Contemporary Treatment of Dentofacial Deformity
691
Click here to load reader
-
Upload
gina-paola-vela-duarte -
Category
Documents
-
view
469 -
download
224
description
TRATAMIENTO DE PACIENTES CON ANOMALIAS DENTOFACIALES
Transcript of Contemporary Treatment of Dentofacial Deformity
-
62 PART I Ine Nature of Dcntofadal Deformity
A B
Fig. 2-38 A. FliTe forct transducers prior to intraoral placement. The larger 6 mm quartz crystal transducer is 6 mm high and separates the teeth by at leasllhat distana in use; the smaUcr piewek-clric
t ran~llcer requircs less than 2 mm separation. A transducer is mounted on the me~ioh\lccal cusp of thc lower molar of a p;Hient before recording occlusal force. UndercUlS and the occlusal surface of other teeth arc waxed out, and composite res in is used to fill any voids between the tr.lllsducl'r's surface and the tooth. B, The transducer is mounted in a silicone rubber carrier, which ensures that it will be in the proper place between the teeth when thc parielll bites down. C, The transducer in place' in the lIIouth, with vertical separation o f the ill ciso r~ being measured.
-
Chapter 2 T HE D EYFW" Mt:NT OF D ENTOFAa .... l D EFORM lIT. I NFJ.UJ':'IlCE.'i ANI) F-ll OLOGIC FACTORS
- -0
g -- ~ 3 -
50
40
30
20
a Swallow Chew Maximum biling force
the size of the tongue when the size of the jaw is reduced. Oc-casionally a failure of adaptation is seen, and in Ihose patients the longue posture may have been a contributing factor in the etiology.
Biting Force and Jaw MorphoLogy One characteristic of long face patients is that the posterio r teeth erupt farther Than normal. Conversely, in short face pa-tients, the teeth are in fraerupted. It seems obvious that bit-ing force, which opposes eruption, could be involved in its control. Is it possible that differences in muscle strength and therefore in biting force are involved in the etiology of long face and short face problems?
Biting force varies depending on what is being chewed, ","here along the den tal arch the force is measured (e.g., it is heavier on the molars than the incisors), and several other \"3riables that can be difficult to control experimemally.34 When biting force is studied, it usually is measured ,vith elec-troni
-
Chaplcr 2 T ill' D IOVhLOI'Mt:NT OF D ENTOFACIAl D EFORM ITY: ISFWF:NCFS " NO Enouxac FACIORS 65
Fig. 2-42 TIIC dassic atiCNOid facies, which consists of n~rrow facial widlh dimension~, protruding maxillary illciMlTS. and lips separated at reSt, has often Ixen attributed to mouln breathing. Becal1se it is perfectly po~ibl c to bn:athc th rough th~ nose when lhe lips are separaTed simply by creating an o ral seal po5teriorly wiTh the soft palale, the facial appearance is not diagnostic of the respiratory mode. On careful study, many of these patients arc found not to be ouligatory mouth breathers.
posture and the development of mandibul3 r prognathism (but not opell bite). These prima tes do not adapt to mouth breathing as readi ly as do humans or in exactly the same way, but the experiments do show the potential (or respiratory adaptations to produce dcntofacial deformity.
Total nasal obstruct ion, such as that produced in the ex-perimental animals, is extremely rare in humans, but case re-ports make it clear that whell t hi ~ does occur, the pattern of fa-dal growth is altered. In human juveniles who develop 10lal nasal obstruction, there is a severe downward and hackwa rd rotation of the mandible, and subsequent growth produces a long face deform ity (Fig. 2-41). Because total obstructioll ill humans is so rare, the im portant clinical question is whether partial nasal obstruction , of the type That occurs chronically in some children. also can produce a long facc dcformit}'.
The question is difficult to answer for two reasons. First, it is difficult 10 quantify tl lC extenT of mouth breathing. This is ex-pressed best as the nasaVoral ratio; that is, as the perceiliage of lotal airflow that passes through tIle nose vcrsus the mouth. "Ie. be certaill of the nasal/oral r(l lio, special instrumentation that measures nas.""\l and oral airflow simultaneously must be used. Second, it is vcry difficult to monitor how an individual is breathing oller considerable periods of timc, as for instance what the breathing pattern is during sleep. Ouservers often as-SW11e that when the lips are sepMated, the person is breathillg through the mOllth. In fact, it is perfectly possible to have 100% nasal breathing when the lips arc apart. The Ill"(;C"Sary seal to pre\"cll t airflow th rough the mOUTh is achieved by placing the tongue ~ga inst the roof of the mouth. A certain pcra:ntage of oral respiration, maintained fo r a certain percentage of the time,
should be the definition of significan t mouth breathing. De-spite years of effort, such a definition has not been produced.
It seems reasonable to assume that in dividuals who re-qui re surgical removal of llypen rophied a(lenoids would have a sign ificant degree of nasal obstruction. The term fi de/wid facies (Fig. 2-42) has appeared in the li terature for at least a century to describe an individual with narrow width dimen-sions, iJlcreased face height, protruding teeth, and lips that are sep~ra ted at rest. The car icature h;Js so me validi ty. In 1970, Linder-Aronson and Woodside~~ documented a ten-dency tow;J rd lengthening of anterior face height in child ren who were scheduled for tonsillectomy and adclloid(:aomy in Stockholm, and later showed that fa ce height in the children who lmd their adenoids removed tended to return toward lhe mean of an untreated control group. Thc differences in fa ce height and mandibular plane angle at all stages were statisti cally significant and undoubtedly real, but their magnil ude was not large.
Data for the extent of mouth hreathing in patients with a long face pattern severe enough to put them in the dcntofacial deformity category come from two types of studies, using indi-rect metllods to infer mollth breathing or direct measurements to quantify oraVnasal r.l.tios. The l15ual indin:ct method is to measure the resistance to nasal airflow, which can be calculated [rom the pressnrc drop across the nasal cavity at measured rates of ai rflow. If nasal resistance is high enough, nasal breathing is impossible and mouth breathing must be occurring. Turvey, Hal l, and W;"lrren39 showed that in a sample of 50 long face pa-tients who would have orthognathic surgery to correct it,l l had moderately elevated nas,1l resistance and 6 had very high
-
64 PART I The Nature of Ucnlofacial Deformity
12 40 60
" 55
10 35 50 9 3() 45 8 ~
40 ~ 7 25 35 -~ 6 20 3() ~ -
5 25 & 4 15 20
3 10 15 2 10 1 5 5 0 0 0 NC LC NA LA NC LC NA LA NC LC NA LA
Swallow Chew Maximum bit ing force
Occlusal Iorce (6 mm opening)
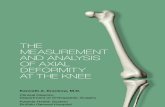
Fig. 2 40 Comparison of occlusal force al 6 111111 molar separa tion in child ren with normal face height (Nc' black cfossharch), long face children (LC, red cross!wldl ), nurmal ad uiLs (NA, b!(lck), and long face adults (LA, red). The implication is that the differences in OCdU Soll force in adults result from failure of the long face grollp 10 &1in strength during adolescence, not from the long face condit ion per $C. (From Proffit WR, Fields HW: OCdllS~1 forces in normal :l!ld long face children,) Dent Res 62:571574, \ 983.)
Fig. 2-41 Cephalometric superimposition showln); the effect of total nasal obstruction produced by a pharyngeal flap operation that sealed off the nose posterioriy. From age 12 (black 01/1/;".::) to age 16 years. 9 months (fe(1 (Jut/ine), the mandible rotated downward and backv.'3rd as the patient grew significa ntly. (Redrawn from McN"amara JA: Influence o f respiratory pattern on craniofacial growth. Angre OrtflDd 51 :269-300, 1981. )
-
PART I The Nature of Dentofacial Deformity
~~~ Normal (N " 16) l ong (N '" 32)
-
0-20 21-40 41 60 61-60 81-100
Nasal respiration (percent)
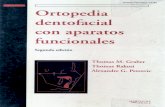
Fig . 2- 43 COlllparison of thc percentage of nasal respiration in long face versus normal face adolescents (all airflow accounted for USUlg spl'Cial instrumentation). Abolll one th ird of the long face group but none of the normal face group have less than 50% nasal respiration. However, most of those in the long fact: group, as in the normal fa~ group. are predominantly nasal breatbers. The data suggest that impaired nasal respiration may contribute to the development of the long face condition hUI that il is not the sole or even the major causC'. (From Fidds HW ct al: Relationship between vertical dentofacial morphology and respiration in adolcM:cnts,Am , Orriwd DemoJtu Orrhop 99:147-154, 1 IJ91.)
resistance, whereas the remaining two thi rds were normal. 11lC.'SC data were taken after growth "''as complete and therefore do not indicate the situation during gmwth. Furthermore, nasal resistance measures what the patient could do, not what he or she does. It is possible that some ind ividuals ill the study with normal nasal resistance nevertheless werc mouth breathers. However, the data do suggest that mouth breathing is not a nec-essary concomitant of the long face condition.
Using a nasal mask to measure na.~l air flow and a body plethysmograph to evaluate total airflow. Fields et al~o calcu-lated the nasal/oral ratios in a group of long face adolesccrlls (again, surgical candidates) and compared the resul ts with the ratios from an adolescent group with normal facial pro-portions. Almost one th ird of the long face group had 50% or less nasal respiration, whereas none of the normal group had so Iowa percentage; however, most of the long face group were predom inantly nasal breathers (Fig. 2-43).
'nlese data seem
-
Chapter 2 THE D EVELOPMEr-. OF D .'flOFAClAl DUOR,\IITY: I ...-FLUI:.N(.ES AN D ETIOlOGIC fACTORS
.mtl.t effect on the neuromuscular system, as in the m uscular _~a\:~-Jless syndromes, or a necessary neuromuscular ad apta-tion, as in obligatory mouth breathing, would produ(;c sim i-tar effects on growth.
In some cases (hem imandibula r hypertrophy bein g the hest example), the etiology of a deformity Illay lie in an al-ttted response of cells to normal growth st im uli. in hemi-mandibular hypertrophy, the inappropriate response is ex-assi'-e growth o f cartilage at the m andibular condyles, but in other types of dcformitic.~ it coul d be d eficient growth in other tissues. A relative resistance to growth hormone by el-
~ts within the mandibular elevatur muscles, fo r instance, coukIlead 10 some types of mandibular deficiency. Simply no mfonnation exists as to how this occurs, if indeed it does.
