Congenital hearing loss - UCSF CME · 2013-11-26 · Congenital hearing loss Which tests and why...
14
11/9/2013 1 Congenital hearing loss Which tests and why does it matter? Dylan K. Chan, MD, PhD Assistant Professor Pediatric Otolaryngology University of California, San Francisco UCSF Otolaryngology Update Saturday, November 9, 2013 11:30-11:50 am I have nothing to disclose Congenital hearing loss Outline How are children identified? Newborn hearing screening, school screening Why to work up? Knowledge, prognosis, counseling, intervention How to work up? History, physical, diagnostic testing Which tests to consider? Imaging, genetic testing, CMV How to decide? Audiogram, cost, side effects, impact Goal is not to provide a strict workup algorithm, but to build understanding to facilitate informed counseling of patients and families Newborn Hearing Screening Goals Birth AABR or DPOAE- based screen (x2 to confirm) By one month Outpatient screen/rescreen By three months Diagnostic audiology evaluation (ABR) Otolaryngology evaluation By six months Community/school services initiated Ongoing audiology/otolaryngology management REFER REFER Confirmed hearing loss Goal diagnosis, medical treatment, and early intervention initiated by 6 months.
Transcript of Congenital hearing loss - UCSF CME · 2013-11-26 · Congenital hearing loss Which tests and why...

11/9/2013
1
Congenital hearing lossWhich tests and why does it matter?
Dylan K. Chan, MD, PhDAssistant ProfessorPediatric OtolaryngologyUniversity of California, San Francisco
UCSF Otolaryngology UpdateSaturday, November 9, 201311:30-11:50 am
I have nothing to disclose
Congenital hearing loss Outline
How are children identified? Newborn hearing screening, school screeningWhy to work up? Knowledge, prognosis, counseling, interventionHow to work up? History, physical, diagnostic testingWhich tests to consider? Imaging, genetic testing, CMVHow to decide? Audiogram, cost, side effects, impact
Goal is not to provide a strict workup algorithm, but to build understanding to facilitate informed counseling of patients and families
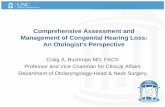
Newborn Hearing Screening Goals
Birth AABR or DPOAE- based screen (x2 to confirm)
By one month Outpatient screen/rescreen
By three monthsDiagnostic audiology evaluation (ABR)Otolaryngology evaluation
By six monthsCommunity/school services initiatedOngoing audiology/otolaryngology management
REFER
REFER
Confirmed hearing
loss
Goal diagnosis, medical treatment, and early intervention initiated by 6 months.

11/9/2013
2
Newborn Hearing Screening Outcomes
Each year in CA:
500,000 infants screened 93% of all births in CA
10,000 infants (1:50) REFER Diagnostic program initiated
1,000 infants (1:500) diagnosed with Congenital SNHL http://trialx.com
Newborn Hearing Screening Outcomes
Each year in CA:
500,000 infants screened 93% of all births in CA
10,000 infants (1:50) REFER Diagnostic program initiated
1,000 infants (1:500) diagnosed with Congenital SNHL
Plus an additional 1:500 children with postnatal permanent childhood hearing impairment (PCHI)
http://trialx.com
All children with SNHL
50% acquired 50% genetic
67% non-syndromic33% syndromic
50% GJB2
50%Non-GJB2
Congenital Sensorineural Hearing Loss Epidemiology
Pendred’sUsher’s
CMVTORCH
infections
All children with SNHL
50% acquired 50% genetic
67% non-syndromic33% syndromic
50% GJB2
50%Non-GJB2
Congenital Sensorineural Hearing Loss Epidemiology
Pendred’sUsher’s
CMVTORCH
infections
Early intervention + hearing aids or cochlear implantation

11/9/2013
3
Congenital Sensorineural Hearing Loss Why test?
Knowledge
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?

11/9/2013
4
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes What else is wrong with my child?
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes What else is wrong with my child?
Family counseling
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes What else is wrong with my child?
Family counseling What does this mean for my other kids?

11/9/2013
5
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes What else is wrong with my child?
Family counseling What does this mean for my other kids?
Intervention
Congenital Sensorineural Hearing Loss Why test?
Knowledge Why can’t my child hear?
Prognosis Is the hearing going to get worse?
Exclusion of other causes What else is wrong with my child?
Family counseling What does this mean for my other kids?
Intervention What can we do about it?
Congenital Sensorineural Hearing Loss How to work up?
HistoryPhysical ExamDiagnostic Tests
History Syndromic hearing loss
Associations with syndromic SNHL apparent from personal or family history
Visual impairment Usher’sBranchial cleft anomalies Branchio-oto-renalThyroid dysfunction/goiter Pendred’sSudden death/arrhythmia Jervell Lange-NielsenRenal/urinary complaints Alport’s, branchio-oto-renalPigmentation disorders Waardenburg

