
Conscious Sedation Slides
68
Conscious Sedation: It Shouldn’t Be a Bad It Shouldn’t Be a Bad Memory! Memory! Ann Willemsen-Dunlap, CRNA, MSN Ann Willemsen-Dunlap, CRNA, MSN
Transcript of Conscious Sedation Slides
Conscious Sedation:
It Shouldn’t Be a Bad Memory!It Shouldn’t Be a Bad Memory!
Ann Willemsen-Dunlap, CRNA, MSNAnn Willemsen-Dunlap, CRNA, MSN

List of Terms Because of the wide range of settings in which this Because of the wide range of settings in which this
presentation will be viewed, a list of generic and presentation will be viewed, a list of generic and proprietary drug names is presented. Please refer to proprietary drug names is presented. Please refer to this slide as necessary throughout the presentation.this slide as necessary throughout the presentation.
Alprazolam = XanaxAlprazolam = Xanax Diazepam = ValiumDiazepam = Valium Flumazinil = RomaziconFlumazinil = Romazicon Lorazepam = AtivanLorazepam = Ativan Methohexital = BrevitalMethohexital = Brevital Midazolam = VersedMidazolam = Versed Naloxone = NarcanNaloxone = Narcan Propofol = DiprivanPropofol = Diprivan Sodium Thiopental = Sodium PentothalSodium Thiopental = Sodium Pentothal
Conscious Sedation-What Is It? Conscious sedation refers to the practice of Conscious sedation refers to the practice of
administering drugs for specific goals:administering drugs for specific goals: Provision of safe analgesia, anxiolysis, sedation, Provision of safe analgesia, anxiolysis, sedation,
and amnesia during stressful procedures.and amnesia during stressful procedures. Safely decreasing adverse psychological responses Safely decreasing adverse psychological responses
associated with stressful procedures.associated with stressful procedures. The return of patients to their pre-procedural level The return of patients to their pre-procedural level
of functioning.of functioning. Information to follow on when standards of Information to follow on when standards of
conscious sedation apply to your patient.conscious sedation apply to your patient.

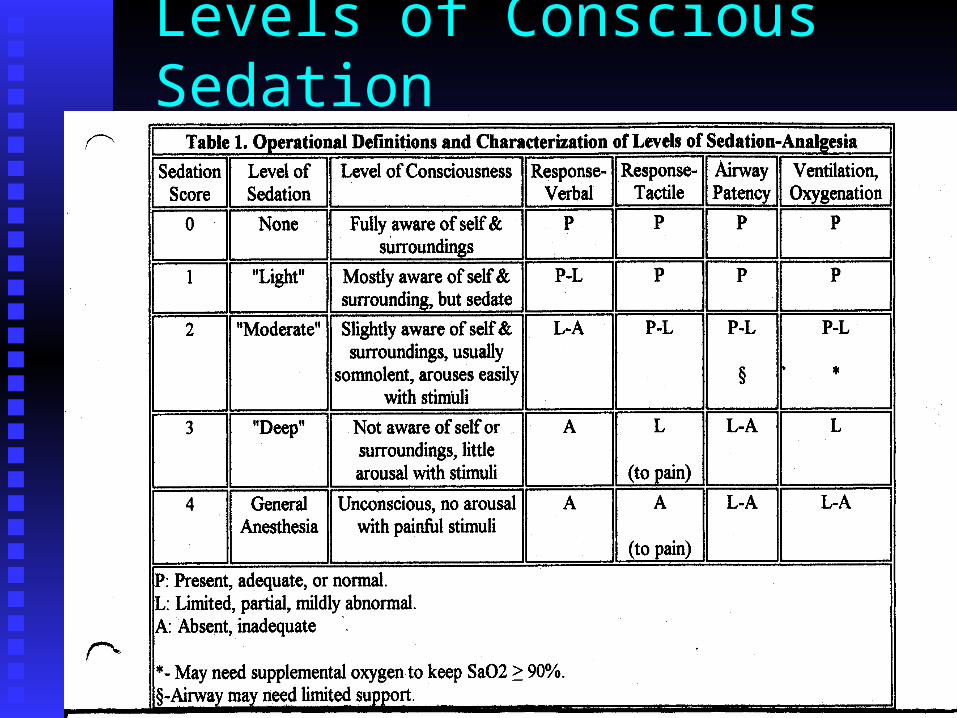
Levels of Conscious Sedation Sedation Score 0 = Fully awakeSedation Score 0 = Fully awake Sedation Score 1 = Light sedation, largely aware of Sedation Score 1 = Light sedation, largely aware of
self/surroundings. Mildly sleepy.self/surroundings. Mildly sleepy. Sedation Score 2 = Moderate sedation, slightly Sedation Score 2 = Moderate sedation, slightly
aware of self/surroundings; somnolent but easily aware of self/surroundings; somnolent but easily aroused with stimulation.aroused with stimulation.
Sedation Score 3 = Deeply sedated; unaware of Sedation Score 3 = Deeply sedated; unaware of self/surroundings. self/surroundings.
Sedation Score 4 = General anesthesia; patient is Sedation Score 4 = General anesthesia; patient is unconscious.unconscious.
Levels of Conscious Sedation
Other Sedation Correlates Sedation Level 0 = Patient unimpaired. Sedation Level 0 = Patient unimpaired. Sedation Level 1 = Slightly decreased level of Sedation Level 1 = Slightly decreased level of
consciousness and verbal response; no other impairments.consciousness and verbal response; no other impairments. Sedation Level 2 = Altered level of consciousness; patient Sedation Level 2 = Altered level of consciousness; patient
maintains patent airway and hemodynamic performance.maintains patent airway and hemodynamic performance. Sedation Level 3 = Poorly responsive patient with Sedation Level 3 = Poorly responsive patient with
decreased airway patency and respiratory drive; at risk for decreased airway patency and respiratory drive; at risk for compromised cardiovascular performance.compromised cardiovascular performance.
Sedation Level 4 = Little or no response to painful stimuli; Sedation Level 4 = Little or no response to painful stimuli; absolute airway compromise; possible impaired absolute airway compromise; possible impaired hemodynamics. hemodynamics.
Patient Assessment Prior To Conscious Sedation The physician, dentist, or independent practitioner The physician, dentist, or independent practitioner
responsible for overall conduct of the conscious responsible for overall conduct of the conscious sedation is generally required to do the following sedation is generally required to do the following within 30 days prior to procedural sedation:within 30 days prior to procedural sedation: perform a history and physical examperform a history and physical exam assign an American Society of Anesthesiologist assign an American Society of Anesthesiologist
(ASA) health class(ASA) health class document a sedation plandocument a sedation plan document NPO status and interval changes if document NPO status and interval changes if
H&P not done immediately prior to procedure.H&P not done immediately prior to procedure.
Focused History and Exam
History should focus on factors that may History should focus on factors that may increaseincrease patient sensitivity to sedatives/analgesicspatient sensitivity to sedatives/analgesics patient risk of patient risk of
respiratory/cardiopulmonary respiratory/cardiopulmonary complicationscomplications
difficulty in managing complications difficulty in managing complications

Focused History, con’t CardiopulmonaryCardiopulmonary diseasedisease may accentuate may accentuate
hemodynamic/respiratory depression caused by hemodynamic/respiratory depression caused by sedatives and analgesics. May require decreased sedatives and analgesics. May require decreased drug dosages; EKG monitoring warranted.drug dosages; EKG monitoring warranted.
Hepatic or renal abnormalitiesHepatic or renal abnormalities may impair drug may impair drug metabolism, causing altered sensitivity and duration metabolism, causing altered sensitivity and duration of action when sedatives/analgesics are administered.of action when sedatives/analgesics are administered.
Medication interactionsMedication interactions between a patient’s routine between a patient’s routine medications & sedatives/analgesics may alter normal medications & sedatives/analgesics may alter normal drug responses.drug responses.