So how doe.~ a dentofacial deformity develop in the ab-sence o f some sp ecific cause? Consider a mandibula r den-cimcy severe enough to rcquire mandib ular advancem ent. It $(Oems Ukcly that such problems a re seen primarily in indi-riduals who were genet ically programmed toward a small momdible and in whom som e other et iologic facto r a lso came IDtO play. An insult 10 growth that would have produced only ~ moderate and orlhodol1tically treal
-
C HAPTER
-
C HAPTER OUTLINE
~socia( Impact of Oentofacial Deformity ~ctions to facial appearance Ef'fat of dentofacial deformity
- tivations and Perceptions in Seeking/Accepting lNtment
ftuences on seeking trcatmel1t Acceptance versus rejection of recommendations for
treatment F -:I:eri ng Information abo ut PsychosociaL
Oiaracteristics Ootaining sensitive information without giving
offense Expectations Evaluation of coping skil ls Social support ~p.aring Patients for Surgery
Techniques and procedures Treatment refusal and delay
.... ,.)nse to Treatment Evaluating perceptions of outcome Functional outcomes Satisfaction with treatment Health- related quality of tife
" .. .,..l'CI1hosocial Factors in Patient Management
A major reason that paticllts seck trcatmem for demo-fac ial problems is 10 overco me social handica ps re-sult ing from an abnormal facial appearance. Func-t ional impairment such as difficulty in chewing food, discom fort, ~l1d pain (especi
-
68 PART I The Nat.ure of Dent-ofacial Deform ity
30. King L, Harr is EF, Tollty EA: Heritability of ct'"phalometric and occl usal variables as assessed from siblings with overt maloc-clusions, Am I Or/ho/l Denl(Jfac Ort/wp 103: 121 -131, 1993.
31. Harris EF, Johnson MG: Heritability of craniometric and oc-clusal variable.~: a longitudinal sib analysis, Am) Orthod IJellto -fac Orthop 99:258-268, 199 L
32. Litton SF et al: A genetic study of Cla5.S III malocclusion, Am J Ort/wd 58565-577, 1970.
33. Proffit WR: Equilibrium theory revis ited, Angle Orthod 48:! 75-186,1978.
34. Fields H\V et al: Variables affecting measurement of vtrtical oc-clusal force, J Dent Res 65:135- 138, 1986.
35. Proffit WR, Fields HW, Nixon WL: Occlusal fon;,'arren 0\,,: Alterations in nasal airway re-sistance following superior repositioning of the maxilla, Am j Orthoil 85: I 09114, 1984.
40. Fields HW l"t al: Rd ationships ut:!\V
-
70 PART I The Nature (If Dt!ntofacial Deformi ty
A B
c o
Fig. 3 -1 AI what age do we begin 10 apply stcrt"Olypes associaled with physical characteristics? AI age 10 these child ren already are easily identified as fitting the "baby face~ catq;ory (A and U) or the "mature face" category (C and D). Research show~ that judgments about intelligence, friendliness, and behavior made by teachers and peers often arc influenced by facial appearance.
PSYCHOSOCIAL IMPACT OF DENTOFACIAL DEFORMITY
Everyone makes judgments aOOUl others from their facial ap-pearance, especially on first acquaintance. The stereotypes of characteristics that go with facial appearance are strongly re-info rced fro m childhood in telev ision shows. movies, and computer lma~cs (Fig. 3-1). For examyle, baby face individ-uals who have large eyes, high erebrows, a large forehead, and a small chill are assumed to he warm, honest, trusrworth}', su bmissive, na"lve, and relatively incompelent (Fig. 3-2), Ma-
lure (ace individuals, with the reverse of the above character-istics, are judged to be strong, dominant, aggressive, and com-petent (Fig. 3_3).3 Physical attractiveness is associated with sodally desirable characteristics, and an unaltractive appear-ance is associated with undesirable characteristics (Table 3- 1), This att ractiveness-halo effect, which is documented in a large body of literature, obviously is pertinent 10 dentofudaJ problems; disproporti.onate faces arc unattractive, and unat-tractive people arc handicapped socially.4
What makes faces attract ive and unattractive? In general, symmetric faces, straight p roflles, and facial proportions that arc close to the pop ulation average are considered the most attractivc.5 Women are judged less attractive if their
-
Chapler 3 PSYCHOSOCIAL ASPECfS OF D FXTOFACIAl D I+OR.\tl IT A..~D ITS TRI:ATMENT 71
A B
c D
Fig. 3 - 2 Pacial views before- (A and B) and after (C and Dj mandibular advancement surgeq' in a man with chin deficiency and a hahy facr, 3ppearance-. Most observers. reflecting the baby fa~ \er~\I.~ the mature face stereOtype, would judge the after-treatment person to be more mature. responsiblc. and reliable.
"".ve skeletal Class II I, and IIIcn are judged more nega-if they are skeletal Class II. This is consistent; baby face
Class II ) fea tures are generally viewed as fe mini ne whereas mature face (more Class 111) (CilturCS are con-
E t jed rnasculine.b
Put of Dentofacial Deformity tllS 'o\"ith denlofacial problems. by definitioll , have ellough ':::':0 frum normal denIal and facial proportions to cause Ji ;en; to react. How far away from the populatiun averages
you be to be pl
-
74 PART I The KOllurc of Dcnlofadal Deformity
A B
c
Fig. 3 4 A and B, Pretreatment facial appearance of a 25-)'car-old patient who chose camoufloge treatment for her skeletal Class II malocclusion. C, Cephalometric superimposition showing the In:3lm cnt effect that was achieved largely by rctraCiioll of the maxillary incisors. In this patient's view, her jaw relationships \wr~' acceptable and did not require treatment.
-
72
PART I The Nature of Dentofacial Deformity
A B
c D
Fig. 3-3 Facial views bdoft" (A alld S) and arler (C and D) maxillary advancement surgery in a woman wi th paranas.11 deficiency and an unes thetic chin prominence. After surgery she is likd )' to be perceived as more personable and affeCTionaTe, again reflecting the stereotypes of fucia l appearance.
of p rognathism attracts unfavorable attention, especially fo r females. Tin: cultural backgrolllul. Artificially enlarged lips would be considered beautiful in some African tr ibes. and in oth-ers tceth filed to points would be admi red. Neither of these wOlild be viewed positively in Western cultu re. Gellder di{fcrcllces. In most bul llQL all racial and ethnic groups, dental and facia l appearance is co nsidered morc importan t fo r fem:l les. Tile social setting. Higher socioeconomic status is associ-ated with greater :lttractiveness, and an unattractive ap-
pearam:e is more of a handicar if you wanl to be upwardly mobile socially. Tile e),'en' of the problem. As McGregor1 has pointed out, i.n some way:. it Gill be easier to live with a severe problem than a less severe one. This is probably be
-
Chapter 3 P!>YCHOSOCIAL ASP[CTS Of D I''-:TOMLlAl U Ef'OR..\lIIT AN I) ITS TR~ATMEN"l 73
"BLE 3-1 'Effects of Facial Appearance during Growth
d Development and in the Social, Work, Education, and Criminal Justice Environments
~ stereotypes emerge when strangers are asked to make ! ' Y,rliEnlS about people based sOlely on physica l appedrance. , ] .," ... social functioning in chiLdren and adolescents has been
I d to physical attractiveness. t:.rironment Attributes of Attractive People " .... tI. and More eye contact and affection froUl parents
a: .dopment Fathers expect to be more involved Perceived by others as better behaved and
friendlier 5ncia1 Pcrcci ~ed by others as warmer
ttiteractions More sensiti~e Ki nder More interesting
Percei~ed as more t rLIstworthy More Likable More persuasive in situations in which listener
has a choice Greater cont rol o~cr job efforts Perceived as more successful
!:'" - . ation Better social relationships with peers Hig her parental expectations for schoolwork
(r1-!inalj ustice Less presumption of criminality More likely to be belie~ed Given shorter sentences
Patients' perceptions of th eir own condition vary greatly. This means that an individual with a severe deformi ty may be affected less than an outside observer might expect, simply 411tGiuse he or she does 1101 perceive il as severe, although olh-ttS obviously do.8 The reverse is equally true; what looks like .. rdatively mild problem to others (.;an have a major impact , bt'Giuse the affected individual perceives it as being severe. P;arients' perception of their own dentofaciaJ condition greatly mats both motivation for treatment and decisions about the t1'pe of treatment (Figs. 3-4 an([ 3-5). This issue is discussed m some detail below.
Patie nts' react ions to the way they a rc perceived and treated vary greatly. Some people handle teasing or perceived ioIighlS better than others, even though they have the same dinical problem and are thought br others to be equally at-tractive. Howa person responds depends on a complex in-lUplay of behavio rs. attitudes, ami beliefs. For example, an .adolescent girl who hus a severe skeletal Class III problem may Dot seek treatment if appearance is not important to her 01" if she doesn't feel any negative comparisons of herself to others. Another girl with the same jaw problem is likely to
seek treatment if she attributes her social isolation to her ap-pearance or to having difficulty eating in public.
MOTIVATIONS AND PERCEPTIONS IN SEEKING/ ACCEPTING TREATMENT
Influences on Seeking Treatment Studies of pati ent motivations have consistently shown that the major reason for seeking correction of dentofacial prob-lem s is to improve facial appearance. Approximately two thirds of those who seek tre
-
Chapter 3 P SYCHOSOCIAL AsPECTS Of< DEI\TOFACIAL DEFORMITY AS D ITS TREATMENT
A B
)
c
Fi g. 3 - 5 A and B, Pretreatment fa cial appearance of a 25-year-old patient who chose orthognathic surgery for her skeletal Class II malocclusion. C, Cephalometric superimposit ion showing the effect of mandibular advancement. In tllt" patient 's view, the jaw relationships were not acceptable and required treatment. Note the similarity between the initial conditions of this patient and the one shown in Fig . . 3-4. The difference was much more in the patient'S perception than in the "objective" clinical findings.
75
-
____ . 7 ... 6 ____ P_A_R_T_I ___ '_I_h_e_N_"_'_u_,,;.,;of Oentofadal Deformit y
tnetic reasons fo r seeking treatment, and pa lients may be lIn~ willing to admit psychosocial motives during an interview, l!
