contribution of the obturator nerve block in the trans-urethral ...
3
47 Indian J. Anaesth. 2004; 48 (1) : 47-49 CONTRIBUTION OF THE OBTURATOR NERVE BLOCK IN THE TRANS-URETHRAL RESECTION OF BLADDER TUMOURS Dr. Dipika Patel 1 Dr. Bhavana Shah 2 Dr. B. M. Patel 3 SUMMARY We selected 50 patients, scheduled for trans-urethral resection of bladder tumor and divided them into two equal groups; Group-SA received only spinal anesthesia and group-SAOB received both Spinal anesthesia + Obturator Nerve Block, for the proposed surgery in addition, obturator nerve block was given with 1% lidocaine 10 ml, unilaterally or bilaterally according to position of the bladder tumor. We observed that in group-SAOB, adductor spasm of lower limb did not occur in most of patients, whereas adductor spasm was seen in almost all the patients of group-SA which disturbed the surgeon. Bladder perforation occurred in 2 patients in group-SA and emergency laparotomy had to be done in 1 patient. We conclude that obturator nerve block is an effective method of preventing adductor spasm and the associated complications is patients undergoing trans urethral resection of bladder under spinal anaesthesia. Keywords : Trans-Urethral resection of bladder tumor, Adductor spasm, Obturator nerve block, Spinal anaesthesia. 1. Assistant Professor 2. Associate Professor 3. Prof. and HOD Department of Anaesthesiology, Gujarat cancer and research institute, Ahmedabad-380016 Gujarat, INDIA. Correspond to : Dr. Dipika Patel A/43, Krushna Krupa, Karmacharinagar-II Ghatlodia, Ahmedabad-380061. Gujarat, INDIA. E-Mail : [email protected] (Accepted for publication on 08-09-2003) Introduction The obturator nerve passes in close proximity to the inferolateral surface of bladder neck and lateral prostatic urethra. As it courses through the pelvis, during trans- urethral operations, resection in these areas invariably stimulates the obturator nerve, with resultant mass contraction of the adductor muscles. The violent jerking of the legs disturbs the surgeon causing inadequate resection and may also lead to an inadvertent bladder perforation. Although stimulation of the obturator nerve is not an uncommon problem, very little has been reported in the literature about its management. Various measures available for its prevention are: 1) Spinal anesthesia 2) Spinal plus general anesthesia 3) Reversal in the polarity of the electrical element 4) Change in the site of the inactive electrode or in current frequency 5) Nerve cooling But unfortunately, all of the above techniques have been proved ineffective. Local obturator nerve blockade has been used extensively in the management of adductor spasm. 1,2 The technique was described in 1965, by Prentiss and associates and they advocated its use preventing the adductor spasm during transurethral operation. 3 Material and methods With approval of the institutional ethics committees and after obtaining of written informed consent, we selected 50 patients, aged between 45 and 80 years belonging to ASA physical status I-III, having inferolateral and bladder neck tumors who were scheduled for trans- urethral resection of bladder tumor and divided them into SA and SAOB groups of 25 patients each. All the patients were administered spinal anesthesia, but in addition, patients of group SAOB received obturator nerve block with 1% lignocaine 10 ml, unilaterally or bilaterally according to tumor position. We monitored NIBP, pulse, SpO 2 and ECG intraoperativly and observed specially for adductor spasm during lateral wall tumor resection in both the groups. Obturator nerve block was administered to the patients in supine position with leg flexed at knee joint and leg slightly abducted a 22 G 10 cm long spinal needle was inserted at a point 2 cm below and 2 cm lateral to pubic tubercle. The needle was advanced perpendicular to the superior ramus of the pubic bone until it touches the bone. The needle was then slightly withdrawn and redirected to walk of the inferior margin of the superior pubic ramus. The needle is advanced up to 1.5 to 2 cm beyond the depth at which pubic ramus is contacted and 10 ml 1% lignocaine was injected in a fan shape manner (fig. 1,2,3,4 and 5).
Transcript of contribution of the obturator nerve block in the trans-urethral ...
