Congenital platelet disorders
11
Congenital Platelet Disorders S. Bellucci, J. P. Caen SUMMA R Y. Congenital platelet disorders include thromhocytopathies and thrombocytopenias, which often occur in association. Thrombocytopathies constitute a model for exploring platelet physiology at the molecular level: adhesion, activation, release phenomena, aggregation. Further advances in understanding thromhocytopenias now require studies of medullary physiology. A better knowledge of these dismhs is necessary to improve their management. In normal primary hemostasis the role of platelets is essential.’ Studies of qualitative constitutional plate- let disorders have been very effective tools for understanding the different mechanisms involved in hemostatic plug formation.2~3 Normally the vessel wall serves as a barrier between the flowing blood and the extravascular space. On!y when this barrier is disrupted can platelets adhere to components of the subendothelium in the presence of plasma factor VIII/van Willebrand factor. Simultane- ously with the platelet adhesion, after stimulation by ADP (secreted by injured endothelial cells), by throm- bin (which is formed by plasma coagulation), or by collagen (the main component of subendothelium) platelets are activated. Activation is marked by sev- eral metabolic events: modification of membrane polyphosphoinositides, intracellular calcium fluxes, activation of phosphorylases and synthesis of prosta- glandins like thromboxane AZ. These phenomena lead to the sequential release of dense granules (mainly ADP) and then of alpha granules (mainly adhesive proteins). The secretion of thromboxane AZ and ADP amplifies this activation step. Then the modification of membrane structure permits the bind- ing of plasma fibrinogen with extracellular calcium S. Behcci, Department of Angiohematology, J. P. Caen, Institut des Vaisseaux et du sang (IVS), Lariboisiire Hospital, 2 rue A. Park, 75010 Paris, France. ions, leading to the formation of platelet aggregates. Finally, platelets contribute to plasma coagulation by providing a phospholipid surface which permits plasma factor activation. Among congenital platelet disorders, the quali- tative platelet disorders will be described first: each functional step can be impaired and thrombocyto- pathies can be classified as defects of adhesion, activa- tion, release or aggregation (Tables 1 and 2). Then the main thrombocytopenias will be set out. At the outset it should be stressed that thrombocytopenia of vary- ing severity and thrombocytopathies often occur in association. Clinical and biological data specific to each disease (Table 2) will be described, with empha- sis on the relation between structural abnormality and functional defect for the thrombocytopathies (Table 1). Therapeutic measures which are very simi- lar for all these different disorders, will be dealt with together at the end of the review. Thrombocytopathies-Defects of Platelet Adhesion to Subendothelium Bernard-Soulier Syndrome This hereditary syndrome was described in i948 by J. Bernard and J. P. Soulier and is characterized by prolonged bleeding time, moderate thrombocyto- penia, normal clot retraction, the appearance of giant B,w,d Ruviwu ,19X8) 2. l&26 ,(, 1988 Longman Group UK Ltd
-
Upload
s-bellucci -
Category
Documents
-
view
220 -
download
6
Transcript of Congenital platelet disorders

Congenital Platelet Disorders
S. Bellucci, J. P. Caen
SUMMA R Y. Congenital platelet disorders include thromhocytopathies and thrombocytopenias, which often occur in association. Thrombocytopathies constitute a model for exploring platelet physiology at the molecular level: adhesion, activation, release phenomena, aggregation. Further advances in understanding thromhocytopenias now require studies of medullary physiology. A better knowledge of these dismhs is necessary to improve their management.
In normal primary hemostasis the role of platelets is essential.’ Studies of qualitative constitutional plate- let disorders have been very effective tools for understanding the different mechanisms involved in hemostatic plug formation.2~3
Normally the vessel wall serves as a barrier between the flowing blood and the extravascular space. On!y when this barrier is disrupted can platelets adhere to components of the subendothelium in the presence of plasma factor VIII/van Willebrand factor. Simultane- ously with the platelet adhesion, after stimulation by ADP (secreted by injured endothelial cells), by throm- bin (which is formed by plasma coagulation), or by collagen (the main component of subendothelium) platelets are activated. Activation is marked by sev- eral metabolic events: modification of membrane polyphosphoinositides, intracellular calcium fluxes, activation of phosphorylases and synthesis of prosta- glandins like thromboxane AZ. These phenomena lead to the sequential release of dense granules (mainly ADP) and then of alpha granules (mainly adhesive proteins). The secretion of thromboxane AZ and ADP amplifies this activation step. Then the modification of membrane structure permits the bind- ing of plasma fibrinogen with extracellular calcium
S. Behcci, Department of Angiohematology, J. P. Caen, Institut des Vaisseaux et du sang (IVS), Lariboisiire Hospital, 2 rue A. Park, 75010 Paris, France.
ions, leading to the formation of platelet aggregates. Finally, platelets contribute to plasma coagulation by providing a phospholipid surface which permits plasma factor activation.
Among congenital platelet disorders, the quali- tative platelet disorders will be described first: each functional step can be impaired and thrombocyto- pathies can be classified as defects of adhesion, activa- tion, release or aggregation (Tables 1 and 2). Then the main thrombocytopenias will be set out. At the outset it should be stressed that thrombocytopenia of vary- ing severity and thrombocytopathies often occur in association. Clinical and biological data specific to each disease (Table 2) will be described, with empha- sis on the relation between structural abnormality and functional defect for the thrombocytopathies (Table 1). Therapeutic measures which are very simi- lar for all these different disorders, will be dealt with together at the end of the review.
Thrombocytopathies-Defects of Platelet Adhesion to Subendothelium
Bernard-Soulier Syndrome
This hereditary syndrome was described in i948 by J. Bernard and J. P. Soulier and is characterized by prolonged bleeding time, moderate thrombocyto- penia, normal clot retraction, the appearance of giant
B,w,d Ruviwu ,19X8) 2. l&26 ,(, 1988 Longman Group UK Ltd

BLOOD REVIEWS 17
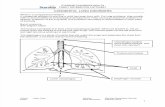
Table 1 Constitutional thrombocytopathies
Thrombocytopathy
Defect of adhesion
Bernard-Soulier syndrome
Molecular abnormality
*GPIb, GPV and GPIX L
Functional abnormality
F VIIIjVWF binding to platelets I Platelet adhesion to subendothelium I
Von Willebrand platelet syndrome *GPIb /” F VIIIjVWF binding to platelets /” Plasmatic FVIIUVWF level L Platelet adhesion to subendothelium I (?)
Defect of reactivity to collagen *GPIa I Platelet adhesion to subendothelium I
Defect of activation
Abnormality in intracellular Ca+ + fluxes
Abnormality in prostaglandin pathway
Defect of secretion of adhesive proteins
Gray platelet syndrome
Defect of secretion of dense granules
6 storage pool disease
Defect of aggregation
Glanzmann disease
Variant thrombasthenia
?
