Surgical debulking of podoconiosis nodules and its impact ...
Upload
domenic-richardsCategory
view
219download
1
Conventional Stenting Following Predilation and/or Debulking Is Bett
er Than Direct Stenting
Myeong-Ki Hong, MD, PhDAsan Medical Center,
Seoul, Korea
Conventional stenting
vs. Direct stenting- Safety & Feasibility- Procedural data & Costs- Procedure-related complications- Long-term outcome- Case selections
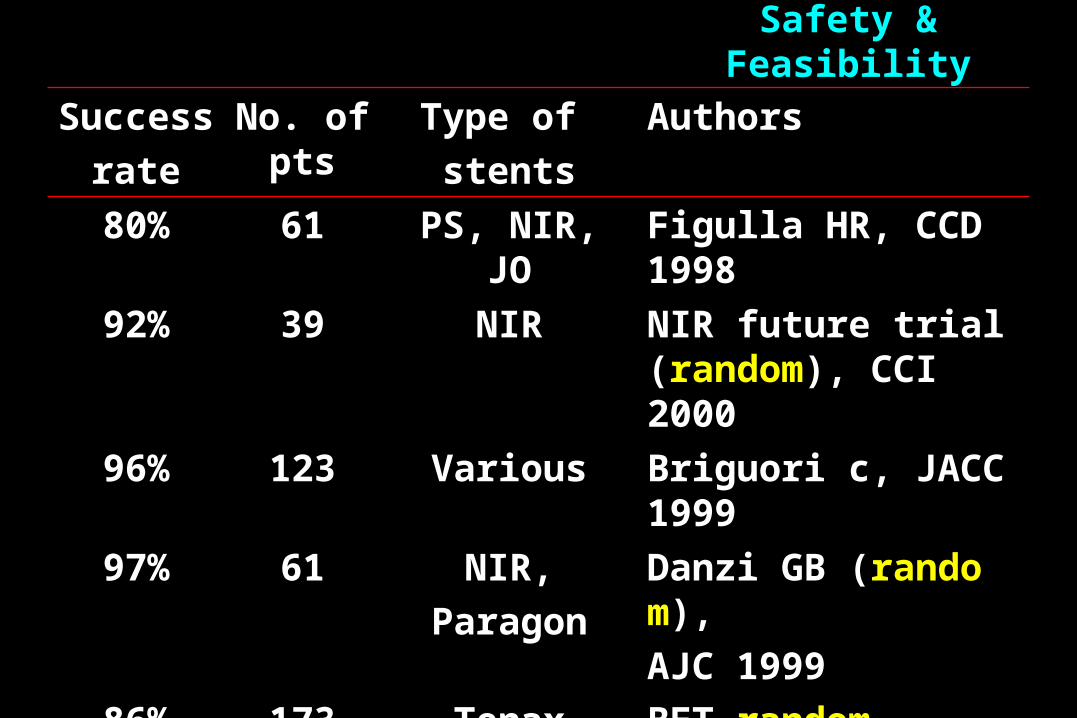
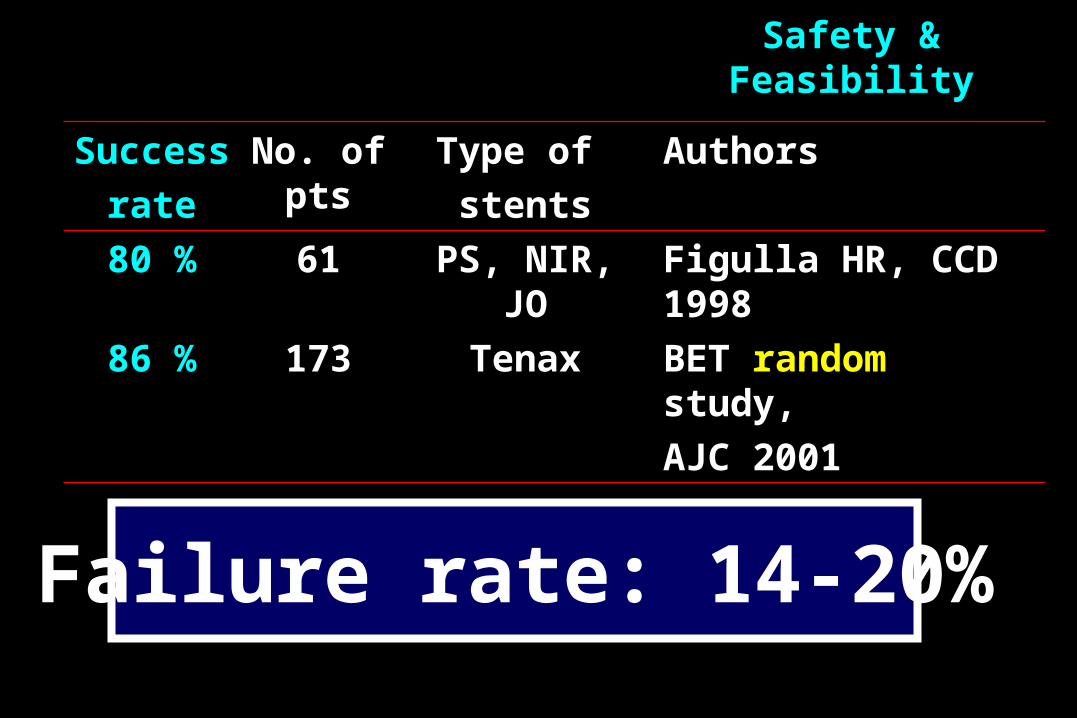
Safety & Feasibility
Success
rate
No. of pts
Type of
stents
Authors
80% 61 PS, NIR, JO Figulla HR, CCD 1998
92% 39 NIR NIR future trial (random), CCI 2000
96% 123 Various Briguori c, JACC 1999
97% 61 NIR,
Paragon
Danzi GB (random),
AJC 1999
86% 173 Tenax BET random study,
AJC 2001

Several studies reported that most cases in the failure of direct stenting was successfully treated after predilation without stent dislodgement & stent damage.
However, …….
Safety & Feasibility
Safety & Feasibility
Success
rate
No. of pts
Type of
stents
Authors
80 % 61 PS, NIR, JO Figulla HR, CCD 1998
86 % 173 Tenax BET random study,
AJC 2001
Failure rate: 14-20%
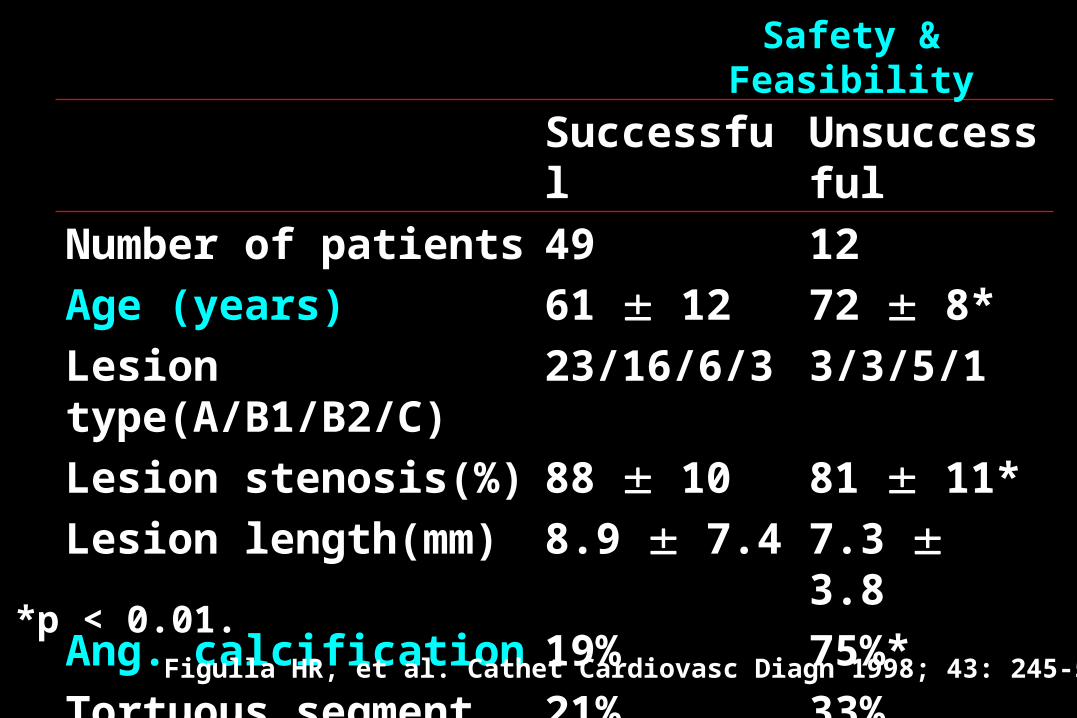
Successful Unsuccessful
Number of patients 49 12
Age (years) 61 12 72 8*
Lesion type(A/B1/B2/C) 23/16/6/3 3/3/5/1
Lesion stenosis(%) 88 10 81 11*
Lesion length(mm) 8.9 7.4 7.3 3.8
Ang. calcification 19% 75%*
Tortuous segment 21% 33%
*p < 0.01.
