dev
elop
ing
a se
t of
staf
f val
ues a
nd b
ehav
iour
s with
a se
ctio
n on
bei
ng p
atie
nt ce
ntre
d.
20
10
10
21
22
13
8 9
9 4
9 14
2
5 4
4 5
2 5
1
4
2
1 1 2
2
1
2 2
3
051015202530
Apr-
14M
ay-1
4Ju
n-14
Jul-1
4Au
g-14
Sep-
14O
ct-1
4N
ov-1
4De
c-14
Jan-
15Fe
b-15
Mar
-15
Re-O
pene
d Co
mpl
aint
sRe
ferr
ed to
Om
buds
man
Uphe
ld b
y O
mbu
dsm
anPa
rtia
lly U
phel
d by
Om
buds
man
0.00
32
0.00
32
0.00
3
0.00
22
0.00
34
0.00
32
0.00
24
0.00
17
0.00
25
0.00
24 0.
0027
3755
5 0.
0028
99
100
95
71
99
98
73
53
77
68
76
89
93
050100
150
200
250
300
350
400
450
500
0
0.00
05
0.00
1
0.00
15
0.00
2
0.00
25
0.00
3
0.00
35
0.00
4
4173
041
760
4179
141
821
4185
241
883
4191
341
944
4197
442
005
4203
642
064
4209
5
% N
ew C
ompl
aint
s as a
pro
port
ion
of T
otal
Act
ivity
New
Com
plai
nts
27
Integrated Quality and PerformanceReport, including Finance

