Connecticut Hospital Association HRO Creating …...Creating Sustainability for High Reliability...
68
Friday, April 15, 2016 Connecticut Hospital Association HRO Creating Sustainability for High Reliability Organizations 8:30 a.m. – 9:00 a.m. Registration and Continental Breakfast 9:00 a.m. – 10:30 a.m. Creating Sustainability for High Reliability Organizations 10:30 a.m. – 10:45 a.m. Program Break 10:45 a.m. – 12:00 p.m. Creating Sustainability for High Reliability Organizations (continued) 12:00 p.m. – 12:15 p.m. Program Wrap-up and Evaluations
Transcript of Connecticut Hospital Association HRO Creating …...Creating Sustainability for High Reliability...

Friday, April 15, 2016
Connecticut Hospital Association HROCreating Sustainability for High Reliability Organizations
8:30 a.m. – 9:00 a.m. Registration and Continental Breakfast
9:00 a.m. – 10:30 a.m. Creating Sustainability for High Reliability Organizations
10:30 a.m. – 10:45 a.m. Program Break
10:45 a.m. – 12:00 p.m. Creating Sustainability for High Reliability Organizations (continued)
12:00 p.m. – 12:15 p.m. Program Wrap-up and Evaluations


Creating Sustainability for High Reliability Organizations held at
The Connecticut Hospital Association 110 Barnes Road Wallingford, CT
Friday, April 15, 2016 9:00 a.m. – 12:15 p.m.
Please circle the extent to which these objectives were met: POOR FAIR GOOD EXCELLENT N/A
1. Amount of useful information and ideas provided: 1 2 3 4
2. Learning Environment and Circumstances (e.g., room, AV, accessibility of the site):
1 2 3 4
3. Usefulness to my hospital of the information and ideas provided: 1 2 3 4
4. Chance that the information and ideas provided will improve my effectiveness and results:
1 2 3 4
POOR BELOW EXPECT-ATIONS
SATIS- FACTORY
GOOD EXCELLENT
5. This activity’s impact on improving your job performance: 1 2 3 4 5
6. Relevance of learning objectives to purpose/goals of activity The purpose of this continuing education activity is to provide healthcare professionals with concepts and tips to prevent High Reliability from becoming a “flavor of the month.”
1 2 3 4 5
7. Appropriateness of audiovisual and teaching aids: 1 2 3 4 5
8. The pace of the activity: 1 2 3 4 5
9. The conference room was conducive to learning and networking: 1 2 3 4 5
10. The program met my overall expectations: 1 2 3 4 5
11. The teaching effectiveness of the speaker: Steve Kreiser 1 2 3 4 5 12. The effectiveness of the teaching strategies: 1 2 3 4 5
I will use the information from today’s session to (please check all that apply): � Create/revise protocols, policies and/or procedures � Change the management and/or treatment of my patients � Other change(s) � I will not make any changes to my practice
Please describe what you plan to do:
Clinical discipline: MD_____________ RN________________ Other______________________________________ [Please indicate] Name (Optional): _____________________________________ Institution:_________________________________
Please turn over for additional evaluation questions.

Creating Sustainability for High Reliability Organizations Evaluation Form Continued
Please circle the extent to which these objectives were met:
POOR BELOW EXPECT-ATIONS
SATIS- FACTORY
GOOD EXCELLENT
Explain the importance of safety metrics and how measurements must be maintained and made visible across the organization.
1 2 3 4 5
Define transparency in terms of making harm visible throughout the organization through various mechanisms, including story-telling and sharing of lessons-learned.
1 2 3 4 5
Describe the importance of hard-wiring structured leadership methods to find and fix system problems and to reinforce and build accountability.
1 2 3 4 5
Explain the importance of physician engagement and ownership of patient safety culture.
1 2 3 4 5
Describe how enhanced cause analysis programs are critical to learning organization improvements.
1 2 3 4 5
What one thing about this activity would you most like to see improved?
What one thing about this activity did you like most?
Please give an example of how the content was relevant or thorough on this issue:
On what other topics would you like to see general CHA education?
Other Comments:
DISCLOSURE: The speaker and members of the Planning Committee have made full disclosures and do not have any commercial or financial interest which would bias the presentation.
PLEASE RETURN THIS FORM TO CHA REGISTRATION TABLE AT THE END OF THE SESSION.

Notes From HRO Creating Sustainability forHigh Reliability Organization
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 1
Connecticut Hospital Association Leadership Workshop
© 2014 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED. This material is a proprietary document of Healthcare Performance Improvement LLC. Reproducing, copying, publishing, distributing, presenting, or creating derivative work products based on this material without written permission from Healthcare Performance Improvement is prohibited.
Building a High Reliability Organization: Sustaining Reliability and Safety Culture
Slide 2
Safety First in Every Meeting Demonstrate Safety First by starting each meeting with a two-minute (or less) statement or story about patient or personal safety: 1. Share your convictions on patient or personal safety 2. Explain how safety contributes to our mission 3. Explain how our policy & practice contribute to safety 4. Tell a story about something good that we did 5. Tell a story about something bad that happened to us 6. Tell a story about harm in another healthcare system 7. Tell a story about another system preventing harm 8. Read a Safety Success Story from your people 9. Read a Safety Success Story from CHA 10. Review our safety behaviors 11. Teach applications of our safety behaviors to our jobs 12. Discuss the importance of reporting problems 13. Discuss the importance of speaking-up for safety 14. Ask staff to be safe, and explain how 15. Thank staff for practicing / working safely

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 2
Slide 3
"Good ideas are not adopted automatically. They must be driven into practice with courageous impatience. Once implemented they can be easily overturned or subverted through apathy or lack of follow-up, so a continuous effort is required."
Admiral Hyman G. Rickover 1900-1986
Slide 4
The “ATM” of Safety Culture Leadership
A – Attention Attention is the currency of leadership.
T – Transparency and Trust Transparency = learning. Trust is the
enabler of transparency.
M – Measure, Measure, Measure from Lee Carter, Chairman of the Board – Cincinnati Children’s Hospital Medical Center

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 3
Slide 5
Sustainment through Measurement
Serious Safety Event • Reaches the patient • Results in moderate to severe harm or death
Precursor Safety Event • Reaches the patient • Results in minimal harm or no detectable harm
Near Miss Safety Event • Does not reach the patient • Error is caught by a detection barrier or by chance
Precursor Safety Events
Serious Safety Events
Near Miss Safety Event
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
A deviation from generally accepted performance standards (GAPS) that…

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 4
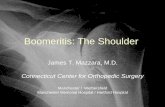
Typical Improvement Curve
Actual increase due to complacency or reverting to old habits
Achieved in 1 to 3 years, approximately
Time
Sign
ifica
nt E
vent
Rat
e
Start of Culture Change
Apparent increase due to healthier event/problem reporting culture
80% reduction in serious preventable harm as a result of prevention activities
Long-term improvement through sustained prevention
Hospital X
Slide 8
Best Practice Tips in Safety Event Classification
Identify a consistent group of people to serve as a “Safety Event Review Panel” to provide expertise, consistency, and integrity in event classification. The group should be a mix of clinicians and methodology experts and senior enough to gain organizational trust.
When classifying an event, use the SEC algorithm and always ask ALL the questions – e.g. Was there a deviation? Did the deviation reach the patient? What was the level of harm?
Charge one person with the responsibility for thinking/asking about precedent.

