Controversies in the Treatment of Neonatal Seizures Lecture 2017 … · 2017-09-04 · § Concerns...
72
Neonatal Seizures Treatment Controversies and Options A clinical perspective K. S. Krishnamoorthy MD Pediatric Neurology Division Mass General Hospital
Transcript of Controversies in the Treatment of Neonatal Seizures Lecture 2017 … · 2017-09-04 · § Concerns...

NeonatalSeizures
TreatmentControversiesandOptionsAclinicalperspective
K.S.Krishnamoorthy MDPediatricNeurologyDivisionMassGeneralHospital

NeonatalSeizures
MostcommonforaconsultinthenewbornICUItcanbedramaticandanxietyprovokingIncidencevaries:1- 3.5/1000livebirthsinterminfantsHigherreportedinpremiesFamiliesconcernedaboutconsequencesandlaterepilepsy

NeonatalSeizures1970- 2017
Milestones
§ HIEwasthemostcommonetiologyandPhenobarbitalwasthefirstlinedrugused
§ Physiology:GABAisinhibitory(1970’s)GABAisexcitatory(2000’s)
§ Braininjury- moststudiesarestillbasedonanimalmodels§ ExtentofbraininjuryinhumanneonatesisnowdefinedbyMRI/MRS§ StandardsnapshotEEGisreplacedbyuseLTM-EEGtechnologyintertiarycenters§ Emphasisonaggressivetreatmentofelectographic seizures§ Etiologyofseizuresbetteridentifiedby4majortools:
MRI/MRSNeurometabolicstudiesEpilepsygeneticpanelsPlacentalPathology

NeonatalSeizures1970- 2017
MajorMilestones2017
HIE(perinatalencephalopathy)stillremainsthemostcommonetiology
*Phenobarbitalslightlydeclinedinusestillremainsthefirstlinedrug(96%)
*Useofphenytoinhassignificantlydeclined
*UseofLevetiracetam(Keppra)hasincreasedten-fold
*AhmadKJPerinatol2016;El-DibMohamedSeminFet&NeonatMed2017

NeonatalSeizures
Whataboutcontroversies……....?

NeonatalSeizuresControversies
ControversiesconcerningNeonatalSeizures.Scher,MS andPainterMJ/Pediatr ClinicsofNorthAmerica1989;36:281
ControversiesinthediagnosisandmanagementofNeonatalSeizures.LowPS.JSingaporePaediatr Soc 1991;33:6-10
Controversies intreatmentofNeonatal Seizures.HahnJS.Pediatr Neurol 1993; 9:330-1
ControversiesintreatmentofNeonatalSeizuresYoungRSKPediatr Neurol 1993; 9:331-2
Neonatalseizures:DiagnosticandTherapeuticControversiesLegido A.RevNeurol 1996;24:694-700

NeonatalSeizuresControversies
Neonatalseizures:DiagnosticandTherapeuticControversiesLegido A.RevNeurol 1996;24:694-700
Currentcontroversiesindiagnosisandmanagementofneonatalseizures.Laroia Laroia N.IndianPediatr.2000 37:367-72
Controversiesinneonatalseizuremanagement.Glass HC,Wirrell E.JChildNeurol.2009 May;24(5):591-9.
Seizures:controversiesandchallengesintranslatingnewtherapiesfromthelabtotheisolette.ChapmanKE,Raol YH,Brooks-Kayal A.Eur JNeurosci.2012 Jun;35(12):1857-65.