Safety & Feasibility
Figulla HR, et al. Cathet Cardiovasc Diagn 1998; 43: 245-52
Stent dislocationFigulla HR, et al. (Cathet Cardiovasc Diagn 1998; 43: 24
5-52)
3 of 61 cases, PS stents2 calcified lesions & 1 extremely tortuous lesion
Manually crimped bare slotted-tube stents on low-profile dilatation balloons
Coil-type stents
Safety & Feasibility
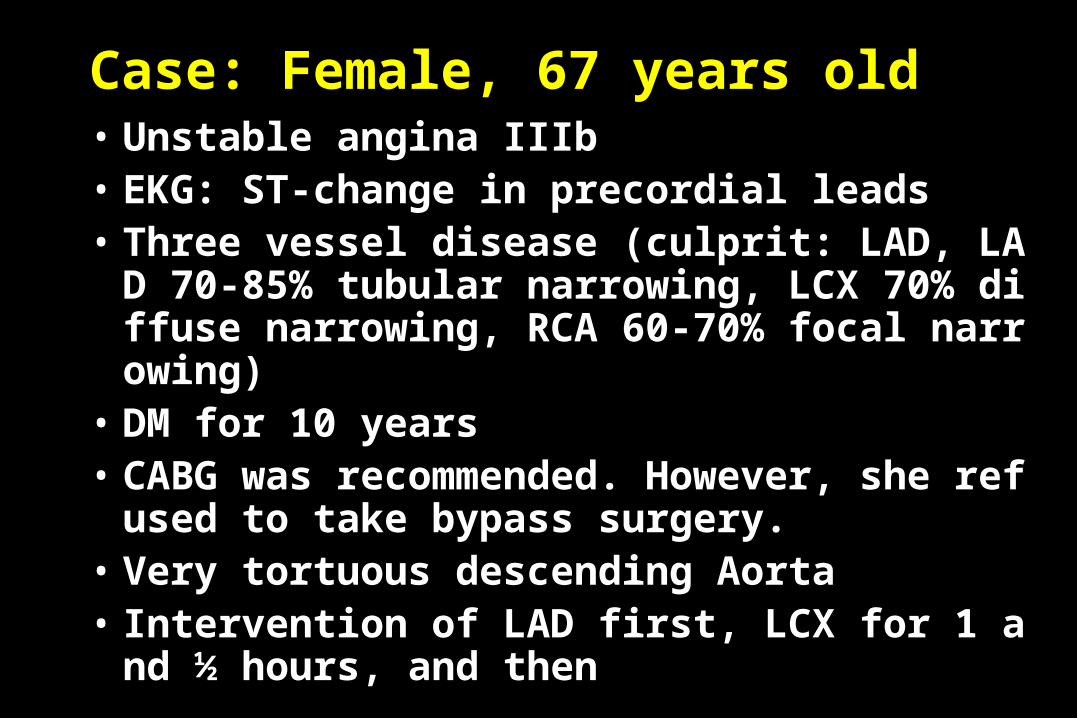
Case: Female, 67 years old• Unstable angina IIIb• EKG: ST-change in precordial leads• Three vessel disease (culprit: LAD, LAD 70-85%
tubular narrowing, LCX 70% diffuse narrowing, RCA 60-70% focal narrowing)
• DM for 10 years• CABG was recommended. However, she refused t
o take bypass surgery.• Very tortuous descending Aorta• Intervention of LAD first, LCX for 1 and ½ hour
s, and then
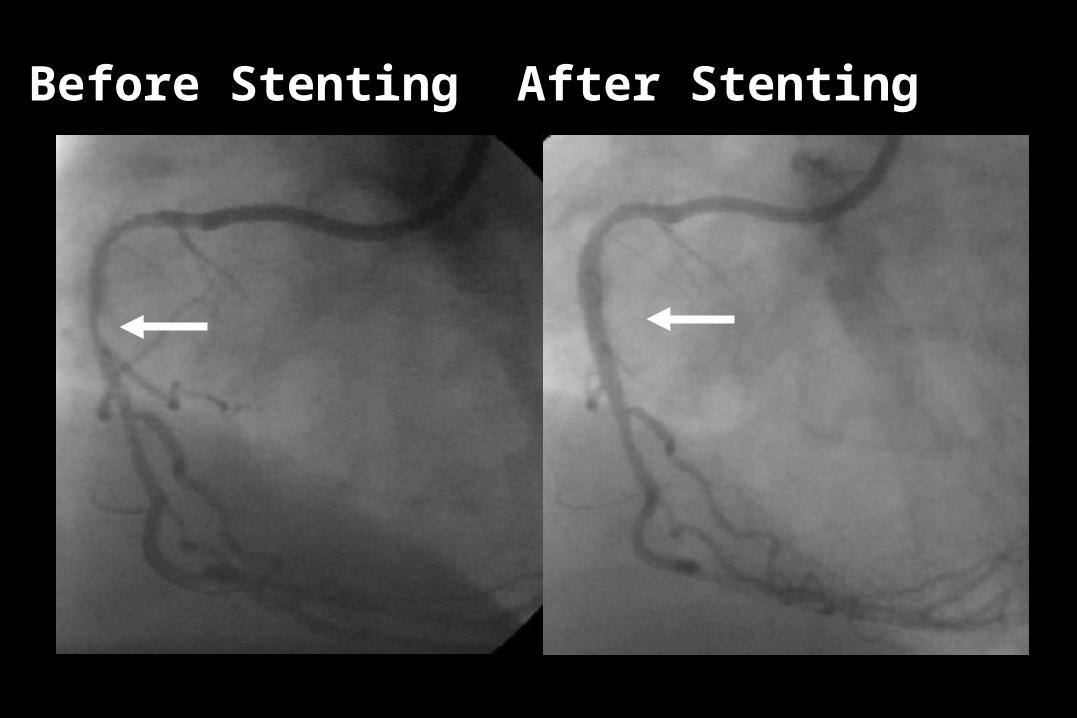
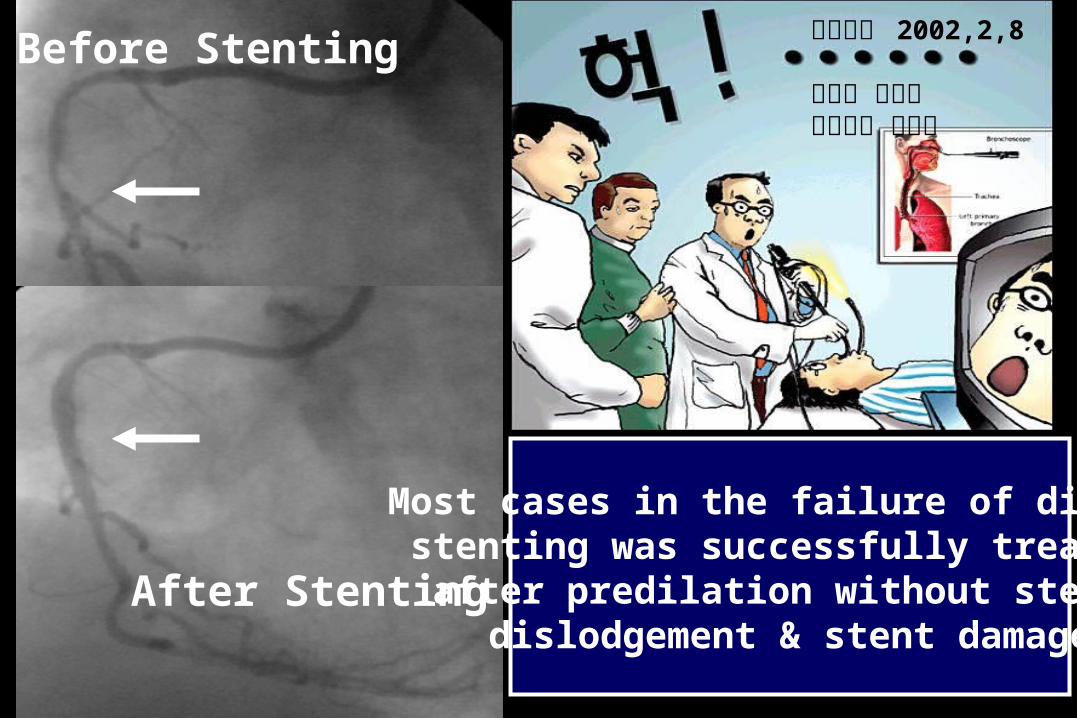
Before Stenting After Stenting
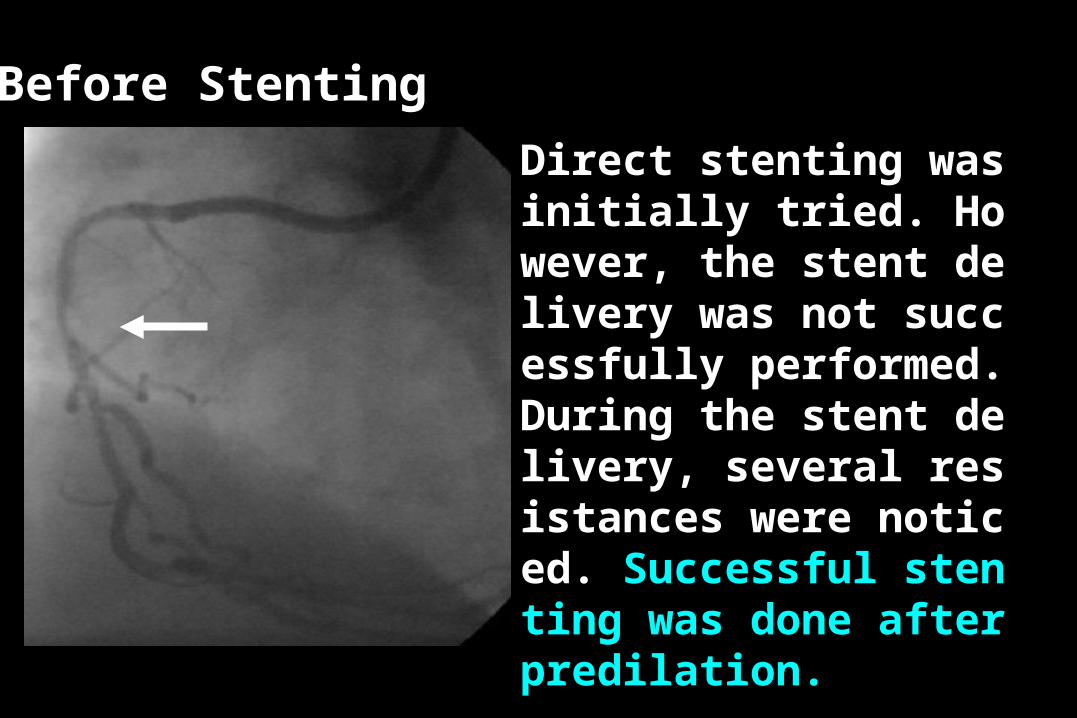
Before Stenting
Direct stenting was initially tried. However, the stent delivery was not successfully performed. During the stent delivery, several resistances were noticed. Successful stenting was done after predilation.
