
Congenital unilateral pulmonary vein stenosis complicating transposition of the great arteries
6
CongenitalUnilateral Pulmonary Vein StenosisComplicating Transposition of the Great Arteries MICHAEL VOGEL, MD, JUDITH ASH, MD, RICHARD D. ROWE, MD, GEORGE A. TRUSLER, MD, and MARLENE RABINOVITCH, MD Four patients with transposition of the great arteries and unilateral pulmonary vein (PV) stenosis, all left-sided, were studied. Two patients had an intact ventricular septum (1 with a patent ductus arterio- sus), 1 patient had a ventricular septal defect and 1 had a ventricular septal defect with pulmonary stenosis. Clinical signs, such as recurrent pneu- monia, unilateral pulmonary edema and pleural effusion, were present preoperatively in 2 patients. Dtagnosis was made at cardiac catheterization by cineangiography in 2 patients and at Mustard op- eration when the PV orifices were inspected in the other 2. PV dilatation was attempted in 3 patients, 1 before correction (age 6 months), 1 during and after it (ages 1 and 3 years, respectively) and 1 during corrective surgery (age 15 months). In the fourth patient only the intracardiac baffle was en- larged near the left PV orifices. In the first patient, at Mustard operation (age 16 months), onty a fibrotic PV without an orifice was found; this patient died after surgery. The mean follow-up in the 3 survivors was 3.2 years (range 2 months to 7.6 years). All have severe residual PV obstruction documented by technetium-99m lung perfusion scans that show decreased flow to the lefl lung (0 to 16% total counts; normal 45 % ); 2 have unilateral pulmonary edema and 1 has pulmonary artery pressure at systemic level. It is believed that in patients wlth transposition of the great arteries, left-sided uni- lateral PV stenosis is a congenital anomaly that becomes progressive as a result of postnatal pref- erential flow to the right lung. (Am J Cardiol 1964;54:166-171) Congenital stenosis of the orifice of a pulmonary vein (PV) was first described in 1951.l Four years later, a study of a patient with unilateral PV stenosis followed2 and since then 17 cases of unilateral PV stenosis2l5 and 11 cases of unilateral PV atresia1620 have been reported. Only once has this condition been associated with transposition of the great arteries (TGA),ls and the patient reported had PV atresia. We report 4 additional patients with TGA and describe how associated con- genital unilateral PV stenosis complicated surgical management and subsequent clinical course. Methods Patients: Records of approximately 30,000 patients with congenital heart disease diagnosed since 1951 are available at The Hospital for Sick Children, Toronto. From these we identified 7 patients with congenital unilateral PV stenosis: From the Departments of Cardiology, Cardiovascular Surgery and Nu- clear Medicine, The Hospital for Sick Children, and the Departments of Pediatrics, Radiology and Surgery, University of Toronto, Toronto, Ontario, Canada. Manuscript received November 15, 1983; revised manuscript received March 20, 1984, accepted March 22, 1984. Address for reprints: Marlene Rabinovitch, MD, Department of Car- diology, The Hospital for Sick Chilben, 555 University Avenue, Toronto, Ontario, Canada M5G 1X8. 166 1 with a structurally normal heart, 2 with anomalous PV drainage and 4 with TGA. The latter form the basis of this report. They come from a consecutive series of 649 patients with TGA (incidence rate, 0.6%). Cardiac catheter studies: Cardiac catheterization studies were performed in the newborn period and before Mustard operation in all 4 patients and also after surgical repair in 2. Patients older than 6 months were sedated with an intra- muscular injection of CMs, a compound that contains phen- ergan, demerol and chlorpromazine, at a dosage of 0.1 ml/kg, intramuscularly. Pressures were recorded using standard fluid-filled catheters. Left ventricular cineangiography was performed routinely in the anteroposterior and lateral pro- jections; to better visualize the pulmonary arteries, the sit- ting-up projection21 was used in 2 patients. Radionuclide lung scans: Lung scans were performed without sedation with the patient sitting up. To assess ven- tilation, the patient breathed a gas-oxygen mixture that contained 10 mCi of xenon-133 through a closed system. The equilibrium phase and washout were recorded with a Picker 5-10 gamma camera interfaced to a MDS As computer. Per- fusion was subsequently assessed after a right antecubital injection of 0.23 mCi/kg of technetium99m macroaggregated albumin. Pulmonary vein measurements: Pulmonary vein mea- surements in 1 age-matched patient with a structurally normal
-
Upload
michael-vogel -
Category
Documents
-
view
215 -
download
0
Transcript of Congenital unilateral pulmonary vein stenosis complicating transposition of the great arteries

Congenital Unilateral Pulmonary Vein Stenosis Complicating Transposition of the Great Arteries
MICHAEL VOGEL, MD, JUDITH ASH, MD, RICHARD D. ROWE, MD,
GEORGE A. TRUSLER, MD, and MARLENE RABINOVITCH, MD
Four patients with transposition of the great arteries and unilateral pulmonary vein (PV) stenosis, all left-sided, were studied. Two patients had an intact ventricular septum (1 with a patent ductus arterio- sus), 1 patient had a ventricular septal defect and 1 had a ventricular septal defect with pulmonary stenosis. Clinical signs, such as recurrent pneu- monia, unilateral pulmonary edema and pleural effusion, were present preoperatively in 2 patients. Dtagnosis was made at cardiac catheterization by cineangiography in 2 patients and at Mustard op- eration when the PV orifices were inspected in the other 2. PV dilatation was attempted in 3 patients, 1 before correction (age 6 months), 1 during and after it (ages 1 and 3 years, respectively) and 1 during corrective surgery (age 15 months). In the fourth patient only the intracardiac baffle was en-
larged near the left PV orifices. In the first patient, at Mustard operation (age 16 months), onty a fibrotic PV without an orifice was found; this patient died after surgery. The mean follow-up in the 3 survivors was 3.2 years (range 2 months to 7.6 years). All have severe residual PV obstruction documented by technetium-99m lung perfusion scans that show decreased flow to the lefl lung (0 to 16% total counts; normal 45 % ); 2 have unilateral pulmonary edema and 1 has pulmonary artery pressure at systemic level. It is believed that in patients wlth transposition of the great arteries, left-sided uni- lateral PV stenosis is a congenital anomaly that becomes progressive as a result of postnatal pref- erential flow to the right lung.
