Achieving the Triple Aim: Better Health and Better Care at Lower Costs

1
Contemporary Triple P
Karen M. T. Turner, PhDDeputy Director (Programs and Innovation)Parenting and Family Support CentreThe University of Queensland
Jenna McWilliam, MOrgPsychHead of Organisational Development
Triple P International Pty Ltd
Disclosure statement
• The Triple P - Positive Parenting Program is owned by The University of Queensland which licenses Triple P International Pty Ltd to disseminate the program worldwide
• Royalties are distributed to the Faculty of Health and Behavioural Sciences, School of Psychology and contributory authors
• Associate Professor Turner is a foundational co-author of Triple P resources
• Jenna McWilliam is an employee of Triple P International Pty Ltd

2
Why Triple P?
3
Our vision
All parents have knowledge, skills and confidence to raise their children a safe, loving, low conflict world
Positive parenting becomes socially
normative
Adverse Childhood Experiences are
minimised
Population‐based approaches to
parenting support become a policy
priority
Who benefits?

3
Good parenting is the clean water of mentalhealth and wellbeing
What a great place to raise children might look like?
4
A great place to raise a family
• Values, supports and celebrates the importance of parenting
• Recognises that the wellbeing of children and families is a shared community responsibility
• Respects a parent’s role in determining the values, skills and behaviours they want to promote in their children and the parenting practices they use to get there
• Promotes the social and cultural connectedness of families
• Supports family self-regulation and autonomy in raising children
• Makes high quality, culturally informed, evidence-based parenting support programs accessible for all families
• Ensures that parents are empowered and skilled to participate in planning and decision making that impacts on children and families
7
Children’s relationships really matter
• Poorer self‐regulation• Risk of SEB problems• Risk of antisocial behavior, substance abuse, school dropout
Poor life course
outcomes
Dysfunctional relationships cause
toxic stress
Positive, nurturing relationships lay the
foundations (Biglan, 2015)
• Secure bonding• Better self‐regulation• Fewer SEB problems• Academic success
Good life course
outcomes

5
A person with 4 or more is…
Adverse childhood experiences (ACEs)
Life course outcomes• 12.2 times as likely to attempt suicide
• 10.3 times as likely to use injection drugs
• 7.4 times as likely to be an alcoholic
• 2.4 times as likely to have a stroke
• 2.2 times as likely to have ischemic heart disease
• 1.9 times as likely to have cancer
• 1.6 times as likely to have diabetes
Types of ACEsAbuse• Physical• Emotional • Sexual
Neglect• Physical• Emotional
Household dysfunction• Mental Illness• Incarcerated relative• Mother treated violently• Substance abuse• Divorce
Broadening our conceptions of competent parenting
10
Core principles of positive parenting
Safe and engaging
environment
Positive learning
environment
Consistent assertive discipline
Reasonable expectations
Taking care of oneself

6
Gender/age of parent
Education /literacy
Employment status
Poverty
Parental mental health
Connectedness to community
Discrimination
Type of Neighbourhood
Prior help seeking
Family of origin experiences
Culturally normative parenting practices
Immigration status
Government policies and
priorities
AcculturationEnablers and barriers
Social influence
Program itself
Parental concern about child behavior
MotivationParticipation
Social infrastructure
Parenting services
Refugee status
Laws
Level of violence
Ecological context matters
Cognitions or affect
Broadening our conceptions of competent parenting
12
Other aspects of parenting
Supporting children’s
relationships with peers
Balancing work and family
responsibilities
Effective communication with teachers Healthy
relationships with extended
family
Being part of the community

7
Why Triple P as a system?
13
Make positive parenting a public health priority

8
A blueprint for a achieving population level change
1. Clear documentation of need
2. An explicit theoretical framework
3. Build a strong evidence base
4. Involve consumers to shape program
5. Use cost‐effective interventions
6. Use diverse access points
7. Use intensive programs sparingly
8. Strengthen social structures to support parenting
9. Employ sustainable system of dissemination
10. Population level outcome data relevant to policy
Adopting a population approach has implications
• Started to focus on different outcomes
• Developed a “system” that blends targeted and universal interventions
• Proportionate Universalism
• Focused on a multidisciplinary, multi-agency workforce
• Needed to be comprehensive (covering multiple stages of development and complexity of problems)
• Needed to be inclusive of all families
• Needed to be culturally informed and relevant
16

