Contaminants from the transplant contribute to intimal ...
18
Contaminants from the transplant contribute to intimal hyperplasia associated with microvascular endothelial cell seeding Cora HP Arts 12 Paul PhA Hedeman Joosten 1 Jan D Blankensteijn 1 Frank JT Staal 3 Peter YY Ng 3 Glenda J Heijnen-Snyder 12 Jan J Sixma 2 Hence JM Verhagen 1 Philip G de Groot 2 Bert C Eikelboom 1 Department of Vascular- and Transplantation Surgery 1 ; Thrombosis and Haemostasis Laboratory, Department of Haematology 2 and Department of Immunology 3 , University Medical Center, Utrecht, The Netherlands Eur J Vasc Endovasc Surg 2002;23(1):29-38 3
Transcript of Contaminants from the transplant contribute to intimal ...

Contaminants from the transplant
contribute to intimal hyperplasia
associated with microvascular
endothelial cell seeding
Cora HP Arts12
Paul PhA Hedeman Joosten1
Jan D Blankensteijn1
Frank JT Staal3
Peter YY Ng3
Glenda J Heijnen-Snyder12
Jan J Sixma2
Hence JM Verhagen1
Philip G de Groot2
Bert C Eikelboom1
Department of Vascular- and Transplantation
Surgery1; Thrombosis and Haemostasis
Laboratory, Department of Haematology2 and
Department of Immunology3, University Medical
Center, Utrecht, The Netherlands
Eur J Vasc Endovasc Surg 2002;23(1):29-38
3

36
Abstract
Objectives: Seeding prosthetic grafts with fat-derived microvascular endo-thelial cells (MVEC) results not only in a nonthrombogenic EC layer, but alsoin intimal hyperplasia. Here we investigated incidence, composition, pro-gression, and cause of this intimal hyperplasia.
Design: EPTFE grafts with MVEC were implanted as carotid interpositionsin 6 dogs with 1 mo, and in 3 dogs with 4, 8 and 12 months follow-up. Graftssodded without cells, implanted in the contralateral carotid, served as a con-trol. In another 3 dogs labelled cells were seeded to investigate the contribu-tion of the seeded cells (2-3 wk).
Materials and methods: MVEC were isolated from the falciform ligament.Cells were pressure sodded on ePTFE grafts. Labelling was performedusing retroviral gene transduction. The grafts were analyzed with immuno-histochemical techniques.
Results: After 1 month, all patent nonseeded grafts (5/6) showed fibrin andplatelet deposition, and all patent seeded grafts (5/6) were covered with aconfluent endothelial monolayer on top of a multilayer of myofibroblasts,elastin and collagen. After long term follow-up, all nonseeded grafts wereoccluded, all patent seeded grafts (4 and 12 months) were covered with anEC-layer with intimal hyperplasia underneath. The thickness of the intimadid not progress after 1 month. Transduced cells were found in the endothe-lial monolayer, hyperplastic intima and luminal part of the prosthesis.
Conclusions: MVEC seeding in dogs results in intimal hyperplasia in allpatent grafts, which contains myofibroblasts. Contaminants from the trans-plant contribute to this intimal hyperplasia.

37
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
Introduction
Seeding autologous endothelial cells onto prosthetic small diameter bypasseshas been developped to improve patency.1 This technique has been studiedextensively over the past years with vein-derived EC. Initial results were disap-pointing as the number of cells harvested appeared to be too low to covergrafts confluently. First culturing the cells and subsequently implantating theseeded graft in a second procedure, resulted in favorable outcomes in animalmodels2-4 and in humans.5-7 Due to the need for cell culture, however, it fails tobecome popular among vascular surgeons. Culture makes the procedureunsuitable for urgent cases, cells may grow poorly or may become contami-nated, and the procedure is expensive.5 For this reason investigators havelooked for other sources of EC.Our group first investigated the possibility of using mesothelial cells (MC) asan alternative for EC. Despite hopeful in vitro results, final in vivo experimentsshowed that these cells did not have the desired antithrombogenic and fibri-nolytic properties.8 Subcutaneous fat tissue was found to be a source of largeamounts of microvascular endothelial cells (MVEC).9 In vitro experiments withcultured cells, statically and under blood flow conditions showed expectingresults.10,11
Via a pressure sodding technique, MVEC can be inserted directly into thecrevices of polymeric grafts,9 resulting in a graft ready for implantation within afew minutes. In dogs, MVEC sodding of small diameter expanded polytetraflu-oroethylene (ePTFE) vascular grafts resulted in a statistically significantimprovement in graft patency.9,12 So far only a limited amount of human stud-ies have been published13-15 with quite disappointing results.13,15 The few sam-ples available for histologic evaluation showed EC on top of a progressivelyconcentric intimal thickening.13,14 Intimal hyperplasia has also been found indogs,9,12 but seems to expand more progressively in humans,13,14 ultimatelyleading to graft occlusion.Aim of this study was to investigate specific characteristics of this MVEC seed-ing related intimal hyperplasia, such as the incidence, composition and pro-gression in time, and the contribution of the seeded cells.