It has been reported. and is generally accepted, that most dentofacial patients have coping ski lls t hat keep them within thc "normal" range o n psychological tests . .'\1 UNC. average scores for dClllofacial pat ients o n the SCL-90-R, a 90-item as-sessm ent tool used to measure current Ic\'cls of psychosocial distress, are only slightlydevated; that is, the group as a whole does not experience psydlOpathologic conditions.!3
This generali1:t1ion conceals the fact that in th is patient population, the percentage of patients with psychological dis-tress and/or psychiatric problems is well "bove normal. Gne quarter of the pret reatment consultations at U~C had p,sy-chological sym l>toms that warranted a "positive diagnosis," which identifies individuals with sufficientl), pronounced dis-tress TO warr;lOt intervention by a mental heah It specialist. Al-most 20% of the patients had sign ificantly elevated scores on the Global Severity Index (GSI ). lJ
lJ evations in this index, the single most sensitive indica-tion in the SCL-90-n of psychological distress, are particu-la rl)' noteworthy because the GSI reprcscllls a composite of dimension s. [n a rccent multicenter randomized clinical trial comparing wire and rigid fixation, 22% of the patienls had sufficient distress for a positive diagllo~ i s,t~ therefore this is not just a North Carolina phenomenon. An even higher per-centage of patients in studies done at UNC and the University of VVashington in Seattle reported being d is tressed just before surger}',15 meaning th at the hi gh prelrea tment scores also cannot be e); p1ained.,s being due only to the st ress of making ., decision about surgery. Patients who~e le~t scores are far outside the Ho rmal ran ge would benefit from face to-face eva luation by a mental health professional.
70
60
050 " E d 40 15 - 30 c
" ~ 20 10
0 Skeletal Class II Skeletal Class 111
Expectr:u (Proffit and Whilfl )
o Actual, 19805 (UNC DFClinic)
Actual. 1990s (UNC DFC!inic)
Long lace
Fig.3 6 The expected versus actual prevalence of patients in the dentofac iaI clinic. J3i!cause the long face group overlaps with the C13ss II and Class 111 groups, the lotal can be more than 100%. fI.'lore Class 111 patients and/or long face patients are seen than expected, wherC"
-
A
78 PART I The Nature of Dentofadal Deformity ~-
4
3
2
Eyes
o College student
Facial Image
Nose
o W
- Chapter 3 PSYCHOSOCIAl ASPEClS Of D H>:TOHCIAL D EFORM I'n' A:-l'y. In Fonsec
-
80 PART I The Nature of Dcnlofacial Deformity
Patients should be encourage
-
Chapter 3 PSYCHOSOCIAL A SPI!.CTS OF DI'.NTOFACTAL D FFORMlJ'Y AI'-l) h s T R.E.AJ ML."lT
BOX 3-1 Psychosocial Assessment and Considerations: General Consultation
1. Pro ... ide private st:tting with minimum of peopLe present. No interruptions during the discussion.
2. Include significant other or famiLy members in the discus-sions if possibLe, particularly when treatment simulations are presented. Emotional support of expected esthetic changes is ... ery
important to patient's recovery. Changes in familial resemblance may be especially
di ffi cult for family members and may cause acceptance problems for patient after surgery.
Family members shouLd be adequately prepared fOf swelLing and/ or bruising that may O(CUI in the first few weeks after surgery.
3. Differentiate between information sharing (patient and fam-ily) and sensitive information gathering (patiet'lt on ly). Patie rlts may be reluchnt to be honest about psychoso
cial issues. motives, at'ld/ or expectations it'l the presence of fami ly members.
Family membels, particularly parents, may be dominant yoices in joint sessions.
during the patient's conversational breaks, so that the patient fttls required to Iill the silence. Open-ended quest ions usually mabie the paticntlo fill the gaps. Such questions are as simple as "C..ould you tell me more about that?" or "Could you tell me more about how you coped with the te
-
Chapt er 3 PSYCHOSOClAL AsI'ECTS or D E:"TOFACIAL D EFORMITY ANI) In TRE'iJl.ffiNT 81
BO X 3-2 PsychosociaL Assessment and Considerations: before Surgery
Initial Orthodontic AS5eisment 1. Present broad outline of treatment options, including
surgery if appropriate. 2. Explore patient's motives for treatment.
What is the patient's main complaint? (Accuracy is not important. but identifi cation of a "con crete" probLem is.)
When and in what circumstances did the patient first be come aware of the problem? (A recent awareness in a pO~ladolescent or a familial fea-ture that creates distress because of a poor parent/child relationship should be explored .)
Why has the patient sought help now? (Seeking treatment du ri ng an acute crisis [e.g., divorce, loss of a job] may be unwise. A waiting period to assure commitment could be recommended.)
3. Explore patient's expectations for treatment. What does the patient want to be different in his or her
tife after treatment? Approach indirectly. Is someone pressuring the patienlto
have treatment? (With whom has the patient discussed the possibiLity of having treatment? What did the person think about it? Has anyone suggested that the patient have faciaL surgery? Who? Why does the patient thin k the suggestion was made?)
Orthodontic Consultation 1. Discuss tIM> patient's problem, solutions, and alternatives fOl
treatment. 00 you and the patient agree on what is the most impor-
tant problem? 2. If surgery is required, schedule an appointment with the
surgeon. 3. Discuss all phases of treatment.
practice dictates that the whole patient be treated, not just the 1ec.'lh and mouth . Then, Ihe slalemen! that treatment is ill ad ,-isM at this time should be made clearly and simply. It can be pointed OUI that excessive st ress or emotio nal problems should be controlled prior to treatment, just as an underlying heart condition or other health probl~m wo uld require. \\'ha lever the reason for delay or refusal, the practitioner should express confidence in his or her decision, yet express nnpathy for the patient (who may be severely disappoint('d). It helps to invite a palient who could be sllccessfully treated after Ihe problem is resolved to return for follow up consul-tations in 12 to 18 months. This goes a long way toward alle-,;ating feelings of rejection in dis.1ppointed patients. For pa bents who have been refused treatmen t, an invitation should ;dso be extended for additional referrals or assistancc in find ing appropriate alternative treatment.
Many treatment refusals or delays invo lve refe rral to a men tal heal lh practitioner, and orthodontists and surgeons
Surgical Consultation 1. Ex plore patient's motives and expectations fo r treatment
(see above) . 2. Review patient's records; discuss problems and possible
solutions. 3. Discuss surgical experience to the extent desired by t he pa
tient (see Preparing Patients for Surgery, p. 80). Provide consent formes) for patient's perusal, not signature.
Presurgical Consultotion 1. Assess patient's psychological well-being and current
stressors. Screen with iI psychological well-being instrument (e.g.,
SCL-90-R) and/or use inteNiew questions with onLy pa-tient present regarding (1) rece nt stressors at work or with fami ly (e.g., aging parents, spousa l problems, chil-dren's behavior or school pertormance); (2) personal or family history of depression or anxiety; (3) alcohol/drug usc; and (4) sleep pallerns.
2. Assess patient's coping skills. Approach indirectly. Ask, Hliow did you deaL with a partic
uLarly stressful event in your life?~ (The particular stressor is not as important as how the patient reacted and what actions he or she took in man-aging the stress.)
What support system does the patient have? (It is important to know not only who will be available for practicaL needs but also who will be available for emo tionaL needs.)
3. Review possible psychological and emotional symptoms that might occur after surgery. Give the patient "permission H to discuss these problems if
they occur; this removes the "1 must be crazy~ response if negative emotions occur.
PrepiHe the patient for counseling referral if required.
often worry about how to do this without offending the pa-tienL To make such referrals go smoothly, ('.0:0 things are nec-essary. First. the referring doctor mUSI become comfor table with the idea of psychological counseli ng as a constructive option for addressing li fe problems that is open to anyone, not jnst the severely mentally ill. Olherwise the patient is likely to detect negative, stigmatizi ng altitudes that can ac-centu~te problems. Second, establishing a collegial relation-sh ip with at least two competent therapists (preferably olle male and one female ) gives the patient a choice of the thera-pist's gender and makes it easy to offer to telephone olle of them now to arrange a consultation. The goal is 10 make it as easy as possible ror patients to get the treatment they need while commu nicating to them that th is therapy is neither frig htening nor unfamiliar. The lherapists need 10 undcrstalld Ihe complexity of treatment for dentofacial problems and the typical recovery from orthognalhic surgery. Inviting thera-pists to participate ill a study c1u h disCllssion or to ~ttend an
-
82 PART I The Nature of Dentofacial Deformity
afternoon of presurgica l and postsurgical evaluation visits will help them appreciate the issues tha t pat ients will face d uring and after treatment.
RESPONSE TO TREATMENT
EvaLuating Perceptions of Outcome The three ways to evaluate the outcome of treatm ent for dcnto fa cial problems are ( I ) measure physical dimensions, clinically and rad iographically; (2) evalu ate function with physiologic tests; and (3) ask the patients what they feci and thi nk. directly or via questionnaires. These last two methods overlap to somc extent, because function is hard to measure, and questions about functioll almost must be used to sup-plem en t clin ical tests. Chapter! 8 focuses on physical and functional outcomes. Here, the emphasis is on what paden ts perceive, as reported by them.
Two recent major sourCt:s of perceptual data exist: ( 1) the results from a multicenter randomized clinical lrial (ReI") led by Ph illips at UNC, which focused on the effects of treatment simulation presentations on orthognathic surgery patients' perceptions of recoverylO; and (2 ) rcporl~ from a multicenter ReT comparing the effects of maxi llomand ibular fixation (MMF) and rigid internal fixation (RlF) following mandibu-
lar ad vancernent. J4 Studies b)' Kiyak and co-workers al the Universi ty of Wash ington in Seattle in the 19805 provided an important basis for these studies.16
All these studies used palient self-report questionnaires to acquire information o n d ifferent aspects of perceived out-comes, including recovery, facial sensation, masticat ion and occlusion , and satisfaction. This work has documented the importance of the parient's emotional and psychological well-being o n the patient's perceived outcomes of treatment. A number of other investigators have published information abo ut percept ions of outcomes, which supplement what is ava ilable for the major sources.
Functional Outcomes Pat ients adapt well to the physical changes produced by treat-ment, but they often have a harder time than they expected in the immed iate postsurgical period.
