Congenital Anomaly Register & Information Service caris review
reviewincluding 1998-2005 data
carisCongenital Anomaly Register & Information Service
Neural tube defects page6
Disorders of the central nervous system page12
inside...
Key points oncongenital anomalies in Wales1998-2005 page4
CAR Sonline ar-y-we
2 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Welcome to the 2005 CARIS annualreview. This year our special articlesfocus on major anomalies of the centralnervous system.
Detailed data tables are available from the CARIS website onwww.wales.nhs.uk/caris
We would like to express our sincerethanks to all contributing healthprofessionals for their continuing support.
Margery Morgan, Lead Clinician Judith Greenacre, Director of InformationDavid Tucker, CARIS Manager
* also accessible through the HOWIS (NHS Wales) website at www.howis.wales.nhs.uk/caris
Write CARIS OfficeLevel 3 West WingSingleton HospitalSWANSEASA2 8QA
Phone 01792 285241(WHTN 0 1883 6122)
Fax 01792 285242(WHTN 0 1883 6123)
e-mail [email protected]
web www.wales.nhs.uk/caris
Published by CARIS ISBN 0-9537080-7-1
© CARIS 2006
CAR Sonline ar-y-we
Desi
gned
by
RIDL
ER W
EBST
ER L
IMIT
ED 0
1792
582
100
Foreword
The CARIS team at the 2005 South Wales Annual Meeting.
We are (left to right) David Tucker, Debbie Rogers, HelenJenkins, Margery Morgan, Val Vye, Judith Greenacre.
CARIS, the Congenital Anomaly Register andInformation Service for Wales, is based at SingletonHospital, Swansea. It is funded by the Welsh AssemblyGovernment and is part of NHS Wales.
CARIS aims to provide reliable data oncongenital anomalies in Wales. These dataare used to assess:
patterns of anomalies in Wales
antenatal screening / interventions
health service provision for affectedbabies and children
possible clusters of birth defectsand their causes
We collect data on any baby or fetus forwhom pregnancy ended after 1st January1998, where the mother is normally residentin Wales at the end of pregnancy.
CARIS uses a multiple source reportingsystem and, at present, over 100 individualsor agencies regularly send us information.Data from clinical and laboratory sources isreported via warning cards, reporting formsand data exchanges. CARIS co-ordinatorsin each trust are responsible for much of theclinical reporting (details available from ourwebsite). In the CARIS office, data arecollated, information is coded and qualitycarefully checked. The data are thenavailable for feedback to clinicians –paediatricians, ultrasonographers, midwives,etc. We also supply information to theNational Assembly for Wales, EUROCAT,International Clearing House for BirthDefects and the Office for National Statistics(NCAS) for surveillance.
We cannot overemphasise the importancewe give to data confidentiality. We operate astrict security and confidentiality policy andhave gained support under Section 60 ofthe Health and Social Care Act 2001. This means that the register can continuecollecting and analysing data.
CARIS has set up an Expert Advisory Groupto advise on future developments andmonitor progress of the register.
Over 37,000 recorded pregnancies occur in Wales each year. Of these, about threequarters are registered as live or still births,the rest ending in termination orspontaneous loss of the fetus before the24th week of pregnancy. About 3% of births take place at home. Wales has 13consultant obstetric units and 10 midwiferyled units. The majority of births take place in these units. However, a significant numberof births to Welsh mothers occur in Englishhospitals. Good links with congenitalanomaly registers that border Wales(Mersey, West Midlands and the South Westof England) remain very important.
Clinical reporting is the most importantsource of information for CARIS, especiallyfor those babies who:
die but do not have a post mortem
survive and have anomalies notrequiring immediate specialist help.
Diagnostic services, particularly ultra soundand pathology, can alert us to a case or give valuable further information.
Regional specialist services, includingcytogenetics, can help by providing moredetails of the anomalies involved.
We also link to other databases, such asPROTOS (Cardiff), the All Wales PerinatalSurvey and the Standard Child HealthComputer System.
annual review | 3
What is CARIS?
12,149 cases with confirmed congenitalanomalies have been reported to CARISwith pregnancy ending between 1st January 1998 and the 31stDecember 2005. These include livebirths, stillbirths, terminations ofpregnancy for congenital anomalies andmiscarriages (although reporting ofmiscarriages will inevitably beincomplete). This means that the gross*rate of known pregnancies affected bycongenital anomaly is 4.8%.
85% of cases were live born. The percentage of all live born babiesaffected by congenital anomalies is 4.0%.CARIS makes every effort to ensure thatbabies who die during the first year of lifeare identified. According to our records,over 96% of live born babies with acongenital anomaly survived to the end of their first year of life. This percentage ishigher than we have reported in previousyears, probably as a result of increasedavailability of data on survivors frominpatient hospital records and communitychild health computer systems.