9
Not a ‘one-size fits all’ approach
Level 5
Level 4
Level 3
Level 2
Level 1
Intensive family intervention………................
Broad focused parenting skills training………...
Narrow focus parenting skills training………….
Brief parenting advice……………………………
Media and communication strategy…………….
Breadth of reachIntensity of intervention
What does the Triple P System look like now?
18
10
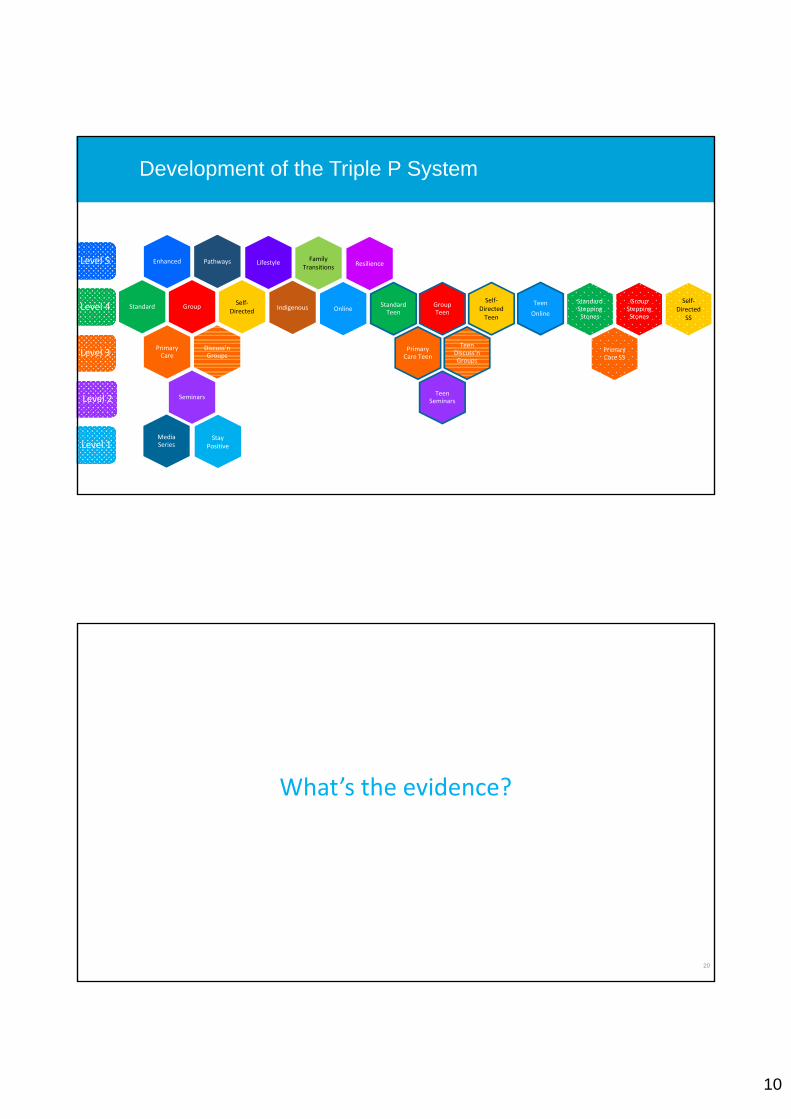
Development of the Triple P System
Standard
Enhanced
GroupSelf‐
Directed
Discuss’nGroups
Primary Care
Seminars
Media Series
Level 5
Level 4
Level 3
Level 2
Level 1
Standard Teen
Group Teen
Self‐Directed Teen
Teen Discuss’nGroups
Primary Care Teen
Teen Seminars
Teen
OnlineIndigenous Online
Pathways
Standard Stepping Stones
Group Stepping Stones
Self‐Directed
SS
Primary Care SS
LifestyleFamily
TransitionsResilience
Stay Positive
What’s the evidence?
20

