CorrectionCorrection IMMUNOLOGY. For the article ‘‘Gain-of-function mutations in complement...
7
Gain-of-function mutations in complement factor B are associated with atypical hemolytic uremic syndrome Elena Goicoechea de Jorge*, Claire L. Harris † , Jorge Esparza-Gordillo*, Luis Carreras ‡ , Elena Aller Arranz*, Cynthia Abarrategui Garrido § , Margarita Lo ´ pez-Trascasa ¶ , Pilar Sa ´ nchez-Corral § , B. Paul Morgan † , and Santiago Rodrı ´guez de Co ´ rdoba* *Centro de Investigaciones Biolo ´gicas, Consejo Superior de Investigaciones Cientı´ficas, Ramiro de Maeztu 9, 28040 Madrid, Spain; † Department of Medical Biochemistry and Immunology, School of Medicine, Cardiff University, Henry Wellcome Building, Heath Park, Cardiff CF14 4XN, United Kingdom; ‡ Servicio de Nefrologı´a, Hospital Universitario de Bellvitge, Feixa Llarga s/n 08907 Barcelona, Spain; and Unidades de § Investigacio ´ny ¶ Inmunologı´a, Hospital Universitario La Paz, Paseo de la Castellana 261, 28046 Madrid, Spain Edited by Douglas T. Fearon, University of Cambridge, Cambridge, United Kingdom, and approved October 25, 2006 (received for review May 2, 2006) Hemolytic uremic syndrome (HUS) is an important cause of acute renal failure in children. Mutations in one or more genes encoding complement-regulatory proteins have been reported in approxi- mately one-third of nondiarrheal, atypical HUS (aHUS) patients, suggesting a defect in the protection of cell surfaces against complement activation in susceptible individuals. Here, we iden- tified a subgroup of aHUS patients showing persistent activation of the complement alternative pathway and found within this subgroup two families with mutations in the gene encoding factor B(BF), a zymogen that carries the catalytic site of the complement alternative pathway convertase (C3bBb). Functional analyses dem- onstrated that F286L and K323E aHUS-associated BF mutations are gain-of-function mutations that result in enhanced formation of the C3bBb convertase or increased resistance to inactivation by complement regulators. These data expand our understanding of the genetic factors conferring predisposition to aHUS, demonstrate the critical role of the alternative complement pathway in the pathogenesis of aHUS, and provide support for the use of com- plement-inhibition therapies to prevent or reduce tissue damage caused by dysregulated complement activation. renal disease H emolytic uremic syndrome (HUS) (MIM 235400) is char- acterized by thrombocytopenia, Coomb’s test-negative mi- croangiopathic hemolytic anemia and acute renal failure (1). The typical form of HUS follows a diarrheal prodrome and is associated with 0157:H7 Escherichia coli infections (2). Five percent to 10% of HUS patients lack an association with infection and have the poorest long-term prognosis (1). This atypical HUS (aHUS) usually occurs in adults and in very young children and is associated with mutations or polymorphisms in the genes encoding the complement regulators factor H (fH, CFH) (3–8), membrane cofactor protein (MCP, MCP) (9, 10), and factor I (fI, IF) (11, 12). The molecular mechanisms underlying aHUS are only now beginning to be understood. In contrast to patients with com- plement deficiencies, aHUS patients present relatively normal complement levels (5). Crucially, functional analysis of several CFH, MCP, and IF aHUS-associated mutations has demon- strated that they affect primarily the control of complement activation on cellular surfaces, whereas complement regulation in plasma is not greatly affected (4, 7, 10, 13). These findings have led to the hypothesis that aHUS results from a defective pro- tection of host cells within the context of a ‘‘normal’’ comple- ment function in the fluid phase (7, 14). From this perspective, a situation that triggers complement activation in the microvas- culature will not be properly controlled, and the amplification of the initial damage will result in tissue destruction. Despite these advances in our understanding of the molecular basis of aHUS, no genetic defect has yet been found in two-thirds of aHUS patients, and incomplete penetrance of the disease in individuals carrying fH, MCP, or fI mutations is relatively frequent, suggesting the existence of additional genetic factors that predispose to aHUS. To provide further insights into the genetic factors predis- posing to aHUS we have examined the hypothesis that genetic variants of complement-activating proteins, resulting in exces- sive activation of the complement system, are also aHUS risk factors. Like mutations in the complement regulators, genetic variations in complement activators have the potential to disrupt the balance between activation and regulation, dys- regulating the complement system and predisposing to pathol- ogy when the complement system undergoes activation. Here, we describe mutations in the gene encoding the com- plement-activator factor B (fB, BF) and demonstrate these to be associated with aHUS. We report their functional characteriza- tion and demonstrate that they are gain-of-function mutations. These data offer a complementary view to the previously described loss-of-function mutations in complement regulators and definitively establish the critical role of the complement alternative pathway in the pathogenesis of HUS. In addition, we analyze the issue of incomplete penetrance of disease in BF mutation carriers and show that, in a large multiple-affected Spanish HUS pedigree, the concurrence of an enhanced acti- vation of the alternative pathway of complement with an im- paired protection of host surfaces likely results in unrestricted activation of the alternative pathway at the cellular surfaces and triggers the development of aHUS. Results and Discussion Complement Profiles in aHUS Patients Identify a Subgroup with Evidence of Alternative Pathway Activation. Our registry of aHUS patients includes 74 individuals extensively studied with regard to complement profiles and genomic analyses of the Author contributions: E.G.d.J. and C.L.H. contributed equally to this work; E.G.d.J., C.L.H., J.E.-G., B.P.M., and S.R.d.C. designed research; E.G.d.J., C.L.H., J.E.-G., E.A.A., C.A.G., P.S.-C., B.P.M., and S.R.d.C. performed research; P.S.-C. contributed new reagents/analytic tools; E.G.d.J., C.L.H., J.E.-G., L.C., M.L.-T., P.S.-C., B.P.M., and S.R.d.C. analyzed data; and E.G.d.J., C.L.H., B.P.M., and S.R.d.C. wrote the paper. The authors declare no conflict of interest. This article is a PNAS direct submission. Abbreviations: aHUS, atypical HUS; HUS, hemolytic uremic syndrome; SPR, surface plasmon resonance; vWfA, von Willebrand factor type A. To whom correspondence should be addressed. E-mail: [email protected]. This article contains supporting information online at www.pnas.org/cgi/content/full/ 0603420103/DC1. © 2006 by The National Academy of Sciences of the USA 240 –245 PNAS January 2, 2007 vol. 104 no. 1 www.pnas.orgcgidoi10.1073pnas.0603420103 Downloaded by guest on March 27, 2020 Downloaded by guest on March 27, 2020 Downloaded by guest on March 27, 2020
Transcript of CorrectionCorrection IMMUNOLOGY. For the article ‘‘Gain-of-function mutations in complement...

