Ocular Manifestations of Systemic Diseases Dr.Turki AL- Turki Consultant Ophthalmlogist

C
REVIEW
CURRENTOPINION Ocular manifestations of drug and alcohol abuse
opyright © Lippincott Will
www.co-ophthalmology.com
a ´ a,b a,b,c
Jason Peragallo , Valerie Biousse , and Nancy J. NewmanPurpose of review
The purpose of this study is to review commonly encountered adverse ocular effects of illicit drug use.
Recent findings
Drug and alcohol abuse can produce a variety of ocular and neuro-ophthalmic side effects. Novel,so-called ‘designer’, drugs of abuse can lead to unusual ocular disorders. Legal substances, when used inmanners for which they have not been prescribed, can also have devastating ophthalmic consequences.
Summary
In this review, we will systematically evaluate each part of the visual pathways and discuss how individualdrugs may affect them.
Keywords
alcohol abuse, drug abuse, drug-induced ocular manifestations, endophthalmitis, fetal alcohol syndrome
INTRODUCTION
Drugs of abuse are substances that are either illicit,and are used by individuals recreationally, or arelegal substances that are used in a manner for whichthey were not prescribed. Effects of these substanceson the visual system can range from mild keratop-athy, to severe vision loss from endophthalmitis oroccipital lesions. The effects of drugs of abuse on thevisual system are best addressed anatomically.Routes of administration include, but are not lim-ited to, oral ingestion, nasal inhalation, intravenousinjection, smoking, topical application or appli-cation to other mucosal surfaces. The developmentof novel substances of abuse and novel routes ofadministration may surprise even the most astuteclinician if substance abuse is not suspected.
aDepartment of Ophthalmology, bDepartment of Neurology andcDepartment of Neurological Surgery, Emory University School of Medi-cine, Atlanta, Georgia, USA
Correspondence to Nancy J. Newman, MD, Department of Ophthal-mology, Neuro-Ophthalmology Unit, Emory University School of Medi-cine, 1365-B Clifton Road NE, Atlanta, GA 30322, USA. Tel: +1 404778 5360; e-mail: [email protected]
Curr Opin Ophthalmol 2013, 24:566–573
DOI:10.1097/ICU.0b013e3283654db2
PRECORNEAL TEAR FILM
Abnormalities of the tear film can induce severevisual dysfunction due to the creation of an irregularrefracting surface.
Smoking has been associated with an increasedincidence of dry eye [1]. The Beaver Dam Eye Studyfound that dry eye symptoms were related to ahistory of heavy alcohol consumption, but not cur-rent alcohol consumption [2].
A recent investigation of patients followingethanol ingestion described detection of ethanolin the tears, along with a decreased tear breakuptime. The proposed mechanisms for the alteredtear function were that ethanol increased tear
iams & Wilkins. Unautho
osmolarity, acted as a solvent and could disturbcytokine production [3
&
]. In this manner, ethanolcould exacerbate the signs and symptoms of dry eyesyndrome. A comparative case–control study [4]between men who drank heavily (at least four drinksper day) and nondrinkers showed that heavy etha-nol ingestion was associated with a decreased tearbreak up time, lower Schirmer I test, as well asaltered conjunctival impression cytology in com-parison to nondrinkers.
CONJUNCTIVA
Conjunctival and ciliary injection is associated withuse of marijuana [5] and with heroin use.
One of the more creative routes of use for heroinwas recently described in a case report from Iran inwhich an individual presented with an unusualchronic conjunctival lesion [6]. Conjunctival biopsyrevealed chronic inflammatory changes secondaryto repeated topical applications of crystallized her-oin into the inferior fornices.
rized reproduction of this article is prohibited.
Volume 24 � Number 6 � November 2013

KEY POINTS
� The abuse of drugs and alcohol can have seriousconsequences for the visual system.
� Novel routes of administration and use of novel drugsof abuse can have consequences for the visual systemthat surprise the most astute clinicians if drug abuse isnot suspected.
� For patients who have unusual presentations, suspicionof drug abuse may be warranted.
Ocular manifestations of drug and alcohol abuse Peragallo et al.
Cornea
The cornea contains the highest concentration ofnerve endings in the entire body. Both prescribedand illicit drugs of abuse topically applied mayanaesthetize the cornea, leading to injuries of theocular surface and predisposition to infectious cor-neal ulcers. Agents often implicated in these injuriesinclude cocaine, crack cocaine [7] and topical anaes-thetics.
Poulsen et al. [7] described a case series of pre-sumed methamphetamine-related corneal ulcera-tion with devastating keratitis that resulted inperforation requiring penetrating keratoplasties [8].