11
Questions about effectiveness are complex
What intervention… delivered by whom…in what context… via which delivery modality is effective with what kind of parent, child or youth problems… at what age… in what family,
cultural and community context?...and how does the intervention effect
come about?Adapted from Gordon Paul (1969). Behavior therapy appraisal and status. McGraw‐Hill
0
200
400
600
800
1000
1200
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
2014
2015
2016
N
1137 authors
499 conceptual papers
353 institutions
274 evaluation studies, including 137 RCTs
30 countries
773 total papers
Building an evidence base takes time
First population trial published
International dissemination begins
Growth of international projects
Program development begins
Program gets a name

12
Types of evidence
• Single-case experiments(Sanders & Glynn, 1981)
• RCTs(Sanders et al., 2000)
• Quasi-experimental studies(Zubrick et al,1995; Doyle et al, 2016)
• Place-based RCTs(Prinz et al, 2009, 2016)
• Evaluations in LMIC(Mejia et al, 2014)
• Meta analyses(Nowak & Heinrichs, 2008; Sanders et al., 2014)
• Service-based evaluations(Santa Cruz, 2016)
• Consumer preference studies(Metzler et al., 2013)
• Training, implementation and supervision studies(Hodge et al., 2016)
• Evaluations in diverse cultures(Sumargi et al., 2015)
• Qualitative studies(Frank et al., 2015)
23
What about long-term effects?
• Sanders et al. (2014) meta-analysis: 70 studies with follow up (2–36 months)
• Hahlweg et al. (2015) conducted 10 year follow up (90% retention) of universally offered Group Triple P
- Significant reductions of child behavioural and emotional problems at 10 year follow up for internalising problems, externalising problems, parenting practices
• Smith (2015) conducted 15 year follow up of linked administrative data in WA
- Higher levels of literacy and numeracy, school attendance (grade 11), fewer emergency room visits
24

13
Competency-based training across diverse cultures
25
Training delivered in 27 countries
From small beginnings…
• 7,170 professional training courses run worldwide
• 108,056 training places
• 76,496 unique practitioners
• Reaching millions of children
26