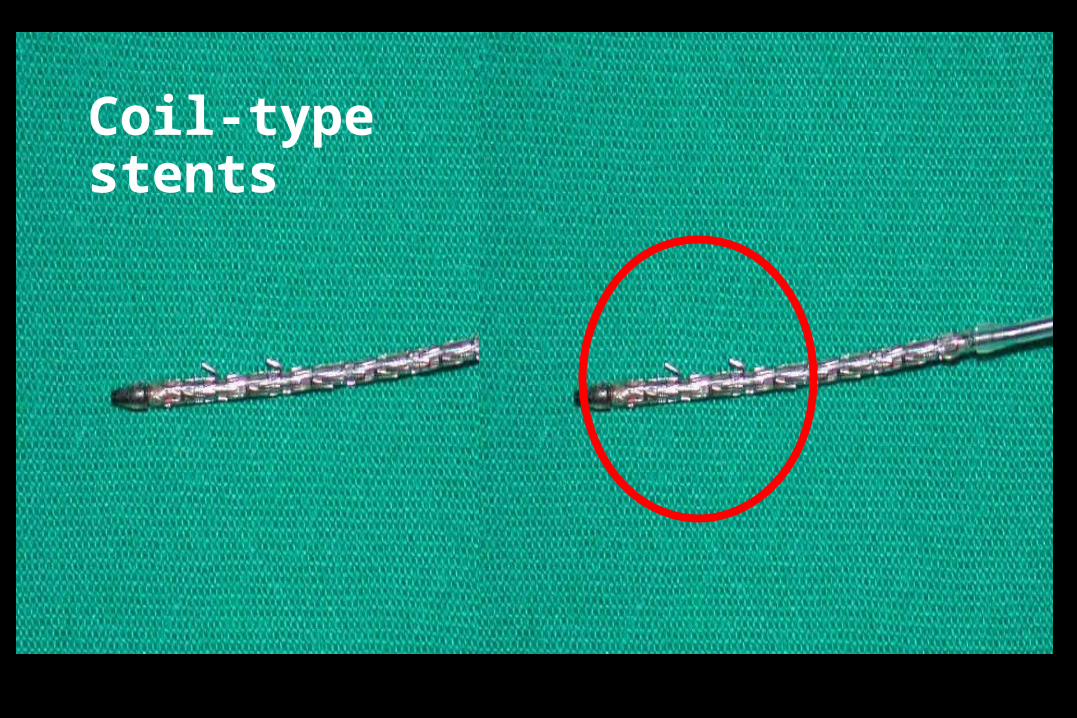
Coil-type stents
Before Stenting
After Stenting
조선일보 2002,2,8
진료실 엿보기내과의사 박성진
Most cases in the failure of direct stenting was successfully treated after predilation without stent dislodgement & stent damage
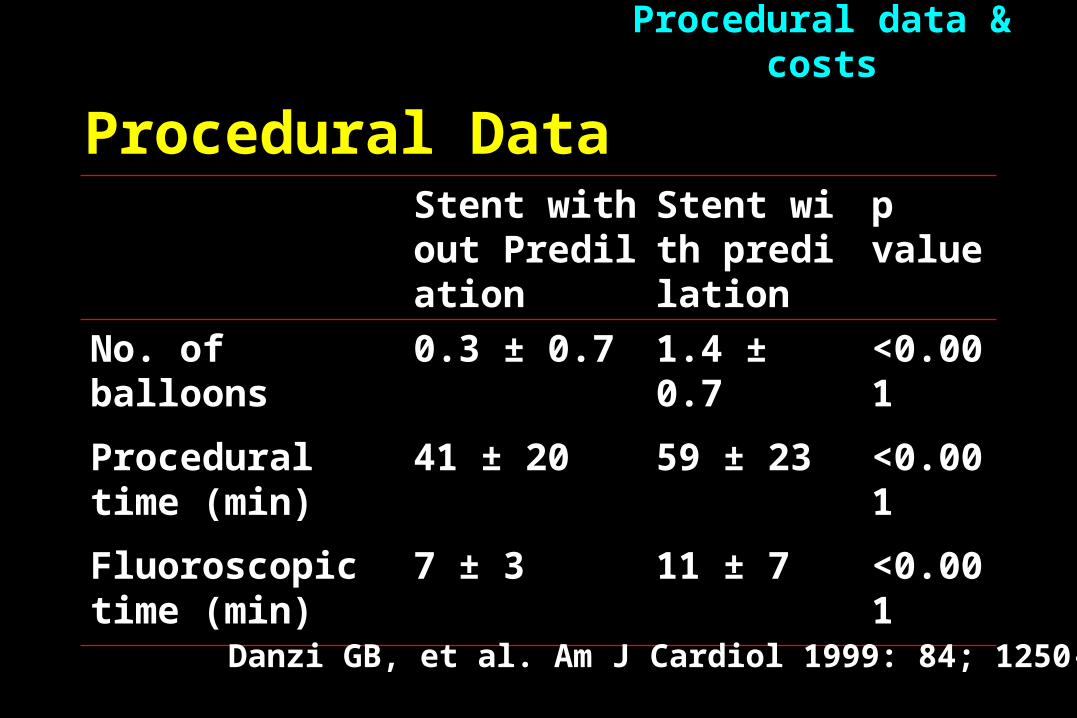
Procedural Data
Stent without Predilation
Stent with predilation
p value
No. of balloons 0.3 ± 0.7 1.4 ± 0.7 <0.001
Procedural time (min)
41 ± 20 59 ± 23 <0.001
Fluoroscopic time (min)
7 ± 3 11 ± 7 <0.001
Procedural data & costs
Danzi GB, et al. Am J Cardiol 1999: 84; 1250-53
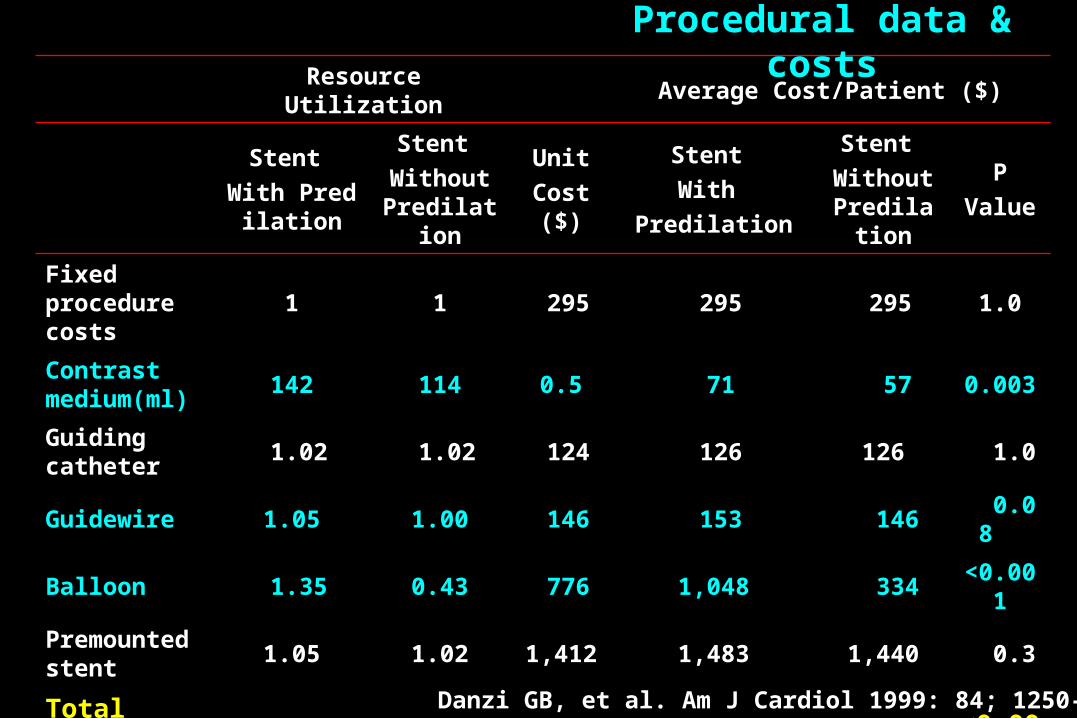
Resource Utilization Average Cost/Patient ($)
Stent
With Predilation
Stent
Without Predilation
Unit
Cost ($)
Stent
With
Predilation
Stent
Without Predilation
P
Value
Fixed procedure costs
1 1 295 295 295 1.0
Contrast medium(ml)
142 114 0.5 71 57 0.003
Guiding catheter
1.02 1.02 124 126 126 1.0
Guidewire 1.05 1.00 146 153 146 0.08
Balloon 1.35 0.43 776 1,048 334 <0.001
Premounted stent
1.05 1.02 1,412 1,483 1,440 0.3
Total procedure costs
3,176 2,398 <0.001
Procedural data & costs
Danzi GB, et al. Am J Cardiol 1999: 84; 1250-53
Procedure-related complications- Post-stent dissection
- Additional stent implantation
- Distal embolization
- No reflow
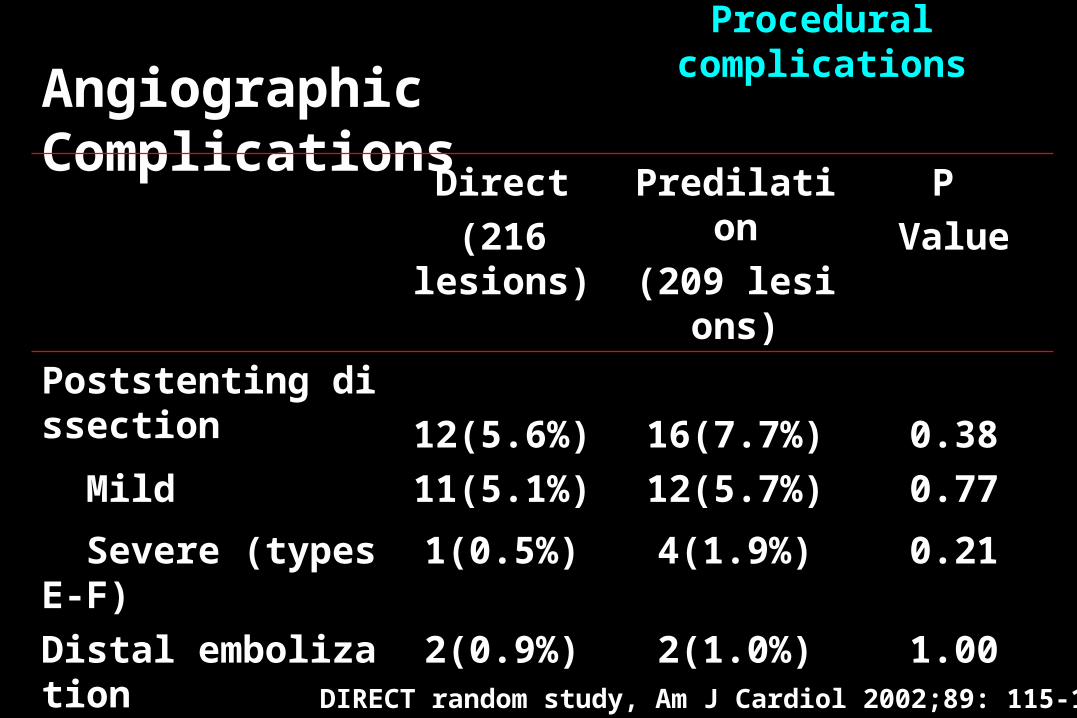
Angiographic Complications
Direct
(216 lesions)
Predilation
(209 lesions)
P
Value
Poststenting dissection 12(5.6%) 16(7.7%) 0.38
Mild 11(5.1%) 12(5.7%) 0.77
Severe (types E-F) 1(0.5%) 4(1.9%) 0.21
Distal embolization 2(0.9%) 2(1.0%) 1.00
No-reflow 4(1.9%) 3(1.4%) 0.96
Procedural complications
DIRECT random study, Am J Cardiol 2002;89: 115-120
52 세 남자 환자가 내원 3시간 전 부터 안정시 발생한 흉통을 주소로 응급실에 내원하였다 . 과거력상 2년전에 운동시 발생하는 2분간의 흉통으로 개인의원에서 협심증으로 진단을 받았고 , 그 후 지속적으로 항협심증 제제를 복용하였다고 하였다 .
