ComprehensiveMetabolomicCharacterization of …If the various types of coronary artery disease (CAD)...
13
Comprehensive Metabolomic Characterization of Coronary Artery Diseases Yong Fan, MS, a Yong Li, MD, PHD, b Yan Chen, MD, PHD, c,d Yi-Jing Zhao, BS, a Li-Wei Liu, BS, a Jin Li, BS, a Shi-Lei Wang, BS, a Raphael N. Alolga, MS, a Yin Yin, MD, PHD, e Xiang-Ming Wang, MD, PHD, f Dong-Sheng Zhao, MD, g Jian-Hua Shen, MD, PHD, h Fan-Qi Meng, MD, PHD, i Xin Zhou, MD, PHD, j Hao Xu, MS, b Guo-Ping He, MS, b Mao-De Lai, MD, PHD, a Ping Li, PHD, a Wei Zhu, MD, PHD, j Lian-Wen Qi, PHD a ABSTRACT BACKGROUND Pathogenesis and diagnostic biomarkers for diseases can be discovered by metabolomic profiling of human fluids. If the various types of coronary artery disease (CAD) can be accurately characterized by metabolomics, effective treatment may be targeted without using unnecessary therapies and resources. OBJECTIVES The authors studied disturbed metabolic pathways to assess the diagnostic value of metabolomics-based biomarkers in different types of CAD. METHODS A cohort of 2,324 patients from 4 independent centers was studied. Patients underwent coronary angiog- raphy for suspected CAD. Groups were divided as follows: normal coronary artery (NCA), nonobstructive coronary atherosclerosis (NOCA), stable angina (SA), unstable angina (UA), and acute myocardial infarction (AMI). Plasma metabolomic profiles were determined by liquid chromatography–quadrupole time-of-flight mass spectrometry and were analyzed by multivariate statistics. RESULTS We made 12 cross-comparisons to and within CAD to characterize metabolic disturbances. We focused on comparisons of NOCA versus NCA, SA versus NOCA, UA versus SA, and AMI versus UA. Other comparisons were made, including SA versus NCA, UA versus NCA, AMI versus NCA, UA versus NOCA, AMI versus NOCA, AMI versus SA, significant CAD (SA/UA/AMI) versus nonsignificant CAD (NCA/NOCA), and acute coronary syndrome (UA/AMI) versus SA. A total of 89 differential metabolites were identified. The altered metabolic pathways included reduced phospholipid catabolism, increased amino acid metabolism, increased short-chain acylcarnitines, decrease in tricarboxylic acid cycle, and less biosynthesis of primary bile acid. For differential diagnosis, 12 panels of specific metabolomics-based biomarkers provided areas under the curve of 0.938 to 0.996 in the discovery phase (n ¼ 1,086), predictive values of 89.2% to 96.0% in the test phase (n ¼ 933), and 85.3% to 96.4% in the 3-center external sets (n ¼ 305). CONCLUSIONS Plasma metabolomics are powerful for characterizing metabolic disturbances. Differences in small-molecule metabolites may reflect underlying CAD and serve as biomarkers for CAD progression. (J Am Coll Cardiol 2016;68:1281–93) © 2016 by the American College of Cardiology Foundation. From the a State Key Laboratory of Natural Medicines, China Pharmaceutical University, Nanjing, Jiangsu, China; b Department of Cardiology, the Affiliated Wujin Hospital of Jiangsu University, Changzhou, Jiangsu, China; c Department of Emergency Center, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China; d Medical Department, Women and Children Health Care Hospital of Jiangsu Province, Nanjing, Jiangsu, China; e Department of Gynecology and Obstetrics, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China; f Department of Geriatric Cardiology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China; g Department of Cardiology, the Second Affiliated Hospital of Nantong University, Nantong, Jiangsu, China; h Department of Cardiology, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, China; i Department of Cardiology, Xiamen Cardiovascular Hospital, Xiamen, Fujian, China; and the j Department of Oncology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China. This study was supported in part by the National Natural Science Foundation of China (81421005, 81571873), National Excellent Doctoral Dissertation of PR China (201278), and Jiangsu Province Science Fund for Distinguished Young Scholars (BK20130025). The authors have reported that they have no relationships relevant to the contents of this paper to disclose. Drs. Yong Fan, Yong Li, and Yan Chen contributed equally to this work. Manuscript received March 3, 2016; revised manuscript received June 7, 2016, accepted June 14, 2016. Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 68, NO. 12, 2016 ª 2016 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER http://dx.doi.org/10.1016/j.jacc.2016.06.044
Transcript of ComprehensiveMetabolomicCharacterization of …If the various types of coronary artery disease (CAD)...

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 8 , N O . 1 2 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 6 . 0 4 4
ComprehensiveMetabolomicCharacterizationof Coronary Artery Diseases
Yong Fan, MS,a Yong Li, MD, PHD,b Yan Chen, MD, PHD,c,d Yi-Jing Zhao, BS,a Li-Wei Liu, BS,a Jin Li, BS,aShi-Lei Wang, BS,a Raphael N. Alolga, MS,a Yin Yin, MD, PHD,e Xiang-Ming Wang, MD, PHD,f Dong-Sheng Zhao, MD,g
Jian-Hua Shen, MD, PHD,h Fan-Qi Meng, MD, PHD,i Xin Zhou, MD, PHD,j Hao Xu, MS,b Guo-Ping He, MS,b
Mao-De Lai, MD, PHD,a Ping Li, PHD,a Wei Zhu, MD, PHD,j Lian-Wen Qi, PHDa
ABSTRACT
Fro
Ca
the
He
Ho
of
UniDe
Affi
Na
Jia
rel
thi
Ma
BACKGROUND Pathogenesis and diagnostic biomarkers for diseases can be discovered by metabolomic profiling of
human fluids. If the various types of coronary artery disease (CAD) can be accurately characterized by metabolomics,
effective treatment may be targeted without using unnecessary therapies and resources.
OBJECTIVES The authors studied disturbed metabolic pathways to assess the diagnostic value of metabolomics-based
biomarkers in different types of CAD.
METHODS A cohort of 2,324 patients from 4 independent centers was studied. Patients underwent coronary angiog-
raphy for suspected CAD. Groups were divided as follows: normal coronary artery (NCA), nonobstructive coronary
atherosclerosis (NOCA), stable angina (SA), unstable angina (UA), and acute myocardial infarction (AMI). Plasma
metabolomic profiles were determined by liquid chromatography–quadrupole time-of-flight mass spectrometry and were
analyzed by multivariate statistics.
RESULTS We made 12 cross-comparisons to and within CAD to characterize metabolic disturbances. We focused on
comparisons of NOCA versus NCA, SA versus NOCA, UA versus SA, and AMI versus UA. Other comparisons were made,
including SA versus NCA, UA versus NCA, AMI versus NCA, UA versus NOCA, AMI versus NOCA, AMI versus SA, significant
CAD (SA/UA/AMI) versus nonsignificant CAD (NCA/NOCA), and acute coronary syndrome (UA/AMI) versus SA. A total of
89 differential metabolites were identified. The altered metabolic pathways included reduced phospholipid catabolism,
increased amino acid metabolism, increased short-chain acylcarnitines, decrease in tricarboxylic acid cycle, and less
biosynthesis of primary bile acid. For differential diagnosis, 12 panels of specific metabolomics-based biomarkers
provided areas under the curve of 0.938 to 0.996 in the discovery phase (n ¼ 1,086), predictive values of 89.2% to
96.0% in the test phase (n ¼ 933), and 85.3% to 96.4% in the 3-center external sets (n ¼ 305).
CONCLUSIONS Plasma metabolomics are powerful for characterizing metabolic disturbances. Differences in
small-molecule metabolites may reflect underlying CAD and serve as biomarkers for CAD progression.
