Consensus Conference Panel Report: Crown-Height Space ... · formed first to increase vertically...
9
Consensus Conference Panel Report: Crown-Height Space Guidelines for Implant Dentistry—Part 2 Carl E. Misch, BS, DDS, MDS,* Charles J. Goodacre, DDS, MSD,† Jon M. Finley, BA, DDS,‡ Craig M. Misch, DDS, MDS,§ Mark Marinbach, CDT, Tom Dabrowsky, LDT, RDT,¶ Charles E. English, DDS,# John C. Kois, DMD, MSD,** and Robert J. Cronin, Jr., BS, DDS, MS†† A ccording to the consensus panel, excessive crown height space (CHS) conditions relate to a CHS that is more than 15 mm. An increased CHS of more than 15 mm is primarily a result of the vertical loss of alveolar bone from long-term edentu- lism. Other causes include genetics, trauma, and implant failure. Treatment of excessive CHS before implant placement includes orthodontic and/or surgical methods. Orthodontics in partially edentulous patients is the method of choice because other surgical or prosthetic methods are usually more costly and have higher risks of compli- cations. Several surgical techniques may also be considered, including block on- lay bone grafts, particulate bone grafts with titanium mesh or barrier mem- branes, interpositional bone grafts, and distraction osteogenesis. A staged ap- proach to reconstruction of the jaws is often preferred to simultaneous implant placement, especially when large vol- ume gains are required. Significant ver- tical bone augmentation may even re- quire multiple surgical procedures. Distraction osteogenesis has sev- eral advantages over onlay bone graft- ing techniques for vertical bone growth. Vertical bone gains are not limited by factors such as graft size or expansion of the existing soft tissue volume. There is no donor site morbid- ity, and the surgery may be performed in an office setting. However, distraction requires patient compliance, and bone volume gains are unidirectional. In ad- dition, clinical studies on distraction osteogenesis have found that secondary bone augmentation procedures are often required for dental implant place- ment. 20,21 C.M. Misch has presented a unique approach to plan intentionally a combined use of vertical distraction and horizontal onlay bone grafting to 3 dimensionally reconstruct the defi- ciency. Osseous distraction is per- formed first to increase vertically the ridge and expand the soft tissue vol- ume. Second, an onlay bone graft is used the complete the repair of the defect (Figs. 1– 8). If too much CHS is present, bone augmentation may be preferred to pros- thetic replacement. Surgical augmenta- tion of the residual ridge height will reduce the CHS and improve implant biomechanics. Augmentation will often permit the placement of wider body im- plants with the associated benefit of in- creased surface area. Prosthetics is the most common method to treat excess CHS but should be the last option used. Gingival colored prosthetic materials (pink porcelain or acrylic resin) on fixed restorations or changing the prosthetic design to a removable restoration should often be considered when restoring ex- cessive CHS. In the maxilla, a vertical loss of bone results with the ridge positions also more palatal. As a consequence, implants are often inserted more pal- atal than the natural tooth position. Removable restorations have several advantages under these clinical situ- ations. The removable prosthesis does not require embrasures for hy- giene. The removable restoration may be removed during sleep to de- crease the effects of an increase in *Professor and Director of Oral Implantology, Temple University, School of Dentistry, Philadelphia, PA; CEO of Misch International Implant Institute, Beverly Hills, MI. †Dean of the Loma Linda University School of Dentistry, Loma Linda, CA. ‡Private practice, Prairie Village, KS. §Clinical Associate Professor at New York University, Department of Implant Dentistry, New York, NY; private practice, Sarasota, FL. Assistant Professor Temple University, School of Dentistry, President of Nu-Life Long Island Dental Laboratories, West Hempstead, NY. ¶Owner of BIT Dental Laboratory Pueblo, CO. #Assistant Clinical Professor of Restorative Dentistry of the University of Tennessee, Memphis, TN and University of Oklahoma, Oklahoma City, OK. **Affiliate Professor in the Graduate Restorative Program at the University of Washington; private practice Seattle, WA. ††Director of the Postdoctoral Prosthodontics Program and Professor at the University of Texas Health Science Center, San Antonio, TX. ISSN 1056-6163/06/01502-113 Implant Dentistry Volume 15 • Number 2 Copyright © 2006 by Lippincott Williams & Wilkins DOI: 10.1097/01.id.0000217907.18396.18 The International Congress of Oral Implantologists sponsored a consensus conference on the topic of Crown Height Space on June 26 –27, 2004 in Las Vegas, Nevada. The panel communicated on several oc- casions before, during, and after the meeting, both as a group and among individuals. A consensus of one opinion was not developed for most issues. However, general guidelines emerged related to the topic. The following article is Part 2 of a sum- mary of several of the guidelines that should be of benefit to the profession at large. (Part 1 appeared in Im- plant Dentistry 2005;14:312–321.) (Implant Dent 2006;15:113–121) Key Words: interarch space, crown height, implant treatment plans, im- plant prosthetics IMPLANT DENTISTRY /VOLUME 15, NUMBER 2 2006 113
Transcript of Consensus Conference Panel Report: Crown-Height Space ... · formed first to increase vertically...

Consensus Conference Panel Report:Crown-Height Space Guidelines for Implant
Dentistry—Part 2Carl E. Misch, BS, DDS, MDS,* Charles J. Goodacre, DDS, MSD,† Jon M. Finley, BA, DDS,‡
Craig M. Misch, DDS, MDS,§ Mark Marinbach, CDT,� Tom Dabrowsky, LDT, RDT,¶ Charles E. English, DDS,#John C. Kois, DMD, MSD,** and Robert J. Cronin, Jr., BS, DDS, MS††
According to the consensuspanel, excessive crown heightspace (CHS) conditions relate
to a CHS that is more than 15 mm. Anincreased CHS of more than 15 mm isprimarily a result of the vertical loss ofalveolar bone from long-term edentu-lism. Other causes include genetics,trauma, and implant failure.
