Coronary perforation after excimer laser coronary ... › content › accj › 23 › 2 ›...
6
330 CoronaryPerforationAfterExcimerLaserCoronaryAngioplasty :The ExchnerLaserCoronaryAngioplastyRegistryExperience DAVIDR .HOLMES, JR .,MD,FACC,GUYS . REEDER,MD, FACC, ZIYADM .B .GHAZZAL,M13,FACC*JOHNF .BRESNAHAN,MD,FACC, SPENCERB .KINGIII, MD, FACC,*MARTINB .LEON,MD,FACC,irFRANK ILTIVATIL, MD,FACNA Rochester,Minnesota ;Atlanta,Georgia ;Washington, D .C. : andLos Angeles,California O*W*WLThisstudyassemedthefrequency ofperforation withexchaer coronaryan y. BackMund. Coronaryarteryperforationafterconventional percutaneoustranshuninalcoronaryangioplasty6extremely rare.Becauselaser corwaary ;mg1kcqpA1ws ;tyinvolvesactual tissue ablation,itInsanIncreasedpotentialforperforation. Methods.All patientsintheExcimerLaserCoronaryAngio- plastyIlegistryweneincludedin Oftprospectivestudy .Thosewho had apoer1foraidUn relatedtothe procedurewerecompared with timewho didnothavethiscomplication . Resuft .Of 2,759 consecutivepatientsin the Excbuer Laser Coronary AngioplastyRegitAry, 36(1 .3%)hadperforation .In these patients, theleftanteriordescendingcoronaryarterywas themostfrequently treatedvessel(53%) . There werenodiffernencesinfibersizesbetweenpatientswithandthosewithout perforation.Amongthepatientswithperforation,36 .1%re- Themechanismofpercutaneoustransluminalcoronaryan- gioplastyinvolvesmechanicalbarotrauma, withvessel stretchandresultantplaqueandintimalormedialfissuresor cracks .Arterialperforationasaresultofthismechanical stretchinjury,although reportedanecdotally,isextremely rare (1-8). Newinterventionaltechnologiesarenowbeing widelyusedforthetreatmentofcoronaryarterydisease . Themechanismofactionof thesenewdevicesisdifferent . Forexample,laserangioplastyinvolvesactualtissueabla- tionandtheproductionofacousticshockwaves (9,10) . It thushasthepotentialforarterialwallperforation(10,11) . Informationisstilllimitedontheincidenceofperforation, thefactorsassociatedwithitandtheoutcomeoftheproce- dure(12-14) .ThepurposeofthisExcimerLaserCoronary Fromthe DivisionofCardiovascularDiseasesandInternalMedicine MayoClinicandMayoFoundation,Rochester,Minnesota ; Divisionof Cardiology,EmoryUniversityHospital,Atlanta,Georgia ;(WashingtonHos- pitalCenter,Washington,D .C . ; andtCedars-SinaiMedicalCenter,Los Angeles,California .Drs .GhazzalandKinghavearoyaltyarrangementwith AdvancedInterventionalSystems,Inc .,Irvine,Californiainvolvingacathe- ternotusedinthisstudy .Dr .Litvackhasafinancialinterestinthesame company . ManuscriptreceivedFebruary16 .1993 ;revisedmanuscript-eceived September21,1993,acceptedSeptember22,1993 . AddressforcomesQndance : Dr.DavidIHolmes,Jr.,MayoClinic,200 FirstStreetSW,Rochester,Minnesota55905 . ©1994by theAmericanCollegeofCardiology quiredcoronaryarterybypasssurgery,16 .7%experiencedan infarctionand5 .6%hadafataloutcome .Amongthepatients withoutperforation,therateswere3 .1%, 3.8%and0.6%, respectively .However,41 .7%of thepatientswithdocumented coronaryarteryperforationdidnotneedcoronaryarterybypass surgery orexperiencemyocardialinfarctionordeath .Noanglo- graphiccharacteristicsdistinguishedlesionswithfromthosewith- outperforation.Thefrequencyofcoronaryarteryperforation declinedovertimewithincreasingoperatorexperience,from 1 .6%inthefirst 1,108patientstoonly0 .4%inthelast1,000 patients(p=0.002). Conclusions . Withincreasingoperatorexperience,therateof perforationwithexcimerlasercoronaryangloplaskyhasde . creased .Whenperforationoccurs,subsequenteventratesin- crease . (JAmCollCardiol1994,23 :330-5) JACCVol .23,No.2 February1994 :330-5 AngioplastyRegistryreportistoassesscoronaryartery perforationoccurring with thisprocedure . ethods Lasersystem .Thelasersystemisa308-nmxenonchlo- ridepulsedexcimerlaserthatismagneticallyswitchedwith apulseduration2:200ns(AdvancedInterventionalSystems) (13,15,16) .Thissystemoperatesonasingle220-Vline,with alaseroutputa200mJ/pulseatupto20to30Hzusing catheterdistaltipenergylevelsof35to60mJ/mm' .During thisRegistryexperience,threeover-the-wiremultifibercath- eterswereusedwithdiatnetc®sof1 .3mm (4F), 1 .6mm (4 .7F)and2 .0mm(6F) . Study patients .beginningin1988,excimerlasercoro- naryangioplastywastestedforthetreatmentofcoronary arterydiseaseatparticipatingcenters(Appendix)afterap- provalbytheinstitutionalreviewboards .Informedconsent wasobtainedfromeachpatient .Criteriaforpatientselection includedsymptomaticordocumentedischemiainthesetting ofcoronaryarterystenosesthatcouldbeaccessedbythe guidewireandlasercatheter . Allpatientsateachcenterwhounderwentlasertreatment wereincludedinthisstudy .Foreachpatient,clinicaland anatomicdataanddetailsandoutcomeoftheprocedure 0735-1097194/$7 .00
Transcript of Coronary perforation after excimer laser coronary ... › content › accj › 23 › 2 ›...

330
Coronary Perforation After Excimer Laser Coronary Angioplasty : TheExchner Laser Coronary Angioplasty Registry Experience
DAVID R. HOLMES, JR., MD, FACC, GUY S . REEDER, MD, FACC,
ZIYAD M. B. GHAZZAL, M13, FACC* JOHN F. BRESNAHAN, MD, FACC,
SPENCER B. KING III, MD, FACC,* MARTIN B. LEON, MD, FACC,ir FRANK ILTIVATIL, MD, FACNA
Rochester, Minnesota ; Atlanta, Georgia ; Washington, D.C. : and Los Angeles, California
O*W*WL This study assemed the frequency of perforationwith exchaer coronary an
y.BackMund. Coronary artery perforation after conventional
percutaneous transhuninal coronary angioplasty 6 extremelyrare. Because laser corwaary ;mg1kcqpA1ws;ty involves actual tissueablation, it Ins an Increased potential for perforation.
Methods. All patients in the Excimer Laser Coronary Angio-plasty Ilegistry wene included in Oft prospective study. Those whohad a poer1foraidUn related to the procedure were compared withtime who did not have this complication .
Resuft. Of 2,759 consecutive patients in the Excbuer LaserCoronary Angioplasty RegitAry, 36 (1.3%) had perforation . Inthese patients, the left anterior descending coronary artery wasthe most frequently treated vessel (53%) . There
were no differn ences in fiber sizes between patients with and those withoutperforation. Among the patients with perforation, 36. 1 % re-
The mechanism of percutaneous transluminal coronary an-gioplasty involves mechanical barotrauma, with vesselstretch and resultant plaque and intimal or medial fissures orcracks. Arterial perforation as a result of this mechanicalstretch injury, although reported anecdotally, is extremelyrare (1-8). New interventional technologies are now beingwidely used for the treatment of coronary artery disease .The mechanism of action of these new devices is different .For example, laser angioplasty involves actual tissue abla-tion and the production of acoustic shock waves (9,10) . Itthus has the potential for arterial wall perforation (10, 11) .Information is still limited on the incidence of perforation,the factors associated with it and the outcome of the proce-dure (12-14). The purpose of this Excimer Laser Coronary
From the Division of Cardiovascular Diseases and Internal MedicineMayo Clinic and Mayo Foundation, Rochester, Minnesota ; Division ofCardiology, Emory University Hospital, Atlanta, Georgia; (Washington Hos-pital Center, Washington, D .C . ; and tCedars-Sinai Medical Center, LosAngeles, California . Drs . Ghazzal and King have a royalty arrangement withAdvanced Interventional Systems, Inc ., Irvine, California involving a cathe-ter not used in this study . Dr. Litvack has a financial interest in the samecompany .