Self-prescription of topical anaesthetics is wellknown to induce severe corneal damage. A series of19 patients from Turkey described individuals whohad suffered occupational injuries such as metallicforeign bodies, welding flash, or chemical injury.These patients were either self-medicated with prop-aracaine hydrochloride (available over the counterin Turkey) prior to hospitalization for corneal dis-ease, or self-medicated while hospitalized. Despitewarnings of the devastating ocular consequences ofanaesthetic abuse, 12 of these patients continued toabuse their topical anaesthetic. These patients werefollowed for at least 1 year, with 15.4% of thepatients becoming legally blind [9]. A psychiatricevaluation may be indicated for patients withtopical anaesthetic abuse if they exhibit signs ofMunchausen’s syndrome [10]. Finally, an orallyingested antitussive agent, benzonatate, has beenreported to be abused as a topical anaesthetic bybreaking the capsules and directly applying thecontained gel [11].
Iris
Multiple drugs of abuse affect pupil size and reac-tion. Use of opiates, both legally and illicitly, leadsto pupillary miosis [5]. Cocaine’s inhibition ofreuptake of norepinephrine causes pupillarymydriasis (useful in clinical practice in determining
Copyright © Lippincott Williams & Wilkins. Unau
1040-8738 � 2013 Wolters Kluwer Health | Lippincott Williams & Wilk
the presence of a Horner syndrome). Methamphet-amine also causes pupillary mydriasis. Increasinguse of a newer designer drug, ‘bath salts’, composedof a variety of molecules in a class of chemicalscalled phenethylamines [which includes meth-amphetamine, 3,4-methylenedioxy-N-methylam-phetamine (MDMA) and methcathinone] has ledto a substantial number of poison control calls inthe USA [12]. Route of administration of bath saltsincludes inhalation, oral ingestion and injection[12]. Sale of 31 specific ‘bath salt’ compounds inthe USA was banned in July 2012. In an analysis of1633 emergency department visits for acute ‘bathsalt’ intoxication, 7.1% of patients had mydriasis,although coingestion of other intoxicants occurredat a rate of 26% [12]. The ocular side effects of thisclass of drug of abuse will need to be further clarifiedif, despite their illegality, these drugs continue toincrease in popularity.
Angle and ciliary body
Inhalation of marijuana leads to an acute short-termdecrease in intraocular pressure [13], suggesting thepossible use of marijuana or its derivatives for thetreatment of glaucoma. However, due to its shortduration of action, lack of long-term studies and theother deleterious effects of marijuana includingdecreasing blood pressure (and possible optic nervehead perfusion), the American Glaucoma Societyissued a position statement that use of marijuanain the treatment of glaucoma is not recommended[14]. A single case of recurrent bilateral angle-closureglaucoma following the use of marijuana andMDMA was reported, with resolution of symptomsafter cessation of MDMA use [15].
The consumption of alcohol has been associatedwith elevated intraocular pressure and glaucoma inseveral studies [16].
Lens
Drugs of abuse rarely directly affect the crystallinelens. However, multiple case reports of cataractsassociated with fetal alcohol syndrome have beenpublished [17]. A single case of bilateral congenitaltriangular cataracts in an infant of a methamphet-amine-abusing mother was reported, but definitecausation was not established [18]. Many studieshave examined the association of alcohol consump-tion with cataract formation. These studies weresummarized and analysed by Wang et al. [16],who found that current evidence supports a mildprotective effect of moderate alcohol consumptionon cataract formation, and an increased prevalenceof cataracts among heavy alcohol consumers. The
thorized reproduction of this article is prohibited.
ins www.co-ophthalmology.com 567

C
Ocular manifestations of systemic disease
Beaver Dam Eye Study found that smokingcigarettes had a dose–response relationship withthe formation of cataracts [19,20]. Further studieshave confirmed the association of cigarette smokingwith cataract formation [1,20].
Retina
Retinal disease from illicit drug use includes embolicphenomena resulting from intravenous drugdelivery. Talc retinopathy (embolic phenomenaresulting from drug impurities delivered intra-venously) was first described in patients who self-injected methylphenidate hydrochloride [21].Refractile particles in the perifoveal arterioles, withpossible retinal ischemia, are seen in patients withtalc retinopathy. It is well documented in theophthalmic literature to occur with other intrave-nously injected drugs as well [22]. Talc retinopathymay actually represent the accumulation of micro-emboli, rather than single embolic particles [23].Localization of talc retinopathy to the inner retinallayers is now possible by demonstrating hyper-reflective areas on ocular coherence tomography,corresponding to refractile bodies seen on fundu-scopy [24]. A recent publication described crystal-line retinopathy as a result of intranasalmethamphetamine use [25]. The mechanisms pro-posed included uptake by lymphoid tissue, anddiffusion into pulmonary capillaries.