In over half of cases only one birth defectwas recorded. In about 12% of cases anunderlying chromosomal disorder wasidentified that could account for many ofthe physical anomalies. The remainder ofcases had multiple anomalies of varyinglevels of complexity.
As in previous years defects of the heartand circulation were the largest singlegroup of anomalies, followed by defectsof the limbs, urinary system andmusculoskeletal system.
Overall rates of congenital anomalycontinue to be higher in male babies.
As before, marked variations incongenital anomaly rates are seenaround Wales, with apparently muchhigher rates for Swansea and Neath Port Talbot compared to other areas.Relatively lower rates are seen in, Mid Wales and parts of North Wales.Some of this variation remains due topersistent differences in reportingpractices across Wales (See Reporting of anomalies in Wales: CARIS Review2003). The areas with highest rates tendto have better survival rates for live bornbabies. This may, again, reflect betterreporting of cases in infancy, allowingmore survivors to be added to thenumbers from better reporting areas.
Rates for many anomalies in Walesappear relatively high when compared to other areas of Britain and Europe. This was also discussed in detail in the2003 CARIS review. We still suspect thatgood reporting in Wales accounts for alarge part of these differences butcontinue to keep the situation underreview.
Data tables and a more detailedcommentary are available on the CARIS website.
4 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Key points on congenital anomalies in Wales 1998-2005
SummaryGross* rates of congenital anomaliesreported is 4.8%.
85% of cases are live born.
96% of live born cases survive to the end of their first year.
Heart and circulatory defects are the largest single group.
Variations in rates exist around Wales.
Congenital anomaly rates in Wales areoften apparently higher than for otherareas of Europe or Britain.
*The gross rate includes all cases of anomaly recorded as miscarriages, terminations of pregnancy, live and stillborn babies
The team has been involved with projects in Wales, the United Kingdom and internationally.
WalesAnnual meetings were held in YsbytyGlan Clwyd and the National BotanicalGardens near Carmarthen. The focuswas on gut anomalies.
CARIS continued to collaborate withAntenatal Screening Wales supportingdevelopment of the new antenatalultrasound module of RADIS (radiologyinformation system) and a populationbased ultrasound soft marker study.
CARIS developed new sources of data,including inpatient data from Alder HeyHospital, relating to North Wales.
United KingdomBINOCAR:
CARIS gave presentations ongastroschisis and clinical coding ofanomalies at the annual meeting. David Tucker was appointed aschairman of the clinical coding working group.
InternationalGastroschisis and hypospadias datawere presented at the EUROCAT(European Collaboration of CongenitalAnomaly Registers) conference inPoznan, Poland in June 2005.
CARIS became a full member of the International Clearing House of BirthDefects, Surveillance and Research(ICBDSR)
We presented Welsh data on anomaliesassociated with maternal anti-depessants (SSRIs) at ICBDSRconference in Malta in September 2005.
Websiteswww.binocar.org.uk
www.eurocat.ulster.ac.uk
www.icbdsr.org
CARIS activity 2005
annual review | 5
6 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
A neural tube defect is a major congenital anomaly caused by abnormaldevelopment of the neural tube. The neural tube is the structure presentduring embryonic life which gives rise tothe central nervous system – the brain andspinal cord. Neural tube defects (NTDs)are among the most common anomaliesthat cause infant death and seriousdisability.
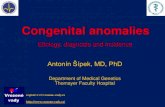
There are different types of neural tubedefects which include anencephaly, spinabifida, and encephalocele. In anencephaly there is absence of thecranial vault (skull) and absence of most or all of the cerebral hemispheres of thebrain. Encephalocele is a hernia of part of the brain and meninges (themembranes covering it) through a skulldefect. Spina bifida is an opening in thevertebral column encasing the spinal cord(figure 1).
436 cases of neural tube defect werereported to CARIS between 1998 - 2005.Of these:
• 185 had anencephaly• 204 had spina bifida• 55 had encephalocele(some cases have more than one type of NTD)
Neural tube defects usually occur asisolated defects but may also beassociated with chromosomal or othermultiple malformation syndromes (e.g. Meckel’s syndrome).
Picture of neural tube defects in WalesHistorically, the recorded prevalence ofneural tube defects in Wales has beenhigher than elsewhere1. A 1957 SouthWales study reported a rate of 115 neuraltube defects per 10,000 births2.Subsequent studies suggest that the ratehas declined. A 1992 study reported a rateof 21 per 10,000 total births, although thisonly covered parts of South Wales3. Data since CARIS was established showan all Wales prevalence rate of 17.1 per10,000 total births for the period 1998-2005 (95% CIs 15.5 to 18.7). The CARISrate for south east Wales for this timeperiod is 16.3 (95% CIs 14.0 to 18.6). The geographical areas studied aredifferent to earlier research making directcomparisons difficult. There is someevidence of a downward trend since 1998(figure 2).