Cyclooxygenase or thromboxane synthetase deficiency
a granules content and a granules number I
Dense bodies number L and function L
*GPIIb and GPIIIa L
*GPIIb/GPIIIa complex absent or abnormal
Defect in enzymatic reactions and metabolic events responsible for activation. Platelet release and aggregation L
idem
release of adhesive proteins I adhesion (?) and aggregation L
Release of ADP I Aggregation L
Fibrinogen binding I Aggregation I
idem
Miscellaneous
Platelet factor 3 deficiency Abnormality in phospholipids involved in binding of factor
Defect of activation in situ of plasmatic factors.
Montreal platelet syndrome
*GP = glycoprotein
Va and Xa.
?
and morphologically abnormal platelets, and defec- platelets.5,6 The platelets also contain an increased tive prothrombin consumption.4 Inheritance is auto- number of dense granules. In the bone marrow, somal and incompletely recessive since heterozygous megakaryocytes are numerous, often multinucleated, individuals show mild biological abnormalities but and present large vacuoles and abnormal demarca- are clinically normal. ’ Hemorrhages are the only tion membranes in ultrastructure.’ consistent symptoms: epistaxis, cutaneous hemor- rhages, gingival or menstrual bleeding are very frequent. Generally the disease is severe, with hemor- rhages requiring numerous transfusions, but mild forms have been described. The mortality rate is about 16%. The platelet count decreases during the natural course of the disease, but the mechanism remains obscure. Platelet morphology is character- istic: the size is always increased, sometimes up to 30 urn in diameter, and typical granulations are clus- tered in the centre of the cell leading to a pseudolym- phocytic appearance. Ultrastructural studies show that the cell membrane system is very abnormal. The surface connected system, the dense tubular system and the microtubular system are much increased and prominent, giving a ‘Swiss cheese’ appearance to some
Functional platelet tests show a prolonged bleeding time, with normal clot retraction. Platelet aggregation mediated by ADP, collagen, epinephrin, arachidonic acid is normal; nevertheless shape change, even when spontaneous, is defective. Thrombin-mediated aggre- gation is delayed. Interestingly, ristocetin-induced aggregation is absent.7 The adhesion to collagen is normal but the adhesion to the subendothelium, as judged by the technique of Baumgartner is very decreased.8 These results led Caen et al to hypothesize that BSS platelets lack a receptor for the von Wille- brand factor (VWF) which is necessary for platelet- subendothelium interaction.9 Subsequent studies showed that microfibrils might be the precise compo- nent of the subendothelium involved in this interac- tion.” The membrane defect is now well defined:
- ?

18 CONGENITAL PLATELET DISORDERS
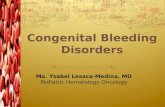
Table 2 Routine platelet function tests in constitutional thrombocytopathies
Platelet aggregation
Platelet Platelet Clot Arachidonic Ionophore Serotonin count size reaction ADP Collagen acid Ristocetin A 23187 release
Bernard-Soulier syndrome
Pseudo Von Willebrand syndrome
Abnormal reactivity collagen
Abnormal Ca + ’ mobilization
Cyclooxygenase deficiency
Thromboxane synthetase deficiency
Gray platelet syndrome
6 storage pool disease
Type I thrombasthenia
Type II thrombasthenia
Montreal platelet syndrome
L 7 N Nor r Nor /* Nor /” nil N N
I 7 N N or I Nor \ N or L ? ?
N N N N nil
N N ? Nor\ L N
N N ? Nor\ L \ or nil N
N N ? Nor\ L L or nil N N L
Nor L Lo
N* \a
N, L or nil N
N, L or nil N
? 79
Norr N N N I L L
Nor\’ L
nil nil
nil nil
N N
N
N
N
N
N N
N nil
N L
/1 N
\ or nil
nil
nil
N
N*
N*
N*
N
*First wave of aggregation only; l decrease of thrombin induced aggregation; N = normal
Bernard-Soulier syndrome (BSS) platelets present an abnormal glycoprotein pattern, with a lack of glyco- protein Ib in particular, as shown by Nurden and Caen’ ’ and confirmed by single or double dimension SDS-gel1 electrophoresis. l2 Recently deficiencies of other glycoproteins have been reported, such as gly- coprotein V and glycoprotein IX.3 The apparent genetic absence of multiple proteins in BSS might be due partly to the presence in normal platelets of a tight membrane complex between glycoprotein Ib and at least one of the other absent glycoproteins. The recent demonstration of a deficiency in both glyco- proteins Ib and IX at the level of megakaryocyte precursors is in agreement with this hypothesis.13
Interestingly, it has been demonstrated that the abnormalities in membrane structure were respon- sible for abnormal functional tests and consequently for hemorrhagic manifestations. Thus, immunologic investigation using polyclonal or monoclonal anti- bodies which recognize glycoprotein Ib has shown that this glycoprotein is the receptor for plasma factor VIII/van Willebrand factor. 14*15 Platelet membrane gel electrophoresis after stimulation by thrombin has suggested that glycoprotein V might be involved in the thrombin-platelet interaction, although it is not the receptor for thrombin.16 Nevertheless the de- crease of glycoprotein V in BSS platelets might ex- plain the delay of thrombin-mediated aggregation and perhaps the defective prothrombin consumption test. Lastly, glycoprotein IX has been shown to function as a receptor for drug-dependent antibody receptor sites, which were found decreased in BSS platelets. 1 ’
Detection of heterozygous subjects is possible since
their platelets give an intermediate response in bind- ing tests with polyclonal or monoclonal antibodies.’ a Similarly, immunofluorescence tests or radioimmuno- logic procedures using monoclonal antibodies should render antenatal diagnosis possible” and indeed much simpler and safer in the coming years, with the advancement of molecular biology and the cloning of the gene for glycoprotein Ib.
Variant Forms of Bernard-Soulier Syndrome
While some thrombocytopathies featuring giant platelets and absence of aggregation with ristocetin present a normal amount of glycoprotein Ib, they comprise a qualitative defect since the migration in SDS gel electrophoresis is abnormal.2 Nevertheless one must bear in mind the considerable genetic polymorphism of the glycoprotein Ib.
The Pseudo von Willebrand Platelet Syndrome
Thrombocytopenic thrombocytopathies associated with an abnormality of plasma factor VIII/VWF were first reported several years ago, namely as the von Willebrand Jurgens syndrome.2 This syndrome is in fact heterogenous since it can be due either to an intrinsic abnormality of factor VIII/VWF (von Wille- brand IIb syndrome) or to a platelet abnormality (pseudo von Willebrand platelet syndrome). In the pseudo von Willebrand platelet syndrome2’ in- heritance seems autosomal dominant. Hemorrhages are the only symptoms; they are most often muco- cutaneous and of variable intensity, sometimes severe. In this syndrome, thrombocytopenia usually fluctu-

BLOOD REVIEWS 19
ates more or less markedly. Platelets are of increased size, without any morphologic abnormalities, but agglutinate spontaneously very readily.