DIPIKA, SHAH, PATEL : OBTURATOR NERVE BLOCK FOR BLADDER TUMOURS 47Indian J. Anaesth. 2004; 48 (1) : 47-49
CONTRIBUTION OF THE OBTURATOR NERVE BLOCK INTHE TRANS-URETHRAL RESECTION OF BLADDER TUMOURS
Dr. Dipika Patel1 Dr. Bhavana Shah2 Dr. B. M. Patel3
SUMMARYWe selected 50 patients, scheduled for trans-urethral resection of bladder tumor and divided them into two equal groups; Group-SAreceived only spinal anesthesia and group-SAOB received both Spinal anesthesia + Obturator Nerve Block, for the proposed surgeryin addition, obturator nerve block was given with 1% lidocaine 10 ml, unilaterally or bilaterally according to position of the bladdertumor. We observed that in group-SAOB, adductor spasm of lower limb did not occur in most of patients, whereas adductor spasmwas seen in almost all the patients of group-SA which disturbed the surgeon. Bladder perforation occurred in 2 patients in group-SAand emergency laparotomy had to be done in 1 patient. We conclude that obturator nerve block is an effective method of preventingadductor spasm and the associated complications is patients undergoing trans urethral resection of bladder under spinal anaesthesia.Keywords : Trans-Urethral resection of bladder tumor, Adductor spasm, Obturator nerve block, Spinal anaesthesia.
1. Assistant Professor2. Associate Professor3. Prof. and HOD
Department of Anaesthesiology,Gujarat cancer and research institute,Ahmedabad-380016 Gujarat, INDIA.Correspond to :Dr. Dipika PatelA/43, Krushna Krupa, Karmacharinagar-II Ghatlodia,Ahmedabad-380061. Gujarat, INDIA.E-Mail : [email protected](Accepted for publication on 08-09-2003)
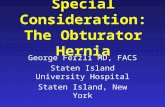
IntroductionThe obturator nerve passes in close proximity to
the inferolateral surface of bladder neck and lateral prostaticurethra. As it courses through the pelvis, during trans-urethral operations, resection in these areas invariablystimulates the obturator nerve, with resultant masscontraction of the adductor muscles. The violent jerkingof the legs disturbs the surgeon causing inadequate resectionand may also lead to an inadvertent bladder perforation.