Sho rt-term effccts of orthognathic surgery on ovcraU function Orthognathic surger y patients now have short hospital stays (typically only one night or no overnight stay at all ) and are mo re comfortable in the immediate post~urgical period when rigid internal fixation is used. Nevertheless, recovery to normal
Percent who scored
-
84 PART I The NUlUre of Dentofacial Deformity
A
B c
Fig. 3 -9 Advanc(s ill knowledge often requi re the use of (omplex and sophisticated equ ipment. A, III order to stlldy facial movements ~nd precisely track soft tissue changes, fo ur SillJult,lneous video
im~ges from different angles of markers on a subj~I's face are computer-coordinated for bIer detailed analysis, B and C, Frontal view of marker movements from res t to smiling. It is likely that subtle differl' llCCS in soft ri~ S\l e movements affect patient pcrccptiollS o f facial features and ernOlional reactions in ways nOI yel understood. (Courtesy Dr. C. Trotman, Chapel Hill, NC.J
significa nt neurosensory deficit. About 21 % of the surgery patients in the UKC study reported difficulty with speaking at 4 \0 6 weeks postsurgcry, but onlr 5% had difficulty with spce
-
Chapter 3 PSVl;HOSOCIAl AsPECrS OF DWTOfAClAl DEFOR.\.Un AND ITs TREATMENT 83
O'onall function takes time, whatewr the fixation method. The U C data (almost all patients had RTF) show that only half the patients felt they hul re turned to previous levels of activ-ity at 4 weeks postslITgery, and 70% felt that way at 6 weeksP
The percentages of the UNC surgery patients who felt un-prepa red for some aspects of the postsurgical period arc shown in Fig. 3-8. Two or more years pOSISurgery, fewer than 10% reported that hospital procedures had not been ex-plained or that they did not know what to expect after being released from the hospital. Bu t approximately one third said they had unexpected difficulty with the postoperati\'e period, md the memory of this was still vivid 2 years laterP Com-municating the elllotional aspects of recovery to patients can be quite difficult. It is generally helpful to ask patients how they might cope with an unexpectn] happening or delay in return to full activity, in addition to providing the percent-ages of possible complications or risks. It is import ant (ur the clinician to know the patient can respond adaptively to unexpe
-
Chapter 3 PSYCHOSOC],\]. A~!'hClS 0 1' O l NTQF,\CIAL D EFOR\I!n' ANn b ~ 1Rf . ... l .\lliNT 85
Percent
Change in Iccting of face or mouth1
Pain associated with change in feeling1
Numbness2
Jaw joint pain or soreooss2
o 20 40 60 80 100 Postsurgery
1 Percent who said Yes 046 Wk . 2Yr ~Percent who scored ~ on scale of '-7. Fig. 3-10 Percentage of patients who report ed lIherations in sensatiou, pain associated with the alteration, or TMJ pain or soreness after orthognathic surgerr. Almost three four ths of the patients, even 2 years afler surgery. reported an all t'ration in sensation, part icu larly on the ch in and lips. Approximately one fourth still reported some numbness. In contrast. fewer than 10% reported joint p;1in l years after surgery.
tirnts in the UNC trial reported pain in the ja\" joint shortly ..ncr surger)" and by 2 years fewe r than 10% reported joint pairu (see rig. 3-10).
Satisfaction with Treatment Esseotially all lo ng- term stlldies show that the great majori ty of dentofaci:tl pat ients are satisfied with the resl ll! of treat-men! and would fl'W Illm end it to others. [n the UNC study, 82% of pati ents repor ted being happy with the result at 4 10 6 weeks. This percentage increased to 90% by 2 years aft er surgery, even though 5% to 40% reported dissat isfaction .... ,i th specific aspects of their treatm ent outcome. Kiyak et al re-ported that females with a tendency toward neuroticism and intro\'erted males were more likely to report problems with immediate postoperative pain. They noted that e\'cn if dis-comfort was anticipated, postsu rgical di~com fort and fu nc-tional problems were causes for short-term dissat isfac tion .36 A reu;nt report has shown that older patiellts and pat ients who are positive about their (.'Sihetic improvement lend to l>c mo re sal isfiedF
In the UNC s tudy, as ill previous STudies, pat ients were quite IJlcascd wilh ti le esthetic results of treatment, aud c"cn al 2 years postsurgery reported receiving positive comments about their appearance. Onc fo urth of the patients agreed thai people they met fo r the first rime reacted m ore posi livel), rhan new acquaitltances had prior to the surgery (Fig. 31 1). Intcrestingly, 15% said they h:td expected more change ill thei r appe:lfallce than was achieved b ut neverthe le.~s repofted
satisfactio n wilh the results. Even when pers isten t problems with sens3tion or function were nuted, the patients usually reported that ther were s:t tisfied with the treatment.
D;lta from the Seattle Sl\ldies of orthognathic surgery Pll -tients in the 19805 showed au illterestin g clip in self-esteem and facial im age at 9 momhs postsurgery, with h igher scores again at 21 months.11i Th is drop WllS due to the o ne third o f the patients whose orthodontic t reatmem sti ll h;ld not been completed al 9 months. From the patiell t 's perspect ive, fi n ish in g the postsurgical orthodou tit:s with in 6 months af ter surgery is highly d esirable. Since that happens mOSt of the tillle now,J8 aided by an earlier return to the orthodon-tist when R1F is used, prolonged postsu rgical orthodontics is less of a factor in sa tisfaction than it used to be. Overall sa tisfactio n was h igh in the U~C trial. Average scores in-creased from 6 weeks to 6 m on ths but remained stable afrer that (Fi g. 3 12) .
Self. im:tge It is interesting to co mpare the outcomcs of no treatment, or thodontic camouflage. and orthognalhic surgery. Kiyak et al succeeded in recalling patients who had rejected treatment after it recommend:ttion for orth ognilthic su rgery, along with patients who had dlUsen only orthodontic camouflage and those who had ch osen surgery.16 Satisf:tction closely paral leled the scoreS patients gave themselves 011 overall body im-age and facial bod}' image scales. As E g. 3- 13 shows, botl! the cam ouflage and surgery patients had positive swres fOf body image that increased arLer [rcatment, bil t the surgery p:tt ients
-
86
High 7
6 c . 0 5 }l
~
4
6 3 2
PART I The Nature of Ocntofadal Dcfonnil),
Percent
Happy with results t:::::::::::::::::::J Would have same surgery again
Positive comments on appearance
Improved interaction on first meeting
o 20 40 60 so ' 00 Postsurgcry
0 4-6Wk . 2Yr
Fig. 3 11 Percentage of patients who reported po~itivc feedback after surgery. At 2 years after surgery, more than 80% of the pOltients reported being happy with the results of treatment and said that they would have the samc surgery again if needed. Approximafely 50% of the patients reported reu:iving posi tive comments on their appearancc 2 years after surgery, and about 25% felt that their interpersonal inTeractions when firsl meeting SO !ll~ne had improved.
t 751h % Median 251h% t ~~- ------ ---------. -",." ....... . ~.:. ;;:-.. -: ::: .... . ............ 0 ..... . 0
3
... Surgery-Orthodontics - . - Orttlodontics Only .. {> .. No trealment
L~ , -'--------------- L~ 2 4-6Wk S Mo End 01 or tho
Postsurgery
Fig. 3-12 Average scores for overall sa tisfaction after surgery. Overall satisfaClion is high, on average. even at 1 to 6 weeks after surgery.
Presurgery 1-2 Days 4-SWk 24Mo Inlerval alter Surgery
Fig. 3-13 Facial body image scores fo r surgical-orthodontics, orthodontics-only, and no treatment patients. The facial body image score was lowest ini tially fo r surgery patients but then sign ificantly improved, reaching its highes t level after 24 mouths. The changes for both the orthodontics-only and thc no treatment groups were not statistically significant, but the decline in the scores for thc untrea ted patient s who were successfully recalled at 2 years is interesting. (From Kiyak HA et al: Predicting psychologic responscs \0 orthognathic surgery,] Oral MlIxilwfac Surg 40: 150~ 155, 1982.)
-
PART I Thc NalW:c of Dcntofadal
PsychosociaL Assessment and Considerations: after Surgery
Immediate Postsurgery 1. Telephone patient to check on his or her progress and to
provide support (this reassures both patient and family) . 2. Assess patient's mood swings and n .. gativ .. emotions.
LISTEN. Provide reassurance that mood swings or transitory de-
pression are not uncommon and will disappear soon.
Postsurgical Orthodontics 1. Rcview trcatment progress with patient. 2. Monitor patient's mood and emotional response. Remem-
ber that pat ients are eager fo r the cornpldiotl of treal-ment. A decrease in satisfaction and facial body image may occur with extended treatment time.
expectations of problems in recovery in the short term after surgery, as well as an increase in the report of d ifficulties and problems in the first 2 months after surgery.1 5 Long-term postsurgica l or~l health outcomes are significantly associated with both presurgic~l and postsurgical overall psychological well_being.1M1
T he bottom line is straightforward: building rapport wirh patients and communicating wi th them throughout treat-ment SO that they understand what is h
-
Chapter 3 PSYCHOSOCIAl ASl'ECrS 01' D ENTOFACIAL DHOR\IITY AND II'!:> TII.5A1'Ml!NI'
-
~
-
.. -
..
'" ,
JD-
",.
0 -Prognathic Retrognathic
Ma;.:iliary Prognathic Retrognalhic
Mandibular
0 ""'Y'lathic surgery t::I Orthodontics only 0 Acquaintance
60
50
0 40 ~ -0 30
" if 20
10
o Short long Protrusive Retrusive
Vortical Dentoalveolar
Orthognathic surgery Orthodontics only D Acquaintance
Fig. 3 - 14 A, Pcrcentage of pati~nts who choose ol'thognathic surgery, patients who choose orthodontics only, alld acquainlances who perceived d ish;Hmon), in m~xil1ar)' and mandibular relationships prior to treatment. B, Percentages who perceived disharmony in their vertical and dentoalvoolar relationships prior to treatment. As expected, patients who elected orthognathic Sllrg~ were more likdy to perceive themselves as outside The normal range, particularly in the maxillary and
m~nr1ibl!lar components. Al though a higher proportion of all These patients viewed themseh'l"li (IS outside the normal rang~ in all four dimensions of d.:ntofadal disharmony, the difference between the orthodoll tic;-only and orthognathic .~urgery patients is much less for the I'ertka! and dCllloolveolar relations than for the maxillary and mandibular relationships.
_w.:d at a lower level and ended up higher, especially on the _ '" bod)' image sC
-
Ch apter 3 PSYCHOSOCIAL AS"'l:cr~ m U~ NTOFACIAL D EFOR.I\l ITY A!\O I IS TRL\1'ME.VI'
-
!"."'an AR et al: The impact of int~rpnsonal support on pa-nen: satisfaClion with orthognathic: surgery, I Oral Maxillofac
s..r~:944-948, 1995, :s ~'U AE et al: l.egal issue& of computer imaging ill pLa~tic
2' go y: a primer, Plust Reco/15fr Sli rg 100; 1601-1608, 1997. ?oed AB et al: The ro le of expe.; tations in patients' reports of posl-operatil'e outcom es and im provemcnt following therapy, ..., Gut 31 : 101\3-1056, 1991.