The use of intranasal cocaine was associatedwith the development of a bilateral, symmetricmaculopathy, presenting as decreased colour sensi-tivity, possibly from an adulterant [26]. A class ofdesigner drugs, the alkyl nitrites, including iso-propyl nitrite and isobutyl nitrite, has been impli-cated in ‘poppers maculopathy’ [27
&
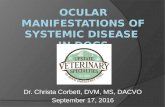
,28,29]. Theoffending agent is inhaled. Symptoms includedecreased central visual acuity, central scotoma,phosphenes and metamorphopsia. These chemicalsmay lead to bilateral vision loss and altered structureof the macula, specifically altered structure at theinner segment/outer segment (IS/OS) retinal junc-tion, as demonstrated on spectral-domain opticalcoherence tomography, and visible on funduscopyas a yellow spot at the fovea [27
&
,28] (Fig. 1). Themechanism of deleterious action on the retina isunclear, but may include nitric oxide toxicity[27
&
,28,29] (Table 1).One of the most devastating consequences of
intravenous drug abuse is the development ofendophthalmitis. Contaminated instruments ofdrug injection are often implicated in the injectionof offending organisms into the bloodstream, whichthen travel to the eye [30]. A variety of organismshas been demonstrated, most frequently Candida,
opyright © Lippincott Williams & Wilkins. Unautho
568 www.co-ophthalmology.com
Aspergillus, Bacillus, Staphylococcus and Pseudomonas,among many others [30].
Retinal vascular occlusive disease is known tooccur with many drugs of abuse, including cocaineand methamphetamine [31–33]. In addition, twocases of branch retinal vein occlusions in youngmen using anabolic steroids for enhanced muscledevelopment have been reported, with proposedetiologic factors of increased blood viscosity, abnor-mal vascular walls and hypertension [34]. In a study[35] comparing African-American patients who usedcocaine with those who did not use cocaine, inves-tigators found a wider retinal venular calibre andincreased arterial branching, and proposed that thismay reflect more generalized central nervous system(CNS) microvascular disease.
Age-related macular degeneration (ARMD) isassociated with alcohol and tobacco use. Smokinghas been found to be related to the incidence andprogression of ARMD in several population-basedstudies [36]. In addition, polymorphisms in severalgenetic loci, including complement factor H, havebeen found to contribute to the additional risk ofdeveloping ARMD in smokers [20]. Several studies,both cross-sectional and prospective, have examinedthe effects of alcohol on the development of ARMD,but with no definite consensus [1]. There is a possibleprotective effect of moderate alcohol consumption,and possible adverse effect of heavy alcohol con-sumption on the development of ARMD [16]. Ameta-analysis of published studies found that heavydrinking wasassociated with an increased risk of earlyARMD [37]. The Beijing Eye Study found no associ-ation of moderate alcohol consumption on the devel-opment of ARMD [38]. However, the MelbourneCollaborative Cohort Study found an increased riskof both early and late age-related ARMD in indivi-duals who consumed more than 20 g of alcohol perday [39].
Optic nerve
The use of alcohol during foetal development canhave the devastating consequential association ofcongenital abnormalities known as foetal alcoholsyndrome. Optic nerve hypoplasia, although not apart of the diagnosticcriteriadescribedbythe Centersfor Disease Control and Prevention in the USA, isfound in 61% of patients with foetal alcohol syn-drome [17]. Interestingly, a recent investigation ofchildren who were exposed to high levels of alcoholin utero in comparison with unexposed childrenrevealed no increase in risk of developing oculardefects. This study suggests that ophthalmic screen-ing should not be used to determine the presence offetal alcohol syndrome, but that children who meet
rized reproduction of this article is prohibited.
Volume 24 � Number 6 � November 2013

FIGURE 1. Poppers maculopathy. (a) Fundus photographs demonstrating bilateral foveal yellow spots. (b) Ocular coherencetomography of the macula demonstrating bilateral damage to the foveal photoreceptors. (c) Fundus autofluorescencephotographs demonstrating central hyperautofluorescence. Courtesy of Dr Catherine Vignal and Pr. Michel Paques, Paris, France.
Ocular manifestations of drug and alcohol abuse Peragallo et al.
the criteria for foetal alcohol syndrome should havesystematic eye examinations [40].
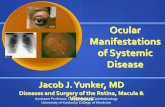
Methanol ingestion most often occurs due toaccidental consumption, and may induce a severeirreversible bilateral toxic optic neuropathy. Theoptic disc may become hyperemic with oedema,followed by pallor and cupping (Fig. 2). The insultappears to be demyelinating early and necrotic late.In a retrospective case series describing visual out-comes of methanol poisoning in which 37 patientswith visual disturbances at presentation were fol-lowed, 62% of patients had complete recovery, 14%had partial recovery, 14% had complete blindnessand 11% had initial partial recovery followed bydeterioration and complete blindness [41]. Treat-ments include ethanol (which competes with meth-anol metabolism) and haemodialysis.
