Coronary CT angiography: Developments and Clinical...
53
Coronary CT angiography: Developments and Clinical Indications Eleni C Vourvouri Cardiologist, PhD, FESC Euromedica Geniki Kliniki , Research Associate ,2nd Cardiology Department, Hippokrateio University Hospital , Thessaloniki 15 th North Hellenic Cardiology Congress Thessaloniki , 26-28/5/ 2016
Transcript of Coronary CT angiography: Developments and Clinical...

Coronary CT angiography:
Developments and Clinical Indications
Eleni C VourvouriCardiologist, PhD, FESC
Euromedica Geniki Kliniki,
Research Associate ,2nd Cardiology Department, Hippokrateio University Hospital, Thessaloniki
15th North Hellenic Cardiology Congress
Thessaloniki , 26-28/5/ 2016

NO CONFLICTS OF INTEREST

12/1/05The promise of the 3-D CT scanBy Avery Comarow
Most of the storefront enterprises that not long ago were pitching elaborate 3-D "multislice" CT scans to the worried well have disappeared. Once scanned, most people didn't come back for rechecks. Or, in many cases, patients discovered that suspicious spots
‘Saving Your Life: Modern Medical Miracles’In a weeklong series, NBC's ‘Today’ show features technological breakthroughs in medicine. Here's more

CT-coronary angiography: developments
Year
Cardiac
motion
Artefacts =
(Temp.
Resolution)
(ms)
Breath hold
time (s)
Spiral
CT
1990
1000
-
EBCT
CA
1995
100
40
4-slice
MS-CT
1998
500
40
12-16 slice
MS-CT
2002
420
20
16 slice
MS-CT
2003
370
20
64 slice
MS-CT
2004
165
10
64 slice
MSCT
Dual
source
2006
75
<10

Year
Cardiac
motion
Artefacts =
(Temp.
Resolution)
(ms)
Breath hold
time (s)
Spiral
CT
1990
1000
-
EBCT
CA
1995
100
40
4-slice
MS-CT
1998
500
40
12-16 slice
MS-CT
2002
420
20
64 slice
MS-CT
2004
165
10
16 slice
MS-CT
2003
370
20
64 slice
MSCT
Dual
source
2006
75
<10
CT-coronary angiography: developments

Expert Review of Medical Devices
2016


• Coronary Calcification (CAS)
• Coronary CT Angiography (CCTA) • Aortic Assessment (anuerysm, dissection)
• Pulmonary Embolism
• Pericardial disease
• Congenital heart disease
• Cardiac thrombi & tumor
• Quantification cardiac anatomy & volumes, global & regional function
• Venous Anatomy – Pulmonary and Coronaryveins pre-procedure
CT – Cardiac Applications

Estimation of presence of coronary artery disease
Age, Sex, Symptoms
Age, Sex, Symptoms,
diabetes, hypertension,
dyslipidaemia and smoking
1.Diamond and Forrester modelN Eng J Med. 1979;300:1350-8
2. Duke clinical scoreAnn Intern Med 1993;118:81-90

Estimation of presence of coronary artery disease
Age, Sex, Symptoms
Age, Sex, Symptoms,
diabetes, hypertension,
dyslipidaemia and smoking
1.Diamond and Forrester modelN Eng J Med. 1979;300:1350-8
2. Duke clinical scoreAnn Intern Med 1993;118:81-90
3. New prediction model
BMJ 2012;344:E3485
Age, Sex, Symptoms,
diabetes, hypertension,
dyslipidaemia and smoking
Coronary Calcium Score

No calcification Mild Severe
CT Calcium Score : Predictive Value
Calcium Score
≤ 10
11 – 100
101 – 400
401 – 1000
> 1000
NP
5946
2044
1432
632
332
All-cause death %
1.0
2.6
3.8
6.3
12.3
Relative Risk Ratio
---
2.5
3.6
6.2
12.3
Shaw Radiology 2003;228:826

Linear Scale of Progressively Higher Event Rates
Hundred of peer-reviewed manuscripts


