Percutaneous cholecystostomy in acute acalculous cholecystitis
Upload
amit-rastogiCategory
view
216download
2
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005), pp. 1391–1401 ( C© 2005)DOI: 10.1007/s10620-005-2852-x
REVIEW
Controversies Concerning Pathophysiology andManagement of Acalculous Biliary-Type
Abdominal Pain
AMIT RASTOGI, MD, ADAM SLIVKA, MD, PhD, ARTHUR JAMES MOSER, MD, and ARNOLD WALD, MD
Acalculous biliary-type abdominal pain is a commonly encountered clinical problem whose patho-physiology is unclear and evaluation and management are controversial. Cholecystokinin cho-lescintigraphy to measure the gallbladder ejection fraction (GEF) has been advocated as a criterionfor cholecystectomy. However, there is no consensus regarding the dose and rate of infusion ofcholecystokinin, both of which can alter the GEF, and the definition of an abnormal ejection frac-tion varies among studies. Many but not all studies have concluded that a low GEF predicts goodoutcomes after cholecystectomy, but most studies suffer from poor methodology and there is onlyone prospective randomized controlled trial. Also, some patients with a normal GEF have respondedto cholecystectomy. Another controversial area has been the role of sphincter of Oddi dysfunction(SOD) in patients with biliary-type pain and gallbladder in situ. Some reports suggest an overlapbetween SOD and low GEF, although a causal relationship has not been established. Yet anothersubject of interest is the role of visceral hyperalgesia in patients with acalculous biliary-type pain. Wehave reviewed the relevant literature relating to these issues and have highlighted the controversialaspects. In the absence of high-quality studies, an evidence-based treatment algorithm is difficult todesign but will be proposed. More prospective controlled trials are warranted to better define theappropriate evaluation and management of patients with this syndrome.
KEY WORDS: acalculous biliary-type abdominal pain; cholecystokinin cholescintigraphy; sphincter of Oddi dysfunction;endoscopic sphincterotomy; gallbladder ejection fraction.
Recurrent biliary-type abdominal pain in patients withan acalculous gallbladder in situ is a perplexing clinicaldilemma. The evaluation and treatment of these patientsare controversial. In one population study, the prevalenceof biliary-type pain without gallstones was estimated to be2.4% (1). Other population screening studies performedwith ultrasonography have shown that the frequency ofbiliary-type pain without gallstones was 7.6% in men (2)and 20.7% in women (3). The diagnosis of “gallbladderdysfunction” is used when laboratory, ultrasonographic,
Manuscript received November 19, 2004; accepted December 14, 2004.From the Division of Gastroenterology, Hepatology & Nutrition, Uni-
versity of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA.Address for reprint requests: Arnold Wald, MD, Division of Gastroen-
terology, Hepatology and Hepatology, University of Pittsburgh Medi-cal Center, 200 Lothrop Street, Pittsburgh, Pennsylvania 15213, USA;[email protected].
and microscopic bile examinations have excluded the pres-ence of gallstones and other structural abnormalities in pa-tients with “typical biliary pain” (4). Other synonyms forthis condition are gallbladder dyskinesia, biliary dyskine-sia, acalculous biliary disease, chronic acalculous chole-cystitis, and chronic acalculous gallbladder disease. “Typi-cal biliary pain” was defined by the “Rome II” Committeeon the Functional Gastrointestinal Disorders (5), whichproposed criteria for gallbladder dysfunction as follows:
Episodes of severe steady pain located in the epigastrium and rightupper quadrant, and all of the following—1) Symptom episodes last30 minutes or more with pain free intervals. 2) Symptoms have occurredon one or more occasions in the previous twelve months. 3) The painis steady and interrupts daily activities or requires consultation with aphysician. 4) There is no evidence of structural abnormalities to explainthe symptoms. 5) There is abnormal gallbladder functioning with regardto emptying.
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 13910163-2116/05/0800-1391/0 C© 2005 Springer Science+Business Media, Inc.

RASTOGI ET AL.
Thus the central symptom in these patients is biliary-type pain and the only objective marker of disease is ab-normal gallbladder emptying. (5)
PATHOPHYSIOLOGY OF SYMPTOMS
Altered gallbladder motility has been the most widelyaccepted abnormality. However, alternative pathophysiol-ogy may be operative in these patients including impair-ment of gallbladder filling, gallbladder hyperalgesia, andfunctional disorders of adjacent structures (5). Techniquesto assess these are not widely available. Gallbladder dys-function may also be associated with structural or histo-logic abnormalities such as a narrowed cystic duct, gall-bladder muscle hypertrophy, and chronic inflammation ofthe gallbladder (6, 7).
Several mechanisms for abnormal gallbladder empty-ing have been hypothesized. Amaral et al. (8) showeda good correlation between gallbladder emptying in re-sponse to an intravenous infusion of cholecystokinin(CCK) in vivo and gallbladder muscle contraction inducedby CCK in vitro. The authors demonstrated that patientswith acalculous gallbladder disease had impaired gall-bladder muscle contraction in response to CCK comparedwith patients who had pigment gallstones. The gallblad-der muscle cells of patients with acalculous gallbladderdisease did not respond normally to receptor-dependentagonists, G-protein activators, and the second messen-ger diacylglycerol, suggesting that the defect resides inthe contractile apparatus. Alternatively, Yap et al. (6) hy-pothesized that narrowing of the cystic duct may impairemptying of the gallbladder and produce thickening ofthe gallbladder muscle, fibrosis, and histologic changesconsistent with chronic cholecystitis.
Little is known about the mechanism of pain in thesepatients. Velanovich (9) theorized that an intrinsic defectin gallbladder motility promotes cholesterol monohydratenucleation and crystal formation within the gallbladderbile. Crystal growth and entrapment in the mucus layer ofthe gallbladder wall and associated chronic inflammationtogether with abnormal motility may lead to pathologicstretching of the gallbladder and pain. On the basis oftheir finding of a narrowed cystic duct in these patients,Yap et al. (6) suggested that the mechanism of pain mightbe similar to that following impaction of a stone in thegallbladder neck in patients with biliary colic. Others havehypothesized that the mechanism for pain is obstructionleading to distension and inflammation of the gallblad-der (4). This might result from incoordination betweengallbladder contraction and relaxation of either the cysticduct or the sphincter of Oddi due to increased resistance ortone. Finally, central projections from visceral nociceptors
to the thalamus and cerebral cortex might lead to visceralhyperalgesia (severe pain evoked by mildly painful stim-uli), which in turn might result in allodynia (a state inwhich innocuous stimuli produce pain). Thus, as in otherfunctional disorders of the gastrointestinal tract, height-ened sensitivity in the biliary tree or in adjacent structuresmay be associated with pain in patients with gallbladderdysfunction. For example, Desautels et al. (10) showedthat postcholecystectomy patients with persistent abdom-inal pain exhibited duodenal-specific visceral hyperalge-sia and that duodenal distension with a barostat devicereproduced symptoms in the vast majority of patients.