(J Am Coll Cardiol 2016;68:1281–93) © 2016 by the American College of Cardiology Foundation.
m the aState Key Laboratory of Natural Medicines, China Pharmaceutical University, Nanjing, Jiangsu, China; bDepartment of
rdiology, the Affiliated Wujin Hospital of Jiangsu University, Changzhou, Jiangsu, China; cDepartment of Emergency Center,
First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China; dMedical Department, Women and Children
alth Care Hospital of Jiangsu Province, Nanjing, Jiangsu, China; eDepartment of Gynecology and Obstetrics, the First Affiliated
spital of Nanjing Medical University, Nanjing, Jiangsu, China; fDepartment of Geriatric Cardiology, the First Affiliated Hospital
Nanjing Medical University, Nanjing, Jiangsu, China; gDepartment of Cardiology, the Second Affiliated Hospital of Nantong
iversity, Nantong, Jiangsu, China; hDepartment of Cardiology, Northern Jiangsu People’s Hospital, Yangzhou, Jiangsu, China;
partment of Cardiology, Xiamen Cardiovascular Hospital, Xiamen, Fujian, China; and the jDepartment of Oncology, the First
liated Hospital of Nanjing Medical University, Nanjing, Jiangsu, China. This study was supported in part by the National
tural Science Foundation of China (81421005, 81571873), National Excellent Doctoral Dissertation of PR China (201278), and
ngsu Province Science Fund for Distinguished Young Scholars (BK20130025). The authors have reported that they have no
ationships relevant to the contents of this paper to disclose. Drs. Yong Fan, Yong Li, and Yan Chen contributed equally to
s work.
nuscript received March 3, 2016; revised manuscript received June 7, 2016, accepted June 14, 2016.

ABBR EV I A T I ON S
AND ACRONYMS
AMI = acute myocardial
infarction
AUC = area under the curve
CAD = coronary artery disease
NCA = normal coronary artery
NOCA = nonobstructive
coronary atherosclerosis
OPLS-DA = orthogonal
projection to latent structure-
discriminant analysis
ROC = receiver-operating
characteristic
SA = stable angina
UA = unstable angina
VIP = variable importance in
the projection
Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1282
C oronary artery disease (CAD) re-mains a leading cause of mortalityworldwide. According to the Global
Burden of Disease Study 2013, CAD wasresponsible for an estimated 8.14 milliondeaths (16.8%) globally that year (1). On thebasis of clinical symptoms, extent of arterialblockage, and myocardial injury, CAD isdivided into different categories: nonob-structive coronary atherosclerosis (NOCA),stable angina pectoris (SA), unstable anginapectoris (UA), and acute myocardial infarc-tion (AMI) (2). UA and AMI are also referredto as acute coronary syndrome (ACS).
If the molecular mechanisms of CAD couldbe deciphered, its incidence and associatedmortality might be reduced. Multiple, com-plex molecular events characterize the pro-
gression of CAD. Atherosclerosis, a common cause ofangina and AMI, is a slow and complicated process(3). What exactly causes plaque, how plaque developsover time, and why plaque dislodges to form a clot arelargely unknown. Experimental models of athero-genesis provide information about the molecularmechanisms of plaque growth. Nevertheless, thetransition from coronary stability to instability isless well understood because animal models of thisprogression are unavailable (4).
SEE PAGE 1294
With early screening and differential diagnosis ofCAD, optimal patient-specific therapies can be initi-ated. The current clinical diagnosis differentiatesbetween the types of CAD on the basis of symptoms,electrocardiogram (ECG), cardiac markers, stresstesting, and coronary angiography (5–7). Among thesemethods, invasive coronary angiography is the diag-nostic “gold standard” (8), but its specialized tech-nology and high cost limit it to a select population (5).On the one hand, a sizable portion of individuals whounderwent invasive angiography had been shown tohave normal coronary arteries (9). On the other hand,episodes of myocardial ischemia or infarction arepossible after atypical symptoms in some patientswith CAD, especially in patients who are elderly orhave diabetes (10).
Abnormal metabolism also characterizes CAD.Metabolic alterations in the heart result in changes inthe metabolome of biofluids (11). Metabolites couldclarify pathogenesis for potential therapeutic targets.A combination of multiple small-molecule metabo-lites may offer excellent diagnostic values (12).Metabolomics, a rapidly expanding field in systemsbiology, measures metabolic alterations in response
to disease progression (12). Plasma, a frequentlyconsidered pool of metabolites, has been a source formetabolic profiling (13). Liquid chromatography massspectrometry provides the most compatible tech-nique for sensitive detection of small-molecule me-tabolites with robust reliability and reproducibility(14,15). This work describes a comprehensive metab-olomic evaluation for identifying types of CAD.
METHODS
PATIENTS AND STUDY DESIGN. Patients enrolledfrom center 1 (the Affiliated Wujin Hospital of JiangsuUniversity, Changzhou, China) between August 2009and December 2015 formed the discovery and testphases. Subjects recruited at 3 other centers consti-tuted the external validation phase between January2014 and December 2015 (center 2, the First People’sHospital, Nantong, China; center 3, Northern JiangsuPeople’s Hospital, Yangzhou, China; and center 4, theFirst Affiliated Hospital of Nanjing Medical Univer-sity, Nanjing, China).
Inclusion criteria were symptoms of chest pain,cardiovascular risk factors, ischemic changes in ECG,or elevated myocardial enzymes. Coronary angiog-raphy was required to confirm the diagnosis. Weexcluded patients with aortic dissection, pulmonaryembolism, malignant tumor, autoimmune disorders,severe infectious diseases, trauma, a recent surgicalprocedure, severe heart failure with left ventricularejection fraction <20%, liver dysfunction (alanineaminotransferase level >135 U/l), severe renaldysfunction (creatinine >3.0 mg/dl), or blood-borneinfectious diseases, including human immunodefi-ciency virus/acquired immunodeficiency syndrome,hepatitis B, and hepatitis C. We also excluded pa-tients with myocarditis, pericarditis, and Takotsubocardiomyopathy. Informed consent was obtainedfrom all patients. This study was performed under theguidance of the Helsinki Declaration and wasapproved by all centers.
Plasma samples were collected before the coronaryangiography surgery and were immediately frozenat �80�C for metabolomic analyses. Acetonitrile waschosen as the optimal extraction solvent over meth-anol, ethanol, methanol/ethanol (1:1), and methanol/acetonitrile/acetone (1:1:1). To ensure data quality formetabolic profiling, pooled quality control sampleswere prepared by mixing equal amounts of plasma(10 ml) from 82 patients with normal coronary arteriesand 125 patients with CAD. Detailed sample prepara-tion methods are in the Online Appendix.
DEFINITION OF CORONARY ARTERY TYPES. Thediagnosis was made on the basis of symptoms,

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1283
laboratory tests, ECG, and coronary angiographic re-sults. Patients with no stenosis in coronary arteriescomprised the normal coronary artery (NCA) group,which also included patients with myocardialbridging, intercostal neuralgia, reflux esophagitis,cervical spondylopathy, and unexplained chest pain.In the AMI group, patients had ischemic chest pain,increased values of cardiac enzymes, and dynamicST-T change on ECG. In the UA group, patients had ahistory of angina (within 1 month), irregular angina atrest or with minimal exertion, and no elevation introponin. The SA group included patients with anginaof stable frequency, lasting up to 10 min, orprovocative-palliative factors. Patients with <50%stenosis in all coronary vessels were in the NOCAgroup. The angiographic data were confirmed inde-pendently by 2 observers in each study.
