Comprehensive Echocardiographic Evaluation of Cardiac ...€¦ · cardiac function and pulmonary...
203
Comprehensive Echocardiographic Evaluation of Cardiac Function and Pulmonary Hemodynamics in the Newly Born during Health and Disease by Amish Jain A thesis submitted in conformity with the requirements For the degree of Doctor of Philosophy Graduate Department of Physiology University of Toronto © Copyright by Amish Jain 2017
Transcript of Comprehensive Echocardiographic Evaluation of Cardiac ...€¦ · cardiac function and pulmonary...

Comprehensive Echocardiographic Evaluation of Cardiac Function and Pulmonary
Hemodynamics in the Newly Born during Health and Disease
by
Amish Jain
A thesis submitted in conformity with the requirements
For the degree of Doctor of Philosophy
Graduate Department of Physiology
University of Toronto
© Copyright by Amish Jain 2017

ABSTRACT OF THESIS
Comprehensive Echocardiographic Evaluation of Cardiac Function and Pulmonary
Hemodynamics in the Newly Born during Health and Disease
by
Amish Jain
Ph.D., 2017, Department of Physiology, University of Toronto
Very little is known about heart function or pulmonary hemodynamics in newborn infants in
either health or disease states. Animal experiments have shown that the immediate period
following birth is characterized by an increase in pulmonary blood flow, a decrease in pulmonary
vascular resistance and closure of fetal shunts. The specific timing and rate of these events in
human neonates are not well documented. The adaptation of an immature heart during this phase
of physiological ‘pulmonary hypertension’ has also not been studied. Persistent pulmonary
hypertension of newborn (PPHN), a frequent outcome of dysregulation of postnatal adaptation, is
associated with significant mortality and morbidity, however, the role of cardiac dysfunction is
not well known. Clinical appraisal of cardiac performance is difficult in neonates. Two
dimensional echocardiography, the only routinely feasible investigation, has undergone
significant technological advancements, making it suitable to study human neonatal cardiac
physiology. In the studies reported herein, I demonstrated the feasibility and utility of employing
quantitative echocardiography measures for studying cardiopulmonary physiology during the
immediate postnatal period, in both health and diseased states. I prospectively established a
comprehensive set of normative values for various echocardiographic indices of biventricular
ii | P a g e

cardiac function and pulmonary hemodynamics during the first two days of life and described
their relative measurement reliability. Subsequently, for the first time, I provided time-sensitive,
quantitative, physiological circulatory data regarding immediate postnatal transition in humans,
starting from < 0.5 hours of life. I demonstrated that in humans, the net decrease in RV afterload
may be slower during the first 10 to 12 hours of life. In addition, I found that in spite of changes
in loading conditions, secondary to changes in heart rate and shunting patterns across ductus
arteriosus and foramen ovale, the right and left ventricular outputs and their ratio remains
relatively constant throughout the first day of life. Further, I demonstrated lower RV function at
< 0.5 hours of age in comparison to measurements performed during the second half of the first
day, suggesting a relative vulnerability of the neonatal right ventricle to high afterload
immediately after birth. Lastly, by employing these methods in neonates with PPHN, I provided
several novel insights into its pathophysiology. I demonstrated that PPHN is characterized by
global dysfunction in both the right and left ventricle, which may be independent of underlying
etiology. In addition, I identified several previously unknown risk factors associated with cardiac
dysfunction in this disorder and showed a linear correlation between functional measures of both
ventricles. I found significant association between RV longitudinal function during the first three
days of life in neonates with PPHN and subsequent occurrence of death or need for
extracorporeal membrane oxygenation, indicating the relevance of RV function in this serious
disorder of postnatal transition.
iii | P a g e

ACKNOWLEDGEMENTS
I would like to start by thanking Dr. Robert Jankov and Dr. Patrick McNamara, my thesis
supervisors, for their constant guidance, patience and unfaltering faith in my abilities. I would
also like to sincerely thank Dr. Luc Mertens, my supervisory committee member and
methodology mentor, for always making himself available, providing high quality critiques and
inspiring me to push intellectual boundaries. I would like to thank my other supervisory
committee members, Drs. Brian Kavanagh and Kim Connelly, for their guidance and many
constructive criticisms. In addition, I would like to particularly thank Dr. Prakesh Shah, one of
my senior colleagues, for his guidance, several rewarding academic conversations and insisting
that I “plan before I do” and “do it the right way”. I would like to acknowledge several other
individuals who helped me bring this work to a successful conclusion. I would like to thank Drs.
Adel Mohamed, Afif El-Khuffash and Regan Giesinger for their assistance with various aspects
of this work and Mrs. Michelle Baczynski for her editorial review of my thesis. I would also like
to express my gratitude to the Department of Paediatrics at Mount Sinai Hospital, in particular
Drs. Shoo Lee and Yenge Diambomba, for their support and understanding during this time.
I wish to thank the Clinician Scientist Development Program of Division of Neonatology at
University of Toronto and Clinician Scientist Training Program at the Hospital for Sick Children
Research Institute for provision of a Doctoral award and Queen Elizabeth II/ Heart and Stroke
Foundation of Ontario for providing me with a Graduate Scholarship.
I give my heartfelt thanks to my wife, Dr. Poorva Deshpande, and the pleasure of our lives,
our sons, Rishik and Reyaansh, for sustaining me and enduring my long absences during this
time. Finally, I wish to sincerely thank the infants and their families for their willingness to
participate in the studies included in this work.
iv | P a g e

TABLE OF CONTENTS
Page
List of figures …………………………………………………………………………. vi
List of abbreviations …………………………………………………………………. xii
Publication of thesis work ………………………………………………………….... xv
Chapter 1: General introduction ……………………………………………………. 1
Chapter 2: Development of an imaging protocol, rationale and specific aims …… 39
Chapter 3: Methodology ……………………………………………………………... 47
Chapter 4: A comprehensive echocardiographic protocol for assessing neonatal
right ventricular dimensions and function in the transitional Period: normative
data and Z scores …………………………………………………………………......
63
Chapter 5: Left ventricular function in healthy term neonates during the
transitional period …………………………………………………………………….
83
Chapter 6: Cardiopulmonary adaptation during the first day of life in humans ... 97
Chapter 7: Cardiac function and ventricular interactions in persistent
pulmonary hypertension of the newborn ……………………………………………
117
Chapter 8: Project summary and clinical significance …………………………….. 138
Chapter 9: Limitations and future directions ……………………………………… 149
Appendix: Additional figures and data ……………………………………………... 160
References …………………………………………………………………………….. 168
v | P a g e

LIST OF FIGURES
Chapter 1
Fig. 1.1 Relationship between changes in pulmonary vascular resistance and
pulmonary arterial compliance.
p.6
Fig. 1.2 Meta-analysis of clinical trials of inhaled nitric oxide treatment in term
neonates presenting in the perinatal period with severe hypoxic respiratory
failure.
p.11
Fig. 1.3 Hemodynamic effects of exposure of neonatal right ventricle to high
afterload.
p.12
Fig. 1.4 Pulmonary arterial hypertension in preterm neonates with chronic lung
disease.
p.15
Fig. 1.5 Cellular architecture differences between the right and left ventricle and
their relationship with differential contraction patterns.
p.18
Fig. 1.6 Post-mortem diffusion tensor imaging in pigs heart showing the course of
myocardial pathways throughout the left and right ventricle.
p.19
Fig. 1.7 Complex three-dimensional architecture of the right ventricle. p.20
Fig. 1.8 Comparative changes in ejection fraction between the right and ventricle
when exposure to increased afterload.
p.21
Fig. 1.9 Response of the right ventricle when exposed to increased afterload over a
prolonged period of time.
p.22
Fig. 1.10 The net effect of variations in factors that are known to influence right
ventricle’s ability to withstand afterload is unknown in neonates.
p.23
Fig. 1.11 Measurement of myocardial velocities using pulsed tissue Doppler p.32
vi | P a g e

imaging.
Fig. 1.12 Assessment of longitudinal deformation from a myocardial wall. p.34
Fig. 1.13 Measurement of fractional area change for the right ventricle from apical
4-chamber view using two-dimensional echocardiography.
p.35
Fig. 1.14 Measurement of tricuspid annular plane systolic excursion as a marker of
right ventricular global longitudinal function using m-mode
echocardiography.
p.37
Fig. 1.15 The majority of established echocardiographic indices of right ventricular
function are limited by the fact that they are derived from a single two
dimensional plane, which may not account for the contractile contribution
of the apex-to-outflow portion of the right ventricle.
p.38
Chapter 2
Fig. 2.1 A comprehensive functional two dimensional echocardiography imaging
protocol designed specifically for use in neonates for the studies involved
in this thesis.
p.41
Fig. 2.2 Right ventricular basal diameter measured from the parasternal long axis
view using echocardiography may corresponds to the posterior depth of the
right ventricular cavity.
p.42
Fig. 2.3 Longitudinal strain of the inferior wall of the right ventricle can be
measured from the new apical 3-chamber view using echocardiography.
p.43
vii | P a g e

Chapter 3
Fig. 3.1 Right ventricular linear dimensions measured using two dimensional
echocardiography.
p.50
Fig. 3.2 Quantification of right ventricle’s function using fractional area change,
tricuspid annular plane systolic excursion and tissue Doppler imaging.
p.51
Fig. 3.3 Measurements of tricuspid inflow early and velocities using pulse wave
Doppler.
p.52
Fig. 3.4 Longitudinal strain measured for right ventricular lateral and inferior walls
from apical 4-chamber and 3-chamber views respectively.
p.54
Fig. 3.5 Measurements of left ventricular dimensions using two dimensional
echocardiography.
p.55
Fig. 3.6 Longitudinal strain for left ventricle measured using speckle tracking
echocardiography.
p.58
Fig. 3.7 Schematic representation of measures of pulmonary vascular resistance
obtained from pulse wave Doppler of the main pulmonary artery.
p.60
Chapter 4
Fig. 4.1 A box plot graph of fractional area change measurements obtained from
right ventricular 4-chamber and 3-chamber views on day 1 and day 2 of
life in healthy term neonates.
p.79
Chapter 5
Fig. 5.1 Peak systolic myocardial velocity in left ventricular free wall and p.93
viii | P a g e

interventricular septum on day 1 and day 2 of life in healthy term neonates.
Fig. 5.2 Bland Altman plots for inter- and intra-observer measurement variability
for mean longitudinal strain and strain rate measured from left ventricular
4-chamber view in a randomly selected subset of 20 scans obtained in
healthy term neonates.
p.97
Chapter 6
Fig. 6.1 Changes in echocardiographic measures of pulmonary vascular resistance
during the first day of life in healthy human neonates.
p.106
Fig. 6.2 A sequentially obtained pulse wave Doppler trace of the main pulmonary
artery from one of the study infants, showing typical changes observed
during the first 24 hours of age in healthy neonates following successful
postnatal transition.
p.107
Fig. 6.3 Box plot graphs of key echocardiographic measures of right ventricular
systolic function at <0.5 hours and 22-24 hours of life in healthy human
neonates following successful postnatal transition.
p.110
Fig. 6.4 Comparison of peak global longitudinal strain measured using speckle
tracking echocardiography from right ventricular lateral wall (GLS-4C)
and inferior wall (GLS-3C) at < 0.5 hours and 22-24 hours of age in
healthy neonates following uncomplicated postnatal transition.
p.111
Chapter 7
Fig. 7.1 Box plot graph showing comparison of tricuspid annular plane systolic p.126
ix | P a g e