Focused History, con’t Patient allergiesPatient allergies must be known and documented. must be known and documented. Alcohol/illicit substance abuseAlcohol/illicit substance abuse may increase may increase
tolerance to sedatives/analgesics while acute use tolerance to sedatives/analgesics while acute use prior to conscious sedation will be additive or prior to conscious sedation will be additive or synergistic with medication effects.synergistic with medication effects.
Tobacco useTobacco use increases airway irritability and risk increases airway irritability and risk of bronchospasm during sedation.of bronchospasm during sedation.
Prior adverse reactionPrior adverse reaction to anesthesia/sedation to anesthesia/sedation may increase risk during subsequent procedures.may increase risk during subsequent procedures.

Focused Airway Assessment The patient undergoing conscious sedation should The patient undergoing conscious sedation should
have a thorough airway assessment focusing onhave a thorough airway assessment focusing on airway classairway class mouth openingmouth opening thyromental distance (distance from chin to thyromental distance (distance from chin to
thyroid)thyroid) range of motion of the neckrange of motion of the neck
For more information: For more information: http://www.vh.org/Providers/ClinGuide/ProceduralSedation/AirwayAssessment.html

Focused Airway Assessment This picture represents This picture represents
a Mallampati Class a Mallampati Class One airway. The entire One airway. The entire uvula and tonsillar uvula and tonsillar pillars are seen. This pillars are seen. This individual should be individual should be easy to mask ventilate easy to mask ventilate or to intubate with a or to intubate with a laryngoscope and laryngoscope and endotracheal tube.endotracheal tube.
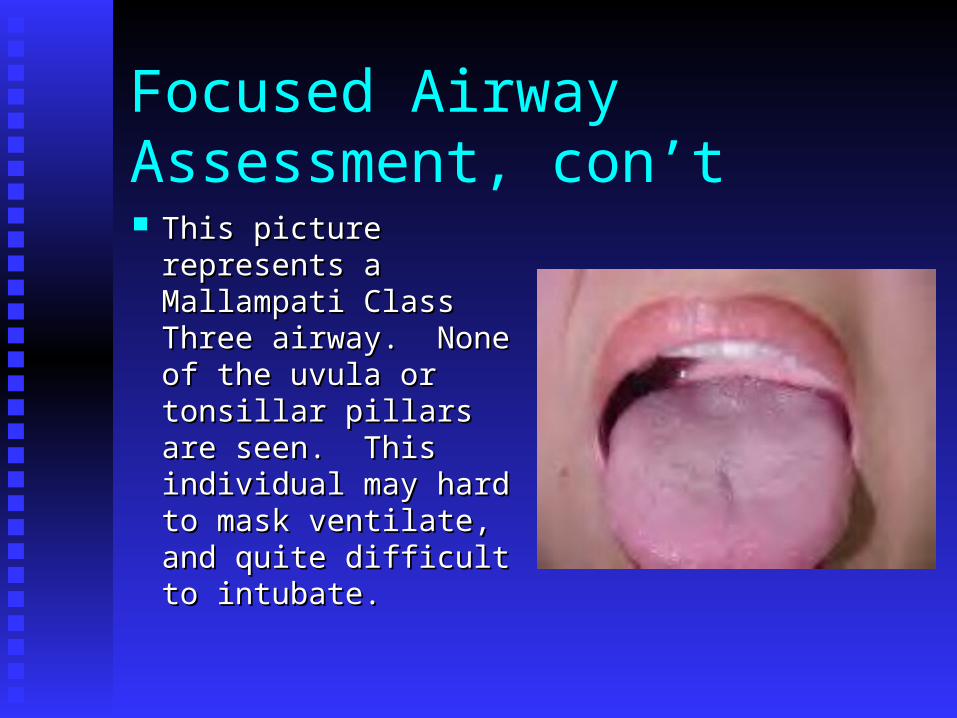
Focused Airway Assessment, con’t This picture represents This picture represents
a Mallampati Class a Mallampati Class Three airway. None Three airway. None of the uvula or of the uvula or tonsillar pillars are tonsillar pillars are seen. This individual seen. This individual may hard to mask may hard to mask ventilate, and quite ventilate, and quite difficult to intubate.difficult to intubate.
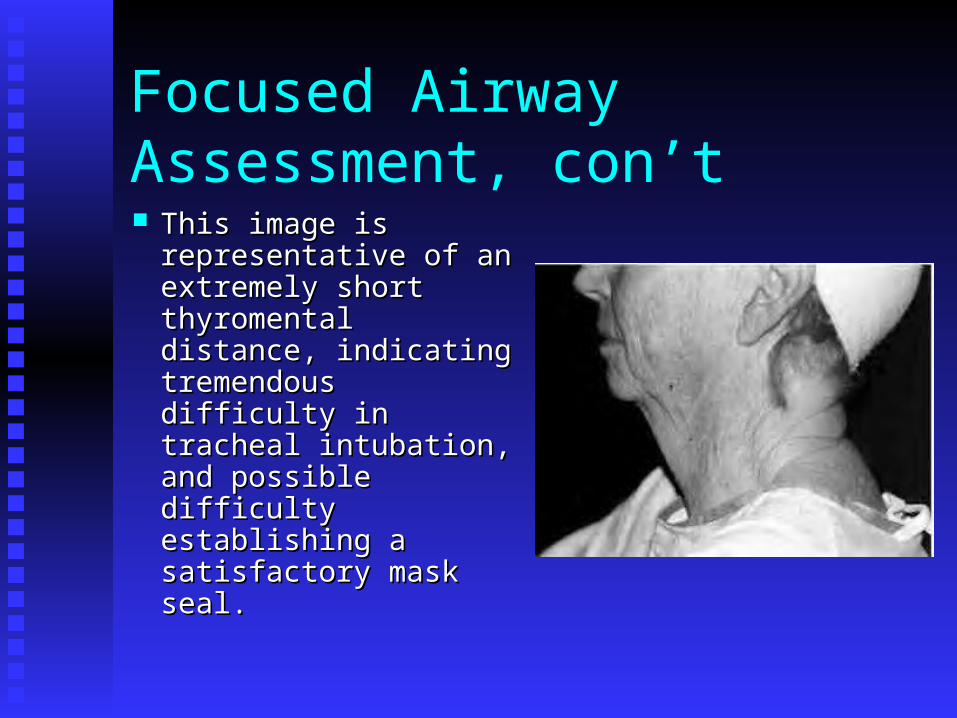
Focused Airway Assessment, con’t This image is This image is
representative of an representative of an extremely short extremely short thyromental distance, thyromental distance, indicating tremendous indicating tremendous difficulty in tracheal difficulty in tracheal intubation, and intubation, and possible difficulty possible difficulty establishing a establishing a satisfactory mask seal.satisfactory mask seal.
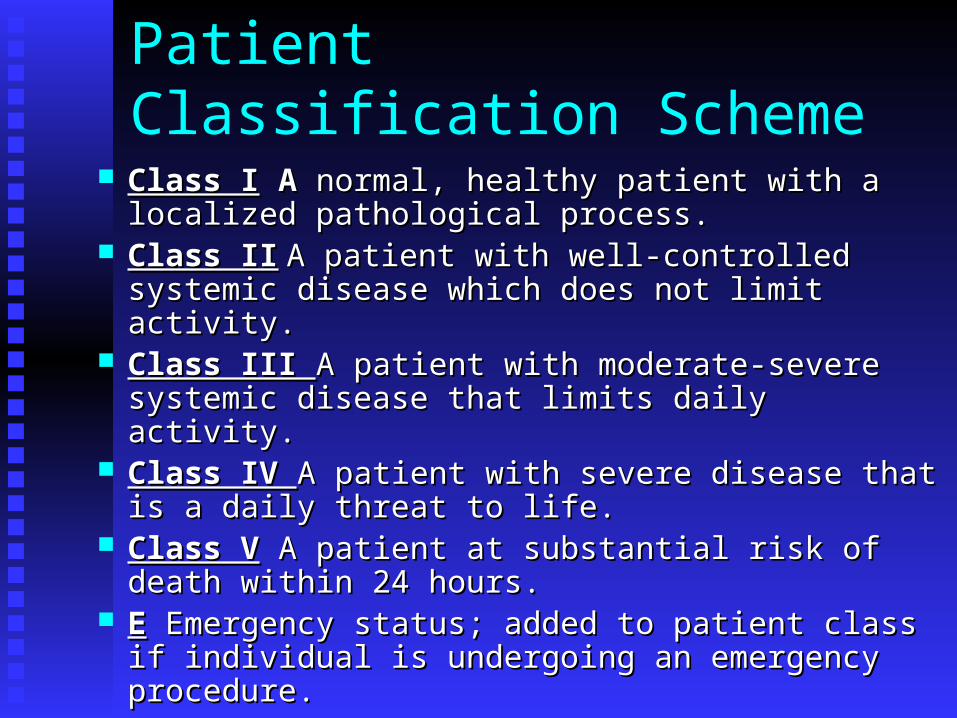
Patient Classification Scheme Class IClass I A A normal, healthy patient with a localized normal, healthy patient with a localized
pathological process.pathological process. Class IIClass II A patient with well-controlled systemic A patient with well-controlled systemic
disease which does not limit activity.disease which does not limit activity. Class III Class III A patient with moderate-severe systemic A patient with moderate-severe systemic
disease that limits daily activity.disease that limits daily activity. Class IV Class IV A patient with severe disease that is a daily A patient with severe disease that is a daily
threat to life.threat to life. Class VClass V A patient at substantial risk of death within A patient at substantial risk of death within
24 hours.24 hours. EE Emergency status; added to patient class if Emergency status; added to patient class if
individual is undergoing an emergency procedure.individual is undergoing an emergency procedure.
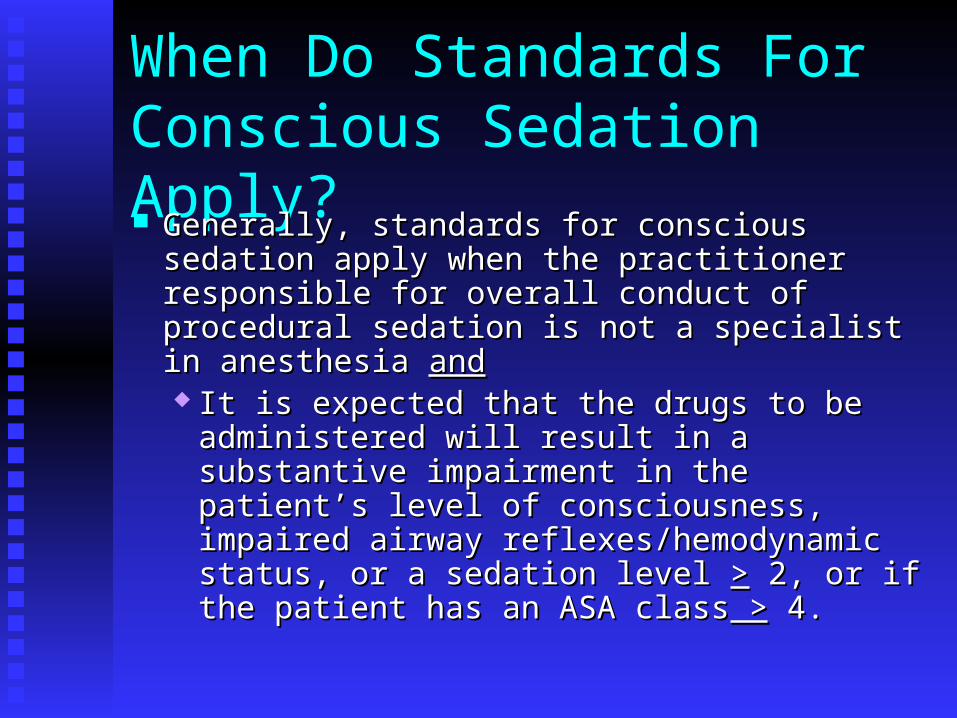
When Do Standards For Conscious Sedation Apply? Generally, standards for conscious sedation apply Generally, standards for conscious sedation apply
when the practitioner responsible for overall when the practitioner responsible for overall conduct of procedural sedation is not a specialist conduct of procedural sedation is not a specialist in anesthesia in anesthesia andand It is expected that the drugs to be administered It is expected that the drugs to be administered
will result in a substantive impairment in the will result in a substantive impairment in the patient’s level of consciousness, impaired patient’s level of consciousness, impaired airway reflexes/hemodynamic status, or a airway reflexes/hemodynamic status, or a sedation level sedation level >> 2, or if the patient has an ASA 2, or if the patient has an ASA classclass > > 4. 4.