Treatment of excessive CHS beforeimplant placement includes orthodonticand/or surgical methods. Orthodonticsin partially edentulous patients is themethod of choice because other surgicalor prosthetic methods are usually morecostly and have higher risks of compli-cations. Several surgical techniques mayalso be considered, including block on-lay bone grafts, particulate bone graftswith titanium mesh or barrier mem-branes, interpositional bone grafts, anddistraction osteogenesis. A staged ap-proach to reconstruction of the jaws isoften preferred to simultaneous implantplacement, especially when large vol-
ume gains are required. Significant ver-tical bone augmentation may even re-quire multiple surgical procedures.
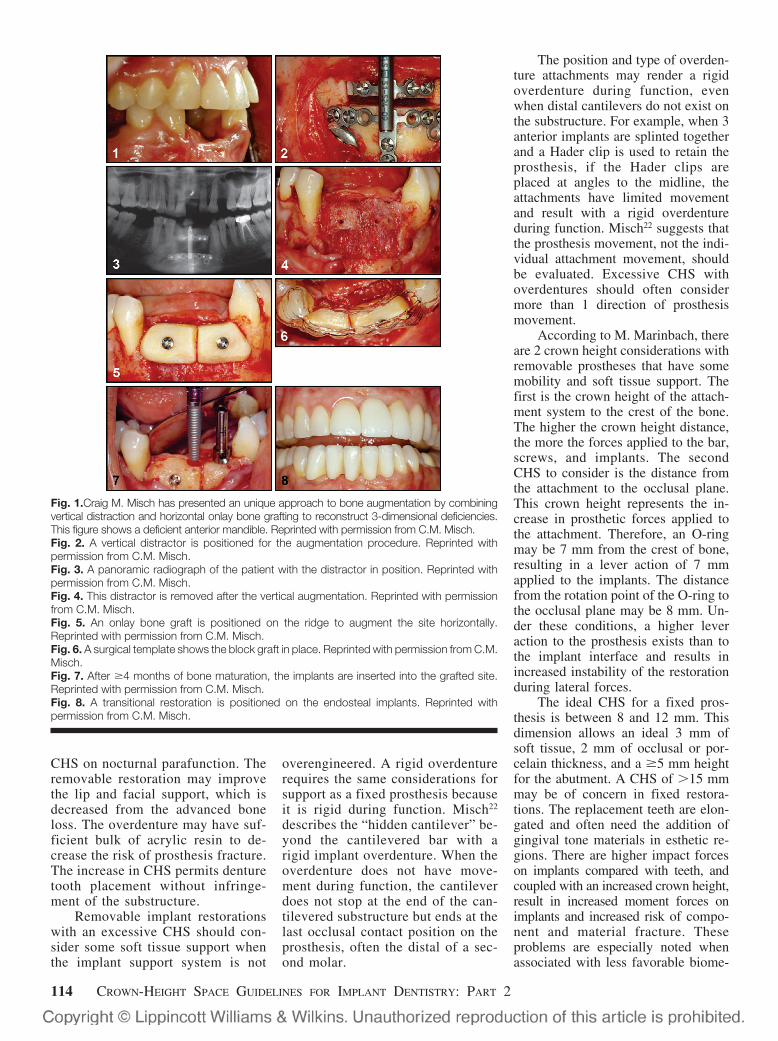
Distraction osteogenesis has sev-eral advantages over onlay bone graft-ing techniques for vertical bonegrowth. Vertical bone gains are notlimited by factors such as graft size orexpansion of the existing soft tissuevolume. There is no donor site morbid-ity, and the surgery may be performed inan office setting. However, distractionrequires patient compliance, and bonevolume gains are unidirectional. In ad-dition, clinical studies on distractionosteogenesis have found that secondarybone augmentation procedures are oftenrequired for dental implant place-ment.20,21 C.M. Misch has presented aunique approach to plan intentionallya combined use of vertical distractionand horizontal onlay bone grafting to 3dimensionally reconstruct the defi-ciency. Osseous distraction is per-formed first to increase vertically theridge and expand the soft tissue vol-ume. Second, an onlay bone graft isused the complete the repair of thedefect (Figs. 1–8).
If too much CHS is present, boneaugmentation may be preferred to pros-thetic replacement. Surgical augmenta-tion of the residual ridge height willreduce the CHS and improve implantbiomechanics. Augmentation will oftenpermit the placement of wider body im-plants with the associated benefit of in-creased surface area. Prosthetics is themost common method to treat excessCHS but should be the last option used.Gingival colored prosthetic materials(pink porcelain or acrylic resin) on fixedrestorations or changing the prostheticdesign to a removable restoration shouldoften be considered when restoring ex-cessive CHS.
In the maxilla, a vertical loss ofbone results with the ridge positionsalso more palatal. As a consequence,implants are often inserted more pal-atal than the natural tooth position.Removable restorations have severaladvantages under these clinical situ-ations. The removable prosthesisdoes not require embrasures for hy-giene. The removable restorationmay be removed during sleep to de-crease the effects of an increase in
*Professor and Director of Oral Implantology, Temple University,School of Dentistry, Philadelphia, PA; CEO of Misch InternationalImplant Institute, Beverly Hills, MI.†Dean of the Loma Linda University School of Dentistry, LomaLinda, CA.‡Private practice, Prairie Village, KS.§Clinical Associate Professor at New York University, Departmentof Implant Dentistry, New York, NY; private practice, Sarasota,FL.�Assistant Professor Temple University, School of Dentistry,President of Nu-Life Long Island Dental Laboratories, WestHempstead, NY.¶Owner of BIT Dental Laboratory Pueblo, CO.#Assistant Clinical Professor of Restorative Dentistry of theUniversity of Tennessee, Memphis, TN and University ofOklahoma, Oklahoma City, OK.**Affiliate Professor in the Graduate Restorative Program at theUniversity of Washington; private practice Seattle, WA.††Director of the Postdoctoral Prosthodontics Program andProfessor at the University of Texas Health Science Center,San Antonio, TX.