38
Methods
Design of the studyEPTFE grafts with falciform derived MVEC were implanted as carotid interposi-tions in dogs.A We studied the incidence and composition of the intimal hyperplasia, usingsix dogs with a follow-up of 1 month.B Three more dogs with a follow up of 4, 8 and 12 months were used to inves-tigate the progression in one year.C To determine whether the seeded cells contribute to the intimal hyperplasia,genetically marked MVEC were seeded in three additional dogs. Follow upwas 2 weeks for one and 3 weeks for the other two dogs.Acetylsalicylic acid, 80 mg a day starting one week before the experiment,was given the first month to prevent platelet aggregation.9 The three dogswhose cells were genetically marked before seeding were also given immuno-suppression, azathioprine, 25-50 mg a day starting one week after implanta-tion of the grafts, as expression of marker peptides on the cell surface resultsin the development of cytotoxic T-cells.16
All grafts were implanted as paired grafts, where one graft served as a control.The relation of intimal hyperplasia to MVEC seeding could be established byimplantation a nonseeded graft on the other side. Possible differences in cellbehaviour due to genetic marking and immunosuppression could be demon-strated by implantation a graft seeded with non-labelled cells on the otherside.
Animal careAnimal experiments were approved by the ethics committee of the Universityof Utrecht. The animal care complied with the Guide for the Care and Use ofLaboratory Animals, Institute of Laboratory Animal Resources, Commission onLife Sciences, National Research Council. Washington: National AcademyPress, 1996. Twelve mongrel dogs, weighing 10-40 kg, were used.
AnaesthesiaAll surgical procedures were carried out as described before.8 Just before thefirst incision, antibiotics (amoxicilline) were administered, and just beforeclamping of the vessels, heparin (100 IE/kg) was given, both i.v.

39
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
Postoperatively pain medication (buprenorfine) and antibiotics (amoxicilline)were administrated i.m., for 4 days.
Isolation of microvascular endothelial cellsMVEC were isolated from the falciform ligament.9 Amounts of fat were incubat-ed for 30 min at 37° C under continuous vigorous shaking with equal volumesof crude collagenase obtained from Clostridium histolyticum (Sigma-AldrichChemie, Steinheim, Germany) (0.4% w/v), BSA (Sigma) (0.4% w/v) inPhosphate Buffered Saline (PBS), pH 7.4. The digested fat was sieved andcentrifuged (1200 rpm; 12 min; room temperature (RT)). The pellets wereresuspended in Medium 199 (Gibco BRL, Life Technologies, Paisley,Scotland). The cellsuspension was centrifuged again (1100 rpm; 5 min; RT)and the pellet was resuspended in sodding medium (Medium 199 with autolo-gous serum in a ratio of 6:1).The cells used immediately for seeding were suspended to a concentration of2x105 cells/cm2 of graft surface. The cells used for identification were seededin a concentration of 1x105 cells/cm2 on fibronectin-coated glass coverslips.The cells used for of genetic labeling were seeded in the same concentrationon Retronectin®-coated (Takara Biomedical Group, Shuzo Co, Shigo, Japan)non-tissue-culture-treated plates.
Identification of isolated cellsMVEC were cultured in EBM-MV2 Bulletkit culture medium (Clonetics,BioWhittaker, Verviers, Belgium)/ 0.5 µM dibutyryl cAMP (Sigma). After conflu-ence, cells were fixed with 3.5% paraformaldehyde (PFA)/ 0.1% Tween. Stainswere performed with sheep anti-canine von Willebrand Factor (vWF) (Kordia,Leiden, The Netherlands), mouse anti-human α-actin (DAKO, Glostryp,Denmark), mouse anti-human vimentin (DAKO) and for visualization FITC-con-jugated goat anti-mouse antibody (Becton and Dickinson, Bedford, Mass.,USA) or -rabbit anti-sheep antibody (DAKO). Incubations were done for 45 minat 37°C, followed by three wash-steps of 10 min. Cells were visualized withconfocal laser microscope (Leica TCS nt, Leica, Heidelberg, Germany).
Retroviral gene transduction of isolated cellsWe used retroviral gene transduction, gene delivery via a replication deficientretrovirus, to tag cells with a marker gene which is readily detectable.17 Nospecies-specific canine marker was available, therefore we initially employed