Key Points In Patient and Family Education Education, individually geared to the patient and family, Education, individually geared to the patient and family,
helps alleviate concerns associated with conscious sedation. helps alleviate concerns associated with conscious sedation. Key points Key points
duration of sedation (children may fear never waking up)duration of sedation (children may fear never waking up) interindividual variability of response to drugsinterindividual variability of response to drugs potential for sedation failurepotential for sedation failure alternatives to sedationalternatives to sedation potential for adverse eventspotential for adverse events plan for monitoring by a nurse during the procedure and plan for monitoring by a nurse during the procedure and
discharge criteria.discharge criteria.
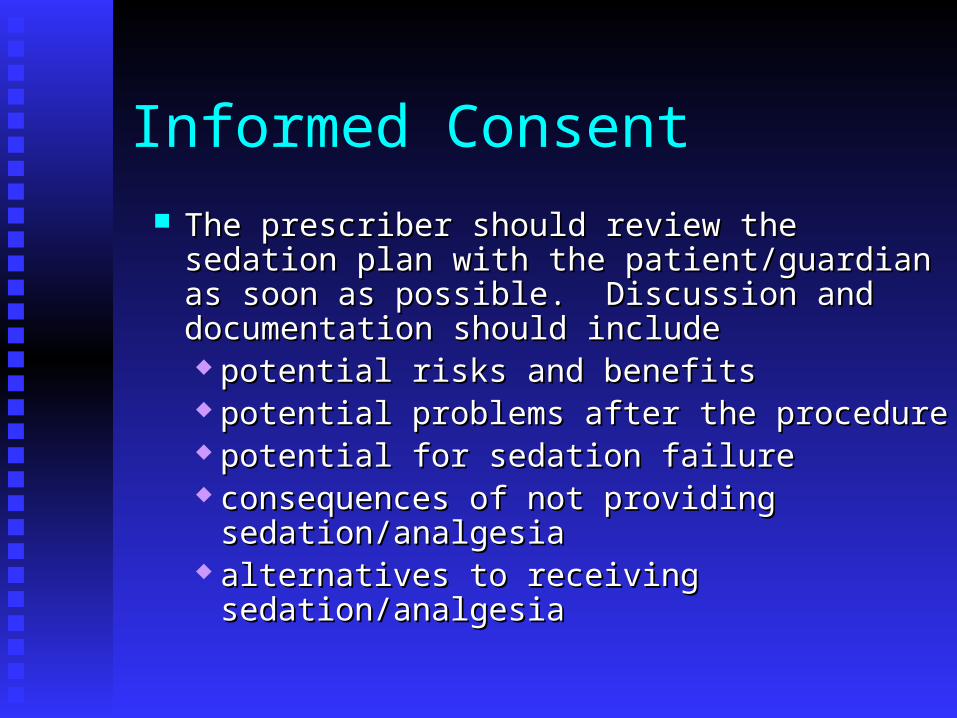
Informed Consent The prescriber should review the sedation plan The prescriber should review the sedation plan
with the patient/guardian as soon as possible. with the patient/guardian as soon as possible. Discussion and documentation should includeDiscussion and documentation should include potential risks and benefitspotential risks and benefits potential problems after the procedurepotential problems after the procedure potential for sedation failurepotential for sedation failure consequences of not providing consequences of not providing
sedation/analgesiasedation/analgesia alternatives to receiving sedation/analgesiaalternatives to receiving sedation/analgesia
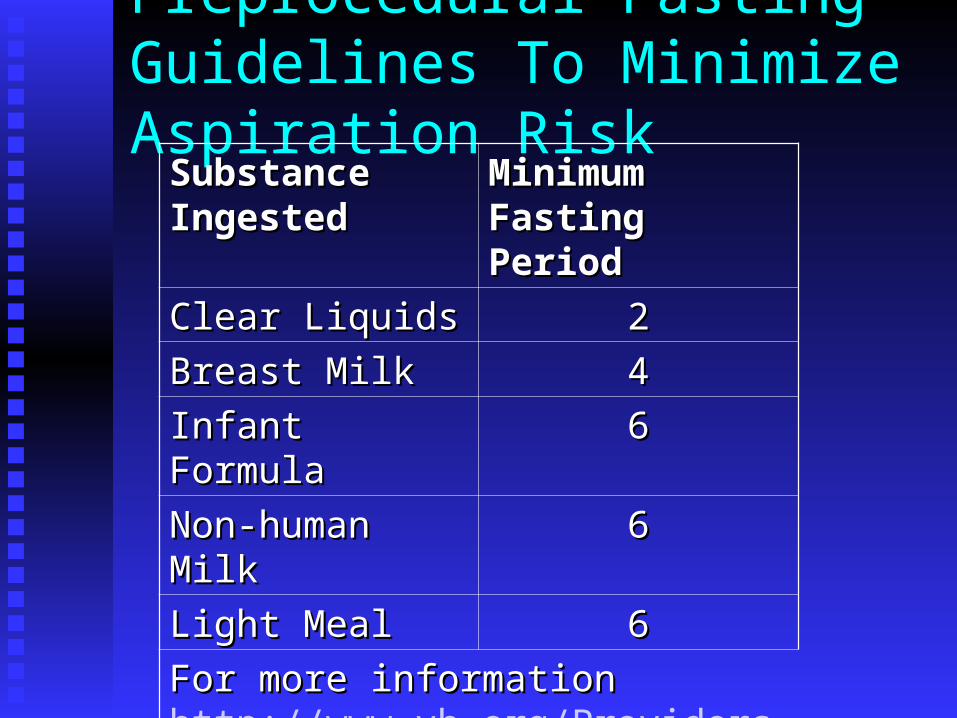
Preprocedural Fasting Guidelines To Minimize Aspiration Risk
Substance Substance IngestedIngested
Minimum Fasting Minimum Fasting PeriodPeriod
Clear LiquidsClear Liquids 22Breast MilkBreast Milk 44Infant FormulaInfant Formula 66Non-human MilkNon-human Milk 66Light MealLight Meal 66For more information For more information http://www.vh.org/Providers/ClinGuide/ProceduralSedation/FastingGuidelines.html
Pharmacology For Conscious Sedation A variety of agents can be used to provide A variety of agents can be used to provide
sedation and analgesia.sedation and analgesia. Opioids are primarily used when analgesia Opioids are primarily used when analgesia
is required for painful procedures.is required for painful procedures. Benzodiazepines and other sedatives are Benzodiazepines and other sedatives are
used to produce sedation, anxiolysis, and used to produce sedation, anxiolysis, and amnesia. Sedative drugs do not provide amnesia. Sedative drugs do not provide analgesia.analgesia.