METABOLOMICS STUDY. Liquid chromatographicseparation for processed plasma was achieved on a100 � 2.1-mm Zorbax Eclipse Plus 1.8-mm C18 columnusing a 1290 Infinity System, whereas mass spec-trometry was performed on a 6530 Quadrupole-Timeof Flight system (all devices from Agilent Technolo-gies, Santa Clara, California). Samples were assignedby the study administrator with a random-numbergenerator in Excel (Microsoft, Redmond, Washing-ton) to receive 3 sequences for samples in the dis-covery phase from center 1, test phase from center 1,and external validation phases from centers 2 to 4.Samples from the 4 independent centers were thenalternated and analyzed according to the generatedrandom order. During analyses of the samplesequence, 1 quality control sample was run afterevery 20 injections. The acquired mass spectrometrydata (.d) were exported to data format (.mzdata) filesby MassHunter Workstation Software (versionB.06.00, Agilent Technologies). Data pre-treatmentprocedures, such as nonlinear retention time align-ment, peak discrimination, filtering, alignment,matching, and identification, were performed inXCMS package (Scripps Center for Metabolomics andMass Spectrometry, La Jolla, California). Detailedparameters for the data analyses are provided in theOnline Appendix. Open database sources, includingthe KEGG, MetaboAnalyst, Human MetabolomeDatabase, and METLIN, were used to identify meta-bolic pathways.
STATISTICAL ANALYSIS. Results are expressed asthe mean � SD for continuous variables and as thenumber (percent) for categorical variables. To maxi-mize identification of differences in metabolic pro-files between groups, the orthogonal projection tolatent structure-discriminant analysis (OPLS-DA)
model was applied using SIMCA version 14.0.1(Umetrics AB, Umea, Sweden). In addition to themultivariate statistical method, the Student t test wasalso applied to measure the significance of eachmetabolite. The resultant p values for each metabo-lite in all cross-comparisons were corrected by Bon-ferroni correction. The p values across all metaboliteswithin each comparison were adjusted to account formultiple testing by a false discovery rate method.Heat maps and hierarchical cluster analyses wereconducted using MeV version 4.6.0. The Cytoscapesoftware package version 3.2.0 (National Instituteof General Medical Sciences, Bethesda, Maryland)was used to plot the correlation networks. Logisticregression analysis and receiver operating character-istic (ROC) analysis were used for diagnosis ofdifferent CAD stages. Statistical analyses were per-formed using SPSS software version 19.0 (IBM Corp.,Armonk, New York). An adjusted p value of <0.05 wasconsidered statistically significant.
RESULTS
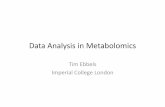
A total of 2,324 patients were enrolled from 4 inde-pendent centers in China (Figure 1). All participantsunderwent coronary angiography to identify thelocation and extent of the blockage. As shown inOnline Figure 1, there was a progressive increase instenosis severity across the groups from NOCA to SA,UA, and then AMI.
The discovery phase included 1,086 randomlyselected participants from center 1, including fromthe following groups: 116 NCA, 276 NOCA, 63 SA, 307UA, and 324 AMI patients. Baseline characteristicsand laboratory data are shown in Table 1. Comparedwith NCA subjects, CAD patients had higher levels ofhemoglobin, glucose, and estimated glomerularfiltration rate, but lower levels of total cholesterol aswell as low- and high-density lipoprotein cholesterol.CAD patients were older than subjects without coro-nary diseases, although there were no statisticallysignificant differences in age among the patientgroups. The percentage of females was lower amongCAD patients than in NCA subjects.
The test phase from center 1 included 933 partici-pants. Their baseline characteristics are shown inOnline Table 1, and numbers participating in theexternal validation phase are shown in Figure 1.Demographic information of external validationbatches is shown in Online Tables 2 to 4.
CROSS COMPARISONS TO AND WITHIN CAD
GROUPS. Typical total ion chromatograms of the 5representative samples obtained are presented inOnline Figure 2. After peak alignment and removal of

FIGURE 1 Study Design
NCA (n = 116)
NOCA (n = 276)
SA (n = 63)
ACS (n = 631)
UA (n = 307) AMI (n = 324)
Myocardial infarction
Discovery phase (n = 1,086)
Plaque formation
Plaque growth
Plaque rupture
Center 1(n = 2,019)
CoronaryAngiography
Patients Suspected withHeart Disease (n = 2,324)
Validation phase (n = 933)
Internal Validation
Disturbed metabolicpathways
Biomarkerpanels
External Validation
CoronaryAngiography
Center 2(n = 71)
Center 3(n = 68)
Center 4(n = 166)
Differentialmetabolites
This study, involving 2,324 patients with suspected heart disease, included both discovery and validation phases. ACS¼ acute coronary syndrome; AMI¼ acute
myocardial infarction; NCA ¼ normal coronary artery; NOCA ¼ nonobstructive coronary atherosclerosis; SA ¼ stable angina; UA ¼ unstable angina.
Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1284
missing values, 2,032 positive-mode features weredetected. A total of 1,130 ions had significantlychanged (p < 0.05). The OPLS-DA model was used tocharacterize the metabolic disturbances. The ionswith variable importance in the projection (VIP)values >1.0 were considered the potentialdifferential metabolites. We compared the variousstages of CAD to normal coronary arteries and witheach other, identifying and characterizing specificmetabolites and metabolic pathways. We focused onNOCA versus NCA for plaque formation, SA versusNOCA for plaque growth, UA versus SA for transitionfrom coronary stability to instability, and AMIversus UA.
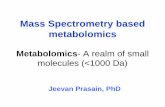
Clear differences were obtained for the following:NOCA versus normal arteries, cumulative R2Y at 0.655and Q2 at 0.503 (Figure 2A); SA versus NOCA, R2Y at0.626 and Q2 at 0.518 (Figure 2B); UA versus SA, R2Y at0.645 and Q2 at 0.548 (Figure 2C); and AMI versusUA, R2Y at 0.641 and Q2 at 0.595 (Figure 2D). Themetabolites with VIP values >1.0 and adjusted
p values <0.05 for each comparison appear in OnlineTable 5. Figures 2E to 2H represent the perturbedpathways. For NOCA versus NCA, metabolismchanged for glycerophospholipid, purine, and sphin-golipid; for SA versus NOCA, glycerophospholipid,valine-leucine-isoleucine, primary bile acid biosyn-thesis, and arginine-proline; for UA versus SA, glyc-erophospholipid, alanine-aspartate-glutamate, andarginine-proline; and for AMI versus UA, glycer-ophospholipid, sphingolipid, and arginine-proline.Disturbance of glycerophospholipid metabolism wasthe most significant in all paired comparisons. TheOPLS-DA plots of 8 other cross-comparisons,including SA versus NCA, UA versus NCA, AMIversus NCA, UA versus NOCA, AMI versus NOCA, AMIversus SA, significant CAD (SA/UA/AMI) versusnonsignificant CAD (NCA/NOCA), and ACS (UA/AMI)versus SA, are shown in Online Figure 3. The differ-ential metabolites and altered metabolic pathways forthese comparisons appear in Online Table 5 andOnline Figure 4, respectively.