MEASUREMENT OF GALLBLADDER
EMPTYING—WHAT IS ABNORMAL?
The normal gallbladder acts as a reservoir for bile dur-ing fasting but empties 25% of its contents every 100–120 min. This is mediated by motilin via cholinergicnerves (11). Eating causes the gallbladder to empty over75% of stored bile via neural (cephalic and local gastro-duodenal reflexes) and hormonal (predominantly CCK)pathways (12). CCK causes gallbladder contraction via adirect effect on smooth muscle by interacting with CCK-A receptors on cholinergic nerves and also by interactingwith sensory neurons of the vagus nerve to activate vagalafferent pathways (12, 13). Vagal efferents from the dor-sal motor nucleus of Vagus then interact with interneuronsin the enteric nervous system, resulting in the release ofacetylcholine to cause gallbladder contraction. The releaseof vasoactive intestinal peptide (VIP) and nitric oxide bynonadrenergic, noncholinergic inhibitory nerves coordi-nate relaxation of the sphincter of Oddi (14–16).
Different techniques have been used to assess meal-stimulated gallbladder emptying; these include CCKcholecystography and transabdominal ultrasonographyemploying a meal or CCK to stimulate gallbladder emp-tying. Cholecystography is now considered obsolete andultrasound methods lack reproducibility (17).
Krishnamurthy et al. (18) introduced a noninvasivetechnique to measure gallbladder emptying using 99m-technetium-labeled hepatobiliary radiopharmaceutical N -α-(2,6- dimethylacetanilide)iminodiacetic acid (99mTcHIDA) and CCK octapeptide. Gallbladder emptying is ex-pressed in terms of the gallbladder ejection fraction (GEF),which is defined as
Gallbladder volume before contraction − Gallbladder volume after contraction × 100
Gallbladder volume before contraction
In their in vitro model which simulated in vivo gall-bladder geometry, the ejection fraction measured by thevolume method was compared to that measured by the
1392 Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005)
ACALCULOUS BILIARY-TYPE ABDOMINAL PAIN
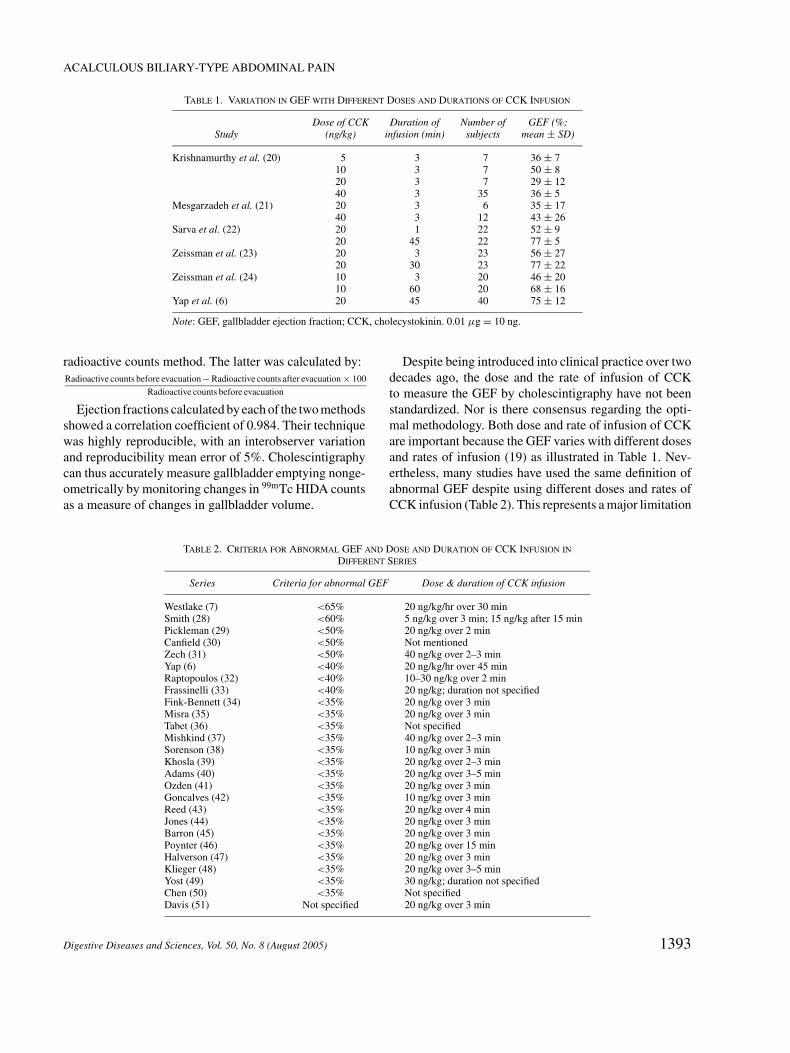
TABLE 1. VARIATION IN GEF WITH DIFFERENT DOSES AND DURATIONS OF CCK INFUSION
Dose of CCK Duration of Number of GEF (%;Study (ng/kg) infusion (min) subjects mean ± SD)
Krishnamurthy et al. (20) 5 3 7 36 ± 710 3 7 50 ± 820 3 7 29 ± 1240 3 35 36 ± 5
Mesgarzadeh et al. (21) 20 3 6 35 ± 1740 3 12 43 ± 26
Sarva et al. (22) 20 1 22 52 ± 920 45 22 77 ± 5
Zeissman et al. (23) 20 3 23 56 ± 2720 30 23 77 ± 22
Zeissman et al. (24) 10 3 20 46 ± 2010 60 20 68 ± 16
Yap et al. (6) 20 45 40 75 ± 12
Note: GEF, gallbladder ejection fraction; CCK, cholecystokinin. 0.01 µg = 10 ng.
radioactive counts method. The latter was calculated by:Radioactive counts before evacuation − Radioactive counts after evacuation × 100
Radioactive counts before evacuation
Ejection fractions calculated by each of the two methodsshowed a correlation coefficient of 0.984. Their techniquewas highly reproducible, with an interobserver variationand reproducibility mean error of 5%. Cholescintigraphycan thus accurately measure gallbladder emptying nonge-ometrically by monitoring changes in 99mTc HIDA countsas a measure of changes in gallbladder volume.