ISSN 1056-6163/06/01502-113Implant DentistryVolume 15 • Number 2Copyright © 2006 by Lippincott Williams & Wilkins
DOI: 10.1097/01.id.0000217907.18396.18
The International Congress ofOral Implantologists sponsored aconsensus conference on the topic ofCrown Height Space on June 26–27,2004 in Las Vegas, Nevada. Thepanel communicated on several oc-casions before, during, and after themeeting, both as a group and amongindividuals. A consensus of oneopinion was not developed for mostissues.
However, general guidelinesemerged related to the topic. Thefollowing article is Part 2 of a sum-mary of several of the guidelines thatshould be of benefit to the professionat large. (Part 1 appeared in Im-plant Dentistry 2005;14:312–321.)(Implant Dent 2006;15:113–121)Key Words: interarch space, crownheight, implant treatment plans, im-plant prosthetics
IMPLANT DENTISTRY / VOLUME 15, NUMBER 2 2006 113
CHS on nocturnal parafunction. Theremovable restoration may improvethe lip and facial support, which isdecreased from the advanced boneloss. The overdenture may have suf-ficient bulk of acrylic resin to de-crease the risk of prosthesis fracture.The increase in CHS permits denturetooth placement without infringe-ment of the substructure.
Removable implant restorationswith an excessive CHS should con-sider some soft tissue support whenthe implant support system is not
overengineered. A rigid overdenturerequires the same considerations forsupport as a fixed prosthesis becauseit is rigid during function. Misch22
describes the “hidden cantilever” be-yond the cantilevered bar with arigid implant overdenture. When theoverdenture does not have move-ment during function, the cantileverdoes not stop at the end of the can-tilevered substructure but ends at thelast occlusal contact position on theprosthesis, often the distal of a sec-ond molar.
The position and type of overden-ture attachments may render a rigidoverdenture during function, evenwhen distal cantilevers do not exist onthe substructure. For example, when 3anterior implants are splinted togetherand a Hader clip is used to retain theprosthesis, if the Hader clips areplaced at angles to the midline, theattachments have limited movementand result with a rigid overdentureduring function. Misch22 suggests thatthe prosthesis movement, not the indi-vidual attachment movement, shouldbe evaluated. Excessive CHS withoverdentures should often considermore than 1 direction of prosthesismovement.
According to M. Marinbach, thereare 2 crown height considerations withremovable prostheses that have somemobility and soft tissue support. Thefirst is the crown height of the attach-ment system to the crest of the bone.The higher the crown height distance,the more the forces applied to the bar,screws, and implants. The secondCHS to consider is the distance fromthe attachment to the occlusal plane.This crown height represents the in-crease in prosthetic forces applied tothe attachment. Therefore, an O-ringmay be 7 mm from the crest of bone,resulting in a lever action of 7 mmapplied to the implants. The distancefrom the rotation point of the O-ring tothe occlusal plane may be 8 mm. Un-der these conditions, a higher leveraction to the prosthesis exists than tothe implant interface and results inincreased instability of the restorationduring lateral forces.
The ideal CHS for a fixed pros-thesis is between 8 and 12 mm. Thisdimension allows an ideal 3 mm ofsoft tissue, 2 mm of occlusal or por-celain thickness, and a �5 mm heightfor the abutment. A CHS of �15 mmmay be of concern in fixed restora-tions. The replacement teeth are elon-gated and often need the addition ofgingival tone materials in esthetic re-gions. There are higher impact forceson implants compared with teeth, andcoupled with an increased crown height,result in increased moment forces onimplants and increased risk of compo-nent and material fracture. Theseproblems are especially noted whenassociated with less favorable biome-
Fig. 1.Craig M. Misch has presented an unique approach to bone augmentation by combiningvertical distraction and horizontal onlay bone grafting to reconstruct 3-dimensional deficiencies.This figure shows a deficient anterior mandible. Reprinted with permission from C.M. Misch.Fig. 2. A vertical distractor is positioned for the augmentation procedure. Reprinted withpermission from C.M. Misch.Fig. 3. A panoramic radiograph of the patient with the distractor in position. Reprinted withpermission from C.M. Misch.Fig. 4. This distractor is removed after the vertical augmentation. Reprinted with permissionfrom C.M. Misch.Fig. 5. An onlay bone graft is positioned on the ridge to augment the site horizontally.Reprinted with permission from C.M. Misch.Fig. 6. A surgical template shows the block graft in place. Reprinted with permission from C.M.Misch.Fig. 7. After �4 months of bone maturation, the implants are inserted into the grafted site.Reprinted with permission from C.M. Misch.Fig. 8. A transitional restoration is positioned on the endosteal implants. Reprinted withpermission from C.M. Misch.
114 CROWN-HEIGHT SPACE GUIDELINES FOR IMPLANT DENTISTRY: PART 2

chanics on cantilevered sections offixed restorations.