Gain-of-function mutations in complementfactor B are associated with atypicalhemolytic uremic syndromeElena Goicoechea de Jorge*, Claire L. Harris†, Jorge Esparza-Gordillo*, Luis Carreras‡, Elena Aller Arranz*,Cynthia Abarrategui Garrido§, Margarita Lopez-Trascasa¶, Pilar Sanchez-Corral§, B. Paul Morgan†,and Santiago Rodrıguez de Cordoba*�
*Centro de Investigaciones Biologicas, Consejo Superior de Investigaciones Cientıficas, Ramiro de Maeztu 9, 28040 Madrid, Spain; †Department of MedicalBiochemistry and Immunology, School of Medicine, Cardiff University, Henry Wellcome Building, Heath Park, Cardiff CF14 4XN, United Kingdom; ‡Serviciode Nefrologıa, Hospital Universitario de Bellvitge, Feixa Llarga s/n 08907 Barcelona, Spain; and Unidades de §Investigacion y ¶Inmunologıa, HospitalUniversitario La Paz, Paseo de la Castellana 261, 28046 Madrid, Spain
Edited by Douglas T. Fearon, University of Cambridge, Cambridge, United Kingdom, and approved October 25, 2006 (received for review May 2, 2006)
Hemolytic uremic syndrome (HUS) is an important cause of acuterenal failure in children. Mutations in one or more genes encodingcomplement-regulatory proteins have been reported in approxi-mately one-third of nondiarrheal, atypical HUS (aHUS) patients,suggesting a defect in the protection of cell surfaces againstcomplement activation in susceptible individuals. Here, we iden-tified a subgroup of aHUS patients showing persistent activationof the complement alternative pathway and found within thissubgroup two families with mutations in the gene encoding factorB (BF), a zymogen that carries the catalytic site of the complementalternative pathway convertase (C3bBb). Functional analyses dem-onstrated that F286L and K323E aHUS-associated BF mutations aregain-of-function mutations that result in enhanced formation ofthe C3bBb convertase or increased resistance to inactivation bycomplement regulators. These data expand our understanding ofthe genetic factors conferring predisposition to aHUS, demonstratethe critical role of the alternative complement pathway in thepathogenesis of aHUS, and provide support for the use of com-plement-inhibition therapies to prevent or reduce tissue damagecaused by dysregulated complement activation.
renal disease
Hemolytic uremic syndrome (HUS) (MIM 235400) is char-acterized by thrombocytopenia, Coomb’s test-negative mi-
croangiopathic hemolytic anemia and acute renal failure (1). Thetypical form of HUS follows a diarrheal prodrome and isassociated with 0157:H7 Escherichia coli infections (2). Fivepercent to 10% of HUS patients lack an association withinfection and have the poorest long-term prognosis (1). Thisatypical HUS (aHUS) usually occurs in adults and in very youngchildren and is associated with mutations or polymorphisms inthe genes encoding the complement regulators factor H (fH,CFH) (3–8), membrane cofactor protein (MCP, MCP) (9, 10),and factor I (fI, IF) (11, 12).
The molecular mechanisms underlying aHUS are only nowbeginning to be understood. In contrast to patients with com-plement deficiencies, aHUS patients present relatively normalcomplement levels (5). Crucially, functional analysis of severalCFH, MCP, and IF aHUS-associated mutations has demon-strated that they affect primarily the control of complementactivation on cellular surfaces, whereas complement regulationin plasma is not greatly affected (4, 7, 10, 13). These findings haveled to the hypothesis that aHUS results from a defective pro-tection of host cells within the context of a ‘‘normal’’ comple-ment function in the fluid phase (7, 14). From this perspective,a situation that triggers complement activation in the microvas-culature will not be properly controlled, and the amplification ofthe initial damage will result in tissue destruction.
Despite these advances in our understanding of the molecularbasis of aHUS, no genetic defect has yet been found in two-thirdsof aHUS patients, and incomplete penetrance of the disease inindividuals carrying fH, MCP, or fI mutations is relativelyfrequent, suggesting the existence of additional genetic factorsthat predispose to aHUS.
To provide further insights into the genetic factors predis-posing to aHUS we have examined the hypothesis that geneticvariants of complement-activating proteins, resulting in exces-sive activation of the complement system, are also aHUS riskfactors. Like mutations in the complement regulators, geneticvariations in complement activators have the potential todisrupt the balance between activation and regulation, dys-regulating the complement system and predisposing to pathol-ogy when the complement system undergoes activation.