Neural Tube Defects
1 Folic acid and the prevention of neural tube defects. DOH 19922 Laurence KM. The apparent declining prevalence of neural tube defects intwo counties of South Wales. Z Kinderchir 40 supplement I: 58-60 (1985)
3 Wales participation in the EUROCAT surveillance of congenital abnormalities:a report of the study in South Glamorgan and Gwent during 1992 (draft).Cotter M. Elder S, Laurence KM. WHCSA March 1994
Vertebrae Nerves & Spinal Cordin Lesion
Spina Bifida Lesion
figure 2: Time trend for neural tube defects in Wales (1998 – 2005).Source: CARIS
figure 1: diagram showing a spina bifida defect
0
5
10
15
20
25
Years
Rat
es p
er 1
0,00
0 to
tal b
irths
1998 1999 2000 2001 2002 2003 2004 2005
All NTDsAnencephaly
Spina BifidaEncephalocele
This report was originally preparedby Siobhan Jones, Specialist Traineein Public Health, National PublicHealth Service for Wales.
annual review | 7
Neural Tube Defects
At local authority level, there are markeddifferences in rates across Wales, that arenot explained simply by known patterns ofvariations in reporting. Rates are generallyhigher in the north and south with muchlower levels in mid Wales, although, atregional level, these differences are notstatisically significant. Carmarthenshire hasthe highest rate of neural tube defects,significantly higher than that for Wales as awhole. This may be a chance finding, butCARIS will work with others to investigatethis further over the coming year.
Wales and EuropeWales has one of the highest rates of neuraltube defects reported in Europe. (Bulgariareports higher rates, but data is notcomplete for comparable years to CARIS).
DiagnosisUltrasoundUltrasound screening is very effective atdetecting neural tube defects. A systematicreview of the effectiveness of ultrasoundscreening reported a detection rate for allneural tube defects of 76.4% on routinesecond trimester ultrasound scan. The detection rate for anencephaly is reportedas 97.4% and 66.7% for spina bifida.
figure 3: Rates of neural tube defects byUnitary Authority (1998-2005)
Source: CARIS
figure 4: Rates of isolated NTD in Europe(1998-2004): Highest reportingregisters submitting complete data.
Source: EUROCAT
Rate 10 - 14
Rate 15 - 19
Rate 20 - 24
Rate 25 - 30
Rate 5 - 9CeredigionPowysConwyMonmouthshireNewportPembrokeshireCardiffWrexhamThe Vale of GlamNeath Port TalbotRhondda CynonDenbighshireMerthyr TydfilSwanseaCaerphillyGwyneddFlintshireTorfaenBlaenau GwentIsle of AngleseyBridgendCarmarthenshire
0
2
4
6
8
10
12
14
16
18
Wal
es
Wes
sex
(Eng
land
)
Eur
ocat
Par
is (
Fra
nce)
Registers
Sax
ony
Anh
alt
(Ger
man
y)
Ant
wer
p (B
elgi
um)
Rat
es p
er 1
0,00
0 to
tal b
irths
Vau
d(S
witz
erla
nd)
Bas
que
Cou
nty
(Spa
in)
Oxf
ord
(UK
)
Mal
ta
Wie
lkop
olsk
a(P
olan
d)
Hai
nuat
(B
elgi
um)
Net
herla
nds
Tusc
any
(Ita
ly)
20no associated chromosomal anomaly
associated chromosomal anomaly
8 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Neural Tube Defects
The review reports the detection rate forencephalocele as 100%, although this isbased on small numbers – 7 out of 7 casesacross 11 studies4.
Anencephaly can be detected by notingabsence of the fetal skull and can besuspected as early as the 9th week. Spinabifida is diagnosed by looking for wideningof the spine and assessing the skin overlyingit. A banana shaped cerebellum and alemon shaped fetal skull are also features.
CARIS data show that an abnormalultrasound was detected in 412 of 436mothers carrying a fetus with a neural tubedefect. In 24 mothers the diagnosis was notmade until delivery or miscarriage. This givesan overall case detection rate of 94.5 %Within this, detection rates for specificdefects are as follows:
• Anencephaly 99.5% (184/185)
• Spina bifida 89.7% (183/204)
• Encephalocele 87.3% (48/55)
4 Bricker L, et al. Ultrasound screening in pregnancy: a systematic review of the clinical effectiveness, costeffectiveness, and women’s view. Health TechnologyAssessment. 2000; Vol 4: No 16
leg
spine
lemonshaped
skull
spina bifida
maternalbladder
dilatedventricle
absent skull
Neural Tube Defects
annual review | 9annual review | 9
Alpha-fetoproteinSerum alpha-fetoprotein is a protein mainlyproduced by the fetal liver. It enters theamniotic fluid through fetal urination anddiffuses across the placenta into thematernal circulation.
Open neural tube defects (not covered by skin) cause alpha-fetoprotein to leakinto the amniotic fluid and give a raisedserum value.
