
Computed Tomography Coronary Angiography in the.5
9
Copyright © Italian Federation of Cardiology. Unauthor ized reproduction of this article is prohibite d. Computed tomography-coronary angiography in the detection of coronary artery disease Anoeshka S. Dharampal, Alexia Rossi and Pim J. de Feyter Compute d tomograp hy-coron ary angiography (CT-CA) is a well-tolerated and reliable non-invas ive imaging technique and cannow be achieved at lowlevels of radiation expos ur e. CT- CA is highly valuabl e to excludecoronar y arte ry disease, but due to over- and underestimation of the severity of coronary lesions, CT-CA cannot replace invasive coronary angiogr aphy. Coronary calcium scorin g has an incremental independent prognostic value beyond traditional risk factor scores(Framingham, European Score) and may be useful to reclassify risk in asymptomatic individuals at intermediate risk. Appropriate indications for CT-CA are evolving, but studies are lacking to demonstrate that CT coronary imaging improves patient outcome. J Cardiovasc Med 2011, 12:554–561 Keywords: asymptomatic, calcium score, computed tomography, coronary angiography, coronary artery disease, coronary imaging, prognostic value, scan mode, spiral, step and shoot, symptomatic Department of Radiology and Department of Cardiology, Erasmus MC, Rotterdam, The Netherlands Correspondence to Anoeshka S. Dharampal, Erasmus MC, Department of Radiology, Room Ca207a, ‘s-Gravendijkwal 230, PO Box 2040, 3015 CE Rotterdam, The Netherlands Tel: +31 10 7033558; fax: +31 10 7034033; e-mail: [email protected] Received 18 April 2011 Accepted 20 May 2011 Introduction The prevalence of cor ona ry artery diseas e (CAD) in Europe is estimated to ra nge between 20000 and 40 000 persons per million suffe ring from angina. Cardio- vascular disease (CVD) is the number one cause of death in the Western world. Each year 4.3 million people die as a result of CVD. Cardiovascular mortality in women or men is accountable for 22 or 21% of all deaths. 1 Computed tomography-coronary imaging Current state-of-the-art-scanners are now considered to have at least 64 slices or pr ef erabl y more to achieve coverage of the heart in less than 10 s which corresp onds to a breath hold of less than 10 s. Techni cal aspects of various state-of-the-art-scanners (>64-slice) are shown in Table 1. 2,3 The increased number of detector rows has improved the coverage of the heart and as resul t the 320- slice scanner is able to acquire the data within two heart beats. 4 The spatial resolution of the 64-slice computed tomogr aphy (CT) scanne rs is approximat ely 0.5– 0.6 mm in clinical use and the newer scanners, althoug h having a better coverage, still have similar spatial resolution. The tempor al resoluti on ranges from 75 to 175 ms, but during fast heart rates (>70beats/min) motion artifacts are still not eliminated, although scanning at higher heart rates is feasible. The coronary arteries can be scanned in a variety of ways usi ng ECG synchr oni zat ion wit h data acqu isi tio n to obtain ECG-phase correl ated images . The scan can be performed by continuously acquiring images throughout the cardiac cycle during several heart beats using the helical scan mode with low-speed table movement. This is also known as the spiral scan at low pitch (table movement/r otati on time) (Fig. 1a). Thi s scan mode has the highest effective radiation dose of all scan modes, but allows image reconstruction throughout the cardiac cycle with the flexibility to choose a motion- free phase of the cardiac cycle to evaluate the coron- aries. This was the scan mode used with the earlier scan generations. With the use of ECG-triggered tube cur- rent modulation, the tube current can be set to lower levels (20 or 4% of the maximum output) in phases that are not used for coronary evaluation ( Fig. 1b and c). This scan mode is associated with a reduction of radia- tion dose. 5,6 Nowadays the most pr ef erred scan mode is the scan which is performed in steps, because of its significant effective radiation dose reduction compared to the spiral scan with low pitch. This so-called ‘step and shoot’ scan acquires data in one specific phase of the heart cycle when less coronar y moti on is exp ected. The scan acquir es data in this specific phase and subsequently moves to the next position and ‘waits’ until the same phase in the next heart beat has arrived to acquire data again. During the movement of the table and ‘waiting’ for the next phase the tube current is switched off (Fig. 2a). Thus, this scan mode can be performed at low effective radiation dose. This scan can also be performed with a wider scan range per heart b eat, also calle d ‘padding ’, with the fle xibil ity to reconstruct also other phases of the cardiac cycle, allow- ing reconstruc tion of coronar y images without, or having the least, motion artifact. To reduce radiation exposure the ECG-triggered tube current modulation can also be applied within this broad scan range when, for example, cardiac function (wall motion and wall thickening) has to be assessed (Fig. 2b). Clinical review 1558-2027 ß 2011 Italian Federation of Cardiology DOI:10.2459/JCM.0b013e32834905dc
-
Upload
ospinu6780 -
Category
Documents
-
view
218 -
download
0
Transcript of Computed Tomography Coronary Angiography in the.5

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 1/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
Computed tomography-coronary angiography in thedetection of coronary artery diseaseAnoeshka S. Dharampal, Alexia Rossi and Pim J. de Feyter
Computed tomography-coronary angiography (CT-CA) is a
well-tolerated and reliable non-invasive imaging technique
and cannow be achieved at lowlevels of radiation exposure.
CT-CA is highly valuable to exclude coronary artery disease,
but due to over- and underestimation of the severity of
coronary lesions, CT-CA cannot replace invasive coronary
angiography. Coronary calcium scoring has an incremental
independent prognostic value beyond traditional risk factor
scores (Framingham, European Score) and may be useful to
reclassify risk in asymptomatic individuals at intermediate
risk. Appropriate indications for CT-CA are evolving, but
studies are lacking to demonstrate that CT coronaryimaging improves patient outcome.