Council of GovernorsJune 2015
.68
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee meeting on 24 April 2015.Author Darren Cattell
1
EXECUTIVE SUMMARY
We remain under Section 111 Monitor Enforcement.
Financially we ended the year as expected, key areas are illustrated below highlighting pressures, nurse bank rate and underlying pay control, as we enter the new financial year:
Performance remains our key area of concern with little improvement in the last month of the year. Improvement trajectories for A&E and RTT are currently being finalised prior to final submission to Monitor for the new year.
Finance
• Underlying pay bill showed a material movement, £0.4m, in month which Divisions need to address as a matter of urgency entering the new financial year.
• Divisions need to now implement exit strategies, outside of agreed new investment measures to deliver care, to mitigate financial risk in quarter 1.
• Divisons are required to close GAP on efficiency plans and implement early delivery 2015/16 to achieve 2015/16 plan.
• Divisions need to improve delivery and have consistent delivery against our finalised 2015/16 CQUIN’s.
• Cash balance at year end was £87.7m.
The Report is being provided for: Trust Board and Council of GovernorsWhich other Committees has this paper been to? Finance and Performance Committee, 24th April 2015
FINANCE EXECUTIVE SUMMARY & KEY PERFORMANCE INDICATORS
Month 12 to 31st March 2015
Trust reforecast following additional measures
investment(£5.6m)
Year end income £0.6m
Nurse bank rate
impact (£0.8m)
BCCrates
impact (£1.0m)
Year end stock,
holiday accrual &
provisions £1.6m
Underlying March pay movement
(0.4m)
2014/15 Year end
(5.6m)
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.69
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee meeting on 24 April 2015.Author Darren Cattell
2
• Capital expenditure for the year was £20.5m., including accruals which is £21.2m behind approved budget and £6.8m behind Monitor forecast.
Standing Financial Instructions Update
A paper was presented to FPC that proposed the following changes to the SFIs to help provide clarity on responsibilities;
1. Amend the delegated authority levels to revised authority levels that reflected the Trust structure and set the operational managers as the dominant authoriser. For purchase orders and contracts the CEO can approve up to £250k.
2. Above the CEO level of £250k, purchase orders and contracts would be approved by Finance and Performance Committee. This had previously been noted in the SFIs as Trust Board, but this duty had been delegated to Finance and Performance Committee for a number of years. This change requires Trust Board approval as Finance and Performance Committee would now be performing a duty that was previously the responsibility of Trust Board.
3. For business cases where there is a request to spend new money, the case could be approved by EMB up to £500k, and above this would require Trust Board approval.
4. There were other several other procedural changes proposed including;
o Self-approval of orders prohibited except for noted exceptions.
o Exceptions to the authority levels for less usual transactions.
Recommendations
Agreed recommendations:
1. Division’s financial performance to be reported at Delivery Unit meetings.2. Additional action to manage medical pay.3. Executive led improvement in areas of poor performance.4. Implement additional measures to improve performance.5. Exit strategies to be in place for winter/additional measures above new investment
decisions.6. Close GAP on 2015/16 SIEP and begin early implementation.7. Further review the decision regarding enhanced bank rates.8. Conclude demand and capacity investment decisions when linked to 4, 5 and 7 above.9. Accept revised SFI’s.
Darren CattellInterim Director of Finance & Performance March 2015Heart of England NHS Foundation Trust
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.70
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
MARCH POSITION
The Trust had an I&E surplus in March.
Appendix 1
The final outturn clinical income value for 2014/15 is £577.4m, £11.1m above plan for theyear. Clinical income was £0.6m higher than expected at the end of the year compared to the forecast due to a combination of JMRA upside relating to fines and penalties, additionalRTT funding and end of year specialised services challenges to drugs and devices expenditure.
The main areas of performance were Specialised Services £6.3m plus additional incomerecovered through Cancer Drugs Fund (CDF) of £4.7m.
The in month expenditure position showed a material movement in underlying pay bill ofc£0.4m. Analysis shows this to be due to the following;
Site
Headlines
£k
Good Hope
Backlog claim of Waiting List InitiativesAdditional Capacity – Ward 3
13334
Heartlands
Additional Locums (sickness / vacancy)
121
Solihull New Waiting List InitiativesIncreased Winter / Thornbury
1525
Trustwide
A&E Nursing (sickness / vacancy)
52
Total 380 The table below summarises our current Finance & Performance position:
Category
Mar
Headlines
Finance Pay control
Costs to delivery performanceEfficiency (SIEP) delivery
Performance
A&E 4 hour18 week admitted RTT / non admitted RTT/ incomplete pathwaysCancer 2 week wait / breast symptoms/ 62 day waitsDiagnostics
Contracting
All contract risk for the JMRA has been covered in theyear end contract settlement, including fines andCQUIN non delivery. Contract negotiations for 15/16are still ongoing for both financial and non financial elements of the contract.
Prepared for Finance and Performance Committee meeting on 24 April 2015.
Author Darren Cattell
1
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.71
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
1. FINANCE
The Trust’s income and expenditure position in March was a £2.8m surplus and a £5.6m lossat year end.
The table below shows the key issues influencing the financial position:
Category Mar
Headlines£m
MedicalStaffing
(0.4)
Expenditure remains unaffordableWaiting List Initiatives spend of £0.4mGreatest pressures in BHH, SOL and GHH
Nursing &Midwifery
(0.7)
Expenditure remains unaffordableEnhanced bank rates continueGreatest pressures in BHH and GHH
SIEP
(0.5)
Most significant shortfalls in BHH, SOL and W&C’s
Overall Position
1.1 SIEP – Actual delivery in month was £1.4m (75% of target). The year end delivery for2014/15 was £16.4m (68%) with the balance of plans being high risk. The focus now mustbe early implementation of 2015/16 plans.
1.4 Cash Deposits – The cash balance at the end of March 2015 was £87.7m. Barring
some insignificant balances held in commercial accounts, this was all held in the Trust’sGBS accounts at the year end. Funds remaining in the GBS current accounts earn 25bpinterest.
1.5 Monitor Targets – The Trust’s Continuity of Service Rating (COSR) at the end of March
was 4. The COSR scale is 1 to 4 with 4 being the highest rating.
1.6 Capital – The total capital expenditure in the year was £20.5m, including accruals which is £21.2m behind the approved budget and £6.8m behind the forecast submitted toMonitor. A carry forward of £20.4m is being requested with the majority of this being dueto slippage on cross site plans.
Prepared for Finance and Performance Committee meeting on 24 April 2015.
Author Darren Cattell
2
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.72
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
2 CONTRACTING LDP meetings continue with HEFT service leads and the CCG. Key items for considerationcurrently are the underlying activity growth assumptions on both the Acute and Community contracts. Discussions are underway at FD level to agree these principles. Subgroup meetings to work up the detail of the KPI’s, CQUINs, SDIPs and other contractual content arecontinuing and an escalation document is currently being drawn up to identify the currentgaps. This will support any required escalation and identify the risks preventing sign off.
3 ESCALATION PROCESS
The current escalation process will be revised in line with organisation needs at the start ofthe new financial year.
4 CURRENT ACTIONS
The below are the updated actions:
1. Division’s financial performance to be reported at Delivery Unit meetings.2. Additional action to manage medical pay.3. Executive led improvement in areas of poor performance.4. Implement additional measures to improve performance.5. Exit strategies to be in place for winter/additional measures above new investment
decisions.6. Close GAP on 2015/16 SIEP and begin early implementation.7. Further review the decision regarding enhanced bank rates.8. Conclude demand and capacity investment decisions when linked to 4, 5 and 7 above.
5 CONCLUSION
With investment in ongoing capacity clear exit strategies from winter and additional measures coupled with early delivery of service improvement efficiency plans will be essential to mitigating financial risk at the start of the new financial year. Additional investment andongoing support needs to impact positively on performance, care and all standards in quarter1 of 2015/16.
6 RECOMMENDATIONS
It is recommended the above actions are implemented.
Darren CattellInterim Director of Finance & PerformanceMarch 2015Heart of England NHS Foundation Trust
Prepared for Finance and Performance Committee meeting on 24 April 2015.
Author Darren Cattell
7
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.73
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
1. A&E Activity 2014/15
• There were 18,154 A&E attendances in Feb-15, 348
attendances, 2% above plan.• In February 85.65% of patients were seen within 4
hours including walk ins.• At Heartlands 81.95% (1,626 breaches) of patients
within 4 hours, 76.52% (1,437 breaches) at Good Hopesite and 97.32% (81 breaches) at Solihull site.
• A&E activity excludes A&E outpatient attendances.• Form TF2A
In-Month Performance
2. Emergency Activity 2014/15 excluding Paediatrics, Paediatric Surgery and Obstetrics
• The Emergency activity was above plan by 1% inFebruary, 56 Spells.
• Heartlands 113 Spells, 4% and Solihull, 14 Spells, were above plan.
• Good Hope 39 Spells, 4% and Women & Childrens, Spells, 15% were below plan in month.
• Following the implementation of PMS2 a potential patient classification issue has been identified. This iscurrently under a detailed review and any necessaryretrospective realignment will be actioned.
• Form TF2A
In-Month Performance
3. Emergency Activity 2014/15, Paediatrics, PaediatricSurgery and Obstetrics
• The activity is above plan by 6%, 55 Spells in Feb-15.• The activity YTD is above plan by 6%, 562.• Following the implementation of PMS2 a potential
patient classification issue has been identified. This is currently under review and any necessary retrospective realignment will be actioned.
In-Month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.74
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
4. AMU, MAU & SAU Activity 2014/15
• There were 1,938 spells during Feb-15, 246 Spells,
15% above plan.• Good Hope 102 spells, 20%, Heartlands, 87, 15% an
Solihull, 58, 9% were above plan in month.• There were 4,813, 25% additional spells YTD.
In-Month Performance
5. Maternity Spells Activity 2014/15
• In February 2015, there were 816 Births Trustwide (5 at Heartlands, 294 at Good Hope, and 12 at Solihull) This compares to the plan of 852 (-4%). In Febru there were 3 planned homebirth (2 at Heartlands andat Good Hope).
In-Month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.75
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
6. Elective & Day Case Activity 2014/15
• The Day case and Elective activity was above plan by
3%, 220 Spells during Feb-15.• Heartlands, 2%, 75 Spells and Women and
Childrens, 32%, 146 Spells were below plan in mont• Solihull Division, 25%, 318 Spells, Clinical Support, 5
Spells, 46% and Good Hope, 69 Spells, 11% were above plan in month.
• Following the implementation of PMS2 a potential patient classification issue has been identified. This is currently under a detailed review and any necessary retrospective realignment will be actioned.
• There were 186 patients treated by the private sector during February and 1,550 YTD. Ophthalmology (58General Surgery (56), ENT (32), Orthopaedics (26),Urology (7), Vascular Surgery (4) and Gynaecology (3)had patients treated by the private sector in month.
• 122 patients were treated in the Vanguard Theatre in February and 897 patients since it opened in September.
• There were 24 cancelled sessions during February,97.22% of the scheduled sessions were utilised. The following specialties cancelled sessions, General Surgery (8), Gynaecology (5), Orthopaedics (4), Thoracic Surgery (2), Urology (2), Vascular Surgery (2) and ENT (1).
• 75% (18) of the Theatre sessions were cancelled due to no surgeon in month.
• In addition 20 sessions were cancelled in the VanguarTheatre during February.
• 121 operations were cancelled on the day during February, 51 (42%) of the cancelled operations were at Good Hope, 44 (36%) at Heartlands and 26 (21%) at Solihull.
In-Month Performance
7. Outpatient Activity 2014/15
• There were 64,935 Outpatient attendances during Feb-15, 719 atts, 1% maottreendances than planned.
• Good Hope 309 atts, 4%, Clinical Support, 123 atts, and Solihull, 922 atts, 4% were above plan in m
• Heartlands (303 atts, 1%) and Women &Childrens (331 atts, 8%) were below plan in month.
Total DNA Rates (February-15):
• Good Hope 8.06% (2,166*)• Heartlands 11.95% (3,780*)• Solihull 7.45% (1,783*)
The DNA rate for first attendances was 14.16% (1,361*) at Heartlands site during Feb-15. Good Hope (8.30%) and Solihull (8.12%) achieved the target of less than 11%.*No. of DNAs.
In-Month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.76
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
8. Performance against Monitor Standards 2014/15
• The overall I&E deficit was £8.4m at the end of month11.
• This deficit was £9.4m adverse to the Monitor plan a£2.8m adverse to the recent reforecast.
• Income was £14.9m favourable to plan while operating expenses were £28.5m adverse to the Monitor plan.
• PDC dividend expenditure was £1.2m favourable to plan, depreciation £3.0m favourable to plan.
• Continuity of Service Rating (COSR) was 4 for mont11, the highest rating.
In-month Performance
9. Income 2014/15
NHS Contract Income (Category A)
There was a trustwide over performance of £0.8m in month,£10.2m YTD.
• Specialised Services income was above plan by £0.4m in February, driven by drugs and vascularexcluded devices.
• Income relating to the Cancer Drugs Fund was £0.4m in month.
In-month Performance
10. Income and Expenditure against Operational Budgets
• The Trust is (£12.5m) over spent at Month 11 of2014/15.
• Pay is over spent by (£9.2m)• Non Pay is over spent by (£6m)• Other Operating Revenue £3.1m over recovered• Form TF1
In-Month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.77
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
11. Operational Budgets 2014/15
Heartlands Hospital (BHH) is over spent by (£15.1m)
Income under recovery (£0m)
Pay over spend (£5.9m)
Non Pay over spend (£9.2m)
Clinical Support Services (CSS) is under spent by £0.2m
Income over recovery £0.3m
Pay under spend £1.5m
Non Pay over spend (£1.6m)
Good Hope Hospital (GHH) is over spent by (£7.2m)
Income over recovery £0m
Pay over spend (£4.6m)
Non Pay over spend (£2.6m)
Solihull Hospital (SOL) is over spent by (£5.4m)
Income over recovery £0.2m
Pay over spend (£1m)
Non Pay over spend (£4.6m)
Womens and Childrens (WC) is over spent by (£2.8m)
Income over recovery £0.8m
Pay over spend (£0.5m)
Non Pay over spend (£3.2m)
In-month Performance
Corporate Directorates (CD) is under spent by £0.8m Income under recovery (£0.1m)
Pay under spend £0.8m
Non Pay under spend £0m
Corporate Trust Wide (CTW) is under spent by £16.7m
Income over recovery £0.8m
Pay over spend (£0.2m)
Non Pay under spend £16m
Facilities (FAC) is under spent by £0.4m
Income over recovery £0m
Pay under spend £0.7m
Non Pay over spend (£0.3m)
Bad Debt provision included within the above: £1m
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.78
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE12. Pay Expenditure
Pay Expenditure is over spent by (£9.2m) at Month 112014/15.
Material variances to operational budget relates to:
• Medical Staffing, which is over spent by (£7.5m) ,• Nursing & Midwifery overspent by (£4.7m),• Off set by other support staff underspend totalling
£3.1m• Form TF3
In-month Performance
13. Non pay Expenditure
Non Pay is over spent by (£6m) at Month 11 in 2014/15.
Material overspends against operational budgets are:
• 2014/15 SIEP shortfall (£7.1m)• Clinical Supplies overspent (£5.2m)• Drugs over performance benefit £2m• Depreciation, Amortisation benefit £2.3m• Miscellaneous Other Expenses £2m
Form TF4
In-month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.79
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
14. Service Improvement Efficiency Plan 2014/15
Feb - In Month Year To Date Forecast @ Month 11
GROUPS Target ActualRec
ActualNon Rec
Variance Target ActualRec
ActualNon Rec
Variance AnnualTarget
Actual(3,4,5)
Variance(0,1,2)
heartlands hospital 625.0 285.6 43.6 (295.9) 6,875.0 2,475.7 499.2 (3,900.2) 7,500.0 3,301.8 (4,198.2)
good hope hospital 183.3 101.6 2.0 (79.7) 2,016.7 837.4 269.1 (910.2) 2,200.0 1,219.5 (980.5)
solihull 291.7 189.3 7.8 (94.6) 3,208.3 1,554.3 123.8 (1,530.2) 3,500.0 1,894.3 (1,605.7)
clinical support services 433.3 242.6 73.2 (117.5) 4,766.7 2,909.5 622.1 (1,235.1) 5,200.0 4,031.3 (1,168.7)
womens & childrens 225.0 51.0 0.1 (173.9) 2,475.0 540.4 0.7 (1,933.8) 2,700.0 592.3 (2,107.7)
facilities 116.7 102.7 19.3 5.3 1,283.3 1,030.6 201.6 (51.2) 1,400.0 1,355.4 (44.6)
corporate directorates 125.0 136.0 6.8 17.7 1,375.0 1,079.3 117.2 (178.5) 1,500.0 1,353.1 (146.9)
corporate trustwide 0.0 166.7 0.0 166.7 0.0 2,633.3 0.0 2,633.3 0.0 2,800.0 2,800.0
TOTAL 2,000.0 1,275.5 152.6 (571.9) 22,000.0 13,060.5 1,833.6 (7,105.9) 24,000.0 16,547.8 (7,452.2)
• The Trust achieved £1.43m (71.4%) efficiency in Month 11.• These results show a (£0.6m) shortfall against target at Month 11.
Based on Month 11 results the forecast out turn is £16.5m delivery of savings (68.9%).
Analysis of forecast:
• £16m in risk category 5 Delivered• £0.2m in risk category 4 Planned with expected delivery• £0.3m in risk category 3 Suggested plans
In-month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.80
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
BALANCE SHEET
15. Combined Capital Expenditure YTD 2014/15 YTD Expenditure was £17.8m, 77.0% of the reforecast YTD Monitor Plan (MP) and 42.9% of total Approved Budget (AB)£41.5m. Orders raised were £25.0m, 108.1% of YTD MP &60.2% of AB.
• Operational was £6.6m, 73.9% of YTD MP, key spends
on LAN & other IT projects• Other was £6.6m, 78.7% of YTD MP; with spend on
replacement MRI Scanner, Energy Sustainability,Document Scanning, Negative Pressure rooms.
• Site Strategy Investment expenditure was £4.4m,79.3% of YTD MP, spend on Hybrid Theatres, Dermatology relocation, AMU refurb at GHH, the Chemotherapy and Rheumatology units
• HPA was £136k, 78.1% of YTD MP
YTD Performance
16. Capital Expenditure in Month 2014/15
M11 In-month expenditure was £2.4m:
• FAC / Site Strategy £2.1m- Hybrid Theatres,
Dermatology relocation SOL, AMU refurbishment at GHH, Energy Sustainability, Ward 3 refurbishment at GHH.
• CD £162k- Corporate Community PC Replacement and iPads, Windows 7 compliance, LAN
• CSS £86k- Negative Pressure Isolation Rooms Ward28 at BHH
• WC £36k- Obstetrics Capacity Risks project at BHH, Bladder Scanner at GHH, 2 Bipad Machines
In-month Performance
• Payment performance in February is about 70%. The
volume of invoices paid in February is 13,535 in line with normal volumes.
• The continued poor payment performance is due to backlog clearing and processing delays following the Readsoft upgrades and will also impact on March performance and beyond.
Cumulative Performance
17. Creditors 2014/15
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.81
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
BALANCE SHEET
18. Debtors 2014/15
• Total debt reduced by £2.423m during February t£19.611m.
• Health Education England paid a training & education invoice for £5.156m during the month
• There was a deterioration in the underpayment of th monthly SLA mandate invoices by £1.387m to acumulative underpayment of £2.885m, in anticipationexpected contract penalties. Thoseunderpaying include Birmingham Cross City CCG£1.664m and Solihull CCG £1.116m.
• Solihull CCG recalled a £2.000m advance on the February SLA mandate payment, but replaced it with a £0.550m in advance of the March SLA mandate payment.
• A resilience funding invoice for £3.472m to Birmingham Cross City Clinical Commissioning Group remains outstanding and disputed. The invoice will be credited shortly and a replacement invoice for £2.129m will issued.
• Ante natal maternity pathways activity debt for April2013 to December 2014 increased to £3.525m ,including £1.719m with Burton Hospitals, £0.860m with Sandwell & West Birmingham Hospitals, and £0.490m with Birmingham Womens Hospital.
• Burton Hospitals Foundation Trust have debts of£2.337m, (including £1.719m for ante natal maternity pathways activity), and have recently placed the account on hold until this Trust settle their debtfor £0.595m
In-month Performance
CASHFLOW
19. Monthly Closing Cash Balance vs Plan 2014/15
• The cash balance at the end of February 2015 was£101.6m, £18.6m above plan.
• Operating cash flows were £17.0m below plan. This was offset by favourable working capital movements of£18.6m. Capital expenditure in cash terms was£14.9m less than plan.
• The half yearly PDC dividend payment was processed in September and this was £1.7m less than planned including a rebate for the last financial year.
• All Trust funds remain in the GBS umbrella as a change in the rules on calculating PDC dividend means that it is currently financially unviable to invest in other commercial banks.
• £75m of funds have been reinvested in the National Loan Fund (NLF) for 6 months at a rate of 49bp. Afurther £9.0m was on deposit with NLF at the month end on a short term basis attracting interest rates of around 40bp.
• Funds in GBS attract 25bp.
In-month Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.82
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
12
M
ay-…
Jun-
12
Jul-1
2 Au
g-12
Sep-
12
Oct
-12
Nov
-12
Dec-
12
Jan-
13
Feb-
13
Mar
-13
Apr-
13
May
-…
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec-
13
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Jan-
14
Feb-
14
Mar
-14
Apr-
14
M
ay-…
Jun-
14
Ju
l-14
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
18 weeks: Reported 1 month in arrears
Admitted Non-admitted HEFT have now resumed reported against the Admitted patient pathway (clock stops), and achieved 79.34% against the 90% target for Jan15, with the aim to continue to see
longer waits in order to help clear the backlog
HEFT managed to see 85.91% of non-admitted patients within 18 weeks against
the 95% target for Jan15
100%
95%
Target
99% 97%
Target
90%
95% 93%
85%
91%
80%
75%
89% 87% 85%
Incomplete Pathways
No data reported in month
100%
99%
98%
97%
96%
95%
94%
93%
92%
91%
90%
Out-turn
Target
A&E
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
Total time in A&E
The 95% target for A&E around 4 hour was not met in February with performance at 85.65%
100%
95%
Target
90%
85%
80%
75%
70%
N.Atkins PM-P&I 20/03/2015 Z:\Data\PMU\Performance Monitoring\KPI 2014-15\2014-15 Trust KPI.xlsbFC 1
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.83
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs Cancers: Reported 1 month in arrears
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
2 weeks 31 day GP
The Trust failed the 93% target for the 2 week GP cancer indicator in January at 91.24%, and also failed the 2 week Breast symptom 93% target, achieving 76.61%
The Trust achieved the 96% target for 31 day cancers in January , out-turning at 98.12% in month
100% 95% 90% 85% 80% 75% 70% 65% 60% 55% 50%
100%
99%
98%
97%
96%
95%
94%
93%
92%
91%
90%
Target
2 week GP 2 week Breast Target
31 day anti-cancer 31 day surgery
The Trust met the 31 day anti-cancer drug target of 98% in January, achieving
100%
100%
The Trust met the 31 day surgery modality cancer target of 94% in January,
achieving 96.72%
Target
99%
98%
97%
96%
95%
94%
93%
92%
91%
90%
Target 99% 97% 95% 93% 91% 89% 87% 85%
Cancers: (continued)
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
62 day cancers 62 day screening
The Trust achieved the 62 day cancer 85% target in January, achieving 86.22% The Trust missed the 62 day national screening cancer 90% target in January,
achieving 50% 100%
95%
Target
100%
90%
T arget
90%
85%
80%
80% 70% 60% 50%
75% 40%
N.Atkins PM-P&I 20/03/2015 Z:\Data\PMU\Performance Monitoring\KPI 2014-15\2014-15 Trust KPI.xlsbFC 1
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.84
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs Infection Control
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec
-13
Jan-
14
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec
-14
Jan-
15
Feb-
15
Mar
-15
c-diff
The target for incidents of c-diff is no more than 6 in February, and in month the
Trust reported 3 cases, with a total of 67 YTD
12
10
8
6
4
2
0
N.Atkins PM-P&I 20/03/2015 Z:\Data\PMU\Performance Monitoring\KPI 2014-15\2014-15 Trust KPI.xlsbFC 1
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.85
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
516.839 527.059 10.220 NHS Clinical Revenue 563.913 577.912 13.999 560.801
0.715 0.539 (0.177) Clinical Revenue - Private Patients 0.780 0.693 (0.087) 0.628
0.165 0.148 (0.017) Clinical Revenue - Overseas Visitors 0.180 0.168 (0.012) 0.163
3.963 3.861 (0.102) Research and Development revenue 4.323 4.188 (0.135) 4.132
20.662 21.376 0.714 Education and Training revenue 22.540 23.088 0.548 22.885
0.446 0.411 (0.035) PFI Specific Revenue 0.487 0.448 (0.039) 0.448
0.468 0.411 (0.057) Donations and Grants received 0.510 0.313 (0.197) 0.711
4.376 4.370 (0.006) Parking Revenue 4.774 4.829 0.055 4.800
0.848 0.954 0.106 Catering Revenue 0.925 1.029 0.104 0.910
0.246 0.264 0.018 Accommodation Revenue 0.268 0.257 (0.011) 0.306
5.944 9.509 3.565 Revenue from non patient services to other bodies
6.485 10.349 3.864 13.922
21.398 22.100 0.701 Miscellaneous other operating revenue 23.399 24.403 1.004 25.715
576.070 591.002 14.932 Total Operating Revenue 628.584 647.677 19.093 635.422
(350.981) (352.767) (1.786) Employee expenses, permanent staff (382.254) (383.759) (1.505) (376.603)
(0.176) (22.504) (22.328) Employee expenses, agency and contract staff (0.192) (24.702) (24.510) (19.900)
(46.180) (53.434) (7.254) Drugs (50.217) (57.160) (6.943) (51.377)
(58.430) (57.375) 1.056 Clinical Supplies (63.551) (61.202) 2.349 (62.338)
(16.116) (15.365) 0.751 Non Clinical Supplies (17.520) (16.315) 1.205 (17.173)
(2.407) (2.451) (0.044) Research and Development Expense (2.626) (2.701) (0.075) (2.636)
(1.826) (2.007) (0.181) Education and Training Expense (1.992) (2.018) (0.026) (2.229)
(1.049) (1.629) (0.580) Consultancy Expense (1.144) (1.926) (0.782) (2.241)
(66.500) (67.404) (0.903) Miscellaneous other Operating expense (72.853) (75.771) (2.918) (75.593)
(3.749) (1.021) 2.727 (Increase)/decrease in impairment of receivables
(4.090) (1.620) 2.470 (2.291)
(0.096) (0.087) 0.009 PFI unitary payment (0.105) (0.095) 0.010 (0.095)
(547.510) (576.043) (28.532) Total Operating Expenses (596.543) (627.269) (30.726) (612.475)
28.560 14.959 (13.601) EBITDA 32.041 20.408 (11.633) 22.947
(0.110) (0.162) (0.052) Gain / loss on asset disposals (0.120) (0.252) (0.132) (0.031)
(20.900) (17.924) 2.976 Total Depreciation and amortisation (22.800) (20.000) 2.800 (18.039)
(6.545) (5.386) 1.159 PDC Dividend expense (7.145) (5.876) 1.269 (5.574)
0.333 0.404 0.071 Total interest receivable 0.364 0.412 0.048 0.385
0.000 0.000 0.000 Other finance costs 0.000 0.000 0.000 (0.003)
(0.275) (0.249) 0.026 Interest expense (0.301) (0.271) 0.030 (0.282)
1.063 (8.359) (9.422) Surplus/(deficit) before impairments 2.039 (5.579) (7.618) (0.597)
0.000 0.000 0.000 Impairment (Losses) / Reversals 0.000 0.000 0.000 (4.759)
1.063 (8.359) (9.422) Surplus/(deficit) after impairments 2.039 (5.579) (7.618) (5.356)
February 2015 Trust Wide Income and Expenditure Form TF1A
Year to Date Full Year
Annual Actual Variance Annual Forecast Variance 2013/14
Plan Actual to Plan Forecast toPlan Plan
£m £m £m £m £m £m £m
Key perfomance Indicators (KPIs)
Year to Date Full Year
Annual Actual Variance Annual Forecast Variance 2013/14Plan Actual to Plan Forecast to
Plan Plan
0.20% (1.39%) (1.59%) Net I&E Margin 0.34% (0.82%) (1.17%) (0.09%) 28.092 14.548 (13.544) EBITDA (£m) adjusted 31.531 20.095 (11.436) 22.236
100.00% 51.79% (48.21%) EBITDA achieved, % of projection 100.00% 63.69% (36.31%) 58.93%
4.88% 2.46% (2.42%) EBITDA margin (%) 5.10% 3.15% (1.95%) 3.50%
28.425 14.952 (13.473) Revenue available for debt service (£m) 31.895 20.507 (11.388) 22.621
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.86
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Last Month This Month Variance to Annual Plan Forecast Variance 31 March Actual
£m
Actual
£m
Plan
£m
£m
£m
from Plan
£m
2014
£m
February 2015
Year to Date
Trust Wide Balance Sheet Form TF1B Full Year
5.100 5.109 (3.486) Intangible Assets, Net 9.238 10.617 1.379 3.051 236.009 237.990 (4.397) Property, Plant and Equipment, Net 245.492 239.824 (5.668) 239.867
4.312 4.302 (0.059) On balance sheet PFI assets 4.350 4.250 (0.100) 4.374 245.421 247.401 (7.941) Fixed Assets, net 259.080 254.691 (4.389) 247.292
2.756 2.762 1.723 Trade Receivables, non current, gross 1.039 2.700 1.661 2.771
(1.711) (1.711) (1.711) Impairment of receivables for bad and doubtful debts, non current 0.000 (1.711) (1.711) (1.711)
1.046 1.052 0.013 Trade and other receivables, net, non current 1.039 0.989 (0.050) 1.060 246.467 248.452 (7.929) ASSETS, NON CURRENT 260.119 255.680 (4.439) 248.352
9.424 9.240 1.362 Inventories 7.878 8.500 0.622 7.996 36.691 26.778 (4.199) NHS Trade Receivables, current, gross 31.002 30.000 (1.002) 21.616 2.215 4.283 (1.387) Non NHS Trade Receivables, current, gross 5.675 4.100 (1.575) 6.270 0.000 0.000 0.000 Other Related Party Receivables 0.000 0.000 0.000 1.049 2.159 1.850 0.156 Other Receivables 1.696 1.500 (0.196) 2.775
(9.046) (9.045) 0.665 Impairment of receivables for bad and doubtful debts, current (10.051) (9.735) 0.316 (9.802)
2.884 2.676 (0.048) Accrued Income 2.726 2.000 (0.726) 1.995 10.046 8.164 0.029 Prepayments 8.142 6.000 (2.142) 6.174 99.671 101.568 18.624 Cash and Cash Equivalants 78.706 83.000 4.294 86.699
154.044 145.513 15.201 CURRENT ASSETS 125.774 125.365 (0.409) 124.771
400.511 393.966 7.273 TOTAL ASSETS 385.893 381.045 (4.848) 373.123
(3.874) (2.716) 0.692 Trade Payables (2.026) (3.000) (0.974) (3.868) (18.101) (17.582) (1.906) Other Payables (19.505) (16.000) 3.505 (2.024) (3.917) (5.472) 1.413 Capital Payables (4.558) (3.654) 0.904 (4.136)
(58.708) (56.344) 13.257 Accruals (42.757) (51.450) (8.693) (47.577) (0.480) (0.480) 0.000 Finance Leases / PFI Leases, Current (0.480) (0.480) 0.000 (0.480) (1.958) (2.448) (0.529) PDC Dividend Payable 0.000 0.000 0.000 0.000
(11.328) (11.154) 3.330 Provisions, current (8.594) (11.100) (2.506) (20.667) (13.004) (11.128) 2.130 Deferred Income (9.006) (6.000) 3.006 (6.605)
(111.370) (107.324) 18.387 CURRENT LIABILITIES (86.925) (91.684) (4.759) (85.356)
42.674 38.189 (3.186) NET CURRENT ASSETS (LIABILITIES) 38.849 33.681 (5.168) 39.415
(7.531) (7.531) 5.181 Provisions, non current (2.580) (7.500) (4.920) 0.000 (1.640) (1.629) (0.112) Finance Leases, non current (1.740) (1.620) 0.120 (1.746) (2.410) (2.393) (0.172) PFI Leases, non current (2.564) (2.375) 0.189 (2.574)
(11.580) (11.553) 4.897 LIABILITIES, NON CURRENT (6.884) (11.495) (4.611) (4.320)
277.560 275.088 (16.012) TOTAL ASSETS EMPLOYED 292.084 277.866 (14.218) 283.447
214.169 214.169 0.000 Public Dividend Capital 214.169 214.169 0.000 214.169 18.575 16.103 (15.018) Retained Earnings / (Accumulated Losses) 32.691 19.459 (13.232) 22.728 44.986 44.986 (0.994) Revaluation Reserve 45.393 44.407 (0.986) 46.719 (0.169) (0.169) 0.000 Miscellaneous Other Reserves (0.169) (0.169) 0.000 (0.169) 277.560 275.088 (16.012) TOTAL TAXPAYERS EQUITY 292.084 277.866 (14.218) 283.447
Last Month Actual
Year to Date
This Month Actual
Variance to
Plan
Key perfomance Indicators (KPIs)
Full Year
Annual Plan Forecast Variance from Plan
31 March
2014
(2.57%) (3.31%) Net Return After Financing (0.16%) (3.00%) (2.84%) 0.20 %
19.050 16.584 Liquidity 18.690 14.452 (4.239) 18.467
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.87
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
February 2015
Trust Wide Cash flow
Form TF1C
Year to Date Full Year
Actual Plan Variance to Plan Annual Plan Forecast Variance fromPlan 2013/14
(8.359)
1.053
(9.412)
Surplus / (Deficit) after tax 2.037
(5.579) (7.616)
(5.357)
- Non - cash flows in operating surplus / (deficit): - - (0.155) (0.059) (0.096) Finance income/charges (0.064) (0.141) (0.077) (0.100)(0.411) - (0.411) Donations and grants received of PPE and intangibles - (0.313) (0.313) (0.711)
- - Other operating non-cash movements - - -17.924 20.900 (2.976) Depreciation and amortisation, total 22.800 20.000 (2.800) 18.039
- - Impairment losses / (reversals) - - 4.7590.162 0.110 0.052 (Gain) / loss on disposal of non current assets 0.120 0.252 0.132 0.0315.386 6.550 (1.164) PDC Dividend Expense 7.145 5.876 (1.269) 5.5741.021 3.989 (2.968) Other 4.353 0.910 (3.443) -
15.568 32.543 (16.975) Operating Cash Flows before movements in WC 36.391 21.005 (15.386) 22.235
Increase / (decrease) in working capital: (1.244) - (1.244) (Increase)/decrease in inventories - (0.504) (0.504) (0.258)
- - (Increase)/decrease in tax receivable - - - -(5.162) (0.282) (4.880) (Increase)/decrease in NHS Trade Receivables (0.308) (8.384) (8.076) (9.193)0.232 (0.052) 0.284 (Increase)/decrease in Non NHS Trade Receivables (0.057) 2.170 2.227 3.913
- - (Increase)/decrease in other related party receivables - 1.049 1.049 -0.925 (0.016) 0.941 (Increase)/decrease in other receivables (0.017) 1.275 1.292 (0.716)
(0.681) (0.025) (0.656) (Increase)/decrease in accrued income (0.027) (0.005) 0.022 0.046
- - (Increase)/decrease in other financial assets - - - -(1.990) (0.074) (1.916) (Increase)/decrease in prepayments (0.081) 0.174 0.255 (1.208)
- - (Increase)/decrease in Other assets (non chartable assets) - - - -4.523 0.082 4.441 Increase/(decrease) in Deferred Income (excl. Govt Grants.) 0.090 (0.605) (0.695) (3.687)
- - Increase/(decrease) in Deferred Income (Govt. Grants) - - - -(9.513) (0.770) (8.743) Increase/(decrease) in Current provisions - (1.663) (1.663) 7.225
- - Increase/(decrease) in post-employment benefit obligations - - - -
- - Increase/(decrease) in tax payable - - - -(1.152) 0.018 (1.170) Increase/(decrease) in Trade Creditors 0.020 (0.868) (0.888) 0.44015.558 12.846 2.712 Increase/(decrease) in Other Creditors 12.862 13.975 1.113 0.084
8.767 (12.276) 21.043 Increase/(decrease) in accruals (12.606) 3.873 16.479 5.801
- - Increase/(decrease) in other Financial liabilities - - - -
- - Increase/(decrease) in Other liabilities (non charitable assets) - - - -10.263 (0.549) 10.812 Increase / (decrease) in working capital, Total (0.125) 10.487 10.612 2.447
7.531 (0.230) 7.761 Increase/(Decrease) in Non-current Provisions - (0.404) (0.404) 0.124
33.362 31.764 1.598 Net cash inflow/(outflow) from operating activities 36.266 31.088 (5.178) 24.806
(17.797)
(15.791)
(2.006) Net cash inflow/(outflow) from investing activities: Property - new land, buildings or dwellings
(18.918) (10.427)
8.491 (12.180)
(3.540) 3.540 Property - maintenance expenditure (3.925) (1.759) 2.166 (3.495)
(2.987) 2.987 Plant and equipment - Information Technology (3.465) (7.599) (4.134) (3.594)
(5.676) 5.676 Plant and equipment - Other (6.675) (6.000) 0.675 (4.149)
- - Property, plant and equipment - other expenditure - - - (2.955)
0.087 (0.087) Proceeds on disposal of property, plant and equipment 0.100 0.114 0.014 -
- - Purchase of investment property - - - -
- - Proceeds on disposal of investment property - - - -
(2.942) 2.942 Purchase of intangible assets (3.614) (1.667) 1.947 (1.527)
- - Proceeds on disposal of intangible assets - - - -
- - Expenditure on capitalised development - - - -1.336 (0.500) 1.836 Increase/(decrease) in Capital Creditors 0.000 (0.482) (0.482) (1.396)
- - Government grants received - - - -
- - Purchase of investments & deposits made - - - -
- - Proceeds on disposal of investments & withdrawals - - - -
- - Other cash flows from investing activities - - - -(16.461) (31.349) 14.888 Net cash inflow/(outflow() from investing activities, Total (36.497) (27.820) 8.677 (29.296)
16.901 0.415 16.486 Net cash inflow/(outflow) before financing (0.231) 3.268 3.499 (4.490)
Net cash inflow/(outflow) from financing activities: - - Public Dividend Capital received - - - 3.055
- - Public Dividend Capital repaid - - - -(1.889) (3.572) 1.683 PDC Dividends paid (7.144) (5.876) 1.268 (5.270)
- - Finance leases - - - -(0.128) (0.128) - Interest element of finance lease rental payments - other (0.139) (0.137) 0.002 (0.139)(0.138) (0.138) - Interest element of finance lease rental payments - On-balance sheet PFI (0.151) (0.150) 0.001 (0.151)(0.108) (0.108) - Capital element of finance lease rental payments - other (0.118) (0.120) (0.002) (0.118)(0.181) (0.181) - Capital element of finance lease rental payments - On-balance sheet PFI (0.197) (0.197) - (0.197)0.404 0.334 0.070 Interest received on cash and cash equivalents 0.364 0.412 0.048 0.385
- - Movement in Other grants/Capital received - - - -
- - Donations received in cash - - - -0.009 - 0.009 (Increase)/decrease in non-current receivables - 0.070 0.070 0.434
- - Increase/(decrease) in non-current payables - - - -
0.001 (0.001) Other cash flows from financing activities 0.001 (0.968) (0.969) (0.476)(2.031) (3.792) 1.761 Net cash inflow/(outflow) from financing activities, Total (7.384) (6.966) 0.418 (2.477)
14.870 (3.377) 18.247 Net increase / (decrease) in cash (7.615) (3.698) 3.917 (6.967)
86.698 86.321 0.377 Opening cash balance 86.321 86.698 0.377 93.66514.870 (3.377) 18.247 Net increase / (decrease) in cash (7.615) (3.698) 3.917 (6.967)
101.568 82.944 18.624 Closing cash balance 78.706 83.000 4.294 86.698
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.88
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
February 2015 Monitor Continuity of Service Ratings (COSR) Form TF1D
Metric
Actual
Year to DateRating
Weight
4
COSR:3
2
1
Capital Service Cover
2.59
4
50.0%
2.50
1.75
1.25
<1.25Liquidity 16.6 4 50.0% 0 -7.0 -14.0 <-14.0
Weighted Average 4.00 100.0% Overriding rules
4
Metric
Actual
FY ReforecastRating
Weight
4
COSR:3
2
1
Capital Service Cover
3.17
4
50.0%
2.50
1.75
1.25
<1.25Liquidity 14.5 4 50.0% 0 -7.0 -14.0 <-14.0
Weighted Average 4.00 100.0% Overriding rules
4
Metric
Actual
FY PlanRating
Weight
4
COSR:3
2
1
Capital Service Cover
4.17
4
50.0%
2.50
1.75
1.25
<1.25Liquidity 18.7 4 50.0% 0 -7.0 -14.0 <-14.0
Weighted Average 4.00 100.0% Overriding rules
4
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.89
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
1
Appendix 2 Standing Financial Instructions Update
1. Introduction
Due to various changes in the Trust over the last year it is necessary to amend the Trust Standing Financial Instructions (SFIs). This paper seeks approval from the Finance and Performance Committee to amend the SFIs in the following areas;
• Amend the delegated authority levels to revised values, new authority levels and to reflect the operational managers as the dominant authoriser.
• Confirm the reporting arrangements for orders and contracts above chief executive level.
• Make self-approval of orders prohibited except for noted exceptions.
• Detail the exceptions to the authority levels.
• Note the authorisation process for approval of business cases.
• Provide clarity on authority levels for contracts
This change will give clarity to the Trust on the relevant approval rights and will mean that controls can apply whilst decision making is speeded up.
2. Reason for change
The Trust is continually evolving and in March 2014 a change to SFIs was approved by Finance and Performance Committee to reflect the structure that was in place at that time. Since then a Delivery Unit structure has been established, new structures in the heartlands division have been set up and a number of corporate posts have been disestablished. Following the recent structure announcements it is now necessary to update the SFIs to make the authority limits workable with the new posts and to clarify responsibilities.
3. Authority Levels
In 2014 the values were updated to reflect the division/ site structure with site Managing Directors that was in place at the time. Separate headings were set up to reflect that the structures within clinical areas were different to those in corporate and estates / facilities areas. In most cases these levels were applied into the Oracle system. The table below shows these values.
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.90
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
2
Table 1 Previous Authority Levels
Role/ Title Corporate Estates Clinical Limit £Ward Manager/ Community
Services Manager C 2,000
Corporate Department Manager, Executive
Assistants.A 2,000
Estates Directorate Managers, Executive
Assistants, .Administrative Assistant.
E 2,000
Health and Safety Officer, Estates Managers, ,Hotel
Services ManagersE 5,000
Corporate Head of Department A 5,000
Matron / Community Services Equivalent C 5,000
Operational Manager C 5,000Catering Manager E 9,999
Corporate Senior Manager/ Business Consultant/
Business PartnerA 9,999
General Manager C 9,999Deputy Head of Hotel
Services E 10,000
Clinical Director C 10,000Programme Office Manager E 64,999
Head of Hotel Services/ Head of Estates E 64,999
Site Head of Operations C 64,999Deputy ED A 64,999
Associate Medical Director C 65,000Site Managing Director C 100,000Trust Medical Director C 100,000
Director of Asset Management E 100,000
Corporate Executive Director A 100,000
Finance Director E 125,000Deputy CEO A C 125.000
CEO A E C 150,000CEO & Chair A E C 250,000
Board A E C Over 250,000
A number of changes are suggested to the authority levels;
a) Increase the authority levels
An increase in the authority levels, particularly at the higher levels is proposed to reflect the expenditure level that is deemed appropriate for these senior posts. This reflects the increased costs over the last few years, the tendency to consolidate more business s into
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.91
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
3
fewer supplier s and the raising of purchase orders for the total service rather than on an invoice by invoice basis.
b) Finance Director Level the same as all other Executive Directors and disestablishing Deputy Chief Executive as an approval level.
Previously the Finance Director has had a greater authority level than the other executive directors (ED) which has meant that for large orders they were required to be reviewed by the FD before it reached the Chief Executive. This had worked well when the Finance Director and the Deputy Chief Executive post were held by the same person. It is proposed that to provide clarity the Finance Director level is the same as all other ED levels so all orders over the value of an ED go the Chief Executive, and if the Chief Executive requires additional clarification, the requisition can be sent to the FD for review.
c) Operational lead the dominant authoriser
Previously the ordering for each cost centre has been through an operational manager who has had an authority level £1 lower than the clinician. In practice this has meant a delay in getting orders agreed as it requires the input of 2 senior people. Now that the triumvirate arrangements exist for each division and directorate, the proposal is that the operational lead will hold responsibility for approving the orders and where there is a query relating to a particular order will ensure that clinical and nursing colleagues are involved. This should streamline the approval process.
There will be some circumstances where a clinical director will be required to approve orders, such as is the case in pathology, and in these situations, they will be slotted into the managerial position in the hierarchy for that area.
d) Include an additional level for group reporting arrangements
In Heartlands and Solihull divisions there is a need for an additional level to be set up to reflect their structure of Group boards below the division. AN additional level of £25k is proposed for these areas.
The table below shows the proposed revised authority levels. Appendix 1 shows a mapping for the current levels to the proposed levels.
Table 2 proposed Authority levels
Role/ Title Revised limit £
Originator level £2,000Manager £5,000Senior Manager £10,000Group Head (applicable in Heartlands and Solihull division only) £25,000Reporting to Executive Director £65,000Executive Director (non-voting) £100,000Executive Director (Voting) £125,000CEO £250,000Board Over £250,000
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.92
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
4
4. Reporting above Chief Executive Level
Currently orders that are in excess of the level of Chief Executive are required to be reported to the Board according to SFIs. However, practice over a number of years has meant that these are reported to the monthly Finance and Performance Committee. It is proposed that the SFIs are amended so that approval of the purchase orders is the responsibility of Finance and Performance Committee. This will include all orders.
5. Prohibiting self-approval
A review by the Trust’s counter fraud team has have found that there have been instances where the person raising the requisition has also approved that order, known as self-approval. The SFIs will need to explicitly state that this is prohibited unless this has been agreed in advance for that service (e.g. renal), code or where exceptional circumstances that have been approved by the manager mean that this is absolutely necessary. This will mean that if an individual is found to be self-approving they can be advised that is not permitted by SFIs.
6. Exceptions to the authority levels
There are a number of exceptions where the authority levels set out for a role are insufficient on a particular cost line for a role that manager is doing. The exceptions that are current practice are set out in the table below and are required to be approved by the Committee. As any new exception requirements are identified they will be added to the exceptions list in the SFIs.
Table 3 Variations to approval levels
Reason Responsible Manager
Variation to normal levels
Trust wide leased car arrangements
Employee services manager
Normal authority level £10k, needs £25k for leased car lines across whole Trust.
NHS logistics invoices Financial Controller Normal authority level £5k, approves invoices of up to £100k (all items have been previously approved by the budget holder vi i-proc, this is the payment of the consolidated invoice) .
Pathology consumables ordering under the Abbots contract
Pathology Manager Normal approval level would be £25k, needs £65k for this contract)
Mobile telephones and travel consolidated invoices
Chief Financial Controller
No change in approval level required, but approving invoices on Trust wide cost lines. Consolidated invoice, expenditure is already approved via manager at the point of agreeing to have the phone or booking travel.
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.93
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
5
Public Dividend Capital Finance Director PDC payments of c£3-4m required twice per year, approved by FD due to timing of requests.
7. Business Cases and Contracts
There are three elements to incurring spend in the Trust.
When a new area of expenditure is identified in the Trust a business case is required. A business case approval process has been set out and recently agreed at an executive directors meeting. This is included in appendix 2. This shows that the SFI levels for approving a business case follow the board meetings/committees at the same levels as the individual roles except at the executive management board (EMB) where the board approvallevel is £500k, whereas the Chief Executive level is £250k.
A contract is required once a business case has been approved or when a contract for existing services has expired. The levels set out in table 1 above apply to signing of contracts as well as for raising purchase orders. Therefore, if a contract is required for several years the total value of that contract needs to be calculated and the contract signed by the relevant approving manager. This may result in the contract being approved by a higher approval level then is required for the annual purchase order for that service. For example, a three year contract at £40k per year will require sign off by the ED at £120k, but the purchase order can be approved by the person reporting into that ED.
These rules around business cases and contracts will need to be made explicit in the SFIs.
8. Next Steps
Once these revisions have been agreed the next steps are as in the table below.
Task Responsibility Due Date
1 Communicate revised approval levels to managers Angeline Jones
End of May
2 Confirm structures OBS Finance team
End of Aril
3 Set up roles and responsibilities in Oracle system Adrian James, Systems Manager
Mid May
4 Update SFI document with these changes, ratify at FPC, put on website
Angeline Jones
June FPC
5 Run a communications programme to make all managers aware of the requirements in SFIs
Angeline Jones
August
Business Case
Contract Purchase Order
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.94
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
6
9. Recommendation
The Finance and performance Committee is requested to approve the following changes to Standing Financial Instructions;
• Approve the proposed changes in authority levels
• Approve making self-approval of orders prohibited except for noted exceptions.
• Approve the exceptions to the authority levels.
Appendix 1 – Tracker from current levels to proposed levels
Role/ Title Previous Limit £
Change Revised limit £
Originator level 0 New level £2,000Ward Manager/ Community Services Manager
2,000Move to generic originator level 0
Corporate Department Manager, Executive Assistants.
2,000Move to generic originator level 0
Estates Directorate Managers, Executive Assistants, .Administrative Assistant.
2,000
Move to generic originator level 0
Manager 0 New level £5,000Health and Safety Officer, Estates Managers, ,Hotel Services Managers
5,000
Move to generic manger level 0
Corporate Head of Department 5,000 Move to generic manger level 0
Matron / Community Services Equivalent 5,000 Move to generic manger level 0
Operational Manager 5,000 Move to generic manger levelCatering Manager 9,999 Move to generic senior manager level 0Corporate Senior Manager/ Business Consultant/ Business Partner
9,999
Move to generic senior manager level 0
General Manager 9,999 Move to generic senior manager level 0Senior Manager 0 New level £10,000Deputy Head of Hotel Services 10,000 Move to generic senior manager level
Clinical Director 10,000 Move to generic senior manager levelGroup Head (applicable in heartlands and Solihull division only)
0New level £25,000
Reporting to Executive Director 0 New level £65,000
Programme Office Manager 64,999 Move to generic reporting to executive
director category0
Head of Hotel Services/ Head of Estates 64,999 Move to generic reporting to executive
director category0
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.95
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee 24 April 2015Author Angeline Jones
7
Site Head of Operations 64,999 Move to generic reporting to executive director category
0
Deputy ED 64,999 Move to generic reporting to executive director category
0
Associate Medical Director 65,000 Move to generic reporting to executive
director category0
Site Managing Director 100,000 Move to generic executive director (non-voting) category
0
Trust Medical Director 100,000 Move to executive director (voting) category
0
Director of Asset Management 100,000 Move to generic executive director
(non-voting) category0
Executive Director (non-voting) 0 New level £100,000
Corporate Executive Director 100,000 Split between executive director Noting
and non-voting categories)0
Finance Director 125,000 Remove additional level, same authority as all EDs
0
Executive Director (Voting) 0 New level £125,000
Deputy CEO 125.000 Remove level 0CEO 150,000 Increase level £250,000CEO & Chair 250,000 Remove level 0Board Over
250,000Over
£250,000
Angeline JonesChief Financial ControllerApril 2015
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.96
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee meeting on 29 May 2015.Author Darren Cattell
1
EXECUTIVE SUMMARY
We remain under Section 111 Monitor Enforcement.
APRIL POSITION
The Trust had a larger I&E loss in April than planned.
April delivered a £2.7m loss when compared to the planned figure of £2.5m.
All 2015/16 contracts are still currently in negotiation for both the financial and non financial elements. Income is therefore prudently estimated based on activity under JMRA principles.
1. FINANCE
The Trust’s income and expenditure position in April was a £2.7m loss versus a planned loss of £2.5m.
The table below shows the key issues influencing the financial position, in terms of actuals but also in terms of plan:
Category Plan Apr Variance Headlines£m £m £m
NHS Clinical Income 49.7 49.7 -
MedicalStaffing (9.6) (10.4) (0.8)
Expenditure remains unaffordableUnderlying pay controls
Waiting List Initiatives spend of £0.4m
Greatest pressures in BHH, SOL and GHH
Nursing &Midwifery (13.6) (14.1) (0.5)
Expenditure remains unaffordableUnderlying pay controls
Enhanced bank rates continueGreatest pressures in BHH and
GHH
SIEP 0.6 0.4 (0.2) Most significant shortfalls in BHH, CSS, W&C’s and SOL
Other (28.4) (27.5) 1.3 Recognition of investment reserves
Overall Position (2.5) (2.7) (0.2)
FINANCE EXECUTIVE SUMMARY & KEY PERFORMANCE INDICATORS
Month 1 to 30th April 2015
Darren Cattell, Interim Director of Finance & Performance
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.97
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee meeting on 29 May 2015.Author Darren Cattell
2
1.1 Medical Staffing – Total medical expenditure remains unaffordable at £10.4m in month compared to a budget of £9.6m. Divisions need to address this as part of their efficiency plans going forwards, where not resolved as part of rebasing capacity.
1.2 Nursing & Midwifery – Nursing expenditure remains unaffordable at £14.1m in month compared to a budget of £13.6m. Divisions need to address this as part of their efficiency plans going forwards, where not resolved as part of rebasing capacity.
1.3SIEP – Actual delivery in month was £0.4m. Further action is required to close the early gap and deliver early implementation to mitigate risk in 2015/16.
1.4 Cash Deposits – The cash balance at the end of April 2015 was £84.0m, slightly ahead of plan. £65m was held on short term deposits with the National Loans Fund at the end of the month attracting rates of around 40bp. Funds remaining in the main GBS current accounts earn 25bp interest.
1.5 Monitor Targets – The Trust’s Continuity of Service Rating (COSR) at the end of Aprilwas 3 in line with the quarter one plan. The COSR scale is 1 to 4 with 4 being the highest rating.
1.6 Capital – The total planned capital expenditure in the year is £50.4m, including carry forwards. Spend year to date was £1.0m against a plan of £2.2m but did not include any accruals as the year end positon was still being finalised.
2 CONTRACTING
Contract negotiations have not yet concluded, the main areas yet to be resolved are CQUINs and Finance. Subgroup meetings are continuing in order to support the delivery of the final contract package, FD meetings are also ongoing with a focus on the underlying activity assumptions. This is pivotal to supporting the choice of contract type (i.e. JMRA) that best supports the Trust strategy in 2015/16.
3 CONCLUSION
The previously highlighted risk with regards to efficiency planning has resulted in a low level of delivery in April, this coupled with underlying pay controls requires an immediate response to mitigate risk in quarter 1 of the new financial year.
ACTION
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.98
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Prepared for Finance and Performance Committee meeting on 29 May 2015.Author Darren Cattell
3
4 RECOMMENDATIONS
The below actions are recommended:
1. Escalate level of risk in relation to efficiency delivery with Executive led response to reduce gap, improve delivery and current forecast.
2. Divisions to commence pay controls as part of controls focus of SIEP planning.3. Release reserves to fund Q1 Enhanced Bank Rate costs pending further review the
decision regarding enhanced nurse bank rates.4. Finalise demand and capacity decisions to release reserves into Operational Budgets.
Darren CattellInterim Director of Finance & PerformanceApril 2015Heart of England NHS Foundation Trust
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.99
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
1. A&E Activity 2015/16
In-Month Performance
• There were 21,507 A&E attendances in Apr-15, 836 attendances, 4% above Apr-14.
• In April 86.25% of patients were seen within 4 hours excluding walk ins.
• At Heartlands 86.45% (1,438 breaches) of patients within 4 hours, 80.23% (1,443 breaches) at Good Hope site and 97.82% (79 breaches) at Solihull site.
• A&E activity excludes A&E outpatient attendances.• Form TF2A
2. Emergency Activity 2015/16 excluding Paediatrics, Paediatric Surgery and Obstetrics
In-Month Performance
• The Emergency activity was below April 2014 by 4%, 181 Spells.
• Heartlands 61, 2%, Good Hope, 112, 11% and Women & Children, 37, 11% were below Apr-14.
• Clinical Support 7, 15% and Solihull, 22, 4% were above Apr-14.
• Following the implementation of PMS2 a potential patient classification issue was identified. This remains under ongoing review and any necessary retrospective realignment will be actioned if applicable.
• Form TF2A
3. Emergency Activity 2015/16, Paediatrics, Paediatric Surgery and Obstetrics
In-Month Performance
• The activity is above Apr-14 by 3%, 24 Spells in Apr-15.
• Following the implementation of PMS2 a potential patient classification issue was identified. This remains under ongoing review and any necessary retrospective realignment will be actioned if applicable.
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.100
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
4. AMU, MAU & SAU Activity 2015/16
In-Month Performance
• There were 2,225 spells during Apr-15, 28 Spells, 1% above Apr-14.
• Good Hope Hospital 38 spells, 6%, Heartlands Hospital, 57, 7% were above April-14 outturn.
• Solihull Hospital was below Apr-14 by 68 Spells, 9%.
5. Maternity Spells Activity 2015/16
In-Month Performance
• In April 2015, there were 842 Births Trustwide (532 at Heartlands, 295 at Good Hope, and 15 at Solihull). This compares to 854 in April 2014 (-1%). In April there were 8 planned homebirth (4 at Good Hope, 2 at Heartlands and 2 at Solihull).
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.101
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
ACTIVITY / WAITING LIST PERFORMANCE
6. Elective & Day Case Activity 2015/16
In-Month Performance
• There were 6,458 Day case and Elective spells during Apr-15, this was 5%, 373 Spells below Apr-14 outturn.
• Heartlands, 9%, 354 Spells, Women and Childrens, 22%, 91 Spells were below Apr-14 in month.
• Solihull Division, 1%, 11 Spells, Clinical Support, 27 Spells, 18% and Good Hope, 34 Spells, 5% were above Apr-14 in month.
• Following the implementation of PMS2 a potential patient classification issue was identified. This remains under ongoing review and any necessary retrospective realignment will be actioned if applicable.
• There were 26 sessions cancelled during Apr-15, 96.96% of the scheduled sessions were utilised. The following specialties cancelled sessions, General Surgery (17), Gynaecology (4), Orthopaedics (2), Thoracic Surgery (2) and Urology (1).
• 92% (24) of the Theatre sessions were cancelled due to no surgeon in month.
• In addition to this, 22 sessions were cancelled in the Vanguard Theartre during April, 59% of the scheduled lists were utilisted.
• 90 patients were treated in the Vanguard Theatre during April.
• There were 202 patients treated by the private sector during April. Ophthalmology (54), General Surgery (48), Orthopaedics (25), ENT (22), Urology (19), Gastroenterology (18), Gynaecology (14), Vascular Surgery (2) had patients treated by the private sector in month.
• There were 75 hospital led cancelled operations on the day during April-15. 38 (51%) of the cancelled operations were at Good Hope, 21 (28%) at Heartlands and 16 (21%) at Solihull.
7. Outpatient Activity 2015/16
In-Month Performance
• There were 68,391 Outpatient attendances during Apr-15, 1,639 atts, 2% additional attendances than Apr-14.
• Clinical Support Services, 505 atts, 11%, Good Hope, 436 atts, 6%, Heartlands 119 atts and Solihull, 708 atts, 3% were above Apr-14 outturn.
• Women & Childrens, 129 atts were below Apr-14 outturn.
Total DNA Rates (Apr-15):
• Good Hope Hospital 8.17% (2,381*) • Heartlands Hospital 12.62% (4,379*) • Solihull Hospital 8.70% (2,038*)
The DNA rate for first attendances was 12.91% (1,438*) at Heartlands site during Apr-15. Good Hope (7.52%) and Solihull (7.90%) achieved the target of less than 11%.*No. of DNAs.
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.102
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
• The overall I&E deficit was £2.7m at the end of month 1.
• The Monitor plan has not yet been set and we expect to be reporting against this in month 2.
• Continuity of Service Rating (COSR) is estimated at 3 (2.5 rounded up) at this early stage of the financial year. The Trust has the lowest score on the capital service cover measure due to recording a negative EBITDA in month 1.
In-month Performance
8. Performance against Monitor Standards 2015/16
NHS Contract Income (Category A)
For the month of April there was trust wide clinical income of £49.7m.
There is no graph showing an analysis of over performance as LDPs have not yet been finalized with commissioners.
In-month Performance
9. Income 2015/16
• The Trust is (£4.2m) over spent at Month 1 of 2015/16. • Pay is over spent by (£2.1m) • Non Pay is over spent by (£3.3m) • Other Operating Revenue £1.2m over recovered • Form TF1
In-Month Performance
10. Income and Expenditure against Operational Budgets
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.103
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
In-month Performance
11. Operational Budgets 2015/16
Corporate Directorates (CD) is under spent by £0m
Income over recovery £0m
Pay under spend £0.1m
Non Pay over spend (£0m)
Corporate Trust Wide (CTW) is under spent by £3.3m
Income over recovery £1.2m
Pay over spend (£0m)
Non Pay under spend £2.1m
Facilities (FAC) is over spent by (£0.1m)
Income under recovery (£0m)
Pay under spend £0.1m
Non Pay over spend (£0.1m)
Bad Debt provision included within the above: £0.1m
Heartlands Hospital (BHH) is over spent by (£3.8m)
Income under recovery (£0.1m)
Pay over spend (£1.2m)
Non Pay over spend (£2.5m)
Clinical Support Services (CSS) is over spent by (£0.5m)
Income under recovery (£0m)
Pay under spend £0.1m
Non Pay over spend (£0.6m)
Good Hope Hospital (GHH) is over spent by (£1.5m)
Income under recovery (£0m)
Pay over spend (£0.8m)
Non Pay over spend (£0.7m)
Solihull Hospital (SOL) is over spent by (£1.1m)
Income under recovery (£0m)
Pay over spend (£0.3m)
Non Pay over spend (£0.7m)
Womens and Childrens (WC) is over spent by (£0.6m)
Income over recovery £0.1m
Pay under spend £0m
Non Pay over spend (£0.7m)
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.104
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Pay Expenditure is over spent by (£2.1m) at Month 1 2015/16.
Material variances to operational budget relates to:
• Medical Staffing, which is over spent by (£1.1m) , • Nursing & Midwifery overspent by (£0.9m). • Professional Bank and Agency (£0.1m) • Agency other (£0.2m)
• Form TF3
In-month Performance
12. Pay Expenditure
INCOME AND EXPENDITURE
Non Pay is over spent by (£3.3m) at Month 1 of 2015/16.
Material overspends against operational budgets are:• Prior and current year SIEP (£3.2m) • Clinical Supplies (£0.8m)
Form TF4
In-month Performance
13. Non pay Expenditure
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.105
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
INCOME AND EXPENDITURE
• The Trust achieved £0.4m (20.9%) efficiency in Month 1. • These results show a (£1.6m) shortfall against target at Month 1.
Based on Month 1 results the year end out turn is £12.7m delivery of savings (53%).
Analysis of Forecast:
• £1.4m in risk category 5 Delivered • £2.0m in risk category 4 Expected Delivery. • £9.3m in risk category 3 Suggested Plans.
Divisions have to date completed 68 Quality Impact Assessments for 2015/16. A further 209 are in progress.
Apr - In Month Year To Date Forecast @ Month 1
GROUPS Target ActualRec
ActualNon Rec
Variance Target ActualRec
ActualNon Rec
Variance AnnualTarget
Actual(3,4,5)
Variance(0,1,2)
heartlands hospital 623.8 93.4 11.0 (519.3) 623.8 93.4 11.0 (519.3) 7,485.0 2,917.3 (4,567.7)
good hope hospital 183.3 31.7 0.6 (151.1) 183.3 31.7 0.6 (151.1) 2,200.0 935.4 (1,264.6)
solihull 289.8 41.6 29.1 (219.1) 289.8 41.6 29.1 (219.1) 3,477.5 2,048.5 (1,429.0)
clinical support services 436.5 4.9 43.9 (387.6) 436.5 4.9 43.9 (387.6) 5,237.5 3,520.6 (1,716.9)
womens & childrens 225.0 3.1 0.0 (221.9) 225.0 3.1 0.0 (221.9) 2,700.0 672.6 (2,027.4)
facilities 116.7 94.3 0.0 (22.3) 116.7 94.3 0.0 (22.3) 1,400.0 1,200.8 (199.3)
corporate directorates 125.0 65.3 0.0 (59.7) 125.0 65.3 0.0 (59.7) 1,500.0 703.4 (796.6)
corporate trustwide 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 760.0 760.0
TOTAL 2,000.0 334.4 84.6 (1,581.0) 2,000.0 334.4 84.6 (1,581.0) 24,000.0 12,758.6 (11,241.5)
In-month Performance
14. Service Improvement Efficiency Plan 2015/16
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.106
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
BALANCE SHEET
Expenditure YTD to month 1 was £975k, 45.2% of the YTD Monitor Plan (MP) and 1.9% of total Approved Budget (AB) £50.6m. Orders raised were £9.1m, 422.6% of YTD MP & 18.0% of AB.
• Other was £442k, 45.3% of MP; with spend various estates projects
• Operational was £357k, 36.6% of MP, key spends on SAN, Windows 7 Compliance project, Ultrasound Machine, LAN
• Site Strategy Investment expenditure was £176k, 18.0% of MP, spend on Dermatology relocation, Endoscopy BHH
YTD Performance
15. Combined Capital Expenditure YTD 2015/16
M1 In-month expenditure was £975k:
• FAC / Site Strategy £509k- Various estates projects • CD £346k- SAN, Document Scanning, Windows 7
Compliance project, LAN • BHH £75k- Ultrasound Machine, Profiling Beds, ECG• SOL £36k- Day Room upgrade, 2 Flexible
Nasendoscope• WC £9k- Ambulatory Blood Pressure Monitors,
Capacity Risks project for Obstetrics at BHH• CSS £1k- Histopathology Archive Provision, BHH
Mortuary Fridge refurbishment
In-month Performance
16. Capital Expenditure in Month 2015/16
• Payment performance in April is about 69%. The volume of invoices paid in April is 15,818. This is a little higher than normal volumes and around 5,400 invoices higher than April 2014.
• The continued poor payment performance is due to backlog clearing and processing delays following the Readsoft upgrades and will also impact on performance into month 2 and 3.
• A special project team is being set up to tackle the backlog of old year invoices and from next month we should be able to report project and business as usual performance separately.
Cumulative Performance
17. Creditors 2015/16
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.107
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
BALANCE SHEET
• Total debt reduced by £2.043m during April to £22.360m.
• NHS England paid several large value invoices in the month, including £0.684m for public health, £0.393m for cancer drugs recharges and £0.361m for clinical excellence awards
• Health Education England paid a training & education invoice for £0.577m during April
• A high volume of smaller value invoices issued during March to both NHS and Non NHS customers were also paid during April
• There are still underpayments of £2.372m against the 2014-15 SLA mandate invoices, including £0.944m by Solihull Clinical Commissioning Group and £1.349m by Birmingham Cross City Clinical Commissioning Group, who have also underpaid the April 2015 SLA mandate invoice by £0.505m, although this was for an estimated value only.
• There are four April 2015 SLA mandate invoices totalling £0.966m still outstanding with NHS England. These were issued late in the month and are expected to be paid shortly
• Ante natal maternity pathways activity debt for April 2013 to March 2015 increased slightly to £3.724m , including £1.957m with Burton Hospitals, £0.617m with Sandwell & West Birmingham Hospitals, and £0.643m with Birmingham Womens Hospital.
• A specialised services over-performance invoice for £3.145m issued to NHS England in March remains outstanding, as does an RTT funding invoice for £1.100m to Solihull Commissioning Group
In-month Performance
18. Debtors 2015/16
CASHFLOW
• The cash balance at the end of April 2015 was £84.0m. • The Monitor plan has not yet been set and we expect
to report against this in month 2. • All Trust funds remain in the GBS umbrella as a
change in the rules on calculating PDC dividend means that it is currently financially unviable to invest in other commercial banks.
• £65m was held on short term NLF deposits at the month end attracting rates of about 40bp.
• Funds in GBS attract 25bp.
In-month Performance
19. Monthly Closing Cash Balance vs Plan 2015/16
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.108
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
N.Atkins PM-P&I 21/05/2015 Z:\Data\PMU\Performance Monitoring\KPI 2015-16\2015-16 Trust KPI.xlsbFC 1
18 weeks: Reported 1 month in arrears
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
HEFT have now resumed reported against the Admitted patient pathway (clock stops), and achieved 82.09% against the 90% target for Apr15, with the aim to ontinue to see
longer waits in order to help clear the backlog
HEFT managed to see 91.02% of non-admitted patients within 18 weeks against the 95% target for Apr15
Admitted Non-admitted
75%
80%
85%
90%
95%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
85%
87%
89%
91%
93%
95%
97%
99%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
HEFT have now resumed reported against the Incomplete pathways, and achieved 89.61% against the 92% target for Apr15
Incomplete Pathways
85%
87%
89%
91%
93%
95%
97%
99%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
Total time in A&E
70%
75%
80%
85%
90%
95%
100%Target
The 95% target for A&E around 4 hour was not met in April with performance at 86.25%
A&E
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.109
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
N.Atkins PM-P&I 21/05/2015 Z:\Data\PMU\Performance Monitoring\KPI 2015-16\2015-16 Trust KPI.xlsbFC 1
Cancers: Reported 1 month in arrears
Cancers: (continued)
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
50%55%60%65%70%75%80%85%90%95%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
2 week GP 2 week Breast Target
The Trust failed the 93% target for the 2 week GP cancer indicator in March at 90.96%, and also failed the 2 week Breast symptom 93% target, achieving 88.41%.
The Trust achieved the 96% target for 31 day cancers in March, out-turning at 98.48% in month. March data is unvalidated.
2 weeks 31 day GP
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
The Trust met the 31 day anti-cancer drug target of 98% in March, achieving 100%.
The Trust met the 31 day surgery modality cancer target of 94% in March, achieving 96.97%.
31 day anti-cancer 31 day surgery
90%
91%
92%
93%
94%
95%
96%
97%
98%
99%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
85%
87%
89%
91%
93%
95%
97%
99%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
The Trust achieved the 62 day cancer 85% target in March, achieving 84.40%.
The Trust missed the 62 day national screening cancer 90% target in March, achieving 62.50%. March data is unvalidated.
62 day cancers 62 day screening
75%
80%
85%
90%
95%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
40%
50%
60%
70%
80%
90%
100%
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Target
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.110
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
N.Atkins PM-P&I 21/05/2015 Z:\Data\PMU\Performance Monitoring\KPI 2015-16\2015-16 Trust KPI.xlsbFC 1
Infection Control
MONITOR - RISK ASSESSMENT FRAMEWORK KPIs
c-diff
In month the Trust reported 2 cases of C-diff, with a total of 2 YTD
0
2
4
6
8
10
12
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
May
-15
Jun-
15
Jul-1
5
Aug-
15
Sep-
15
Oct
-15
Nov
-15
Dec-
15
Jan-
16
Feb-
16
Mar
-16
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.111
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Year to Date
AnnualPlan
Actual
Full Year
VarianceActual to
Plan
AnnualPlan
Forecast
£m £m £m £m £m
VarianceForecast to
Plan
£m
2014/15
£m
0.000 49.677 49.677 NHS Clinical Revenue 0.000 0.000 0.000 577.495
0.000 0.046 0.046 Clinical Revenue - Private Patients 0.000 0.000 0.000 0.589
0.000 0.011 0.011 Clinical Revenue - Overseas Visitors 0.000 0.000 0.000 0.161
0.000 0.436 0.436 Research and Development revenue 0.000 0.000 0.000 4.190
0.000 1.969 1.969 Education and Training revenue 0.000 0.000 0.000 22.841
0.000 0.037 0.037 PFI Specific Revenue 0.000 0.000 0.000 0.448
0.000 0.000 0.000 Donations and Grants received 0.000 0.000 0.000 0.501
0.000 0.346 0.346 Parking Revenue 0.000 0.000 0.000 4.781
0.000 0.097 0.097 Catering Revenue 0.000 0.000 0.000 1.014
0.000 0.027 0.027 Accommodation Revenue 0.000 0.000 0.000 0.278
0.000 1.546 1.546 Revenue from non patient services to other bodies
0.000 0.000 0.000 10.480
0.000 1.613 1.613 Miscellaneous other operating revenue 0.000 0.000 0.000 24.080
0.000 55.804 55.804 Total Operating Revenue 0.000 0.000 0.000 646.860
0.000 (32.939) (32.939) Employee expenses, permanent staff 0.000 0.000 0.000 (386.163)
0.000 (3.004) (3.004) Employee expenses, agency and contract staff 0.000 0.000 0.000 (25.630)
0.000 (5.500) (5.500) Drugs 0.000 0.000 0.000 (58.544)
0.000 (5.534) (5.534) Clinical Supplies 0.000 0.000 0.000 (62.776)
0.000 (1.473) (1.473) Non Clinical Supplies 0.000 0.000 0.000 (16.608)
0.000 (0.302) (0.302) Research and Development Expense 0.000 0.000 0.000 (2.709)
0.000 (0.205) (0.205) Education and Training Expense 0.000 0.000 0.000 (2.411)
0.000 (2.489) (2.489) Premises 0.000 0.000 0.000 (29.218)
0.000 (1.279) (1.279) CNST 0.000 0.000 0.000 (12.795)
0.000 (1.061) (1.061) Purchase of healthcare services non NHS 0.000 0.000 0.000 (9.228)
0.000 (0.659) (0.659) Purchase of healthcare services NHS 0.000 0.000 0.000 (7.352)
0.000 (0.279) (0.279) Consultancy Expense 0.000 0.000 0.000 (1.833)
0.000 (1.714) (1.714) Miscellaneous other Operating expense 0.000 0.000 0.000 (13.103)
0.000 (0.067) (0.067) (Increase)/decrease in impairment of receivables
0.000 0.000 0.000 0.029
0.000 (0.008) (0.008) PFI unitary payment 0.000 0.000 0.000 (0.095)
0.000 (56.513) (56.513) Total Operating Expenses 0.000 0.000 0.000 (628.434)
0.000 (0.709) (0.709) EBITDA 0.000 0.000 0.000 18.427
0.000 0.000 0.000 Gain / loss on asset disposals 0.000 0.000 0.000 (0.195)
0.000 (1.425) (1.425) Total Depreciation and amortisation 0.000 0.000 0.000 (18.360)
0.000 (0.573) (0.573) PDC Dividend expense 0.000 0.000 0.000 (5.656)
0.000 0.019 0.019 Total interest receivable 0.000 0.000 0.000 0.441
0.000 0.000 0.000 Other finance costs 0.000 0.000 0.000 (0.003)
0.000 (0.020) (0.020) Interest expense 0.000 0.000 0.000 (0.262)
0.000 (2.708) (2.708) Surplus/(deficit) before impairments 0.000 0.000 0.000 (5.608)
0.000 0.000 0.000 Impairment (Losses) / Reversals 0.000 0.000 0.000 0.000
0.000 (2.708) (2.708) Surplus/(deficit) after impairments 0.000 0.000 0.000 (5.608)
Key perfomance Indicators (KPIs)Year to Date
AnnualPlan
Actual
Full Year
VarianceActual to
Plan
AnnualPlan
Forecast VarianceForecast to
Plan
2014/15
NaN (4.85%) NaN Net I&E Margin NaN NaN NaN (0.84%)
0.000 (0.709) (0.709) EBITDA (£m) adjusted 0.000 0.000 0.000 17.925
NaN -Infinity NaN EBITDA achieved, % of projection NaN NaN NaN 63.69%
NaN (1.27%) NaN EBITDA margin (%) NaN NaN NaN 2.77%
0.000 (0.689) (0.689) Revenue available for debt service (£m) 0.000 0.000 0.000 18.366
Trust Wide Income and Expenditure Form TF1AApril 2015
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.112
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Year to Date
Last Month Actual
This Month Actual
Full Year
Variance to Plan
Annual Plan Forecast
£m £m £m £m £m
Variance from Plan
£m
31 March 2015
£m
3.553 3.655 3.655 Intangible Assets, Net 0.000 0.000 0.000 3.553242.015 241.468 241.468 Property, Plant and Equipment, Net 0.000 0.000 0.000 242.015
4.206 4.196 4.196 On balance sheet PFI assets 0.000 0.000 0.000 4.206249.775 249.319 249.319 Fixed Assets, net 0.000 0.000 0.000 249.775
2.592 2.534 2.534 Trade Receivables, non current, gross 0.000 0.000 0.000 2.592
(1.461) (1.461) (1.461) Impairment of receivables for bad and doubtful debts, non current 0.000 0.000 0.000 (1.461)
1.131 1.072 1.072 Trade and other receivables, net, non current 0.000 0.000 0.000 1.131250.906 250.391 250.391 ASSETS, NON CURRENT 0.000 0.000 0.000 250.906
8.491 8.634 8.634 Inventories 0.000 0.000 0.000 8.49123.658 28.360 28.360 NHS Trade Receivables, current, gross 0.000 0.000 0.000 23.6585.627 4.582 4.582 Non NHS Trade Receivables, current, gross 0.000 0.000 0.000 5.6270.244 0.244 0.244 Other Related Party Receivables 0.000 0.000 0.000 0.2442.377 1.533 1.533 Other Receivables 0.000 0.000 0.000 2.377
(8.396) (8.456) (8.456) Impairment of receivables for bad and doubtful debts, current 0.000 0.000 0.000 (8.396)
2.465 2.539 2.539 Accrued Income 0.000 0.000 0.000 2.4656.075 10.841 10.841 Prepayments 0.000 0.000 0.000 6.075
87.671 84.019 84.019 Cash and Cash Equivalants 0.000 0.000 0.000 87.671128.212 132.295 132.295 CURRENT ASSETS 0.000 0.000 0.000 128.212
379.118 382.687 382.687 TOTAL ASSETS 0.000 0.000 0.000 379.118
(6.655) (8.272) 8.272 Trade Payables 0.000 0.000 0.000 (6.655)(14.700) (15.149) 15.149 Other Payables 0.000 0.000 0.000 (14.700)(5.684) (3.179) 3.179 Capital Payables 0.000 0.000 0.000 (5.684)
(46.638) (52.778) 52.778 Accruals 0.000 0.000 0.000 (46.638)(0.480) (0.480) 0.480 Finance Leases / PFI Leases, Current 0.000 0.000 0.000 (0.480)0.000 (0.573) 0.573 PDC Dividend Payable 0.000 0.000 0.000 0.000
(8.748) (8.066) 8.066 Provisions, current 0.000 0.000 0.000 (8.748)(6.501) (6.430) 6.430 Deferred Income 0.000 0.000 0.000 (6.501)
(89.405) (94.926) 94.926 CURRENT LIABILITIES 0.000 0.000 0.000 (89.405)
38.807 37.370 37.370 NET CURRENT ASSETS (LIABILITIES) 0.000 0.000 0.000 38.807
(6.747) (7.531) 7.531 Provisions, non current 0.000 0.000 0.000 (6.747)(1.609) (1.598) 1.598 Finance Leases, non current 0.000 0.000 0.000 (1.609)(2.377) (2.360) 2.360 PFI Leases, non current 0.000 0.000 0.000 (2.377)
(10.733) (11.489) 11.489 LIABILITIES, NON CURRENT 0.000 0.000 0.000 (10.733)
278.980 276.272 276.272 TOTAL ASSETS EMPLOYED 0.000 0.000 0.000 278.980
215.309 215.309 215.309 Public Dividend Capital 0.000 0.000 0.000 215.30919.432 16.724 16.724 Retained Earnings / (Accumulated Losses) 0.000 0.000 0.000 19.43244.408 44.408 44.408 Revaluation Reserve 0.000 0.000 0.000 44.408(0.169) (0.169) (0.169) Miscellaneous Other Reserves 0.000 0.000 0.000 (0.169)278.980 276.272 276.272 TOTAL TAXPAYERS EQUITY 0.000 0.000 0.000 278.980
Infinity 11.84% Net Return After Financing NaN NaN NaN -19.08 %
Year to Date
Last Month Actual
This Month Actual
Full Year
Variance to Plan
Annual Plan Forecast Variance from Plan
31 March 2015
0.000 16.896 Liquidity NaN NaN NaN 19.154
Key perfomance Indicators (KPIs)
Form TF1BTrust Wide Balance SheetApril 2015
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.113
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Trust Wide Cash flow
Actual Plan Variance to Plan Annual Plan Forecast Variance from Plan 2014/15
(2.708) (2.708) Surplus / (Deficit) after tax - (5.608) Non - cash flows in operating surplus / (deficit): -
0.001 0.001 Finance income/charges - (0.176) - Donations and grants received of PPE and intangibles - (0.501) - Other operating non-cash movements -
1.425 1.425 Depreciation and amortisation, total - 18.360 - Impairment losses / (reversals) - - (Gain) / loss on disposal of non current assets - 0.195
0.573 0.573 PDC Dividend Expense - 5.656 0.067 0.067 Other - (0.029)
(0.642) - (0.642) Operating Cash Flows before movements in WC - - - 17.897 Increase / (decrease) in working capital:
(0.143) (0.143) (Increase)/decrease in inventories - (0.495) - (Increase)/decrease in tax receivable -
(4.702) (4.702) (Increase)/decrease in NHS Trade Receivables - (2.042) 1.045 1.045 (Increase)/decrease in Non NHS Trade Receivables - (0.733)
- - (Increase)/decrease in other related party receivables - (0.244) 0.844 0.844 (Increase)/decrease in other receivables - 0.398
(0.074) (0.074) (Increase)/decrease in accrued income - (0.470) - (Increase)/decrease in other financial assets -
(4.766) (4.766) (Increase)/decrease in prepayments - (0.942) - (Increase)/decrease in Other assets (non chartable assets) -
(0.071) (0.071) Increase/(decrease) in Deferred Income (excl. Govt Grants.) - (0.104) - Increase/(decrease) in Deferred Income (Govt. Grants) -
(0.682) (0.682) Increase/(decrease) in Current provisions - (5.173) - Increase/(decrease) in post-employment benefit obligations - - Increase/(decrease) in tax payable -
1.617 1.617 Increase/(decrease) in Trade Creditors - 4.156 0.449 0.449 Increase/(decrease) in Other Creditors - 12.645 6.140 6.140 Increase/(decrease) in accruals - (1.237)
- Increase/(decrease) in other Financial liabilities - - - Increase/(decrease) in Other liabilities (non charitable assets) - -
(0.343) - (0.343) Increase / (decrease) in working capital, Total - - - 5.759 0.784 - 0.784 Increase/(Decrease) in Non-current Provisions - -
(0.201) - (0.201) Net cash inflow/(outflow) from operating activities - - - 23.656 Net cash inflow/(outflow) from investing activities:
(0.915) (0.915) Property - new land, buildings or dwellings - (7.560) - Property - maintenance expenditure - (1.333) - Plant and equipment - Information Technology - (3.616) - Plant and equipment - Other - (5.857) - Property, plant and equipment - other expenditure - - Proceeds on disposal of property, plant and equipment - - Purchase of investment property - - Proceeds on disposal of investment property - - Purchase of intangible assets - (2.169) - Proceeds on disposal of intangible assets - - Expenditure on capitalised development -
(2.505) (2.505) Increase/(decrease) in Capital Creditors - 1.548 - Government grants received - - Purchase of investments & deposits made - - - Proceeds on disposal of investments & withdrawals - - - Other cash flows from investing activities - -
(3.420) - (3.420) Net cash inflow/(outflow() from investing activities, Total - - - (18.987)
(3.621) - (3.621) Net cash inflow/(outflow) before financing - - - 4.669 Net cash inflow/(outflow) from financing activities:
- Public Dividend Capital received - 1.140 - Public Dividend Capital repaid - - PDC Dividends paid - (4.851) - Finance leases -
(0.012) (0.012) Interest element of finance lease rental payments - other - (0.139) (0.013) (0.013) Interest element of finance lease rental payments - On-balance sheet PFI - (0.151) (0.010) (0.010) Capital element of finance lease rental payments - other - (0.118) (0.016) (0.016) Capital element of finance lease rental payments - On-balance sheet PFI - (0.197) 0.019 0.019 Interest received on cash and cash equivalents - 0.441
- Movement in Other grants/Capital received - - Donations received in cash - - (Increase)/decrease in non-current receivables - 0.179 - Increase/(decrease) in non-current payables - - Other cash flows from financing activities -
(0.031) - (0.031) Net cash inflow/(outflow) from financing activities, Total - - - (3.696)
(3.652) - (3.652) Net increase / (decrease) in cash - - - 0.973
87.671 86.321 0.377 Opening cash balance 87.671 87.671 - 86.698 (3.652) - (3.652) Net increase / (decrease) in cash - - - 0.973 84.019 86.321 (3.275) Closing cash balance 87.671 87.671 - 87.671
Form TF1C
Year to Date
April 2015
Full Year
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.114
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
April 2015
Year to DateMetric Actual Rating Weight 4 3 2 1
Capital Service Cover -1.11 1 50.0% 2.50 1.75 1.25 <1.25Liquidity 16.90 4 50.0% 0 -7.0 -14.0 <-14.0
Weighted Average 2.50 100.0%
Monitor Continuity of Service Ratings (COSR) Form TF1D
COSR:
Finance Executive Summary and Key Performance Indicators