Here, we describe mutations in the gene encoding the com-plement-activator factor B (fB, BF) and demonstrate these to beassociated with aHUS. We report their functional characteriza-tion and demonstrate that they are gain-of-function mutations.These data offer a complementary view to the previouslydescribed loss-of-function mutations in complement regulatorsand definitively establish the critical role of the complementalternative pathway in the pathogenesis of HUS. In addition, weanalyze the issue of incomplete penetrance of disease in BFmutation carriers and show that, in a large multiple-affectedSpanish HUS pedigree, the concurrence of an enhanced acti-vation of the alternative pathway of complement with an im-paired protection of host surfaces likely results in unrestrictedactivation of the alternative pathway at the cellular surfaces andtriggers the development of aHUS.
Results and DiscussionComplement Profiles in aHUS Patients Identify a Subgroup withEvidence of Alternative Pathway Activation. Our registry of aHUSpatients includes 74 individuals extensively studied with regardto complement profiles and genomic analyses of the
Author contributions: E.G.d.J. and C.L.H. contributed equally to this work; E.G.d.J., C.L.H.,J.E.-G., B.P.M., and S.R.d.C. designed research; E.G.d.J., C.L.H., J.E.-G., E.A.A., C.A.G., P.S.-C.,B.P.M., and S.R.d.C. performed research; P.S.-C. contributed new reagents/analytic tools;E.G.d.J., C.L.H., J.E.-G., L.C., M.L.-T., P.S.-C., B.P.M., and S.R.d.C. analyzed data; and E.G.d.J.,C.L.H., B.P.M., and S.R.d.C. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS direct submission.
Abbreviations: aHUS, atypical HUS; HUS, hemolytic uremic syndrome; SPR, surface plasmonresonance; vWfA, von Willebrand factor type A.
�To whom correspondence should be addressed. E-mail: [email protected].
This article contains supporting information online at www.pnas.org/cgi/content/full/0603420103/DC1.
© 2006 by The National Academy of Sciences of the USA
240–245 � PNAS � January 2, 2007 � vol. 104 � no. 1 www.pnas.org�cgi�doi�10.1073�pnas.0603420103
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

complement-regulatory genes CFH, MCP, IF, and DAF. Wefound mutations in CFH, MCP, or IF in �30% of unrelatedaHUS patients in our cohort [see supporting information (SI)Fig. 6a], in concordance with 50% figures from other aHUScohorts (3–12).
A majority of patients in our aHUS cohort present normal C3,C4, and hemolytic complement levels (SI Fig. 6b), in agreementwith reports describing that, in general, HUS patients are nothypocomplementemic (5). We noticed, however, that some ofthe patients without mutations in the complement-regulatorygenes, including patients H21, H49, H55P, H65, and H71,present evidence of alternative pathway activation. They con-sistently show very low levels of C3 and normal or elevated levelsof C4 over multiple determinations (SI Fig. 6b), and analysis oftheir plasma by Western blot showed the presence of theactivation product Ba (SI Fig. 6c). Interestingly, H55P belongs toa large multiple-affected aHUS Spanish kindred in which diseasesegregated with the MHC region in chromosome 6q24, includingthe BF gene (15, 16).
Identification of BF Mutations in Patients with Alternative PathwayActivation. Although an earlier report excluded BF mutations inanother aHUS cohort (16), the above observations prompted usto search for mutations in BF in the group of patients showingevidence of alternative pathway activation. Two patients in thissubgroup (H21; pedigree BRA and H55P; pedigree PER)carried missense mutations in heterozygosis in the BF gene.Genomic sequencing of BF in H55P revealed a heterozygousmutation (c.858C�G; F286L) in exon 6, encoding the vonWillebrand type A domain of fB. The F286L missense mutationsegregates with the low levels of C3 that are present in differentmembers of family PER and is inherited by all HUS-affectedmembers of this pedigree (Fig. 1; and see SI Table 1). Genomicsequencing of BF in H21 revealed another heterozygous muta-tion (c.967A�G; K323E) in exon 7, also encoding a residuewithin the von Willebrand type A domain of fB. K323E is a de
novo mutation absent in H21 parents (Fig. 1). Parental sampleintegrity in family BRA was confirmed by genotyping markers inthe RCA gene cluster in chromosome 1q32. Neither F286L norK323E mutations were present in a control population of 100normal individuals.