TABLE 1 Baseline Characteristics of Discovery Phase Patients
NCA(n ¼ 116)
NOCA(n ¼ 276)
SA(n ¼ 63)
UA(n ¼ 307)
AMI(n ¼ 324) p Value for Trend
Age, yrs 57.7 � 8.4 61.6 � 8.3 64.6 � 8.2 65.0 � 9.2 63.6 � 10.8 <0.001
Female 46.6 49.3 36.5 30.6 21.2 <0.001
LVEF 60.1 � 9.1 62.5 � 8.9 62.4 � 6.9 61.7 � 6.8 55.4 � 9.2 <0.001
Body mass index, kg/m2 24.6 � 3.9 24.8 � 3.8 25.4 � 3.4 24.7 � 3.1 24.3 � 3.3 0.196
Blood pressure, mm Hg
Systolic 129.6 � 18.2 134.5 � 16.8 141.6 � 18.7 140.0 � 17.4 133.6 � 20.7 <0.001
Diastolic 81.5 � 11.0 82.9 � 11.0 82.8 � 9.1 81.5 � 10.2 83.0 � 14.6 0.171
Heart rate, beats/min 75.2 � 10.8 73.1 � 10.6 71.2 � 8.8 71.3 � 9.5 73.9 � 13.5 0.002
Comorbidity
Hypertension 55.2 69.2 85.7 76.9 71.1 <0.001
Diabetes mellitus 12.1 16.7 23.8 29.3 29.8 <0.001
Current smoker 19.8 18.5 15.9 28.0 33.9 <0.001
Drinking history* 6.0 5.8 4.8 4.9 4.9 0.974
Medication
Aspirin 83.3 88.9 100.0 100.0 100.0 <0.001
Clopidogrel 66.7 81.5 100.0 100.0 100.0 <0.001
Beta-blocker 83.3 77.8 64.3 70.3 84.9 <0.001
Nitrates 38.9 37.0 57.1 70.9 62.3 <0.001
Statins 72.2 85.2 92.9 97.6 97.0 <0.001
Calcium-channel blocker 16.7 22.2 32.1 50.3 21.6 <0.001
ACEI 61.1 33.3 50.0 57.0 77.4 <0.001
ARB 16.7 40.7 39.3 24.8 20.1 <0.001
Heparin 16.7 11.1 3.6 27.9 74.4 <0.001
Diuretic agent 38.9 14.8 7.1 6.1 33.7 <0.001
Digitalis 27.8 3.7 0.0 0.6 5.5 <0.001
GP IIb/IIIa antagonists 0.0 3.7 0.0 23.0 54.3 <0.001
Hypoglycemic drugs 16.7 22.2 21.4 20.0 26.6 <0.001
PPI 55.6 92.6 78.6 93.9 97.5 <0.001
Trimetazidine 22.2 25.9 35.7 38.8 42.2 <0.001
Laboratory data
HbA1C, % 6.0 � 0.7 6.2 � 0.9 6.4 � 1.0 6.4 � 1.1 6.4 � 1.3 <0.001
Glucose, mmol/l 5.7 � 1.8 5.7 � 1.7 5.8 � 1.4 5.9 � 1.9 6.6 � 2.6 <0.001
TG, mmol/l 2.0 � 1.6 2.0 � 1.4 1.8 � 1.0 1.9 � 1.5 1.7 � 1.1 0.001
TC, mmol/l 4.5 � 1.2 4.7 � 1.1 4.4 � 1.1 4.3 � 1.1 4.2 � 1.0 <0.001
HDL-C, mmol/l 1.2 � 0.3 1.2 � 0.3 1.1 � 0.3 1.1 � 0.3 1.0 � 0.3 <0.001
LDL-C, mmol/l 2.6 � 0.7 2.7 � 0.8 2.6 � 0.9 2.6 � 0.3 2.7 � 1.0 0.331
BUN, mmol/l 5.6 � 1.6 5.7 � 1.7 5.6 � 1.5 5.8 � 1.6 5.7 � 1.8 0.965
CR, mmol/l 74.4 � 16.9 76.5 � 19.6 83.0 � 20.1 78.2 � 18.7 80.5 � 23.4 0.079
Values are mean � SD or %. *Patients with $50 g alcohol per day.
ACEI ¼ angiotensin-converting enzyme inhibitor; AMI ¼ acute myocardial infarction; ARB ¼ angiotensin receptor blocker; BUN ¼ blood urea nitrogen; CR ¼ creatinine;GP ¼ glycoprotein; HbA1C ¼ glycosylated hemoglobin; HDL-C ¼ high-density lipoprotein cholesterol; LDL-C¼ low-density lipoprotein cholesterol; LVEF ¼ left ventricularejection fraction; NCA ¼ normal coronary artery; NOCA ¼ nonobstructive coronary atherosclerosis; PPI ¼ proton pump inhibitor; SA ¼ stable angina; TC ¼ total cholesterol;TG ¼ triglyceride; UA ¼ unstable angina.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1285
CORRELATION NETWORK OF DIFFERENTIAL
METABOLITES IN CAD PLASMA. By 12 comprehen-sive cross-comparisons of different CAD groups, 89differential metabolites were identified, from which44 were confirmed using reference compounds. Theconcentrations of these 89 metabolites in normal ar-teries and the CAD groups are summarized in OnlineTables 6 to 8. Figure 3A is a heat map showing theaverage normalized quantities of the 89 differentialmetabolites in normal arteries and the CADgroups. Among them, 27 metabolites were elevated;
62 metabolites decreased in order according to thefollowing groups: NCA, NOCA, SA, UA, and AMI.
To investigate the latent relationships of the 89differential metabolites, the Pearson correlation co-efficients between the metabolites were calculated onthe basis of the average normalized quantities ofmetabolites (Online Figure 5). Highly correlated me-tabolites with jrj > 0.9 are connected with lines in thenetwork for a view of the disturbed metabolism ofCAD (Figure 3B). Most metabolites in tricarboxylicacid cycle and phospholipids were down-regulated in

FIGURE 2 OPLS-DA Score Plots and Disturbed Metabolic Pathways
15
10
5
0
-5
6 4 2 0 -2 -4 -6 -8 -10 0 50 100 150 200 250 300 350
10
40015
5
0
-5
050
100150
200250
300350
400 6
42
0-2
-4-6
-8-10 Num
t[1]
to[1]NOCA vs. NCA
15
10
5
0
-5
10 8 6 4 2 0 -2 -4 0 50 100 150 200 250 300 350
050
100150
200250
300
350 10
8
6
42
0-2
-4
10
15
5
0
-5
t[1]Num
to[1]SA vs. NOCA
050
100150
200250
300350
400 8
6
4
2
0
-2
10
15
5
0
-5
-10
200 50 100 150 200 250 300 350 400
8 6 4 2 0 -2
20
10
5
0
-5
-10
15
t[1]Num
to[1]UA vs. SA
0100
200300
400
500
6003
21
0
-2-3
-4-5
-1
4
4
6
2
0
-4
-6
8
-2
10100 0 100 200 300 400 500 600
4 3 2 0 -1 -2 -4 -5-3110
6
4
0
-2
-4
8
2
-6
t[1] Num
to[1]AMI vs. UA
Glycerophospholipid metabolism
Linoleic acid metabolismPurine metabolism
Sphingolipid metabolism
Glycerophospholipid metabolism
Sphingolipid metabolism
Valine, leucine and isoleucine metabolism
Primary bile acid biosynthesisArginine and proline metabolism
Glycerophospholipid metabolism Glycerophospholipid metabolism
Glycine, serine and threonine metabolism
Arachidonic acid metabolism
Arginine and proline metabolism
Alanine, asparatate and glutamate metabolism
Linoleic acid metabolismSphingolipid metabolism
Primary bile acid biosynthesisArginine and proline metabolism
NOCA vs. NCA SA vs. NOCA
UA vs. SA AMI vs. UA
0.00 0.05 0.10 0.15Pathway Impact
5.0
4.5
4.0
3.5
3.0
2.5
2.0
-log
(p)
6
5
4
3
2
1
-log
(p)
0.00 0.02 0.04 0.05Pathway Impact
0.01 0.03
3.5
3.0
2.5
2.0
1.5
1.0
-log
(p)
0.00 0.10 0.20 0.25Pathway Impact
0.05 0.15 0.00 0.10Pathway Impact
0.05 0.15
7
6
5
4
3
2
-log
(p)
1
A B
C D
E F
G H
The orthogonal projection to latent structure-discriminant analysis (OPLS-DA) score plots compared (A) NOCA to NCA, (B) SA to NOCA, (C) UA
to SA, and (D) AMI to UA. The disturbed metabolic pathways showed various metabolism changes when comparing (E) NOCA to NCA, (F) SA to
NOCA, (G) UA to SA, and (H) AMI to UA. Abbreviations are as in Figure 1.
Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1286

FIGURE 3 Differential Metabolites in CAD Types and Metabolite Correlation Network
LysoPC 16:1Glycodeoxycholic acidLysoPC 18:2LysoPC 16:0PalmitoylethanolamideCholine5-Hydroxy tryptamineThreonineAcetylcarnitineLysoPC 14:0Tryptophan2α-Methyl-5α-androstane-3, 17-dioneTrimethylamine3-OctanoneDecenyl acetateFumaric acidMG 18:0/0:0/0:0PhosphatidylcholineCerP d18:0/16:0N-MethylisoleucineLysoPE 22:6Undecan-3-olEthylchenodeoxycholic acidLysoPE 20:4LysoPE 22:5Succinic acidValineLysoPC 20:3Indole-3-ethanolLysoPC 24:0LysoPC 22:5LysoPC 22:6LysoPE 16:0LysoPE 18:0LysoPE 20:13-Methyl-2-butene-1-thiolPE 12:0/22:6LysoPC 20:5PG 13:0/14:0LysoPE 18:3PG 15:0/14:0GlycerophosphocholineLysoPE 22:1PE 20:0/0:0PE 18:0/0:0PI 18:2/0:02-Nonynoic acidLysoPC 20:4PE 21:0/0:0Octadecadienoic acidCerP d18:1/8:0LysoPC 10:0LysoPC 18:0LysoPE 18:1PI 18:3/0:02-OctenoylcarnitinePhosphocholineDocosahexaenoic acidLysoPC 18:1Glycocholic acidγ-Aminobutyric acid
MethylglutarylcarnitineCarnitine1-MethyladenosineDicyclohexylamine
Paraxanthine2-Hydroxylauric acidCarnosineCreatineHuppuric acidPI 20:4/0:0N-Phenylacetyl-L-glutaminePhytosphingosineTrimethylamine N-oxideLysoPC 18:4LysoPC 18:3LysoPE 18:2IsobutyrylcarnitineMalic acidAspartic acidEicosatertraenoic acidEicosatrienoic acidIsoleucylprolinePropionylcarnitineSphinganineTrp Arg LeuLysoPC 20:1
Glutarylcarnitine
0 0.98 1.11
NCA
NOCA
SA UA AMI
NCA
NOCA
SA UA AMI
Bile acids
Amino acids
Short chain acylcarnitines
TCA cycle metabolites
Phospholipids
A B
In the heat map of the 89 differential metabolites in different coronary artery disease (CAD) stages (A), the colors changing from blue to orange indicate
more metabolites. In the correlation network of metabolites with |r| > 0.9 (B), orange plots indicate up-regulated metabolites and blue plots indicate
down-regulated metabolites in CAD. Arg ¼ arginine; CerP ¼ ceramide 1-phosphate; Leu ¼ leucine; LysoPC ¼ lysophosphatidylcholine; LysoPE ¼ lyso-
phosphatidylethanolamine; MG ¼ monoradylglycerol; PG ¼ glycerophosphoglycerol; PI ¼ phosphatidylinositol; TCA ¼ tricarboxylic acid; Trp ¼ tryptophan;
other abbreviations as in Figure 1.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1287
CAD groups and had highly correlated coefficients.Levels of some correlated amino acids were up-regulated. Short-chain acylcarnitines, in the centerof the network, bridged the altered metabolites.Metabolites of bile acids decreased. The disturbedmetabolic pathways are detailed in Online Figure 6 onthe basis of the KEGG Pathway Database.DIFFERENTIAL DIAGNOSIS OF METABOLIC BIOMARKERS.
Accurate diagnosis of the stage of CAD is fundamentalfor personalized treatment of coronary disease. Fordifferential diagnosis, the criteria of metabolomics-based biomarkers are VIP >1.5 and adjusted pvalue <0.05. As summarized in Table 2, there were 10specific metabolic biomarkers for distinguishingNOCA from NCA, 8 for SA versus NOCA, 10 for UAversus SA, and 9 for AMI versus UA; additionalmetabolomics-based biomarker comparisons are pro-vided in Online Table 5.
The ROC presentations, on the basis of the logisticregression of each biomarker panel from the discovery
phase, appear in Figure 4; the areas under the curve(AUC), sensitivity, and specificity are 0.952, 94.2%,and 80.7% for NOCA versus NCA (n ¼ 392) (Figure 4A);0.993, 96.4%, and 95.6% for SA versus NOCA (n ¼ 339)(Figure 4B); 0.990, 97.4%, and 91.1% for UA versusSA (n ¼ 370) (Figure 4C); and 0.992, 94.5%, and 95.3%for AMI versus UA (n ¼ 631) (Figure 4D), respectively.For additional cross-comparisons, AUCs ranged from0.938 to 0.996, sensitivities from 83.3% to 99.1%, andspecificities from 90.9% to 97.2% (Online Figure 7).ROC curves with AUC, sensitivity, and specificityvalues for the 12 cross-comparisons in the test phasesand 3-center external validation sets are shown inOnline Figure 8. Logistic regression analysis of diag-nostic biomarkers in all cross-comparisons appears inOnline Table 9.
On the basis of the highest prediction sensitivityand specificity of the ROC in the discovery phase, theoptimal cut-off values were 0.635 for NOCA versusNCA, 0.205 for SA versus NOCA, 0.692 for UA versus

TABLE 2 Statistical Analysis of Diagnostic Biomarkers: Discovery Phase
MetabolitesRetentionTime (min)
Mass-to-ChargeRatio VIP Value Fold Change* p Value† Adjusted p Value‡ Adjusted p Value§
NOCA vs. NCA
LysoPC 16:0 7.094 496.346 2.049 0.802 <0.0001 <0.001 <0.001
LysoPC 18:4 7.086 516.316 2.036 0.691 <0.0001 <0.001 <0.001
LysoPC 18:2 6.727 520.344 2.013 0.674 <0.0001 <0.001 <0.001
LysoPC 18:0 8.288 524.371 1.844 0.782 <0.0001 <0.001 <0.001
LysoPE 18:2 7.088 478.328 1.623 0.740 <0.0001 <0.001 <0.001
LysoPC 18:3 6.279 518.323 1.617 0.664 <0.0001 <0.001 <0.001
LysoPC 18:1 7.349 522.356 1.576 0.665 <0.0001 <0.001 <0.001
Palmitoylethanolamide 5.001 300.288 1.561 0.647 <0.0001 <0.001 0.004
LysoPC 16:1 6.425 494.324 1.548 0.725 <0.0001 <0.001 <0.001
Phytosphingosine 5.132 318.302 1.520 1.362 <0.0001 <0.001 0.005
SA vs. NOCA
LysoPC 16:0 7.094 496.346 2.068 0.729 <0.0001 <0.001 <0.001
Palmitoylethanolamide 5.001 300.288 1.991 0.733 <0.0001 <0.001 <0.001
PI 20:4/0:0 7.416 621.372 1.927 1.474 <0.0001 <0.001 <0.001
LysoPC 18:2 6.737 520.343 1.712 0.764 <0.0001 <0.001 <0.001
Phosphocholine 0.689 184.073 1.629 0.677 <0.0001 <0.001 <0.001
Phosphatidylcholine 8.081 326.168 1.593 0.472 <0.0001 <0.001 <0.001
Ethylchenodeoxycholic acid 4.576 443.315 1.575 0.611 <0.0001 <0.001 <0.001
Phytosphingosine 5.654 318.300 1.508 1.540 <0.0001 <0.001 <0.001
UA vs. SA
Creatine 0.972 132.103 2.166 1.532 <0.0001 <0.001 <0.001
2-hydroxylauric acid 6.352 217.179 2.070 1.524 <0.0001 0.002 0.005
Tryptophan 4.106 205.096 2.142 1.869 <0.0001 <0.001 <0.001
Phosphocholine 0.689 184.073 1.547 0.806 <0.0001 <0.001 <0.001
Isobutyrylcarnitine 1.533 232.154 1.710 1.331 <0.0001 0.002 0.002
LysoPC 16:0 7.094 496.346 1.697 0.751 <0.0001 <0.001 <0.001
Propionylcarnitine 0.978 218.138 1.602 1.165 <0.0001 <0.001 <0.001
Acetylcarnitine 0.733 204.124 1.594 1.484 <0.0001 <0.001 <0.001
Aspartic acid 0.967 134.107 1.679 0.863 <0.0001 <0.001 <0.001
LysoPC 18:1 7.349 522.356 1.620 0.771 <0.0001 0.003 0.006
AMI vs. UA
N-phenylacetyl-L-glutamine 2.232 265.118 2.451 1.314 <0.0001 <0.001 <0.001
LysoPC 20:3 7.081 546.355 2.227 0.845 <0.0001 <0.001 <0.001
Trp Arg Leu 1.985 474.284 1.955 1.456 <0.0001 <0.001 <0.001
Sphinganine 7.687 302.148 1.701 1.391 <0.0001 <0.001 <0.001
LysoPC 18:2 6.737 520.343 1.684 0.941 <0.0001 0.002 0.002
LysoPC 14:0 6.151 468.308 1.665 0.897 <0.0001 0.002 0.003
Eicosatetraenoic acid 9.098 305.248 1.577 1.259 <0.0001 <0.001 <0.001
Glycocholic acid 4.636 466.316 1.563 0.749 <0.0001 <0.001 <0.001
Eicosatrienoic acid 9.601 307.261 1.537 1.282 <0.0001 <0.001 <0.001
*Fold change with a value >1 indicates a relatively higher concentration present in the patients with severe coronary artery disease in each cross-comparison. †From Studentt test. ‡Adjusted by Bonferroni correction across multiple comparisons within each metabolite. §Adjusted by false discovery rate method across the 89 metabolites within eachcomparison.
