COPINION Body composition phenotypes and obesity paradox · PINION Body composition phenotypes and...
17
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved. C URRENT O PINION Body composition phenotypes and obesity paradox Carla M. Prado a , M. Cristina Gonzalez b , and Steven B. Heymsfield c Purpose of review The obesity paradox is a highly controversial concept that may be attributed to methodological limitations related to its identification. One of the primary concerns is the use of BMI to define obesity. This index does not differentiate lean versus adipose tissue compartments (i.e. body composition) confounding health consequences for morbidity and mortality, especially in clinical populations. This review will describe the past year’s evidence on the obesity paradox phenomenon, primarily focusing on the role of abnormal body composition phenotypes in explaining the controversies observed in the literature. Recent findings In spite of the substantial number of articles investigating the obesity paradox phenomenon, less than 10% used a direct measure of body composition and when included, it was not fully explored (only adipose tissue compartment evaluated). When lean tissue or muscle mass is taken into account, the general finding is that a high BMI has no protective effect in the presence of low muscle mass and that it is the latter that associates with poor prognosis. Summary In view of the body composition variability of patients with identical BMI, it is unreasonable to rely solely on this index to identify obesity. The consequences of a potential insubstantial obesity paradox are mixed messages related to patient-related prognostication. Keywords body composition, body composition phenotypes, obesity paradox, sarcopenia, sarcopenic obesity INTRODUCTION Obesity is a widespread public health problem afflicting many countries around the world. Although obesity conveys a clear unfavourable prog- nosis for morbidity and mortality in the general population, this association seems blunted in some chronic conditions with obese individuals present- ing with a survival advantage over their counter- parts, a phenomenon termed the ‘obesity paradox’ or ‘reverse epidemiology’. The obesity paradox is a controversial concept that can be attributed to methodological limitations of the studies wherein it has been observed. One of the criticisms is the use of anthropometrics estimates such as BMI to define obesity. Body weight and BMI do not depict the different proportions of lean versus adipose tissues (i.e. body composition), con- founding health consequences for morbidity and mortality, especially in clinical scenarios [1 & ]. This review will describe the past year’s evidence on the obesity paradox phenomenon, primarily focusing on the role of abnormal body composition pheno- types in explaining the controversies observed in the literature. OBESITY PARADOX: OPPOSING STATES OF KNOWLEDGE The obesity paradox has been reported in patients with different types of cardiovascular disease, dia- betes, cancer, renal disease, chronic obstructive pulmonary disease (COPD) and in older age [2]. In these studies, survival advantages are reported in those with increased BMI (obese compared to nor- mal weight patients), contradicting the sharp increase in mortality with a more than 30 kg/m 2 BMI observed in the general population. a Department of Agricultural, Food and Nutritional Science, University of AB, Edmonton, Alberta, Canada, b Post Graduate Program in Health and Behavior, Catholic University of Pelotas, Pelotas, RS, Brazil and c Pennington Biomedical Research Center, Baton Rouge, Los Angeles, USA Correspondence to Carla M. Prado, PhD, Alberta Institute for Human Nutrition, Department of Agricultural, Food and Nutritional Science, University of Alberta, 4-002 Li Ka Shing Centre, Edmonton, AB T6G 2P5, Canada. E-mail: [email protected] Curr Opin Clin Nutr Metab Care 2015, 18:535–551 DOI:10.1097/MCO.0000000000000216 1363-1950 Copyright ß 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-clinicalnutrition.com REVIEW
Transcript of COPINION Body composition phenotypes and obesity paradox · PINION Body composition phenotypes and...

REVIEW
CURRENTOPINION Body composition phenotypes and obesity paradox
Copyrig
1363-1950 Copyright � 2015 Wolte
a b c
Carla M. Prado , M. Cristina Gonzalez , and Steven B. HeymsfieldPurpose of review
The obesity paradox is a highly controversial concept that may be attributed to methodological limitationsrelated to its identification. One of the primary concerns is the use of BMI to define obesity. This indexdoes not differentiate lean versus adipose tissue compartments (i.e. body composition) confounding healthconsequences for morbidity and mortality, especially in clinical populations. This review will describe thepast year’s evidence on the obesity paradox phenomenon, primarily focusing on the role of abnormalbody composition phenotypes in explaining the controversies observed in the literature.
Recent findings
In spite of the substantial number of articles investigating the obesity paradox phenomenon, less than 10%used a direct measure of body composition and when included, it was not fully explored (only adiposetissue compartment evaluated). When lean tissue or muscle mass is taken into account, the general findingis that a high BMI has no protective effect in the presence of low muscle mass and that it is the latter thatassociates with poor prognosis.
Summary
In view of the body composition variability of patients with identical BMI, it is unreasonable to rely solelyon this index to identify obesity. The consequences of a potential insubstantial obesity paradox are mixedmessages related to patient-related prognostication.
Keywords
body composition, body composition phenotypes, obesity paradox, sarcopenia, sarcopenic obesity
aDepartment of Agricultural, Food and Nutritional Science, University ofAB, Edmonton, Alberta, Canada, bPost Graduate Program in Health andBehavior, Catholic University of Pelotas, Pelotas, RS, Brazil andcPennington Biomedical Research Center, Baton Rouge, Los Angeles,USA
Correspondence to Carla M. Prado, PhD, Alberta Institute for HumanNutrition, Department of Agricultural, Food and Nutritional Science,University of Alberta, 4-002 Li Ka Shing Centre, Edmonton, AB T6G2P5, Canada. E-mail: [email protected]
Curr Opin Clin Nutr Metab Care 2015, 18:535–551
DOI:10.1097/MCO.0000000000000216
INTRODUCTION
Obesity is a widespread public health problemafflicting many countries around the world.Although obesity conveys a clear unfavourable prog-nosis for morbidity and mortality in the generalpopulation, this association seems blunted in somechronic conditions with obese individuals present-ing with a survival advantage over their counter-parts, a phenomenon termed the ‘obesity paradox’or ‘reverse epidemiology’.
The obesity paradox is a controversial conceptthat can be attributed to methodological limitationsof the studies wherein it has been observed. One ofthe criticisms is the use of anthropometrics estimatessuch as BMI to define obesity. Body weight andBMI do not depict the different proportions of leanversus adipose tissues (i.e. body composition), con-founding health consequences for morbidity andmortality, especially in clinical scenarios [1
&
]. Thisreview will describe the past year’s evidence on theobesity paradox phenomenon, primarily focusingon the role of abnormal body composition pheno-types in explaining the controversies observed inthe literature.
ht © 2015 Wolters Kluwe
rs Kluwer Health, Inc. All rights rese
OBESITY PARADOX: OPPOSING STATESOF KNOWLEDGE
The obesity paradox has been reported in patientswith different types of cardiovascular disease, dia-betes, cancer, renal disease, chronic obstructivepulmonary disease (COPD) and in older age [2]. Inthese studies, survival advantages are reported inthose with increased BMI (obese compared to nor-mal weight patients), contradicting the sharpincrease in mortality with a more than 30 kg/m2
BMI observed in the general population.
r Health, Inc. All rights reserved.
rved. www.co-clinicalnutrition.com

KEY POINTS
� Obesity paradox is a topic of intense interest yet withnotably contradictory findings.
� Shortcomings associated with these contradictoryfindings may be explained by the inadequacy of BMIas an obesity classifier.
� Variability in body composition phenotypes (i.e.adipose versus muscle tissues) of contemporarypopulation indicates different nutritional status even inindividuals with identical BMI.
� The use of body composition analysis indicates thatexcess adipose tissue has no protective effect in thepresence of low muscle mass.
Nutrition and physiological function
Prolonged survival with increased BMI may beexplained by a variety of factors such as these indi-viduals receiving higher rates of optimal medicalattention/treatment. The availability of energyreserves during acute catabolic illness is alsoanother plausible explanation leading to survivalbias, index event bias or reverse causation [3]. Theprotective effect of anti-inflammatory cytokines oradipokines, including soluble tumour necrosis fac-tor-alpha receptors and lipopolysaccharides, is alsohypothesized to neutralize the inflammatorymilieu of catabolic diseases [3]. Higher BMI mayalso be related to protective factors such asyounger age.
Nonetheless, several shortcomings should beconsidered when interpreting studies reportingthe obesity paradox. These include:
(1)
FIGU
fat m
536
use of incorrect reference values (lower overallBMI reference ranges) [4];
Copyright © 2015 Wolters Kluwer
Obese with nlean ma
Obese with low lean mass
RE 1. Illustration scheme of potential differences in body cass and black represents lean mass).
www.co-clinicalnutrition.com
(2)
Hea
ormal ss
omp
collider stratification bias, a type of selectionbias wherein the conditioning on a variableaffected by exposure shares common causeswith the outcome producing a spurious protec-tive prognostic effect of obesity [5];
(3)
observational and cross-sectional study designs;and(4)
inadequacy of BMI as an obesity classifier.As discussed by Heymsfield and Cefalu [6], theuse of BMI as a health risk phenotype has severallimitations. BMI accounts for about two-thirds ofthe between-individual variability in total adiposity.In spite of the high correlation of BMI with adi-posity, a two to three-fold variation in visceral adi-posity is observed at any given BMI, illustrating howBMI is not a specific index of abnormal fat accumu-lation. Therefore, among equally overweight indi-viduals, differences in overall quantity anddistribution of adipose tissue, muscularity, nutri-tional status disease risk factors (disease severityand comorbidities), age, race and sex may explainthe greater risk for shorter survival [4,6].
Of our particular interest, and the focus of thisreview, is the use of BMI to diagnose obesity in viewof the variability in body composition phenotypesof the contemporary population. As we will discussnext, BMI does not accurately depict different com-ponents of body composition and is thereforeunable to predict the prognostic effect of individualtissues, Fig. 1.
BODY COMPOSITION PHENOYPES:DEMYSTIFYING THE OBESITY PARADOX?
Higher BMI is generally found to be associated withgreater muscle mass and strength. This is because fat
lth, Inc. All rights reserved.