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 5
Slide 9
Best Practice Tips in Safety Event Classification
Keep a record of challenging event classification cases and classification rationale. This record provides a useful reference when assessing similar future cases and enables the group to look at changes in their own perspectives in event classification.
What happens in the discussions, stays in the discussions. The group speaks with one voice outside the meetings.
Slide 10

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 6
Slide 11
Use SSER to Make Harm Visible …and more importantly, our efforts to eliminate it!
Slide 12
Present SSER Data Monthly to… Overall Board of Directors (high level view) Quality Committee of the Board (deeper dive) Executive Leadership Team Overall Leadership Team Quality and safety committee Patient Safety Coaches MEC (and any other standing medical staff committees) Physician champions

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 7
Beyond SSER – The SSE+PSER
with permission of Holy Redeemer Health System
The SSE+PSER… Prevents complacency during long event-free stretches Heightens awareness of the wealth of learning opportunities from “lesser events”
At Holy Redeemer: The SSER and SSE+PSER is monitored at the Board and Senior Leader levels. The SSE to PSE ratio at this Holy Redeemer division is 1:16. (In a state of optimal reporting health, the ratio likely is 1:100 or more.)
SSE PSE
What It Tells Us How many people did we injury?
How many people received an error in care with minimal or no harm?
Message We Want To Send Reduce…and eliminate! Freely report and learn
Slide 14
Worker Safety Improvements (5 hospital system – Southern US)
$0
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
CY 07 CY 08 CY 09 CY 10
Workman's Compensation Costs
Over $1, 200,000 saved year to date!
02468
101214161820
Sep-06
Oct-06
Nov-06
Dec-06
Jan-07Feb-07M
ar-07A
pr-07M
ay-07Jun-07Jul-07A
ug-07S
ep-07O
ct-07N
ov-07D
ec-07Jan-08Feb-08M
ar-08A
pr-08M
ay-08Jun-08Jul-08A
ug-08S
ep-08O
ct-08N
ov-08D
ec-08Jan-09Feb-09M
ar-09A
pr-09M
ay-09Jun-09Jul-09A
ug-09S
ep-09O
ct-09N
ov-09D
ec-09Jan-10Feb-10M
ar-10A
pr-10M
ay-10Jun-10Jul-10A
ug-10S
ep-10O
ct-10N
ov-10D
ec-10Jan-11Feb-11M
ar-11A
pr-11
Month
Monthly Lost Time Claims July 06 - April 2011
802 Over 300 Serious Injuries prevented
90% reduction in OSHA IIR

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 8
Measurement of Safety Culture
Sentara Safety Dashboard
Leading Indicator • Safety Culture Survey Scores Real Time Indicators • Safety Behavior Pulse Checks
• Leaders • Staff • Physicians
• Safety Success Stories Received & Communicated • Number of Events Reported Lagging Indicators • Serious Safety Event Rate (SSER) • # Serious Safety Events • # Precursor Safety Events • #/$ Professional Liability Claims & Suits • OSHA Employee IRR • #/$ Worker’s Comp Injuries

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 9
Slide 17
Sustainment through Rigorous Reinforcement of
Safety Habits
Slide 18
Safety Success Stories Brief narrative about a person who
engaged in a safe practice and the outcome experienced as a result.
A challenge to leaders and staff to reflect and consider how their behaviors protect (or harm) their patients.
Not about measuring event totals, but the
ability of people to capture how actions (behaviors) affect patient outcomes.
Shared across the organization to recognize the individual and reinforce safe practices.

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 10
What Makes a Great Story Great??? Everyday excellence – not just the great saves Language we can all understand Name names to recognize Link to a behavior expectation
More Clever: Use the number of published safety success stories as
a real-time metric.
Share Safety Success Stories
Nurse on 3 West Exercises a Questioning Attitude Jessica Tyler picked up a unit of blood from the Blood Bank for a sickle cell patient. Validating, she noticed that the unit of blood did not have a specific label that she was used to seeing on units of blood for sickle cell patients. Verifying, she asked the Blood Bank Technician about the missing label. The Technician looked at the patient profile, and realized that the patient indeed was a sickle cell patient and should receive irradiated blood. Great example of using a Questioning Attitude to catch an error that could have harmed one of our patients. Well done Jessica!
More Clever: All in it together – leaders take the quiz, too!
Quiz for Knowledge

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 11
Safety Habit Audits
Safety Habit Survey – SBH
100 100 100 100 100100 100 100 100 100
0102030405060708090
100
Attention to Detail CommunicateClearly
QuestioningAttitude
Handoff Effectively Wingman
January 2010
February 2010
Percentage of Surveyed Staff Who Could Name the Safety Habits (BBEs)
2010 Goal = 60% surveyed will be able to name all 5 Safety Habits

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 12
Safety Habit Survey – SBH
100 100 100 100 100100 100 100 100 100
0102030405060708090
100
Attention toDetail
CommunicateClearly
QuestioningAttitude
HandoffEffectively
Wingman
January 2010February 2010
Percentage of Surveyed Leadership Who Could Name the Safety Habits (BBEs)
2010 Goal = 60% surveyed will be able to name all 5 Safety Habits
Safety Habit Survey – SBH
70
55
20
10 10
60
0
7570
60
9086
7167 67
90
71
8681 81
0102030405060708090
100
STAR RB/RB CQ PhNC SBAR VV STOP 5Ps PCh Pco
January 2010February 2010
STAR – Stop, Think, Act, Review SBAR – Situation, Background, Assessment, Recommendation/Request PCh – Peer Checking
RB/RB – Read Back, Repeat Back VV – Validate and Verify PCo – Peer Coaching
CQ – Clarifying Questions STOP - Stop
PhNC – Phonetic & Numeric Clarification 5Ps – Patient/Project, Plan, Purpose, Problems, Precautions
Percentage of Surveyed Staff Who Could Name the Error Prevention Tools
2010 Goal = 60% surveyed will be able to correctly tie 1 EPT to each Safety Habit