excursion (TAPSE) between neonates with persistent pulmonary
hypertension of newborn (PPHN) and healthy controls.
Fig. 7.2 Box plot graphs for overall global peak longitudinal strain for the right and
the left ventricle in neonates with persistent pulmonary hypertension of
newborn (PPHN) and healthy controls.
p.126
Fig. 7.3 Linear correlations between right ventricular (RV) and left ventricular
(LV) overall global peak longitudinal strain (GLS) and RV and LV
myocardial performance index measured using tissue Doppler imaging
(MPI’).
p.128
Fig. 7.4 A box plot graph comparing TAPSE for neonates with persistent
pulmonary hypertension of newborn (PPHN) who survived until discharge
without ECMO vs. those who either died or needed ECMO.
p.130
Chapter 8
Fig. 8.1 A schematic presentation of the long term research strategy developed
during the conduct of this thesis, highlighting research questions for my
ongoing and future work.
p.146
Chapter 9
Fig. 9.1 Future plan to refine diagnostic criteria for chronic pulmonary
hypertension in preterm neonates with chronic lung disease and facilitate
early identification of at-risk neonates.
p.157
Fig. 9.2 A parasternal short axis view obtained using two dimensional p.158
x | P a g e

echocardiography in a preterm neonate with significant chronic pulmonary
hypertension demonstrating severe RV dilatation.
Appendix (additional figures)
Fig. 4.2 Measurement of peak longitudinal strain of right ventricular inferior wall
(GLS-3C) using speckle tracking echocardiography from one of the study
infants.
p.161
Fig. 4.3 Bland-Altman plots showing intra- and inter-observer measurement
variability was lower for biplane-fractional area change (global-FAC) in
comparison to single-plane measurements acquired from RV apical 4
chamber view (FAC-4C) or from RV apical 3 chamber view (FAC-3C).
p.162
Fig. 4.4 Bland-Altman plots showing intra- and inter-observer measurement
variability was relatively lower for global peak longitudinal strain (GLS-
global) obtained by averaging GLS acquired from RV apical 4 chamber
view (GLS-4C) and from RV apical 3 chamber view (GLS-3C) in
comparison to its individual components.
p.163
Fig. 4.5 Bland-Altman plots for inter and intra observer measurement variability
for myocardial performance index calculated using time periods measured
from color flow Doppler (MPI) and tissue Doppler imaging (MPI’).
p.164
Fig. 4.6 Modest linear correlation observed between right ventricular peak systolic
myocardial velocity (s’) measured from tissue Doppler imaging and
speckle racking echocardiography derived peak longitudinal strain of right
ventricular lateral wall.
p.165
xi | P a g e

LIST OF ABBREVIATIONS
2D, Two-dimensional
4C, 4-chamber view
3C, 3-chamber view
a’, Late diastolic myocardial velocity measured using TDI
B-4C, Basal diameter in 4C
B-PLAX, Basal diameter in PLAX
BW, Birth weight
BA, Bland-Altman analysis
cPHT, Chronic pulmonary hypertension
CNLD, Chronic neonatal lung disease
CMRI, Cardiac magnetic resonance imaging
COV, Coefficient of variation
ECMO, Extracorporeal membrane oxygenation
ELBW, Extremely low birth weight
EDA, End-diastolic area
ESA, End-systolic area
e’, Early diastolic myocardial velocity measured using TDI
EF, Ejection fraction
FAC, Fractional area change
GLS, Global longitudinal strain
GLS-4C, Global longitudinal strain of RV lateral wall
xii | P a g e

GLS-3C, Global longitudinal strain of RV inferior wall
iNO, inhaled nitric oxide
IVRT’, Isovolumic relaxation time measured using TDI
IVRT, Isovolumic relaxation time measured using color flow Doppler
ICC, Intraclass correlation coefficient
IQR, Interquartile range
LV, Left ventricular
LVEDD, Left ventricular end-diastolic diameter
LVESD, Left ventricular end-systolic diameter
LVSV, Left ventricular stroke volume
LVO, Left ventricular output
MPI’, Myocardial performance index measured using TDI
MPI, Myocardial performance index measured using color flow Doppler
MvE, Early mitral diastolic inflow peak velocity
MvA, Late mitral diastolic inflow peak velocity
NICU, Neonatal intensive care unit
PVR, Pulmonary vascular resistance
PAH, Pulmonary arterial hypertension
PPHN, Persistent pulmonary hypertension of the newborn
PHT, Pulmonary hypertension
PLAX, Parasternal long axis view
PAAT, Pulmonary artery acceleration time
PVRI, Pulmonary vascular resistance index
xiii | P a g e

PDA, Patent ductus arteriosus
PFO, Patent foramen ovale
PAATi, PAAT indexed to total duration of cardiac cycle
RV, Right ventricular
RVET, Right ventricular ejection time measured using color flow Doppler
RVET’ Right ventricular ejection time measured using TDI
RVSP, Peak right ventricular systolic pressure
RVSV, Right ventricular stroke volume
RVO, Right ventricular output
RVETi, RVET indexed to total duration of cardiac cycle
s’, Peak systolic myocardial velocity measured using TDI
STE, Speckle tracking echocardiography
SF, Shortening fraction
SD, Standard deviation
SVR, Systemic vascular resistance
SAX, Parasternal short axis view
TDI, Tissue Doppler imaging
TAPSE, Tricuspid annular plane systolic excursion
TvE, Early tricuspid diastolic inflow peak velocity
TvA, Late tricuspid diastolic inflow peak velocity
VTI, Velocity time integral
xiv | P a g e

PUBLICATION OF THESIS WORK
1. Amish Jain, Adel Mohamed, Afif El-Khuffash, Kim A. Connelly, Frederic Dallaire, Robert P Jankov, Patrick J McNamara, Luc Mertens. “A Comprehensive Echocardiographic Protocol for Assessing Neonatal Right Ventricular Dimensions and Function in the Transitional Period: Normative Data And Z-scores”. Journal of American Society of Echocardiography 2014; 27(12):1293-3041. Co-author contributions to this work included assistance in patient enrolment (Adel Mohammed), echocardiographic analysis for calculating inter-rater reliability data (Afif El-Khuffash) and calculation of Z-scores (Frederic Dallaire).
2. Amish Jain, Afif F. EL-Khuffash, Bart C.W. Kuipers, Adel Mohamed, Kim A. Connelly, Patrick J McNamara, Robert P. Jankov, Luc Mertens. “Left Ventricular Function in Healthy Term Neonates During the Transitional Period”. Journal of Pediatrics. 2016 Nov 28. Pii: S0022-3476(16)31231-8. Doi: 10.1016/j.jpeds.2016.11.0032. Co-author contribution to this work included assistance in patient enrolment (Adel Mohammed), echocardiographic analysis for calculating inter-rater reliability data (Bart C.W. Kuipers) and teaching and assistance with statistical analysis (Afif El-Khuffash).
3. Amish Jain, Bart C.W. Kuipers, Adel Mohamed, Brian Kavanagh, Prakesh S Shah, Luc Mertens, Robert P. Jankov, Patrick J McNamara. “Cardiopulmonary Adaptation During the First Day after Birth in Humans”. Manuscript in preparation for submission to Circulation. Co-author contribution to this work included assistance in patient enrollment (Adel Mohammed), echocardiographic analysis for calculating inter-rater reliability data (Afif El-Khuffash) and teaching and assistance with statistical analysis (Prakesh Shah).
4. Amish Jain, Afif El-Khuffash, Claar H. van Herpen, Maura Helena, Regan Giesinger, Dany Weisz, Luc Mertens, Robert P. Jankov, Patrick J McNamara. “Cardiac Function and Ventricular Interactions in persistent pulmonary hypertension of the newborn”. Manuscript in preparation for submission to Circulation Imaging. Co-author contribution to this work included assistance in identification of study patients and their echocardiograms (Claar H. van Herpen ) and collection of clinical data (Maura Helena and Regan Giesinger).
xv | P a g e 1Reprinted (Chapter 4) in compliance with Elsevier’s Author User Rights policy.
2Reprinted (Chapter 5) in compliance with Elsevier’s Author User Rights policy.

Chapter 1: General Introduction
1 | P a g e

1.1. The clinical relevance of the right ventricle
From the time of William Harvey’s 1628 treatise, De Motu Cordis, correctly describing the
pulmonary circulation, until well into the 20th century, the right ventricle remained largely
ignored, being considered a passive conduit and therefore less important than the systemic
ventricle (1). This notion was further fuelled by experimental observations by Fineberg and
Wiggers in 1936 and Taquini and co-workers in 1960, investigating the effect of an acute rise in
right ventricular (RV) afterload by artificially and variably constricting the pulmonary trunk in
an experimental adult dog model (2, 3). These experiments indicated that up to 50% constriction
of the pulmonary artery resulted in no appreciable change in ventricular pressure or cardiac
output. Additional constriction resulted in an increase in RV systolic pressure but cardiac output
was maintained until almost a 2/3rd occlusion of the pulmonary artery. However, these
experiments were performed with an open pericardium and had the fundamental flaw of failing
to account for the effect of pericardial constraint on inter-ventricular interactions. The belief that
the right ventricle was a relatively dispensable component of the cardiovascular system also
contributed to the development of the Fontan Kreutzer procedure, described separately in 1971
by Dr. Francois Marie Fontan in France and in 1973 by Dr. Guillermo Kreutzer in Argentina, as
a surgical correction for tricuspid atresia (4, 5). Since then, Fontan’s circulation, which involves
creating a pressure passive system for pulmonary blood flow by diverting the deoxygenated
blood returning to the heart via the great veins directly to the pulmonary artery, while the
functioning single ventricle (morphologically the right or left ventricle depending on the
underlying cardiac defect) is used as a pump exclusively for systemic circulation, has become the
model to study and understand the circulatory consequences of an absent right ventricle. Short
and long term follow up of these patients has demonstrated that although sustainable circulation
2 | P a g e

is feasible without a functioning right ventricle, it is with significant and often life limiting
consequences, most notably chronic venous congestion and low cardiac output (6). Furthermore,
in the absence of a right ventricle, even a small rise in pulmonary vascular resistance (PVR) is
poorly tolerated and often results in a catastrophic systemic decompensation. Ultimately,
Fontan’s circulation is said to “impact organ system[s] in an indolent and relentless manner, with
progressive decline in functionality likely” (7).
Over the last three decades there has been an increasing recognition of the critical
importance of RV function in health and disease. There is accumulating evidence of a key
prognostic role in several disorders of the cardiovascular system, including congestive heart
failure, left sided heart failure, coronary artery disease, valvular heart disease, post cardiac
surgery and congenital structural heart defects such as Ebstein’s anomaly and tetralogy of Fallot
(8-12). However, in no other disorder is the significance of preserving RV function more
recognized than in pulmonary arterial hypertension (PAH) (13). Although the hallmark feature in
PAH is raised pulmonary arterial pressure, it is now widely regarded as a “right heart failure
syndrome” (14). This is because of the consistent observation across studies, irrespective of
methods used for its assessment, that in this disorder, the severity and progression of symptoms
and clinical outcomes are less related to PVR or mean pulmonary artery pressure than the ability
of the right ventricle to cope with increased afterload while maintaining its size, function and
filling pressures (Table 1.1) (15). Tolerance of the right ventricle to afterload is variable between
individuals and known to depend on factors such as the underlying disorder, gender, age at
presentation and the rate of rise in pulmonary arterial pressure (16, 17).
3 | P a g e

