
Continuing Education Webinar Series Program Handouts... · Presentation Recording •Session will...
62
Continuing Education Webinar Series
Transcript of Continuing Education Webinar Series Program Handouts... · Presentation Recording •Session will...

Continuing Education
Webinar Series

All Content © 2015 Immucor, Inc.
22 February Donor Selection of Solid Organ
Transplant: Is Virtual Xmatch better
than real?
28 February Proficiency, Competency, and QC: A
practical approach to CLIA
requirements and AABB, CAP, and
Joint Commission Expectations
22 March
Clinical Significance of HLA Antibodies
in Solid Organ Transplantations
Future Webinars
Link to register:
https://immucor.webinato.com/register

All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc.
Handouts
http://www.immucor.com/en-us/Pages/Educational-Program-Handouts.aspx

All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc.
Continuing Education
• ABHI, PACE, Florida and California DHS
• 1.0 Contact Hours
• Each attendee must register to receive CE at: https://www.surveymonkey.com/r/HLAImmucor
• Registration deadline is March 2, 2018
• Certificates will be sent via email only to those
who have registered by March 16, 2018

All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc.
Presentation Recording
• Session will be recorded and posted.
– Access information will be sent to each
registrant when the recording becomes
available
• CE credits will be issued to anyone who
listens to the recording within one year of
the original presentation date (today).
Learn website: learn.immucor.com

All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc.
Questions?
• You are all muted
• Type in questions

All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc. All Content © 2015 Immucor, Inc.
• Course content is for information and illustration
purposes only. Immucor makes no
representation or warranties about the accuracy
or reliability of the information presented, and
this information is not to be used for clinical or
maintenance evaluations.
• The opinions contained in this presentation are
those of the presenter and do not necessarily
reflect those of Immucor.

Testing for HLA Antibodies: We’re Not the Chemistry Lab
Michael D. Gautreaux, Ph.D., D.ABHI

Impact of HLA Ab in Transplantation
•Pre- and peri-transplant – Access to transplantation
– Short-term survival (hyperacute, accelerated)
•Post-transplant – Survival
» Acute and chronic rejection
– Marker for rejection response

PRA
• Panel Reactive Antibody
• Percent Reactive Antibody
• Intended to be an assessment of transplantability.
• 20% PRA means that a recipient should crossmatch positive with 20% of donors
• DO NOT CONFUSE WITH TITER
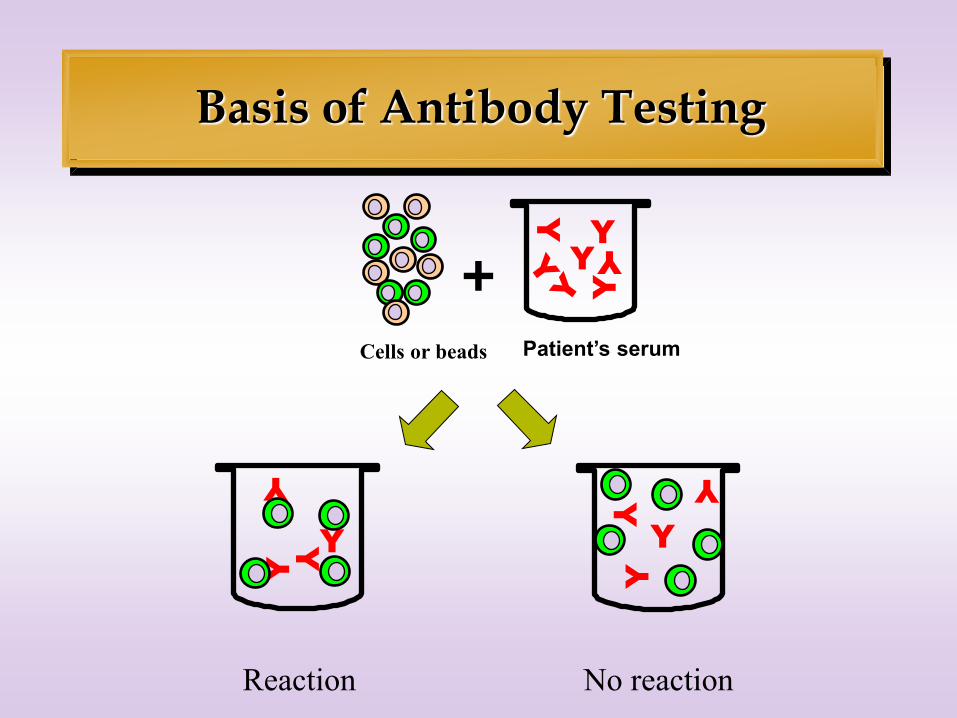
Basis of Antibody Testing
+ Y
Y
Y Y
Y
Patient’s serum Cells or beads
Reaction No reaction
Y
Y
Y Y
Y Y