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 13
Safety Habit Survey – SBH
70
50
30 30 30
70
0
90
70
60
70 70 70 70 70 70 70 70 70 70
0102030405060708090
100
STAR RB/RB CQ PhNC SBAR VV STOP 5Ps PCh Pco
January 2010February 2010
Percentage of Surveyed Leadership Who Could Name the Error Prevention Tools
STAR – Stop, Think, Act, Review SBAR – Situation, Background, Assessment, Recommendation/Request PCh – Peer Checking
RB/RB – Read Back, Repeat Back VV – Validate and Verify PCo – Peer Coaching
CQ – Clarifying Questions STOP - Stop
PhNC – Phonetic & Numeric Clarification 5Ps – Patient/Project, Plan, Purpose, Problems, Precautions
2010 Goal = 60% surveyed will be able to correctly tie 1 EPT to each Safety Habit
Other Reinforcement Mechanisms Start unit-based Huddles with an Error Prevention Tool of the Week (the Sesame Street approach) Have a Safety Habit or Error Prevention Tool of the month - Highlight it in stories - Make it the focus on Rounding to Influence - Make it the focus of Safety Coaching
Integrate Safety Habits and Error Prevention Tools into simulation activities and skills fairs Ensure annual refresher training occurs - With commitment statements
Posters, screen savers, badges, pens, mousepads, etc. Leverage multi-media whenever possible (MedStar)

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 14
Sustainment through Integration into HR
Performance Reviews and Hiring Criteria
Integration into Annual Performance Reviews

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 15
Specific Expectations
HR Integration at Main Line
• Every employee has the goal to demonstrate mastery of EP tools by providing evidence of the use of 4 different tools as they apply to their scope of work. • The attached document was developed for staff to document their accomplishments to be submitted to their manager (some expect it quarterly). Or they can enter it directly into the electronic system for performance management.

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 16
What is a behavioral interview? Behavioral-based interviewing involves discovering how the interviewee acted in specific employment-related situations. The logic stems from how you behaved in the past will predict how you will behave in the future (i.e. past performance predicts future performance.)
Critical to the sustainment of a safe and reliable culture is hiring new personnel who will fit into the culture we have created.
Managing Turnover
Peer
Person
r Leader Behavioral interviews have been found to be helpful in hiring personnel with the attitude and character we want.
During transformation, members select the culture To sustain culture, the culture must select its members
Individual Accountability - Hiring for Fit

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 17
Sustainment through Transparency
Slide 34
The HRO Difference Harm is visible – Risk is visible

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 18
Slide 35
Make Harm Visible
Slide 36
“Success teaches us nothing; only failure teaches...
Develop the capacity to learn from experience.”
Admiral Hyman G. Rickover, US Navy (27 January 1900 – 8 July 1986)
Known as the “Father of the Nuclear Navy”
"It is necessary for us to learn from others' mistakes. You will not live long
enough to make them all yourself.”

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 19
Slide 37
Safety Event Communication A nurse received a telephone order from a physician for a medication. She was unfamiliar with the medication and called the pharmacy for assistance. The pharmacist gave instructions on how to calculate the dose. The nurse was concerned about preparing the medication herself but the patient needed the medication urgently so she calculated and administered the dose. The dose was incorrect and the patient required intervention from the rapid response team. Whenever you have concerns it is your responsibility to STOP, validate and verify. If you have attempted to verify, and still have questions or concerns, it is important that you seek out another expert to help you. DO NOT proceed until your concerns are resolved. Also, if you are doing an unfamiliar task or something you have not done in a long time, don’t be afraid to ask for a cross check. When doing complex tasks, two heads are better than one. Challenge Questions: Have you ever been asked to do an unfamiliar or new task? What did you do? Who are the experts you can consult if you need a cross check? If you need to verify?
• Written in simple language • Avoids naming or blaming
Reinforces organization’s error prevention tools and safety behaviors
Challenge questions enable staff to apply lessons learned to own environment
Share Lessons Learned
Slide 38
Held at each site – open to all “SBAR” presentation of Serious Safety Event RCA S – Brief description of event B – Sequence of events A – Inappropriate acts and root causes R – Corrective actions to prevent recurrence
Layman’s language Discussion about lessons learned - Link to Safety Behaviors - How could this happen in other places? - How can we apply lessons learned?
Clif Knight, MD – Chief Medical Officer Community Health Network
with permission of Community Health Network w
Lessons Learned Lunch Series

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 20
Slide 39
BREAK
Slide 40
Sustainment through Physician Engagement

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 21
Slide 41
HPI Lessons-Learned
“Physicians do not make safety transformation happen but they can prevent it from happening.”
More accurately stated:
“No hospital can achieve a state of high reliability without the full engagement of the
medical staff.
True physician leadership, optimally from the outset, is required to achieve and sustain a safe
environment for patients.”
Slide 42
Sharp End Provider to Blunt End Influencer
Proportion of time by: Residents? Attendings? Division chiefs? Department chairs? CMO?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 22
Slide 43
Vive la Difference
Sharp End Provider Know and comply with behavior expectations for error prevention – make them personal work habits Encourage the practice of behavior expectations for error prevention in others
Blunt End Leader Demonstrate in word and actions safety as a core value that cannot be compromised at any time Find and fix causes of system and process problems that challenge safe, high quality care Reinforce and build accountability for behavior expectations for error prevention
Slide 44
Critical Impact of Physicians on Safety Transformation
Significant contribution to errors associated with patient injury Unequaled impact on hospital morale through their considerable influence on hospital staff and leaders Strengths may become liabilities – intelligence, independence, analytical, sense of urgency Profound impact on long-term hospital culture – sustained improvements require physician ownership Ensure a strong Peer Review program is in place - To respond to both technical and behavioral issues - Integrate Safety Event Classification and Fair and Just criteria

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 23
Slide 45
The Disruptive Path Attributes
Intelligence
Independence
Objectivity
Analytic Capability
Sense of Urgency
Influence
Liabilities
Elitest
Team averse
Impersonal
Critical
Impatient
Aggressive
Unreliability
Condescending
Abrasive
Belligerent
Blaming
Insensitivity
Sabotage
Derived from Overcoming Your Strengths, by Lois P. Frankel, PhD
Slide 46
The Success Path Attributes
Intelligence
Independence
Objectivity
Analytic Capability
Sense of Urgency
Influence
Strengths
Competence
Confidence
Thinking Critically
Problem Solving
Safety First
Team Building
Reliability
Preoccupation with failure Sensitivity to operations Reluctance to simplify Commitment to resilience Deference to expertise