TABLE 2. CRITERIA FOR ABNORMAL GEF AND DOSE AND DURATION OF CCK INFUSION IN
DIFFERENT SERIES
Series Criteria for abnormal GEF Dose & duration of CCK infusion
Westlake (7) <65% 20 ng/kg/hr over 30 minSmith (28) <60% 5 ng/kg over 3 min; 15 ng/kg after 15 minPickleman (29) <50% 20 ng/kg over 2 minCanfield (30) <50% Not mentionedZech (31) <50% 40 ng/kg over 2–3 minYap (6) <40% 20 ng/kg/hr over 45 minRaptopoulos (32) <40% 10–30 ng/kg over 2 minFrassinelli (33) <40% 20 ng/kg; duration not specifiedFink-Bennett (34) <35% 20 ng/kg over 3 minMisra (35) <35% 20 ng/kg over 3 minTabet (36) <35% Not specifiedMishkind (37) <35% 40 ng/kg over 2–3 minSorenson (38) <35% 10 ng/kg over 3 minKhosla (39) <35% 20 ng/kg over 2–3 minAdams (40) <35% 20 ng/kg over 3–5 minOzden (41) <35% 20 ng/kg over 3 minGoncalves (42) <35% 10 ng/kg over 3 minReed (43) <35% 20 ng/kg over 4 minJones (44) <35% 20 ng/kg over 3 minBarron (45) <35% 20 ng/kg over 3 minPoynter (46) <35% 20 ng/kg over 15 minHalverson (47) <35% 20 ng/kg over 3 minKlieger (48) <35% 20 ng/kg over 3–5 minYost (49) <35% 30 ng/kg; duration not specifiedChen (50) <35% Not specifiedDavis (51) Not specified 20 ng/kg over 3 min
Despite being introduced into clinical practice over twodecades ago, the dose and the rate of infusion of CCKto measure the GEF by cholescintigraphy have not beenstandardized. Nor is there consensus regarding the opti-mal methodology. Both dose and rate of infusion of CCKare important because the GEF varies with different dosesand rates of infusion (19) as illustrated in Table 1. Nev-ertheless, many studies have used the same definition ofabnormal GEF despite using different doses and rates ofCCK infusion (Table 2). This represents a major limitation
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 1393

RASTOGI ET AL.
when evaluating the validity of this test to make clinicaldecisions.
Efforts to define a universally accepted standard doseand rate of infusion of CCK to assess GEF have beenhampered by a failure of consensus among variousinvestigators. Krishnamurthy et al. (20) studied 5, 10, 20,and 40 ng/kg infused over 3 min. The highest mean GEFoccurred with 10 ng/kg, and with higher doses >25%of subjects had intense abdominal pain, nausea, tran-sient bradycardia, or hypotension. They defined a GEFof <35% as abnormal, which was defined as 2 SD belowthe mean of only seven subjects who received 10 ng/kgCCK. Mezgarzadeh et al. (21) found that the mean GEFswith 20 and 40 ng/kg CCK over 3 min were not signifi-cantly different. Sarva et al. (22) compared 20 ng/kg CCKinfused over 1 min versus 45 min. The lower limit of nor-mal (mean – 2SD) with the 1-min infusion was 34% ver-sus 67% with the 45-min infusion. As the range of GEFwas larger with the 1-min infusion, they concluded that a45-min infusion was the superior method. Zeissman et al.(23) compared 3- and 30-min infusions of 20 ng/kg CCK.With the 3-min infusion, clinically useful normal valuescould not be established because of a large standard devia-tion (Table 1). Moreover, 35% of the healthy subjects hada GEF <35%. In contrast, the mean GEF was higher andthe range was narrower with the 30-min infusion. The au-thors concluded that the 30-min infusion was preferable,as it was more physiological, resulted in more completeemptying, and had fewer side effects and less variability.Of note, the mean GEF in female subjects was substan-tially lower with both infusions compared to that in males.Zeissman et al. (24) then compared 10 ng/kg CCK infusedover 3 or 60 min. As with the 20 ng/kg dose, the 3-min in-fusion produced a GEF too variable to establish a clinicallyuseful normal range, whereas clinically useful normal val-ues were established for both 45- and 60-min infusions(>31% and >41%, respectively). Only one subject had aGEF <35%. Yap et al. (6) administered 20 ng/kg/hr CCKover 45 min in 40 healthy subjects (19 males and 21 fe-males). The maximum mean GEF was observed 15 minafter termination of CCK infusion. They defined an abnor-mal GEF as <40% on the basis of 3 SD below the mean.
The differences in GEF obtained with rapid versus 30-to 60-min infusions can be explained by the pharmacoki-netics of CCK. Hopman et al. (25) demonstrated that witha 60-min infusion, the pattern of serum CCK levels mim-ics those seen after intraduodenal instillation of fat. On theother hand, following a 1-min infusion, serum levels riserapidly, peak at supraphysiologic levels, and quickly re-turn to baseline. Maximal gallbladder contraction occursat 15–20 min. With longer periods of infusion, gallblad-der contraction occurs until the infusion is discontinued.
Therefore, gallbladder contraction during a 60-min infu-sion was not only stronger but also more consistent andlonger-lasting than that after bolus injection. Moreover,with physiologic infusion rates of CCK, the gallbladdercontracts, but the fundus and the cystic duct do not (26).With supraphysiologic dose rates, the gallbladder, fundus,and cystic duct may contract simultaneously, resulting inobstruction to bile flow and a decreased GEF.
To summarize, the available evidence suggests that 30-to 60-min infusions of CCK are more physiologic andtherefore clinically more appropriate. Nevertheless, moststudies have used shorter durations of infusions (Table 2).As the shorter durations of CCK infusion may result in dif-ferent normative values of GEF and some suggest that clin-ically useful normative values cannot be obtained, com-paring published studies is difficult.
MANAGEMENT
The management of patients with acalculous biliary-type pain poses a therapeutic dilemma. Since the intro-duction of laparoscopic surgery there has been a rise inthe cholecystectomy rate (27) both for calculous gallblad-der disease and for acalculous biliary-type pain. Whethercholecystectomy is appropriate for acalculous biliary-typepain remains controversial. A review of the literature re-veals that assessing outcomes of cholecystectomy for acal-culous disease is fraught with methodological problems.All but three of the published studies are retrospective re-views (28–49, 51), which have well-known limitations andare subject to potential bias. In two series the data werecollected prospectively (7, 50). There has been only oneprospective randomized controlled trial (6). Most studieslack a clear definition of acalculous biliary pain and haveused different doses and rates of infusion of CCK to assessGEF. Not unexpectedly, the definitions of abnormal GEFvary. Finally, many studies consist of small numbers of pa-tients and, often, employ subjective parameters to assesstreatment responses.