PRA Techniques
•Complement-dependent cytotoxicity
•(original gold standard; usually augmented)
•Flow cytometry
•(mostly solid phase)
•Solid Phase
•(ELISA & Luminex)
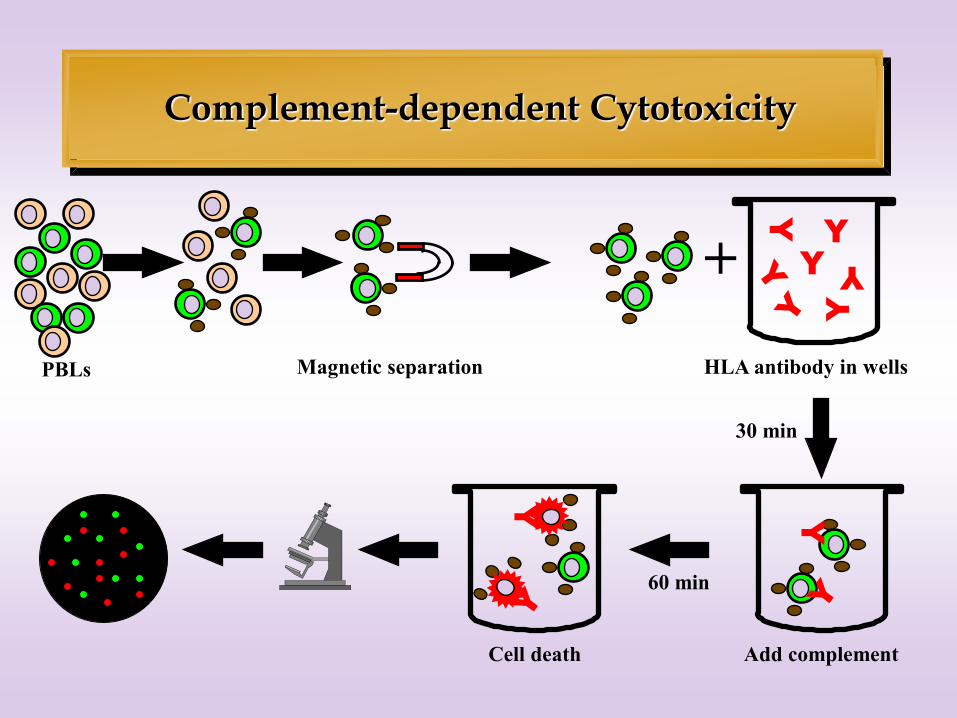
Complement-dependent Cytotoxicity
+
30 min
Add complement
60 min
Y
Y
Y
Y
Y
Y
Cell death
Y
Magnetic separation HLA antibody in wells PBLs
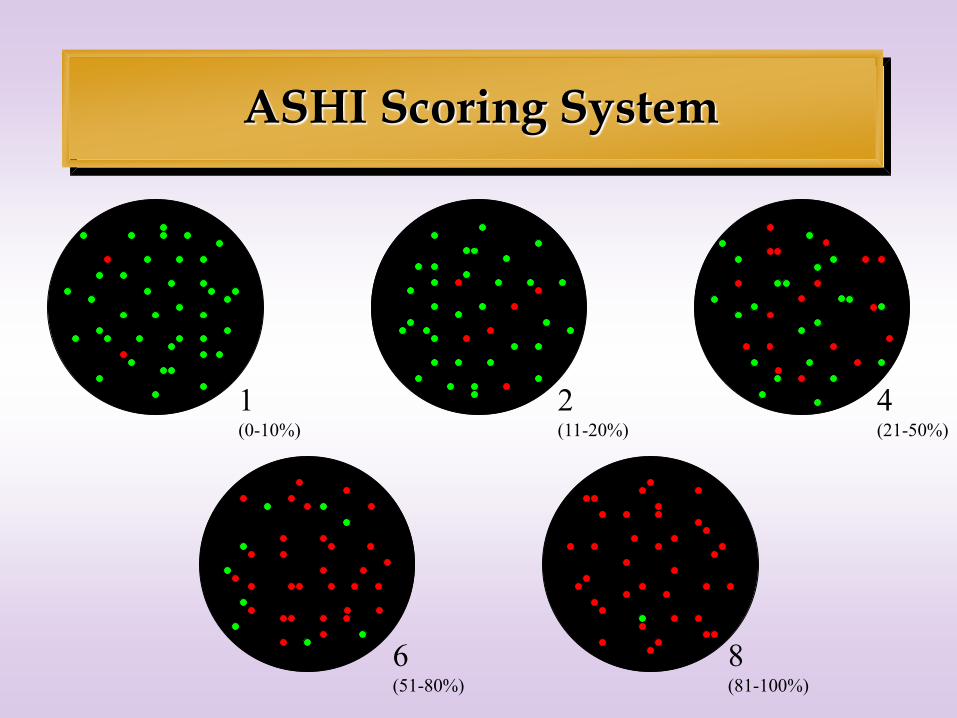
ASHI Scoring System
1 (0-10%)
2 (11-20%)
4 (21-50%)
6 (51-80%)
8 (81-100%)

Determination of Significance
+ -
+
a
TP
+/+
b
FP
-/+
-
c
FN
+/-
d
TN
-/-
Correlation Coefficient (r)
r = a*d - b*c
SQRT (A*B*C*D)
Chi square (c2)
c2 = r 2 * T
Serum
reactivity
Antigen
A = a + b
B = c + d
C = a + c D = b + d
T = Total #
p value depends on degrees of freedom
2 x 2 tables have 1 degree of freedom
c2 2.7055 3.8415 6.6349 7.8794
p 0.1 0.05 0.01 0.005

+ -
+ 14 3
- 1 21
A2
Serum
reactions
r = a*d - b*c
SQRT (A*B*C*D)
r = 14*21 - 3*1
SQRT (17*22*15*24)
r = 0.793
c2 = 0.7932 * 39
c2 = 24.52
p < 0.0001
c2 = r 2 * T

Luminex - xMAP
Luminex’s xMAP Technology combines fluidics, optics, and digital signal processing with proprietary microsphere technology to deliver multiplexed assay capabilities that are configured to perform a wide variety of bioassays quickly, cost-effectively and accurately.
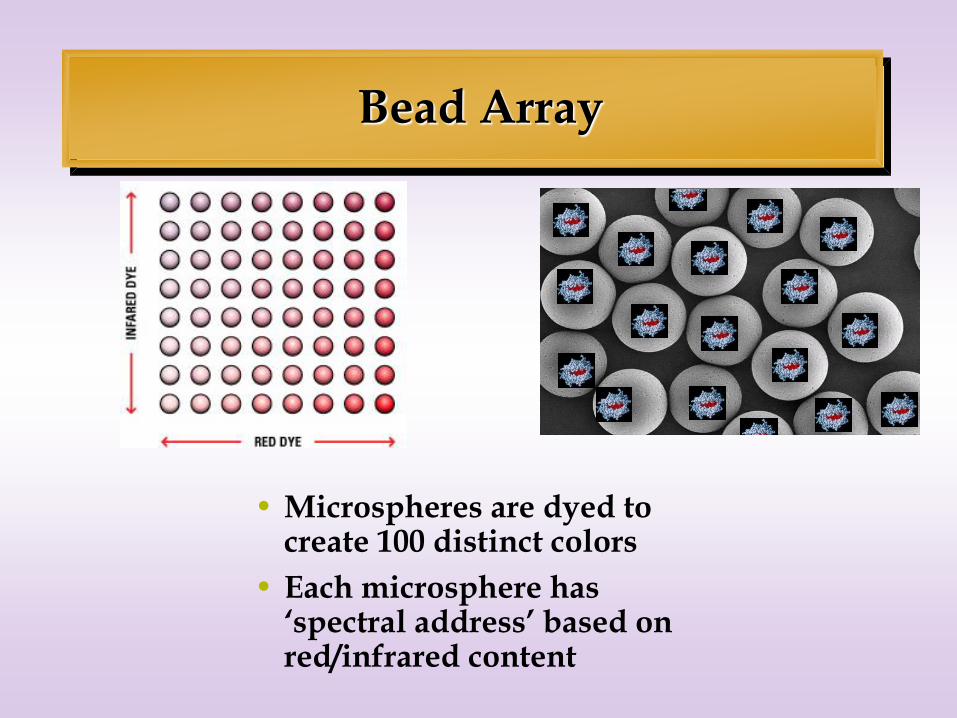
Bead Array
• Microspheres are dyed to create 100 distinct colors
• Each microsphere has ‘spectral address’ based on red/infrared content
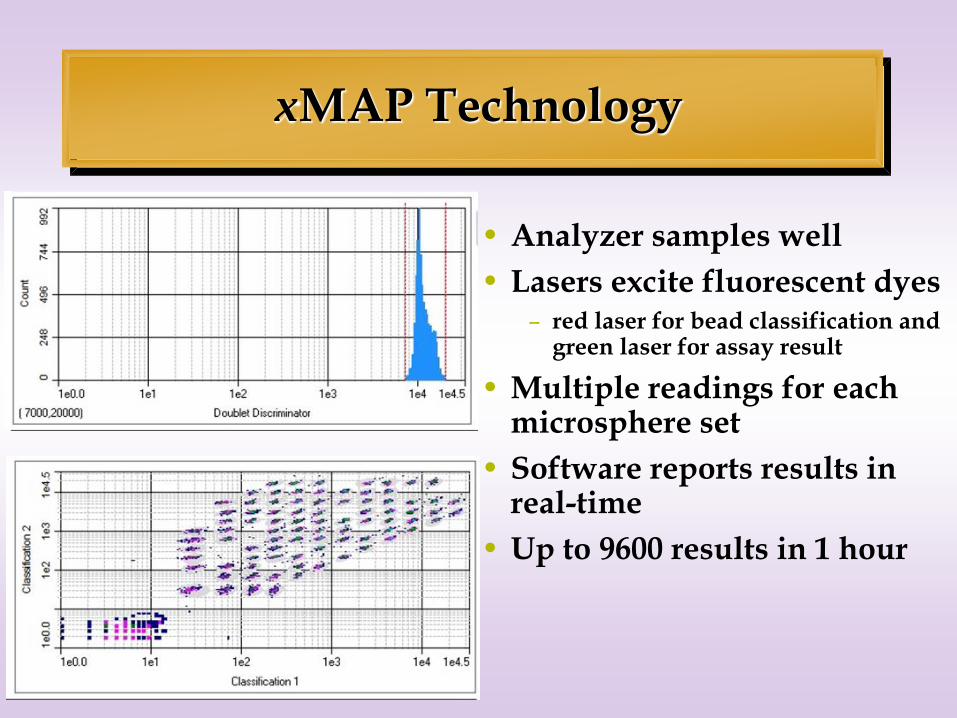
• Analyzer samples well
• Lasers excite fluorescent dyes – red laser for bead classification and
green laser for assay result
• Multiple readings for each microsphere set
• Software reports results in real-time
• Up to 9600 results in 1 hour
xMAP Technology