=- '
-
-ABLE 4-1
tofada l Treatment Paradigms -.. 'eter - treatment goal
Angle Paradigm Ideal dental occlusion Ideal jaw relationships
Chapter 4 EVAlt:.>l.TlON Of FACIAl SOFT T 1SSLlOS
Soft Tissue Para digm NormaL soft tissue proportions ilnd adaptation Functional ocdusion
93
_,.Wt tissue relationships Ideal hard tissue prolK'rtions produce ideal soft tissues.
Ideal soft tissue pro~o rtions define ideal hard tissue relationships.
; .. sti< emphasis not approach
Dental casts, cephalometric radiographs Ob:ain ideaL dental and skeLetaL relationships,
and the soft tissues will be OK.
Clinical examination of soft tissues Plan ideal soft tissue relalionships. and then place
the teeth and jaws as needed to achielle this. F : "'0 emphasis
. of result TM joint in relation to dental occlusion Related primarily to dental occlusion
Soft tissue movement in relation to dental display Related primarily to soft tissue pressures/equilibrium
effects
4-1 Facial soft tissue proportions are la rgely determined by underlying fac ial skeleton ; however, this is not the sole
, lklminanl, and it is the soft tissue proportions, not the skeletal i'u-~unions, tha t are the go~l of treatment,
""i;C1 harmoll}' and balance and the Slomatognathic sysTem function ideally. Angle illustrat ed this idealized view
the skull "Old Glory" and the neoclassical Greek sculp-lIiUe of the head and face of Apollo Bclvt'd ere. ignoring t,he a"1 that the (Afr ican) skull with its perfectly aligned teeth __ incompatible with the (classic Greek) face. The goal of '::'eUJnent was to produce perfect occlusion of the teeth, and :rial beau ty naturally wou ld follow as." nature's intended .Iul form" was achi eved . Th;'! t idea was discredited l!lauy -..:an ago, and early in the cephalometric era it was docu -
!lted that hani Tissue cha racteristics did not rrliablydeter-jne facial features3; however, the basic concept-that
dentit ion and fac ial skeleton determined the goals of "tt;iunenl-remainoo intact until recently.
In the modern biologicalmodcl, variation is the theme, ..J the clinician's task is to achieve the desired facial and den-
outcomes within the ability of the individual to adapt .,m.lmsiologically to the morphologic changes. The desired out-acllt$ h;lVe both functional and esthetic components, 'both
""h ich are strongly in fluenced by lhe soft tissues of the
head and neck. It has laken a cen tu ry not necessarily to lea rn but w accept that it is the soft tissues that largely determine the limitations of orthodontic and orthogllathic treatment. These soft tissue limitations include:
Pressures exerted on the teeth by the lips, cheeks, and tongue
Limitations of rhe periodontal attach ment Neuromuscular influences on mandib ular position The contours of the soft tissue faciaL mask Lip-tooth relationships and anterior tooth display dur-
ing facial animalion5
Thus an important goal of treatment planning for den to-facial problems is to ascertain an individual's available limits of soft tissue adaptation and the most desirable hard tissue-soft tissue relationships. Given the primacy of the soft tissues, clin-icians must establish treatment plans for the denti tion and fa-cial skeleton by "reverse engineering," deducing what would have to be done to the hard tissues in order 10 achieve the de-sired soft tissue outcomes.
This is the biologically driven "soft tissue paradigm" that will shape the treatment of dentofucial problems in the nvcnty-fi rst century. I! is iniLially an unsettli ng shift in mindset fo r at least two reasons: (1) it is revolutionary in that it represents a major change in our conceptual fr.Jlllework and (2) documen-tation (records and their measurements), the key elemen t in dentofacial diagnosis and treatment planning, must be ap-proached differently. Since tl1e morpholllctric tools fo r evalu -ating the facial soft tissues are not as good as those for mea-suring dental and skeletal characteristics. the new paradigm places greater emphasis on d inical examination of the patient. It de-emphasizes the dental casts and cephalometric radio-graphs that have been the basis of dentofacial diagnosis and treatment planning. Once the new paradigm is accepted, ho,,'-ever, treatment goals and procedures make sense in a new way.
In this section of the book, we present a systematic ap-proadl to diagnosis and treatment plan ning buil t around the new paradigm and emphasizing soft tissue considerations ill
-
CHAPTER
CHAPTER OUTLINE
The Soft Tissue Paradigm Growth and Maturation of Facial Soft Tissues
Growth and maturation of the lips Growth and maturation of the nose Maturational changes in the soft tissue chin
The Aging Face Soft tissue changes in younger adults Changes at older ages
Current Concepts of Smite Evaluation Methods for evaluation of the smile The smile related to the natura l dentition Smile arc flattening in orthodontic treatment
Assessment of Facial Soft Tissues: Frontal View Vertical facial proportions Transverse facial and dental proportions
Soft Tissue Proportions: Profile View Projection of the forehead Nasal and paranasal relationships Lip projection Chin projection Throat form
,
New Esthetic Concepts in Orthognathic Surgery Ocdusal plane rotation Increasing dentaL and skeletal voLume
Summary
92
he contours of the face reflect the underlying facial skeleton ( Fig. 4- J), so skeletal disproportions in-evitably affect the fucial 50ft tissues. It is recognized
now that the soft tis5ue effects of dentofacial treatment pro-vide its major benefits. functionally and esthetically. It has not always been this way. It is only recently that a soft tissue par-adigm, focusing the treatment of dentofacial problems on the son tissues of the face, has emerged in orlhodontics and Of-thognathic surgery.
THE SOFT TISSUE PARADIGM l\ paradigm can be thought of as a set of shared beliefs and
as.~umptions that represel1l the conceptual fo undation for an area of science or clinical practice. Those who work in that area may differ on details, but they share the concept. Ad-vances occur as new information is added incrementall),; a scientific structure is erected as if laying brick upon brick of new fllldiJlgs and insights. The introduction of a new para-digm meets great resistance ini tiall)" beca use the sciemific structure is destroyed and must be rebuilt . In that progres-sion, loday's truths may become tomorrow's myth s. Nonethe-less, once a paradigm shift has occurred, a veritable explosion of new ideas and information leads to rapid advances in the field. 1
A significant shift in the conceptual underpinnings of or-thodontics and orthognathic surger),. the major treatment modalities for dentofacia l problems. is occurring nol'l (Table 4- 1). Since the specialty was established 100 years ago, orlho OOlitic theory and practice have been based OIl the Angle par-ad igm.2 It is predicated on a teleological belief syslem lhal a.~sumes that when a "natural " delltitional state of ideal alignment and occlusion occu rs, the face should also be in
-
I 94 PART II Diagnostic and Treatment Planning Approaches facial esthetics. The theory of equilibrium of soft tissue pres-sures as a determinant of stability after treatment, the effect of tooth movement on periodontal structures, and neuromus-cular adaptation to orthodontic and orthognath ic treatment did not receive as much attention as perhaps i l deserved in the past, but at least these subjects were included in the train-ing most orthodontists and oral-maxillofacial surgeons re-ceived. 13ecause much of the necessarv consideration of facial , soft proportions is new to these clinicians, the goal of this chapter is to provide the necessary background for applica-tion of this aspect of the soh tissue paradigm to treatment of dentofaci;]l problems.
GROWTH AND MATURATION OF FACIAL SOFT TISSUES
A discussion i. over time- may see-m unne-ceS.
-
Lips grow earlier in girls than boys, and ill the so ft tissues as in the skeleton, a cephalocaudal gradient of growth is ou-sen-ro. This means that during childhood and adolescence, the soft t issues of the lower face grow more and for a longer rime than those of the upper face . Most of the vertical growth of the upper lip is achieved in females by age 14, whereas the Io .... er lip co ntinues to grow vertically to age 16. In males, growth of both the upper and lower lips continues into the bte teens, with more growth o f the lower lip (Fig. 4_4).7-9
lip thickness (which is observed ill cephalometric radio-yaphs and is not easily measured cli nically) increases during dllldhood and adolcscmce, reaches a maximum at the con clusion of the adolescent growth spurt (about age 14 i ll girls, .age 16 in boys), and then decreases in the late teens (Fig. 4--5).8,10 Girls have greater lip thickness than boys at all ages. h is interesting that the decrease in lip full ness that is charac-omstic of aging (and for \\'hich women no\.,,- often seek treat-Uit"llt by collagen injection ) begins a t so early an age ill both genders (Fig. 4-6).
Growth and Maturation of the Nose Although ~veral papers have appeared i.1l the orthodoutic li t
a-ature,6.lI-I~ nasal growth as a facfor in dentofacial diagnosis DJd treatment planni ng has not received as m uch emphasis as II. should.
In both males and fema les, the nose grows more verticallr rhan in anteroposterior projection. In boys, a spurt of growth
i
"
" " .o.g. !Ye1llS)
1_ Male ... Femal, I "
1_ MI\l
-
Class I male
Class I female
Chapter 4
Class II male
Class II lemale
Fig. 4-7 Patterns of nasal grOl1 til, based on cephalometric data from the Bolton growth study (i_p._. longitudinal data for whi te childrp.n of northern European deS(:ent). Note that both males and females show more growth in ver tical height than anteroposTl'r ior projeCTion of the nOse. but downward growth is greater iUlllales. Buys have an adolescent growth spurT in nost' length. whereas girls o ften do not_ A dors,11 hump in the nose often develops when Class 1Ililalocclusiun is prescnt and is more pronounced in boy!;. (I:rom Chaconas SJ: A STa tistical evaluation of nasal growth , Am J Orl/lOliS6:403 414, 1969.)
