Conflict of Interest Disclosure - ASPMN Conference Documents/Handouts/Fri… · – The use of...
11
1 A Nonpharmacologic Approach to Pain Management Using Aromatherapy: A Train-the-Trainer Model Victoria Boyce MSN RN AHN‐BC Mary Natschke RN BAS HNB‐BC IAC St John Hospital & Medical Center Detroit, Michigan Conflict of Interest Disclosure • Victoria Boyce—no conflict of interest • Mary Natschke—no conflict of interest • Picture of hospital
Transcript of Conflict of Interest Disclosure - ASPMN Conference Documents/Handouts/Fri… · – The use of...

1
A Nonpharmacologic Approach to Pain Management Using
Aromatherapy: A Train-the-Trainer Model
Victoria Boyce MSN RN AHN‐BCMary Natschke RN BAS HNB‐BC IACSt John Hospital & Medical Center
Detroit, Michigan
Conflict of Interest Disclosure
• Victoria Boyce—no conflict of interest
• Mary Natschke—no conflict of interest
• Picture of hospital

2
Statement of Intention for Pain Management
• As a community of holistic nurses at St John Hospital &Medical Center, we will safely manage our patient's pain with a non‐judgmental approach using allresources available. We will be mindful of our patient’s unique pain experience and advocate for care thatfacilitates comfort and healing.
• (St John Hospital & Medical Center Professional NursePractice Council 2014)
HCAHPS“During this hospital stay, how often did the hospital staff do everything they could to help you with your pain?”
PC.01.02.07 The hospital either treats the patient’s pain or refers the patient for treatment.Note: Treatment strategies for pain may include pharmacologic and nonpharmacologic approaches. Strategies should reflect a [patient]‐centered approachand consider the patient’s current presentation, the health care providers’ clinical judgment, and the risks and benefits associated with the strategies, including potential risk of dependency, addiction, and abuse.
The Joint Commission

3
Historical Roots• Ancient Egypt
• China & India
• Greece
• France
• Hippocrates
• America
• Modern Day
Ancient civilizations incorporated aromatics as part of their practice.
Aromatherapy Through the Ages
• Renee‐Maurice Gattefosse
Father of Aromatherapy
“Aromatherapie” defined in 1937
• Marguerite Maury – Austria biochemist
• Jean Valnet – French surgeon WWII
• Robert Tisserand – Safety expert
What are Essential Oils?• Tiny droplets contained in glands,sacs or veins of different plant parts: leaves, stems, bark, flowers, roots and fruits
• Highly concentrated, potent• Volatile, flammable• Each EO has 80‐300 chemicalconstituents

4
Aromatherapy in Clinical Practice
“Aromatherapy . . . the art and science of utilizing naturally extracted aromatic essences from plants to balance, harmonize and promote the health of body, mind and spirit. It seeks to unify physiological, psychological and spiritual processes to enhance an individual’s innate healing process.” www.naha.org
o Stress/anxiety
o Headaches/migraines
o Insomnia
o Chronic or acute pain relief
o Arthritis & rheumatism(sub‐acute phase)
o Chronic muscular/jointaches and pain
o Pregnancy and childbirthmassage
o Reducing inflammation
o Enhancing immunity
o Relieving muscle spasms
o Relax and soothe thenervous system
Aromatherapy used for . . .
Physiologic response to Aromatherapy
Dominate nostril correlates with the dominate hand
Largest organ of the body

5
Methods of Administration
• Diffusion
• Topical
• Inhalation
Contraindications/allergies• Patients who identify an allergy
or sensitivity to the essential oilor
• Patients who are admitted withreactive airway disease
or• Acute episode of a-fib or
tachycardia (peppermint only)
Safety• Keep Out Of Reach Of Children (KOOROC)
• Keep EO’s away from light and heat sources
• Do Not take orally
• DILUTE, DILUTE, DILUTE
• Remember: Less is More
• Be aware of sensitivities and/or allergies