(Am J Cardiol 1964;54:166-171)
Congenital stenosis of the orifice of a pulmonary vein (PV) was first described in 1951.l Four years later, a study of a patient with unilateral PV stenosis followed2 and since then 17 cases of unilateral PV stenosis2l5 and 11 cases of unilateral PV atresia1620 have been reported. Only once has this condition been associated with transposition of the great arteries (TGA),ls and the patient reported had PV atresia. We report 4 additional patients with TGA and describe how associated con- genital unilateral PV stenosis complicated surgical management and subsequent clinical course.
Methods
Patients: Records of approximately 30,000 patients with congenital heart disease diagnosed since 1951 are available at The Hospital for Sick Children, Toronto. From these we identified 7 patients with congenital unilateral PV stenosis:
From the Departments of Cardiology, Cardiovascular Surgery and Nu- clear Medicine, The Hospital for Sick Children, and the Departments of Pediatrics, Radiology and Surgery, University of Toronto, Toronto, Ontario, Canada. Manuscript received November 15, 1983; revised manuscript received March 20, 1984, accepted March 22, 1984.
Address for reprints: Marlene Rabinovitch, MD, Department of Car- diology, The Hospital for Sick Chilben, 555 University Avenue, Toronto, Ontario, Canada M5G 1X8.
166
1 with a structurally normal heart, 2 with anomalous PV drainage and 4 with TGA. The latter form the basis of this report. They come from a consecutive series of 649 patients with TGA (incidence rate, 0.6%).
Cardiac catheter studies: Cardiac catheterization studies were performed in the newborn period and before Mustard operation in all 4 patients and also after surgical repair in 2. Patients older than 6 months were sedated with an intra- muscular injection of CMs, a compound that contains phen- ergan, demerol and chlorpromazine, at a dosage of 0.1 ml/kg, intramuscularly. Pressures were recorded using standard fluid-filled catheters. Left ventricular cineangiography was performed routinely in the anteroposterior and lateral pro- jections; to better visualize the pulmonary arteries, the sit- ting-up projection21 was used in 2 patients.
Radionuclide lung scans: Lung scans were performed without sedation with the patient sitting up. To assess ven- tilation, the patient breathed a gas-oxygen mixture that contained 10 mCi of xenon-133 through a closed system. The equilibrium phase and washout were recorded with a Picker 5-10 gamma camera interfaced to a MDS As computer. Per- fusion was subsequently assessed after a right antecubital injection of 0.23 mCi/kg of technetium99m macroaggregated albumin.
Pulmonary vein measurements: Pulmonary vein mea- surements in 1 age-matched patient with a structurally normal
July 1, 1984 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 54 167
TABLE I Pulmonary Vein Measurement at Autopsy in Age- Matched Patllents*
Pulmonary Vein Lumen
Age at Diameter Autopsy Diagnosis Cause of Death (mm)
2 days Complete heari Heart failure LUPV 7 block LLPV 6
7 days TGA, PDA Heart failure LUPV 7 LLPV 6
2mo TGA, VSD, PA lband Died at operation LUPV 7 PDA ligation LLPV 7
8mo TGA, after Blalock- Endocarditis LUPV 9 Hanlon procedure LLPV 8
11 mo TGA, Mustard Died after mustard LUPV 11
I’/* yr operation operation LLPV 10
TGA, VSD, PDA Heart failure LUPV 8 LLPV 6
l Measurements taken on specimens, which were previously fixed in formalin.
LLPV = lefl lower pulmonuy vein; LUPV = left upper pulmonary vein; PA = pulmonary artery: PDA = patent ductus atteriosus; TGA = transposition of the great arteries; VSD = ventricular septal defect.
heart but congenital complete heart block and in 5 patients with TGA are listed in T,sble I. All these hearts had been fied in formalin, so that the size of the pulmonary veins measured was probably somewhat underestimated; measurements of the PV in our 4 patients were done in vivo.
Resuks (Tables I to Ill)
Case 1: Catheteriz,ation on the first day of life re- vealed TGA with intact ventricular septum and a small patent ductus arteriosus (PDA). A balloon atria1 sep- tostomy was performed, but because of inadequate mixing, a Blalock-Hanlon septectomy was performed 2 weeks later. By the time of elective cardiac catheter- ization before the Mustard procedure, the PDA had closed and left ventricular and pulmonary artery pres- gures were normal.
At age 1 year a Mustard repair was done and poat- operatively the child had recurrent left pleural effusions. Cardiac catheterization revealed prolonged transit of contrast material through the left pulmonary vascular bed and significant elevation in left pulmonary artery wedge pressure suggesting obstruction to the left-sided PVs. Reoperation was carried out. The interatrial pericardial baffle was found to be narrowed at the left PV orifices (4 mm) and the size of the PV orifices themselves were reduced. The left lower PV was 5 to 6 mm in diameter; the left uljper PV branched at the point of entrance to the atrium and each branch was narrowed, measuring 2 to 3 mm in diameter. The in- traarterial baffle was :revised and the PV channel was enlarged to 10 mm. Subsequently, the left pleural effusions regressed slowly.