Council of GovernorsJune 2015
.115
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Safe
ty S
itRep
– A
pril
2015
1
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.116
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
April
201
5
Saf
ety
S
ituat
ion
Rep
ort
Stat
us
Stra
tegi
c ris
ks (U
pdat
ed A
pril
15)
•Reg
ular
repo
rts p
rovi
ded
to B
oard
and
EM
B to
disc
uss S
trat
egic
Risk
s.
Red
(≥ 1
5) o
pera
tiona
l ris
ks.
•The
re a
re e
leve
n op
erat
iona
l red
risk
s cur
rent
ly o
pen.
Sev
en h
ave
been
val
idat
ed in
201
4/15
and
fo
ur re
mai
n op
en fr
om 2
013/
14
• One
new
red
risk
(Mar
ch 2
015)
rela
ting
to lo
ss o
f JAG
acc
redi
tatio
n fo
r End
osco
py u
nits
acr
oss
HEFT
SUIs
and
inci
dent
s •T
here
has
bee
n on
e ne
w S
UI’s
dec
lare
d sin
ce th
e la
st re
port
. Miss
ed d
iagn
osis
of p
neum
otho
rax.
•T
wo
SUI r
epor
ts h
ave
been
clos
ed si
nce
last
repo
rt “
Subo
ptim
al ca
re o
f det
erio
ratin
g pa
tient
“ an
d “M
issed
dia
gnos
is of
pne
umot
hora
x“
Mor
talit
y •T
he T
rust
is st
ill u
nabl
e to
mea
sure
mor
talit
y re
liabl
y us
ing
HSM
R.
•Cru
de m
orta
lity
show
s a p
eak
and
decl
ine
in n
umbe
r of i
npat
ient
em
erge
ncy
deat
hs.
•The
late
st S
umm
ary
Hosp
ital-l
evel
Mor
talit
y In
dica
tor (
SHM
I) sc
ore
for J
ul 1
3 to
Jun
14 is
109
, thi
s is
with
in th
e HS
CIC
‘as e
xpec
ted’
ban
ding
.
IMR
(Dec
embe
r 201
4)
•Cur
rent
ly 9
risk
s and
6 e
leva
ted
risks
hig
hlig
hted
thro
ugh
the
Dece
mbe
r 14
“int
ellig
ent m
onito
ring
repo
rt” (
was
11
and
5 in
dra
ft v
ersio
n iss
ued
in O
ctob
er 1
4)
•Was
9 ri
sks
and
7 el
evat
ed ri
sks i
n pr
evio
us (J
une
IMR)
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.117
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Sum
mar
y ris
k pr
ofile
^Dat
e ris
k ra
ted
as re
d (≥
15) a
nd a
gree
d at
Risk
For
um
*Sco
re w
ith m
itiga
tion
in p
lace
: m
itiga
ting
actio
n to
redu
ce th
e ris
k ne
eds t
o ta
ke p
lace
with
in o
ne m
onth
in
orde
r to
redu
ce th
e ris
k to
acc
epta
ble
leve
l (i.e
. Am
ber)
.
•W&
C –
Wom
en's
and
Child
ren'
s Ser
vice
s •C
SS –
Clin
ical
Sup
port
Ser
vice
s
3
RED
OPE
RATI
ON
AL R
ISKS
-Mon
itorin
g by
site
s / d
ivis
ion.
Risk
Sum
mar
y: R
ed
Site
Di
visi
on
Dat
e^
Initi
al
Curr
ent*
Loss
of J
AG A
ccre
dita
tion
acro
ss H
EFT
- NEW
Al
l BH
H M
arch
15
15
15
The
Join
t Adv
isory
Gro
up (J
AG) o
ffer a
vol
unta
ry q
ualit
y ac
cred
itatio
n sy
stem
for e
ndos
copy
uni
ts in
Eng
land
. Alth
ough
it is
a
volu
ntar
y sc
hem
e it
is ac
cept
ed a
s the
serv
ice
stan
dard
. The
re a
re 2
ele
men
ts o
f the
pro
cess
; firs
tly a
site
visi
t eve
ry 5
yea
rs a
nd
seco
ndly
ele
ctro
nic
subm
issio
ns e
very
6 m
onth
s. H
EFT
last
mad
e a
subm
issio
n in
Sep
tem
ber 2
014
and
was
adv
ised
that
, as o
ur
wai
ting
times
exc
eede
d 5
wee
ks,
our a
ccre
dita
tion
was
def
erre
d. A
noth
er su
bmiss
ion
is to
be
mad
e at
the
end
of A
pril
and
shou
ld th
e w
aitin
g tim
es st
ill e
xcee
d 5
wee
ks th
en a
ccre
dita
tion
wou
ld b
e re
mov
ed. B
ased
on
the
curr
ent b
ack
log
with
in
endo
scop
y, w
ith a
pro
ject
ed re
turn
to 5
wee
k di
agno
stic
tim
es n
ot e
xpec
ted
until
Q3
2015
, it i
s hig
hly
unlik
ely
that
acc
redi
t atio
n w
ill b
e gr
ante
d as
this
is a
core
mea
sure
of t
he se
rvic
e. If
we
do n
ot h
old
JAG
accr
edita
tion
then
the
Nat
iona
l bow
el sc
reen
ing
prog
ram
me
will
be
with
draw
n fr
om H
EFT
and
no c
onsid
erat
ion
will
be
give
n to
hos
t the
bow
el sc
ope
prog
ram
me.
Staf
fing
the
A&E
Serv
ice
at S
HH
SH
BHH
Feb
15
15
15
Prov
ision
of 2
4 ho
ur A
&E
serv
ice
is de
pend
ent o
n ad
equa
te st
affin
g w
ith a
ppro
pria
te sk
ill m
ix..
Alm
ost a
ll m
edic
al sh
ifts a
t So
lihul
l are
now
cov
ered
by
locu
ms.
Nur
sing -
wise
, rec
eive
d fu
ndin
g fo
r for
an
addi
tiona
l ass
essm
ent n
urse
in re
spon
se to
our
last
CQ
C as
sess
men
t but
una
ble
to re
crui
t. EN
P-w
ise th
e pr
opos
ed ch
ange
s to
the
serv
ice
at S
olih
ull h
ave
crea
ted
anxi
ety
abou
t job
se
curit
y an
d m
any
staf
f are
revi
ewin
g th
eir o
ptio
ns fo
r the
futu
re. E
NPs
are
a h
ighl
y de
sirab
le g
roup
of s
taff
both
for o
ther
EDs
an
d fo
r prim
ary
care
. In
term
s of s
afet
y w
e ar
e un
able
to g
uara
ntee
qua
lity
stan
dard
s aro
und
asse
ssm
ent.
Una
ble
to a
lway
s en
sure
locu
ms h
ave
up to
dat
e tr
aini
ng /
com
pete
ncie
s. T
his i
s com
poun
ded
if th
e nu
rsin
g st
aff /
EN
Ps w
orki
ng w
ith th
em a
re
bank
staf
f and
is se
t with
in a
hos
pita
l site
that
has
litt
le o
n -sit
e ba
ck u
p fo
r unw
ell c
ases
. It i
s bec
omin
g in
crea
singl
y di
fficu
lt to
ob
tain
ade
quat
e nu
mbe
rs o
f sta
ff in
all
grou
ps o
f an
appr
opria
te ca
libre
to p
rovi
de a
safe
qua
lity
serv
ice.
Impl
icat
ions
of S
olih
ull C
CG E
RG p
ropo
sals
Al
l SH
Fe
b 15
16
16
In Ju
ne 2
014
Solih
ull C
CG p
ublis
hed
plan
s dev
elop
ed th
roug
h th
eir E
ffect
iven
ess R
evie
w G
roup
(ERG
). H
EFT
serv
ices
affe
cted
by
the
ERG
prop
osal
s are
: (1)
Non
-ren
ewal
: Virt
ual W
ards
; Hea
rt F
ailu
re; H
ospi
tal L
iaiso
n N
ursin
g; N
utrit
ion
Serv
ice;
Cas
tle P
ract
ice
Diet
etic
s and
Pod
iatr
y; p
lus B
alsa
ll Co
mm
on P
ract
ice
ENT;
(2) A
ctiv
ity th
resh
old:
MSK
; Pod
iatr
y; (3
)Con
trac
t ren
egot
iatio
n:
Diab
etes
; SAL
T (C
hild
ren)
; OT
(Pae
diat
ric).I
t is i
mpo
rtan
t to
high
light
that
the
re a
re im
plic
atio
ns o
f ERG
on
wid
er ca
re p
athw
ays
utili
zed
by p
atie
nts c
ared
for b
y HE
FT.
HEFT
are
cur
rent
ly in
form
al n
egot
iatio
ns re
gard
ing
ERG
prop
osal
s. A
s par
t of t
hese
ne
gotia
tions
info
rmat
ion
rega
rdin
g th
e CC
G im
pact
ass
essm
ent o
f ERG
pro
posa
ls ha
s bee
n re
ques
ted.
Dela
y in
dia
gnos
tic E
ndos
copy
test
s Al
l BH
H O
ct 1
4 15
20
The
endo
scop
y se
rvic
e is
not m
eetin
g re
quire
d tim
esca
les f
or d
iagn
ostic
end
osco
py te
stin
g of
out
-pat
ient
(2 w
eek
wai
t en
dosc
opy
requ
ests
, urg
ent r
eque
sts)
and
in-p
atie
nt re
ques
ts (e
spec
ially
upp
er G
I ble
ed w
hich
shou
ld b
e co
mpl
eted
with
in 2
4 ho
urs)
. GP
two
wee
k w
ait c
ance
r pro
form
a re
ques
ts a
re b
eing
com
plet
ed w
ithin
tim
efra
mes
. Urg
ent e
ndos
copy
requ
ests
cu
rren
tly w
ithin
4 -6
wee
ks (s
houl
d be
2).
Upd
ate:
A fu
rthe
r 600
pat
ient
s hav
e be
en id
entif
ied
that
wer
e no
t on
the
wai
ting
list
syst
em w
hich
has
incr
ease
d th
e ov
eral
l wai
ting
list t
o 15
80 p
atie
nts.
The
add
ition
al b
ackl
og n
ow m
eans
that
the
num
ber o
f pa
tient
s wai
ting
mor
e th
an 1
8 w
eeks
stan
ds a
t 195
with
pro
ject
ed re
turn
to 5
wee
k di
agno
stic
tim
e no
t exp
ecte
d un
til Q
3 20
15/1
6. T
here
hav
e be
en a
n in
crea
sing
num
ber o
f clin
ical
ly si
gnifi
cant
cas
es w
ith d
elay
ed d
iagn
osis.
STRA
TEGI
C RI
SKS-
Mon
itorin
g by
EM
B,
QRC
& T
B (a
s at A
pril
15)
Sum
mar
y &
scor
e
Futu
re fi
nanc
ial r
isk
(↔ 1
6)
Patie
nt fl
ow
(↔ 1
6)
Abili
ty o
f the
Tru
st to
un
dert
ake
stra
tegi
c co
nfig
urat
ion
(↔
12)
Staf
f Mor
ale
(↔
16)
18 W
eeks
(↔
12)
Brea
st R
ecal
l (↔
12)
Mor
talit
y (↔
12)
Enfo
rcem
ent A
ctio
n
(↔ 1
6)
PMS2
(↔
20)
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.118
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Rem
aini
ng R
ed R
isks
from
201
3/14
Impl
emen
tatio
n of
IT sy
stem
for S
exua
l Hea
lth –
Lill
ie
BHH
CSSD
M
ar14
16
16
Pote
ntia
l los
s of v
ascu
lar s
ervi
ce (i
f una
ble
to p
rovi
de h
ybrid
th
eatr
e an
d lo
ss o
f com
miss
ioni
ng o
f the
se se
rvic
es)
Hybr
id th
eatr
e bu
ild n
ow u
nder
way
– ri
sk re
mai
ns a
t 16.
BHH
BHH
Mar
14
16
16
Impa
ct o
f ext
ende
d st
ay in
ED.
Re
view
ed Ja
n 20
15 –
risk
upg
rade
d to
20
GHH
BHH
BHH
Jan1
4 15
20
Chem
othe
rapy
pre
scrib
ing
/ adm
inist
ratio
n in
abs
ence
of E
P BH
H BH
H O
ct13
15
15
4
RED
OPE
RATI
ON
AL R
ISKS
-Mon
itorin
g by
site
s / d
ivis
ion.
Risk
Sum
mar
y: R
ed
Site
Di
visi
on
Dat
e^
Initi
al^
Curr
ent *
Sexu
al H
ealth
IT sy
stem
una
ble
to m
eet s
tatu
tory
repo
rtin
g BH
H CS
S Ju
l14
6 16
The
Tele
care
syst
em cu
rren
tly u
sed
to re
cord
att
enda
nce
and
drug
trea
tmen
t is u
nabl
e to
mee
t man
dato
ry d
ata
requ
irem
ents
for P
ublic
Hea
lth E
ngla
nd,
HIV
and
AIDS
Rep
ortin
g Sy
stem
(HAR
S). A
s wel
l as t
he re
puta
tiona
l im
pact
this
may
hav
e on
com
miss
ioni
ng d
ecisi
ons,
orga
nisa
tiona
l non
com
plia
nce
may
re
sult
in a
10%
fine
(equ
ates
to a
ppro
xim
atel
y £4
00k
for 1
4/15
cont
ract
val
ue).
The
depa
rtm
ent o
pted
to
impl
emen
t a n
ew (H
ARS
com
plia
nt) I
T sy
stem
. Cl
imat
e–HI
V bu
t tec
hnic
al d
iffic
ultie
s in
the
IT sy
stem
s / in
terf
aces
with
oth
er T
rust
syst
ems m
eans
that
they
rem
ain
unab
le to
com
ply
with
thes
e st
atut
ory
repo
rtin
g re
quire
men
ts. U
pdat
e: P
redi
cted
“Go
live”
dat
e is
Mar
ch 2
015.
Risk
scor
e to
be
revi
ewed
.
Impa
ct o
f una
ccep
tabl
e de
lay
for b
ackl
og o
f cas
es re
quiri
ng
com
plex
end
ovas
cula
r ane
urys
m re
pair
(EVA
R)
BHH
BHH
July
14
15
16
The
deat
h of
a p
atie
nt fr
om a
rupt
ured
thor
acic
ane
urys
m w
hilst
wai
ting
for a
dat
e fo
r tre
atm
ent a
t HEF
T id
entif
ied
a p
oten
tial 9
2 pa
tient
s on
the
EVAR
pat
hway
with
out a
n op
erat
ion
date
who
wer
e no
t rec
orde
d as
par
t of t
he H
EFT
wai
ting
list.
Follo
win
g va
lidat
ion
the
back
log
is 41
pa
tient
s who
are
cur
rent
ly li
sted
for s
urge
ry (w
ith a
noth
er p
oten
tial 2
4 pa
tient
s who
may
filte
r int
o th
e sy
stem
as t
he d
ecis
ion
is ta
ken
to
trea
t). T
he o
ldes
t cas
e is
38 w
eeks
from
dec
ision
to a
dmit.
38
addi
tiona
l list
s are
requ
ired
to a
ddre
ss th
e ba
cklo
g. U
pdat
e: P
lan
to c
lear
ba
cklo
g by
end
of M
arch
15
is on
trac
k, so
me
dela
ys in
rece
ivin
g co
mpl
ex g
raft
s but
neg
otia
tion
is on
goin
g to
exp
edite
this.
Emer
genc
y Re
scue
from
Lift
s at B
HH a
nd R
SU
BHH/
GHH
Corp
Au
g 14
16
16
In th
e ev
ent o
f a li
ft fa
iling
and
pas
seng
ers b
eing
trap
ped,
est
ates
staf
f are
trai
ned
annu
ally
to h
and
win
d th
e lif
t to
the
next
floo
r. Th
is ye
ar th
e tr
aine
r de
emed
it u
nsaf
e to
und
erta
ke th
is ta
sk/p
rovi
de tr
aini
ng fo
r the
lift
s in
the
mai
n w
ard
bloc
k at
BHH
and
RSU
at G
HH (d
ue to
the
load
ing
and
effo
rt re
quire
d to
han
d w
ind
the
lift).
The
lift
s in
mai
n w
ard
bloc
k (B
HH) f
ail a
ppro
xim
atel
y 1/
mon
th a
nd th
e lif
ts in
RSU
app
roxi
mat
ely
2/m
onth
. The
refo
re e
stat
es st
aff
will
hav
e to
per
form
this
task
, des
pite
thei
r tra
inin
g ha
ving
exp
ired.
A sa
fe sy
stem
of w
ork
for t
he re
leas
e of
pas
seng
ers f
rom
thes
e lif
ts is
bei
ng d
evel
oped
as
an
inte
rim m
easu
re
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.119
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Mor
talit
y | H
eadl
ines
•
The
con
firm
ed r
ebas
ed 2
013/
14 H
SM
R is
107
.9,
whi
ch is
an
outli
er fo
r th
at y
ear
•D
ue to
issu
es w
ith P
MS
2 an
d in
put e
rror
, HS
MR
dat
a fro
m J
uly
onw
ards
is
not
rel
iabl
e fo
r m
orta
lity
mea
sure
men
ts b
ut w
ill b
e pu
blis
hed
by D
r Fo
ster
The
late
st H
SM
R a
s pr
ovid
ed b
y D
r Fos
ter
for N
ovem
ber i
s 91
.3.
•C
rude
num
ber o
f dea
ths
of d
eath
s ar
e be
ing
mon
itore
d un
til th
e is
sue
is
reso
lved
. •
Ther
e w
as a
mar
ked
rise
in th
e w
eekl
y nu
mbe
r of d
eath
s ov
er D
ecem
ber
whi
ch p
eake
d at
the
end
of
Dec
embe
r/beg
inni
ng o
f Ja
nuar
y. T
his
was
as
soci
ated
with
incr
ease
d co
nges
tion
in p
atie
nt fl
ow a
nd a
lso
mirr
ors
the
Flu
A s
pike
– th
is is
in li
ne w
ith th
e fin
ding
s of
the
Publ
ic H
ealth
Eng
land
(P
HE
) re
port
into
sea
sona
l flu
. The
re w
as a
dec
line
in c
rude
num
bers
of
deat
hs t
hrou
ghou
t Ja
nuar
y w
hich
has
sta
bilis
ed a
t a
slig
htly
hig
her
num
ber t
han
the
pre-
win
ter l
evel
, pos
sibl
y as
soci
ated
with
a m
inor
rise
in
Flu
B p
ositi
ve c
ases
sin
ce th
e st
art o
f Feb
ruar
y •
The
late
st S
umm
ary
Hos
pita
l-lev
el M
orta
lity
Indi
cato
r (S
HM
I) sc
ore
for J
ul
13 to
Jun
14
is s
light
ly h
ighe
r tha
n la
st q
uarte
r at 1
09, t
his
is w
ithin
the
HS
CIC
‘as
expe
cted
’ ban
ding
.
Dr F
oste
r HSM
R, 2
010/
11 to
Apr
-Nov
201
4/15
Mor
talit
y He
adlin
es
5
Gra
ph :
Trus
t wee
kly
num
ber o
f de
aths
to
12th
Apr
il 20
15
HSM
R De
c 12
- Nov
14 re
base
d us
ing
13/1
4 be
nchm
ark
CQ
C m
orta
lity
outli
er a
lert
s •
No
new
or o
pen
CQ
C m
orta
lity
outli
er a
lerts
Gra
ph s
how
ing
thre
e w
eekl
y av
erag
e nu
mbe
r of d
eath
s an
d +v
e flu
test
s
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.120
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Site
HSM
R Ap
ril 2
008-
Nov
embe
r 20
14
Dr F
oste
r pro
vide
d HS
MR
data
to b
e us
ed w
ith ca
utio
n fr
om Ju
ly o
nwar
ds d
ue to
PM
S2 in
put e
rror
s with
resp
ect t
o ty
pe o
f adm
issio
n
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.121
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Su
mm
ary
SUI p
rofil
e Ap
ril 2
015
7
OPE
N S
UI I
NVE
STIG
ATIO
NS
(as a
t 09/
04/1
5)
Site
/ D
ivis
ion*
Di
rect
orat
e Da
te
(N =
Nev
er E
vent
; P =
Pre
vent
ed N
ever
Eve
nt)
Stat
us
BHH
BHH
Mul
tiple
M
ay14
Sa
lmon
ella
Out
brea
k (M
ay /J
une)
201
4/18
537
Draf
t rep
ort r
ecei
ved
and
QA
proc
ess c
omm
ence
d O
pen
BHH
BHH
Card
iolo
gy
Dec1
4 De
lay
in D
iagn
osis
of B
reas
t Can
cer 2
014/
4130
8 Pa
tient
dia
gnos
ed w
ith m
etas
tatic
bre
ast c
ance
r in
Dece
mbe
r 14
afte
r hav
ing
an a
bnor
mal
ity n
oted
on
CT s
can
in 2
011,
w
hilst
und
er t
he c
are
of t
he c
ardi
olog
y te
am (
coin
cide
ntal
fin
ding
). A
reco
mm
enda
tion
was
mad
e w
ithin
the
CT
scan
re
port
to re
fer t
o Br
east
Ser
vice
, w
hich
doe
s not
app
ear t
o ha
ve b
een
actio
ned.
Ope
n
BHH
BHH
Gast
ro
Jan
15
Dela
yed
diag
nosis
201
5/14
30
Patie
nt re
ferr
ed to
gas
troe
nter
olog
y in
June
201
4, fo
llow
ing
resu
lts o
f an
abno
rmal
abd
omin
al u
ltras
ound
sca
n an
d CT
sc
an. T
he re
ferr
al w
as m
arke
d as
urg
ent.
The
patie
nt’s
firs
t out
patie
nt a
ppoi
ntm
ent w
as in
Sep
t 201
4, a
del
ay o
f app
rox
3 m
onth
s fr
om p
oint
of
refe
rral
to
first
out
patie
nt a
tten
danc
e. B
etw
een
Sept
embe
r an
d De
cem
ber
2014
the
pat
ient
un
derw
ent
furt
her
diag
nost
ic in
vest
igat
ions
and
was
giv
en a
dia
gnos
is of
mul
tifoc
al h
epat
oma
on a
bac
kgro
und
of
cirr
hosis
at
the
begi
nnin
g of
Jan
uary
201
4. T
he p
atie
nt h
as b
een
give
n a
limite
d pr
ogno
sis a
nd is
rec
eivi
ng p
allia
tive
care
.
Ope
n
BHH
BHH
Gast
ro
Jan
15
Dela
yed
Diag
nosis
201
5/14
35
In O
ctob
er 2
013,
an
urge
nt G
P re
ferr
al w
as s
ent
to t
he T
rust
reg
ardi
ng a
pat
ient
with
a 6
mon
th h
istor
y of
upp
er
abdo
min
al p
ain
and
wei
ght l
oss.
Ref
erra
l was
rece
ived
ear
ly N
ovem
ber 2
013,
and
mar
ked
“for
pan
crea
tic c
linic
soo
n”.
The
patie
nt h
ad a
com
plex
hist
ory
of im
pact
ed c
omm
on b
ile d
uct
ston
e w
hich
req
uire
d tr
eatm
ent
in 2
009
(mul
tiple
ER
CP’s
and
unsu
cces
sful
sur
gery
). Th
is ur
gent
ref
erra
l is
reco
rded
as
bein
g re
ceiv
ed o
n IC
ARE
in Ja
n 20
14. T
he P
atie
nt
was
firs
t see
n in
out
patie
nts
in A
pril
2014
and
sub
sequ
ently
und
erw
ent d
iagn
ostic
inve
stig
atio
ns a
nd M
DT d
iscus
sions
. In
June
201
4 th
e pa
tient
was
giv
en a
dia
gnos
is of
met
asta
tic c
olon
can
cer a
nd w
as re
ferr
ed to
onc
olog
y te
am fo
r fur
ther
m
anag
emen
t. Th
e pa
tient
die
d in
Oct
ober
201
4.
Ope
n
BHH
BHH
Gast
ro
Jan
15
Serv
ice
Failu
re 2
015/
1438
Du
ring
late
Dec
embe
r 201
4, a
n in
crea
se in
the
back
log
of p
atie
nts
wai
ting
for d
iagn
ostic
inve
stig
atio
ns w
as id
entif
ied,
th
is po
sitio
n w
as re
view
ed a
nd c
larif
ied
early
Janu
ary
2015
, with
an
addi
tiona
l 600
pat
ient
s co
nfirm
ed a
s no
t bei
ng o
n th
e ga
stro
ente
rolo
gy d
iagn
ostic
wai
ting
list,
som
e da
ting
back
to
Sept
embe
r 20
14. I
n Ju
ne 2
014,
a c
orpo
rate
risk
was
ra
ised
rela
ting
to a
bac
klog
in g
astr
oent
erol
ogy
for d
iagn
ostic
inve
stig
atio
ns a
nd a
pla
n w
as a
gree
d an
d pu
t int
o pl
ace
to m
anag
e th
e ba
cklo
g.
Ope
n
GHH
GHH
Mor
tuar
y
Feb
15
Wro
ng b
ody
rele
ase
2015
/604
7 Pa
tient
A d
ied
at G
HH a
nd w
as t
rans
ferr
ed t
o an
offs
ite m
ortu
ary.
Dec
ease
d pa
tient
B w
ith a
sim
ilar
nam
e w
as a
lso
tran
sfer
red
from
a d
iffer
ent t
o th
e sa
me
offs
ite m
ortu
ary.
Due
to
a de
cisio
n ch
ange
for
patie
nt A
to b
e cr
emat
ed n
ot
burie
d, it
was
nec
essa
ry fo
r pat
ient
A to
be
tran
sfer
red
back
to G
HH fo
r am
endm
ents
of r
equi
red
pape
rwor
k. In
err
or
patie
nt B
was
tran
sfer
red
to G
HH in
stea
d of
pat
ient
A. P
atie
nt B
was
then
rele
ased
for c
rem
atio
n in
stea
d of
pat
ient
A.
The
erro
r w
as n
oted
whe
n th
e pa
thol
ogy
labo
rato
ry r
outin
ely
rang
the
off
site
mor
tuar
y to
see
if
they
had
any
ou
tsta
ndin
g de
ceas
ed p
atie
nts
for G
HH. P
atie
nt A
was
ide
ntifi
ed a
s stil
l bei
ng a
t the
offs
ite m
ortu
ary.
Ope
n
NB
. Lin
ked
to “D
elay
in d
iagn
ostic
End
osco
py
test
s” R
isk
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.122
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Sum
mar
y SU
I pro
file
April
201
5
8
OPE
N S
UI I
NVE
STIG
ATIO
NS
(as a
t 09/
04/1
5)
Site
/ D
ivis
ion*
Di
rect
orat
e Da
te
(N =
Nev
er E
vent
; P =
Pre
vent
ed N
ever
Eve
nt)
BHH
BHH
ED
Fe
b 15
Su
bopt
imal
care
of d
eter
iora
ting
patie
nt 2
015/
6003
Pa
tient
adm
itted
with
a h
istor
y of
che
st p
ain.
Whi
lst b
eing
cle
rked
the
patie
nt su
ffere
d a
card
iac
arre
st. T
he p
atie
nt w
as
succ
essf
ully
res
usci
tate
d bu
t fo
und
to h
ave
a po
tass
ium
of 9
.1m
mol
s. A
ppro
pria
te t
reat
men
t w
as g
iven
to
low
er t
he
pota
ssiu
m h
owev
er: t
he p
atie
nt s
uffe
red
a fu
rthe
r tw
o ca
rdia
c ar
rest
s an
d de
spite
pro
long
ed re
susc
itatio
n th
e pa
tient
di
ed. T
he p
atie
nt’s
pot
assiu
m a
t thi
s po
int w
as 8
.4m
mol
s. I
t wou
ld a
ppea
r tha
t for
a p
erio
d of
six
hour
s the
pat
ient
did
no
t hav
e a
repe
at p
otas
sium
che
ck o
r rec
eive
any
trea
tmen
t for
hyp
erka
laem
ia.
Ope
n
SOL
SOL
Acut
e M
ed/A
MU
M
ar 1
5 M
issed
dia
gnos
is of
pne
umot
hora
x 201
5/10
303
Patie
nt r
efer
red
at t
he w
eeke
nd v
ia G
P w
ith a
hist
ory
of b
reat
hles
snes
s, c
hest
pai
n, a
sthm
a an
d re
duce
d ai
r en
try
on
left
sid
e of
the
ches
t. Af
ter e
xam
inat
ion
and
inve
stig
atio
ns th
e cl
inic
ians
rev
iew
ed t
he p
atie
nts’
CXR
whi
ch i
dent
ified
th
e pr
esen
ce o
f a
poss
ible
lun
g m
ass
or a
bsce
ss.
Afte
r se
vera
l ho
urs
the
patie
nts
sym
ptom
s ha
d se
ttle
d an
d th
e ob
serv
atio
ns w
ere
with
in n
orm
al p
aram
eter
s. T
he p
atie
nt w
as d
ischa
rged
hom
e w
ith a
man
agem
ent p
lan
for a
n ur
gent
CT
, bro
ncho
scop
y, a
nd fo
llow
up
with
the
resp
irato
ry te
am to
exc
lude
lung
mas
s or
abs
cess
whi
ch w
ere
arra
nged
. The
CX
R w
as r
outin
ely
revi
ewed
3 d
ays
late
r by
a r
adio
logi
st w
ho id
entif
ied
a la
rge
pneu
mot
hora
x w
ith c
olla
psed
lung
. Th
ere
wer
e se
vera
l att
empt
s b
y cl
inic
ians
to c
onta
ct th
e pa
tient
, ho
wev
er it
was
foun
d th
at th
ey h
ad fl
own
abro
ad o
n ho
liday
. Onc
e co
ntac
t was
mad
e th
ey w
ere
advi
sed
to a
tten
d ho
spita
l The
pat
ient
was
trea
ted
succ
essf
ully
abr
oad
and
retu
rned
to th
e U
K th
ree
wee
ks la
ter.
Oth
er a
spec
ts o
f clin
ical
man
agem
ent u
nder
revi
ew.
NEW
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.123
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Su
mm
ary
SUI p
rofil
e : R
ecen
tly cl
osed
9
Rece
ntly
Clo
sed
SUI I
NVE
STIG
ATIO
NS
(as a
t 09/
04/1
5)
Site
/ D
ivis
ion*
Sp
ecia
lty
Date
(N
= N
ever
Eve
nt; P
= P
reve
nted
Nev
er E
vent
St
atus
SH
SH
Oph
thal
mol
ogy
Dec1
4 In
sert
ion
of in
corr
ect l
ens (
Nev
er E
vent
) 201
4/41
293
Patie
nt u
nder
wen
t ca
tara
ct s
urge
ry in
her
left
eye
in J
anua
ry 2
014
with
suc
cess
ful o
utco
me.
Pat
ient
the
n un
derw
ent
surg
ery
on ri
ght e
ye in
July
201
4. B
oth
of th
e le
nses
cho
sen
for h
er su
rger
ies w
ere
base
d up
on b
iom
etry
she
unde
rwen
t in
Nov
embe
r 201
3. In
Dec
embe
r 201
4, it
was
iden
tifie
d th
an a
n in
corr
ect l
ens
had
been
inse
rted
into
her
righ
t eye
and
as
a re
sult
she
had
poor
refr
acto
ry o
utco
mes
and
requ
ired
furt
her s
urge
ry.
Initi
al in
vest
igat
ion
has
iden
tifie
d th
at th
e w
rong
bi
omet
ry w
as in
the
patie
nt’s
elec
tron
ic m
ed iS
OFT
reco
rd th
at w
as u
sed
to se
lect
the
lens
requ
ired.
Clos
ed
Oph
thal
mol
ogy
shou
ld d
evel
op a
stan
dard
ope
ratin
g pr
oced
ure
for t
he ti
mel
y es
cala
tion
of p
atie
nts
in th
e ev
ent o
f poo
r sur
gica
l out
com
es
Oph
thal
mol
ogy
shou
ld c
onsid
er p
urch
asin
g so
ftw
are
whi
ch a
llow
s the
stor
age
of th
e IO
L Mas
ter b
iom
etry
dat
a an
d pr
into
ut w
ithin
the
Med
iSO
FT sy
stem
, so
all b
iom
etry
is a
vaila
ble
elec
tron
ical
ly.
Lead
bio
met
rist s
houl
d ex
plor
e w
ith M
ed iS
OFT
if th
ey a
re a
ble
to fa
cilit
ate
a lo
ck d
own
of d
ata
with
in th
e sy
stem
with
any
furt
her i
nfor
mat
ion
bein
g ad
ded
as a
n ad
dend
um.
Oph
thal
mol
ogy
shou
ld re
view
the
com
pete
ncie
s of
all
clin
ical
nur
se sp
ecia
lists
and
offe
r fur
ther
trai
ning
rega
rdin
g re
frac
tive
outc
omes
and
lens
cho
ice
if re
quire
d.
Oph
thal
mol
ogy
shou
ld m
anda
te th
at a
ll th
e su
rgeo
ns a
nd sc
rub
nurs
es a
re a
war
e of
the
prev
ious
lens
cho
ice
whe
n th
ey a
re o
pera
ting
on a
seco
nd e
ye.
BHH
BHH
ED/A
MU
Fe
b 15
De
terio
ratin
g pa
tient
201
4/36
858
A pa
tient
was
disc
harg
ed h
ome
follo
win
g a
faile
d en
dosc
opy
proc
edur
e. T
he p
atie
nt p
rese
nted
in
ED 2
hou
rs p
ost
proc
edur
e w
ith d
iffic
ulty
in b
reat
hing
and
mar
ked
surg
ical
em
phys
ema
. A C
T sc
an c
onfir
med
a p
erfo
rate
d oe
soph
agus
an
d th
e pa
tient
was
tran
sfer
red
to A
MU
. The
follo
win
g m
orni
ng th
e pa
tient
suf
fere
d a
card
iore
spira
tory
arr
est a
nd d
ied.
Co
ncer
ns h
ave
been
raise
d re
gard
ing
the
man
agem
ent o
f the
pat
ient
’s c
are.
Clos
ed
Ther
e sh
ould
be
agre
emen
t am
ongs
t EN
T, th
orac
ic, U
pper
GI s
urge
ons a
nd G
astr
oent
erol
ogy
for “
Susp
ecte
d Pe
rfor
ated
Oes
opha
geal
Pat
hway
” in
term
s of c
lear
ow
ners
hip,
man
agem
ent
supp
orte
d by
the
Trus
t to
agre
e a
solu
tion,
esp
ecia
lly o
ut o
f hou
rs. T
o be
put
on
the
trus
t Upp
er G
I sur
gica
l risk
regi
ster
.
Ther
e sh
ould
be
care
ful c
onsid
erat
ion
of H
DU a
dmiss
ion
for a
ll pa
tient
s w
ith su
rgic
al e
mph
ysem
a se
cond
ary
to o
esop
hage
al p
erfo
ratio
n, d
iscus
sed
with
and
revi
ewed
in p
erso
n by
the
criti
cal c
are
team
.
All p
atie
nts w
ith a
susp
ecte
d pe
rfor
atio
n on
adm
issio
n in
wor
king
hou
rs sh
ould
be
revi
ewed
by
an a
ppro
pria
te sp
ecia
lity
regi
stra
r in
pers
on, m
ust b
e di
scus
sed
with
thei
r con
sulta
nt o
n ca
ll. E
NT
shou
ld b
e in
volv
ed fo
r cer
vica
l lev
el o
esop
hage
al p
erfo
ratio
n an
d U
pper
GI s
urge
ons
or th
orac
ic fo
r bel
ow c
ervi
cal l
evel
per
fora
tions
. St
aff s
houl
d be
rem
inde
d no
t to
rely
sole
ly o
n M
EWS
as th
e in
dica
tor o
f sev
erity
of i
llnes
s. If
an
over
all a
sses
smen
t of c
once
rn is
pre
sent
it sh
ould
be
esca
late
d to
med
ics a
s app
ropr
iate
. St
aff s
houl
d be
rem
inde
d of
the
crite
ria to
invo
ke th
e Se
psis
6 Pa
thw
ay a
nd th
e im
plem
enta
tion
of th
e bu
ndle
.
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.124
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
SUI:
Aug
ust 2
013
GHH
Care
of E
lder
ly
Opi
ate
over
dose
in o
piod
nai
ve p
atie
nt –
Pr
even
ted
Nev
er E
vent
Th
emes
: Com
mun
icat
ion/
non
adhe
renc
e to
po
licy
SUI:
Sep
tem
ber 2
013
SHH
T&O
The
atre
s Re
tain
ed ri
bbon
gau
ze fo
llow
ing
THR
– N
ever
Eve
nt
Them
es:
Com
mun
icat
ion/
non
adh
eren
ce
to p
olic
y/po
or a
war
enes
s of d
uty
of
cand
our
Com
mun
icat
ion
Doc
umen
tatio
n
M
edic
atio
n
Saf
er
Surg
ery
Det
erio
ratin
g Pa
tient
Com
mun
icat
ion
•Vita
l and
iski
lls re
sour
ces
•Nur
sing
safe
ty m
anua
ls •S
afet
y w
alka
roun
ds a
nd re
spon
sive
safe
ty re
view
pro
cess
es
•Risk
y bu
sines
s fo
rum
for j
unio
r do
ctor
s
Docu
men
tatio
n •S
urgi
cal s
afet
y ch
eckl
ist /
audi
t •N
ursin
g M
etric
s •A
nnua
l Tru
st-w
ide
docu
men
tatio
n au
dit
•Saf
ety
ther
mom
eter
•N
G tu
be p
olic
y an
d gu
idel
ine
S
UI T
hem
es (R
oot c
ause
s and
con
trib
utor
y fa
ctor
s) a
nd S
ched
ule
5 le
tter
s rec
eive
d by
HEF
T Co
mm
on th
emes
from
SU
Is a
nd a
ssoc
iate
d w
ork-
stre
ams
Dete
riora
ting
Patie
nt
Re-e
stab
lishe
d De
terio
ratin
g Pa
tient
Rec
ogni
tion
Grou
p Vi
tal a
nd iS
kills
reso
urce
s M
ews a
udit
Nur
sing
met
rics
Less
ons o
f the
mon
th
SUI a
t a g
lanc
e re
port
Ac
tion
card
s bei
ng p
rodu
ced
for i
ssue
to su
rgic
al re
gist
rars
man
datin
g th
e ci
rcum
stan
ces w
here
they
mus
t con
tact
thei
r con
sulta
nt
SUI:
Sept
embe
r 201
3 G
astr
oent
erol
ogy
BHH
Inju
ry d
urin
g liv
er b
iops
y Th
emes
: Com
mun
icat
ion
SUI:
July
201
3 SH
H ED
U
nexp
ecte
d In
fant
Dea
th
Them
e: D
ocum
enta
tion/
Com
mun
icat
ion
SU
I: A
ugus
t 201
3 GH
H U
rolo
gy/E
D De
lay
in ti
mel
y in
terv
entio
n an
d es
cala
tion
of th
e de
terio
ratin
g pa
tient
Th
emes
: Com
mun
icat
ion/
Non
esc
alat
ion
of
clin
ical
con
cern
s.
Med
icat
ion
•Saf
e M
edic
atio
n Pr
actic
e Gr
oup
•Med
icat
ion
Mat
ters
new
slett
ers
•Impr
ovem
ent t
o EP
syst
em
•New
Med
icin
es G
roup
for r
evie
win
g al
l sev
ere
harm
inci
dent
s fr
om
med
icat
ion
inci
dent
s •N
ew R
CA fo
r all
seve
re h
arm
m
edic
atio
n in
cide
nts
•Pat
ient
Saf
ety
Team
dev
elop
ed to
ol
for l
ive
info
rmat
ion
rela
ting
to m
issed
do
se a
nti-b
iotic
s.
SUI:
July
201
3 SH
H O
phth
alm
olog
y W
rong
lens
inse
rtio
n– N
ever
Eve
nt
Them
es: T
heat
re c
heck
ing
proc
edur
es/c
omm
unic
atio
n
SUI:
Oct
ober
201
3 Va
scul
ar S
urge
ry B
HH
Une
xpec
ted
deat
h fo
llow
ing
surg
ery
Them
es: N
on a
dher
ence
to V
TE p
olic
y/
com
mun
icat
ion/
docu
men
tatio
n SU
I: O
ctob
er 2
013
Gene
ral S
urge
ry B
HH
Wro
ng S
ite S
urge
ry –
Nev
er E
vent
Th
emes
: Doc
umen
tatio
n/co
mm
unic
atio
n
Safe
r Sur
gery
•S
harin
g th
e le
arni
ng fr
om th
eatr
e re
late
d N
ever
Eve
nts
•Kno
win
g th
e ris
k. P
erio
pera
tive
risk
asse
ssm
ent /
com
mun
icat
ion
tool
•S
afet
y w
alk
abou
t in
all t
heat
res a
cros
s sit
es
SUI:
Sept
embe
r 201
3 Ga
stro
ente
rolo
gy
Surg
ery
BHH
Dela
y in
esc
alat
ing
dete
riora
ting
patie
nt
Them
es: D
elay
in e
scal
atin
g pa
tient
to
cons
ulta
nt le
vel/p
oor r
ecog
nitio
n of
the
dete
riora
ting
patie
nt
Ser
ious
Unt
owar
d In
cide
nt T
hem
es /N
ever
Eve
nts
July
201
3 –A
pril
2014
SUI:
Oct
ober
201
3 Pa
thol
ogy
BHH
De
lay
repo
rtin
g pa
thol
ogy
spec
imen
s Th
emes
: Und
er e
ffici
ency
, lac
k of
ca
paci
ty, p
oor o
rgan
isatio
n
Lear
ning
tool
s
•SU
I at
a g
lanc
e re
port
s and
cas
cade
syst
em
•Mor
talit
y di
gest
•S
afet
y le
sson
of t
he m
onth
•W
eekl
y Q
ualit
y an
d Sa
fety
Mee
tings
•D
evel
opin
g Da
re to
Sha
re M
eetin
gs
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.125
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
SUI:
May
201
4 –
ITU
BHH
Ce
ssat
ion
of in
otro
pic
drug
infu
sion
Them
es:
Com
mun
icat
ion/
non
adhe
renc
e to
stan
dard
ope
ratin
g po
licie
s
SUI:
June
201
4 –
Paed
iatr
ics G
HH
Dela
y in
reco
gniti
on a
nd e
scal
atio
n of
a si
ck
child
. Th
emes
: Co
mm
unic
atio
n/ d
elay
in
reco
gniti
on a
nd e
scal
atio
n
Com
mun
icat
ion
Doc
umen
tatio
n
M
edic
atio
n
Saf
er
Surg
ery
Det
erio
ratin
g Pa
tient
Pa
tient
Han
dove
r
Com
mun
icat
ion
•Vita
l and
iski
lls re
sour
ces
•Nur
sing
safe
ty m
anua
ls •S
afet
y w
alka
roun
ds a
nd re
spon
sive
safe
ty re
view
pro
cess
es
•Risk
y bu
sines
s fo
rum
for j
unio
r do
ctor
s •J
unio
r doc
tor r
isky
busin
ess
mem
ory
bank
.
Docu
men
tatio
n •S
urgi
cal s
afet
y ch
eckl
ist /
audi
t •N
ursin
g M
etric
s •A
nnua
l Tru
st-w
ide
docu
men
tatio
n au
dit
•Saf
ety
ther
mom
eter
•C
onse
nt P
olic
y
S
UI T
hem
es (R
oot c
ause
s and
con
trib
utor
y fa
ctor
s) a
nd S
ched
ule
5 le
tter
s rec
eive
d by
HEF
T Co
mm
on th
emes
from
SU
Is a
nd a
ssoc
iate
d w
ork-
stre
ams
Dete
riora
ting
Patie
nt
Re-e
stab
lishe
d De
terio
ratin
g Pa
tient
Rec
ogni
tion
Grou
p Vi
tal a
nd iS
kills
reso
urce
s M
ews a
udit
Nur
sing
met
rics
Less
ons o
f the
mon
th
SUI a
t a g
lanc
e re
port
De
terio
ratin
g pa
tient
cam
paig
n Se
psis
pilo
t in
AMU
on
all t
hree
site
s to
impr
ove
trea
tmen
t for
seps
is
SUI:
Augu
st 2
014
– Pa
edia
tric
s BHH
U
nexp
ecte
d De
ath
of a
chi
ld
Them
es:
Ow
ners
hip
of p
atie
nts
by
paed
iatr
ic te
am re
gard
less
of s
peci
ality
pa
tient
is u
nder
.
SUI:
Apr
il 20
14 –
Sur
gery
BHH
U
nexp
ecte
d pa
tient
dea
th
Them
es:
Patie
nt S
uici
de
SUI:
May
201
4 –
Paed
iatr
ics B
HH
Prev
ente
d N
ever
Eve
nt
Opi
ate
over
dose
in o
piod
nai
ve p
atie
nt
Them
es: C
omm
unic
atio
n/no
n ad
here
nce
to
polic
y
Med
icat
ion
•Saf
e M
edic
atio
n Pr
actic
e Gr
oup
•Med
icat
ion
Mat
ters
new
slett
ers
•Impr
ovem
ent t
o EP
syst
em
•New
Med
icin
es G
roup
for r
evie
win
g al
l sev
ere
harm
inci
dent
s fr
om
med
icat
ion
inci
dent
s •P
atie
nt S
afet
y Te
am d
evel
oped
tool
fo
r liv
e in
form
atio
n re
latin
g to
miss
ed
dose
ant
i-bio
tics.
SUI:
May
201
4 –
Gast
roen
tero
logy
BHH
De
lay
in e
scal
atio
n of
det
erio
ratin
g pa
tient
Th
emes
: Po
or r
ecog
nitio
n of
det
erio
ratin
g pa
tient
/d
elay
in
es
cala
ting
patie
nt
to
cons
ulta
nt le
vel
SUI:
Augu
st 2
014
- Vas
cula
r Sur
gery
BHH
De
ath
whi
lst o
n a
wai
ting
list
Them
es:
Lack
of a
neur
ysm
pat
hway
co-
ordi
nato
r.
SUI:
July
201
4 –
Card
iolo
gy B
HH
Dela
y in
reco
gniti
on o
f sic
k pa
tient
Th
emes
: Com
mun
icat
ion/
reco
gniti
on a
nd
inte
rven
tion
follo
win
g ch
ange
in te
lem
etry
Safe
r Sur
gery
•S
harin
g th
e le
arni
ng fr
om th
eatr
e re
late
d N
ever
Eve
nts
•Kno
win
g th
e ris
k. P
erio
pera
tive
risk
asse
ssm
ent /
com
mun
icat
ion
tool
•S
afet
y w
alk
abou
t in
all t
heat
res a
cros
s sit
es
•No
Mar
k –
No
Go C
ampa
ign
for s
afer
su
rger
y
SUI:
Augu
st 2
014
– O
bste
tric
s BH
H In
trap
artu
m S
tillb
irth
Them
es:
Ser
ious
Unt
owar
d In
cide
nt T
hem
es /N
ever
Eve
nts
Apr
il 20
14 –
Oct
ober
201
4
SUI:
July
201
4 –
ED B
HH
Dela
y in
dia
gnos
is of
sub
arac
hnoi
d ha
emor
rhag
e Th
emes
: Lac
k of
com
mun
icat
ion
Lear
ning
tool
s
•SU
I at
a g
lanc
e re
port
s and
cas
cade
syst
em
•Mor
talit
y di
gest
•S
afet
y le
sson
of t
he m
onth
•W
eekl
y Q
ualit
y an
d Sa
fety
Mee
tings
•P
atie
nt sa
fety
and
lear
ning
less
ons
boar
ds p
ilote
d in
AM
U B
HH
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.126
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Sche
dule
5 S
ectio
n 7
(form
erly
Rul
e 43
) / C
oron
er’s
conc
erns
In
ques
t sch
edul
ed fo
r 16th
Mar
ch 2
015
asso
ciat
ed w
ith a
n in
cide
nt b
eing
inve
stig
ated
th
roug
h th
e Tr
ust S
UI p
roce
ss a
s “de
terio
ratin
g pa
tient
”. S
TEIS
201
4/36
858
Nar
rativ
e co
nclu
sion
– Pa
tient
die
d fr
om re
cogn
ised
com
plic
atio
n of
an
inve
stig
ativ
e en
dosc
opy.
No
sche
dule
5 se
ctio
n 7
12
Forw
ard
look
: Pot
entia
l for
adv
erse
inqu
est c
oncl
usio
n In
ques
t sch
edul
ed fo
r 25
Mar
ch 2
015
asso
ciat
ed w
ith d
elay
in re
cogn
ition
of c
hang
e in
te
lem
etry
mon
itorin
g w
hich
was
form
erly
inve
stig
ated
thro
ugh
the
Trus
t’s S
UI p
roce
ss
STEI
S 20
14/2
2609
Inqu
est a
djou
rned
resc
hedu
led
to 2
2nd M
ay 2
015
SUI p
rofil
e by
man
agem
ent t
eam
(as a
t 09/
04/1
5)
Site
/Div
10
/11
11
/ 1
2
12/
13
13/1
4 14
/15
BHH
5
5 3
(1x
N)
9 (2
xN)
15
GHH
0 2
(2xN
) 2
(1xN
) 3
(2xN
; 1x
PN)
0
SHH
1 (1
xN)
2(2x
N)
1 1
(1xN
) 2(
1xN
)
W&
C 5
3(2x
N)
5 (1
xN)
1 6
(1xP
N)
CSS
2(1x
N)
5 0
1 2
Nev
er (o
r PN
) Eve
nts
2 of
14
6 of
17
3 of
11
6 of
15
2 of
25
Nev
er e
vent
s in
201
2/13
rela
te to
: 1
wro
ng s
ite s
urge
ry (G
ener
al S
urge
ry)
1 In
appr
opria
te a
dmin
istra
tion
of d
aily
ora
l met
hotre
xate
(T&O
) 1
reta
ined
tam
pon
(O&G
) N
ever
eve
nts
in 2
013/
14 re
late
to:
2
wro
ng im
plan
t (T&
O /
Thea
tres
and
Oph
thal
m /
Thea
tres)
2
reta
ined
fore
ign
obje
cts
(Gen
Sur
g / T
heat
res
and
T&O
/ th
eatre
s)
Prev
ente
d :
Opi
oid
over
dose
of o
pioi
d na
ive
patie
nt (E
lder
ly)
1 w
rong
site
sur
gery
(Gen
eral
Sur
gery
)
Nev
er e
vent
s in
201
4/15
rela
te to
: Pr
even
ted:
1 O
pioi
d ov
erdo
es o
f opi
oid
naiv
e pa
tient
(Pae
diat
rics)
1x
wro
ng im
plan
t (O
phth
alm
olog
y)
12
SUI p
rofil
e by
loca
tion
(as a
t 09/
04/1
5)
Site
10
/11
11 /
12
12/
13
13/1
4 14
/15
BHH
8
11
7 (2
x N
) 7
(1xN
) 17
(1xP
N)
GHH
5
1
3 (1
xN)
4 (2
xN;
1xPN
) 6
SHH
0 5
1 3
(2xN
) 2(
1xN
)
Oth
er
1 0
Tota
l 14
17
11
15
25
Su
mm
ary
SUI p
rofil
e M
arch
201
5 an
d in
ques
t upd
ate
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.127
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
13
CQC
IMR
Dec
embe
r
Safety Sitrep - April 2015