Obese with high lean mass
osition in individuals with identical BMI (grey represents
Volume 18 � Number 6 � November 2015

Body composition phenotypes and obesity paradox Prado et al.
and lean masses are expected to grow in harmonywith each other. Although this may be true for themajority of individuals, the assessment of in-vivobody composition has highlighted that this is not aubiquitous phenomenon. High body weight (henceBMI) and fat mass can coexist with obesity, a syn-drome known as ‘sarcopenic obesity’. In fact, theconcurrent appearance of low muscle and high adi-pose tissue can occur at any given BMI across the agespectrum [7,8]. We used North-American popu-lation-cohort data to illustrate the variability inbody composition phenotypes at different agesand across the BMI categories. With our proposedclassification criteria to define abnormal body com-position, we reported that normal-weight individ-uals could present with diverse body compositionphenotypes such as high adiposity–high muscular-ity, low adiposity–low muscularity or even highadiposity–low muscularity (i.e. analogous to sarco-penic obesity). Each of these phenotypes is likely tobe associated with diverse nutritional status.
Oreopoulos et al. [9] reported that BMI misclas-sified 41% of body fat status in patients with chronicheart failure. A higher muscularity and/or loweradiposity were independently associated withadvantageous prognostic factors in these patients.Similar findings were more recently confirmed inpatients with cancer: those with excess fat mass weremisclassified as overweight or even normal weightaccording to BMI criteria [10
&
]. Such misclassifi-cation may explain the controversial results of theobesity paradox reported in studies using BMI as aclassification criterion for obesity. These findingshighlight the need for further studies investigatingthe obesity paradox phenomenon in the context ofbody composition assessment.
THE PAST YEAR EVIDENCE AT A GLANCE
The obesity paradox may certainly be considered atopic of high interest in the scientific communitywith a total of 71 published articles in the past yearalone. Within this time frame, we found 25 reviewarticles, four meta-analyses and 42 original articlesdiscussing this phenomenon. Out of the originalarticles (N¼42), 31 used only BMI to classifyobesity, whereas seven used a surrogate assessmentof body composition (e.g. waist or hip circumfer-ence, skinfold thickness) and four used a directassessment of body composition.
Studies using BMI as the sole indicator ofobesity
Table 1 depicts a summary of the studies in whichonly BMI was used to define obesity [3,5,11–39].
Copyright © 2015 Wolters Kluwe
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
Patient cohorts included various forms of cardio-vascular diseases, investigated in the majority of thestudies (N¼21/31). Other patient cohorts includedthose with rheumatoid arthritis, peptic ulcer, per-itonitis and sepsis, diabetes mellitus type 2, demen-tia, COPD, lung resection, mechanical ventilationand a cohort of nondiseased individuals.
Table 1 summarizes that the obesity paradox(higher BMI associated with better prognosis) wasreported in 13 out of 31 studies. Out of these, twostudies observed this association in overweight butnot obese individuals [14,18]; one observed it inmen but not women [27]; one in short but notlong-term outcomes (mortality rate) [34], and onein some outcomes (myocardial infarction and sep-ticemia) but not survival [26]. Mixed findings werereported in two studies when patients were stratifiedby ventilated versus nonventilated group (only theformer showing obesity paradox) [30] and low ver-sus high cardiorespiratory fitness [13], with only theformer showing the paradox. The remaining (andmajority) of the studies failed to demonstrate aprognostic advantage to having excess body weight(Table 1).
The four meta-analyses reported the following:Sharma et al. [40] investigated the relationship ofBMI with all-cause and cardiovascular mortality andhospitalization in six studies of patients with chronicheart failure. The authors concluded that risk forcardiovascular mortality and incidence of hospital-ization was lowest in overweight patients but foundno differences in all-cause mortality. Severe obesitywas associated with poor overall cardiovascular out-comes, suggesting that apparent effect of adipositydoes not occur at the extreme levels of obesity. In aseparate meta-analysis of 36 studies, the same groupinvestigated the obesity paradox after coronary arterydisease revascularization procedures [41]. Whenlooking at total mortality, cardiovascular mortalityand myocardial infarction, only cardiovascularmortality was found to be lower in overweightpatients. In both studies, detailed data on cardio-vascular risk factors, severity/stage of disease or unin-tentional weight loss were not available, which doesnot rule out the possibility of residual confoundingeffects in the reported results.
Niedziela et al. [42] reported the relationshipbetween BMI and total mortality in 26 studies ofpatients after acute coronary syndrome. The authorsconcluded that overweight, obese and severelyobese patients presented with lower mortality thanthose with normal BMI. The authors noted thatalthough obesity was associated with comorbidities,these patients were younger and had less bleedingcomplications, which could have influencedsurvival.
r Health, Inc. All rights reserved.
rved. www.co-clinicalnutrition.com 537

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le1
.Su
mm
ary
ofst
udie
spu
blis
hed
inth
epa
stye
arin
whi
chon
lyBM
Iwas
used
tode
fine
obes
ity
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
of
ob
esit
yp
ara
do
x(D
efin
itio
n)O
bes
ity
pa
ra-
do
xre
po
rted
?Fi
ndin
gs
Bake
ret
al.
[11]
Toin
vest
igat
ew
heth
erw
eight
loss
mig
htex
plai
nth
eob
esity
para
dox
inpa
tient
sw
ithrh
eum
atoi
dar
thritis
Patie
nts
with
rheu
mat
oid
arth
ritis
N¼
1674
4BM
Icat
egor
ies:
unde
rwei
ght
<20
kg/m
2;
norm
alw
eight
�20
–25
kg/m
2;
over
wei
ght
�25
–30
kg/m
2;
obes
e�
30
kg/m
2
No
Wei
ght
loss
atan
annu
aliz
edra
teof�
3kg
/m2
was
asso
ciat
edw
ithth
egre
ates
trisk
ofde
ath
The
resu
ltsdi
dno
tsup
port
abi
olog
ical
lypr
otec
tive
role
ofob
esity
onm
orta
lity
risk
Bana
cket
al.
[5]
Tode
mon
stra
teth
atth
eob
esity
para
dox
may
beex
plai
ned
byco
llide
rst
ratif
icat
ion
bias
and
toes
timat
eth
ebi
asin
gef
fect
sof
unm
easu
red
com
mon
caus
esof
CV
Dan
dm
orta
lity
Parti
cipa
nts
inth
eN
HA
NES
III(1
988
–1994)w
hore
porte
dha
ving
CV
D
N¼
16
001
Obe
se:
BMI>
30
kg/m
2;
nono
bese
BMI1
8.5
–29.9
kg/m
2
Yes
The
adju
sted
tota
leffe
ctes
timat
ede
mon
stra
ted
anin
crea
sed
num
ber
ofde
aths
amon
gob
ese
indi
vidu
als
rela
tive
tono
nobe
seco
unte
rpar
ts,
butt
heco
ntro
lled
dire
ctef
fect
show
eda
para
doxi
cal
decr
ease
inm
orta
lity
amon
gob
ese
indi
vidu
als
with
CV
DTh
em
edia
tor–
outc
ome
rela
tions
hip
expl
ains
the
obse
rved
prot
ectiv
eef
fect
ofob
esity
onm
orta
lity.
The
auth
ors
conc
lude
dth
atse
lect
ion
bias
can
mak
ean
appa
rent
lyha
rmfu
lre
latio
nshi
pap
pear
prot
ectiv
e
Buck
and
Møl
ler
[12]
Toex
amin
eth
eas
soci
atio
nbe
twee
nBM
Iand
mor
talit
y
Patie
nts
treat
edsu
rgic
ally
for
perfor
ated
pept
icul
cer
N¼
1699
BMIa
ccor
ding
toW
HO
crite
ria
with
post
hoc
anal
ysis
usin
gfe
wer
gro
ups
No
Bein
gov
erw
eight
orob
ese
had
noef
fect
onm
orta
lity
Cla
rket
al.
[3]
Toco
mpa
reth
eef
fect
ofob
esity
and
rela
ted
risk
fact
ors
on10-y
ear
mor
talit
y
70
orol
der
Afric
ande
scen
tliv
ing
inth
eU
nite
dSt
ates
and
Nig
eria
N¼
2466
BMIa
ccor
ding
toW
HO
crite
ria
No
No
mor
talit
yad
vant
age
was
obse
rved
for
the
over
wei
ght
orob
ese
Nutrition and physiological function
538 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Cla
rket
al.
[13]
Toev
alua
teth
ere
latio
nshi
pbe
twee
nBM
Icat
egor
ies,
CRF
defin
edby
PKV
O2
and
clin
ical
outc
omes
inad
vanc
edsy
stol
icH
F
Patie
nts
with
adva
nced
syst
olic
HF
refe
rred
tohe
artt
rans
plan
tatio
nfo
llow
edun
tilde
ath,
urgen
tsta
tus
1A
hear
ttra
nspl
anto
rve
ntricu
lar
assi
stde
vice
1675
patie
nts,
pros
pect
ive
coho
rt,2
year
sfo
llow
-up
3su
bgro
ups
acco
rdin
gto
BMI:
norm
al(1
8.5
–24.9
kg/m
2);
over
wei
ght
(25
–29.9
kg/m
2)an
dob
ese
(�30
kg/m
2)
Hig
hle
veli
fPK
VO
2
>14
ml/
kg/m
in
Mix
edfin
ding
sO
besi
typa
rado
xw
asco
nfirm
edju
stin
the
low
erC
RFle
vel.
Ther
ew
asno
asso
ciat
ion
with
obes
ityan
dbe
tter
surv
ival
inpa
tient
sw
ithhi
ghe
rC
RF,
indi
catin
gth
atim
prov
edfu
nctio
nal
capa
city
may
atte
nuat
eth
eob
esity
para
dox
Cos
tanz
oet
al.