40
the widely-used green fluorescent protein (GFP) marker. Because of autofluo-rescence of the prosthesis, GFP fluorescence was difficult to detect and aGFP-specific antibody was used. Cells of another two dogs were transducedwith truncated low affinity nerve growth factor receptor (LNGFR), a humanreceptor. Two days before start of the transduction, producer cells (Phoenix-GFP, titer 1-2x106 or Frapé-1, 1x107 IU/ml) were plated in different concentra-tions.17 After 24h, producer cells with the highest concentration were coveredwith EBM-MV2 Bulletkit culture medium without hydrocortison. The next daythis MVEC-medium was harvested, filtered, and after addition of cAMP andhydrocortison, applied to the MVEC. Transductions were repeated for four andthree successive days in case of GFP- and LNGFR-transduction, respectively.One week after isolation transduced and mock(non)-transduced cells weretrypsinized, washed and resuspended for seeding as mentioned above.Small amounts of cells were withheld to determine the transduction efficiency,defined as the percentage of cells that express the marker gene. LNGFR-transduced cells were stained with mouse anti-human LNGFR (200-3-G6-4(20.4)) (American Type Culture Collection, Manassa, VA, USA)/ PerPE-conju-gated rabbit anti-mouse IgG1 (Southern Biotechnology Association, Allebama,USA). Transduction efficiency was established with a flow cytometer (Calibur,Becton and Dickinson, San José, CA, USA).
Graft preparing and soddingStandard ePTFE grafts (8 cm length, 4 mm diameter, 30 µm fibril length; gen-erous gift from WL Gore & Associates, Flagstaff, Arizona, USA) were used. Onboth ends luerlock connectors were attached. Half an hour before MVEC-sod-ding, the grafts were filled under pressure, one end closed, with soddingmedium to replace trapped air in the interstices of the graft. The cell suspen-sion was introduced into the graft with a lumbar puncture needle, from bottomto top. Subsequently, a syringe filled with sodding medium, four times the vol-ume of the prosthesis, was attached to the luerlock connector. The mediumwas pressed through the graft in about 1 to 2 minutes. Earlier experimentswith a pressure gauge mounted in the system, had shown that so the neces-sary pressure of 5 pounds per square inch (psi) was obtained and main-tained.9

41
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
Graft implantationGraft implantation was performed as described before.8 A 3 to 4 cm piece wasremoved and, to match the retraction, a 5 cm graft was implanted.
Assessment of graft patencyThe patency of the grafts during follow-up was assessed in three ways. ADoppler investigation was done, for the first 9 dogs after 1 and 4 weeks andthen once a month, for the 3 dogs of the transduction experiment weekly.Selective angiography was performed of all dogs with a follow-up of onemonth and of the dog with a follow-up of 12 months, just prior to explantation.In all dogs, an incision was made in the native artery distal to the graft aftermore distal cross-clamping, just before termination.
Graft explantationGraft explantation was performed as described before.8 The grafts were fixedfor histology and scanning electron microscopy (SEM).
Scanning electron microscopySections of the graft were prepared as described before,8 and examined witha scanning electron microscope (Philips, Eindhoven, The Netherlands).
Histopathology and immunohistochemistryParaffin slides were made. Haematoxylin and eosin (HE), elastic von Gieson(EvG) and immunohistochemical stains were performed. For each dog the inti-mal thickness was determined as follows: For every graft, 4 cross sectionswere taken at a distance of 0.3 cm. For every cross section, at a regular dis-tance of 300 µm, the thickness was measured. For every cross section, 32measurements were obtained. The cell density in the hyperplastic intima wasdetermined by counting nuclei in circumscribed areas of the same cross sec-tions (4 measurements/cross section). Measurements were performed with alight microscope equipped with a JAC-CCD camera (Copenhagen, Denmark)coupled to a matrox frame grabber (Matrox Electronic systems Ltd., Quebec,Canada) using Optimas 6.0 software (DVS, Breda, The Netherlands).Immunohistochemical stainings were preceded by endogenous peroxidaseblocking and citrate boiling, or Triton-serum blocking as in the case of GFP-and LNGFR-staining. Endogenous peroxidase blocking was performed with1.5% H2O2 in phosphate-citrate buffer (citric acid mono-hydrate 8.32 g/l,