11/9/2013
6
History Non-syndromic hearing loss
Causes of non-syndromic SNHL apparent from history
Infectious Toxoplasmosis, syphilis, rubella, CMV, HSV, meningitis
Ototoxic drugs Gentamicin, cisplatinGenetic Family history, consanguinityHyperbilirubinemia JaundiceTrauma EVA-related sudden hearing loss
Physical Exam Syndromic hearing loss
Associations with syndromic SNHL apparent from physical exam
Goiter Pendred’sCraniofacial abnormalities MultipleBranchial cleft anomalies Branchio-oto-renalPreauricular pits Branchio-oto-renalPigmentation abnormalities Waardenburg’s
Diagnostic tests Congenital hearing loss
What next?
1) Work up potential causes revealed in H&P• Visual loss -> ophthalmology consult• Urinary problems -> renal US• Branchial cleft anomalies -> renal US• Goiter or thyroid problems -> TFTs, genetic testing (SLC26A4), imaging (EVA)• History of syncope or arrhythmia -> EKG• ANY syndromic association -> genetics consult
Diagnostic tests Congenital hearing loss
What next?
1) Work up potential causes revealed in H&P• Visual loss -> ophthalmology consult• Urinary problems -> renal US• Branchial cleft anomalies -> renal US• Goiter or thyroid problems -> TFTs, genetic testing (SLC26A4), imaging (EVA)• History of syncope or arrhythmia -> EKG• ANY syndromic association -> genetics consult
2) If H&P unrevealing:• do NOT empirically pursue these tests for specific syndromic causes.• DO consider one of three core diagnostic tests

11/9/2013
7
Non-syndromic hearing loss Core diagnostic tests
1) Imaging1) CT2) MRI
2) Genetic testing1) Connexin 26/302) Pendred’s3) Usher’s4) Complete hearing loss gene array testing
3) CMV testing1) Urine PCR (active infection)2) Newborn blood spot PCR (congenital infection)
Non-syndromic hearing loss Core diagnostic tests
1) Imaging1) CT2) MRI
2) Genetic testing1) Connexin 26/302) Pendred’s3) Usher’s4) Complete hearing loss gene array testing
3) CMV testing1) Urine PCR (active infection)2) Newborn blood spot PCR (congenital infection)
Bony anomalies CT
Right: http://www.nidcd.nih.gov/health/hearing/pages/eva.aspxLeft: http://american-hearing.org/disorders/congenital-deafness/
Enlarged vestibular aqueductMondini dysplasia
Bony anomalies MRI vs. CT
Right: http://www.nidcd.nih.gov/health/hearing/pages/eva.aspx

11/9/2013
8
Nerve anomalies MRI
Oblique sagittal plane FIESTA MRI – internal auditory canal
Normal anatomy Cochlear nerve aplasiaYan et al., 2013
Nerve anomalies CT
Normal anatomy Cochlear nerve aplasia
Narrowing of IACNot always seen on CT
(~50% of cases of known, MRI-demonstrated cochlear nerve hypoplasia)
Yan et al., 2013
Nerve anomalies CT
Yan et al., 2013
Narrowing of cochlear nerve canal <1.5 mmSlightly more demonstrable on CT than IAC narrowing
(~70% of cases of known, MRI-demonstrated cochlear nerve hypoplasia)
Imaging CT vs MRI
CT
Somewhat better bony anatomy
MRI
Much better neural anatomy

11/9/2013
9
Imaging Side effects and costs
CT
Somewhat better bony anatomy
RadiationLess sedation
Less expensive
MRI
Much better neural anatomy
No radiationMore sedation
More expensive
Imaging CT and MRI risk
Miglioretti et al., 2013
Single anesthetic exposure before age 3
Ing et al., 2012
Up to 1:570 risk of cancer with a single head CT under 5 years
Two-fold risk of neurocognitive disability with single anesthetic under 3 years
Could not adjust for disease confounder
Imaging Impact
How does information gleaned from imaging affect patient management?
EVA recommendations regarding head trauma
Temporal-bone abnormalities surgical planning
Cochlear nerve hypoplasia cochlear implant candidacy
Imaging CT vs MRI
Recommendations
1) Cochlear implant candidates MRI with or without CT
2) All others MRI or CT at appropriate age after discussion with parents