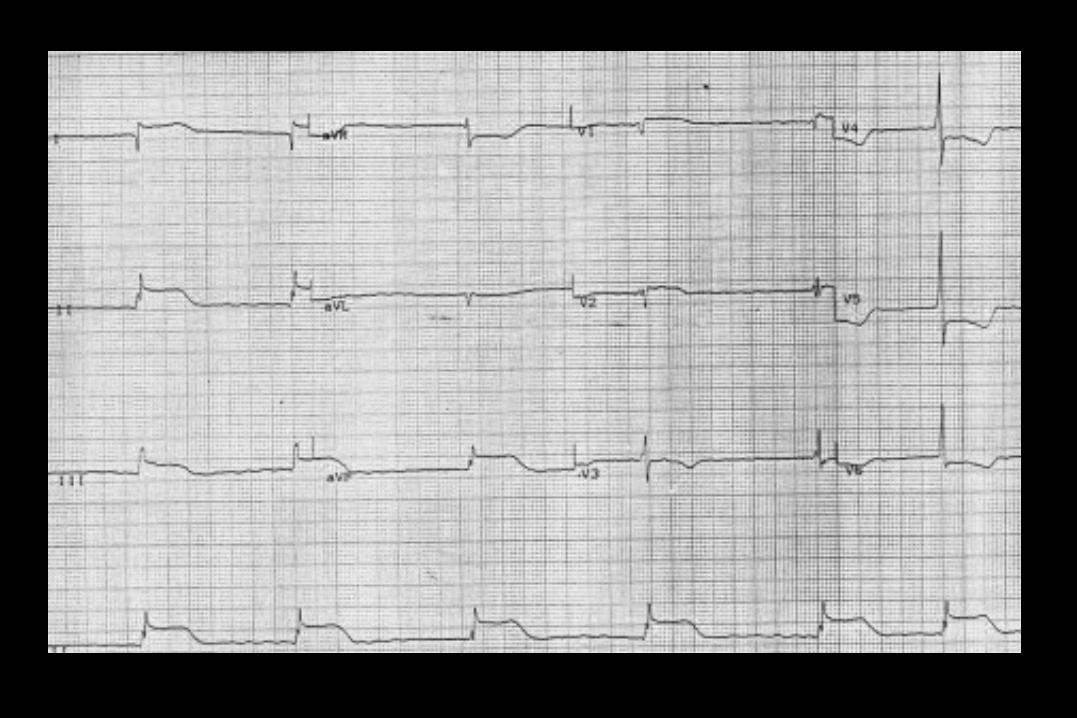
내원 당일 흉통은 안정시 발생하였으며 , 3 시간 동안 지속되었다 . 응급조치로서 sublingual NTG 를 3회 반복 투여하였으나 증상의 호전이 없어서 응급실에 내원하였다 . 내원 당시 혈압은 100/70mmHg 이었으며 , 심전도 소견은 다음과 같았다 .
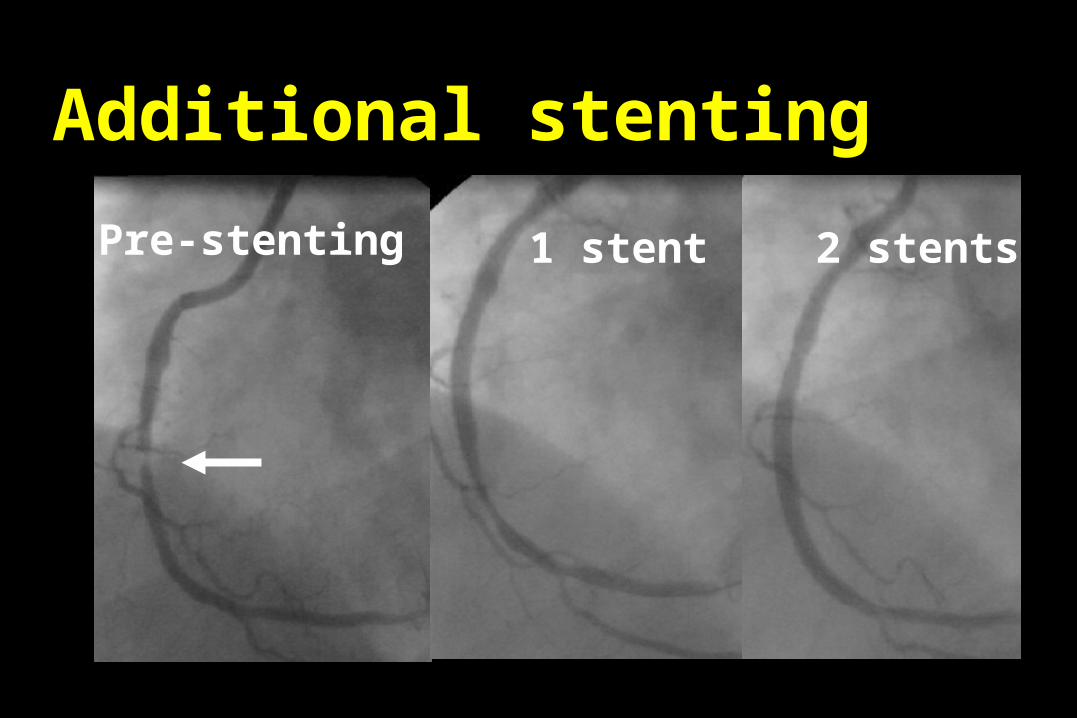
Pre-stenting 1 stent 2 stents
Additional stenting
Pre-stenting 2 stents
하나 더 !I will NEVER do direct stenting again.
조선일보 2002,3, 진료실 엿보기내과의사 박성진
?
Role of IVUS in Direct
Stenting
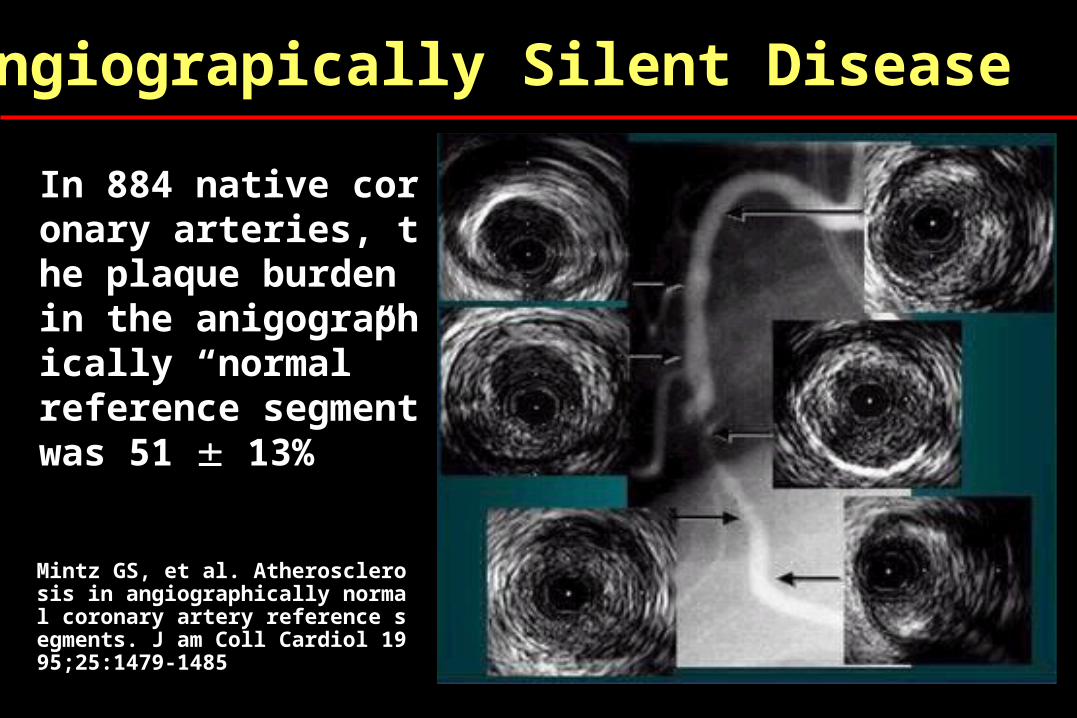
Angiograpically Silent Disease
In 884 native coronary arteries, the plaque burden in the anigographically “normal”reference segment was 51 13%
Mintz GS, et al. Atherosclerosis in angiographically normal coronary artery reference segments. J am Coll Cardiol 1995;25:1479-1485
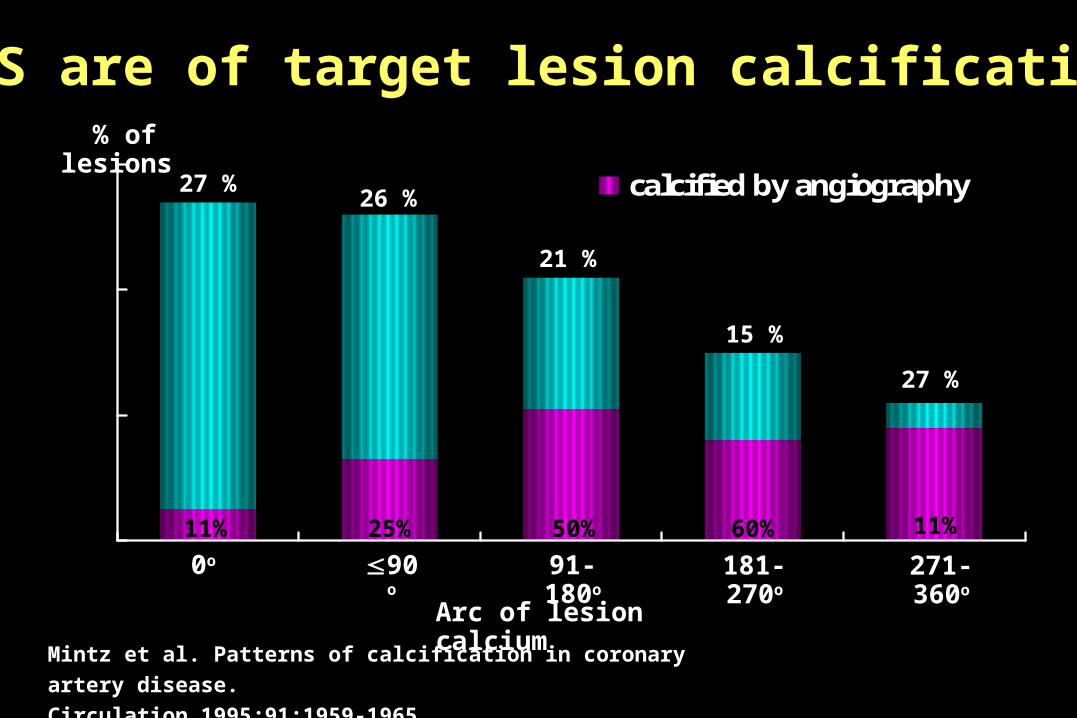
IVUS are of target lesion calcification
Mintz et al. Patterns of calcification in coronary artery disease.
