Convention Modes of Mechanical Ventilation. DR.purwOKO
53
Convention Modes of Mechanical Ventilation Purwoko SMF Anestesiologi & Terapi Intensif RSUD Dr. Moewardi
-
Upload
isnia-wahib -
Category
Documents
-
view
89 -
download
4
description
ventilator
Transcript of Convention Modes of Mechanical Ventilation. DR.purwOKO

Convention Modes of Mechanical Ventilation
PurwokoSMF Anestesiologi & Terapi
IntensifRSUD Dr. Moewardi

2
PRESSURE
TIME
Inspirasi Ekspirasi
PLATEAU PRESSURE
PEAK PRESSURE
0
KURVA NAFAS SPONTAN DAN VENTILASI MEKANIK

Respiratory Failure
• Tipe 1 : gagal nafas oksigenasi : Lung failure• Tipe 2 : gagal nafas ventilasi : Pump failure• Kombinasi tipe 1 dan 2• PaO2 < 60 mmHgdengan FiO2 60%
PaCo2 > 50 – 55 mmHgKecuali : alkalosis metabolik terkompensasi PPOK Shunting intrakardiak Aklimatisasi High altitude

Penanggulangan gagal nafas
Gagal nafas mengancam, Gagal nafas akut, Gagal
nafas mengancam nyawa?
Terapi oksigen : kanul, simple-mask, rbm, non-
rbm ventimask
Kausal (?) : antidotum
NIPPV
IPPV

IPPV
Terapi supportif (airway-pressure therapy)
Udara masuk karena ada perbedaaan tekanan
Diberikan sejumlah volume
Tekanan
Ada hubungan antara tekanan dan volume
P-V relationship : static mechanics
Ada hubungan antara tekanan dan flow :
dynamic mechanics

IPPV beberapa mode of ventilation
Conventional (primary)
modes
Dual – control modes
Biphasic pressure modes

Prinsip Kerja Ventilator (umum)
Pneumatik/ mekanik
Sumber gas : Oksigen dan compressed air
Katub inspirasi, katub ekspirasi, sirkuit ventilator
Elektronik/ mikroprosesor
Sistem kontrol, panel kontrol, monitor dan alarm
Sistem untuk sinkronisasi ventilator - pasien

Sumber Gas Ventilator
Suplai Sentral atau Lokal
Oksigen (penuh 130 atm, 1990 – 2200 psi)
Udara tekan (compression air)
Oxygen – Air mix (Blender) mengatur FiO2
Reducing valve outlet 45 – 55 psi
Working pressure 40 – 60 psi

Kondisi Gas Inspirasi
Harus cukup hangat (370 C)
Harus cukup lembab
1. Heat moisture exchanger (HME) : di Y-piece
Kendala HME : dead space , resistensi ,
hipotermia, air leaks, Vt sangat besar, sekret >>,
CO2 (k.i)
2. Heated humidifier (di dalam jalur inspirasi)
Dead space tak , Resistensi tak

Sistem Kontrol
Modus ventilasi mekanik ditentukan oleh kontrol
:
Fungsi awal inspirasi (Initiation / Trigger)
Akhir inspirasi (Limit / Target)
Awal ekspirasi (Cycle off)

Initiation / Trigger
• Control breath machine – triggered (time –
based)
• Assisted breath patient – triggered
Pressure – trigger (-2 cmH2O)
Flow – trigger (fixed, adjusted, flow by)
Cegah : *self – cycling auto triggering
*respons delay
Limit / Target
Dipakai untuk memberi nama Mode Target volume Volume control Target tekanan Pressure control
Target volume awasi pressureTarget pressure awasi volume
Faktor yang mempengaruhi target : resistesi tube, jalan nafas, compliance, aktifitas muskular, PEEPi

Cycle off
Target ditentukan oleh : volume (tidal volume)
dan pressure (airway pressure)
Cycle off ditentukan oleh :
Elapse time
Inspiratory flow rate
Target dan cycle off dapat saling terkait

Cycle off
Time-based cyclingDipakai pada : controlled atau assist – controlSetting Ti:
*langsung (sekian detik)*berdasar kombinasi f dan I:R ratio*berdasar peak flow rate dan volume tidal Flow-based cyclingDipakai pad: assist-spontaneous, fully spontaneousExpiratory trigger sensitivity : nilai absolut, 25%
dari peak flow rate, dapat diatur