[14]
Toin
vest
igat
eth
eas
soci
atio
nbe
twee
nBW
and
prog
nosi
s
Patie
nts
with
T2D
N¼
10
568
BMIa
ccor
ding
toW
HO
crite
ria
Yes
(ove
rwei
ght
gro
upon
ly)
Bein
gov
erw
eight
was
asso
ciat
edw
itha
low
erm
orta
lity
risk
,bu
tbei
ngob
ese
was
not
Ove
rwei
ght
and
obes
ew
ere
mor
elik
ely
tobe
hosp
italiz
edfo
rca
rdio
vasc
ular
reas
ons
Deh
lend
orff
etal
.[1
5]
Toin
vest
igat
ew
heth
erth
eob
esity
para
dox
inst
roke
patie
nts
isva
lidor
anar
tific
ialf
indi
ngs
due
tose
lect
ion
bias
All
patie
nts
adm
itted
toa
hosp
italf
orst
roke
inD
enm
ark
N¼
53
812
BMIa
ccor
ding
toW
HO
crite
ria
No
BMIw
asin
vers
ely
rela
ted
tom
ean
age
atst
roke
onse
tTh
ere
wer
eno
diffe
renc
esin
the
risk
ofde
ath
byst
roke
inth
efir
stw
eek
orm
onth
afte
rth
est
roke
amon
gBM
Igro
ups
Dile
ttiet
al.
[16]
Toin
vest
igat
eth
eim
pact
ofBM
Ion
long
-term
clin
ical
outc
omes
afte
rim
plan
tatio
nof
zota
rolim
usel
utin
gst
ents
inpa
tient
sw
ithC
VD
Patie
nts
treat
edfo
rC
VD
N¼
5127
BMIt
ertil
es1,
low
orno
rmal
wei
ght
:�
25.9
5kg
/m2;
2,
over
wei
ght
:>
25.9
5–
29.7
4kg
/m2;
3,
obes
e>
29.7
4kg
/m2
No
Att
he2-y
ear
follo
w-u
p,th
ere
wer
eno
diffe
renc
esbe
twee
npa
tient
sin
BMI
terti
le1
com
pare
dw
ith3
inte
rms
ofta
rget
lesi
onfa
ilure
,m
ajor
card
iac
even
ts,
card
iac
deat
h,m
yoca
rdia
lin
farc
tion,
lesi
onre
vasc
ular
izat
ion
orpr
obab
lest
entt
hrom
bosi
s
(Con
tinue
d)
Body composition phenotypes and obesity paradox Prado et al.
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-clinicalnutrition.com 539

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le1
(Con
tinue
d)
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
of
ob
esit
yp
ara
do
x(D
efin
itio
n)O
bes
ity
pa
ra-
do
xre
po
rted
?Fi
ndin
gs
Farr
eet
al.
[17]
Toev
alua
teth
ehy
poth
esis
that
patie
nts
with
chro
nic
HF
and
obes
ityha
veat
tenu
ated
neur
ohor
mon
alac
tivat
ion
Chi
nese
patie
nts
with
chro
nic
HF
N¼
742
4BM
Icat
egor
ies:
unde
rwei
ght
<20
kg/m
2;
norm
alw
eight
20
–25
kg/m
2;
over
wei
ght
25
–30
kg/m
2;
obes
e>
30
kg/m
2
No
Hig
her
BMIa
ndob
esity
wer
eas
soci
ated
with
low
erno
repi
neph
rine
leve
lsin
mul
tiple
linea
rre
gre
ssio
n;no
repi
neph
rine
atte
nuat
edth
epr
ogno
stic
impa
ctof
BMI
Nor
epin
ephr
ine
was
anin
depe
nden
tpre
dict
oror
wor
seou
tcom
esin
both
obes
ean
dno
nobe
segro
ups.
No
asso
ciat
ion
betw
een
BMIa
ndm
orta
lity
wer
efo
und,
whe
nle
vels
ofth
isho
rmon
ew
asta
ken
into
acco
unt
Gar
cia-
Ptac
eket
al.
[18]
Toin
vest
igat
eth
eas
soci
atio
nbe
twee
nBM
Ian
dm
orta
lity
risk
Patie
nts
with
dem
entia
,at
the
time
ofde
men
tiadi
agno
sis
N¼
11
398
BMIa
ccor
ding
toW
HO
crite
ria
and
addi
tiona
lcut
off
with
inno
rmal
rang
e(’sl
imin
divi
dual
s,BM
I18.5
–22.9
kg/m
2)
and
‘nor
mal
’gr
oup,
BMI2
3–2
4.9
kg/m
2)
Yes
(ove
rwei
ght
gro
upon
ly)
Hig
her
BMIc
ateg
orie
sw
ere
asso
ciat
edw
ithre
duce
dm
orta
lity
risk
upto
and
incl
udin
gth
eov
erw
eight
cate
gor
ySe
x-sp
ecifi
can
alys
isre
veal
eda
redu
ctio
nin
mor
talit
yw
ithin
crea
sing
BMIu
pto
BMIo
f29.9
kg/m
2fo
rm
enan
d24.9
kg/m
2fo
rw
omen
Her
rman
net
al.
[19]
Tode
fine
the
asso
ciat
ion
betw
een
BMIa
ndac
ute
and
long
-term
outc
omes
Patie
nts
with
ST-seg
men
tm
yoca
rdia
linf
arct
ion
(with
in12
h)
N¼
3579
4BM
Iqua
rtile
s:<
24.5
kg/
m2,
24.5
–27.1
,27.1
–30.1
and>
30
kg/m
2
No
Alth
ough
in-h
ospi
tal3
-yea
rou
t-of
-hos
pita
lmor
talit
yw
asde
crea
sed
with
incr
easi
ngBM
I,th
isw
asno
long
ertru
eaf
ter
mod
elad
just
men
t;by
incl
udin
got
her
cova
riat
esin
the
mod
el,
BMIw
asno
long
erpr
edic
tive
ofac
ute
orlo
ng-te
rmm
orta
lity
Hu
etal
.[2
0]
Toin
vest
igat
ew
heth
erBM
Iis
apr
ogno
stic
fact
orin
idio
phat
hic
pulm
onar
yar
terial
hype
rtens
ion
Patie
nts
with
idio
phat
hic
pulm
onar
yar
terial
hype
rtens
ion
N¼
173
WH
Oca
tegor
ies:
3BM
Ica
tego
ries
:un
derw
eight
<18.5
kg/m
2,
norm
alw
eight
18.5
–24.9
kg/m
2
and
over
wei
ght
and
obes
e25
–34.9
kg/m
2
Yes
Hig
her
BMIw
asas
soci
ated
with
low
erm
orta
lity
risk
;pa
tient
sw
ithex
cess
BMI
had
alo
wer
risk
ofde
ath
than
norm
alw
eight
and
unde
rwei
ght
ones
Nutrition and physiological function
540 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Hua
nget
al.a
[21]
Toin
vest
igat
eth
eas
soci
atio
nbe
twee
nbo
dyco
mpo
sitio
nan
dC
AD
outc
omes
Chi
nese
patie
nts
with
angi
ogra
phic
ally
valid
ated
CA
D
N¼
3280
BMIq
uarti
les.
Aut
hors
have
also
used
aneq
uatio
nca
lled
‘bod
yad
ipos
ityes
timat
or’,
whi
chca
lcul
ated
%FM
usin
gag
e,se
xan
dBM
I.Th
ele
anm
ass
isth
enes
timat
edfrom
asu
bseq
uent
form
ula
Qua
rtile
sof
lean
mas
sw
ere
used
toca
tegor
ize
patie
nts
into
low
vers
ushi
ghle
anm
ass
No
Hig
her
lean
mas
sbu
tnot
FMw
asas
soci
ated
with
low
erca
use
mor
talit
yra
te
Kha
lidet
al.
[22]
Toev
alua
teth
epr
ogno
stic
impa
ctof
prem
orbi
dob
esity
Patie
nts
with
HF
N¼
1487
BMIa
ccor
ding
toW
HO
crite
ria
Yes
Ove
rwei
ght
and
obes
epa
tient
sha
dlo
wer
mor
talit
yth
anno
nobe
se
Kim
etal
.[2
3]
Toin
vest
igat
eth
eim
pact
ofob
esity
onin
itial
neur
olog
ical
seve
rity
Patie
nts
with
isch
aem
icst
roke
N¼
2670
BMIe
valu
ated
inqu
intil
es(Q
1,<
21.2
kg/m
2;
Q2,
21.2
–23.0
kg/m
2Q
3,
23.1
–24.5
kg/m
2;
Q4,
24.6
–26.2
kg/m
2;
Q5,
�26.3
kg/m
2)
No
Alth
ough
obes
ityw
asas
soci
ated
with
bette
rsh
ort-t
erm
func
tiona
lou
tcom
es;
this
asso
ciat
ion
was
lost
afte
rin
itial
neur
olog
ical
seve
rity
was
incl
uded
inth
em
odel
.Th
eref
ore,
the
latte
rm
ight
bea
mor
eim
porta
ntpr
ogno
stic
fact
or
Kon
igst
ein
etal
.[2
4]
Toan
alys
eth
eef
fect
ofBM
Ion
outc
omes
Elde
rlyhi
gh-
risk
patie
nts
with
seve
reao
rtic
valv
est
enos
isun
derg
oing
trans
fem
oral
TAV
I
N¼
409
BMIa
ccor
ding
toW
HO
crite
ria
Yes
Obe
sity
and
over
wei
ght
wer
ein
depe
nden
tlyas
soci
ated
with
bette
rou
tcom
e
Littn
erov
aet
al.
[25]
Toas
sess
shor
t-ter
m/l
ong-
term
mor
talit
yra
tes
with
resp
ectt
oth
eBM
I.
Patie
nts
hosp
italiz
edfo
rH
FN¼
5057
Patie
nts
divi
ded
into
two
grou
ps:
BMIo
f18.5
–25
kg/m
2an
dw
ithBM
I>
25
kg/m
2
Yes
Long
-term
mor
talit
yw
aslo
wer
inov
erw
eight
/obe
sepa
tient
s
Lope
z-D
elgad
oet
al.