Manuscript received February 16 . 1993 ; revised manuscript -eceivedSeptember 21, 1993, accepted September 22, 1993 .
Address for comes Qndance: Dr. David I Holmes, Jr., Mayo Clinic, 200First Street SW, Rochester, Minnesota 55905 .
©1994 by the American College of Cardiology
quired coronary artery bypass surgery, 16 .7% experienced aninfarction and 5 .6% had a fatal outcome. Among the patientswithout perforation, the rates were 3.1%, 3.8% and 0.6%,respectively . However, 41 .7% of the patients with documentedcoronary artery perforation did not need coronary artery bypasssurgery or experience myocardial infarction or death . No anglo-graphic characteristics distinguished lesions with from those with-out perforation. The frequency of coronary artery perforationdeclined over time with increasing operator experience, from1.6% in the first 1,108 patients to only 0.4% in the last 1,000patients (p = 0.002).
Conclusions . With increasing operator experience, the rate ofperforation with excimer laser coronary angloplasky has de .creased . When perforation occurs, subsequent event rates in-crease .
(J Am Coll Cardiol 1994,23 :330-5)
JACC Vol. 23, No. 2February 1994 :330-5
Angioplasty Registry report is to assess coronary arteryperforation occurring with this procedure .
ethodsLaser system . The laser system is a 308-nm xenon chlo-
ride pulsed excimer laser that is magnetically switched witha pulse duration 2:200 ns (Advanced Interventional Systems)(13,15,16). This system operates on a single 220-V line, witha laser output a200 mJ/pulse at up to 20 to 30 Hz usingcatheter distal tip energy levels of 35 to 60 mJ/mm' . Duringthis Registry experience, three over-the-wire multifiber cath-eters were used with diatnetc®s of 1 .3 mm (4F), 1 .6 mm(4.7F) and 2.0 mm (6F) .
Study patients . beginning in 1988, excimer laser coro-nary angioplasty was tested for the treatment of coronaryartery disease at participating centers (Appendix) after ap-proval by the institutional review boards. Informed consentwas obtained from each patient . Criteria for patient selectionincluded symptomatic or documented ischemia in the settingof coronary artery stenoses that could be accessed by theguide wire and laser catheter .
All patients at each center who underwent laser treatmentwere included in this study . For each patient, clinical andanatomic data and details and outcome of the procedure
0735-1097194/$7 .00

JACC Vol. 23, No. 2February 1994 :330-S
were prospectively collected in the central Excimer LaserCoronary Angioplasty Registry .
This study identified patients who had a perforationrelated to the procedure . The outcome of these patients wascompared with that of patients who underwent laser angio-plasty but did not have this complication . After a perforationwas identified, subsequent management decisions were atthe discretion of the responsible cardiologist and were notdictated by any common prot .x ol .
Procedure. Standard percutaneous techniques wereused. Selection of catheter size was at the discretion of eachoperator but depended on the size of the target lesion andvessel. General recommendations included use of a 1 .3-mmcatheter in a vessel of - 1 .8-mm diameter, a I .6-mm catheterin a vessel of 2:2.3-mm diameter and a 2 .0-mm catheter in avessel of 2t3 .0-mm diameter. After the stenosis or occlusionwas crossed, the catheter was advanced immediately prox-imal to the lesion, and lasing was initiated . Dui- ing lasing, thecatheter was advanced at approximately I mm/s . After theinitial lasing, operators could stop if the result was satisfac-tory, sequentially increase the catheter size or switch toconventional angioplasty .
Periprocedural medications included heparin (10,000 to15,000 U), aspirin (usually given before and continued afterthe procedure), nitrates (both sublingual and parenteralduring the procedure) and calcium channel antagonists .