Conventional mode of mechanical ventilation
VCV : Volume Control Ventilation
VAV : Volume Assist Ventilation
VACV : Volume Assist-Controlled Ventilation
IMV : Intermittent Mandatory Ventilation
SIMV : Synchronized IMV
PSV : Pressure Support Ventilation
PCV : Pressure Controlled Ventilation

VCV: Volume Controlled Ventilation
Ventilator memberikan nafas sesuai preset rate dan preset volume tidal
Tidak boleh ada nafas spontan Hanya pada pasien tanpa usaha nafas
Keuntungan : Otot pernafasan istirahatKerugian :Tidak ada interaksi ventilator – pasien
Perlu sedasi dan/ atau pelemas ototPotensial mengganggu hemodinamik
VAV: Volume Assisted Ventilation
Volume cycled (presed vol tidal) Vt diberikan sesuai preset rate Ventilator dpt meningkatkan nafas bila usaha
nafas pasien meningkatKeuntungan :
Pasien “menentukan” bantuan ventilasi Kerja nafas menurunKerugian : Gangguan hemodinamik, hiperventilasi

SIMV : Synchronized Intermittent Mandatory
VentilationMode untuk proses weaning (pasca bedah dll)Mulai dengan 10x, diturunkan bertahap Volume cycled (preset Vt) dan preset rate Nafas spontan boleh Vent’tor memberi nafas sinkron dg awal inspirasi Bisa digabung dengan pressure supportKeuntungan : interaksi vent – pasien >
Efek pada hemodinamik <Kerugian : Kerja nafas dapat meningkat

PSV : Pressure Support Ventilation
Mode untuk proses weaning (FRC rendah, nafas cepat/dangkal, kelelahan otot)
Mulai dengan 20 cm H2O, diturunkan bertahapMemberikan bantuan inspirasi spontanMeningkatkan usaha nafas pasienPasien mengendalikan: rate, insp. Time, aliran gas dan VtDapat digunakan bersama SIMV
Keuntungan: Pasien > nyaman, interaksi pasien – vent baik, kerja nafas menurun.Kerugian: back up hanya alarm apnea, toleransi psn bervariasi
PCV: Pressure Controlled Ventilation,
IRV: Inverse Ratio Ventilation Machine – triggered, preset pressure, time cycled
Controlled atau Assisted bergantung effort PIP (Peak Inspiratory Pressure) “dibatasi” Setting tepat flow rate, Ti dan mean-Paw IVR
(1:1 atau 2:1) untuk inflasi alveolar, rekruitmen dan oksigenasi
Perlu sedasi atau pelemas otot Hati2 auto-PEEP atau PEEPi Open Lung Concept pada ARDS

CPAP: Continuous Positive Airway Pressure
Mode untuk proses weaning (sebelum T-piece)
Bukan mode “asli”
Nafas spontan
Tekanan base line tinggi
Rate dan Vt bergantung pada usaha nafas pasien
PEEP Dapat dipasang pada semua mode of ventilation FRC meningkat Mencegah kolaps alveoli yang patent(<10cmH2O)
Mengembangkan alveoli yang kolaps (>10cmH2O) Pada edema paru Mendistribusi extravascular lung water Memperbaiki FRC Lung compliance, difusi oksigen
Aplikasi PEEP Mulai 5cmH2O ditingkatkan 2 – 3cmH2O
Pantau tanda vital, PaO2
Efek samping Barotrauma Hipotensi Penurunan curah jantung Peningkatan dead space alveolar Perburukan oksigenasi
Pedoman Memulai Ventilasi Mekanik
Pilih mode paling familiar FiO2 mulai 100% turun bertahap, SpO2 > 92%
Vt awal 8 – 10 cc /kgBB RR dan MV sesuai kebutuhan klinik I/E 1:2 PEEP (mengurangi FiO2, membantu oksigenasi
mis: pada edema paru diffus) Hindari tek inspirasi terlalu tinggi (kurangi flow rate atau
volume tidal) Hb, curah jantung, sat. oksige darah arteri Sedasi, analgesi, perubahan posisi Bila hipotensi, ingat tension pneumotorak
Sasaran Ventilasi Mekanik
Oksigenasi : FiO2 awal tinggi bukan masalah Pertahankan saturasi O2 > 92% Peran PEEPVentilasi : Sesuaikan dengan kebutuhan klinik Nilai pH dan PaCO2 bersama-sama Perlu hipo/ hiperventilasi pada keadaan khusus :
Acidemia, hiperkapnia kronik