Copyright © Lippincott Williams & Wilkins. Unau
1040-8738 � 2013 Wolters Kluwer Health | Lippincott Williams & Wilk
Visual-evoked potentials (VEPs) can be used tomeasure the integrity of the visual pathways, specifi-cally optic nerve function. A study in children whohad in-utero exposure to methadone and other drugsof abusehad abnormal VEPs in 60%, suggesting a veryhigh rate of optic nerve toxicity [42].
Several patients with Wernicke’s encephalop-athy (ataxia, ophthalmoplegia and confusion) havebeen reported with disc oedema and visual loss fromoptic neuropathies [43–46]. Li et al. [43] described apatient with Wernicke’s encephalopathy with opticneuropathies in whom they found a mitochondrialDNA mutation that causes Leber hereditary opticneuropathy (LHON). They propose that when thereis vision loss in cases of Wernicke’s encephalopathy,an underlying genetic predisposition for LHONshould be investigated.
thorized reproduction of this article is prohibited.
ins www.co-ophthalmology.com 569

C
Table 1. Commonly abused drugs and frequentophthalmic or visual manifestations
Drug Ocular/visual manifestation
Alcohol Dry eye
Foetal alcohol syndrome
Ocular trauma
Diplopia
Wernicke’s encephalopathy
Methanol Toxic optic neuropathy
Cocaine Corneal anaesthesia
Keratitis
Corneal ulceration
Mydriasis
Retinal emboli
Retinal venous occlusion
Orbital disease
Stroke
Hallucinations
Methamphetamine Keratitis
Corneal ulceration
Mydriasis
Retinal venous occlusion
Intraretinal haemorrhage
Talc retinopathy
Stroke
Hallucinations
Heroin/Methadone Talc retinopathy
Endophthalmitis
Miosis
Marijuana Conjunctival injection
Decreased intraocular pressure
Nystagmus
Hallucinations
LSD Mydriasis
Hallucinations
Palinopsia
Phencyclidine Decreased corneal reflex
Diplopia
Nystagmus
‘Bath salts’ Mydriasis
Alkyl nitrites Maculopathy
Barbiturates Ptosis
Diplopia
Nystagmus
LSD, lysergic acid diethylamide.
Ocular manifestations of systemic disease
The so-called ‘tobacco-alcohol amblyopia’, inwhich an optic neuropathy is attributed to the toxiceffects of combined tobacco and alcohol use, shouldbe eliminated from the medical lexicon [47]. This is
opyright © Lippincott Williams & Wilkins. Unautho
570 www.co-ophthalmology.com
not to say that tobacco does not contribute to theexacerbation of optic neuropathies. However, thecontribution of alcohol use to the development ofan optic neuropathy is likely due to malnutrition,and not the direct toxic effects of ethanol use. TheCuban optic neuropathy epidemic associated theuse of tobacco, especially cigars, and malnutrition,with vision loss from an optic neuropathy [48].Susceptible individuals who harbour the mitochon-drial DNA mutations associated with LHON shouldbe counselled to avoid smoking. Kirkman et al. [49]found that smoking significantly increased the riskof vision loss in patients harbouring mutations forLHON. Although not statistically significant, theseindividuals also had a trend towards visual loss withheavy alcohol intake [49].
OrbitIntranasal cocaine abuse can have devastating con-sequences for the orbit due to local ischemic damageleading to bony destruction, sometimes with pneu-mocele [50]. Intranasal cocaine abuse has led tosevere sinusitis extending into the orbit causingan optic neuropathy and orbital apex syndrome[51,52]. In one case of orbital cellulitis, superiorophthalmic vein thrombosis resulted from directintraorbital injection of heroin [53].
EYE MOVEMENTS (STRABISMUS,CRANIAL NEUROPATHIES ANDNYSTAGMUS)
Eye movement abnormalities may occur withnumerous drugs of abuse, including phencyclidine,lysergic acid diethylamide (LSD) and opioids [54].Cocaine may induce or exacerbate myastheniagravis [55]. Previous cases of acute esotropia follow-ing heroin withdrawal have been described [56].Heroin detoxification was found to lead to a trendtowards an esodeviation at distance in a prospectivestudy of patients undergoing detoxification [57].
Fetal alcohol syndrome is also associated withstrabismus, as well as with prolonged saccadic reac-tion times, saccadic direction errors and decreasedsaccadic velocity, suggestive of frontal lobe dysfunc-tion [17,58]. Strabismus is common with infantileexposure to other drugs of abuse as well, and hasbeen reported in 14% of infants of opiate-dependentmothers, more than 10 times that of the generalpopulation [59].