Circulation 1995;91:1959-1965.
calcified by angiography
Arc of lesion calcium
0o 90o 91-180o 181-270o 271-360o
% of lesions
27 %
11%
26 %
25%
21 %
50%
15 %
60%
27 %
11%
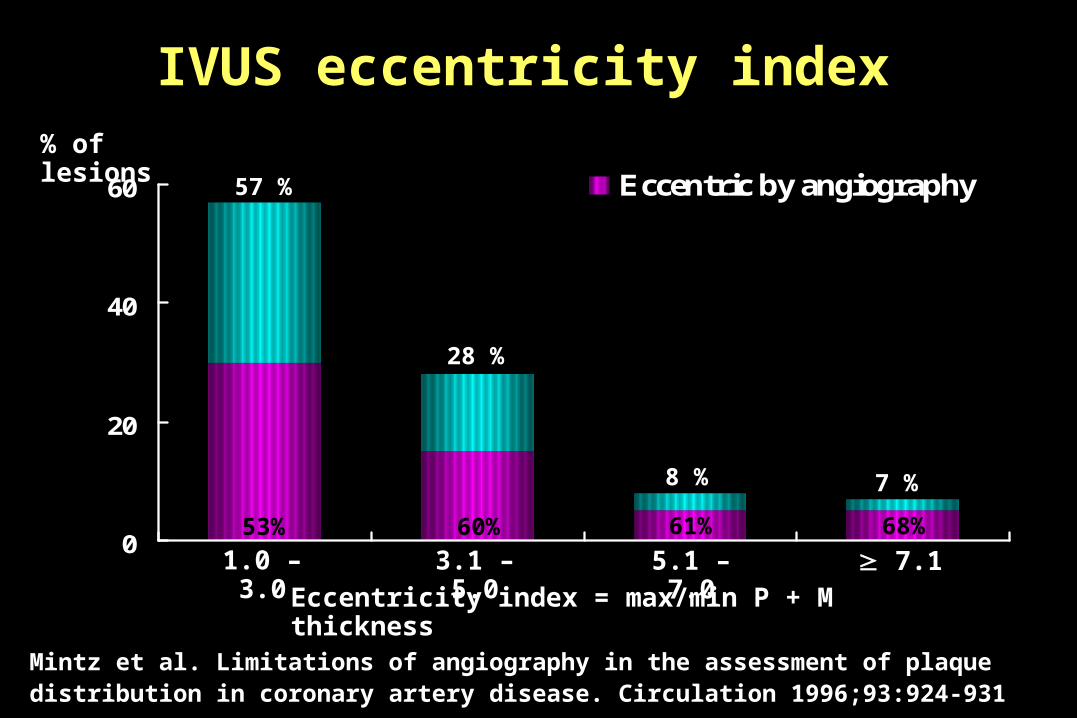
IVUS eccentricity index
Mintz et al. Limitations of angiography in the assessment of plaque distribution in coronary artery disease. Circulation 1996;93:924-931
0
20
40
60 Eccentric by angiography
Eccentricity index = max/min P + M thickness
1.0 – 3.0 3.1 – 5.0 5.1 – 7.0 7.1
57 %
53%
28 %
60%
8 %
61%
7 %
68%
% of lesions
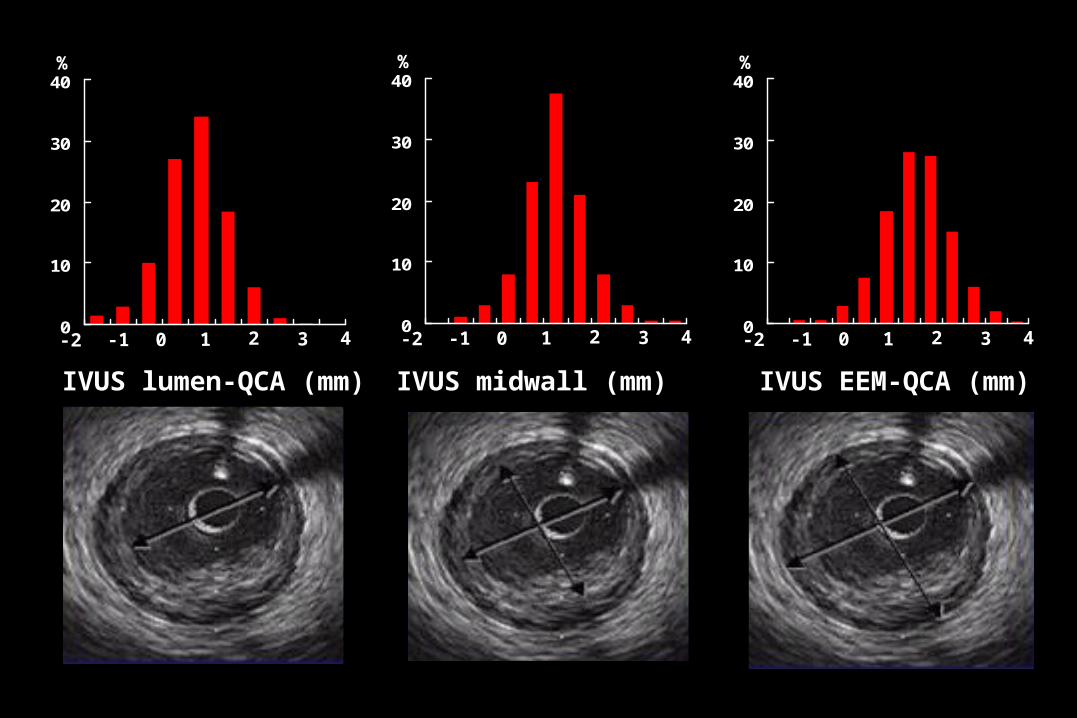
IVUS lumen-QCA (mm) IVUS midwall (mm) IVUS EEM-QCA (mm)
0
10
20
30
40
-2 -1 0 1 42 3
%
0
10
20
30
40
-2 -1 0 1 42 3
%
0
10
20
30
40
-2 -1 0 1 42 3
%
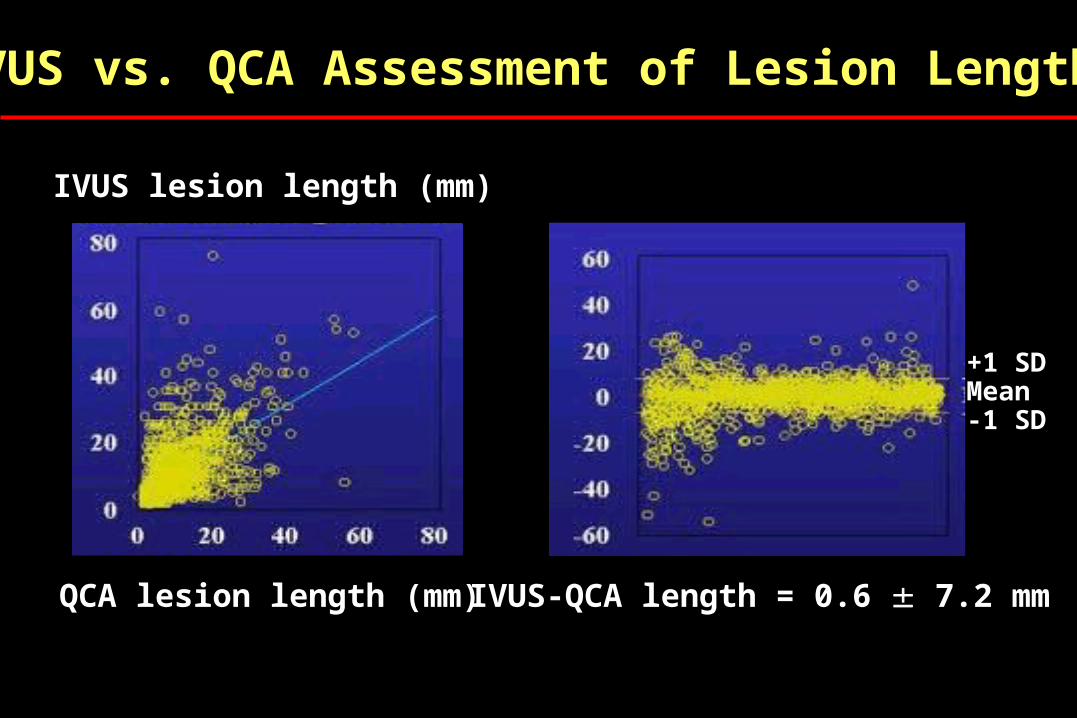
IVUS vs. QCA Assessment of Lesion Length
IVUS lesion length (mm)
QCA lesion length (mm) IVUS-QCA length = 0.6 7.2 mm
+1 SDMean-1 SD
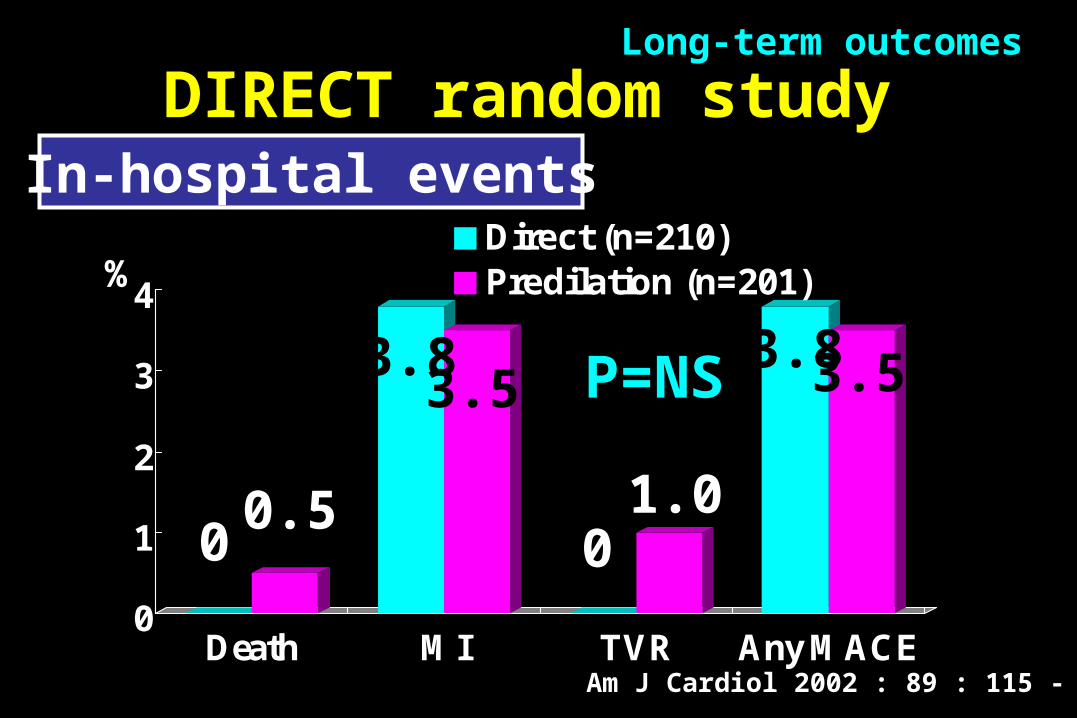
DIRECT random study
0
1
2
3
4
Death MI TVR Any MACE