A CHS of more than 15 mmmeans a large amount of metal mustbe used in the substructure of a tradi-tional fixed restoration to keep porce-lain to its ideal 2-mm thickness. Finetuning techniques for traditional fixedrestorations allowed T. Dabrowsky tomanufacture and monitor a multiplefull-mouth cement retained prosthesiswith a large CHS, delivered in variouscenters across United States. He con-firms that a CHS of more than 15 mmrequires a large amount of metal tosupport properly a uniform porcelainlayer at its ideal 2-mm thickness.
Controlling surface porosities ofmetal substructures after casting astheir different parts cool down atdifferent rates becomes increasingly dif-ficult. Furthermore, when the casting isreinserted into the oven to bake theporcelain, the heat is maintainedwithin the casting at different rates, sothe porcelain cools down in differentregions at different rates.23 If not con-trolled properly, both of these factorsincrease the risk of porcelain fractureafter loading.24 For excessive CHS, con-siderable weight of the prosthesis (ap-proaching 3 oz of alloy) may affectmaxillary trail placement appointmentsbecause the restoration does not remainin place without the use of adhesive.Because noble metals must be used tocontrol alloy’s heat expansion or corro-sion, costs of such implant restorationsare dramatically increased. Proposedmethods to produce hollow frames toalleviate described problems or the useof special custom trays to achieve thepassive fit of similar screw retain porce-lain to metal restorations, double or tri-ple the labor costs.25
An alternative method to fabricatefixed prostheses in interarch situations�15 mm is the fixed complete dentureor hybrid prosthesis, with a smallermetal framework, denture teeth, andacrylic resin to join these elementstogether. The reduced metal frame-work compared to a porcelain to metalfixed prosthesis has less dimensionalchanges and may more accurately fitthe abutments, which is important fora screw-retained restoration. It is lessexpensive to fabricate than a porcelainto metal fixed prosthesis, is highly es-thetic (premade denture teeth), easily
replaces teeth and soft tissue in ap-pearance, and is easier to repair if frac-ture occurs. Because resin acts as anintermediary between the teeth andmetal substructure, the impact forceduring dynamic occlusal loading mayalso be reduced. Therefore, this typeof fixed prosthesis is often indicatedfor implant restoration of a large CHScase. On occasion, undercontoured in-terproximal areas are designed by thelaboratory in restorations of large CHSto assist oral hygiene and have beenreferred to as a “high water” restora-tion. This is an excellent method in themandible, however, it results in foodentrapment, affects air flow patterns,and may contribute to speech prob-lems in the anterior maxilla.
REDUCED CHSLess than ideal space for pros-
thetic replacement of the dentitionmay be caused by several factors, in-cluding skeletal discrepancies (deepbite), a reduced vertical dimension ofocclusion from attrition or abrasion,minimal bone atrophy following toothloss, and supra-eruption of unopposedteeth. Traditional prosthetic and re-storative procedures are indicated torestore the proper occlusal vertical di-mension (OVD) and plane of occlu-sion. However, on occasion, evenwhen the opposing arch is corrected,the CHS may still be inadequate (I�8mm). The 8-mm requirement for CHSconsists of 2-mm occlusal materialspace, 4-mm abutment height, and 2mm above the bone for the biologicwidth dimension.
The OVD may be increased byorthodontics in partially edentulouspatients and is the preferred method.This process may also require a surgi-cal component with orthognathic sur-gery, such as a LeFort I osteotomy andsuperior repositioning. Prosthetics isthe most common method used. How-ever, this procedure often requirestreatment of at least 1 entire arch.
When the opposing teeth are inthe correct position and the CHS isinsufficient, additional space may begained surgically with osteoplasty andsoft tissue reduction of 1 arch, pro-vided adequate bone height remainsafter the procedure for predictable im-plant placement and prosthetic sup-
port (Figs. 9 and 10). If a removableimplant supported prosthesis isplanned, an aggressive alveoloplastyshould often be performed followingtooth extraction to provide adequateprosthetic space. Additional pros-thetic space can be obtained in manyclinical situations by soft tissue re-duction, especially in the maxilla.Soft tissue reduction should be per-formed in conjunction with secondstage surgery if the implants heal ina submerged location. This processallows the thicker tissue to protectthe implants from uncontrolled load-ing by a soft tissue supported pros-thesis during healing. If the implantsheal permucosal, the reduction pro-
Fig. 9. Reduced CHS may be increased dur-ing implant insertion by performing an osteo-plasty before implant insertion. Reprinted withpermission from C.E. Misch.Fig. 10. The implants in position after an os-teoplasty. The CHS is more ideal. Reprintedwith permission from C.E. Misch.Fig. 11. Reduced CHS in a fixed restorationmay use a custom abutment with less taper,larger diameter, and roughened for improvedcement restoration. Reprinted with permis-sion from J. Finley.
IMPLANT DENTISTRY / VOLUME 15, NUMBER 2 2006 115

cedures should be performed duringimplant placement. Soft tissue reduc-tion procedures may include gingivec-tomy, removal of connective tissue, orapically repositioning flaps. Effortsshould be made to maintain adequatekeratinized tissue around the implants.Soft tissue reduction also has the benefitof decreased probing depths around theimplants.
However, the definition of CHS isfrom the bone to the occlusal plane,and, therefore, although the prostheticspace is improved, the CHS remainssimilar when only soft tissue reductionis performed. Too little CHS can befurther complicated when the surgeonplaces the implant above the bone.When the CHS is less than ideal, J.M.Finley states there are several pros-thetic factors to consider:
1. Available space to use2. Taper of abutment3. Surface area of abutment4. Cement type5. Surface finish6. Occlusal topography and material7. Load placed on restoration8. Fit of restoration to abutment9. Retention of prosthesis
10. Implant manufacturer11. Platform to occlusal plane dimension
The consequences of decreasedCHS include a decrease in abutmentheight, which may lead to inade-quate retention of the restoration, inad-equate bulk of restorative material forstrength or esthetics, and poor hygieneconditions compromising long-termmaintenance. In addition, the final res-toration flexes inversely to the cube ofthe thickness of material. A fixed pros-thesis half as thick will flex 8 times asmuch, and will further result in loss ofcement retention, loosening/fracture offixation screws, and/or porcelain frac-ture.26 Inadequate thickness of occlusalporcelain or acrylic, or unsupported oc-clusal material caused by inadequatemetal substructure design may also re-sult in complications, such as compo-nent fracture.