14
What’s new?
27
Working towards population level change
28

15
Intensive early intervention with vulnerable families
• €100 toys annually and book packs
• Facilitated access to enhanced preschool
• Public health workshops
• Facilitated access to local services
• Access to social events
High treatment = PLUS
• Baby massage (year 1)
• Triple P (PC, Discussion Groups, Group - years 2-3)
• Mentoring (until 4 or 5 years)
29
Effects on cognitive functioning
British Ability Scales (Elliot et al, 1997)
30
16
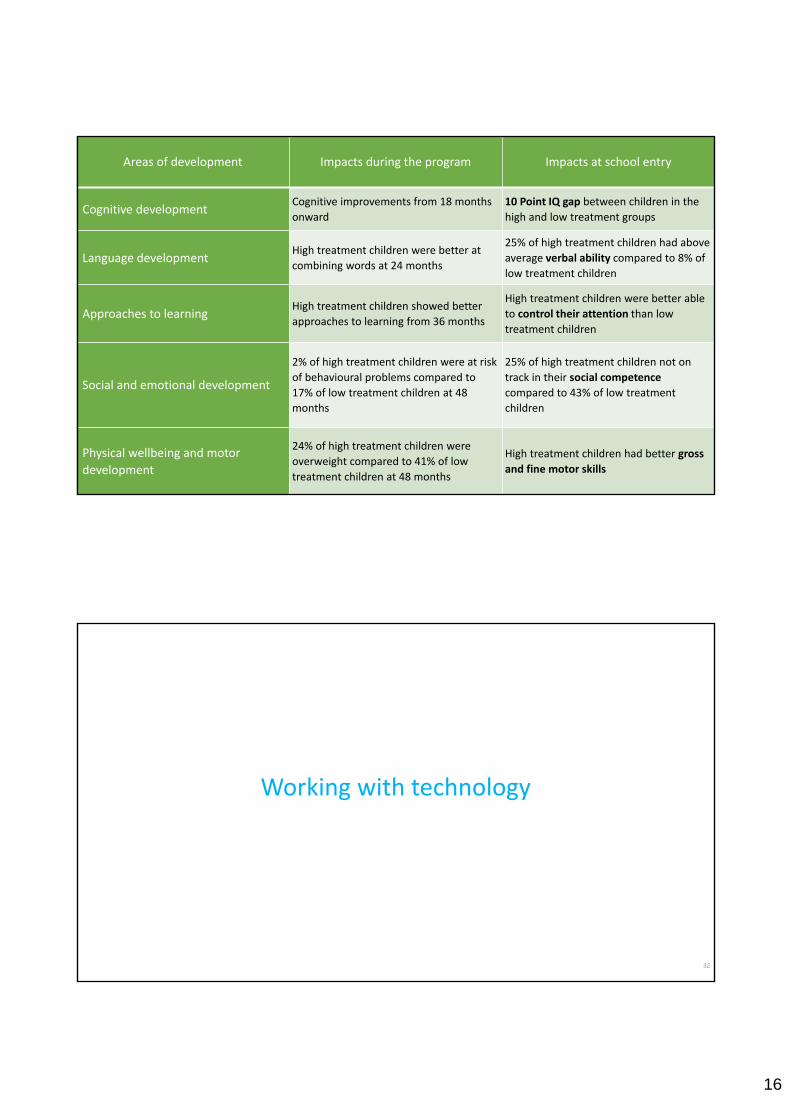
Areas of development Impacts during the program Impacts at school entry
Cognitive developmentCognitive improvements from 18 months
onward
10 Point IQ gap between children in the
high and low treatment groups
Language developmentHigh treatment children were better at
combining words at 24 months
25% of high treatment children had above
average verbal ability compared to 8% of
low treatment children
Approaches to learningHigh treatment children showed better
approaches to learning from 36 months
High treatment children were better able
to control their attention than low
treatment children
Social and emotional development
2% of high treatment children were at risk
of behavioural problems compared to
17% of low treatment children at 48
months
25% of high treatment children not on
track in their social competence
compared to 43% of low treatment
children
Physical wellbeing and motor
development
24% of high treatment children were
overweight compared to 41% of low
treatment children at 48 months
High treatment children had better gross
and fine motor skills
Working with technology
32

17
• Mentor introduces and summarises modules
• Video clips of families in action• Interactive exercises• Individual goal setting, feedback and weekly
check in• Downloadable worksheets • Personalised and printable parent workbook
(email or Word file; full text and bullet point versions)
• Downloadable podcasts• Review and reminder strategies (text
messages, emails)• Self‐regulatory focus with decreasing
support
Triple P Online:
Providing support where parents are looking for it
Does adding phone support improve outcomes?
Up to 8 weekly telephone consultations with a Triple P practitioner
• To discuss parenting-related questions/issues
• To promote parent’s self-regulatory skills
• To encourage program adherence
Day & Sanders (2016)

18
Primary child outcomes
Pre-FU
WL vs Active* (d = 0.3)
TPOL vs TPOLE** (d = 0.34)
100
110
120
130
140
150
160
TPOL TPOLE WLGroup
EC
BI I
nte
nsi
ty s
core
Time
Pre
Post
FU
Phone support aids module completion
0
10
20
30
40
50
60
70
80
90
100
Module1
Module2
Module3
Module4
Module5
Module6
Module7
Module8
TPOL with phone support TPOL without phone support
With phone support
Without phone support
Minimum dose
(70.2 % vs 40.8%)

19
Implications
TPOL:
• works (7 RCT’s) for children with early onset conduct problems and ADHD
• is very cost-effective
• effects enhanced by professional support for some parents
• can be used in stepped care approach
• engagement process very important
• useful to screen for pre-existing levels of adjustment difficulties (e.g. depression) to decide if support is desirable
37
Working in LMICs
38