_ Analysis Software

HLA Antibody Testing by Luminex
Does the MFI of anti-A2 affect the sCr? AM MFI is 2,500 but PM is 3,000 What is your cut-off MFI? Well, that MFI is too low to matter. MFI STOP!!!!!!! MFI MFI
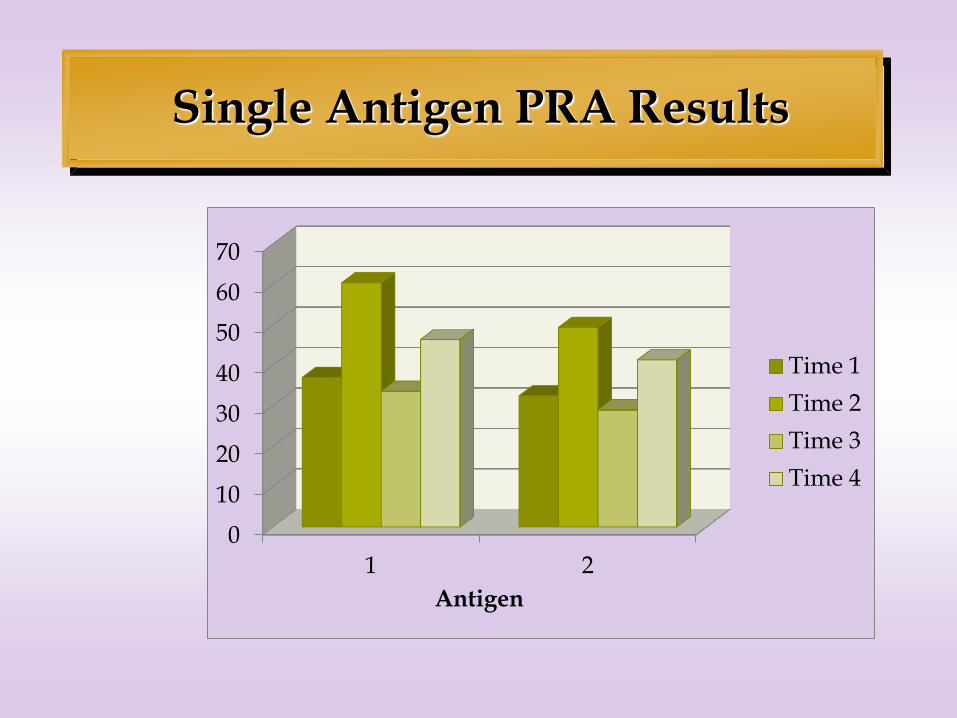
Single Antigen PRA Results
0
10
20
30
40
50
60
70
1 2
Antigen
Time 1
Time 2
Time 3
Time 4
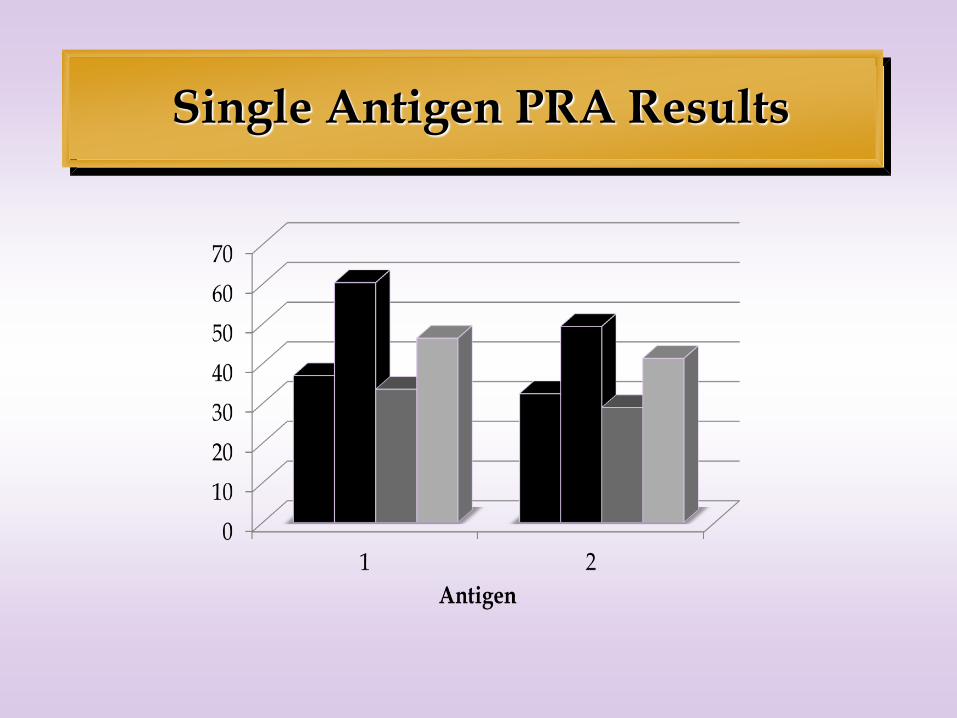
Single Antigen PRA Results