According to J.M. Finley, differ-ent implant companies have differentminimum restorative requirements.Having the occlusal space above theabutment of 1 mm and reducing theabutment height to the top of the re-taining screw may determine the min-
imum restoration space. The smallestminimum restoration space is ob-served with Osseotite� (4.21 mm; 3iImplant Innovations, Inc., Palm BeachGardens, FL), Replace Select� (4.35mm; Nobel BioCare™, Zurich, Swit-zerland), BioHorizons� (4.5 mm; Bio-Horizons Implant Systems, Inc., Bir-mingham, AL), and Frialet� 2 (4.56mm; Essenmed). Astra� (6.6 mm;Astra Tech LTD, Gloucestershire,UK), Lifecore� (6.84 mm; LifecoreBiomedical, Inc., Chaska, MN), andStraumann� (7.05 mm; Straumann,Andover, MA) find the largest resto-ration space requirements.
When a cemented restoration isdesired, the CHS may influence therestoration technique (indirect vs. di-rect). Because additional abutmentheight for retention may be gained bya subgingival margin, the indirecttechnique of making an implant bodylevel impression has considerable ad-vantage. Making direct intraoral im-pressions of the abutments for cementretention that are subgingival morethan 1 mm is often difficult. An im-plant body level impression oftenpermits the subgingival restorationto be placed more than 1 mm sub-gingival because the crown margincan be positioned in the laboratorywith higher accuracy and, therefore,a benefit in a reduced CHS, espe-cially when the soft tissue is severalmillimeters thick. The indirect tech-nique permits custom abutments,which can provide an increased di-ameter and increases the surface areafor retention. A custom abutmentmay also be fabricated to decreasethe total occlusal convergence angleto increase retention for cementedprostheses (Fig. 11).
The retention and resistance dif-ference between a 3 and 5-mm highimplant abutment may be as high as40% for a 4.5-mm diameter abutment.Less than 3 mm of abutment heightindicates a screw retained crown, 3–4mm requires a screw retained or resincemented restoration, and more than 4mm of abutment height allows the op-erator’s preference (Table 1). Splint-ing implants together whether they arescrew retained or cement retained canalso increase retention.
Conditions such as cement hard-ness, surface condition of the abut-
ment, and occlusal material (porcelainvs. metal) are also to be considered inlimited CHS situations. The occlusalmaterial is important to consider inreduced CHS for primarily 2 reasons.When metal is used as the occludingsurface, it is possible to provide higherretention for the prosthesis as a resultof an increase in abutment height. Theabutment height may be higher be-cause the occlusal space requiredabove the abutment is only 1 mm,whereas porcelain requires 2 mm ofocclusal space and acrylic resin �3mm. Another factor is the strength ofthe material. Metal occlusal surfacesprovide the highest resistance to frac-ture and should be considered whenthere is limited CHS. When a screw isused to retain the crown, the strengthof occlusal porcelain is reduced by40%.
Acrylic resin requires the most di-mension for strength and is muchmore likely to fracture when the CHSis limited. This reason is why acrylicresin overdentures require more CHSthan a porcelain-metal fixed prosthe-sis. The surgeon may magnify theprosthetic problem of limited CHS byplacing the implant at an angle to theideal position. Angled abutments losesurface area of retention from theabutment screw hole and further com-promise the limited space conditions.In addition, a 30° taper on an abutmentto correct parallelism loses more than30% of the abutment surface area anddramatically decreases the retentionfor the abutment.
Overdentures have an increasein complications in situations of redu-ced CHS. Removable prostheses havespace limitations related to the pres-ence or absence of a connecting bar,the type and position of attachment(s),and the restorative material (metal vs.resin). According to C.E. English, theminimum CHS for individual attach-
Table 1. Available SpaceRecommendations
● Less than 3 mm abutment height usescrew retention
● More than 3 mm but less than 4 mmabutment height use screw retention orvary cement type to make non-retrievable
● More than 4 mm abutment height canuse retrievable cement
116 CROWN-HEIGHT SPACE GUIDELINES FOR IMPLANT DENTISTRY: PART 2

ments approximates 4.5-mm CHS forLocator�-like attachments (ZimmerDental, Carlsbad, CA), and between12 and 15 mm for a bar and “O” rings(Figs. 12 and 13).27 Hader bars andclips require at least 7-mm CHS. M.Marinbach reports that the ideal CHSfor removable prostheses is �14 mm,and the minimum height is 10.5 mm(Fig. 14 and Table 2). The lowest pos-sible profile of an attachment used foroverdentures in reduced CHS permitsthe component to fit within the con-tours of the restoration, provide morebulk of acrylic resin to decrease frac-ture, and allows for the denture toothto be positioned without hollow gri-nding, which may decrease strengthand/or retention to the resin base.
Overdenture bars may be screw orcement retained. The most commonmethod of retention for a fixed pros-thesis is cement retention (Table 3).The most common method of bar re-tention by almost the same percentagefor overdentures is screw retention(Table 4). Yet, the advantages of ce-ment retention for a fixed prosthesisapply to an overdenture bar (Table 5).Therefore, in minimum CHS situa-
tions, the screw retained bar has aclear advantage, but in ideal to exces-sive CHS situations, the cemented barshould often be considered (Table 6).