Raised alpha-fetoprotein levels werereported in 100 cases of neural tubedefect reported to CARIS. This representsabout a quarter of all cases. Reporting of raised AFP levels to CARIS is notcomplete as this is no longer a screeningtest for neural tube defects in Wales.However, in practice, if a raised AFP isdetected on routine Down screening it islikely to prompt an earlier antenatalanomaly scan.
Risk factorsIn the majority of cases the cause of a neural tube defect is unknown. However some women are at increasedrisk of having a baby with the condition. The factors that can lead to this increased risk are:
• Mothers with a history of a previouspregnancy resulting in a fetus with aneural tube defect
• Mothers with type 1 diabetes mellitus
• Mothers with low serum folate levels
Low serum folate levels can arise because of:
• Low dietary intake of folic acid
• Taking certain epileptic drugs that canaffect folate metabolism
• A genetic defect called methylenetetrahydrofolate reductase deficiency.
CARIS has the following data on these risk factors.
• Epilepsy was reported in 3.9% (13 / 331)mothers of babies with a neural tubedefect where epilepsy status is recorded.
• Diabetes was reported in 4.7% (16 / 338) mothers of babies with aneural tube defect where diabetic statusis recorded.
• 9 mothers were recorded as having had a fetus with a neural tube defect in previous pregnancies. This gives arecurrence risk of 2.1% in Wales (the lower end of quoted rates in theliterature)5. It is likely that this figure willrise as CARIS collects further years of data.
5 Harper, PS. Practical Genetic Counselling (5th Edn)1998. Butterworth.
Neural Tube Defects
10 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Folic Acid CampaignThe research evidence on folatesupplementation suggests that it reducesthe prevalence of neural tube defectssubstantially6. Guidance on periconceptualfolic acid supplementation was first issuedby the Department of Health in 1991. In 1992 the UK Expert Advisory Groupwent on to state that first occurrences ofneural tube defects could be reduced byincreasing folic acid consumption.Currently, folic acid supplements arerecommended for all women prior toconception and during the first 12 weeksof pregnancy to help reduce the incidenceof neural tube defects5,7. The recom-mended dose for women who are not athigh risk of having a fetus affected by aneural tube defect is 400 mcgs daily.
It has been noted that although there wasa decline in neural tube defect affectedpregnancies between 1988 and 1999,there has been no detectable impact ofthe 1992 recommendation to increase folic acid intake8. There are a number ofsuggestions as to why this might be the case:6-8
• The high proportion of unplannedpregnancies limits the use of pre-conceptual supplements
• There is a slow spread of information towomen of child bearing age and primarycare providers about the importance offolic acid supplementation
• Women who know about the benefits offolic acid supplementation and who plantheir pregnancies are not taking it at theright time
These findings have led to a debate aboutthe fortification of flour as a public healthmeasure, to increase the folic acid intakeof all women of childbearing age. The Scientific Advisory Committee onNutrition (SACN) has been considering this issue. In its report, Folic Acid and thePrevention of Disease (DOH 2005), it concluded that ‘the universal fortification of flour with folic acid would significantlyreduce the number of conceptions andbirths affected by neural tube defects’8. In June 2004 it was agreed not tointroduce mandatory fortification at thattime. This was due to concerns aboutvitamin B12 deficiency and in particular the risks to older people. There is concernthat folate may mask signs of vitamin B12deficiency7.
SACN are reviewing the issue and havedelayed the release of the latest reportwhile they continue to evaluate increasedfolic acid intake.
10 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
5 Harper, PS. Practical Genetic Counselling (5th Edn)1998. Butterworth.
6 Lumley J et al. Periconceptual supplementation withfolate and / or multivitamins for preventing neural tubedefects (Review) 2001. Accessed on line 2006 TheCochrane Collaboration. www.thecochranelibrary.com
7 Abramsky L et al. Has advice on periconceptual folatesupplementation reduced neural tube defects? TheLancet; 1999. Vol:354
8 SACN. Draft report on folate and disease prevention.Nov 2005 www.sacn.gov.uk
annual review | 11annual review | 11
Neural Tube Defects
Figure 8 shows the pattern of folic acidsupplementation in mothers reported toCARIS with a fetal abnormality and a fullycompleted CARIS form. There arelimitations to the data as the recording ofthis information is not always consistent inthe medical notes. The information wasunrecorded or not found in 28% of casenotes. In another 30% of case notes folicacid was recorded as taken but the starttime was unrecorded. It can also bedifficult for mothers to accurately recalltheir folic acid intake and the data in thiscan be subject to recall bias. Only 10% of mothers appear to take folic acid asrecommended.
Our data also shows that around 15% of mothers never took folic acid. As mightbe expected some mothers who have nottaken folic acid preconceptually start whenthey realise they are pregnant.