Assay Classification
Class Result Standardization
Method
References, Calibrators,
Controls
Qualitative Positive or Negative Single or dual 1 reference sample, positive and negative controls
Semi-quantitative Arbitrary units Single or dual Negative and bi-level positive controls; References unique for test system made from pooled patient sera
Quantitative Units related to recognized reference preparation
Multipoint standard curve
Tri-level controls; Reference calibrated towards a qualified reference preparation

SABs are not quantitative – why?
• Quantitative assay = result in units/volume
• Don’t have the necessary components
• Not standardized – Challenging from biologic and technical perspectives
• So says regulatory authorities – (intended use)
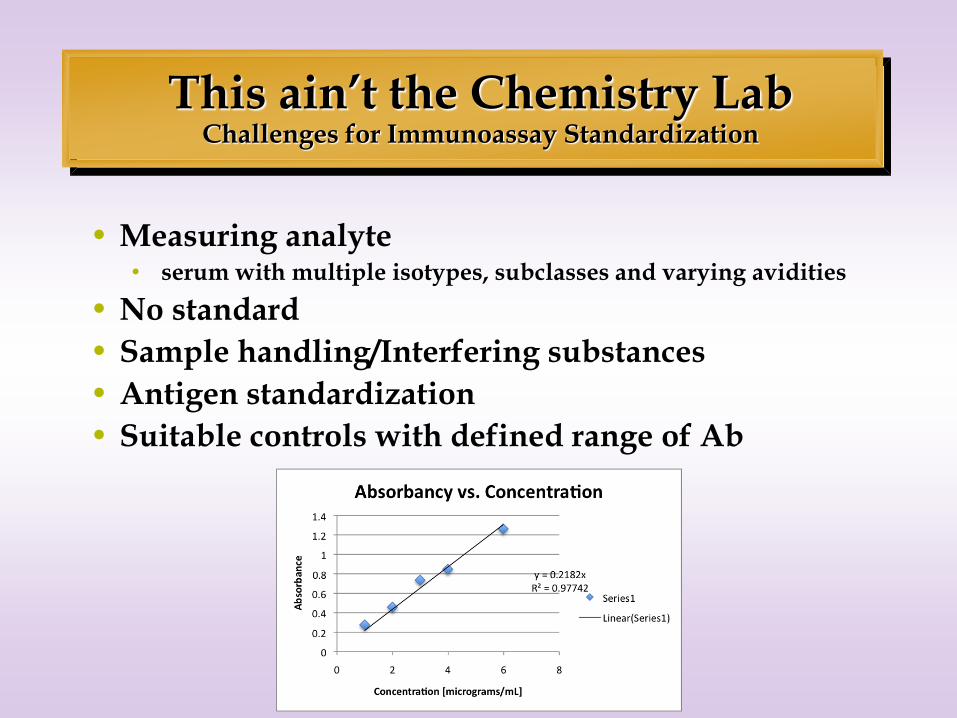
This ain’t the Chemistry Lab Challenges for Immunoassay Standardization
• Measuring analyte • serum with multiple isotypes, subclasses and varying avidities
• No standard
• Sample handling/Interfering substances
• Antigen standardization
• Suitable controls with defined range of Ab
Factors affecting all assays
•Affinity vs Avidity
•Polyclonal vs monoclonal
•Inhibitors
•Accuracy vs Precision
•Birthday cake!!
Yeah, you still gotta worry about all that biology, chemistry and physics stuff.
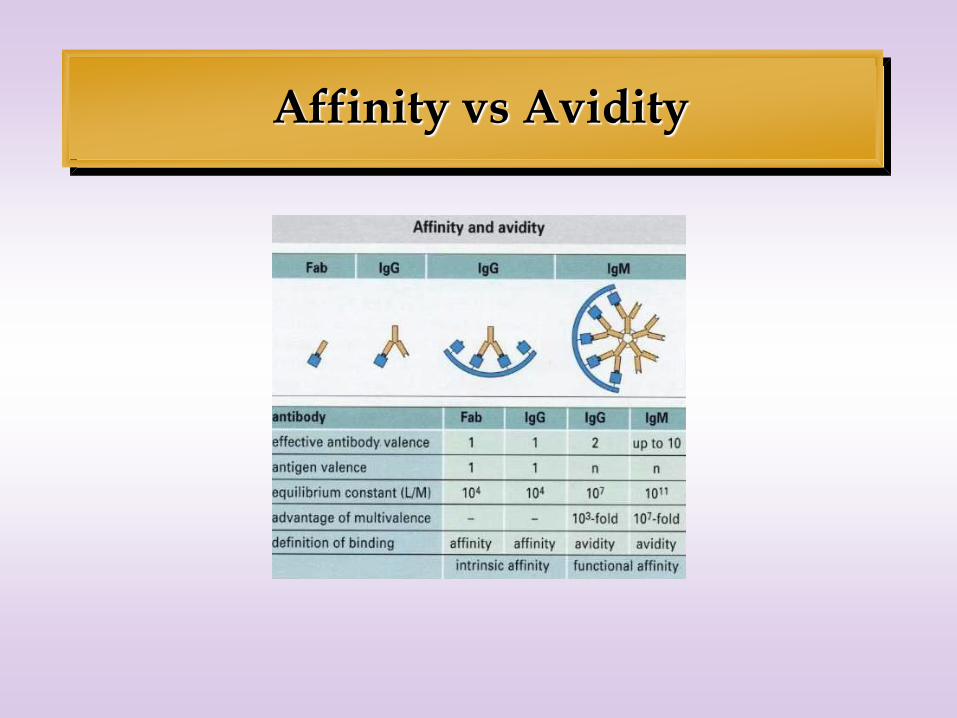
Affinity vs Avidity