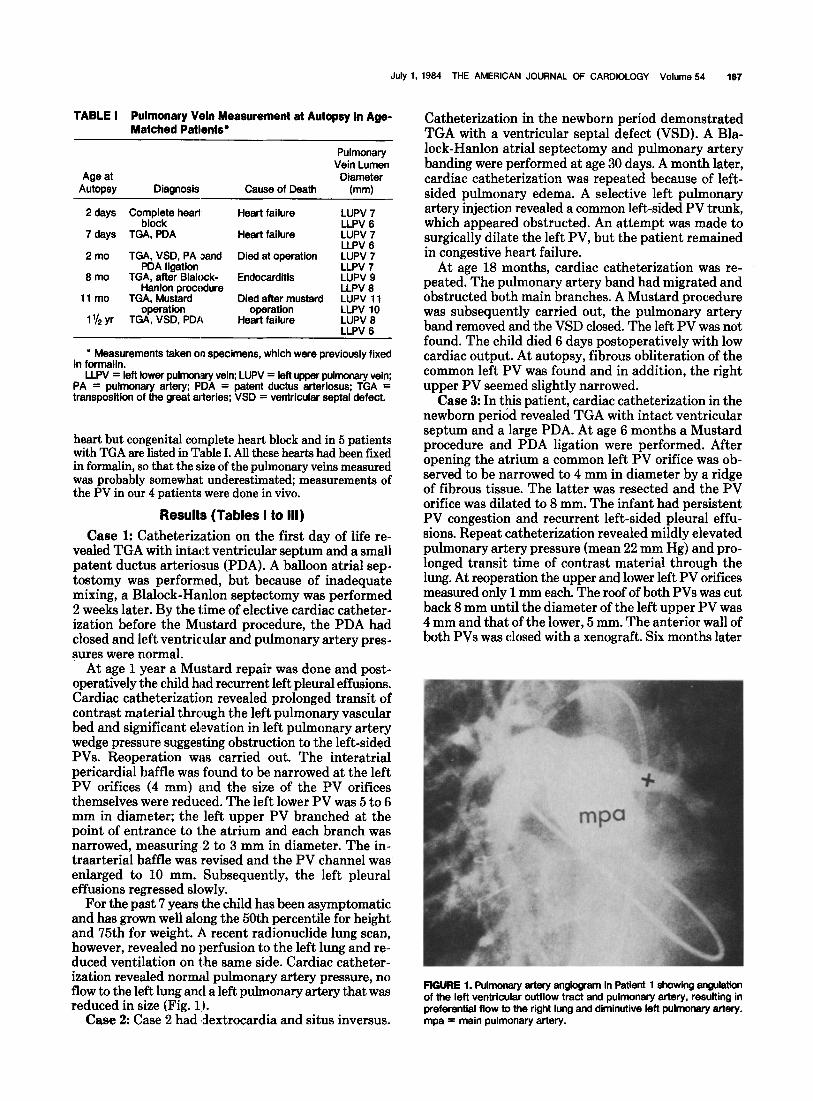
For the past 7 years the child has been asymptomatic and has grown well along the 50th percentile for height and 75th for weight. A recent radionuclide lung scan, however, revealed no perfusion to the left lung and re- duced ventilation on the same side. Cardiac catheter- ization revealed normal pulmonary artery pressure, no flow to the left lung and a left pulmonary artery that was reduced in size (Fig. 1).
Case 2: Case 2 had ldextrocardia and situs inversus.
Catheterization in the newborn period demonstrated TGA with a ventricular septal defect (VSD). A Bla- lock-Hanlon atria1 septectomy and pulmonary artery banding were performed at age 30 days. A month later, cardiac catheterization was repeated because of left- sided pulmonary edema. A selective left pulmonary artery injection revealed a common left-sided PV trunk, which appeared obstructed. An attempt was made to surgically dilate the left PV, but the patient remained in congestive heart failure.
At age 18 months, cardiac catheterization was re- peated. The pulmonary artery band had migrated and obstructed both main branches. A Mustard procedure was subsequently carried out, the pulmonary artery band removed and the VSD closed. The left PV was not found. The child died 6 days postoperatively with low cardiac output. At autopsy, fibrous obliteration of the common left PV was found and in addition, the right upper PV seemed slightly narrowed.
Case 3: In this patient, cardiac catheterization in the newborn peridd revealed TGA with intact ventricular septum and a large PDA. At age 6 months a Mustard procedure and PDA ligation were performed. After opening the atrium a common left PV orifice was ob- served to be narrowed to 4 mm in diameter by a ridge of fibrous tissue. The latter was resected and the PV orifice was dilated to 8 mm. The infant had persistent PV congestion and recurrent left-aided pleural effu- sions. Repeat catheterization revealed mildly elevated pulmonary artery pressure (mean 22 mm Hg) and pro- longed transit time of contrast material through the lung. At reoperation the upper and lower left PV orifices measured only 1 mm each. The roof of both PVs was cut back 8 mm until the diameter of the left upper PV was 4 mm and that of the lower, 5 mm. The anterior wall of both PVs was closed with a xenograft. Six months later
FIGURE 1. Pulmonary artery anglogram in Patient 1 showing anguiation of the left ventricular outflow tract and pulmonary artery, resulting in preferential flow to the right lung and diminutive IefI pulmonary artery. mpa = main pulmonary artery.