Bleeding time is usually prolonged whatever the platelet count. Platelet aggregation induced by physiological agents is most often normal or slightly decreased but the main abnormality is the increased reactivity of platelets to ristocetin, especially in low doses.’ Furthermore platelets agglutinate with nor- mal plasma or with factor VIII von Willebrand fac- tor without ristocetin. 2o In the plasma, the factor VIIIc level is slightly decreased. The factor VIII/ von Willebrand factor is also decreased and the level of ristocetin cofactor is lower than its immunological level. The decrease of high multimeric forms of factor VIII/van Willebrand factor is confirmed by immuno- electrophoresis and SDS agarose electrophoresis. These results may be explained by an abnormal platelet membrane structure with more glycoprotein Ib than in normal platelets.21 This abnormality may account for the increased binding of high multimeric forms of factor VIII/van Willebrand factor in direct experiments in vitro. 21 Hemorrhagic manifestations might thus be due to a decrease of circulating F VIII/VWF leading to defective adhesion of platelets to the subendothelium.
As already mentioned, this syndrome must be distinguished from von Willebrand IIb syndrome where factor VIII/VWF is intrinsically abnormal, lacking high multimeric forms.22 In the latter, platelet numeration, size, and glycoprotein Ib content are normal.2’ The infusion of normal factor VIIIjVWF cryoprecipitates shows a normal rate of disappear- ance, confirming the normal platelet function in vivo.23 This constitutes the therapeutic management of this syndrome, which differs considerably from that of the pseudo von Willebrand syndrome (see section on ‘Therapy’).
Defect of Reactivity to Collagen
Sometimes, hemostatic tests of a patient complaining of hemorrhagic manifestations reveal decreased plate- let aggregation only after stimulation by collagen. A more precise study of such cases would be useful for understanding the mechanism of this abnormality. Indeed, a case of thrombocytopathy due to a specific defect in response to collagen was recently analyzed: collagen induced neither adhesion, nor activation, nor platelet aggregation. Specific techniques of SDS poly- acrylamide gel electrophoresis revealed a defect in glycoprotein Ia, which is evidence for its involvement in the reactivity of platelets with collagen.24
To sum up, studies of thrombocytopathies featuring defects of adhesion to subendothelium have shown the importance of two major glycoproteins in this func- tional step: glycoprotein Ib has been shown to be the receptor of factor VIIIlvon Willebrand factor, which forms a bridge between platelets and components of subendothelium (microJibrils and, under some circum-
stances, collagen); glycoprotein Ia has been found to be implicated in the reactivity of platelets with collagen.
Thrombocytopathies due to a Disorder in Platelet Activation
Defect of Calcium Mobilization
Some thrombocytopathies are characterized by a defect of aggregation in response to all inducers although membrane structure and granule constitu- ents appear normal. In addition, after stimulation, thromboxane BZ is synthesized normally, ruling out a disorder in the prostaglandin metabolic pathway. Studies using ionophore A 23187, which normally permits the mobilization of calcium outside its storage vesicles, are a tool for investigating such thrombocy- topathies, as are measurements employing Quin 2 or other components, where esterification consecutive to calcium fluxes is followed by a modification of spontaneous fluorescence. These thrombocytopathies have recently been described25 and the exact step of calcium metabolism which is affected still requires investigation. Lastly, similar defects have also been reported in patients presenting associated neurologic manifestations.26
Thrombocytopathies due to an Abnormality in the Prostaglandin Metabolic Pathway
After stimulation by agonists such as collagen, ADP or thrombin, normal platelet activation involves the hydrolysis of membrane phospholipids, and the liber- ation of arachidonic acid. Arachidonic acid is then converted into endoperoxides by the cyclooxygenase enzyme and then to thromboxane A2 by the throm- boxane AZ synthetase enzyme. Isomerases can also convert endoperoxides into primary prostaglandins F2 alpha, D2 and E2 but in smaller quantities. Exceptionally cyclooxygenase27*28 or thromboxane synthetase 2*29 deficiencies have been reported. Bleed- ing time is generally slightly prolonged and hemor- rhages are of variable intensity. Platelets do not aggregate after stimulation by collagen, thrombin or arachidonic acid. Cyclooxygenase deficiency is char- acterized by normally balanced but decreased prosta- glandin synthesis, and definite aggregation after stimulation by natural endoperoxide. Thromboxane AZ synthetase deficiency is marked by a reorientation of prostaglandin synthesis towards more prostaglan- dins E2 or Dz, at the expense of thromboxane A2 synthesis; in addition, natural endoperoxide-induced aggregation remains decreased.
Finally, a defective sensitivity of platelets to throm- boxane A2 has been suggested:30 nevertheless, in the case described one cannot rule out a defect of intra- cellular calcium mobilization. Besides, the hypothesis of an abnormality of thromboxane AZ receptors has not been supported by studying for example the reactivity to endoperoxide analogues which have the

20 CONGENITAL PLATELET DISORDERS
same receptor on platelets as thromboxane AZ and which can by themselves, induce platelet aggregation.
Thus, a precise knowledge of the constitutional thrombocytopathies marked by abnormal platelet acti- vation is important since many drugs (calcium inhibi- tors; non steroid anti-inflammatory drugs) mimic these disorders.
Thrombocytopathies due to a Quantitative or Qualitative Defect in Dense Bodies
Idiopathic Dense Bodies Deficiency (6 storage pool disease)
Several families have been described where inheri- tance of this disorder was autosomal dominant.2*31 There was complete failure of aggregation after colla- gen stimulation and a decreased response after ADP or adrenalin action with rapid disaggregation and without the second wave of aggregation. Later on it was shown that aggregation induced by arachidonic acid was decreased too. These abnormalities were due to a decreased number of dense bodies as shown by the mepacrine test or ultrastructural studies.2 Normal constituents of dense bodies (serotonin, nucleotides) were thus decreased, as was their release after stimuli such as ADP or thrombin. Except after induction by collagen, prostaglandin synthesis was preserved. Platelet-membrane phospholipids and glycoproteins were normal. The storage pool disease only excep- tionally occurs alone. 32 It may be associated with a defect in alpha granules or with other constitutional disorders, as outlined below. In these constitutional disorders, like the Chediak-Higashi syndrome, a de- fect of dense body release can be demonstrated even if their number remains normal.
Dense-bodies Deficiency in Hermansky-Pudlak Syndrome
A quantitative and functional defect in dense bodies was reported in the Hermansky-Pudlak syn- drome.33’34 In this autosomal recessive disorder char- acterized by the triad of tyrosine positive occulocuta- neous albinism, accumulation of ceroid-like pigment in macrophages and prolonged bleeding time, the hemorrhagic tendency is present but moderate.