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 24
Slide 47
Medical Staff Stratification for Safety Culture Leadership
Where are our physicians and how can we engage them?
Characteristics Actions to Engage in Safety Culture Leadership
Level 3 Blunt End Leader for the Common Best
Influences changes in systems and processes to improve the sharp end condition in the interest of all providers and patients
Crystallize role of blunt end leaders Actively engage as leaders and as influencers of Level 1 and 2 physicians
Level 2 Blunt End Leader for My Own Good
Influences changes in systems and processes to improve the sharp end condition for their own benefit
Educate about blunt end role and expectations Develop strategies to:
-Move the willing and able to Level 3 -Moderate the unmovable -Manage disruptors
Level 1 Sharp End Provider
Functions primarily as a care provider, delivering care and service to patients or supports the delivery of care and service
Encourage accountability for individual and team behaviors for safe, productive practice
© 2008 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Slide 48
How Rigorously have you Engaged your Medical Staff?
Were physicians required to take the patient safety error prevention training as part of being credentialed? - Is it part of credentialing criteria for new members? - Are physicians required to take refresher training?
Did they attend patient safety training with staff? - If not, how did they get the training? - Did any physicians step up to become trainers?
Is patient safety, including SSER, discussed in medical staff meetings? - Do physicians start their meetings with safety first?
Are disruptive physicians dealt with fairly and consistently (or do we ride the fence?) Have you identified physician safety champions?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 25
Slide 49
Physician Safety Champions
Concept—select a respected, influential group of physician leaders to mold a high-reliability medical staff culture, beginning with patient safety
Not necessary to influence everyone to tilt the culture, only a segment equivalent to the square root of the number of participants—
Edwards Deming, Ph D
Slide 50
Physician Champions Additional initial education on concepts/ theory Potential roles: - Periodically attend daily huddle - Periodically round with operations colleague - Assist with education of other physicians - Meet periodically as a group of physician champions for additional skill
building and feedback - Serve as a resource to other committees and members of their own group - Participate in strategic safety/ reliability planning
Have high standards and promote professional atmospheres - Provide a safety and reliability perspective in medical staff meetings, medical
group meetings or informal gathering of colleagues - Share stories to reinforce importance of patient safety while also providing
relevant information

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 26
Slide 51
Sustainment through Structured High Reliability
Leadership
Slide 52
Leadership Method (not micro-management)
“A well-led institution has predictable leadership…
you can conjecture what its managers are doing and what they
are likely to do next.”
Scott Snair West Point Leadership Lessons

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 27
Slide 53
Define & Demonstrate Safety First at the “blunt end”
Reinforce & Build Accountability for behaviors at the “sharp end”
Find Problems & Fix Causes in systems and processes
Three Roles of HRO Leaders
Set the set point
Manage to prevent, detect, and manage drift
© 2008 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Slide 54 Slide 54
CHA High Reliability Leadership Methods
Build and Reinforce Accountability Leaders make reliability a reality by building a culture of collegial teamwork where sound practice habits are adopted by all to reduce human error. Leaders reinforce good habits, correct poor ones, never punish honest mistakes, yet are not afraid to hand out fair consequences to those who choose to adopt reckless behaviors. - Rounding to Influence with 5:1 Feedback - Fair and Just Accountability using the Performance Management Decision Guide - Safety Absolutes - Safety Coaches
Find and Fix System Causes Leaders remove barriers that impede team members from performing effectively and take active steps to find and fix the holes in the Swiss Cheese before they lead to patient or employee harm. - Daily Safety Check-in - Pre-Task and After-Action Huddles - Start the Clock on Safety Critical Issues - Leadership workgroups - Top 10 Lists with Action Plans - Unit Top 2 & Patient Communication Boards
Set the Tone of Safety as a Core Value Leaders show the way by setting expectations and setting good examples. Leaders model, inspire, train and encourage team members to keep themselves and others safe each and every day. - Safety First in Every Meeting - Thank those who Voice Safety Concerns - Safety First in Decisions – What’s best for the Patient? - Communicate Lessons from Safety Events - Encourage Error, Problem and Event Reporting - Educate for Safety Every Day

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 28
Slide 55
Are you Starting Meetings with Safety? Demonstrate Safety First by starting each meeting with a two-minute (or less) statement or story about patient or personal safety: 1. Share your convictions on patient or personal safety 2. Explain how safety contributes to our mission 3. Explain how our policy & practice contribute to safety 4. Tell a story about something good that we did 5. Tell a story about something bad that happened to us 6. Tell a story about harm in another healthcare system 7. Tell a story about another system preventing harm 8. Read a Safety Success Story from your people 9. Read a Safety Success Story from CHA 10. Review our safety behaviors 11. Teach applications of our safety behaviors to our jobs 12. Discuss the importance of reporting problems 13. Discuss the importance of speaking-up for safety 14. Ask staff to be safe, and explain how 15. Thank staff for practicing / working safely
Slide 56
© 2008 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Do your Leaders Prepare to Participate?
Do Senior Leaders lead, or at least attend and engage, in the huddle?
Do you follow a set agenda?
Are leaders comfortable bringing up
their event reports?
Do you track items for follow-up?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 29
Slide 57
Do you Start the Clock on Safety-Critical Issues?
Start the Clock sense of urgency These are the clock ticker issues – issues that pose a significant threat. They may be local or global in nature.
Mobilize those with the expertise to solve the problem and authority to empower action using Condition-Problem-Cause solving
Priority for resolution should be stated (e.g. solved today, solved within 24 hrs); a single-point owner should be identified; the owner should have an action plan; and the issues should be tracked at Daily Check In.
Start the Clock Response to Safety Critical Issues at Community Health North
For these types of issues, Barb Summers at Community was known to request, “Page me by 3:00 pm today with a status report.” Her rationale was twofold – to demonstrate the sense of urgency and to be made aware of any barriers to resolution that may need to be addressed before close of business.
Slide 58
Do you have Unit-Based Safety Huddles?
Do they follow structured agendas?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 30
Slide 59
Do you have a Top 10 List?
A leadership tool for focusing efforts… • Shared awareness of issues • Prioritized by safety-critical and urgency • Focus attention and effort on solving problems and
problem causes to prevent recurrence • When a problem is resolved, a new problem is added –
always 10 on the Top 10
Problem Resolution Rate (PRR) = Problems Solved/Problems Identified
Slide 60
Do you have Standardized Action Planning?
1. Assign Executive Sponsor 2. Assign Problem Owner 3. Are goals as described on target? 4. Identify high-level actions (Level 1)
– Assign ONE Problem Owner for each Level 1 Action
5. Identify sub-level action steps (Level 2) – Assign ownership: Who might be best qualified to solve the problem(s)
identified? – What resources might this individual need?
6. Designate Due Dates for each action

