
Psychosocial interventions in drug misuse - National Treatment
Computerized Psychosocial Treatment for Offenders with Substance Use
Disorders: Study Outcomes
Michael Chaple , PhD Center for the Integration of Research & Practice (CIRP) National Development & Research Institutes, Inc. (NDRI)
Stanley Sacks, PhD Center for the Integration of Research & Practice (CIRP) National Development & Research Institutes, Inc. (NDRI)
Lisa Marsch, PhD Dartmouth Medical School, Dartmouth Psychiatric Research Center
2014 National Frontier and Rural ATTC Addiction Treatment Technology Summit August 26-27, 2014— Chicago, Illinois
Supported by The Department of Health and Human Services National Institutes of Health (NIH), National Institute on Drug Abuse (NIDA) grant: 5RC2DA028967. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute On Drug Abuse or the National Institutes of Health.

Conflict of Interest
Neither Dr. Chaple nor Dr. Sacks, have any financial relationships that relate to the topic of this presentation.
Dr. Marsch is affiliated with HealthSim, LLC, the developer of the computer-based Therapeutic Education System.
2

ResearchAgency Principal Investigator
National Development & Research Institutes (NDRI) Stanley Sacks Lisa A. Marsch
University of California – Los Angeles (UCLA) Michael Prendergast
Temple University Steven Belenko
University of Kentucky Carl Leukefeld
University of Miami Michael French
3
Collaborating Agencies
Background Despite the high prevalence of substance use
disorders among prisoners (53% in State, 45% in Federal1), about ¼ of prisoners in need of drug treatment actually receive it while incarcerated2
To increase the number of inmates receiving services, a computer-based, psychosocial treatment program, the Therapeutic Education System (TES) was developed.
This study evaluated the comparative effectiveness of TES relative to Standard Care.
4
1 Mumola, C. &Karberg, J. (2006). Drug use and dependence, state and federal prisoners, 2006. Bureau of Justice Statistics, Office of Justice Programs.
2 Taxman, F.S., Perdoni, M.L., & Harrison, L.D. (2007a). Drug treatment services for adult offenders: The state of the state. Journal of Substance Abuse Treatment, 32(3), 239-254. Chandler, R.K., Fletcher, B.W., &Volkow, N.D. (2009). Treating drug abuse and addiction in the criminal justice system. Journal of the American Medical Association, 301(2), 183-190.

TES Technology Theoretically grounded in the Community
Reinforcement Approach (CRA) & Cognitive Behavioral Therapy (CBT)
Uses “fluency-based” Computer-Assisted Instruction (CAI) based in the “precision teaching” approach3
Experiential learning environment, using interactive videos & exercises
5 3 Binder, C. (1993). Behavioral fluency: A new paradigm. Educational Technology, 33, 8-14.

TES Content 12-week intervention; typically once a week for 2 hours
Thirty-two (32) Core modules broadly classified as: • Substance Use/Abuse (e.g., Drug Refusal Skills) • Risk Reduction for HIV/AIDS, Sexually Transmitted Infections (e.g.,
Drug Use, Triggers for Risky Sex) • Cognitive and Emotional Modulation (e.g., Managing Negative
Thinking, Anger Management) • Psychosocial Functioning (e.g., Effective Problem Solving,
Communication Skills)
Sixteen (16) optional modules provide more advanced information on risk reduction and psychosocial functioning
6

Control Condition
The Control condition (or Standard Care) consisted of the interventions usually offered for drug treatment at the prison.
Curriculum consisted primarily of psycho-education and relapse prevention approaches
Typically once per week for 2 hours for a total of 8-12 weeks
Groups were conducted by staff members who specialize in substance abuse treatment, and who have a minimum credential certifying their advanced training (e.g. CAC)
7

Study AIMS Evaluation of TES relative to Standard Care examining:
AIM 1. Comparative effectiveness
AIM 2. Cost and cost-effectiveness
Key Outcomes for both AIMS include: Substance use (e.g. any use, weeks of abstinence) HIV risk behavior (i.e. drug and sex-related) Self-reported Criminal Activity & Reincarceration rates
8

9
Study Design
TES (E) N=258
Random Assignment
Correctional Facility* N=513
* 10 sites in 4 research centers linked to the NIDA funded CJDATS network
Standard Services (C) N=255

Eligibility criteria for the study:
1) Identified by Department of Corrections as needing SUD Tx; 2) Nearing prison release; 3) Minimum or minimum-restricted security risk; 4) Voluntarily consented to enter the study.
Sample
State Field Site Prisons Total E C CO NDRI 7 327 165 162 WA UCLA 1 62 31 31
PA Temple University 1 57 29 28
KY University of Kentucky 1 67 33 34
Total N 10 513 258 255
Baseline Recruitment:
15 subjects were not released from prison as expected; thus final sample = 498