Table 1.1(15): Measurements to predict outcome in adults with severe PAH (RV function related measurements shown in bold)
Study (year) No. of patients
Etiology Predictive measurements
Right heart catheterization Fuster (1984) D’Alonzo (1991) Sandoval (1994) McLaughlin (2002) Sitbon (2002) Humbert (2010) Benza (2010)
120 194 61
162 178 354
2716
PPH PPH PPH PPH PPH
IPAH PAH
Mixed venous oxygen saturation (SvO2) RAP, PAP, CO RAP, CO RAP, CO Lack of change in PVR CO RAP, PVR
Echocardiography Eysmann (1989) Raymond (2002) Bustamente (2002) Forfia (2006) Utsunomiya (2009) Ghio (2010) Sachdev (2011) Brierre (2010) Ghio (2011) Haeck (2012) Fine (2013) Ernande (2013) Ameloot (2014) Smith (2014) [24] Yeo (1998) Grunig (2013)
26 81 25 63 50 59 80 79
72
150 575 142 78 97 53
121
PPH PPH PPH
PAH/CTEPH/RD PAH IPAH PAH
PAH/CTEPH/RD
PAH PH PH
PAH/CTEPH PAH/CTEPH PAH/CTEPH
PPH PAH/CTEPH
Pericardial effusion Pericardial effusion, RAS, EI RAS, TR TAPSE Tricuspid E/e’ TAPSE, EI RV strain PAP, pericardial effusion, EI, TAPSE, MPI, IVC RV diameter RV longitudinal strain by speckle tracking RV longitudinal strain by speckle tracking RV isovolumetric contraction velocity TAPSE, dp/dt 3D speckle area strain MPI Stress echo (Δ TR velocity with exercise)
MRI Van Wolferen (2007) Moledina (2013) Yamada (2012) Veerdonk vd (2011) Swift (2014) Freed (2012)
64
100 41
110 80 58
IPAH PAH IPAH PAH IPAH
PH
SV, RVEDV, LVEDV EF, SV RV EDV EF ESV LGE
PPH primary pulmonary hypertension, PAH pulmonary arterial hypertension, IPAH idiopathic PAH, CTEPH chronic thromboembolic pulmonary hypertension, RD respiratory disease, LVD left ventricular disease, RAP right atrial pressure, PAP pulmonary artery pressure, CO cardiac output, RAS right atrial surface area, EI eccentricity index, TR tricuspid regurgitation, TAPSE tricuspid annular plane systolic excursion, RV right ventricular, MPI myocardial performance index, IVC inferior vena cava, SV stroke volume, EDV end-diastolic volume, ESV end-systolic volume, EF ejection fraction, LGE late gadolinium enhancement. Note: Irrespective of the method of assessment, parameters of RV function are more commonly associated with patient outcomes than those reflective of pulmonary vascular disease; indicating the clinical relevance of RV function in PAH. Table adapted from Naeiji R. Curr Hypertens Rep. 2015;17(5):35.
1.2. Right ventricular afterload
One of the reasons for a dichotomy between the severity of PAH and RV dysfunction and
related clinical outcomes is the commonly employed oversimplified practice of using PVR or its
4 | P a g e

surrogates as an exclusive measure of RV afterload for quantifying disease severity and
monitoring its progression or response to therapies. PVR is derived by using the measurement of
mean forward flow through the pulmonary vascular bed and is most influenced by changes in the
diameter of small peripheral arteries and arterioles, indicating that it represents the static
component of RV afterload. The blood flow in the pulmonary circulation requires a transmission
of pulsatile waves of pressure and flow down the pulmonary vascular tree, which by virtue of
having bifurcations, is characterized by several upstream deflections of pressure waves; thus
adding a dynamic or pulsatile component to the afterload experienced by the right ventricle. This
additional burden on RV workload is dependent upon the compliance of the pulmonary arterial
circuit (distensibility or pulsatility), determined mainly by the larger pulmonary arteries (up to
the first five branches) (18). Pulmonary arterial compliance has been shown to have an inverse
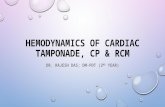
hyperbolic relationship with PVR (Figure 1.1) (19). Hence, increased resistance is preceded by
reduced compliance in evolving PAH. However, in advanced disease, arterial stiffness has
already reached its peak thereby any further increase in RV afterload is almost entirely secondary
to PVR. The ability of the large pulmonary arteries to maintain a high compliance can
significantly minimize the net afterload experienced by the right ventricle, even in the setting of
rising PVR.
5 | P a g e

Figure 2.1: Inverse hyperbolic relationship between changes in PVR and pulmonary arterial compliance in two patients with pulmonary arterial hypertension at different baseline values of PVR (A mild and B severe). Figure from Jan-Willem et at. Eur Heart J. 2008; 29(13):1688-95.
There is an increasing recognition that pulmonary vascular disease is not only contributed
to by sustained pulmonary vasoconstriction (high PVR), but also vascular remodelling and a
resulting reduction in arterial compliance, which can contribute significantly towards increasing
RV workload, particularly early in the disease process (20). However, finding a robust
quantitative measure of net RV afterload has remained an elusive clinical objective. Pulmonary
vascular impedance is said to be such a measure, as it encompasses both the static and dynamic
aspects of RV afterload, however, it can only be measured with right heart catheterization.
Catheterization derived measure of pulmonary vascular impedance in pediatric PAH patients has
recently been shown to correlate better with clinical outcomes in comparison to PVR alone (21).
While we search for the ideal hemodynamic measure of RV afterload, it appears that close
monitoring of RV function itself is the best method for monitoring clinically significant changes
in disease progression, as well as response to commonly used therapies. In fact, several experts
have recently proposed RV function in PAH as the target for drug therapies and an end point for
clinical trials (22, 23). This may be a critical detail in pulmonary hypertensive disorders in
6 | P a g e

newborn infants, where due to lack of feasibility of catheterization, our current methods for
detecting pulmonary vascular disease are even more rudimentary.
1.3. Clinical context: Postnatal adaptation and neonatal pulmonary hypertensive disorders
Transition from intra- to extra-uterine life
Birth is a unique physiological event characterized by complex and sudden changes
affecting several organ systems, most notably the respiratory and cardiovascular system (24).
Fetal life is characterized by non-participation of lungs and dependence on placental circulation
for gas exchange, along with its other metabolic functions. The fetal circulation in arranged in
series. The majority of venous return coming from the placenta bypasses the hepatic circulation
via the ductus venosus, reaching the inferior vena cava just before its entry into the right atrium
(25). Enabled by the anatomical location of the inferior vena cava and the high volume of
umbilical venous return, most oxygenated blood jets across to the left side through foramen
ovale (FO), which is kept widely open by the higher right atrial pressure compared to the left. Of
the remaining blood pumped into the pulmonary artery by the fetal right ventricle, a large
proportion joins the systemic circulation via the ductus arteriosus (DA) without passing through
the pulmonary vascular bed; the end result is that only 10-20% of total biventricular cardiac
output enters the lungs during fetal life. This, however, increases to approximately 30% by late
gestation secondary to the increase in reactivity of the fetal pulmonary vasculature during third
trimester (26). In addition to the anatomical features, these circulatory features are made possible
by the high PVR of the fluid filled fetal lungs and low systemic vascular resistance (SVR) in the
fetus secondary to its attachment to the placental circulation. Maintenance of fetal circulation as
well as its rapid adaptation after birth to a parallel circulation, where almost the entire cardiac
output must pass through the lungs for oxygenation, is a result of a cascade of concurrently
7 | P a g e

occurring, interconnected but not completely understood mechanical, biochemical and hormonal
factors (27-30).
The sentinel event which triggers dramatic circulatory adaptation at birth is onset of
ventilation (31). A sudden and rhythmic distension of lungs with air enabled by the high negative
pressure of first few breaths taken by the newly born cause displacement of lung fluid from
alveolar to interstitial space. This results in establishment of an air-liquid interface in the
ventilated alveoli and a large initial drop in PVR. Although the specific mechanism(s) by which
ventilation alone reduces PVR are not yet known, the following factors are postulated to play key
role: 1) straightening of airways and untwisting of pulmonary vessels due to alveolar expansion,
2) recruitment of intra-acinar arteries, 3) increased capillary diameter caused by an increase in
the transmural pressure across alveolar-capillary interface secondary to the newly developed
surface tension inside the alveoli and 4) improvement in ventilation-perfusion matching caused
by the vasodilatory effects of increased alveolar oxygen and the production of nitric oxide (28,
30). Coinciding with the fall in PVR secondary to ventilation, is the sudden increase in SVR after
the umbilical cord is cut and the placenta is removed from the systemic circulation. One of the
consequences of these dramatic changes in the PVR: SVR ratio is a change in the directionality
of the flow across DA, resulting in a net left to right shunt (i.e. systemic to pulmonary
circulation). Increased systemic-pulmonary shunting across the DA is thought to be a key
determinant of an initial rapid rise in pulmonary blood flow after birth. The abrupt gush of blood
into the pulmonary vascular bed (both arterial and venous) exposes the endothelium to increased
shearing forces which, in addition to an increase in oxygen tension is thought to induce
production of vasodilatory mediators (e.g. nitric oxide, bradykinin, prostacyclin) and inactivate
production of vasoconstrictor mediators (e.g. thromboxane, endothelin, leukotrienes) (29).
8 | P a g e

Contributory changes are also observed in pulmonary vascular smooth muscle cells, which
undergo remodelling and progressive thinning starting shortly after birth.
From a cardiac perspective, an acute rise in pulmonary blood flow causes a significant
increase in left heart preload and a rise in left atrial pressure. This, along with a reduction in
volume and force of venous return from inferior vena cava and lowering of right atrial pressure,
results in closure of the FO. The increase in arterial oxygen concentration, bradykinin production
and reduction in circulating levels of prostaglandins induce constriction of DA soon after birth
followed by functional closure within days. Absence of flow across the ductus venosus following
removal of the placental circulation initially results in constriction of its sphincter followed by
closure. The RV mass at the time of birth is 20% above adult values when indexed to body
surface area, while the mass of the left ventricle is 30% lower (32). Following birth the mass of
the left ventricle increase rapidly over the first two weeks of life but that of the right ventricle
decreases more slowly over months.
Our knowledge of transitional physiology as highlighted above is mostly derived from
animal experiments. The physiologic changes in humans after birth are comparable; however, the
rate and timing of these events is not well understood. Up to 10% of neonates are known to
require resuscitation at birth and dysregulation of postnatal adaptation is a common reason for
need for intensive care treatment. The availability of reliable and clinically relevant physiologic
measures of heart function, pulmonary and systemic hemodynamics in humans may not only
help understand species specific differences but may have direct diagnostic, monitoring and
therapeutic relevance leading to changes in the approach to clinical care. For instance, a recent
physiological study conducted in human fetuses has shown that much less blood bypasses the
liver via the ductus venosus than was previously assumed based on animal experiments; this
9 | P a g e

highlights the importance physiology studies in humans (25). In addition, cardiac functional
adaptation in the first day following birth has not been evaluated.
Acute pulmonary arterial hypertension in neonates
Acute PAH in the immediate postnatal period, also known as persistent pulmonary
hypertension of the newborn (PPHN), is an acute cardiopulmonary illness that accounts for up to
10% of all admissions to tertiary neonatal intensive care units (NICUs) (33). Phenotypically, it is
characterized by severe hypoxemic respiratory failure secondary to the failure of a physiological
transition of the pulmonary circulation from a high resistance intra-uterine to a low resistance
extra-uterine circuit. PPHN may arise secondary to other disorders of postnatal transition such as
perinatal asphyxia, meconium aspiration syndrome, respiratory distress syndrome, sepsis or
pulmonary hypoplasia (e.g. congenital diaphragmatic hernia) (33). The incidence of PPHN in
developed countries ranges from 1 to 2 per 1000 live births, with a reported mortality of
approximately 10% (33, 34). Surviving neonates commonly require advanced and prolonged
cardio-respiratory support and are at an increased risk of long-term adverse medical and
neurodevelopmental outcomes (34-37). Although treatment with inhaled nitric oxide (iNO), the
only approved pulmonary vasodilator agent in neonates, has reduced the need for extracorporeal
membrane oxygenation (ECMO), it has failed to impact mortality or long term outcomes (Figure
1.2) (38). A lack of impact of pulmonary vasodilator therapies on long-term outcomes has also
been described in older patients with PAH.
10 | P a g e