Pharmacology: Points To Ponder
Drugs administered for conscious sedation should Drugs administered for conscious sedation should allow a patient to be calm, comfortable and allow a patient to be calm, comfortable and cooperative.cooperative.
Clinical endpoints for conscious sedation may Clinical endpoints for conscious sedation may include a respiratory rate of 10-12 in an adult and a include a respiratory rate of 10-12 in an adult and a slurring of speech.slurring of speech.
A drug should be allowed to exert its full effect A drug should be allowed to exert its full effect before administering additional doses or another before administering additional doses or another drug.drug.
When combining opioids and sedatives, administer When combining opioids and sedatives, administer the opioid first to ensure the patient receives the opioid first to ensure the patient receives analgesia prior to painful stimulation.analgesia prior to painful stimulation.

More Points To Ponder
Patients who receive Patients who receive sedatives may become sedatives may become disinhibited and, at disinhibited and, at times, uncooperative.times, uncooperative.

Another Point To Ponder All medications have All medications have
the potential to cause the potential to cause unplanned deep unplanned deep sedation. When that sedation. When that happens providers happens providers may find themselves may find themselves up to their bottom up to their bottom ends in alligators!ends in alligators!

Opioids The opioids provide analgesia and The opioids provide analgesia and
some sedation, as well as alterations some sedation, as well as alterations of mood and perception of of mood and perception of surroundings. They may also surroundings. They may also depress cough reflexes.depress cough reflexes.
Examples includeExamples include morphinemorphine hydromorphone hydromorphone meperidinemeperidine fentanyl depicted at rightfentanyl depicted at right
Some opioids like meperidine and Some opioids like meperidine and fentanyl are synthetic substances, fentanyl are synthetic substances, while others are natural.while others are natural.
Opioids, con’t Opioids exert their agonist actions at opioid Opioids exert their agonist actions at opioid
receptors concentrated in the CNS.receptors concentrated in the CNS. Opioids are highly lipid-soluble and are therefore Opioids are highly lipid-soluble and are therefore
rapidly and extensively distributed to tissues.rapidly and extensively distributed to tissues. Opioids tend to accumulate in reservoirs of fat, Opioids tend to accumulate in reservoirs of fat,
potentially producing long-lasting effects. potentially producing long-lasting effects. Opioids are metabolized in the liver, but some Opioids are metabolized in the liver, but some
active metabolites are excreted via the kidneys.active metabolites are excreted via the kidneys.
Opioids, con’t
Opioids exhibit some adverse effects Opioids exhibit some adverse effects includingincluding decreased respiratory drive/apneadecreased respiratory drive/apnea potential increased PCOpotential increased PCO22/decreased PO/decreased PO22
altered hemodynamicsaltered hemodynamics and bradycardiaand bradycardia GI upset & itchingGI upset & itching
True allergic reactions are fairly rare.True allergic reactions are fairly rare.

Opioids: Special Considerations Elderly patientsElderly patients are often more sensitive to are often more sensitive to
the effects of opioids because of decreased the effects of opioids because of decreased hepatic or renal function and increased depots hepatic or renal function and increased depots of fat-soluble drugs. Consider reduced doses.of fat-soluble drugs. Consider reduced doses.
Pediatric patientsPediatric patients, particularly those under 6 , particularly those under 6 month, exhibit increased sensitivity to opioids month, exhibit increased sensitivity to opioids because of immature blood-brain barrier and because of immature blood-brain barrier and renal function.renal function.
MeperidineMeperidine should not be administered to should not be administered to patients who have taken MAO inhibitors patients who have taken MAO inhibitors within the past two weeks. Meperidine+MAO within the past two weeks. Meperidine+MAO inhibitors=Seizuresinhibitors=Seizures
Opioids: Relative Potency
A standard way of evaluating opioid potency is A standard way of evaluating opioid potency is to compare equianalgesic doses of a drug with to compare equianalgesic doses of a drug with morphine.morphine. Morphine is 10x more potent than Morphine is 10x more potent than
meperidne.meperidne. Morphine is 10x less potent than Morphine is 10x less potent than
hydromorphone.hydromorphone. Morphine is 100x less potent than fentanyl.Morphine is 100x less potent than fentanyl.