Methods
Prospective, longitudinal, repeated measures study with randomization
Self-Report Data collected at Baseline (in prison) and 3- and 6-months post-prison release Criminal Activity, Illegal Drug Use, HIV Risk Behavior,
Reincarceration data (DOC) collected at 12-months
Follow-up Interview Rates: 3-months = 86.1% (88.4% Experimental; 83.4% Control) 6-months = 80.0% (81.2% Experimental; 78.2% Control)
11

Any Illegal Drug Use
0102030405060708090
100
Baseline 6MPP
78
36
82
38 E-TES
C
Perc
ent
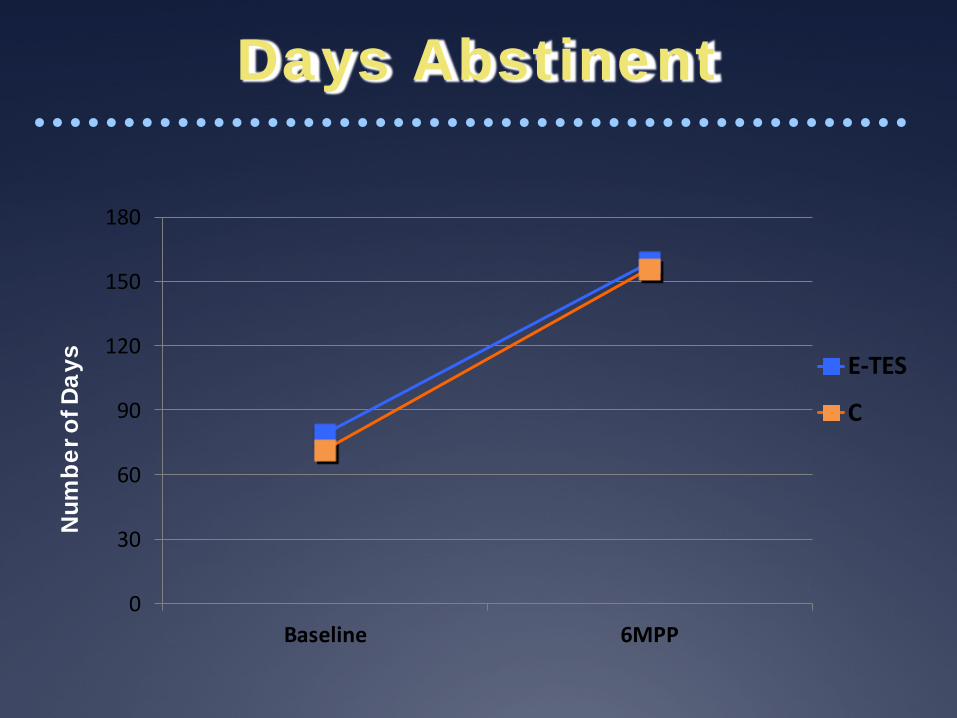
Days Abstinent
0
30
60
90
120
150
180
Baseline 6MPP
E-TES
C
Num
ber o
f Day
s
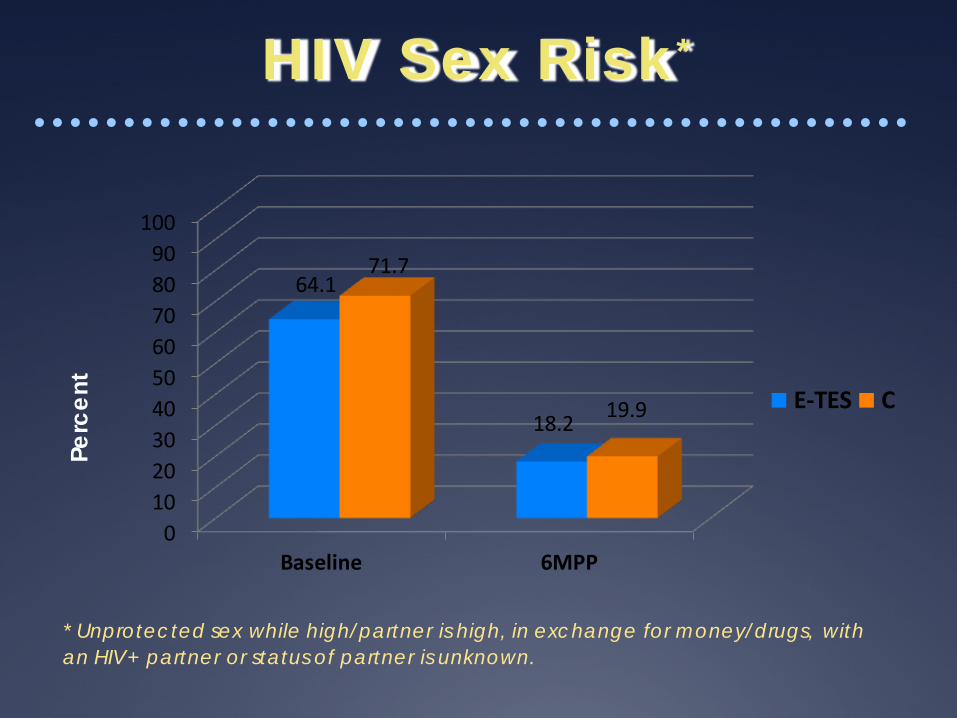
HIV Sex Risk*
0102030405060708090
100
Baseline 6MPP
64.1
18.2
71.7
19.9 E-TES C
* Unprotected sex while high/partner is high, in exchange for money/drugs, with an HIV+ partner or status of partner is unknown.
Perc
ent