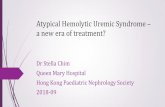
Structure–Function Analyses Identify BF Gain-of-Function Mutationsin aHUS. fB is a zymogen that carries the catalytic site of thecomplement alternative pathway convertase C3bBb. Upon in-teraction with C3b, fB is cleaved by factor D (fD) into twofragments, Ba and Bb. Ba is released, whereas Bb remains boundto C3b, forming the C3bBb alternative pathway convertase, anactive serine protease that cleaves additional C3 into C3b. TheBb fragment of fB comprises two protein domains: a vonWillebrand factor type A (vWfA) domain and a serine protease(SP) domain (17). From structural studies, the fB vWfA domainis globular, composed of several parallel �-sheets surrounded byseven �-helices (18, 19). Site-directed mutagenesis of fB residuesat the C3b-Bb interface in the fB vWfA domain have identifiedseveral residues that are critical for the interaction between C3band fB and influence the normal dissociation of Bb from C3b,whether it is spontaneous or promoted by the complementregulatory proteins FH, DAF, or complement receptor 1 (CR1).In particular, the mutation D279G, in close proximity to theMg2�-binding site within the fB vWfA domain, caused resistanceto decay acceleration mediated by all three regulators andincreased C3b-binding affinity and C3bBb stability (20). Both ofthe BF mutations F286L and K323E identified here in the aHUSpatients alter residues at the C3b–Bb interface in the vWfAdomain in close proximity to D279 (Fig. 2). This finding led usto suspect that these mutations might alter stability of the C3bBbconvertase and activity of the alternative pathway. The mutationK323E changes a fully exposed residue with a positive charge toone with a negative charge. The mutation F286L influencesY319, another fully exposed residue, modifying the edge-to-facestacking interaction between F286 and Y319. The substitution
Fig. 1. Mutations in the BF gene in two aHUS pedigrees. Pedigrees of families PER and BRA are described. Individuals are identified by numbers withineach generation (in Roman numerals). Affected individuals are indicated with filled symbols. Deceased individuals are crossed. Carriers of BF mutationsare indicated by an asterisk. For each BF mutation, the chromatogram corresponding to the DNA sequence surrounding the mutated nucleotide in BF isshown for the appropriate HUS patient and for a control sample. The nucleotide and amino acid numbering are referred to the translation start site (Ain ATG is � 1; Met is � 1).
de Jorge et al. PNAS � January 2, 2007 � vol. 104 � no. 1 � 241
IMM
UN
OLO
GY
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

F286L likely decreases mobility restrictions to Y319 at theC3b–Bb interface (Fig. 2).
To functionally characterize the effects of the K323E andF286L mutations, we purified fB from plasma of appropriatecarriers and normal controls (SI Fig. 7a). We monitored for-mation and decay of the C3 convertase in real time using surfaceplasmon resonance (SPR) (21). To assess the effects of muta-tions, C3b was coated on the biosensor chip surface via thethioester group, and fB from controls or patients was flowedacross the surface in the absence or presence of the fB cleavingenzyme fD (2 �g/ml) to form the proenzyme or activatedenzyme, respectively.
fB isolated from patient H55P demonstrated a much morerapid and efficient formation of the C3bB complex (Fig. 3a). Inthe presence of fD, the expected enhanced formation of theC3bBb complex was seen for control fB, whereas the kinetics ofcomplex formation for fBF286L were not further enhanced fromthat obtained in the absence of fD (Fig. 3b). However, the rateof decay of the mutant convertase was increased compared withcontrol. These differences were observed despite the proteinpurified from patient H55P comprising both normal and mutantfB. To better define the effect of this mutation on convertaseformation, we generated recombinant fBWT and fBF286L proteins(SI Fig. 7b). As a positive control, we also generated fBD279G,previously identified in point mutation studies to increase sta-bility of the convertase (20). Convertase formation and decaywith recombinant fBs was visualized by SPR. In the absence offD, high levels of C3bB were formed with recombinant fBF286L,as seen with native fBF286L (Fig. 4a), suggesting that initialbinding between C3b and fBF286L was more efficient. However,in the presence of fD, fBF286L appeared to form low levels ofactive enzyme, a consequence of enhanced rate of decay, par-ticularly apparent at low concentrations of fB (Fig. 4b; 10 �g/mlshown here). As the concentration of recombinant fB wasincreased, the level of enzyme formed by fBF286L approachedthat formed by recombinant fBWT (Fig. 4c; 37 �g/ml). From
these data, we conclude that, when supply of fB is unlimited (200�g/ml in plasma), fBF286L will generate abundant, rapidly cyclingC3-convertase; in this regard, fBF286L behaves as a gain-of-function mutation that will enhance generation of C3b, dysregu-lating the alternative pathway. The findings explain the increasedlevels of fB cleavage and C3 consumption found in carriers of thefBF286L mutation.
Similar experiments were carried out to test the K323Emutation. fB was isolated from the plasma of patient H21 andused to form convertase on the C3b-coated chip. In contrast tofB from patient H55P, enzyme formation and decay of H21 fBwas indistinguishable from control fB, either in the presence orabsence of fD (Fig. 3). Similarly, when recombinant proteinswere analyzed, enzyme formation by fBWT and fBK323E werecomparable (Fig. 4). To further explore the defect in fBK323E, weused SPR to compare the ability of DAF and fH to decay thecleaved, activated enzyme. Convertase was formed on the C3bsurface by flowing recombinant fBWT or fBK323E in the presenceof fD. Enzyme was allowed to decay naturally for severalminutes, and then soluble DAF (600 nM) was flowed across thesurface. fBWT was rapidly released from the C3b surface,whereas C3bBb formed from fBK323E was clearly more resistantto accelerated decay (Fig. 5a); some Bb remained, even after asecond injection of soluble DAF. Similarly, this enzyme wasmore resistant to accelerated decay by fH (Fig. 5b). In contrastto DAF, which rapidly dissociates from the convertase afterdecay (21), fH binding to C3b is stable. During injection of fH(40 nM) onto the convertase surface, an overall change inamount of protein bound to the surface was evident, a balancebetween fH binding and Bb release. To visualize the change dueto fH binding only, a separate injection of fH was carried out on
Fig. 2. Structural implications for the HUS-associated BF mutations. Diagramof the von Willebrand type A domain of fB. Insight II (BYOSYM softwarepackage; Molecular Simulations, San Diego, CA) was used to draw structure byusing PDB files 1Q0P and 1RS0�A. The positions of the residues Phe-286 andLys-323 that are mutated in the HUS patients are indicated. The position of theMg2� ion and that of the Asp-279 and Tyr-319 are also indicated. Notice theedge-to-face stacking of Phe-286 and Tyr-319 residues. Numbering of residuesis referred to with the initial methionine as ‘‘1’’ and therefore includes thesequence of the N-terminal signal peptide. Residue Asp-279 was described asAsp-254 by Hourcade et al. (32).