J Cardiovasc Med 2011, 12:554–561
Keywords: asymptomatic, calcium score, computed tomography,coronary angiography, coronary artery disease, coronaryimaging, prognostic value, scan mode, spiral, step and shoot,symptomatic
Department of Radiology and Department of Cardiology, Erasmus MC,Rotterdam, The Netherlands
Correspondence to Anoeshka S. Dharampal, Erasmus MC, Department ofRadiology, Room Ca207a, ‘s-Gravendijkwal 230, PO Box 2040, 3015 CERotterdam, The NetherlandsTel: +31 10 7033558; fax: +31 10 7034033;e-mail: [email protected]
Received 18 April 2011 Accepted 20 May 2011
IntroductionThe prevalence of coronary artery disease (CAD) in
Europe is estimated to range between 20000 and
40 000 persons per million suffering from angina. Cardio-
vascular disease (CVD) is the number one cause of death
in the Western world. Each year 4.3 million people die as
a result of CVD. Cardiovascular mortality in women or
men is accountable for 22 or 21% of all deaths.1
Computed tomography-coronary imagingCurrent state-of-the-art-scanners are now considered to
have at least 64 slices or preferably more to achieve
coverage of the heart in less than 10 s which corresponds
to a breath hold of less than 10 s. Technical aspects of
various state-of-the-art-scanners (>64-slice) are shown in
Table 1.2,3 The increased number of detector rows has
improved the coverage of the heart and as result the 320-
slice scanner is able to acquire the data within two heart
beats.4 The spatial resolution of the 64-slice computed
tomography (CT) scanners is approximately 0.5– 0.6 mm
in clinical use and the newer scanners, although having a
better coverage, still have similar spatial resolution. Thetemporal resolution ranges from 75 to 175 ms, but during
fast heart rates (>70 beats/min) motion artifacts are still
not eliminated, although scanning at higher heart rates
is feasible.
The coronary arteries can be scanned in a variety of ways
using ECG synchronization with data acquisition to
obtain ECG-phase correlated images.
The scan can be performed by continuously acquiring
images throughout the cardiac cycle during several heart
beats using the helical scan mode with low-speed table
movement. This is also known as the spiral scan at low
pitch (table movement/rotation time) (Fig. 1a). This
scan mode has the highest effective radiation dose of all
scan modes, but allows image reconstruction throughout
the cardiac cycle with the flexibility to choose a motion-
free phase of the cardiac cycle to evaluate the coron-
aries. This was the scan mode used with the earlier scan
generations. With the use of ECG-triggered tube cur-
rent modulation, the tube current can be set to lower
levels (20 or 4% of the maximum output) in phases that
are not used for coronary evaluation (Fig. 1b and c).This scan mode is associated with a reduction of radia-
tion dose.5,6
Nowadays the most preferred scan mode is the scan
which is performed in steps, because of its significant
effective radiation dose reduction compared to the spiral
scan with low pitch. This so-called ‘step and shoot’ scan
acquires data in one specific phase of the heart cycle
when less coronary motion is expected. The scan acquires
data in this specific phase and subsequently moves to the
next position and ‘waits’ until the same phase in the next
heart beat has arrived to acquire data again. During themovement of the table and ‘waiting’ for the next phase
the tube current is switched off (Fig. 2a). Thus, this scan
mode can be performed at low effective radiation dose.
This scan can also be performed with a wider scan range
per heart beat, also called ‘padding’, with the flexibility to
reconstruct also other phases of the cardiac cycle, allow-
ing reconstruction of coronary images without, or having
the least, motion artifact. To reduce radiation exposure
the ECG-triggered tube current modulation can also be
applied within this broad scan range when, for example,
cardiac function (wall motion and wall thickening) has to
be assessed (Fig. 2b).
Clinical review
1558-2027 ß 2011 Italian Federation of Cardiology DOI:10.2459/JCM.0b013e32834905dc

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 2/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
Another scan mode is the spiral scan with high pitch. Thisscan mode can only be used in patients with a low and
regular heart rate (<60 beats/min). The prolonged cardiac
cycle in low heart rates enables one quick spiral scan to be
performed in the diastolic phase of the heart to obtain
motion-free images of the coronaries with a very low
effective radiation dose (Fig. 3).
Each scan mode has its advantages and disadvantages, as
summarized in Table 2. In every scan mode the effective
radiation dose (Table 2)7,8 can be lowered by choosing
the right scan settings and also by changing the scan
mode.9 The highest image quality of CT-scan is achieved
in patients with lowest heart rates and this also allows useof scan mode and settings associated with lower radiation
exposure. Heart rate lowering medication is recom-
mended in patients with heart rate greater than
60 beats/min. At very low regular heart rates
(<60 beats/min) the high-pitch spiral scan mode can be
performed with lowest radiation dose.10 The ‘step and
shoot’ scan mode is preferred above the low-pitch spiral
scan in all regular and variable heart rates as this is
associated with a significantly lower effective radiation
dose.11 Other means to reduce radiation dose are the use
of lower tube voltage and tube current according to the
patient’s length and weight.12 ECG-triggered tube cur-
rent modulation should be preferred in either spiral scanwith low pitch or in ‘step and shoot’ scan for the assess-
ment of cardiac function (Figs 1c and 2b).9 In these scans,
using ‘pulsing’, the tube current is kept to 100% in the
phases that are used for coronary evaluation, and in the
other phases the tube current is lowered to levels of 20 or
4% to reduce the effective dose significantly.5,6
Recently, an iterative reconstruction algorithm has been
introduced in cardiac CT which has improved the con-
trast to noise ratio. Preliminary data suggest that iterative
reconstruction may further reduce the radiation dose
(44%) with preservation of the image quality.13
CT-CA in the detection of coronary artery disease Dharampal et al. 555
Table 1 Technical aspects of the new-generation CT scanners
Slices acquiredp er rot ation Scanner description
Detectorwidth (mm)
Longitudinal (z-axis)coverage (cm)
Rotationtime
Temporalresolution
Longitudinal (Z-axis)spatial resolution
64 (a) 32 detector rows 0.6 1.92 330 83 0.4Dual sourceSingle focal spot
128 (b) 64 detector rows 0.6 3.84 300 150 0.33Single source CT
Dual focal spot256 (c) 64 detector rows 0.6 3.84 285 75 0.33Dual source CTDual focal spot
256 (d) 128 detector rows 0.625 8 270 135 0.42Single source CTDual focal spot
320 (e) 320 detector rows 0.5 16 350 175 0.45Single source scannerSingle focal spot
Technical aspects of the (a) 64 (Siemens healthcare, Somatom Definition), (b) 128 (Siemens Healthcare, Somatom Definition ASþ), (c) 256 (Philips Heathcare, BrilianceiCT), (d) 256 (Siemens Healthcare,Somatom Definition Flash)and (e) 320-slice (Toshiba Medical systems, Aquilion One) scanners.2,3 Singlesource CT:one unit roentgentube and the detector rows; dual source CT: two units of roentgen tube and detector rows; single focal spot: the focal spot of the roentgen tube only has one position fromthe detector rows; dual focal spot: roentgen tube alternates from two different positions. Rotation time: the rotation time of the tube and detector unit. Longitudinal (z-axis)coverage:scan coverage at onerotationwithout table movement.Temporalresolution:time windowin which data forimagereconstruction is acquired (shorter time windoweliminates motion artifacts); spatial resolution: the degree of blurring in an image and the ability to discriminate objects and structures of small size.