NeonatalSeizures
Areasofcontroversy
Whatisthebestwaytoto detectandmonitorneonatalseizures?
Areclinicalonlyorelectrographiconlyeventstrulyseizures?
Doneonatalseizurescausebraininjury?
Howaggressivelyshouldneonatalseizuresbetreated?
Roleolderdrugsversusnewerdrugsinthetreatmentofneonatalsz ?
Howlongdoyoutreatinfantswithneonatalseizures?GlassHJCN2009

NeonatalSeizuresTreatment
WhyControversies
§ Moststudiesonbraininjuryarefromstudiesonanimalmodels
§ NoevidencebasedguidelinestotreatNS
§ Noclearpolicytotreatacuteclinicalsz (eg:1st choice;2nd choiceetc)
§ Nouniformprotocolstotreatelectrographicseizures
§ Norandomizedcontrolledstudiescomparingdifferentdrugs
§ Concernsaboutthelongtermsideeffectsofolddrugs(phenobarb)
§ Limitedpharmacokineticdataaboutnewerdrugs

NeonatalSeizuresControversiesinTreatment
Objectives
Whytreatneonatalseizures?Whynottotreatneonatalseizures?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewerdrugsHowlongtotreat?

NeonatalSeizures
WhyTreatConcernsaboutBrainInjury
Thereiscompellingevidencepredominantlyfromanimalstudies (Sankar 1998)
Thereisa55-70foldincreaseriskforCP;5foldincreaseforIDand18foldincreaseriskforlaterepilepsy(Holden1982)
BothclinicalandEEGseizurescausesevereneurologicalsequelaeinhumansneonates(Legido A;Pediatrics2001)
HIEwithseizureswasassociatedwithworseoutcomethanwithoutseizures(GlassHJofPediatrics2009)
Seizuresmayexacerbateunderlyingbraininjuryinthesettingofhypoxicischemicencephalopathy(Dzhala V2000;Wirrel 2001)

NeonatalSeizuresWhyTreat
BrainInjuryVOLPE2012

NeonatalSeizuresWhytreat
Volpe JJ 2012
Brain Injury

NeonatalSeizures
WhyTreatRiskofPostNeonatalEpilepsy
§ Riskofpostneonatalepilepsyvariesfrom15- 35%(Scher1993)
§ Treatmentofearlyseizuresmaypreventlaterepilepsy.*In2observationalstudiestreatingsubclinicalsz(EEG)wereassociatedwithlowerincidenceofpostnatalepilepsy8.3- 9.4%
(*(HellstromWestas1995;*Toet2005)
§ EarlyMRIpatternsmaypredictlaterepilepsy(JungDE2015)

NeonatalSeizures
Objectives
Whytreatneonatalseizures?Whynottotreatneonatalseizures?Whattotreat?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewdrugsHowlongtotreat?

NeonatalSeizuresWhynottotreat
§ Mostseizuresarerelatedtoacutereversibletransientcauses
§ Mostseizuresmayresolveinamatteroffewdays
§ Earlytreatmentmaynotpreventlaterepilepsy
§ Riskofpostneonatalepilepsyismostlybasedonetiologyofneonatalseizures
§ Dataofacuteandlongtermconsequencesaremostlyfromanimalmodels(seizuresinanimalmodelsareinducedbychemicals;neuronallossshownintheseexperimentalmodelsmaynotberelevantinhumaninfant)
§ Adverseeffectsoftheanticonvulsantsusedareofconcern
§ Noclearhumandatatosupportthenotionthataggressivetherapyofneonatalseizuresimproveslongtermoutcome.(epileptogenesis andlaterepilepsy)
*Guillet etalfoundthatrecurrencewasindependentofpheonobarb prophylaxisin146children:30%withRxvs23%withoutRx

NeonatalSeizures
Objectives
Whytreatneonatalseizures?Whynottreatneonatalseizures?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewerdrugsHowlongtotreat?

NeonatalSeizuresHowaggressivelytotreat?
Electroclinicaldissociation
OverestimationClinicallyevidentseizurelikebehaviormaynothaveEEGcorrelation
UnderestimationElectrographicseizuresmaynothaveclinicalorbehaviorcorrelation
*MizrahiE1987;ClancyR1995

NeonatalSeizuresHowAggressivelytoTreat
ClinicaleventswithoutEEGchanges
§ Manyneonatalbehaviorsmayresembleseizureseg:jitteriness
§ Neonatalbehaviours maybebrainstem“releasephenomenon
§ Neonatalseizuresmayoriginateinsubcortical/brainstemregions
eg:inferiorcolliculiinratsmaygeneratepaddlingortreadingmovts