168 PULMONARY VEIN STENOSIS IN TRANSPOSITION
TABLE II Hemodynamic Data in Patlents with Transposttlon of the Great Arteries and Pulmonary Vein Steno&
Arterial Blood Gas
Case Age at study
Saturation Aorta
(%) RV
Pressure (S/D) (mm Hg)
LV Ao PA LPC RPC pH
PCO* PO*
(mm Hg)
1 TdaY 7mo 2 yr
9% yr 2
K:
1.5 yr 73 8518 8512 85185
3 l&Y 8mo 2”/4 yr 5 I8 yr Room air 100% FlO2
4 1daY 4mo 8mo 10015
. . .
. . . 12015
. . . 83131 95155
. . . 28117
5 . . . 7.31 48 82 . . . . . . 7.25 54 180
. . . . . . . . . . . . . . .
. . . . . . . . . . . . . . .
. . . . . . . . . . . . . . .
Ao = aorta: LPA = left pulmonary artery; LPC = left pulmonary capillary; LV = left ventricle; PA = pulmonary artery; RPA = right pulmonary artery; RPC = right pulmonary capillary; RV = right ventricle; S/D = systolic/diastolic.
Ei 97
94
i:
;: 95
tt
tt :8 10015
aata 7512
55110 5317 100/12 95112
8817 4213
55138
88148 4019
10018 8018 100/50 78140 110/a lOOl8 I lot88 100185
3818 84147 2113 81151 3013 100/50
2513 105155
80112 75/53 7815 75/50
1517 LPA 28/l 1 RPA 23111
1817
Distal band: LPA 1718 RPA 3715
Proximal band: 7817
Proximal band: 85120
. . . . . . 7.27 :: 19
. . . . . . 7.38 ‘1’9’ ‘i’ 7.33 41 1::
. . . 8 7.38 45 83
... ... ...
... ... ...
.........
...... 7.38
...... 7.44 38 x:
...... 7.35 3x 87
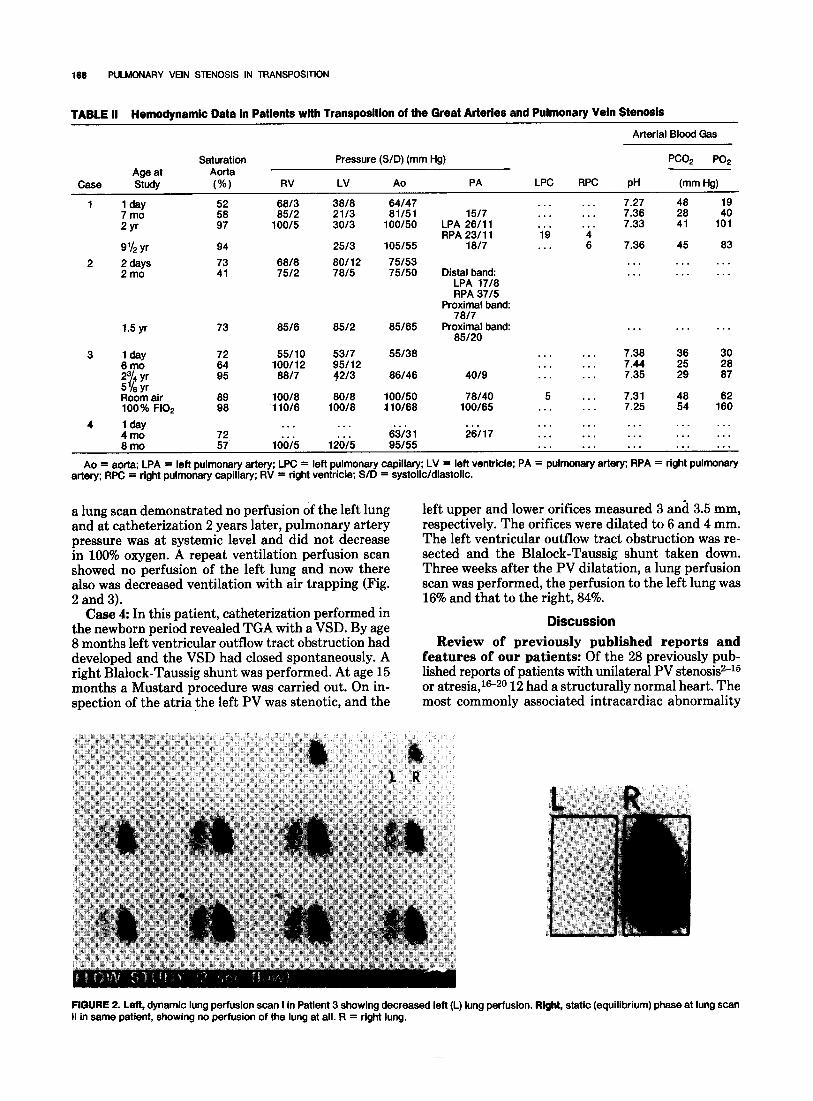
a lung scan demonstrated no perfusion of the left lung and at catheterization 2 years later, pulmonary artery pressure was at systemic level and did not decrease in 100% oxygen. A repeat ventilation perfusion scan showed no perfusion of the left lung and now there fso;; decreased ventilation with air trapping (Fig.
. Case 4: In this patient, catheterization performed in
the newborn period revealed TGA with a VSD. By age 8 months left ventricular outflow tract obstruction had developed and the VSD had closed spontaneously. A right Blalock-Taussig shunt was performed. At age 15 months a Mustard procedure was carried out. On in- spection of the atria the left PV was stenotic, and the
left upper and lower orifices measured 3 and 3.5 mm, respectively. The orifices were dilated to 6 and 4 mm. The left ventricular outflow tract obstruction was re- sected and the Blalock-Taussig shunt taken down. Three weeks after the PV dilatation, a lung perfusion scan was performed, the perfusion to the left lung was 16% and that to the right, 84%.