Fig. 3. SPR analysis of fBs purified from plasma. (a) Formation of C3bBcomplexes. Control fB (fBWT) and fB purified from H21 (fBK323E) formed similarlevels of the proenzyme, whereas fB purified from H55P (fBF286L) formed C3bBcomplexes much more rapidly and to a much higher level. (b) Formation ofC3bBb complexes. fBWT and fBK323E formed similar levels of complexes withC3b. fBF286L formed high and similar levels of complexes with C3b in theabsence or presence of fD. Resp. Diff, response difference; RU, resonanceunits.
242 � www.pnas.org�cgi�doi�10.1073�pnas.0603420103 de Jorge et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

the C3b surface in the absence of any fB (Fig. 5b; dashed blackline). During fH injection onto recombinant fBWT convertase,the balance between fH binding and Bb release resulted in aninitial small increase in mass. To distinguish between bound fHand residual Bb, DAF was then injected. No further decay wasseen, confirming that fH had decayed the convertase. In con-trast, when DAF was flowed over an identical convertase thathad not been decayed by fH, efficient decay was seen (Fig. 5b).When fH was flowed over the fBK323E convertase, a much largermass change, the balance between fH binding and Bb decay, wasseen, indicating that decay was impaired; injection of DAF afterfH caused further decay, confirming presence of residual Bb(Fig. 5c). Taken together, these data demonstrate that each ofthe mutant fB proteins cause increased alternative pathwayactivation. Formation of the C3bB proenzyme by mutant fBF286Lis much enhanced, which will produce more active enzyme invivo, whereas fBK323E forms a C3bBb enzyme more resistant todecay by DAF and fH, also causing increased enzyme activity invivo. This finding of gain-of-function mutations in the BF geneand their association with aHUS illustrates the important con-tribution of the alternative pathway C3 convertase to the patho-genesis of aHUS.
Polymorphisms in the BF gene have recently been associatedwith age-related macular degeneration (AMD) (22), a diseasethat has been shown to strongly associate with polymorphisms inthe CFH gene and where the macular pathology is driven bycomplement activation (23–26). Two BF polymorphisms wereidentified that were protective for AMD, one of which had beenshown to reduce the activity of fB measured in hemolytic assaysand the other in the signal peptide, was suggested to modulatesecretion of fB. The observed protection in each case wasascribed to a reduced activity of the complement alternative
pathway. This report provides timely support for our suggestionthat genetic changes that alter the function of fB may influencepathology driven by alternative pathway activation.
Disease Penetrance in Carriers of BF Mutations Is Modulated by OtherComplement-Associated Risk Alleles. Within the HUS pedigreereported here, we have identified a total of 11 individualscarrying the F286L BF mutations, but only 7 of them havedeveloped HUS thus far, and the majority of the healthy carriersare old enough to assume that they are not at risk (Fig. 1; andsee SI Table 2). Incomplete penetrance of the disease has alsobeen reported for the aHUS-associated mutations in the CFH,MCP, and IF genes (7, 9–11). Previously we, and others, havereported that two relatively frequent CFH and MCP SNPshaplotype blocks are strongly associated with aHUS (27, 28). Wehave proposed that concurrence of different susceptibility allelesgreatly influences predisposition to aHUS and provides anexplanation for the incomplete penetrance of aHUS in carriersof mutations in the complement regulator genes (28, 29). Toinvestigate whether penetrance of the disease in BF mutationscarriers is influenced by other aHUS genetic risk factors, wegenotyped the CFH and MCP aHUS-associated SNP haplotypeblocks and found that, among carriers of the F286L mutation, allof the HUS patients presented the MCPggaac risk allele, whereasamong the healthy carriers (I-2, II-5, III-12, and IV-1) only theyoungest, and probably still at risk, individual IV-1 harbored theHUS-associated MCPggaac risk allele. Of note, the single af-fected individual with the K323E mutation also presented theMCPggaac risk allele. These data strongly suggest that the HUSphenotype associated with the BF gain-of-function mutations ismodulated by common complement regulator gene variants,
Fig. 4. SPR analysis of recombinant fB proteins. (a) Formation of C3bB complexes. fBWT and fBK323E formed similar levels of the proenzyme, whereas fBF286L
formed C3bB complexes much more rapidly and to a much higher level, similar to those formed by the fBD279G mutant described by Hourcade et al. (20). (b)Formation of C3bBb. At 10 �g/ml, fBWT and fBK323E formed similar levels of complexes with C3b. fBF286L formed lower levels of complexes with C3b in the presencethan in the absence of fD as a consequence of accelerated rate of spontaneous decay of the cleaved fB. (c) Formation of C3bBb. At 37 �g/ml, fBF286L formed highlevels of proenzyme, but when fD was included in the incubation, levels of activated enzyme formed by either recombinant fBWT or fBF286L were comparable.Resp. Diff, response difference; RU, resonance units.
de Jorge et al. PNAS � January 2, 2007 � vol. 104 � no. 1 � 243
IMM
UN
OLO
GY
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

such as the MCPggaac allele, associated with increased risk ofdeveloping HUS (28).