NeonatalSeizuresHowaggressivelytotreat
EEGchangeswithoutclinicalevents
Oftenseeninneonateswithveryfrequentelectrographicseizures
*Clancyetal*reportedthatonly21%ofEEGseizureshadclinicalcorrelation*Epilepsia1988
**Wietstocketalreported24%withEEGseizureshadnoclinicalcorrelates**JChildNeurol2016
***BuraniqiEetalreported23%ofpremies(MeanGA32.8wks)withelectrographicseizureshadnoclinicalcorrelates
***JChildNeurol2017Lackofclinicalcorrelatesmostcommonlyseenafterloadingdosesofanticonvulsants

NeonatalSeizuresHowAggressivelytotreat?
Electroclinical Dissociation
Clinicalonly:thereissomedebateifclinicalonlyevents(noEEGcorrelates)shouldbeaggressivelytreatedornot.SomeclinicaleventsmayhaveseizurefocuswhichmaynotberecordedbyscalpEEG.DuetopotentialsideeffectsoftheAEDmanymaynotpursuewithtreatingtheseeventsandcarefulmonitoringisreasonable.Isolatedclinicaleventsmaynotbedetrimentalbutrecurrenteventsmayneedacarefulre-looktoconsidertreatment.
Electrographicseizures:Mostclinicianswillopttotreatelectrographicseizures.

Doseizurespredictoutcome?
Van Rooji Pediatrics 2010

NeonatalSeizuresSurvey
*Areelectrographicneonatalseizuresharmful?
YesDon’knowPediatricNeurologists38%47%Neonatalogists 34%43%
*Wouldyoutreatelectrographicseizures?YesNoDon’tknow
PediatricNeurologists40% 30% remainingNeonatologists38%35%remaining
*Basan HPed Neurol 2008

NeonatalSeizures
HowaggressivelyshouldNSbetreated?
Goalistoeliminatebothclinicalandelectrographicseizures
Totreatonlyclinicaleventswithoutelectrographiccorrelatesisdebatable

NeonatalSeizuresaEEG (AmplitudeIntegratedEEG)
aEEG iswidelyusedinEuorpe andinmanyUStertiarycenters
aEEG :easeapplication;interpretationatbedsidebytrainednurses/MD’s
*aEEG isconsideredlowaccuracyforseizuredetection
*aEEG actualsensitivityforindividualseizuredetection12- 38%
ConventionalLTMEEGwithconcurrentvideoisstillgoldstandard
**ACNSadvocatesuseofcontinuousLTMinthediagnosisofNS
*Snelhass RAClin Neurophysiol 2007;**2011

NeonatalSeizures
Beware:Themisuseoftechnologyandthelawofunintendedconsequences:*FreemanJM:JAmSocietyofExp NeuroTherapeutics2007
“Whetherseizuresorsubclinicalseizuresthemselvescauseharmtothedevelopingbrainisunclear.Theeffectivenessofmedicationsfortreatmentofseizuresinthenewbornhasnotbeenwellestablished.ThereforetheconsequencesofautomatedEEGforthedetectionofsubclincal neonatalseizuresarelikelytobesimilartotheintroductionofelectronicfetalmonitoring:creationofanotherpseudodiseasefollowedbyunwarrantedinterventionandincreasedlegalliability”
*LateProfJohnFreemanfromJohnsHopkins

NeonatalSeizures
Objectives
Whytreatneonatalseizures?Whattotreat?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewdrugsHowlongtotreat?

NeonatalSeizures
WhattoTreatWith§ Firstlineandsecondlinedrugshaveremainedthesameoverdecades§ Noevidencebasedclinicalguidelinesarestillavailable§ Verylittleevidencetosupporttheuseofonedrugovertheother
§ IncreasingrecognitionofneuronalapoptosisrelatedtoolderAED’ssuchasphenobarbital;phenytoin;VPAanddiazepam
§ Poorefficacyofphenobarb anddiazepammayberelatedtoexcitatorynatureofGABAreceptorsinthenewborn(animals)
§ Lackofrandomizedplacebocontrolledtrialsmakesitdifficulttoknowtheabsoluteefficacyofvariousoldandnewanticonvulsants
§ Manypublishedstudiesarenot basedonLTMEEG’s.
§ Limitedpharmacokineticstudiesandsafetydataonnewerdrugs

NeonatalSeizuresAntiConvulsantDrugTherapy
“thereislittleevidencetosupporttheuseofanyoftheanticonvulsantscurrentlyusedintheneonatalperiod”
BoothD.CochraneDatabase2004

NeonatalSeizuresAntiConvulantDrugTherapy
ThereisconcernandconcensusthatcurrentlyusedAEDsareoftenineffectivefortreatmentofneonatalseizures.
SankarR,PainterMJ.Neurology2005

NeonatalSeizuresAntiConvulantDrugTherapy
*WHOevidenceguidelinesonneonatalseizuresemphasizethelackofevidenceforthemanagementofneonatalseizures.
*WHOGuidelinesonneonatalseizures,Geneva2011

NeonatalSeizuresAnticonvulsantDrugTherapy
Wearenotalone!
Thereareothertypesofseizuredisordersandepilepsythathavenowellstudiedrandomizedcontroldrugtrials:
Lennox-GastautsyndromeInfantilespasmsESES(electricalstatusepilepsticusinsleep)EarlyInfantileandEarlyMyoclonicEncephalopathy(EIEE/EMEE)

NeonatalSeizuresAnticonvulsantDrugtherapy
OldDrugs
Phenobarbital
Phenytoin(fosphenytoin)

NeonatalSeizuresAnticonvulsantDrugTherapy
WhyusePhenobarbital?
Useasfirstlinedrugfordecadesforneonatalseizures
AvailabilityworldwideCheapPharmacokineticswellstudiedandpredictableLonghalf-lifeespeciallyinHIEbabies(>120hrs).CrossestheBBBinlessthan30minutesLessproteinbinding(33%)Useasmaintenanceorallyisfeasible

NeonatalSeizuresAnticonvulantDrugTherapy
PainterandScher NEJM1999
(PhenobarbitalvsPhenytoin)AdoubleblindplacebocontrolledstudySeizuresweremonitoredoncontinuousLTMEEG
DrugIVrouteResponsePhenobarb 43%+Phenytoin 57%
Phenytoin 45%+Phenobarb 62%
Conclusion:Overallresponsewitheitherdrug<50%Nosignificantdifferencesbetweenthese2drugsincontrollingelectrographicseizures

NeonatalSeizuresTreatmentJChildNeurol2009:24;148

NeonatalSeizuresHellstrom-WestasL.ActaPaedrica2015
Hellstrom-Westas,L

NeonatalSeizures
ConcernsaboutPhenobarbitalExperimentaldataemerged3decadesagoaboutphenobarbitalexposurehadadverseeffectsonsurvivial andmorphologyofculturedneuronsoffetalmousetissueandraisedconcernsaboutitsuseinthetreatmentofneonatalseizure
(BergeyGK1991SerranoEE1988)
Recentevidencethatevenbrieftreatmentwithconventionalanticonvulsantssuchasphenobarbital,diazepam,phenytoinandvalproate allincreaseapoptoticneuronaldeathinnormalimmaturerodentmodelsincortexthalamusbasalganglia
Bittigau P.ProcNatlAcad Sci2002
Neuronalapoptosisinratneuronsatserumconcentrationlevel25-35mc/mlBiitigau P.AnnNYAcad Sci2003

NeonatalSeizuresAnticonvulsantDrugTherapy
WhyusePhenytoin/Fosphenytoin?
Anotheroldwithwellstudiedpharmacokineticsanduses
Wellestablishedashighlyeffectivedrugforstatusepilepticus
LesscardiovascularsideeffectsCrossesBBBin<20minutesConvertedtophenytoinbyphosphatasesin<8minutesIVEffectiveinneonatalseizuresabolishingclinicalandEEGseizures
Combinedwithphenobarbitaliseffectivein65%

