Correlation of partial env gene sequences with disease progression parameters in HIV-positive...
6
Med Microbiol Immunol (2012) 201:271–276 DOI 10.1007/s00430-011-0226-x 123 ORIGINAL INVESTIGATION Correlation of partial env gene sequences with disease progression parameters in HIV-positive pregnant women from India Supriya Singh · Shashi Khare · Sudha Prasad · R. L. Ichhpujani · S. S. Negi · Sachin Kumar · D. S. Rawat · L. S. Chauhan · Arvind Rai Received: 22 August 2011 / Accepted: 27 December 2011 / Published online: 25 January 2012 © Springer-Verlag 2012 Abstract Ever since the beginning of the epidemic of HIV, one of the poignant aspects of HIV infection is transmission of the virus from mother to child. It is not known whether pregnancy accelerates the progression of HIV infection from a clinically asymptomatic stage to a progressive clinical phase. Present study was carried out to understand disease progression in pregnant women from India. We studied co-receptor utilization (the major determinant of HIV disease progression), N-glycosylation sites, and sequence variability. Blood samples were collected from 25 HIV sero-positive patients, eleven from the antenatal risk group (experimental group), nine from heterosexual male, and Wve from hetero- sexual female risk group (control group). Partial env gene was ampliWed by PCR and sequenced. BLAST search and phylogenetic analysis were used to determine the subtype. The deduced amino acid sequence of the V3 region was used to predict co-receptor, determine sequence variability and N-glycosylation site. The experimental group comprising the antenatal risk group did not exhibit any diVerence in terms of co-receptor, N-glycosylation, and sequence variability when compared with the control, non-pregnant group. Pregnancy does not seem to accelerate the clinical course of HIV infec- tion. The female body during the gestation phase possibly acquires certain strategies to impede or at least alleviate the disease progression during the crucial immune-compromised pregnancy phase, which would otherwise adversely aVect the mother as well as the fetus during the infection. Keywords Co-receptor · Pregnancy · HIV · Sequence variability · N-glycosylation · Envelope gene · Hypervariable region (V3–V5) · V3 loop Introduction Ever since the beginning of the HIV epidemic, one of the poignant aspects is the vertical transmission of the Human ImmunodeWciency virus (HIV), from an HIV-positive S. Singh · S. Khare · S. Kumar · L. S. Chauhan Division of Microbiology, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, India e-mail: [email protected] S. Khare e-mail: [email protected] S. Kumar e-mail: sk_ronin@rediVmail.com L. S. Chauhan e-mail: [email protected] S. Prasad Department of Obstetrics and Gynaecology, Maulana Azad Medical College, Bahadur Shah Zafar Marg, Delhi Gate, New Delhi, Delhi 110002, India e-mail: [email protected] R. L. Ichhpujani · L. S. Chauhan Centre for AIDS and Related Diseases, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, India e-mail: [email protected] S. S. Negi · D. S. Rawat · L. S. Chauhan · A. Rai (&) Division of Biochemistry and Biotechnology, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, India e-mail: [email protected] S. S. Negi e-mail: [email protected] D. S. Rawat e-mail: [email protected]
-
Upload
arvind-rai -
Category
Documents
-
view
214 -
download
2
Transcript of Correlation of partial env gene sequences with disease progression parameters in HIV-positive...