Arg ¼ arginine; Leu ¼ leucine; LysoPC ¼ lysophosphatidylcholine; LysoPE ¼ lysophosphatidylethanolamine; PI ¼ phosphatidylinositol; Trp ¼ tryptophan; VIP ¼ variableimportance in the projection; other abbreviations as in Table 1.
Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1288
SA, and 0.475 for AMI versus UA. The cut-off valueswere then used to predict the different stages of CADin the test phase and external sets. Predictive valuewas 95.0% for NOCA versus NCA in the test phase and91.5% in the 3-centered external validation sets(Figure 4E); 94.5% for SA versus NOCA in the testphase and 89.7% in the validation sets (Figure 4F);91.8% for UA versus SA in the test phase and 96.4% in
the validation sets (Figure 4G); and 96.0% forAMI versus UA in the test phase and 85.3% in thevalidation sets (Figure 4H). Predictive values foradditional comparisons ranged from 89.2% to 95.0%in the test phase and from 86.8% to 94.5% in the3-centered external validation sets (Online Figure 9).Odds ratios of the 12 biomarker panels after adjust-ment for possible confounding comorbidities, and

FIGURE 4 Diagnostic Outcomes and Prediction Accuracies
1.0
0.8
0.6
0.4
0.2
0.00.0 0.2 0.4 0.6 0.8 1.0
1-Specificity
Sens
itivi
ty
1.0
0.8
0.6
0.4
0.2
0.00.0 0.2 0.4 0.6 0.8 1.0
1-Specificity
Sens
itivi
ty
1.0
0.8
0.6
0.4
0.2
0.00.0 0.2 0.4 0.6 0.8 1.0
1-Specificity
Sens
itivi
ty
1.0
0.8
0.6
0.4
0.2
0.00.0 0.2 0.4 0.6 0.8 1.0
1-Specificity
Sens
itivi
ty
NOCA vs. NCA SA vs. NOCA
UA vs. SA AMI vs. UA
AUC = 0.952CI: 0.928-0.976Sensitivity: 94.2%Specificity: 80.7%
AUC = 0.993CI: 0.988-0.999Sensitivity: 96.4%Specificity: 95.6%
AUC = 0.990CI: 0.980-1.000Sensitivity: 97.4%Specificity: 91.1%
AUC = 0.992CI: 0.987-0.997Sensitivity: 94.5%Specificity: 95.3%
1.0
0.5
0.0
1.0
0.5
0.0
1.0
0.5
0.0
1.0
0.5
0.0
NCA(n = 119)
NOCA(n = 220)
Test phase
NCA(n = 32)
NOCA(n = 11)
Nantong
NCA(n = 32)
NOCA(n = 14)
Yangzhou
NCA(n = 31)
NOCA(n = 45)
Nanjing
External validation sets
NOCA(n = 220)
SA(n = 72)
Test phase
NOCA(n = 11)
SA(n = 7)
Nantong
NOCA(n = 14)
SA(n = 7)
Yangzhou
NOCA(n = 45)
SA(n = 14)
Nanjing
External validation sets
SA(n = 72)
UA(n = 280)
Test phase
SA(n = 7)
UA(n = 9)
Nantong
SA(n = 7)
UA(n = 7)
Yangzhou
SA(n = 14)
UA(n = 41)
Nanjing
External validation sets
UA(n = 280)
AMI(n = 242)
Test phase
UA(n = 9)
AMI(n = 12)
Nantong
UA(n = 7)
AMI(n = 8)
Yangzhou
UA(n = 41)
AMI(n = 35)
Nanjing
External validation sets
Cut off value=0.635
Cut off value=0.205
Cut off value=0.692
Cut off value=0.475
NOCA vs. NCA SA vs. NOCA
UA vs. SA AMI vs. UA
A B
C D
E F
G H
The diagnostic outcomes in the discovery phase are shown via the receiver-operating characteristic (ROC) curves for comparison between (A)
NOCA versus NCA, (B) SA versus NOCA, (C) UA versus SA, and (D) AMI versus UA. The prediction accuracies by the biomarkers in test phase and
validation sets were compared between (E) NOCA versus NCA, (F) SA versus NOCA, (G) UA versus SA, and (H) AMI versus UA. AUC ¼ area under
the curve; CI ¼ confidence interval; other abbreviations as in Figure 1.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1289

Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1290
concomitant treatments in all cross-comparisons areprovided in Online Table 10. The 12 CAD-associatedplasma metabolite signatures remained significant(adjusted p value <0.05) after adjustment forcomorbidities and concomitant treatments.
DISCUSSION
This work described a comprehensive metabolomicevaluation for 2,324 patients who underwent coro-nary angiography in 4 independent centers. Meta-bolic phenotypes revealed significant patterndifferences between patients with CAD and no coro-nary disease and within CAD types. With 89 signifi-cantly regulated metabolites in plasma samples, thechanges suggested that CAD may involve a universalmetabolic disturbance. Phospholipid catabolism andthe tricarboxylic acid cycle decreased, amino acidmetabolism and short-chain acylcarnitines increased,and primary bile acid biosynthesis declined duringCAD progression. Combinations of metabolic bio-markers offered excellent predictive values for dis-tinguishing each CAD type from normal coronaryarteries and from one another (Central Illustration).
The group without coronary disease had 335(14.4%) participants who experienced angina-likechest pain and discomfort but had a normal arteryconfirmed by angiography. Comparison with thisgroup made possible distinctions in patients withconfusing symptoms. The extent of coronary arteryblockage revealed positive correlations with theseverity of CAD. All the NOCA patients had <50%stenosis. As calculated, 63.2% of SA, 61.8% of UA, and71.4% of AMI patients showed blockage $70%. Incontrast, only a small portion of patients with UA orAMI had a blockage <50%.