Complement Dysregulation Is the Unifying Event in aHUS Patients.The efficiency of the complement system as an innate defensemechanism against microbial infections depends on a fine con-trol that avoids the wasteful consumption of its components andrestricts its activation to the surface of microorganisms, thuspreventing nonspecific damage to host tissues. Genetic andfunctional analyses of the complement-regulatory proteins fH,MCP, and fI have shown that this critical control of complementactivation may be impaired in aHUS patients (4, 7, 10). Theidentification of gain-of-function mutations in BF associatedwith aHUS reinforces this view and illustrates that dysregulation
of the complement system may also result from an abnormallyincreased activity of the alternative pathway enzymes. Thesefindings implicate other complement components in the samepathway as BF, such as C3 and CFP (encoding properdin), aspotential candidate genes contributing to aHUS susceptibility.
In conclusion, these data demonstrate the critical role of thealternative complement pathway in the pathogenesis of aHUSand expand our understanding of the genetic factors conferringpredisposition to aHUS. Furthermore, they support the hypoth-esis that susceptibility to aHUS involves the concurrence ofmultiple factors (genetic and environmental) contributing todysregulation in the alternative pathway. This hypothesis pro-vides an explanation for the incomplete penetrance of thedisease in carriers of aHUS-associated mutations. The involve-ment of genetic factors may also be relevant in explaining thesevere or fatal outcome of some individuals with the morecommon diarrhea-associated typical HUS. Lastly, our findingsprovide further support for the use of complement inhibitiontherapies in aHUS and perhaps also in severe forms of typicalHUS to prevent or reduce tissue damage caused by dysregulatedcomplement activation.
Patients, Materials, and MethodsPatients. This study includes a total of 74 aHUS patients selectedon the basis of a clinical history of HUS with non-diarrhea-associated origin. Of special relevance are patients H55P, H55,H85, and H112, all members of a large multiple-affected Spanishpedigree, referred to as family PER, and H21, the propositus infamily BRA; specific clinical details are provided in SI Text. Allprotocols included in these studies have been approved bynational and/or local institutional review boards, and all subjectsgave their informed consent.
Complement Analyses. C3, C4, fH, and fI levels were measured inserum or plasma as described (5, 30, 31). FB plasma levels weredetermined by ELISA using a polyclonal goat anti-human fBantibody (New Scientific Company, Cormano, Milan, Italy) asthe capture antibody and a monoclonal mouse anti-human fB(JC1, in house) as the detection antibody. To assess complementfunction and regulation, we used the standard hemolytic assaysCH50 and AP50 and a fH-dependent hemolytic assay (13).Expression levels of the membrane regulators MCP and DAF inperipheral blood lymphocytes (PBLs) were determined by flowcytometry as described (28).
Genotyping. Patients and relatives were screened for mutationsand polymorphisms in CFH, MCP, IF, and BF genes. DNA fromthese individuals was extracted from PBLs or from buccalmucosa cells by using standard procedures. Each exon of theCFH, MCP, and IF genes was amplified from genomic DNA byusing specific primers derived from the 5� and 3� intronicsequences as described (5, 10, 11). All BF exons were amplifiedfrom genomic DNA in three amplicons of 1,800, 2,500, and 2,000bp (see SI Text). Automatic sequencing was performed in an ABI3730 sequencer using a dye terminator cycle sequencing kit(Applied Biosystems, Foster City, CA). Genotyping of HUS-associated CFH and MCP SNPs was performed by resequencingor by allelic discrimination using TaqMan probes (AppliedBiosystems).
FB Purification. FB from patients and controls was purified in onechromatographic step as follows. Two to 5 ml of plasma-EDTAwere directly applied to a Sepharose column coated with the JC1mouse monoclonal anti-human fB antibody and previously equil-ibrated with Tris�HCl (20 mM, pH 7.4) containing NaCl (50mM). After extensive washes with equilibration, acetate (0.1 M,pH4, containing NaCl 500 mM) and borate (0.1 M, pH 8,containing NaCl 500 mM) buffers, the proteins bound to the
Fig. 5. fBK323E convertase decay by sDAF or fH monitored by SPR. (a) Decayby sDAF. C3bBb was allowed to decay spontaneously for several minutesbefore injection of sDAF. Bb from fBWT was removed from the surface byaccelerated decay, whereas Bb formed from fBK323E demonstrated a muchslower rate of accelerated decay. (b) Decay of fBWT by fH. After a period ofspontaneous decay, fH or buffer (‘‘natural decay’’) was injected over thesurface. Mass of protein bound reflected a balance between fH binding to C3band Bb release. To visualize the binding of fH to C3b in isolation, fH wasinjected over the C3b surface (‘‘only fH’’). To confirm efficiency of fH decay,DAF was flowed and released no more Bb. (c) Decay of fBK323E by fH. Injectswere as described above. Bb from fBK323E was much less efficiently decayed byfH as evidenced by the increased protein mass at the surface during the injectand the presence of residual Bb revealed by DAF-mediated decay. Resp. Diff,response difference; RU, resonance units.
244 � www.pnas.org�cgi�doi�10.1073�pnas.0603420103 de Jorge et al.
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

column were eluted with 1 ml of glycine (100 mM, pH 2.5),followed by equilibration buffer. Twenty microliters of Tris�HCl(2M, pH 8) were added to the 500-�l eluted fractions toequilibrate pH. Those fractions containing fB were pooled anddialyzed against Hepes (10 mM, pH 7.4) containing 50 mMNaCl.