Discussion
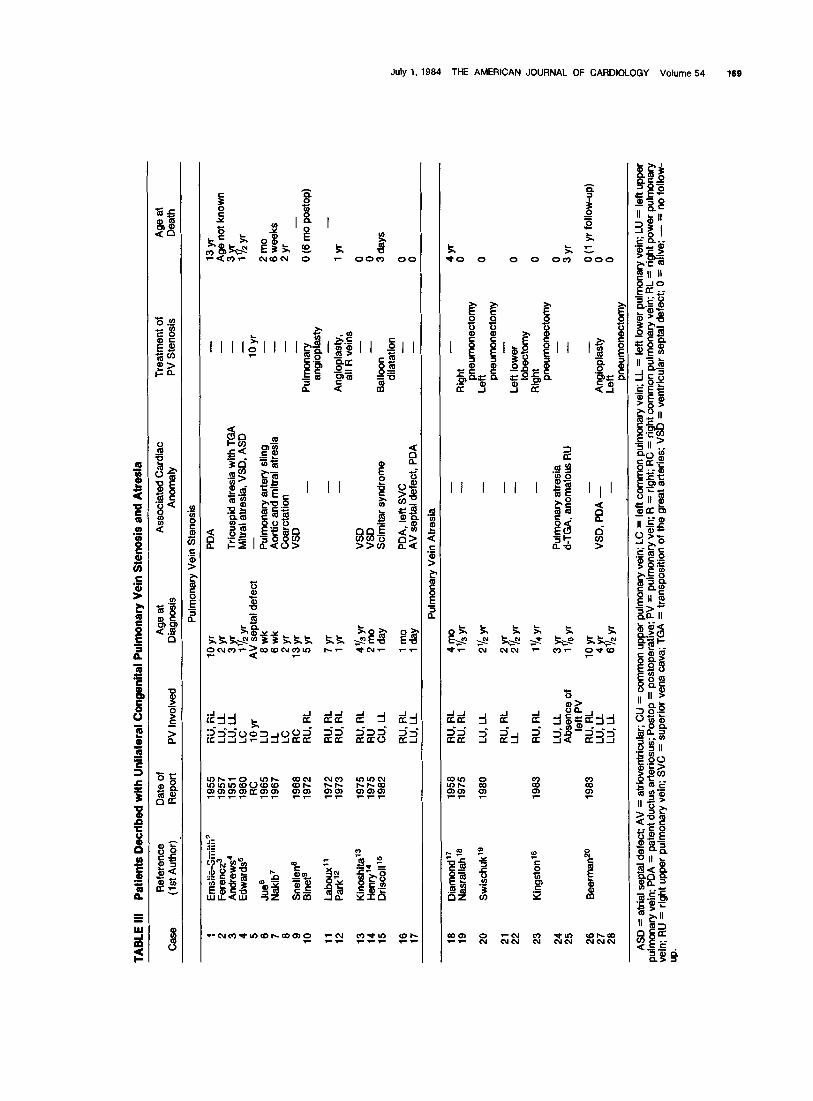
Review of previously published reports and features of our patients: Of the 28 previously pub- lished reports of patients with unilateral PV stenosiss-15 or atresia,i6-20 12 had a structurally normal heart. The most commonly associated intracardiac abnormality
FIGURE 2. Left, dynamic lung perfusion scan I in Patient 3 showing decreased left (L) lung perfusion. Right, static (equilibrium) phase at lung scan II in same patient, showing no perfusion of the lung at all. R = right lung.
TA
BL
E I
II P
atie
nts
Dec
rib
ed
wit
h U
nila
tera
l C
on
gen
ital
P
ulm
on
ary
Vei
n S
ten
osi
s an
d A
tres
ia
Ref
eren
ce
Dat
e of
A
ge
at
Ass
ocia
ted
Car
diac
T
reat
men
t of
A
ge a
t
Cas
e (1
st A
utho
r)
Rep
ort
PV
Inv
olve
d D
iagn
osis
A
nom
aly
PV
Ste
nosi
s D
eath
Pul
mon
ary
Vei
n S
teno
sis
Eii
iSlk
-Sii
iiih
’
Fer
encz
3 A
ndre
ws’
E
dwar
ds5
Jlle
s N
akib
7
..-.C
.-
lJO
P
1957
19
51
1960
R
C
1965
19
67
Sne
llet+
19
66
Bin
ets
1972
1972
R
U,
RL
1973
R
U,
RL
Kin
oshi
ta13
19
75
Hen
ry14
19
75
Dri
scol
l l5
19
62
k RC
R
U,
RL
RU
, R
L
z.