42
Na2HPO4 21.52 g/l; pH 5.8±0.1) for 15 min. Citrate boiling was done in citratebuffer (Na3citrate dihydrate 2.94 g/l; pH 6.0) for 10 min. Triton-serum blockingwas done with 0.4% Triton X-100/5% horse serum in PBS for 1 hour. As pri-mary antibodies sheep anti-canine vWF, mouse anti-human α-actin, mouseanti-human vimentin, mouse anti-GFP (Clonetech Laboratories, Palo Alto, CA,USA), mouse anti-human LNGFR and mouse anti-human CD3 (DAKO) wereused. Peroxidase/DAB stainings were done with Vectastain Elite ABC Kit andDAB kit for peroxidase staining (Vector Laboratories, Burlingame, CA, USA),according to the manufactures’ recommendations.
Statistical analysisResults are presented as the median (1st-3rd quartile range).
Results
Isolation and identification of microvascular endothelial cellsFrom the falciform ligament 15-40 grams of fat were obtained. The yield ofMVEC was 7 (6.5-8) x105 cells/gram. No growth failures were observed.Immunocytochemical staining of cells cultured on glass coverslips showedbesides vWF-positive cells, some α-actin-positive cells and cells solely positivefor the marker vimentin. The vWF- and vimentin-positive cells were identifiedas EC. The percentage of EC was estimated to be between 50 and 60%,based on immunocytochemistry and morphology. The α-actin- and vimentin-positive cells were identified as myofibroblasts. The cells solely positive forvimentin were identified as fibroblasts, based on their morphology, elongationwith branched shoots without contact inhibition, and the absence of α-actinexpression (fig. 1a-c).
A. Incidence and composition of intimal hyperplasia after onemonth of follow-up
Patency: All of the grafts were palpated and found to be open just prior to clo-sure of the wound. In one dog no doppler signals were found on both sidesafter one week, while in the other five dogs bilateral doppler sounds remainedpresent until the end of the follow-up. Angiography at termination showedbilateral occlusion in the dog without doppler signals. All other grafts were

patent without any signs of stenosis. No angiographic difference existedbetween the MVEC sodded grafts and the controls. Macroscopic examinationat the time of explantation showed that the occluded grafts had a bluish colorrepresentative of thrombus, no pulsations were present. The other grafts hada white color and clear pulsations.
Figure 1Immunocytochemistry of a confluentlayer of first passage canine MVEC.A. Cells positive for the marker againstvWF, and so identified as EC (magnifi-cation, x 340).B. Cells positive for the marker againstα-actin, and so identified as myofibrob-lasts (magnification, x 340).Cells solely positive for the markervimentin, identified as fibroblasts, basedon their morphology (elongated cellswith branched shoots, without contactinhibition) and the absence of α-actinexpression (magnification, x 310).
43
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
44
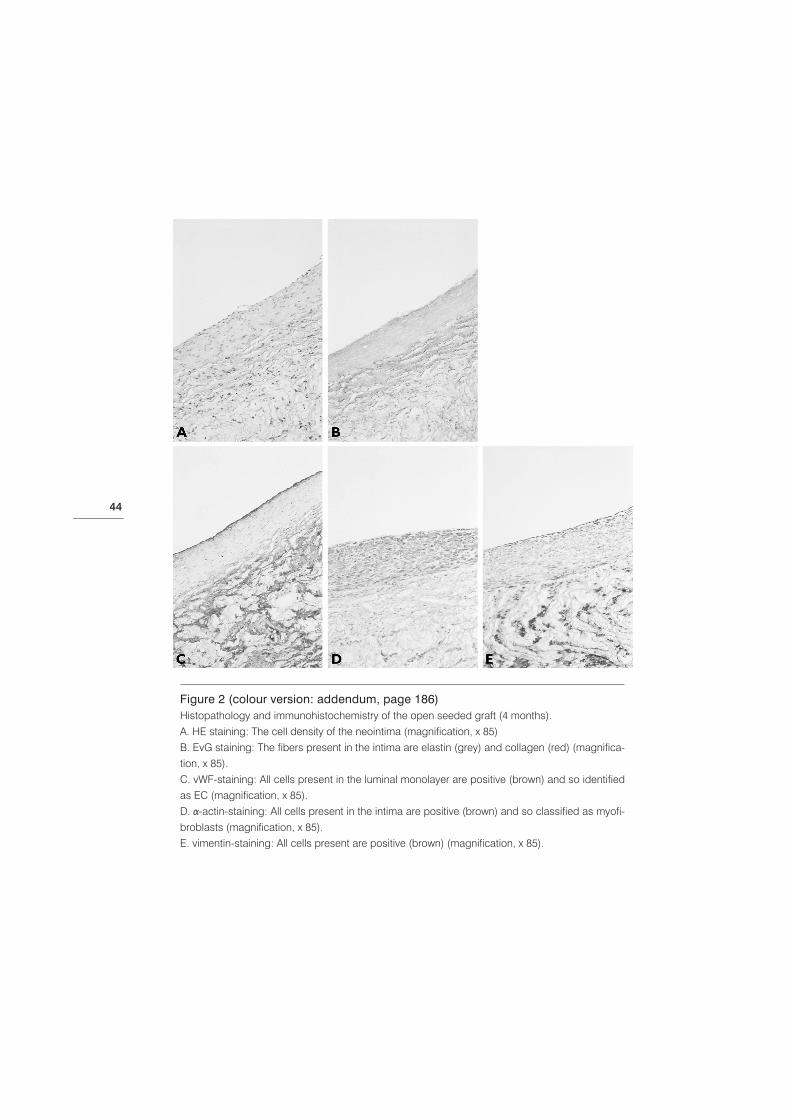
Figure 2 (colour version: addendum, page 186)Histopathology and immunohistochemistry of the open seeded graft (4 months).A. HE staining: The cell density of the neointima (magnification, x 85)B. EvG staining: The fibers present in the intima are elastin (grey) and collagen (red) (magnifica-tion, x 85).C. vWF-staining: All cells present in the luminal monolayer are positive (brown) and so identifiedas EC (magnification, x 85). D. α-actin-staining: All cells present in the intima are positive (brown) and so classified as myofi-broblasts (magnification, x 85). E. vimentin-staining: All cells present are positive (brown) (magnification, x 85).