Throughout the course of this Registry experience, therewere periodic investigator meetings to discuss patient selec-tion and complications. The limited number of perforationswere discussed often and in some detail . On the basis ofobservations made by the investigators from their ownpractice experiences-and theoretic concerns about lasingnormal arterial wall- bifurcation lesions, severely eccentriclesions and severely angulated lesions were thought to be atrisk, as were chronic total occlusions, in which there wasconcern that the guide wire might be intramural rather thanintraluminal . Investigator concerns and discussion of indi-vidual anecdotal cases led operators to become more cau-tious in approaching these subsets of lesions . In addition, theimportance of not lasing when the catheter could not beadvanced was recognized .
Angiographic assessment . Orthogonal views of the coro-nary artery stenosis were obtained at baseline, after laserangioplasty and after conventional angioplasty (if it wasrequired). An attempt was made to use identical prqj~ctionsat the time each angiogram was obtained . Stenosis diameterand lesion length were usually measured with electronic ormanual calipers at each center. Each angiogram coded asshowing a perforation was reviewed by two of us (D.R.H .,G.S.R.), and specific angiographic features were identified(Table 1). The lesion characteristics of the patients withperforation were then compared with the records of 195patients who underwent excimer laser coronary angioplastyat the Mayo Clinic but did not have perforation . The arterialsegments treated in these 195 patients were prospectivelycoded for lesion characteristics .
11OLMES ET AL .
331PERFORATION WITH EXCIMER LASER ANGIOPLASTY
Table II . Definition of Angiographic Morphology in PatientsTreated with Excinter Laser Coronary Angioplasty
Feature
Lesion length
Calcification
Eccentric
Bifurcation
Ostial
Angulation
Comment
Discrete <10 mm ; tubular 10 to 20 mm ;diffuse >20 mm
Patchy or nodular radiopaque deposits withinthe arterial wall
Lumen contained within outer one-third ofdiameter of apparently normal lumen
Presence of a branch vessel originating at thetarget lesion
Lesion to be treated arising at the ostium ofthe arterial segment
Present when angle formed by the centerlinethrough the lumen proximal to the stenosisand the centerline through the lumen distalto 'he stenosis forms an angle X45'
Definitions, A perforation was defined as the extralumi-nal, extravascular appearance of contrast medium . Accord-ing to the prospective criteria of the Advanced Interven-tional Systems Registry, immediate laser success wasdefined as a-20% reduction in the lumen diameter of thestenosis or a minimal lumen diameter >0.8 mm with a1 .3-mm catheter, > I mm with a 1 .6-mm catheter or > 1 .5 mmwith a 2 .0-mm catheter. A procedural success was defined asa diameter stenosis <50% at the end of the procedure(irrespective of whether coronary angioplasty was used),with no in-hospital death, coronary artery bypass grafting,Q wave myocardial infarction or need for an additionalcatheter revascularization procedure later during the hospi-tal period .
Statistical analysis . The frequency of perforation wasassessed over time in the Excimer Laser Coronary Angio-plasty Registry . Differences in baseline characteristics be-tween the patients with and those without perforation wereassessed for the entire Registry . Specific lesion morphologyand characteristics of the perforation were assessed byanalysis of the patients with perforation and of 195 patientswho underwent laser angioplasty at the Mayo Clinic but didnot have perforation .
Continuous variables were expressed as mean valueSD. Dichotomous variables were expressed as frequencies .Differences between groups were assessed with unpairedStudent t test for continuous variables and Pearson chi-square analysis for dichotomous variables . The p valueswere two-tailed, and p < 0 .05 was considered statisticallysignificant .
Results
Of 2,759 consecutive patients who underwent excimerlaser coronary angioplasty from August 24, 1988 to March 6,1992, coronary artery perforation was identified in 36 (1 .3%) .The mean age was 63 .1 years, and 22 patients (61%) weremale. Ten patients (28%) had undergone previous coronary

332
HOLMES ET AL .PERFORATION WITH EXCIMER LASER ANGIOPLASTY
TaW 2. Arterial Segment Treated and Catheter Size Used in2,759 Patients Who Had Excimer Laser Coronary Angioplasty
LAD - left anterior descending coronary artery ; LCx - left circumflex
coronary artery ; LMCA = left main coronary artery ; RCA - right coronary
artery .
angioplasty, seven (19%) had undergone previous coronaryartery bypass grafting .