Figure 1.2: Meta-analysis of clinical trials of inhaled nitric oxide treatment in term neonates presenting in the perinatal period with severe hypoxic respiratory failure. iNO treatment reduced need for extracorporeal membrane oxygenation but not death. Finer NN, Barrington KJ. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD000399.
Acute PAH in neonates may also occur later in postnatal life, after the initial decrease
in PVR from fetal levels, secondary to disorders such as sepsis, pneumonia or aspiration.
Although sepsis- related acute PAH in neonates is associated with a high mortality, it remains a
largely unstudied disorder. Irrespective of the variation in underlying etiology, the hemodynamic
11 | P a g e

and clinical sequelae of high PVR are expected to be similar and include a complex but not
completely understood interplay of reduced pulmonary blood flow, perfusion-ventilation
mismatch, hypoxemia, acidosis, persistence of fetal shunts and cardiac dysfunction (Figure 1.3)
(39). How a relatively immature neonatal right ventricle copes with increased afterload, its direct
or indirect effect on the left ventricle and the systemic circulation, as well as its role in eventual
patient outcomes, remains largely unexplored.
Figure 1.3: Hemodynamic effects of exposure of neonatal right ventricle to high afterload may involve a complex, but incompletely understood, interplay between hypoxemia, ventilation-perfusion mismatch and cardiac dysfunction. The severity and relative importance of each alteration may vary between individual patients. Figure from Jain A, McNamara PJ. Semin Fetal Neonatal Med. 2015;20(4):262-71.
There is an urgent need for comprehensive high quality studies examining heart function
in neonatal acute PAH. The few studies that exist on RV function in neonates with PPHN
generally have a small number of patients, include a high proportion of neonates with conditions
12 | P a g e

such as congenital diaphragmatic hernia that has a different pathogenesis from PPHN and
employ a few select echocardiographic measures. Nonetheless, these studies have suggested that
RV dysfunction may be a common finding in neonates with PPHN and may be associated with
adverse clinical outcomes; thus emphasizing the importance of comprehensive interrogation of
this problem (Table 1.2) (37, 40-45). The ability to predict which neonates are at risk of
subsequent deterioration will help formulate clinical surveillance policies, reduce the need to act
in response to unforeseen deteriorations and provide opportunities for clinical studies of early
therapeutic interventions.
Table 1.2: Studies on RV function in neonates with PPHN
Study (year)/ Type Population/ No. of patients Measurements tested Conclusion Sernich (2006) Prospective case-control
Congenital diaphragmatic hernia (CDH) with PHT on echocardiography (N=10) Age matched control (N=24)
MPI, PEP/RVET, PEP/PAAT
Early RV dysfunction is present in neonates with CDH and PHT, which improves post-surgical repair as PHT improves.
Peterson (2009) Retrospective cohort
Acute PHT during first 28 days of age (N=63)
RV-EDA, RV-ESA, FAC, LV-EDA, LV-ESA, MV E/A, LVOT-VTI, PDA shunt type
Decreased LV size and output correlates with subsequent need for advanced therapies
Patel (2009) Prospective case-control
Cases: Consecutive NICU patients with PHT on echocardiography (n=15, 11 CDH) Controls: NICU patients with no PHT on echocardiogram (N=28)
RV myocardial velocities measured using tissue Doppler imaging
Quantifying RV function using TDI in neonates with PHT is feasible and demonstrates evidence of systolic and diastolic dysfunction
Moenkemeyer (2014) Retrospective cohort
Cases: CDH (N=20) pulmonary: systemic systolic pressure, RV myocardial velocities measured using tissue Doppler imaging
RV diastolic dysfunction diagnose by lower early diastolic velocity associated with increased duration of respiratory support
Agarwal (2015) Retrospective cohort
Cases: PHT < 1 week age (N=117) Controls: 35 (< 1 week of age)
RV SD/DD measured from tricuspid regurgitant jet, LVO, RVO, MPI, EI
The RV SD/DD ratio is a sensitive prognostic marker for need for ECMO or death
Zakaria (2015) Retrospective case-control
Cases: NICU patients with PHT on echocardiography (N=30, age range 1 to 11 days) Controls: NICU patients without PHT on echocardiography (N=69, age range 5-52 days)
TAPSE, RV s’ measured using tissue Doppler imaging, RV FAC
TAPSE most sensitive measure to distinguish PHT neonates from controls
Malowitz (2015) Cases: PHT on TAPSE, RV/LV end- TAPSE, Global RV strain
13 | P a g e

Retrospective cohort echocardiography < 7 days of age (N=86)
diastolic diameter ratio, FAC, RV 4 chamber global strain, PDA shunt type
and right to left PDA shunt associated with progression to death or ECMO
PHT pulmonary hypertension, MPI myocardial performance index, PEP pre-ejection time in main pulmonary artery, RVET right ventricular ejection time, PAAT pulmonary artery acceleration time, RV right ventricular, LV left ventricular, EDA end diastolic area, ESA end systolic area, FAC fraction area change, MV E/A mitral valve early: late inflow velocity ratio, LVOT-VTI left ventricular outflow tract velocity time integral, PDA patent ductus arteriosus, SD systole duration, DD diastole duration, LVO left ventricular output, RVO right ventricular output, MPI myocardial performance index, EI eccentricity index, TAPSE tricuspid annular plane systolic excursion, s’ peak systolic velocity, ECMO extracorporeal membrane oxygenation.
Chronic pulmonary hypertension in neonates
Chronic pulmonary hypertension (cPHT) in neonates is inextricably linked to abnormal
development of the lung, most commonly in chronic neonatal lung disease (CNLD), a frequent
complication of infants born ≤ 1,000 g (known as extremely low birth weight [ELBW] infants)
(46, 47). Advances in neonatal care over the past 25 years have had a major impact on the
survival of ELBW infants. This has also resulted in a greater burden of morbidities. Overall, the
incidence of CNLD in ELBW infants is around 50%, leading to more than 10,000 new cases per
year in the United States alone (48). In Canada, CNLD affects almost 60% of all ELBW infants
(> 800 new cases each year) (47). Pathologically, CNLD is characterized by sustained
pulmonary vasoconstriction and exaggerated vasoreactivity to hypoxemic episodes during early
disease, which after an ill-defined period of time is complicated by characteristic developmental
alterations in the pulmonary vascular bed including vascular hypoplasia and arterial wall
remodeling, as exemplified by smooth muscle hyperplasia and distal extension of smooth muscle
into normally non-muscular arteries; resulting in a relatively ‘fixed’ and often progressive
elevation of PVR (49-51) (Figure 1.4 panel A). Our understanding regarding the prevalence and
relevance of pulmonary vascular disease in CNLD is just beginning to take shape, with the
majority of studies being published in the last few years (52-59). Recent reports have now
confirmed the high prevalence of ‘significant’ cPHT in CNLD (approximately 30-40%) and its
14 | P a g e

close link with the severity of underlying lung disease (Figure 1.4 panels B and C) (52).
Further, we now know that cPHT in CNLD is independently associated with higher in-hospital
mortality, increased duration of need for respiratory support and longer hospitalization. Severe
cPHT diagnosed late after discharge from initial hospitalization appears to be particularly
malignant, resulting in death of more than half cases from RV failure within two years of
diagnosis (55) (Figure 1.4 panel D).
Figure 1.4: A. Illustration demonstrating characteristic features of arterial wall remodelling seen in chronic neonatal lung disease (muscularization of normally non-muscular distal arteries, intimal fibrosis and medial hypertrophy resulting in narrowing of vascular lumen). B. Overall 30-40% of all extremely low birth weight infants (ELBW) will develop significant chronic pulmonary arterial hypertension (PAH), however this incidence is closely linked to severity of underlying lung disease (panel C.). D. Severe PAH in neonates with CNLD diagnosed after discharge from initial hospitalization is known to be particularly malignant with a high mortality rate secondary to RV failure. Panel A is adapted from Yen-Chun Lai et al. Circ Res. 2014;115:115-130; Panel C is from An HS et al. Korean Circ J 2010; 40:131-136; and D from Khemani E et al. Pediatrics 2007; 120:1260-1269.
15 | P a g e

However, the diagnosis of cPHT in these patients is usually made by qualitative and
limited echocardiography criteria that have low sensitivity and are not suitable for early
identification of the disease; the latter is imperative if the focus of care is to maximize the
potential impact of therapeutic interventions and minimize the process of abnormal pulmonary
vascular development. There is a need to develop sensitive, non-invasive, quantitative measures
to enable the study of RV function, given the likelihood that it is a major contributor to adverse
outcomes for this vulnerable and understudied patient population. The field of echocardiographic
evaluation of the right ventricle in extreme preterm neonates is just beginning to develop, with
recent studies demonstrating the feasibility of employing RV-specific indices in this patient
population and describing ‘normal’ values (60-66).
1.4. Differences between the right and the left ventricles
For many years, both ventricles were thought to be similar and the disorders affecting the
right ventricle were commonly managed based on information derived from studies of the left
ventricle (1). However, it has become increasingly clear that the right ventricle is fundamentally
different and needs to be studied and understood independent of left ventricular performance.
Important inter-ventricular differences exist in embryonic origin, cellular architecture,
morphology and functional physiology.
Embryonic origin: The widely accepted view that all structures of the adult heart arise from a
single set of progenitor cells referred to as the ‘primary heart field’, was dispelled as recently as
the year 2001, when three separate groups of researchers, using avian and murine experimental
models, demonstrated the existence of a second contiguous but unrelated region in the
pharyngeal mesoderm contributing cells to the developing outflow tract, referred to as the
‘secondary heart field’ (67-69). Since its discovery, researchers using refined techniques,
16 | P a g e

including lineage-tracing experiments, have shown that even though all myocytes of a
developing heart are clonally related, they arise from two distinct lineages: the primary heart
field giving rise to the final left ventricle while the right ventricle, outflow tracts and atria arise
from the secondary heart field (70-72).
Cellular architecture: At a cellular level, the mature myocardium is formed by a complex three-
dimensional meshwork of intermingled myocytes scattered in an extensive fibrous matrix.
Despite the absence of anatomically separate muscular sheets or bands, the myocardial wall can
still be considered as distinct ‘layers’ based on the changing orientation of the myocardial grain
through its depths (73). Here, there are important differences between the two ventricles, which
also explain the differences observed in their respective predominant contraction patterns
(Figure 1.5A). The right ventricular myocardium can be said to have two ‘layers’: superficial
and deep. The myocytes aggregated in the superficial subepicardial layer are oriented
circumferentially, while the deep layer consists of fibers running longitudinally from the base to
the apex. Hence, the right ventricle contracts predominantly in the longitudinal direction, except
for the subpulmonary infundibulum, where the majority of myocytes are oriented in a circular
fashion. In contrast, the LV has an additional middle ‘layer’ of myocytes and a more complex
orientation. The subepicardial layer of the LV is oriented obliquely at an angle of 60 - 80o to the
equatorial plane (called the helical angle), the middle layer has predominantly circular fibers
running parallel to the equator and the deep subendocardial layer has longitudinally oriented
fibers. This complex geometry results in the left ventricle deforming in multiple planes during
each contraction including, longitudinal, circumferential, radial, as well as a twist around its axis
(Figure 1.5B) (74). Interestingly this cellular architectural pattern remains fairly constant from
early fetal to adult life (73).
17 | P a g e