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 31
Slide 61
NOT about punishing the person
Building intrinsic motivation of the individual to meet performance
expectations
How do you Build Accountability?
Copyright 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Slide 62
Three Sources of Accountability
Leaders Vertical
Accountability
Peers Horizontal
Accountability
Individual Intrinsic
Accountability
Optimal Accountability
Accountab
I di id lid l
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 32
Slide 63
Fr
Accountability: Where Are We Today?
© 2010 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
L
I P
Free for All
L
I P
Leader Centric
L
I P
Team Survival Characteristics:
Significant blunt-end/sharp-end disconnect. Leader not aware of status of operations at the front line. Individual standards thrive. Workers work around each other, not with each other.
Characteristics: At worst, accountability is top-down driven and punitive; breeds fear. At best, L/I relationship reflects balanced feedback and trust. Yet condition is leader-dependent and, over time, exhausting for the Leader.
Characteristics: Leader is disconnected, yet high degree of teamwork and cross monitoring to get the work done. At best, good results can mask lack of leadership involvement. At worst, practice may differ sharply from – or, over time, deviate from – best-practice expectations.
Characteristics: Individuals “hired for fit” – high degree of motivation to do the right thing. High degree of teamwork and cross-monitoring, focused on best-practice standards. Leader provides real-time, 5:1 feedback; finds and fixes system problems. Strength in I and P accountability results in lesser relative L effort.
Optimal
P I
L
Slide 64
Fr
The Path to Optimal Accountability
© 2010 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
L
I P
Free for All
L
I P
Leader Centric
L
I P
Team Survival
Optimal
P I
L
Team Building
P I
L
Standard Setting
P I
L

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 33
Slide 65
Rounding to Influence
Connect to a core value
Assess knowledge and reinforce the specific behavior expectations
Identify problems impacting ability to follow the behavior expectations
Ask about commitment actions
♥
Slide 66
Have you Developed RTI Scripts? Rounding Focus: Attention to Detail 1. Core Value:
Have you been to our CHAMP safety training? When did you go? We’re rounding today to talk about those Safety Habits and tools because we want to ensure we are doing everything we can to keep our patients safe. (share some data or a story to get buy-in)
2. Can-do:
Can you tell me about the A in CHAMP? 1. Attention to Detail 2. Self check using STAR – Stop, Think, Act, Review 3. Helps to avoid skill-based errors when we are rushing, distracted,
interrupted, multi-tasking, fatigued 4. Like being at the candy machine, it helps us focus when in that auto-
pilot mode
3. Concerns: Is there anything that makes doing or thinking STAR difficult?
4. Commitment: Can I count on you to think STAR during your day? Use it when you’re getting a medication, tracing a line, doing the Timeout, loading a medication dispenser, doing 2-patient ID. There are so many times during the day when STAR can help avoid an error.

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 34
Slide 67
Have you Set RTI Leader Expectations?
Senior Leaders – 2-4 times a month Directors – twice a week Managers – daily
How do you hold leaders accountable for these expectations? - Go from Huddle - Round in pairs - Log-in forms - One-on-one’s - Report out at leadership meetings
Slide 68
Do you Provide 5:1 Feedback?
Positive Feedback Encouraging someone to continue practicing an observed behavior Top Positive Reinforcements 1. Head nod 2. “Yes” 3. “Thank you”
Negative Feedback Discouraging someone from continuing to practice an observed behavior Top Negative Reinforcements 1. Furrowed brow 2. “No” 3. Offering a practice tip
Adapted from Bringing Out the Best in People, by Dr. Aubrey Daniels (1994)
5 positive bits of feedback for every 1 bit of negative feedback

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 35
Slide 69
How Effectively Have you Implemented Fair and Just?
Train all your leaders on the effective use of the PMDG Ask managers if they applied the PMDG when responding to specific events
Assign HR as the process owner for PMDG implementation However, ensure all leaders understand Fair and Just is owned by Operations Ensure the PMDG is officially referenced in HR policies
Round-To-Influence on the importance of reporting and learning from errors and events
Emphasize the approach you are taking to Fair and Just “We don’t punish unintended human error, but there has to be fair consequences when people choose not to comply”
Do managers review the PMDG with staff whenever a performance deviation occurs, or only when they are seeking to show why they need
to “write up” the employee?
Slide 70
Performance Management Decision Guide Adapted from James Reason’s Decision Tree for Determining the Culpability of Unsafe Acts and
the Incident Decision Tree of the National Patient Safety Agency (United Kingdom National Health Service)
Did the individual intend the act?
Would individuals in the same profession and with comparable knowledge, skills, and experience act the same under similar circumstances?
Did the individual depart from policies,
procedures, protocols, or generally accepted
performance expectations?
Is there evidence of ill health or substance abuse?
Did the individual act with malicious intent
(i.e. to cause individual harm or other damage)?
Were there deficiencies in related training, experience,
or supervision?
Were the policies, procedures, protocols, or performance expectations available, understandable,
workable, and in routine use?
Did the individual have a known medical condition?
Were there significant mitigating circumstances?
Is there evidence that the individual chose to take an
unacceptable risk OR has a trend in poor performance or
decision making?
(Consult Human Resources) Disciplinary action Report to professional group or regulatory body Law enforcement referral
Identify Contributing System Factors
(Consult Human Resources) Disciplinary action Job-fit consideration
Identify Contributing System Factors
(Consult Human Resources) Console Coaching Mentor assignment Increased supervision Performance improvement plan Adjustment of duties
Identify Contributing System Factors
(Consult Human Resources) Occupational health referral Adjustment of duties Leave of absence
If substance abuse: Substance abuse testing Disciplinary action
Identify Contributing System Factors
Yes
Yes
Yes Yes
No No
Deliberate Act Test Incapacity Test Compliance Test Substitution Test
Yes
No
No
No
No No No
No
Console and/or Coach the
Individual AND Find & Fix Process
Problems
Start
Yes
Revision 3, April 2009 © 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Yes
Yes
No
Yes
Medical Condition and/or Substance Abuse
Possible Reckless or Negligent Behavior
Possible Unintended Human Error
Possible System Induced Error
Malevolent or Willful Misconduct
Yes
D1
D2
I1
I2
C1
C3
C2
C4
S1
S2

