Positron Emission Tomography/Computed Tomography: Protocol ...
Upload
saanvi2011Category
view
302download
4description

DR. SUNITA KUMAWATDEPTT. OF OPHTHALMOLOGY
S.P.M.C. BIKANER
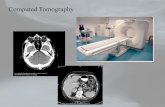
COMPUTED TOMOGRAPHY

Computer tomography (CT), originally known as computed axial tomography (CAT or CT scan) and body section rentenography.
Designed by Godfrey N. Hounsfield to overcome the visual representation challenges in radiography and conventional tomography

Plain radiography involves X-rays that pass through the patient, and create an image directly on a photographic film.
Image is basically a shadow.
Shadows give you an incomplete picture of an object's shape

Thus a three dimensional structure is depicted on a two dimensional plane, giving rise to disturbing superimposition.

CT completely eliminates the superimposition of images of structures outside the area of interest.
The word "tomography" is derived from the Greek tomos (slice) and graphein (to write).
● definition - imaging of an object by analyzing its slices

Cross section slices
Think like looking into a loaf of bread by cutting it into thin slices and then viewing the slices individually.

Because of inherent high-contrast resolution of CT, tissues that differ in physical density by less than 1% can be distinguished.
It provides quicker scans, is able to image bone directly, shows the presence of calcification better, and is the modality of choice in patients with suspected metallic orbital foreign bodies.

CT generally more widely available and cheaper.
Allows us to discern the location, extent and configuration of the lesion and lesion’s effect on adjacent structures.
In addition, knowing the precise location of a lesion, it facilitates the planning of an appropriate surgical approach to minimise morbidity.

The CT machine: Principle
X-rays are attenuated, on their way through tissues due to absorption of energy.
Different tissues provide different degrees of X-ray attenuation, and it is this property that forms the basis of CT imaging technique.
CT machine combines X radiation and radiation detectors coupled with a computer to create cross sectional image of any part of the body.

The X-ray tube of the CT machine emits a thin collimated fan-shaped beam of X-rays that are attenuated as they pass through the tissues.
They are detected by an array of special detectors.

Within these detectors, X-ray photons generate electrical signals, which are converted into images.
High density areas are arbitrarily depicted as white whereas low density areas appear black.
CT images contain information from thin slices of tissue only, and are thus devoid of superimposition.

Slice thickness: Spatial resolution of a CT depends on
slice thickness. The thinner the slice, the higher the resolution.
Vary from 1-10 mm. Usually, 2mm cuts are optimal for the eye
and orbit. In special situations (like evaluation of the
orbital apex), thinner slices of 1mm can be more informative.

Thin slices are good for spatial resolution, but require higher radiation dose, a greater number of slices, and eventually longer examination time. The choice of slice thickness therefore is a balance of these factors.

CT terminology
Attenuation Hyperattenuating (hyperintense): tissue
with high protien content (lens, clotted blood, tenacious mucus secretions)
Hypoattenuating (hypointense): pathologies with high water content (edema, necrosis)
Isoattenuating (isodense)

Attenuation is measured in Hounsfield units.
2000 HU Scale: (-1000 to 1000)1. -1000 is air (allows 100% transmission
of X-rays)2. 0 is water3. 1000 is cortical bone

What we can see The brain is grey
White matter is usually dark grey (40)
Grey matter is usually light grey (45)
CSF is black (0)Things that are bright on CTBone or calcification (>300)ContrastHemorrhage (Acute ~ 70)Hypercellular massesMetallic foreign bodies

Tissue window:Tissues around the orbit form a spectrum of
composition and density, ranging from air (within the para-nasal sinuses) to the bony orbit.
Tissue window refers to the selection of a small range from this variable spectrum to decipher the finer details of the tissue of interest. Each tissue window has a specific window width and window level. Thus we have bone window, soft tissue window, brain window and so on

A thorough evaluation of any tissue is possible only when it is scanned under appropriate window settings.
Soft-tissue window is best for evaluating orbital soft tissue lesions, whereas fractures and bony details are better seen with bone window settings

Window width(WW): refers to the span of CT numbers on the Hounsfield scale that are selected to display the given image.
Can vary from a few CT numbers to the entire range available on the system.
Since the Hounsfield scale usually ranges from –1000 to +1000 HU or above, the maximum WW can be approximately 2000.

Thus at a WW of 2000, air will be black and bone will be white. The rest of the tissues will be depicted in shades of gray between these two extremes of the spectrum.
A wider WW thus depicts a large number of tissues, and bone details can be better appreciated.

Window level (WL):Midpoint of the selected
span of Hounsfield value,(point midway between totally black and totally white).
Eg:WW of 100 with a WL of +50 displays all tissues with Hounsfield value ranging from zero to +100 HU.
Values above +100 HU will be white, those below zero will be black.

Those between the two will have all shades of gray. This window setting is ideal for soft tissue evaluation.
WW of 2000 with a WL of +200 displays all tissues with Hounsfield value ranging from –800 HU to +1200 HU.
This setting is ideal for evaluation of bone.

Intraocular structures show very low variations in tissue consistency and thus need a fairly narrow window setting,
whereas structures within the orbit show a wide variation in tissue consistency, and require a wide window setting.

Contrast enhancement: Contrast study involves imaging the area of
interest after intravenous injection of a radiological contrast medium.
Most orbital pathologies can be easily visualised without infusion of a contrast medium as orbital fat provides intrinsic background contrast.
A contrast-enhancing lesion is one which becomes bright or more intense after contrast medium infusion.

Cotrast agent Increases tissue’s Hounsfield value and thus increases its brightness.
Evaluation of optic chiasma, perisellar region and extraorbital extensions of orbital tumours is best possible with contrast enhancement.
Contrast enhancement also helps to define vascular and cystic lesions as well as optic nerve lesions, particularly meningioma and glioma.