Figure 1.5: A. The orientation of myofibers in superficial (subepicardial), middle and deep (subendocardial) components of the right and left ventricle. While the right ventricle has only two orientations – circumferential in superficial and middle and longitudinal in deep layers, the left ventricle demonstrates a more complex orientation with superficial oblique fibres changing to circumferential in middle followed by longitudinal orientation in deep ‘layer’. Due to this orientation, the left ventricle deforms in multiple planes as shown in panel B. The right ventricle on the other hand primarily contracts in longitudinal plane. Panel A is adapted from Siew Yen Ho Eur J Echocardiogr 2009;10:iii3-iii7 and panel B from Wei Yu et al. Eur Heart J Cardiovasc Imaging. 2013 Feb;14(2):175-82.
Using post-mortem diffusion tensor imaging to track myocardial pathways in pig hearts,
Smerup et al have recently demonstrated that each myocardial pathway in the left and the right
ventricle, instead of being a discrete bundle, possessed endocardial, mid wall and epicardial
components, which seamlessly and reproducibly transform into each other, smoothly changing
its angulation as it travels through the thickness of the myocardial wall (75). This study, similar
to previous histological reports, showed a direct continuation of fibers between both ventricles in
the superficial layers (Figure 1.6).
18 | P a g e

Figure 1.6: Post-mortem diffusion tensor imaging in pigs heart showing myocardial pathways throughout the left and the right ventricle intruding from the epicardium to the endocardium while seamlessly changing their orientation as they travel through the depth of the myocardium. Panel e clearly shows pathways crossing over from the left to the right ventricle (red color). Figure from Smerup et al. Anat Rec (Hoboken). 2009;292(1):1-11.
19 | P a g e

Gross anatomy: Considerable dissimilarities exist in the shape and orientation of the right
ventricle compared to the left. These are important determinants of their varied functional
physiology and are essential to understand to be able to appreciate the challenges involved in RV
imaging, particularly with the use of two-dimensional modalities. Anatomically, each ventricle
can be described in three parts – the inlet which consists of atrioventricular valves and papillary
muscles, the apex consisting of trabeculated myocardium and the infundibular smooth outflow
region (76). The right ventricle is the most anterior chamber of the heart, with its anatomical
regions arranged such as to give it a peculiar crescent shape as it ‘wraps’ around the left ventricle
(Figure 1.7) (77).
Figure 1.7: The right ventricle has a complex three-dimensional architecture. It is the most anterior structure of the heart (A), with its inflow (black dotted line) and outflow tract (black arrow) in different two-dimensional planes with an angle of approximately 37.5o between them. The right ventricle appears triangular in the sagittal plane (B) and crescentic wrapping around the left ventricle in the coronal plane (C). This complex shape necessitates evaluation of RV function from multiple two dimensional planes. Figure adapted from Ho SY and Nihoyannopoulos P. Heart. 2006 Apr;92 Suppl 1:i2-13. RV right ventricle, LV left ventricle, RA right atrium, Ao Aorta, PT pulmonary trunk.
The tricuspid and pulmonary valves are well separated from each other by a muscular
supraventricular crest. This is in sharp contrast to the left ventricle, which has a more circular
profile and has the mitral and aortic valves side by side in fibrous continuity. The wide angle
between the RV inlet and outlet requires the inflow region to start contracting first, which creates
a peristaltic wave of contractile motion to keep the intra-cavity circulation moving in the right
20 | P a g e

direction (towards the pulmonary valve) (78). Intra-ventricular dyssynchrony could alter this
balance, compromising the overall efficiency of contraction. In addition, the outlet of the right
ventricle is raised above the ventricular base by a freestanding muscular sleeve, forming the
subpulmonary infundibulum. While this ensures that the RV outflow region remains independent
of the left ventricle, it creates an acute angle of approximately 37.5 degrees between the plane of
the inlet and outlet of the right ventricle (79), necessitating the RV outflow tract to play an
important contributory role in the overall RV contractile function. Unlike the inlet and outlet, the
apex of both ventricles are arranged directly next to each other (80).
1.5. Response of the right ventricle to increase in afterload
Physiologically, a mature adult right ventricle is known to be more tolerant to preload but
sensitive to changes in afterload, presumably due to its thin wall and large surface area. The
slope of decline in ejection fraction in response to rising afterload has been shown to be steeper
for the right ventricle in comparison to the left in adults (Figure 1.8) (9). However, the relative
tolerance of both ventricles to afterload has not been studied in newborns.
Figure 1.8: The slope of regression is steeper for the reduction in ejection fraction determined using angiography in response to rise in afterload for the right ventricle in comparison to the left ventricle. Figure from Nagel E et al. Eur Heart J. 1996;17(6):829-36.
21 | P a g e

Clinically, end stage RV failure is characterized by a dilated, poorly contracting right
ventricle, high RV end diastolic pressure, elevated central venous pressure and reduced cardiac
output. Although a normally functioning right ventricle may rapidly progress to RV failure when
exposed to a high afterload, more often this is preceded by homeotropic adaptation (increased
RV contractility and output without dilatation) or heterotropic adaptation (increased contractility
and output accompanied by RV dilatation) (14, 81). Homeotropic adaptation may occur without
any demonstrable change in ventricular morphology or, after a period of time, may be
accompanied by RV hypertrophy (compensatory increase in RV wall thickness maintaining
normal function and output). Heterotropic adaptation on the other hand is likely to lead to high
RV end-diastolic pressure but could be clinically mild in the early phase (RV congestion) before
progressing to frank RV dilatation (RV congestion + grossly dilated RV with preserved systolic
function and cardiac output; Figure 1.9) (82, 83).
Figure 1.9: The right ventricle undergoes progressive dilatation when exposed to increased afterload for prolong period as occurs in pulmonary hypertension. The right ventricle may rapidly become dysfunctional or may undergo adaptive hypertrophy which by compensating for the increased wall stress, allows the right ventricle to pump against high resistance without failing. With increasing duration and/or severity of pulmonary hypertension, the
22 | P a g e

compensatory mechanisms fail, resulting in RV dysfunction before culminating in frank RV failure. RV congestion/dilatation is primarily characterized by diastolic dysfunction (i.e. heart failure with normal ejection fraction). This evolution proceeds more rapidly when PHT is diagnosed during neonatal and infancy period in comparison to adults and older children. Preterm neonates may have even lower capacity to adapt. RV right ventricle, LV left ventricle.
The clinical goal in management of PAH is to identify at risk patients by recognizing early
RV compromise before it culminates in end stage RV failure (84, 85). The ability of the right
ventricle to ‘cope’ with rising afterload varies with the severity and rate of progression of PAH,
as well as with the underlying etiology (13, 86, 87). Inter-patient variability may be considerable
(54, 55). Pulmonary stenosis and Eisenmenger’s syndrome are two examples of disorders where
in spite of exposure to a high afterload, RV function remains preserved for a long period, while
in patients with PAH, exposure to high afterload results in RV failure (86, 87).
1.6. Is the neonatal right ventricle more or less tolerant to afterload?
Consistent with developmental and structural differences, the right ventricle also has many
unique physiological properties governing its function in physiological and pathological
conditions (88). The net influence of variations under these conditions may influence a newborn
heart’s tolerance to increases in afterload (Figure 1.10).
Figure 1.10: The net effect of variations in factors that are known to influence right ventricle’s ability to withstand afterload is unknown in neonates.
23 | P a g e

The factors which may favourably impact RV tolerance to afterload in the newborn period
include higher RV muscle mass and wall thickness, and lower pericardial constraint. Higher RV
free wall mass (relative hypertrophy) and surface area could be a major advantage during the
newborn period, as it may result in lower wall stress, increased inotropy via Anrep’s effect and
higher ability to increase cardiac output in response to a rise in preload via Frank-Starling’s
mechanism. Wall stress is a measure of effective afterload as sensed by the ventricular wall and
is inversely related to wall thickness. Anrep’s effect refers to the myocardium’s intrinsic
autoregulatory ability to increase its contractility in response to a rise in afterload without any
contribution from extrinsic factors and has been shown in vitro to be higher in the right ventricle
because of its higher surface area (89, 90). The Frank-Starling mechanism represents a
physiological limit for the ventricular wall to increase its surface area and output in response to
increased preload without undergoing dilatation and is related to the muscle mass available for
‘recruitment’ (91).
In contrast, the factors which may adversely impact the newborn right ventricle’s tolerance
to increase workload include, higher oxygen demand due to increased muscle mass, relatively
less coronary blood supply secondary to a higher RV diastolic pressure, a lower duration of
hangout period and a lower contribution from force-frequency relation. The hangout period, a
property unique to the right ventricle, refers to the time period during which blood continues to
be ejected forward into the pulmonary circulation from the right ventricle in spite of a negative
ventriculo-arterial pressure gradient (after completion of RV systole). It is thought to be a result
of the forward momentum of the blood overcoming extremely low pulmonary pressures in
mature hearts and contributes to low RV energy requirements (92). The force-frequency relation
refers to a unique property of the myocardial muscle by which its isometric contractility
24 | P a g e

increases in response to a rise in heart rate. The force-frequency curve has been shown to be flat
in in-vitro experiments conducted using ventricular tissue obtained from neonates undergoing
surgical repair for major congenital heart defects (93). In addition, neonatal hearts are known to
be ‘stiffer’ and more dependent on loading conditions for proper functioning, likely secondary to
structural immaturity, as suggested by a higher collagen content, the presence of predominantly
uninucleated cells, a paucity of T tubules and a relative deficiency in calcium handling capacity
(94).
The ability of the neonatal right ventricle to cope with prolonged exposure to high
afterload is not known. The neonatal right ventricle, by virtue of being accustomed to working
against a relatively high resistance during fetal life, could be more tolerant to pulmonary
hypertension (PHT). However, studies have suggested that cPHT secondary to CNLD presenting
in early infancy, is particularly malignant due to an accelerated deterioration in RV function and
a shorter interval between diagnosis and death (95, 96). On the other hand, in patients with
congenital pulmonary stenosis and Eisenmenger’s syndrome, the right ventricle appears to adapt
and tolerate higher afterload for prolonged periods (as much as decades in some cases), at least
in part, by undergoing hypertrophy and re-expression of fetal genes (87). It is therefore likely,
that in line with the pulmonary hypertensive disorders of adults and older children, RV function
plays a key role in determining outcomes in acute and chronic PHT in neonates; therefore early
identification and treatment may favorably alter the clinical course for these patients. This may
be even more important for premature neonates, as their immature right ventricle may have an
even lower capacity to adapt.
25 | P a g e