6
Storage
• Keep caps tightly closed
• Store in cool place away from light
• Use a dark colored glass bottle
• Expiration date two years (2) from openingbottle
Labeling
Name of oil
Date and time
Initials
Handoff report Lavender9‐18‐151800/mn
Sweet Orange9‐20‐150130/mn
Developing an Aromatherapy Program
• Clinicalaromatherapy expert
• Literature review
• Benchmarking

7
Policy & Procedure• Who can use it?
• Where do I find therapeutic grade oils?
• What oils do you want and why?
• MSDS sheets
• Diffusion? Skin application? Inhalation?
• What about “scent free” zones?
• Contraindications?
Online Validation Process
Step One: On‐line module developed
– Power point slides
– Read 2 Articles
– Review Policy & Procedure
– Post test questions (Pass 90%)

8
Clinical Validation ProcessStep 2 (Hands on with RN Validator)
– Training record check off
– Verbalizes assessment, safety, oil selection, route
– Assembles equipment, demonstrates competencyin preparing for administration
– Verbalizes how to establish a healing environment
– Evaluate response, documents appropriately
– Discuss ongoing plan of care, hand‐off report
Clinical Validator Workshop• Designed for RN’s – Train the Trainer approach
• Initially an 8 hour workshop
• More in‐depth training than validation process– The use of aromatherapy in the context of holisticnursing and the healing environment
– Overview of supporting evidence
– Validation process and documentation
– Actual validation teach back in class
Where Are We Now?• 6 hospitals and multiple out‐patient facilitieswithin the health system offer aromatherapy .
• Presently there are over 200 RN validators in theHealth System from all clinical areas.
• All nursing units are using aromatherapy to somedegree
• Recently developed a separate form for our EMR

9

10
Lessons Learned• Acquire expertise in Clinical Aromatherapy• Start small – few basic essential oils• Consider hospital ordering system• Documentation• Consider specialty area’s (i.e. Ped’s, OB, ED, pre/post op, ICU’s, and outpatient settings)
• Use it – keep it visible – tell your stories• Always naysayers . . . Do it anyway• Leadership support – aromatherapy is an expectationfor our patients comfort and well‐being.
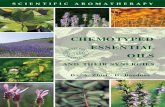
Metrics
71.18%
65.73% 65.19%
59.96%
68.99%
67.59%
67.02%65.63%
69.25% 69.90%
67.12%
70.54%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
FY15 Pain Mangement HCAHPS Scores
Pain Management HCAHPS Scores FY15 Target‐67.5%
Case Study

11
• Buckle, Jane (2003) Clinical Aromatherapy Essential Oils in Practice. Elsevier Limited. New York, N.Y.
• Buckle, Jane (2001) The Role of Aromatherapy in Nursing Care. Journal of Holistic Nursing Practice. March 2001 57‐72.
• Cooksley, V. (2015) Aromatherapy; A Holistic Guide to Natur4al Healing with Essential Oils.
• Denner, S. (2009). Lavandula angustifolia miller: English lavender. Journal of Holistic Nursing Practice. January/February 2009 57‐64.
• Dossey, Barbara M., Keegan, L. and Guzzetta C. (2012) Holistic Nursing: A Handbook for Practice (6th
Edition) Jones and Bartlett, Boston
• Halm, M. (2008). Essential oils for management of symptoms in critically ill patients. American Journalof Critical Care 17 (2) 160‐163.
• Joint Commission Perspectives® Nov. 2014, Vol 34: 11
• Nord, D and Belew, J. (2009). Effectiveness of the essential oils lavender and ginger in promoting children’s comfort in a periansethesia setting. Journal of Perianesthesia Nursing 24 (5) 307‐312
• Smith M C and Kyle L. (2008). Holistic foundations of aromatherapy for nursing. Journal of HolisticNursing Practice January/February 2008 3‐9.
• The Institute of Integrative Aromatherapy. www.aroma‐RN.org
• Tisserand, R. & Balazs T. Essentail Oils Safety (rev edition) 2014 London: Churchill Livingston.
• www.NAHA.org