Dense-bodies DeJieiency in Chediak-Highashi Syndrome
In this syndrome, occulocutaneous albinism and hair abnormalities have been reported. The clinical course is marked by severe bacterial or fungal infections but hemorrhagic manifestations are very mild or absent except during acute phases of the disease where they are due to exaggerated fibrinolysis. Abnormal gran- ules have been found in several cells such as melano- cytes, neutrophils, monocytes, macrophages and fibroblasts, but not in platelets and very rarely in
megakaryocytes.2 Subsequent functional platelet studies demonstrated a decrease of dense bodies and/or defective release of their constituents.2*35*36
Dense-body Deficiency in the Wiskott-Aldrich Syndrome
The characteristic features of this syndrome, whose transmission is sex linked, are extensive eczema, recurrent infections due to severe lymphocyte T im- mune deficiency, and an intense thrombocytopenia.37 Hemorrhages are often alarming, sometimes fatal, and have prompted several platelet-function studies. Platelets appeared of reduced size (about l/3 of the normal volume) and showed decreased aggregation after ADP, collagen or adrenalin.2 A decreased num- ber of dense granules may account for this platelet dysfunction,2 but a defect of ADP metabolism3* or of glycolysis39 cannot be excluded. A decrease in sialo- glycoproteins have been reported,40 namely of glyco- protein L 115 on lymphocytes and glycoprotein Ib and Ia on platelets. These interesting data showing that a structural abnormality may be present on several hematopoietic cells might explain the different characteristics of this syndrome. Nevertheless a de- crease of platelet glycoprotein Ib and Ia was not always confirmed by subsequent studies,41 which is evidence for the heterogeneity of the syndrome and perhaps for the occurrence of structural modifications during the clinical course.
Dense-body Deficiency in Thrombocytopenia with Absent Radii
This deficiency is not constant and when present might increase the risk of hemorrhagic manifestations encountered in this disorder.2
Thrombocytopathy with Defect of Adhesive Proteins and other Constituents of Alpha Granules
In 197 1, Raccuglia described a syndrome associating thrombocytopenia, hemorrhagic tendency and mor- phologic abnormalities in platelets and megakaryo- cytes.42 He termed this condition ‘gray platelet syn- drome’ because of the lack or paucity of granules leading to a peculiar gray colour of platelets on Wright-stained blood smears. Platelets were slightly larger than normal, and ultrastructural and cyto- chemical studies showed that they contained a normal number of mitochondria, dense bodies, peroxisomes and lysosomes but specifically lacked alpha gran- ules.43 Studies of megakaryocytes showed that they also lacked alpha granules43 although the Golgi zone appeared normally developed. Ultrastructural studies and immunological procedures using monoclonal or polyclonal antibodies confirmed a defect in the pack- aging of proteins in the precursors of alpha granules which were unable to mature.43*44 The platelet alpha

BLOOD REVIEWS 21
granule content (platelet factor 4, betathrombo- globulin, fibrinogen, platelet derived growth factor (PDGF), thrombospondin, fibronectin) was found to be 15% of the normal values.45 By contrast, dense bodies, lysosomes and peroxisomes were normally present, and serotonin, adenine nucleotides, lysoso- ma1 enzymes and catalase were found in normal (or even increased) amounts within the platelets. Prosta- glandin metabolism was also normal. Functional studies showed normal adhesion to polymerized type III collagen, while aggregation was slightly decreased after ADP and especially after collagen, thrombin, epinephrine or ionophore A 23 187 stimulation.46
A concomitant defect of serotonin release was shown, suggesting that alpha granules may play a role in the release or aggregation mechanisms synergisti- cally with dense granules. On the other hand, no abnormalities of surface-labelled glycoproteins have been described. 45 The mechanism of the hemorrhages is not perfectly known: it is possible that following endothelial damage, the secretion of alpha granule proteins by platelets may be important in achieving the high local concentration of these proteins that is critical for cell contact (factor VIII/van Willebrand factor; fibronectin; thrombospondin) and thrombin generation (fibrinogen, factor V,) within the develop- ing aggregates. Another interesting point is the dis- covery of myelofibrosis as confirmed by histological examinations which showed very numerous fibro- blasts in the bone marrow and large deposits of collagen fibres in the extracellular spaces, especially around megakaryocytes.43
It has been shown that PDGF is present only in the early precursors of megakaryocytes, and that the other alpha granule constituents cannot be stored in matrix alpha granules. 47 PDGF concentration in medullary sinusoids might thus be higher than nor- mal, possibly enhancing myelofibrosis since it has been shown to promote fibroblast and smooth muscle cell proliferation.48
Thrombocytopathies due to Defective Aggregation
Glunzmann Thrombastheniu
Described by Glanzmann in 1918, thrombasthenia associates absence of clot retraction with normal platelet count and morphology. Hemorrhages are very frequent: they are cutaneous and mucous and very often insidious when they affect the nasophar- ynx. In 1972, Caen4’ distinguished two types of thrombasthenia. Type I thrombasthenia was charac- terized by a lack of aggregation, decreased intraplate- let fibrinogen and the absence of clot retraction. It was then shown that the specific platelet antigen PLA’ was lacking. In type II thrombasthenia, plate- let fibrinogen content was only decreased, as was clot retraction or the level of specific PLA’ antigen, while platelet aggregations remained absent.
Blood films from thrombasthenic patients reveal no morphologic abnormalities except that no spontane- ous platelet aggregates are observed. Ultrastructural examinations are normal. Functional platelet studies confirm the absence or the decrease of clot retraction which was reported initially, and which remains a useful tool for diagnosis. Similarly, the lack of platelet aggregation, documented by Caen et al in 1962 has been better elucidated: platelets do not aggregate in response to ADP, collagen, thrombin, adrenalin, arachidonic acid or after ex vivo adhesion to rat aortic subendothelium according to the Baumgart- ner technique.’ Nevertheless, the initial reactions of shape change, and ADP or thrombin binding to the membrane were normal. On the other hand, adhesion to collagen or to subendothelium in vitro was normal, as was ristocetin-induced agglutination. * In 1974, Nurden and Caen demonstrated a membrane struc- tural abnormality, using SDS polyacrylamide gel electrophoresis: glycoproteins IIb and IIIa were not detectable in type I thrombasthenia.” These results were subsequently confirmed by several teams using single or double dimension SDS-gel electrophoresis techniques; ’ * it was also shown that these glycopro- teins were present at 15%-20% of normal levels in type II thrombasthenia. Immunological studies by immunoprecipitationsl or crossed-immuno-electro- phoresis5* using polyclonal or monoclonal antibodies were in agreement with these findings and showed that glycoproteins IIb and IIIa formed a calcium divalent mediated complex which is present prior any platelet activation.53 Using more sensitive SDS-poly- acrylamide gel electrophoresis procedures, residual amounts of glycoprotein IIb (up to 3%) and IIIa (up to 10%) have recently been demonstrated in type I thrombasthenia, thus ruling out the hypothesis of deletion of structural genes encoding for these glyco- proteinsJ4 The decrease of these two glycoproteins has also been noted on megakaryocyte membranes of thrombasthenic patients. 55 Recent molecular biology research seems to show that glycoprotein IIIa synthe- sis requires the prior synthesis of glycoprotein IIb (J. P. Rosa personal communication).