45
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
Histopathology: All patent seeded grafts were covered with a neointima, con-sisting of an intact cell monolayer, with characteristics of EC, on top of a multi-layer of cells and fibers (fig. 2a). The fibers present in the intima were identifiedas collagen and elastin (fig. 2b). The neointima found in all patent seededgrafts showed a variable thickness in axial as well as transversal direction. Theintimal thickness was 143 (116-152) µm and the cell density 2.9 (2.9-4.1)x103/mm2 (table 1). All patent nonseeded grafts showed a covering consistingof fibrin and platelets. Both occluded grafts, the MVEC sodded and the con-trol, were filled with a thrombus consisting of platelets and fibrin.SEM: The patent seeded grafts were covered with a smooth confluent celllayer with EC-morphology. No fibrin formation was seen, nor signs of plateletaggregates. The occluded grafts and all nonseeded patent grafts showed acti-vation of coagulation (fibrin and platelet deposition). No endothelialization waspresent in the patent nonseeded grafts except for the peri-anastomotic pan-nus.Immunohistochemistry: Cells present in the inner monolayer of the neointi-ma which covered all patent seeded grafts were all vimentin- and vWF-posi-tive, identifying them as EC (fig. 2c,e). Cells present in the multilayer betweenthe monolayer of EC and the prosthesis were all vimentin- and α-actin-positive,classifying them as myofibroblasts (fig. 2d,e).
Table 1
follow up 1 mo 4 mo 8 mo 12 mo
dog number 1 2 3 4 5 6 7 8 9
median n.a. 152 188 116 143 9 21 n.a. 21
thickness (µm)
quartile range n.a. 98-192 154-230 100-140 89-174 5-30 6-93 n.a. 9-47
median cell density n.a. 2.1 4.3 2.9 2.9 4.1 3.6 n.a. 1.7
(x103/mm2)
quartile range n.a. 1.9-2.7 3.5-5.1 2.4-3.1 2.3-3.5 2.6-5.3 2.9-5.1 n.a. 0.6-2.2
Median (1st-3rd quartile range) thicknesses and median (1st-3rd quartile range) intimal cell densitiesof the sodded grafts with 1-12 months follow up. The results of two dogs (1 and 8 months follow up)were not available (n.a.), due to occlusion of the sodded grafts.

46
B. Changes in thickness and composition of the neointimaduring a follow-up of 12 months
Patency: Immediately after implantation, the grafts in the three dogs with afollow-up of 4, 8 and 12 months, respectively, were palpated and found to beopen. At the time of explantation two of the three seeded grafts were patent.All non-seeded ones and the seeded one with a follow-up of 8 months wereoccluded (fig. 3). Doppler investigation showed that the occlusions hadoccurred between 1 and 4 weeks of follow-up. Angiography of the dog with afollow-up of 12 months showed a patent seeded graft without any signs ofstenosis and an occluded nonseeded graft.Histopathology: The patent seeded grafts with a follow-up of 4 and 12months showed an intact cell monolayer, with characteristics of EC, coveringa multilayer of cells and fibers (fig. 2a,b). The intimal thicknesses after 4 and12 months were 21 (6-93) µm and 21 (9-47) µm, and the cell densities were 3.6(2.9-5.1)x103/mm2 and 1.7 (0.6-2.2)x103/mm2, respectively (table 1). No differ-ences were found in identity of fibers between a follow-up of one month andthe longer follow-ups of 4 and 12 months (fig. 2b). Simular to one month of fol-low up, a variable thickness in axial as well as transversal direction was found.All nonseeded grafts and the graft with a follow-up of 8 months were occludedwith an organized thrombus, consisting of connective tissue, cells andmicrovessels.SEM: Again, the patent seeded grafts were covered with a smooth confluentcell layer with EC-morphology, without deposition of fibrin and platelet aggre-gates.Immunohistochemistry: No differences were found in identity of cellsbetween follow-up of one month and the longer follow-ups of 4 and 12 months(fig. 2c-e).
Figure 3Macroscopy just after explantation of thegrafts (left: open graft sodded with MVEC,right: occluded graft sodded withoutMVEC).