Fig. 1
Low-pitch spiral scan mode. (a) Spiral scan without ECG-triggeredtube current modulation. Reconstructions are possible throughout thecardiac cycle. In this scan one specific phase of the cardiac cycle (dark
grey columns) is reconstructed for the evaluation of the coronaries.(b) Spiral scan with ECG-triggered tube current modulation. Tubecurrent is reduced to 4% in the phases that are not used for coronaryevaluation. Reconstruction of the heart is possible throughout thecardiac cycle and they can be used for functional assessment.Reconstructions in the full dose, 100% tube current pulsing range areused for coronary evaluation. In this scan one specific phase of thecardiac cycle (dark grey columns) is reconstructed for the evaluation ofthe coronaries. (c) Spiral scan with ECG-triggered tube currentmodulation. Tube current is reduced to 20% in the phases that are notused for coronary evaluation. Reconstructions of the heart are possiblethroughout the cardiac cycle and they can be used for functionalassessment. Reconstructions in the full dose, 100% tube currentpulsing ranges are used for coronary evaluation. In this scan onespecific phase of the cardiac cycle (dark grey columns) isreconstructed for the evaluation of the coronaries.
8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 3/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
Computed tomography-coronary angiographylimitationsThe spatial resolution of computed tomography-coronary
angiography (CT-CA) compared to invasive coronary
angiography is still limited and may result in over- and
underestimation of the severity of coronary lesions.Severely calcified obstructions are scored less accurately
due to the blooming artif acts.14 Small vessels are often
more difficult to evaluate15 due to the partial volume
effects. The temporal resolution is limited and coronary
motion artifacts at high heart rates may hinder precise
evaluation of the coronaries. The best-quality images are
obtained when the heart rate is less than 60 beats/min.
Heart rate lowering medication is always recommended,
even when using the newer-generation CT-scanner that
can handle higher heart rates. Variable heart rates and
irregular heart rhythm are sometimes problematic and may
cause motion and stack artifacts.16,17 Although breath holdduration during scanning is minimal (approximately 10s)
respiratory movement, which also causes cardiac motion
(Fig. 4), may occur and result in misalignment of the
reconstructions. In large-sized patients a large amount of
the radiation beam is absorbed by tissue, resulting in noisy
images, which may hamper accurate evaluation of the
coronaries. However, with postprocessing techniques such
as acquiring one-half rotation data instead of one-quarter
rotation data, the image noise will decrease, but the
associated decrease of temporal resolution renders these
images more vulnerable for coronary motion.18
CT-CA requires the use of iodinated contrast agents toenhance the lumen.19 Patients with previous allergic
reactions to contrast agents, insufficient renal function
and hyperthyroidism are considered not eligible for CT
angiography.
Coronary calciumThe presence of coronary calcium is a marker for coronary
atherosclerosis. A higher amount of calcium is associated
with a higher likelihood of obstructive CAD, but this is
not calcium-site specific. Pooled analysis (n¼ 10 355
symptomatic patients) showed a sensitivity of 98%,
556 Journal of Cardiovascular Medicine 2011, Vol 12 No 8
Fig. 2
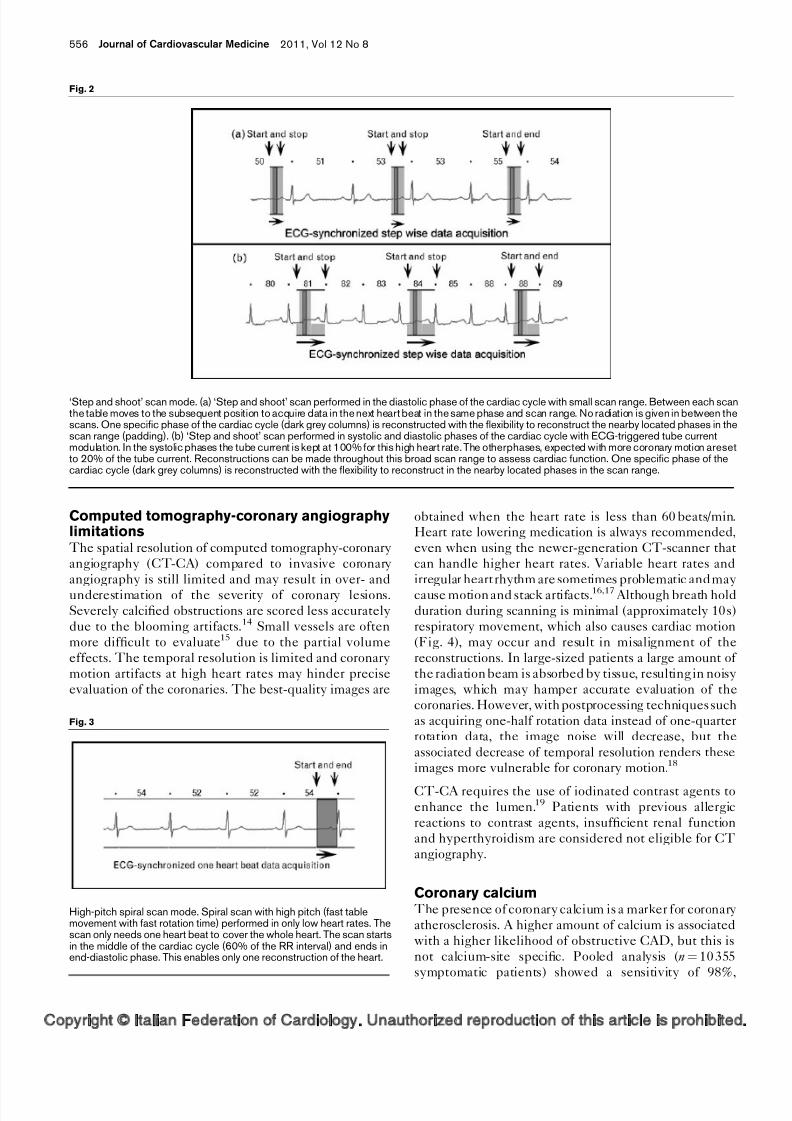
‘Step and shoot’ scan mode. (a) ‘Step and shoot’ scan performed in the diastolic phase of the cardiac cycle with small scan range. Between each scanthe table moves to the subsequent position to acquire data in the next heart beat in the same phase and scan range. No radiation is given in between thescans. One specific phase of the cardiac cycle (dark grey columns) is reconstructed with the flexibility to reconstruct the nearby located phases in thescan range (padding). (b) ‘Step and shoot’ scan performed in systolic and diastolic phases of the cardiac cycle with ECG-triggered tube currentmodulation. In the systolic phases the tube current is kept at 100% for this high heart rate. The otherphases, expected with more coronary motion aresetto 20% of the tube current. Reconstructions can be made throughout this broad scan range to assess cardiac function. One specific phase of thecardiac cycle (dark grey columns) is reconstructed with the flexibility to reconstruct in the nearby located phases in the scan range.