Direct (n=210)Predilation (n=201)
0.50 0
3.83.5 3.5
1.0
3.8P=NS
%
Am J Cardiol 2002 : 89 : 115 - 120
Long-term outcomes
In-hospital events
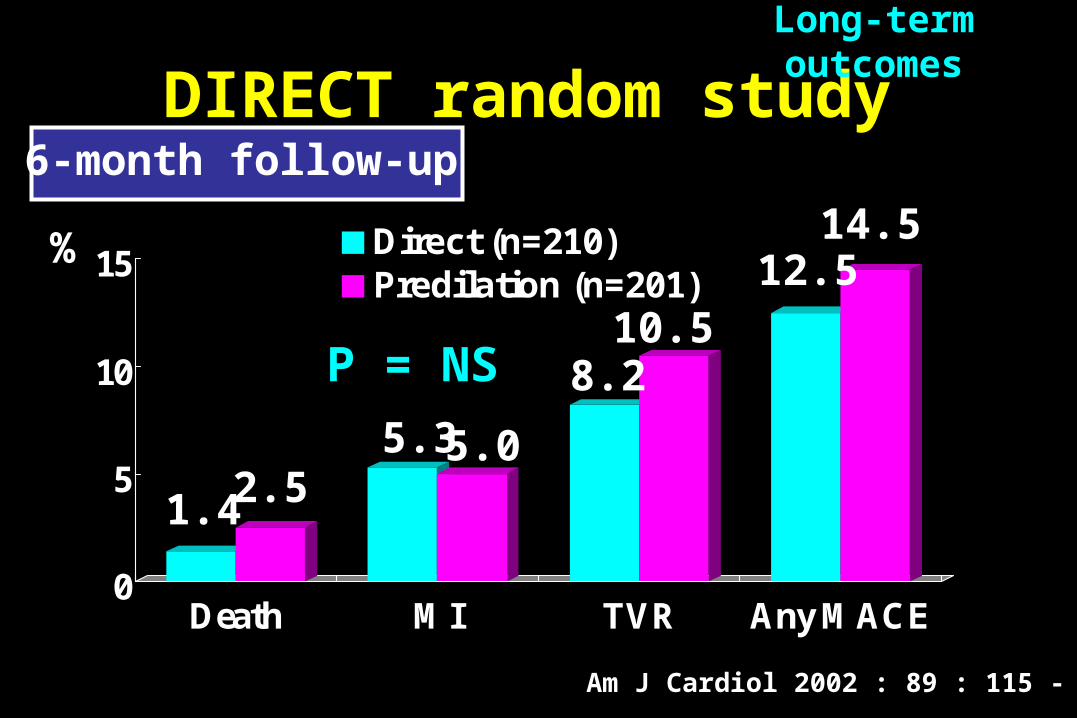
0
5
10
15
Death MI TVR Any MACE
Direct (n=210)Predilation (n=201)
2.51.4
8.2
14.5
10.512.5
P = NS
5.3 5.0
%
DIRECT random study
Long-term outcomes
Am J Cardiol 2002 : 89 : 115 - 120
6-month follow-up
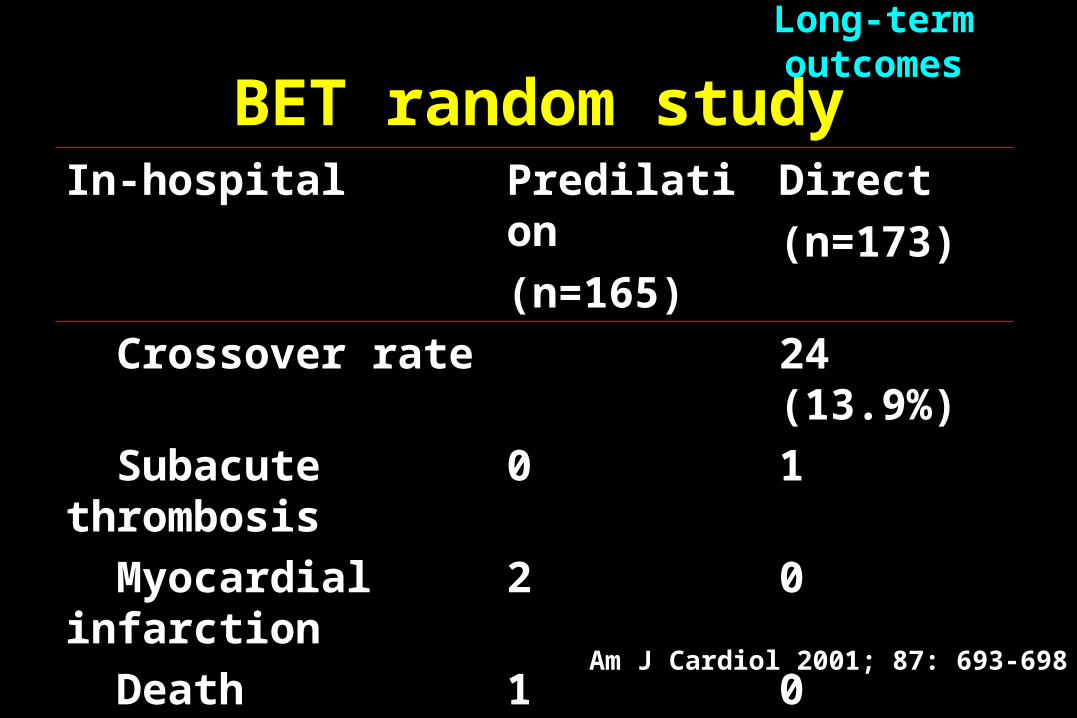
BET random studyIn-hospital Predilation
(n=165)
Direct
(n=173)
Crossover rate 24 (13.9%)
Subacute thrombosis 0 1
Myocardial infarction
2 0
Death 1 0
Hematoma 1 2
Clinical success (%) 97.5 98.3
P=NS
Long-term outcomes
Am J Cardiol 2001; 87: 693-698
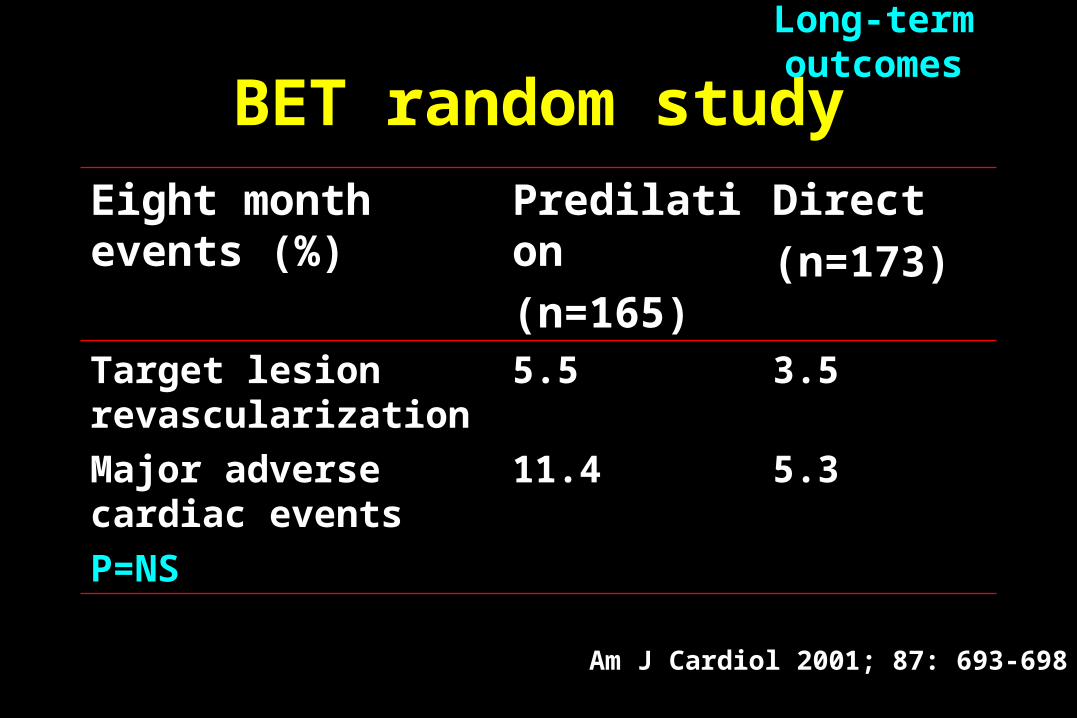
Eight month events (%)
Predilation
(n=165)
Direct
(n=173)Target lesion revascularization
5.5 3.5
Major adverse cardiac events
11.4 5.3
P=NS
BET random studyLong-term outcomes
Am J Cardiol 2001; 87: 693-698
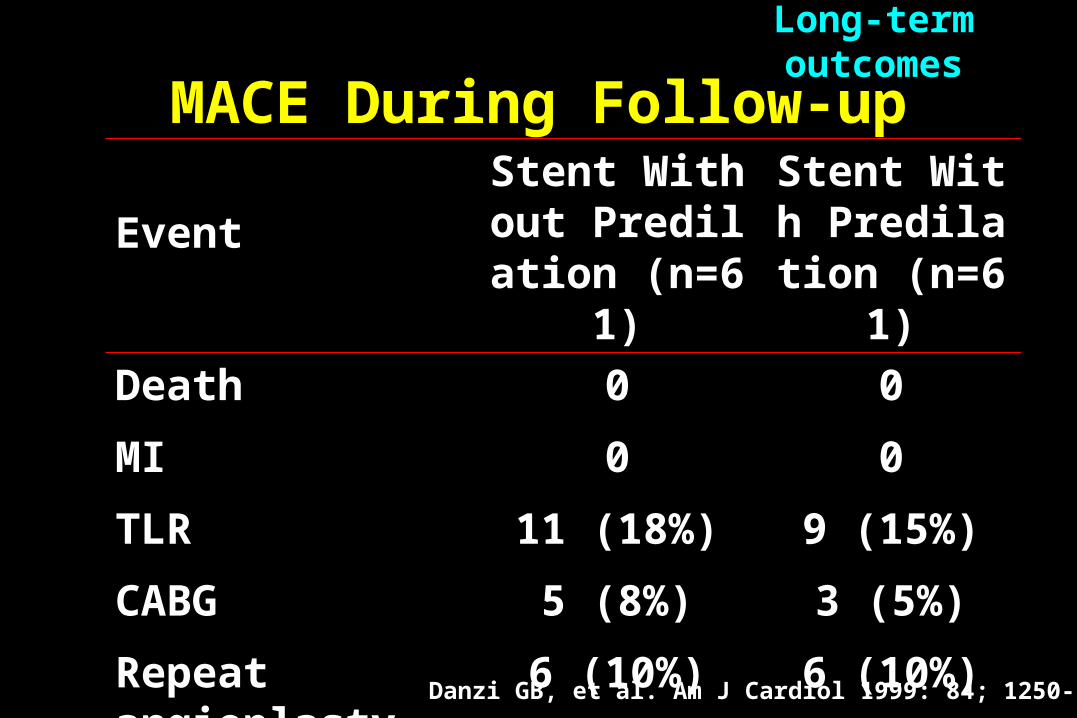
MACE During Follow-up
Event