Ventilator Induced Lung Injury
Potential to Produce or Augment Injury High Peak Inflation Pressures Alveolar Overdistention Shear Forces Alveolar Recruitment/ Derecruitment PEEP has Beneficial Role Correct Ventilator Management Strategy
Favorably Impacts Outcome

Biotrauma Ventilatory strategies with high tidal volumes and
low PEEP can lead to bacterial translocation from the lung into the systemic circulation
Nahum A, et al.Crit Care Med 1997; 25: 1773-1743 Verbugge SJ, et al.Intensive Care Med 1998; 24: 172-177 High tidal volume low PEEP ventilation has been
shown to increase cytokines in BAL fluid and in the systemic circulation
Ranieri VM, et al.JAMA 1998. 282: 54-61

Lung Protective Strategies by Pflex
Keep PEEP above llower Pflex
to avoid alveolar
underrecruitment
Keep tidal breathing between upper and lower Pflex to avoid
alveolar overdistension
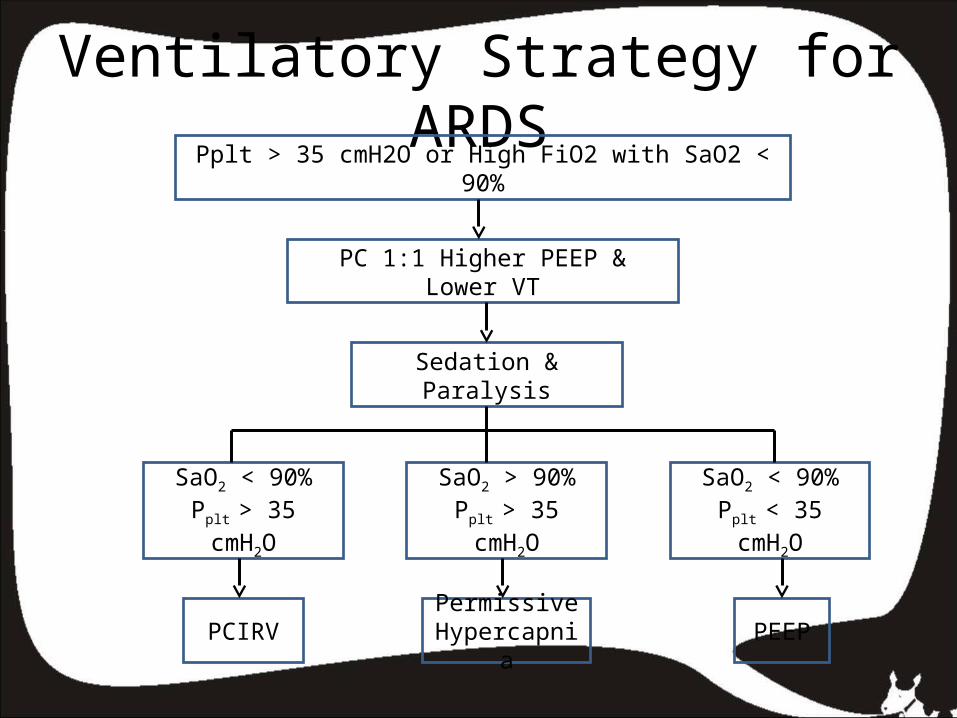
Ventilatory Strategy for ARDSPplt > 35 cmH2O or High FiO2 with SaO2 < 90%
PC 1:1 Higher PEEP & Lower VT
Sedation & Paralysis
SaO2 < 90%Pplt > 35 cmH2O
SaO2 > 90%Pplt > 35 cmH2O
SaO2 < 90%Pplt < 35 cmH2O
PCIRVPermissive Hypercapni
aPEEP

Jenis Pernapasan Kendali
Breath Type Initation (Tigger)
Limit (Target)
Cycle-off
Mandatory Mesin Mesin Mesin
Assisted Pasien Mesin Mesin
Supported Pasien Mesin Pasien
Spontaneous Pasien Pasien Pasien