Polyclonal vs Monoclonal
Roitt IM, Brostoff JB, Male DK. Immunology – Fifth Edition.
Mosby Internation Ltd. 1998.
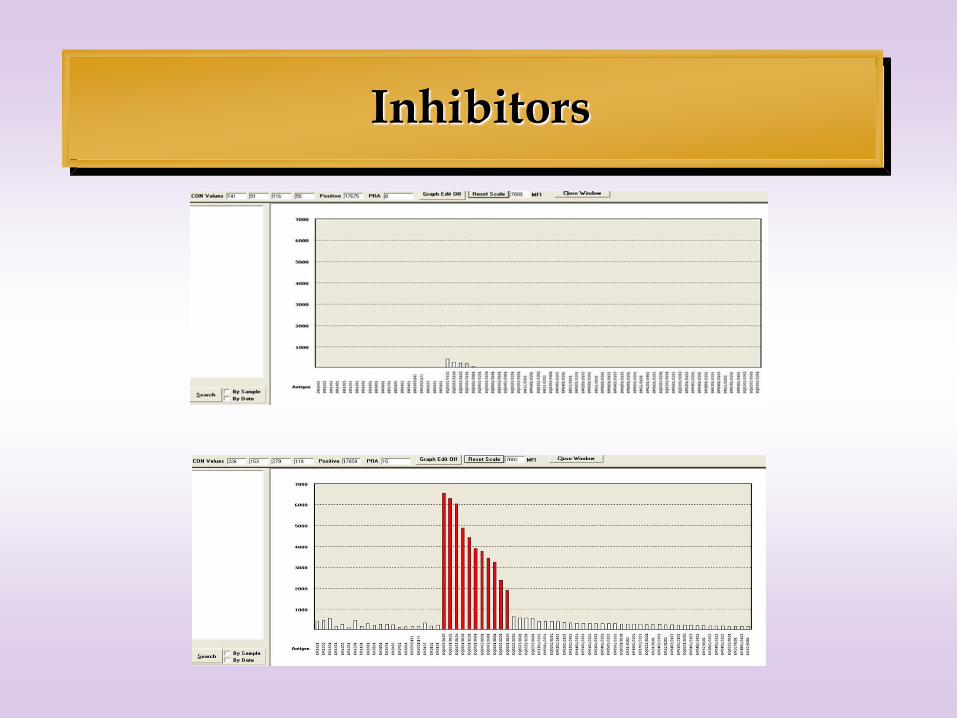
Inhibitors
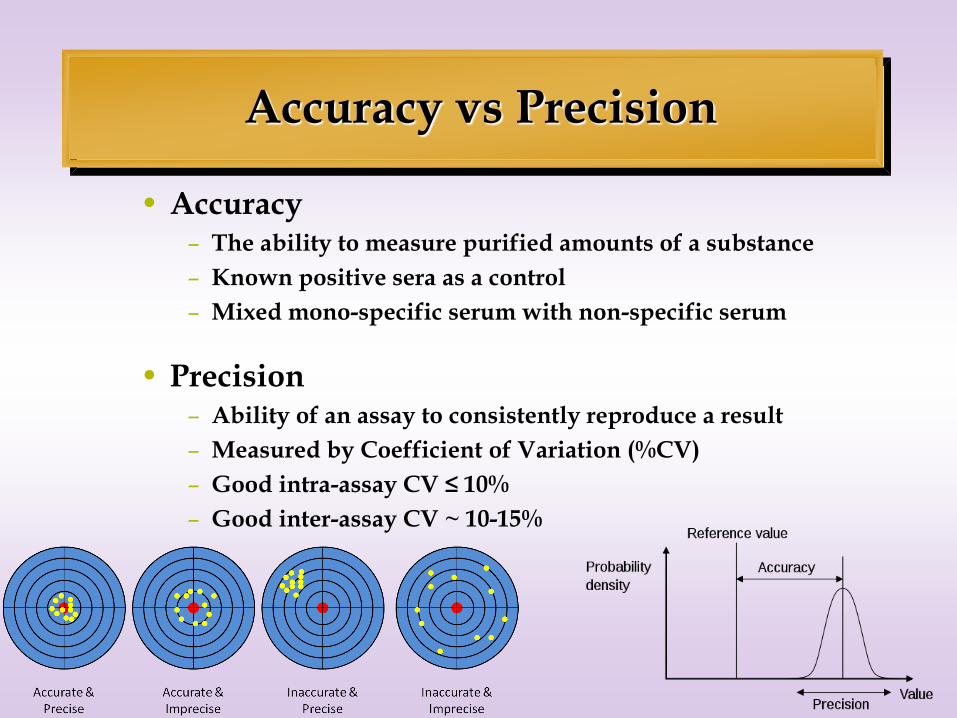
Accuracy vs Precision
• Accuracy – The ability to measure purified amounts of a substance
– Known positive sera as a control
– Mixed mono-specific serum with non-specific serum
• Precision – Ability of an assay to consistently reproduce a result
– Measured by Coefficient of Variation (%CV)
– Good intra-assay CV ≤ 10%
– Good inter-assay CV ~ 10-15%

Intra-assay %CV

Inter-assay %CV

The Real World
• SOPs are routinely deviated
– Lunch
– Birthday cake!
• Ambient conditions change
• Lasers fade
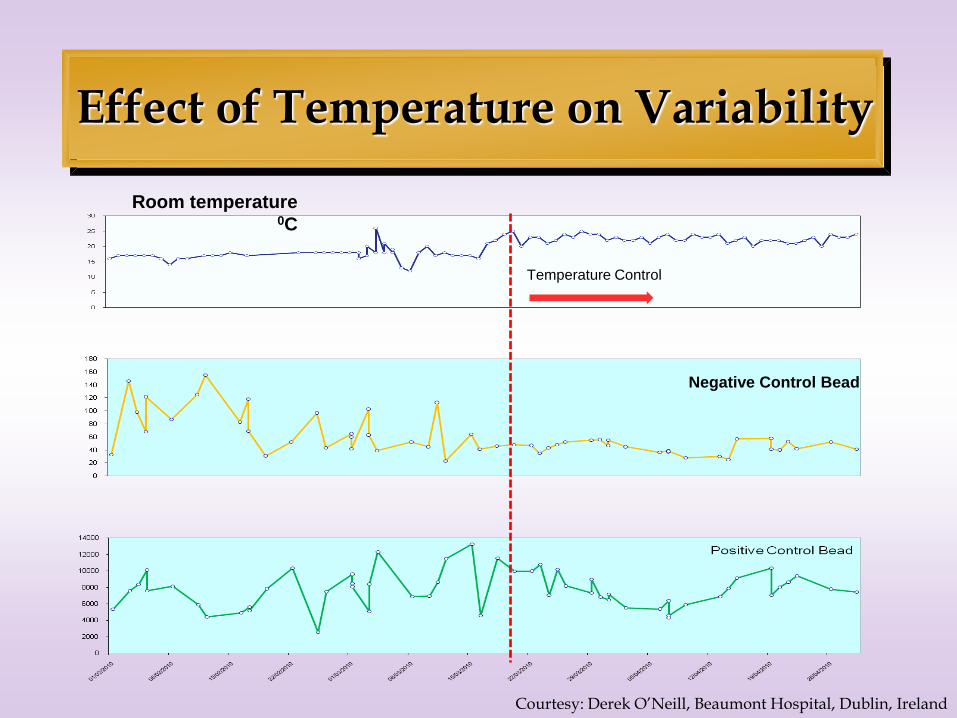
Effect of Temperature on Variability
Room temperature 0C
Temperature Control
Negative Control Bead
Courtesy: Derek O’Neill, Beaumont Hospital, Dublin, Ireland