[26]
Toqu
antif
yth
eef
fect
ofdi
vers
ede
gre
esof
high
BMIo
ncl
inic
alou
tcom
esaf
ter
card
iac
surg
ery
Patie
nts
unde
rgoi
ngal
lki
nds
ofca
rdia
csu
rger
yN¼
2449
BMIa
ccor
ding
toW
HO
crite
ria
Yes
for
2ou
tcom
esbu
tno
tsur
viva
l
Obe
sity
incr
ease
dpe
riop
erat
ive
myo
card
ial
infa
rctio
nan
dse
ptic
aem
iaaf
ter
card
iac
surg
ery,
but
did
nota
ffect
inho
spita
lm
orta
lity
Mig
ajet
al.
[27]
Toin
vest
igat
ew
heth
erob
esity
influ
ence
onou
tcom
eof
patie
nts
with
AC
Sva
ries
bygen
der
Patie
nts
with
AC
SN¼
341
BMIa
ccor
ding
toW
HO
crite
ria
Yes
,m
enon
lyO
nly
mal
epa
tient
sco
ntribu
ted
toth
eob
esity
para
dox
The
influ
ence
ofob
esity
onou
tcom
esse
ems
tobe
depe
nden
tofse
x (Con
tinue
d)
Body composition phenotypes and obesity paradox Prado et al.
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-clinicalnutrition.com 541

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le1
(Con
tinue
d)
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
of
ob
esit
yp
ara
do
x(D
efin
itio
n)O
bes
ity
pa
ra-
do
xre
po
rted
?Fi
ndin
gs
Num
asaw
aet
al.
[28]
Toin
vest
igat
eth
eim
pact
ofBM
Ion
in-h
ospi
tal
com
plic
atio
ns
Patie
nts
unde
rgoi
ngPC
IN¼
10
142
BMIa
ccor
ding
toW
HO
crite
ria
No
Nor
mal
-wei
ghtp
atie
nts
are
ata
gre
ater
risk
for
in-h
ospi
tal
com
plic
atio
nsth
anob
ese
Paul
etal
.[2
9]
Inve
stig
ate
the
impa
ctof
obes
ityon
in-h
ospi
tal
mor
bidi
tyan
dm
orta
lity
afte
rlu
ngre
sect
ion
Patie
nts
who
unde
rwen
tel
ectiv
ew
edge
rese
ctio
n,lo
bect
omy
orpn
eum
onec
tom
y
N¼
5216
BMIa
ccor
ding
toW
HO
crite
ria
No
BMIw
asno
tapr
edic
tor
ofm
orbi
dity
orm
orta
lity,
even
inth
em
orbi
dly
obes
e(B
MI
>35
kg/m
2)
Bein
gov
erw
eight
appr
oach
edsi
gni
fican
ceas
apr
edic
tor
for
decr
ease
dpu
lmon
ary
com
plic
atio
ns
Sasa
buch
iet
al.
[30]
Eval
uate
the
asso
ciat
ion
ofBM
Iwith
mor
talit
yin
the
ICU
inpa
tient
sw
ithan
dw
ithou
tmec
hani
cal
vent
ilatio
n
Patie
nts
adm
itted
toth
eIC
Uw
ithan
dw
ithou
tm
echa
nica
lven
tilat
ion
N¼
334
238
5BM
Icat
egor
ies:
unde
rwei
ght
(<18.5
kg/m
2),
low
norm
al(1
8.5
–22.9
kg/m
2),
high
norm
al(2
3–24.9
kg/m
2),
over
wei
ght
(25.0
–29.9
kg/
m2)
and
obes
e(>
30
kg/m
2)
Mix
edfin
ding
sIn
the
vent
ilate
dgro
up,
patie
nts
with
ahi
ghe
rBM
Iha
dlo
wer
mor
talit
y,bu
tm
orta
lity
incr
ease
dw
ithin
crea
sing
BMIi
nth
eno
nven
tilat
edgro
up
Shah
etal
.[3
1]
Inve
stig
ate
the
role
ofBM
Ion
mor
talit
yan
dim
pact
ofdy
sgly
cem
ia
Patie
nts
with
hype
rtens
ion
and
atle
asto
neot
her
CH
Drisk
fact
or,
with
out
DM
N¼
5423
4BM
Icat
egor
ies:
unde
rwei
ght
(<22
kg/m
2);
norm
alw
eight
(22
–25
kg/m
2);
over
wei
ght
(25
–30
kg/m
2);
and
obes
e(>
30
kg/m
2)
No
Impa
ired
fast
ing
glu
cose
was
asso
ciat
edw
ithal
l-cau
sem
orta
lity
and
obes
ityw
asas
soci
ated
with
low
eral
l-ca
use
mor
talit
y;ho
wev
er,
this
was
nots
igni
fican
tafte
rex
clud
ing
smok
ers
and
unde
rwei
ght
indi
vidu
als
Taki
guc
hiet
al.
[32]
Inve
stig
ate
the
asso
ciat
ion
ofBM
Iwith
card
iac
func
tion,
neur
ohor
mon
alfa
ctor
s,co
mor
bidi
ties,
and
prog
nosi
s
Hos
pita
lized
HF
patie
nts
N¼
648
BMIa
ccor
ding
toW
HO
crite
ria
Yes
Car
diac
and
all-c
ause
mor
talit
ypr
ogre
ssiv
ely
incr
ease
dfrom
obes
eto
over
wei
ght
,no
rmal
and
unde
rwei
ght
gro
upBM
Iwas
anin
depe
nden
tpr
edic
tor
ofca
rdia
can
dal
l-ca
use
mor
talit
y.A
ll-ca
use
mor
talit
yw
ashi
ghe
rin
the
unde
rwei
ght
gro
up
Nutrition and physiological function
542 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Taw
ket
al.
[33]
Inve
stig
ate
the
asso
ciat
ion
betw
een
BMIa
ndag
ew
ithth
ese
verity
ofsu
bara
chno
idha
emor
rhag
ean
dfu
nctio
nalo
utco
me
Patie
nts
with
suba
rach
noid
haem
orrh
age
N¼
274
4BM
Icat
egor
ies:
unde
rwei
ght
orno
rmal<
25
kg/m
2;
over
wei
ght2
5–29.9
kg/m
2;
mod
erat
ely
obes
e30
–34.9
kg/m
2;
seve
rely
orve
ryse
vere
lyob
ese
>35
kg/m
2
No
BMIw
asno
tass
ocia
ted
with
mea
sure
sof
func
tion
orse
verity
ofbl
eedi
ng
Utz
olin
oet
al.
[34]
Inve
stig
ate
the
asso
ciat
ion
ofBM
Ion
mor
talit
yin
patie
nts
with
seve
repe
rito
nitis
Patie
nts
with
perito
nitis
and
seps
isw
hone
eded
inte
nsiv
eca
refo
rm
ore
than
2da
yspo
stop
erat
ivel
y
N¼
253
4BM
Igro
ups:
unde
rwei
ght
<21
kg/m
2;
norm
alw
eight
21
–25
kg/m
2;
over
wei
ght
26
–30
kg/m
2;
and
>30
kg/m
2;
also
com
pare
dob
ese
(BM
I>30
kg/m
2)
and
non
obes
egro
ups
Yes
,sh
ortt
erm
only
Surv
ival
at28
days
was
best
inth
eob
ese
and
wor
stin
the
unde
rwei
ght
Ove
rwei
ght
patie
nts
wer
eno
tmor
elik
ely
tobe
disc
harg
edho
me
No
diffe
renc
esw
ere
obse
rved
in5-y
ear
surv
ival
betw
een
gro
ups
Wan
get
al.
[35]
Tode
term
ine
the
rela
tion
betw
een
BMIa
ndm
orta
lity
Patie
nts
with
esta
blis
hed
AF
and
HF
N¼
2016
BMIc
ateg
oriz
edac
cord
ing
toth
eC
hine
seob
esity
wor
king
grou
p–
unde
rwei
ght
,<
18.5
kg/m
2;
norm
alw
eight
,18.5
to<
24
kg/m
2;
over
wei
ght,
24
to<
28
kg/
m2;
obes
e,�
28
kg/m
2
Yes
Obe
sean
dov
erw
eight
patie
nts
had
bette
rsu
rviv
alth
anno
rmal
wei
ght
Wita
ssek
etal
.[3
6]
Toin
vest
igat
eth
eim
pact
ofBM
Ion
mor
talit
yPa
tient
sw
ithST
-ele
vatio
nm
yoca
rdia
linf
arct
ion
N¼
6938
BMIa
ccor
ding
toW
HO
crite
ria
No
AU
-sha
ped
dist
ribu
tion
betw
een
BMIg
roup
sw
asre
porte
dw
ithth
elo
wes
tm
orta
lity
obse
rved
inob
ese
clas
sIa
ndhi
ghe
stin
unde
rwei
ght
.N
onet
hele
ss,
adju
stm
entf
orco
variat
esel
imin
ated
diffe
renc
esbe
twee
ngro
ups
Low
ercr
ude
in-h
ospi
tal
mor
talit
yof
obes
ecl
ass
Ico
uld
bepa
rtial
lyex
plai
ned
bylo
wer
age
and
low
erco
mor
bidi
tyra
tes
Woh
lfahr
teta
l.[3
7]
Toas
sess
the
asso
ciat
ion
ofob
esity
atth
etim
eof
stro
kead
mis
sion
and
wei
ght
loss
afte
rst
roke
with
tota
lmor
talit
y
Patie
nts
hosp
italiz
edfo
rth
eir
first
isch
emic
stro
keN¼
511
BMIa
ccor
ding
toW
HO
crite
ria
Wei
ght
loss
defin
edby
aw
eight
loss
of>
3kg
No
Nor
mal
wei
ght
atho
spita
lizat
ion
and
wei
ght
loss
afte
rst
roke
are
inde
pend
ently
asso
ciat
edw
ithhi
ghe
rm
orta
lity
Obe
sity
and
over
wei
ght
atad
mis
sion
dono
tdec
reas
eth
erisk
asso
ciat
edto
wei
ght
loss
(Con
tinue
d)
Body composition phenotypes and obesity paradox Prado et al.