Severe malnutrition leading to thiaminedeficiency, seen in some chronic alcoholics andpostbariatric surgery patients, can lead to Wer-nicke’s encephalopathy. The classic clinical triadof Wernicke’s encephalopathy is ophthalmoplegia,ataxia and confusion, but this triad is rarely
rized reproduction of this article is prohibited.
Volume 24 � Number 6 � November 2013

FIGURE 2. Fundus photographs of a patient with bilateral optic neuropathies secondary to methanol ingestion. Photographsshow bilateral disc atrophy following disc oedema. The patient’s vision was light perception in each eye.
Ocular manifestations of drug and alcohol abuse Peragallo et al.
complete in patients with Wernicke’s. MRIfindings include symmetric T2 hyperintensitiesand contrast enhancement in the mammillarybodies, dorsal medial thalamic nuclei, tectal plateand periaqueductal grey areas (Fig. 3). Wernicke’sencephalopathy can lead to extraocular motilitydisturbances, including cranial nerve palsies, verti-cal gaze palsies and nystagmus [60].
The cranial nerves themselves are rarely affectedin isolation by substance abuse. A case of isolatedbilateral sixth nerve palsy presumed to be fromMDMA abuse was attributed to the interaction ofthe drug with serotonin receptors in the sixth nerves[61]. Sixth nerve palsy may accompany papilledemafollowing the intake of any drug that raises intra-cranial pressure, as seen, for example, in a case ofethylene glycol ingestion [62].
Copyright © Lippincott Williams & Wilkins. Unau
FIGURE 3. MRI findings in Wernicke syndrome. (a) FLAIR axialarea (arrow). (b) T2 coronal imaging demonstrating hyperintensit
1040-8738 � 2013 Wolters Kluwer Health | Lippincott Williams & Wilk
Nystagmus is common with many drugs ofabuse, including phencyclidine, opiates, marijuanaand barbiturates. In-utero exposure of the develop-ing foetus to benzodiazepines and opiates can leadto a fine horizontal pendular nystagmus. The nys-tagmus can be associated with the development of aneonatal abstinence syndrome that is severe enoughto require treatment [42,63].
CENTRAL NERVOUS SYSTEM
Hallucinations are often a desired effect of numer-ous drugs of abuse, such as LSD, psilocybin, alcohol,barbiturates, phencyclidine, MDMA and marijuana.So-called flashbacks, or recurrent hallucinations,can occur years, or even decades, following even asingle prior use of LSD [64–66]. An unusual side
thorized reproduction of this article is prohibited.
imaging demonstrating hyperintensity of periaqueductal greyy of periaqueductal grey area (arrow).
ins www.co-ophthalmology.com 571

C
FIGURE 4. Axial computed tomographic scan of the brainwithout contrast demonstrating a left empyema with lefthaemorrhagic parietal-occipital infarction. Underlying causewas an embolus in a patient with infectious endocarditisfrom intravenous heroin use. The brain lesion resulted in aright homonymous hemianopia.
Ocular manifestations of systemic disease
effect of LSD is palinopsia, prolonged or persistentafterimages [64].
Similar to the effects of sympathomimeticscausing vascular occlusive and haemorrhagic dis-ease within the eye, these substances can affectthe brain. Cocaine and methamphetamine use area classic cause of ischemic stroke, intracerebralhaemorrhage and subarachnoid haemorrhage[67,68]. Small vessel vasculopathy affecting theCNS can be induced by amphetamines [68]. There-fore, any young adult presenting with an acutehaemorrhagic or ischemic stroke should be screenedfor substance abuse. Cardiogenic emboli in patientswith a history of intravenous drug use may beinfectious (endocarditis) and result in strokes andassociated visual symptoms (Fig. 4).
Trauma
The use of alcohol and other substances of abuse isassociated with a higher risk of penetrating oculartrauma and traumatic brain injury. Rates of drug and
opyright © Lippincott Williams & Wilkins. Unautho
572 www.co-ophthalmology.com
alcohol use among open globe injury patients rangefrom 24 to 73% [69].
The production of illicit drugs, in addition tothe consumption, has proven hazardous to ocularhealth. A case series of four patients reported ther-mal and alkali burns from a ‘shake and bake’ meth-amphetamine laboratory explosion [70]. A caseseries from the University of Iowa described theocular thermal and alkali injuries suffered by eightpatients who presented to their burn care unit aftermethamphetamine production accidents [71].
CONCLUSION
Drugs of abuse are an increasing cause of morbidityand mortality within our society, despite efforts toeliminate them from distribution and use. Novelmaterials are being used in the drug abuser’s arsenalof self-inflicted damage, and we must be able torecognize the effects of these compounds on thevisual system. For patients with unusual presenta-tions, maintaining a high suspicion of drug abuseis prudent.