A*0201 (donor Specific)
B*3701 B*1503
Temp 0C
Rxn
Score
MFI Rxn
Score
MFI Rxn
Score
MFI
Day of
transplant
serum
cold 4 707 2 186 6 2077
Day 7 post-
transplant
serum Run 1
cold 4 1162 6 2077 6 3000
Day 7 post-
transplant
serum Run 2
warm 1 21 2 159 4 1032
Patient serum variability: Post-transplant monitoring
Courtesy: Derek O’Neill, Beaumont Hospital, Dublin, Ireland

Luminex Summary
• Luminex assays should be carried out under controlled conditions
• Luminex results should be interpreted by experienced personnel
– take measurement error into account.
• SAB assays are at best semi-quantitative.
• Resist the siren call of MFI

Other PRA Testing Considerations
• Polyclonal vs. monoclonal
• CYNAP
• Monospecific vs. polyspecific
• Cross Reactive Groups (CREGS)

Antibody Specificity
•Monospecific – serum that has specificity for a single HLA antigen
•Polyspecific – serum that reacts with more than one distinct HLA antigen

Cross-reactive epitope groups (CREGs)
• Multiply reactive sera can result from:
– multiple “private” specificity antibodies
» antibodies specific for one specific determinant
– “true crossreactive” antibodies
» one antibody that bind to structurally similar private epitopes
– antibodies to “public” epitopes
» one antibody that binds to a unique epitope shared among several different HLA antigens (Bw4 or Bw6)

CREG Epitope Locations

B7 CREG appears safe
30-86-48
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
22000
24000
CO
N1
CO
N2
CO
N3
CO
N4
A*0
101
A*0
201
A*0
203
A*0
206
A*0
301
A*1
101
A*1
102
A*2
302
A*2
402
A*2
403
A*2
501
A*2
601
A*2
902
A*3
001
A*3
101
A*3
201
A*3
301
A*3
303
A*3
402
A*3
601
A*4
301
A*6
601
A*6
602
A*6
801
A*6
802
A*6
901
A*7
401
A*7
405
A*8
001
B*0
702
B*0
703
B*0
801
B*1
302
B*1
401(B
64)
B*1
402(B
65)
B*1
501(B
62)
B*1
502(B
75)
B*1
503(B
72)
B*1
512(B
76)
B*1
513(B
77)
B*1
516(B
63)
B*1
518(B
71)
B*1
801
B*2
703
B*2
705
B*2
708
B*3
501
B*3
701
B*3
801
B*3
901
B*4
001(B
60)
B*4
002(B
61)
B*4
101
B*4
201
B*4
402
B*4
501
B*4
601
B*4
701
B*4
801
B*4
901
B*5
001
B*5
101
B*5
201
B*5
301
B*5
401
B*5
501
B*5
601
B*5
701
B*5
802
B*7
301
B*7
801
B*8
101
B*8
202
Cw
*0102
Cw
*0210
Cw
*0303
Cw
*0304
Cw
*0401
Cw
*0403
Cw
*0501
Cw
*0602
Cw
*0701
Cw
*0702
Cw
*0704
Cw
*0801
Cw
*0802
Cw
*1202
Cw
*1402
Cw
*1502
Cw
*1601
Cw
*1701
Cw
*1801
Pro
be 7
7
Raw
MF
I-B
G
Pt. PRA consistently >90% (multispecific)
Pt. HLA-A11, -; B56, 65 (? sensitization)

B Ag specificities narrowed
45-30-96
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
22000
24000
CO
N1
CO
N2
CO
N3
CO
N4
A*0
101
A*0
201
A*0
203
A*0
206
A*0
301
A*1
101
A*1
102
A*2
302
A*2
402
A*2
403
A*2
501
A*2
601
A*2
902
A*3
001
A*3
101
A*3
201
A*3
301
A*3
303
A*3
402
A*3
601
A*4
301
A*6
601
A*6
602
A*6
801
A*6
802
A*6
901
A*7
401
A*7
405
A*8
001
B*0
702
B*0
703
B*0
801
B*1
302
B*1
401(B
64)
B*1
402(B
65)
B*1
501(B
62)
B*1
502(B
75)
B*1
503(B
72)
B*1
512(B
76)
B*1
513(B
77)
B*1
516(B
63)
B*1
518(B
71)
B*1
801
B*2
703
B*2
705
B*2
708
B*3
501
B*3
701
B*3
801
B*3
901
B*4
001(B
60)
B*4
002(B
61)
B*4
101
B*4
201
B*4
402
B*4
501
B*4
601
B*4
701
B*4
801
B*4
901
B*5
001
B*5
101
B*5
201
B*5
301
B*5
401
B*5
501
B*5
601
B*5
701
B*5
802
B*7
301
B*7
801
B*8
101
B*8
202
Cw
*0102
Cw
*0210
Cw
*0303
Cw
*0304
Cw
*0401
Cw
*0403
Cw
*0501
Cw
*0602
Cw
*0701
Cw
*0702
Cw
*0704
Cw
*0801
Cw
*0802
Cw
*1202
Cw
*1402
Cw
*1502
Cw
*1601
Cw
*1701
Cw
*1801
Pro
be 7
7
Raw
MF
I-B
G
Pt tx with B44 mismatch
6/2005 66% (A68, B44)
4/2006 100% (B44 strongest)
B specificities B44, 45, 76, 82