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-clinicalnutrition.com 543

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le1
(Con
tinue
d)
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
of
ob
esit
yp
ara
do
x(D
efin
itio
n)O
bes
ity
pa
ra-
do
xre
po
rted
?Fi
ndin
gs
Yam
auch
iet
al.
[38]
Inve
stig
ate
the
asso
ciat
ion
betw
een
BMIa
ndin
hosp
italm
orta
lity
inel
derly
patie
nts
with
CO
PD
Elde
rlypa
tient
s(a
ge>
65
year
s)ad
mitt
edto
the
hosp
italf
orC
OPD
N¼
263
940
BMIa
ccor
ding
toW
HO
crite
ria
Nor
mal
wei
ght
was
furth
erdi
vide
din
tolo
w-n
orm
al(B
MI1
8.5
–22.9
kg/m
2)
and
high
norm
al(2
3.0
–24.9
kg/m
2)
Yes
Ove
rwei
ght
and
obes
epa
tient
sha
da
low
erm
orta
lity
than
low
–nor
mal
wei
ght
patie
nts
Hig
her
mor
talit
yw
asas
soci
ated
with
age,
mal
egen
der,
seve
redy
spne
a,lo
wer
leve
lofco
nsci
ousn
ess,
and
low
erac
tiviti
esof
daily
livin
g
Zaf
rir
etal
.[3
9]
Inve
stig
ate
the
prog
nost
icsi
gni
fican
ceof
BMIa
ndBS
Ain
chro
nic
HF
patie
nts
Syst
olic
HF
patie
nts,
atth
efir
stvi
sitt
oth
eH
Fcl
inic
N¼
630
Terti
les
ofBM
I(T1�
25.5
kg/
m2;
25.5<
T2�
30.4
;T3>
30.4
kg/m
2)
and
BSA
(T1�
1.7
9;
1.7
9<
T2�
1.9
9;
T3>
1.9
9)
No
An
inve
rse
asso
ciat
ion
ofBM
Ian
dBS
Ate
rtile
sw
ithm
orta
lity
risk
was
obse
rved
The
obes
itypa
rado
xw
asat
tenu
ated
afte
rm
ultiv
aria
tean
alys
isan
ddi
dno
tper
sist
afte
rad
just
men
tfor
age
(obe
sepa
tient
sw
ere
youn
ger
)
AC
E,an
gio
tens
in-c
onve
rting
enzy
me;
AC
S,ac
ute
coro
nary
synd
rom
e;A
F,ar
terial
fibrilla
tion;
AM
I,ac
ute
myo
card
iali
nfar
ctio
n;BS
A,
body
surfac
ear
ea;
BW,
body
wei
ght
;C
ABG
,co
rona
ryar
tery
bypa
ssgra
ft;C
AD
,co
rona
ryar
tery
dise
ase;
CH
D,
coro
nary
hear
tdis
ease
;C
KD
,ch
roni
cki
dney
dise
ase;
CO
PD,
chro
nic
obst
ruct
ive
pulm
onar
ydi
seas
e;C
RF,
card
iore
spirat
ory
fitne
ss;
CTO
,ch
roni
cto
talo
cclu
sion
;C
VD
,co
rona
ryva
scul
ardi
seas
e;D
M,
diab
etes
mel
litus
;G
FR,
glo
mer
ular
filtra
tion
rate
;H
DL,
high
dens
itylip
opro
tein
;H
F,he
artf
ailu
re;
IABP
,in
tra-a
ortic
ballo
onpu
mpi
ng;
ICU
,in
tens
ive
care
unit;
LAD
,le
ftan
terior
desc
endi
ng;
LVED
D,
left
vent
ricu
lar
end-
dias
tolic
dim
ensi
ons;
LVEF
,le
ftve
ntricl
eej
ectio
nfrac
tion;
Mpa
p,m
ean
pulm
onar
yar
tery
pres
sure
;m
RAP,
mea
nright
arte
rial
pres
sure
;N
T-pr
oBN
P,N
-Ter
min
alpr
obr
ain
type
atriur
etic
pept
ide;
NYH
A,
New
Yor
kH
ealth
Ass
ocia
tion;
PAD
,pe
riph
eral
arte
rydi
seas
e;PC
I,pe
rcut
aneo
usco
rona
ryin
terv
entio
n;PC
WP,
pulm
onar
yca
pilla
ryw
edge
pres
sure
;pr
oBN
T,N
-term
inal
pro-
brai
nna
triur
etic
pept
ide;
PKV
O2,
peak
oxyg
enup
take
;PV
R,pu
lmon
ary
vasc
ular
resi
stan
ce;
SBP,
syst
olic
bloo
dpr
essu
re;
SCA
,su
dden
card
iac
arre
st;
STEM
I,ST
elev
atio
nm
yoca
rdia
linf
arct
ion;
SVO
2,
mix
edve
nous
oxyg
ensa
tura
tion;
T2D
,ty
pe2
diab
etes
;TA
VI,
trans
cath
eter
aorti
cva
lve
impl
anta
tion;
WC
,w
aist
circ
umfe
renc
e.aA
lthou
gh
this
stud
yus
edbo
dyco
mpo
sitio
nte
rmin
olog
y,th
eca
lcul
atio
nsw
ere
derive
dfrom
BMI,
age
and
sex.
Nutrition and physiological function
544 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Body composition phenotypes and obesity paradox Prado et al.
Ahmadi et al. [43] investigated the obesity para-dox in kidney transplant recipients in four studies,reporting a higher mortality in obese patients usingpretransplantation BMI. Notably, all of these meta-analysis studies reported a higher risk of shortersurvival among underweight patients. Ahmadiet al. [43] highlighted that unlike obesity, beingunderweight consistently predicted survival. There-fore, there are paradoxical or differing resultssuggesting that the presence of obesity paradox isunlikely in such a scenario [43].
Using data from 89 studies with a total of1 300 794 patients wherein risk estimates were pro-vided for short and long-term mortality on cardio-vascular events, Wang et al. [44] reported a J-shapedrelationship between mortality and BMI in patientswith coronary artery disease. Underweight patientspresented with the highest risk and the overweightand obese with the lowest. Nonetheless, inconsist-ent findings were reported when the long-term datawere evaluated. The long-term inverse relationshipbetween BMI and mortality was attenuated, disap-pearing after 5 years of follow-up. Grades II and IIIobesity were associated with lower risk of short-termmortality but higher risk after 5 years of follow-up.
Studies using surrogate assessments ofbody composition
Additional anthropometric measurements such aswaist and/or hip circumference, skinfold thicknessmeasurements and circumferences were used inseven studies, in which three reported the obesityparadox (one observing it in men only) and theremaining disproving such phenomenon (Table 2)[45–55]. Using an inception cohort of adults withdiabetes, Bozorgmanesh et al. [45] highlighted theneed of adjusting for a measure of central adipositywhen investigating the effect of obesity andmortality. The lack of a value for waist circumfer-ence would have led to an overestimation of themortality associated with an increased BMI in theirdatabase of newly diagnosed patients with diabetes.The authors noted that there is a ‘BMI-paradox’,which is not a sufficient marker of obesity.
The need for further measurements of nutri-tional assessment when investigating the obesityparadox was highlighted in the study by Gastelur-rutinia et al. [47
&&
]. In patients with heart failure,nutritional status (undernourished) was an inde-pendent prognostic factor above and beyond BMIand percentage body fat (calculated using surrogatetools). Therefore, in this study, BMI masked truenutritional status.
Using arm circumferences and skinfoldmeasurements of patients receiving elective surgery,
Copyright © 2015 Wolters Kluwe
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
Rodriguez-Garcia et al. [49] found no differences innosocomial infection and length of hospital staycomparing obese and nonobese patients; nonethe-less, the authors have not controlled for confound-ing variables; only bivariate analysis was conducted.In patients with acute coronary syndrome, Shehabet al. [50] showed that in-hospital and peri-hospitalmortality was not associated with weight, BMI orwaist circumference.
Studies using body compositionassessments
There is a clear need for further body compositionassessment studies to elucidate the contradictoryevidence on the obesity paradox phenomenon asonly four have been published in the past year.Among these, the methodologies utilized were com-puted tomography (CT, two studies), dual-energyX-ray absorptiometry (DXA) or bioelectrical impe-dance analysis (BIA), Table 2.
In 72 patients with COPD, survival was notdifferent between higher versus lower BMI patients(although a trend towards longer survival wasobserved in those with higher BMI) [52
&&
]. Over-weight and obese patients had better lung function,exercise capacity and larger muscle cross-sectionalarea than those with normal BMI. These variableswere able to confound the trend of improved sur-vival in those with excess BMI.
An interesting study in older adults with type 2diabetes; Murphy et al. [54
&&
] used CT-assessed bodycomposition and functional assessments to test theassociation between these variables and mortality.Using multivariate analysis adjusted for demo-graphic and diabetes-risk factors, they reportedhigher risk in normal-weight patients than over-weight ones. The authors further performed amediation analysis to test if adipose tissue, musclesize and physical function would affect the associ-ations between BMI and mortality. From thisanalysis, thigh muscle size mediated 46% of theeffect of the higher risk found in normal-weightpatients. When comparing four groups: over-weight/normal weight and high/low muscle(according to the respective sex-specific median),the authors concluded that being overweight wasonly protective in patients with high muscle massand that the highest mortality was found in the twolow muscle mass groups (either in patients withnormal weight or overweight). These resultsare similar to what has been reported in cancerpatients [10
&
]. Using BIA to assess body compo-sition, Gonzalez et al. [10
&
] reported that the obesityparadox was only present in cancer patients whenobesity was defined by BMI. BMI was not able to
r Health, Inc. All rights reserved.
rved. www.co-clinicalnutrition.com 545

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le2
.Su
mm
ary
ofst
udie
spu
blis
hed
inth
epa
stye
arin
whi
chbo
dyco
mpo
sitio
nor
surr
ogat
eas
sess
men
tsw
ere
used
toin
vest
igat
eth
eob
esity
para
dox
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
(s)
of
ob
esit
yp
ara
do
x(D
efin
itio
n)
Bo
dy
com
po
siti
on
ass
essm
ent
or
surr
og
ate
Ob
esit
yp
ara
do
xre
po
rted
?Fi
ndin
gs
Surrogate
bodycompositionmethods
Bozo
rgm
anes
het
al.