Fig. 3
High-pitch spiral scan mode. Spiral scan with high pitch (fast tablemovement with fast rotation time) performed in only low heart rates. Thescan only needs one heart beat to cover the whole heart. The scan startsin the middle of the cardiac cycle (60% of the RR interval) and ends inend-diastolic phase. This enables only one reconstruction of the heart.
8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 4/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
specificity of 40%, positive predictive value of 68% and
negative predictive value of 93% for the detection of
obstructive disease.20 Absence of coronary calcium is
associated with a very low likelihood of obstructive
CAD, but is not excluded particularly in younger patients
with acute coronary syndrome.
The traditional method to quantify coronary calcification
is the Agatston score. This score is derived from the
number, area (mm2) and the maximum attenuation
within the calcified lesion.21 Large studies in asympto-
matic individuals have shown that the calcium score(Agatston score) is independent and incremental to the
traditional factors for the prediction of cardiovascular
events, in men as well as in women.22–25 Area under
the curve analysis demonstrated a significant improve-
ment of the prediction of the cardiovascular events using
calcium score additional to the traditional risk factor
model (Table 3). The presence of coronary calcifications
in women is associated with a 5.2-fold greater risk of
adverse coronary events compared to women without
calcifications.26 The absence of calcium was associated
with an excellent 10-year survival of 99.4%.22 Higher
calcium score was associated with more adverse event
rates (Table 4). The risk for a cardiovascular event hasbeen shown to increase by 9.9-fold in the presence of a
calcium score of at least 400 compared to the absence of
calcium.27
The Multi-Ethnic Study of Atherosclerosis (MESA)28
and Heinz Nixdorf Recall (NHR)29 study have shown
that calcium score allows further reclassification of
individuals at intermediate risk into lower or higher-
risk categories. The net reclassification improvement,
which quantifies the correctness of upward and down-
ward reclassification, was 55% ( P < 0.001) and 21.7%
( P <0.001), respectively.24,29
CT-CA in the detection of coronary artery disease Dharampal et al. 557
Table 2 Advantages and disadvantages of the low-pitch spiral, ‘step and shoot’ and high pitch spiral scan
Advantages Disadvantages Radiation dose (mSv)
Spiral scan low pitch Possible in all heart rates (low, intermediate,high, regular and variable heart rates)
Highest radiation dose from all scan modes $13.37,9
Functional information available with 20%and also 4% tube current outside thepulsing window
In irregular heart rates the pulsing can be suboptimal
Possibility to search for motion-free images
in nearby phase reconstructions
Several heart beats (3–5) are necessary for wholeheart reconstruction
Stack and breathing artifacts can occur
‘Step and shoot’ scan No heart rate lowering medication necessary In case of variable heart rates more contrast mediumis needed
$1.48,11
Possible at every regular and slightly variableheart rate Suboptimal in irregular heart rates
Low radiation dose Several heart beats (3 – 5) are necessary for wholeheart reconstructionPossibility to search for motion-free images in
nearby phase reconstruction Breath hold has to be held for several heart beats (6–10)for the whole scanFunctional information available in broad scan
ranges without and with pulsing Stack and breathing artifacts can occurHigh pitch spiral Single heart beat scan Heart rate dependency and vulnerability $0.8710
No stack artifacts Higher and variable heart rates show more movementartifactsNo breathing artifacts
Heart rate lowering medication is needed in heart rates>60 beats/min.