Imaging planes
1. Axial 2. Coronal3. Sagittal
Plane-axial imaging parellel to infra-orbitomeatal line

The plane inclined at 30° to the orbito-meatal line best depicts the optic canal and the entire anterior visual pathway.


Passages of the Bony Orbit
1.Superior orbital fissure
2.Inferior orbital fissure
3.Optic canal

Components of CT scan:1. Patient data and laterality2. Slice thickness3. Type of CT scan:

Axial scan


Coronal scan


Approach to differential diagnosis:
General principle:Location,Anatomic structure,Imaging feature andClinical presentation of patient.

Using a compartmental approach, a lesion is first localized to one of four compartments:
1. Globe,2. Optic nerve sheath complex,3. Intraconal space,4. Extraconal space.

Once primary location of a lesion determined we should consider other parameters:
Characterstics of margins of lesion,Associated bony changes,Enhancement pattern,Pathophysiologic basis,Age of presentation .

Imaging in different pathophysiologies

Trauma
CT is the procedure of choice in evaluating patients with orbital trauma. It is a rapid test that can detect bony and soft tissue injury, haemorrhage and foreign bodies.
May be blunt, penetrating or involve implantation of foreign bodies.
The classical injury seen in blunt trauma is the blowout fracture. This commonly involves the floor and medial wall of the orbit.

Orbital fracture
A “tear drop” shape pointing toward the fracture, indicating muscle sheath tethering.


Orbital fracture
Inferior and medial blow out fractures:
Coronal CT showing displacement of bony fragments of left orbital floor and fracture of left lamina papyracea.

Orbital fracture
Partial herniation of medial rectus and orbital fat into left ethmoid air cells through fractured lamina papyracea.
Intra orbital emphysema, should raise suspicion of a blowout fracture.

Orbital fracture

Orbital fracture

Globe rupture
Anterior chamber is shallow,
Density in AC is higher,
Area of high density in vitreous .
Globe is flat on posterior side.

Proptosis
A line connecting the most distal tips of lateral orbital walls is drawn.
The distance from ant. Margin of globe to this line should not exceed 21 mm.

Intra ocular foreign body
Axial scan of a patient with retained intraocular foreign body. The radiodense streaks radiating from the foreign body represent beam hardening artifact which is typically seen with metallic foreign bodies

Intra ocular foreign body

Infections
Patient with right periorbital inflammation.
Axial CT demonstrates right lid swelling and extent of preseptal inflammatory swelling.


Bilateral discrete lacrimal gland enlargement

Sub periosteal abscess

Fronto ethmoid mucocoele:

Thyroid associated ophthalmopathy
Isodense Fusiform enlargement of extraocular muscle with sparing tendinous attatchment.
Additional increased orbital fat, lacrimal gland enargement, eyelid edema, stretching of optic nerve may be seen.

Thyroid ass. ophthalmopathy

Orbital pseudotumor
Moderate diffuse enhancement Presenting as infiltrative soft tissue mass in
right orbit with loss of normal tissue planes.

Orbital pseudotumor
Focal &infiltrative, poorly circumscribed, thickening on lacrimal and orbital structures may be seen.
Thickening of muscles involves tendinous insertion.

Optic neuritis
CT usualy normal,May show minimal optic nerve enlargement,Best imaging is MRI, Ct showing thickening and straightening of optic nerve

Optic nerve glioma
Usually involve optic nerve, chiasm, and optic tract.
Causes enlargement and tortuosity these structures.
optic nerve may show kinking & tortuosity or fusiform enlargement.
Iso to slightly hypointense.

Optic nerve glioma
Enlargement of optic canal
Tubular thickening of the right intraorbital optic nerve.(a)
(b, different patient) There is marked fusiform enlargement of the left
optic nerve causing anterior displacement of the globe.

Optic nerve sheath meningioma
Segmental or diffuse thickening of optic nerve
Fusiform and uniform thickening of optic nerve sheath.
Normal optic nerve running through the tumor have “tram- track” appearance on axial and saggital images.

Lymphoma
On CT it appears commonly as hyperdense contrast enhancing mass.
Axial, oblique sagittal and coronal contrast enhancing CT showing patient with preseptal lymphomatous mass (arrow)

Retinoblastoma
Hyperattenuating mass.
Presence of calcification
Margins may smooh or irregular.
Enhances on contrast.



Metastasis
Aggressive destruction of b/l orbital walls.Intra orbital and extradural enhancing soft
tissue mass.

Fibrous dysplasia
Fibrous dysplasia most commonly involves the frontal or sphenoid bone.
It characteristically produces expansion of the bone shown as prominent calcified bone density material on CT.

Dermoid cyst
Well defined non enhancing low density lesions.
Bony erosion may occur related to their slow growth
Dermoid cyst showing low fat density contents, and remodeling of the adjacent bone.

Capillary haemangioma
Extraconal in location and tend to occur in anterior part of orbit.
On CT: Well circumscribed or infiltrative lesions with characteristic intense homogenous enhancement.
Intracranial extension through superior orbital fissure or optic canal can occur

Cavernous haemangioma
Coronal CT scan showing left cavernous haemangioma. mass is intraconal, well defined, homogeneous, with smooth margins
HyperdenseWell circumscribed

Encapsulated Can be easily separated from the optic nerve
and extraocular muscles.

Orbital lymphangioma
Axial CT scan of A case of orbital lymphangioma irregular margin, heterogenous consistency, and the presence of phleboliths;

Degenerative
Optic drusen: on CT, disc shows calcification.