20
Children’s exposure to violence is a major public health issue
39
Children’s exposure to violence is a major public health issue
150 million (14%) of girls and 73 million (7%) of boys under age 18 experience forced sexual intercourse and other forms of sexual violence involving touch
Source: UN Secretary General's Study on Violence Against Children (2013)
The role of parenting programs globally
• WHO Global Violence Prevention Initiative and UNODC calls for development, adaptation, implementation and evaluation of EBPs for LMIC
• Two meta analyses highlight the lack of quality research
- Mejia, A., Calam, R., & Sanders, M.R. (2012). A review of parenting programs in developing countries: Opportunities and challenges for preventing emotional and behavioural difficulties in children. Clinical Child and Family Psychology Review.
- Knerr, W., Gardner, F., Cluver, L (2013). Reducing harsh and abusive parenting and increasing positive parenting in low- and middle-income countries: a systematic review. Prevention Science.
• Programs developed in one country can be successfully used in other
- Gardner, F., Knerr, W., & Montgomery, P. (2015). Transporting evidence-based parenting programs for child problem behaviour (age 3-10) between countries: Systematic review and meta-analysis. Journal of Clinical Child and Adolescent Psychology.
40

21
What’s next?
41
We’ve only just begun…
• World population: 7.3 billion
• World population of children aged 0-14: 1.9 billion
• 145 million children are born each year (399,926/day or 278/minute)
• World population from less developed countries: 6 billion
• 28/196 (12.76%) countries have contributed to the published evidence base on Triple P
42
Population Reference Bureau. (August, 2015). 2015 World Population Data Sheet. Retrieved from www.prb.org
United Nations, Department of Economic and Social Affairs, Population Division. (2015). World Population Prospects: The 2015 Revision, Key Findings and Advance Tables. Working Paper No. ESA/P/WP.241

22
Good parenting and problems of global significance
Parenting support and major environmental problems
44
Depletion of fish stock due to damage to coastal reefs
Pollution as a result of burning biomass to meet basic energy
needs
Working with climate scientists/marine biologists on family‐based cultural change
Working with engineers interested in poverty reduction
and sustainable energy
Animal welfare Working with veterinary scientists

23
A final word
We have learnt a lot about how to build the capacity of parents to raise well adjusted
children
Activation of community‐wide processes to
support positive parenting
Population‐based approaches to
parenting support should become a policy priority
Population level change in parenting is an achievable goal
Triple P International

24
Challenges
• Innovations to address to major challenges:
- How to increase the reach of parenting support across a community
- How to implement evidence-based programs effectively
- Digital innovation
The challenge: reaching all families
• How can we increase parenting skills across a community?
• How can we achieve a meaningful, population level change in family resilience and functioning and children’s emotional and behavioural outcomes?

25
How are we addressing this challenge?
• Refining the Triple P public health approach
• Communications and engagement strategies
• Supporting community readiness and collaboration
• Supporting flexible delivery of existing programs
• Triple P Online
Example: Queensland Government Triple P initiative
• Universal parenting program led by the Department of Communities, Child Safety and Disability Services
• Aims to give parents practical skills and tools, and help build their confidence
• Aims to reach a large number of families
• Complements reforms in child protection
• Makes a range of Triple P services available to parents free of charge
26
Progress so far
• By the end of 2016, we had reached 50,280 parents through:
- 12,752 parents attending seminars
- 23,585 parents attending a range of light touch and more intensive programs
- 13,942 parents accessing Triple P Online
Stay Positive materials

27
Billboards and bus stop signs

28
Bus wrap
Communication with parents

29
The challenge: Effective implementation
“What shall be implemented, how will the task be carried out, and who shall do the work of implementation?”
• What refers to the effective intervention (the EBP)
• How is the process to establish what needs to be done (the set of purposeful implementation activities)
• Who refers to who will do the work to accomplish positive outcomes (implementation teams)

30
The Triple P Implementation Framework
The challenge: Digital innovation
• Harnessing the benefits of digital services
• For parents:
- Communications and engagement strategies
- Triple P Online
• For practitioners:
- Online presentation materials
- Automatic Scoring and Reporting Application

31
Summary
• Focus on increasing reach to make population level impact across communities
• Invest in strategies to support effective program implementation to increase reach, high quality delivery and sustainability
• Harness the benefits of digital services
Karen [email protected]
Jenna [email protected]
Triple P Internationalwww.triplep.net
Triple P Blogwww.triplepblog.net
Triple P Evidence Base www.pfsc.uq.edu.au/evidence