Although stimulation of the obturator nerve is notan uncommon problem, very little has been reported inthe literature about its management. Various measuresavailable for its prevention are:
1) Spinal anesthesia2) Spinal plus general anesthesia3) Reversal in the polarity of the electrical element4) Change in the site of the inactive electrode or in
current frequency5) Nerve cooling
But unfortunately, all of the above techniques havebeen proved ineffective.
Local obturator nerve blockade has been usedextensively in the management of adductor spasm.1,2 Thetechnique was described in 1965, by Prentiss and associatesand they advocated its use preventing the adductor spasmduring transurethral operation.3
Material and methodsWith approval of the institutional ethics committees
and after obtaining of written informed consent, weselected 50 patients, aged between 45 and 80 yearsbelonging to ASA physical status I-III, having inferolateraland bladder neck tumors who were scheduled for trans-urethral resection of bladder tumor and divided them intoSA and SAOB groups of 25 patients each. All the patientswere administered spinal anesthesia, but in addition,patients of group SAOB received obturator nerve blockwith 1% lignocaine 10 ml, unilaterally or bilaterallyaccording to tumor position. We monitored NIBP, pulse,SpO2 and ECG intraoperativly and observed speciallyfor adductor spasm during lateral wall tumor resection inboth the groups.
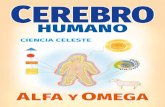
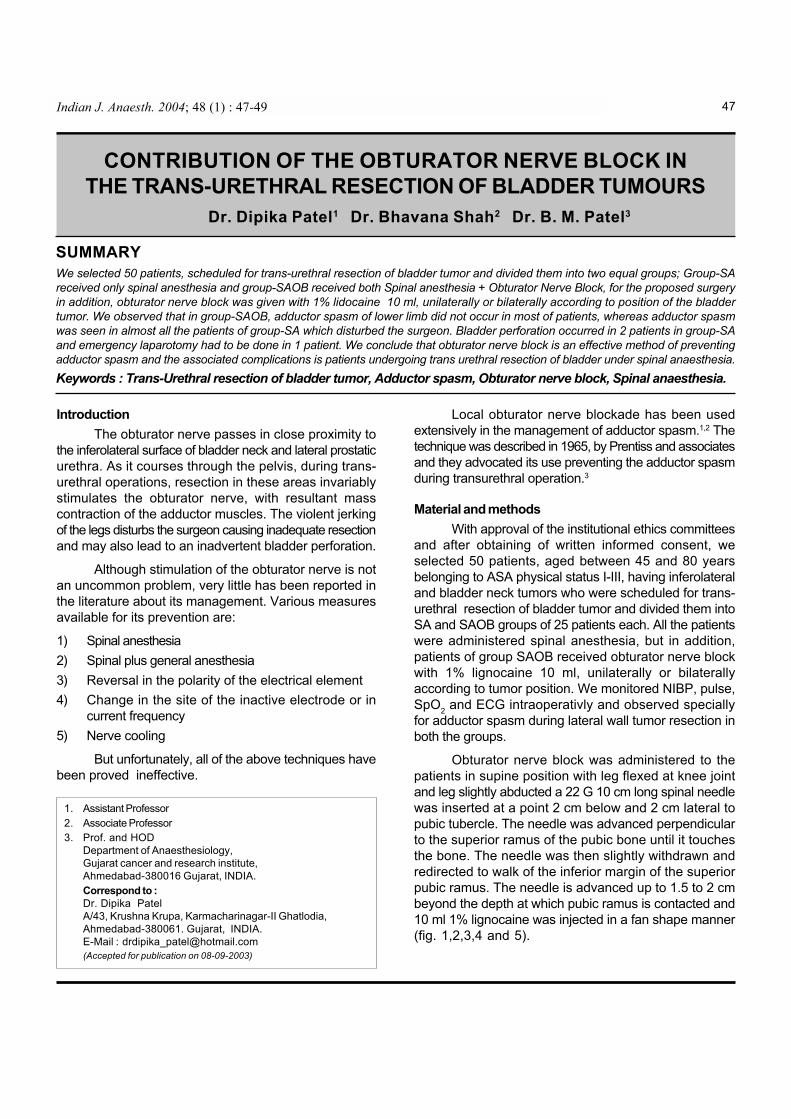
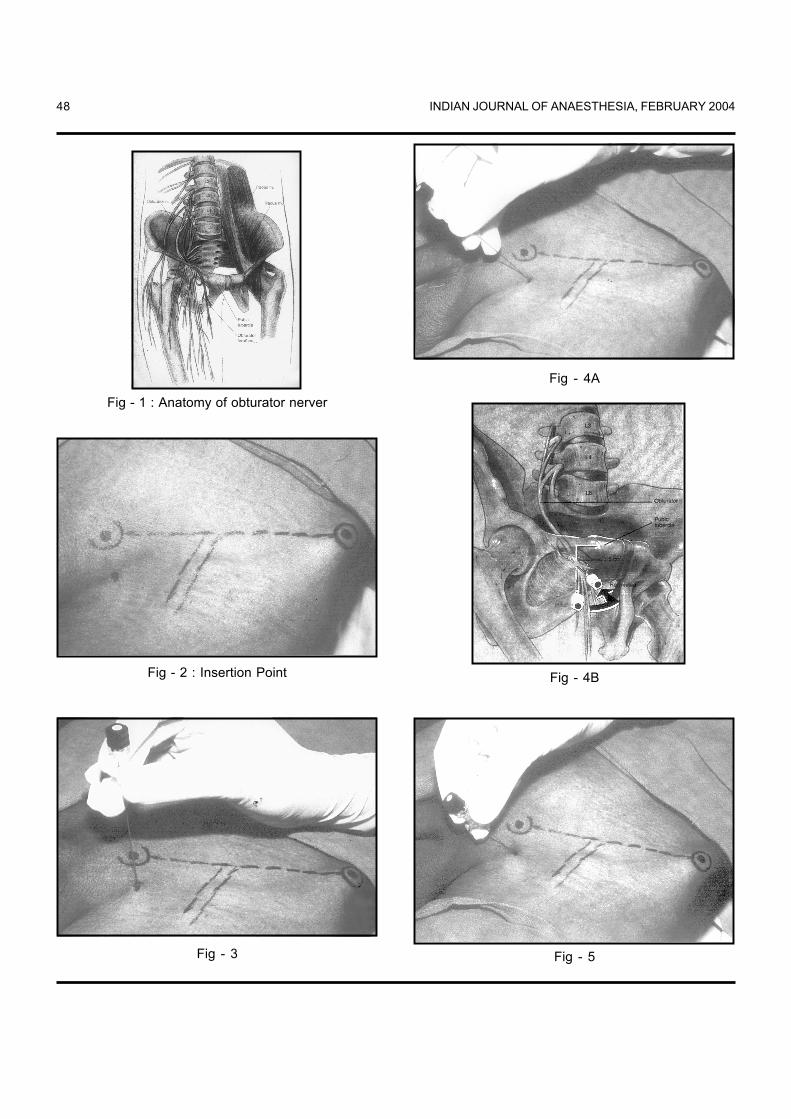
Obturator nerve block was administered to thepatients in supine position with leg flexed at knee jointand leg slightly abducted a 22 G 10 cm long spinal needlewas inserted at a point 2 cm below and 2 cm lateral topubic tubercle. The needle was advanced perpendicularto the superior ramus of the pubic bone until it touchesthe bone. The needle was then slightly withdrawn andredirected to walk of the inferior margin of the superiorpubic ramus. The needle is advanced up to 1.5 to 2 cmbeyond the depth at which pubic ramus is contacted and10 ml 1% lignocaine was injected in a fan shape manner(fig. 1,2,3,4 and 5).