This defect of the glycoprotein IIb/IIIa complex accounts for the lack of aggregation. It is well known that platelet aggregation requires plasma fibrinogen binding to the platelet membrane.’ This fibrinogen binding was absent in type I thrombasthenia2v56 and markedly decreased in type II thrombasthenia,57 which suggests that the glycoprotein IIb/IIIa complex might be the receptor for plasma fibrinogen. This has been documented by direct in vitro experiments.58 Thrombospondin expression at the platelet surface during activation might stabilize the interaction of fibrinogen with this complex.5g The lack of clot retraction is not well understood. This phenomenon does not require direct binding between glycoprotein IIIa and alpha actinin, which is present in normal amounts in thrombasthenic platelets. However, gly- coprotein IIIa seems to participate in anchoring the

22 CONGENITAL PLATELET DISORDERS
cytoskeleton to the membrane during platelet aggre- gation but not by direct interaction with alpha ac- tinin. On the other hand, it has recently been shown that glycoproteins IIb/IIIa might be involved in other adhesive protein binding such as factor VIII/van Willebrand factor, fibronectin61T62 and that this bind- ing is defective in thrombasthenia.63*64 The physio- logical relevance of these findings remains unknown. Lastly, the specific platelet antigens, such as PLA’ and Lek”, present on glycoprotein IIIa and glycopro- tein IIb respectively, are lacking in type I thrombas- thenia and decreased in type II thrombasthenia.’
As for the Bernard-Soulier syndrome, immunologi- cal tests can detect heterozygous individuals whose platelets contain glycoproteins IIb and IIIa at 50% of normal levels,18 and whose platelets aggregate normally. Theoretically, immunological tests should also lead to antenatal diagnosis.” However, blood collection remains dangerous, even fatal, for the thrombasthenic fetus because of the high risk of hemorrhage. Antenatal diagnosis should be facili- tated by advances in molecular biology and by direct determination of glycoprotein IIb and IIIa genes on trophoblastic samplings.
Variant Forms of Thrombasthenia
Exceptional variant forms have been reported.65*66 Glycoproteins IIb and IIIa are present either in normal or subnormal amounts but platelet aggrega- tion remains null. The functional abnormality may be due to a defect in the formation of the complex between glycoproteins IIb and IIIa as demonstrated recently by Nurden et al. 65 Alternatively, there might be a defect in the exposure of the fibrinogen site, even if the glycoprotein IIb/IIIa complex is present, as suggested in the case of the variant thrombasthenia Paris I-Lariboisiere.66
Thus, studies of Glanzmann thrombasthenia and its variant forms supply a particularly interesting model
for elucidating the role of glycoproteins, which appear ubiquitous, as receptors for adhesive proteins. As for platelet-platelet, or platelet-vessel wall interaction, pharmacological agents which can inhibit this function should play an important role in the prevention of thrombosis or atherosclerosis.
Defect of Platelet Coagulant Activity
During the release reaction, platelet factor 3 (PF3), which is a lipoprotein complex, becomes available in the plasma membrane of platelets to supply a cata- lytic surface for the interaction with plasma clotting factors. Methods for measuring PF3 availability are very difficult and indirect, and depend on the ability of activated platelets to shorten the recalcification time or the plasma Stypven time or to generate thrombin.2
As noted by Weiss et a16’ and Minkoff et a1,68 patients with aggregation or release defects often
show impairment of PF3 activity as well. However, an isolated PF3 deficiency occasionally occurs: three such cases have been reported:67,68,69 hemorrhagic manifes- tations were often severe, prothrombin consumption was decreased, but the bleeding time was prolonged only in one case. 69 The exact mechanism responsible for this defect in PF3 availability has yet to be elucidated: an abnormality of membrane phospholipids mobiliza- tion leading to defective binding of factor V,-factor X, to platelets is strongly suggested.”
Miscellaneous
Other thrombocytopathies have been described in which the exact functional defect is still unknown.
The Montreal-Platelet Syndrome
The Montreal-Platelet syndrome (MPS), first de- scribed by Lacombe and D’Angelo,‘i is characterized by autosomal dominant inheritance, the appearance of giant platelets on peripheral blood smears, prolonged bleeding time, greatly reduced platelet count, sponta- neous platelet aggregation, normal clot retraction, and thromboplastin formation. Ristocetin-induced aggre- gation is normal in MPS, but thrombin-induced aggregation is either low or absent. Shape change is abnormal and has been attributed to a subtle shift in the mechanism which regulates membrane reorganiza- tion during platelet shape change.72
Other Macrothrombocytic Thrombocytopathies
Other macrothrombocytic thrombocytopathies were described as having autosomal dominant or co-domi- nant inheritance before being studied by modem techniques. Platelet survival and bone marrow mega- karyocytes are usually normal, but abnormalities of platelet function have frequently been noted, in ad- dition to thrombocytopenia. Some of the cases are identical to those reported as familial thrombopenia with hypogranular platelets (see below). Further studies are necessary to ascertain whether there is any biochemical defect and to classify these thrombocyto- pathies more accurately.2
Epstein’s Syndrome
In Epstein’s syndrome, transmitted as an autosomal dominant trait, mild thrombocytopenia with giant platelets is associated with nephritis and nerve deafness; a platelet-release defect has been reported, although not systematically. The bleeding tendency is presumably chiefly attributable to thrombocytopenia.2
Thrombocytopathies in Hereditary Connective Tissue Disorders
An abnormal bleeding tendency may occur in indi- viduals with genetically determined connective tissue

BLOOD REVIEWS 23
disorders, such as osteogenesis imperfecta, Marfan’s syndrome, Ehlers-Danlos syndrome and pseudoxan- thoma elasticum.2 Among these, the Ehlers-Danlos syndrome is the most commonly associated with bleeding. Abnormalities of platelet function, especi- ally decrease or lack of collagen-induced aggregation, lack of the second wave after ADP aggregation, and abnormal PF3 activity, have been described in each of these disorders.
Excessive hemorrhage in this group of conditions is more likely to result from the abnormality of the connective tissue itself.
Thrombocytopenias
Some constitutional thrombocytopenias are associ- ated with thrombocytopathy and have already been described: for example the Bernard-Soulier syndrome, the gray platelet syndrome, or the Wiskott-Aldrich syndrome.
May-Hegglin Thrombocytopenia
This rare hematologic condition is characterized by the presence of basophilic inclusions (Diihle bodies) in the leukocytes, giant platelets, and a variable degree of thrombocytopenia.2 Although purpura or other minor bleeding episodes have occasionally been noted in association with the anomaly, the majority of reported cases have been asymptomatic; nevertheless, some significant, even alarming, instances of hemor- rhages have been reported.
Concerning the characteristic laboratory findings, it is now well established that Diihle bodies in the granulocytes are rich in RNA and probably represent a defective maturation of normal granulation. In addition, the platelet count is variable; thrombocyto- penia may be present, absent, or intermittent; the giant platelets vary in size and shape, and are some- times up to 20 pm in length; optically, their granula- tions seem normal. White and Gerrard2 as well as Hamilton et al2 found a significant increase in the number of giant granules in two patients. Indirect estimation of alpha granule number by measuring betathromboglobulin gives normal values in relation to platelet mass. Megakaryocyte ultrastructure is also normal, but certain investigators claim to have observed abnormal demarcation membranes and de- layed maturation, suggesting dysmegakaryocyto- poiesis.
Functionally, the platelets are normal as regards ADP, collagen, and ristocetin aggregation and PF3 availability. Their membrane glycoproteins are also normal. Finally, with new improved management, survival is considered normal. This anomaly thus appears to be a defect in maturation affecting both leukocytes and megakaryocytes, sometimes leading to bleeding manifestations in good correlation with the degree of thrombocytopenia.