Of the 436 pregnancies affected by aneural tube defect, 200 mothers werereported as having taken folic acidsupplements at some time during thepregnancy. 37 mothers reported taking itpreconceptually. The proportions betweenneural tube defect mothers and all othermothers registered with CARIS are verysimilar for history of folic acidconsumption.
figure 8: History of starting folic acid from 8244 mothers in Wales with pregnancy ending in congenital anomaly, 1998-2005.Source: CARIS
15%
10%
6%
10%
1%
30%
28%
not taken
preconceptually
weeks 1-4
weeks 5-12
started after 1st trimester
started - notknown when
not recorded
12 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Congenital anomalies of the centralnervous system include disorders of thebrain and spinal cord.
The basic structure of the brain and spinalcord develops in the first eight weeksfollowing the last menstrual period. This isa complicated embryological pathway andas a result abnormal development of thebrain is common (CARIS data shows agross rate of 3.7 per 1000 live andstillbirths).
figure 9: central nervous system at 6 weeks gestation
Brain development9
12 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Disorders of the Central Nervous System
9 Before we are Born. Essentials of embryology and BirthDefects (6th Edn). Moore & Persaud. 2003 (Philadelphia)Saunders.
Week 1 - Last menstrual period.
Week 5 - Neural plate forms from the primitive streak andcurves to form the neural groove.
Week 6 - Neural groove forms the neural tube with toptwo thirds becoming the brain and the lowerthird becoming the spinal cord. The top endcloses first (failure to close can causeanencephaly or neural tube defect).Lumen of the tube forms the ventricular systemand central canal.Substance of the tube forms the brain andcord. Forebrain, midbrain and hindbraindevelop.
Week 7 - Forebrain divides into two parts:i) cerebral hemispheres, caudate, putamen
and lateral ventriclesii) thalami, hypothalamus, globus pallidus
and third ventricle.Midbrain develops with formation of theaqueduct of Sylvius connecting the third andfourth ventricles.Hindbrain divides into two parts whichcontribute to the fourth ventricle:
i) pons, cerebellar hemispheres and vermisii) medulla
(problems at this stage can causeholoprosencephaly and agenesis of thecorpus callosum).
Weeks 9/10 - Cerebral cortex forms as neurones migratealong fibres stretching from the lining of theventricles to the brain surface.
Weeks 23/27 - Development of gyri (ridges) and sulci (grooves).
Weeks 32/33 - Development of secondary and tertiary sulci(problems at this stage can cause lissencephalyand schizencephaly).
mid brain
forebrain
optic cup
hind brain
spinal cord
annual review | 13
The early weeks of pregnancy representthe most vulnerable period of braindevelopment but it continues to besuseptible to problems until delivery. Risks include sensitivity to medicationsparticularly anti-convulsants, warfarin andanti-malarials, alcohol and recreationaldrugs. Environmental influences such asinfection or irradiation can similarly affectdevelopment.
Microcephaly
Though literally meaning small head, theterm refers to restricted brain growth andoften is associated with learning disability.
It can be present at birth or may developin the first few years of life.
The baby’s head fails to grow normally asit matures.
Antenatal diagnosis10
Microcephaly is suspected when theultrasound measurement of headcircumference lies below the 3rd centile for gestational age. The face appears ofnormal size.
It is important to exclude an underlyingstructural abnormality of the brain (neuraltube defects, holoprosencephaly).Associated chromosomal disorders shouldbe excluded.
figure 10: fetal brain development
Causes
a) Genetic causes – most chromosomaldisorders, Angelman syndrome, Meckel- Gruber syndrome
b) Neurological disorders – von Recklinghausen disease, tuberous sclerosis
c) Environmental factors –cytomegalovirus, ionizing radiation,drugs including alcohol
Paediatric problems
Some children with microcephaly will havenormal intelligence and a head that growsbigger but still remaining below the normalgrowth curves.
Common features in the baby:• high pitched cry• small head• poor feeding• seizures • cerebral palsy• developmental delay• learning disability
annual review | 13
Disorders of the Central Nervous System
10 Textbook of Fetal Abnormalities. Twining P, McHugo J,Pilling D. 2000. Churchill Livingstone.
Congenital Anomalies of the Brain
wall
3 primaryvesicles
5 secondaryvesicles
adult derivativesof
cavity
forebrain
mid brain
hind brain
spinal cord
cerebalhemispheres
lateralventricles
third ventricle
aqueduct
upper part offourth ventricle
lower part offourth ventricle
walls cavities
thalami, etc
midbrain
ponscerebellum
medulla
14 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Microcephaly
Outcome
No treatment exists to restore the baby’shead to a normal size and shape. Supportis required to maximise potential and copewith associated disabilities. Medicationmay help to manage fits, hyperactivity andneuromuscular symptoms.
Some infants will only have mild disabilityand the prognosis will vary with eachindividual.
130 cases have been reported to CARISbetween 1998 – 2005 giving a grossprevalence rate of 5.1 per 10,000 totalbirths (95% CIs 4.2 to 6.0).
figure 11: Highest rates of isolatedmicrocephaly in Europe and the EUROCATaverage (1998 – 2004) Source: EUROCAT
Hydrocephalus
Hydrocephalus occurs when an abnormalamount of cerebrospinal fluid (CSF)accumulates in the ventricular system ofthe brain. The fluid can cause pressure inthe brain and result in mental and physicalproblems.