Aplikasi Fungsi Pernafasan dengan Ventilator
Fungsi Mode Parameter primer Keterangan
Initation Control Interval waktu Trigger: mesin
Assist Ambang tek (-) jalan nafas Trigger: mesin
Limit Volume Preset volume tidal Variasi tek jln nafas
Pressure Tekanan jalan nafas tercapai
Variasi volume tidal
Cycle-off Volume Volume preset tercapai
Pressure Tekanan preset tercapai
Time Interval waktu terlewati Ins. Pause (aliran nol)
Flow Menurun sp laju aliran minimal
Pola aliran inspirasi
Penutup Mode apapun yang dipakai, VM hanyalah bantuan
fisiologik, bersifat sementara
Perbaikan terhadap penyebab gangguan tersebut merupakan tujuan utama
Hendaknya selalu diingat efek samping yang tidak diinginkan
Dalam memenuhi oksigenasi tidak hanya ventilasi tetapi perfusi juga berperan sangat penting
Gunakan ventilator yang paling familiar
Mech. Ventilation is still more art than science

Lesson from Protective Ventilation Strategy
PEEP to open the alveoli Low VT to prevent over distention
Pplat < 30 cm H2O Higher respiratory rate to
overcome acidosis permissive hypercapnea
Frequent recruitment
APRV

APRV Is similar to CPAP in that the pt. is allowed to
breathe spontaneously without restriction
Combines two separate levels of CPAP and the pt. may breathe spont. From both levels
Periodically, pressure is dropped to the lower level, reducing mean airway pressure
During spont, expir. the CPAP is dropped (released) to a lower level which simulates an effective axhalation and CO2 removal

Problem with Older Modes
More work of breathing
Less patient comfort
Either Volume or Pressure is not assured
less security
Need more frequent adjusment

Volume – Assured Pressure Support (VAPS)
• Parameters set : Pressure limit = plateau pres. seen during VC Respiratory rate Peak flow rate PEEP FiO2
Trigger sensitivity Minimum tidal volume

Volume – Assured Pressure Support (VAPS)
Amato et al. Chest 1992; 102: 1225 –
1234
VAPS vs AC
Lower WOB
Lower Raw
Less PEEPi

Pressure – Regulated Volume Control
Pressure limited
Time cycled
Adaptive pressure ventilation (Galileo)
Autoflow (Evita 4)
Automatically adjust pressure support level to
minimum needed to maintain constant set TV

Automode
Siemens Servo 300A
Combines volume Support and PRVC into a
single mode
Switches between PS and PC, with pt effort
determining whether the breath will be VS or
PRVC

Automode
If pt makes no effort, you get PRVC
As pt begins to breathe spontaneously, switch
to VS
Mean airway pressure could become too low
No evidence to advocate its use

Adaptive Support Ventilation
Hamilton Galileo
Dual control, breath to breath mode
Pressure limit of spontaneous and mandatory
breaths is constantly adjusted
Based on idea that a pt will breathe a TV and
rate that minimizes elastic and resistive loads

Adaptive Support Ventilation
Parameters set: Ideal BW High pressure alarm PEEP FiO2
Flow cycle variable (10 – 40%) of initial peak flow, and % volume control (20 – 200%)
Ventilator delivers as volume control 100 ml/kg/min for adults 200 ml/kg/min for childres
Adaptive Support Ventilation
If pt makes no effort to breathe, ventilator
delivers required minute ventilation as PC
If pt starts to breathe spontaneously,
ventilator gradually reduces number of
mandatory breaths and lower pressure
support level as necessary to keep minute
ventilation above the minimum setting

Adaptive Support Ventilation
If pt spontaneous TV is more than the
target and rate is less, the pressure limit
is reduced and rate of mandatory
breaths is increased
If TV > target and rate > target,
pressure limit is lowered and number of
mandatory breaths is reduced

Adaptive Support Ventilation
1. Potential Advantages matches ventilation to lung condition quicker, automatic weaning decreased risk of lung damage2. Potential Disadvantages leaks my defeat algorithm operator must select appropriate % of minute
ventilation to support deadspace may cause problems