NeonatalSeizuresAnticonvulsantDrugTherapy
ConcernsaboutPhenytoin
*Inratneuronstriggersneuronalapoptosisatadoseof20mg/kg
(ie:Plasmaconcentrationof10- 15mc/ml)
Reducedproteinbindingandlikelytoincreasefreephenytoinlevels
Maydisplacefreebilirubinandincreasesriskforkernicterus
Lastlyphenytoinisnotideallyusedorallyasamaintenancedrugforneonatalseizures
*BittigauP.AnnNYAcadSc2003

NeonatalSeizures
OldDrugs
Despiteproblemsandlessefficacybothphenobarbitalandfosphenytoinstillremainmainstayintheinitialdrugtherapyforneonatalseizures

NeonatalSeizures
Objectives
Whytreatneonatalseizures?Whattotreat?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewerdrugsHowlongtotreat?

NeonatalSeizures
NewerAntiepilepticDrugs(AED)
LevetiracetamTopiramateBumetanideFlupirtine(potassiumchannelopenertestedinrats)

NeonatalSeizures
NewerAED’s
MostnewerAED’sarecurrentlyofflabelreportedascaseseries
Clinicaluseanddataareinsufficienttorecommendthemasfirstline.
Levetiracetamandtopiramatehavefavorablepharmacokineticprofiles.
Topiramateandlevetiracetamdonotcauseneuronalapoptosisordisruptsynapticdevelopmentinanimalmodels(KimJJ2007)
TopiramateandLevmayhaveneuroprotectiveproperties.(Kim,J.2007)
Experiencewithnewerdrugsisreportedonlyascaseseries.

NeonatalSeizuresLevetiracetam
AnimalDataNoneurotoxiceffectsin7dayoldratsatdosesupto100mg/kg( Manthley DExp Neurol 2005)
- LEVgivenprophylacticallytoHIEinducedratsreducedclinicalandelectricalseizures- (Talos DMPediatr Res2013)
- LEVappearedtoexertadiseasemodifyingeffectonHIEinducedseizures)- Giler CExp Nneurol 2004)
LEVsignificantlyreducedthenumberofapoptoticcellsinthehippocampus,cerebralcortexandthalami(Kilicdag HEarlyHumDev2013)
- LEVsupressed acuteseizuresinducedbyperinatalhypoxiaand- diminshed laterlifeseizuresusceptibilityandseizureinducedneuronal- injuryinrodentneonatalseizuremodel.(JensenFEPediatr Res2011)-
- LEVandTopiramatehavenoeffectsonapoptosisinthedevelopingbrain.- (Talos DMPediatr Res2013)
-

NeonatalSeizuresLevetiracetam
ClinicalData(Total144cases)Allcaseseries
*AbendNS;JChildNeurol 2011*Ramantani G;Eur JPediatr Neurol 2011*KhanO;PediNeurol 2011*KhanO;PediNeurol 2013*Rakshabhuvankar A;JClic Neurosci 2013*Neininiger MP:Neuropediatrics 2015*Lo-YeeYau M;WorldJClin Pedi2015
(Doserange10- 55MG/KGResponserate35- 100%(overall90%)
Surveyshaveindicatedlevetiracetam beingusedassecondline(SilversteinF2008)
AdoubleblindrandomizedcontrolledtrialofIVLevetiracetam iscurrentlyinprogressinChildren’sHospital,SanDiego,Ca.
AnobservationalstudycomparingLevandPhenobarbitalasfirstlineiscurrentlyinprogressatUniv ofCincinnati

NeonatalSeizuresLevetiracetam
ClinicalStudy
RamantaniGetalEurJPedNeurol2011
AprospectivestudyusingLEVasfirstlinedrugN38pretermandterminfantsDoserange10mg/kgloadtomax60mg/kgSomeneededphenobarbitalIVforpersistentseizures30/38infantsbecameseizurefreeinoneweekEEGmarkedlyimprovedin24infantsin4weeks.