The left anterior descending coronary artery was the mostcommonly treated vessel in patients with and without perfo-ration (Table 2) . In patients with perforation, the left anteriordescending artery was more frequently treated (53% vs .37%, p < 0 .02). For the remaining vessels, the frequencies oftreatment were similar between the two groups. There wereno differences between the two groups in the catheter sizeused. A 1 .6-mm catheter was used most frequently in eachgroup (44% in the group with perforation, 47% in the groupwithout perforation, p = NS) .
The outcome of the procedure was substantially differentbetween the two groups (Table 3) . In patients with coronaryartery perforation, treatment was based on the clinicalsetting. Typically, use of heparin was discontinued . If theperforation was broad based and large, particularly if on-going ischemia was present, urgent coronary artery bypassgrafting was usually performed. For patients in whom pro-longed inflation was utilized, inflation times were maintained
TAlle 3. Outcome in 2,759 Patients Who Had Excimer LaserCoronary Angioplasty
Perforation
No Perforation(n = 36)
(n = 2 .723)
CABG = coronary artery bypass grafting; MI = myocardial infarction ;PTCA = percutaneous transluminall coronary angioplasty .
JACC Vol. 23, No . 2February 1994:330-5
as long as possible, limited by clinical ischemia. Patientswith perforation had markedly greater rates of coronaryartery bypass grafting, myocardial infarction and death thandid patients without perforation (p < 0.001). The procedurewas successful and not associated with myocardial infarc-tion, death or coronary artery bypass grafting in 93% ofpatients without perforation but in only 42% of patients withperforation (p < 0,001) . In the patients with perforation whodid not undergo coronary artery bypass grafting, adjunctivecoronary angiopiasty was always performed .
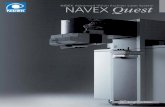
The perforations ranged from small, discrete, extralumi-nal opacifications to large, more broadly based collections ofcontrast medium (Fig . I and 2). The perforation usuallyoccurred in the lesion (63%), although in 22% it occurredWho the lesion . In two patients, the perforation occurredin a chronic total occlusion after the guide wire had beenpassed. Whether the guide wire was initially subintimal inthese patients could not be determined . In one patient, themovement of the laser catheter was filmed and appeared tobe more rapid than the recommended I mm/s . A mean of 1 .6laser passes were made per lesion treated.
Comparison of the baseline lesion characteristics of thepatients with perforations with those of the 195 Mayo Clinicpatients who underwent excimer laser angioplasty but didnot have a perforation (Table 4) showed that there weremore angulated lesions and more ostial lesions in the patientswho developed a perforation. However, the differences werenot statistically significant .
The effect of increasing experience on the incidence ofperforation was assessed in the larger group of 2,888 patientsentered up to September 1992 in the Excimer Laser Coro-nary Angioplasty Registry . In this group, coronary arteryperforation occurred in 1 .2% overall. Perforation occurred in1 .6% of the first 1,888 patients and in only 0 .4% of the last1,000 patients (p = 0 .002).
Discussion
Coronary artery perforation with conventional coronaryangioplasty, although reported anecdotally, is extremelyrare and is usually related to the guide wire rather than to themechanism of dilation itself (1-8) . In contrast, with laserang;oplasty, tissue ablation itself may result in perforation .In an in vitro postmortem human heart study in which a240-Am quartz optical fiber was used, perforation sites werecharacterized by extensive calcific deposits, side branchlocation and tortuous segments (10) . Despite the high fre-quency in early in vitro studies with bare quartz fibers, withthe more current technology used in the Excimer LaserCoronary Angioplasty Registry, coronary artery perforationwas very uncommon, occurring in only 1 .3% of 2,759patients .