Acknowledgements
None.
Conflicts of interest
The authors report no conflicts of interest. This study wassupported in part by a departmental grant (Departmentof Ophthalmology) from Research to Prevent Blindness,Inc., New York, by core grant P30-EY06360 (Depart-ment of Ophthalmology). Dr Newman is a recipient ofthe Research to Prevent Blindness Lew R. WassermanMerit Award.
REFERENCES AND RECOMMENDEDREADINGPapers of particular interest, published within the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest1. Klein BE, Klein R. Lifestyle exposures and eye diseases in adults. Am JOphthalmol 2007; 144:961–969.
2. Moss SE, Klein R, Klein BEK. Prevalence of and risk factors for dry eyesyndrome. Arch Ophthalmol 2000; 118:1264–1268.
3.&
Kim JH, Kim JH, Nam WH, et al. Oral alcohol administration disturbs tear filmand ocular surface. Ophthalmology 2012; 119:965–971.
A case–control study of 35 heavy consumers of alcohol demonstrating altered tearfilm function and altered ocular surface structure compared with normal individuals.4. Cumurcu T, Gunduz A, Cumurcu BE, et al. The changes in tear film para-
meters and impression cytology in heavily drinking men. Cornea 2013;32:237–241.
5. McLane NJ, Carroll DM. Ocular manifestations of drug abuse. Surv Ophthal-mol 1986; 30:298–313.
6. Alipour F, Hashemi H, Pirim N, Asghari H. Ocular manifestations of trans-conjunctival heroin abuse: a case report of an unusual route of substanceabuse. Cornea 2010; 29:110–112.
7. Poulsen EJ, Mannis MJ, Chang SD. Keratitis in methamphetamine abusers.Cornea 1996; 15:477–482.
8. Ghosheh FR, Ehlers JP, Ayres BD, et al. Corneal ulcers associated withaerosolized crack cocaine use. Cornea 2007; 26:966–969.
rized reproduction of this article is prohibited.
Volume 24 � Number 6 � November 2013

Ocular manifestations of drug and alcohol abuse Peragallo et al.
9. Yagci A, Bozkurt B, Egrilmez S, et al. Topical anesthetic abuse keratopathy: acommonly overlooked healthcare problem. Cornea 2011; 30:571–575.
10. Ansari H, Garibaldi DC, Jun AS. Anaesthetic abuse keratopathy as a manifesta-tion of ocular Munchausen’s syndrome. Clin Exp Ophthalmol 2006; 34:81–92.
11. Hendershot AJ, Colling L, Mauger TF. Corneal anesthetic abuse from the useof topical benzonatate (Tessalon Perle). Cornea 2011; 30:1518–1519.
12. Warrick BJ, Hill M, Hekman K, et al. A 9-state analysis of designer stimulant,‘bath salt,’ hospital visits reported to poison control centers. Ann Emerg Med2013. [Epub ahead of print]
13. Zhan G, Camras CB, Palmberg PF. Effects of marijuana on aqueous humordynamics in a glaucoma patient. J Glaucoma 2005; 14:175–177.
14. Jampel H. American Glaucoma Society position statement: marijuana and thetreatment of glaucoma. J Glaucoma 2010; 19:75–76.
15. Trittibach P, Frueh BE, Goldblum D. Bilateral angle-closure glaucoma aftercombined consumption of ‘ecstasy’ and marijuana. Am J Emerg Med 2005;23:813–814.
16. Wang S, Wang JJ, Wong TY. Alcohol and eye diseases. Surv Ophthalmol2008; 53:512–525.
17. Bruce BB, Dean AL, Newman NJ, Biousse V. Neurologic and ophthalmicmanifestations of fetal alcohol syndrome. Rev Neurol Dis 2009; 6:13–20.
18. Clarke ME, Schloff S, Bothun ED. Triangular congenital cataract morphologyassociated with prenatal methamphetamine exposure. J AAPOS 2009;13:408–409.
19. Klein BE, Klein R, Linton KL, et al. Cigarette smoking and lens opacities: theBeaver Dam Eye Study. Am J Prev Med 1993; 9:27–30.
20. Galor A, Lee DJ. Effects of smoking on ocular health. Curr Opin Ophthalmol2011; 22:477–482.
21. Atlee WE. Talc and cornstarch emboli in eyes of drug abusers. JAMA 1972;219:49–51.
22. Kim RW, Juzych MS, Eliott D. Ocular manifestations of injection drug use.Infect Dis Clin N Am 2002; 16:607–622.
23. Zoumalan CI, Marmor MF. Revisiting talc retinopathy. Arch Ophthalmol 2007;125:988.
24. Shah VA, Cassell M, Poulouse A, et al. Talc retinopathy. Ophthalmology2008; 115:755–755; e2.
25. Kumar RL, Kaiser PK, Lee MS. Crystalline retinopathy from nasal ingestion ofmethamphetamine. Retina 2005; 26:823–824.