Two Specific Opioids FentanylFentanyl may cause chest wall and glottic may cause chest wall and glottic
rigidity, particularly when administered rapidly. rigidity, particularly when administered rapidly. This may make manual ventilation very difficult.This may make manual ventilation very difficult.
MeperidineMeperidine should be used cautiously in patients should be used cautiously in patients with renal/hepatic disease, those at risk for seizure with renal/hepatic disease, those at risk for seizure due to accumulation of its active metabolite, due to accumulation of its active metabolite, normeperidine, and in those with little cardiac normeperidine, and in those with little cardiac reserve.reserve.
For more information: For more information: http://www.vh.org/Providers/ClinGuide/ProceduralSedation/Opioids.html
Benzodiazepines (BZD) This class of drugs This class of drugs
provides sedation, provides sedation, amnesia, anxiolysis, and amnesia, anxiolysis, and even anticonvulsant even anticonvulsant properties by occupying properties by occupying the GABA receptor in the the GABA receptor in the brain. GABA is the major brain. GABA is the major inhibitory inhibitory neurotransmitter in the neurotransmitter in the CNS.CNS.
Benzodiazepines include Benzodiazepines include the drugs midazolam, the drugs midazolam, diazepam, lorazepam, and diazepam, lorazepam, and alprazolam.alprazolam.

Benzodiazepines, con’t Lipid solubility of BZDs determines onset & Lipid solubility of BZDs determines onset &
duration of a single bolus dose. duration of a single bolus dose. Duration of action of BZDs is also related to Duration of action of BZDs is also related to
blood level.blood level. The short duration of a single, small dose The short duration of a single, small dose
of BZD is due to rapid redistribution out of of BZD is due to rapid redistribution out of the CNS, while repeated doses of these the CNS, while repeated doses of these drugs prolongs their duration of action.drugs prolongs their duration of action.
Benzodiazepines: Adverse Effects & Special Considerations BZDs may cause dose-related respiratory BZDs may cause dose-related respiratory
depression, hypotension, and tachycardia, depression, hypotension, and tachycardia, particularly in the elderly.particularly in the elderly.
Midazolam administered rapidly is particularly Midazolam administered rapidly is particularly likely to produce apnea.likely to produce apnea.
BZDs are generally contraindicated in pregnancy.BZDs are generally contraindicated in pregnancy. Diazepam and lorazepam may cause Diazepam and lorazepam may cause
thrombophlebitis.thrombophlebitis.

Benzodiazepines: Relative Potency
Midazolam is 3-4x more Midazolam is 3-4x more potent than diazepam.potent than diazepam. 10 mg diazepam=2.5-10 mg diazepam=2.5-
3mg midazolam.3mg midazolam. Lorazepam is 5x more Lorazepam is 5x more
potent than diazepam.potent than diazepam. 10 mg diazepam=2mg 10 mg diazepam=2mg
lorazepam.lorazepam. At right is a crystalline At right is a crystalline
pictograph of midazolam.pictograph of midazolam.
Barbiturates Barbiturates enhances Barbiturates enhances
GABA effects within GABA effects within the central nervous the central nervous system, depress system, depress sensory cortex, and sensory cortex, and alter cerebellar alter cerebellar function.function.

Barbiturates Barbituates include Barbituates include
sodium pentothal and sodium pentothal and methohexital. methohexital.
Barbiturates provide Barbiturates provide sedation but no sedation but no analgesia.analgesia.
Barbiturates, con’t
Adverse effectsAdverse effects Respiratory depression/apneaRespiratory depression/apnea Laryngospasm, bronchospasmLaryngospasm, bronchospasm Tachycardia and hypotensionTachycardia and hypotension CNS depression OR excitationCNS depression OR excitation Twitching & myoclonus, often mistaken Twitching & myoclonus, often mistaken
for seizuresfor seizures

Barbiturates CautionsCautions
Frequently produces deep sedation; should Frequently produces deep sedation; should be used only by those with hospital be used only by those with hospital privileges in deep sedation.privileges in deep sedation.
Use cautiously in those with heaptic/renal Use cautiously in those with heaptic/renal disease, congestive heart failure, or disease, congestive heart failure, or hypovolemiahypovolemia
Contraindicated in patients with porphyia.Contraindicated in patients with porphyia. Very alkaline; causes tissues damage if Very alkaline; causes tissues damage if
extravastion occurs.extravastion occurs. Methohexital may induce seizures; not used Methohexital may induce seizures; not used
in those with seizure disorder.in those with seizure disorder.
Chloral Hydrate Drug’s mechanism of action is unknown.Drug’s mechanism of action is unknown. Primary effects are due to the active Primary effects are due to the active
metabolite, trichlorethanol.metabolite, trichlorethanol. Metabolized by the liverMetabolized by the liver Degree of CNS depression is related to dose Degree of CNS depression is related to dose
and frequency of administration.and frequency of administration. No analgesic properties.No analgesic properties. Onset of action may be delayed 30-60 min. Onset of action may be delayed 30-60 min.
with a duration of action of 60-90 min. May with a duration of action of 60-90 min. May last up to eight hours in some instances.last up to eight hours in some instances.
Chloral Hydrate: Special Considerations
Respiratory depression may be delayed four Respiratory depression may be delayed four hours or more following administration.hours or more following administration.
Increased risk of airway obstruction in children Increased risk of airway obstruction in children with enlarged tonsils & adenoids.with enlarged tonsils & adenoids.
May cause dysrhythmias in patients with May cause dysrhythmias in patients with structural or other heart disease.structural or other heart disease.
May cause paradoxical agitation, particularly May cause paradoxical agitation, particularly in patients with neurological disorders; less in patients with neurological disorders; less effective in children >5 yrs .effective in children >5 yrs .
Liquid form may cause mucosal irritation Liquid form may cause mucosal irritation throughout the body. throughout the body.

Diphenhydramine Antihistamine that works at H-1 Antihistamine that works at H-1
receptors in the GI tract, blood receptors in the GI tract, blood vessels, and respiratory tract.vessels, and respiratory tract.
Used for mild sedation & its Used for mild sedation & its antihistamine properties.antihistamine properties.
May cause paradoxical May cause paradoxical excitement.excitement.
May produce hypotension, May produce hypotension, tachycardia, and urinary retention.tachycardia, and urinary retention.
Metabolized in the liver.Metabolized in the liver. Causes anticholinergic effects in Causes anticholinergic effects in
conjunction with MAO inhibitors.conjunction with MAO inhibitors. Use with caution in infants and Use with caution in infants and
young children.young children.
Ketamine This drug carries an increased risk of deep This drug carries an increased risk of deep
sedation and should be used only by those sedation and should be used only by those with hospital privileges in deep sedation.with hospital privileges in deep sedation.
Derivative of the street drug phencyclidine.Derivative of the street drug phencyclidine. Induces a functional dissociation between the Induces a functional dissociation between the
cortical & limbic systems to create a sensory cortical & limbic systems to create a sensory isolation and “trance-like” state.isolation and “trance-like” state.
A potent pain reliever as the drug prevents A potent pain reliever as the drug prevents cortical interpretation of noxious stimuli.cortical interpretation of noxious stimuli.