No breath hold necessary in un-cooperativepatients
Reconstruction in other phase is not possibleLowest amount of contrast materialOnly diastolic imagesVery low radiation doseNo functional informationMaximum field of view is 33 cm
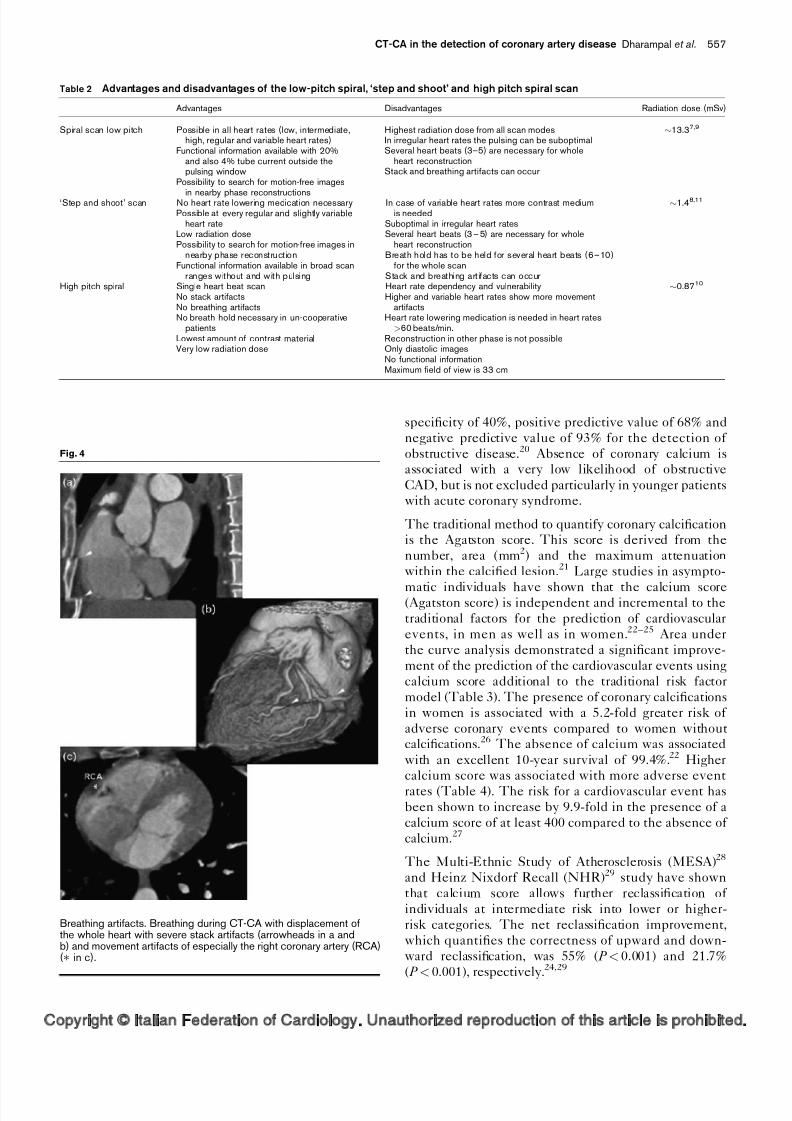
Fig. 4
Breathing artifacts. Breathing during CT-CA with displacement ofthe whole heart with severe stack artifacts (arrowheads in a andb) and movement artifacts of especially the right coronary artery (RCA)(Ã in c).

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 5/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
However, the beneficial effects on outcome following
reclassification into lower or higher-risk category with
subsequent less or more intense control of risk factors
have not been demonstrated in appropriate clinical trials.
Computed tomography-coronary angiographySixty-four-slice CT-CA is currently the most widely used
non-invasive technique for the anatomic assessment of
CAD (Fig. 5). The diagnostic accuracy has been assessed
in a large number of single-centre trials but most impor-
tantly in three large-sized multicentre clinical trials per-
formed in symptomatic patients with low to intermediate
likelihood of pretest of CAD (Table 5).14,30,31
Overall, these studies demonstrated that CT-CA without
obstructive CAD reliably excluded the presence of sig-
nificant (>50% diameter stenosis) CAD (Fig. 6). How-
ever, overestimation of the severity of coronary lesionsresulted in a rather low positive predictive value, and a
high number of false-positive outcomes, which was most
evident on a per vessel assessment. This is caused by the
still limited spatial resolution of the current scanners and
therefore CT-CA today is not ready to replace invasive
coronary angiography. The role of CT-CA in the diag-
nosis of patients with stable angina pectoris is not firmly
established. Discussion remains as to whether a diagnos-
tic functional test, such as bicycle stress test, single-
photon emission computed tomography (SPECT) myo-
cardial perfusion imaging, or stress echo, or a diagnostic
anatomic test, CT-CA, should be used. It has recently
been shown that CT-CA may be useful as a first-line
558 Journal of Cardiovascular Medicine 2011, Vol 12 No 8
Table 3 Prediction of cardiovascular events in asymptomatic individuals using traditional risk factors model and by expanding the modelwith calcium score
N Women (%) Follow-up years AUC (RF model) AUC (RFþ calcium score model)
Budoff et al.22 (referral patients) 25 253 46 6.8 0.611 0.813Erbel et al.29 (NHR, population based cohort) 4129 53 5.0 0.681 0.749Polonsky et al.24 (MESA, population based cohort) 5878 54 5.8 0.76 0.81Jain et al.23 (MESA, population-based cohort) 4965 52 5.8 Women: 0.805; men: 0.714 Women: 0.835; men: 0.785
AUC, area under the receiver operating curve; RF, traditional risk factor model (Framingham).
Table 4 Prognostic value of calcium score determined by Agatstonmethod
Calcium score
MESA28 (n¼6809,53% female) (FU 3.75 years)(Hazard rate)
HNR29 (n¼4129,53% female) (FU 5 years)(Hazard rate)
0 1 11–100 6.09 (2.52–14.7) 1.71 (0.84–3.47)101–400 9.58 (4.96–22.6) 3.98 (1.95–8.12)>400 9.94 (4.06–24.3) 9.94 (5.10–19.41)Ln (casc þ1) 1.41 (1.31 –1.51)Ã 1.31 (1.22–1.41)
Prognostic value of calcium score determined by Agatston method in Multi-EthnicStudy of Atherosclerosis (MESA) (
Ã
Polonsky et al.24) and Heinz Nixdorf Recallstudy.
Fig. 5
Detection of obstructive coronary artery disease (CAD) with computed tomography-coronary angiography (CT-CA). A 46-year-old man, with typicalcomplaints, hypercholesterolaemia, stopped smoking 10 years previously. Calcium score: 192. Heart rate during CT-CA: 60 beats/min. High-pitchspiral mode scan was used with effective radiation dose CT-CA: 0.95 mSv. CT-CA (I) shows a pinpoint stenosis in the proximal right coronary artery(RCA). Axial projection (a–c) through the RCA shows the area stenosis of the obstructive lesion in the proximal RCA. Invasive coronary angiography(II) confirms the obstructive stenosis.