SUMMARY
Biomechanical related issues are 1of the most common causes of implantfailure and/or prosthetic complica-tions. Therefore, force magnifiers areimportant considerations. A lever is avery effective agent to increase force.Crown height is a vertical lever and,therefore, is an important element toconsider in implant dentistry.
At the World Meeting of Interna-tional Congress of Oral Implantolo-gists, a consensus of the issues relatedto CHS was not able to be developed.
Fig. 12. An implant overdenture with reducedCHS may use independent implants, whichreduce the space requirements for a con-necting bar. Reprinted with permission fromC. English.Fig. 13. A connecting bar with an implantoverdenture requires a CHS of at least 10.5mm but is easier when �14 mm exist. Re-printed with permission from C. English.Fig. 14. The space above a connecting barmust accommodate a denture tooth, acrylicresin base, and attachment. Reprinted withpermission from M. Marinbach.
Table 2. Space Requirements for Bar-Overdenture
NormalHeight
CompromisedHeight
Thickness of soft tissue (mm) 2.0 2.0Hygiene space under bar (mm) 1.5 0.0Thickness of bar (mm) 4.0 3.0Clip and housing (mm) 1.5 1.5Acrylic denture base (mm) 2.0 1.5Tooth (mm) 3.0 2.5Total height requirement (mm) 14.0 10.5
Table 3. Screw-in Versus Cementable Crowns on Implants
Table 4. Screw-in Versus Cementable Bar Overdentures
Table 5. Advantages of Cemented Bars
● Low or no cost for abutments● Lower laboratory fees● Little need for model verification jigs● Ability to easily adjust fit chair-side● Totally passive frameworks are possible● Passive fit is easy to verify
IMPLANT DENTISTRY / VOLUME 15, NUMBER 2 2006 117

However, guidelines related to CHSemerged. These guidelines included:
Biomechanical Concerns
1. The CHS is measured from the oc-clusal plane to the crest of the bone.
2. Mechanical complications are thehighest cause of complications af-ter the prosthesis is placed.
3. Mechanical complications are of-ten caused by excessive stresses.
4. Excessive stress can cause im-plant failure, crestal bone loss,implant fracture, screw loosening,occlusal material fracture, pros-thesis fracture, and/or attachmentwear and fracture.
5. The crown height is a verticalcantilever.
6. The biomechanics are more unfa-vorable as the CHS increases.
7. An increase in CHS increases theforces on cantilevered and/or an-gled loads.
8. Crestal bone loss around the im-plant increases the CHS and,therefore, increases the momentforces to the implant and prosthe-sis components.
9. CHS does not have a specificideal dimension. With fixed resto-rations, the acceptable range forCHS is between 8 and 12 mm.
10. Removable implant restorationsoften require a CHS of �12 mm,especially when a bar connectsthe individual implants.
11. Stresses applied to implants areconcentrated in the crestal region,so increasing implant length isless effective to reduce the effectsof crown height compared to anatural tooth root.
12. Methods to decrease stress shouldbe considered when the CHS isincreased (i.e., increase implantnumber, size, and surface area ofdesign, splint implants together,shorten cantilevers, consider re-movable restorations, add soft tis-sue support in overdentures).
13. An increase in prosthetic compli-cations occur with either limitedor excessive CHS.
General Statements
1. The OVD is not a specific dimen-sion.
2. The existing OVD may be used asa starting position to evaluate, notnecessarily the end point.
3. When the OVD is modified, bothvertical and horizontal componentsof tooth position, esthetics, andfunction are modified.
4. The OVD should be determinedearly in a treatment plan becauseany modification may require dif-ferent guidelines for implant num-ber, position, and/or angulation.
5. Methods to modify OVD includeorthodontics, surgery, and/or pros-thetics, in that order.
Excessive CHS
1. Excessive CHS in fixed prosthesesincreases mechanical complica-tions.
2. Gingival replacement proceduresshould be evaluated before implantplacement when excessive CHSexists for fixed restorations.
3. Metal and porcelain shrinkage ismore of a problem in traditionalfixed prosthetic cases with exces-sive CHS.
4. Hybrid fixed prostheses of dentureteeth, metal substructure, andacrylic resin are often suggested inexcessive CHS.
5. Overdentures are often indicated incompletely edentulous patientswith excessive CHS.
6. When rigidly attached overdenturesare used in excessive CHS, the im-plant support should be as great asthat used with a fixed prosthesis.
7. When mobile overdentures areused in the presence of an exces-sive CHS, there should be goodsoft tissue support.
8. Overdentures may have 2 differentcomponents of the CHS: the crestdistance from the crest of the boneto the height of the attachment andthe distance from the attachment tothe occlusal plane.
Reduced CHS
1. Structural integrity problems of arestoration increase with a reducedCHS.
2. Surgical procedures during implantplacement may increase a CHS.
3. Complications of an insufficientCHS may be increased by the sur-gical position of the implant (i.e.,poor angulation, leaving the im-plant above the bone several milli-meters).
4. Different implant systems have adifferent minimum CHS related tothe height of the prosthetic compo-nents.
Disclosure
The authors claim to have no fi-nancial interest in any company orany of the products mentioned in thisarticle.
REFERENCES
1. Jensen OT, Cockrell R, Kuhlke L, etal. Anterior maxillary alveolar distractionosteogenesis: A prospective 5-year clinicalstudy. Int J Oral Maxillofac Implants. 2002;17:507-516.
2. Garcia AG, Martin MS, Vila PG, et al.Minor complications arising in alveolar dis-traction osteogenesis. J Oral MaxillofacSurg. 2002;60:496-501.