LL
i9
yr
f ‘: Y
1 I2
yr
AV
se
ptal
de
fect
6w
k 6w
k 2
yr
13yr
5
yr
7 yr
1
yr
;%,y
t&Y
--_
WJA
Tri
cusp
id
atre
sia
with
T
GA
M
itral
at
resl
a,
VS
D,
AS
D
- Pul
mon
ary
arte
ry
slin
g A
ortic
an
d m
itral
at
resi
a
- - - loyr
- -
Coa
rcta
tion
-
VS
D
- - - -
VS
D
VS
D
Sci
mita
r sy
ndro
me
Pul
mon
ary
angi
opla
sty
- A
ngio
plas
ty,
all
R v
eins
-
Bal
loon
-
dila
tatio
n
13yr
A
ge
not
know
n
3Yr
1 l2yr
2mo
6 w
eeks
2
yr
- 0
(6 m
o po
stop
)
lyr
-
0 0 3 da
ys
16
17
rtU
J.R
$ 1
mo
PD
A,
left
SV
C
- 0
1 da
y A
V
sept
al
defe
ct,
PD
A
- 0
Pul
mon
ary
Vei
n A
tres
ia
:x
20
f :
23
a”s
tt 28
Dia
mon
d17
1958
N
asra
llah’
* 19
75
Sw
isch
uk’s
19
80
Kin
gsto
n1B
19
83
Bee
rman
zO
1983
RU
, R
L 4m
o -
- 4
yr
RU
, R
L 1
‘Is y
r -
Rig
ht
0 pn
eum
onec
tom
y LU
, LL
2%
yr
- Le
ft 0
pneu
mon
ecto
my
RU
, R
L 2Y
r -
-
LL
2 I2
yr
- Le
ft lo
wer
0
lobe
ctom
y R
U,
RL
1’14
yr
- R
ight
0
pneu
mon
ecto
my
LU,
LL
3Yr
Pul
mon
ary
atre
sia
- 0
Abs
ence
of
1
lsyr
d-
TG
A,
anom
alou
s R
U
- 3
yr
left
PV
R
U,
RL
10 y
r -
0 (1
yr
follo
w-u
p)
LU,
LL
VS
D,
PD
A =
LU
, LL
4Y
r 6
1s yr
-
$iop
last
y 8
pneu
mon
ecto
my
AS
D
=
atria
l se
ptal
def
ect;
AV
=
at
riove
ntric
ular
; C
U =
co
mm
on
uppe
r pu
lmon
ary
vein
; LC
=
left
com
mon
pu
lmon
ary
vein
; LL
=
left
low
er
pulm
onar
y ve
in;
LU =
le
ft up
per
pulm
onar
y ve
in;
WA
=
pa
tent
du
ctus
ar
terio
sus;
P
osto
p =
po
stop
erat
ive;
P
V =
pu
lmon
ary
vein
; R
=
right
; R
C =
rig
ht c
omm
on
pulm
onar
y ve
in;
RL
=
right
po
wer
pu
lmon
ary
vein
; R
U =
rig
ht
uppe
r pu
lmon
ary
vein
; S
VC
=
su
perio
r ve
na
cava
; T
GA
=
tr
ansp
ositi
on
of t
he
grea
t ar
terie
s;
VS
D
=
vent
ricul
ar
sept
al
defe
ct;
0 =
al
ive;
-
=
no f
ollo
w-
up.
170 PULMONARY VEIN STENOSIS IN TRANSPOSITION
was a VSD, which was present in 4 patients. Although there appears in general to be an equal distribution of left- and right-sided obstructions, 3 of the 4 patients with VSD had a right-sided obstruction. We describe 4 patients with an uncommonly associated intracardiac abnormality-TGA. Moreover, the location of the ob- struction was consistently left-sided.
In almost all previously reported cases the patients died; 3 of 4 of our patients are alive and are being fol- lowed in our department. Reported symptoms of PV stenosis include hemoptysis,sJiJ7~2e unilateral pulmo- nary edema and pleural effusions,3J3JsJ8,20 recurrent unilateral pneumonia, cyanosis2y6*7 and pulmonary hypertension.gJ3*20 Complete absence of symptoms has also been described.21 In our series, 2 patients (Cases 1 and 2) presented with pleural effusions and pulmonary edema, which led to catheterization and an angiographic diagnosis of PV stenosis, confirmed at operation. In the other 2 patients (Cases 3 and 4), the PV stenosis was an unexpected finding at operation, detected because the PV orifices were carefully inspected and measured.
Most trials of balloon dilatation15 and angioplasty12J3 in patients with PV stenosis (congenital or acquired) have been unsuccessful. Only 2 patients treated with angioplastygJ0y21 were symptom-free, but neither catheterization nor lung scans have been performed.
Our series, however small, represents the first in which hemodynamic, angiographic and radionuclide data are available after the surgical procedure. Although the 3 survivors can be considered symptom-free, they all have either severely reduced or absent flow to the left lung and 1 has pulmonary hypertension.