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 6/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
diagnostic test in symptomatic patients with a low to
intermediate pretest likelihood of CAD.32
Prognostic value of computed tomography-coronary angiographyCT-CA in symptomatic patients is associated with an
independent and incremental prognostic value beyond
traditional clinical risk factors33–38 as is shown in the
improvement of the C-statistic after including CT-CA in
the model with the traditional risk factors (Table 6).
The presence, extent, severity of coronary plaques and
total coronary plaque burden as determined with CT-CA
confer prognostic value, and in general the presence of
extensive CAD is associated with a worse outcome. As
may be expected, the absence of CAD or the presence of
minimal CAD is associated with an excellent outcome,
with a 10-year survival rate of 98.3%.37
CT-CA based on density values (attenuation values
expressed in Houndsfield units) allows crude character-ization of coronary plaques into calcified, non-calcified or
mixed (noncalcified and calcified) plaques.39 High expec-
tations were generated by the potential that CT-CA
might be able to identify lipid plaques which are con-
sidered to be vulnerable plaques. Although the density
values of fibrous plaques on average are higher than the
density values of lipid plaques, due to the overlap of these
density values, unfortunately, lipid plaques cannot be
distinguished from fibrous plaques.40 CT-CA also allows
assessment of remodelling of the coronary artery associ-
ated with coronary atherosclerosis.41 Motoyama et al.42
demonstrated that the combination of the presence of
low-density plaque and expansive remodelling, repre-senting a vulnerable plaque, indeed was predictive of
adverse events. More studies are needed to confirm
this observation.
Computed tomography-coronary angiographyin asymptomatic patientsOnly very limited information is available concerning the
prognostic value of CT-CA in asymptomatic individuals.
CT-CA was performed in asymptomatic patients who
were at high risk or had diabetes type II. Obstructive
CAD (>50% diameter stenosis) was present in 5–30% of
these patients.43–48 Hadamitzky et al.45 reported that in
451 individuals with a follow-up duration of 27.5 months,
CT-CA had independent predictive value beyond
traditional risk factors.
New developmentsCT-CA provides anatomic assessment of the extent and
severity of CAD and has diagnostic accuracy to detect
obstructive disease. However, the presence of obstruc-
tive disease, in particular in the presence of minimal
luminal stenosis (40–70% diameter stenosis), does not
reliably predict myocardial ischaemia, and often requires
additional functional testing with SPECT, stress echo or
magnetic resonance myocardial perfusion.
A recent promising new CT-development is the intro-
duction of adenosine stress-induced CT myocardial
CT-CA in the detection of coronary artery disease Dharampal et al. 559
Table5 Multicenter clinical trials of multislice computed tomography forthe detectionof obstructive coronary arterydisease on a perpatientand vessel level
Sensitivity Specificity PPV NPV N Prevalence (%)
Patient levelMeijboom et al .30 99 (98–100) 64 (55–73) 86 (82–90) 97 (94–100) 360 68Budoff et al.14 95 (85–99) 83 (76–88) 64 (53–75) 99 (96–100) 230 25Miller et al.31 85 (79–90) 90 (83–94) 91 (86–95) 83 (75–89) 291 56
Vessel levelMeijboom et al .30 95(92–97) 77 (74–80) 59 (55–63) 98 (96–99) 1440 26Budoff et al.14 84 (74–91) 90 (88–92) 51 (43–59) 99 (98–99) 910 10Miller et al.31 75 (69–81) 93 (90–94) 82 (77–86) 89 (86–92) 866 31
NPV, negative predictive value; PPV, positive predictive value. N , number of patients and number of total vessels; prevalence of obstructive disease on a per patient andvessel level detected by invasive coronary angiography.
Fig. 6
Exclusion of obstructive disease with CT-CA. A 56-year-old woman,with typical complaints, positive family history, hyperglycaemia nottreated, hypertension. Calcium score: 1.8. Heart rate during CT-CA:73 beats/min. ‘Step and shoot’ scan mode used with broad pulsing(30–76% of the heart cycle) because of variable heart rhythm, resultedin an effective radiation dose of 8 mSV. CT-CA shows no significantlesions in (a) right coronary artery, (b) left main, left anterior descendingand (c) left main, circumflex coronary arteries.

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 7/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
perfusion to identify myocardial ischaemia.49,50 This
would allow assessment of anatomy and function using
CT-cardiac imaging, which may be of clinical and
prognostic value. In addition, delayed enhancement
CT imaging is able to identify the viability of dysfunc-
tional left ventricular myocardium after myocardial
infarction.
In the future, with new-generation scanners and aggres-
sive radiation dose reduction, integration of coronary
anatomy, ischaemia and viability may be achieved with
cardiac CT during a single investigation.
ConclusionComputed tomography-coronary imaging has great
potential to provide anatomic information about obstruc-
tive and non-obstructive coronary plaques, in asympto-
matic individuals as well as in symptomatic patients.
The prognostic value of calcium scoring has been estab-
lished and reclassification of individuals at intermediate
risk to a lower or higher-risk category may further refine
risk stratification and lead to a more cost-effective risk
control strategy. Studies are under way to confirm this
concept. Currently, the prognostic value of CT-CA is not
firmly established, but the improved CT-image qualitywith newer-generation CT scanners will increase insights
into the progression of coronary atherosclerosis, from
earlier subclinical plaque to the more advanced sympto-
matic phase of CAD.
The high negative predictive value of CT-CA, to exclude
the presence of CAD renders CT as a suitable first-line
diagnostic test in symptomatic patients with low to inter-
mediate pretest likelihood of CAD, and may be con-
sidered an alternative to bicycle stress testing, SPECT
myocardial perfusion imaging or stress echo. Clinical
randomized trials should explore whether diagnostic
and treatment strategy using CT-CA as an alternativeto current standard care will improve clinical outcome in
symptomatic patients with stable angina, and whether
such a strategy is cost-effective.