Ketamine Produces CNS Produces CNS
stimulation & inhibits stimulation & inhibits catecholamine uptake, catecholamine uptake, so direct myocardial so direct myocardial depressant effects are depressant effects are overcome.overcome.
May cause nystagmus, May cause nystagmus, vocalizations, and vocalizations, and myoclonus.myoclonus.
Ketamine While producing While producing
sedation, amnesia, & sedation, amnesia, & analgesia, ketamine analgesia, ketamine may also produce may also produce dreams & delirium. dreams & delirium. This is minimized by This is minimized by co-administering small co-administering small doses of midazolam.doses of midazolam.
Ketamine: Other Considerations Ketamine produces heavy secretions; consider co-Ketamine produces heavy secretions; consider co-
administration of glycopylorrate as a drying agent.administration of glycopylorrate as a drying agent. May be given IM May be given IM oror IV so useful when IV access IV so useful when IV access
is difficult.is difficult. Causes increased intracranial pressure, Causes increased intracranial pressure,
exacerbation of congestive heart failure, and may exacerbation of congestive heart failure, and may decrease B/P in catecholamine-depleted patients.decrease B/P in catecholamine-depleted patients.
Onset of action is ~1 min. IV & 10-20 min. IM. Onset of action is ~1 min. IV & 10-20 min. IM. Baseline level of consciousness returns ~15 min Baseline level of consciousness returns ~15 min after single IV dose.after single IV dose.
Propofol This drug carries an increased risk of This drug carries an increased risk of
progression to deep sedation and should be progression to deep sedation and should be used only by those with hospital privileges used only by those with hospital privileges in deep sedation.in deep sedation.
Propofol is thought to mediate activity at Propofol is thought to mediate activity at the GABA receptor in the CNS.the GABA receptor in the CNS.
Propofol has no analgesic properties but Propofol has no analgesic properties but does produce sedation and amnesia.does produce sedation and amnesia.
Propofol
Propofol is widely Propofol is widely distributed in the body distributed in the body and is eliminated via and is eliminated via hepatic & pulmonary hepatic & pulmonary systems. systems.
No dosage No dosage adjustments necessary adjustments necessary in patients with in patients with hepatic/renal disease.hepatic/renal disease.
To prevent hypotension To prevent hypotension consider reduced doses consider reduced doses in the elderly, in the elderly, hypovolemic, or hypovolemic, or patients receiving other patients receiving other narcotics/sedatives.narcotics/sedatives.
Supports rapid bacterial Supports rapid bacterial growth; discard 6 hrs growth; discard 6 hrs after opening.after opening.

The Lytic Cocktail A fixed combination of meperidine, promethazine, A fixed combination of meperidine, promethazine,
and chlorpromazine.and chlorpromazine. Long history of use in pediatric sedation.Long history of use in pediatric sedation. Commonly called DPT, an acronym for demerol, Commonly called DPT, an acronym for demerol,
phenergan, and thorazine.phenergan, and thorazine. Its use is strongly discouraged; equivalent or Its use is strongly discouraged; equivalent or
superior sedation may be achieved with single superior sedation may be achieved with single agents or individualized combinations of sedatives agents or individualized combinations of sedatives & narcotics.& narcotics.

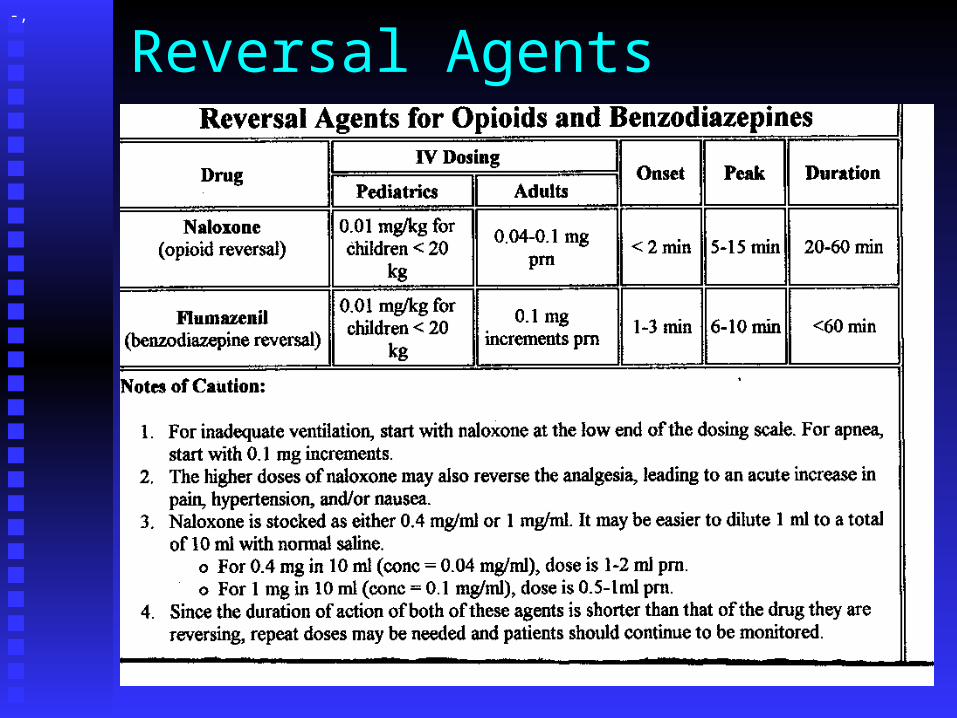
Reversal Agents: Naloxone
Naloxone is an opioid antagonist which Naloxone is an opioid antagonist which binds to CNS opioid receptors to displace binds to CNS opioid receptors to displace opioid agonists.opioid agonists.
Reverses respiratory depression and Reverses respiratory depression and sedation associated with opioids.sedation associated with opioids.
May be displaced from CNS receptors by May be displaced from CNS receptors by additional doses of opioid.additional doses of opioid.
Reversal Agents: Naloxone
Naloxone’s half-life is ~30 min; opioids’ Naloxone’s half-life is ~30 min; opioids’ half-life is 4-6 hours.half-life is 4-6 hours. Patients receiving naloxone will therefore Patients receiving naloxone will therefore
require a longer period of monitoring to require a longer period of monitoring to watch for recurrent respiratory watch for recurrent respiratory depression.depression.
May need additional doses of naloxone.May need additional doses of naloxone. Monitor for one hour after last dose of Monitor for one hour after last dose of
naloxone.naloxone.
Reversal Agents: Naloxone Naloxone may cause severe Naloxone may cause severe
pain if entire analgesic effect pain if entire analgesic effect of narcotics is reversed.of narcotics is reversed.
Overadministration of Overadministration of naloxone results in naloxone results in tachycardia, hypertension, tachycardia, hypertension, severe pain, nausea & severe pain, nausea & vomiting, and even vomiting, and even pulmonary edema related to pulmonary edema related to sympathetic outflow.sympathetic outflow.

Reversal Agents: Flumazenil Flumazenil binds to GABA receptors in the Flumazenil binds to GABA receptors in the
CNS to reverse effects of benzodiazepines.CNS to reverse effects of benzodiazepines. Flumazenil may be displaced from receptors Flumazenil may be displaced from receptors
by administration of additional BZDs.by administration of additional BZDs. Flumazenil reverses sedation, respiratory Flumazenil reverses sedation, respiratory
depression & paradoxical agitation, and depression & paradoxical agitation, and causes cessation of amnesia following its causes cessation of amnesia following its administration.administration.