Med Microbiol Immunol (2012) 201:271–276
DOI 10.1007/s00430-011-0226-xORIGINAL INVESTIGATION
Correlation of partial env gene sequences with disease progression parameters in HIV-positive pregnant women from India
Supriya Singh · Shashi Khare · Sudha Prasad · R. L. Ichhpujani · S. S. Negi · Sachin Kumar · D. S. Rawat · L. S. Chauhan · Arvind Rai
Received: 22 August 2011 / Accepted: 27 December 2011 / Published online: 25 January 2012© Springer-Verlag 2012
Abstract Ever since the beginning of the epidemic of HIV,one of the poignant aspects of HIV infection is transmissionof the virus from mother to child. It is not known whetherpregnancy accelerates the progression of HIV infection froma clinically asymptomatic stage to a progressive clinicalphase. Present study was carried out to understand diseaseprogression in pregnant women from India. We studiedco-receptor utilization (the major determinant of HIV diseaseprogression), N-glycosylation sites, and sequence variability.Blood samples were collected from 25 HIV sero-positivepatients, eleven from the antenatal risk group (experimentalgroup), nine from heterosexual male, and Wve from hetero-sexual female risk group (control group). Partial env genewas ampliWed by PCR and sequenced. BLAST search andphylogenetic analysis were used to determine the subtype.The deduced amino acid sequence of the V3 region was usedto predict co-receptor, determine sequence variability andN-glycosylation site. The experimental group comprising theantenatal risk group did not exhibit any diVerence in terms of
co-receptor, N-glycosylation, and sequence variability whencompared with the control, non-pregnant group. Pregnancydoes not seem to accelerate the clinical course of HIV infec-tion. The female body during the gestation phase possiblyacquires certain strategies to impede or at least alleviate thedisease progression during the crucial immune-compromisedpregnancy phase, which would otherwise adversely aVect themother as well as the fetus during the infection.
Keywords Co-receptor · Pregnancy · HIV · Sequence variability · N-glycosylation · Envelope gene · Hypervariable region (V3–V5) · V3 loop
Introduction
Ever since the beginning of the HIV epidemic, one of thepoignant aspects is the vertical transmission of the HumanImmunodeWciency virus (HIV), from an HIV-positive
S. Singh · S. Khare · S. Kumar · L. S. ChauhanDivision of Microbiology, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, Indiae-mail: [email protected]
S. Kharee-mail: [email protected]
S. Kumare-mail: [email protected]
L. S. Chauhane-mail: [email protected]
S. PrasadDepartment of Obstetrics and Gynaecology, Maulana Azad Medical College, Bahadur Shah Zafar Marg, Delhi Gate, New Delhi, Delhi 110002, Indiae-mail: [email protected]
R. L. Ichhpujani · L. S. ChauhanCentre for AIDS and Related Diseases, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, Indiae-mail: [email protected]
S. S. Negi · D. S. Rawat · L. S. Chauhan · A. Rai (&)Division of Biochemistry and Biotechnology, National Centre for Disease Control (NCDC), 22-Sham Nath Marg, Delhi 110054, Indiae-mail: [email protected]
S. S. Negie-mail: [email protected]
D. S. Rawate-mail: [email protected]
123

272 Med Microbiol Immunol (2012) 201:271–276
mother to her child during the course of pregnancy or post-partum transmission as a repercussion of breastfeeding. Inthe past, there have been several reports of deaths of preg-nant women, as a result of HIV infection [1, 2], whichcompelled us to believe that pregnancy may have eVect onthe course of HIV infection. AIDS was a major cause forpregnancy-related mortality during 1975–1989 in the majorcities of United States [3]. HIV infection in 1988 wasresponsible for 90% of all deaths among child-bearingwomen in Rwanda, Africa [4]. The natural history and clinicalpresentation of various infections is diVerent in the two sexes.For instance, Kaposi’s sarcoma is less frequent in women thanin men. As a consequence of the unique hormonal and immu-nological environment during the course of pregnancy, HumanimmunodeWciency virus may possibly evolve in a diVerentmanner and may accelerate the HIV infection. Pregnancy isknown to have an impact on the course of various other bacte-rial, viral, parasitic, and fungal infections. Tuberculosis is anexample of a bacterial infection that is commonly associatedwith HIV. Thus, studying about the impact of pregnancy onthe course of HIV infection seems intriguing.