~
j0 C;\\ '7-
-
,
2 3
4
/
Males (x SD, mm) Females (K:I: SO. mm)
T, T2 T3 T, T2 T3 (1) ANS/SlS Class I 13'O I '2 15-21-3 17'U l '9 '" 1' -9t l -S 14-7 t t 3" 15-0i l "6
Class II 12'7 1'5 15-0 t '-9 16'6t 2'3" 11 '5 :::2-0 13-3 Hi"" 13'S:I: O g
(2) SOlUl Class I 15'5+ 1'4 17'7 i 2'6 19'9:1:2-7" 13'9 + 2-2 16-5:1: 2' "'' 16'9 2- , Class II 15'9 ~ 1 '3 17S t S 21'Ot2'6' " 14" ::: 2'1 16-6:1:2'9'" 17'2+ 2 '7
(3) Ultl Class I 14'4 :1: 1'3 15-4+ 1'6 17-0:1: 2' 1'" 12'3 ~ 1 ' 8 15'5:1: 1'5'" 16'2:1: 1 6 Class II 14'5:1: 1'S 16'2 1'7 17-7 :1: 1'9 ' 13-2 2-0 15'7 :1: 2 '2 I S'6 I-I
(4) PglPgs Claf>S I 11'1:1:2-0 11-8 :1: 1'7 13-4 .1. 1'4-" 11'5 + 1'6 13O.tl4" 13'S 1'3 Class II 10'4 1'5 12-0 tl '8 13'O t 1'3" 1'-9 2A 12-92'9' 13'2 t2-1
Fig. 4 - 8 Soft tissuc lip thickness cornpau d wi th chin thickness in males and females at ages 7. 12, and 17. Note that soft tissue thickness at the chin is less than lip thicknes-~. This d ifferenr.e increases eluring preadolescent grov.'fh anel remains the same d llriu); adoieS(:cncc. (From GCIlCOOV lS, Sinclair PM, Dechow PI.: Devel()pment of the nose and soft ti ssue profile, A'ig/e OrrhOi! 60: 191 - 198, 1990.)
97
-
96 PART II Diagn01>li~ and Treatment Planning Approaches
A B c
Fig. 4-6 Typical changes in fronl.al and profile soft tissue facial dimensions in a boy who did not have onhodontic treatment, dur ing normal growth. A, Age 5. Note that there is more display of \"crmilioll of the ulolper than the lower lip. B, Age II. Note the increase in lip fullness, reflected in thc frontal vi"-' in greate r vermi lion d isplay. C, Age 18. Lip fullness and vermilion display 1131'1' decreased with maturation. This decrease occurs at surprisingly young ages. as early as age 14 in girls.
Maturational Changes in the Soft Tissue Chin In the analysis of this th ird major soft tissue mass of the fa ce, extensive data exist to document the increasing projection of the bony chin during growth and maturation, Wh at changes occur in soft tissue projection of the chin? As with other soft
tis.~ue charaacrislics. these are gender and age related, In preadolescent girls, soft tisslle thickness of the ch in is
greater than in boys: o n the average, 11,7 nun versus 10,8 mm measured from pogonion (Pg) to soft t issue pogon ion (Pg')
at age 1 2.~ However, females had only a 1.6 mm increase up to age 17, whereas males had a 2.4 mill increase in tissue thick-ness over this period (Fig. 4-8). As a resul t, both sexes had similar ( 13.3 m m ) soft t issue chin thicknesses at age 17. The size of the mandibular corpus and the thickness of the bony symphysis fo r bo th sexes arc approximately the same at 7 yea rs, and th e gro\\1:h curves for males and females are paral-lel 1.0 each otha until age 15, after which m ales have larger changes. 16 'I'he increased chin projection seen ill males during
-
98 PART II Diagnostic a nd Treatment Plan ning Approachc!>
growth, therefore, is due mort: to underlying skeletal changes in late adolescence than to soft tissue changes. Perhaps more important, there is no reason to expect that the amount of soft tissue that covers the bony chill will change significantly during growth.
What is 1 he clinical siguific
-
Chapter 4 E VAW.\ 'I IO I\ OF F..-.cIAL SOn T ISSUES
A B c
Fig. 4-9 The effect of soft tissue aging in a pat ient who had surgical correct ion of mandiblllaT deficiency and vcrtical maxillary excess, A, Age 25, at completion of treatment . S, Age 35, 10 years later. C, Age 40, 15 years later. The skeletal and dental relationships were quite ~table, so relapse of treatment effects had 110thillg 10 do with the facial soft tissue changes. These a re typical of advancing age: sligbt jowling, submental fat deposition, deepening of the nasolabial groove, and droop of the comm issures.
3.50
3.00
~ 2.50 E E -
" 2.00 -
~ 1.50 ~ -~ .~
1.00 0 ~
0 ~ 0.50
0.00
-0.50 less than 30
1 Maxillary Mandibular
30 to 39 4010 1\9 Age (yems)
50 to 59 greater than 60
Fig. 4-10 Incisor display at rest. With aging, both men and women show k'SS of their upper incisors and more of their lower incisors (Le., display of upper incisors is a YOll thful dlJraC"kris tic). (From ViS !{(;, Arllndo GC: Kinetics of anterior tooth di~play, J Prosthet Dent 39:502-50'1, 1978 .)
-
, j II called the social smile, and the spontaneous smile has :- . Ii referred to as the enjorment smile. Since it was ,..1- line who first scientifically described the enjormenr
7 _, Ekman suggested thaI it be called the Duchenne smile h "Jr of this almost fo rgotten scientific pioneer. What dif-
an "'Ptes the social smile from the enjoyment smile is not .. tivity of the orbicularis oris musculature, but instead
ar poll ticipation of the orbicularis oculi. I n the enjorment 7:, there is a crinkling around the eyes that cannot be du-.. >1 .1 with a social smile. It is for this rcason that it has
__ $I said that we smile with O Uf eyes a ~ well as our lips. ~, the strained or forced smile is
-
100 PART II Uiagno~lic and Treatment Plann ing Approaches
Fig_ 4 - 11 "Ihe dC(rcasc in maxillary incisor display with maturation and aging is the result of an increase in the height of the upper lip, o!'specially phil:rum height. Note that as lip height increases, incisor displa)' decreases, cspcr-ially l>eyond age JO. (From Oickens S, Sarver, OM, Proffit \VR: The dynamics of the maxillary incisor and the upper lip: a cross sectional study of res ting and srnik hard and soft ti ssue characteristics, World J Orth()ll (ill press).
SUfe line is Olle of the determinant.s of the relative youthful -ness o f a smile. The best guideline is that 75% \0 100% of the ma:-.::illary incisor should be visible beneath the inlercommis-SUfe line in order to hay\, a YOllthful smi le.
Changes at Older Ages Wha t happens as patients get o lder (beyond the m id-40s)? For the most part, the changcs St'Cll in i'ounger ad ult life con-ti n ue. The mOSI comprehensive data available on th is age group are fou nd in Beh renu' reports of subjects fro m Ihe Boiton-llrush growth studies who responded to long-term recall and wcre seen when they were over 60, many in their 70S.23 Soft tissue changes noted ill these older adults included:
Nasa l projection There was an increase in nasal projection, and the nasal tip moved more inferiorly. The plastic surg;;ry li terature 011 ag-ing, whi le not quant ifying the changes, has always described a decrease in the vert ical posi tion (or "droop~) of the nasal tip. This occurred in both genders but was greater in males.2~
Lip thickness The lips followed the statistical curves established at earlier ages: they became less prominent and also tended 10 move inferiorly. The fu rther "th inning" of the lips in o ld age was not due so much to soft tissue shrinkage as to a changc in drape. That is, the upper lip tended to rolate down and back from the base of the nose, leading to less mrtxillary incisor exposure.
Naso la bial ch anges With the decrease in li p promi ncncc and lowering of the nrt5.11 tip, the nasolabial angle becam e- more aClltc. As thc nasal tip descends and rotates, the lip descends with it in what is best termed a clockwise rotation of the nasolabial complex.
The ChlHlgCS obscfI'ed with growth, maturatio n, and ag-ing serV(' as an important background for observation o f the soft tissues in indi"idual patients, who need to be viewcd from two perspectives: their situation at present and what it will be in the future .
CURRENT CONCEPTS OF SMILE EVALUATION It is impo rtan t to collsider the soft tissues during facial an-imation, not just at re.~I. By far the most important aspect of facial an i mation is the smile, which i .~ a cri t ically impo r-ta nt part of social interact ion. The smile and facial displ:l)' as related to communication and expression of em ot ion must be taken seriously in the context of dentofacial prob-lems. The importance of the smile so metimes is not appre-ciated simp ly because the psychosocial impact o f dentofa-cial deformi t )', and the impo rtance of red ucing these handicaps as a treatment goal, has not been acknowledged. A patienl whose treatment has resulted in normal jaw rela-tionsh ips and en:cIlcllt dental occlusion still may nOI have a pleasing smile, and ma y conti nue to have a psychosocial handicap lIlll ess anterior tooth d isplay during speech and smiling were considered when treatment was planned.
Interestingly, few objective criteria exist for assessing at-tributes of the smile, establishing tooth-lip relationsh ips for best esthetics, or evaluating Vit rious patterns o f soft tissue an-imation. II still is necessary to judge smiles subjectively, but this can be do ne systema tically in the context of whitl is known now about the effect o f varying tooth positions rela-t ive to an imation o f the lips.
Methods for Evaluation of the Smile One of the major goals of orthodontics andlor orthognathic surgery is to enhance anterior toot h display d uring speech and smiling. A balanced sm ile is achieved by appropriately positioning the teeth and gingiv
-
102 PART IT Diagnostic and Treatment Phmning Approaches
Oil smile) is not as altractive as complete tooth display or even some gingival display.u8 Males show less of the upper in -
cisor~ and lIlorc of the lower incisors than females, at rest and on smile.n It is also a characteristic of aging to show less of the upper incisOlS at rest and on smile, so that, to a degree, morc tooth display gives a more feminine and youthful smile.
The transverse dimension of the smile This characteristic is referred to in terms of "broadness 10 the smile" and the presence and amount of"buccaJ corridors."29 RecenLly, excessively wide buccal corridor.s have been referred to by some orthodontists as "negative space," to be eliminated by transverse expansion of the maxilla. It is well documented in tIle prosthodonlic literature that one of the characteristics of an unrealistic "denture smile" is a lack of buccal corridors. Presumably the same is true in the natural dentition; maxil-lary transverse expansion, like anYl 11 ing else, can he overdone.
Although this smile feature has been thought of primarily in krms of maxillary widlh, there is evidence Lllat the buccal corridors are also heavily influenced by the anteroposterior position of the maxilla Ielative to the lip drape . .lO This means, that moving the maxilla forward also reduces the size of the buccal corridors and decreases negative space (Fig. 1-IS).
Fig. 4 -14 Some gingival display on smile is esthetically appealing, because this is a youthful characteristic. (From Sarwr DM: The importance of incisor positioning in Ihe esthetic smile an:, Am J Or/hod Dellfojac Orthop 120:98-111, 2001.)