Thrombocytopenia with Megakaryocytopenia
Thrombocytopenia with megakaryocytopenia may be associated with other abnormalities, such as absence of radii or cardiac malformations. In this syndrome thrombocytopenia is complicated by a thrombocyto- pathy resembling a storage pool defect. However, this disease may exist in an isolated form. It is fortunately exceptional, because its prognosis is very severe.’
Familial Thrombocytopenia
In some families, hereditary thrombocytopenia oc- curs’ without associated defects and closely resembles acquired immunologic thrombopenic purpura {ITP). On examination of the peripheral smear, thrombocy- topenia of variable intensity is the only abnormality. Platelet size is generally increased and megakaryo- cytes are normal or increased in number in the bone marrow. Bleeding manifestations usually begin in infancy and, in exceptional cases, during the neonatal period; this is in contrast with acquired ITP which is usually (but not always) seen in children over a year of age. The prognosis is usually very good. Transmis- sion is autosomal dominant and sometimes autoso- ma1 recessive.
Platelet function has not been studied very exten- sively much but seems normal or only slightly de- creased: platelet survival is normal. The disorder therefore seems to be of medullary origin.
Hereditary Hypogranular Thrombocytopenia
This affection was described by Fonio, Flemmeler, Falcao and then by Kurstjens and Libanska. It is associated with a severe bleeding tendency, thrombo- cytopenia and hypogranular platelets, and is inherited as an autosomal dominant syndrome. An unusual coincidence has been noted between this affection and the blood group 0.
Megakaryocyte and platelet ultrastructure have been shown to be abnormal, with a reduced number of dense or alpha granules; platelet function studies have often revealed defective aggregation and release. Thus, if appears that these cases do not differ greatly from the more recent descriptions of alpha or com- bined storage pool disease.
Therapy
There is no treatment to cure constitutional thrombo- cytopathies or thrombocytopenias, nor any prophy- lactic treatment for spontaneous bleeding. A healthy way of life can be recommended to patients to avoid the risk of hemorrhagic trauma. Drugs capable of interfering with hemostasis and especially with plate- let function are contraindicated. Local hemostatic measures are often sufficient to control bleeding and can be attempted before platelet transfusions. Arterial embolism may sometimes be very effective for severe epistaxis.

24 CONGENITAL PLATELET DISORDERS
Attempted therapy with corticosteroids and plasma infusions has generally been unsuccessful. Somewhat surprisingly, however, it has been found that infusion of cryoprecipitates shortens bleeding time and con- trols surgical bleeding in patients with storage pool deficiency, even though the platelet abnormalities remain unaffected.
Splenectomy has been performed in some patients and has induced a slight increase of platelet count in thrombocytopathies, without any improvement of the functional abnormalities. Splenectomy is generally contraindicated in the case of associated immunologic deficit but can be effective for platelet thrombocyto- pathia in the Wiskott-Aldrich syndrome.2
The main therapeutic approach is supportive ther- apy by platelet transfusions. If possible, platelet con- centrates from a single donor and as HLA-compatible as possible, is preferable in order to limit HLA immunization. In thrombocytopathies with a mem- brane molecular defect, specific alloimmunizations against the missing glycoproteins have been reported. These specific antiplatelet antibodies (such as anti- factor VIII in hemophiliacs) make further trans- fusions ineffective. In the platelet von Willebrand syndrome, platelet concentrates must be sometimes associated with cryoprecipitates if the plasma level of factor VIII/van Willebrand factor is very decreased. Finally, when hemorrhagic manifestations are severe and refractory to platelet infusions, bone marrow transplantation may be the only remaining thera- peutic course and has been successfully performed in the Wiskott-Aldrich syndrome,2 the Chediak-Higashi syndrome’ and Glanzmann thrombasthenia.73
Conclusion
Our understanding of thrombocytopathies has now reached the molecular level; genetic engineering should permit further progress and even therapeutic advance- ment. Current knowledge has greatly contributed to the understanding of platelet physiology, hemorrhagic disorders, and also thrombotic diseases. For thrombo- cytopenias, the culture of megakaryocytes should lead to some progress. The diagnosis of thrombocytopenias is greatly facilitated by immunologic and biochemical tests and can generally be made without undue diffi- culty, although some thrombocytopathies are still diffi- cult to classify. Earlier detection of these inherited disorders has given rise to both therapeutic precau- tions, as discussed, and supportive therapy, leading to an important decrease in mortality. Certain particu- larly severe forms should even benefit from bone marrow transplantation. Last, it can be hoped that some accurate biochemical data on thrombocytopath- ies may even lead to prenatal diagnosis.
References I. Weiss H J 1975 Platelet physiology and abnormalities of
platelet function New England Journal of Medicine 293: 531-541, 580-588
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Bellucci S, Tobelem G, Caen J P 1983 Inherited platelet disorders. Progress in Hematology 13: 223-263 George J N, Nurden A T, Philipps D R 1984 Molecular defects in interactions of platelets with the vessel wall. New England Journal of Medicine 104: 1084-1098 Bernard J, Soulier J P 1948 Sur une nouvelle variete de dystrophie thrombocytaire hemorragique congenitale. Semaine des Hopitaux de Paris 97: 3217-3223 Maldonado J E, Gilchrist G S, Bridgen L P, Bowie E J W 1975 Ultrastructure of platelets in Bernard-Soulier syndrome. Mayo Clinic Proceedings 50: 402-405 White J G, Gerrard J M 1976 Ultrastructural features of abnormal blood platelets. A review. American Journal of Pathology 83: 589-632 Caen J Pi Levy-Toledano S 1973 Interaction between platelets and von Willebrand factor provides a new scheme for primary haemostasis. Nature New Biology 244: 1599160 Weiss H J, Tschopp T B, Baumgartner H R, Sussman H, Johnson M M, Egan J J 1974 Decreased adhesion of giant (Bernard-Soulier) platelets to subendothelium. Further implications of the role of the von Willebrand factor in hemostasis. American Journal of Medicine 57: 920-925 Caen J P, Nurden A T, Jeanneau C, Michel H, Tobelem G, Levy-Toledano