Hadamitzky M et al, Eur Heart J 2013
Pundziute G et al, JACC 2007



Kaplan Meier for MORTALITY-FREE
Survival
Kaplan Meier for MACE-FREE
Survival


APPROPRIATE USE CRITERIA
ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS
2013 Multimodality Appropriate Use Criteria for the Detection and Risk
Assessment of Stable Ischemic Heart Disease
A Report of the American College of Cardiology Foundation Appropriate Use
Criteria Task Force, American Heart Association, American Society of
Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society
of America, Heart Rhythm Society, Society for Cardiovascular Angiography and
Interventions, Society of Cardiovascular Computed Tomography, Society for
Cardiovascular Magnetic Resonance, and Society of Thoracic Surgeons
Journal of the American College of Cardiology
2014 by the American College of Cardiology
Foundation

Appropriateness Indications
• Evaluation of patients with Chest Pain and uninterpretable ECG or
inability to exercise
• Evaluation of patients with Chest Pain and non diagnostic stress tests
• Evaluation of patients with cardiovascular risk factors and atypical symptoms
• Congenital Heart Disease
• Coronary Anomaly (suspicion)
• Prior to redo cardiac surgery
• In the emergency room for acute chest pain in pts with low to intermediate risk
Maybe in asymptomatic high risk patients

Post revascularization
(PCI or CABG)
Symptomatic
Post revascularization
(PCI or CABG)
Asymptomatic


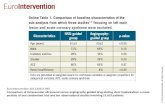
PLAQUE CHARACTERIZATION

Plaque Type
Calcified
Partly calcified
“Mixed“
Non-calcified

Motoyama, JACC 2007
Schuijf et al, Acad Radiol 2007
Hoffmann, AJC 2006
Post-hoc Analysis of Plaques in ACS:
- More non-calcified components than stable lesions
- Positive Remodeling (87%)
-- “Spotty“ calcification
- Lower CT attenuation (< 30 HU)

Atherosclerotic plaque characteristics-APCS
Positive Remodelling RI (Remodelling Index) >=1,10
Low attenuation plaque: HU <30
Spotty calcification < 3mm

RI=Maximum
Reference
Maximun
Reference


CCTA
STRENTH AND WEAKNESS

First
AuthorTechnique Patients
Not
evaluable
Sensitivit
ySpecificity
Negative
Predictive
Value
Leschka 64-slice CT 67 -- 94% 97% 99%
Leber 64-slice CT 59 7% 73% 97% 99%
Ehara 64-slice CT 69 8% 90% 94% 95%
Raff 64-slice CT 70 12% 86% 95% 98%
Fine 64-slice CT 66 4% 95% 96% 92%
Ropers 64-slice CT 82 4% 95% 93% 99%
Mollet 64-slice CT 52 2% 99% 95% 99%
Nikolaou 64-slice CT 72 10% 86% 95% 97%
Schlosser 64-slice CT 61 100% 95% 100%
Mühlenbru 64-slice CT 51 - 87% 95% 98%
Meijboom 64-slice CT 104 - 92% 91% 99%
Schuijf 64-slice CT 60 - 85% 98% 99%
Oncel 64-slice CT 80 - 96% 98% 99%
Herzog 64-slice CT 50 - 89% 92% 97%
Ehara 64-slice CT 69 8% 90% 94% 95%
Shabestari 64-slice CT 143 2% 94% 97% 97%
Cademartii 64-slice CT 72 0% 100% 98.6% 100%
Hausleiter 64-slice CT 114 8% 92% 92% 99%
Meijboom 64-slice CT 254 - 88% 94% 99%
Andreini 64-slice CT 200 3% 99% 96% 100%

MPS vs. STRESS ECHO MPS vs. CTCA
Meta-analysis including 17 studies,
1405 pts, in which MPS was directly
compared to Stress echocardiography
Schinkel AFL et al,
Eur Heart J 2003
MPS: pooled data from
50 studies,6971 pts. Mean
prevalence of CAD 75%
CTCA: pooled sens. Spec.
In series totaling 1653 pts
Mean prev. of CAD 63%
Carli MF, Hachamovitch R,
Circulation 2007