Council of GovernorsJune 2015
.128
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
Integrated Improvement plan

Council of GovernorsJune 2015
.129
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement plan
Title: HEFT Integrated Improvement Plan (IIP)
Attachments: 1
From: Dr Andrew Catto, Deputy CEO & Executive Medical Director
To: Board of Directors and Council of Governors
The Report is being provided for: Decision Y/N Discussion Y/N Assurance Y/N Endorsement Y/N The BoD is being asked to:
Review the IIP and consider if the IIP reaches the standard of an effective recovery plan given the current operational and regulatory context of the Trust.
Key points/Summary: The IIP:
Describes the HEFT programme management methodology Describes the next 30 / 60 / 90 days and the action HEFT will take Provides a framework around the assurance process HEFT will use Describes the programme structure and the governance arrangements in
the six constituent IIP programmes Recognises certain risks and constraints to delivery Describes a range of programme metrics to inform progress against the
HEFT improvement journey Recommendation(s): That the IIP is implemented in full and that the Executive Management Board manages and monitors the implementation of the IIP using the IIP Programme Board. The BoD and External Stakeholder Engagement Group will be updated on progress with the IIP. Assurance Implications: Strategic Risk Register Y/N Performance KPIs year to date Y/N
Resource/Assurance Implications (e.g. Financial/HR) Y/N Information Exempt from
Disclosure Y/N
Which other Committees has this paper been to? (e.g. F&PC, QRC, etc.)
Executive Management Board and Board of Directors Forum in draft format.
Stakeholder Engagement Group 20th May 2015

Council of GovernorsJune 2015
.130
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
HEART OF ENGLAND NHS FOUNDATION TRUST
INTEGRATED IMPROVEMENT PLAN
RECOVERY PLAN

Council of GovernorsJune 2015
.131
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
D o c u m e n t C o n t r o lChange history
V e r s i o n R e a s o n / S u m m a r y o f C h a n g e s
D a t e A u t h o r
V0.6 6th Draft - comments from Execs and Board +Executive summary &
revised Comms plan
18/5/15 Stuart A Brown
Document approvals - this document requires the following approvals
N a m e T i t l e V e r s i o n a n d D a t e
Andrew Foster Interim Chief Executive May 2015 - V0.6Andrew Catto Deputy Chief Executive and
Medical Director & SROMay 2015 - V0.6
Darren Cattell Interim Director of Finance May 2015 - V0.6Sam Foster Chief Nurse May 2015 - V0.6
Jonathan Brotherton Director of Operations May 2015 - V0.6Hazel Gunter Director of Workforce May 2015 - V0.6
Monitor Regional representative May 2015 - V0.6
Distribution
N a m e T i t l e D a t e o f i s s u e
V e r s i o n
This document will remain in DRAFT Format until formal agreement and acceptance by Monitor and the Trust Board as the definitive description of the IIP, it’s constituent programmes and the methodology and approach that will be used to deliver the IIP
Safe Effective Caring Responsive Well led
Page 2 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6

Council of GovernorsJune 2015
.132
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
TABLE OF CONTENTS1. ...........................................................Executive Summary 62. ....................................................................Introduction 132.1. .................................................................Purpose of this Document 13
2.2. ..........................................................................................Context 14
2.3. ....................................................................................Background 21
2.4. ...........................Sponsorship of the Integrated Improvement Portfolio 23
2.5. ..............................................................Key Priorities and Timelines 23
2.6. ......................................The 30 day challenge - Getting back on Track 24
3. ......................................................Vision and Objectives 263.1. ............................................................................................Vision 26
3.2. ......................................................................................Objectives 26
4. .....................................Programme Management & PMO 284.1. .........................................................................Structure of the IIP 28
4.2. .......................................................................................Approach 30
4.3. ...................................................................................Methodology 30
4.4. ......................................................................................PMO Tools 31
4.5. ............................................................Managing Interdependencies 33
4.6. .................................................Benefits management and realisation 34
4.7. ................................................................What does good look like? 34
5. ............................................................................Metrics 366. .........................................................Programme Profiles 396.1. .....................................................Governance Recovery Programme 39
6.2. ...................................................................Urgent Care Programme 41
6.3. ............................................................................IM&T Programme 43
6.4. .................................................................Cultures and Engagement 44
6.5. ...............................................................................Scheduled Care 47
Safe Effective Caring Responsive Well led
Page 3 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6

Council of GovernorsJune 2015
.133
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
6.6. ........................................................................................Mortality 49
7. .........................................................Programme Costing 537.1. .........................................................Programme Management Costs 53
8. ...................................................................Stakeholders 568.1. .......................................................................Stakeholders Profiles 56
8.2. .................................................Stakeholder mapping & Management 56
9. ....................................................Scheduling/Milestones 599.1. ..........................................................................Thirty Days (o+30) 59
9.2. ...........................................................................Sixty Days (0+60) 60
9.3. ....................................................................................Ninety Days 60
10. ..............................................................................Risks 6310.1. .................................................Managing Risks Within The Portfolio 63
10.2. ..................................................................Links To Strategic Risks 64
11. ....................................................................Constraints 6611.1. ......................................................................Types Of Constraints 66
11.2. ............................................................................Potential Impact 66
12. ............................................................Communications 6812.1. ..........................................................Tactical Approach For The IIP 68
12.2. ....................................................................................Objectives 68
12.3. ...................................................Supporting the IIP implementation 68
12.4. ...................................................................Clinical communication 69
12.5. ..................................................................................Governance 69
12.6. .................................................................Culture and Engagement 69
12.7. .....................................................................................Resources 70
12.8. .............................................................................Implementation 71
13. ..........................................................Gateway Reviews 7313.1. ......................................................................Schedule Of Reviews 74
13.2. ....................................................................Description Of Review 75
13.3. ......................................Governance And Resources For The Reviews 75
14. ....................................................................Appendices 7714.1. ..................................................Appendix I -CCG “Unit of Planning” 77
14.2. .............................................Appendix II - PMO SAMPLE TEMPLATES 78
Safe Effective Caring Responsive Well led
Page 4 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6

Council of GovernorsJune 2015
.134
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
14.3. .......................Appendix III - Sample of an Outcome relationship map 82
14.4. ....................................................Appendix IV - Main IIP Dashboard 83
14.5. ..................................................Appendix V - Monitor Undertakings 84
14.6. .........................Appendix VI - Interim Governance On Boarding Form 86
Safe Effective Caring Responsive Well led
Page 5 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6

Council of GovernorsJune 2015
.135
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
1.EXECUTIVE SUMMARY
Heart of England NHS Foundation Trust (HEFT) is a multi site acute and community services provider with locations at Heartlands Hospital, Good Hope Hospital and Solihull Hospital, employing approximately 11000 staff across the three sites.During the twelve months preceding the publication of this document HEFT have been the subject to a number of reviews, the subsequent reports have not cast HEFT in a positive light in a number of areas which includes both clinical and managerial disciplinesThis has had direct and indirect consequences for HEFT, including major leadership changes with the highly publicised resignation in November 2014 of Dr Mark Newbold as the Chief Executive Officer. This followed the relatively recent change in the Chair, Mr. Les Lawrence was appointed as the new Chairman succeeding Lord Hunt. in July 2014. Further changes in the executive leadership team followed which understandably created a certain amount of instability and concern amongst those remaining in the leadership team and HEFT staff alike.Running in parallel to some of these events was the enforcement action that Monitor accepted under section 106 of the Health and Social Care Act ("the Act") and was compelled to impose upon HEFT on 20 December 2013 in relation to the Licensee's governance arrangements for urgent care. Amendments were accepted to those undertakings on 21 October 2014, following breaches of additional access and outcome performance indicators. As a consequence of these collective actions Monitor appointed an Improvement Director to work with HEFT to support a number of improvement initiatives. Following the resignation of Dr Mark Newbold the Medical Director, Dr Andrew Catto was appointed as the Interim Chief Executive Officer to immediately fill the void and bring some stability to the Trust. Dr Catto set about constructing a number of plans and initiatives designed to improve clinical services, safeguard the reputation of HEFT, Improve the leadership team and fill the gaps left by departing Executives - appointing an Interim Director of Finance and Director of Information Management &Technology (IM&T). Dr Catto led the development of an integrated leadership support and resilience programme (LSRP) between December 2014 and February 2015. The key programmes in the LSRP, which was presented to Monitor, key stakeholders and national clinical leaders, comprised the 7 work streams of governance, mortality / congestion, culture / engagement, safe staffing, IM&T /PMS2, performance and executive leadership, which have latterly become known as the Integrated Improvement Plan (the IIP). Further refinement has seen the IIP change, evolve and expand to include a number of Trust wide improvement programmes such as Urgent Care and Scheduled care whilst other smaller programmes have merged with others to form larger programmes. The IIP now consists of six primary change programmes see Fig 1 below:
Safe Effective Caring Responsive Well led
Page 6 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6

Council of GovernorsJune 2015
.136
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
Scheduled Care Governance Urgent Care IM&T Mortality Cultures & Engagement
Integrated Improvement Plan
Figure 1 - Integrated Improvement Plan
However whilst there was a common intention to run these programmes as an Integrated programme the reality was that the programme management arrangements needed to support this approach were not in place at the time of conception, not even in an embryonic form.HEFT established a Programme Management Office (PMO) in January 2015 and engaged a small number of Interim resources to support the delivery of the IIP. Following the appointment of Mr Andrew Foster on the 16th of February the LSRP evolved into the Pyramid of Priorities, developed by Mr Andrew Foster which is based on a six phases of the delivery model as described in Fig 21 below:
4"
Recovery
1. Clarity (Governance & Strategy)
2. Quality Improvement 3. Staff Engagement
Internal Communications Board Development
Management Capacity Stakeholder Relationship
Safe Staffing ICT Investment
Estates Investment Mortality Reduction
Deloitte Governance Plan Monitor Enforcement Undertakings
• A&E • RTT
• Scheduled Care • Cancer
CQC Recommendations Kennedy Report Silverman Report
The$Pyramid$of$Priori.es$$Feb to April 2015.Creation of The Plan - conceptually based on the original January 2015 Leadership and Resilience Plan. Limited PMO capacity initially arising from simultaneous focus on establishing the Programme Office and running several other improvement programmes synchronously.
Clear Executive Leadership. Deputy CEO manages and assure the Plan. Interim DoF manages the timeliness and quality of submission. Supported by very experienced Programme Manager, Stuart Brown. Focused one week piece of work commissioned from Deloitte to align the dashboard metrics with the IIP.
1 2 3
4 5 6
Creating the Narrative – From the Deloitte Governance Report to the Resilience Plan to the Pyramid of Priorities to the IIP and Dashboard.
IIP is perceived as centre stage in the organisation - with buy-in from the Board, CoG and external stakeholders.
Introducing a Layered Approach to presentation and implementation so that the IIP can be seen in a national context, at full Trust level, at site, at service and down to the individual member of staff.
The IIP and our suite of strategies merge and become the entire plan enabling us to shift from back foot to front foot in September 2015.
Figure 2- Pyramid of Priorities and the Six Phase plan
As the last quarter of 2014/15 passed and the year end approached the Executive Management Board (EMB) and subsequently Monitor started to voice concern about the lack of clarity and intent surrounding the IIP. concerns were also raised about the quality and format of the reporting. There was confusion about the metrics and how meaningful they were/are not and the ambiguity that some of the reporting formats seemed to indicate. In March 2015 the Interim Director of Finance (DoF) and the Chief Nurse moved to engage additional interim support to deliver a Governance recovery programme based on the findings and recommendations of the Deloitte report commissioned by Monitor, who decided to share the report with the EMB to help them understand the breadth and depth of the challenges facing HEFT.
Safe Effective Caring Responsive Well led
Page 7 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
1 This is explained in more detail in Item 2.2 of the main body of the document

Council of GovernorsJune 2015
.137
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
In April 2015, a new stakeholder group was established comprising the HEFT executive team, NHS England, Lead Clinical Commissioning Groups (CCG’s), Monitor and the Care Quality Commission (CQC). This innovative approach, supported by the Monitor Director of Improvement replaced the Quality Steering Group (QSG)The implementation of the Governance recovery programme and subsequent analysis by the Interim DoF and Chief Nurse, coupled with the outputs of the first stakeholder meeting in April, heightened awareness within the EMB that the IIP PMO was not functioning as efficiently as desired or at the level required. Immediate action was taken with the appointment of Dr Andrew Catto as the Senior Responsible Owner (SRO) for the whole of the IIP and the transfer from the Governance recovery programme of one of the interim resources to lead the IIP as Programme Director. To lead the reform and restructure of the PMO this task also included the development and publication of this IIP recovery document.The plans and processes described in this document are built around a tried and tested methodology with an identified recovery timeline based on a 30/60/90 day phasing which aligns perfectly with Mr Andrew Foster’s six delivery phrases.Note : One of the biggest challenges facing HEFT is the current structure of the divisions and the directorate structures which are diverse in both their management and governance processes; as well as their cultures which present a number of issues in their own right. This recovery plan does not seek to address the divisional structure as part of the IIP at this point in time. It is felt that evolution rather than revolution is all that we can really hope to achieve within the life cycle of the IIP. In the third week of April a decision was made to restructure the PMO see Fig 3 below, with administration and governance moving under the Interim DoF and Strategic direction and delivery moving to Dr Andrew Catto. Since this decision was made there have been a number of movements within the PMO itself with additional specialist resources being added to bolster the skills and expertise needed to ensure and assure delivery.
Head of PMO
Director of Finance and PerformanceDarren Cattell
Programme Director IIP
Project Manager - Support to Culture & Engagement
Programme Manager - Support to Governance
Project Manager - Mortality/Congestion
Seconded team from Deloitte
Project Manager - Support to Urgent Care
Band 2 Administrator - Vacant
Project Manager - Support to Planned Care
Project Manager IM&T
Figure 3 - PMO structure
Safe Effective Caring Responsive Well led
Page 8 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6

Council of GovernorsJune 2015
.138
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
Essentially each programme within the IIP will have a dedicated programme/project manager to provide support around change management techniques and processes and to provide support and rigour around the reporting requirements. The majority of these positions have been filled with existing personnel but we have also recruited a small number of additional subject matter experts to provide the necessary PMO management and leadership that is required. An additional Programme manager has been engaged to support the Governance programme and provide additional support to the PMO. A new Head of PMO will join the Trust on Thursday 21st of May. The following table provides detail on the current and near future manning arrangements available to the PMO:
Name Title Area of responsibility
Stuart A Brown IIP Programme Director IIP Programme
James Weller - joins 21/5 Head of PMO IIP PMO
Phill Wilson Project manager IIP Programme & Governance programme
Paul Arford Programme manager Urgent Care Programme
Lara Williams - joining date tbc
Project manager Mortality and Congestion
Vacant Project manager IM&T
Danielle Goddard Project manager Culture and Engagement
Name Title Area of responsibility
Change
Nick Varney Head of PMO and IIP
IIP Programmes Moves to Surgical reconfiguration
Keith Hawley Project manager Governance programme support and ad-hoc support as directed by Head
of PMO
Will leave the Trust on 11th of June or sooner if mutually
agreeable
Work commenced on the development of the narrative that describes the IIP and the delivery methodology on the 24th of April, in the form of a document Mind Map setting out the structure and content of the document. This was approved by the Deputy CEO and Interim DoF on the same day. The first draft of the narrative document was received at EMB the following week and then presented for discussion at the Trust Board on the 5th of May.
Safe Effective Caring Responsive Well led
Page 9 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6

Council of GovernorsJune 2015
.139
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Integrated Improvement Plan
The recovery plan is based on a 30/60/90 day plan, the following graphic Figure 4 describes the current status against that plan:
Improving
30
60
90
10
20
40
50 70
80
100
110 Cruis
ing
Pace
atta
ined
WARNING
Figure 4 - Recovery plan status
The 30/60/90 phases are described in full detail in the main body of the document in section 9.The programme gateway process has already begun with the support of Deloitte undertaking a programme delivery status assessment during the week commencing 11th of May 2015. The outcome of the assessment was in line with the internal assessments made by the SRO’s for the individual programmes.HEFT faces a significant se of challenges which it must overcome if we are to deliver the IIP on-time and within an agreed financial window. However there are a number of factors that bode well for the Trust in it’s quest to deliver the IIP:
• The Executive Leadership Team are totally committed to the delivery of the IIP and the determination to embed quality at every level of the organisation and make it a natural part of the “day job”;
• Engaging our staff,patients, commissioners and the wider health economy is at the center of our delivery strategy;
• We have a willing staff body who want to see change that genuinely improves patient care and staff wellbeing and want to play their part in delivering it;
• We have tangible hands on support from our regulator - they have provided access to best practice examples of “the way to do it” they have worked with us to engage constructively and beneficially with Deloitte’s and they have provided us with an Improvement Director who makes a positive contribution to our endeavors ;
Safe Effective Caring Responsive Well led
Page 10 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6

Council of GovernorsJune 2015
.140
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• We believe that the recent changes we have made to the structure and operating model of the PMO will now give us the drive and rigor that we need to deliver the IIP;
In conclusion, this is our plan and this is the journey we are committed to, we know we have a long way to go but we know we will achieve the desired outcomes and we know that patient care will be significantly improved as a result of HEFT completing this journey.
Andrew Foster - Interim CEO! ! Dr Andrew Catto - Deputy CEO
.............................................. ...................................................
Safe Effective Caring Responsive Well led
Page 11 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.141
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 2 - INTRODUCTION
Safe Effective Caring Responsive Well led
Page 12 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.142
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
2.INTRODUCTION
HEFT has been striving to drive a number of improvement programmes across the Trust in the areas of: Unscheduled care, Planned care , Governance - including performance, Mortality, Culture and engagement and IM&T. The set of programmes is the Integrated Improvement Plan (IIP).Having established a Programme Management Office (PMO) in January 2015 the Trust has made progress but it has lacked pace . Monitor, the Trust CEO and Executive Management Board (EMB) have expressed concerns about the format and quality of IIP reporting. Following a recent performance review with Monitor the Trust was asked to provide a comprehensive plan to get the IIP back on track as quickly as possible. The finalised plan will be presented to Monitor prior to May 20th 2015.
2.1.PURPOSE OF THIS DOCUMENT
This document details the narrative, proposed IIP plans, governance arrangements and programme and high level project interdependencies for the recovery of the portfolio of programmes comprising HEFT’s Integrated Improvement Programme – the IIP. (see Figure 5 below). The IIP articulates six specific programmes of work that are required to ensure the programme(s) are on track and maintaining traction and pace at a time of significant pressure for HEFT. The ultimate aim of the IIP is to deliver sustained change, by an engaged workforce, committed to improving high quality embedded care delivery.
Scheduled Care Governance Urgent Care IM&T Mortality Cultures & Engagement
Integrated Improvement Portfolio
TRUST Board
The IIP Programme Boardis ultimately Accountable (via the Executive Management Board to Trust Board
Fig 5 - The Integrated Improvement Programme(IIP)
The purpose of this document is to provide the Board of Directors, Regulators and stakeholders with the assurance on delivery. Assurance by clearly articulating the detail of the HEFT improvement plans, improvement metrics and the timeline for delivery.
Safe Effective Caring Responsive Well led
Page 13 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.143
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
This document:
• describes the corporate Programme and Project Management (PPM) function, its role, responsibilities and relationships. PPM will be used extensively to support operational and corporate teams with delivery and also serve as robust assurance function. It is important to acknowledge that operational teams are responsible for the delivery of the IIP, not the PMO;
• lays firm foundations for multi programme delivery, communication, assurance and future reviews; and
• provides the basis for developing more detailed plans, and for considering how other initiatives relate to corporate PPM, so that current and future activities across HEFT can be aligned to maximum effect to support the delivery of HEFT’s strategic objectives. Ultimately this plan will be aligned to the Trust’s suite of strategies in September 2015.
2.2.CONTEXT2.2.1.Heart of England NHS Foundation Trust (HEFT)
Heart of England NHS Foundation Trust (HEFT) regulatory and quality chronologyIn July 2013 the Care Quality Commission announced that HEFT would be one of the 18 first wave Trusts to be inspected by a more robust new style inspection. At that time, HEFT was considered neither low nor high risk but a ‘variety of risk points’[Ref: http://www.cqc.org.uk/content/cqc%E2%80%99s-new-hospital-inspection-programme-start-tomorrow]. However, HEFT had been subject to registration conditions by the CQC when in April 2010 the regulator registered HEFT on condition it made improvements to three essential standards of care when it introduced a new registration system for all health and adult social care services. Two conditions were removed in October 2010 and the final condition in February 2011. HEFT underwent a further unannounced 3 day inspection in December 2014, the findings from which have now been received from the CQC and published on the CQC website2.The current overall status of HEFT as assessed by the CQC is: Requires improvement. [ref: http://www.cqc.org.uk/provider/RR1]In December 2013 HEFT was one of thirteen hospital trusts named by Dr Foster Intelligence (DFI) as having higher than expected higher mortality indicator scores for the period April 2012 to March 2013 in their Hospital Guide 2013.[4] although based on the Health and Social Care Information Centre (HSCIC)[ref http://www.hscic.gov.uk/] HEFT mortality was at the upper limit of expected. The principle reason for the difference being the statistical methodology adopted by DFI and HSCIC.In June 2014 Mr. Les Lawrence was appointed as the new Chairman succeeding Lord Hunt. In July 2014, NHSE in discussion with key Trust stakeholders, held a risk summit that focussed on key quality risks and performance concerns. The resulting action plan
Safe Effective Caring Responsive Well led
Page 14 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
2 The resultant action plans do not form part of this narrative at this point in time but will do in future iterations
Integrated Improvement Plan

