COORDINATED AND COLLABORATIVE RESPONSES Implementing a Multidisciplinary Approach to Child...
15
COORDINATED AND COLLABORATIVE RESPONSES Implementing a Multidisciplinary Approach to Child Protective Services in Montgomery County, Maryland Utilizing a Child Advocacy Center Model (CAC)
-
Upload
shon-wilkinson -
Category
Documents
-
view
213 -
download
0
Transcript of COORDINATED AND COLLABORATIVE RESPONSES Implementing a Multidisciplinary Approach to Child...

COORDINATED AND COLLABORATIVE RESPONSES
Implementing a Multidisciplinary Approach to Child Protective Services
in Montgomery County, Maryland Utilizing a Child Advocacy Center
Model (CAC)

DESCRIPTION OF THE CAC MODEL
• Incorporates a multidisciplinary team approach to respond to allegations of child abuse to minimize the potential traumatic impact of disclosure
• Teams of Child Protective Service workers and law enforcement conduct joint forensic interviews using video equipment and a standardized protocol (R.A.T.A.C. – Rapport building, Anatomy identification, Touch inquiry, Abuse scenario and Closure)
• Forensic medical examination by Board certified Child Abuse pediatrician
• Collaboration with the State’s Attorneys Office to review the forensic interview
• MDT review and decision making (CPS, FCD, SAO, OCA)

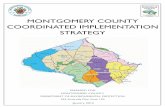
CAC MODEL
Comm.Providers
SAO
OCA
VA
FCD
CPS/CWS
Juv. Ct.
MCPS
CAC

CAC Services• Mental health evaluation and assessment by
Board Certified Forensic Social Worker• Referral for Treatment• Crisis Intervention and emotional support• Victim Advocacy• Forensic Medical Services• Nurse Case Management• Mental Health Treatment • Education, Prevention and Training• Transportation Services








CAC vs CPS models• Particular to MoCo (other CACs in Maryland)• CPS: Non forensic interviewing without video Possible need for multiple interviews Police not present Location may not be child friendly CAC: Offers immediate intervention Child friendly environment Centralized point of service Coordinated and collaborative response Inclusive of other disciplines

Case examples• Guidance counselor calls CPS screening – case assigned to CPS S/A unit for
investigation.• FCD and CPS conduct joint forensic interview• 14 y.o. girl discloses sexual abuse by father over period of 5 years • Safety plan with non-offending parent • Police asked alleged perpetrator to come to station• Father admitted sexual relationship• Police obtained warrant and searched home – confiscated camera and computer• Child assessed by mental health specialist (EL) and referred for treatment• Forensic Medical evaluation and exam• Continuing CPS assigned; MDT convened for case review• SAO prepares case for prosecution• Mother doesn’t believe child; not supportive or cooperative with services• Child dissociating in therapy; attending Support Group; child recants• CPS considers removal/court action/convenes FIM and another MDT• Father accepted plea and was sentenced to 15 years

Implications for Future Research
• Comparison study of CAC models – disclosure and recantation rates
• Prosecution rates using MDT • Revictimization rates• CAC’s impact on Non-Offending caregiver
(ability to protect)

References
• Cross, T.P. et al. (2008). Evaluating Children’s Advocacy Centers: Response to Child Sexual Abuse. Juvenile Justice Bulletin, No.218530. Washington, D.C. U.S. Department of Justice. Office of Juvenile Justice and Delinquency Prevention.
• Faller, K.C. & Palusci, V. J. (2007). Children’s Advocacy Centers: Do they lead to postive case outcomes? Invited Commentary. Child Abuse & Neglect, 31(10), 1021-1029.
• Wolfteich, P. & Loggins, B. (2007) Evaluation of the CAC Model: Efficiency, Legal and Revictimization Outcomes. Child and Adolescent Social Work Journal, 24(4), 333-352.