Class II – DQ Abs pop out
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
22000
CO
N1
CO
N2
CO
N3
DP
B1*0
101/D
PA
*0103
DP
B1*0
101/D
PA
*0201
DP
B1*0
101/D
PA
*0202
DP
B1*0
101/D
PA
*0301
DP
B1*0
201/D
PA
*0103
DP
B1*0
301/D
PA
*0103
DP
B1*0
301/D
PA
*0201
DP
B1*0
401/D
PA
*0103
DP
B1*0
401/D
PA
*0201
DP
B1*0
401/D
PA
*0202
DP
B1*0
401/D
PA
*0301
DP
B1*0
402/D
PA
*0103
DP
B1*0
402/D
PA
*0201
DP
B1*0
402/D
PA
*0301
DP
B1*0
501/D
PA
*0103
DP
B1*0
501/D
PA
*0201
DP
B1*0
501/D
PA
*0202
DP
B1*0
501/D
PA
*0301
DP
B1*1
301/D
PA
*0103
DP
B1*1
301/D
PA
*0201
DP
B1*1
401/D
PA
*0103
DP
B1*1
401/D
PA
*0201
DP
B1*1
701/D
PA
*0201
DP
B1*1
801/D
PA
*0103
DP
B1*1
801/D
PA
*0201
DP
B1*1
901/D
PA
*0103
DP
B1*1
901/D
PA
*0201
DP
B1*1
901/D
PA
*0301
DP
B1*2
801/D
PA
*0103
DP
B1*2
801/D
PA
*0201
DP
B1*2
801/D
PA
*0202
DQ
B1*0
202/D
QA
*0302
DQ
B1*0
202/D
QA
*0201
DQ
B1*0
402/D
QA
*0302
DQ
B1*0
402/D
QA
*0401
DQ
B1*0
401/D
QA
*0401
DQ
B1*0
301/D
QA
*0302
DQ
B1*0
301/D
QA
*0501
DQ
B1*0
302/D
QA
*0302
DQ
B1*0
302/D
QA
*0201
DQ
B1*0
303/D
QA
*0302
DQ
B1*0
303/D
QA
*0401
DQ
B1*0
501/D
QA
*0104
DQ
B1*0
601/D
QA
*0104
DR
B1*0
101
DR
B1*0
103
DR
B1*0
401
DR
B1*0
701
DR
B1*0
801
DR
B1*0
901
DR
B1*1
001
DR
B1*1
101
DR
B1*1
201
DR
B1*1
301
DR
B1*1
401
DR
B1*1
501
DR
B1*1
601
DR
B1*0
301 (
17)
DR
B1*0
303 (
18)
DR
B3*0
101 (
52)
DR
B3*0
202 (
52)
DR
B4*0
101 (
53)
DR
B5*0
101 (
51)
Pt. always called DR 52 (previous MM)
DQ specificity confounded by DR 52 and 53

CREG Epitope Locations

HLA-A Cross Reactivities
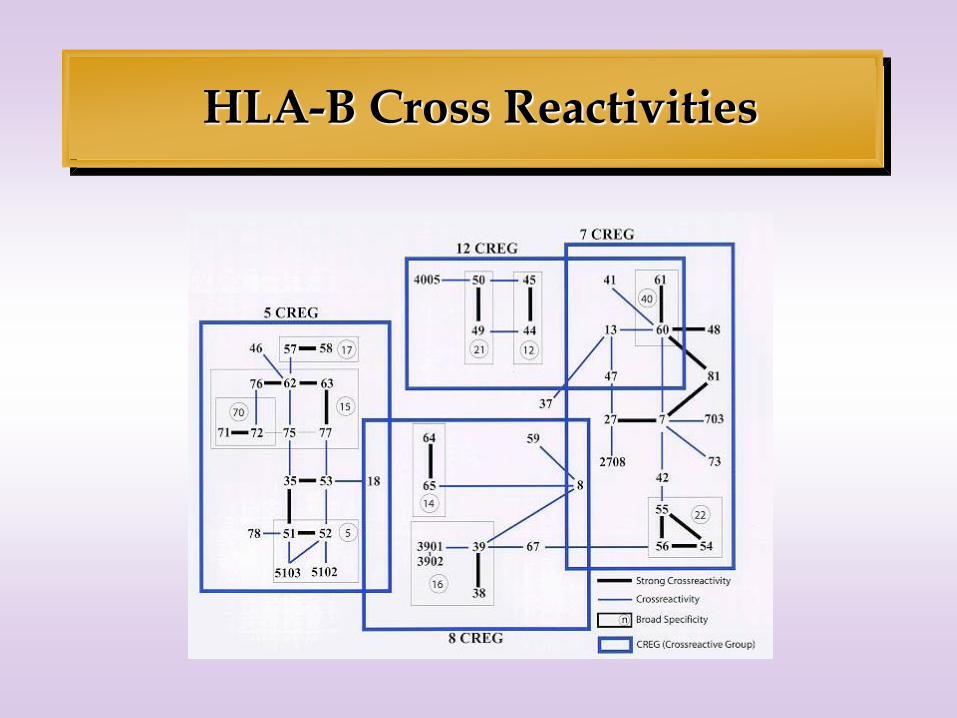
HLA-B Cross Reactivities
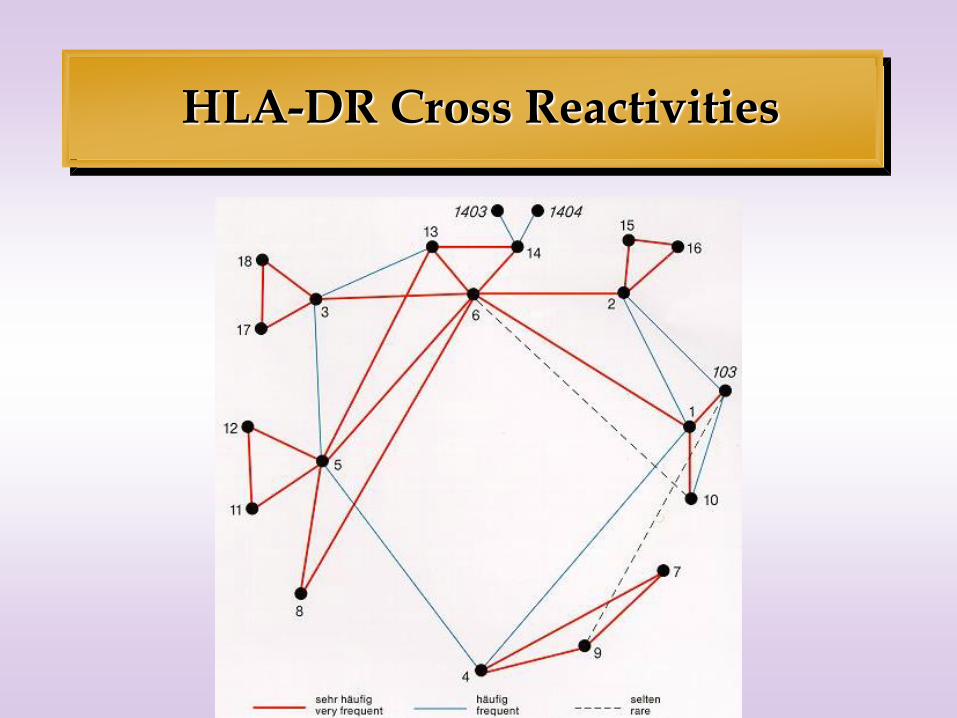
HLA-DR Cross Reactivities