Council of GovernorsJune 2015
.144
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
was monitored by the unusual step of HEFT attending meetings of the NHSE quality summit. HEFT was represented by the Chief Nurse and Executive Medical Director, ensuring that a strong focus on quality was maintained.Dr Mark Newbold resigned as Chief Executive in November 2014 after HEFT had a condition placed on its license by Monitor on 21 October 2014 relating to performance , governance and mortality. Dr Andrew Catto was appointed interim Chief Executive until 16th February 2015 when he was succeeded by Mr Andrew Foster as Interim Chief Executive. Following Dr Newbold's resignation, a number of changes were made at Executive Director level with the appointment of external interim Directors of Finance and IM&T. The Director of Patient Experience and External Affairs left HEFT in March 2015. The then interim CEO Dr Catto, with the support of the Board of Directors, developed an integrated leadership support and resilience programme (LSRP) between December 2014 and February 2015. The key programmes in the LSRP, which was presented to Monitor, key stakeholders and national clinical leaders, comprised the 7 work streams of governance, mortality / congestion, culture / engagement, safe staffing, IM&T /PMS2, performance and executive leadership.The LSRP evolved into the current pyramid of priorities (see Fig 6 below) developed by Mr Andrew Foster.
4"
Recovery
1. Clarity (Governance & Strategy)
2. Quality Improvement 3. Staff Engagement
Internal Communications Board Development
Management Capacity Stakeholder Relationship
Safe Staffing ICT Investment
Estates Investment Mortality Reduction
Deloitte Governance Plan Monitor Enforcement Undertakings
• A&E • RTT
• Scheduled Care • Cancer
CQC Recommendations Kennedy Report Silverman Report
The$Pyramid$of$Priori.es$$
Safe Effective Caring Responsive Well led
Page 15 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.145
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Fig 6
The CEO Andrew Foster and executive team are focussed on 3 high level deliverables see Figure 7 below:
CLARITYCULTURE
&ENGAGEMENT
QUALITY
Fig 7 - High level deliverables
In April 2015, a new stakeholder group was established comprising the HEFT executive team, NHS England, Lead CCGs, Monitor and the CQC. This innovative approach, supported by the Monitor Director of Improvement replaced the QSG. 2.2.2.The IIP in the context of the National Picture
The healthcare system is facing very significant care delivery changes and enduring financial pressures. With an ageing population, people are living longer with more complex health needs and often multi-morbidity, therefore the need for services will continue to grow faster than funding, meaning that the NHS and social care must innovate and transform service delivery, within the resources available, ensuring that patients, and their needs, are always put first. The planning guidance establishes key criteria:• Strategic plans covering a five year period, with first two years at operating plan level• An outcomes focused approach, with stretching local ambitions expected of
commissioners, alongside credible and costed plans to deliver them• Citizen inclusion and empowerment to focus on what patients want and need• More integration between providers and commissioners• More integration with social care – cooperation with Local Authorities on Better Care
Fund planning • Plans must be explicit in dealing with the financial gap and risk and mitigation
strategies. - No change not an option
It should also be noted that Acute Service providers have been under significant operational pressures for sustained periods of time, in some case providers have not seen the expected seasonal drops in emergency activity since the Winter of 20113/14. This has resulted in adverse publicity for some Trusts and for the wider NHS as a whole.Also at the time of writing and publication of this document the General Election is fast approaching so focus and publicity around the NHS is at a heightened level.
Safe Effective Caring Responsive Well led
Page 16 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.146
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
2.2.3.NHS Outcomes Framework
Clinical outcomes are of key importance to patients and the Department of Health published a refreshed iteration of its NHS outcomes framework for 2015/16 [ref https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/385749/NHS_Outcomes_Framework.pdf]. The Outcomes Framework comprises 5 domains: • Preventing people from dying prematurely• Enhancing quality of life for people with long-term 2 conditions• Helping people to recover from episodes of ill health or following injury• Ensuring that people have a positive experience of care• Treating and caring for people in a safe environment and 5 protecting them from
avoidable harmThese 5 outcomes are aligned to the development of the HEFT clinical strategy. 2.2.4.The IIP in the context of the Local Health Economy
HEFT serves a diverse range of communities in Birmingham East and North, Solihull, Sutton Coldfield and South Staffordshire; with up to 1.2 million people visiting HEFT every year and a base commissioning population of over 1 million people. A number of these populations have significantly challenging health needs. All CCG’s are supported by and provided with extensive access to a number of tools to inform their planning and commissioning intentions - PHE CCG Outcomes benchmarking support packs http://www.england.nhs.uk/la-ccg-data/#ccg-info]. HEFT predominantly serves three Clinical Commissioning Groups (CCG’s) : Birmingham Cross City , Sandwell and West Birmingham CCG and Solihull CCG , with a combined population catchment area of circa 1 400 000. However all in all there are 10 commissioning bodies that purchase services from HEFT at the following levels:
• NHS Birmingham Cross City CCG £231.5M• NHS Birmingham South And Central CCG £14.7M• NHS Sandwell And West Birmingham CCG £8.0M• NHS Solihull CCG £134.6M• NHS South East Staffs And Seisdon Peninsular CCG £33.5M• NHS Walsall CCG £6.2M• NHS Warwickshire North CCG £6.3M• Birmingham and the Black Country Area Team £112.6M• Health Education England £23M• Birmingham City Council £7.0M
Safe Effective Caring Responsive Well led
Page 17 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.147
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Five year key priorities for each the lead CCGs are as follows:
Key Priorities Solihull CCG
Birmingham Cross City
CCG
Sandwell and West
Birmingham CCG
Preventing illness, Improving Health Programme X
High quality primary care X X X
Better community provision X X X
Whole system approach - i.e. Your Care Connected (Joint commissioning) X X X
Commissioning elective care based on achieving better outcomes from interventions
X X
Urgent Care X X
Hospital transformation/Outpatient transformation X X
Mental Health - high quality and responsive X X
Children's and maternity services X
Preventing readmissions X
Long term conditions X
Intermediate care X
Stroke services X
Pathway management X
Effectiveness review X
HEFT has developed an excellent working relationship with commissioners and local authority partners in the delivery of the Better Care Funds (BCF) in Birmingham and Solihull with senior executive representation on BCF Boards. Regular dialogue between HEFT and Solihull / Birmingham Cross City CCGs established as an action of the quality summit ensures close dialogue between the very senior leaders.
Safe Effective Caring Responsive Well led
Page 18 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.148
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
2.2.5.The IIP in the context of The Divisional Landscape
the following points provide a high level summary of the Divisional position in relations to the IIP:• The clinical services are delivered through 5 clinical divisions ( 3 site based, 2 specialty
based ) supported by 27 directorates• The management teams at division and directorate level are formed by a triumvirate
model ( doctor, nurse and manager ) • A mixture of site specific and cross site specialties/directorates• The Trust is failing across a range of key performance indicators and is under scrutiny
by the regulators• Significant additional corporate management support recently introduced to improve
performance• An Executive view that HEFT needs to become a highly devolved clinical led,
organisationSo this poses the question - What should good look like in a clinically led, management supported devolved division?• They should have a written plan setting out service priorities, key objectives,
timescales and leads;• A clear structure supported with roles and responsibilities;• Clear decision making arrangements with responsibilities and authority set out. As a
minimum a formal divisional board with recorded agreements;• Performance management framework at team and individual level;• Intelligent use of KPI’s supported with improvement/change capabilities;• Staff comms and engagement processes;• High quality leadership distributed and every level ( ward to board);• Effective relationships with key stakeholders ( executives, other divisions and CCG’s );• A distinctive culture characterised by positive behaviors, clinical leadership, drive for
quality and a common purpose.Why would you need good clinical leadership?Good hospitals are run by good strong clinical leadership which empowers clinicians but also makes them accountable (See Fig 8 - Driving clinical leadership) and HEFT is no different in their aspiration to become a “beacon” for clinical leadership. However HEFT also recognises that we are have some way to go before we can be recognised as having that characteristic. The current divisional and directorate structure presents a number of complex challenges for the senior management team of HEFT which question the long term viability of the
Safe Effective Caring Responsive Well led
Page 19 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.149
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
current model which is based on site primacy. Many of the directorates operate with different management models which increases the level of complexity.
Clinical decisions impact
on the use of resources
Clinicians know how to cut costs
effectively
Clinicians deliver the patient experience
Clinicians deliverclinically effective
interventionsClinicians deliver
patient safety
Clinicians know where the waste is (productivity)
Most clinicians want to do it
better
Clinical Traction
Fig 8 - Driving clinical leadership
The Executive team have recognised the need to make some tactical changes in order to bring about some improvements in the current operating model (COM), now is not the time for a radical restructure of the COM and it may be some time before the optimum conditions for radical restructuring exist. They have also recognised that the COM represents a not inconsiderable risk to the overall delivery of the IIP. Some of the characteristics of the COM are manifest in some of the things that have been observed during a recent piece of work that was commissioned by Andrew Foster Divisions believe they have lost the right to manage their own business ( eg interim support, PMO, improvement boards etc) :• There is a lack of clarity on roles responsibilities boundaries and accountability across
sites and specialities; • General/Senior Management -sufficient capacity was observed at appropriate grade
mix with varying capability;• Managers at all tiers were working at levels below what was required;• Varying degrees of clinical leadership is in place;• The divisions do not have meaningful engagement with each other; • There appears to be a lack of synergy between divisions in the pursuit of corporate
objectives ( strong silo working ); • There are significant differences in the way the divisions operate but there is a lot of
problem processing and blaming others and not enough drive for change and improvement;
• Bidding for resources to solve problems is the starting point;• Getting to the reality has been a challenge.
Safe Effective Caring Responsive Well led
Page 20 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.150
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
As mentioned above there needs to be some tactical changes to the COM and as we said this means that the issues identified in this analysis are key to delivery and is underpinned by a combination of cultural, process and structural issues. The recent clarity that the Associate Medical Director (AMD) is the divisional accountable officer is an important starting point. In addition to the engagement events held with staff, the next key engagement opportunity is for EMB (attended by all AMDs) to receive the analysis and agree a shared way forwards. This will be held on 5th May 2015. 2.2.6.The IIP in the context of individual HEFT staff members - Staff Engagement
The staff at HEFT are our biggest and most valuable asset. Without a strong, committed and well -motivated workforce we will not, despite our best intentions, deliver the level of service that we aspire to or the patient experience and level of care that our patients deserve. Furthermore, it has long been recognised that engagement of employees with their work and organisation is a factor in their job performance, but the research evidence has been steadily increasing over recent years. West and colleagues have carefully studied the relationship between employee engagement and a variety of individual and organisational outcome measures, including staff absenteeism and turnover, patient satisfaction and mortality, and safety measures, including infection rates. [Ref West http://www.kingsfund.org.uk/sites/files/kf/employee-engagement-nhs-performance-west-dawson-leadership-review2012-paper.pdf] Culture and Engagement is a crucial, pivotal IIP programme in the IIP Portfolio. For the Culture & Engagement programme, the objectives are to develop a working environment in which staff feel significantly more engaged, and to reap the benefits of the associated improvements in performance and patient outcomes. This will be achieved by introducing a more structured approach to staff engagement, including senior team led large scale listening events, strong governance around how feedback is turned into action, and the introduction of the more locally focused Engaging Teams Programme, to build sustainable skills and capability across our teams.A programme of Listening Events has commenced across the 3 main sites and ‘you said – we did’ feedback to staff is evident throughout the Trust. Focussed listening sessions have been held in high clinical risk areas such as the Emergency Department (ED) .
2.3.BACKGROUND
The need to develop and deliver a robust well managed IIP spans a period of least three years during which a number of reviews and interventions have highlighted a number of quality, performance, engagement and governance concerns about HEFT. The concerns are not specific to one site or HEFT department, as they sit across a broad range of clinical services, subject matter and impact on all sites. In addition, the Deloitte review of governance identified the absence of Programme Management methodology throughout HEFT as a major shortcoming. A PMO at HEFT was developed using interim staff in late January 2015 and additional expertise was identified in early April 2015 to
Safe Effective Caring Responsive Well led
Page 21 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.151
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
facilitate the development of the PMO into supporting the delivery a robust IIP methodology. Expert subject reviews by the Emergency Care Intensive Support Team (ECIST), Mr Stan Silverman FRCS, Deloitte - CQC as part of their previous standard inspection regime and more latterly under the new CQC Enhanced inspection regime. This led, in part, to further Monitor intervention and the issuing of Monitor Undertakings. The Silverman report, commissioned by the Executive Medical Director (delivered 29th September 2014) reached the following important conclusions:The Board of the Heart of England FT receive only partial assurance in regard to mortality as reports are based largely on information derived from coding data. The Board is uninformed about the potential shortfalls in care that might be revealed through structured review of all deaths.There is potential to vastly increase knowledge about safety and risk through the incident reporting system which currently appears to be suboptimal.There is a lack of compliance with guidance on best clinical practice in HEFT.Clinical staff are under severe pressure, morale is poor, and engagement is poor.Multidisciplinary working and good team working are poorly developed. Silo working is widespread.Clinical congestion is likely to be the biggest factor in causing raised mortality indicators. This can be addressed to a large extent by transforming clinical practice. The HEFT executive has focused on clinical congestion as the greatest threat to the delivery of safe care in the Emergency Department and this IIP has a strong focus on this key quality risk. We have triangulated these outcomes with other expert reviews and reports such as IST/ECIST, and the Deloitte Governance Review. Whilst they carry specific recommendations on leadership, board assurance and risk management, there is a common narrative considering they have been conducted independently.2.3.1. Monitor Undertakings
As HEFT’s regulator Monitor have a duty to provide assurance to the Secretary of State (SoS) for Health about the safety and financial viability of HEFT. The following undertakings represent the action that Monitor have agreed to take in order to provide that assurance. What is obvious from the timelines against the specific actions and milestones is that HEFT have not been able to meet Monitors expectations and assurance given to the SoS. This is further evidence of the need for this recovery plan.BACKGROUND: PREVIOUS AND CURRENT REGULATORY ACTIONMonitor accepted enforcement undertakings under section 106 of the Health and Social Care Act ("the Act") from the Licensee on 20 December 2013 in relation to the Licensee's governance arrangements for urgent care. Monitor then accepted amendments to those undertakings on 21 October 2014, which were made following breaches of additional access and outcome performance indicators. These are referred to collectively as the
Safe Effective Caring Responsive Well led
Page 22 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.152
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
"existing undertakings". The undertakings (detailed in the Appendices) relate to breaches of the additional licence condition imposed under section 111 of the Acton 21 October 2014 ("the additional condition") and the broader governance conditions of the licence, and are without prejudice to the existing undertakings. The additional condition requires the Licensee to ensure that it has in place sufficient and effective Board, management and clinical leadership capacity and capability, as well as appropriate governance systems and processes.Full details of the Monitor Undertakings are contained in the appendices in Appendix V.
2.4.SPONSORSHIP OF THE INTEGRATED IMPROVEMENT PORTFOLIOOwnership and strategic direction of the IIP sits with the Deputy Chief Executive, and the collective responsibility for the delivery and the sustainability of the changes arising from this programme resides with the Executive Management Board and the Board of Directors.Monitor and The Care Quality Commission (CQC) will receive assurance from HEFT on the progress of IIP via the monthly external stakeholder group and secure evidence that HEFT remains financially viable and delivering safe care throughout the period of change implementation and beyond.
2.5.KEY PRIORITIES AND TIMELINES
There are six stages to the development and delivery of the IIP, Fig 9 below describes the six stage maturity model. (also appears in the Exec Summary)
Feb to April 2015.Creation of The Plan - conceptually based on the original January 2015 Leadership and Resilience Plan. Limited PMO capacity initially arising from simultaneous focus on establishing the Programme Office and running several other improvement programmes synchronously.
Clear Executive Leadership. Deputy CEO manages and assure the Plan. Interim DoF manages the timeliness and quality of submission. Supported by very experienced Programme Manager, Stuart Brown. Focused one week piece of work commissioned from Deloitte to align the dashboard metrics with the IIP.
1 2 3
4 5 6
Creating the Narrative – From the Deloitte Governance Report to the Resilience Plan to the Pyramid of Priorities to the IIP and Dashboard.
IIP is perceived as centre stage in the organisation - with buy-in from the Board, CoG and external stakeholders.
Introducing a Layered Approach to presentation and implementation so that the IIP can be seen in a national context, at full Trust level, at site, at service and down to the individual member of staff.
The IIP and our suite of strategies merge and become the entire plan enabling us to shift from back foot to front foot in September 2015.
Fig 9- IIP Six Stage Maturity Model
Safe Effective Caring Responsive Well led
Page 23 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.153
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Monitor have formally expressed concerns regarding progress to date on the IIP. (Andrew Foster has received a formal letter from Monitor expressing their concern around the progress of the IIP and it’s reporting architecture). There is specific concern that the presentation and content of the IIP thus far requires further development. This is acknowledged by the executive team and this document,along with other decisive action, will add traction to the delivery of the IIP and support the implementation of stage 5 of this process namely that the IIP is perceived as centre stage.The first iteration of this document and the high level plan metrics were received at EMB on 29th April and the first meeting of the IIP programme board was held on 29th April 2015.The draft IIP and metrics will be received at the Board of Directors on 5th May 2015.It is stressed that the IIP is a live document that will continue to evolve up to the stakeholder meeting when the final definitive version 1.0 will be published.
2.6.THE 30 DAY CHALLENGE - GETTING BACK ON TRACKThe next 30 days are a critical period for HEFT, a period where we have to demonstrate to the BoD, Monitor and the commissioners that the IIP has the required traction and pace to provide the required level of assurance. During this period we will be implementing the following actions:Additional skilled resources will be added to the PMO to provide additional support to the programmes that sit on the critical path;All programmes will be scheduled to undergo a rigorous Gateway review to assess their capability to deliver against the current agreed timelines. If it is determined that the delivery schedule is at risk a recovery action plan will be developed and implemented;
Safe Effective Caring Responsive Well led
Page 24 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.154
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 3- VISION & OBJECTIVES
Safe Effective Caring Responsive Well led
Page 25 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.155
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
3.VISION AND OBJECTIVES
3.1.VISION
The HEFT 2020 Vision consists of the clinical strategy, quality strategy, quality improvement strategy and corporate strategy, supported by strategies for IT, HR and business. Each of the divisions will subsequently produce a strategic portfolio adding local detail to the Vision and their strategic deployment plans.
3.2.OBJECTIVESOur key objectives are to:
• Improve the quality of care, including the outcomes, the safety and the experience for all ;
• Engage with patients, carers, staff, our community, stakeholders and partners to redesign our services to provide improved access to services at the right time in the right place;
• Innovate and research new treatments and new ways of delivering care.
In five years time
Heartlands will be the centre for complex and emergency care. Based in the heart of the East
Birmingham community it has facilities which mean we can provide leading edge clinical services, some
of which have a national reputation. By concentrating some specialist care we will provide
the best outcomes and care.
Good Hope will continue to provide a full acute and emergency medical service. The recent investment in the new A&E department means it has a strong and sustainable future to manage this workload to
high standards. Over time the hospital will undertake less emergency surgery but will be home to some
surgical specialties, many of which serve a regional population.
Solihull Hospital and Community Services will become the centre of an integrated care system. For patients this means that their health and social care services will be aligned and integrated around their
individual needs. This is important since many of the patients at Solihull are elderly and the hospital care is often only one part of an overall package of care
and support they are receiving.It is planned that Solihull will have an urgent care facility which will be closely linked to primary care. The Hospital will continue to provide acute care but closely linked to the specialist centre at Heartlands.
Heart of England run community services in Solihull providing a wide range of support to people of all
ages.In Solihull we are already developing plans to bring together a wide range of public sector services. This will include “one stop shops” where people can seek help relating not just to their health but also for their overall well being, including leisure services, local
safety, finance and council services.In the future we will deliver more care in peoples’
homes and in community facilities across all of our catchment area and will work more closely with
partners so that our patients and their carers see all their care needs are joined up with less handovers
between individuals and organisations
Fig 10 - 5 Year aspiration
Safe Effective Caring Responsive Well led
Page 26 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.156
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 4-PROGRAMME MANAGEMENT AND PMO
Safe Effective Caring Responsive Well led
Page 27 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.157
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
4.PROGRAMME MANAGEMENT & PMO
HEFT made a conscious decision in the third quarter to adopt a programme management approach and establish a fully functioning effective programme management office (PMO). The effectiveness and influence of the PMO to date has been variable. Confidence in the delivery of the programmes that make up the IIP now needs to move to the next level in order to provide Monitor, The Board and Commissioners with the level of assurance that they require. Based on this analysis HEFT is recruiting additional resources with an enhanced level of capability to provide the necessary skill mix and capacity to provide the drive delivery and provide the assurance required.
4.1.STRUCTURE OF THE IIP
Programme DirectorScheduled Care - Amanda Markell
UC Work Streams
Scheduled Care Work Streams
IM&T Work Streams
Mortality Work Streams
GRP Work Streams
PMO Rigour“Light touch”
PMO Rigour“Light touch”
PMO RigourLight touch
PMO Rigour“Light touch”
Work StreamLeadsClinical
Champion
Project manager
Work StreamLead
Clinical Champion
Project manager
Work StreamLead
Clinical Champion
Project manager
Programme DirectorGovernance - Angela
Hopper
Programme BoardGovernance
SROProgramme BoardScheduled Care
SRO
Tight knit Teams that
“Hunt as a Pack”Work at Pace
& Deliver on time!
Tight knit Teams that
transfer skills andKnowledge
& Deliver on time!
IIP Programme Board
Executive Management Board
SRO
ProgrammeDirector
Programme Board - Urgent Care
SRO
Programme DirectorUC - Andrew Stenton
ProgrammeBoardIM&T
SRO
Programme DirectorIM&T - Caroline Sadler
Programme BoardMortality
SRO
Work StreamLead
Clinical Champion
Project manager
Work StreamLead
Clinical Champion
Project manager
Programme DirectorMortality - Ann Keogh
PMO Rigour“Light touch”
PMO Rigour“Light touch”
ProgrammeBoardCultures & Behaviors
SRO
Programme DirectorCultures &
Engagement - Alex Covey
Cultures & Engagement Work Streams
Work StreamLead
Clinical Champion
Project manager
PMO Support & Delivery Resources
Fig 11 - IIP Structure
4.1.1.Matrix working
Managing the interdependencies within a programme of this size and complexity is challenging, with plenty of opportunities for silo working and duplication of effort. Individual Programme Directors and Work Stream leads will need to work effectively to mitigate any risk of this happening.
Safe Effective Caring Responsive Well led
Page 28 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.158
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
The programme directors for each of the constituent IIP programmes will meet regularly with the IIP Programme Director, weekly for the next 30 days and fortnightly thereafter to review progress and resolve any interdependency issues 4.1.2.Personnel
In the third week of April a decision was made to restructure the PMO see Fig 12 below, with administration and governance moving under the Interim DoF and Strategic direction and delivery moving to Dr Andrew Catto.
Head of PMO
Director of Finance and PerformanceDarren Cattell
Programme Director IIP
Project Manager - Support to Culture & Engagement
Programme Manager - Support to Governance
Project Manager - Mortality/Congestion
Seconded team from Deloitte
Project Manager - Support to Urgent Care
Band 2 Administrator - Vacant
Project Manager - Support to Planned Care
Project Manager IM&T
Figure 12 - PMO Structure
Since this decision was made there have been a number of movements within the PMO itself with additional specialist resources being added to bolster the skills and expertise needed to ensure and assure delivery. The following table describes the current manning levels of the PMO, this may be subject to change and additions as the requirements become clearer over the coming weeks.
Name Title Area of responsibility
Stuart A BRown IIP Programme Director IIP Programme
James Weller - joins 21/5 Head of PMO IIP PMO
Phill Wilson Project Manager IIP Programme & Governance programme
Paul Arford Programme Manager Urgent Care Programme
Lara Williams - joining date tbc
Project manager Mortality and Congestion
Vacant Project manager IM&T
Danielle Goddard Project manager Culture and Engagement
The following table details the movements out of the PMO:
Safe Effective Caring Responsive Well led
Page 29 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.159
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Name Title Area of responsibility
Change
Nick Varney Head of PMO and IIP
IIP Programmes Moves to Surgical reconfiguration
Keith Hawley Project manager Governance programme support and ad-hoc support as directed by Head
of PMO
Will leave the Trust on 11th of June or sooner if mutually
agreeable
4.1.3.Corporate Fit
The PMO is directly accountable to the Deputy Chief Executive for the full scope of the IIP and is also accountable to the Director of Finance for the performance and finance element of all programmes.
4.2.APPROACH4.2.1.Assurance role
A programme assurance role is a very different model to the delivery driver model and requires different skill mixes and styles. The assurance roles is to all intents and purposes a very light touch review and report type approach and is not designed to provide intense challenge or roll your sleeves up support. The skill mix for an assurance PMO is generally fulfilled by staff that do not necessarily have subject matter expertise but do have the necessary programme management process knowledge and capability. 4.2.2.Delivery Driver
This role is much more focussed on tangible support to the projects and work streams and is usually staffed by personnel with a mixture of programme management skills and subject matter knowledge and capability in order to provide hands on support to projects and where necessary to offer leadership expertise to help remove blockages if required.
4.3.METHODOLOGYThe PMO will follow the standard Managing Successful Programmes (MSP) framework and the Prince2 frameworks originally developed by the Office of Government Commerce (OGC). This will ensure that we are following a consistent approach to programmes and projects and that an assurance regime is naturally embedded in the process.
Define Develop DeliverAssure
Fig 13 - Managing Successful Programmes
Safe Effective Caring Responsive Well led
Page 30 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.160
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
4.4.PMO TOOLS 4.4.1.New Programme and Project Development
Each time a new programme or project is required it will follow a clearly defined development process, that addresses the key stages of a project - a copy of these stages can be found in the appendices in Appendix II 4.4.2.Software
The PMO is currently using a combination of Microsoft office applications to track and manage the IIP and constituent programmes which is both clunky and does not provide the opportunity for “real time” management and update - it also makes version control somewhat more challenging.A number of web based products are available such as Share point, PM3, Smartsheet, Basecamp - at very competitive prices. Packages.A brief review process will be undertaken as part of the “The 30 day challenge” to select the most suitable and user friendly package to provide a constructive and un-intrusive PMO tool that is capable of delivering the appropriate level of reporting direct to the relevant recipients i.e members of the Executive Management Board (EMB), Programme Directors, etc,etc. 4.4.3.Lean/Kaizen
Lean and Kaizen are proven methodologies for designing, developing and implementing change.Where appropriate we will use Lean methodology to effect and deliver change and we will use Kaizen events to implement those changes.4.4.4. PMO Templates
The PMO will be introducing additional/replacement templates into the PMO suite of documents that are designed to streamline the processes and improve efficiency whilst at the same time reducing the level of complexity and time required to complete the various documents.The document suite will include the following standard templates3:Programme/Project/Work stream Unique Identification Number (UIN) Reference tableBecause of the number of different reviews and reports that inform the IIP we currently have a plethora of different cross references within the various programmes. From the 1st of May we will initiate a revised Programme UIN system - this will be a HEFT generated UIN system.
Safe Effective Caring Responsive Well led
Page 31 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
3 Samples of which can be found in the appendices
Integrated Improvement Plan

Council of GovernorsJune 2015
.161
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
So that we do not lose the various threads of the individual reviews and reports from Deloitte, Silverman, Monitor, CQC, etc we will produce a PMO document that cross references the links from the IIP UIN system and these reports/reviews. This will be known as the Book of Reference (BR) Project status report (PSR)
A one side of A4 that describes the progress against predetermined milestones and timelines, reports risk status, reports any issues and describes the activity for the next period;Highlight report -
A more detailed report that can be used to appraise EMB of progress and outcomes to date.Master Risk register & Programme risk registers
Records risks, issues, opportunities, actions, dependencies, decisions and lessons learned.The IIP Master Risk log will feed into the Trust Strategic Risk Register/LogException report ;
Describes a situation where the programme or project has deviated against time, cost, resource or quality tolerances. The exception report asks the Programme Board to:
• Approve or reject the situation; • Defer making a decision until later; • Request more information; • Make a concession for the project manager to proceed without the need for any
corrective action;• Instruct the project manager to resolve the problem; • Give advice and guidance to the project manager; • Request an exception plan based on one of the options (theirs or the project
manager’s); • Seek advice and guidance from corporate or programme management ;or • Instruct that the project be prematurely closed.Change control form
A change request is a formal proposal for an alteration to some product or system relating to the programme or individual project/work stream. The IIP Change Control Form is aligned to the process described in Fig 14 below.It is the work steam lead’s responsibility to raise a change form as soon as it becomes evident that a deviation from scope is required and/or inevitable. Scope changes must follow the agreed change process so programme directors must ensure that the work stream leads act in a timely manner.
Safe Effective Caring Responsive Well led
Page 32 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.162
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Work stream/Project identifies need to deviate from the work
plan
Change is determined as
Legitimate
Change requestrejected
NO
Change is determined as
Material
Programme Lead and Executive Lead determine whether the change is material:
Materiality defined as one or other of:Extends timeline and impacts critical path
Impacts other ProgrammesImpacts the final output?
Change request
approved
NO
ProgrammeBoard
ConsidersYES Change is
implementedAPPROVES
RISK REVIEW &
MITIGATION PLANNING
REJECTS
Change Control Process
Fig 14 - IIP Change control process
4.5.MANAGING INTERDEPENDENCIESManaging interdependencies is a critical success factor for both the individual programmes and projects and the overarching IIP itself. As part of the Gateway review process a thorough analysis of the interdependencies will be undertaken using a workshop environment. Once we have clarity on the links and the potential impacts they will be managed via the matrix working arrangements described in 4.1.1We will also consider using a technique called Outcome relationship mapping, Outcome Relationship Mapping is a simple but powerful technique for exploring complex changes by identifying and analysing the potential impacts in other areas that would be affected by the change(s) which any organisation is seeking to implement - both internal and external to the organisation. Outcome relationship mapping can also be used to help:• Clarify policy/strategy effects, gaps, overlaps & contradictions• Strategic scoping & prioritisation• Planning and the setting up of portfolios, programmes and projects• Look for strategic risks (barriers, problems of success and associated risks)• Evaluation, identification of measures and targets & learning lessons• Communicate the vision
Safe Effective Caring Responsive Well led
Page 33 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.163
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Define organisation and programme structures and identify relationships between teams, programmes & projects
• Stocktaking existing initiatives • Benefits realisation planning• Business Case developmentAn example of an Outcome relationship map can be found in the appendices in Appendix III
4.6.BENEFITS MANAGEMENT AND REALISATIONEach work stream must develop a benefits map and a benefits management and realisation plan. A benefit profile must contain as a minimum:• Benefit owner;• Description of the benefit;• Related issues and risks to the full realisation of the benefit;• Financial profile of the benefit;• Any dependencies on other programmes or projects outside the boundary of the parent
programme that the benefit realisation relies on;• Details of the beneficiary i..e Patient, Staff, Infrastructure, Quality & Safety;• Evidence that demonstrates when the benefit has been realised;• Other benefits that this benefit contributes to.
4.7.WHAT DOES GOOD LOOK LIKE? This defines what a successful PMO and Programme management function looks like, so we will measure the success of the PMO and Programme Director on the following key criteria:• On time performance of all constituent programmes and projects;• Delivery of programmes and projects within the agreed budgets;• On time performance of reporting timescales;• BRAG ratings are performing as expected;• Programme temperature - EMB, Trust Board and Monitor have confidence in the PMO
and Programme Director that the IIP is maintaining the desired momentum or exceeding expectations.
Safe Effective Caring Responsive Well led
Page 34 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.164
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 5- METRICS
Safe Effective Caring Responsive Well led
Page 35 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.165
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
5.METRICS
The Trust have commissioned Deloitte's to work with us to develop the metrics that will be used to track progress of the IIP and its constituent programmes and projects. Where possible and practical we will be using both a leading KPI and a Lagging KPI for all the metrics we have agreed with Deloitte's and the Programme Executive leads (SRO’s) and the individual Programme Directors.5.1.Metrics
Individual programmes have a newly developed, in collaboration with Deloitte’s, set of metrics that will measure their progress against their key milestones and objectives. The specific metrics which have been developed for each individual IIP programme are contained in a separate document - IIP Dashboard. An image of the dashboard is contained in the appendices of this document in Appendix IV. The PMO will also provide reports against standard PMO disciplines, 5.2.Reporting Timetable
Each work stream will be required to complete a weekly PSR4 for the PMO and a comprehensive monthly Highlight report.Programme level reports will be required in accordance with the table shown below in 4.3.1 5.3.Reporting To Who
5.3.1. Monitor
IIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - Monthly
Individual IIP programme updates to
be provided by 5th working day
Updates to be collated and circulated by 8th working
day
IIP-3rd Monday of month for assurance
EMB- 3rd Tuesday of
month for final sign off
Submit to Monitor - 3rd Thursday of the month
May 08 - May 15 - May 18 - May 19 - May 21 - May
June 05 - June 12 - June 16 - June 17 - June 18 - June
July 07 - July 14 - July 20 - July 21 - July 22 - July
Aug 07 - Aug 12 - Aug 17 - Aug 18 - Aug 20 - Aug
Sept 07 - Sept 10 - Sept 14 - Sept 15 - Sept 17 - Sept
Safe Effective Caring Responsive Well led
Page 36 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
4 the latest copy of each PSR will be made available for the fortnightly EMB meetings
Integrated Improvement Plan

Council of GovernorsJune 2015
.166
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
IIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - MonthlyIIP Reporting Timeline - Monthly
Oct 07 - Oct 12 - Oct 19 - Oct 20 - Oct 22 - Oct
Nov 06 - Oct 11 - Nov 16 - Nov 17 - Nov 19 - Nov
Dec 07 - Dec 10 - Dec 14 - Dec 15 - Dec 17 - Dec
5.3.2. NHSE, CCG’s and Local authorities
Should the CCG’s and Local Authorities require formal reporting of HEFT’s IIP then the reports will be provided in accordance with the Monitor reporting timeline as shown in 4.3.15.3.3.Internal
See 4. 2 and 4.3.1
Safe Effective Caring Responsive Well led
Page 37 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.167
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 6- PROGRAMME PROFILES
Safe Effective Caring Responsive Well led
Page 38 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.168
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.PROGRAMME PROFILES
6.1.GOVERNANCE RECOVERY PROGRAMMEBackground:
In 2014 Deloitte were commissioned to undertake an independent review of Governance arrangements at Heart of England NHS Foundation Trust against Monitors’ well-led framework for governance reviews. The final report was published in October 2014. Throughout the review a number of significant governance concerns were noted:• Lack of plans to support the implementation of the trust wide strategy – such as a
quality strategy;• A need to significantly strengthen risk management arrangements within the trust
including oversight form board level;• Significant concerns around the culture of the trust;• A complex structure lacking in clarity in accountability;• A weak governance structure.Deloitte recognised that the governance arrangements in the trust did not meet the requirements of a Foundation Trust, and identified a number of material areas where progress improvements were required:• Organisational Development;• Strategic Focus;• Board Leadership and cohesion;• Board Oversight;• Risk management and Board Assurance Framework.The final report was grouped under the four themed areas outlined within the Monitor well led framework. • Strategy and Planning;• Capability and Culture;• Process and Structures;• Measurement;Mr#Andrew Foster was appointed to HEFT in February 2015 as interim CEO. He revised the executive portfolios to include Governance within the portfolio of the Chief Nurse. The Chief Nurse has worked with the executive team and the PMO to develop the Trust Governance Recovery programme (GRP) in response to the Deloitte 2014 Governance review. As Senior Responsible Officer (SRO) for the GRP, the Chief Nurse will:
Safe Effective Caring Responsive Well led
Page 39 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.169
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Be accountable for ensuring that the GRP meets its objectives and delivers the projected benefits within the agreed IIP Programme framework;
• Ensure that the executive team is fully aware of their roles in delivery of the programme and that the programme is sufficiently resourced;
• Ensure that the change process maintains its business focus, has clear authority and that the overall context including risk is actively managed;!
• Be the visible owner of the programme reporting to the IIP Board and Trust Board.Resources:The Executive Team have appointed four senior experienced interims to support key internal staff to deliver the GRP; this is a critical component of the IIP.The programme will deliver the recommendations from the Deloitte Governance review, in addition to both the implementation of a revised performance management framework and a refreshed Trust Assurance Framework.The Trust are also engaged with Deloitte to scope support with the delivery of a training programme, and consultation with the site and divisional teams to enable the development of an integrated quality governance dashboard and supporting processes regarding assurance and performance across a range of indicators and data sources. The proposal will include the opportunity for Deloitte subject experts to take up short-term secondments in the trust. Deloitte are also engaged with the Trust to refresh the trusts’ BAF. The Executive Team will revise alignment of the internal audit programme in line with the integrated plan.The Executive Team will also quality assure the GRP with external stakeholders such as Monitor, CCGs, NHSE and the patients association for the elements relating to patient experience. Monitoring successful delivery of the GRP will be seen through the key metrics under the IIP as agreed with Monitor. The Governance Programme Board, and IIP Programme Board will oversee this delivery. The SRO/Exec lead - Sam Foster -Chief Nurse
My role as the Executive lead (SRO) for this programme is to ensure that we maintain grip, pace and focus and that the programme delivers on it’s objectives, that we provide the requisite level of assurance to the Trust Board and to Monitor that we can and will achieve a greatly improved approach and understanding of our strategic risks and how they relate to our operational performance and our public reputation.
Sam Foster - Chief Nurse
Safe Effective Caring Responsive Well led
Page 40 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.170
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.2.URGENT CARE PROGRAMME
To deliver a consistent and efficient patient pathway for patients presenting into the Trust’s urgent care systems.Impact of the programme
As a result of reducing variability within our processes, flow through patient processes will be improved. Consequently, delays for patients at the beginning of their pathway will be reduced and clinical risk reduced. Improvements urgent care pathway will also reduce the interference that urgent care demand creates within the elective inpatient pathways due to competition for bed capacity. Accordingly there will be positive impact on patient quality, overall costs and Trust performance against both the 4 hour emergency and 18 week admitted standards.Elements of the Programme
The Programme addresses all stages in the care of a patient, from first attendance through to discharge from the Hospital’s Services. Each of the three sites have specific plans to address both local constraints to delivery and common threads across all sites.The main elements being addressed are:• Flow within the Emergency Departments (ED) themselves:• Physical and staffing capacity;• Coordination and balancing of operational capacity within the ED to match the needs of
patients;• Internal Professional Standards and escalation processes to ensure appropriate
responses within ED and to requests from ED for support;• Bringing specialist opinion and decision making to the ‘front door’;• Ambulatory Care - presenting an alternative route for advice and treatment for ambulant
patients;• Reducing demand on both ED and admission capacity;• Ensuring that capacity for Ambulatory Care patients is sufficient and is available to
times of peak demand 7 days per week;• Reviews of the type of patient which can be managed through this route;• Promotion of ‘pull’ model from the A&E;• Developing existing links with GPs for direct referral;• Short Stay – many medical patents do not require a traditional specialist bed and can
be managed within acute medicine on a reduced Length of Stay;• Sizing of acute medical short stay capacity to match presenting demand, 7 days per
week;
Safe Effective Caring Responsive Well led
Page 41 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.171
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Reviewing and updating guidance to ensure that appropriate patients are managed with Short Stay;
• Promoting and investing in a Frailty Service such that these patients receive a rapid assessment and are signposted to an appropriate service. In many cases this can avoid the patient losing the capability to manage in their usual place of residence;
• Delivering a model of care focussed of regular senior review of patients to ensure a rapid turnaround;
Discharge and external capacity;• Redesigning clinical coordination within each ward’s daily routine such that each
patient’s Length of Stay is appropriate;• Identifying and removing blocks to rapid discharge once a patient becomes Medically
Suitable for Discharge, 7 days per week;• Redesigning how each Hospital Site coordinates internal flow to ensure delays and
variability are reduced or eliminated;• Planning for known period of increased demand to ensure the Trust responds in a
planned, predictable and effective manner.Trust and site capacity and demand matching
• Review of physical capacity to ensure appropriate use of existing, or commissioning of additional, based upon demand.
The SRO/Exec Lead - Jonathan Brotherton Director of Operations“The Urgent Care Improvement Programme is a key element of the overall Improvement Plan for the Trust; ensuring that all unplanned patients are quickly assessed and appropriately treated. This programme involves the vast majority of our clinical services and so it is appropriate that, as Director of Operations, I act as its Senior Responsible Owner. I have an engaged clinical and managerial team working with me to deliver the significant changes that are required. I believe that together we will lift our performance and reduce, to the lowest possible level, the clinical risk to our patients”
Jonathan Brotherton - Director of Operations
Safe Effective Caring Responsive Well led
Page 42 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.172
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.3.IM&T PROGRAMME
Our focus is on the opportunities and innovation that Information Management & Technology (IM&T) can offer to the Trust and sets out how the Trust can deal with rapid changes both in respect of the internal and potentially external health economies.The IM&T (IIP) element is based on the outcomes of the audits undertaken by Deloitte and Ideal. These outcomes of collective observations and recommendations have been documented and form the benchmark for the readiness activities which are currently being actively monitored via the IIP. The planning is also expanded into three sub-level plans for:
• Quick Wins - Benchmark Project Closure Readiness
• Stabilisation - Benchmark Business as Usual Readiness • Exploitation - Improvement Planning to Realise Benefits
The detailed sub-level plans are monitored on a daily basis and for further assurance a detailed project plan is currently under development.Our planning identifies requirements to drive and support innovation, improved access to Trust, Community, GP and Patient Services via robust and resilient technology and infrastructure. We are working toward improved data quality and reporting as we must ensure that the use of Trust information improves our patients’ safety and experience.Moving forward, the IIP will ensure improve Trust communications, engagement, more effective and co-ordinated planning to assist with closing service gaps that will ultimately prepare us for any future challenges.SRO/Exec Lead - Jonathan Rex - Director of IM&T
Appointed in an interim capacity to initially stabilise the IT function as well as some key project recovery and then review, with some carefully selected 3rd party consultancy, the capability and capacity of the department. In parallel there was a need to re-engage the IT function with the clinical and corporate functions and bring all that together in to an IT Strategy which aligned and underpinned the emerging corporate strategy.
Jon - Director of IM&T
Safe Effective Caring Responsive Well led
Page 43 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.173
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.4.CULTURES AND ENGAGEMENT
The aim of the Culture and Engagement work stream is to:
• Systematically improve LEADERSHIP capability across the Trust• Step change Staff ENGAGEMENT across all areas of the workforce• Strengthen VALUES led cultureWithin LEADERSHIP,
The objectives are to develop the Board and senior leadership team in order that the Trust is able to operate effectively, and to develop a strong pipeline of future leaders so that the Trust is able to implement its strategy effectively. The first steps within this are to provide a clear analysis of the current leadership position, as relates to both individuals and development provision, and to work with the Board and senior leaders to agree both the current and future need in terms of leadership and to develop a practical plan that supports the long term development whilst prioritising immediate need with pace. Systems will be put in place to effectively monitor, review and take appropriate actions at both individual and Trust level.Visible outcomes will be an agreed HEFT Leadership Development Framework, Succession Plans for senior roles and a bespoke Leadership Development Programme.Within staff ENGAGEMENT,
The objectives are to develop a working environment in which staff feel significantly more engaged, and to reap the benefits of the associated improvements in performance and patient outcomes. This will be achieved by introducing a more structure approach to staff engagement, including senior team led large scale listening events, strong governance around how feedback is turned into action, and the introduction of the more locally focused Engaging Teams Programme, to built sustainable skills and capability across our teams.Visible outcomes will be improved engagement within local teams; and across the Trust, as measured by the Staff Survey. Within VALUES,
The objectives are to develop and strengthen a Trust culture where Values are key, and how we are with each other and our patients is a defining factor. The first steps are to develop a set of staff-generated Trust Values and associated behavioural frameworks. To launch the Values in a way which engages and motivates staff to embed them into local working practices, and to build sustainability by incorporating the Values into infrastructure such as appraisals, recruitment, leadership development programmes and induction.
Safe Effective Caring Responsive Well led
Page 44 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.174
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Visible outcomes will be a set of Trusts Values, a behavioural framework, Values base to the bespoke leadership development programme and a Board and senior team appraisal process in place.The SRO - Hazel Gunter - Director of Workforce
“My personal role is to lead the development of this programme to ensure it delivers on the outcomes and assuring the Board on this project, whilst also supporting the senior executives in their part of the culture and engagement programme”
Hazel Gunter
6.4.1.Key Milestones
Engagement:• Preparation of new quarterly Pulse Staff Engagement Survey based on WWL model;• Implement Workforce Committee chaired by NED and a Staff Engagement Steering
Committee chaired by Chief Executive;• Implement senior led Staff Engagement Events reporting to the Staff Engagement
Steering Committee;• Roll out Pulse Staff Engagement Survey across 25% of the workforce per quarter;• Implement "Engaging Teams" programme for first cohort;• Undertake analysis of first quarterly Pulse Staff Engagement Survey results at Trust
level;• Agree baselines for all nine categories of the quarterly Pulse Staff Engagement Survey
and forecast targets for the 3 key enablers.Values:• Develop and agree Trust values through Trust wide consultation for Board approval
and sign off;• Develop a locally led Trust values implementation plan;• Identify and recruit appropriate resource accountable for delivery of the values
implementation plan and appraisal process;• Define and develop permanent culture metric once values are agreed;• Launch value based appraisal process for Board and complete full appraisal cycle.Leadership:• Provide clear analysis of current leadership development offering within the Trust;• Define current and future leadership needs;• Conduct a gap analysis between defined needs and current status;• Develop and implement a practical plan to improve leadership across the Trust;
Safe Effective Caring Responsive Well led
Page 45 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.175
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Agree a bespoke Leadership Development Framework and then implement a bespoke Leadership Development Programme;
• Implement a system to monitor and track delivery of the Leadership Development Programme;
• Implement succession plan for all executive board members.
Safe Effective Caring Responsive Well led
Page 46 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.176
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.5.SCHEDULED CARE
To ensure that patient waiting times are minimised at all stages of the scheduled care patient pathway based upon joint trust and CCG patient access standards.Impact of the programmeAs a result of implementing a programme of robust development and management of performance against trajectories, along with identification of underlying factors that influence our ability to consistently ensure patients are treated as quickly as possible within each milestone of their pathway, the scheduled care programme will deliver a return to the 18 week and cancer performance standards. The work streams identified therefore focus both on the “here and now” as well schemes that will transform the way in which services are delivered to ensure sustainable change and improvement. Joint working with our partners to achieve success is key and is reflected within the programme and supporting structures which ensure performance is monitored, scrutinised, root causes understood and associated actions developed.
Elements of the programmeThe programme addresses all elements of scheduled care and key milestones within the patient pathway, from referral through to follow up and including the diagnostic and therapeutic elements of the patient journey. Whilst there is 1 overall plan, this is supported by specialty level trajectories and where necessary, specific recovery plans for those specialties identified as a “red risk”. The main elements of the programme are Planned care/RTT:• Reduce the backlog of patients >18 weeks to a level where RTT targets are achieved
and maintained;• Monitor performance and manage any deviations against specialty specific trajectories;• Manage closely patients on open clock pathways to further reduce risk to patients
breaching the 52 week standard;• Improve data quality by applying a multi-faceted approach that includes input from
operational, IT, finance and performance teams;• Provide a single waiting list that is clean and through which teams have full visibility of
their patients and their pathway position and status;• Centralise waiting list management functions to reduce risk and ensure equity of patient
waiting times across all sites for the same procedure;• Publish and launch a Patient Access Policy that has been developed in conjunction with
the IST and CCG colleagues and supports teams in better managing patients in line with DoH and local RTT rules;
• Provide greater certainty to our most vulnerable patients by ensuring that no category 1 patient is cancelled due to “no bed” being available;
Safe Effective Caring Responsive Well led
Page 47 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.177
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Ensure that all cancer target are achieved, most critically the 2ww target for cancer and breast symptomatic achievement of which is challenging due to multiple factors including increase in referrals, high median wait times, patients not being aware of their reason for referral and high numbers of patients choice breaches;
• Work with other Trusts and CCG’s to revise specialty specific referral forms for 2ww that provide greater guidance to GPs at the point of referral;
• Implement new best practice pathways in our specialties that have a higher proportion of 62 day breaches due to their complexity, most notably Lung and Urology;
• Forward look and plan for changes in demand as a result of revised guidance from NICE and publicity campaigns;
• Provide a workforce and resource capacity for the whole of scheduled care that enables delivery and creates further capacity;
• Provide a governance structure and clear roles and responsibilities for scheduled care that support service improvements as well as the ability to monitor and manage performance of the position.
SRO/Exec Lead - Jonathan Brotherton - Director of Operations“My role as the SRO for this programme is to drive improvements in patient flow right across the whole of HEFT, so identifying the links between this programme and the Urgent Care Programme and then managing those interdependencies is critical to the successful delivery of both programmes and the realisation of the full range of benefits for patients and staff alike”
Jonathan Brotherton
Safe Effective Caring Responsive Well led
Page 48 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.178
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6.6.MORTALITY
Key objectives of the programme:There should be a Trust wide policy that all deaths will be reviewed. This should be with the intent of looking for suboptimal clinical care rather than to determine whether or not the death was avoidable or inevitable.The outputs of these reviews should be fed to the Mortality and Morbidity Performance Group for triangulation across specialities and with the outcomes of reviews of incident reports, patient experience, complaints and other data sources such as Trainee survey reports.Messages about hospital mortality should regularly go out to staff so that they are aware of the situation and know what they can do to improve matters.There should be a review of the incident reporting system in order to encourage incident reporting and make best use of the reports including near misses to improve safetyImproving flow through the Trust should be a high priority. Rather than a “magic bullet “ approach, it would be best to focus on the impact of accumulation of marginal differences. These should include:
• Better working between the ED and the specialities to get specialists as close to the “front door” as possible;
• Considering using the recommendations of the Royal College of Physicians Future Hospital Programme;
• A system of specialities “pulling” patients from ED; • Increasing the range and scope of ambulatory emergency clinics and making their
operational policies explicit; • Use of ward round checklists and adhering to the Royal College of Physicians and
Royal College of Nursing guidance on ward rounds; • Reviewing the processes for prescribing and dispensing TTO drugs; • Daily (7 days a week) senior review of all patients including all outliers; • Reviewing compliance with the 10 standards for 7 day working by undertaking the self-
assessment exercise on the NHS IQ website and developing an action plan; • Aim to achieve the same numbers of discharges per day at weekends as on weekdays; • Reduce non-medically indicated ward transfers; consider a policy of requiring all such
transfers to be discussed with the responsible consultant first .All clinical directorates should agree pathways and standards for care of non-elective admissions and undertake regular audits of compliance with results reported back to clinicians.
Safe Effective Caring Responsive Well led
Page 49 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.179
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Consider the use of an electronic track and trigger system for detection of deteriorating patients and escalation of care. A programme to improve staff engagement, multidisciplinary team working and empowerment (such as Listening into Action) should be considered as a matter of urgency. This should be prioritised to those clinical teams where poor engagement and team working are well known Review the interactions between consultants and coders to help improve the quality of medical notes and the way diagnoses are recorded. Consider using appraisal as a lever to improve consultant recording of diagnoses and engagement with the coding process. When these outcomes are triangulated with other reviews and reports such as the IST reviews and the Deloitte Governance Review, which carries very specific recommendations on Leadership, Board Assurance and Risk management, they all tell as similar story and make similar recommendations, albeit the reviews are approaching things from different angles,based on different criteria and carried out independently of each other.Key milestones:
Mortality process:• Review current Mortality and Morbidity Performance Group, including ToR,
membership, roles and responsibilities and agree reporting governance;• Agree pro forma and screening method for mortality case review;• Identify resources to support pilots;• Pilot redefined Trust process with AMU and Cardiology;• Submit proposal to Trust Board outlining the governance and reporting arrangements
for MMPG within the Trust BAF;• Pilot analysis and full Trust roll out of compulsory process to all Clinical Groups or
Directorates;• Define mechanism to identify and approve Quality Improvement schemes and
governance to support improvement monitoring.Education:
• Draft and agree education materials;• Develop schedule and timetable of engagement events;• Delivered all engagement as a mixture of open event or targeted events by Directorate.Coding :• Scope and develop clinical coding work stream to improve clinical engagement in
coding; • Complete visits to each directorate to increase clinical engagement in coding.Future Information Requirements:
Safe Effective Caring Responsive Well led
Page 50 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.180
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Undertake visits to exemplar organisations with regards to advance mortality / morbidity analytics;
• Draft Business Case for Trust Board approval for development of Trust advanced mortality / morbidity analytics capability.
“My role as the Director of Medical Safety (Clive Ryder is SRO for this programme ) is very clear to me, to ensure that the programme is properly managed and resourced. To ensure that the Trust develops and implements robust policies and processes that enable us to fully understand the reasons that underpin our mortality rates and provide opportunities to improve our survival rates”
Dr Ann Keogh - Director of Medical Safety
Safe Effective Caring Responsive Well led
Page 51 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.181
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 7- PROGRAMME COSTING
Safe Effective Caring Responsive Well led
Page 52 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.182
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
7.PROGRAMME COSTING
7.1.PROGRAMME MANAGEMENT COSTS
The following tables describe the running costs for the PMO for the next twelve months and for IIP Programme resources that might work within the services themselves but are still deemed as supernumerary or interim.Each of the IIP Programmes is responsible for managing its own budget and recruitment of substantive and interim resources. The PMO has got a mixture of resources working out of the PMO itself although they don’t necessarily have reporting lines directly into the PMO. This will be reviewed over the coming weeks to ensure the most effective and efficient structure to support the delivery of the IIP programmes.An interim governance process (see Fig 15 below) is also being introduced to ensure that we have control over recruitment and the on boarding processes5
Project lead identifies
additional need to Programme
Director
Resource available internally
Arrange/Negotiate
secondment
YES
AATR1* approved?
Log risk and escalate to IIP
programme Director
NO
Recruit/ EngageYES - identifysource
Deploy resourceONBOARD
Interim Support Engagement process
NO
Signatures required from:Programme Exec Lead
Programme DirectorDirector of FinanceExec Director for IIP
Finance department reviews interim
consultancy contract and signs
* Appointment of Additional Temporary Resource Form
Fig 15 - Interim Governance process for Interim/temporary support to the IIP
Safe Effective Caring Responsive Well led
Page 53 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
5 Samples of PMO reporting and other process templates can be found in the Appendices
Integrated Improvement Plan