Identification of lesions at risk . Identification of lesions atrisk for perforation remains difficult. Recently, Bittl et al .(17) reported a 3% rate of perforation in a group of 764patients treated with another excimer laser system (Spec-
Perforation(n = 36)
No Perforation(n = 2,723)
No. % No . % p Value
Treated segmentLAD 19 53 1,007 37 < 0 .02RCA 9 25 790 29 NSLCx 4 11 408 15 NSVein graft 3 8 436 16 NSLMCA 1 3 82 3 NS
Catheter size (mm)1 .3 7 19 602 22 NS1 .6 16 44 1,273 47 NS2 .0 II 31 714 26 NSUnknown 2 6 133 5 NS
No . % No. % p ValueEventCABG 13 36 .1 85 3 .1 < 0,001Q wave Ml 6 16 .7 105 3 .8 < 0.001Death 2 5 .6 16 0 .6 < 0 .001
No MI, death or CABG 15 41 .7 191 7 .0 < 0 .001Adjunctive PrCA 26 72 .2Successful procedure 15 42 .0 2,532 93 .0 < 0.001

JACC Vol. 23, No . 2February 1994:330-5
Figure 1 . Left anterior oblique view of right coronary artery . A, Dif-fuse disease beginning at acute marginal vessel . B, After lasing, thereis a perforation at the beginning of the lesion, at the side branch(arrow). C, Perforation grows in size (arrow) .
tranetics Corp .) . In their series of 23 patients, 14 had noclinical complications. Multivariate analysis documentedbifurcation lesions to be associated with increased perfora-tion, although the p value was only 0 .049. In addition, vesselperforation was more common when the laser catheter waslarge relative to the diameter of the target vessel or when thevessel was small . In the present series, the latter factor wasavoided. There were no other angiographic characteristicsthat predicted perforation in the analysis by Bittl et al . (17) .
In the present series, identification of high risk lesionswas difficult . Although the left anterior descending coronaryartery was the most commonly treated segment in thepatients who had perforation, it was also the most commonlytreated segment in the patients who did not have perforation .There were no differences in the size of catheter used or inthe number of lasing passes made . Identification of otherprocedural variables is difficult retrospectively . However, inone patient, advancement of the catheter was more rapidthan is recommended, and in two patients, the perforationoccurred during treatment of a chronic total occlusion . Inthese two patients, the wire may have been subintimal, andperforation was thus perhaps more likely . There, were noother recorded procedural details that were different .
HOLMES ET AL .PERFORATION WITH EXCtMER LASER ANGIOPLAS FY 333
Specific lesion morphology could potentially confer anincreased risk of perforation (10) . In this series, our ability topredict complications on the basis of anatomy was limited .Although there were differences in lesion characteristicsbetween patients with and without perforation, they werenot statistically significant . Recently, the effect of morpho-logic predictors of immediate complications after excimerlaser coronary angioplasty was analyzed in a multicenterexperience of 200 patients who underwent 203 proceduresusing a centralized angiographic core laboratory (18) . Le-sions were divided into two groups : lesions associated withprocedural complications (dissection, spasm, thrombus, em-bolus, aneurysm, acute occlusion, perforation, Q wavemyocardial infarction or emergency coronary bypass sur-gery) and lesions not associated with complications . Byunivariate analysis, three factors were associated with oneor more complication, including an abrupt proximal face ofthe lesion (p = 0 .051), an eccentricity index of 30% (p =0.01) and a larger proximal artery diameter (p = 0 .01). Bymultivariate analysis, only the eccentricity index and prox-imal vessel diameter were important . Even though there wasa statistically higher incidence of any complication with aneccentricity index ?30%, 20% of patients with this charac-

334 HOLMES ET AL .PERFORATION WITH EXCIMER LASER ANGIOPLASTY
teristic had a successful result with the laser procedure . Incontrast, visual assessment of whether eccentricity waspresent usually had no predictive value . In the current
Table 4. Angiographic Characteristics in Patients Who HadExcimer Laser Coronary Angioplasty
NoPerforation
Perforation(n = 36)
(n = 195)
JACC Vol. 23 . No. 2February 1994 :330-5
Firm 2 . Right anterior oblique view of left anterior descendingcoronary artery . A, Mid-left anterior descending coronary arterylesion is to be treated. B, After lasing, a small perforation is seen(arrow). C, This is then dilated, and a residual ectatic segment is left(arrow).
series, the number of patients with perforation was small,and there were no significant lesion characteristics thatidentified patients at increased risk of perforation .
