CONGENITAL ANOMALIES.ppt
39
Congenital Anomalies Julniar M Tasli Herman Bermawi
-
Upload
iqiqiqiqiq -
Category
Documents
-
view
73 -
download
2
Transcript of CONGENITAL ANOMALIES.ppt
-
Congenital Anomalies
Julniar M TasliHerman Bermawi
-
CONGENITAL ANAOMALIES
Objective : The purpose of this lecture is to provide the student recognizing, diagnosing, stabilizing and making decision of transport as needed to reveral center
-
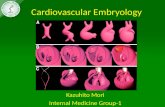
OverviewCongenital anomalies are abnormalities present at birth. They are malformations in structure, position, or function of an organ or system.They are a common cause of mortality and disability in early life. Causes range from inherited, genetic disorders to teratogenic insults to the developing fetus.
-
Task: List of congenital anomaliesOtolaryngologyNeurological disordersCardiovascular disordersRespiratory disordersGastrointestinal disordersGenitourinary disorders
-
Task: Recognition investigation management: Otolaryngology (common)Choanal atresia/stenosisCleft lip/palate
-
Task: Recognition : Choanal atresiaBilateral atresia:Cyanosis, alleviated by cryingRespiratory distressDifficulty with feedingUnilateral atresia: Presented usually later in life
-
Task: Diagnosis : Choanal atresiaFully examination head & neckPass 6F soft catheter into nostrilMinimize congestion by avoiding multiple attempts Direct examination into the nostrils (flexible fiberoptic bronchoscope)
-
Cleft lip palate (CL/P)Incidence (US): 1 in 1000 births (white)2 in 1000 (asian)3.6 in 1000 (native Indian) 0.3 in 1000 (black)Common in male; 90% unilateralPrenatal diagnosis: US starting 16weeks
-
Cleft lip palate (CL/P)Etiology: failure of normal orofacial development during the 6th-12th wks of embryonic lifeManagement:Pre-operative: feeding problem Encourage breast-feedingOther devices:HabermanCheck weight gain frequently (weekly)Operative:3-5 mo: closure lip, nasal, alveolar clefts8-10 mo: palatoplastyPost-operative: prevention of infection
-
Pierre-Robin sequenceSequence: stunted growth of mandible displacement of tongue clefting of palate (roof of mouth)Associated with:Sticklers syndrome (collagen mutation)Velocardifacial syndrome (Chr 22q11 deletionAirway patency problem, if severe tracheostomyFeeding problem, if severe, may need gastrostomy placementFirst stage repair:tongue-lip adhesion (glossopexy)
-
Pierre-Robin sequenceDistraction OsteogenesisTracheostomyAfter reconstruction
-
DiagnosisPhysical ExaminationInvestigationManagement
-
Task: Recognition investigation management: Neurological disorders (common)HydrocephalusMeningomyelocele
-
HydrocephalusPorencephalic cystDandy-Walker malformationHydrocephalusIncidence 1 in 1000 live birthAssociated with:Aqueductal stenosis (33%)Myelomeningocele Arnold-Chiari malformation (28%)Dandy-Walker (7%)PHH (post-hemorrhagic hydrocephalus)
-
Etiologies of Congenital hydrocephalusEngorged vein ~ ICPAccumulation of CSFoversecretion of CSF:Papilloma of the choroid plexusIncreased venous pressure Obstruction of CSF pathwaysIntraventricular block at the level of the foramen of Munro, 3rd ventricle, Sylvian aqueduct, or 4th ventricle Extraventricular block from inflammation or tumours Deficient resorption Venous hypertension Abnormalities of the arachnoid villi Unknown mechanisms
-
TreatmentProgressive: treatment (VP shunt)
Aqueductal stenosisMyelomeningocele with associated HydrocephalusCongenital communicating hydrocephalusDandy-WalkerNon-progressive (brain atrophy): no treatment
Brain malformation: holoprosencephaly, lissencephalyHydrancephalyAtrophy post infectionPeriventricular leukomalacia
-
DiagnosisPhysical ExaminationInvestigationManagement
-
Task: Recognition investigation management: respiratory disorders (common)Esophageal atresia and tracheoesophageal fistulaCongenital diaphragmatic hernia
-
Baby EM , female, FT, 1 hr of life. Agitation, tachypnea, drooling of saliva. Chooking with the first feeding, inability to pass a NG suction catheterTracheoesophageal fistulaFail of esophagotracheal septum to separate the esophagus and the trachea
-
Types of TEFDiagnosis: (1) NG insertion; (2) X-ray; (3) fluoroscopy; (4) bronchoscopy
-
Stabilization then transportTracheoesophageal Fistula & Esophageal AtresiaHead: keep at 450 angleInsert NGT & suctionAvoid bag-mask, intubate if neededPrevent potential aspiration through fistula: minimize abdominal manipulationExamine for Vertebral, Anal, Cardiac, Tracheal, Esophageal, Renal and Limb anomaliesRecognize life-threatening condition: abdominal distention with deteriorating vital signs: gastric decompression (with large bore needle)
-
DiagnosisPhysical ExaminationInvestigationManagement
-
This infant was brought to your attention at ~ 30 minutes of life for respiratory distress (tachypnea, cyanotic and grunting). Rales bilaterally. What is your differential diagnosis:.