Council of GovernorsJune 2015
.183
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Safe Effective Caring Responsive Well led
Page 54 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.184
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 8- STAKEHOLDERS
Safe Effective Caring Responsive Well led
Page 55 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.185
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
8.STAKEHOLDERS
8.1.STAKEHOLDERS PROFILES
Understanding our stakeholders will help us manage their expectations and their levels of influence and interest in the IIP. Although it is sometimes an uncomfortable analysis to share publicly it is an essential part of programme management, there are numerous examples of large scale change programmes and projects that have failed because organisation did not understand their stakeholders, their level of expectation and their power to derail the programme or project. Therefore we will undertake a detailed profiling exercise to ensure that we don’t fall into the same trap. So we will be asking ourselves some or all of the following questions and reviewing them on a quarterly basis:
• What financial or emotional interest do they have in the outcome of our work? Is it positive or negative?
• What motivates them most of all?• What information do they want from us?• How do they want to receive information from us? What is the best way of
communicating our message to them?• What is their current opinion of our work? Is it based on good information?• Who influences their opinions generally, and who influences their opinion of us? Do
some of these influencers therefore become important stakeholders in their own right?• If they are not likely to be positive, what will win them around to support our
programmes and projects?• If we don't think we will be able to win them around, how will we manage their
opposition?• Who else might be influenced by their opinions? Do these people become stakeholders
in their own right? The outcome of the profiling exercise (the profiles) will be shared with the SRO’s.
8.2.STAKEHOLDER MAPPING & MANAGEMENTHow and when we communicate with our various stakeholders is critical to the success of the programme, so coupled with the IPP Communications Strategy we will pro-actively manage our stakeholder communications to ensure that our stakeholders are kept informed about the progress of the IPP and its constituent programmes.The following diagram (Fig 16) representative of how we will map our stakeholders and define the type and level of communications with them. As the IPP progresses through the various stages of Definition, Development Delivery and Assurance individual stakeholders will move up and down the grid depending on their level of interest and influence in the programme at a given point in time.
Safe Effective Caring Responsive Well led
Page 56 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.186
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
KEY:1. CEO HEFT 2. DoF HEFT3. Chair HEFT4. Dep CEO5. Monitor Impr Dir6. Chief Nurse
7.Director of Operations 8. Programme Director -IPP 9. Programme Director - Gov 10.Programme Director - UC 11.Programme Director - SC12.Programme Director - C&E
13.Programme Director - Mort 14. Programme Director - IM&T15. Monitor16. CCG’s17. NHSE18. Director of Clinical Gov19. Head of OD20. Clinical Direcors
KEEP INFORMED
MAINTAIN INTEREST
ACTIVE CONSULTATION
KEY PLAYERS - Critical partners
WRITTEN
MOREFACE TO FACE
LEVE
L O
F IN
TERE
ST
INFLUENCE
21. Andrew Windsor - Income 22. Consultants & Junior Docs23.Ward managers & clerks24.Estates & Facilities25. Staff26.Commissioning Support Unit.27.Health and Wellbeing Board28. Patients
1
2
3
4
56
7
89
1011
12
13
14
15
16
1718
19
20
21
22
23
24
25
26
27
EXAM
PLE
28
Fig 16 - Stakeholder map
We will centralise communications with our key stakeholders through the communication team. Developing a core database of our stakeholders and tracking our interaction with them will ensure we are communicating consistently and effectively. The trust stakeholder communications plan is currently being updated, and will then be further developed using the feedback from the stakeholder review, currently being carried out on behalf of the trust by Deloitte.
Safe Effective Caring Responsive Well led
Page 57 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.187
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 9- SCHEDULING & MILESTONES
Safe Effective Caring Responsive Well led
Page 58 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.188
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
9.SCHEDULING/MILESTONES
9.1.THIRTY DAYS (O+30)The next 30 days will be focused on ensuring that we have stabilised the IIP and it’s constituent programmes, as stated in 13.1 - Gateway Schedule. The following schematic (Fig 17 ) describes other PMO focussed activities that will take place during the next 30 days.It is evident that the IIP has lost some of it’s earlier momentum and grip so it is vital that we reinvigorate the programme as quickly as we can whilst at the same time increasing staff awareness of the programme and it’s objectives. We will need to overcome what is often referred to as “change fatigue” and the perception in some areas that they are being “done to” and that HEFT is placing too much emphasis on interim support and programme boards.As we will be making some changes to processes and documentation the next thirty days are likely to be punctuated with periods of frenetic intensive activity so that we do not lose any further momentum.One of the key features of 0+30 will be the Programme gateway reviews.
All programmes to have Gateway review 0
Review of PMO
templates
W/C 27/4 W/C 4/5 W/C 11/5 W/C 18/5
Adjust &
Streamline
Implement & EmbedChanges
Implement and Embed newley developed IIP Metrics
PMO Resource review - to ensure sufficient capacity to support IIP
delivery
Embed new B/R/A/G reporting format and reporting timetable
HEFT/ Monitor
Stakeholder Meeting
20/5
W/C 25/5
Fig 17 - The next 30 days
Safe Effective Caring Responsive Well led
Page 59 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.189
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
9.2.SIXTY DAYS (0+60)By the time we reach the end of the first thirty days of the recovery phase we will have a clear understanding of which of the IIP programmes are performing to the required standard and which require support and intervention.So during 0+60 (see Fig 18 below) we will be undertaking “deep dives” on the full range of constituent projects and work streams to carry out similar analysis. During this period we will also be reviewing the BRAG reporting format to ensure that we are meeting Monitors expectations and providing the desired level of assurance - should we conclude that we are not we will establish a small task and finish group to deliver a remedial action plan .We will also be initiating a series of “re-ignition” events for the IIP to ensure that we regain the early momentum and engagement. These will be based on a the “European Cafe” format where different groups of staff from all levels of the organisation come together for short sharp high intensity workshops/briefing events.
Stakeholder profiling and mapping
MonitorSubmission
18/6
W/C 1/6 W/C 8/6 W/C 15/6 W/C 22/6
GovernanceProgramme Board - 25/6
IIP “re-ignition”
Events
Embedding the new Communications plan
Commence project/work stream “deep dives”(Gateway 2*)
Review effective use of new B/R/A/G reporting format and reporting timetable to ensure
compliance ready for next reporting cycle
HEFT/ Monitor
Stakeholder Meeting
20/6
W/C 29/6* this is based on the assumption that projects and work streams have undergone a Gateway 1 - Business Case
ScheduledCare
ProgrammeBoard
3/6
Fig 18 - The next 60 days
9.3.NINETY DAYS We intend to gain momentum very quickly over the next 30 and 60 days so we fully expect that a number of challenging but nevertheless important milestones will need to be achieved during this period.The following diagram (Figure 19) describes the next 90 days in the life cycle of the rejuvenated IIP and PMO. This diagram identifies a selection of some of those milestones.
Safe Effective Caring Responsive Well led
Page 60 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.190
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Days 0+30 Days 0+60 Days 0+ 90
See 9.1 0+30 days
See 9.2 0+60 days
When the process for ongoing review and actioning of 2ww delay reasons are embedded
May
Plann
ed C
areUr
gent
Care
Morta
lityGo
verna
nce
Cultu
re an
d En
gage
met
June July August
When the 7day a week service in AEC is established
When a standard forward planning process for periods of increased demand is implemented
A selection of Milestones that are due to be delivered in the next 90+ days
When full SOP Protocol for board rounds is implemented
When rapid assessment and treatment process for majors is implemented.
When the Medical redesign for Consultants across BHH is complete
When a written policy for the management of outliers is implemented
When an effective recruitment strategy for senior staff is implemented
When AEC is the default for emergency medical referrals
When the single PTL / waiting list is launched
When the processes for management of patients on an Open Clock Pathway are embedded
When the Trust achieves avoidance of all breaches of the 52 week standard
When the Implementation Plan to be developed to deliver the Reconfiguration is complete
When the new Mortality Policy is implemented across Directorate
When the Engaging Leadership Programme starts
When the Senior Leaders have implemented a systematic and effective cascade process
When the Trust values and behaviours are introduced
When the patient metrics are in place
When the PMF Framework is implemented across Organisation
When the Governor engagement exercise is complete
When the Kennedy work stream is closed
When succession planning system is in place
When the Forward Training Programme is complete
Figure 19 - The next 90 days
Safe Effective Caring Responsive Well led
Page 61 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.191
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 10- RISK
Safe Effective Caring Responsive Well led
Page 62 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.192
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
10.RISKS
10.1.MANAGING RISKS WITHIN THE PORTFOLIO
As the IPP is going to follow MSP methodology it makes sense to use a recognised Risk management methodology, Management of Risk (M_o_R) that aligns to MSP. We will be managing risk and issues not just recording them. We will use a standard 5x5 scoring matrix for likelihood and impact as depicted in Fig 20 below:
1 2 3 4 5
2
3
4
5
1
Risk = Likelihood x Impact
EG - Likelihood 3 x Impact 3= Risk score 9= Amber
1 2
2
3 4 5
3
4
5
4 6 8 10
6 9 12 15
8 12 16 20
25201510
Likelihood
IMPACT
Fig 20 - Risk Matix
Each programme within the IIP will be required to maintain it’s own Risk Register that feeds into the main IIP risk register. Each project/Work stream will be expected to feed into the programme risk register and to manage risk effectively, escalating risks to the Programme Director if particular risk(s) start to increase in likelihood and impact.Risk management must become a business as usual discipline within HEFT, and reform of the approach to risk management is a major work stream within the Governance programme. The IIP programme has the resources and expertise to provide wide ranging in-house training on risk management practices and methodologies.The PMO will support a number of risk awareness and management training events as part of the work around the implementation of the new BAF. Each programme and constituent project and work stream will undertake a risk workshop in May 2015, recognising that this is a retrospective exercise we believe that it is an essential step to confirm that we have captured all the risks, developed robust mitigation plans and made the links to other programmes and projects. The following diagram (Figure 21)describes the minimum information that will be required for the risk registers:
Safe Effective Caring Responsive Well led
Page 63 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.193
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
UIN Risk description
Risk owner
Risk score
Risk actionee Mitigation planRisk
responseMitigated risk score Comments
Unique identification number- assigned by
the PMO and identifies the risk throughoutthe lifecycle of the
programme
Describes what the risk is and where it originates
from and how it will be manifest
The senior manager orDirector whose business area
is most effected by the risk
This is the result of multiplying the impact
score (1-5) by the Likelihood score (1-5) i.e. Riskscore = 3 x 5 = 15
The individual or departmentwho will be responsible for
managing and delivering the agreed response to the risk
This will describe the Trust's approach to risk management of
this particular type of risk - Transfer,Terminate, Treat/Mitigate,
Tolerate
Describes the actions that willbe taken to reduce the likelihood andimpact of a given risk or group of risks
The recalculated risk scoreafter the mitigation has been taken,
sometimes referred to as the residual risk
Date raised
The date the risk was first discussed and entered into
the Risk log
Fig 21- Risk register entry guide
10.2.LINKS TO STRATEGIC RISKSOne of the main work streams in the Governance programme is the redesign and implementation of a much more robust risk management framework for the Trust. This is due to be in place by early September 2015 - in the run up to that implementation the PMO will work collaboratively with the Governance programme to ensure that programme risks are fully analysed and mitigation plans fully developed and recorded in the strategic risk register if the risk is deemed to be of such magnitude that it constitutes a strategic risk to HEFT.
Safe Effective Caring Responsive Well led
Page 64 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.194
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 11- CONSTRAINTS
Safe Effective Caring Responsive Well led
Page 65 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.195
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
11.CONSTRAINTS
11.1.TYPES OF CONSTRAINTS
11.2.External
At the time of writing of this plan the Country is officially in Purdah6 which places obvious constraints on HEFT and indeed Monitor from making announcements about major reconfigurations in public services. The General Election itself provides uncertainty and constraints for all public sector bodies, especially this general election due to the complete uncertainty of the outcome. Certain outcomes of the election may provide an endorsement of HEFT’s plans whilst other outcomes may not and may initiate other demands on HEFTS reconfiguration plans or even more radical intervention.11.3.Internal
The main internal constraints that are likely to impact the delivery of the IIP are related to resource, insufficient capacity may slow down the programme , insufficient capability could threaten delivery overall.
11.4.POTENTIAL IMPACTThe internal constraints are likely to slow down the delivery in the first instance, prolonged resource starvation will of course introduce change fatigue and resent across the front line staff body initially i.e “we have heard it all before” and then there is a risk that this will potentially spread upwards through the senior management ranks and possibly even to Executive level.The external constraints have to a degree receded at the point when this final draft has been published. The outcome of the General election is now known and to all intents and purposes we can say with some confidence that the direction of travel will likely remain the same as it was pre-election.
Safe Effective Caring Responsive Well led
Page 66 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
6 Purdah is the pre-election period in the United Kingdom , specifically the time between an announced election and the final election results.[1] The time period prevents central and local government from making announcements about any new or controversial government initiatives (such as modernisation initiatives or administrative and legislative changes) which could be seen to be advantageous to any candidates or parties in the forthcoming election. Where actual advantage to candidates is proven in law based on precedent cases to have been given this amounts to a breach of Section 2 of the Local Government Act 198
Integrated Improvement Plan

Council of GovernorsJune 2015
.196
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 12- COMMUNICATIONS
Safe Effective Caring Responsive Well led
Page 67 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.197
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
12.COMMUNICATIONS
12.1.TACTICAL APPROACH FOR THE IIPEffective, clear and engaging communication is critical to the success of any major programme of change; HEFT’s IIP is no different. It is our intention to pursue a proactive communications approach to ensure that our messages are focussed and unambiguous. Our approach will be proportionate, driven, not least by the need to safeguard the reputations of HEFT and our partner organisations whilst at the same time providing transparency around progress and processes. The delivery of the communications and engagement strategy will be the responsibility of the IIP PMO and Heart of England’s communication team.
12.2.OBJECTIVESTo ensure that staff and stakeholders understand the changes that are taking place, and feel engaged and supported throughout the process by keeping them updated, using effective channels of communications including sufficient opportunities for feedback. We will work across all IIP programme areas to support delivery of the key objectives: • Improving the quality of care, including the outcomes, the safety and the experience for
all;• Engaging with patients, carers, staff, our community, stakeholders and partners to
redesign our services to provide improved access to services at the right time in the right place; and
• Innovating and researching new treatments and new ways of delivering care.The key work streams for the communications team are broadly defined below.
12.3.SUPPORTING THE IIP IMPLEMENTATIONClearly set out the overall programme’s strategy that will be used to communicate with key stakeholders and partners over the life cycle of the programme.We will: • Ensure that we communicate programme information in a timely and accurate manner
which is open and transparent;• Establish tailored local and cross CCG Borders stakeholder engagement processes;• Ensure a process for strategic coordination across the participating organisations to
ensure consistent messages and timelines;• Help staff to understand the vision for the delivery of the IIP;• Build awareness and involvement in the transition process;• Build trust and confidence in the process;
Safe Effective Caring Responsive Well led
Page 68 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.198
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Ensure staff can raise and share their concerns, thoughts and ideas;• Help staff to feel enthused and motivated to be part of the new arrangements;• Support the HR processes around the transformation processes; and• Ensure key external stakeholders are kept informed and involved – particularly EMB,
Trust Board, Monitor, Staff Forums & Patients and their friends and families..
12.4.CLINICAL COMMUNICATIONincreasing knowledge about safety and risk and improving patient flow, patient quality, and trust performance against all clinical targets.We will:• Work closely with clinicians to improve the way we communicate with our front line staff,
through face to face regular meetings;• Explore the tools that are most effective for engaging out internal audience through
research• Develop a handbook (hard copy and online) which all front line staff can access easily
and which can be readily updated, which contains information on our targets and current status;
• Produce a series of guides which clearly explains to all staff our processes and procedures;
• Develop specific communications packages around Mortality, Urgent Care and Scheduled Care improvement plans;
• Continue to work closely with the IT team to support implantation of all IM&T systems and help with communicating any planned changes to staff effectively.
12.5.GOVERNANCE
Sufficient and effective Board, management and clinical leadership capacity and capability, as well as appropriate governance systems and processes.We will:
• Support the organisation in the development and delivery of its strategic objectives; • Support the implementation of new systems and processes;• Communicate changes to any governance effectively;• Promote a trust wide understanding of the need for improving governance .
12.6.CULTURE AND ENGAGEMENTDevelop a working environment in which staff feel significantly more engaged, and to reap the benefits of the associated improvements in performance and patient outcomes. We will:
Safe Effective Caring Responsive Well led
Page 69 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.199
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• Improve communications with governors and stakeholders, working in consultation to streamline and target our message and delivery channels;
• Clearly define our stakeholders through mapping; • Have a clear plan which addresses the issues raised in the Deloitte stakeholder review;• Fully support the patient engagement work stream by developing a plan to support
effective communications with patients about how to give feedback to the trust; • Fully supporting the Staff Engagement programme with the introduction of the values,
quality champions.We will achieve this by clearly identifying our internal channels, facilitating engagement across teams and promoting synergy.We will provide structure and guidelines for clear communications within a vast organisation where responsibility is devolved in order to empower teams to communicate with their audience and we will offer support where necessary.Ultimately we will provide a strong sustainable framework for effectively communicating with our staff, stakeholders and the media, which is fit for purpose and enhances the reputation of the trust both regionally and nationally.
12.7.RESOURCES
Currently the trust’s communications resources are disparate and need to work more effectively together. Corporate services functions such as events, web design, intranet management, graphic design, multimedia, and GP communications are not controlled within the communications team.As a team of five the focus has historically been on reactive external communications so has needed some reorganisation. In order to fully support the implementation of the IIP we are in the process of reorganising the current communications team and are taking on 3 new members of staff. Of these three one will primarily support the overall IPP delivery, one will support the culture and staff engagement agenda. The existing internal communications officer will lead on clinical communications. The Head of Communications will support the team, attend relevant meetings and specifically support governance and stakeholder work alongside patient experience.The other team members will focus on external communication and have a strong focus on becoming a proactive rather than reactive public relations function. Our external communications strategy will be broadly aligned to the internal communications strategy with subtle changes in messaging as appropriate to the audience(s) being targeted.Managing the interdependencies of the communications requirements within a programme of this size and complexity is challenging, we have chosen to work on the communication as a close group within one team to try to minimise the risk of silo working and duplication of effort. There is currently no budget allocation for communication to support the implementation of the IIP other than funding for one post. This needs to be resolved.
Safe Effective Caring Responsive Well led
Page 70 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.200
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
12.8.IMPLEMENTATIONOver the next 30 days we will have the resource in place to produce a clear strategy and timeline to support the IIP. This will outline deliverables for each key communications work stream within the IIP. Implementation of the IIP Communications Strategy will take place during the latter half of May 2015 and will be fully embedded by the end of June.Each IIP Programme will be expected to allocate sufficient resource to manage the communications plan for their programme. They will be expected to work closely with the HEFT communications team and the Organisational Development senior management team to ensure that outgoing messaging is well thought out and appropriately targeted.The plan will support a go live date of September 2015 (we will try to bring this forward). It will also include details on how this will be measured and evaluated and sustained in the future.
Safe Effective Caring Responsive Well led
Page 71 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.201
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 13-GATEWAY REVIEWS
Safe Effective Caring Responsive Well led
Page 72 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.202
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
13.GATEWAY REVIEWS
Although the original OGC Gateway review process has now ceased to be a service offered by Central Government the process and logical review stages still have merit and still add valuable oversight and assurance to public sector programmes.
Programmes
Develop programme
mandate
Start Programme
Ke
y D
ec
isio
nP
oin
t
Gateway 0Strategic
Assessment
Develop programme
Brief
Ke
y D
ec
isio
nP
oin
t
Gateway 0Strategic
Assessment
ProgrammeDelivery
Manage Delivery
Manage Delivery
Manage Delivery
1/4
ly
Asse
ssm
en
tnP
oin
t
1/4
ly
Asse
ssm
en
tnP
oin
t
Gateway 0Progress
&Governance Assessment
Gateway 0Progress
& Governance Assessment
ProgrammeClosure & Move
to BAUCLOSE
Gateway 0Benefits
RealisationAssessment
Projects
Develop Business
Case
Gateway 1Business
Justification
Ke
y D
ec
isio
nP
oin
t Develop Delivery Strategy
Ke
y D
ec
isio
nP
oin
t Assign/Procure
Resources
Develop& DeliverProducts
Ke
y D
ec
isio
nP
oin
t
Gateway 2Delivery
Justification
Gateway 3Resource
Justification
Ke
y D
ec
isio
nP
oin
t Handoverto
BAU
Gateway 4Readiness
forService
Ke
y D
ec
isio
nP
oin
t
Gateway 5Operational
review
Close Project
Gateway 5Benefits
Realisation
Figure 22 - Gateway review process
We will compliment the Gateway process with the self assessment processes and challenges that P3M3 provides7 around :
• Management Control; • Benefits Management; • Financial Management ;• Stakeholder Engagement ;• Risk Management; • Organizational Governance; • Resource Management.Each programme will undergo a retrospective Gateway 0 review to assure the decision and/or identify any flaws or gaps in the strategic assessment that supported the decision to initiate the programme in the first instance.Individual projects and work streams will be subject to a set of reviews during the life cycle of the project as shown in Fig 22 above.
Safe Effective Caring Responsive Well led
Page 73 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
7 Further details of which can be found in the Appendices
Integrated Improvement Plan

Council of GovernorsJune 2015
.203
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
13.1.SCHEDULE OF REVIEWSThe formal review schedule, which commenced in May 2015 utilising Deloitte , Programmes will be further reviewed by the Gateway panel ( see 12.3) in the first instance in June 2015 and quarterly thereafter. Projects will be reviewed monthly and will be required to submit a monthly highlight report and weekly project status report (PSR).For the purposes of scheduling each project will be assigned a unique identification number (UIN) - for example a Governance project will could have the following UIN - IIP-GV-018. The following tables sets out the timetable for May, subsequent schedules are contained in the appendices.
Programme W/C 25/5 W/C 1/6 W/C 8/6 W/C 15/6
Urgent Care X - GW-0
Scheduled Care X- GW-0
Mortality X-GW-0
Governance X-GW-0
IM&T X - GW-0
Culture and Engagement X - GW -0
Table - Gateway 0 review schedule - Programmes
Programme Project W/C 22/6 W/C 29/6 W/C 6/7 W/C 13/7
Urgent Care
Scheduled Care
Mortality
Governance
IM&T
Safe Effective Caring Responsive Well led
Page 74 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
8 UIN used for the Gateway process will be aligned to the UIN numbering system being implemented for Programme workbooks and other reporting architecture.
Integrated Improvement Plan

Council of GovernorsJune 2015
.204
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Programme Project W/C 22/6 W/C 29/6 W/C 6/7 W/C 13/7
Culture and Engagement
Table - Gateway 1 review schedule - projects/work streams
13.2.DESCRIPTION OF REVIEW
Each review will be a structured review with a set agenda circulated in advance and will centre on check and challenge around the key themes identified above from the P3M3 project assurance methodology.
13.3.GOVERNANCE AND RESOURCES FOR THE REVIEWSThe Gateway review process will be accountable to Trust EMB and will report monthly to them9.The review panel will work on a “Star Chamber” approach10 - (“a court or other group that meets privately and makes judgements that can be severe”) with standing panel members and individual SRO’s required to attend as necessary. The standing members of the panel will be:
• Deputy Chief Executive and Medical Director (or delegated Deputy);• IIP Programme Director;• Finance representative;• Head of PMO.
Safe Effective Caring Responsive Well led
Page 75 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
9 This may be by way of a verbal update or a written brief depending on the length of the Board agenda
10 This approach can also be adopted for the CIP Programme(s) if and when it comes into the IIP
Integrated Improvement Plan

Council of GovernorsJune 2015
.205
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
At the Heart of it……
IntegratedImprovement
Plan
SECTION 14-APPENDICES
Safe Effective Caring Responsive Well led
Page 76 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.206
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.APPENDICES
14.1.APPENDIX I -CCG “UNIT OF PLANNING”
Fig 23 - Unit of planning
Safe Effective Caring Responsive Well led
Page 77 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.207
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.2.APPENDIX II - PMO SAMPLE TEMPLATES
Fig 24 - Project exception report
Fig 25 - Project exception report
Safe Effective Caring Responsive Well led
Page 78 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.208
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Fig 26 - Highlight report
Safe Effective Caring Responsive Well led
Page 79 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.209
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Fig 27 - Sample project closure and review report
Safe Effective Caring Responsive Well led
Page 80 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.210
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Define project brief
Define project scope
Define initial milestone plan
Define the business case
Project Startup and Initiation
Project Planning Project Delivery Project Closure andBenefits realisation
Prioritise and schedule project
Manage change and progress
Manage communications
Develop comms plan
Refine project plan
Document project plan (Gant format if preferred)
Develop risk and issues logs
Launch project
Manage project outputs/products
Manage project stages
Close project
Review project outcomes
Evaluate benefits realisation
Direct/Manage Project
Document and review lessons learned
Fig 28 - Project stages
Safe Effective Caring Responsive Well led
Page 81 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.211
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.3.APPENDIX III - SAMPLE OF AN OUTCOME RELATIONSHIP MAP
Seamless integration between Community Mental Health Teams, Community Health
Services & Social Care Teams achieved
1
More working with voluntary and
community sector
2More care & support provided at home or
near to home
3
Better integrated services
4
Fewer handovers5
More effective & efficient care
provision
6Reduced need for
nursery & residential care
7
Better joint commissioning arrangements
8
More use of community-based
services
9
Reduced demand for emergency & planned
hospital care
10
Reduced costs11
Single commissioning process, services &
work
12
Better managed admissions &
discharge
13
Transfer delays eliminated
14Reduced pressure in
A&Es & wards
15
Reduced stress16
Better care17
Faster & better recovery
18
Figure 28 - Outcome relationship map
Safe Effective Caring Responsive Well led
Page 82 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.212
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.4.APPENDIX IV - MAIN IIP DASHBOARD
Figure 29 - Screenshot of IIP Metrics Dashboard - Sample data
Safe Effective Caring Responsive Well led
Page 83 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.213
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.5.APPENDIX V - MONITOR UNDERTAKINGSOn the basis of the grounds set out below, and having regard to its Enforcement Guidance, Monitor has decided to accept from the Licensee the enforcement undertakings specified below pursuant to its powers under section 106 of the Act.Monitor has agreed to accept and the Licensee has agreed to give the following undertakings, pursuant to section 106 of the Act:Improvement programme:
• The Licensee is developing an Integrated Leadership Support and Resilience Programme ('the improvement programme') in response to leadership, clinical and governance concerns including those identified in the mortality review and the governance review;
• The Licensee will provide Monitor with its improvement programme covering the period from 1 January 2015 to 31 March 2015 by 23 January 2015, or such day to be subsequently agree;
• The Licensee will provide Monitor with its improvement programme covering the period from 1 April 2015 to 31 July 2015 by 13 February 2015, or such day to be subsequently agreed;
• .The Licensee will agree with Monitor:• milestones for the delivery of each major element of the improvement programme
and;.• success measures to monitor the delivery of the programme
For the period between 1 January 2015 and 31 March 2015 by 31 January 2015, or such day to be subsequently agreed, and for the period between 1 April 2015 and 31 July 2015 by 27 February 2015, or such day to be subsequently agreed.• The Licensee will implement the improvement programme according to the milestones
agreed with Monitor;• The Licensee will monitor its performance against the improvement programme and will
send Monitor written monthly updates summarising its performance. The monthly updates will:
• include actual performance against the actions outlined in the improvement programme;
• include any failures to deliver or risks to the delivery of actions in line with the milestones agreed for the improvement programme;
• include details of any mitigations to the identified failures to deliver or risks to delivery;
• include actual performance against the success measures agreed with Monitor;• be sent to Monitor for the first time in respect of February 2015;
Safe Effective Caring Responsive Well led
Page 84 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.214
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
• be sent to Monitor within fourteen working days of the end of the month to which the written update relates; and
• be sent to Monitor until such time as Monitor agrees that the improvement programme has been delivered in full or the monthly updates are no longer require;
• The Licensee will implement comprehensive and effective management and governance arrangements to enable the delivery of the improvement programme. Such arrangements will as a minimum enable the Licensee's Board to:
• Obtain clear oversight over the progress in delivering the improvement programme;• Obtain an understanding of any risks to the successful achievement of the
improvement programme; and• Hold individuals to account for the delivery of its actions.
Improvement Director• The Licensee must cooperate with an Improvement Director appointed by Monitor for
the purpose of monitoring the work of the Licensee's Board and overseeing the implementation of the Licensee's improvement programme. In particular the Licensee must;
• Invite the Improvement Director to attend meetings of the Board, and permit the Director's participation at such meetings;
• Allow the Improvement Director reasonable access to the Licensee's premises; and• Provide such information, and allow such access to documents or records, as the
Improvement Director may reasonably request.
Safe Effective Caring Responsive Well led
Page 85 of 86Doc id.: HEFT IIP Recovery Plan V0.6Doc. Owner: Stuart A Brown Doc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.215
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
14.6.APPENDIX VI - INTERIM GOVERNANCE ON BOARDING FORM
Figure 30 - Temporary resource on- boarding form
Safe Effective Caring Responsive Well led
Page 86 of 86Doc id.: HEFT IIP Recovery Plan V0.6!Doc. Owner: Stuart A BrownDoc. Status: V0.6
Integrated Improvement Plan

Council of GovernorsJune 2015
.216
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
Integrated Improvement Programme Dashboard Reporting Period: 21/05/2015
Culture and Engagement Mortality
What will we deliver? Current Month
DoT What will we deliver? Current Month
DoT
1.00 1.00
1.00 1.00
2.00 1.00
1.00
How will we measure success? 2014/15 Outturn
Current Month
DoT 2015/16 IIP Target
2015/16 YTD Actual 2015/16 FOT How will we measure success? 2014/15 Outturn
Latest data DoT 2015/16 IIP Target
2015/16 YTD Actual
2015/16 FOT
Permanent Culture Metric (TBD by 30/09/2015) Avoidable mortality (TBD by 01/01/2016)National Survey Overall Engagement Score 3.53 N/A 3.63 SHMI 109.20 104.70 100.00 Staff Engagement Survey (FFT) Staff Recommender Index % (Likely / Very Likely) 51% N/A 61% Deaths per Week 98.00 53.00 TBCStaff Engagement Survey (FFT) Staff Recommender Index Mean Score 3.26 N/A 3.40
Scheduled Care Urgent Care
What will we deliver? Current Month
DoT What will we deliver? Current Month
DoT
1.00 1.00
1.00 1.00
1.00
How will we measure success? 2014/15 Outturn
Current Month
DoT 2015/16 IIP Target
2015/16 YTD Actual 2015/16 FOT How will we measure success? 2014/15 Outturn
Current Month
DoT 2015/16 IIP Target
2015/16 YTD Actual
2015/16 FOT
Reduction in admitted pathways backlog 1,309.00 N/A 589.00 Time to Treatment in Ed (Minutes) - Admitted (95th Percentile) 981.80 683.00 480.00 Percentage of patients waiting less than 42 days (First OP appointment) 64.28% 61.43% 80.00% Time to Treatment in ED (Minutes) - Non-admitted (95th Percentile) (TBD by 30/04/2015) 298.00 269.00 240.00 Median wait time for 2 week cancer wait 12.50 13.00 10.00 Patients length of stay of 14 days or more 340.00 343.00 250.00
Median Time to Treatment in ED (Minutes) 63.00 52.00 60.00
Governance Recovery IM&T
What will we deliver? Current Month
DoT What will we deliver? Current Month
DoT
1.00 1.00
1.00 1.00
1.00 1.00
1.00 1.00
1.00
1.00
How will we measure success? 2014/15 Outturn
Current Month
DoT 2015/16 IIP Target
2015/16 YTD Actual 2015/16 FOT How will we measure success? 2014/15 Outturn
Current Month
DoT 2015/16 IIP Target
2015/16 YTD Actual
2015/16 FOT
Governor Engagement Questionnaire Metric (TBD post analysis by 1/08/2015) TBC Total number of open PMS2 system generated anomalies 50.00 50.00 0.00Formal Complaints Metric (TBD by June 2015) TBC Overall how satisfied are you with the service you received? 100.00% 92.31% 95.00%Percentage of Cost Improvement Plans with approved Quality Impact Assessment 18% 19% 100.00% Percentage of Service Desk calls resolved within SLA 97.30% 96.76% 97.00%Percentage of SUIs closed within 60 days 25% N/A 95.00%Number of patients falling twice or more during the same admission� 32.00 50.00 TBC Indicator to be developed by Programme Team
SOL Urgent Care Redesign
Engagement:A more engaged workforce through the definition and implementaion of a Trust-wide staff engagement programme
Mortality Governance Process:Refine and implement revised governance process and supporting mechanisms to capture and review mortality data with supporting processes
Values and Culture:Define a set of Trust values and embed within the culture of the organisation
Mortality Education:Develop and roll out education programme to improve Executive and Clinical understanding with regards to mortality information
Leadership:Define and implement a bespoke Trust Leadership Development Programme
Future Information Requirements:Research best practice and define Trust vision for mortality analytics
Coding:Improve clinical engagement and understanding of clinical coding
Planned Care / RTT:Implement series of initiatives to comply with nationally mandated scheduled care targets
BHH Urgent Care Redesign
Cancer:Implement series of initiatives to comply with nationally mandated cancer targets
GHH Urgent Care Redesign
Kennedy Review:Assess residual work and transfer to PMO; determine executive lead and map in to action plan
Strategy and Market Review:Develop a Trust IM&T strategy to support the Trust Corporate strategy
Strategy Development and Planning:Develop Trust strategy and establish a Data Quality Strategy and Stakeholder Engagement Survey
Improving Performance Management and Data Quality:Implement a Performance Management Framework, associated reporting data quality and governance strategies and processes
Patient Experience:A refreshed patient experience dashboard and systems to ensure learning and remediation are in place
PMS2 Recovery:Review of PMS2 to ensure fit for purpose and reliable and subsequent remediation of issues identified
Governor Engagement:To assess, refresh and implement governor engagement arrangements
Competence:Review of competence and capability of the ICT Function to support the Trusts needs and subsequent remediation of issues identified
Management of Risk and BAF:Implement revised Board Assurance Framework to strengthen the understanding of key strategic risks. Develop committee reporting structure to Trust Board.
IM&T Governance and IM&T Project Governance:Develop and implement a Trust IM&T governance structure and IM&T programme governance arrangements
HEFT IIP Dashboards 18 05 2015.xlsx - Summary 1

Council of GovernorsJune 2015
.217
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
CULTURE AND ENGAGEMENTHAZEL GUNTERALEX COVEY
OVERVIEW OF MILESTONES
Project % Complete AssessmentEngagement 67% On targetValues/Culture 35% On targetLeadership 13% Behind Schedule
KEY METRICSENGAGEMENT
VALUES / CULTURE
LEADERSHIP
DETAILED MILESTONES
% Complete Date Due Assessment
100% 01/05/2015 Completed on time
100% 30/11/2014 Completed on time
100% 31/03/2015 Completed on time
100% 01/05/2015 Completed on time
70% 03/06/2015 On target
0% 01/07/2015 On target0% 31/07/2015 On target
70% 19/06/2015 On target
30% 19/06/2015 Behind schedule
60% 30/06/2015 Behind schedule
15% 30/09/2015 On target0% 01/04/2016 On target
70% 31/05/2015 Behind schedule5% 30/06/2015 Behind schedule0% 31/07/2015 Behind schedule
20% 30/09/2015 Behind schedule
10% 31/07/2015 Behind schedule0% 31/12/2015 Behind schedule0% 01/04/2016 Behind schedule0% 30/06/2016 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Culture and Engagement Dashboard
Launch values based appraisal process for Board and complete full appraisal cycle.
Resource now in place to take forward
CommentaryKey OutputThe completeness of the engagement workstreamsThe completeness of the values and cultures workstreamsThe completeness of the leadership workstreams
Plan in place and on track, event scheduled and distribution of pre-surveys commenced
Key Output
Scheduled to go to Board for sign off 02.06.15
Resource requirement identified for OD Manager, interviews w/e 15.05.15
Survey in place
(NB: ED reports to Urgent Care Improvement Board.) 5 events held, 9 additional events scheduled
Agree baselines for all nine categories of the quarterly Pulse Staff Engagement Survey and forecast targets for the 3 key enablers.Values / Culture
Identify and recruit appropriate resource accountable for delivery of the values implementation plan and appraisal process.
Resource requirement identified for OD Manager, interviews w/e 15.05.15
Define and develop permanent culture metric once values are agreed.
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Undertake analysis of first quarterly Pulse Staff Engagement Survey results at Trust level.
Implement "Engaging Teams" programme for first cohort
Develop and agree Trust values through Trust wide consultation for Board approval and sign off.Develop a locally led Trust values implementation plan.
CommentaryEngagement
Committee dates planned, ToRs etc established
Preparation of new quarterly Pulse Staff Engagement Survey based on WWL model.
Implement Workforce Committee chaired by NED and a Staff Engagement Steering Committee chaired by Chief Executive.
Implement senior led Staff Engagement Events reporting to the Staff Engagement Steering Committee.
Roll out Pulse Staff Engagement Survey across 25% of the workforce per quarter.
Provide clear analysis of current leadership development programmes within the Trust.
Implement succession plan for all executive board members.
Leadership
Define current and future leadership needs. Initial stakeholder meetings underwayConduct a gap analysis between defined needs and current status
Develop a practical plan to improve leadership across the Trust.Agree a bespoke Leadership Development Framework and then implement a bespoke Leadership Development Programme.Implement a system to monitor and track delivery of the Leadership Development Programme.
Identify current leadership support active across the Trust within senior teams and, ensuring a cohesive approach, communicate the support available.
2.00
2.50
3.00
3.50
4.00
Q1 2015/16 Q2 2015/16 Q3 2015/16 Q4 2015/16
Scor
e
Temporary Culture Metric Staff Engagement Survey (Pulse)
Clarity Enabler
Actual Target
0%
20%
40%
60%
80%
100%
Q32014/15
Q42014/15
Q12015/16
Q22015/16
Q32015/16
Q42015/16
Permanent Culture Metric
Actual Target
2.00
2.50
3.00
3.50
4.00
Q1 2015/16 Q2 2015/16 Q3 2015/16 Q4 2015/16
Scor
e
Temporary Culture Metric Staff Engagement Survey (Pulse)
Trust Enabler
Actual Target
Board Succession Plan
Staggered delivery of 1+1 Succession Plans commencing from Q1 2016/17.
Metric provider: Alex Covey
Last provided: N/A Next expected date: July 2016
3.53
3.63 3.75 3.80
2.5
3
3.5
4
4.5
Scor
e
National Staff Survey Overall Engagement Score
Actual Target
45% 51% 54% 57% 59% 61%
35%
45%
55%
65%
75%Sc
ore
Staff Engagement Survey (FFT) Staff Recommender Index
% (Likely/Very Likely)
Actual Target
3.24 3.26
3.28 3.31 3.34 3.40
2.20
2.60
3.00
3.40
3.80
Scor
e
Staff Engagement Survey (FFT) Staff Recommender Index
Mean Score
Actual Target
0%
50%
75% 100% 100%
0%
20%
40%
60%
80%
100%
Executive Board Members roles with an approved Succession Plan
Actual Target
Staff Engagement Survey (Pulse) Clarity and Trust Enablers
Enablers scored out of five. Range
typically 2.0-4.0.
Awaiting first actual measure following Pulse survey results for
Q1 2015. No target available until Q2 2015 Pulse survey results are
calculated and volatility understood.
Metric provider: Alex Covey
Last provided: n/a
Permanent Culture Metric
Indicator to be developed by 30.09.2015
Metric provider: Alex Covey
Last provided: n/a Next expected date: October 2015
NSS Overall Engagement Score.
Annual measure - scores out of five.
Typical range for a high score is 3.8 and low score is 3.6.
Metric provider: Alex Covey
Last provided: 30th April 2015 Next expected date: April 2016
Staff Engagement Survey (FFT) Staff Recommender Index
% and Mean Score
Answer to question: How likely to recommend Trust as a place to work?
% = proportion of positive recommendations (either a score of 4 (likely) or 5 (very likely)).
Mean = reflects average of all five scores from all responses.
Metric provider: Alex Covey Last provided: 30th April 2015 Next expected date: July 2015
TBC upon agreement of Values and delivery of Values implementation plan.
IIP PMO recommended
HEFT IIP Dashboards 18 05 2015.xlsxCULTURE AND ENGAGEMENT 2