These limitations notwithstanding, the proportion ofpatients with acalculous biliary-type pain and abnormalGEF by cholescintigraphy who respond to cholecystec-tomy has ranged from 38% to >90% (Table 3). Al-though most studies have reported high response rates,the possibility of publication bias should be considered.In the only published prospective randomized controlledtrial, Yap et al. (6) studied 21 patients with an abnor-mal GEF and acalculous biliary-type abdominal pain.Eleven patients were randomized to cholecystectomyand 10 to no surgery, with a mean follow-up of almost3 years. An independent observer not involved in the ini-tial treatment and using a standard format of questions
1394 Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005)

ACALCULOUS BILIARY-TYPE ABDOMINAL PAIN
TABLE 3. RESPONSE TO CHOLECYSTECTOMY AND CHOLECYSTECTOMY IN PATIENTS WITH AN ABNORMAL GEF
Abnormal GEF
Cholecystectomy No cholecystectomy
Asymptomatic Improvement No improvement Asymptomatic Improvement No improvement
Yap (6) 10 1 0 0 1 9Westlake (7) 15* — 8 — — —Smith (28) 42* — 6 — — —Pickleman (29) 13 — 1 — — —Canfield (30) 188* — 12 — — —Zech (31) 56 2 1 4* — 7Raptopoulos (32) 3 — 5 — — —Fink-Bennett (34) 110* — 1 13* — 69Misra (35) 58 9 2 0 12 17Tabet (36) 25 22 6 — — —Mishkind (37) 26* — 1 12* — 3Sorenson (38) 11 — — — — —Khosla (39) 20 8 2 — 2 3Adams (40) 35 — 10 — — —Ozden (41) 27 — 13 4* — 4Goncalves (42) 35 9 — 16* — 18Reed (43) 18 10 2 — — —Jones (44) 26 — 3 — — —Barron (45) 38 — — — — —Poynter (46) 17 7 2 — — —Halverson (47) 9 — 2 — — —Klieger (48) 27 — 1 — — —Yost (49) 27* — — 6* — —
*Differentiation between asymptomatic and improved was not made.
relating to pain determined whether the patient was worse,the same, improved, or asymptomatic based on the fre-quency but not the severity of pain symptoms. Followingcholecystectomy, 10 patients became asymptomatic and1 improved, whereas all patients who did not undergosurgery continued to be symptomatic. The authors con-cluded that cholecystectomy alleviates biliary-type pain inpatients with a reduced GEF. The main criticism of thesedata is the absence of sham controls, as the placebo effectin patients with functional disorders is known to be signif-icant. However, physicians have used an abnormal GEFto suggest a diagnosis of chronic acalculous gallbladderdisease in clinical practice.
Others have come to different conclusions when theyhave evaluated the hypothesis that a low GEF predictsgood outcomes following cholecystectomy. Westlakeet al. (7) followed 26 patients with chronic right upperquadrant pain without demonstrable gallstones on ultra-sound who underwent a cholecystectomy. Eighteen pa-tients (69%) improved after cholecystectomy. However,patients who did not improve following cholecystectomyhad a lower GEF (mean = 25%) than those who did(mean = 39%). The authors concluded that the predic-tive value of GEF in patients with acalculous right up-per quadrant pain who would improve with cholecystec-tomy was poor. In a retrospective review of 78 patientswith acalculous biliary-type pain and a subnormal GEF,
Goncalves et al. (42) observed that 6 of 34 patients whodid not undergo cholecystectomy had resolution of symp-toms with expectant treatment. Another 10 patients werefound to have a diagnosis unrelated to the gallbladder asthe cause of pain and all reported symptomatic improve-ment or resolution of pain with appropriate therapy. Theremaining 18 patients reported either no change or wors-ening of their symptoms. The authors concluded that anabnormal GEF alone does not always predict symptomaticgallbladder disease and that alternate diagnoses must beconsidered. Similarly, Mishkind et al. (37) reported that12 of 15 patients (80%) with a subnormal GEF who didnot undergo a cholecystectomy reported lessening or res-olution of symptoms on follow-up. The authors cautionedagainst recommending cholecystectomy to patients whohave an abnormal GEF as the only criterion of gallbladderdisease. Ozden et al. (41) found a 68% symptom reso-lution rate following cholecystectomy in patients with alow GEF but this was similar to the rate for those managedwithout surgery (50%). They questioned the clinical utilityof a low GEF in patients with suspected chronic acalculousgallbladder disease. Finally, Frassinelli et al. (33) found noassociation between GEF and subjective patient relief fol-lowing cholecystectomy. Thus, opinion is divided regard-ing the utility of GEF as a predictor of response to chole-cystectomy, as many patients with acalculous biliary-typepain and an abnormal GEF improve without surgery.
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 1395

RASTOGI ET AL.
TABLE 4. RESPONSE TO CHOLECYSTECTOMY AND NO CHOLECYSTECTOMY IN PATIENTS WITH A NORMAL GEF
Normal GEF
Cholecystectomy No cholecystectomy
Asymptomatic Improvement No improvement Asymptomatic Improvement No improvement
Yap (6) 8 — 6 60 — —Westlake (7) 3 — — — — —Smith (28) 3* — 2 — — —Pickleman (29) 5 — — — — —Zech (31) 1 — — 9 — 3Raptopoulos (32) 1 — — — — —Fink-Bennett (34) 10* — — 130 — 9Misra (35) — — — 35 — 9Mishkind (37) 2 — — 5 3 6Sorenson (38) — — — 5 — 1Khosla (39) 2 — — 9 1 2Adams (40) 4 — 1 — — —Ozden (41) — — — 18 — 10Jones (44) 3 — 1 — — —Klieger (48) 3 — 10 — — 11
*Differentiation between asymptomatic and improved was not made.
Generally, surgery has not been recommended for pa-tients with acalculous biliary-type pain and a normal GEF.Nevertheless, some patients with a normal GEF do have afavorable response after cholecystectomy (Table 4). Fink-Bennett et al. (34) reported that 10 of 11 patients witha GEF >35% who underwent cholecystectomy becameasymptomatic. Yap et al. (6) performed cholecystectomyin 14 patients with a normal GEF, 8 (57%) of whom be-came asymptomatic. Davis et al. (51) observed that pa-tients with acalculous biliary-type pain had a mean GEFof 83% ± 17%, versus 68% ± 27% in normal volunteers.They concluded that the assessment of gallbladder con-traction by any method is not a validated criterion for thepresence of gallbladder disease. Adams et al. (40) opinedthat GEF does not predict who will benefit from cholecys-tectomy and that patients with a “good history” of biliary-type pain should undergo cholecystectomy when there isno evidence of other disorders. Their conclusion is iden-tical to that of Jones et al. (44). Although patients with anormal GEF undergoing cholecystectomy are few, thesereports challenge the validity of GEF as a prognostic or di-agnostic modality when evaluating surgery as a treatmentoption. The summary of the studies in Table 4 demon-strates that approximately 70% of patients (45 of 65) witha normal GEF improved after cholecystectomy, comparedto 84% (275 of 326) without cholecystectomy.