Reversal Agents: Flumazenil
The half-life of BZDs may be >12 hrs; The half-life of BZDs may be >12 hrs; flumazenil’s half-life is only ~45 min. flumazenil’s half-life is only ~45 min.
Patients will require monitoring for 1 hr. Patients will require monitoring for 1 hr. after last dose of flumazenil.after last dose of flumazenil.
May precipitate sz in patients with May precipitate sz in patients with underlying disorder.underlying disorder.
Reversal Agents-,

Monitoring & Oxygen Administration
Oxygen saturation should be recorded prior to Oxygen saturation should be recorded prior to administration of supplemental oxygen & prior to administration of supplemental oxygen & prior to initiating sedation. Pulse oximeter initiating sedation. Pulse oximeter tonetone should be should be in the in the ““onon”” position. position.
Oxygen should be administered to all patients Oxygen should be administered to all patients undergoing conscious sedationundergoing conscious sedation Begin at 2L/min via nasal cannulaBegin at 2L/min via nasal cannula Changes in rate/mode of oxygen delivery may Changes in rate/mode of oxygen delivery may
be made at the discretion of the team.be made at the discretion of the team.
Monitoring & Oxygen Administration
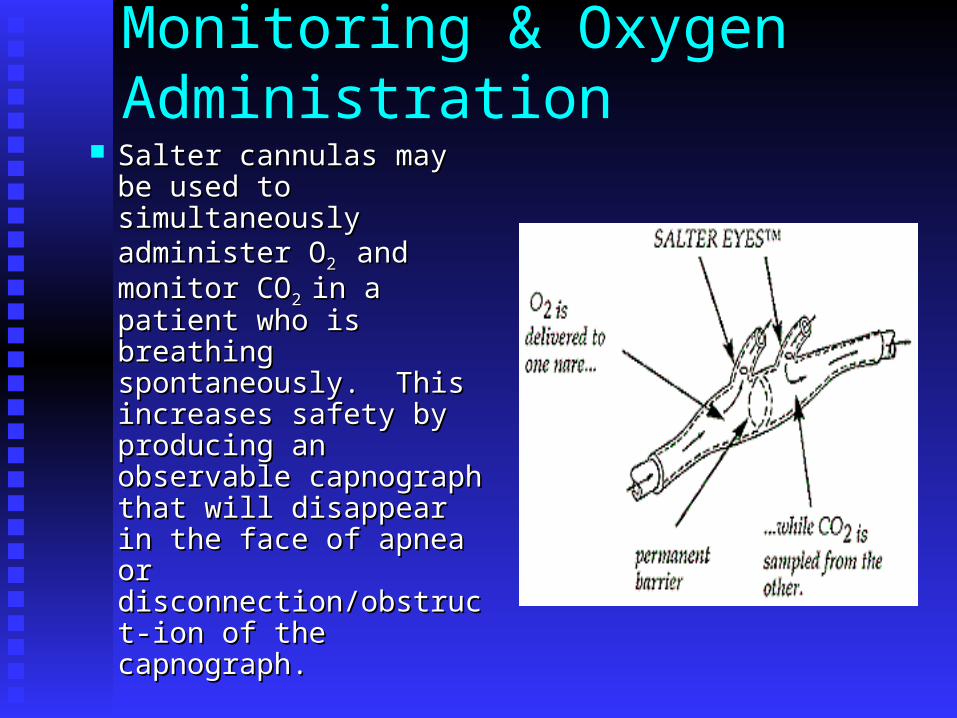
Salter cannulas may be Salter cannulas may be used to simultaneously used to simultaneously administer Oadminister O2 2 and and monitor COmonitor CO2 2 in a in a patient who is breathing patient who is breathing spontaneously. This spontaneously. This increases safety by increases safety by producing an producing an observable capnograph observable capnograph that will disappear in that will disappear in the face of apnea or the face of apnea or disconnection/obstruct-disconnection/obstruct-ion of the capnograph.ion of the capnograph.
Monitoring Respiration RespirationRespiration
Baseline assessment made & recorded Baseline assessment made & recorded prior to administration of drugs and at prior to administration of drugs and at least every 15 minutes thereafter.least every 15 minutes thereafter.
Note and record respiratory rateNote and record respiratory rate Continually observe for adequacy of Continually observe for adequacy of
spontaneous ventilation/airway patency.spontaneous ventilation/airway patency. Auscultate; Watch the chest rise & fall!Auscultate; Watch the chest rise & fall! May utilize capnometryMay utilize capnometry
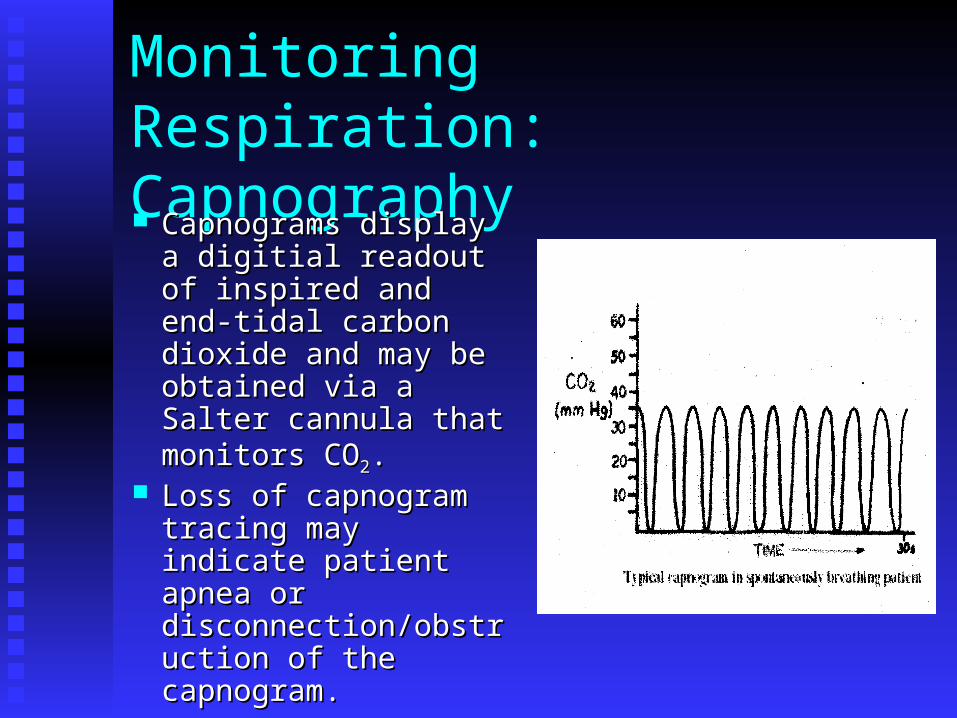
Monitoring Respiration: Capnography Capnograms display a Capnograms display a
digitial readout of digitial readout of inspired and end-tidal inspired and end-tidal carbon dioxide and carbon dioxide and may be obtained via a may be obtained via a Salter cannula that Salter cannula that monitors COmonitors CO22. .
Loss of capnogram Loss of capnogram tracing may indicate tracing may indicate patient apnea or patient apnea or disconnection/obstructdisconnection/obstruction of the capnogram.ion of the capnogram.

Monitoring B/P & Heart Rate Baseline measurements and recordings are Baseline measurements and recordings are
required.required. Assess & document 2-3 minutes after Assess & document 2-3 minutes after
administration of any drug, when the administration of any drug, when the patient’s condition changes, and at least patient’s condition changes, and at least every 15 minutes.every 15 minutes.
Consider EKG monitoring for patients with Consider EKG monitoring for patients with cardiac disease or at risk for dysrhythmias.cardiac disease or at risk for dysrhythmias.