Stent Without Predilation (n
=61)
Stent With Predilation (n
=61)
Death 0 0
MI 0 0
TLR 11 (18%) 9 (15%)
CABG 5 (8%) 3 (5%)
Repeat angioplasty 6 (10%) 6 (10%)
Long-term outcomes
Danzi GB, et al. Am J Cardiol 1999: 84; 1250-53
Case SelectionPossible inappropriate lesions for direct stenting1. Long lesion2. Presence of severe calcium by fluoroscopy3. Total occlusion4. Inadequate positioning of the stent due to severe ste
nosis impairment of distal coronary flow5. Significant angulation(bend > 45°)6. Bifurcation lesion7. Severe tortuosity of the vessel proximal to the target
segment8. Poor guiding catheter beck-up support
Major disadvantage of direct stenting
1. Potential failure to cross the stenosis with stent
2. Potential risk of encountering an undilatable lesion
Case selection
The case selection must be the most important
factor for direct stenting
Case selection
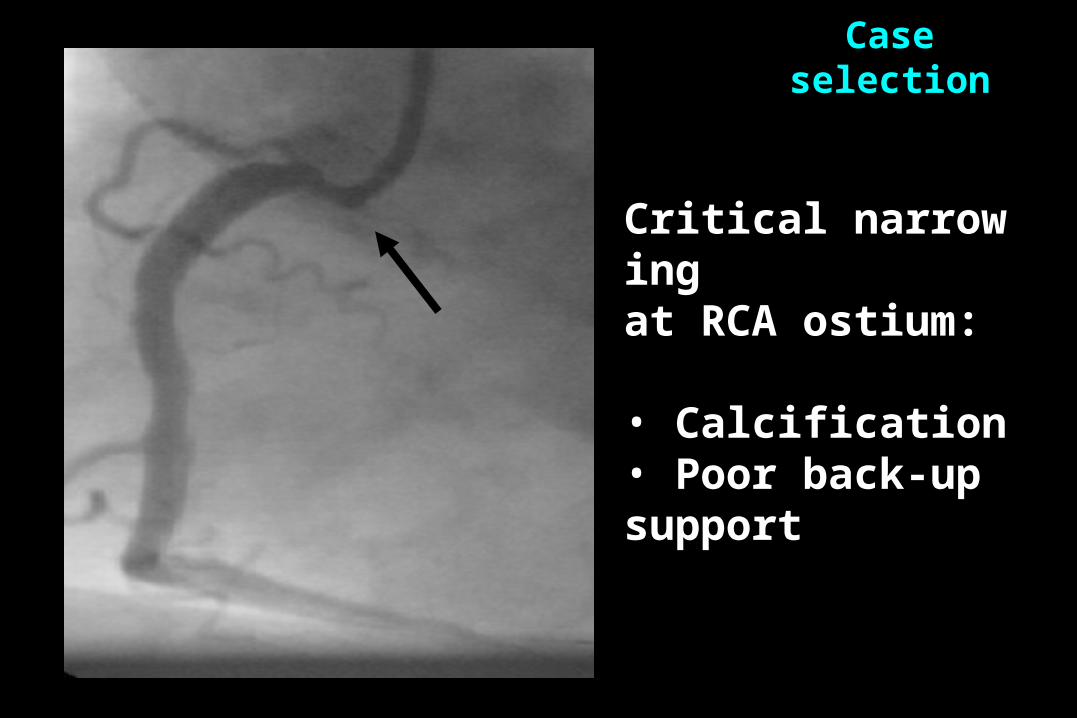
Critical narrowing at RCA ostium:
• Calcification• Poor back-up support