[45]
Tote
stw
heth
erth
eco
ntribu
tions
ofan
thro
pom
etric
variab
les
are
nonl
inea
ran
dw
heth
erW
Can
dH
Pco
ntribu
teto
the
obes
itypa
rado
x
Adu
ltsfrom
Iran
with
new
onse
tdia
bete
sat
base
line
exam
inat
ion
orin
cide
ntdi
abet
esin
any
ofth
etw
ofo
llow
-up
s
NU
1322
BMIt
ertil
esm
edia
n:1st
:24.9
kg/m
2;
2nd
:28.9
kg/m
2
and
3rd
:33.8
kg/
m2
WC
and
HC
,w
aist
-to
-hip
ratio
No
Ther
ew
asa
nonl
inea
rre
latio
nshi
pbe
twee
nW
Can
dal
l-cau
sem
orta
lity,
butt
his
rela
tions
hip
was
inve
rse
and
linea
rfo
rH
CA
fter
adju
stm
ents
for
WC
and
HC
,th
ere
wer
eno
asso
ciat
ions
betw
een
BMIa
ndal
l-cau
sem
orta
lity
Cep
eda-
Val
ery
etal
.[4
6]
Tote
stth
ehy
poth
esis
whe
ther
CA
Ddi
seas
eis
less
com
plex
and
seve
rein
obes
eth
anit
isin
nono
bese
indi
vidu
als
Patie
nts
with
AM
IN
U95
BMI�
30
kg/m
2
and/
orW
C�
102
cmin
men
and�
88
cmin
wom
en
WC
Yes
Obe
sity
atth
etim
eof
AM
Iis
asso
ciat
edw
ithle
ssse
vere
CA
D
Gas
telu
rrut
iaet
al.
[47
&&
]To
asse
ssan
dco
mpa
reth
epr
ogno
stic
impa
ctof
mea
sure
sof
nutri
tiona
lsta
tus
BMIa
ndbo
dyfa
t
Am
bula
tory
hear
tfa
ilure
patie
nts
NU
214
BMIa
ccor
ding
toW
HO
crite
ria
Nut
ritio
nals
tatu
sw
asfu
rther
asse
ssed
byal
bum
inan
dly
mph
ocyt
e
Four
anth
ropo
met
ric
mea
sure
men
tsus
edto
calc
ulat
ebo
dyde
nsity
and
derive
%FM
.M
alnu
tritio
ncl
assi
fied
into
one
oftw
oca
tego
ries
:al
bum
in,
lym
phoc
yte
coun
t,sk
info
lds
and
arm
circ
umfe
renc
e�
2be
low
norm
al;
orsk
info
lds,
albu
min
and
lym
phoc
yte
coun
t�1
belo
wno
rmal
No
BMIa
nd%
FMw
ere
not
inde
pend
entp
redi
ctor
sof
2-y
even
tfre
esu
rviv
alM
alnu
tritio
nw
asa
bette
ran
din
depe
nden
tpr
edic
tor
ofsu
rviv
alth
anBM
I
Nutrition and physiological function
546 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Moh
ebiet
al.
[48]
Toev
alua
teth
eas
soci
atio
nof
seve
ralt
ypes
offa
tdi
stribu
tion
mea
sure
sw
ithth
erisk
ofal
l-cau
sem
orta
lity
inC
KD
patie
nts
Patie
nts
with
CKD
from
Tehr
anN
U1860
BMIa
sa
cont
inuo
usva
riab
leW
eight
,W
Can
dH
CYes
,m
enon
lyD
iffer
entr
esul
tsac
cord
ing
tose
x:in
men
with
CKD
,af
ter
cont
rolli
ngfo
rco
nfou
nder
san
dm
edia
tors
,ha
ving
mor
efa
t(W
C,
HC
orBM
I)re
sults
ina
bette
rsu
rviv
al.
This
effe
ctw
asno
tfou
ndin
wom
en
Rodr
igue
z-G
arci
aet
al.
[49]
Toco
mpa
reLO
San
dN
Iin
cide
nce
betw
een
obes
ean
nono
bese
surg
ical
patie
nts
Surg
ical
Mex
ican
-H
ispa
nic
patie
nts
(gas
trosu
rger
y,ne
uros
urger
yan
dpr
octo
logy
depa
rtmen
ts)
NU
82
WH
Oca
tegor
ies
AC
,TS
F,A
MA
and
AFA
No
NIa
ndLO
Sw
ere
sim
ilar
inob
ese
and
nono
bese
patie
nts
Sheh
abet
al.
(2014)
[50]
Toas
sess
the
in-h
ospi
tala
ndpe
r-hos
pita
lmor
talit
yrisk
inre
latio
nto
patte
rns
ofad
ipos
ity
Patie
nts
with
AC
SN
U7930
BMIa
ccor
ding
toW
HO
crite
ria
and
WC�
102
cmin
men
and�
88
cmin
wom
en
WC
No
In-h
ospi
tala
ndpe
ri-h
ospi
tal
mor
talit
yw
asno
tas
soci
ated
with
obes
ityde
fined
byBM
Iand
WC
Sobi
czew
skiet
al.
[51]
Toex
amin
eth
eas
soci
atio
nof
BMIa
ndad
ipos
etis
sue
dist
ribu
tion,
mea
sure
dby
WC
with
card
iova
scul
arrisk
inpa
tient
sw
ithC
HD
CH
Dpa
tient
sN
U1345
3su
bgro
ups
acco
rdin
gto
BMI:
norm
al(1
8.5
–24.9
kg/m
2);
over
wei
ght
(25
–29.9
kg/m
2)
and
obes
e(�
30
kg/m
2)
WC
quar
tiles
:I
(WC
<91
cm),
II(W
C91
–96.9
cm),
III(W
C97
–104
cm)an
dIV
(WC�
104
cm)
Yes
Direc
trel
atio
nshi
p(W
C)
and
anin
vers
ere
latio
nshi
p(B
MI)
for
both
tota
land
CV
mor
talit
y.BM
Ihad
apr
otec
tive
effe
ctfo
rto
tal
and
CV
mor
talit
yaf
ter
cont
rolli
ngfo
ral
lthe
othe
rfa
ctor
s.Th
ehi
ghe
strisk
gro
upfo
rbo
thto
tal
and
CV
mor
talit
yw
asBM
I<25
kg/m
2w
ithW
C�
104
cm
(Con
tinue
d)
Body composition phenotypes and obesity paradox Prado et al.
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights reserved. www.co-clinicalnutrition.com 547

Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved.
Tab
le2
(Con
tinue
d)
Ref
eren
ceO
bje
ctiv
eC
linic
al
po
pu
lati
on/
Cha
ract
eris
tics
Sam
ple
size
Mea
sure
(s)
of
ob
esit
yp
ara
do
x(D
efin
itio
n)
Bo
dy
com
po
siti
on
ass
essm
ent
or
surr
og
ate
Ob
esit
yp
ara
do
xre
po
rted
?Fi
ndin
gs
Directassessmentofbodycomposition
Gal
esan
uet
al.
[52
&&
]To
inve
stig
ate
ifob
esity
para
dox
inch
roni
cob
stru
ctiv
epu
lmon
ary
dise
ase
(CO
PD)
can
beex
plai
ned
byfa
tac
cum
ulat
ion
orco
nfou
ndin
gfa
ctor
s
Patie
nts
with
CO
PDat
tend
ing
are
habi
litat
ion
prog
ram
me
NU
190
2BM
Isub
gro
ups:
norm
alw
eight
<25
kg/m
2;
over
wei
ght
/obe
se�
25
kg/m
2
Mid
-thig
hm
uscl
ecr
oss-se
ctio
nal
area
from
CT
(MTC
SAC
T)
No
The
tend
ency
ofa
bette
rsu
rviv
alin
over
wei
ght
/ob
ese
CO
PDpa
tient
sdi
sapp
eare
daf
ter
cont
rolli
ngfo
rpe
akw
ork
rate
,M
TCSA
CT
and
parti
alpr
essu
reof
carb
ondi
oxid
e
Hon
get
al.
[53]
Toin
vest
igat
eth
ere
latio
nshi
pbe
twee
nva
riou
sob
esity
mar
kers
and
mor
talit
y
Asi
an(K
orea
n)pa
rtici
patin
gin
alo
ngitu
dina
lstu
dyon
agin
g
NU
1000
BMI(
quar
tiles
ofth
edi
stribu
tion)
VA
Tan
dSA
Tad
ipos
etis
sue
asse
ssed
byC
TTo
talf
atm
ass
and
%as
sess
edby
BIA
Yes
BMIa
ndV
AT
wer
ein
vers
ely
asso
ciat
edw
ithal
l-cau
sem
orta
lity
over
ape
riod
of6
year
s(lo
wes
tw
ithhi
ghe
stqu
artil
eof
BMIa
ndth
ird
ofV
AT)
.To
talf
atm
ass
was
not
asso
ciat
edw
ithm
orta
lity
Mur
phy
etal
.[5
4&
&
]To
inve
stig
ate
the
effe
ctof
adip
ose
tissu
e,m
uscl
esi
zean
dph
ysic
alfu
nctio
non
the
rela
tions
hip
betw
een
BMI
mor
talit
y
Dia
betic
olde
rad
ults
from
Icel
and
NU
637
BMIa
ccor
ding
toW
HO
crite
ria
Thig
hm
uscl
ear
ea,
VA
T,SA
Tan
dIM
AT
No
Nor
mal
-wei
ght
parti
cipa
nts
had
elev
ated
mor
talit
yrisk
than
over
wei
ght
ones
Inno
rmal
-wei
ght
indi
vidu
als,
mor
talit
yrisk
was
atte
nuat
edaf
ter
adju
stm
ents
for
mus
cle
size
Mus
cle
size
med
iate
d46%
ofth
eef
fect
ofno
rmal
wei
ght
onm
orta
lity
Adi
pose
tissu
edi
dno
tat
tenu
ate
mor
talit
yrisk
Pern
aet
al.