Outcome of perforation . When it occurs, perforation isvariable in extent, from small, localized extravasation totamponade . In this series, in-hospital event rates of coronaryartery bypass grafting, infarction, and death were all mark-edly increased compared with rates in the control group .Two of the patients had a fatal outcome. Coronary arterybypass grafting was performed in 36% of patients withperforation but in only 3 .1% of those without perforation .However, in 42% of patients, despite documented coronaryperforation, myocardial infarction and the need for coronaryartery bypass grafting were avoided . In these patients,adjunctive coronary angioplasty allowed stabilization of theangiographic findings and cessation of contrast extravasation .
Study limitations . There are several limitations of thisstudy. The number of perforations was small, and a beta
Characteristic No . % No . % p Value
Eccentric IS 42 97 50 0.48Angulated >45' 11 31 37 19 0.18Branch lesion 6 17 39 20 0.8Ostial 5 14 14 7 0.3Lesion morphology
Discrete 14 39 68 35Diffuse 17 47 74 38 0 .25Tubular 5 14 52 27

JACC Vol. 23, No . 2February 1994:330-5
error is possible . It is also possible that central reading ofangiograms from all sites night have identified specificfeatures. Patients were selected for the procedure at theoperator's discretion . Patients with very eccentric lesions,severe bends or major branch involvement were usually notselected for the procedure, in part because of the concernwith regard to the possibility of perforation or major dissec-tion. Wider use of the device in these patients could haveresulted in a higher incidence of perforation . In addition,there may be other, unmeasured anatomic features thatresult in the catheter being directed against the less involvedwall rather than the wall with the most plaque burdenWhether quantitative angiography or intravascular ultra-sonography would help identify specific lesion characteris-tics cannot be determined from this series .
Changes in the technique-for example, changes in thespeed of advancement-could have had an impact on perfo-ration . There did appear to be a learning curve in eitherpatient selection or technique to avoid or prevent perfora-tion . Perforation occurred in 1 .6% of the first 1,888 patientsbut in only 0 .4% of the last 1,000 patients .
Conclusions . Coronary artery perforation is a rare com-plication of excimer laser coronary angioplasty, occurring in1 .3% of patients in the Registry. In addition, with increasingexperience, the rate has decreased even further, to only0.4% in the last 1,000 cases . When coronary artery perfora-tion occurs, subsequent event rates are increased, although40% of patients can he treated with conventional coronaryangioplasty and have a good outcome .
Appendix
Centers Participating in the Excimer LaserCoronary Angioplasty Registry
Abbott Northwestern Hospital, Alvarado Hospital Medical Cen-ter, Baptist Medical Center of Oklahoma, Carolinas Medical Center,Cedars-Sinai Medical Center, The Christ Hospital, Daniel FreemanMemorial Hospital, Doctors Medical Center, Emory UniversitySchool of Medicine, Georgetown University Hospital, Goleta Val-ley Community Hospital, Hillcrest Medical Center, Hoag MemorialHospital-Presbyterian, Massachusetts General Hospital, The MayoClinic, Medical College of Virginia, The Mercy Hospital of Pitts-burgh, The Methodist Hospital, Miami Heart Institute, PresbyterianMedical Center of Philadelphia, Rober` Wood Johnson UniversityHospital, Rush-Presbyterian-St . Luke's Medical Center, St . Fran-cis Regional Medical Center, Saint John's Hospital and HealthCenter, St . Luke's Hospital of Kansas City, St . Luke's MedicalCenter (Milwaukee), St . Luke's Medical Center (Phoenix), St .Vincent Hospital and Health Care Center, Shands Hospital Univer-
HOLMES ET AL .
335PERFORATION WITH EXCIMER LASER ANGIOPLASTY
sity of Florida, South Miami Hospital, Summit Medical Center, TheUniversity of Alabama at Birmingham, University of Maryland atBaltimore, Washington Hospital Center, William Beaumont Hospi-tal .
ReferencesI . Kimbiris D, Iskandrian AS. Goel I, % al . Transluminal coronary angio-
plasty complicated by coronary artery perforation . Cathet CardiovascDiagn 1992 :8 :481-5 .