1.7. Assessment of right ventricular function in neonates
Clinical evaluation of RV performance in neonates is challenging: In older patients, RV failure
is considered as a “dyspnea fatigue syndrome” as its primary symptoms, if not in an advanced
stage, are commonly linked to respiratory difficulties and exercise intolerance. Assessment of
RV performance in neonates poses a unique challenge. A large number of at-risk neonates have
associated parenchymal lung disease, which masks the symptoms of pulmonary vascular disease
and RV dysfunction (82, 97). Exercise tolerance in neonates and infants can mainly be assessed
based on changes in feeding ability. The clinical signs (e.g. jugular venous pressure) commonly
utilized in older patients are not easy to elicit in neonates. Physiological monitoring parameters
feasible in neonates in NICUs (blood pressure, heart rate, capillary refill time) can only monitor
the adequacy of systemic circulation and left heart function and that too with limited sensitivity.
In the context of PHT/RV dysfunction, alterations in these indices usually appear late in the
disease process (37, 98, 99). In summary, there are no established clinical parameters, with a
high degree of sensitivity or specificity, which can help in the clinical appraisal of RV function
in neonates. The diagnosis of significant pulmonary vascular disease and RV dysfunction in
neonates is often dependent on clinical awareness and a high index of suspicion.
Two-dimensional (2D) echocardiography is the clinical ‘gold standard’ for neonates: In older
children and adults, right heart catheterization and cardiac magnetic resonance imaging (CMRI)
are often used to confirm the diagnosis of PAH and quantify RV size and function, while
echocardiography is commonly used for screening, frequent monitoring or diagnostic assessment
of sick unstable patients in intensive care units (1, 100-102). Cardiac catheterization and MRI are
generally not feasible in the majority of newborns with PHT for a variety of reasons that include,
small patient size, high risk of complications, clinical instability and need for out-of-facility
26 | P a g e

transport. Rarely, when feasible, these investigations can only be performed sporadically and are
not suitable for longitudinal assessments or to monitor response to therapies. Two-dimensional
echocardiography is a safe, relatively quick and generally well-tolerated, non-invasive bedside
investigation that provides clinically relevant information in real time and is ideally suited for
sequential evaluations. It is the investigation of choice for cardiovascular assessment in this
population. However due to a paucity of systematic studies establishing normative data for
quantitative indices, lack of information on reliability testing and knowledge of specific cut-off
values to define clinically significant dysfunction, the evaluation of heart function has for the
most part remained qualitative in neonates (103, 104). With improvements in technology, studies
in this field are beginning to emerge (41, 62, 63, 105-109).
Challenges in right ventricle imaging using 2D echocardiography: The unusual anatomy of the
right ventricle makes it considerably more challenging to assess and judge the adequacy of its
functional performance (77, 110). First, the RV wall lies anteriorly, making it difficult to
visualize due to the relatively inferior near-field resolution of ultrasound. This problem becomes
accentuated in newborns owing to a thin chest wall; hence, the need for higher frequency
ultrasound transducers to ensure reliable imaging. Second, as discussed above, in comparison to
the simple ellipsoidal shape of the left ventricle, the right ventricle has a more complex
geometry. It appears crescentic, wrapping around the left ventricle in the coronal section,
triangular in the sagittal plane and, unlike the left ventricle, has its inflow and outflow in
different planes, making it necessary to employ multiple 2D frames to visualize the entire
chamber (77). Many of these problems can now be overcome with the advent of high frequency
ultrasound transducers (10-12 MHz), high quality image optimization techniques and newer
27 | P a g e

imaging modalities such as tissue Doppler imaging (TDI) and deformation imaging, as described
below.
1.8. Ventriculo-ventricular interactions - need for biventricular function assessment:
Various experiments using mature heart models have confirmed the strong and direct
relationship between function and geometry of both ventricles. An artificial non-contractile right
ventricle (created by replacing its free wall with a patch or by electrical isolation), demonstrates
a significant systolic pressure generation secondary to left ventricular (LV) contraction, but the
reverse was not found to be true (111, 112). Preservation of normal RV dimension appears to be
of critical importance. Acute dilatation of the RV not only dampens the ‘right sided’ contribution
of LV contraction but, if severe, can adversely impact LV systolic performance. The individual
contribution of factors which are responsible for these interactions have been poorly isolated but
include: 1) dysfunction of the shared myocardial fibres between both ventricles, 2)
intraventricular septal dysfunction, 3) trans-septal transmission of intra-cavity pressure from one
ventricle to the other, 4) the hemodynamic effects of low RV output resulting in low LV preload
or high LV diastolic pressure causing secondary post-capillary PHT and 5) the mechanical effect
of ventricular dilatation potentiated by pericardial constraint which, by limiting the volume of
heart chambers, results in diastolic dysfunction in the setting of ventricular dilatation. The
adverse effect of pericardial constraint is inversely related to the ventricular wall thickness. In
addition, RV dilatation will cause leftward shift of the interventricular septum, reducing LV
filling capacity (preload), which adversely impacts its contractility and output.
1.9. Echocardiography methods for heart function assessment in neonates
A number of 2D echocardiography methods have been developed for assessment of
ventricular size and function. Detailed guidelines have been published describing standard
28 | P a g e

methodology, normal values and clinically relevant interpretations for these variables in adults
and older children (113-115). No such guidelines exist for neonates or infants, presumably due to
lack of information regarding reliability testing, normative data and clinical utilization. With
technological advancements in echocardiography equipment and increased availability of newer
imaging modalities, many of the established techniques are now being employed in neonates and
preliminary reports describing the feasibility and normal values for related indices are beginning
to emerge. However, high quality normative datasets are still missing for the majority of indices
(Table 1.3) (104, 116). In the studies described in subsequent chapters, I utilized a wide array of
functional indices derived using a comprehensive imaging protocol developed based upon, but
not restricted to, the guidelines published by American Society of Echocardiography (ASE).
While the standard commonly used techniques are defined in the methods chapter, some specific
newer methods are described below.
Table 1.3: Echocardiographic indices of ventricular dimensions and function and availability of normal data for neonates Echo window Adult data Neonatal data Description RV Dimensions Basal diameter Apical 4C Available NA Anterior cavity Mid-cavity diameter Apical 4C Available NA Anterior cavity Base-apex length Apical 4C Available NA Anterior cavity RV areas Apical 4C Available NA Anterior cavity RV Functional indices FAC Apical 4C Available NA Systolic function (anterior cavity) TAPSE Apical 4C Available Available Longitudinal systolic function
(base-apex) TDI (peak systolic) Apical 4C Available Available Longitudinal systolic/diastolic
function 2D Strain (lateral wall) Apical 4C Available Limited Systolic function (base-apex) MPI Apical 4C Available Available Global function LV Dimensions Basal diameter Apical 4C Available NA Anterior cavity Base-apex length Apical 4C Available Available Anterior cavity LV volume Apical 4C Available Limited Anterior cavity LV Functional indices Fractional shortening Parasternal
short axis Available Available Systolic function (dependent on
septal motion) Ejection fraction (Simpson’s)
Apical 4C Available Limited Systolic function
29 | P a g e

TDI (peak systolic) Apical 4C Available Available Longitudinal systolic/diastolic function
2D Strain Apical 4, 3 and 2 chamber views
Available NA (only apical 4C described in few neonates)
Systolic function (base-apex)
MPI Apical 4C Available Available Global function FAC fractional area change, TAPSE tricuspid annular plane systolic excursion, TDI tissue Doppler imaging, 2D two dimensional, MPI myocardial performance index, 4C 4 chamber view, NA: not available
Myocardial Tissue Doppler Imaging (TDI):
Traditionally, spectral pulsed Doppler echocardiography, due to its property of detecting
high velocity low amplitude motion, has been used in routine clinical practice to evaluate the
velocity of blood flow. Tissue Doppler imaging (TDI), is a robust technique, relatively recently
introduced to the field of neonatology, which enables detection of velocities directly from the
tissue (117-121). Contrary to spectral Doppler echocardiography, TDI detects low velocity, high
amplitude motion, ideally suited for studying the movement of the myocardial wall, while
avoiding artefacts from movement of blood (122, 123). Unlike conventional methods of
functional assessment, which mainly assess changes in cavity dimension and blood flow
velocities, this modality directly assesses muscle wall characteristics. TDI captures information
using high frame rates; the resulting high temporal resolution facilitates reliable and reproducible
measurements of the velocities of the myocardial wall during various phases of cardiac cycle, as
well as the measurements of the duration of these phases (systolic and diastolic times /
isovolumic contraction and relaxation times). Currently, there are two methods available to
derive these measurements - pulsed TDI and colour TDI (124, 125). Of these, pulsed TDI is the
preferred approach due to its advantages of high temporal resolution, ease and speed of
measurement and high inter-rater reliability. I used pulsed TDI method in studies described in
chapters 4 to 7. As the name suggests, it involves measuring TDI velocities by spectral analysis
using pulse wave Doppler technique. By convention, use of this method is restricted for
30 | P a g e

assessment of RV and LV free wall and septal motion at the base, which is then considered as a
marker of global longitudinal function of the respective myocardial wall.
Images are usually obtained from an apical four-chamber view. The sector width of the
field of view is usually narrowed to only include the wall of interest. This ensures that the
temporal resolution is enhanced and a frame rate of over 200 frames per second is obtained. A
pulsed wave Doppler sample is then placed at the base of the respective wall while minimizing
the angle of insonation, less than 20 degrees in all cases to avoid underestimation of velocities
(Figure 1.11A). The sample gate is narrowed to only capture the velocity of the area of interest
(usually 1 – 2 mm) and peak velocities are recorded in systole (s’), early (e’) and late (a’)
diastole, as well as during isovolumic contraction and relaxation (126). The duration of these
phases can also be easily measured (Figure 1.11B). Using the values of event timings,
myocardial performance index (MPI’), a simple hemodynamic variable which represents global
ventricular function, can be calculated using a simple formula; MPI’ = [isovolumic contraction
time (IVCT) + isovolumic relaxation time (IVRT)]/ejection time (107, 127-129).
31 | P a g e