ROLE OF SPHINCTER OF ODDI DYSFUNCTION
IN PATIENTS WITH ACALCULOUS
GALLBLADDER
Whether sphincter of Oddi dysfunction (SOD) con-tributes to acalculous biliary-type pain in patients with
an intact gallbladder is an ongoing controversy whichhas not been well investigated. Classically, SOD has beenimplicated in the pathogenesis of recurrent epigastric orright upper quadrant abdominal pain following cholecys-tectomy. These patients are classified as having biliarytypes I–III (Table 5). Some clinical reports have suggestedthat SOD may exist in patients with an intact gallbladder,although most are published as abstracts. The underly-ing premise of such studies is that SOD may exist be-fore cholecystectomy and may be the underlying causeof symptoms in some of these patients. Two related issuesare whether there is any correlation between SOD and lowGEF and whether endoscopic sphincterotomy (ES) ratherthan laparoscopic cholecystectomy should be performedas first-line therapy in patients with acalculous biliary-typepain.
Ruffolo et al. (21) explored the relationship betweenSOD and low GEF in 81 patients with acalculous biliary-type abdominal pain and normal liver enzymes. Of 30 pa-tients with a normal GEF who underwent sphincter ofOddi manometry (SOM), 17 (57%) had elevated basal
TABLE 5. POSTCHOLECYSTECTOMY “BILIARY-TYPE”PAIN CLASSIFICATION OF BILIARY SOD
Type 1 Biliary painAbnormal liver enzyme levelsFixed SO stenosis on radiograph
Type 2 Biliary painand
Transient elevation of enzyme leveland/or
Dilated bile ductand/or
Delay in emptying of bile ductType 3 Biliary pain only
1396 Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005)

ACALCULOUS BILIARY-TYPE ABDOMINAL PAIN
sphincter pressures. Of 36 patients with an abnormal GEFwho had successful SOM, 20 (56%) had elevated pres-sures. Furthermore, there were no statistically significantdifferences in GEF between patients with normal versuspatients with elevated SO pressures. Kalloo et al. (53)also correlated GEF with SO pressures in 30 patientswith biliary-type abdominal pain, with acalculous gall-bladder. Seven of the 30 patients (23%) had an elevatedbasal SO pressure (>40 mm Hg). Mean GEF in patientswith elevated SO pressure was similar to that in patientswith normal sphincter pressure. Moreover, the frequencyof abnormal GEF (<35%) was similar in both groups. Sotoet al. (54) found a high prevalence of elevated basal SOpressures in patients with biliary-type symptoms and anacalculous gallbladder. A large majority of patients (83%)were found to have SO pressures >40 mm Hg on trancysticbiliary manometry. They also observed a poor correlationbetween GEF and SO pressures. Choudhary et al. (55)described 35 patients with intact gallbladder and elevatedSO pressures, 43% of whom had sustained pain relief afterES alone. Of the 20 nonresponders or those who relapsedafter initial response to ES, 11 underwent cholecystec-tomy, with good pain relief in 8. GEF was not measuredin this study. The combination of ES and cholecystectomyproduced good or excellent responses in 66% of patients.Clearly there is some evidence to suggest that SOD maybe present in some patients with biliary-type pain and in-tact gallbladder. However, there is both a poor correlationand a lack of cause-and-effect data linking GEF and SObasal pressures. GEF does not accurately predict responseto laparoscopic cholecystectomy or biliary ES in patientswith acalculous biliary pain and a gallbladder in situ.
It is also important to emphasize that a number of condi-tions other than gallbladder dysfunction may be associatedwith a low GEF. Kellow et al. (56) demonstrated that sub-jects with diarrhea-predominant irritable bowel syndrome(IBS) had less gallbladder contraction in response to CCKthan did those with constipation-predominant IBS. Soodet al. (57) demonstrated that patients with IBS had higherfasting gallbladder volumes and lower gallbladder emp-tying compared to healthy controls. Tabet et al. (36) ob-served that patients with gallbladder dyskinesia exhibiteda higher incidence of symptoms compatible with IBS com-pared to patients with gallstones. This may explain whysymptoms may persist after cholecystectomy in patientswith gallbladder dyskinesia and supports the hypothesisthat biliary dyskinesia may be a manifestation of a general-ized motor abnormality of the gastrointestinal tract. Otherconditions in which GEF is decreased include diabetes(58), pregnancy (58), idiopathic slow transit constipation(60), obesity (61, 62), and cirrhosis (63). Furthermore,Cole et al. (64) showed that abnormal GEF is often ac-
companied by impaired gastric emptying, suggesting thatdysmotility can involve the gallbladder, stomach, and duo-denum simultaneously. Various drugs including atropine(65), morphine (66), octreotide (67), nifedipine (68), andprogesterone (69) can lower GEF. Therefore, these drugsshould be stopped before measuring GEF. Failure to rec-ognize these causes may result in unnecessary cholecys-tectomy if a low GEF is used as a criterion for surgery.
Based on the incomplete responses to surgery and en-doscopic therapy, there must be alternative explanationsfor symptoms in patients with acalculous biliary pain. Pa-tients with postcholecystectomy SOD type III were shownto have duodenal but not rectal hyperalgesia, and duodenaldistension mimicked pain in most patients (10). This site-specific sensitivity could occur by different mechanisms.Pain may have originated in the gallbladder and/or the bil-iary tree and, through sensory convergence in the dorsalhorn, resulted in duodenal hyperalgesia. Alternatively, theduodenum may have been the original source of symptomsrather than the gallbladder or biliary tree. Finally, hyper-algesia may have been present both in the biliary tree andin the duodenum. Whether these derangements were op-erative at the initial presentation of symptoms prior tocholecystectomy must be considered and warrants furtherstudies of visceral hyperalgesia in patients with acalculousbiliary-type pain.
MANAGEMENT STRATEGIES
The occurrence of biliary-type pain in patients with anacalculous gallbladder continues to remain a difficult andconfusing problem for clinicians. There is general agree-ment that gallstone disease and structural abnormalitiesmust be excluded before the diagnosis of a functional dis-order can be considered. A widely accepted approach fo-cuses on the evaluation of gallbladder and SO functionwith the premise that CCK-cholescintigraphy can identifypatients who will respond to cholecystectomy and ERCPwith SOM can identify which patients may respond tobiliary ES either prior to or after cholecystectomy.