2 . Saffitz JE. Rose TE, Oaks JB, Roberts WC . Coronary arterial ruptureduring coronary angioplasty . Am I Cardiol 1983 :51 :902-4 .
3 . Meier B . Benign coronary perforation during percutaneous transluminalcoronary angioplasty . Br Heart I 1985 ;54:33-5 .
4 . Grollier G, Buries H, Commeau P. Foucault JP, Potier JC . Coronaryartery perforation during coronary angioplasty . Clin Cardiol 1986 :9 :27-9 .
5 . Goldman MH, Masden RR, Yared S . Acute rupture of the left anteriordescending coronary artery secondary to percutaneous transluminalangioplasty . Am Heart J 1986 ;112 :1325-8 .
6. Sleffenino G . Meier B, Finci L, et al . Acute complications of electivecoronary angiopiasty : a review of 500 consecutive procedures . Br HeartJ 3988 .59 :151-8.
7 . NassarH, Hasin Y, Gotsman MS. Cardiac tamponade following coronaryarterial rupture during coronary angioplasty . Cathet Cardiovasc Diagn1991 :23 :177-9 .
8 . Gonzalez-Santos JM, Vallejo JL, Pineda T, Zuazo JA . Emergencysurgery after coronary artery disruption complicating PTCA . Report offour cases . Thorac Cardiovasc Surg 1985 :33 :244-7 .
9. Tomaru T . Geschwind HJ, Boussignac G, Lange F, Tahk SJ . Character-istics of shock waves induced by pulsed lasers and their effects on arterialtissue : comparison of excimer, pulse dye, and holmium YAG lasers . AmHeart J 1992 :123 :896-904 .
10. Isner JM, Donaldson RF, Funai JT, et al . Factors cantributing toperforations icbc-hing from laser coronary angioplasty : observations in anintact human postmortem preparation of intraoperative laser coronaryangioplasty . Circulation 1985 ;72 Suppi 11 :11-191-9 .
11 . Parker JD, Ganz P, Selwyn AP, Bittl JA . Successful treatment of anexcimer laser-associated coronary artery perforation with the Stackperfusion catheter . Cathet Cardiovasc Diagn 1991 ;22 :118 -23-
12. Sanborn TA, Bittl JA, Hershman RA, Siegel RM . Percutan-ous coronaryexcimer laser-assisted argiopiasty: initial multicenter experience in 141patients . J Am Coll Cardiol 1991 ;17 Suppl B :169B-73B .
13. Cook SL, Eigler NL, Shefer A, Goldenberg T, Forrester JS, Litvack F .Percutaneous excimer laser coronary angioplasty of lesions not ideal forballoon angioplasty . Circulation 1991,84 :632-43 .
14 . Geschwind HL Dubois-Rande J-L, Zelinsky R, Morelle IF, BoussignacG. Percutaneous coronary mid-infra-red laser angioplasty . Am Heart J1991 ;122 :552-8 .
15. Pacala TJ, McDerrnid IS, Laudenslager JB . Ultranarrow linewidth,magnetically switched, long pulse, xenon chloride laser. I Appi Nysiol1984 :44 :658-60 .
16 . Grundfest WS, Litvack F, Forrester JS, et al . Laser ablation of humanatherosclerotic plaque without adjacent tissue injury . J Am Coll Cardiol1985 ;5 :929-33 .
17 . Bittl JA, Ryan TJ Jr . Keaney J1 Jr, et al . Coronary artery perforationduring excimer laser coronary angioplasty . J Am Coll Cardiol 1993 ;21 :1158-65.
18 . Ghazzal ZMB. Hearn JA, Litvack F, et al . Morphological predictors ofacute complications after percutaneous excimer laser coronary angio-plasty : results of a comprehensive angiographic analysis : importance ofthe eccentricity index . Circulation 1992 ;86 :820-7 .












![Applications of excimer laser in nanofabricationchouweb/publications/211 Xia... · Applications of excimer laser in nanofabrication ... Since its invention in 1960 [1, 2], laser has](https://static.fdocuments.in/doc/165x107/5b7961717f8b9a02268d8364/applications-of-excimer-laser-in-nanofabrication-chouwebpublications211-xia.jpg)