The Human ImmunodeWciency virus comprises an outerenvelope, in which are embedded 72 spikes of gp160. Gly-coprotein 160 is the env precursor protein of HIV, which isfurther cleaved into gp120 and gp 41. The gp120 is the sub-unit responsible for the binding with the primary receptor,CD4 receptor, and co-receptors CCR5 and CXCR4. TheHIV env gp 120 can be divided into Wve constant (C1–C5)and Wve variable regions (V1–V5). The V1–V2 regions areinvolved in several aspects of infection in the macrophagessuch as an eYcient virus production in macrophages. TheV3 loop has been a region of interest among the researchersfor long, owing to its signiWcant role in viral infectivity,virus neutralization, replication eYciency, and spread in thehost cells (viral tropism). The V4 and V5 regions are thecomparatively less Xexible regions and have been shown tohave a role in CD4 binding and neutralizing antibodyresponses [5]. The virus attacks the human cells by interac-tion with CD4, the primary receptor for HIV. The interac-tion also involves a co-receptor, CCR5 and CXCR4 beingthe major co-receptors [6]. Binding with the CD4 co-recep-tor causes a conformational change in gp 120 and revealsthe co-receptor-binding site [7, 8]. Based on diVerences ingrowth properties and cytopathic eVect on PBMC’s, HIVproduces syncytium-inducing (SI) and non-syncytiuminducing (NSI) viruses in vitro [9]. A SI cell phenotype is acluster of multinucleate cytoplasm with no visible cellboundaries. Such a phenotype is absent in NSI viruses. NSIviruses utilize CCR5 as their major co-receptor, whereas SIviruses utilize CXCR4 co-receptor [9–11]. The newlyinfected patients primarily exhibit CCR5 (R5) co-receptorusage, whereas people in later stages exhibit CXCR4 (X4)co-receptor usage [12]. Co-receptor prediction is critical for
monitoring disease progression. The present study was car-ried out to study the progression of HIV infection in thepregnant women by studying the co-receptor usage, theprimary determinant of HIV disease progression, number ofN-glycosylations, and sequence variability. Previous stud-ies do not provide any indication whether pregnancy accel-erates progression of HIV infection to AIDS. But it is quitepossible that pregnant women are more vulnerable to HIV-related complications. Most of the published data on co-receptor utilization, replication eYciency, and cytopathiceVects relate to HIV-1 subtype B, while limited informationis available with regard to subtype C. Interestingly, there isno data on co-receptor utilization in HIV-1-positive sub-type C pregnant women. Therefore, the present study wascarried out on HIV-positive samples from India belongingto the following two categories: (1) HIV-positive pregnantwomen and (2) HIV-positive cases from other risk groups. Thestudy focuses on predicting the co-receptor, analyzingsequence variability between the two groups, and studying thenumber of N-glycosylation sites using bioinformatics tools.
Materials and methods
Twenty-Wve HIV sero-positive samples were taken. Ethicalapproval was obtained from the ethical committee ofNational Centre for Disease Control (NCDC) and MaulanaAzad Medical College (MAMC). The samples were fromdiVerent risk groups including heterosexual males, hetero-sexual females, and antenatal cases. Informed consent wasobtained from all participants. Whole blood (3–4 ml) wasdrawn in K2EDTA vacutainers, and PBMC’s were isolatedimmediately after collection of whole blood using Ficoll’sReagent. Genomic DNA, including proviral DNA of HIV,was extracted with the help of QIAamp DNA Blood Minikit, according to the manufacturer’s protocol, and theextracted DNA was run on 0.8% agarose gel to check thequality and quantity. PCR for �-globin was carried outusing previously reported primers, PC03 and PC04, toascertain the quality of the extracted DNA and to verify thatthe genomic DNA isolated is suitable for PCR ampliWca-tion [13]. Nested PCR was carried out for the hypervariableregion (V3–V5) of the env gene with the help of the previ-ously reported primers ED3 and ED14. These amplify a2-kb fragment, spanning from the Wrst exon of rev and thecomplete surface (SU) protein-coding sequence of envgene. The second round of ampliWcation was carried outusing the primers ES7 and ES8 to amplify 0.7-kb region ofthe env gene [14]. AmpliWcations were carried out in ABI9700 thermal cycler using Go Taq PCR core system II(Promega), in order to amplify the »0.7-kb amplicon of theenv (V3–V5) gene of HIV. The ampliWed products weresubjected to sequencing using the Big Dye terminator kit
123

Med Microbiol Immunol (2012) 201:271–276 273