The exact cause of NOCA, which produces anginaand AMI, remains largely unknown. Compared withpatients with normal coronary arteries, patients withNOCA had down-regulated lysophosphatidylcholines,lysophosphatidylethanolamine 18:2, and phosphati-dylethanolamine and up-regulated phytosphingo-sine. As shown in Online Figure 10, a large portion oflysophosphatidylcholines and lysophosphatidyletha-nolamines in plasma was generated from phosphati-dylcholines and phosphatidylethanolamines by theactivity of lecithin cholesterol acyltransferase. Lowlecithin cholesterol acyltransferase activity has beenlinked to CAD (16,17). Elevated levels of sphingolipidsare characteristic of obesity and cardiovascularrisks (18).
Plaques from atherosclerosis grow to inducesignificant stenosis in a coronary artery. Comparedwith the NOCA, the SA group had down-regulation
of phosphocholine, phosphatidylethanolamine,phosphatidylcholine, ethylchenodeoxycholic acid,lysophosphatidylcholine 16:0, and lysophosphati-dylcholine 18:2, and up-regulation of phytosphingo-sine and phosphatidylinositol 20:4/0:0. Usually,phosphatidylcholine is metabolized by intestinalmicrobiota to produce proatherogenic species,choline, and trimethylamine oxide. The decrease ofphosphatidylcholine has implications for CAD (19).Ethylchenodeoxycholic acid activates the farnesoidX receptor, an endogenous sensor for bile acids.The inverse correlation between it and CAD has beenreported (20). Phosphatidylinositol, an activator ofintracellular Ca2þ, was up-regulated in SA. Increasedphosphatidylinositol 20:4/0:0 affirmed the seriousvascular calcification in patients with SA (21).
When coronary arteries are severely narrowedby atherosclerosis or when plaques rupture and pro-duce clots, angina pectoris becomes unstable. Thetransition from coronary stability to instability is lesswell understood. Compared with stable angina, un-stable angina up-regulates creatine, 2-hydroxylauricacid, tryptophan, isobutyrylcarnitine, propio-nylcarnitine, and acetylcarnitine, and down-regulatesaspartic acid, phosphocholine, lysophosphatidylcho-line 16:0, and lysophosphatidylcholine 18:1. Theincreased creatine corresponds to a decrease in theactivity of the creatine kinase system. The creatinekinase system protects the cardiovascular system fromischemia and increases contractility (22). 2-hydrox-ylauric acid is a medium-chain fatty acid associatedwith fatty acid metabolic disorders during plaquerupture (23). Tryptophan is closely associated withimmune system activation and inflammation (24).With the detection of tryptophan, we assumed thatthe levels of inflammation and immune activityincreased in UA compared with SA. Elevated levelsof short-chain acylcarnitines suggest activated fattyacid metabolism in UA (25). Reduced aspartic acidcorresponds to the high risk of myocardial damagein UA (26). Phosphocholine was reduced more in UAthan SA.
Compared with UA, AMI up-regulated N-phenyl-acetyl-L-glutamine, sphinganine, eicosatertraenoicacid, eicosatrienoic acid, and tryptophan-arginine-leucine, and reduced glycocholic acid, lysophospha-tidylcholine 14:0, lysophosphatidylcholine 18:2, andlysophosphatidylcholine 20:3. The elevation of N-phenylacetyl-L-glutamine suggests a perturbed phe-nylalanine metabolism during the transition fromUA to AMI (27). Up-regulation of sphinganine, anintermediate of sphingoid base biosynthesis (28),suggests that sphingolipid metabolism is hampered inAMI. Studies have linked elevated sphingolipids to

CENTRAL ILLUSTRATION Metabolomic Characterization and Differential Diagnosis of CAD Types
Fan, Y. et al. J Am Coll Cardiol. 2016;68(12):1281–93.
Patients suspected with coronary artery disease (CAD) underwent coronary angiography and were divided into appropriate groups: normal coronary artery (NCA),
nonobstructive coronary atherosclerosis (NOCA), stable angina (SA), unstable angina (UA), and acute myocardial infarction (AMI). The metabolomic profiles were
determined by liquid chromatography–mass spectrometry (LC-MS). Differential metabolites were identified by multivariate statistics. The specific metabolic pathways
were characterized using significant CAD (NCA/NOCA) versus nonsignificant CAD (SA/UA/AMI) as an example. The significantly changed metabolites were used for
differential diagnosis. Orthogonal projection to latent structure-discriminant analysis (OPLS-DA) score plot showed clear discrimination between significant versus
nonsignificant CAD. Receiver-operating characteristic (ROC) analysis provided area under the curve (AUC) of 0.938 with sensitivity of 83.3% and specificity of 91.6% in
the discovery phase, and offered a predictive value of 93.0% in the test phase and 100.0% in the 3-centered external validation sets.
J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1291
cardiovascular diseases and obesity, confirming ourfindings. The presence of eicosatertraenoic acid andeicosatrienoic acid in greater proportions reflects theinflammation experienced in AMI (29). Glycocholicacid, crucial in bile acid synthesis and cholesterolmetabolism (30), was down-regulated in patients withAMI because the metabolism of cholesterol and phos-pholipids was inhibited (31). Tryptophan-arginine-leucine, an ingredient to generate amino acids, was athigh levels in these patients. Our results proved that
activated amino acid biosynthesis is an indicator forAMI (32).
The potential applications in clinical diagnosisincluded: 1) differential diagnosis of significant versusnonsignificant CAD; 2) if CAD is not significant, a dif-ferential diagnosis of NOCA versus NCA is required;3) if CAD is significant, a differential diagnosis of ACSversus SA is required; and 4) if not SA, a differentialdiagnosis of AMI versus UA is required. The sensi-tivities, specificities, and predictive values of the

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE:
Chromatographic analysis of human plasma can
identify metabolic abnormalities of phospholipid
catabolism; amino acid metabolism; and synthesis of
short-chain acylcarnitines, tricarboxylic acid cycle
byproducts, and primary bile acids that are associated
with various clinical presentations of CAD.
TRANSLATIONAL OUTLOOK: Additional studies
are needed to correlate the effects of therapeutic
interventions for patients with different forms of CAD
with plasma levels of metabolic biomarkers.
Fan et al. J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6
Metabolomics of Coronary Artery Disease S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3
1292
metabolic biomarkers we discovered were muchhigher than reported with noninvasive methods suchas coronary computed tomographic angiography (33).These biomarkers separate individuals who maybenefit from additional testing with invasive angiog-raphy from individuals who will not.
STUDY LIMITATIONS. First, the use of this techniquecould exclude other classes of lipids and amino acids.A dual analytical platform, such as gas chromatog-raphy mass spectrometry together with liquid chro-matography–mass spectrometry, is recommended infuture studies. Second, because of lacking a central-ized core laboratory, it is possible there were site-to-site and observer-to-observer variations in theadjudication of coronary stenosis. Third, our studypopulation consisted of middle-aged to elderly Chi-nese patients. In future studies, the scope could bebroadened to include other ethnicities within Asiaand other races such as Caucasians and Africans.Younger age groups suspected of or confirmed withCAD could be considered.
CONCLUSIONS
We reported a comprehensive metabolomic evalua-tion for identifying clinically relevant perturbationsin circulating metabolites in CAD. This evaluationimproved the understanding of CAD pathogenesisand facilitates target screening for therapeutic inter-vention. Novel biomarkers predict and differentiatebetween CAD types; such differentiation may reduceunnecessary invasive coronary angiography, enhancepredictive value, and complement current diagnosticmethods.