Figure 1.11: Measurement of myocardial velocities using pulsed tissue Doppler imaging. By convention measurements are performed at the basal segment of the RV free wall, inter-ventricular septum and LV free wall (A). Peak velocities in each phase of cardiac cycle as well as event timings can then be easily measured (B). For the right ventricular, peak systolic myocardial velocity (s’) has been shown to increase with gestational age; Koestenberger et al. Neonatology. 2013;103(4):281-6. Panel A courtesy of Dr. Afif El-Khuffash.
The main disadvantages of this technique are low spatial resolution, only registering
motion parallel to the line of interrogation at the base, and inability to differentiate a tethering
effect i.e., movement of a non-contractile wall segment due to contraction of an adjacent
segment. While pulsed TDI measures peak myocardial velocities, color TDI is an angle
independent offline method, which allows measurements of mean myocardial velocities at
various segments. However, it has poor inter-rater reliability and relatively lower temporal
resolution. Normative data for pulsed TDI velocities for preterm and term neonates is now well
established (63, 106, 121, 125, 130). Previous studies have demonstrated a positive linear
relationship between gestational age and RV s’ (Figure 1.11 C) (63). In older patients, RV s’
32 | P a g e

correlates well with MRI obtained RV ejection fraction, in the absence of regional dysfunction
(131).
Deformational imaging – 2D speckle tracking echocardiography (STE):
Deformation refers to the change in shape of the myocardium from its baseline state at end-
diastole to its deformed state at end-systole (Figure 1.12A). This occurs as a result of sarcomere
shortening during contraction and leads to a reduction in cavity size and ejection of blood from
the ventricle (132). The direction and type of deformation is dependent on the orientation of the
myocytes and as described above, is thought to be predominantly longitudinal for the right
ventricle (and circumferential to a lesser extent), while the left ventricle undergoes longitudinal,
circumferential as well as radial (thickening) deformation (74). Myocardial strain is the term
used to define this deformation occurring in systole relative to the original length at end diastole
and is expressed in a percentage (%) (133). Longitudinal and circumferential deformations are
assigned a negative strain to indicate shortening, and radial deformation a positive strain to
indicate thickening. Strain rate refers to the speed at which myocardial deformation occurs and is
expressed in 1/s. One major advantage of strain and strain rate imaging is the ability to quantify
both global as well as regional wall function (134-136).
Two-dimensional speckle tracking echocardiography is an imaging technique that
measures deformation by tracking the movement of speckles within the myocardial wall.
Speckles are acoustic backscatter generated by the ultrasound beam and form a unique pattern in
each wall segment (137). Those speckles can be tracked frame-by-frame using offline software,
which then directly measures strain and calculates the strain rate for various segments of the
ventricular wall to generate a strain curve (Figure 1.12B). The values obtained from various
segments can then be averaged to obtain an overall global value for the respective wall. This
33 | P a g e

technique has been validated by ultrasonomicrometry in the longitudinal direction and it has
been widely applied to the left ventricle and most recently to the right ventricle in older patients
(74, 132, 138-145) and children (138, 142, 146-148). A major advantage of STE over color TDI,
the aforementioned method of measuring myocardial deformation, is that it is angle independent
i.e. not dependent on the alignment of the wall relative to the ultrasound beam (141).
Furthermore, it possesses a relatively improved signal to noise ratio. The main disadvantage of
STE is a limitation of the software to track speckles when image quality is suboptimal; as a
result, dropouts and reverberations can negatively affect tracking. In neonates, a frame rate to
heart rate ratio of 0.7 to 0.9 has been suggested to minimize inter-rater measurement variability
(105). This is important due to the higher heart rates in neonates. In term neonates, the normal
data for STE derived deformation parameters has not been fully established. Few small studies
have suggested its feasibility, described normal LV values derived exclusively from the apical 4-
chamber (apical-4C) view (instead of the standard 4, 3 and 2 chamber views) and have
highlighted the potential utility of strain and strain rate for evaluation of pathological states in
preterm and term neonates (109, 127, 149-157).
Figure 1.12: A. Longitudinal deformation refers to the change in length of a segment from its baseline shape in diastole to its deformed shape in systole. Strain refers to the degree of change in shape relative to the baseline and is
34 | P a g e

expressed in (%). B. Strain peaks during end systole at aortic valve closure (AVC) and returns to baseline during diastole at mitral valve closure (MVC). On the other hand strain rate peaks in mid systole and returns to baseline at AVC when no deformation occurs. SRe: early diastolic strain rate; SRa: late diastolic strain rate (during atrial contraction). Figure courtesy of Dr. Afif El-Khuffash.
Additional 2D echocardiography derived RV specific functional measures:
Fractional area change (FAC): Fractional area change is the relative change in the area of the
RV cavity in end-systole compared to end-diastole expressed as a percentage and by convention
is calculated from measurements of the RV cavity areas as visualized in the RV-focused apical-
4C view (Figure 1.13). FAC is the RV equivalent of ejection fraction and represents global
pump function. In older patients, FAC has been shown to have a good correlation with MRI
measured RV ejection fraction (158). A major disadvantage of this measure is the dependence on
a high quality 2D image, as manual tracing of RV endocardial borders is required. This may be
more challenging in neonates given the increased trabeculations in the right ventricle. A recent
study has demonstrated the feasibility of using this index in preterm neonates and reported higher
RV areas and lower FAC in patients with CNLD compared to controls (61).
Figure 1.13: Fractional area change is calculated for the right ventricle from apical-4C view by measuring RV areas in end-diastole (EDA) and end-systole (ESA) and then applying the simple formula of FAC (%)= [(EDA-
35 | P a g e

ESA)EDA] x100. FAC shows good correlation with MRI derived ejection fraction in adults. Anavekar et al. Echocardiography. 2007;24(5):452-6. Figure courtesy of Dr. Luc Mertens.
Tricuspid annular plane systolic excursion (TAPSE): TAPSE is a linear measurement of the
maximum displacement of the tricuspid annulus during each contraction, as obtained from the
RV-focused apical-4C view using M mode echocardiography by placing the cursor through the
tricuspid valve annulus (159) (Figure 1.14). In adults with PAH, TAPSE has been shown to be a
sensitive marker of clinical prognosis and global RV longitudinal function (base to apex). In
addition it has been shown to be reflective of the extent of RV remodelling and disproportion in
the sizes of the right and left heart and severity of PVR (159-162). Preliminary reports in term
neonates with PPHN have suggested TAPSE to be a potentially useful index for measurement of
RV function and prognosis, however its relevance in comparison to other markers has not been
tested (43, 44). Similar to RV s’, TAPSE in preterm neonates has been shown to increase with
gestational age (62). TAPSE has several advantages such as simplicity of measurement,
immediate bedside availability of results and high inter-rater reliability. Its disadvantage is that it
only indicates longitudinal function of the RV free wall, does not account for the function of the
outflow tract and may be falsely elevated by LV motion (163).
36 | P a g e

Figure 1.14: Tricuspid annular plane systolic excursion (TAPSE) is a simple measure of global longitudinal function of the right ventricle and is shown in preterm and term neonates to have a linear positive correlation with birth weight and gestational age. Koestenberger et al. Neonatology. 2011;100(1):85-92.
1.10. Application of echocardiographic indices during the newborn period
A number of factors need to be considered for application of published imaging guidelines
in the newborn population, particularly during the first few days of life, normally characterized
by significant circulatory changes - a fall in PVR, an increase in pulmonary blood flow and
closure of fetal shunts. First, given that the majority of neonates with acute PHT present during
the early postnatal period, it is crucial to know the influence of normal physiological transition, if
any, on the normal values of echocardiography-derived parameters. Second, by convention, most
of the established RV functional parameters are derived exclusively from a single 2D view (RV-
focused apical-4C view), which only visualizes the anterior RV cavity and thus may not account
for the significant contribution of the RV infundibulum (Figure 1.15) (8). Third, the RV cavity
dimensions as measured in the apical-4C view are influenced by interventricular septal motion,
which is physiologically ‘abnormal’ during the first few days of life in neonates (164). There is a
clinical need to develop and test comprehensive imaging protocols for quantifying cardiac
37 | P a g e

function in neonates. Such protocols should ideally make use of multiple modalities as available
and include parameters derived from 2D views other than the apical-4C view. To prevent
misinterpretation of the results obtained in disease states, information is required regarding the
effect of physiological changes occurring during normal newborn transition on various
functional parameters.
Figure 1.15: The majority of established echocardiographic indices of RV function are derived from one 2D plane (apical 4C view), which only visualizes the anterior RV cavity (yellow shaded area) and may not account for the contractile contribution of a significant portion (infundibulum; green shaded area). Schematic adapted from Sheehan F and Redington A. Heart. 2008;94(11):1510-5.
38 | P a g e

Chapter 2: Development of an imaging protocol, rationale and
specific aims
39 | P a g e

2.1 Development of an imaging protocol and novel indices for quantifying RV function
The development of the comprehensive functional imaging protocol used in subsequent
studies, as summarized below, was undertaken during my clinical fellowship prior to
commencement of my graduate studies in the Department of Physiology. As summarized in
chapter one, a number of 2D echocardiography techniques suitable for studying ventricular
function in neonates are now available. These methods have been extensively used in older
patients to study the left ventricle, and more recently the right ventricle in PAH (165). While
sporadic use of some of these indices in neonates have emerged, clinical assessment of heart
function has remained qualitative for the most part, presumably due to lack of quality normative
datasets for the majority of available indices, as well as their relative reliability testing. This is
particularly true for the immediate postnatal period, which is marked by important changes in
biventricular loading conditions and is also the period during which the majority of cases of
neonatal acute PHT are encountered. These considerations coupled with my own experience in
neonatal echocardiography and the American Society of Echocardiography’s latest guidelines led
us to define a comprehensive functional two-dimensional echocardiography imaging protocol
suitable for neonates (Figure 2.1) (113-115). This protocol integrated various available
modalities and enabled quantitative estimation of right and left ventricular size, systolic and
diastolic function using multiple 2D planes, as well as quantified pulmonary hemodynamics
using standard measures previously employed in neonates.
40 | P a g e

Figure 3.1: A comprehensive functional two dimensional echocardiography imaging protocol designed specifically for use in neonates for the studies involved in this thesis.
In addition, as also highlighted in the introductory chapter, currently established indices of
RV function have the limitation of being exclusively derived from a single 2D view (the apical-
4C view), which only allows visualization of the RV lateral wall and a part of its crescentic
cavity (base to apex). Hence, these measures may not account for the contribution of a
significant part of the right ventricle (apex to outflow) and may be influenced by the shape and
movement of the interventricular septum, which is particularly important in the immediate
postnatal period. Under these considerations, I incorporated the following additional imaging
sequences and developed related functional indices to allow a more comprehensive RV
41 | P a g e

functional assessment in neonates, independent of the effect of the interventricular septum
(technical details provided with methods in chapter 3).
Basal diameter -PLAX: This linear dimension was developed to allow measurement of the
previously unmonitored ‘posterior depth’ of the RV cavity. From the parasternal long axis view
(PLAX) of the RV inflow, the antero-inferior linear dimension of the RV cavity, the RV basal
diameter (B-PLAX), can be measured (Figure 2.2).
Figure 2.2: In addition to the four standard linear dimensions measured from the apical 4C view, RV basal diameter was also measured from the parasternal long axis view of the RV inflow. Anatomically this corresponded to the posterior depth of the RV cavity. Schematic adapted from Sheehan F and Redington A. Heart. 2008;94(11):1510-5.
RV apical 3 chamber view (3C): The rationale of developing indices using this view, was to
allow quantitative estimation of the functional contribution of the ‘wrap around’ infundibular
portion of the RV cavity (Figure 2.3A). From the standard apical imaging window, a short axis
view of the right ventricle can be obtained, visualizing both its inflow and outflow portions
within the same 2D view along with the RV inferior wall (Figure 2.3B). This view was then
used to measure the end-systolic (ESA-3C) and end-diastolic (EDA-3C) areas of the visualized
RV cavity and calculate the related fractional area change (FAC-3C). Further, using 2D STE, the
42 | P a g e

inferior wall of the right ventricle could be tracked and the peak global longitudinal strain of the
inferior wall (GLS-3C) obtained (Figure 2.3C).
Figure 2.3: A. The green shaded area highlights the infundibular ‘wrap around’ portion of the right ventricle which is usually not included in RV functional assessment. B. A short axis view of the right ventricle obtained from the standard apical acoustic window. This view allow simultaneous visualization of the inflow and outflow portion of the right ventricle, its posterior cavity and inferior wall. C. The RV inferior wall seen in this view can be tracked using speckle tracking echocardiography and its longitudinal strain can then be measured. Schematic in panel A adapted from Sheehan F and Redington A. Heart. 2008;94(11):1510-5. Panel B reproduced from Jain et al. J Am Soc Echocardiogr. 2014;27(12):1293-304.
2.2 Rationale and aims
Cardiovascular decision-making in critically ill neonates is complicated by a lack of
accurate and reliable measures of the adequacy of ventricular performance, and limited
understanding of the interplay between cardiovascular physiology in neonatal disease and
outcomes. Assessment of cardiovascular well-being in the immediate period after birth is even
more challenging due to physiological changes in fetal shunts and vascular resistance. Unlike
older patients, the clinical symptoms and signs of cardiovascular compromise in neonates, in
particular RV dysfunction, are non-specific and more definitive investigations, such as cardiac
catheterization and CMRI, are generally not feasible. With relatively recent technical
advancements, 2D echocardiography has become more suitable for cardiac functional imaging in
neonates. It offers the potential of a timely and longitudinal evaluation of myocardial
43 | P a g e