Unfortunately the validity of CCK-CS has not been es-tablished and a low GEF (however defined) might not pre-dict a good outcome after cholecystectomy (70). More-over, even using optimal technique to perform CCK-CSdoes not allow a definition of low GEF to be made withconfidence.
Given the paucity of well-designed studies and the lackof accurate markers of disease, it is difficult to proposean evidence-based treatment algorithm for patients withacalculous biliary-type pain with a gallbladder in situ. Itis important to emphasize that SOD increases the risk forpost-ES pancreatitis, which occurs in up to 22% of patients
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 1397

RASTOGI ET AL.
Fig 1. Suggested management of biliary-type pain in patients with an intact gallbladder.
(71%). Freeman et al. (72) found that a suspected diag-nosis of SOD independently tripled the risk of post-ESpancreatitis to a frequency of 23%. Although laparoscopiccholecystectomy is a comparatively safe procedure, thereis a rate of clinically significant complications rangingbetween 5% and 8% (73, 74).
In view of these considerations, we believe that a conser-vative approach to treatment should be adopted, to includecareful evaluation of psychological issues and the use ofagents with putative modulating effects on chronic visceral
pain such as tricyclic antidepressants (TCAs) (75, 76).We concede that such a recommendation is not evidencebased, as there is a conspicuous absence of clinical trialsof such agents in patients with this syndrome. However,use of TCAs is accepted in other disorders characterizedby chronic or recurrent visceral pain (75, 76), and thepossible role of visceral hyperalgesia is supported by ourstudies in SOD type III (10). Furthermore, the use of suchan approach carries little risk and may obviate the needfor more invasive therapeutic interventions. A suggested
1398 Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005)

ACALCULOUS BILIARY-TYPE ABDOMINAL PAIN
approach to management (Figure 1) differs from that ad-vocated by the Rome II Committee in that pharmaco-logic therapy is advocated when a diagnosis of functionalbiliary-type pain is made; CCK-CS should then be con-sidered if symptoms do not resolve. Patients should becarefully informed that the results of CCK-CS do not nec-essarily predict a good response to cholecystectomy andthat the cause of their pain may not reside in the gallblad-der. High-quality trials of tricyclic agents in sufficientlylarge and well-characterized patient populations carriedout for sufficiently lengthy durations are needed. Simi-larly, higher-quality trials are needed to assess the validityof CCK-CS to determine if patients with a low GEF willbenefit from cholecystectomy.
REFERENCES
1. Barbara L, Sama C, Morselli Labate AM, Taroni F, Rusticalli AG,Festi D, Sapio C, Roda E, Banterle C, Puci A, Formentini F, ColasantiS, Nardin F: A population study on the prevalence of gallstone dis-ease: The Sirmione Study. Hepatology 7:913–917, 1987
2. GREPCO (The Rome Group for Epidemiology and Prevention ofCholelithiasis): The epidemiology of gallstone disease in Rome,Italy. I. Prevalence data in men. Hepatology 8:904–906, 1988
3. GREPCO (The Rome Group for Epidemiology and Prevention ofCholelithiasis): Prevalence of gallstone disease in an Italian adultfemale population. Am J Epidemiol 119:796–805, 1984
4. Corazziari E, Shaffer EA, Hogan WJ, Sherman S, Toouli J:Functional disorders of the biliary tract and pancreas. Gut45(Suppl II):II48–II54, 1999
5. Corazziari E, Shaffer EA, Hogan WJ, Sherman S, Toouli J: Func-tional disorders of the biliary tract and pancreas. In Rome II:The Functional Gastrointestinal Disorders, 2nd ed. Drossman DA,Corazziari E, Talley NJ, Thompson WG, Whitehead WE (eds).McLean, VA, Degnon Associates, 2000, pp 433–482
6. Yap L, Wycherly AG, Morphett AD, Toouli J: Acalculous biliarypain: cholecystectomy alleviates symptoms in patients with abnor-mal cholescintigraphy. Gastroenterology 101:786–793, 1991
7. Westlake PJ, Hershfield NB, Kelly JK, Kloiber R, Lui R, SutherlandR, Shaffer EA: Chronic right upper quadrant pain without gall-stones: Does HIDA scan predict outcome after cholecystectomy?Am J Gastroenterol 85:986–990, 1990
8. Amaral J, Xiao Z, Chen Q, Yu P, Biancani P, Behar J: Gallblad-der muscle dysfunction in patients with chronic acalculous disease.Gastroenterology 120:506–511, 2001
9. Velanovich V: Biliary dyskinesia and biliary crystals: A prospectivestudy. Am Surg 63:69–74, 1997
10. Desautels SG, Slivka A, Hutson WR, Chun A, Mitrani C, DiLorenzoC, Wald A: Postcholecystectomy pain syndrome: pathophysiologyof abdominal pain in sphincter of Oddi type III. Gastroenterology116:900–905, 1999
11. Stolk MF, van Erpecum KJ, Smout AJ Akkermans LM, Jansen JB,Lamers CB, Peeters TL, van Berge-Henegouwen GP: Motor cycleswith phase III in antrum are associated with high motilin levels andprolonged gallbladder emptying. Am J Physiol 264:G596–G600,1993
12. Takahashi T, May D, Owyang C: Cholinergic dependence of gall-bladder response to cholecystokinin in the guinea pig in vivo. Am JPhysiol 261:G565–569, 1991
13. Mawe GM: The role of cholecystokinin in ganglionic transmis-sion in the guinea pig gallbladder. J Physiol (Lond) 439:89–102,1991
14. Mawe GM, Gokin AP, Wells DG: Actions of cholecystokinin andnorepinephrine on vagal input to ganglion cells in guinea pig gall-bladder. Am J Physiol 267:G1146–G1151, 1994
15. Wiley JW, O’Dorisio TM, Owyang C: Vasoactive intestinal polypep-tide mediates cholecystokinin-induced relaxation of sphincter ofOddi. J Clin Invest 81:1920–1924, 1988
16. Pauletzki JG, Sharkey KA, Davison J, et al.: Involvement ofL-arginine–nitric oxide pathways in neural relaxation of the sphinc-ter of Oddi. Eur J Pharmacol 232:263–270, 1993