(ABI, USA) in the ABI 3130xl genetic analyzer (ABI,USA). A BLAST search was carried out to conWrm theidentity of strains. The subtype was determined with thehelp of HIV-1 Rega Subtyping Tool [15]. The env genesequences obtained in the present study were submitted toGenBank at http://www.ncbi.nlm.nih.gov (accession num-bers: HM630277-HM630292). The sequences were alignedand translated with the help of MEGA software, version 4.We used the V3 loop amino acid sequence for co-receptorprediction, sequence variability, and number of N-glycosy-lations. Co-receptor prediction was performed with the helpof web based “C-PSSM” (PSSM, Position-speciWc scoringmatrix), (ds) Kernel (http://genome.ulaval.ca/hiv-dskernel)and Geno2pheno (http://coreceptor.bioinf.mpi-inf.mpg.de/)methods [16]. Sequence variability was also studied inthe two groups, with the help of the “Entropy” tool
(http://www.hiv.lanl.gov), which applies Shannon entropyas a measure of sequence variability in amino acid sequence.We looked for diVerences in the number of N-glycosylationsites with the help of “N-Glycosite” tool between the preg-nant group and non-pregnant group [17]. Sequence logosof V3 sequences from HIV-infected pregnant patients andHIV-infected patients from other risk groups were createdusing the online available web logo tool (http://weblogo.berkeley.edu/logo.cgi). Size of each character displays the pro-portion of sequences in which a particular amino acid occurs.
Results
The mean CD4 count in the antenatal risk group was »326,whereas in the other risk groups, it was »407 with the majorchunk of antenatal cases possessing a CD4 in the range of200–400, and the count was quite dispersed in the other riskgroups (Table 1). 50% of our patients were primigravida, thatis, they conceived for the Wrst time. We also had a fewfemales with children from previous pregnancies, and somereported of abortions in the past. Majority of our study sub-jects (50%, i.e., 4/8) were in the third trimester, 37.5% (3 of8) were in second trimester, and 12.5% (1 of 8) were in theWrst trimester of pregnancy at the time of sampling (Table 2).
Sub-typing
The sequences were found to belong to subtype C, as deter-mined by the REGA sub-typing tool.5 (http://dbpartners.stanford.edu/RegaSubtyping/).
Table 1 Table showing the range of CD4 counts in the ANC groupand in the other risk group category
Range (CD4 levels)
ANC risk group (frequency)
Other risk groups (frequency)
<100 0 1
101–200 1 0
201–300 4 2
301–400 2 1
401–500 0 2
501–600 0 1
601–700 0 0
701–800 1 0
801–900 0 1
Table 2 Table showing clinical and immunological details for theantenatal risk group including the CD4 count, history of previous preg-nancies, the gestation period at the time of sampling, and the duration
of gestation which is calculated from the date of LMP (last menstrualperiod) to the date on which the patient delivered
Accession number
Risk group CD4 count
Details of previous pregnancies
Gestation period at the time of sampling
Duration of gestation(as calculated from the LMP to date of delivery)
HM630277 ANC 278 Gravid-5, Parity-3, Abortion-1, Live Birth-1
Third trimester, 7 months, 15 days
8 months, 27 days
HM630278 ANC 215 Gravid-2, Parity-0, Abortion-1, Live Birth-0
Second trimester, 4 months, 22 days
8 months, 11 days
HM630281 ANC 284 Gravid-1, Primi Second trimester, 3 months, 3 days
8 months, 22 days
HM630284 ANC 311 Gravid-2, Parity-0, Abortion-1, Live Birth-0
Second trimester, 5 months, 2 days
8 months, 25 days
HM630285 ANC 214 Gravid-1, Primi Third trimester, 7 months 27 days
8 months, 1 day
HM630288 ANC 316 Gravid-1, Primi Third trimester, 8 months, 2 days
8 months, 22 days
HM630289 ANC 800 Gravid-3, Parity-2, Live Births-2
Third trimester, 7 months 5 days
8 months, 25 days
HM630292 ANC 191 Gravid-1, Primi Second trimester, 5 months, 17 days
8 months, 14 days
123

274 Med Microbiol Immunol (2012) 201:271–276
Co-receptor
Co-receptor usage prediction is critical for monitoringdisease progression. The changes within the V3 regionsuch as increased amino acid charge, insertions, and spe-ciWc amino acid variation are all factors that are predic-tive of CXCR4 usage of subtype C viruses as has beenreported in other subtypes [18]. We used the web basedPSSM method, (ds) Kernel and Geno2 for predicting thesame. There were discrepancies in co-receptor predic-tion for two of our samples (HM630280, HM630285).Majority of sequences, including those from the antena-tal risk group, were found to utilize the co-receptorCCR5, as the predominant co-receptor, and no signiW-cant diVerence in the net positive and negative chargesbetween the two groups were observed as determined bythe PSSM method (Table 3).