Any Drug Injection
0102030405060708090
100
Baseline 6MPP
16.52.5
23.4
6.2
E-TES C
Perc
ent

Any Criminal Activity
0102030405060708090
100
Baseline 6MPP
80
46
80
46E-TES
C
Perc
ent

Reincarceration: 12M PP
0102030405060708090
100
Any Offense New Offense Violation
27.5
7.420.121.4
6.715.1
E-TES
C
Perc
ent

18
Summary
Preliminary findings indicate • Both groups improved after prison release • No significant differences between TES and
Standard Care for criminal activity, substance use, and HIV risk behavior on any of the key outcome measures post prison release
• Therefore, further economic analysis will be concentrated on cost minimization

Additional Related Publications Marsch, L.A., Bickel, W.K. (2004). Efficacy of computer-based HIV/AIDS education for injection drug users.
American Journal of Health Behavior, 28(4), 316-327. DOI: 10.5993/AJHB.28.4.3
Bickel, W.K., Marsch, L.A., Buchhalter, A., & Badger, G. (2008). Computerized behavior therapy for opioiddependent outpatients: A randomized, controlled trial. Exp Clin Psychopharmacol, 16, 132-143.
Marsch, L.A., Bickel, W.K., &Grabinski, M.J. (2007). Application of interactive, computer technology to adolescent substance abuse prevention and treatment. In Cohall, A.T., Rickert, V. & Ryan, O. (Eds.), Harnessing Technology for Adolescent Health Promotion, pp. 342-356. American Academy of Pediatrics.
Marsch, L.A., Grabinski, M.J., Bickel, W.K., Desrosiers, A., Guarino, H., Muehlbach, B., Solhkhah, R., Talfique, S., & Acosta, M. (2011). Computer-Assisted HIV Prevention for Youth with Substance Use Disorders. In Special Issue on Technology and Substance Use Disorders (Guest Editor: Marsch, L.A.). Substance Use and Misuse, 46, 46-56.
Marsch, L.A. Guarino, H., Acosta, M., Aponte-Melendez, Y., Cleland, C., Grabinski, M., Brady, R., & Edwards, J.A. (2014). Web-based behavioral treatment for substance use disorders as a partial replacement of standard methadone maintenance treatment. Journal of Substance Abuse Treatment, 46: 43-51.
19
Study Publications Chaple, M., Sacks,S., McKendrick, M., Marsch, L.A., Belenko, S., Leukefeld, C., Prendergast ,
M. & French, M (2014). Feasibility of a computerized intervention for offenders with substance use disorders: A research note. Journal of Experimental Criminology, 10: 105-127. doi: 10.1007/s11292-013-9187-y
Chaple, M., Sacks,S., McKendrick, M., Marsch, L.A., Belenko, S., Leukefeld, C., Prendergast , M. & French, M (2014).(2014). A comparative study of the therapeutic education system for incarcerated substance abusing offenders. Accepted for publication in Prison Journal.

Contact information:
Michael Chaple, PhD Co-Principal Investigator
National Development & Research Institutes, Inc. 71 W 23rd Street, 8th Floor
New York, NY 10010 tel212.845.4539 fax 212.845.4650
http://www.ndri.org [email protected]
Acknowledgements: The authors wish to acknowledge the important collaboration with the
Dept. of Corrections in Colorado, Kentucky, Pennsylvania and Washington State in the conduct of this study.
20


