17. Shaffer E: Acalculous biliary pain: new concepts for an old entity.Dig Liver Dis 35 (Suppl 3):S20–S25, 2003
18. Krishnamurthy GT, Bobba VR, Kingston E: Radionuclide ejectionfraction: a technique for quantitative analysis of motor function ofthe human gallbladder. Gastroenterology 80:482–490, 1981
19. Krishnamurthy GT, Bobba VR, Kingston E, Turner F: Measure-ment of gallbladder emptying sequentially using a single dose of99mTc-labelled hepatobiliary agent. Gastroenterology 83:773–776,1982
20. Krishnamurthy GT, Bobba VR, Kingston E: Optimization of oc-tapeptide of cholecystokinin (OP-CCK) dose for gallbladder empty-ing. In Proceeding of the Third World Congress of Nuclear Medicineand Biology. Raynaud C (ed). Paris, France, Pergamon Press, 1982,pp 2244–2247
21. Mesgarzadeh M, Krishnamurthy GT, Bobba VR, Langrell K: Filling,postcholecystokinin emptying, and refilling of normal gallbladder:effects of two different doses of CCK on refilling: Concise Commu-nication. J Nucl Med 24:666–671, 1983
22. Sarva RP, Shreiner DP, Van Thiel D, Yingvorapant N: Gallbladderfunction: methods for measuring filling and emptying. J Nucl Med26:140–144, 1985
23. Ziessman HA, Fahey FH, Hixson DJ: Calculation of a gallbladderejection fraction: advantage of continuous Sincalide infusion overthe three-minute infusion method. J Nucl Med 33:537–541, 1992
24. Ziessman HA, Muenz LR, Agarwal AK, Zaza AAM: Normal val-ues for Sincalide cholescintigraphy: comparison of two methods.Radiology 221:404–410, 2001
25. Hopman WPM, Jansen JBMJ, Rosenbusch G: Gallbladder contrac-tion induced by cholecystokinin: Bolus injection or infusion? BrMed J 292:375–376, 1986
26. Courtney DF, Clanachan AS, Scott GW: Cholecystokinin constrictsthe canine cystic duct. Gastroenterology 85:1154–1159, 1983
27. Legorreta AP, Silber JH, Constantino GN, Kobylinski RW, ZatzSL: Increased cholecystectomy rate after the introduction of laparo-scopic cholecystectomy. JAMA 270:1429–1434, 1993
28. Smith A, Chapman C, Cunningham P: The utility of CCK DISIDAscan in the treatment of occult biliary tract disease. Am Surg 61:220–225, 1995
29. Pickleman J, Peiss RL, Henkin R, Salo B, Nagel P: The role of Sin-calide cholescintigraphy in the evaluation of patients with acalculusgallbladder disease. Arch Surg 120:693–697, 1985
30. Canfield AJ, Hetz SP, Schriver JP, Servis HT, Hovenga TL, CiranglePT, Burlingame BS: Biliary dyskinesia: a study of more than 200 pa-tients and review of the literature. J Gastrointest Surg 2:443–448,1998
31. Zech ER, Simmons LB, Kendrick RR, Soballe PW, Olcese JAM,Goff WB II, Lawrence DP, DeWeese RA: Cholecystokinin enhancedhepatobiliary scanning with ejection fraction calculation as an indi-cator of disease of the gallbladder. Surg Gynecol Obstet 172:21–24,1991
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 1399

RASTOGI ET AL.
32. Raptopoulos V, Compton CC, Doherty P, Smith EH, D’Orsi CJ,Patwardhan NA, Goldberg R: Chronic acalculous gallbladder dis-ease: multiimaging evaluation with clinical–pathologic correlation.Am J Roentgenol 147:721–724, 1986
33. Frassinelli P, Werner M, Reed JF, Scagliotti C: Laparoscopic chole-cystectomy alleviates pain in patients with acalculous biliary dis-ease. Surg Laparosc Endosc 8:30–34, 1998
34. Fink-Bennett D, DeRidder P, Kolozsi WZ, Gordon R, Jaros R:Cholecystokinin cholescintigraphy: detection of abnormal gallblad-der motor function in patients with chronic acalculous gallbladderdisease. J Nucl Med 32:1695–1699, 1991
35. Misra DC, Blossom GB, Fink-Bennett D, Glover JL: Results ofsurgical therapy for biliary dyskinesia. Arch Surg 126:957–960,1991
36. Tabet J, Anvari M: Laparoscopic cholecystectomy for gallbladderdyskinesia: clinical outcome and patient satisfaction. Surg LaparoscEndosc 9:382–387, 1999
37. Mishkind MT, Pruitt RF, Bambini DA, Hakenewerth AM, ThomasonMH, Zuger JH, Novick T: Effectiveness of cholecystokinin-stimulated cholescintigraphy in the diagnosis and treatment of acal-culous gallbladder disease. Am Surg 63:769–774, 1997
38. Sorenson MK, Fancher S, Lang N, Eidt JF, Broadwater JR:Abnormal gallbladder nuclear ejection fraction predicts success ofcholecystectomy in patients with biliary dyskinesia. Am J Surg166:672–675, 1993
39. Khosla R, Singh A, Miedema BW, Marshall JB: Cholecystectomyalleviates acalculous biliary pain in patients with a reduced gallblad-der ejection fraction. South Med J 90:1087–1090, 1997
40. Adams DB, Tarnasky PR, Hawes RH, Cunningham JT, BrookerC, Brothers TE, Cotton PB: Outcome after laparoscopic chole-cystectomy for chronic acalculous cholecystitis. Am Surg 64:1–6,1998
41. Ozden N, DiBaise JK: Gallbladder ejection fraction and symptomoutcome in patients with acalculous biliary-like pain. Dig Dis Sci48:890–897, 2003
42. Goncalves RM, Harris, JA, Rivera DE: Biliary dyskinesia: naturalhistory and surgical results. Am Surg 64:493–498, 1998
43. Reed DN Jr, Fernandez M, Hicks RD: Kinevac-assisted cholescintig-raphy as an accurate predictor of chronic acalculus gallbladder dis-ease and the likelihood of symptom relief with cholecystectomy.Am Surg 59:273–277, 1993
44. Jones DB, Soper NJ, Brewer JD, Quasebarth MA, Swanson PE,Strasberg SM, Brunt LM: Chronic acalculous cholecystitis: laparo-scopic treatment. Surg Laparosc Endosc 6:114–122, 1996
45. Barron LG, Rubio PA: Importance of accurate preoperative diagno-sis and role of advanced laparoscopic cholecystectomy in relievingchronic acalculous cholecystitis. J Laparoendosc Surg 5:357–361,1995
46. Poynter MT, Saba AK, Evans RA, Johnson WM, Hasl DM: Chronicacalculous biliary disease: Cholecystokinin cholescintigraphy isuseful in formulating treatment strategy and predicting success aftercholecystectomy. Am Surg 68:382–384, 2002