Council of GovernorsJune 2015
.218
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
IM&TJONATHAN REXCAROLINE SADLER
OVERVIEW OF MILESTONES
Project Key Output % Complete AssessmentPMS2 Recovery
Review of PMS2 to ensure fit for purpose and reliable and subsequent remediation of issues identified. 100% On target
Competence Review of competence and capability of the ICT Function to support the Trusts needs and subsequent remediation of issues identified.
70% On target
IM&T Governance and IM&T Project GovernanceDevelop and implement a Trust IM&T governance structure and IM&T programme governance arrangements. 77% On target
Strategy and Market Review Develop a Trust IM&T strategy to support the Trust Corporate strategy. 20% On target
KEY METRICSPMS2 Recovery
Competence Indicators
DETAILED MILESTONES
% Complete Date Due Assessment
100% 31/03/2015 Completed on time100% 01/02/2015 Completed on time100% 01/04/2016 Completed on time100% 28/04/2015 Completed on time100% 31/05/2015 Completed on time
100% 28/02/2015 Completed on time100% 31/01/2015 Completed on time100% 31/01/2015 Completed on time20% 30/09/2015 On target0% 30/06/2015 On target0% 30/09/2015 On target
100% 28/02/2015 Completed on time65% 30/09/2015 On target80% 01/06/2015 On target
100% 31/03/2015 Completed on time
40% 31/08/2015 On target
0% 31/05/2015 On target15% 31/05/2015 On target80% 01/06/2015 On target
0% 31/07/2015 On target
0% 11/09/2015 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Culture and Engagement Dashboard
Commission and perform a full technical review of PMS2.
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Commentary
Note the competence and capability will be revisited once the ICT strategy is drafted and again once the ICT strategy is finalised.
Key Output CommentaryPMS2 Recovery
Identify and recruit an interim ICT Director.
Reinstate the PMS2 project board.Develop and deliver enhanced PMS2 training for end users. Ongoing - training commenced in April as planned.Project sign off by the Project Board.Review lessons learned from the PMS2 project and implement an associated action plan. PMS2 User Group established to exploit leassons learned and action plan as per Business As Usual.CompetenceIdentify and recruit a NED capable of providing challenge relating to IM&T.
Establish a clinical IM&T sub-group with an agreed terms of reference and membership to provide clinical input to IM&T projects.
Commission and perform an independent review of the ICT function and capability.Develop and implement an action plan following the independent review of the ICT function and capability.Revisit the competence requirements upon agreement of the draft ICT strategy.Revisit the competence requirements upon agreement of the final ICT strategy.IM&T Governance and IM&T Project GovernanceEstablish an IM&T Steering Committee with suitable executive sponsorship. IM&T Steering Committee established and operational. Chaired by the relevant NED.
Establish and pilot the CCIO position to lead the clinical IM&T sub-group. CCIO resource confirmed. Interim Director of ICT to advise confirmation to proceed.Review, refresh and implement IM&T governance process and arrangements and enforce for new projects.
Governance arrangements for all existing in-flight projects to be reviewed and refreshed as necessary. IM&T Steering Committee and Clinical IT Committee in place to review Governance. CCIO post to support Governance requirements.
Obtain feedback on the draft IM&T strategy.
Refine the IM&T strategy and submit for Board approval.
Strategy and Market ReviewCommission and perform an independent strategic and market review.Perform strategy workshops with the clinical sub-group and representatives from the directorates. Dates scheduled for 3 x workshops at BHH, GHH and Sol.Develop an initial draft of the IM&T strategy. Meetings commenced. Deloitte to develop ICT strategy.
01,0002,0003,0004,0005,0006,0007,0008,0009,000
No.
of A
nom
alie
s
Open PMS2 System Generated Anomalies
Actual
88%
90%
92%
94%
96%
98%
100%
Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15
Overall how satisfied are you with the service you received?
Satisfied Target
90%
92%
94%
96%
98%
100%
Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15
Service desk calls resolved in SLA
Actual Target
Overall ICT Satisfaction Score
This is based on a monthly survey requesting feedback and measuring overall satisfaction for the ICT team. The
percentage of respondents who were satisfied overall is measured each month by this means.
Metric provider: Jonathan Rex Last provided: 14th May 2015
Next expected date: 14th June 2015
Service desk calls resolved in SLA
The percentage of calls resolved within agreed Service Level Agreements by the ICT helpdesk.
Metric provider: Jonathan Rex Last provided: 14th May 2015
Next expected date: 14th June 2015
Clearance of PMS2 System generated anomalies
This metric represents the number of open issues with regards to PMS2 System generated anomalies. Note this does not
include anomalies generated by user error.
Metric provider: Jonathan Daniels Last provided: 28th April 2015
Next expected date: 28th May 2015
IIP PMO recommended
HEFT IIP Dashboards 18 05 2015.xlsxIM&T 3

Council of GovernorsJune 2015
.219
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
GOVERNANCE RECOVERYSAM FOSTERANGELA HOPPER
KEY MILESTONE TRACKER
Project Key Output % Complete Date Due Assessment
Board Leadership and Development
Develop a clear set of values and behaviours for the Trust and improve board cohesion N/A N/A N/A
Patient Experience A refreshed patient experience dashboard and systems to ensure learning and remediation are in place 29% 30/06/2015 On target
Culture and Values Development
Implement an Organisation Development Plan N/A N/A N/A
Governor Engagement To assess, refresh and implement governor engagement arrangements 62% 30/07/2015 On target
Management of Risk and BAFImplement revised Board Assurance Framework to strengthen the understanding of key strategic risks. Develop committee reporting structure to Trust Board.
9% 30/09/2015 On target
Kennedy Review Assess residual work and transfer to PMO; determine executive lead and map in to action plan 90% 29/06/2015 On target
Strategy Development and Planning
Develop Trust strategy , Annual planning process and Stakeholder Engagement process 29% 31/03/2016 On target
Improving Performance Management and Data Quality
Implement a Performance Management Framework, associated reporting data quality and governance strategies and processes 54% 30/06/2016 On target
KEY PERFORMANCE TRACKERPATIENT EXPERIENCE
GOVERNOR ENGAGEMENT
MANAGEMENT OF RISK AND BAF
Apr-13May-13Jun-13Jul-13
Aug-13Sep-13Oct-13Nov-13Dec-13Jan-14Feb-14Mar-14Apr-14
May-14Jun-14Jul-14
Aug-14Sep-14Oct-14Nov-14Dec-14Jan-15
Replaces "Communication and Information reporting" and "People Engagement"
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Commentary
N/A: Transferred to Culture and Engagement workstream
N/A: Transferred to Culture and Engagement workstream
Replaces "Improving Risk Management" and "Improving structures and committee membership"
18% 19%
0%
20%
40%
60%
80%
100%
120%
28/0
4/20
15
05/0
5/20
15
12/0
5/20
15
19/0
5/20
15
26/0
5/20
15
02/0
6/20
15
09/0
6/20
15
16/0
6/20
15
23/0
6/20
15
30/0
6/20
15
07/0
7/20
15
14/0
7/20
15
% of CIP Plans with approved QIA
Trust Target Actual Planned Improvement
0%
20%
40%
60%
80%
100%
120%
Apr
May Jun Jul
Aug
Sep
Oct
Nov De
c
Jan
Feb
Governor Engagement Metric
Trust Target Actual Planned Improvement
Governor Engagement Questionnaire
Governor questionnaire to be developed by 30.04.2015, analysis to
be carried out mid July
Metric provider: Kevin Smith Last provided:
Next expected date:
Issue 1
Complaints often have more than one issues raised therefore the primary number is not fully reflective of the
possible areas of concern.
The second figure represents where attitude and behaviour is a sub theme.
National Averages and Planned
Improvements TBC by SRO.
Metric provider: Richard Brown Workstream lead: Helen Shoker
Last provided: 28th April 2015 Next expected date: 13th May 2015
0
20
40
60
80
100
120
0%
5%
10%
15%
20%
25%
30%
2014/15 May Jul Sep Nov Jan Mar
Formal complaints closed within planned timescales
Trust Target Actual Planned Improvement Total Complaints
119 151
123
303 288
213
247
23 23 19 25 0
50
100
150
200
250
300
350
Q1 2014/15 Q2 2014/15 Q3 2014/15 Q4 2014/15 Q1 2015/16 Q2 2015/16
No.
of C
ompl
aint
s
Top three areas of formal complaints Issue 1 - Staff Attitude and Behaviour
National Average No. of complaints for Issue (All)
Planned Improvement (All) Total Complaints
No. of complaints for Issue (Primary) Planned Improvement (Primary)
Patient Complaints
Trust currently achieving 26.5% of complaints response within 25 working days.
The trust is developing complaints handling which is
alligned to national guidance and regulatory compliance, anticipated to implement July 2015.
This will provide robust complaint handling data, by which performance can be measured.
Metric provider: Richard Brown Workstream lead: Helen Shoker
Last provided: n/a Next expected date: 13th May 2015
230 218
179
303 288
213
247
38 33 24 29
0
50
100
150
200
250
300
350
Q1 2014/15 Q2 2014/15 Q3 2014/15 Q4 2014/15 Q1 2015/16 Q2 2015/16
No.
of C
ompl
aint
s
Top three areas of formal complaints Issue 2 - Delays and Cancellations
National Average No. of complaints for Issue (All)
Planned Improvement (All) Total Complaints
No. of complaints for Issue (Primary) Planned Improvement (Primary)
92
120
88
303 288
213 247
0
50
100
150
200
250
300
350
Q1 2014/15 Q2 2014/15 Q3 2014/15 Q4 2014/15 Q1 2015/16 Q2 2015/16
No.
of C
ompl
aint
s Top three areas of formal complaints
Issue 3 - Query Appropriate Treatment
National Average No. of complaints for Issue (All)
Planned Improvement (All) Total Complaints
No. of complaints for Issue (Primary) Planned Improvement (Primary)
Issue 2
Complaints often have more than one issues raised therefore the primary number is not fully reflective of the
possible areas of concern.
The second figure represents where attitude and behaviour is a sub theme.
National Averages and Planned
Improvements TBC by SRO.
Metric provider: Richard Brown Workstream lead: Helen Shoker
Last provided: 28th April 2015 Next expected date: 13th May 2015
Issue 3
Complaints often have more than one issues raised therefore the primary number is not fully reflective of the
possible areas of concern.
The second figure represents where attitude and behaviour is a sub theme.
Awaiting primary reason data for this
issue.
Metric provider: Richard Brown Workstream lead: Helen Shoker
Last provided: 28th April 2015 Next expected date: 13th May 2015
To be defined once questionnaire rolled out
% of QIAs with conditions approved at Trust Board
Metric to be developed as part of Trust's new QIA approval process.
Metric provider: Aidan Quinn
Last provided: n/a Next expected date: n/a
0
5
10
15
20
25
30
35
May
-13
Jul-1
3
Sep-
13
Nov
-13
Jan-
14
Mar
-14
May
-14
Jul-1
4
Sep-
14
Nov
-14
Jan-
15
Mar
-15
No.
of p
ress
ure
ulce
rs
Number of grade 2 hospital acquired pressure ulcers determined as avoidable
Actual - Grade 2
0
10
20
30
40
50
60
70
80
Apr-
13
May
-13
Jun-
13
Jul-1
3
Aug-
13
Sep-
13
Oct
-13
Nov
-13
Dec-
13
Jan-
14
Feb-
14
Mar
-14
Number of patients falling twice or more during the same admission (April 13 - March 15)
Target Actual Planned Improvement
0
20
40
60
80
100
120
140
160
180
Apr-
12
Jul-1
2
Oct
-12
Jan-
13
Apr-
13
Jul-1
3
Oct
-13
Jan-
14
Apr-
14
Jul-1
4
Oct
-14
Jan-
15
Apr-
15
Jul-1
5
Oct
-15
Jan-
16
IR1 Medication - Administration Errors
Target Actual Planned Improvement
Number of patients falling twice or more during the same admission
Target TBC as part of contractual
negotiations by 31.05.2015
Metric provider: Diane Povey Last provided: 28th April 2015
Next expected date: 22nd May 2015
Medication IR1
The number of medicine administraton errors reported each
month.
Trust target to be developed as part of contractual negotiations by
31.05.2015
Metric provider: Tim Burroughes Last provided: 13th May 2015
Next expected date: 13th June 2015
0%
20%
40%
60%
80%
100%
120%
Apr
May Jun Jul
Aug
Sep
Oct
Nov De
c
Jan
Feb
% of QIAs with conditions approved at Trust Board
Trust Target Actual Planned Improvement
25%
3
0
1
2
3
4
5
0%
20%
40%
60%
80%
100%
Q4 2014/15 Q1 2015/16 Q2 2015/16 Q3 2015/16 Q4 2015/16
% of SUI closed within 60 days
Actual Planned Improvement Total no of SUIs
To be developed
% of CIP Plans with approved QIA
All CIP plans will have undertaken a Quality Impact Assessment by Medical
Director and Director of Nursing as part of the new QIA process being
developed by Finance to review each new CIP plan as developed and
approved.
Metric provider: Adam Winstanley Last provided: 13th May 2015
Next expected date: 22nd May 2015
% of SUI closed within 60 days
To comply with new statutory national guidance
Metric provider: Sarah Carr-Cave
Last provided: 28th April 2015 Next expected date: July 2015
Number of grade 2 hospital acquired pressure ulcers determined as avoidable
Target TBC as part of contractual
negotiations by 31.05.2015
Metric provider: Diane Povey Last provided: 13th May 2015
Next expected date: 13th June 2015
IIP PMO recommended
IIP PMO recommended
Data from April 2015 may be
subject to change
Monthly Reporting to be developed
Monthly Reporting to be developed Monthly Reporting to be developed
Monthly Reporting to be developed
HEFT IIP Dashboards 18 05 2015.xlsxGOVERNANCE RECOVERY 4

Council of GovernorsJune 2015
.220
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
IMPROVING PERFORMANCE AND DATA QUALITY MANAGEMENT
DETAILED MILESTONES
% Complete Date Due Assessment
60% 30/06/2015 On target
50% 30/06/2015 On target
50% 30/09/2015 On target
5% 30/09/2015 On target
5% 30/09/2015 On target5% 30/09/2015 On target
100% 30/04/2015 Completed on time
10% 08/07/2015 On target0% 30/07/2015 Not started
100% Active from Jan 2015 Completed on time100% Active from Jan 2015 Completed on time
Improving Risk Management5% 05/06/2015 On target0% 18/08/2015 On target
10% 15/07/2015 On target
10% 31/08/2015 On target
50% 17/07/2015 On target0% 17/07/2015 On target0% 08/09/2015 On target
20% 28/05/2015 On target0% 20/06/2015 On target0% 03/07/2015 On target
10% 30/09/2015 On target
75% 31/03/2016 On target
100% 15/05/2015 Completed on time
0% 15/06/2015 On target
40% 08/09/2015 On target
100% 30/04/2015 Completed on time50% 24/05/2015 On target
0% 30/09/2015 On target
0% 30/11/2015 On target0% 31/03/2016 On target0% 01/08/2015 On target0% 01/08/2015 On target
100% 27/01/2015 Completed on time100% 31/03/2015 Completed on time
0% 30/06/2015 On target100% 30/04/2015 Completed on time98% 19/05/2015 On target0% 30/06/2015 On target
60% 30/06/2015 On target60% 30/09/2015 On target10% 31/03/2016 On target
100% 19/12/2014 Completed on time80% 31/05/2015 On target50% 31/05/2015 On target0% 31/06/2015 On target0% 30/03/2016 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Governance Recovery Dashboard
Draft strategy developed. To be submitted to Board 26.5.15. External capacity provided to support this.
Data quality metrics agreedDQ Strategy implemented - Refresh Divisional and Board architecture for DQ
Core KPI’s across domains including divisionally specific KPIs approved by EMBCore KPIs approved by Board Agreed PMF architecture specifically for the FPC is in placeCommunication plan for PMF including launch eventPMF embeddedDraft Data Quality Strategy
Staff consultation completed. Analysis in progress.
Process developed for engaging external stakeholders in developing corporate strategy (Recovery and On-going) Not yet started
Dependent on Board approval
Going to June Board
DQ Strategy approved by IGC
Core KPI’s across domains including divisionally specific KPIs proposed to executives
Identify supporting strategies including Quality StrategySupporting strategies specified and developed and aligned to corporate strategy Planning processes and cycle which enable:-Definition of strategy owners and stakeholders; delivery schedules-Delivery of directorate, other clinical and supporting strategies which include outcomes-Stakeholder engagementAnnual planning process and cycle communicated to all key staffOrganisation operating according to planning process and cycleAgreed overall future role for the newly established Citizens Assembly as well as its role in strategy development
PMF approved by Board
Draft PMFPMF approved by EMB
New BAF Committee and divisonal board structure and report pathways launched
Divisional leaders trained (interdependent on Leadership programme within Culture and Engagement workstream)
Due to start 15.6.2015
Corporate strategy developed with evidence of stakeholder engagement and clear responsibilities and timelines for delivery of strategic goals
Documented shared expectations including programme for governor training and evaluation process Dependent on outcome of workshopBoard members presentations to governors on a rotational basis BAURoutine reports from Executive team highlighting key issues (ahead of meetings to enable time for review) BAU
Board Assurance Framework (to include committee structure improvement) drafted BAF work commenced with external support
Board trained on BAF (interdependent on Leadership programme within Culture and Engagement workstream) Workshop planned for 15/7/15
Working with IIP leadership to design launch events
Risk management strategy drafted First draft completePlanned for 17/7/15
Finance to issue or CIP scheme to GM's and CD's for QIA completion
Develop SEIP policy to include QIA approval and monitoring structures
Risk management strategy launched at Board Planned for 8/9/15
Establish weekly meeting report to review QIA at SIEP meetingsFinance provided summary status and next steps to chief nurse and chief medical officer
Facilitated workshop session on shared expectations Workshop booked
Refreshed patient experience metrics clearly visible across Trust and prominent within BAF and PMF; also visible to external stakeholders Collaborative action plan in place to deliver
New systems developed and documented which ensure learning from events, trends and best practice; remediation and evaluation of interventions to demonstrate impact / improvement
Linked to BAF & PMF workstreams
Sub Board leadership teams appropriately use systems to inform achievements, performance and delivery Linked to BAF & PMF workstreamsUpdated web site functionality for patient feedback and engagement Scoping commencedGovernor Engagement
Questionnaire to assist in understanding between Governors and Trust BoardQuestionnaire issued and responses starting to arrive. Reminder sent.
Board Assurance Framework agreed As above
Refreshed patient experience dashboard fed in to PMF work stream Dashboard progressing in line with strategy development
Key Output CommentaryPatient Experience
Patient experience metrics and feedback processes assessed against ‘what good looks like’ and remediation plan documented12/14 actions have commenced, 2 have risks associated with timescales
On track
New serious reporting framework (March 2015) and never events guidance implementedTarget date for policy refresh is 15/06/2015 (June EMB to approve)
DQ Strategy embedded and Board applying suite of metrics to assure on data quality
Risk management strategy approved by QRC
Citizens Assembly has informed Trust strategy development & review processImproving Performance Management and Data Quality Management
Initial metrics to go to Board in May
Strategy developed and agreedGoing to IGC in MayGoing to IGC in MayDependent on above
Shared with execs and approved by PMBAs aboveJune Board
Comms aligning with wider workstream
Discussed at exec meeting 13.5.15
Scheduled to reestablish working group for annual planning process development 09/09/2015
Strategy Development and Planning
Process developed for engaging internal stakeholders in developing corporate strategy (Recovery and On-going)
Target Actual Planned Improvement
Placeholder: KPI to be defined upon definition of data quality metrics
HEFT IIP Dashboards 18 05 2015.xlsxGOVERNANCE RECOVERY 5

Council of GovernorsJune 2015
.221
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
SCHEDULED CAREJONATHAN BROTHERTONAMANDA MARKALL
KEY MILESTONE TRACKER
Project Key Output % Complete Month Due AssessmentPlanned care/RTT Implement series of initiatives to comply with nationally mandated scheduled care targets 63% 31/03/2016 On targetCancer Implement series of initiatives to comply with nationally mandated cancer targets 41% 31/12/2015 On target
KEY METRICS
Mar-15Apr-15
May-15Jun-15Jul-15
Aug-15Sep-15Oct-15
Nov-15Dec-15Jan-16Feb-16Mar-16
DETAILED MILESTONES
% Complete Date Due Assessment
50% 31/03/2016 On target
100% 01/05/2015 Completed on time
30% 31/12/2015 On target
60% 30/06/2015 On target
75% 31/03/2016 On target
65% 30/09/2015 On target
75% 31/05/2015 On target
10% 31/12/2015 On target
40% 30/09/2015 On target
40% 31/08/2015 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Scheduled Care Dashboard
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Commentary
Key Output CommentaryPlanned Care/RTTMonitor and manage performance against trajectories Unvalidated position positive, with performance ahead of trajectory
The Trust will have no avoidable breaches to 52 week standard There were however 59 unavoidable breaches due to the closure of legacy open clock pathways and this will continue until all legacy open clock pathways are closed.
Centralise management of all surgical specialty IPWL Directorate meetings planned with remaining non-centralised specialties in June and July
Agree and embed processes to ensure appropriate management of patients on an Open Clock Pathway Processes have been agreed and are being closely monitored until they are fully embedded.
Transfer all waiting list management standalone systems to PMS2 Only 3 out of 100 systems still outstanidng to be transferred. Plans are in development to migrate and a manual data quality process is being developed for all 3 systems in theinterim to mitigate any risk.
Ensure that no "category 1" patient will have their surgery cancelled due to "no bed" There have been no cancellations of patients on BHH or Solihull sites with, or suspected of having cancer in April. There was 1 cancellation on the BHH site due to no Critical Care bed. RCA has been undertaken, escalation process has been reiterated and further actions have been put into place.
Cancer
Implement new best practice pathways in Urology and Lung to improve 31/62 day performance Whilst fundamental agreement has been reached for some elements of both pathways, consistent improvement in performance is yet to be seen. A refresh of both pathways is taking place in May with workshops with the MDT planned.
New trajectory to be agreed based on revised plans which illustrates an improvement in performance and achievement of 93% 2 week wait standard Individual specialties' plans to deliver a median wait time of 10 days or less to be in place by end of May.
Through delivery of revised plans reduce the median wait time to 10 days or less by cancer site. Only 1 cancer site out of 10, achieved a median wait of 10 days in April. 70% of cancer site median wait times were 12 or 13 days. No site had median wait times over 13 days.
Develop and embed processes with CCG to share information and find solutions to improve levels of patient choice breaches. Fundamental agreement and support from CCG address patient choice breaches. Gynaecology referral form will be launched in early June following cross organisatonal facilitation by CCG. Referring GP has to acknowledge on all new referral forms (skin has already been launched and urology and lung are in development), that the patient has been told they are on a cancer pathway. An electronic audit of all new referral forms will take place in Q2 and Q3 and the results of this will be discussed directly with GPs and at CCG forum. Regular communications regarding 2ww guidance is sent to all GPs. Further work in Q1 to identify conversion rates by GP practice to be undertaken and circulated. Conversion rates for some sites is as low at 4% Patient stories to be anonymised and circulated to GPs to highlight the importance of patients being made aware at referral that they are on a cancer pathway.
0
200
400
600
800
1,000
1,200
1,400
1,600
Mar-15 May-15 Jul-15 Sep-15 Nov-15 Jan-16 Mar-16
No
of P
atie
nts
Admitted Pathways Backlog Trajectory
National Target Actual Planned Backlog Clearance
Admitted Pathway Backlog
This indicator demonstrates the expected reduction in backlog of patients waiting more than 18 weeks for their care to be completed on an admitted pathway. The rise in backlog in Quarter 2 reflects the expected increase in
backlog in Gastroenterology which will begin to reduce in August .
Acheiving the expected reduction in backlog will enable the 90% Admitted RTT Standard to be acheived.
National submission of RTT data occurs on the 14th working day of each month. Performance for April is expected to be ahead of trajectory and will be available on the 22/5/15.
Metric provider: Robert Watkins
Last provided: 28th April 2015 Next expected date: 22nd May 2015
40%
50%
60%
70%
80%
90%
Apr-13 Aug-13 Dec-13 Apr-14 Aug-14 Dec-14 Apr-15 Aug-15 Dec-15
% of patients waiting less than 42 days for first OP appointment
Trust Target Actual Planned Improvement
0
2
4
6
8
10
12
14
16
Apr-13 Jul-13 Oct-13 Jan-14 Apr-14 Jul-14 Oct-14 Jan-15 Apr-15 Jul-15 Oct-15
Days
Median wait time for two week cancer waits
Target Actual Planned Improvement
% of patients waiting less than 42 days for first OP appointment (surgical specialties and gastroenterology)
Data shows % of patients waiting less than 42 days for first OP appointment
for those patients who have had a first appointment. The data measures the time from their referral into the Trust, up until that date of first attendance.
This indicator demonstrates the expected increase in patients being seen withing 42 days of GP referral received in the organisation ,to patient being seen in an out patient clinic.
Acheiving the standard of 80% will provide greater certainty that patient pathways (both Admitted and Non -Admitted) will be completed within 18 weeks,as there will be adequate time to undertake necessary diagnostic
and theraputic procedures.
Metric provider: Robert Watkins Last provided: 13th May 2015
Next expected date: 13th June 2015
Median wait time for two week cancer waits
This indicator demonstrates the expected reduction in median wait time s for patients on a 2 week wait pathway, from GP referral to being seen in an out patient clinic ,or for Upper and Lower GI , to undergoing diagnostic
endoscopic proceure. Acheiving the standard of 10 days or less will significantly imrove performance of the 2 week wait standard and
, for those patients who are positibvely diagnosed , will give greater certainty that their treatment will be completed within 31 or 62 days.
Metric provider: Robert Watkins
Last provided: 13th May 2015 Next expected date: 13th June 2015
IIP PMO recommended
HEFT IIP Dashboards 18 05 2015.xlsxSCHEDULED CARE 6

Council of GovernorsJune 2015
.222
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
URGENT CAREJONATHAN BROTHERTONANDREW STENTON
KEY MILESTONE TRACKER
Project Key Output % Complete Month Due Assessment
BHH Urgent Care Implement series of initiatives to improve compliance with the national emergency care 4 hr standard. 27% 31/03/2016 On target
SOL Urgent care Implement series of initiatives to maintain compliance with the national emergency care 4 hr standard. 34% 31/03/2016 On target
GHH Urgent Care Implement series of initiatives to improve compliance with the national emergency care 4 hr standard. 18% 31/03/2016 On target
KEY METRICS
04/05/1405/05/1406/05/1407/05/1408/05/1409/05/1410/05/1411/05/1412/05/1413/05/1414/05/1415/05/1416/05/1417/05/14
DETAILED MILESTONES
% Complete Date Due Assessment
29%30/03/2016 On target
20%30/03/2016 On target
33% 01/10/2015 On target33%
01/07/2015 On target
29% 30/03/2016 On target10%
01/10/2015 On target
35%08/01/2016 On target
47% 01/10/2015 On target
25%30/08/2015 On target
20% 13/10/2015 On target
27%08/01/2016 On target
50%30/09/2015 On target
11%30/11/2015 On target
14%30/10/2015 On target
40%30/09/2015 On target
20%31/10/2015 On target
15%30/09/2015 On target
10%31/07/2015 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Urgent Care Dashboard
Improving ED flow to improve patient experience and reduce 4 hr breaches GP in ED model agreed, first phase in place. Additional ED consultant cover in place.
Development of a site-wide bed reconfiguration plan Bed requirements assessed. Ward 3 opened - effectiveness to be assessed.
Develop and approach that sustains effective communications with all stakeholders Initial discussions with GPs gaining ground towards joint developments
AMU and short stay areas development Acute Medical cover in place 7 days per week Initial frailty model in place.
Development of the Ambulatory Emergency Care Process Revised opening hours in place with temporary solution.
Development of improved patient flow, discharge and Post Acute Care ie: Discharge to Assess Business Case developed. Drive 4 Discharge process in place
GHH
Key Output CommentaryBHH
Interim staffing structure in place, Real time bed information project progressing
Consolidated Plan to Improve Discharge Significant progress for targeted pilot wards
SOL
Development of Site Escalation and Site Office Structures and Systems Interim staffing solution in place Business Case nearing completion
Development of the Ambulatory Emergency Care Policies reviewed and agreed, model of care agreed
Improvement Programme for the AMU and Short Stay Areas Bed model and senior staffing model agreed
Consolidated Plan to Improve Discharge 'Improving Discharge' initiative continues to be driven until embedded.
Improvement programme for the ED Departments Interim solution in place for staffing model
Development of Site Escalation and Site Office Structures and Systems
Development of improved Post Acute Care Provision to support early discharge Discharge to assess discussions progressing
Develop and deliver supporting Comms and Engagement for the whole programme Successful roll-out of Drive 4 Discharge initiative with good understanding and engagement
Improvement programme for the ED Departments Clarification of roles and enhancement of senior clinician availability. Plan completed for Majors Area expansion
Development of the Ambulatory Emergency Care AEC established, agreements on additional opening hours for BHH
Improvement Programme for the AMU and Short Stay Areas Drive 4 Discharge process in place
Focus on improvements in ED following initial improvements in flow
Focus on maintaining performance
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Commentary
Focus on creating flow in Acute pathways.
100
200
300
400
04/05/14 04/10/14 04/03/15 04/08/15 04/01/16
No.
of P
atie
nts
Patient length of stay of 14 days or more
National Target Actual Planned Improvement
300
400
500
600
700
800
900
1,000
1,100
Feb-14 May-14 Aug-14 Nov-14 Feb-15 May-15 Aug-15
Min
utes
Time in the Emergency Department - Admitted (95th percentile)
Admitted Target Admitted Actual Planned Improvement
0
10
20
30
40
50
60
70
Feb-
14
Mar
-14
Apr-
14
May
-14
Jun-
14
Jul-1
4
Aug-
14
Sep-
14
Oct
-14
Nov
-14
Dec-
14
Jan-
15
Feb-
15
Mar
-15
Apr-
15
Min
utes
Median Time to Treatment in ED
Target Actual
150
200
250
300
350
400
Feb-14 Jun-14 Oct-14 Feb-15 Jun-15 Oct-15 Feb-16
Min
utes
Time in the Emergency Department - Non-admitted (95th percentile)
Non-admitted Target Non-admitted Actual Planned Improvement
Patient length of stay of 14 days or more
This 14 day indicator demonstrates the
number of patients on site at midnight,whose Length of Stay exceeds 14 days. Achieving the Trust target of 250 would support the release of beds
which will improve flow on site and reduce front end pressure.
Metric provider: Mark Patel
Last provided: 13th May 2015 Next expected date: 20th May 2015
Median time to Treatment in ED
This ED indicator reflects the amount of initial delay experienced by a patient once they have arrived in ED. Any delays at this point can have a significant impact on 4hr
breach performance. This indicator is crucial and supports the Trust's intention to improve the current breach profile to
meet and exceed the national emergency care standard
Metric provider: Robert Watkins
Last provided: 14th May 2015 Next expected date: 13th June 2015
Time in the Emergency Department - Admitted
(95th percentile)
This indicator demonstrates the average length of time patients will wait, who require admission to an acute bed. The target for the Trust being 4 hrs or less. Achieving and
maintaining this level of performance will be a result of the improvement
work around the ED, AMU and Hospital Flow projects.
Metric provider: Robert Watkins
Last provided: 14th May 2015
Time in the Emergency Department - Non-admitted
(95th percentile)
This indicator demonstrates the average length of time patients will wait, who are discharged from the Trust. Early decision making by a senior clinician within ED in
this respect will help will improve the 4 hr performance.
Metric provider: Robert Watkins
Last provided: 14th May 2015 Next expected date: 13th June 2015
IIP PMO recommended
HEFT IIP Dashboards 18 05 2015.xlsxURGENT CARE 7

Council of GovernorsJune 2015
.223
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
HEFT IIP Dashboards
DRAFT FOR DISCUSSION ONLY
MORTALITYCLIVE RYDERANN KEOGH
KEY MILESTONE TRACKER
Project Key Output % Complete Date Due Assessment
Mortality Governance ProcessRefine and implement revised process and supporting mechanisms to capture and review mortality data with supporting governance process
60% 28/02/2016 On target
Mortality Education Develop and roll out education programme to improve Executive and Clinical understanding with regards to mortality information
5% 31/01/2016 On targetOn target
Future Information Requirements Research best practice and define Trust vision for mortality analytics 5% 31/12/2015 On targetCompleted on time
Coding Improve clinical engagement and understanding of clinical coding 30% 31/01/2016 On targetCompleted late
KEY METRICS
DR FOSTER, QUARTERLY SHMI
PeriodFY2014/15 Q1FY2013/14 Q4FY2013/14 Q3FY2013/14 Q2FY2013/14 Q1FY2012/13 Q4FY2012/13 Q3FY2012/13 Q2FY2012/13 Q1FY2011/12 Q4FY2011/12 Q3FY2011/12 Q2
Oct 11-Sept 12Jan 12-Dec12Apr 12-Mar13Jul 12-Jun 13Oct 12-Sept 13Jan13-Dec 13
DETAILED MILESTONES
% Complete Date Due Assessment
70% 31/05/2015 On target80% 30/06/2015 On target
30% 30/06/2015 On target
5% 31/08/2015 On target
0% 31/08/2015 On target0% 28/02/2016 On target
10% 28/02/2016 On target
5% 31/07/2015 On target0% 31/07/2015 On target0% 31/01/2016 On target
Coding30% 31/05/2015 On target20% 31/01/2016 On target
10% 31/08/2015 On target0% 31/12/2015 On target
Last Updated: 18th May 2015Heart of England NHS Foundation Trust Mortality Dashboard
Review current Mortality and Morbidity Performance Group, including ToR, membership, roles and responsibilities and agree reporting governance
PROGRAMME:SENIOR RESPONSIBLE OFFICER:
PROGRAMME DIRECTOR:
Commentary
Key Output CommentaryMortality Governance Process
Agree pro forma and screening method for mortality case review
Identify resources to support pilotsLead resource identified and discussions commenced on potential role. First round interviews for interim support were unsuccessful, further applications received and interviews to be scheduled.
Pilot redefined Trust process with AMU and CardiologyInitial scoping completed with AMU and completed in broad agreement. Initial scoping session with Cardiology to be scheduled.
Delivered all engagement as a mixture of open event or targeted events by Directorate
Submit proposal to Trust Board outlining the governance and reporting arrangements for MMPG within the Trust BAF.Pilot analysis and full Trust roll out of compulsory process to all Clinical Groups or Directorates
Define mechanism to identify and approve Quality Improvement schemes and governance to support improvement monitoring Mechanism defined conceptually. Documentation and consultation to be performed before piloting.
EducationDraft and agree education materialsDevelop schedule and timetable of engagement events
Draft Business Case for Trust Board approval for development of Trust advanced mortality / morbidity analytics capability
Scope and develop clinical coding work stream to improve clinical engagement in coding Plan developed for priority areasComplete visits to each directorate to increase clinical engagement in coding Visits have commencedFuture information requirementsUndertake visits to exemplar organisations with regards to advance mortality / morbidity analytics Two visits completed, remainder identified and to be scheduled.
Four box Screening and Review Metric This tool will allow us to identify avoidable mortality. SRO and
Programme Director to develop metric by 01.01.2016
Metric provider: Last provided:
SHMI The latest Summary Hospital-level Mortality Indicator (SHMI) score for Oct 13
to Sept 14 is 104.7, which is within the ‘as expected’ banding. An equivalent metric for HSMR is being considered for future iterations by the
SRO, Programme Directors and the PMO.
Metric provider: Dylan Gibbons Last provided: 13th May 2015 Next expected date: May 2016
0
20
40
60
80
100
120
140
2011-Q4 2012-Q2 2012-Q4 2013-Q2 2013-Q4 2014-Q2 2014-Q4
HSM
R Ra
tio
Seven Day Mortality (HSMR Ratio)
Trust Target Weekend Weekday
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
2011-Q4 2012-Q2 2012-Q4 2013-Q2 2013-Q4 2014-Q2
Four Box Screening and Review Metric
Trust Target Weekend Weekday
Avoidable Mortality placeholder. Pilot by July 15. Launch across Trust
December 15.
0.80
0.90
1.00
1.10
1.20
1.30
1.40
1.50
2011
-Q4
2012
-Q1
2012
-Q2
2012
-Q3
2012
-Q4
2013
-Q1
2013
-Q2
2013
-Q3
2013
-Q4
2014
-Q1
2014
-Q2
2014
-Q3
% of Cases Reviewed placeholder
Trust Target Weekend Weekday
Cases Reviewed placeholder - AMU and Cardiology by July 15. Launch across
Trust December 15.
Seven Day Mortality HSMR Further review to consider change in weekend/weekday picture over last 2 quarters
and impact of PMS2
Metric provider: Dylan Gibbons Last provided: 28th April 2015 Next expected date: June 2015
% of Cases reviewed
Metric provider: Last provided: n/a
Next expected date:
IIP PMO
% of Cases reviewed
Metric provider: Dylan Gibbons Last provided: 13th May 2015
Next expected date: 13th June 2015
0
20
40
60
80
100
120
14 28 42 56 70 84 98 112
126
140
154
168
182
196
210
224
238
252
266
280
294
308
322
336
350
364
378
392
406
420
434
Adult Emergency Deaths - 16 and over
2007 2008 2009 2010 2011
2012 2013 2014 2015
70.0
80.0
90.0
100.0
110.0
120.0
130.0
140.0
Apr-
07
Aug-
07
Dec-
07
Apr-
08
Aug-
08
Dec-
08
Apr-
09
Aug-
09
Dec-
09
Apr-
10
Aug-
10
Dec-
10
Apr-
11
Aug-
11
Dec-
11
Apr-
12
Aug-
12
Dec-
12
Apr-
13
Aug-
13
Dec-
13
Apr-
14
Aug-
14
Dec-
14
HMSR using Dr Fosters 95% Confidence levels
80.085.090.095.0
100.0105.0110.0115.0120.0125.0
Quarterly SHMI using Dr Fosters 95% Confidence levels
SHMI Trust Target80859095
100105110115120
SHM
I Rat
io
SHMI
Trust Target Actual
Deaths per Week This tool provides early warning of changes in death rates from the historical norm. This allows us to be aware of and consider these changes ahead of published risk adjusted data (HSMR/SHMI). There was a marked rise in the weekly number of deaths over Dec 14 which peaked at the end of Dec/ beginning of Jan 15. Associated with increased congestion in patient flow and mirrored the Flu A spike – this is in line with the findings of the Public Health England (PHE) report into seasonal flu. There was a decline throughout Jan, which has stabilised at a slightly higher number than the pre-winter level, possibly associated with a minor rise in Flu B positive cases since the start of Feb 15. Target to be developed by SRO and Programme Director.
Metric provider: Dylan Gibbons Last provided: 13th May 2015
Next expected date: 20th May 2015
75.0
85.0
95.0
105.0
115.0
125.0
135.0
Apr-
07
Aug-
07
Dec-
07
Apr-
08
Aug-
08
Dec-
08
Apr-
09
Aug-
09
Dec-
09
Apr-
10
Aug-
10
Dec-
10
Apr-
11
Aug-
11
Dec-
11
Apr-
12
Aug-
12
Dec-
12
Apr-
13
Aug-
13
Dec-
13
Apr-
14
Aug-
14
Dec-
14
Monthly Trust Summary HSMR
Sep 14 10 year Benchmark Trust mean Trust UCL Trust LCL
Potential alternative metrics to be agreed with SRO
0.0
2.0
4.0
6.0
8.0
10.0
12.0
Q1 2013/14 Q2 2013/14 Q3 2013/14 Q4 2013/14 Q1 2014/15 Q2 2014/15 Q3 2014/15
Deaths per day at the trust
Weekday Weekend
Potential alternative metrics to be agreed with SRO
Potential alternative metrics to be agreed with SRO
Potential alternative metrics to be agreed with SRO
HEFT IIP Dashboards 18 05 2015.xlsxMORTALITY 8

Council of GovernorsJune 2015
.224
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Dementia StrategyPresentation

Council of GovernorsJune 2015
.225
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Minutes of Meetingheld on 14 Apr and 5 May 2015

Council of GovernorsJune 2015
.226
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Minutes 14 April 2015
COUNCIL OF GOVERNORS
Minutes of a meeting of the Council of Governors
of Heart of England NHS Foundation Trust held in St Johns Hotel, Warwick Road, Solihull
on 14 April 2015
PRESENT: Mr Les Lawrence (Chairman)
Mrs A Begum Mrs K Bell Mrs E Coulthard Dr O Craig Mr R Handsaker Mr R Hughes Mr M Hutchby Mrs S Hutchings Mr P Johnson Mr M Kelly
Ms A Khan Mrs H Lane Mr A Lydon Mrs A McGeever Mrs M Meixner Mr O’Leary Dr M Pearson Mrs J Thomas Mr D Treadwell Dr M Trotter
In attendance: Mr D Cattell Dr A Catto Mr A Edwards Mrs A Hudson (Minutes)
Ms K Kneller Mrs S Foster Mr K Smith (Company Secretary)
15.031 APOLOGIES AND WELCOME
Mr Lawrence welcomed everyone to the meeting and apologised for the absence of the Chair’s Report, this had been due to IT issues; a full report would be submitted to the next meeting. The Chair welcomed Ms Natalie Shaw, of PwC, who was in attendance to present item 10. Mr O’Leary apologised for missing the last meeting as he had been in hospital at the time. Apologies for Governors had been received from Cllr Aikhlaq, Dr Burgess, Mr Fletcher, Mr Orriss, Dr Needham and Mrs Steventon. Apologies for Directors had been received from Mr Brotherton, Dr Cadigan, Mr Lock, Ms Lord and Dr Rao.
15.032 DECLARATION OF INTEREST – Governors
The Chair referred to the Register of Interests and asked that Governors notify the Company Secretary of any changes so that the Register could be updated accordingly.
15.033 DECLARATION OF INTEREST – Directors The Register of Interests for Voting Directors was noted.