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 36
Slide 71
Safety Absolutes are NOT a discipline program
- Instead, they are a communication program for leaders
- “SO IMPORTANT, we do it each and every time”
- Should reduce “unintended” non-compliance
Should be used to encourage peers to speak up
- “That’s a Safety Absolute – we need to do it – I’ll help you”
Absolute: the highest priority for exact compliance
- Compliance must come before any other consideration, including revenue, speed or personal desire
There can still be unintended Safety Absolute violations or Safety Absolute errors driven by system problems
How Effectively have you Implemented Safety Absolutes?
Slide 72
Keys to Safety Coach Program Success
Executive Sponsorship (and expectations)
Engaged lead coach = engaged coaches
Effective Communication and agendas
Manager support - Get them to the monthly meetings! - Explain to your entire staff what they are all about - Reward and recognize them whenever possible - Meet with coaches monthly to discuss goods and
others
Recruit individuals who are well respected by their peers, good communicators and passionate about safety

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 37
Slide 73
Do you Measure the Safety Coach Program?
Qualified Safety Coaches by unit Attendance at monthly meetings Number of observations made monthly Linked to senior leader incentives
Do senior leaders and physicians at your institution truly understand and support the Safety Coach program?
Do they come to the Safety Coach meetings periodically and talk to
the Coaches as part of the monthly agenda?
Do they thank them in public venues for what they are doing?
Slide 74
Sustainment through Best Practice Cause Analysis

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 38
Slide 75
Best-Practice Cause Analysis Cause analysts trained in enhanced techniques Executive Sponsor & Operational Leader ownership Charter for event investigation 1:1 fact finding interviews Use of appropriate analytical cause tool - RCA, ECFC, ACA, CCA
Knowledge of failure mode taxonomies Transportability review Corrective Actions to Prevent Recurrence with single person accountability & operational ownership
Slide 76
Five Focus Areas for Cause Analysis Program Improvement
Enhance cause analysis methods and
capabilities
Refine cause analysis oversight
Implement robust lessons learned
program
Enhance safety event detection and
screening process
Integrate cause analysis concepts into
peer review
3
2
4
5 Enhance safety event detection and
screening process
1

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 39
Slide 77
Do you have an RCA Advisory Group?
Purpose Provide oversight and operational ownership
of the cause analysis program and organizational learning from events
Typical Members
- Chief Operating Officer - Chief Nursing Officer - Vice President of Medical Affairs - Patient Safety Officer - Director of Quality - Director of Risk Management
Slide 78
Role & Responsibilities
Know what “good root cause” looks like Establish a sense of urgency for root cause identification and root cause correction Ask questions to drive effective cause analysis and to determine if effective cause analysis has been conducted Keep board and senior leadership informed Promote organizational learning – we are hostages of each other Measure and communicate performance Monitor for fair and just response

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 40
Slide 79
RCA Advisory Group Metrics Report Safety Event Metrics 1. Event Counts
- # of safety events – SSE, PSE, NME
- # of JC sentinel events
- # of state reportable events
2. SSER
3. Days Since Last SSE - Point in time days since last
- Record run (longest days since last stretch)
4. Ratio of SSE to SSE+PSE (indicator of degree of harm)
5. # of SSE Discovered Through External Means
Cause Analysis Metrics 1. Total Events Reported 2. Cause Analysis Counts
- # RCA - # ACA
3. RCA Cycle Time (average days to complete an RCA)
4. CATPR Status & Effectiveness - # CATPR past due - % of actions still in place (of those
audited) 5. Organizational Learning
- Lessons Learned communicated - % Required Responses received
Slide 80
Do you Assign RCA Executive Sponsors? A senior leader who “owns” the quality of the overall RCA outcomes - to assure correct root
cause and corrective actions to prevent recurrence.
Responsibilities
Acts to stabilize the situation Charters the RCA Team Meets with RCA Team to discuss and agree on investigation scope and objectives Establishes priority and allocates resources Communicates investigation status Ultimately responsible for the root solution and implementation of corrective actions Addresses any issues team has with finalizing project Provides reports to hospital committees and other reporting groups
People Involved in the Event
RCA Team Sponsor
RCA Analyst Leader/Coordinator
Stakeholders & Subject Matter
Experts
RCA Analysts

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 41
Slide 81
Do you Write Team Charters?
A clear, careful, and specific problem statement created by team sponsor for RCA Project Team members
Charter should indicate: - Members of the team - Subject experts to be involved - Leadership to be involved - Timeframe for project to be
completed - Expectations regarding updates
on project status - Other related issues from
previous events to incorporate into analysis
Root Cause Analysis Investigation
RCA Team Charter Date: [Insert date] To: [Insert name]
Root Cause Analysis Team Leader From: [Insert name]
Root Cause Analysis Executive Sponsor Subject: Root Cause Analysis Team Charter for
[insert title] Thank you for agreeing to lead an interdisciplinary team to investigate the event [insert description] on [insert date] on [insert location]. I am asking that you conduct a formal root cause analysis of the described incident. You and the Root Cause Analysis Team Members [insert names of Analyst Team] are:
expected to make this investigation one of the top three priority actions of the day relieved of all other duties until the investigation is complete.
In addition to your RCA team members, the members of the Root Cause Analysis Project Group should also include:
[Name, Title] (department representative) [Name, Title] (subject matter expert) [Name, Title] [Name, Title]
Please add other expertise to the project team if you find it necessary. In your root cause analysis investigation, I am requesting a complete assessment of what happened, how it happened, and why it happened. Your report should include root causes and contributing factors, especially any failed system barriers and/or management barriers. Your report should address any generic implications of this occurrence to all other high-risk areas. Let me know as soon as possible if you identify any issues that need to be quickly communicated outside the department, even if you have not yet completed your analysis. Please provide me with regular progress briefings. I would like a detailed examination of internal and external operating experience. (For example: What opportunities did we fail to make use of to prevent this event? What lessons-learned did we overlook?) In particular, since this case addresses the broader issue of [insert details as appropriate], I would like you to address any recommendations that are relevant from a system perspective. When your analysis is completed, I request that you provide a briefing to senior leadership. Please notify me of any emergent issues associated with the investigation. I would like a final report including an action plan within 30 days. I will be responsible for communicating with the leadership team and to all external agencies. You and the Root Cause Analysis Project Team will be responsible for updating the department(s) involved. This charter may be revised by our mutual agreement. [Insert names of analysts], thank you for agreeing to participate in this activity and helping us to identify processes that will result in improved patient outcomes.
Slide 82
Do you use the Three Meeting Model? Operations Owns – Quality Supports
SOE = Sequence of Events CATPR = Corrective Actions to Prevent Recurrence
Investigate occurrence to
determine SOE & proximate causes
Determine failure scenario including
individual and system causal factors for each inappropriate act
Establish root causes and
conceptualize CATPR
Meeting #1 (Facts)
• Review Charter • Confirm scope of event • Identify & coordinate
interviews & data gathering
Meeting #2 (Causes)
• Agree on facts & proximate causes
• Build consensus for possible root causes
RCA Sponsor, Stakeholders & Subject Matter Experts
RCA Analyst Team
• Stabilize situation
• Control evidence
Meeting #3 (Corrections)
• Consensus on root causes
• Finalize Corrective Action plan
RCA Team