It is the most frequent brain anomaly with aprevalence of around 1 per 1000 live births(CARIS data).
CausesHydrocephalus may occur as an isolatedcongenital anomaly11 or may be associatedwith genetic conditions, intraventricularhaemorrhage, maternal infections or neural tube defects.
When the condition is associated withchromosomal anomalies, outlook is poorwith a high mortality and only half of thesurvivors developing normally.
For isolated hydrocephalus withoutassociated anomalies, the outlook is much better.
The physical causes for the excess fluidinclude:
a) aqueduct stenosis – the canalconnecting the 3rd and 4th ventriclebecomes blocked meaning only thelateral and 3rd ventricles are dilated
b) posterior fossa obstruction (DandyWalker syndrome, Arnold Chiarimalformation related to neural tubedefect)
c) choroid plexus adenoma - increasedproduction of CSF
d) impaired resorption of CSF byarachnoid villi.
Disorders of the Central Nervous System
11 Ouaba J et al. Prenatal isolated mild ventriculomegaly:outcome in 167 cases BJOG 2006; 113: 1072-1079
0
2
4
6
8
10
12
Sax
ony
Anh
alt
(Ger
man
y)
Hai
naut
(Bel
gium
)
Ant
wer
p(B
elgi
um)
Registers
Rat
es p
er 1
0,00
0 to
tal b
irths
Wal
es
Par
is (
Fra
nce)
EU
RO
CA
T
Net
herla
nds
Bas
que
Cou
nty
(Spa
in)
Wes
sex
(Eng
land
)
Wie
lkop
olsk
a(P
olan
d)
14
no associated chromosomal anomaly
associated chromosomal anomaly
EUROCAT data shows particularly highrates of microcephaly in Saxony Anhalt(Germany). Wales rates are significantlyhigher than for EUROCAT as a whole butcomparable to several other registers whohave submitted data for a comparableperiod (figure 11).
annual review | 15
figure 12: ultrasound showinghydrocephalus
Antenatal diagnosisThis is possible in the second trimester.Measurements of the lateral ventriclesgreater than 10 mm indicate enlargedventricles or ventriculomegaly. The choroidplexus can be seen as thinned or hangingdown in the ventricle and may be an earlysign of ventriculomegaly.
Isolated ventriculomegaly is consideredmild when measuring between 10 and15mm. There is a reported survival rate of 85%, with 85% of these childrendeveloping normally. Other anomaliesshould be sought and a fetal karyotypeoffered as the aneuploidy rate can be high.
Magnetic resonance12 can be of value.Poor prognostic features includemeasurements greater than 12mm,progressive enlargement, asymmetricalventriculomegaly and bilateralventriculomegaly. Female sex also appearsto adversely affect outcome. In most caseswith no associated malformations,ventriculomegaly regresses or remainsstable. Experience of antenatal ventriculo-amniotic shunting has not beenencouraging.
Paediatric problems13
The accumulation of cerebrospinal fluidcauses accelerated growth of the skullresulting in an increase in headcircumference, widening of the fontanellesand sutures of the baby.
Symptoms
Headache or irritabilityVomitingAnorexiaDrowsiness
Signs
Tense anterior fontanelle and splayedsuturesScalp vein distensionSunsetting (loss of upward gaze)Neck retraction or rigidityPupillary changesNeurogenic stridor Decerebration – absence of cerebralfunction
annual review | 15
Disorders of the Central Nervous System
12 Whitby EH, Paley MNJ, Griffiths PD. Magneticresonance imaging of the fetus. The Obstetrician &Gynaecologist 2006;8:71-77.
13 Forfar & Arneil’sTextbook of Pediatrics. (5th Edn)Campbell & McIntosh. 1998. Churchill Livingstone.
lemonshaped skull
choroidplexus
dilatedventricle
Outcome of hydrocephalus
Management depends on the cause of the hydrocephalus. The primary treatmentinvolves positioning of a shunt draining thecerebrospinal fluid from the ventricles intothe peritoneal cavity. This relieves thepressure on the brain and helps normaldevelopment.
CARIS has postnatal confirmation of 237 cases of hydrocephalus. This gives agross prevalence of 9.3 per 10,000 totalbirths (95% CIs 8.1 to 10.5). 150 caseswere detected antenatally giving adetection rate of 63.3%. Antenatal ventriculomegaly resolvedspontaneously in 30 cases.
figure 13: Highest rates of isolatedhydrocephaly in Europe and the EUROCATaverage (1998-2004) Source: EUROCAT
Dandy Walker Syndrome
This results from a failure in thedevelopment of the cerebellar vermisresulting in:
– communication between 4th ventricleand cisterna magna
– a posterior fossa cyst
– cerebellar hypoplasia
Antenatal diagnosis by ultrasound andmagnetic resonance
Associations
• chromosomal abnormalities (particularly trisomies) – 15-45%
• CNS associations• holoprosencephaly• agenesis of the corpus callosum• occipital encephalocoele• neuronal migration disorders• ventriculomegaly
Outlook – poor and depends onkaryotype and other abnormalities
Dandy Walker Syndrome
55 cases have been reported to CARISgiving a gross prevalence of 2.2 per10,000 total births (95% CIs 1.6 to 2.7). Of these, 14 were associated withchromosomal anomalies (26%).