References1 Rayner M, Allender S, Scarborough P. British Heart Foundation Health
Promotion Research G. Cardiovascular disease in Europe. Eur J
Cardiovasc Prev Rehabil 2009; 16 (Suppl 2):S43–S47.2 Hsiao EM, Rybicki FJ, Steigner M. CT coronary angiography: 256-slice and
320-detector row scanners. Curr Cardiol Rep 2010; 12:68–75.3 KetelsenD, Fenchel M,BuchgeisterM, etal. Estimation of radiationexposure
of different dose saving techniques in 128-slice computed tomographycoronary angiography. Eur J Radiol 2011. doi: 10.1016/
j.ejrad.2011.01.052.
4 Rybicki FJ,OteroHJ, Steigner ML,etal. Initial evaluationof coronary imagesfrom 320-detector row computed tomography. Int J Cardiovasc Imaging
2008; 24:535–546.5 Lim SJ, ChooKS,ParkYH,etal. Assessmentof left ventricularfunction and
volume in patients undergoing 128-slice coronary CT angiography withECG-based maximum tube current modulation: a comparison withechocardiography. Korean J Radiol 2011; 12:156–162.
6 Nakazato R, Tamarappoo BK, Smith TW, et al. Assessment of leftventricular regional wall motion and ejection fraction with low-radiationdose helical dual-source CT: comparison to two-dimensionalechocardiography. J Cardiovasc Comput Tomogr 2011; 5:149–157.
7 Rist C, Johnson TR, Muller-Starck J, et al. Noninvasive coronaryangiography using dual-source computed tomography in patients withatrial fibrillation. Invest Radiol 2009; 44:159–167.
8 Alkadhi H, Stolzmann P, Desbiolles L, et al. Low-dose, 128-slice, dual-
source CT coronary angiography: accuracy and radiation dose of the high-pitch and the step-and-shoot mode. Heart 2010; 96:933–938.9 Weustink AC, Mollet NR, Neefjes LA, et al. Preserved diagnostic
performance of dual-source CT coronary angiography with reducedradiation exposure and cancer risk. Radiology 2009; 252:53–60.
10 Achenbach S,MarwanM, RopersD, et al. Coronary computed tomographyangiography with a consistent dose below 1 mSv using prospectivelyelectrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J
2010; 31:340–346.
11 Earls JP, Berman EL, Urban BA, et al. Prospectively gated transversecoronary CT angiography versus retrospectively gated helical technique:improved image quality and reduced radiation dose. Radiology 2008;246:742–753.
12 Pflederer T, Rudofsky L, Ropers D, et al. Image quality in a low radiationexposure protocol for retrospectively ECG-gated coronary CTangiography. AJR Am J Roentgenol 2009; 192:1045–1050.
13 Leipsic J, Labounty TM, Heilbron B, et al. Estimated radiation dosereduction using adaptive statistical iterative reconstruction in coronary CTangiography: the ERASIR study. AJR Am J Roentgenol 2010; 195:655–660.
14 Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography forevaluation of coronary artery stenosis in individuals without knowncoronaryartery disease: results from the prospective multicenter ACCURACY(Assessment by Coronary Computed Tomographic Angiography ofIndividuals Undergoing Invasive Coronary Angiography) trial. J Am Coll
Cardiol 2008; 52:1724–1732.15 Nikolaou K, Knez A, Rist C, et al. Accuracy of 64-MDCT in the
diagnosis of ischemic heart disease. AJR Am J Roentgenol 2006;187:111–117.
16 MarwanM, PfledererT, SchepisT, etal. Accuracy of dual-source computedtomography to identify significant coronary artery disease in patients withatrial fibrillation: comparison with coronary angiography. Eur Heart J 2010;31:2230–2237.
17 Weustink AC, Neefjes LA, Kyrzopoulos S, et al. Impact of heart rate
frequency and variability on radiation exposure, image quality, anddiagnostic performance in dual-source spiral CT coronary angiography.Radiology 2009; 253:672–680.
18 Leschka S, Stinn B, Schmid F, et al. Dual source CT coronary angiographyin severely obese patients: trading off temporal resolution and image noise.Invest Radiol 2009; 44:720–727.
19 Fleischmann D. CT angiography: injection and acquisition technique.Radiol Clin North Am 2010; 48:237–247; vii.
20 Sarwar A, Shaw LJ, Shapiro MD, et al. Diagnostic and prognostic value ofabsence of coronary artery calcification. JACC Cardiovasc Imaging 2009;2:675–688.
21 Agatston AS,JanowitzWR, Hildner FJ,Zusmer NR,ViamonteM Jr,DetranoR. Quantification of coronary artery calcium using ultrafast computedtomography. J Am Coll Cardiol 1990; 15:827–832.
22 Budoff MJ, Shaw LJ, Liu ST, et al. Long-term prognosis associated withcoronary calcification: observations from a registry of 25,253 patients.J Am Coll Cardiol 2007; 49:1860–1870.
560 Journal of Cardiovascular Medicine 2011, Vol 12 No 8
Table6 Prediction of cardiovascular eventsin symptomatic patients by traditional risk factors model andby expandingthe model with CT-CA
Study N Female (%) Follow-up (years) AUC with RF model AUC with RF and CT-CA model
Ostrom et al.37 2538 30.0 6.5 0.69 0.83Chow et al.34 2609 47.4 2.1 0.72 0.81 (severity CAD)Carrigan et al.33 227 39.0 2.3 0.6 0.75 (total plaque score)
AUC, area under the receiver operating curve; CAD, coronary artery disease; RF, traditional risk factors.

8/3/2019 Computed Tomography Coronary Angiography in the.5
http://slidepdf.com/reader/full/computed-tomography-coronary-angiography-in-the5 8/8Copyright © Italian Federation of Cardiology. Unauthorized reproduction of this article is prohibited.