Case selection
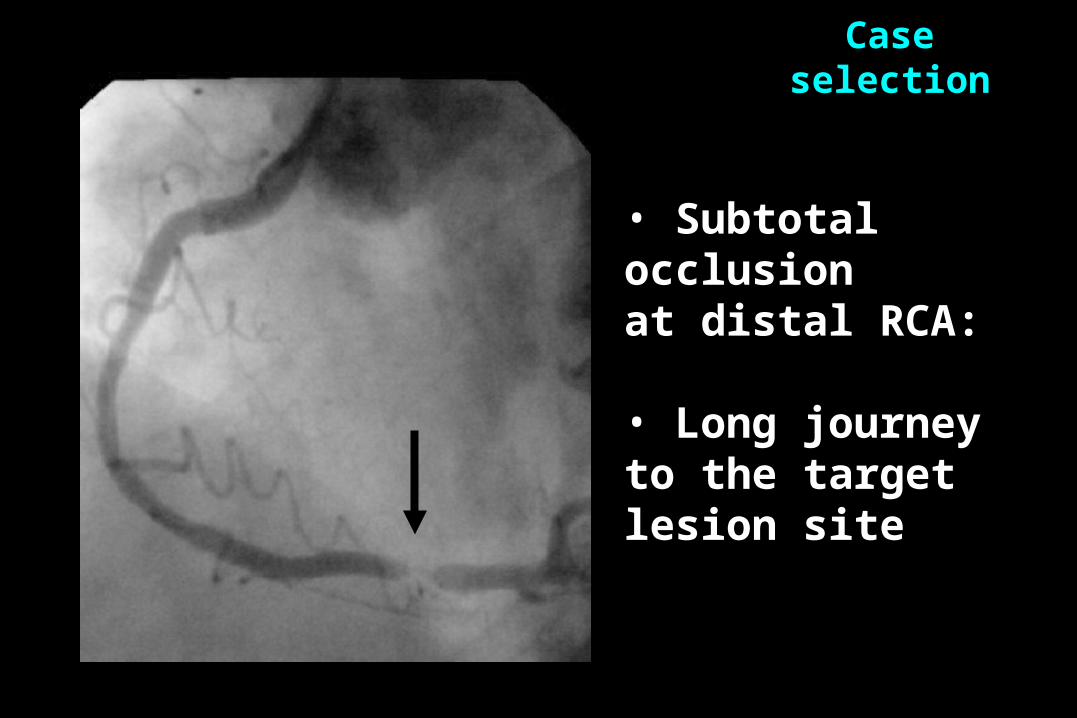
• Subtotal occlusion at distal RCA:
• Long journey to the target lesion site
Case selection
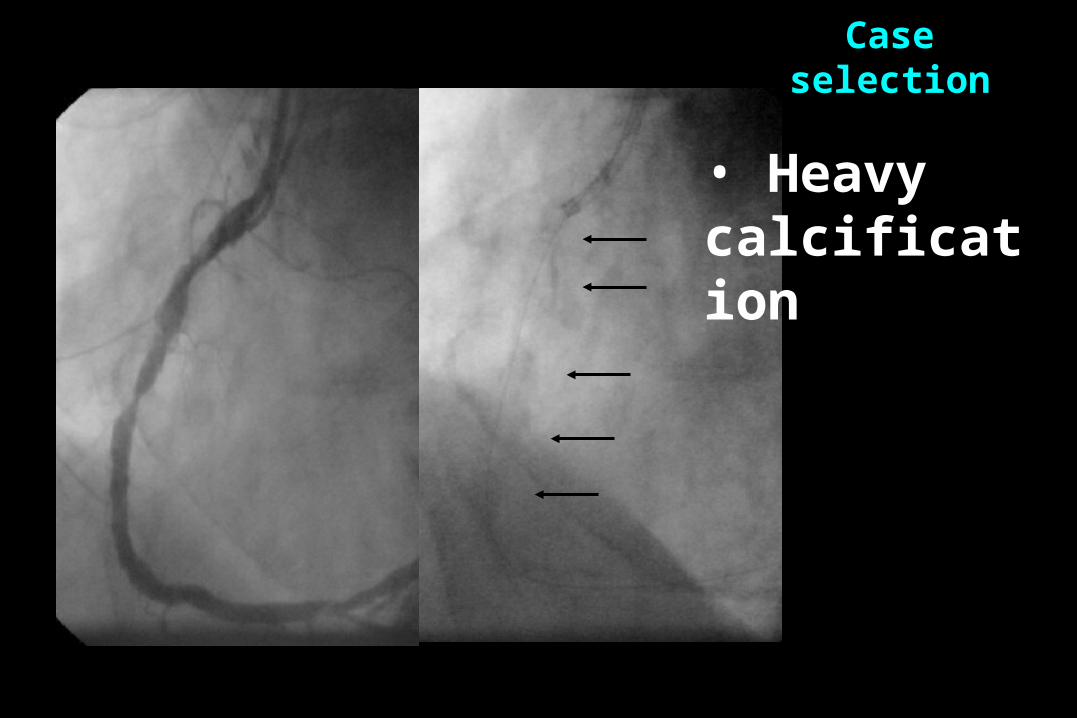
• Heavy calcification
Case selection
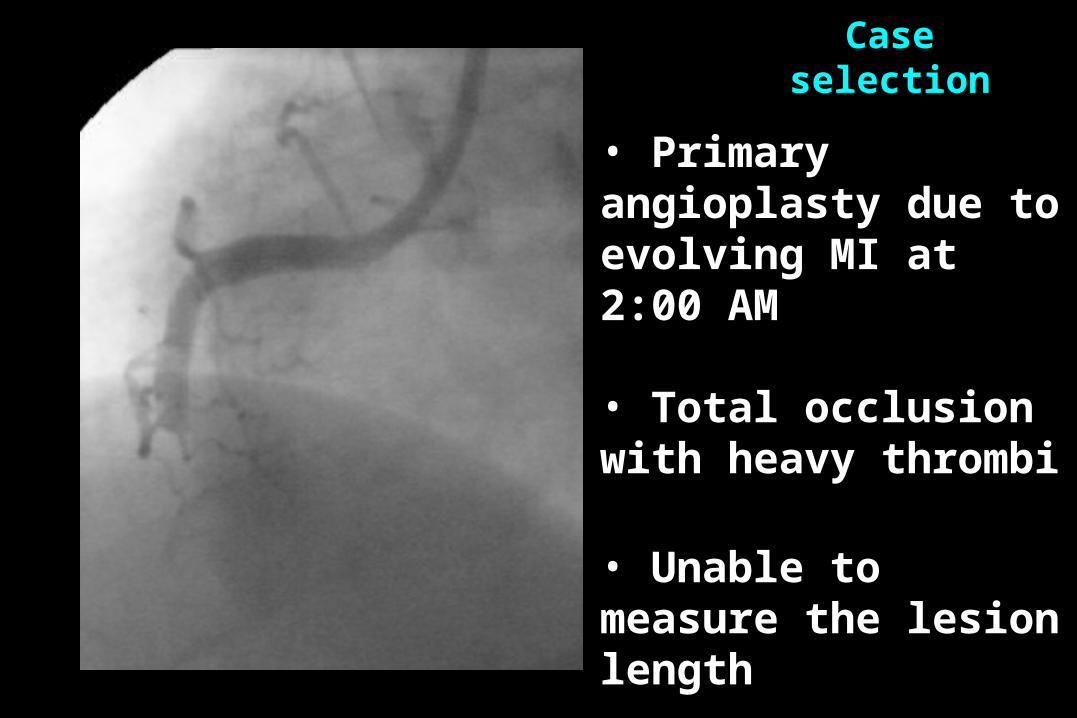
• Primary angioplasty due to evolving MI at 2:00 AM
• Total occlusion with heavy thrombi
• Unable to measure the lesion length
Case selection
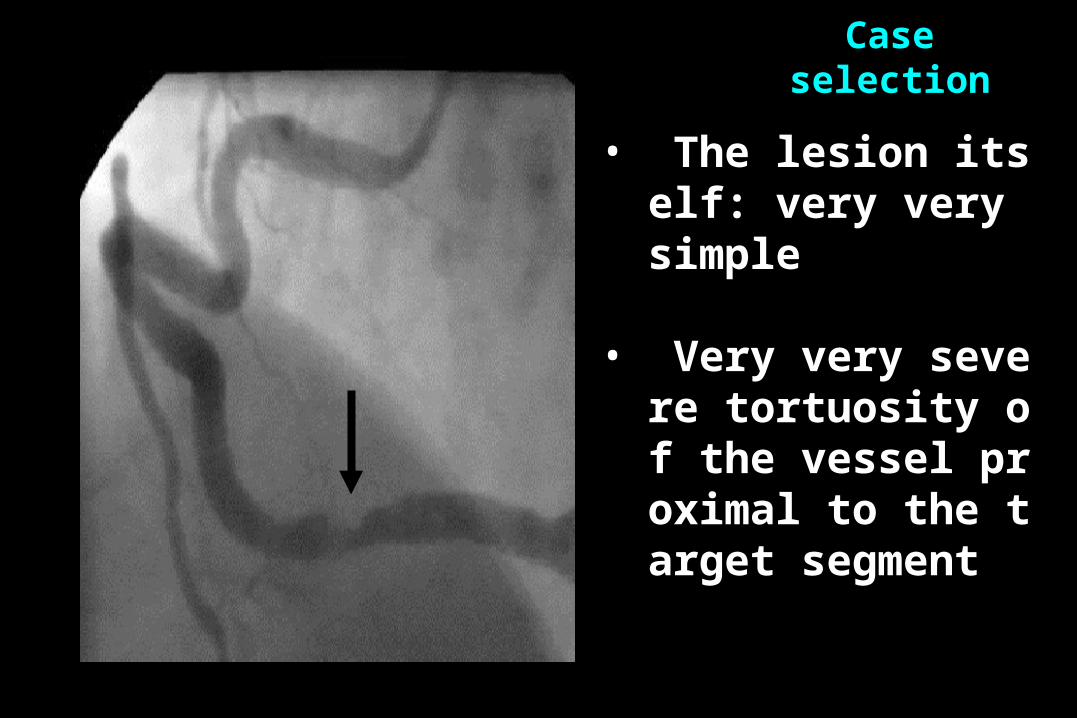
• The lesion itself: very very simple
• Very very severe tortuosity of the vessel proximal to the target segment
Case selection
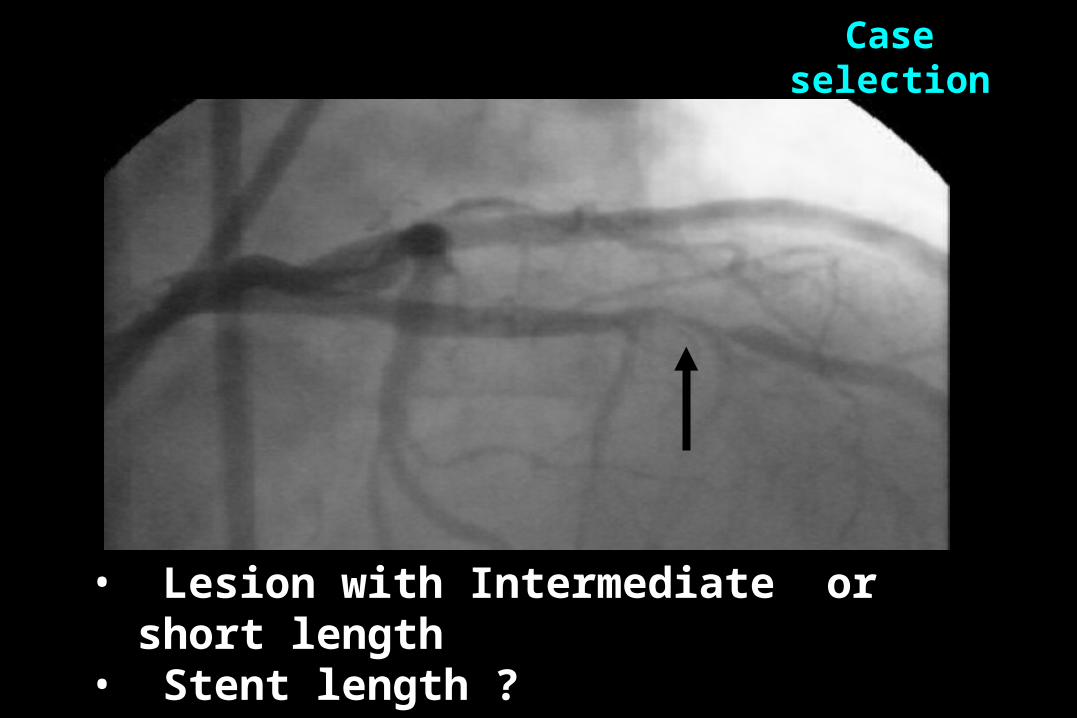
• Lesion with Intermediate or short length• Stent length ?
Case selection
치료 전 치료 후
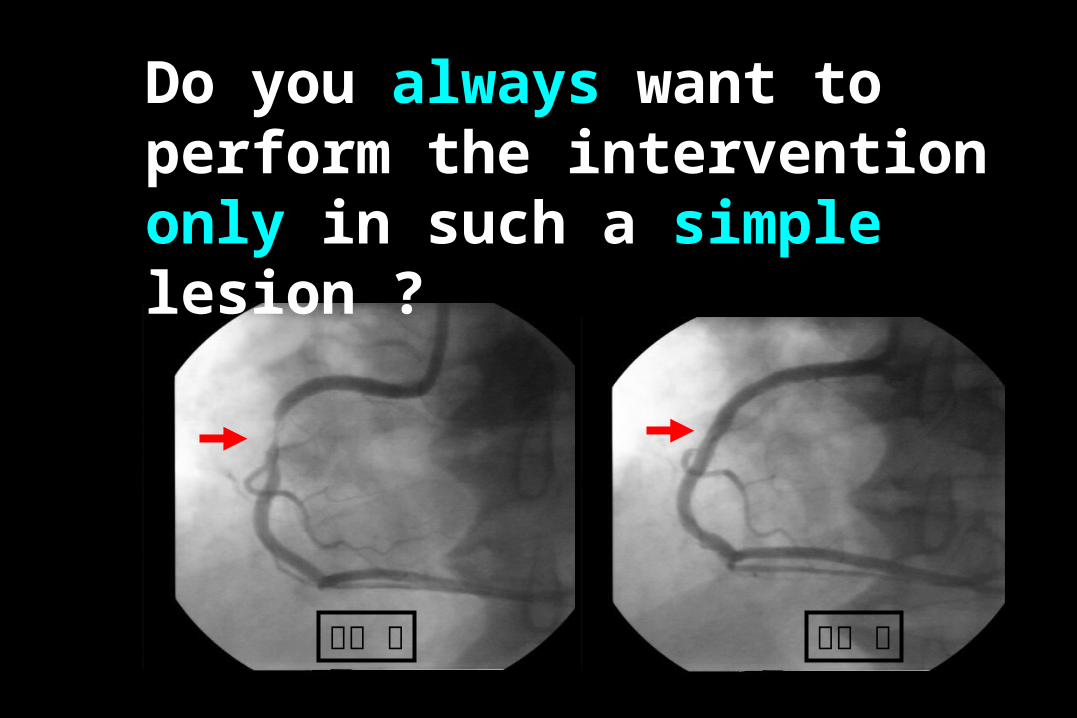
Do you always want to perform the intervention only in such a simple lesion ?
Heart
Liverspleen
간 빼고 , 쓸개 빼고 ,
뺀 김에 심장도 빼고나면
남는 것은 ?
Simple lesion Lipid Tx
CABG
?
Therefore, conventional stenting following predilation is better t
han direct stenting.