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 42
Slide 83
Do you use Events and Causal Factor Charting to get from Proximate to Root Cause?
A high fall risk patient was undergoing bedside physical therapy. The physical therapist was assisting the patient back to bed when a nurse stopped by to talk to the therapist about another patient. The PT and RN walked out of the room without turning
bed alarm back on. Ten minutes later, patient found on floor by tech with a fractured wrist.
Therapist walks out of
room with RN and does not
re-engage bed alarm
Was distracted by conversation
with RN
No visual reminder in room about bed alarm
No prompt on therapy record
to check for bed alarm
Organization did not create situational awareness
regarding fall precautions for ALL care team members
Individual Failure (her individual reason
for doing what she did)
System Failures (how the system
influenced her actions)
Root Cause
WHY?
WHY?
WHY?
PROXIMATE CAUSE (inappropriate action)
Slide 84
Do you Monitor for Action Plan Completion?
Close the
Loop
Create control loop through Executive Owner • Action item owners must report to the executive owner when the
action items are completed
Create database of required actions and issue periodic reports • Action item owners enter completion information directly into report
or action plan on shared drive; executive owner reviews for completion.
Review action plan completion at senior leadership, RCA Advisory Group or other safety oversight meetings Ensure periodic audits are conducted to monitor for effectiveness and sustainment of corrective actions

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 43
Slide 85
Summary and Wrap Up
Slide 86
1. Safety is a core value and fundamental to our mission.
2. Harm happens on our watch, in our hospital.
3. Serious harm events are preventable and a continuous journey towards ZERO is the only acceptable goal.
4. We improve reliability and safety by the right mix of process, people and system design.
5. It will take everyone: Board, senior leaders, operational leaders, staff and physicians.
What Does It Take?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 44
Slide 87
What Do I Need to Do? Review SSER data quarterly and put a face on safety Propose Safety and Quality Aims “Aim High, Aim Wide, take Dead Aim”, for example:
“We will reduce Serious Safety Events by 80% across the entire institution in the next three years”
Develop and Approve Safety and Quality Improvement Plan to achieve Aim
Hospital Boards
Set the bar Challenge leaders Safety first in decisions
Slide 88
Deliver a safety message through electronic or other means (newsletter) to all associates Measure, teach, reinforce, role model and inspire staff to make safety a core value
- Start meetings with Safety Moments - Thank those who voice safety concerns - Put Safety First in decision making
Conduct a Daily Safety Huddle with Directors and/or Managers Conduct weekly Rounds to Influence
Ask about errors and great catches Ask about conditions that make staff most concerned they will make an error or mistake that could result in harm to a patient or employee? Ask staff to report errors and make a commitment to them to establish a fair and just culture
Conduct monthly RCA oversight meetings Receive update on latest SSER and days since last event Review outstanding RCAs (including action plans and status) Review progress on process indicators and action plan that support safety and quality transformation
Hospital Leaders
Set the tone Relentless Drumbeat Personal Involvement Put a Face on Safety
What Do I Need to Do?

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 45
Slide 89
Step 1: Set Expectations Define concrete and prescriptive Safety
Behaviors & Error Prevention Tools proven to help reduce human error
Step 2: Educate & Train Educate and build skills in the use of the
Safety Behaviors and Error Prevention Tools Step 3: Reinforce & Build
Accountability Practice the Safety Behaviors and Tools
while making them personal work habits
Clinical and Non-clinical Staff
What Do I Need to Do?
Slide 90
1. Serve as good role models
Exhibit safe behaviors in everyday work 2. Provide 5:1 Feedback
Positively reinforce safe and reliable practices on the part of staff and colleagues Coach staff and colleagues real-time when you see the opportunity
3. Have high standards and promote professional atmospheres
Provide a safety and reliability perspective in medical staff meetings, medical group meetings or informal gathering of colleagues Share stories to reinforce importance of patient safety while also providing relevant information
4. Work with nurse leaders, administrative leaders and front line staff toward a common purpose
What Do I Need to Do? Physicians and Providers

Healthcare Performance Improvement, LLC Phone: 757.226.7479 Fax: 757.226.7478 www.hpiresults.com
Page 46
Slide 91
Healthcare Performance Improvement 5041 Corporate Woods Drive, Suite 180 | Virginia Beach, VA 23462
Tel: (757) 226-7479 • www.hpiresults.com
The HPI Team
Steve Kreiser Senior Consultant Cell: (757) 353-7833 • [email protected]







• Every employee has the goal to demonstrate mastery of EP tools by providing evidence of the use of 4 different tools as they apply to their scope of work.
• The attached document was developed for staff to document their accomplishments to be submitted to their manager (some expect it quarterly, others just want 4/yr). Or they can enter it directly into the electronic system for performance management.
• All of the Recruiters ask at least one Patient Safety question of all applicants: “Tell me about a time when you observed a situation where a patient could have been harmed. What did you do? What was the result?”

Error Prevention Tool Quarterly Report
Name Date Select the quarter of submission:
First Quarter Second Quarter Third Quarter Fourth Quarter 2013
A different example must be used for each quarter
Select the Error Prevention Tool and explain how you specifically used the tool:
Attention to detail – We focus our attention to always think before we act, especially in high risk situations. Self checking using STAR.
StopThink Act Review
Communicate Clearly – We’re responsible for professional, clear, and complete verbal and written communication.
3 way Repeat Back & Read Back Phonetic and Numeric Clarifications Clarifying Questions
Handoff Effectively – We provide effective handoffs of patient, tasks, and materials by taking the time to give appropriate information and ensuring understanding and ownership.
SituationBackground Assessment Recommendation
Speak up for Safety – We use good judgment at all times to ensure our actions are the best. We use an assertion and escalation technique to act on a responsibility to protect patients & co-workers in a manner of mutual respect.
Question & Confirm Use ARCC to escalate safety concerns
Ask a Question Make a Request Voice a Concern Use Chain of Command
Stop the Line
Got your Back! – We make reliability by building our own sound practice habits and in our co-workers. We’re accountable not just for our own actions by for our teammates’ as well.
Peer Checking Peer Coaching
Utilize the space below to explain how you utilized the error prevention tool….