Monitoring Level of Consciousness Pt. Response to commands/light tactile Pt. Response to commands/light tactile
stimuli should be frequently assessed using stimuli should be frequently assessed using the patient sedation scale.the patient sedation scale.
Document the patient’s level of Document the patient’s level of consciousness at least every 15 minutes.consciousness at least every 15 minutes.
Link to Pediatric Vital Signs Charts http://www.vh.org./Providers/ClinGuide/Pr
oceduralSedation/pedvitalsigns.html
Monitoring & Intervention Pts responding only to painful stimulation Pts responding only to painful stimulation
are deeply sedated and at risk for airway are deeply sedated and at risk for airway compromise.compromise.
Immediately evaluateImmediately evaluate Instruct pt to take a deep breath, Instruct pt to take a deep breath,
physically stimulate patient and instruct physically stimulate patient and instruct again to take a deep breath. again to take a deep breath.
A provider with privileges in deep sedation A provider with privileges in deep sedation or anesthesia personnel should be or anesthesia personnel should be immediately available to provide airway immediately available to provide airway and/or hemodynamic support as necessary.and/or hemodynamic support as necessary.
Monitoring & Intervention
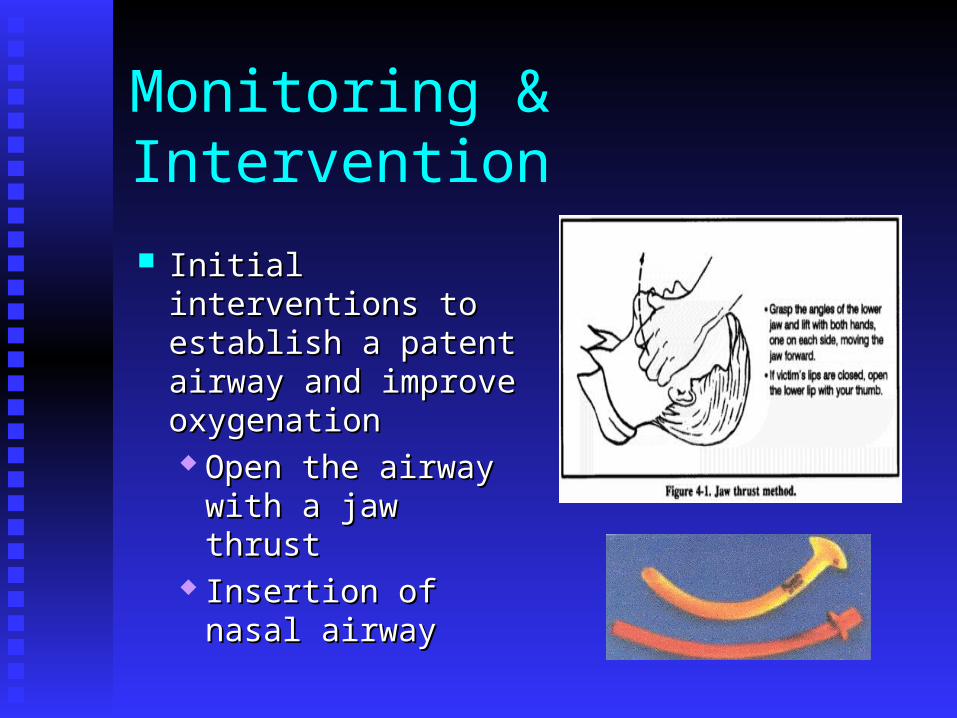
Initial interventions to Initial interventions to establish a patent establish a patent airway and improve airway and improve oxygenation oxygenation Open the airway Open the airway
with a jaw thrustwith a jaw thrust Insertion of nasal Insertion of nasal
airwayairway

Monitoring & Intervention Other interventions to Other interventions to
establish a patent establish a patent airway and improve airway and improve oxygenation include oxygenation include increasing oxygen increasing oxygen concentration and concentration and manually ventilating manually ventilating the patient with a bag-the patient with a bag-valve mask device.valve mask device.
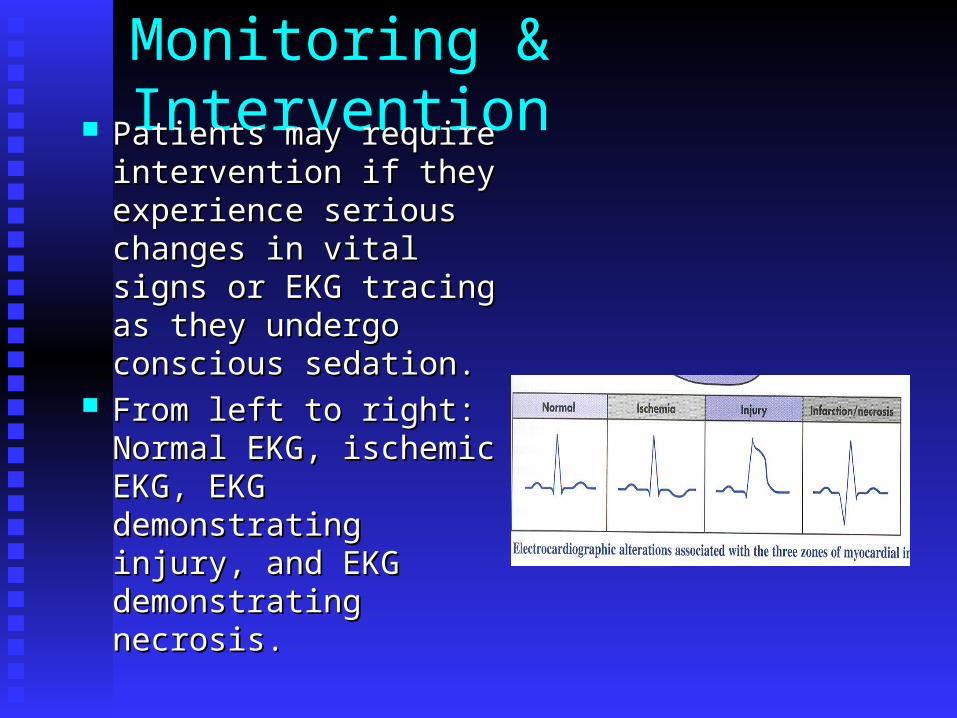
Monitoring & Intervention Patients may require Patients may require
intervention if they intervention if they experience serious experience serious changes in vital signs or changes in vital signs or EKG tracing as they EKG tracing as they undergo conscious undergo conscious sedation.sedation.
From left to right: From left to right: Normal EKG, ischemic Normal EKG, ischemic EKG, EKG EKG, EKG demonstrating injury, and demonstrating injury, and EKG demonstrating EKG demonstrating necrosis.necrosis.
Monitoring & Equipment It is the responsibility of the person It is the responsibility of the person
monitoring the patient to ensure that the monitoring the patient to ensure that the following items are following items are present & operationalpresent & operational prior to initiating conscious sedation:prior to initiating conscious sedation: Source of oxygen & suctionSource of oxygen & suction Suction cathetersSuction catheters Nasal cannula, simple face masks, & Nasal cannula, simple face masks, &
blow-by sets for oxygen deliveryblow-by sets for oxygen delivery Pulse oximeter & probesPulse oximeter & probes B/P machine /manometer and cuffsB/P machine /manometer and cuffs EKG machine and/or stethoscope.EKG machine and/or stethoscope.

Emergency Equipment A number of items must be immediately A number of items must be immediately
available & operational before undertaking available & operational before undertaking procedural sedation.procedural sedation. Supplemental monitorsSupplemental monitors Basic & advanced airway management Basic & advanced airway management
equipmentequipment IV supplies IV supplies Emergency drugsEmergency drugs DefibrillatorDefibrillator
For Complete Listing For Complete Listing http://www.vh.org/Providers/ClinGuide/ProceduralSedation/EquipmentList.html

Recovery & Discharge The recovery period lasts from the The recovery period lasts from the
conclusion of the test/operative procedure conclusion of the test/operative procedure until the patient has returned to baseline.until the patient has returned to baseline.
Saturation should be monitored Saturation should be monitored continuously, and vital signs/level of continuously, and vital signs/level of consciousness recorded at regular intervals.consciousness recorded at regular intervals.
Discharge instructions should be clearly Discharge instructions should be clearly written and reviewed with written and reviewed with patient/responsible adult.patient/responsible adult.

Conclusion Conscious sedation Conscious sedation
that is carefully that is carefully planned and carried planned and carried out by a thoughtful, out by a thoughtful, well-trained health well-trained health care team will allow care team will allow both caregivers and both caregivers and patients to have a patients to have a positive experience positive experience rather than a bad rather than a bad memory.memory.








![Conscious Sedation In The Provision of Dental Care · patients requiring dental care and Conscious Sedation is a fundamental component of this. [2] q Competently provided Conscious](https://static.fdocuments.in/doc/165x107/5e80f906b673072b2a542a7a/conscious-sedation-in-the-provision-of-dental-care-patients-requiring-dental-care.jpg)