N-glycosylation
Glycosylation refers to the addition of saccharides to pro-teins and lipids. The viral proteins undergo glycosylation.N-glycosylation is the most common and involves additionof oligosaccharides to asparagine (N). In the V3 loop, nodiVerence in the number of N-glycosylation sites betweenthe two groups was observed. One N-linked glycosylationsite at position 6 of the V3 loop of the env gene of HIV waspresent in all the sequences, irrespective of the risk group.
Sequence variability
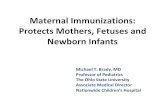
The sequence variability at each of the amino acid positionsin the V3 loop was determined between the two groups.Entropy diVerence between the two groups was found to beinsigniWcant (Figs. 1, 2).
Table 3 Table showing the risk group, net positive and positive charge, predicted co-receptor, and the clinical stage of HIV of the diVerent sam-ples in the study
ANC antenatal care, HM heterosexual male, HF heterosexual female
Accession number
Risk group Cd4 count Age/sex Web PSSM Score Tropism
Geno2pheno (ds) Kernel Clinical manifestations
HM630277 ANC 278 19/F ¡30.51 R5 R5 R5 Asymptomatic
HM630278 ANC 215 27/F ¡29.93 R5 R5 R5 Asymptomatic
HM630279 HM 468 29/M ¡29.93 R5 R5 R5 Asymptomatic
HM630280 HF 240 35/F ¡24.05 R5 X4 R5 Asymptomatic
HM630281 ANC 284 25/F ¡28.60 R5 R5 R5 Asymptomatic
HM630282 HM 298 29/M ¡29.07 R5 R5 R5 Asymptomatic
HM630283 HM 536 30/M ¡29.13 R5 R5 R5 Asymptomatic
HM630284 ANC 311 22/F ¡29.93 R5 R5 R5 Asymptomatic
HM630285 ANC 214 23/F ¡18.91 X4 R5 R5 Asymptomatic
HM630286 HF 398 28/F ¡26.17 R5 R5 R5 Asymptomatic
HM630287 HM 806 37/M ¡29.93 R5 R5 R5 Asymptomatic
HM630288 ANC 316 20/F ¡29.62 R5 R5 R5 Asymptomatic
HM630289 ANC 800 24/F ¡29.17 R5 R5 R5 Asymptomatic
HM630290 HF 83 29/F ¡29.05 R5 R5 R5 Asymptomatic
HM630291 HF 431 31/F ¡28.47 R5 R5 R5 Asymptomatic
HM630292 ANC 191 22/F ¡26.17 R5 R5 R5 Asymptomatic
Fig. 1 Entropy plot of the V3 loop, showing sequence vari-ability in non-pregnant (a) and pregnant (b) HIV-positive sam-ples. x-axis: entropy; y-axis: sequence position in alignment. Absence of any sites with a sig-niWcant entropy diVerence (P < 0.05) between the two groups was observed
123

Med Microbiol Immunol (2012) 201:271–276 275
Discussion
Co-receptor usage prediction is critical for monitoringdisease progression. Predictive methods for inferring co-receptor usage based on the third hyper-variable loopregion (V3) loop region of the viral env gene coding for theenvelope glycoprotein gp120 can help us with monitoringdisease progression while avoiding expensive phenotypictests. The CCR5 co-receptor utilization is an indicative ofthe initial, asymptomatic stage of the infection. In theimmune-compromised, pregnancy stage, the virus can beexpected to lead to a co-receptor switching from CCR5 toCXCR4. Interestingly, this was not the case; the virus in thepregnancy phase was found to utilize the CCR5 co-receptorin majority of the cases, which has been found using threeco-receptor-predicting softwares. Utilization of CCR5 asthe primary co-receptor could be a host strategy, in order tocontinue with a successful pregnancy, and not let the virusaVect the immune-compromised physiology.