-Gold standard for diagnosis of lesion-specific ischemia
-Improves event-free survival and cost effectiveness
FFR <0,80 lesion specific ischemia
FFR -Fractional flow reserve

1. DISCOVER-FLOW(Diagnosis of Ischemia-Causing Stenoses Obtained Via
Noninvasive Fractional Flow Reserve) Study
2. De FACTO
(Determination of Fractional Flow Reserve by
Anatomic Computed Tomographic Angiography
FFR CT

DISCOVER-FLOW(Diagnosis of Ischemia-Causing Stenoses Obtained Via
Noninvasive Fractional Flow Reserve) Study
103 patients with suspected or known CAD ,
4 centers (Korea, Latvia, USA)
FFR-CT produced sensitivity and negative predictive value similar
to CT alone but much higher scores for specificity (82%vs 40%)
and positive predictive value (74%vs 47%)

-FFRCT improved diagnostic accuracy (20%) in
discrimination of hemodynamically significant
lesions due to higher sensitivity and specificity
-for intermediate lesions improvement in
sensitivity
De FACTO
(Determination of Fractional Flow Reserve by
Anatomic Computed Tomographic Angiography


Subjects analysed 254
10 participating centers worldwide
Norgaard JACC 2014;63:1145-1155


CCTA Invasive angiography FFR FFRCT= no ischemia
No ischemia
ischemia

Additive diagnostic value of atherosclerotic plaque
characteristics to non-invasive FFR for identification of
lesions causing ischaemia: results from a prospective
international multicentre trial
Ryo Nakazato, MD; Hyung-Bok Park, MD; Heidi Gransar, MSc;
Jonathon A. Leipsic, MD; Matthew J. Budoff, MD; G.B. John Mancini, MD;
Andrejs Erglis, MD; Daniel S. Berman, MD; James K. Min
EuroIntervention 2015 Sep

64–STAT randomized trial
Acute Chest Pain in ED
• Goldstein et al. JACC Feb 2007;49:863
Acute Chest Pain

CCTA (n=99) SOC (n=98)
• Reduced diagnostic time by 77% (3.4 hr vs. 15.0 hr, p<0.001)
• Lower costs ($1586 vs. 1872, p<0.001) [15%]
• Fewer repeat evaluations for CP (2% vs. 7%)
• Nondx 5% with newer CT scans
• Both approaches 100% safe (2-years)
Goldstein et al. J Am Coll Cardiol 2007.
Exclusion of CAD in acute chest pain
CCTA immediately excluded or identified CAD as cause of
CP in 75% patients (67 normal cors, 8 severe CAD).

Fifty percent of patients with acute chest pain and low to
intermediate likelihood of
ACS are free of CAD by CT and have no ACS.


ROMICAT II, U Hoffmann




Pulmonary Embolism
Coronary Artery
Aortic Dissection
RCA & LAD Stenosis
53 year old male with chest pain

CONCLUSIONS
• Tremendous growth in evolution of cardiovascular computed tomography
• Numerous multicenter trials and registries about clinical value of CCTA
CAC and CCTA improve selection of patients for preventive care-
Pharmacotherapy and Lifestyle Modification
All of the data suggest that CCTA is superior or at least equivalent to other
non-invasive tests

CTCA has high negative predictive value for
obstructive CAD. After a negative CTCA no other test
is needed
High value of CTCA in sequential or follow-up testing
in symptomatic patients
In asymptomatic patients CAC may be appropriate
in intermediate and high- risk individuals and either
stress or anatomic imaging (CTCA) in higher-risk
individuals
Conclusions 1

PLAQUE CHARACTERIZATION
•High- risk plaques = positive remodelling, low attenuation
and spotty calcification
•FFR -CT : novel non- invasive method for determining lesion-
specific ishemia
Increases accuracy, specificity and PPV of CCTA
•The combination of atherosclerotic plaque characteristics (PR,
LAP, SC) and FFR-CT may improve identification of lesion
specific ischemia
Conclusions 2