Recombinant fB Mutants. The full-length human fB cDNA fromclone IRAUp969B085D6 (RZDP) was introduced in the eu-karyote expression vector pCI-Neo (Promega, Madison, WI),and the F286L, K323E, and D279G mutations introduced bysite-directed mutagenesis using the QuikChange site-directedmutagenesis kit (Stratagene, La Jolla, CA) according to themanufacturer’s instructions. All of the constructs were com-pletely sequenced to confirm that no additional mutations hadbeen introduced. Recombinant fB proteins were expressed instably transfected, cloned CHO cells cultured in Ham’s F-12medium containing 1% FBS and 0.5 mg/ml G418 sulfate (Ge-neticin; GIBCO-BRL, Carlsbad, CA). FB recombinant proteinswere purified from the cell supernatants by affinity chromatog-raphy, as described above.
SPR Analysis of Convertase Formation and Decay. Interactions of fBwith C3b were analyzed on a BIAcore 3000 (BIAcore, Uppsala,Sweden) at 25°C. C3b was deposited on the surface of a CM5chip as described (21). In brief, human C3, fB, and fD (Com-plement Technology, Tyler, TX) were flowed to seed the chipsurface with small amounts of C3bBb; successive cycles of C3,followed by factors B and D, resulted in dense coating of the chipwith C3b coupled in the ‘‘native’’ conformation via the thioesterto hydroxyl groups on the carboxy-methyl dextran surface. Thesurface was stabilized by a short injection of 50 mM diethyl-
amine, pH 11. fB proteins (37 �g/ml, fB purified from patientplasma; 10 �g/ml, recombinant fB) were then flowed over theC3b surface at 20 �l/min in HBS/Mg2� (10 mM Hepes, pH 7.4/50mM NaCl/1 mM MgCl2) with or without 2 �g/ml fD. Interactionswere analyzed by using BIAcore BIAevaluation software, anddata from a blank reference cell were subtracted to correct forchanges in refractive index of flowed solutions.
To analyze DAF-mediated decay of convertase formed byrecombinant fB, the chip surface was coated with C3b asdescribed above and fB (10 �g/ml) with fD (2 �g/ml) wereflowed across to form active enzyme. Soluble DAF (600 nM) wasflowed across the surface for 60 s, and decay was monitored inreal time. To analyze decay by fH, convertase was formed byusing 20 �g/ml fB and 2 �g/ml fD. After convertase formation,either buffer (natural decay) or fH (40 nM) was injected, anddecay was monitored in real time. To remove residual Bb fromthe surface, soluble DAF was injected at 2 �M. Because theoverall change in mass at the chip surface after injection of fHwas a combination of fH binding and Bb decay, fH was alsoinjected over the surface in the absence of convertase formationto assess the mass change that was due to fH binding alone.
We are grateful to all members of families PER and BRA and thecollaborating clinicians for their participation in this study. We alsothank the members of the DNA sequencing laboratory at the Centro deInvestigaciones Biologicas (CIB) and Dr. M. Garcıa-Lacoba of theBioinformatics Department (CIB) for invaluable help. This work wassupported by Spanish Ministerio de Educacion y Cultura GrantSAF2005-00913; Spanish Fondo de Investigaciones Sanitarias GrantsG03/054, G03/011, FIS 03/0621, and FIS 01/A046; and Wellcome TrustGrants 068823/Z and 068599. J.E.-G. was supported by EuropeanMolecular Biology Organization Long-Term Fellowship LTF 522-2006.
1. Moake JL (2002) N Engl J Med 347:589–600.2. Karmali MA (2004) Mol Biotechnol 26:117–122.3. Caprioli J, Bettinaglio P, Zipfel PF, Amadei B, Daina E, Gamba S, Skerka C,
Marziliano N, Remuzzi G, Noris M (2001) J Am Soc Nephrol 12:297–307.4. Manuelian T, Hellwage J, Meri S, Caprioli J, Noris M, Heinen S, Jozsi M,
Neumann HPH, Remuzzi G, Zipfel PF (2003) J Clin Invest 111:1181–1190.5. Perez-Caballero D, Gonzalez-Rubio C, Gallardo ME, Vera M, Lopez-Trascasa
M, Rodrıguez de Cordoba S, Sanchez-Corral P (2001) Am J Hum Genet68:478–484.
6. Richards A, Buddles M, Donne R, Kaplan B, Kirk E, Venning M, TielemansC, Goodship J, Goodship T (2001) Am J Hum Genet 68:485–490.
7. Sanchez-Corral P, Perez-Caballero D, Huarte O, Simckes AM, Goicoechea E,Lopez-Trascasa M, Rodrıguez de Cordoba S (2002) Am J Hum Genet 71:1285–1295.
8. Warwicker P, Goodship THJ, Donne RL, Pirson Y, Nicholls A, Ward RM,Turnpenny P, Goodship JA (1998) Kidney Int 53:836–844.
9. Noris M, Brioschi S, Caprioli J, Todeschini M, Bresin E, Porrati F, Gamba S,Remuzzi G (2003) Lancet 362:1542–1547.
10. Richards A, Kemp EJ, Liszewski MK, Goodship JA, Lampe AK, Decorte R,Muslumanogglu MH, Kavukcu S, Filler G, Pirson Y, et al. (2003) Proc NatlAcad Sci USA 100:12966–12971.
11. Fremeaux-Bacchi V, Dragon-Durey MA, Blouin J, Vigneau C, Kuypers D,Boudailliez B, Loirat C, Rondeau E, Fridman WH (2004) J Med Genet 41:e84.
12. Kavanagh D, Kemp EJ, Mayland E, Winney RJ, Duffield JS, Warwick G,Richards A, Ward R, Goodship JA, Goodship THJ (2005) J Am Soc Nephrol16:2150–2155.
13. Sanchez-Corral P, Gonzalez-Rubio C, Rodriguez de Cordoba S, Lopez-Trascasa M (2004) Mol Immunol 41:81–84.
14. Rodriguez de Cordoba S, Esparza-Gordillo J, Goicoechea de Jorge E, Lopez-Trascasa M, Sanchez-Corral P (2004) Mol Immunol 41:355–367.