The smile arc A characteristi c of the esthetic smile that has not been recog-nized very well is the relationship of the curvature of the up-
A
Fig. 4-15 One of the effects of moving the maxillary arch fon"~rd is to decreJse the ~mount of space in the buccal corridors. This is the result of the wider portion of the maxilla coming forward . A, Prior to and (B) following maxillary advancement. Although the maxillary dental arch was not widened, the buccal corridur widlh has decreased. (From Sarver DM, Proffit 'WK Ackman IL: Diagnosis and treatment planning in orthodontics. In Gr~ber TM, Vanarsdall RL, editors: Orthodontics: currenf p'illciple.~ (md techniques, ed 3, St Louis, 2000, Mosby,)
B
-
jIIIII!!: mrrrior teeth to the curvature of the lower lip on smile, emile arc. The ideal smile arc has the curvature of the 8J1UY incisal edges parallel to the curvatu re o f the lower .,-... smile, and the term consonatlt is used to describe this
relationship (Fig. 4-16, A ). A rl O/lCOliSOltallt, or flat, l' Me is characterized by the maxillary incisal curvature
fbner than the curvalli re of the lower lip on smile (Fig. S . In his recent cosmetic dentistry text, Gol(lsteinJ I re-
bed to the same th ing in slightly different rerms. He de-w h f
-
C.hapter 4 EYAWAflUN
"" improvement in facial appear:lOce d uring animation U as at rest.
of their importance can significantly improve treatment outcomes.
These conccpts of smile estheTics are not new, but they .Itt only now beginning to be appl ied in the context of or-T .... :Iontic and orthognathic lrCtllment planning. Awareness
I.n the following sections o f lhis chapter, we emphasize sys-tematic analysis of facial di1l1ensions and proportions. An in -tegrated approach to development of the diagnostic database,
A
Fig . 4-18 A, Flattening of the smile arc also can occur from :lltr ition of the incisors, as shown by this individual with severe wear of these tL"Cth. 8 , Restoration of t he missing tooth structure (in thi~ case, with laminates on the facial surface of the incisors) can restore the smile arc.
A B c
Fig. 4-19 C.H., age 28, fuci~1 views prior to tre~tment. The p;lticm had or thodontic treatment wilh premolar extraction in her early teens, then surgery to set the mandible back at age 21. A, The frontal view at rest shows that [he lower facial height was 10nK, with a disproportionately long ch in . The upptr lip comprised only 25% of Ihe lo\\'er face versus 75% for the lower lip and chin. Her nasal width was slightly narrower than the intercanthal width, and the vermilion display of the upper lip was slightly les.o; than that of the lower lip. B, On 5mile, both the transvcrse [ooth. lip relationships and the amount of gingival display anteriorly were good. However, Ihere was sl ightly more gingival display in thc posh:rior aspect of thc smile [han the anterior. There was a moderate posterior cant to the maxillary arch that contributed to the flat smile arc. C, On profile, thc nasal tip was slightly overprojected and located more inferiorly than desirable. The nasolabial angle was sl ightl)' acute because or the low nasal tip placement. The upper lip was not as procumbent as the lower lip, and the mandible was slightly ahead of the maxilla. (From Sarver DM: The imporlance of incisor positioning in the e~ t hetic ~m i l e He, Am ] Orthod Dell/ofae Orr/lop 120:98-111 ,200 1.)
B
-
PART U Diagnostic and Treatmen t Planning Approaches
taking into account the relationship of the incisal edges to the lower lip curvature, positioning of the incisors relative to the smile arc may be compromised. How often would that occur? Perhaps in as many as one third or the patients. Just as patients get individualized treatment plans, they also should have in-dividualized designs for appliance placement.
Bracket placem ent that unwillingly leads to superio r repositioning of the incisal edges of maxillary inciso rs relative to the posterior buccal segments For examplr, with an emphasis on the goal of attaining ca-n ine guidance, it is possible to create relative intrusion of the maxillary incisors while extruding the maxillary canines. The 14-year-old pa tient in Fig. 4-17 ha s canine guidance, and articulator-mounted casts would be judged to show an excel-lent result; however, there is a nonconso nant smile arc with SO% of the upper incisors displayed on smile. Canine guid ance does not have to be achieved at the expense o f the ap-pearance of the smile, but it can happen.
Bracke t placement that elo ngates lower incisor.~ a nd re(llIires m axillar y intrusion fo r overbite correcti on Placing the lower illcisor brackets close to the gingival mar-gins in an effort to a\,oid occilisal int erferences that miglll cause loss of brackets results in extrusion of the lower incisors (see Fig. 4-17, BJ. If this requires vertical com pensation of the upper incisors to open tlle bite, flattening of the smile arc is likely.
Maxilla r y incisor in tr usion to decrease gingival display without considering the lower lip contour on smile If the smile arc relat io nship has not been noted and evalu-ated, unwanted flattening of the smile arc may result from the
A
llse of maxillary intrusion arches in adults or maxillary arch-wires with an accentuated curve of Spec at any age.
The patient 's inher ent growth pattern AckerlJla n's study of smile arc fhittcning26 showed that, al -though treated patients have a higher rate of smile arc flat-tening, this occurred in 5% of the untreated popUlation as well. Theoretically, this would be more likely in patieng with growth in the brach}facial (skeletal deep bite) pattern.
Habits Habits may also be a factor in flattening of the smile arc. The reduction in
-
PARTll Diagnostic and Treatmcni Planning Approaches
A
Fig . 4 20 CJ I. , before (Al and after (8 ) trcatmCJlt that involve:Fig. 4 21 C.H., cephalometric ~uperimposition showing the changes prod uced by clockwise rotation of the occlusal and mandib ular planes wilh 5upC'rior repositioning of the postcriQf maxilla via LeFort i osteotomy and rolalion of the mandible via bilateral sagittal split osteotomies, combined WiT h vertical reduction genioplasty and rhinoplasty. Note that the maxillary incisor position was maintained ver tically and hor izon talt)' while the palata l plane rota ted aroun d the incisal edge, resulting in advancement of the bOIlY support of the nose and augmentation of the paranas.al areas. The clockwise rotation of the mandible resul ted in less projt ion of the chin and better chin -lip balance; chin height was reduced by Ihe genioplasty; and the nasal lip was ele\'aled and shortened. (From Sarver OM: The imporlance of incisor positioning ill the esthetic smile are, Am J Or/hod De1llrJfa{ Ortlwp 120:98-111, 200 \. )
B
-
Chapter 4 EVALUATION OF FACIAl SOfT TISSUES
A B
c o
Fig. 4 -22 A to D,CII., age 29, facial views at the completion of treatment. Rotation of the jaws, reduction in chin height, and refinement of the nose all were key components o f the esthetic improvement. Note the improved rdationship of the: upper to the lower lip, \\ilh increased vermilion display in the upper lip; the improvement in vertic.11 proportionality of the face, due prim arily to the reduction in chin height; and the improved appearance of the midface. The contribution of the advancement of the maxiJI:l and the effect of gre;tler upper lip projection relative to the lower lip, as well as the refinement of the midface with rhinoplasty, ca n be appreciale
-
A
Fig. 4 - 23 An appropri ate proportional rcl3tionship of the height and width uf the face is import~nt. A, Patie ll l with a shorl lowcr face and a chief complaint of "my fact' is too rolllld,~ which reflects her perception of the disproportion between facial width and height. B, Vertical geniopl:lsty via a downgraft of the lower border of the mandible lenglh
-
108 PART It Diagnostic and Treatment Plan ning Approaches
which builds on the information provided here, is presented in the next chapter.
ASSESSMENT OF FACIAL SOFT TISSUES: FRONTAL VIEW
Systematic assessment of the facial begins with thc fro ntal view. Normative values for selected facial dimensions for Caucasians of northern European ancestry. taken from the studies of F:ukas,34 are provided in Table 4-2. In a sense, e\'erything is relative. Thai is never more true than when fa-cial proportions are assessed. Proportional relationships, which are mOfe important than absolute values, are shown
TABLE 4 2
Facial Anthropometric Measurements (Young AduLts) Parameter Male Zygomatic width (zy-zy) (mm) 137 (4.3) Gonial width (go-go) 97 (5.S) Intercanlhal distance 33 (2.7) PupiL-rnidfac:ial distance 33 (2.0) NasaL base width 35 (2.6) Mouth width 53 (3.3) Face height (N-gn) 121 (6.8) lower face height (subnasale-gn) 72 (6.0) Upper Lip vermi lion 8.9 (1.5) lower lip vermiLion 10.4 (1.9) Nasolabial angLe (de9rees) 99 (8.0) Nasofrontal angle (degrees) 131 (8.1)
Female" 130 (5.3) 91 (5 .9) 32 (2.4) 32 (1.8) 31 (1.9) 50 (3.2) 112 (5.2) 66 (4.5) 8.4 (1.3) 9.7 (1.6) 99 (8.7) 134 (1.8)
Data frOIll Farkas lG: Allthropometry of the head mId face in medi-rilll', ed 2, :New York, 1994, Ravcn Press. ' Standard deviation is in parentheses.
TABLE 43
FaciaL Indices (Young AduLts) IndelC Measurements Facial n-gn/zy-zy MandibLe-face width go-go/zy-zy Upper face n-sto/zy-zy Mandible width-face height go-go/n-gn Mandibular 5to-gn/go-go
in Table 4-3. It should be kept in mind tha t even these are merely gu idelines; by no means all normal or acceptable faces will have exactly these proportions.
Attractive faccs tend to have proportions and relationships thaI are slightly different from the normative values (which merely reflects the fact tha l lhe average individual may not be particularly artractive). As we have emphasized, some at-tractive faces have quite different proporLiolls, so it must be kept ill mind thaI the ideal proportions are merely guidelines. Nevertheless, they are an important part of background in-formation and a place to start in analysis.
In judging facial soft tissue proportions, the first thing that should be doni' is to examine the ratio between the height and width of the face, which is the facial index. Neither heigllt 1I0r width ca n be viewed independently. The complaint of a round face is
-
110 PARTn Diagnostic and Trea tm ent Planning Approaches
Fig. 4- 26 The 45-dcgree view of the face provides an excellent view of the key points in nasal anatomy: the shape of the dorsum, the ~double b reak" at the suprat ip and infratip, the columella length, and the contour of the nasal cartilage that creates the "scroll" of the nostrils. (From Sar\'er.~)
A
Fig. 4-27 Exce5s;\"C lown face height has two major components: vrrtical maxillary excess alld excessive chin height , both of which may he present in the same patient. On clinical examination, pure vertical maxillary excess is chara(tcrizcd by excessive length of the upper part o f the lower third of th"
fac~, witl! lip separation at rest so that the upper incisors are expoSKo, and with normallowcr lip-l own inciso r to chin distance. Exct'ssive chin height is apparent when the lip-chin distance is increased. A, This 16-ycar-old girl's long face is due primarily to vertical maxillary txcess, \.J u t as often is the case, the incisor-chin distance is slightly increased as well. B, This i 8-year-old boy's long bce is due as much or mort' to vertic.11 chin excess as 10 vertica l maxillary excess (see fig. 4-28 for additional facial views and cephalometric radiographs).