NeonatalSeizuresLevetiracetam
ClinicalStudyFalsaperlaRJPediatrNeurosci2017
AprospectivestudyusingLEVasfirstlinedrugN=16neonates(12termand4preterm)LEVinitialdose10mg/kgBIDMaintenanceDoseupto40mg/kgBIDAllrespondedtoLEVmonotherapyResponsewithin24- hoursto15days(mean96hrs)

NeonatalSeizuresLevetiracetam
LEViscurrentlyoftenusedassecondorthirdlinetreatmentforneonatalseizures
AvailabilityofIVpreparationhasenableditsuseofflabel
MechanismisactioninunknownbutsuggestiveofinteractionwithSVP2A(synapticvesicleprotein)
Itisnotlinkedtoplasmaproteins-sonoriskofdisplacementofotherproteinboundsubstancesMinimalhepaticmetabolisminvolved
ItisnotmetabolizedbycytochromeP450system
Meanhalflifeinneonatesrangefrom9to18hoursQ8hourlydosemaybepreferable
SeveralanimalstudieshavesuggestedLEV’ssafetyinthenewborninfants(doesnotcauseapoptoticdegeneration)
APhase2randomizedstudyasfirstlinedrugbeingconductedatUniv ofCaatSanDiego

NeonatalSeizuresLevetiracetam
HumanStudiesinNeonatalSeizures
Studiesaboutitsusepublishedaresmallretrospectiveseries
MostofthemreceivedLEVassecondorthirdlinedrugtreatment
Methodologicalissuesmakethemdifficulttointerprettheresults
Manyoftheneonateshavealreadyreceivedotherdrugs
UnclearifseizurecessationisLEVefficacyornaturalresolution
CurrentevidencesuggeststhatLEVworksbestin30%ofneonates
El-DibM.andSoulJ.SemFetal&NeonatalMed2017

NeonatalSeizuresLevetiracetam
CurrentUse
AsfirstlinedrugforneonatalseizuresisstillnotprevalentStudiesareunderwayofLEVasfirstlinedrugforneonatalseizures
Assecondlineiswidelycatchingup.AlmosteveryoneusesLEVasthirdlineforneonatalseizures

NeonatalSeizuresAnticonvulsantDrugTherapyNewerDrugsTopiramate(AMPAModulator)
TPMhasmultiplemechanismsofaction(Koh&JensenAnnNeurol 2001)
InanimalsmodelswithcerebralischemiaTPMreducedseverityofbraininjuryaloneorwithhypothermia.(Scubert S.2005;BrainRes)
Inanimalsmodelsnotshowntohaveanyharmfuleffectsondevelopingbrain
Neuroprotective effectshavebeendescribedinratsrelatedtoAMPAmediatedeffectsandkainate receptorinhibition(Koh&JensenAnnNeurol 2001)
Nocleardataonhumanneonates/noIVformulationlimitsuse.
Susceptibletodruginteractionsandeffectsofhypothermia(CP450)(PedNeurol 2011;2012)
Lowriskforapoptosis(Sem Fetal&NeonatalMed2017)
TrialasadjuvantwithhypothermiainHIEcurrentlyinprogressinUSAandItaly

NeonatalSeizuresAnticonvulsantDrugTherapyNewerDrugs
*Bumetanide(NKCC1transporterinhibitor)
§ Aloopdiureticwidelyusedfordecadesinneonatesasadiuretic
§ InhibitsNKCCL(Cl-cotransporter)thatishighlyexpressedinimmatureneurons
§ BlockadeofNKCCLdecreasesneuronalCl levelsandrestoresGABAinhibition
§ CombiningwithphenobarbitalaugmentsGABAinhibitionandmaycontrolseizuresnotcontrolledbyphenobarbitalalone
§ **AugmentsneuroprotectiveeffectsofphenobarbitalinHIEmodelswithhypothermia
§ AlargedoubleblindmulticenterRCTstudycompletedatHarvard(SoulJ,StaleyKJetal).
*Dzhazla V,StaleyKAnnNeurol **LiuYPedRes2012