3. Misch CE. Treatment options formandibular implant overdentures. In:Misch CE, ed. Contemporary Implant Den-tistry. 1st ed. St. Louis, MO: Mosby; 1993:228-229.
4. Bridger DV, Nicholls JI. Distortion ofceramometal fixed partial dentures duringthe firing cycle. J Prosthet Dent. 1981;45:507-514.
5. Bertolotti RL, Moffa JP. Creep rateof porcelain-bonding alloys as a function oftemperature. J Dent Res. 1980;59:2062-2065.
6. Bryant RA, Nicholls JI. Measure-ment of distortion in fixed partial denturesresulting from degassing. J Prosthet Dent.1979;42:515-520.
7. Smyd E. Mechanics of dentalstructures: Guide to teaching dental engi-neering at undergraduate level. J ProsthetDent. 1952;2:668-692.
8. English CE. The mandibular over-denture supported by implants in the ante-rior symphysis: A prescription for implantplacement and bar prosthesis design.Dent Implantol Update. 1993;4:1-4.
Table 6. Cement-Retained Versus Screw-Retained
Cement-RetainedBars
Screw-Retained
Bars WithAbutments
Bars Direct toImplant
Problems with trajectory ofimplants
Big Small Moderate
Parallelism of implants Big Small ModerateLimited space Same Same SamePassive fit Easy Difficult DifficultCost of parts Low Highest HighLaboratory charges for bar Low High HighChair time Least Moderate MostTechnique sensitivity Least Moderate Most
118 CROWN-HEIGHT SPACE GUIDELINES FOR IMPLANT DENTISTRY: PART 2

Reprint requests and correspondence to:Carl E. Misch, DDSSuite 25016231 Fourteen Mile RoadBeverly Hills, MI 48025Phone: (248) 642-3199Fax: (248) 642-3794E-mail: [email protected]
Abstract Translations
GERMANAUTOR(EN): Carl E. Misch, BS, DDS, MDS*, Charles J.Goodacre, DDS, MSD**, Jon M. Finley, BA, DDS***, CraigM. Misch, DDS, MDS#, Mark Marinbach, CDT##, TomDabrowsky, LDT, RDT###, Charles E. English, DDS�, JohnC. Kois, DMD, MSD��, and Robert J. Cronin, Jr., BS,DDS, MS��� *Professor und Leiter der Oralimplantolo-gie, Temple Universitat, zahnmedizinische Fakultat, Phila-delphia, PA, USA. CEO des Misch International ImplantInstitute, Beverly Hills, MI, USA. **Dekan der zahnmediz-inischen Fakultat der Loma Linda Universitat, Loma Linda,CA, USA. ***Privat praktizierender Arzt, Prairie Village,KS, USA. #Klinischer A.O. Professor an der Universitat vonNew York, Abteilung fur Implantierungszahnheilkunde, NewYork, NY, USA.; privat praktizierender Arzt, Sarasota, FL,USA. ##Assistenzprofessor an der Temple Universitat, zahn-medizinische Fakultat, Vorsitzender der Nu-Life Long IslandZahnlaboratorien, West Hempstead, NY 15522. ###Eigen-tumer des BIT Zahnlabors Pueblo, CO, USA. �KlinischerAssistenzprofessor fur wiederherstellende Zahnheilkunde ander Universitat von Tennessee, Memphis, TN, USA und derUniversitat von Oklahoma in Oklahoma City. ��Privatdoz-ent im Wiederherstellungsprogramm fur Graduierte an derUniversitat von Washington; privat praktizierender Arzt inSeattle, WA, USA. ���Leiter des Prothetikprogramms furPostdoktoranden und Professor and der Universitat desMedizinalwissenschaftszentrum von Texas, San Antonio, TX,USA. Schriftverkehr: Carl E. Misch, DDS, 16231 FourteenMile Road, Suite 250, Beverly Hills, MI 48025. Telefon:248-642-3199, Fax: 248-642-3794
Diskussionsbericht der meinungsbildenden Konferenz: derUberkronungshohenspalt und die Richtlinien fur die Im-plantierungszahnheilkunde: Teil II
ZUSAMMENFASSUNG: Die Internationale Kommissionder Oralimplantologen (ICOI) veranstaltete vom 26. bis 27.Juni 2004, in Las Vegas, Nevada, eine meinungsbildendeKonferenz zum Thema des Uberkronungshohenspalts. DerAusschuss außerte sich zu verschiedenen Gelegenheiten vor,wahrend und nach dem Meeting und hier sowohl in derKomplettgruppe wie auch als Einzelpersonen. Zu denmeisten Themen konnte kein einheitlicher Konsens erzielt
werden. Zumindest aber konnten allgemeine Richtlinien inBezug auf das Hauptthema aufgestellt werden. Der nachfol-gende Bericht stellt Teil II einer Zusammenfassung ver-schiedener dieser Richtlinien dar, die fur die Gesamtheit desBerufsstandes von Vorteil sein konnten (Teil I wurde in derImplant Dent 2005;14:312-321, veroffentlicht).