[55]
Toev
alua
teth
ere
latio
nshi
pam
ong
sarc
open
ia,
adip
osity
and
met
abol
icm
arke
rsan
dits
impa
cton
loss
ofm
uscl
em
ass
Elde
rlypa
tient
sad
mitt
edin
aph
ysic
alan
dm
edic
ine
and
reha
bilit
atio
ndi
visi
onof
anIta
lian
inst
itute
NU
290
BMIa
sco
ntin
uous
variab
leD
XA(le
anm
ass,
fat
mas
s,an
droi
dan
dgyn
oid
fat)
Yes
The
use
ofa
com
posi
teva
riab
lem
odel
dem
onst
rate
dth
atan
incr
ease
inad
ipos
ityan
dle
vels
ofm
etab
olic
mar
kers
atno
rmal
rang
esis
prot
ects
agai
nstm
uscl
elo
ss
Nutrition and physiological function
548 www.co-clinicalnutrition.com Volume 18 � Number 6 � November 2015

Met
abol
icva
riab
les
(alb
umin
,lo
w-
dens
itylip
opro
tein
chol
este
rol,
high-
dens
itylip
opro
tein
chol
este
rol,
tota
lch
oles
tero
l,tri
glyc
erid
es,
C-
reac
tive
prot
ein,
hom
ocys
tein
e,fo
late
and
vita
min
B12
The
auth
ors
conc
lude
dth
atth
eir
findi
ngs
mig
htin
dica
tea
prot
ectiv
eef
fect
ofad
ipos
ityco
mpa
tible
with
the
obes
itypa
rado
x
AC
,ar
mci
rcum
fere
nce;
AC
S,ac
ute
coro
nary
synd
rom
e;A
FA,
arm
sfa
tare
a;A
MA
,ar
mm
uscl
ear
ea;
CA
D,
coro
nary
arte
rydi
seas
e;C
HD
,co
rona
ryhe
artd
isea
se;
CKT,
chro
nic
kidn
eydi
seas
e;C
T,co
mpu
ted
tom
ogra
phy;
DXA
,du
al-e
nerg
yX-
ray
abso
rptio
met
ry;
FM,
fatm
ass;
HC
,hi
pci
rcum
fere
nce;
IMA
T,in
term
uscu
lar
adip
ose
tissu
e;LO
S,le
ngth
ofho
spita
lsta
y;LV
EF,
left
vent
ricu
lar
ejec
tion
frac
tion;
NI,
noso
com
ial
infe
ctio
n;N
R,no
trep
orte
d;SA
T,su
bcut
aneo
usad
ipos
etis
sue;
TSF,
trice
pssk
info
ld;
VA
T,vi
scer
alad
ipos
etis
sue;
WC
,w
aist
circ
umfe
renc
e.
Body composition phenotypes and obesity paradox Prado et al.
Copyright © 2015 Wolters Kluwe
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
identify the majority of patients with excess fat massand low muscle mass was an independent risk factorfor higher mortality. Excess fat mass had no protec-tive effect in the presence of low muscle mass andthe shorter survival time was indeed observed in thesarcopenic obesity group.
Two studies noted the obesity paradox usingdirect assessment of body composition. In the studyby Hong et al. [53], higher visceral adiposity assessedby CT scan and not BIA-assessed total fat mass wasassociated with reduced all-cause mortality in eld-erly Asian individuals (mean age 76 years). All-causemortality was lowest within the highest and thirdBMI and visceral adiposity quartiles, respectively.Furthermore, visceral adiposity was a marker formortality in a U-shaped pattern. Interestingly andunfortunately, the authors have not explored theeffect of fat free mass (and hence muscle mass) intheir model, even though that was assessed by BIA.CT-assessed muscle mass was also not evaluated. Asthe authors discussed, muscle mass is an importantvariable that can explain their findings. Finally, thestudy by Perna et al. [55] examines the associationamong low muscle mass, adiposity and metabolicmarkers in Italian older individuals. In a complexstatistical analysis called canonical correlationanalysis and structural equation modelling, individ-ual scores of metabolic profile were created andcorrelated with muscle mass. The authors noted anegative association between sarcopenia severityand adiposity/metabolic profile, indicating a protec-tive effect of adiposity on muscle loss. Therefore,although their results confirmed the obesity para-dox, an increase of adiposity and levels of metabolicparameters were protective in respect to muscle loss[55].
CONCLUSION
A perpetuation of the contradictory findings relatedto the obesity paradox is highlighted in this review,independent of the definition of obesity being solelybased on BMI, surrogate or direct assessments ofbody composition.
There is enough evidence in the literature high-lighting the value of body composition assessment toevaluate and predict nutritional status, and emergingevidence that body composition phenotypes maydemystify the obesity paradox phenomenon. None-theless, less than 10% (four out of 42) of the originalarticles published in the past 12 months included adirect assessment of body composition and, amongthese, a full description of compartments (e.g. musclemass) was not conducted/explored.
In view of the body composition variability ofpatients with identical BMI, particularly in clinical
r Health, Inc. All rights reserved.
rved. www.co-clinicalnutrition.com 549

Nutrition and physiological function
populations, it is unreasonable to rely solely on thisindex as a marker to identify obesity. Furthermore,differences in fluid shifts that may occur in theseclinical conditions may also impact the accuracy ofBMI [47
&&
], potentially overestimating BMI measure-ments (e.g. heart failure patients).
The use of sophisticated body compositionassessment tools is still limited (especially in epide-miological settings). Notwithstanding, it is unlikelythat we will substantially advance our knowledgewithout the use of this science. As we have pre-viously discussed [1
&
,7], Hippocrates could havemeasured body weight and BMI. We are in an erain which sophisticated tools are needed and in linewith any other evolving field of health-relatedresearch.
If body composition phenotypes can indeedelucidate the dichotomous relationship betweenBMI and prognostication in a variety of clinicaland nonclinical conditions, the need is urgent forsuch a research approach. The consequences of apotential insubstantial obesity paradox are mixedmessages advising individuals to become obese inthe hopes of improving outcomes. Finally, adjustingfor important confounding bias originating fromeach specific condition under study is also import-ant and potentially mediators of the risk factorassociated with obesity.
Acknowledgements
The authors would like to acknowledge Isabella Barbosa,Sarah Purcell, Camila Orsso and Bianca Caroline Orssofor their assistance in creating drafting and/or formattingthe tables, figure and references.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDEDREADINGPapers of particular interest, published within the annual period of review, havebeen highlighted as:
& of special interest&& of outstanding interest1.&
Prado CM, Heymsfield SB. Lean tissue imaging: a new era for nutritionalassessment and intervention. JPEN J Parenter Enteral Nutr 2014; 38:940–953.
This review article synthesizes the importance of body composition assessment inview of the variability of body composition in contemporary populations, providingthe summary of evidence on the limitations of BMI-defined obesity in clinicalsettings.2. Banack HR, Kaufman JS. The obesity paradox: understanding the effect of
obesity on mortality among individuals with cardiovascular disease. Prev Med2014; 62:96–102.
3. Clark DO, Gao S, Lane KA, et al. Obesity and 10-year mortality in very oldAfrican Americans and Yoruba-Nigerians: exploring the obesity paradox.J Gerontol A Biol Sci Med Sci 2014; 69:1162–1169.
Copyright © 2015 Wolters Kluwer
550 www.co-clinicalnutrition.com
4. Despres JP. Obesity and cardiovascular disease: weight loss is not the onlytarget. Can J Cardiol 2015; 31:216–222.
5. Banack HR, Kaufman JS. Does selection bias explain the obesity paradoxamong individuals with cardiovascular disease? Ann Epidemiol 2015;25:342–349.
6. Heymsfield SB, Cefalu WT. Does body mass index adequately convey apatient’s mortality risk? JAMA 2013; 309:87–88.
7. Prado CM, Siervo M, Mire E, et al. A population-based approach to definebody-composition phenotypes. Am J Clin Nutr 2014; 99:1369–1377.
8. Siervo M, Prado CM, Mire E, et al. Body composition indices of a load-capacity model: gender- and BMI-specific reference curves. Public HealthNutr 2015; 18:1245–1254.
9. Oreopoulos A, Ezekowitz JA, McAlister FA, et al. Association between directmeasures of body composition and prognostic factors in chronic heart failure.Mayo Clin Proc 2010; 85:609–617.
10.&
Gonzalez MC, Pastore CA, Orlandi SP, et al. Obesity paradox in cancer: newinsights provided by body composition. Am J Clin Nutr 2014; 99:999–1005.
By using body composition assessment, this study shows that the obesity paradoxis present in cancer patients only when obesity is defined by BMI. Patients withsarcopenic obesity had the poorest prognosis.11. Baker JF, Billig E, Michaud K, et al. Weight loss, the obesity paradox, and the
risk of death in rheumatoid arthritis. Arthritis Rheumatol 2015; 67:1711–1717.
12. Buck DL, Moller MH. Influence of body mass index on mortality after surgeryfor perforated peptic ulcer. Br J Surg 2014; 101:993–999.
13. Clark AL, Fonarow GC, Horwich TB. Impact of cardiorespiratory fitness on theobesity paradox in patients with systolic heart failure. Am J Cardiol 2015;115:209–213.
14. Costanzo P, Cleland JG, Pellicori P, et al. The obesity paradox in type 2diabetes mellitus: relationship of body mass index to prognosis: a cohortstudy. Ann Intern Med 2015; 162:610–618.
15. Dehlendorff C, Andersen KK, Olsen TS. Body mass index and death by stroke:no obesity paradox. JAMA Neurol 2014; 71:978–984.