NeonatalSeizures

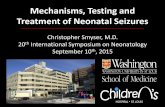
NeonatalSeizures
GABA acts excitatory in immature neurons due to over expression ofNKCC1 and under expression of KCC2 resulting in increased intraneural Cl ions and depolarization ( excitation)
Mature neurons have over expression of KCC2 and low intraneuronal Cl ions concentration resulting in GABA induced hyperpolarization(inhibition) Mruk AL 2015

NeonatalSeizuresAnticonvulsantDrugTherapyNewerDrugs
Flupirtine(Potassiumchanelopeners)
*Arecentstudyinratshasshownexcellentefficacy
In5minutescompletelyabolishedelectrographicandclinicalsz
PotentialuseinhumansinKCNQ2andKCNQ3epilepsies
RaolYHetalAnnNeurol2009

NeonatalSeizuresAnticonvulsantDrugTherapy
*AED’sadministeredforNeonatalSeziures
(N- 420)(from8tertiarycarecenters)
DrugN%Phenobarbital387(92%)Levetiracetam130(31%)Fosphenytoin116(27%)
Benzodiazepine81(19%)Midazolaminfusion34(8%)Vitamins(B6etc)32(8%)
*GlassHetalJournalofChildNeurology2016

NeonatalSeizuresAntiConvulsantDrug Therapy
*Informalpersonalpollofneonatalneurologistsfrom4majortertiarycenters:
1. Everyoneusesphenobarbital asthefirstchoice2. SecondchoiceisstillFosphenytoin in2/4centers
3. SecondchoiceisLevetiracetam in2/4centers4. SecondchoiceofIVMidazolam in1/4ifEEGshowsstatus5. AllagreethatpracticesvaryaccordingtotheAttendings6. UseofTopomax isstillnotcommonbecausenoIVform.
7. NooneusesPentobarbitalcomaintheneonates

NeonatalSeizuresPretermBabies
92 preterm infants ( < 28 weeks to 37 weeks)Phenobarbital was initial drug used in majority of infants HIE and ICH most common causes. More subclinical seizure detected in preterm ( 24% ) than term(14% ) Mortality was twice ( 35% ) in preterm than term ( 15%)Recommending routine LTM EEG monitoring in preterm infants

NeonatalSeizures
HypothermiaTherapeutichypothermiaisstandardofcareinneonatalHIE
*Hypothermiaislikelytoreduceseizureburden
**Hypothermiamightaffectbiotransformationofdrugsviahepatic
cytochromeenzymesP450(CYP450)
**EffectofhypothermiaisexaggeratedinHIEhinderingdrugmetabolism
andelimination
Bothphenobarbandphenytoinmetabolismbutlevetiracetamisnot
depressedbyhypothermia
*JPediatr**CritCareMed200**ExpertopinDrugMetabToxicol2011

NeonatalSeizuresAEDTherapy
PersistentElectrographicSz
§ Mostelectrographicsz respondtooptimaldosesphenobarb/fosphenytoin
§ Usuallyresponseseenin24– 72hours
§ MaytryIVlorazepam0.05MG/kgbolusx1-2doses
§ IVLevetiracetamisgainingaroleasanexcellentoption
§ IVMidazolamcontinuousinfusionisusedinselectedcases
§ IVPentobarb infusionisonlyveryrarelyusedintheneonates
§ IVLidocaineisusedinEuropecommonlybutnotinUSA
§ TrialofPyridoxine(B6)iswarrantedinallintractablecases

NeonatalSeizures
Midazolam
AnticonvulsanteffectatGABAreceptors
Apoptosishasnotbeenwellstudied
Concernsaresedation,mortalityandlengthyhospitalstayetc
Efficacyas2nd or3rd lineforrefractoryNShasbeenpublishedascaseseries
Smallsamplesizeandmethodologicalissueshamperinterpretation
UseofmidazolammaybeconsideredforrefractoryNS

NeonatalSeizuresDrugTherapy
VitaminTherapyUseinselectedintractablecases
Pyridoxine(Vit B6)100- 200mgIVwithconcurrentEEG
Biotin5-15mgtid (PO)
Folinic acid4mg/kg/IV/PO/tid
Pyridoxal4Phosphate30mg/kg/dayPOdividedTID