Glycosylation of variable loops, such as the V3 loop, ofthe envelope region, are in direct contact with the immunecells of the host. The N-glycosylations have a role inrestricting access to the host receptor-binding sites, thusallowing it to for immune escape from the host. Such astrategy limits the viral exposure to the host immune sys-tem. We did not observe any diVerence in the number ofN-glycosylations in the pregnant group, when comparedwith other risk groups. This implies that the virus does notuse the N-glycosylation strategy in pregnant cases in orderto acquire a survival advantage. In other words, the preg-nancy physiology is such that it does not allow the virus,for immune escape in terms of glycosylation sites.
The diVerence in sequence variability (entropy),between the pregnant and the non-pregnant group, was notnon-signiWcant. The sequence variability exhibited in the
constructed entropy plot shows that in the pregnant group,the immune selective pressure is able to maintain the V3loop sequence, as in the control group, thereby suggestingthat pregnancy does not accelerate HIV infection in termsof sequence variability.
Additionally, it would be useful to observe the above-mentioned parameters in HIV-/TB-infected pregnantfemales as TB is a frequent infection in the Indian subconti-nent. The reason for this would be that subtype C is morepathogenic than subtype B and is known to majorly utilizeCCR5 as the major co-receptor. Also, as observed in astudy by Biru etl al, HIV/TB patients from a diverse humanpopulation from subtype B and C were studied, and it wasobserved that the HIV/TB patients utilized CCR5 co-recep-tor. This is in contrast with the patients infected only withHIV who exhibited CXCR4 co-receptor usage. The HIV/TB group showed a faster HIV-1 env sequence evolutionand a higher viral divergence that probably cause anenhanced pathogenesis when an HIV patient is infectedwith tuberculosis [19].
The cause for the reported deaths discussed earlier couldhave possibly occurred due to the fact that those pregnantwomen were already experiencing an advanced stage of theHIV infection which is evident from their clinical predica-ments, which was accompanied by certain pathologieswhich further exacerbated the pregnancy. In addition, thereports date back to the 1980s mostly, when the present daymolecular techniques that involve sequencing and co-receptor prediction with the help of bioinformatics had notbeen developed or had just started to develop. Therefore,those retrospective reports suVered as a result of methodo-logical and technical diYculties.
In conclusion, pregnancy does not seem to allow thevirus to aVect the immune-compromised mother, by switch-ing co-receptor, or creating N-glycosylation sites in the V3
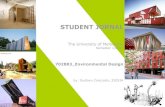
Fig. 2 Sequence logos of (a) V3 Sequences from ANC HIV-infected patients (b) V3 Sequences from HIV-infected patients from other riskgroups. Size of each character displays the proportion of sequences in which a particular amino acid occurs
123

276 Med Microbiol Immunol (2012) 201:271–276
loop, or increasing sequence variability. During pregnancy,the body possibly behaves in a manner such that the infec-tion is alleviated and does not adversely aVect the mother orthe child. This could be through the help of up-regulationand down-regulation of various host restriction factors,cytokines, etc., which need to be studied. Other genes alsoneed to be studied, for sequence variability, N-glycosyla-tion, and other immune pressure revealing parameters at thetime of pregnancy, when compared with the non-pregnantcontrols. Studies on such crucial aspects need to be lookedinto for studying the disease progression during the preg-nancy phase.
Acknowledgments The Wrst author deeply acknowledges thepatients for giving consent for this study. Without them, this study wouldnot have been possible. Author SS acknowledges Wnancial supportfrom the Council of ScientiWc and Industrial Research (CSIR), Delhi,India, during the course of this study. We sincerely thank R S Rautellafor his guidance. We would also like to thank Uma Sharma, MeghaSinghal, Rohit Chawla, and Arti Bahl for their discussions over thework. Authors also thank the staV of the HIV/AIDS Division of NCDCfor their assistance in collecting samples and providing serological andclinical data.