23 Jain A, McClelland RL, Polak JF, et al. Cardiovascular imaging forassessing cardiovascular risk in asymptomatic men versus women: themultiethnic study of atherosclerosis (MESA). Circ Cardiovasc Imaging
2011; 4:8–15.24 Polonsky TS, McClellandRL, JorgensenNW, etal. Coronary artery calcium
score and risk classification for coronary heart disease prediction. JAMA
2010; 303:1610–1616.25 RaggiP, Gongora MC,GopalA, CallisterTQ, BudoffM, Shaw LJ.Coronary
arterycalcium to predict all-causemortalityin elderlymen andwomen. J Am
Coll Cardiol 2008; 52:17–23.26 Lakoski SG, Greenland P, Wong ND, et al. Coronary artery calcium scores
andriskfor cardiovascular eventsin women classifiedas ‘low risk’ based onFramingham risk score: the multiethnic study of atherosclerosis (MESA).Arch Intern Med 2007; 167:2437–2442.
27 Budoff MJ, Nasir K, McClelland RL, et al. Coronary calcium predicts eventsbetter with absolute calcium scores than age-sex-race/ethnicitypercentiles: MESA (Multi-Ethnic Study of Atherosclerosis). J Am Coll
Cardiol 2009; 53:345–352.28 BudoffMJ, McClellandRL, Nasir K, etal. Cardiovascular events with absent
or minimal coronary calcification: the Multi-Ethnic Study of Atherosclerosis(MESA). Am Heart J 2009; 158:554–561.
29 Erbel R, Mohlenkamp S, Moebus S, et al. Coronary risk stratification,discrimination, and reclassification improvement based on quantification ofsubclinical coronary atherosclerosis: the Heinz Nixdorf Recall study. J Am
Coll Cardiol 2010; 56:1397–1406.30 Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice
computed tomography coronary angiography: a prospective, multicenter,
multivendor study. J Am Coll Cardiol 2008; 52:2135–2144.31 Miller JM, RochitteCE,Dewey M, etal. Diagnostic performance of coronary
angiography by 64-row CT. N Engl J Med 2008; 359:2324–2336.32 Weustink AC,Mollet NR,Neefjes LA, etal. Diagnostic accuracy and clinical
utility of noninvasive testing for coronary artery disease. Ann Intern Med
2010; 152:630–639.33 Carrigan TP, Nair D, Schoenhagen P, et al. Prognostic utility of 64-slice
computed tomography in patients with suspected but no documentedcoronary artery disease. Eur Heart J 2009; 30:362–371.
34 Chow BJ, Wells GA, Chen L, et al. Prognostic value of 64-slice cardiaccomputed tomography severity of coronary artery disease, coronaryatherosclerosis, and left ventricular ejection fraction. J Am Coll Cardiol
2010; 55:1017–1028.35 Hadamitzky M, Distler R, Meyer T, et al. Prognostic value of coronary
computed tomographic angiography in comparison with calcium scoringand clinical risk scores. Circ Cardiovasc Imaging 2011; 4:16–23.
36 Min JK, Shaw LJ, Devereux RB, et al. Prognostic value of multidetector
coronary computed tomographic angiography for prediction of all-causemortality. J Am Coll Cardiol 2007; 50:1161–1170.
37 Ostrom MP, Gopal A, Ahmadi N, et al. Mortality incidence and the severityof coronary atherosclerosis assessed by computed tomographyangiography. J Am Coll Cardiol 2008; 52:1335–1343.
38 RubinshteinR, Halon DA,Gaspar T, Peled N, Lewis BS.Cardiac computedtomographic angiography for risk stratification and prediction of latecardiovascular outcome eventsin patients with a chest pain syndrome. Int J
Cardiol 2009; 137:108–115.39 Springer I, Dewey M. Comparison of multislice computed tomography with
intravascular ultrasound for detection and characterization of coronaryartery plaques: a systematic review. Eur J Radiol 2009; 71:275–282.
40 Pohle K, Achenbach S, Macneill B, et al. Characterization of noncalcifiedcoronary atherosclerotic plaque by multidetector row CT: comparison toIVUS. Atherosclerosis 2007; 190:174–180.
41 Achenbach S, Ropers D, Hoffmann U, et al. Assessment of coronaryremodeling in stenotic and nonstenotic coronary atherosclerotic lesions bymultidetector spiral computed tomography. J Am Coll Cardiol 2004;43:842–847.
42 Motoyama S, Sarai M, Harigaya H, et al. Computed tomographicangiography characteristics of atherosclerotic plaques subsequentlyresulting in acute coronary syndrome. J Am Coll Cardiol 2009; 54:49–57.
43 Bachar GN, Atar E, Fuchs S, Dror D, Kornowski R. Prevalence and clinicalpredictors of atherosclerotic coronary artery disease in asymptomaticpatients undergoing coronary multidetector computed tomography. Coron
Artery Dis 2007; 18:353–360.44 Choi EK, Choi SI, Rivera JJ, et al. Coronary computed tomography
angiography as a screening tool for the detection of occult coronary arterydisease in asymptomatic individuals. J Am Coll Cardiol 2008; 52:357–
365.45 Hadamitzky M, Meyer T, Hein F, et al. Prognostic value of coronary
computed tomographic angiography in asymptomatic patients. Am J
Cardiol 2010; 105:1746–1751.46 Iwasaki K, MatsumotoT, Aono H, Furukawa H, Samukawa M. Prevalence of
subclinical atherosclerosis in asymptomatic patients with low-to-intermediate risk by 64-slice computed tomography. Coron Artery Dis
2011; 22:18–25.47 Rivera JJ, Nasir K, Choi EK, et al. Detection of occult coronary artery
disease in asymptomatic individuals with diabetes mellitus usingnoninvasive cardiac angiography. Atherosclerosis 2009; 203:442–448.
48 Romeo F, Leo R, Clementi F, et al. Multislice computed tomography in anasymptomatic high-risk population. Am J Cardiol 2007; 99:325–328.
49 Bamberg F, Klotz E, Flohr T, et al. Dynamic myocardial stress perfusionimaging using fast dual-source CT with alternating table positions: initialexperience. Eur Radiol 2010; 20:1168–1173.
50 Bastarrika G, Ramos-Duran L, Rosenblum MA, Kang DK, Rowe GW,
Schoepf UJ. Adenosine-stress dynamic myocardial CT perfusion imaging:initial clinical experience. Invest Radiol 2010; 45:306–313.
CT-CA in the detection of coronary artery disease Dharampal et al. 561


