Automatic Tube Compensation
Drager Evita 4
Overcome WOB added by artificial
airways
Improved patient/ ventilator synchrony by
providing variable fast inspiratory flow

Automatic Tube Compensation
Due to varying inspiratory flow rates, no
single level of pressure support can
actually fully compensate for WOB
caused by ETT
Autotube uses known static resistence
for each size and type of ETT/ tracheal
tube, and measures flow rates

Automatic Tube Compensation
Pressure is applied and continuously
adjusted proportional to resistance
Tracheal pressure (cm H2O) = proximal
airway pressure (cm H2O) – tube
coefficient (cm H2O/L/sec) x flow2 (L/min)

Automatic Tube Compensation
Potential Advantages simulates breathing without tube decreases patient work of breathing Potential Disadvantages actual tube resistance may change- secretions, kinking May not simulate actual conditions- swelling after extubation

Proportional Assist Ventilation
The goal is to maintain a constant fraction of
work per breath done by ventilator
If ventilator is set to give 80% volume and flow
assist, if the tidal volume increases, the pressure
increases to keep the amount of patient work
constant

Proportional Assist Ventilation
Potential Advantages support matched to need- Only abnormal load is supported better machine – patient synchrony- Theoretically the best mode Potential Disadvantages leaks defeat ventilator algorithm no ventilation if patient stops breathing

Conclusion
Modern ventilators offer several potentially
very useful new modes designed for variety
of purposes
Most of newer modes offer the benefits of
pressure-limited breaths with the security of
an assured minimum tidal volume
More patient comfort with less patient work
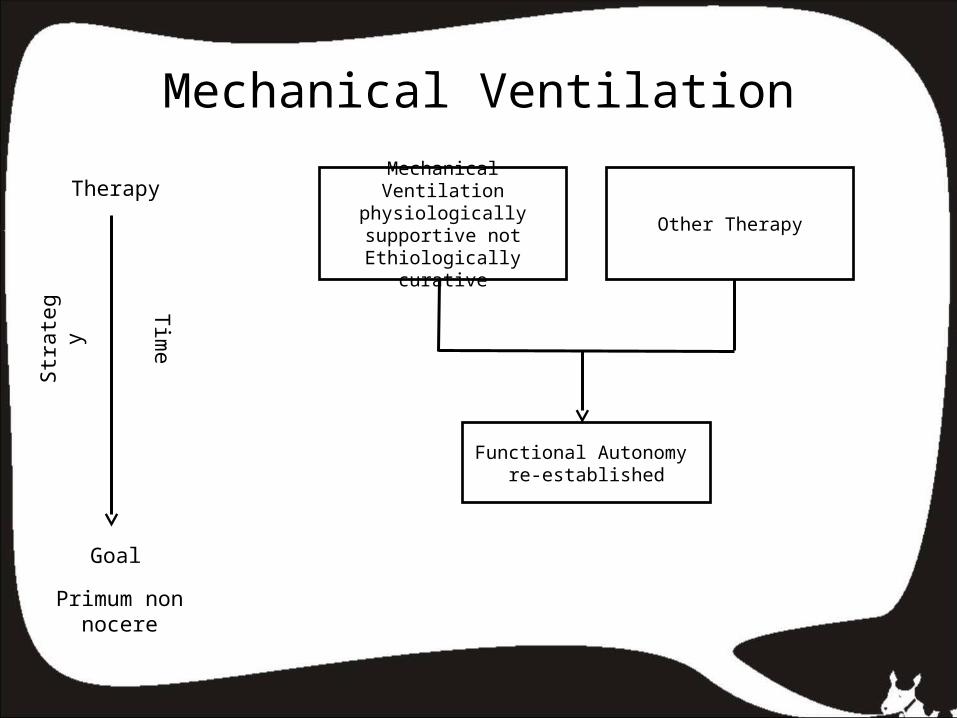
Mechanical Ventilation
Mechanical Ventilation physiologically supportive not
Ethiologically curative
Other Therapy
Functional Autonomy re-established
Therapy
Goal
Tim
e
Str
ate
gy
Primum non nocere






![Dual controlled modes of mechanical ventilation [onarılmış]](https://static.fdocuments.in/doc/165x107/5871a5ac1a28abda6a8b471f/dual-controlled-modes-of-mechanical-ventilation-onarilmis.jpg)