47
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
C. Contribution of the seeded cells to the intimal hyperplasiaTransduction efficiency: Transduction efficiency of the GFP-transducedcells was 35% (fig. 4a’), while the transduction efficiency of the LNGFR-trans-duced cells was 80% (75-85%) (fig. 4b’).
Figure 4 (colour version: addendum, page 187)A. Immunohistochemistry of a graft sodded with GFP-transduced cells. The intima is visible withpositive cells (brown) (magnification, x 250). A'. Flow cytometry analysis of GFP-transduced cells. Fluorescence of transduced cells (filled)compared with that of mock-transduced cells (open).B. Immunohistochemistry of a graft sodded with LNGFR-transduced cells. Positive cells (black)are visible in the EC monolayer, the intima and the luminal part of the prosthesis (magnification,x 165). B'. Flow cytometry analysis of LNGFR-transduced cells. Fluorescence of transduced cells (filled)compared with that of mock-transduced cells (open). C. Immunohistochemistry of a graft sodded with transduced cells. A large T-cell infiltrate is pre-sent (brown) (magnification, x 165).

48
Patency: All grafts seeded with marker-transduced cells were similar to allgrafts seeded with mock-transduced cells in that they remained patent, assuggested by Doppler investigation and later proven after explantation by inci-sion in the native artery distal to the graft.Histopathology, SEM and immunohistochemistry: In all dogs, the graftsseeded with transduced cells showed a similar EC-layer with intimal hyperpla-sia underneath as the grafts seeded with mock-transduced cells on the otherside, and as the seeded grafts of both above mentioned experiments withoutlabelled cells.Destination of transduced cells: In all three dogs, marker-positive cellscould be detected in the EC monolayer, multilayer of myofibroblasts and lumi-nal part of the prosthesis (fig. 4a,b). No such marker-positive cells were foundin the prosthesis sodded with mock-transduced cells.Immunoreaction against transduced cells: A distinct T-cell infiltrate waspresent in the neointima covering the graft, sodded with marker-transducedcells, and in the graft itself (fig. 4c), but not in mock-transduced grafts. This T-cell infiltrate was less abundantly present in the graft with a follow-up of 2weeks than in the grafts with a follow-up of 3 weeks. The infiltrate was notpresent in the grafts sodded with mock-transduced cells.
Discussion
Seeding of venous EC has been used to increase the patency of prostheticgrafts. Although the results were satisfactory, the technique did not find gener-al acceptance. The mean reason is that low yield of EC from veins makes cellculture necessary. To avoid problems due to cell culture, alternative cells andsources for EC have been explored. Subcutaneous fat has been introduced asa source of large numberss of MVEC,9-11 being able to form a nonthrombo-genic luminal EC layer in vivo. A fat-derived MVEC seeding related problem,however, is the development of a thickened intima, which can result in occlu-sion of the graft.The intimal hyperplasia found after seeding of MVEC is much more extensivethan after seeding of more pure vein-derived EC, both in humans,18 and inother species.3 An until now unproven suggestion is that the neointima, found

49
cha
pte
r 3
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
after seeding of MVEC, exists of cells seeded on the graft as impurities of thetransplant.5,12
Aim of this study was to investigate specific characteristics of MVEC seeding-associated intimal hyperplasia in terms of incidence, composition, and pro-gression in time, and the contribution of the seeded cells. We found thatMVEC, isolated from the falciform ligament, consisted of a combination of EC,fibroblasts and myofibroblasts. In all patent seeded grafts a confluent EC lin-ing as well as intimal hyperplasia was present. The thickened intima consistedof a multilayer of myofibroblasts, elastin and collagen. Thickness and cell den-sity of the intima did not progress after one month. All patent non-seededgrafts were covered with platelets and fibrin and did not show any intimalhyperplasia. After marking the seeded cells we found that the transplantedcells were present in the EC monolayer, the intima, and the luminal part of theprosthesis.Here we have shown for the first time that contaminants of the transplant con-tribute to MVEC seeding related intimal hyperplasia. Using a fluorescent dye,it has been shown that after 3 weeks of follow up, EC lining prosthetic graftsoriginate from the seeded cells.19 In another study no evidence was found,however, for the hypothesis that intima formation is due to seeded cells.20 Thedifferences compared to our study were that the seeding density was muchlower than the recommended density we used;6,9 that the polyester used wasmore porous and such more easily populated from the surrounding tissue;20
and that venous EC were used which are more pure than MVEC.Retroviral transduction did not affect the results of cell seeding, as could beestablished by using a graft sodded with non-labelled cells as a control.Furthermore the immunosuppression, given to the dogs of the transductionexperiment, did not affect the structure of the EC-layer and intimal hyperplasiapresent on the grafts. No differences existed compared to the EC-layer andintimal hyperplasia present on the seeded grafts of both other experimentswithout immunosuppression.Not all cells present in the EC monolayer, intima and inner third of the prosthe-sis expressed the marker. The transduction efficiency was not 100%, besidesthe transduced cells can be destroyed by cytotoxic T-cells present, despiteimmunosuppression. Furthermore we can not exclude the contribution of cellscoming from both vessel ends or from tissue around the prosthesis. The con-tribution of these endogenous cells is higher, however, when a very porous