Tips for Leaders• Redirect unrelated reports and conversation• Give clear direction about prioritization• For issues, identify a single Problem Owner and time
for resolution (“page me by 3:00 this afternoon if the equipment has not been fixed”)
Lines for Leadersto encourage high-reliability thinking• How do you know you had no problems?• What immediate actions did you take?• Is this happening in other places? Could this happen
in other places?• What other areas does this impact?• How are you preparing your team for that task?• What Safety Behavior error prevention technique
should be used?If any deficiencies that impact safe care:• That’s a Safety Critical Issue that requires Rapid
Response…
We huddle at the start of the day to maintain situational awareness of immediate problems impacting SAFETY & QUALITY of patient care at the front line.
We give direction about priority and responsibility for problem resolution.
Daily Check-InAn HPI Leadership Method for Performance Excellence
Daily Check-In Agenda1. LOOK BACK – Significant safety or quality
issues from the last 24 hours/last shift
2. LOOK AHEAD – Anticipated safety or quality issues in next 24 hours/next shift
3. Follow up on Start-the-Clock Safety Critical Issues
How We Do It• Include direct reports and others who know the status of operations in your areas of responsibility.• Establish a standing time. Schedule the time on your calendar and stick to it.• Keep it short – 10 to 15 minutes at the most – and hold it as a “stand-up” meeting.• Keep it focused. Follow a routine, 3-point agenda:
Prepare to ParticipateConsider yourself and ask others:• Do we have any high-risk patients or
procedures?• Do we anticipate any non-routine procedures or
tasks?• Are we dealing with any situations or conditions
that distract our ability to focus or think critically about our patients?
• Are there any safety issues that I know about that may impact other departments?
• Do we have what we need to deliver safe, quality care? Are there any deficiencies in information, equipment, supplies, or staff that will make it hard to deliver safe, high quality care?
• What conditions outside our unit or outside our hospital could impact our ability to deliver safe, quality care today?
If any of the above…What actions am I taking to have a safe day?If no issues…
We have what it takes toCreate a Safe Day
Mobilize to solve safety-critical issues or deficiencies:1. Identify the Problem Owner and experts2. State time to resolve with a “start-the-clock” sense
of urgency – how quickly can we close this hole in the Swiss cheese
3. Add issue to a “start-the-clock” follow-up list
Start-the-Clock Safety Critical Issues
Revision 0, December 2008© 2008 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.


Rel
iabi
lity
& S
afet
y Tr
ansf
orm
atio
n M
etric
s
Des
ired
Dire
ctio
nP
rior
Yea
rC
urre
ntY
ear
Goa
l
AH
RQ
Sur
vey
on P
atie
nt S
afet
y C
ultu
reO
vera
ll P
erce
ptio
n of
Saf
ety
Man
agem
ent S
uppo
rt fo
r Saf
ety
Sup
ervi
sor S
uppo
rt fo
r Saf
ety
Team
wor
k A
cros
s U
nits
Non
-pun
itive
Res
pons
e to
Err
or
Des
ired
Dire
ctio
nP
rior
Yea
rJa
nFe
bM
arAp
rM
ayJu
nJu
lAu
gS
ep
Oct
Nov
Dec
YTD
Goa
l
% o
f lea
ders
who
com
plet
ed
initi
al e
rror
pre
vent
ion
educ
atio
n%
of s
taff
who
com
plet
ed
initi
al e
rror
pre
vent
ion
educ
atio
n%
of m
edic
al s
taff
who
com
plet
ed
initi
al e
rror
pre
vent
ion
educ
atio
nN
umbe
r of S
afet
y S
ucce
ss S
torie
s sh
ared
0N
umbe
r of S
afet
y C
oach
es0
Num
ber o
f Saf
ety
Coa
ch O
bser
vatio
ns0
Pra
ctic
e E
ffect
iven
ess
- Hig
h-R
elia
bilit
y Le
ader
Met
hods
S
corin
g G
uide
lines
on
Tab
#2 R
ows
4-27
Mes
sage
on
Mis
sion
- S
afet
y Fi
rst
Dai
ly S
afet
y C
heck
-In -
Faci
lity-
Wid
eD
aily
Saf
ety
Che
ck-In
- D
epar
tmen
t-Bas
edTo
p Te
n Li
stR
ound
ing
To In
fluen
ceFa
ir C
ultu
reP
ract
ice
Effe
ctiv
enes
s - E
rror
Pre
vent
ion
Beh
avio
rsS
corin
g G
uide
lines
on
Tab
#2 R
ows
29-3
8S
TAR
Com
mun
icat
ion
Cla
rifie
rsH
ando
ffsS
BA
RV
alid
ate
and
Ver
ifyTe
am C
heck
ing
Team
Coa
chin
gS
peak
Up
for S
afet
yN
umbe
r of S
afet
y A
bsol
ute
Vio
latio
ns
Des
ired
Dire
ctio
nB
asel
ine
Bas
elin
eD
ate
Prio
rY
ear
Jan
Feb
Mar
Apr
May
Jun
Jul
Aug
Sep
O
ctN
ovD
ecY
TDG
oal
Ser
ious
Saf
ety
Eve
nt R
ate
(SS
ER
)To
tal S
erio
us S
afet
y E
vent
s0
Tota
l Pre
curs
or S
afet
y E
vent
s0
Tota
l Eve
nt R
epor
ts0
Rat
io o
f SS
E to
SS
E +
PS
E#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!#D
IV/0
!N
umbe
r of I
ncid
ents
/Eve
nts
Rep
orte
d0
Em
ploy
ee In
jury
& Il
lnes
s R
ate
Em
ploy
ee D
ays
Aw
ay R
estri
cted
& T
rans
ferr
edN
umbe
r of P
rofe
ssio
nal L
iabi
lity
Cla
ims
& S
uits
0V
alue
of L
iabi
lity
Cla
ims
& S
ettle
men
ts$0
Lead
ing
Indi
cato
rs (P
redi
ctiv
e P
erfo
rman
ce M
easu
res)
Rea
l-Tim
e In
dica
tors
(Pro
cess
Mea
sure
s)
Lagg
ing
Indi
cato
rs (O
utco
me
Mea
sure
s)
Org
aniz
atio
n N
ame
Rep
ort A
s O
f [D
ate]
Ent
er o
rgan
izat
ion-
spec
ific
conf
iden
tialit
y st
atem
ent
Rel
iabi
lity
Impl
emen
tatio
n &
Sus
tain
abili
tyIn
dexS
M(R
ISI)
HP
I Rel
iabi
lity
Impl
emen
tatio
n S
usta
inab
ility
Inde
x (R
evis
ion
0, S
epte
mbe
r 201
4)©
201
4 H
ealth
care
Per
form
ance
Impr
ovem
ent,
LLC
. ALL
RIG
HTS
RE
SE
RV
ED
.