16. Diletti R, Garcia-Garcia HM, Bourantas C, et al. Impact of body mass indexon long-term clinical outcomes after second-generation drug eluting stentimplantation: insights from the international global RESOLUTE program.Catheter Cardiovasc Interv 2015; 85:952–958.
17. Farre N, Aranyo J, Enjuanes C, et al. Differences in neurohormonal activitypartially explain the obesity paradox in patients with heart failure: the role ofsympathetic activation. Int J Cardiol 2015; 181:120–126.
18. Garcia-Ptacek S, Kareholt I, Farahmand B, et al. Body-mass index andmortality in incident dementia: a cohort study on 11 398 patients fromSveDem, the Swedish Dementia Registry. J Am Med Dir Assoc 2014;15:e441–e447.
19. Herrmann J, Gersh BJ, Goldfinger JZ, et al. Body mass index and acute andlong-term outcomes after acute myocardial infarction (from the HarmonizingOutcomes with Revascularization and Stents in Acute Myocardial InfarctionTrial). Am J Cardiol 2014; 114:9–16.
20. Hu EC, He JG, Liu ZH, et al. Survival advantages of excess body mass index inpatients with idiopathic pulmonary arterial hypertension. Acta Cardiol 2014;69:673–678.
21. Huang BT, Peng Y, Liu W, et al. Lean mass index, body fat and survivalin Chinese patients with coronary artery disease. QJM 2015; 108:641–647.
22. Khalid U, Ather S, Bavishi C, et al. Premorbid body mass index and mortalityafter incident heart failure: the ARIC Study. J Am Coll Cardiol 2014;64:2743–2749.
23. Kim Y, Kim CK, Jung S, et al. Obesity-stroke paradox and initial neurologicalseverity. J Neurol Neurosurg Psychiatry 2015; 86:743–747.
24. Konigstein M, Havakuk O, Arbel Y, et al. The obesity paradox in patientsundergoing transcatheter aortic valve implantation. Clin Cardiol 2015;38:76–81.
25. Littnerova S, Parenica J, Spinar J, et al. Positive influence of being overweight/obese on long term survival in patients hospitalised due to acute heart failure.PLoS One 2015; 10:e0117142.
26. Lopez-Delgado JC, Esteve F, Manez R, et al. The influence of body mass indexon outcomes in patients undergoing cardiac surgery: does the obesityparadox really exist? PLoS One 2015; 10:e0118858.
27. Migaj J, Prokop E, Straburzynska-Migaj E, et al. Does influence of obesity onprognosis differ in men and women? A study of obesity paradox in patientswith acute coronary syndrome. Kardiol Pol 2015. [Epub ahead of print]
28. Numasawa Y, Kohsaka S, Miyata H, et al. Impact of body mass index on in-hospital complications in patients undergoing percutaneous coronary inter-vention in a Japanese real-world multicenter registry. PLoS One 2015;10:e0124399.
29. Paul S, Andrews W, Osakwe NC, et al. Perioperative outcomes after lungresection in obese patients. Thorac Cardiovasc Surg 2014. [Epub ahead ofprint]
30. Sasabuchi Y, Yasunaga H, Matsui H, et al. The dose-response relationshipbetween body mass index and mortality in subjects admitted to the ICU withand without mechanical ventilation. Respir Care 2015; 60:983–991.
31. Shah RV, Abbasi SA, Yamal JM, et al. Impaired fasting glucose and body massindex as determinants of mortality in ALLHAT: is the obesity paradox real?J Clin Hypertens (Greenwich) 2014; 16:451–458.
Health, Inc. All rights reserved.
Volume 18 � Number 6 � November 2015

Body composition phenotypes and obesity paradox Prado et al.
32. Takiguchi M, Yoshihisa A, Miura S, et al. Impact of body mass index onmortality in heart failure patients. Eur J Clin Invest 2014; 44:1197–1205.
33. Tawk RG, Grewal SS, Heckman MG, et al. Influence of body mass index andage on functional outcomes in patients with subarachnoid hemorrhage.Neurosurgery 2015; 76:136–141.
34. Utzolino S, Ditzel CM, Baier PK, et al. The obesity paradox in surgical intensivecare patients with peritonitis. J Crit Care 2014; 29:e881–e885.
35. Wang J, Yang YM, Zhu J, et al. Obesity paradox in patients with atrialfibrillation and heart failure. Int J Cardiol 2014; 176:1356–1358.
36. Witassek F, Schwenkglenks M, Erne P, et al. Impact of body mass index onmortality in Swiss hospital patients with ST-elevation myocardial infarction:does an obesity paradox exist? Swiss Med Wkly 2014; 144:w13986.
37. Wohlfahrt P, Lopez-Jimenez F, Krajcoviechova A, et al. The obesity paradoxand survivors of ischemic stroke. J Stroke Cerebrovasc Dis 2015; 24:1443–1450.
38. Yamauchi Y, Hasegawa W, Yasunaga H, et al. Paradoxical associationbetween body mass index and in-hospital mortality in elderly patients withchronic obstructive pulmonary disease in Japan. Int J Chron Obstruct PulmonDis 2014; 9:1337–1346.
39. Zafrir B, Goren Y, Salman N, et al. Comparison of body mass index and bodysurface area as outcome predictors in patients with systolic heart failure.Cardiol J 2015. [Epub ahead of print]
40. Sharma A, Lavie CJ, Borer JS, et al. Meta-analysis of the relation of body massindex to all-cause and cardiovascular mortality and hospitalization in patientswith chronic heart failure. Am J Cardiol 2015; 115:1428–1434.
41. Sharma A, Vallakati A, Einstein AJ, et al. Relationship of body mass index withtotal mortality, cardiovascular mortality, and myocardial infarction after cor-onary revascularization: evidence from a meta-analysis. Mayo Clin Proc 2014;89:1080–1100.
42. Niedziela J, Hudzik B, Niedziela N, et al. The obesity paradox in acute coronarysyndrome: a meta-analysis. Eur J Epidemiol 2014; 29:801–812.
43. Ahmadi SF, Zahmatkesh G, Streja E, et al. Body mass index and mortality inkidney transplant recipients: a systematic review and meta-analysis. Am JNephrol 2014; 40:315–324.
44. Wang ZJ, Zhou YJ, Galper BZ, et al. Association of body mass index withmortality and cardiovascular events for patients with coronary artery disease: asystematic review and meta-analysis. Heart 2015. [Epub ahead of print]
45. Bozorgmanesh M, Arshi B, Sheikholeslami F, et al. No obesity paradox-BMIincapable of adequately capturing the relation of obesity with all-causemortality: an inception diabetes cohort study. Int J Endocrinol 2014;2014:282089.
Copyright © 2015 Wolters Kluwe
1363-1950 Copyright � 2015 Wolters Kluwer Health, Inc. All rights rese
46. Cepeda-Valery B, Chaudhry K, Slipczuk L, et al. Association between obesityand severity of coronary artery disease at the time of acute myocardialinfarction: another piece of the puzzle in the ‘obesity paradox’. Int J Cardiol2014; 176:247–249.
47.&&
Gastelurrutia P, Lupon J, de Antonio M, et al. Body mass index, body fat, andnutritional status of patients with heart failure: the PLICA study. Clin Nutr2014. [Epub ahead of print]. doi: 10.1016/j.clnu.2014.12.013.
Using surrogate measurements of body composition, the authors highlighted theneed for further measurements of nutritional assessment when investigating theobesity paradox, showing that the use of BMI masked patient’s true nutritionalstatus.48. Mohebi R, Simforoosh A, Tohidi M, et al. Obesity paradox and risk of mortality
events in chronic kidney disease patients: a decade of follow-up in TehranLipid and Glucose Study. J Ren Nutr 2015; 25:345–350.
49. Rodriguez-Garcia J, Gamino-Iriarte A, Rodea-Montero ER. Nutritional statusand nosocomial infections among adult elective surgery patients in a Mexicantertiary care hospital. PLoS One 2015; 10:e0118980.
50. Shehab A, Al-Dabbagh B, AlHabib K, et al. The obesity paradox in patientswith acute coronary syndrome: results from the Gulf RACE-2 study. Angiology2014; 65:585–589.
51. Sobiczewski W, Wirtwein M, Jarosz D, et al. Superiority of waist circumfer-ence and body mass index in cardiovascular risk assessment in hypertensivepatients with coronary heart disease. Blood Press 2015; 24:90–95.
52.&&
Galesanu RG, Bernard S, Marquis K, et al. Obesity in chronic obstructivepulmonary disease: is fatter really better? Can Respir J 2014; 21:297–301.
The authors suggested that the obesity paradox in patients with COPD only existswhen confounding factors are not taken into account. Muscle mass assessed bymid-thigh muscle cross-sectional area, together with hypercapnia, and exercisecapacity were important confounders that should be considered when interpretingthe association between increased BMI and survival in these patients.53. Hong ES, Khang AR, Roh E, et al. Counterintuitive relationship between
visceral fat and all-cause mortality in an elderly Asian population. Obesity(Silver Spring) 2015; 23:220–227.
54.&&
Murphy RA, Reinders I, Garcia ME, et al. Adipose tissue, muscle, and function:potential mediators of associations between body weight and mortality inolder adults with type 2 diabetes. Diabetes Care 2014; 37:3213–3219.
This study used state-of-the-art body composition assessment accounting for bothmuscle and adipose tissue compartments and its contribution to the obesity paradox.55. Perna S, Guido D, Grassi M, et al. Association between muscle mass and
adipo-metabolic profile: a cross-sectional study in older subjects. Clin IntervAging 2015; 10:499–504.
r Health, Inc. All rights reserved.
rved. www.co-clinicalnutrition.com 551
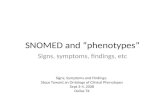


![Gut Microbiome and Obesity: A Review of Literature · 2017. 6. 20. · that obesity may be associated with gut microbiome configuration in humans [6] and that obesity phenotypes can](https://static.fdocuments.in/doc/165x107/61144e0e5b0e88613b1ab151/gut-microbiome-and-obesity-a-review-of-literature-2017-6-20-that-obesity-may.jpg)