NeonatalSeizuresFuture DrugTherapy
MikatiMSemPedNeurol2016

NeonatalSeizuresAcuteDrugTherapy
UsualStrategy
LoadwithPhenobarb 20mg/kg-maygoup
with5mg/kgincrementsto30mg/kg-40mg/KgBepreparedtointubateinthosewith40mg/Kg
IfnoresponseAddIVFosphenyoin 20mg/kgIfnoresponse
Maytryanotherdose5mg/kgIVIfnoresponse
GiveIVLevetiracetam20mg/KgMaytrydosesupto40- 50MG/KGIV
IfnoresponseConsiderIVMidazolaminfusion

NeonatalSeizuresAcuteDrugTherapy
ModifiedStrategy
LoadwithPhenobarb 20mg/kg-maygoupwith5mg/kgincrementsto30mg/kg-40mg/Kgbepreparedtointubateinthosewith40mg/Kg
IfnoresponseLoadIVLevetiracetam40-60mg/kg(highdose)
IfnoresponseLoadIVFosphenytoin 20mg/kg
IfnoresponseTryPyridoxine100-200mgIV
IfnoresponseConsiderIVMidazolaminfusion

NeonatalSeizures
Objectives
Whytreatneonatalseizures?Whattotreat?Howaggressivelytotreat?Whattotreatwith?OlddrugsNewdrugsHowlongtotreat?

NeonatalSeizures
HowLongtoTreatThereislittleagreementonthisissue/noclearpolicy/guidelinesexistTherearenorandomizedcontrolledstudiescomparingtheeffectsofAEDtreatmentvs notreatmentonshortandlongtermoutcome.*SurveyshaveindicateddurationofRxdaystoyears–nouniformity**Neonatologiststendadvocateshorterdurationthanneurologists
*Massingale TWJPerinatol 1993;Bartha AIPediNeurol 2007;Basan H2008**Basan H2008;Wickerstrom RPediNeurol 2013
Ingeneral,infantswithsevereHIEbraininjury;corticalmalformations,largebleedsandgeneticepilepsiesmayneedlongerdurationoftreatment.

NeonatalSeizuresDrugTherapy
CriteriatostopAEDtherapy
§ 80%-85%ofneonateswillneedonlyshorttermmaintenence therapy(weeks)§ *Mayconsidertodiscontinueiffollowingcriteriaaremet:
NoseizurerecurrenceNormalfollowup EEGNormalNeurologicalExamination
*VolpeJJPediatrics1989
§ ThosewhoneedlongtermAEDtherapy(15-20%)haveconsequencesofsevereHIE/malformations/metabolic/genetic/meningoencephalitis

NeonatalSeizuresConclusionsofControversies
CurrentstateoftreatmentforneonatalseizuresThereisnoevidencebasedstudiestosupportcurrentAEDuse
Currentmanagementislargelybasedonoldtradition;caseseriesandclinicalexperience
Clinicaltrialsinneonateshavelogisticalandethicalproblems
AED’sbasedonagespecificmechanismsmightholdpromiseuseofnewerdrugs
Trialsoflevetiracetam,topiramateandbumetanidearebeingconductedmethodicallyandmayalterfuturedrugtreatmentofneonatalseizures
Thereisastrongneedformoreevidencebasedstudiesanddataforthemanagementofneonatalseizures.

ControversiesinNeonatalSeizures
KeyReferencesChapmanKE.European JournalofNeuroscience;2012:1857-65Pressler RM.Seminars inFetal&NeonatalMedicine;2013:216-223Spagnoli C.ItalianJournalofPediatrics;2013:37-39
ShettyJ.DevelopMed&ChildNeurol ;2015:40- 43Wietstock SO.JChildNeurol 2016:328-332GlassHC.JournalofChildNeurol 2009:591-99El-Dib,M.SeminarsinFetal&NeonatalMedicine2017;1-7
Mruk AL.JPediatr Pharmacol Ther 2015:76-89

ControversiesinNeonatalSeizures
Thankyouforyourkindattention