15. Carreras L, Romero R, Requesens C, Oliver AJ, Carrera M, Clavo M, AlsinaJ (1981) J Am Med Assoc 245:602–604.
16. Kavanagh D, Kemp EJ, Richards A, Burgess RM, Mayland E, Goodship JA,Goodship THJ (2006) Mol Immunol 43:856–859.
17. Smith CA, Vogel CW, Muller-Eberhard HJ (1984) J Exp Med 159:324–329.18. Bhattacharya AA, Lupher JML, Staunton DE, Liddington RC (2004) Structure
(London) 12:371–378.19. Ponnuraj K, Xu Y, Macon K, Moore D, Volanakis JE, Narayana SVL (2004)
Mol Cell 14:17–28.20. Hourcade DE, Mitchell LM, Oglesby TJ (1999) J Immunol 162:2906–2911.21. Harris CL, Abbott RJM, Smith RA, Morgan BP, Lea SM (2005) J Biol Chem
280:2569–2578.22. Gold B, Merriam JE, Zernant J, Hancox LS, Taiber AJ, Gehrs K, Cramer K,
Neel J, Bergeron J, Barile GR, et al. (2006) Nat Genet 38:458–462.23. Edwards AO, Ritter R, III, Abel KJ, Manning A, Panhuysen C, Farrer LA
(2005) Science 308:421–424.24. Hageman GS, Anderson DH, Johnson LV, Hancox LS, Taiber AJ, Hardisty LI,
Hageman JL, Stockman HA, Borchardt JD, Gehrs KM, et al. (2005) Proc NatlAcad Sci USA 102:7227–7232.
25. Haines JL, Hauser MA, Schmidt S, Scott WK, Olson LM, Gallins P, SpencerKL, Kwan SY, Noureddine M, Gilbert JR, et al. (2005) Science 308:419–421.
26. Klein RJ, Zeiss C, Chew EY, Tsai J-Y, Sackler RS, Haynes C, Henning AK,SanGiovanni JP, Mane SM, Mayne ST, et al. (2005) Science 308:385–389.
27. Caprioli J, Castelletti F, Bucchioni S, Bettinaglio P, Bresin E, Pianetti G,Gamba S, Brioschi S, Daina E, Remuzzi G, et al. (2003) Hum Mol Genet12:3385–3395.
28. Esparza-Gordillo J, Goicoechea de Jorge E, Buil A, Berges LC, Lopez-Trascasa M, Sanchez-Corral P, Rodriguez de Cordoba S (2005) Hum Mol Genet14:703–712.
29. Esparza-Gordillo J, Goicoechea de Jorge E, Garrido CA, Carreras L, Lopez-Trascasa M, Sanchez-Corral P, Rodriguez de Cordoba S (2006) Mol Immunol43:1769–1775.
30. Esparza-Gordillo J, Soria JM, Buil A, Almasy L, Blangero J, Fontcuberta J,Rodriguez de Cordoba S (2004) Immunogenetics 56:77–82.
31. Gonzalez-Rubio C, Ferreira-Cerdan A, Ponce IM, Arpa J, Fontan G, Lopez-Trascasa M (2001) Arch Neurol 58:1923–1928.
32. Hourcade DE, Mitchell L, Kuttner-Kondo LA, Atkinson JP, Medof ME (2002)J Biol Chem 277:1107–1112.
de Jorge et al. PNAS � January 2, 2007 � vol. 104 � no. 1 � 245
IMM
UN
OLO
GY
Dow
nloa
ded
by g
uest
on
Mar
ch 2
7, 2
020

Correction
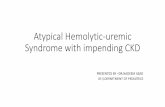
IMMUNOLOGY. For the article ‘‘Gain-of-function mutations incomplement factor B are associated with atypical hemolyticuremic syndrome,’’ by Elena Goicoechea de Jorge, Claire L.Harris, Jorge Esparza-Gordillo, Luis Carreras, Elena AllerArranz, Cynthia Abarrategui Garrido, Margarita Lopez-Trascasa, Pilar Sanchez-Corral, B. Paul Morgan, and SantiagoRodrıguez de Cordoba, which appeared in issue 1, January 2,2007, of Proc Natl Acad Sci USA (104:240–245; first publishedDecember 20, 2006; 10.1073�pnas.0603420103), the authors notethat in Fig. 2, the Lys323 residue of factor B was placedincorrectly; the correct location is outside of the C3b–Bb inter-face. In addition, residue Tyr344 was mislabeled as Tyr319. Thecorrected figure and its legend appear below. These errors do notaffect the conclusions of the article.
Fig. 2. Diagram of the von Willebrand type A domain of fB. Insight II (BYOSYMsoftware package; Molecular Simulations, San Diego, CA) was used to drawstructure by using PDB files 1Q0P and 1RS0�A. The positions of the residuesPhe286 and Lys323 that are mutated in the HUS patients are indicated. Theposition of the Mg2� ion and that of the Asp279 and Tyr344 residues are alsoindicated. Note the edge-to-face stacking of the Phe286 and Tyr344 residues.Numbering of residues is referred to with the initial methionine as ‘‘1’’ andtherefore includesthesequenceoftheN-terminal signalpeptide.ResidueAsp279was described previously as Asp254 by Hourcade et al. (32).
www.pnas.org�cgi�doi�10.1073�pnas.0704511104
www.pnas.org PNAS � June 19, 2007 � vol. 104 � no. 25 � 10749
CORR
ECTI
ON