26. Ascaso FJ, Cruz N, Del Buey MA, Cristobal JA. An unusual case of cocaine-induced maculopathy. Eur J Ophthalmol 2009; 19:880–882.
27.&
Davies AJ, Kelly SP, Naylor SG, et al. Adverse ophthalmic reaction in poppersusers: case series of ‘poppers maculopathy’. Eye 2012; 26:1479–1486.
A case series of seven patients with maculopathy following poppers use ispresented. In this study, it is stressed that thorough investigation of drug usehistory with foveal damage is necessary.28. Vignal-Clermont C, Audo I, Sahel JA, Paques M. Poppers-associated retinal
toxicity. N Engl J Med 2010; 363:1583–1584.29. Audo I, Sanharawi ME, Vignal-Clermont C, et al. Foveal damage in habitual
poppers users. Arch Ophthalmol 2011; 129:703–708.30. Kim RW, Juzych SM, Eliott D. Ocular manifestations of injection drug use.
Infect Dis Clin N Am 2002; 16:607–622.31. Hazin R, Cadet JL, Kahook MY, Saed D. Ocular manifestations of crystal
methamphetamine use. Neurotox Res 2009; 15:187–191.32. Kannan B, Balaji V, Kummararaj S, Govindarajan K. Cilioretinal artery occlu-
sion following intranasal cocaine insufflations. Indian J Ophthalmol 2011;59:388–389.
33. Rahman W, Thomas S, Wiselka M, Bibby K. Cocaine-induced chorioretinalinfarction. Br J Ophthalmol 2008; 92:150–151.
34. Damasceno EF, Neto AM, Damasceno NAP, et al. Branch retinal veinocclusion and anabolic steroids abuse in young bodybuilders. Acta Ophthal-mol 2009; 87:580–581.
35. Leung IY, Lai S, Ren S, et al. Early retinal vascular abnormalities in African-American cocaine users. Am J Ophthalmol 2008; 146:612–619.
36. Cong R, Zhou B, Sun Q, et al. Smoking and risk of age-related maculardegeneration: a meta-analysis. Ann Epidemiol 2008; 18:647–656.
37. Chong EW, Kreis AJ, Wong TY, et al. Alcohol consumption and the risk of age-related macular degeneration: a systematic review and meta-analysis. Am JOphthalmol 2008; 145:707–715.
38. Xu L, You QS, Jonas JB. Prevalence of alcohol consumption and risk of oculardiseases in a general population: the Beijing Eye Study. Ophthalmology2009; 116:1872–1879.
39. Adams MK, Chong EW, Williamson E, et al. 20/20: alcohol and age-relatedmacular degeneration: the Melbourne Collaborative Cohort Study. Am JEpidemiol 2012; 176:289–298.
40. Flanigan EY, Aros S, Bueno MF, et al. Eye malformations in children with heavyalcohol exposure in utero. J Pediatr 2008; 153:391–395.
Copyright © Lippincott Williams & Wilkins. Unau
1040-8738 � 2013 Wolters Kluwer Health | Lippincott Williams & Wilk
41. Sanaei-Zadeh H, Zamani N, Shadnia S. Outcomes of visual disturbances aftermethanol poisoning. Clin Toxicol 2011; 49:102–107.
42. Hamilton R, McGlone L, MacKinnon JR, et al. Ophthalmic, clinical andvisual electrophysiological findings in children born to mothers prescribedsubstitute methadone in pregnancy. Br J Ophthalmol 2010; 94:696–700.
43. Li JM, Rucker JC. Irreversible optic neuropathy in Wernicke encephalopathyand Leber hereditary optic neuropathy. J Neuro-ophthalmol 2010; 30:49–53.
44. Kulkarni S, Lee AG, Holstein SA, Warner JE. You are what you eat. SurvOphthalmol 2005; 50:389–393.
45. Longmuir R, Lee AG, Rouleau J. Visual loss due to Wernicke syndromefollowing gastric bypass. Semin Ophthalmol 2007; 22:13–19.
46. Cooke CA, Hicks E, Page AB, et al. An atypical presentation ofWernicke’s encephalopathy in an 11-year-old child. Eye 2006; 20:1418–1420.
47. Phillips PH. Toxic and deficiency optic neuropathies. In: Miller NR, NewmanNJ, editors. Clinical neuro-ophthalmology, 6th ed. Philadelphia, PA: LippincottWilliams & Wilkins; 2005. pp. 458–459.