References
1. Wetli CV, Roldan EO, Fojaco RM (1983) Listeriosis as a cause ofmaternal deaths: an obstetric complication of AIDS. Am J ObstetGynecol 147:7–9
2. Rawlison KF, Zubrow AB, Harris MA et al (1984) DisseminatedKaposi’s sarcoma in pregnancy: a manifestation of acquiredimmunodeWciency syndrome. Obstet Gynecol 63:2S–6S
3. Mertz KJ, Parker AL, Halpin GJ (1992) Pregnancy-related mortal-ity in New Jersey, 1975 to 1989. Am J Pub Health 82:595–599
4. Lindan CP, Allen S, SeruWlira A et al (1992) Predictors of mortal-ity among HIV-infected women in Kigali, Rwanda. Ann Int Med116(4):320–328
5. Sirois S, Sing T, Chou KC (2005) HIV-1 gp120 V3 loop for struc-ture-based drug design. Current protein and peptide. Science6:413–422
6. Doms RW, Peiper SC (1997) Unwelcomed guests with masterkeys: how HIV uses chemokine receptors for cellular entry. Virol-ogy 235:179–190
7. Ling H, Usami O, Xiao P et al (2004) The N-Terminal of the V3Loop in HIV Type 1 gp120 Is Responsible for Its Conformation-Dependent Interaction with Cell Surface Molecules. AIDS ResHum Retrovir 20(2):213–218
8. Hartley O, Klasse PJ, Sattentau QJ et al (2005) V3: HIV’s Switch-Hitter. AIDS Res Hum Retrovir 21(2):171–189
9. Fenyö EM, Morfeldt-Månson L, Chiodi F et al (1988) Distinctreplicative and cytopathic characteristics of human immunodeW-ciency virus isolates. J Virol 62(11):4414–4419
10. De Jong JJ, De Ronde A, Keulen W et al (1992) Minimal require-ments for the human immunodeWciency virus type 1 V3 domainsto support the syncytium-inducing phenotype: analysis by singleamino acid substitution. J Virol 66:6777–6780
11. Maas JJ, Gange SJ, Schuitemaker H et al (2000) Strong associa-tion between failure of T cell homeostasis and the syncytium-inducing phenotype among HIV-1-infected men in the AmsterdamCohort Study. AIDS 14(9):1155–1161
12. Regoes Banhoefter (2005) The HIV co-receptor switch: a popula-tion dynamical perspective. Trends Microbiol 13(6):269–277
13. Khoja S, Ojwang P, Khan S et al (2008) Genetic analysis of HIV-1subtypes in Nairobi, Kenya. PLoS ONE 3(9):e3191
14. Delwart EL, Shpaer EG, Louwagie J et al (1993) Genetic relation-ships determined by a DNA heteroduplex mobility assay: analysisof HIV-1 env genes. Science 262(5137):1257–1261
15. de Oliveira T, Deforche K, Cassol S, Salminen M, Paraskevis Det al (2005) An automated genotyping system for analysis of HIV-1and other microbial sequences. Bioinformatics 21:3797–3800
16. Jensen MA, Coetzer M, Wout AB et al (2006) A reliable pheno-type predictor for human immunodeWciency Type 1 subtype Cbased on envelope V3 sequences. J Virol 80(10):4698–4704
17. Zhang M, Gaschen B, Blay W et al (2004) Tracking globalpatterns of N-linked glycosylation site variation in highly variableviral glycoproteins: HIV, SIV, and HCV envelopes and inXuenzahaemagglutinin. Glycobiology 14(12):1229–1246
18. Coetzer M, Cilliers T, Ping LH et al (2006) Genetic characteristicsof the V3 region associated with CXCR4 usage in HIV-1 subtypeC isolates. Virology 356:95–105
19. Biru T, Lennemann T, Sturmer M, Stephan C, Nisius G, Cinatl J,Staszewski S, Gurtler LG (2010) Human immunodeWciency virustype-1 group M quasispecies evolution: diversity and divergencein patients co-infected with active tuberculosis. Med MicrobiolImmunol 199:323–332
123