S, Sultan Y, Valensi F, Bernard J 1976 Bernard-Soulier syndrome: a new platelet glycoprotein abnormality. Its relationship with platelet adhesion to subendothelium and with factor VIII von Willebrand protein. Journal of Laboratory and Clinical Medicine 87: 586596 Fauvel F, Grant M E, Legrand Y L, Souchon H, Tobelem G, Jackson D S, Caen J P 1983 Interaction of blood platelets with a microfibrillar extract from adult bovine aorta: requirement for von Willebrand factor. Proceedings of the National Academy of Sciences USA 80: 551-554 Nurden A T, Caen J P 1975 Specific roles for surface glycoproteins in platelet function. Nature 255: 720-722 Nurden A T, Caen J P 1979 The different glycoprotein abnormalities in thrombasthenic and Bernard-Soulier platelets. Seminars in Hematology 16: 234-250 Hourdille P, Belloc F, Heilmann E, Pica M, Nurden A T 1987 Megakaryocytes from the marrow of a patient with Bernard-Soulier syndrome lacked GPIb and were deficient in GP IX. XIth International Congress on Thrombosis and Haemostasis, Brussels Tobelem G, Levy-Toledano S, Bredoux R, Michel H, Nurden A T, Caen J P 1976 New approach to determination of specific functions of platelet membrane sites. Nature 263: 427428 Ruan C, Tobelem G, Caen J P 1981 Liaison du facteur VIII/Willebrand aux plaquettes de syndrome de Bemard- Soulier et de thrombasthtnie de Glanzmann. Nouvelle Revue Francaise d’Hematologie 23: 89-93 Jeandrot-Perrus M, Guillin M C, Nurden A T Gamma human thrombin: lack of correlation between a platelet functional response and glycoprotein V hydrolysis. Thrombosis and Haemostasis, submitted for publication Berndt M C, Caen J P Platelet glycoprotein in progress in hemostasis and thrombosis. Spaet Ed. Grime and Stratton,
P7 Montgomery R R, Kunicki T J, Taves C, Pidard D, Corcoran M 1983 Diagnosis of the Bernard-Soulier syndrome and Glanzmann’s thrombasthenia with a monoclonal assay on whole blood. Journal of Clinical Investigation 71: 385-389 Gruel Y, Boizard B, Daffos F, Forestier F, Caen J P, Wautier J P 1986 Determination of platelet antigens and glycoproteins in the human fetus. Blood 68: 488492 Weiss H J, Meyer D, Rabinowitz R, Pietu G, Girma J P, Vicic W J, Rogers J 1982 Pseudo von Willebrand’s disease: an intrinsic platelet defect with aggregation by unmodified human factor VIII/van Willebrand factor and enhanced adsorption of its high molecular weight multimers. New England Journal of Medicine 306 326-333 Bryckaert M C, Pietu G, Ruan C, Tobelem G, Girma J P, Meyer D, Larrieu M J, Caen J P 1985 Abnormality of glycoprotein Ib in two cases of ‘pseudo’ von Willebrand’s disease. Journal of Laboratory and Clinical Medicine 106: 393400 Ruggeri Z M, Pareti F I, Mannucci P M, Ciavarella N, Zimmerman T S 1981 Heightened interaction between

BLOOD REVIEWS 25
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
31.
38.
39.
40.
41.
platelets and factor VIII/van Willebrand factor in a new Griscelli C 1987 Analysis of the membrane glycoproteins of subtype of von Willebrand’s disease. New England Journal platelets in the Wiskott-Aldrich syndrome. Blood, submitted of Medicine 302: 1047-1051 for publication Ruggeri Z M, Lombardi R, Gatti L 1982 Type IIB von Willebrand’s disease: Differential clearance of endogenous versus transfused large multimer von Willebrand factor. Blood 60: 1453-1456
42. Raccuglia G, Fat P 1971 Gray platelet syndrome: a variety of qualitative platelet disorder. American Journal of Medicine 51: 818-828
43. Nieuwenhuis H K, Akkerman J W N, Houdij W P M, Sixma J J 1985 Human blood platelets showing no response to collagen fail to express surface glycoprotein Ia. Nature 318: 470-472 Hardisty R P, Machin S J, Nokes T J C, Rink T J, Sharon W 1983 A new congenital defect of platelet secretion: impaired responsiveness of the platelets to cytoplasmic free calcium. British Journal of Haematology 53: 543-557 Koike K, Rao A K, Holmsen H, Mueller P S 1984 Platelet secretion defect in patients with the attention deficit disorder and easy bruising. Blood 63: 427-433 Malmsten C, Hamberg M, Svensson J, Samuelsson B 1975 Physiological role of an endoperoxide in human platelets: Hemostatic defect due to platelet cyclooxygenase deficiency. Proceedings of the Natural Academy of Sciences USA 72: 1446-1450
44.
Breton-Gorius J, Vainchenker W, Nurden A T, Levy- Toledano S, Caen J P 1981 Defective alpha granule production in megakaryocytes from gray platelet syndrome. Ultrastructural studies of bone marrow cells and megakarocytes growing in culture from blood precursors. American Journal of Pathology 102: 10-19 Cramer E M, Vainchenker W, Vinci G, Guichard J, Breton- Gorius J 1985 Gray-platelet syndrome: immunoelectron microscooic localization of fibrinoeen and von Willebrand
45.
46.
Lagarde M, Byron P A, Vargaftig B B, Dechavanne M 1978 Impairment of platelet thromboxane A2 generation and of the platelet release reaction in two patients with congenital deficiency of platelet cyclooxygenase. British Journal of Haematology 38: 251-266 Defreyn G, Machin S J, Carreras L 0, Dauden M V, Chamone D A F, Vermylen J 1981 Familial bleeding tendency with partial platelet thromboxane AZ synthetase deficiency: reorientation of cyclic endoperoxide metabolism British Journal of Haematology 49: 29-41 Samama M, Lecrubier C, Conard J, Hotchen M, Breton- Gorius J, Vargaftig B, Chignard M, Lagarde M, Dechavanne M 1981 Constitutional thrombocytopathies with subnormal response to thromboxane Al. British Journal of Haematology 48: 293-303 Hardisty R M, Hutton R A 1967 Bleeding tendency associated with a new abnormality of platelet behaviour. Lancet i: 983-984
factor in ‘platelets and megakaryoc”$es. Blood 66: 1309-l 3 16 Nurden A T, Kunicki T T J, Dupuis D, Soria C, Caen J P 1982 Specific protein and glycoprotein deficiencies on platelets isolated from two patients with the gray platelet syndrome. Blood 59: 709-718 Levy-Toledano S, Caen J P, Breton-Gorius J, Rendu F, Cywiner-Golenzer C, Dupuy E, Legrand Y, Maclouf J 1981 Gray platelet syndrome: alpha granule deficiency. Its influence on platelet function. Journal of Laboratory and Clinical Medicine 98: 83 l-884
47.
48.
49.
50.
51.
Weiss H J, Witte L D, Kaplan K L, Lages B A, Chemoff A, Nossel H L, Goodman D S, Baumgartner H R 1979 Heterogeneity in storage pool deficiency: studies on granule- bound substances in 18 patients including variants deficient in alpha granule platelet factor 4, betathromboglobulin and platelet derived growth factor. Blood 54: 1296-1319 Hermansky F, Pudlak P 1959 Albinism associated with hemorrhagic diathesis and unusual pigmented reticular cells in the bone marrow: report of two cases with histochemical studies. Blood 14: 162-169
52.
53.