ACKNOWLEDGMENT The authors thank Sally Kozlikfrom the University of Chicago for editing ourmanuscript.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Lian-Wen Qi, State Key Laboratory of Natural Medi-cines, China Pharmaceutical University, Departmentof Pharmacognosy, 24# Tongjia Lane, ZhongyangRoad, Nanjing, Jiangsu 210009, China. E-mail: [email protected]. OR Dr. Wei Zhu, the First Affiliated Hos-pital of Nanjing Medical University, Department ofOncology, 300# Guangzhou Road, Nanjing, Jiangsu210029, China. E-mail: [email protected]. OR Dr.Ping Li, State Key Laboratory of Natural Medicines,China Pharmaceutical University, Department ofPharmacognosy, 639# Longmian Road, Nanjing,Jiangsu 210009, China. E-mail: [email protected].
RE F E RENCE S
1. Naghavi M, Wang H, Lozano R, et al. Global,regional, and national age-sex specific all-causeand cause-specific mortality for 240 causes ofdeath, 1990–2013: a systematic analysis for theGlobal Burden of Disease Study 2013. Lancet2015;385:117–71.
2. Epstein SE, Zhou YF, Zhu J. Infection andatherosclerosis emerging mechanistic paradigms.Circulation 1999;100:e20–8.
3. De Backer GG. The global burden of coronaryheart disease. Medicographia 2009;31:343–8.
4. Libby P, Ridker PM, Hansson GK. Progress andchallenges in translating the biology of athero-sclerosis. Nature 2011;473:317–25.
5. Bassand J-P, Hamm CW, Ardissino D, et al.Guidelines for the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes.Eur Heart J 2007;28:1598–660.
6. Lindahl B, Toss H, Siegbahn A, Venge P,Wallentin L. Markers of myocardial damage and
inflammation in relation to long-term mortality inunstable coronary artery disease. N Engl J Med2000;343:1139–47.
7. Hambrecht R, Wolf A, Gielen S, et al. Effect ofexercise on coronary endothelial function in pa-tients with coronary artery disease. N Engl J Med2000;342:454–60.
8. Achenbach S, Daniel WG. Noninvasive coronaryangiography—an acceptable alternative? N Engl JMed 2001;345:1909–10.
9. Patel MR, Peterson ED, Dai D, et al. Low diag-nostic yield of elective coronary angiography.N Engl J Med 2010;362:886–95.
10. Amsterdam EA, Wenger NK, Brindis RG, et al.2014 AHA/ACC guideline for the management ofpatients with non–ST-elevation acute coronarysyndromes: a report of the American College ofCardiology/American Heart Association Task Forceon Practice Guidelines. J Am Coll Cardiol 2014;64:e139–228.
11. Sabatine MS, Liu E, Morrow DA, et al.Metabolomic identification of novel biomarkers ofmyocardial ischemia. Circulation 2005;112:3868–75.
12. Cheng M-L, Wang C-H, Shiao M-S, et al. Meta-bolic disturbances identified in plasma are associ-ated with outcomes in patients with heart failure:diagnostic and prognostic value of metabolomics.J Am Coll Cardiol 2015;65:1509–20.
13. Sreekumar A, Poisson LM, Rajendiran TM, et al.Metabolomic profiles delineate potential role forsarcosine in prostate cancer progression. Nature2009;457:910–4.
14. Huang Q, Tan Y, Yin P, et al. Metabolic char-acterization of hepatocellular carcinoma usingnontargeted tissue metabolomics. Cancer Res2013;73:4992–5002.
15. Gika HG, Theodoridis GA, Wingate JE,Wilson ID. Within-day reproducibility of an HPLC-MS-based method for metabonomic analysis:

J A C C V O L . 6 8 , N O . 1 2 , 2 0 1 6 Fan et al.S E P T E M B E R 2 0 , 2 0 1 6 : 1 2 8 1 – 9 3 Metabolomics of Coronary Artery Disease
1293
application to human urine. J Proteome Res 2007;6:3291–303.
16. Ganna A, Salihovic S, Sundström J, et al.Large-scale metabolomic profiling identifies novelbiomarkers for incident coronary heart disease.PLoS Genet 2014;10:e1004801.
17. Stegemann C, Pechlaner R, Willeit P, et al.Lipidomics profiling and risk of cardiovasculardisease in the prospective population-based Bru-neck study. Circulation 2014;129:1821–31.
18. Wymann MP, Schneiter R. Lipid signalling indisease. Nat Rev Mol Cell Bio 2008;9:162–76.
19. Tang WHW, Wang Z, Levison BS, et al. Intes-tinal microbial metabolism of phosphatidylcholineand cardiovascular risk. N Engl J Med 2013;368:1575–84.
20. Lin Z, Pan X, Wu F, et al. Fibroblast growthfactor 21 prevents atherosclerosis by suppressionof hepatic sterol regulatory element-binding pro-tein-2 and induction of adiponectin in mice. Cir-culation 2015;131:1861–71.
21. Masuda M, Miyazaki-Anzai S, Keenan AL, et al.Saturated phosphatidic acids mediate saturatedfatty acid–induced vascular calcification andlipotoxicity. J Clin Invest 2015;125:4544–58.
22. Bottomley PA, Panjrath GS, Lai S, et al.Metabolic rates of ATP transfer through creatinekinase (CK Flux) predict clinical heart failureevents and death. Sci Transl Med 2013;5:215re3.
23. Rizos EC, Ntzani EE, Bika E, et al. Associationbetween omega-3 fatty acid supplementation and
risk of major cardiovascular disease events: asystematic review and meta-analysis. J Am MedAssoc 2012;308:1024–33.
24. Mellor AL, Sivakumar J, Chandler P, et al.Prevention of T cell–driven complement activationand inflammation by tryptophan catabolism dur-ing pregnancy. Nat Immunol 2001;2:64–8.
25. Koves TR, Ussher JR, Noland RC, et al. Mito-chondrial overload and incomplete fatty acidoxidation contribute to skeletal muscle insulinresistance. Cell Metab 2008;7:45–56.
26. Lazo M, Rubin J, Clark JM, et al. The associa-tion of liver enzymes with biomarkers of subclini-cal myocardial damage and structural heartdisease. J Hepatol 2015;62:841–7.
27. Shah SH, Sun JL, Stevens RD, et al. Baselinemetabolomic profiles predict cardiovascularevents in patients at risk for coronary artery dis-ease. Am Heart J 2012;163:844–50.
28. Knapp M, Baranowski M, Lisowska A,Musiał W. Decreased free sphingoid base concen-tration in the plasma of patients with chronicsystolic heart failure. Adv Med Sci 2012;57:100–5.
29. Akasaka H, Ruan KH. Identification of the two-phase mechanism of endogenour omega-6 fattyacid, arachidonic acid, regulating vascular inflam-mation by targeting cyclooxygenase-2 andmicrosomal prostaglandin E2 synthase-1. Posterpresented at: 65th Annual American College ofCardiology Scientific Sessions; April 3, 2016;Chicago, Illinois.
30. Sayin SI, Wahlström A, Felin J, et al. Gutmicrobiota regulates bile acid metabolism byreducing the levels of tauro-beta-muricholic acid,a naturally occurring FXR antagonist. Cell Metab2013;17:225–35.
31. Chapman MJ, Ginsberg HN, Amarenco P,et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients athigh risk of cardiovascular disease: evidence andguidance for management. Eur Heart J 2011;32:1345–61.
32. Lewis GD, Wei RU, Liu E, et al. Metaboliteprofiling of blood from individuals undergoingplanned myocardial infarction reveals earlymarkers of myocardial injury. J Clin Invest 2008;118:3503–12.
33. Achenbach S, Giesler T, Ropers D, et al.Detection of coronary artery stenoses bycontrast-enhanced, retrospectively electrocardio-graphically-gated, multislice spiral computed to-mography. Circulation 2001;103:2535–8.
KEY WORDS angina, diagnosticbiomarkers, disturbed metabolic pathways,metabolite, plasma
APPENDIX For a supplemental Methodssection as well as figures and tables, please seethe online version of this article.