INDIAN JOURNAL OF ANAESTHESIA, FEBRUARY 200448
Fig - 1 : Anatomy of obturator nerver
Fig - 2 : Insertion Point
Fig - 3
Fig - 4A
Fig - 4B
Fig - 5

DIPIKA, SHAH, PATEL : OBTURATOR NERVE BLOCK FOR BLADDER TUMOURS 49
ObservationsOut of 25 patients of group SA almost all patients
developed adductor spasm of varying degree disturbingthe surgeon. Bladder perforation occurred in 2 patientsand emergency laparotomy had to be performed in onepatient. Out of 25 patients of group SAOB, only onepatient developed adductor spasm of milder variety andthe spasm was completely absent in the remaining 24patients.
Complications of the obturator nerve block:Likely, complications because of improper needle
placement :
1) Visceral puncture2) Intravascular injection
Technique is contraindicated in infection over groin area.
Alternative approaches of nerve block :1) Inter-adductor approach4
2) Inguinal para-vesicular or 3 in 1 block
DiscussionThe adduction of thigh results from direct stimulation
of the motor neurons within the obturator nerve. Thus,elimination of the contraction can be achieved throughblockade of the neuromuscular transmission with agentsuch as succinylcholine or other neuromuscular blockingdrugs5 or local anaesthetic blockade distal to the site ofstimulation.
Neuromuscular blockade has been advocated fortransurethral operations by Hobika4, Narins5 but it hasinherant disadvantage of requiring general anesthesia andoften endotracheal intubation.6
Richard R Augsparger and Robert E Donle hadadministered obturator nerve block in 13 patients, plannedfor TURBT. Out of 13 procedures, 11 resulted in completeablation and 2 resulted in approximately 80% reduction ofthe adductor spasm.7
Atnassoff P G Weiss B M et al had studied variousmethods for prevention of adductor spasm in transurethralresection of bladder tumor surgery and did electromyographiccomparison of obturator nerve block to 3 in 1 block method.8
In our study, we had administered obturator nerveblock with spinal anesthesia in patients of group SAOBand observed for development of adductor spasm. Out of25 patients, 24 patients resulted in complete ablation ofspasm and 1 resulted in approximately 80 % reduction of
adductor spasm. This may be attributed to the presence ofaccessory obturator nerve in 2% of the patients population.
In control group SA in almost all the patientsadductor spasm of varying degree which was disturbing tothe surgeon. Bladder perforation occurred in 2 patientsand emergency exploratory laparotomy had to be done inone patient.
The associated complications of the obturator nerveblock as noted in the literature include visceral punctureand intra vascular injection of the drug both of which mayoccur due to improper placement of the needle. Obturatornerve block is contraindicated in patients having localinfection at the site of puncture of the needle. In suchpatients alternative approaches viz. interadductor approachor 3 in 1 block or inguinal para-vascular approach may beattempted.
We infer that, the obturator nerve block can be aneffective and safe method to prevent adductor spasm intrans-urethral resection of lateral wall bladder tumor, underspinal anaesthesia.
References1. Creevy, C. D : Preventing stimulation of the obturator nerve
during transurethral surgery. The Journal of Urology 1969;101: 368.
2. Deliveliotis C, Alexopoulou K, Ple ramenors D. Thecontribution of obturator nerve Block in TURBT. Acta urologyBelgium: 1995; 63(3): 51-54.
3. Prentiss R J, Harvey G W Bethard, W F Boatwright D E andPennington R D. Massive adductor muscle contraction intransurethral surgery : cause and prevention:Development ofnew electrical circuitry. The Journal of Urology: 1965; 93:263.
4. Hobika J H and Clarke B G: Use of neuromuscular blockingdrugs to counteract thigh-adductor spasm induced by electricalshocks of the obturator nerve during trans-urethral resectionof bladder tumors.The Journal of Urology 1961; 85: 295.
5. Narins L and Lief P A: Abolition of mass femoral muscularcontractions during Transurethral resection: Journal mountSinai Hosp 1957; 24: 23.
6. Richard R Augspurger and Robert E Donotle, Prevention ofobturator nerve stimulation during trans-urethral surgery. TheJournal of Urology 1980; 123: 170-171.
7. Atnassoff P G Weiss B M Brull J J et al. Electromyoghraphiccomparison of Obturator Nerve block to 3 in 1 block. AnesthAnalg 1995; 81: 529-533.
8. Wassef M R : Interadductor approach to obturator nerveblockade for spastic condition of adductor thigh muscles. RegAnesth 1992; 18: 13-17.