Transposition of the great arteries and pulmo- nary vein stenosis (congenital rather than ac- quired): It is sometimes difficult to determine if the PV stenosis is congenital or acquired postoperatively in
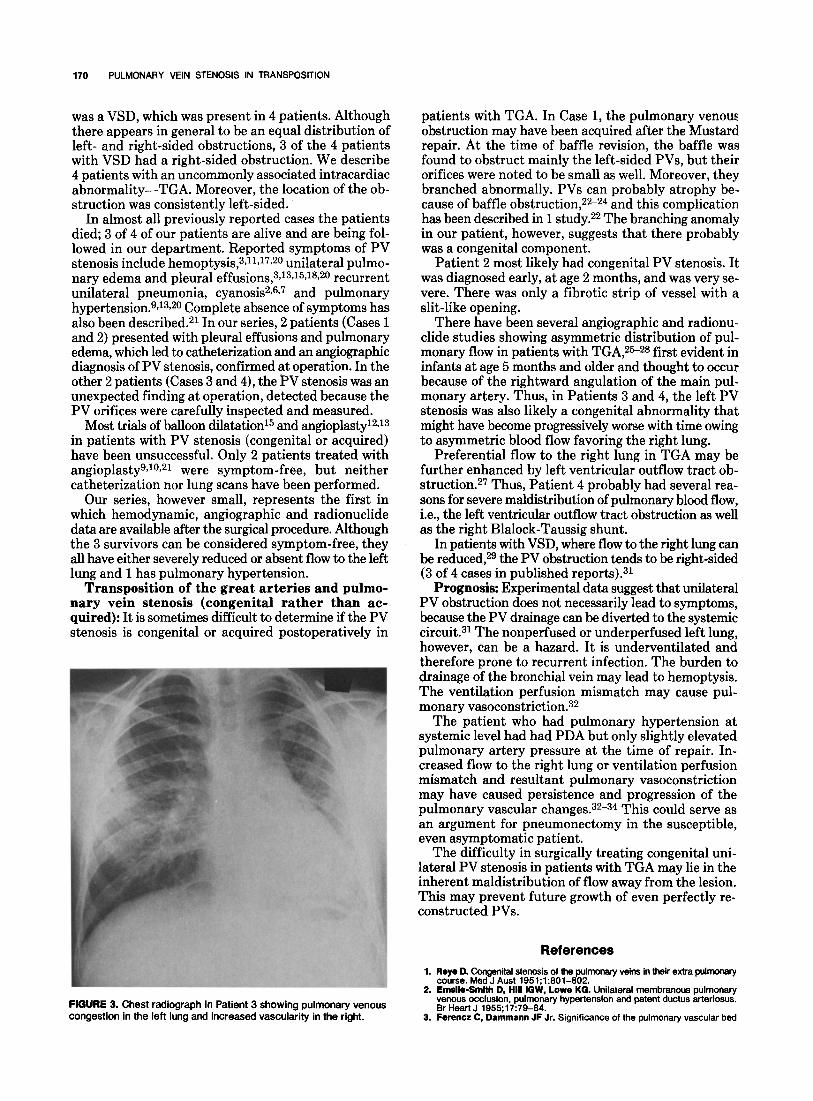
FIGURE 3. Chest radiograph in Patient 3 showing pulmonary venous congestion in the left lung and increased vascularity in the right.
patients with TGA. In Case 1, the pulmonary venous obstruction may have been acquired after the Mustard repair. At the time of baffle revision, the baffle was found to obstruct mainly the left-sided PVs, but their orifices were noted to be small as well. Moreover, they branched abnormally. PVs can probably atrophy be- cause of baffle obstruction,22-24 and this complication has been described in 1 study.22 The branching anomaly in our patient, however, suggests that there probably was a congenital component.
Patient 2 most likely had congenital PV stenosis. It was diagnosed early, at age 2 months, and was very se- vere. There was only a fibrotic strip of vessel with a slit-like opening.
There have been several angiographic and radionu- elide studies showing asymmetric distribution of pul- monary flow in patients with TGA,s5-2s first evident in infants at age 5 months and older and thought to occur because of the rightward angulation of the main pul- monary artery. Thus, in Patients 3 and 4, the left PV stenosis was also likely a congenital abnormality that might have become progressively worse with time owing to asymmetric blood flow favoring the right lung.
Preferential flow to the right lung in TGA may be further enhanced by left ventricular outflow tract ob- struction.27 Thus, Patient 4 probably had several rea- sons for severe maldistribution of pulmonary blood flow, i.e., the left ventricular outflow tract obstruction as well as the right Blalock-Taussig shunt.
In patients with VSD, where flow to the right lung can be reduced,2g the PV obstruction tends to be right-sided (3 of 4 cases in published reports).31
Prognosis: Experimental data suggest that unilateral PV obstruction does not necessarily lead to symptoms, because the PV drainage can be diverted to the systemic circuit.31 The nonperfused or underperfused left lung, however, can be a hazard. It is underventilated and therefore prone to recurrent infection. The burden to drainage of the bronchial vein may lead to hemoptysis. The ventilation perfusion mismatch may cause pul- monary vasoconstriction.32
The patient who had pulmonary hypertension at systemic level had had PDA but only slightly elevated pulmonary artery pressure at the time of repair. In- creased flow to the right lung or ventilation perfusion mismatch and resultant pulmonary vasoconstriction may have caused persistence and progression of the pulmonary vascular changes.32-s4 This could serve as an argument for pneumonectomy in the susceptible, even asymptomatic patient.
The difficulty in surgically treating congenital uni- lateral PV stenosis in patients with TGA may lie in the inherent maldistribution of flow away from the lesion. This may prevent future growth of even perfectly re- constructed PVs.
1.
2.
3.
References
Reye D. Congenital stenosis of the pulmonary veins in their extra pulmonary course. Med J Aust 1951;1:801-802. Emefie-Smfth D, HI8 IGW, Lowe KG. Unilateral membranous pulmonary venous occlusion, pulmonary hypertension and patent ductus arteriosus. Br Heart J 1955;17:79-84. Ferencz C, Dammann JF Jr. Significance of the pulmonary vascular bed
July I.1984 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 54 171
4.
5.
6.
7.
6.
9.
10.
11.
12.
13.
14.
15.
16.
17.
16.