Council of GovernorsJune 2015
.227
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
15.034 CHIEF EXECUTIVE’S REPORT
The pre-circulated report was taken as read; Mr Foster reiterated he was continuing to focus on the three main priorities of Clarity, Quality and Engagement and it was noted that: Clarity - work had commenced on reporting lines and developing the Strategy for the organisation. Quality - the main concern was around the Emergency Departments and safety issues that resulted when it became congested. Plans were in place to consider the short, medium and long term priorities. Mr Foster was working towards a more celebrated approach to quality that included encouraging staff to become Quality Champions, an initiative that had proved successful at Wrightington, Wigan and Leigh NHS Foundation Trust (WWL). Engagement - there had been 8 staff engagement events held to date with future events planned; feedback so far had been positive. The Trust had been on a difficult journey especially over the last year and Mr Foster believed the Board’s acceptance of the Deloitte Governance Report had been a critical point and catalyst to make improvements. Mr Foster formally thanked Dr Catto and the Board for supporting the changes required. Dr Pearson referred to the Deloitte Governance Report and was concerned to know whether Governors were at fault for the poor systems in governance it highlighted and questioned why Nursing was now responsible for Governance. Mr Foster responded that Mrs Foster had been appointed to lead on Governance as part of the realignment of roles in the executive team and added that in most foundation trusts Governance sat within the remit of Nursing. He went on to say that Mrs Foster was developing a document setting out the roles and responsibilities for everyone in the organisation and this would be circulated upon completion. Mrs Foster advised that she was pleased to be taking on the added responsibilities that included Governance and Patient Experience and advised that she had appointed a Governance Support Team to move work forward and agreed to prepare a briefing paper for the next meeting. Dr Trotter referred to recently circulated structures and questioned some of the changes, including that of Director of Medical Safety. Dr Catto advised that as a result of the realignment Clinical Effectiveness and Quality Improvement formed part of his portfolio and changes in structures and reporting were in transition, the role of the Director of Medical Strategy had changed and was now the responsibility of the Deputy Medical Director - Quality & Safety. Both Dr Catto and Mrs Foster emphasised that the structures in the organisation were in transition but it was clear that the Medical and Nursing teams needed to work closely together going forward. In response to a question from Mr Lydon, Mr Foster confirmed that many of the new structures of responsibility were based on those in place at WWL. Mr Lydon advised that he had resigned as a member of the CoG Quality and Risk Committee as it was his opinion that the committee was dysfunctional and seldom received minutes and reports in a timely fashion. He asked whether there was a similar issue with the Board Quality and Risk Committee in particularly citing the lack of information within the Safety Sitrep Report around the spike in mortality in 2012/13 and asked why this had not been highlighted to Governors. The Chair advised it had not been raised with Governors as the Board had been satisfied that there was no significant issue at that time.
Minutes 14 April 2015

Council of GovernorsJune 2015
.228
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Mr Foster noted that as part of the work on clarity, each of his direct reports had been reviewed and each layer in turn would be doing the same. The Emergency Departments had a high impact on quality and safety and thus was the number one issue to be addressed. Dr Catto advised that heightened mortality had been raised as a risk in January 2015. The meeting discussed the earlier reference to Governance and the statutory duties of Governors. It was agreed that Mr Smith would produce a short paper setting out the distinctions between Governors’ responsibilities and Governance. (Action: KS)
15.035 INTEGRATED QUALITY & PERFORMANCE REPORT, INCLUDING FINANCE
Dr Catto presented an overview of the report. Mr Brotherton had sent apologies as he was attending the Systems Resilience Group meeting with the CCG. There were three areas of focus; 18 week RTT target, cancer targets and Emergency Departments (EDs). Work continued to address poor performance which including longstanding issues and the need to learn from shortcomings in previous strategies and a lack of modelling; rectification work included capacity modelling led by Mr Cattell and staff engagement being undertaken as part of Mr Foster’s work. The 18 week RTT target had not been achieved due to a series of issues that included, amongst other things, hidden waiting lists and IT issues. The hidden waiting lists mainly consisted of Gastroenterology patients that had come to light as a result of inefficient practices. Other factors had included higher cancellation rates for elective procedures due the number of acute patients occupying surgical beds. The Board had, that morning, discussed and agreed to extra investment to improve the situation. April had seen a return to full reporting off RTT performance; an enormous amount of work had been undertaken over the last 6 months to close open clocks, together with reviews to ensure no significant harm to patients. Cancer performance had improved despite a continued increase in demand. There had been a dip in the 62 day target in March but following improvements the Trust was back on trajectory. Urgent care continued to experience an increase in demand and flow was slow but work was underway to address this. There had been a surge in the number of 999 calls with the Trust seeing up to 10 ambulances arriving at EDs within 30 minute timeframes that resulted in unsafe EDs. Teams were demoralised as a result of the constant pressure and non-delivery of A&E standards over the last 10 quarters. The report set out a list of actions that had been put in place to help address the issues; however feedback from ED colleagues had been that they did not feel the benefit from those actions, as a result ad hoc ED listening events had taken place and steps had been taken to overhaul the escalation management system; some success had been seen including earlier ward discharges and patients movement from AMU to wards, however ED still remained the greatest operational and safety risk. Finance and Performance Mr Cattell advised that the Trust continued to spend money in a planned manner on patient care including ED and outplacement of surgical patients. The Trust had not previously planned for the right level of patient activity and this had resulted in unplanned flex which was inefficient and costly to run. It was also noted that: Capital spend was a little behind plan due to a pause whilst the Board
considered a Strategic Plan; The Trust was on track to deliver the forecasted year end position; COSR rating was 4;
Minutes 14 April 2015

Council of GovernorsJune 2015
.229
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
The Trust remained in a strong cash position; Contracting discussions continued in order to agree the right levels of activity for
2015/16. It was important that the Trust managed its risk in relation to excess planned activity.
Mrs Foster reported that the corporate nursing team continued to monitor staffing levels. Ward 3 at GHH had been re-commissioned. Following a visit to WWL Quality Champion work had begun. Dr Catto, Mrs Foster and the Governance Recovery Team had begun investigative work around SUIs and how the Trust could take learning forward. Staff sickness was at its lowest for six months. Fall rates had shown a downward trend over the last three months. The report on the Salmonella outbreak at the Trust been received and had been complimentary on how the Trust had handled the situation. Open visiting had commenced across all sites from the 1 April 2015 and had multiple benefits for patients and carers; the greatest benefits were for dementia and end of life patients. Following several questions from the Governors, including Messrs Hughes and Treadwell, on open visiting Mrs Foster agreed to circulate the Trust Visitor Code to Governors; it set out how the Trust would manage open visiting including night time visits. Mrs Foster added that ward sisters had the authority to manage visitors locally in order to keep the ward environment safe. Overall the benefits were expected to outweigh the burdens. (Action: SF/KS) Mr Hughes congratulated Mrs Foster and the team for initiating open visiting. He went on to ask about staff recruitment and noted that he had never seen any advertisements in the local papers for staff. Mrs Foster advised that the Trust successfully recruited regionally, nationally and worldwide. All trusts, including HEFT, used NHS Jobs to advertise for staff; HEFT also attended university open days, etc. Ms Gunter added that the Trust had just held a very successful recruitment event and several others were planned but it needed to keep in mind that recruitment and retention remained a constant challenge. Mrs McGeever noted the great work underway to improve patient flow and in response to several points Dr Catto advised that the Trust now had a long of list actions that needed to be taken to achieve effective discharges, including TTO planning. Discharge lounges had been reinstated on all sites and this had resulted in a positive impact. In response to a question from Dr Pearson about complaints analysis and in particular those related to cancelled operations, Dr Catto advised that urgent care did sometimes take precedence over elective surgery; he and Mrs Foster, who was now responsible for complaints, had arranged for the Complaints Manager from Airedale to review the Trust’s complaints processes. Mr Lydon referred to discharges and explained that he believed that Social Services had a responsibility to help get patients out of hospital and, from his own experience, knew how long this could take. He felt that the Trust needed to challenge Social Services to improve. Mr Lydon asked for an update on falls that included what type of patients experience falls. Mrs Foster advised that she would be attending the next Governors Breakfast
Minutes 14 April 2015

Council of GovernorsJune 2015
.230
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Meeting, in May, to talk about falls and invited Governors to forward questions via Mr Smith prior to the meeting in order that she could provide answers to detailed questions. The Chair suggested that Mary Ross, Clinical Director for Therapies, should also attend a Breakfast Meeting to give an update on the SIDs work she had implemented to reduce the re-admittance of elderly patients. (Action: KS)
15.036 RECOMMENDATION FOR RE-APPOINTMENT OF PROF LAURA SERRANT
The Chair referred to the pre-circulated paper setting out the recommendation for re-appointment of Prof Laura Serrant to the role of Non-executive Director. The Council of Governors approved the proposal and re-appointed Prof Serrant for a second three year term with retrospective effect from 1 April 2015.
15.037 NED APPRAISALS
The Chair advised that he had carried out the annual appraisal of the longer serving Non-executive Directors (NEDs) that had included discussions around the output from the 360 degree reviews, their strengths and weaknesses and he had agreed objectives with each NED for the coming year. Although appraisals had not been undertaken for the most recently appointed NEDs, Mr Edwards and Ms Kneller, their objectives had been agreed for the coming year.
15.038 CHAIR’S APPRAISAL Mr Lawrence left the room and Mr Smith took the chair for this item of business. Mr Hughes advised that he and Mr Lock, Senior Independent Director, had undertaken the Chair’s appraisal in line with previous years, using the same process as the NED appraisals, including a 360 degree review, to which the responses had been exemplary. Some improvement was required around managing the Chair’s frustration with poor performance. Five objectives had been set: Working towards the removal of the Monitor enforcement undertakings by 1
January 2016; Taking reasonable steps to appoint a substantive Executive Team by 1 January
2016; Leading the Board to work in a cohesive manner; Engagement with key external stakeholders; Demonstrating culture change, including winning the trust of staff. Mr Lydon questioned how and when the range of responses had been gained; Mr Hughes advised the questionnaire had been completed in September and had included tick box answers and spaces for comments. Mr Lydon noted that Lord Hunt, the previous chair, had been appraised as ‘extremely satisfied’ and that the Trust had been in a difficult place ever since. He suggested that the questions asked were not critical enough and that narrative answers, rather than tick boxes, should be used. Mr Hughes agreed to take on board these comments, reiterating that no major weaknesses had been raised as part of Mr Lawrence’s appraisal process. Mr Lawrence returned to the room and resumed the chair.
15.039 Quality Account & Report Update
Minutes 14 April 2015

Council of GovernorsJune 2015
.231
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Mrs Foster presented an overview of the progress made on the 2014/15 Quality Account and the setting of objectives for 2015/16. It was noted that the Quality Account was an annual report to the public from providers of NHS services. Its primary purpose was to encourage boards and leaders of NHS organisations to assess the quality of services provided. The HEFT 2014/15 Quality Account was subject to internal review, external consultation and assurance from PwC, the Auditors, and needed to be compliant with the Monitor Annual Reporting Manual requirements. The report had been submitted to the Overview and Scrutiny Committee for comment; feedback had included the need for more benchmarking data, narrative and less jargon. The draft report would be circulated to Governors as part of the consultation process. The priorities for 2015/16 were:
Reduction of grade 2 pressure sores; Improving clinical outcomes for stroke; Reduction of incidence of multiple falls; Friends and family test response rates in ED.
In response to question from Mr Lydon, Mrs Foster advised that the priorities were new and replaced those set out in the 2014/15 Quality Account, The next step was the assurance review by PwC. The Trust’s performance on 18 week RTT and cancer waiting targets would be considered as part of this review. Dr Pearson questioned whether the Trust would have the means to be able to spot another ‘Paterson’ type event. Dr Catto and Mrs Foster advised that discussions with Deloitte were ongoing regarding the development of a dashboard to track underperformance and, although it was absolute impossible to give absolute assurance, current systems were much better at picking up irregularities. In response to a question from Mr Hughes, Dr Catto advised that operations were not observed unless a specific concern had been raised but could be videoed with the relevant consent. In response to a question from Mr Lydon, Dr Catto explained he didn’t regard the number of SUI’s and never events as a problem for the organisation, given its size; he would be more concerned if he thought there was under-reporting. Dr Catto preferred a culture where all incidents were reported and then downgraded, if appropriate, as this built trust and confidence with stakeholders. Mr Foster added that ‘Paterson’ had been a shocking case and one where several people within the organisation had known of the practice but felt unable to do anything about it. Going forward it was about a changing that type of culture and empowering people to raise concerns.
15.040 EXTERNAL AUDITOR UPDATE Ms Shaw advised that the external audit of systems and controls was underway and would continue over the next 6-7 weeks at the end of which PwC would produce its opinion on the Annual Report and Accounts for 2014/15. To date no significant issues or material weakness on financial controls and systems had been identified. In respect of economy, efficiency and effectiveness, it was expected that a modified opinion would be issued as a result of the Monitor enforcements undertakings.
Minutes 14 April 2015

Council of GovernorsJune 2015
.232
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
15.041 MINUTES OF PREVIOUS MEETINGS
The minutes of the meetings held on 3 February 2015 and 4 March 2015 were approved as a true record.
15.042 MATTERS ARISING
14.080 Decision not to purchase Chest Clinic building – Mr Cattell advised that the Trust leased the building used by the Chest Clinic from Birmingham City Council at a very low rent and the cost to purchase and refurbish would be very high; therefore it had been agreed not to purchase but to continue to lease. Mr O’Leary questioned whether it might be appropriate for the Chest Clinic to move to more suitable premises; Mr Cattell indicated that this might also be more expensive than the current arrangement but that it would be kept under review. 14.080 Overseas patients – Mr Smith advised that this had been fully reported at the March 2014 meeting and undertook to circulate the report on this subject from that meeting. (Action: KS) In response to a question from Mr Treadwell on whether attendees at A&E should be asked for sight of their passports, Mr Cattell advised that a vast amount of work was underway nationally on managing overseas visitors accessing the NHS and a report on how these changes would affect the Trust would be presented when these were understood. 14.080 Progress of decked car park for Good Hope – the Chair explained that a report on capital prioritisation, which would address this subject, would be brought in due course. 14.082.2 Substantive chair for F&SP – discussions were ongoing. 14.082.3 Progress of hospital environment projects and attendance of Mr Sellars – The Chair had discussed this with Mr Sellars and he would routinely be attending future meetings when possible to report on such issues. 14.082.6 Consider the need to strengthen administrative support to CoG committees – the pre-circulated paper describing committee membership and support was noted. 14.084 Report on CIP/SIEP and pay bill overspend rectifications. Mr Cattell noted that this had been covered within the finance section of the Integrated Performance Report 15.017 Investigate heating issues in BHH Tower Block and report back. Mr Mike Taylor, Head of Estates, reported that an energy efficiency survey had been undertaken on the whole of the block and showed that the 40 year old heating coil system within the ceiling was outdated; however rectification work had already been undertaken to mitigate the issues, this included installation of more valves, additional insulation and installation of computerised systems to monitor temperature variances. Maintenance teams would be looking to carry-out further works including draft proofing windows in readiness for the coming winter. A full report on the planned works would be submitted to the Hospital Environment Committee.
15.043 ATTENDANCE RECORD - Governors The report was noted.
Minutes 14 April 2015

Council of GovernorsJune 2015
.233
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
The Chair advised that attendance records for CoG sub-committees were also being developed.
15.044 CHAIR’S REPORT
As advised at the beginning of the meeting a full report would be presented to the next ‘formal’ meeting.
15.045 ANY OTHER BUSINESS Mr Treadwell had submitted the following items:
Acronyms should be avoided in Board and CoG reports and where they are used a key should be provided – noted.
Implementation of an attendance register for members of the public to sign in
when attending Public Board and CoG meetings - noted. Mr Lydon noted that the Trust’s AGM did not see much public attendance compared to the UHB AGM and questioned whether the Trust would consider a central venue and increased publicity for the event. He also advised that UHB did not rotate its meetings between different venues. The Chair noted that UHB only had one site whereas the Trust had three main sites; therefore rotation was appropriate for the Trust. The Chair agreed to consider the suggestion of a central venue and increased publicity for the forthcoming AGM. (Action: Chair/KS)
15.046 DATE OF NEXT MEETING
5 May 2015 at the Harry Hollier Lecture Theatre, Good Hope Hospital, Sutton Coldfield. There being no further business the meeting closed.
…………………… Chairman
Minutes 14 April 2015

Council of GovernorsJune 2015
.234
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
COUNCIL OF GOVERNORS
Minutes of a meeting of the Council of Governors
of Heart of England NHS Foundation Trust held in the Partnership Learning Centre, Good Hope Hospital, Sutton Coldfield
on 5 May 2015
PRESENT: Mr L Lawrence (Chair)
Mrs K Bell Dr Burgess Mrs E Coulthard Dr O Craig Mr A Fletcher Prof H Griffiths Mr M Hutchby Mrs S Hutchings Mr P Johnson
Mr M Kelly Mr A Lydon Mr O’Leary Mr Orriss Dr M Pearson Ms L Steventon Mrs J Thomas Mr D Treadwell Dr M Trotter
In attendance: Mrs S Bradshaw (Minutes) Mr D Cattell Dr A Catto Prof M Cooke Mr A Foster Mrs S Foster Mrs H Gunter
Ms K Kneller Mr D Lock Ms A Lord Mr J Sellars Mr K Smith (Company Secretary) Mrs J Tunney
Members of the public 15.047 APOLOGIES AND WELCOME
Apologies for Governors had been received from Mrs Begum, Mr Hughes, Mrs Lane, Mrs McGeever, Mrs Meixner and Dr Needham. Apologies for Directors had been received from Mr Brotherton, Dr Cadigan, Dr Rao, Mr Edwards and Prof Serrant.
15.048 MONTH 12 PERFORMANCE REPORT
Dr Catto presented the on behalf of Mr Brotherton. The themes in the report were similar to the previous month’s report. The main areas of concern were urgent care, referral to treatment (RTT), 62 day cancer targets, diagnostic support (in particular endoscopy) and Gastroenterology. The increased demand in urgent care in March was noted resulting in high bed occupancy and congestion in Emergency Departments (EDs). The RTT targets had not been met in the month but RTT reporting had re-commenced and there was an improvement in the RTT admitted backlog. There had been a strong focus on Gastroenterology, where additional capacity had been agreed. There had been improvements in the 2 week wait and breast symptomatic targets. Performance against the 31 day cancer target had been good but there was a shortfall against the 62 day cancer targets. Mrs Foster presented on quality and safety issues. The biggest risks were around the emergency pathway and safe staffing. Recruitment within Europe had proved less and less successful and therefore other countries, outside Europe, were being looked at. The
Minutes 5 May 2015

Council of GovernorsJune 2015
.235
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
2
Philippines was being looked at for nurses and the University of Islamabad for doctors. The Trust’s vacancy rate remained static and there was an overreliance on agency staff. Harms continued below the national averages (pressure ulcers and falls). A review of complaints and SUI (Serious Untoward Incidents) processes was underway. The draft CQC report from the visit in December 2014 has been received to check for factual accuracy; it contained no surprises. The final report would follow. Mrs Bell asked about recruitment from Greece; Mrs Foster explained that the Trust had sent three nurses to Greece on a recruitment campaign but only managed to recruit two nurses. In response to a question from Mr Orriss regarding the lengthy delay of the CQC report, Dr Catto explained that there were two main reasons (1) a key member of CQC staff had been on lengthy sick leave, and (2) there had been much internal discussion at CQC about ratings. It was still not clear whether or not CQC would state an overall rating in the final report. Mrs Steventon asked whether the Trust came out better in this inspection than the last. Dr Catto explained that the Trust remained rated the same; mainly yellow (‘needs improvement’) with some green and some red. Dr Catto believed it was an accurate picture of how the Trust stood in December 2014. Mrs Thomas asked if the CQC would do an interim assessment before they published the final report, given the delay. Dr Catto stated that there would be no reassessment despite the delay and the fact that the Trust had made progress in some areas since the inspection. Mr Treadwell asked if the Foreign Office had been approached to assist with the overseas recruitment. Mrs Foster replied that the Home Office set the policy on the visa regime which dictated where the Trust could recruit from, also that neither the Home Office nor the Foreign Office would act as recruitment agency on the Trust’s behalf. Mrs Foster outlined a new practice that had been introduced to reduce congestion in Emergency Departments (ED). The new scheme was ‘safer placement on wards’ and placed a limited number of ED patients awaiting discharge and transfer on wards related to their condition. These patients were nursed beside the nurses’ station. In practice this had meant one extra patient on eight separate wards in Good Hope. This approach had good clinical engagement. Dr Catto explained that this was a measure that had been carefully thought through; he referred to research which indicated that patients preferred to be placed on a ward, pending discharge, rather than in ED. Mrs Coulthard asked whether the reinstated discharge lounge at Good Hope was helping. Mrs Foster replied that it had six beds and 19 chairs and was working well so far. Mrs Coulthard noted that there had been no beds on A&E majors available at Good Hope after 8.00pm the previous Saturday evening. Dr Catto explained that when patients arrive at A&E the Trust does whatever it can to provide appropriate treatment. Dr Pearson questioned the use of flawed mortality rates (such as HSMR) given the understanding that congestion drives mortality. Dr Catto explained that due to the problems with the introduction of the new patient administration system (PMS2), HSMR would be an unreliable mortality indicator for the Trust for a while; however the Trust was monitoring crude mortality and undertaking a review of each death to ensure that trends and spikes were understood. Dr Catto noted that mortality spikes and the flu did seem to correlate over the winter.
Minutes 5 May 2015

Council of GovernorsJune 2015
.236
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
3
Mr Kelly explained that he and the late Gerry Robinson campaigned against the closure of the discharge lounges and he was therefore pleased to see them reinstated. Mrs Foster explained that the original discharge lounge on the ground floor had not been large enough to take beds and a number of the patients awaiting discharge were bed bound, so this arrangement did not work. The new lounge could take both beds and chairs. Mr Orriss asked about parking at Good Hope in the context of discharging ED cases from wards which would require more pick up time for relatives and carers. Mr Sellars explained that the 30 minute free tariff applied across all sites. The Chair asked Mr Sellars to discuss this further at the next Hospital Environment Committee meeting. Mr Lydon asked about mortality spike in 2013/14. Dr Catto explained that mortality spikes in ED were usually a surrogate for the entire hospital and that being clinically unwell in ED was not good for patients who were exposed to greater risk in that environment. Mr Webster congratulated the Trust on moving people that were awaiting discharge or transfer from ED to wards. He went on to note that the general consensus was that the Trust was in trouble but that not enough was being done to publicise the good things that the Trust was doing. He was also concerned about the possible inappropriate use of hospitals for patients near the end of their lives. His experience with his wife, who was terminally ill, had been that she had been sent to A&E several times, against his wishes, by her nursing home. He felt that the nursing home didn’t want his wife to die in their care although her demise was expected. Dr Catto acknowledged the dilemma of care and nursing homes tending to transfer end of life patients to hospital when little or nothing could be done to prolong their lives.
15.049 REPORTS FROM COG COMMITTEE CHAIRS
Finance and Strategic Planning Mr Fletcher presented the minutes and reported that there had been problems over some dates being changed and that the meetings had been less well attended as a result. Mr Cattell apologised and confirmed that this was being looked into. Mr Fletcher reported that Mr Johnson has chaired the March meeting, which had been a good meeting, and that the committee was looking to appoint a new chair. Mrs Bell would chair the next meeting.
Hospital Environment Committee Mrs Coulthard presented the minutes and highlighted that Good Hope’s fete would take place on 18 July 2015. Mrs Coulthard reminded the meeting that the A&E canopy was being installed at Good Hope and that it was hoped that it would be finished by end month. The next meeting would be at the Chest Clinic and interested Governors were invited to attend. The new signage for Good Hope had arrived but had taken seven years to organise! The privacy domes and speakers for A&E had taken four years to organise! Mrs Coulthard also raised the issue of the Good Hope Multi-storey car park which was thought to have been ‘written off’ in the capital prioritisation programme. Mr Foster said that a multi-storey car park for Good Hope could be considered in the ten year capital strategy but it would be competing against other projects for prioritisation. Mr Treadwell reported he had raised the issue of a Doctor’s mess and was pleased to note that there now was one at Good Hope. Mrs Steventon asked about parking concessions for foster carers. Mr Sellars responded that the special rate of £10 for 20 visits was available for all patients and their carers at the relevant Ward Managers’ discretion.
Minutes 5 May 2015

Council of GovernorsJune 2015
.237
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
4
Mrs Coulthard raised the issue of there being nowhere for medical staff to eat after 3.00pm. Mr Cattell noted that F&SP was looking into this and would ask Mr Gould to prepare a report for the Hospital Environment Committee. (Action: D Cattell) Mr Orriss explained that the Good Hope car park had been approved three years previous by the Board and that he couldn’t understand why it hadn’t been built by now. Mr Fletcher noted that car parks for both Good Hope and Heartlands had been discussed for the last three or four years and he was disappointed that there had been little communication back to the Governors regarding any change of plan. Mrs Coulthard explained that Mr Sellars had described two options for the Good Hope car park to the Hospital Environment Committee a few months previous and that there had been no suggestion of the project being abandoned at that point. The Chair asked Mr Cattell and Mr Sellars to prepare a full paper on the car park history and situation for the next ‘formal’ meeting. (Action: D Cattell/ J Sellars) Membership and Community Engagement Mr Fletcher explained that the last meeting had been cancelled. Patient and Staff Experience Mr Kelly explained that DNAs had continued to decrease from 90,000 to 80,000 and the friends and family test response rate was sitting at Heartlands 44%, Solihull 45% and Good Hope 20%. Complaints were running at less than 1% of patients with the key areas being; delays and cancellations, attitudes and behaviour, appropriate treatments, poor information and medication issues. Thee PLACE inspections had showed some examples of poor conditions for staff. Dr Pearson suggested that benchmarking the complaints rate against other Trust to see how the Trust’s performance compared. Mr Orriss asked whether patients were being texted reminders as he had not been when recently attending appointments at Good Hope. Mrs Foster confirmed that patients were generally texted reminders and that this should be considered further by the Patient and staff Experience Committee.
Quality and Risk Mrs Steventon asked that the minutes from the 26 January meeting be taken as read and reported that the committee had changed its strategy to drilling down into the work of the Board Quality and Risk Committee. The issue of cross-over with the Patient and Staff Experience Committee was being considered again. Mrs Gunter had given an update on the work done by the Kennedy Task Force. Mrs Foster was coming to the next meeting on 12 May. Mr Lydon reported that he had resigned from the committee as he was not happy with the accuracy and lack of timeliness of the minutes. He felt that the executives supporting the committee were lacking grip and would have preferred more regular un-minuted meetings with quarterly formal meetings. Mrs Steventon reported that having reviewed the minutes the previous week with the minute taker, it was discovered that the draft minutes were being held up in the management chain. Mr Fletcher suggested that minutes should be sent to committee chairs within seven days. The Chair emphasised that it was important that there be no interference by Trust officers and that the draft committee minutes should go directly to the committee chairs for review. Mrs Foster said that she would resolve the issue of a suitable minute taker for committee.
Minutes 5 May 2015

Council of GovernorsJune 2015
.238
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
5
Kennedy Task Force Dr Pearson reported that he had no update on the Kennedy Task Force and that the continuing work arising from the Kennedy Report was expected to be completed through routine channels but that there might be an alternative scrutiny arrangement. It was agreed that Dr Pearson should continue to represent the CoG in relation to any new scrutiny arrangement.
15.050 REPORT ON THE WORK OF THE BOARD AUDIT COMMITTEE
Ms Lord introduced herself; she had been a Non-executive Director since May 2013 and chair of the Audit Committee since July 2013. Every foundation trust has to have an Audit Committee. The Board must put in place governance processes and systems of control. The Audit Committee reviews these and is an assurance committee - not an operational committee. Ms Lord explained that ‘reassurance’ is when someone asks if everything is okay and is told ‘yes’; by contrast ‘assurance’ is when someone asks to see that everything is okay and is shown an evidence base that demonstrates everything is okay. The Committee only Non-executive Directors as members, to ensure its independence from management, but is supported by Internal Audit, External Audit, finance and other subject experts. It should be chaired by a qualified accountant, which Ms Lord is. The Committee initiates reviews of systems and controls and looks at the outcome of those reviews, the recommendations made and the actions taken. Most of the reviews are done by Internal Audit. Internal Audit is outsourced, currently to Deloitte, in common with many large organisations. Since Ms Lord took the chair certain governance failings had been noted within the Trust, including the Board Assurance Framework. Ms Lord was a strong supporter of the Deloitte Governance Review and welcomed the huge amount of work currently being done on the improvement programme, especially that led by Mrs Foster. Under Ms Lord’s chairmanship, the Committee reviewed the work of the then current internal auditor (KPMG), went out to tender and appointed Deloitte. The new auditors provide more rigorous and advice. Each year Internal Audit undertake a series of core internal control reviews which generally give substantial assurance. This year Deloitte had carried out three reviews where moderate assurance was received (1) CQC compliance, (2) IT controls, and (3) Procurement, and a limited assurance review of the Board Assurance Framework and Strategic Risk Register. From the programme of reviews a series of recommendations are created. There were over 100 overdue responses when Ms Lord became chair; there were now only four. Ms Lord acknowledged the hard work of Mrs Angeline Jones, Chief Financial Controller, and her team in chasing responses. The results of the reviews in 2014/15 had led to the Head of Internal Audit’s Opinion being graded as one of ‘Limited Assurance’. Ms Lord also explained the work of the Local Counter Fraud Service (LCFS), conducted by Deloitte, which proactively works to deter and prosecute fraud against the Trust. This year there had been 23 referrals; as a result four dismissals and two potential prosecutions had been progressed. The Audit Committee also considers the external auditors’ reports (PwC) in relation to the Annual Report and Accounts, including the Quality Account. For the year 2014/15 it is likely that the Trust would receive a modified conclusion on economy, efficiency and effectiveness as a result of the Monitor enforcement action. PwC test three indicators in the Quality Account; one is the 18 week RTT performance, which the Trust would be unable to report on for 2015/16, so an alternative would be reviewed instead.
Minutes 5 May 2015

Council of GovernorsJune 2015
.239
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
6
Mr Lydon stated that an important issue for the coming year would be the tender for the external auditors’ service. He thought that PwC would have had to provide a modified opinion regarding economy, efficiency and effectiveness in relation to 2013/14. Ms Lord explained that they had taken expert technical advice at that time and concluded that this was not the case. Ms Lord clarified what the external audit function could and could not do. Mr Lydon asked whether the external auditors were responsible for flagging issues and whether they did. Ms Lord explained that there was an agreed process for this and confirmed that the external auditors view was absolutely objective. Mrs Steventon asked what the Head of Internal Audit’s Opinion was for 2014/15. Ms Lord replied that the outgoing auditors reported no concerns at that time. Mr Kelly asked about the performance of the previous internal auditors; Ms Lord compared it to the banking crisis in that the problems were not seen until after the event. Mr Kelly asked whether the Audit Committee dealt with debtors. Ms Lord explained that the Audit Committee looks at whether debtors are accurately recorded and the process for their management but not with specific reference to individual debtors. Mr Lydon asked whether Monitor could recommend good audit firms; Ms Lord explained that this was not something that Monitor did and explained that reputable audit firms had a checklist approach to audit and were all independent of their client organisations. Dr Pearson asked whether clinical audit was covered by the Audit Committee. Ms Lord outlined that Audit Committee sees the structure of clinical reviews but the reviews would be considered by the Quality and Risk Committee from a clinical perspective. Dr Pearson asked what Ms Lord would do if she felt that she did not have sufficient assurance. Ms Lord replied that she would raise it with the full Board; Dr Pearson suggested that such issues be raised with the Governors too.
15.051 2015/6 ANNUAL PLAN
Mr Cattell referred to the report included in the pack. The Annual Plan Return (APR) was due for submission to Monitor by 14 May and it will have its final sign off by Board Monitor Standing Committee but Mr Cattell would also take a summary of the final form plan to the F&SP. The Trust would be striving to improve its performance and governance over coming months and had developed an Integrated Improvement Plan to help to achieve this; it would also require the development of a suite of strategies. All of this would be referred to in the narrative of the APR. The plan recognised that the Trust expected to spend £10m more than it received in income to help fix the things that were broken, including performance against national targets such as 4-hour A&E, 18 week RTT and 2 week waits. Mrs Coulthard asked if the funds were in place for Surgery Reconfiguration. Mr Cattell confirmed that there was a general allowance for this but noted that the Trust wouldn’t know exactly what was required until the public consultation exercise being run by the CCGs was completed. Mr Lydon asked whether investment in sub-acute beds was a priority. Mr Cattell confirmed that this was still on the Trust’s agenda as it clearly related to flow but at this stage it was not clear what was required, or when.
Minutes 5 May 2015

Council of GovernorsJune 2015
.240
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
7
Mr Treadwell asked about emergency evacuation of patients. Mr Foster confirmed that the Trust has an emergency plan and that in the event of a full scale emergency it is normal to rely on neighbouring hospitals.
15.052 ANY OTHER BUSINESS
Mrs Steventon reminded the meeting that the Friends of Solihull Hospital would be running the Solihull fete on 30 May. Mr Treadwell asked if the trust was aware of the ‘Hug in a Hospital’ event; Mr Foster confirmed that the Trust was aware. In response to a question from Mrs Thomas, the Chair confirmed that the staff engagement events were going well and that the latest events had considered the outline strategy for the Trust.
15.053 DATE OF NEXT MEETING
2 June 2015 at The Village Hotel, The Green Business Park, Dog Kennel Lane, Shirley, Solihull B90 4GW. There being no further business the meeting closed.
…………………… Chairman
Minutes 5 May 2015

June 2015
Council of Governors
.241
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Matters Arising

Council of GovernorsJune 2015
.242
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Matters Arising
COUNCIL OF GOVERNORS
Matters Arising & Decisions/Recommendations Tracker
Dat
e ra
ised
Min
ute
No
Detail
Act
ion
by
Due Status
Com
plet
ed
24 Nov 2014 14.080
Report to go to F&SP Cttee regarding decision not to purchase Chest Clinic building.
DC Feb2014 Oral update given to CoG. 14 Apr 15
14.080 Receive full briefing from AQ/AJ on overseas patient income.
Chair Feb2014
Report presented at March 2014 meeting to be circulated by e-mail - KS.
18 May 15
14.080 Report on progress of decked car park for Good Hope.
AC Feb2014
Report on capital prioritisation to be brought to the CoG in due course.
14 Apr 15
14.082.2
Consider arrangements for appointment of substantive chair for F&SP Cttee.
Chair Feb2014 Discussions continuing.
14.082.3
Consider issues raised by E Coulthard regarding lack of focus, grip and pace regarding hospital environment projects.
AC Feb2014
J Sellars to routinely attend future CoG meetings to report on such issues.
14 Apr 15
14.082.6 Consider the need to strengthen administrative support for CoG Cttees
Chair Feb2014
Report on resource given to CoG.
14 Apr 15
14.084
Report to CoG on CIP/SIEP and pay bill overspend/ rectification status
DC Feb2014 Report given to CoG. 14 Apr 15
14.087
Consider with Lead Governor and CoG Cttee chairs whether an oversight and scrutiny Cttee might be appropriate.
Chair Apr2014 Ongoing.
3 Feb 2015 15.012
Consider Governor attendance at CoG and Committees with Lead Governor
Chair May2015 Ongoing.
15.017 Investigate heating issues in BHH Tower Block and report back.
DC Apr2015 Oral report given to CoG. 14 Apr 15
14 Apr 2015 15.034
Produce paper setting out the distinctions between Governance and Governors’ responsibilities.
KS Jun2015
15.035 Circulate Trust Visitor Code to Governors. SF/KS Apr
2015 Completed. 14 Apr 15
15.035
Invite Mary Ross, Clinical Director for Therapies, to a Breakfast Meeting to give an update on SIDs work.
KS Jun2015

Council of GovernorsJune 2015
.243
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Matters Arising
15.045
Chair agreed to consider a central venue and increased publicity for the 2015 AGM.
LL/KS Jul 2015
5 May 2015 15.049
Ask J Gould to prepare report for HEC on solution for clinical staff not being able to get a hot meal after 3.00pm (based on F&SP deliberations).
DC Jun2015
15.049
Prepare a full paper on the car park history and situation (BHH and GHH) for the next ‘formal’ meeting.
DC/JS Jun2015

Council of GovernorsJune 2015
.244
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Governance and Governors' responsibilities
Governance andGovernors' responsibilities

Council of GovernorsJune 2015
.245
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Governance and Governors' responsibilities
Governance and Governors’ responsibilities
Governance The Board has a duty to promote the success of the Trust so as to maximise the benefits for the members of the Trust as a whole and for the public who will be treated by the Trust.
Governance is the means by which the Board leads and directs the organisation so that decision-making is effective and the right outcomes are delivered.
Good governance incorporates, amongst other things, corporate governance and quality governance. Robust corporate and quality governance arrangements complement and reinforce one another. Other important aspects of governance include, for example, finance governance and research governance.
Governance arrangements delegate responsibility from the Board down to the operating levels in the organisation. In the case of quality, this means that although individuals and clinical teams are at the frontline and responsible for delivering quality care, it is the responsibility of the Board to create a culture within the organisation that enables clinicians and clinical teams to work at their best, and to have in place arrangements for measuring and monitoring quality and for escalating issues, including, where needed, to the Board. The same applies equally to other aspects of governance.
Some important features of good governance are strong leadership capability and capacity, clear strategies, robust structures (e.g. Board, clinical and operational committees which meet regularly and have appropriate terms of reference), clear lines of accountability, robust and timely flows of information, appropriate policies and procedures, etc.
Governors’ responsibilities Governors have an important role to play in making the Trust publicly accountable for the services it provides. They should do this by exercising their statutory powers and responsibilities; these come from the National Health Service Act 2006 and the Health and Social Care Act 2012 and can be summarised as:
Hold the Non-executive Directors, individually and collectively, to account for the performance of the Board.
Represent the interests of the members of the Trust as a whole and the interests of the public.
Approve “significant transactions”. Approve an application by the Trust to enter into a merger, acquisition,
separation or dissolution. Decide whether the Trust’s non-NHS work would significantly interfere with
its principal purpose, which is to provide goods and services for the health service in England, or performing its other functions.
Approve amendments to the Trust’s constitution. Appoint and, if appropriate, remove the Chair. Appoint and, if appropriate, remove the other Non-executive Directors. Decide the remuneration and allowances and other terms and conditions of
office of the Chair and the other Non-executive Directors. Approve (or not) any new appointment of a Chief Executive. Appoint and, if appropriate, remove the Trust’s auditor. Receive the Trust’s annual accounts, any report of the auditor on them, and
the annual report at a general meeting of the Council of Governors.

Council of GovernorsJune 2015
.246
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Governance and Governors' responsibilities
Governors should be committed to encouraging improvements in governance on a continuing basis by exercising their powers and responsibilities, such as holding the Non-executive Directors to account for the performance of the Board, but ultimately the legal responsibility for good governance sits with the Board.
Kevin Smith Company Secretary 18 May 2015

Council of GovernorsJune 2015
.247
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Attendance Record

Council of GovernorsJune 2015
.248
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
21.1.15 16.3.1505.01.15 04.03.15
Mohammed Aikhlaq Ap - 7 Ab Ab Ap - 7 3Arshad Begum Ap - 7 Ap - 2 Ap7 Ap-1 3Kath Bell Ap - 3 5Nicola Burgess Ab Ap -1 Ap - 4 Ab 3Barry Clewer Ap - 1 Ap - 2 Ab 3Elaine Coulthard Ap - 6 Ap - 2 5Olivia Craig Ap - 1 Ap - 7 Ap - 7 Ap - 7 3Carol Doyle Ap - 7 Ap - 7 Ap - 7 Ap - 7 3Albert Fletcher Ap - 3 6Helen Griffiths Ab Ap-7 Ap - 7 4Ron Handsaker Ap - 4 Ap- 4 Ap- 4 4Emma Hale Ap-4 6Richard Hughes Ap - 7 6Michael Hutchby 7Susan Hutchings 7Phillip Johnson Ap - 1 6Michael Kelly 7Attiqa Khan Ab Ab Ab Ap-1 Ap-1 2Heidi Lane Ap - 7 Ap -1 Ap - 7 Ap-4 3Andrew Lydon Ap - 6 6Anne McGeever Ap - 4 Ap - 4 Ap - 4 Ap - 4 3Margaret Meixner Ap-1 6Catherine Needham Ap - 2 6David O'Leary Ab Ap -1 Ap - 7 Ap-2 3Barry Orriss Ap - 3 6Mark Pearson Ap-1 6Jim Ryan Ab Ap-1 5Elizabeth Steventon Ap - 3 Ap - 3 Ap-2 4Joy Townsend Ap - 3 Ap - 7 0Jean Thomas Ab 4David Treadwell Ap - 6 6Matthew Trotter Ap - 6 6Total 18 20 21 24 20 22 18
Board 9 6 7 8 9 8 8Public 2 0 3 3 2 5N.B. J Ryan went to St Johns Hotel, Solihull for 23 July meeting (per front cover of pack) so claims attendance
Key: Ap 1 = No reason statedAp 2 = Sickness Ap 3 = Holiday Ap 4 = Care Cover Obligations (Child/Elderly/Relatives etc)Ap 5 = Bereavement Ap 6 = Unavailable due to change of meeting date Ap 7 = Other (prior engagement etc)Ab = Absent (no apology received)
2014/15
Total attended NAME
27.5.1423.7.14 15.9.14 24.11.14
03.02.15

Council of GovernorsJune 2015
.249
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Mohammed Aikhlaq Ap- 7 AbArshad Begum Ap-1Kath Bell
Nicola Burgess Ap-1
Elaine Coulthard
Olivia Craig
Carol Doyle Ab Ap-1Albert Fletcher Ap - 3
Helen Griffiths Ap - 3
Ron Handsaker AbEmma Hale Ab AbRichard Hughes Ap-1Michael Hutchby
Susan Hutchings
Phillip Johnson
Michael Kelly
Attiqa Khan AbHeidi Lane Ap-1Andrew Lydon
Anne McGeever
Margaret Meixner Ap-1Catherine Needham Ap-1 Ap-4David O'Leary
Barry Orriss Ap- 2
Mark Pearson
Jim Ryan AbElizabeth Steventon Ap-1
Jean Thomas
David Treadwell
Matthew Trotter
Board 5 8Public 4 3
Key: Ap 1 = No reason statedAp 2 = Sickness Ap 3 = Holiday Ap 4 = Care Cover Obligations (Child/Elderly/Relatives etc)Ap 5 = Bereavement Ap 6 = Unavailable due to change of meeting date Ap 7 = Other (prior engagement etc)Ab = Absent (no apology received)
14.04.15 02.03.15 07.10.15 04.11.15 Jan-16
2015/16
NAME 05.05.15 02.06.15 08.07.15 Feb-16 Mar-16

June 2015
Council of Governors
.250
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Chair's Report

June 2015
Council of Governors
.251
Agenda
WelcomeDeclaration
ofInterest
Apologies MinutesMatters Arising
Chairman'sReport
Chief Executive's
Report
IntegratedQualityReport
Any Other
Business
Attendance Record
IntegratedImprovement
Plan
DementiaStrategy
Presentation
Governanceand
Governors'responsibili-
ties
Any Other Business
Dates of Future Meetings
8 July 2015
Harry Hollier Lecture Theatre, Good Hope Hospital, Sutton Coldfield
Refreshments will be available from 3.30pm

Agenda
Produced by the Company Secretary’s Office