TABLE 1. Overview of common molecular targets for non-HLA antibody responses, allograft types with confirmed injury phenotypes and corresponding time frames, as well as experimental evidence for pathogenicity of non-HLA antibodies with corresponding references Antibody target Human allograft type Time-frame Experimental evidence MICA Kidney (28–31, 35–39), heart (33), Hyperacute, acute, chronic — pancreas (31) Vimentin Heart (52) Chronic Mouse (57), non-human primate (55, 56) AT1R Kidney (46) Acute Rat renal allograft (46) ICAM-1 Heart (58) ? — HLA, human leukocyte antigens; AT1R, angiotensin type 1 receptor; ICAM-1, intercellular adhesion molecule-1.
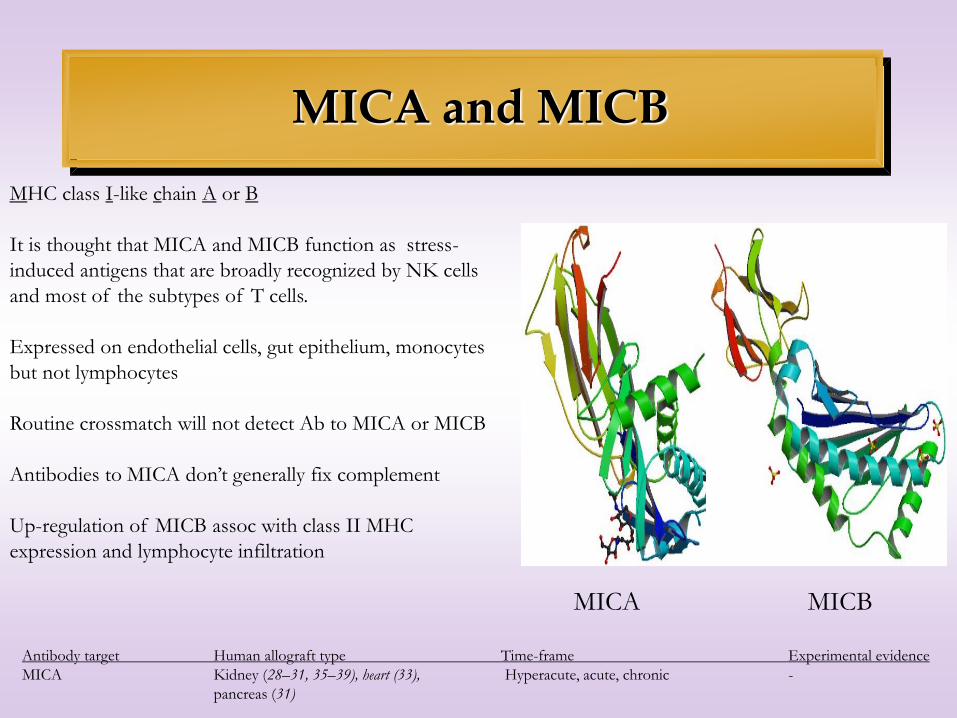
MICA and MICB
MICA
MHC class I-like chain A or B
It is thought that MICA and MICB function as stress-
induced antigens that are broadly recognized by NK cells
and most of the subtypes of T cells.
Expressed on endothelial cells, gut epithelium, monocytes
but not lymphocytes
Routine crossmatch will not detect Ab to MICA or MICB
Antibodies to MICA don’t generally fix complement
Up-regulation of MICB assoc with class II MHC
expression and lymphocyte infiltration
MICB
Antibody target Human allograft type Time-frame Experimental evidence
MICA Kidney (28–31, 35–39), heart (33), Hyperacute, acute, chronic -
pancreas (31)

Vimentin
Vimentin is a member of the intermediate filament family,
and is part of the cytoskeletal network.
Non-polymorphic protein found in abundance in
endothelium and smooth muscle cells.
antibodies to vimentin are considered “auto-reactive”
In a monkey model, anti-vimentin antibodies are associated
with chronic cardiac rejection but not kidney rejection.
????
Antibody target Human allograft type Time-frame Experimental evidence
Vimentin Heart (52) Chronic Mouse (57), non-human primate (55,
56)

Angiotensin type 1 Receptor (AT1R)
• AT1 receptor has vasopressor effects and regulates aldosterone secretion. It is an important effector controlling blood pressure and volume in the cardiovascular system.
• Antibodies to AT1R have been associated with pre-eclampsia and are implicated with severe vascular rejection.
• Article describes a patient who received a 6 Ag match kidney and then had a sudden onset of malignant hypertension that mimicked the pre-eclampsia she suffered >20 years before.
Angiotensin type II
Antibody target Human allograft type Time-frame Experimental evidence
AT1R Kidney (46) Acute Rat renal allograft (46)
A receptor like AT1R

ICAM and anti-GBM
• Antibodies to ICAM found in cardiac transplant patients.
• Antibodies to agrin and perlecan are associated with duplication of the GBM - a hallmark of transplant glomerulopathy.

Mechanisms of Injury
• Complement-mediated injury
• Antibody-dependent Cellular Cytotoxicity – for non-C’ fixing Abs (like those against MICA/B)
• May contribute to structural changes
• Signalling?
Perspective
• With exceptions of MICA and AT1R, routine testing for these antibodies are not currently available.
• Question as to whether non-HLA antibody related pathologies represent “true” rejections of the transplanted organ or organ-specific autoimmune phenomena.
• Non-HLA Abs may find application as biomarkers of immune response and herald the need for more suitable immunosuppression.

All Content © 2015 Immucor, Inc.
Questions?
• You are all muted
• Type in questions

All Content © 2015 Immucor, Inc.
We like you!
Like us on social media!

All Content © 2015 Immucor, Inc.
Questions?
• You are all muted
• Type in questions

All Content © 2015 Immucor, Inc.
Continuing Education
• ABHI, PACE, Florida and California DHS
• 1.0 Contact Hours
• Each attendee must register to receive CE at:
https://www.surveymonkey.com/r/HLAImmucor
• Registration deadline is March 2, 2018
• Certificates will be sent via email only to those
who have registered by March 16, 2018
All Content © 2015 Immucor, Inc.
22 February Donor Selection of Solid Organ
Transplant: Is Virtual Xmatch better
than real?
28 February Proficiency, Competency, and QC: A
practical approach to CLIA
requirements and AABB, CAP, and
Joint Commission Expectations
22 March
Clinical Significance of HLA Antibodies
in Solid Organ Transplantations
Future Webinars
Link to register:
https://immucor.webinato.com/register


