47. Halverson JD, Garner BA, Siegel BA, Alexander R, EdmundowiczSA, Campbell W, Miller JE: The use of hepatobiliary scintigraphy inpatients with acalculous biliary colic. Arch Intern Med 152:1305–1307, 1992
48. Klieger PS, O’Mara RE: The clinical utility of quantitative cho-lescintigraphy: the significance of gallbladder dysfunction. ClinNucl Med 23:278–282, 1998
49. Yost F, Margenthaler J, Presti M, Burton F, Murayama K: Cholecys-tectomy is an effective treatment for biliary dyskinesia. Am J Surg178:462–465, 1999
50. Chen PFM, Nimeri A, Pham QHT, Yuh J, Gusz JR, ChungRS: The clinical diagnosis of chronic acalculous cholecystitis.Surgery130:578–583, 2001
51. Davis GB, Berk RN, Scheible FW, Witztum KF, Gilmore IT, StrongRM, Hofmann AF: Cholecystokinin cholecystography, sonography,and scintigraphy: detection of chronic acalculous cholecystitis. AmJ Roentgenol 139:1117–1121, 1982
52. Ruffolo TA, Sherman S, Lehman GA, Hawes RH: Gallbladder ejec-tion fraction and its relationship to sphincter of Oddi dysfunction.Dig Dis Sci 39:289–292, 1994
53. Kalloo AN, Sostre S, Meyerrose GE, Pasricha PJ, Szabo Z:Gallbladder ejection fraction. Nondiagnostic for sphincter of Oddidysfunction in patients with intact gallbladders. Clin Nucl Med19:713–719, 1994
54. Soto DJ, Arregui ME: Kinevac stimulated ultrasound corre-lated with biliary manometry and clinical outcome in patientswith chronic acalculous cholecystitis. Gastroenterology 120:A471,2001
55. Choudhry U, Ruffolo T, Jamidar P, Hawes R, Lehman G: Sphinc-ter of Oddi dysfunction in patients with intact gallbladder: thera-peutic response to endoscopic sphincterotomy. Gastrointest Endosc39:492–495, 1993
56. Kellow JE, Miller LJ, Phillips SF, Zinsmeister AR, Charboneau JW:Altered sensitivity of the gallbladder to cholecystokinin octapeptidein irritable bowel syndrome. Am J Physiol G650–G655, 1987
57. Sood GK, Baijal SS, Lahoti D, Broor SL: Abnormal gallbladderfunction in patients with irritable bowel syndrome. Am J Gastroen-terol 88:1387–1390, 1993
58. Schreiner DP, Sarva RP, Van Thiel D, Yingvorapant N: Gallbladderfunction in diabetic patients. J Nucl Med 27:357–360, 1986
59. Braverman DJ, Johnson ML, Kern F: Effects of pregnancy and con-traceptive steroids on gallbladder function. N Engl J Med 302:362–364, 1980
60. Hemingway D, Neilly JB, Finlay IG: Biliary dyskinesia in idiopathicslow-transit constipation. Dis Col Rectum 39:1303–1307, 1996
61. Marzio L, Capone F, Neri M, Mezzetti A, De Angelis C, CuccurulloF: Gallbladder kinetics in obese patients. Effect of a regular mealand low caloric meal. Dig Dis Sci 33:4–9, 1988
62. Vezina WC, Paradis RL, Grace DM, Zimmer RA, Lamont DD,Rycroft KM, King ME, Hutton LC, Chey WY: Increased volume anddecreased emptying of the gallbladder in large (morbidly obese, tallnormal, and muscular normal) people. Gastroenterology 98:1000–1007, 1990
63. Kao CH, Hsieh JF, Tsai SC, Ho YJ, Chen SD: Evidence of im-paired gallbladder function in patients with liver cirrhosis by quanti-tative radionuclide scintigraphy. Am J Gastroenterol 95:1301–1304,2000
64. Cole A, Solomon G, Miner PB: The triangle of dysmotility: con-cordance of impaired gastric emptying with abnormal gallbladderemptying. Am J Gastroenterol 96:A51, 2001 (abstr)
65. Garrigues V, Ponce J, Cano C, Sopena R, Hoyos M, Del Val A,Berenguer J: Effect of selective and non-selective muscarinic block-ade on cholecystokinin-induced gallbladder emptying in man. DigDis Sci 37:101–104, 1992
66. Worobetz LJ, Baker RJ, McCallum JA, Wells G, Sullivan SN:The effect of naloxone, morphine and an enkephaline analogue oncholecystokinin octapeptide stimulated gallbladder emptying. Am JGastroenterol 77:509–511, 1982
67. Xian-Feng Z, Shi YF, Qin-Dai, Zhu XF, Shi YF, Qin-Dai, ZhangJX, Harris AG: Effect of small doses of somatostatin analogue—octreotide, on gallbladder contractility in normal chinese adults. DigDis Sci 37:105–108, 1992
1400 Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005)

ACALCULOUS BILIARY-TYPE ABDOMINAL PAIN
68. Clas D, Hould FS, Rosenthal L, Arzoumanian A, Fried GM: Nifedip-ine inhibits cholecystokinin-induced gallbladder contraction. J SurgRes 46:479–483, 1989
69. Shaffer EA, Taylor PJ, Logan K, Gadomski S, Corenblum B: Theeffect of progestin on gallbladder function in young women. Am JObstet Gynecol 148:504–507, 1984
70. DiBaise JK, Oleynikov D: Does gallbladder ejection fraction predictoutcomes after cholecystectomy for suspected chronic acalculousgallbladder dysfunction. A systematic review. Am J Gastroenterol98:2605–2611, 2003
71. Vandervoort J, Soetikno RM, Tham TCK, Wong RCK, Ferrari Jr AP,Montes H, Roston AD, Slivka A, Lichtenstein DR, Ruymann FW,Van Dam J, Hughes M, Carr-Locke DL: Risk factors for complica-tions after performance of ERCP. Gastrointest Endosc 56:652–656,2002
72. Freeman ML, DiSario JA, Nelson DB, Fennerty MB, Lee JG,Bjorkman DJ, Overby CS, Aas J, Ryan ME, Bochna GS, ShawMJ, Snady HW, Erickson RV, Moore JP, Roel JP: Risk factors forpost-ERCP pancreatitis: a prospective multicenter study. Gastroin-test Endosc 54:425–434, 2001
73. The Southern Surgeons Club: A prospective analysis of 1518laparoscopic cholecystectomies. N Engl J Med 324:1073–1078,1991
74. Orlando III R, Russell JC, Lynch J, Mattie A: Laparoscopic chole-cystectomy: a statewide experience. Arch Surg 128:494–499, 1993
75. Cannon RO III, Quyyumi A, Mincemoyer R, et al.: Imipramine inpatients with chest pain despite normal coronary angiograms. N EnglJ Med 330:1411–1417, 1996
76. Wald A: Psychotropic agents in irritable bowel sydrome. J ClinGastroenterology 35(Suppl):553–557, 2002
Digestive Diseases and Sciences, Vol. 50, No. 8 (August 2005) 1401