Disorders of the Central Nervous System
16 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
0
2
4
6
8
10
12
14
Sax
ony
Anh
alt
(Ger
man
y)
Wal
es
Ant
wer
p(B
elgi
um)
Registers
Rat
es p
er 1
0,00
0 to
tal b
irths
Par
is(F
ranc
e)
Wes
sex
(Eng
land
)
EU
RO
CA
T
Wie
lkop
olsk
a(P
olan
d)V
aud
(Sw
itzer
land
)
Hai
nuat
(B
legi
um)
Bas
que
Cou
nty
(Spa
in)
Oxf
ord
(UK
)
Tusc
any
(Ita
ly)
Net
herla
nds
16
no associated chromosomal anomaly
associated chromosomal anomaly
Arnold Chiari Malformation
This is the commonest anomaly of thecerebellum involving:
• Descent of cerebellar vermis throughforamen magnum into vertebral canal of upper cervical spine
• CSF absorption impaired resulting inhydrocephalus
• Banana sign of cerebellum on ultrasound
• Association with neural tube defect
figure 14: ultrasound showing bananashaped cerebellum
Arnold Chiari Malformation
78 cases reported to CARIS giving a grossprevalence of 3.1 per 10,000 total births(95% CIs 2.4 to 3.7). 73 cases occurredas part of a neural tube defect (94%). 1 case was associated with Meckel-Gruber syndrome and the remaining 4 cases were isolated.
Holoprosencephaly
This results when the forebrain fails to divide into the lateral ventricles.Holoprosencephaly is a rare disorder (1 in 15,000 to 20,000 live births quoted).A recent study in the West Midlandsreported 1 in about 6000 births andterminations with a higher prevalence in
non-white ethnic groups. Though mostaffected infants die within 6 months somecan survive infancy (5 out of 16 livebirths inthis study)14. CARIS data include 36 cases,giving a gross prevalence of 1.4 per10,000 total births (95% CIs 0.9 to 1.9) or1:7090 cases - a similar finding to that ofthe West Midlands register.
Defects in forebrain development usually also include facial abnormalities.There is a strong association with majorabnormalities, trisomy 13 and otherchromosomal problems.
It is thought that this severe spectrum of anomalies stems from genetic orenvironmental problems occurring as early as the fifth to the seventh week ofdevelopment. There is an association withmaternal diabetes.
figure 15: ultrasound showingholosencephaly
Antenatal diagnosisThis is usually diagnosed in the secondtrimester. Fused thalami can be seenprotruding into the large single ventricle.There is microcephaly and brachycephaly(when the biparietal diameter is largecompared to the head circumference). The cavum septum pellucidum is absentand the cerebral mantle is incomplete.
Disorders of the Central Nervous System
annual review | 17
14 Ong S et al. An epidemiological study of holoprosencephaly from a regional congenital anomaly register: 1995 – 2004. (in press)
banana shapedcerebellum
skull bone
fused thalami
absent forebrain
Holoprosencephaly
Outcome
Because of the severity of the defect the prognosis is poor. Termination ofpregnancy is usually offered.
Genetic counselling for future pregnanciesis essential, with a quoted recurrence riskof 6% in those where there was nochromosomal abnormality.
Among CARIS cases, 6 were liveborn, of which 2 died within the first year of life.This gives a survival prevalence at 1 yearof life of 11% of recorded cases or 0.2 per 10,000 total births .
2 fetal losses and 1 stillbirth were reported.In the remaining 27 cases, pregnancy wasterminated.
17 cases had chromosomal abnormalitiesof which 12 were Trisomy 13.
Just one mother was known to haveinsulin dependent diabetes.
Lissencephaly and Schizencephaly
The surface of the brain hemispheres isinitially smooth. As growth occurs sulci(grooves) and gyri (convolutions) develop.These both allow a large increase in thesurface area of the cerebral cortex withoutgreatly expanding the size of the cranium.
Lissencephaly (smooth brain)
In this condition, the brain fails to developnormal gyri and sulci that are features of amature brain. In normal development, thebrain surface is featureless until the lateralsulcus develops during the fifth month.The brain then becomes increasinglyfolded with fissures and sulci from 28weeks. As the brain surface may not begin
to look like the adult appearance until aslate as 36 weeks gestation, this conditionis rarely diagnosed antenatally. Magneticresonance imaging has been reported asbeing useful diagnostically.