11/9/2013
10
Non-syndromic hearing loss Core diagnostic tests
1) Imaging1) CT2) MRI
2) Genetic testing1) Connexin 26/302) Pendred’s3) Usher’s4) Complete hearing loss gene array testing
3) CMV testing1) Blood/urine PCR (active infection)2) Newborn blood spot (congenital infection)
Genetic testing GJB2/GJB6
1/2000 general population1/10-1/50 carrier frequency
20% of congenital SNHL20% of patients with postnatal permanent childhood hearing impairment20% progressive20% asymmetric
Strong association of ethnicity with mutation, prevalence, and hearing
35delG
R143W
235delCV37IW24X
167delCcIVS1+1G>A
Cx26 hearing loss Common mutations
Chan et al., 2013
Cx26 hearing loss Severity
0%
50%
100%
T/T NT/T NT/NT
profound
severe
moderate
mild
N = 1531 Snoeckx et al., 2006
Perc
ent o
f ind
ividu
als
Genotypei.e. 35delG i.e. V37I
% of
all Cx
26 he
aring
loss

11/9/2013
11
Cx26 hearing loss Progression
Chan et al., 2010
Perc
ent o
f ind
ividu
als
Genotype
* p < 0.01
Genetic testing Disease-specific panels
Gene Location #genes tested
Turnaround time
Cost (approximate)
Indication
GJB2/GJB6 (Connexin 26)
Stanford,multiple
2 1-3 wks $400 Non-syndromicSNHL
SLC26A4(Pendred’s)
Stanford, Cincinnati, Boston
1-3 4 wks $1100 SNHL + EVA or thyroiddysfunction
Usher’s panel Cincinnati,Boston
9 8-12 wks $2500 SNHL + visual dysfunction
Genetic testing Next-generation sequencing arrays
Platform Location #genes tested
Turnaround time
Cost (approximate)
OtoSeq Cincinnati 23 12 wks $3500 (self)$4300 (insurance)
OtoGenome Boston 70 8-12 wks $4000
OtoScope Iowa 66 6 months $1500
Genetic Testing Impact
Any cause identified genetic counseling/family planning
Syndromic association identified careful screening for associated phenotype
Specific mutations increased risk of progressive hearing loss, ototoxicity
Future therapeutic options gene therapy

11/9/2013
12
Non-syndromic hearing loss Core diagnostic tests
1) Imaging1) CT2) MRI
2) Genetic testing1) Connexin 26/302) Pendred’s3) Usher’s4) Complete hearing loss gene array testing
3) CMV testing1) Urine PCR (active infection)2) Newborn blood spot (congenital infection)
Congenital CMV infection1:500 newborns (higher with lower socioeconomic status)
CMV Epidemiology
10% symptomatic
30-65% SNHL
90% asymptomatic
7-15% SNHL (by age 6)
Overall 20-30% of CMV (+) with SNHL
10-60% of SNHL with CMV (+)Misono et al., 2011
Prenatal healthy pregnant women and newborns not routinely tested for CMV
Newborn screening saliva PCR assays (not routinely done)
Neonatal (up to three weeks) PCR assay from urine or blood
Postnatal PCR assay from dried heel sticks performed for newborn screening
CMV Testing options
Prognosis High risk of progressive hearing loss
Treatment IV ganciclovir, PO valganciclovir. Side effects, unclear treatment window
Cochlear implantation Overall benefit, but outcomes worse
CMV Impact

11/9/2013
13
Non-syndromic hearing loss Core diagnostic tests
1) Imaging1) CT2) MRI
2) Genetic testing1) Connexin 26/302) Pendred’s3) Ushers4) Complete hearing loss gene array testing
3) CMV testing1) Urine PCR (active infection)2) Newborn blood spot (congenital infection)
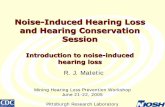
Core diagnostic tests How to choose?
1) Diagnostic yield 2) Audiogram configuration 3) Cost4) Side effects5) Potential for intervention/changes in management
Non-syndromic hearing loss Core diagnostic tests
Test Imaging Genetics CMV
Diagnosticyield
10-30%Audiogram dependent
10-30%Ethnicitydependent
10-30%Region dependent
Audiogram (Unilateral HL)
+++ + ++
Cost + (CT)++ (MRI)More with sedation
+ (Cx26)+++ (full screen)
+ (urine PCR)? (blood spot)
Risks/side effects
++/+++ + +
Impact +++ (for CI)+ (for others)
++ +++ (for neonates)+ (for others)
Core diagnostic tests How to choose?
Cochlear implant candidate MRI/CT -> Cx26/CMV
Unilateral imaging at appropriate age -> Cx26/CMV
All others Cx26/CMV -> imaging at appropriate age. Consider demographics.
If no findings, consider full genetic array testing

11/9/2013
14
Core diagnostic tests How to choose?
Cochlear implant candidate MRI/CT -> Cx26/CMV
Unilateral imaging at appropriate age -> Cx26/CMV
All others Cx26/CMV -> imaging at appropriate age. Consider demographics.
If no findings, consider full genetic array testing
Discuss with parents!
Thanks