48. The Cuba Neuropathy Field Investigation Team. Epidemic optic neuropathy inCuba: clinical characterization and risk factors. N Engl J Med 1995;333:1176–1182.
49. Kirkman MA, Yu-Wai-Man P, Korsten A, et al. Gene-environment interactionsin Leber hereditary optic neuropathy. Brain 2009; 132:2317–2326.
50. Ayala C, Watkins L, Deschler DG. Tension orbital pneumocele secondary tonasal obstruction from cocaine abuse: a case report. Otolaryngol Head NeckSurg 2002; 127:572–574.
51. Leibovitch I, Khoramian D, Goldberg RA. Severe destructive sinusitis andorbital apex syndrome as a complication of intranasal cocaine abuse. Am JEmerg Med 2006; 24:499–501.
52. Shen CC, Silver AL, O’Donnell TJ, et al. Optic neuropathy caused by naso-orbital mass in chronic intranasal cocaine abuse. J Neuro-ophthalmol 2009;29:50–53.
53. Ghosheh FR, Kathuria SS. Intraorbital heroin injection resulting in orbitalcellulitis and superior ophthalmic vein thrombosis. Ophthal Plast ReconstrSurg 2006; 22:473–475.
54. Firth A. Ocular effects of criminal drug use. Can J Ophthalmol 2006; 41:140–143.
55. Valmaggia C, Gottlob I. Cocaine abuse, generalized myasthenia, completeexternal ophthalmoplegia, and pseudotonic pupil. Strabismus 2001; 9:9–12.
56. Firth AY. Heroin and diplopia. Addiction 2005; 100:46–50.57. Firth AY, Pulling S, Carr MP, Beaini AY. Orthoptic status before and
immediately after heroin detoxification. Br J Ophthalmol 2004; 88:1186–1190.
58. Green CR, Munoz DP, Nikkel SM, Reynolds JN. Deficits in eye movementcontrol in children with fetal alcohol spectrum disorders. Alcohol Clin Exp Res2007; 31:500–511.
59. Gill AC, Oei J, Lewis NL, et al. Strabismus in infants of opiate-dependentmothers. Acta Paediatr 2003; 92:379–385.
60. Kumar N. Acute and subacute encephalopathies: deficiency states(nutritional). Semin Neurol 2011; 31:169–183.
61. Schroeder B, Brieden S. Bilateral sixth nerve palsy associated with MDMA(’Ecstasy’) abuse. Am J Ophthalmol 2000; 129:408–409.
62. Delany C, Jay WM. Papilledema and abducens nerve palsy following ethyleneglycol ingestion. Semin Ophthalmol 2004; 19:72–74.
63. Mulvihill AO, Cackett PD, George ND, Fleck BW. Nystagmus secondary todrug exposure in utero. Br J Ophthalmol 2007; 91:613–615.
64. Sunness JS. Persistent afterimages (palinopsia) and photophobia in a patientwith a history of LSD use. Retina 2004; 24:805.
65. Kawasaki A, Purvin V. Persistent palinopsia following ingestion of lysergic aciddiethylamide (LSD). Arch Ophthalmol 1996; 114:47–50.
66. Levi L, Miller NR. Visual illusions associated with previous drug abuse. J ClinNeuro-ophthalmol 1990; 10:103–110.
67. Toossi S, Hess CP, Hills NK, Josephson SA. Neurovascular complications ofcocaine use and a tertiary stroke center. J Stroke Cerebrovasc Dis 2010;19:273–278.
68. Ho EL, Josephson SA, Lee HS, Smith WS. Cerebrovascular complications ofmethamphetamine abuse. Neurocrit Care 2009; 10:295–305.
69. Rahman I, Maino A, Devadason D, Leatherbarrow B. Open globe injuries:factors predictive of poor outcome. Eye 2006; 20:1336–1341.
70. Chan AY, Storck SA, Stone DU. Ocular injuries from shake and bakemethamphetamine labs. J Okla State Med Assoc 2011; 104:409–412.
71. Charukamnoetkanok P, Wagoner MD. Facial and ocular injuries associatedwith methamphetamine production accidents. Am J Ophthalmol 2004;138:875–876.
thorized reproduction of this article is prohibited.
ins www.co-ophthalmology.com 573


![Ocular Manifestations of Biopsy-Proven Pulmonary ...downloads.hindawi.com/journals/joph/2018/9308414.pdf · ocular sarcoidosis [2–4]. Ocular sarcoidosis can occur with-out apparent](https://static.fdocuments.in/doc/165x107/60094e678ad2796c001b27fc/ocular-manifestations-of-biopsy-proven-pulmonary-ocular-sarcoidosis-2a4.jpg)