There is an association with disorders ofneuronal migration, midline developmentand several syndromes including agenesisof the corpus callosum. Abnormalities ofchromosome 17 can be present.
Disorders of the Central Nervous System
18 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
6 cms
8 cms
12 cms
figure 16: development of cortigal gyral patterns
With such pathology the prognosis is poorwith learning problems and developmentaldelay.
17 cases of this defect have been reportedto CARIS giving a gross prevalence of 0.7per 10,000 total births. A microdeletionfrom chromosome 17 (Miller-Diekersyndrome) was associated with 1 case.
Polymicrogyria forms part of the same spectrum of brain anomaly and 4 cases have been reported to CARIS (a gross prevalence rate of 0.2 per 10,000 total births).
Schizencephaly (split brain)
This occurs when there is a complete cleft through the cerebral hemisphere. This means that there is a communicationbetween the ventricular system and thesubarachnoid space. The clefts are usuallyin the parietal lobe, may be unilateral, andare often asymmetric.
Schizencephaly is thought to be related to a disorder of blood supply and cocainehas been implicated in its development.
Again magnetic resonance imaging (MRI)offers the best chance of diagnosing thecondition.
The outlook ranges from seizuremanagement alone to dealing withhemiparesis, global development delayand motor problems.
Just 3 cases have been reported to CARIS giving a gross prevalence of 0.1 per 10,000 total births.
Agenesis of the Corpus Callosum
The corpus callosum connects the twocerebral hemispheres across the midline.Its fibres are fully formed by the 20th weekof gestation.
Diagnosis
• Antenatal ultrasound – mild ventriculo-megaly, absent cavum septum pellucidum
• MRI can be helpful in making a diagnosis
Associations
• Other CNS disorders, geneticsyndromes, inborn errors of metabolism,and aneuploidy (trisomies 8,13,18)
Outlook
• Isolated agenesis has 85% chance ofnormality
Agenesis of the Corpus Callosum
43 cases have been reported of eithertotal or partial agenesis. This gives a grossprevalence rate of 1.7 per 10,000 totalbirths (95% CIs 1.2 to 2.2).
12 cases were associated withchromosomal anomalies, including 5 casesof Trisomy 18 and 2 cases of Trisomy 13.Two cases had teratogenic causes (1 fetal alcohol syndrome & 1 warfarinembryopathy).
Intrauterine Infection andthe Fetal BrainInfection affecting the fetal brain can causehaemorrhage, cerebral necrosis fromischaemia, calcification or ventriculomegaly.
Infection can also cause anaemia andthrombocytopenia which result in the mostcommon problem, an intracranial bleed. This can occur into the ventricles and causehydrocephalus or bleed into the brainsubstance forming a porencephalic cyst(lined with white matter and filled with CSF).
Disorders of the Central Nervous System
annual review | 19
Disorders of the Central Nervous System
20 | annual review CONGENITAL ANOMALY REGISTER & INFORMATION SERVICE
Infection early in the pregnancy may affect neuronal migration and causelissencephaly.
Microcephaly can be seen in infection withcytomegalovirus, rubella, toxoplasmosis,varicella, human immunodeficiency virus(HIV).
Hydrocephaly can be seen in infection withCMV, herpes simplex, treponema pallidumand varicella.
CARIS has some data on congenitalinfections, especially where associatedanomalies are suspected (table 3). It islikely however, that many cases gounnoticed or unreported.
Table 3: All congenital infections reported Source: CARIS
CongenitalInfection number
Parvovirus 14
Cytomegalovirus 12
Hepatitis (B & C) 10
Total viral infections 40
Congenital pneumonia 44
Toxoplasmosis 6
Diastematomyelia
Diastematomyelia involves tethering of the spinal cord caused by a bony orcartilaginous spur of the vertebral column.The cord is divided around the spur andusually reunites below it.
Embryologically it derives from persistenceof the neuroenteric canal which then splitsthe cord.
Maternal diabetes has been reported to be linked to the condition.
figure 17: ultrasound showingdiastomatomyelia
There is a strong association with neuraltube defects (36%). Kyphoscoliosis andskin changes above the area are common.
Antenatal diagnosis
On ultrasound, widening of the posteriorossification centres can be seen togetherwith the presence of a central focusrepresenting the spur.
Magnetic resonance offers further definitionof the spinal cord especially if there isassociated spina bifida.
Outcome
It is important to exclude spina bifida ifdiastematomyelia is discovered antenatally.
Babies born with this may be entirelynormal or have neurological problems assevere as spastic paraplegia.
Early surgery to remove the bony spur canprevent progressive tethering of the cord asthe baby grows.
Only 5 cases have been reported to CARISgiving a gross prevalence of 0.2 per 10,000total births. 2 cases are associated withknown syndromes (1 VATER associationand 1 caudal dysplasia sequence).
spinal column
bony spur