50
prosthesis is used than when a less porous prosthesis is used, as we did inour study.20
Although it is possible that the positive myofibroblasts present in the intimaare transdifferentiated MVEC, it is most likely that the positive myofibroblastsare contaminants from the transplant. First, fibroblast-like cells are present inisolates of canine fat-derived MVEC. Second, a neointima forms less exten-sively after the seeding of vein-derived EC, which contain less contaminatingcells.3,4 And third, single cell culture studies have shown that although certaincell types (e.g. interstitial EC from heart valves) can transdifferentiate, humanumbilical cord EC and dermal MVEC cannot.21,22
The myofibroblasts present in the neointima showed other characteristics thanthe impurities present in the transplants, because they stained all positive forα-actin. The expression of myofibroblast-specific characteristics can beinduced by the surroundings, as a time-dependent maturation of myofibrob-lasts present in the neointima has been found.23 Immediately after implanta-tion cells resemble fibroblasts, afterwards they gradually change into smoothmuscle cells with an increased expression of α-actin.12
As mentioned before,24 all thickened intimas showed a variable thickness inaxial as well as transversal cross-section, which might be explained by varia-tions in bloodflow,25 density of graft material, or velocity of the formation of aconfluent EC layer.26,27
From the present study we conclude that contaminants from the transplantcontribute to intimal hyperplasia associated with microvascular endothelial cellseeding. Further purification of fat-derived MVEC should reduce intimal hyper-plasia. Hopefully, this will lead to a smaller degree of stenosis and thrombosisand improve results of MVEC seeded grafts used for bypass and other vascu-lar surgery.
Acknowledgements
We thank:
- The Netherlands Heart Foundation for their financial support (grant 97.165).
- The biotechnicians and animal care takers of the ‘Joint Animal Laboratory’ of the University of Utrecht for
the performance of anaesthesia and assistence during the operations and for the animal care.
- WL Gore & Associates, Flagstaff, Arizona, USA for their generous gift of ePTFE.