B
-
TABLE 4-4
incisor Display by Race MilAN I NC ISO K Ex I'OSIJK (mm)
k e Maxiltary Incisor MandibuLar Incisor White 2.43
1.5 7 1.86
0.98 1. 42 1.58
D ,U from Vig RG, Brundo GC: Kinetic.s of anterior tooth displa)" Prw.lwt De", 39:502-5{}4, 1978.
~ contour of the alae from the base of Ihe nose to its tip - wid be well defined to for m a "scroll" (Fig. 4-26).
In the ideal lower third of the face, the upper lip comprises upper one thi rd and the lower lip and chi n make up the
two thirds. Excessive lower face height can be caused and this almost always is
.! ,. 2lpanied by excessive display of gingiva on smiling as well. ETUSSive 1001h displa}' may be a resuit of both hard tissue
_ soft tissue factors, such as the followi ng: ,
Shor, philtrum lJeigllt. In a child, this has been shown to lK almost always a result of incomplete lip growth. Tn w adult, a short philtrum is si mply an anatomical vari
~. but when nott"d, it must be considered in the over-~ treatment plan.
- \ OtiCllI maxillary excess. Excessive vert ical growth of the maxilla.
Vestive croWIJ height. This is !;Cen when the smile line travels to the gingival margin, but excessiw tooth shows .at rest. Simple measurement of crown height reveals wbelhcr the tooth is too long.
lingually tipped maxillary illcisors. Lingual tippi ng or
Chapler 4 EVALUAnON O~ FACIAl. SOtT TtssL"lS 111
the upper incisors, either through normal Class" com-pensation or o rthodon tic retractio n without torque control, brings the incisa l edges downward as weU as back and increases their display (Fig. 429).
inadequate incisor display. Failure to show any of the upper incisor at rest or failure to show most of the clinical crown on smile indicates too lillie display (Fig. 1-30). Th is also may bt" a resuit of both hard tissue and soft tissue factors> which include the followi ng:
Excessive philtrum height. This is rarely seen except in the older adult and is a result of soft tissue aging and loss of elasticity.
Vertical maxillary deficiency. Inadequate vertical growth of the max iUa.
Inadeqllate crown height (loss offootll structure). This is seen when the smile lillC travels to the gi ngival margill, but only 1 mm or even no tooth shows at rest . Simple measurement of crown height reveals whether the tooth is too short.
Flared maxillary il/cisors. Flaring of the upper incisors, which rotates the incisal edges up as well as facially. Thi,~ can occur through naturally occurring dental compen-sa tion for Class 111 growth, Class 111 orthodontic treat-ment, or upper incisors resting on the lower lip in the presence of excessive overjet.
Transverse Facial and DentaL Proportions The "rule of fifths" (E g. 4-31) describes the ideal transverse relationships of the face; the face is divided sagittally into five symmetri(; and equal parts, and each of the segments should be th e width of one eye.3S The rule emphasizes the total dentofacial area and is based Oil proportional relationships, not absol ute measurements.
The central fifth of the face The middle fifth of the face is delineated by the inner canthus of the eyes. A line from the inner canUlus should be coinci-dent with the ala of the base of rhe nose; that is> the width of I he alar base of the nose should equal the in ner canthal d is-tance (Fig. 4-32). If the iUlLer cdnthal distance is smaller Ihan an eye width, the 1I0se should be slightly wider.
The width of the alar base is heavily influenced uy inher-ited ethnic characteristics. Bealusc noses vary in prominence, shape, and width among nidal and ethnic groups> il is very important to be sensitive to the ethnicity of the patielll whe21 variations ill nasal proportions are discussed.
The medial fifths of the face For ideallransverse proportionality of the face> the width of Ihe mouth and the interpupillary distance should be the same (see Fig. 4-31) . A line frOIll the outer canthus of the eyes should be coincident with the gon ial angles of the mandible; that is, the bigonial width should equal the outer canthal dis-tance. If the width of the ramus has heen affected by a con-genital defeCf or disease process , th e amount of transverse
-
A
A
Chapler 4 EVAl.UATION OF FALlA!. SOrT T ISSUES
,
,.' , " , " ( .; ,I,
Fig . 4 -29 A, When the maxillar}' incisors have been rippe
-
112
D, E
PART Il a n d Treatm ent Plan n ing Approach es
A B
c
Fig. 4 28 A and 8 , If thc amount of incisor displu)' at rest is excessive, an unesthetic display of gingiva on smile is quite likely to be preseu t, bUllhc reyerse is nOI necessarily true; gingival di\play on smile, in a patien I with normal i ndsor -I ip relationsh ips at rest. rarely is a problem. In this patient with vertical lllaxilbl'Y cxcc~~ (also ,ee Fig. 4-27, A), Jlote that the incisal edge of the upper incisor is below the lower border of the upper lip at rest, ami there is ('xccssivc gingival display on smile. C, On the cephalometric rad iograph , note the incisor-lip relat ionship at rest. It is important to obtain the cephalometric radiograph with the lips at rest so that this resting lip relatio nship can be observed. The patient 's orthognathic surgery involved moving the maxilla up both an teriorly and posterioriy, with more vertical movement posteriorly. D and E, In this patient with a long face due to a combination of moderate vertical maxillary excess and eXCCS$ chin heieht. note that the relationship of the upper incisors to the upper lip is nearly normal at rest and on smile, with the lower inci$Or~ displayed. on smile. ". On the cephalometric radiograph. compare the incisor lip rdationship with that of the palient in pa rt C. For th is palient. the vertical correct ion was obtained at surgery wi th approximately equal parIS uf superiur repositioning of thc posterior maxill a and tlpward-forw~ rrl movemcn! of the c.hin.
J
F
-
Fi g. 4 31 Ideal sagittal facial proportions fo llow the "rule of fifths,~ with each fi ft h appro)(imatcly the dimension of one eye width. (From Sar\"er.4)
Fig. 4 32 In ideal transverse proportions, the inner canthal d istance and The nasal widTh are The 5.1me (the inner canthus of each C).,. lines up with the lateral aspect o f the nostril) and the in-!erpupillar)" distance and the mo uth width are the same (thc pupils of the eyes line up with the commissures).
A
Fig. 433 A, This patient 's bigonial width was signifICantly less than Ihe upper fa ce width and ou t of proportion wi th the urul e of fifths. She had chronic ar thritis. with bil ateral condylar resorption. anterior open bite, and narrow bigonial width. 11, After leFort I o~ teotomy for optn hite correction was performed. gonial angle implants were placed to improve tlu:: billonial width. (From Sarver.4)
B
-
~ugmentation of the ram us sho uld be determined from ulis rdationship (Fig. 4-33).
The o uter fifths o f the face 'The outer fi ft hs of th e face are measured from the outer ca n-thus of the eye and gonial angles to the helix of the ear. Th is dimension is largely composed of the wid th of the ears. Pro-truding or malformed ears call be a part o f a dentofacial de-ixmity and should be acknowled ged as a potential problem. .0\5 " i th noses, there are racial and ethnic variations that makc ear form a delicate subject, bu t otoplasty is q ui te successful .. correcting ear discrepancies. 11 should be offered if the ear IS
-
A
A
Chapter 4 EVAI1IATIOS 01: FACIAL SoFT TlSWES
Fig. 4 -35 A, This girl's appearance of prolrusive lips, whith was her chid complaint, was due more to the imbalance ~tween the position of her lower lip and chin than to protrusion of both lips. a ,Advancemen t genioplasty wilh no orthodontic treatment corrected the protrusi\'l~ appearanCe without the undesirable re traction o f the upper lip that would have resulted from o rthodontic treatment to retract the incisors.
Fig. 4-36 A, This girl's complainl also Il"dS protrush'e lips, but they ~'ere marked I)' everted. and lip strain was present with the lips together. a, In hrr case, premolar ext raction and retraction of incisors also produced excellent profile esthetics. Similar to augmenting the chin (s.:e Fig. 4-35), rdracting the incisors also reduces both lip protrusion and lip separation al rest. (From 5.1rvO"r.)
B
B
117
-
116 PART II Diagnostic and Treatment Pklnning Approaches
coincident wilh the base of the nose. From inferior to superior, the forehead should slope posteriorly at about as-degree all-gle. A steeper angle contributes to the appearance of greater fa-cial convexity, and a lesser angle makes the profile look flatter. Although these characteristics may be noted on clinical exami-nation, it would be ll ighly unusual for a surgeon to recommend altering the forehead because of the morbidity of the procedures required tu do !hdl.
Nasal and Paranasal ReLationships The nose dominates the midface on profile (see Fig. 4-34). Its size ~ nd projection must be considered in the context of lip and chin projection; all other things being equa!, the bigger the nose, the mo re lip and chin p rom inence are needed to achieve reasonable facial balance.
A dorsal hump in the nose is apparent on frontal exami-nation bUl often .;;all be appreciated beller from the profile view, especially by p;"ttients, who rarely see their profile and often are surprised by their nose when they examine profile images carefully. I n an ideally contoured nose, the radix (the depth of the concavity at the base of the forehead) should on profile view obscure rhe eyel ash all lhe opposi te side. The bridge (nas"l dorsum) should then be a straight line from the base of the radix to the nasal tip cartilage, and there should be a sligh t prominence of the lip rehl\ive to the bridge. The nil~ I tip is slightly triangular rather than rounded or amorphous, with a distinct break in contour between the supra tip and the tip and again between the infratip and the columella (the "double break" that is sought in rhinoplasty).
It also is important to note the prom inence, or lack of it, of the paranasal areas of the maxilla. Normally, on profile view a convexity of the cheeks lateral to the nose partially conceals the alar base. Paranasal deficiency, a flatm:ss of the cheeks in this area, often is present in patients with maxil-lary deficiency. It contributes to an overall appearam;c of a sunken-in midface, but it may make the nose look bigger on profile simply because little or nOlle of the total nasal pro -jection is concealed.
The esthetic outcome of orthodontic and/or orthogna