in congenital heart disease. V. Lesions of the left side of the heart causing obstruction of the pulmonary venous return. Circulation 1957;26:1046- 1056. Andrewa EC Jr. Five cases of an undescrlbed form of pulmonary interstitial fibrosis caused by obstruction of the pulmonary veins. Johns Hopkins Hosp Bull 1975:100:28-39. EC&& jE. Congenital stenosis of pulmonary veins. J Lab Invest 1960;
Jbe KL, Reghlb 0, Amplaltz K, Adams P, Edwards JE. Anomalous ori B
in of the left pulmonary artery from the right pulmonary artery. Report o 2 cases and review of the literature. AJR 1965:95:598-610. Naklb A, Moller JH, Kanjuh VI, Edwards JE. Anomalies of the pulmonary veins. Am J Cardiol 1967;:20:77-90. Snellen HA, Bruins C. Anomalies of venous return. In: Watson, H, ed. Pe- diatric Cardiology. St. Louis, MO: CV Mosby, 1968:427-428. Blnet JP, Bouchard F. Lanalols J, Chetochine F. Conso JF, Pottemain M. Unilateral congenital steno& of the pulmonary veins. J Thtiac Cardiovasc Suro 1972:63:397-402. Bouchard b, &et JP, Chstochlne F, Cons0 JF, Langlofs J, Pottemaln M. Un MS de st6nose des voines pulmonaires diagnostiqub et trait6 avec succ6.s. Arch Mal Coeur 1!372;65:1143-1153. Laboux L, Mlchaud JL, Cornet E. Atresie unilaterale des veines pulmo- naires. Signes cllniques, h6modynamiques et angiographiques & propos d’une observation. Arch Mal Coeur 1972:65:1155-i 158. Park SC, Neches WH, Lenlsx CC, Zuberbuhfer JR, Sfewers RW, Bafnwon HT. Successful preoperative diagnosis and surgical repair of pulmonary vein stenosis (abstr). Circulation 1973;47, 48:Suppl IV:IV-33. Klnoshlta T, Yamazakl Y, Kuakawa M, Adkl K, Yoshlzuml K. Extrapul- monarv vein stenosis associated with ventricular se~tal defect (abstr). Jon Circ J i975;39:874. Henry M, Hoeffel JC, Pernot C. Congenital localized stenosis of the pul- monary veins. Pediatr Radio1 1975;4:49-52. Drlscofl J, Hessleln PS, Mulllna CE. Congenital stenosis of individual pul- monarv veins. Clinical soeclmm and unsuccessful treatment bv transvenous balloon dilation. Am J~~ardliol 1682;49:1767-1772. . KIngston HM, Pate1 RG, Watson GH. Unilateral absence or extreme hy- poplasia of pulmonary veins. Br Heart J 1983;49:148-153. Dfamond I. The Harnman-Ri~zh syndrome in childh&. Report of a case with unilateral pulmonary arterial and venous stenosis and atrlovenous occlusion. Pediatrics 1958:22:279-288. Nasrallah AT, Mulllna CE, Sfnger D, Harrlson 0, McNamara DG. Unlfateral pulmonary vein atresia: diagnosis and treatment. Am J Cardiol 1975;36: 969-973.
19,
20.
21.
22.
23.
24.
25.
26.
27.
26.
29.
30.
31.
32.
33.
34.
Swlschuk LE, L’Heureux P. Unilateral pulmonary vein atresia. AJR 1980:135:667-672. Beerman LB, Oh KS, Park SC, Freed MD, Sondhelmer HM, Frlcker FJ, Mathews RA, Flacher DR. Unilateral oulmonary vein atresia: clinical and radiographic spectrum. Pediatr Cardi& 1983:4[105-112. Bargeron LM Jr, Elllotf LP, Soto B, Bream PR, Curry GC. Axial cineangl- ography in congenital heart disease. Circulation 1977;56:1075-1083. Lock JE, Lucas RV, Ampfatx K, Besslnger FB. Silent unilateral pulmonary venous obstruction. Occurrence after surgical correction of tratisposltion of the great arteries. Chest 1973;73:224-227. Kawaahlma Y, Ueda T, Nalto Y, Morlkawa E, Manabe H. Stenosis of pul- monary veins. Ann Thorac Surg 1971;12:196-202. Trualer GA, Mustard WT. Palliative and reparative procedures for trans- position of the great arteries. Ann Thorac Surg 1973;17:410-422. Muster AJ, Paul M, Levln D, Conway J, Newfeld E. Diminished left pul- monary blood flow in transposition of the great arteries (abstr). Am J Cardiol 1973;31:150. Bernard0 AV, Dusrynakl D, Subramanlan S. Pulmonary blood flow distrl- bution in transposition of the great arteries. Am J Cardiol 1976;38:62- 66. Muster AJ, Paul MH, Van Grondefle A, Conway JJ. Asymmetric distribution of the pulmonary blood flow between the right and left lungs in d-transpo- sition of the great arteries. Am J Cardiol 1976;38:352-361. Rablnovltch I, Rosenthal A, Sade RY, Castaneda AR, Trevea S, Nada AS. Regional lung function studies and radionuclide angiography in d- transposition of the great arteries. Pediatr Res 1977;l I:11 17-1121. Dollery CT, West JB, Wllcken EL, Hugh-Jones P. A comparison of the pulmonary blood flow between left and right lungs in normal subjects and patients with congenital heart disease. Circulation 1961;24:617-625. Sade RM, Freed MD, Matthews EC, Castaneda AR. Stenosis of individual pulmonary veins. Review of the literature and report of a surgical case. J Thorac Cardiovasc Surg 1979;67:953-962. Wyatt JP, Burke DR, Hanlon CR. Morphologic study of canine lungs after ligation of the pulmonary veins. Am J Pathol 1953;29:291-303. Rablnovltch M, Konstam MA, Gamble WJ, Papanlcolaou N, konovitx MJ, Treves S? Reid L. Changes in pulmonary blood flow affect vascular response to chronic hypoxia in rats. Circ Res 1983;52:432-441. Clarkaon PM, Neutze JM, Wardlll JC. Barratt-Boyea BG. The oulrnonary vascular bed in patients with complete transpositibn of the g&t arteries. Circulation 1975:53:539-543. Morgan JR, Mlll& BL, Dlacoff OR, Andrewa EJ. Hemodynamic and an- giocardiographic evaluation after Mustard procedure for transposition of the great arteries. J Thorac Cardiovasc Surg 1972;64:878-890.

