1 Herring MB, Compton RS, Gardner AL.
Clinical experience with endothelial seeding
in Indianapolis. In: Zilla R, Fasol R, Deutsch
M, eds. Endothelialization of vascular grafts:
1st European workshop on advanced
technologies in vascular surgery. Vienna:
Karger-Basel, 1987:218-24.
2 Williams SK. Endothelial cell transplantation.
Cell Transplant 1995;4:401-10.
3 Graham LM, Burkel WE, Ford JW et al.
Expanded polytetrafluoroethylene vascular
prostheses seeded with enzymatically
derived and cultured canine endothelial
cells. Surgery 1982;91:550-9.
4 Zilla P, Fasol R, Preiss P et al. In vitro
endothelialization of vascular prostheses.
In: Zilla P, Fasol R, Callow A, eds. Applied
Cardiovascular Biology 1989. Vienna: Basel,
Karger: Int Soc Appl Cardiovasc Biol,
1989:56-72.
5 Zilla P, von Oppell U, Deutsch M. The
endothelium: a key to the future. J Card
Surg 1993;8:32-60.
6 Swedenborg J, Bengtsson L, Clyne N et al.
In vitro endothelialisation of arteriovenous
loop grafts for haemodialysis. Eur J Vasc
Endovasc Surg 1997;13:272-7.
7 Deutsch M, Meinhart J, Fischlein T et al.
Clinical autologous in vitro
endothelialization of infrainguinal ePTFE
grafts in 100 patients: a 9-year experience.
Surgery 1999;126:847-55.
8 Verhagen HJ, Blankensteijn JD, de Groot
PG et al. In vivo experiments with
mesothelial cell seeded ePTFE vascular
grafts. Eur J Vasc Endovasc Surg
1998;15:489-96.
9 Williams SK, Rose DG, Jarrell BE.
Microvascular endothelial cell sodding of
ePTFE vascular grafts: improved patency
and stability of the cellular lining. J Biomed
Mater Res 1994;28:203-12.
10 Hedeman JP, Verhagen HJ, Heijnen-Snyder
GJ et al. Thrombomodulin activity of fat-
derived microvascular endothelial cells
seeded on expanded polytetrafluorethylene.
J Vasc Res 1999;36:91-9.
11 Hedeman JP, Verhagen HJ, Heijnen-Snyder
GJ et al. Thrombogenesis of different cell
types seeded on vascular grafts and
studied under blood-flow conditions. J Vasc
Surg 1998;28:1094-103.
12 Baitella-Eberle G, Groscurth P, Zilla P et al.
Long-term results of tissue development
and cell differentiation on Dacron
prostheses seeded with microvascular cells
in dogs. J Vasc Surg 1993;18:1019-28.
13 Schmidt SP, Meerbaum SO, Anderson JM
et al. Evaluation of expanded
polytetrafluoroethylene arteriovenous
access grafts onto which microvessel-
derived cells were transplanted to “improve”
graft performance: preliminary results. Ann
Vasc Surg 1998;12:405-11.
14 Park PK, Jarrell BE, Williams SK et al.
Thrombus-free, human endothelial surface
in the midregion of a Dacron vascular graft
in the splanchnic venous circuit—
observations after nine months of
implantation. J Vasc Surg 1990;11:468-75.
15 Meerbaum SO, Sharp WV, Schmidt SP.
Lower Extremity Revascularisation with
Polytetrafluoroethylene Grafts Seeded with
Microvascular Endothelial Cells. In: Zilla P,
Fasol R, Callow A, eds. Applied
Cardiovascular Biology 1990-91. Int Soc
Appl Cardiovasc Biol. Basel: Karger,
1992:107-19.
16 Roitt. The recognition of the antigen. In:
Blackwell Scientific Publications Editorial
Offices, ed. Essential Immunology. Oxford:
Marston Book Services Ltd, 1997:1-15.
References
51
Ce
ll se
ed
ing
re
late
d i
nti
ma
l h
ype
rpla
sia
cha
pte
r 3

17 Ng YY, Veenhuizen P, Lokhorst H et al.
Frape-1 and Frape-3: two different
recombinant retroviruses encoding the
same human marker gene. Cancer Gene
Ther 2000;7:624-8.
18 Fischlein T, Zilla P, Meinhart J et al. In vitro
endothelialization of a mesosystemic shunt:
a clinical case report. J Vasc Surg
1994;19:549-54.
19 Williams SK, Kleinert LB, Rose D et al.
Origin of endothelial cells that line
expanded polytetrafluorethylene vascular
grafts sodded with cells from
microvascularized fat. J Vasc Surg
1994;19:594-604.
20 Hollier LH, Fowl RJ, Pennell RC et al. Are
seeded endothelial cells the origin of
neointima on prosthetic vascular grafts? J
Vasc Surg 1986;3:65-73.
21 Petroll WM, Jester JV, Bean JJ et al.
Myofibroblast transformation of cat corneal
endothelium by transforming growth factor-
beta1, -beta2, and -beta3. Invest
Ophthalmol Vis Sci 1998;39:2018-32.
22 Paranya G, Kaushal S, Vineberg S et al.
Semilunar valve endothelial cells
transdifferentiate in vitro to a smooth
muscle phenotype. American Journal of
Pathology 2001;159:1335-43.
23 Patel S, Shi Y, Niculescu R et al.
Characteristics of coronary smooth muscle
cells and adventitial fibroblasts. Circulation
2000;101:524-32.
24 Kleinert LB, Hoying JB, Williams SK. The
neointima formed in endothelial cell sodded
ePTFE vascular grafts results from both
cellular-hyperplasia and extracellular-
hypertrophy. Cell Transplant 1996;5:475-82.
25 Thompson MM, Budd JS, Eady SL et al. The
effect of transluminal endothelial seeding on
myointimal hyperplasia following
angioplasty. Eur J Vasc Surg 1994;8:423-
34.
26 Dardik A, Liu A, Ballermann BJ. Chronic in
vitro shear stress stimulates endothelial cell
retention on prosthetic vascular grafts and
reduces subsequent in vivo neointimal
thickness. J Vasc Surg 1999;29:157-67.
27 Allaire E, Clowes AW. Endothelial cell injury
in cardiovascular surgery: the intimal
hyperplastic response. Ann Thorac Surg
1997;63:582-91.
52