. How do you differentiate themCongenital Diaphragmatic HerniaEsophageal atresia with blind pouchCNS depression
-
1: 2000-5000Left : common 70% (through foramen of Bochdalek)Initial treatment: stabilization of pulmonary function, prevention of PPHNSurgical repair: after CR stableMortality ~40%Congenital Diaphragmatic HerniaA diaphragmatic defect occurs at 8-10 wks of gestation, owing to failure of closure of the pleuroperitoneal canal, thus the presence of the abdominal viscera in the thoracic cavity
-
Stabilization then transportofcongenital diaphragmatic herniaAvoid bag-mask & intubate promptlyInsert NGT & suctionInsert umbilical arterial and venous linesNothing by Mouth (NPO)Transfer to the treatment center
-
DiagnosisPhysical ExaminationInvestigationManagement
-
Task: Recognition investigation management: Gastrointestinal disorders (common)GastroschisisOmphaloceleImperforate anus
-
How do you differentiate omphalocele and gastroschisis?
Which one is associated with chromosomal abnomalities?
-
PathogenesisGastroschisis:Umbilical veins 2 1Left moves centrallyRight: regresses and may creating a weak spot (~6wk of gestation) and created the defect when intestines returns into the abdominal cavity at ~10th week of gestation)Teratogen exposureGeneticOmphalocele:Intestinal loops fail to return to the abdominal cavity at ~ 11 wkDue to abnormal embryonic development, thus high rate of associated defects & chromosomal abnormalities
-
CharacteristicsGastroschisisOmphalocele
LocationRight of umbilicuswithin the ringCover sacabsentpresentAppearancematted, edematoususually normalOther anomalies10-20%45-80%GIintestinal atresia, midgutrarevolvulus, intestinal stenosisnon-GIrarecommon (heart:28%; GU(20%) CDH(12%)Chromosomerare50%, trisomiesBowel functionslownormal to slowpost- Sx
-
Stabilization then transportGastroschisis, OmphalocelePrevent hypothermia: cover with clear plastic, avoid gauze that usually stick to the bowel)Insert NGT & suctionPrevent bowel ischemia: place the baby on sidePrevent infection: start IV antibiotic : Ampicillin + GentamycinOmphalocele: examine for Cardiac, Renal, Imperforate anus, Chromosome:Trisomy 13,18,21,Beckwith-Wiedemann Syndrome (large tongue, gigantism, hypoglycemia), CHARGE association.Gastroschisis: look for other intestinal atresia
-
Immediate Surgery: primary closure vs. stages closure (silo):Silo reduction: gradual fitting of abdominal content into the cavityTo promote epithelialization: apply silver nitrate/silver sulfadiazine
-
DiagnosisPhysical ExaminationInvestigationManagement
-
This baby was about to be discharged home, when an astute intern checked the anal opening and found a dimple instead of an opening. By the way, rectal temperature has been recorded for more than 24 hours.
-
Clinical manifestationLook for fistula:Male: perineal or rectourethral, rectovesical (rare) : meconium in the urineFemale: perineal or vestibular (posterior to hymen) or cloaca (single opening for rectum, vagina and urethra50-60% may have other anomalies:V-vertebraeA-imperforate anusC-cardiac (12-22%)TE- tracheoesophageal fistulaR-renal and GU anomaliesL-radial limbs abnormalities
-
Diagnosis & TreatmentDilatation for perineal or vestibular fistulaAll other fistulae required distal colostogram to determine the anatomyColostomy for all other fistulaDefinitive reconstruction
-
DiagnosisPhysical ExaminationInvestigationManagement
-
TERIMAKASIH