SPANISHAUTOR(ES): Carl E. Misch, BS, DDS, MDS*, Charles J.Goodacre, DDS, MSD**, Jon M. Finley, BA, DDS***, CraigM. Misch, DDS, MDS#, Mark Marinbach, CDT##, TomDabrowsky, LDT, RDT###, Charles E. English, DDS�, JohnC. Kois, DMD, MSD��, y Robert J. Cronin, Jr., BS, DDS,MS��� *Profesor y Director de Implantologıa Oral,Temple University, Facultad de Odontologıa, Filadelfia, PA,EE.UU. Jefe Ejecutivo del Misch International Implant Insti-tute, Beverly Hills, MI, EE.UU. **Decano de la Faculta deOdontologıa de Loma Linda University, Loma Linda, CA,EE.UU. ***Practica Privada, Prairie Village, KS, USA.#Profesor Clınico Asociado de New York University, Depar-tamento de Odontologıa de Implantes, Nueva York, NY,EE.UU. Practica Privada, Sarasota, FL, EE.UU. ##ProfesorAsistente, Temple Univeristy, Facultad de Odontologıa,Presidente de Nu-Life Long Island Dental Laboratories, WestHempstead, NY 15522. ###Dueno del BIT Dental Labora-tory, Pueblo, CO, EE.UU. �Profesor Clınico Asistente deOdontologıa de Restauracion de la Universidad de Tennes-see, Memphis, TN, EE.UU. y de la Universidad de Oklahomaen Oklahoma City. ���Profesor Afiliado del Programa deRestauracion para Graduados de la Universidad de Wash-ington. Practica Privada, Seattle, WA, EE.UU. ���Directordel Programa de Prostodontica Postdoctoral y Profesor delCentro de Ciencias de la Salud de la Universidad de Texas, SanAntonio, TX, USA. Correspondencia a: Carl E. Misch, DDS,16231 Fourteen Mile Road, Suite 250, Beverly Hills, MI 48025.Telefono #: 248-642-3199, Fax #: 248-642-3794
Informe del panel de una conferencia de consenso: Pautaspara el espacio de la altura de la corona para la odontologıade implantes: parte II0
ABSTRACTO: El Congreso Internacional de ImplantologosOrales (ICOI por sus siglas en ingles) patrocino una confer-
IMPLANT DENTISTRY / VOLUME 15, NUMBER 2 2006 119

encia de consenso sobre el tema espacio de la altura de lacorona entre el 26 y 27 de julio del 2004 en Las Vegas,Nevada. El panel se comunico en varias ocasiones antes,durante y despues de la reunion, como grupo y como indi-viduos. El consenso de una sola opinion no se logro en lamayorıa de las cuestiones. Sin embargo, surgieron pautasgenerales relacionadas con el tema. El siguiente trabajo es laParte II de un resumen de varias de las pautas que deberıanser de utilidad para la profesion en general. (La PARTE 1aparecio en Implant Dent 2005;14:312-321)
PORTUGUESEAUTOR(ES): Carl E. Misch, Bacharel em Ciencia,Cirurgiao-Dentista, Mestre em Odontologia*, Charles J. Goo-dacre, Cirurgiao-Dentista, Mestre em Odontologia**, Jon M.Finley, Bacharel em Letras, Cirurgiao Dentista***, Craig M.Misch, Cirurgiao-Dentista, Mestre em Odontologia#, MarkMarinbach, Tecnico Dentario Certificado##, Tom Dab-rowsky, Tecnico Dentario Licenciado, Tecnico Dentario Reg-istrado###, Charles E. English, Cirurgiao-Dentista�, John C.Kois, Doutor em Odontologia, Mestre em Odontologia��, eRobert J. Cronin, Jr., Bacharel em Ciencia, Cirurugiao-Dentista Mestre em Ciencia��� *Professor e Diretor Im-plantologia Oral, Temple University, Faculdade de Odon-tologia, Filadelfia, PA, USA. CEO do InstitutoInternacional de Implantes Misch, Beverly Hills, MI, USA.**Decano da Faculdade de Odontologia da UniversidadeLoma Linda, Loma Linda, CA, USA. ***Clınica Particular,Prairie Village, KS, USA. #Professor Associado Clınico naUniversidade de Nova York University, Departamento de
Odontologia de Implante, New York, NY, USA. ClınicaParticular, Sarasota, FL, USA. ##Professor Assistente daTemple University, Faculdade de Odontologia, Presidentedos Laboratorios Dentarios Nu-Life de Long Island, WestHempstead, NY 15522. ###Proprietario do BIT LaboratorioDentario Pueblo, CO, USA. �Professor Clınico Assistente deOdontologia Restauradora da Universidade de Tennessee,Memphis, TN, USA e Universidade de Oklahoma me Okla-homa City. ��Professor Afiliado no Programa de Pos-Graduacao em Restauracao da Universidade de Washington.Clınica Particular Seattle, WA, USA. ���Diretor Programade Prostodontia em Nıvel de Pos-Doutorado e Professor noCentro de Ciencias da Saude da Universidade do Texas, SanAntonio, TX, USA. Correspondencia para: Carl E. Misch, DDS,16231 Fourteen Mile Road, Suite 250, Beverly Hills, MI 48025Telefone #: 248-642-3199, Fax #: 248-642-3794. 0
Relato de Painel de Conferencia de Consenso: Espaco daAltura da Coroa (CHS) Diretrizes para Odontologia deImplante: Parte II0
RESUMO: O Congresso Internacional de ImplantologistaOrais (ICOI) patrocinou uma conferencia de consenso sobreo topico de Espaco da Altura da Coroa em 26-27 de junho de2004 Las Vegas, Nevada. O painel comunicou-se em diversasocasioes antes, durante e apos a reuniao, tanto como grupoquanto entre indivıduos. Um consenso de uma opiniao nao foidesenvolvido para a maior parte das questoes. Contudo, dire-trizes gerais emergiram em relacao ao topico. O paperseguinte e a Parte II de um resumo de varias das diretrizes quedeveriam ser de benefıcio para a profissao em geral. (PARTE1 apareceu em Implant Dent 2005;14:312-321)
120 CROWN-HEIGHT SPACE GUIDELINES FOR IMPLANT DENTISTRY: PART 2

JAPANESE
IMPLANT DENTISTRY / VOLUME 15, NUMBER 2 2006 121