54. Rendu F, Nurden A T, Lebret M, Caen J P 1979 Relationship between mepacrine-labelled dense body number, platelet capacity to accumulate 14C-5HT and platelet density in the Bernard-Soulier and Hermansky- Pudlak syndromes. Thrombosis and Haemostasis (Stutg) 42: 694704
Kaplan D R, Chao F C, Stiles C D, Antoniades H N, Scher C D 1979 Platelet alpha granules contain a growth factor for fibroblasts. Blood 53: 1043-1052 Caen J P, Deschamps J F, Bodevin E, Bryckaert M C, Dupuy E, Wasteson A 1987 Megakaryocytes and myelofibrosis in gray platelet syndrome. Nouvelle Revue Francaise D Hematologie 29: 109-l 14 Caen J P 1972 Glanzmann thrombasthenia. Clinics in Haematology 1: 383-392 Nurden A T, Caen J P 1974 An abnormal platelet glycoprotein pattern in three cases of Glanzmann’s thrombasthenia. British Journal of Haematology 28: 253-260 Degas L, Dautigny A, Brouet J C, Colombani M, Ardaillou N, Caen J P, Colombani J 1975 A molecular defect in thrombasthenic platelets. Journal of Clinical Investigations 56: 236240 Hagen I, Nurden A T, Bjerrum 0 J, Solum N 0, Caen J P 1980 Immunochemical evidence for protein abnormalities in platelets from patients with Glanzmann’s thrombasthenia and Bernard-Soulier syndrome. Journal of Clinical Investigation 65: 722-731 Pidard D. Montgomery R R, Bennet J S, Kunicki T J 1983 Interaction of AP-2, a monoclonal antibody specific for the human platelet glycoprotein IIb-IIIa complex, with intact platelets. Journal of Biology and Chemistry 25& 12582-12586 Nurden A T, Didry D, Kieffer N, McEver R 1985 Residual amounts of glycoproteins IIb and IIIa may be present in the platelets of most patients with Glanzmann’s thrombasthenia. Blood 65: 1021-1024
55.
Buchanan G R, Handin R I 1976 Platelet function in the Chediak-Higashi syndrome. Blood 47: 941-948 Rendu F, Breton-Gorius J, Lebret M, Klebanoff C, Buriot D, Griscelli C, Levy-Toledano S, Caen J P 1983 Evidence that abnormal platelet functions in human Chediak-Higashi syndrome are the result of lack of dense bodies. American Journal of Pathology If 1: 307-3 14 Baldini M G 1972 Nature of the platelet defect in the Wiskott-Aldrich syndrome. Annals of the New York Academy of Sciences 201: 437444 Grottum K A, Hovig T. Holmsen H, Abrahamsen A F. Jeremic M, Seip M 1969 Wiskott-Aldrich syndrome: qualitative defects and short platelet survival. British Journal of Haematology 17: 373-388 Shapiro R S, Gerrard J M, Perry G S, White J G, Krivit W, Kersey J H 1978 Wiskott-Aldrich syndrome: detection of a carrier state of metabolic stress of platelets. Lancet i: 121-123 Parkman R, Remold-O’Donnel E, Kenney D M, Perrine S, Rosen F S 1981 Surface protein abnormalities in lymphocytes and platelets from patients with Wiskott- Aldrich syndrome. Lancet ii: 1387-l 389 Pidard D, Didry D, Lx Deist F, Bellucci S, Nurden A T,
56.
Hourdille P, Fialon P, Belloc F, Namur M, Boisseau M R, Nurden A T 1986 Megakaryocytes from the marrow of a patient with Glanzmann’s thrombasthenia lacked gp IIt-IIIa complexes. Thrombosis and Hemostasis 56: 66-70 Coller B S 1980 Interaction of normal, thrombasthenic and Bernard-Soulier platelets with immobilized fibrinogen: defective platelet-fibrinogen interaction in thrombasthenia. Blood 55: 169-178
57.
58.
Lee H, Nurden A T, Thomaidis A, Caen J P 1981 Relationship between fibrinogen binding and the platelet glycoprotein deficiencies in Glanzmann’s thrombasthenia type I and type II. British Journal of Haematology 48: 48-57 Nachman R L. Leune L L K 1982 Comalex formation of
59.
60.
61.
62.
platelet membiane glicoproteins IIb III; with fibrinogen. Journal of Clinical Investigation 69: 263-269 Gartner T K, Gerrard J M, White J G, Williams D C 1982 Fibrinogen is the receptor for the endogenous lectin of human platelets. Nature 289: 688690 Langer b G, Gonnella P A, Nachmias V T 1984 Alpha actinin and Vinculin in normal and thrombasthenic platelets. Blood 63: 60(X14 Plow E F, Srouji A H, Meyer 0, Marguerie G, Ginsberg M H 1984 Evidence that three adhesive proteins interact with a common recognition site on activated platelets. Journal of Biology and Chemistry 259: 5388-5391 Gartner T K. Bennett J S 1985 The tetrapeptide analogue of

26 CONGENITAL PLATELET DISORDERS
63.
64.
65.
66.
61.
the cell attachment site of fibronectin inhibits platelet aggregation and fibrinogen binding to activated platelets. Journal of Biology and Chemistry 260: 11891-l 1894 Ginsberg M H, Forsyth J, Lightsey A, Chediak J, Plow E F 1983 Reduced surface expression and binding of fibronectin by thrombin stimulated thrombasthenic platelets. Journal of Clinical Investigation 71: 619-624 Ruggeri Z M, Bader R, De Marco L 1982 Glanzmann’s thrombasthenia: Deficient binding of von Willebrand factor to thrombin stimulated platelets. Proceedings of the National Academy of Sciences USA 79: 60386041 Nurden A T, Rosa J P, Fournier D, Legrand C, Didry D, Parquet A, Pidard D 1987 A variant of Glanzmann’s thrombasthenia with abnormal glycoprotein IIbIIIa complexes in the platelet membrane. Journal of Clinical Investigation 79: 962-969 Caen J P, Rosa J P, Soria C, Boizard B 1983 Variant de thrombasthenie Paris I Lariboisibre, anomalie moltculaire du complexe glycoprotbinique plaquettaire IIb/IIIa. Comptes Rendus de l’Acad&mie des Sciences de Paris 296: 417-419 Weiss H J 1987 Platelet aggregation, adhesion and adenosine diphosphate release in thrombopathia (platelet factor 3 deficiency). American Journal of Medicine 43: 570-578
68.
69.
70.
71.
72.
73.
Girolami A, Brunett A, Fioretti D 1973 Congenital thrombocytopathy (platelet factor 3 defect) with prolonged bleeding time but normal platelet adhesiveness and aggregation. Acta Haematologica 50: 116-123 Minkoff M, Wu K K, Walasek J 1980 Bleeding disorder due to an isolated platelet factor 3 deficiency. Archives of Internal Medicine 140: 366367 Miletich J P, Kane W H, Hofmann S L, Stanford N, Majerus P W 1979 Deficiency of factor Xa-factor Va binding sites on the platelets of a patient with a bleeding disorder. Blood 54 1015-1022 Lacombe M, D’Angelo G 1963 Etude sur une thrombopathie familiale. Nouvelle Revue Fran&se D Hematologie 3: 611-614 Milton J G, Frojmovic M M 1979 Shape changing agents produce abnormally large platelets in a hereditary “giant platelets syndrome (MPS)“. Journal of Laboratory and Clinical Medicine 93: 154-I 61 Bellucci S, Devergie A, Gluckman E, Tobelem G, Lethielleux P, Benbunan M, Schaison G, Boiron M 1985 Complete correction of Glanzmann’s thrombasthenia by allogeneic bone-marrow transplantation. British Journal of Haematology 59: 635-641