performance and/or pulmonary hemodynamics in sick neonates, however a robust
comprehensive normative dataset and information on relative measurement reliability is lacking.
Further, availability of these methods, if reliable, also offer an opportunity to study and
understand the cardio-pulmonary adaptive changes and their specific timing in relation to normal
physiological transition from an intra-uterine to an extra-uterine environment in humans. To
date, our knowledge of these events is mostly based on animal models and limited to circulatory
changes. It is important to understand the effect of postnatal circulatory changes on
echocardiography-derived indices of cardiac function, as the majority of sick newborns present
clinically within the first 48 hours of life. Defining normative data and normal physiologic
adaptation is an essential pre-requisite of determining whether deviations seen in any
echocardiography measurement is reflective of a disease process. The overall long term objective
of this work is to understand the incidence, progression and short and long term clinical
significance of cardiac dysfunction in neonatal pulmonary hypertensive disorders and to
facilitate early identification of at-risk neonates. Currently, there are major gaps in our
understanding of the factors governing the high rates of adverse outcomes observed in neonatal
PHT. Right heart function, a likely key prognostic factor, has been grossly understudied in
neonates because of technological lag and a lack of appreciation of its probable critical role in
clinical outcomes. High quality, comprehensive and systematic clinical studies are critical to
understand these factors and to establish methods for early identification of infants at highest
risk. The specific aims for the studies conducted for this thesis are as follows:
44 | P a g e

Chapter 4 (RV function) and Chapter 5 (LV function):
• To test the feasibility and reliability of a comprehensive echocardiographic protocol
including novel indices specifically developed for use in neonates, for quantifying RV
and LV dimensions and function in healthy term human neonates.
• To establish normative data for indices derived using 2D echocardiography, TDI and 2D
STE.
• To investigate the effect of early transitional changes on these measurements by
comparing results obtained on days 1 and 2 of life.
Chapter 6:
• To delineate the natural history of pulmonary vascular resistance, right and left
ventricular outputs and transitional shunts during the first 24 hours of life in humans.
• To study the cardiac functional adaptation associated with the immediate postnatal
period.
• To investigate the reproducibility of echocardiographic measures of pulmonary vascular
resistance and cardiac outputs in another larger cohort of healthy neonates.
Chapter 7:
• To identify echocardiographic correlates of biventricular size, function, and
hemodynamics, including shunt patterns, in neonates presenting with persistent
pulmonary hypertension of the newborn (PPHN) during the first 3 days of life by
employing a comprehensive imaging protocol as described in Chapters 4 and 5.
• To investigate associations between key echocardiographic findings and subsequent
adverse clinical outcomes in neonates with PPHN.
45 | P a g e

• To identify risk factors associated with cardiac dysfunction in neonates with PPHN.
• To examine inter-ventricular functional correlations in PPHN during the immediate
postnatal period.
46 | P a g e

Chapter 3: Methodology
47 | P a g e

3.1 Study design and sites
The work encompassed in this thesis included performing and analyzing echocardiograms
for two prospective observational studies conducted in healthy term human newborns (Chapter
4-6) and one retrospective cohort study including analysis of echocardiograms for newborns
admitted to the NICU with a diagnosis of PPHN (Chapter 7). The studies in Chapters 4 to 6 were
carried out in the well Mother and Baby Unit and Labour ward of Mount Sinai Hospital, and the
study described in chapter 7 was performed in the NICU of the Hospital for Sick Children; both
sites are teaching hospitals affiliated with the University of Toronto, Ontario, Canada.
3.2 Ethics
All studies received approval from the institutional Research Ethics Board. For prospective
studies, informed consent was obtained from the parents of recruited infants. A consent waiver
for the retrospective study was obtained from the Research Ethics Board.
3.3 Echocardiography material and personnel
I performed all scans using a Vivid 7 ultrasound scanner with a 10 MHz transducer or a
Vivid E9 ultrasound scanner with a 12 MHz transducer (GE Medical Systems, Milwaukee, WI).
Studies were digitally stored as DICOM raw data and analyzed off-line, in a random order, at
completion of recruitment for each study using a dedicated workstation (EchoPAC, version
BT10, GE Medical Systems). Wherever applicable, only the raw measurements were recorded
initially, while the calculations to generate the final results were carried out after completion of
the analysis of echocardiograms. For work described in chapter 7, to ensure blinding, clinical
data was collected separately and was merged with echocardiography data prior to statistical
48 | P a g e

analysis. All scans were analyzed as per published guidelines and the indices described below
were collected (113, 114).
3.4 Right ventricular parameters
RV linear dimensions:
The majority of linear dimensions were measured from the RV-focused apical-4C view
(Figure 3.1A). Tricuspid valve annular diameter (TVA) was defined as a straight line joining the
hinge points of the anterior and septal valve leaflets. The basal diameter (RV B-4C) was
measured at the basal third of the RV cavity as the maximal distance from the RV lateral wall to
the septum while maintaining a parallel orientation to the TVA. A straight line joining the mid-
point of the TVA to the RV apex constituted the RV length (RVL). The mid-cavity diameter (MC-
4C) was defined by a straight distance between the RV lateral wall and the septum running
parallel to the TVA but passing through the mid-point of RVL. In addition, as previously
described, with the aim of quantifying the antero-inferior dimension of the RV cavity, I
measured the B-PLAX using the PLAX RV-inflow view (Figure 3.1B). This view was obtained
by anteriorly tilting the ultrasound probe from the standard PLAX view until the interventricular
septum was no longer in view and was replaced on screen by the RV anterior wall and attached
tricuspid valve leaflet. The measurement was then performed as the maximal diameter at the
basal one-third of the RV cavity from its anterior to inferior walls, while maintaining a parallel
orientation with the TVA. All dimensions were measured in end-diastole.
49 | P a g e

Figure 4.1: A. Anterior RV cavity dimensions measured in apical 4C view: 1. Tricuspid valve annular diameter (TVA), 2. Basal diameter (B-4C), 3. RV length (RVL), 4. Mid cavity diameter (MC-4C), B. RV basal diameter measured from parasternal long axis view (B-PLAX), corresponding to the posterior depth of the RV cavity. Figure from Jain et al. J Am Soc Echocardiogr. 2014;27(12):1293-304.
Functional measurements obtained from the apical-4C view:
Fractional area change (FAC-4C): The RV areas at end-diastole (EDA4C) and end-systole
(ESA4C) were calculated by manually tracing the RV endocardial borders including the RV
trabeculations within the area (Figure 3.2A). FAC-4C (expressed as a %) was calculated using
the formula [(EDA4C – ESA4C)/EDA4C] x 100.
Tricuspid annular plane systolic excursion (TAPSE) was measured using M-mode
echocardiography with the line of interrogation passing through the lateral aspect of tricuspid
annulus while maintaining vertical alignment with the apex (Figure 3.2B).
Myocardial velocities: Pulsed TDI of the tricuspid annulus was obtained by placing a pulse
wave sample (gate 2 mm) on the basal segment of the RV free wall just below the lateral
tricuspid annulus. Peak systolic (s’), early diastolic (e’), late diastolic (a’), as well as peak
isovolumetric contraction (IVCV’) velocities were measured. From the Doppler tracings, the
time intervals including the closing to opening of the tricuspid valve (TcOt’), isovolumic
50 | P a g e

relaxation time (IVRT’), duration of systole (systole’ = beginning to the end of s’= RVET’) and
diastole (diastole’= beginning of e’ to end of a’) were obtained (Figures 3.2C & 3.2D). e’:a’,
TvE:e’, systole’:diastole’ and the TDI-based myocardial performance index [MPI’= (TcOt’-
RVET’)/ RVET’] were then calculated.
Figure 3.2: A. Fractional area change measured from the apical-4C view (FAC-4C), B. Tricuspid annular plane systolic excursion (TAPSE) is the downward vertical distance the tricuspid annulus moves (yellow arrow) during systole and is measured using m-mode echocardiography C. and D. Using pulsed tissue Doppler imaging, various RV myocardial velocities (cm/s) and time periods (msec) are measured at the basal segment of the RV free wall, just below the lateral tricuspid annulus. Time from closing to opening of tricuspid valve (TcOt’)= from the end of a’ to beginning of next e’; right ventricle ejection time (RVET’)= start to end of s’; isovolumetric relaxation time (IVRT’)= end of s’ to beginning of e’. s’/e’/a’/IVCV’ systolic/early diastolic/late diastolic/isovolumetric contraction velocities. Figure from Jain et al. J Am Soc Echocardiogr. 2014;27(12):1293-304.
Tricuspid valve inflow was assessed by placing a pulsed wave sample gate of 2 mm at the tip of
the tricuspid valve leaflets during diastole with the Doppler beam parallel to the inflow as
visualized using color Doppler echocardiography. Early (TvE) and late (TvA) inflow velocities
and their ratio (TvE:TvA) were measured. The area under the curve for the tricuspid inflow was
51 | P a g e

estimated as velocity time integral (VTI) measured by tracing the borders of the inflow Doppler
(Figure 3.3A). Conventional myocardial performance index (MPI) was also calculated by
measuring the time between end of TvA and beginning of next TvE wave (TcOt), along with the
right ventricular ejection time measured from pulse wave Doppler of right ventricular outflow
tract (RVET) (Figure 3.3B).
Figure 3.3: Measurements of tricuspid inflow early (TvE) and late (TvA) velocity as well as velocity time integral (VTI). Myocardial performance index (MPI) can also be calculated from measurement of duration between closing and opening of tricuspid valve (TcOt) from tricuspid inflow Doppler and right ventricular ejection time (RVET) from pulmonary artery Doppler.
Peak longitudinal strain of the RV lateral wall: The grey scale images recorded at a frame rate of
80-100 frames/sec were analyzed off-line using 2D speckle-tracking analysis software
(EchoPAC, version 10, GE Medical Systems). The RV lateral wall endocardial border was
52 | P a g e

manually traced at end-systole from the lateral basal attachment of the tricuspid valve to the apex
(133). The width of the region of interest was reduced to the smallest allowed by the software.
The software’s automated tracking was visually inspected before accepting the results. The
tracing points were manually re-positioned in cases of inadequate tracking. A maximum of 10
minutes was allowed to obtain adequate tracking before the image was deemed ‘non-analyzable’.
Overall peak GLS of the RV lateral wall (GLS-4C) was calculated by averaging peak GLS of the
basal, mid and apical segments (Figure 3.4A).
The RV-3 chamber view:
From the apical window, a ‘RV-focused apical-3-chamber view’ (RV-3C) was acquired by
rotating the transducer counter clockwise from the standard RV-4C view while maintaining a
slight rightward tilt to keep the RV in view. The probe was rotated until the left heart was
completely out of the view, the ascending aorta was in the center of the image and simultaneous
visualization of RV inflow, outflow and the inferior wall was achieved. Precaution was taken to
avoid visualizing the anterior wall of the right ventricle. Our aim was to ‘capture’ the maximum
RV cavity while keeping these anatomical landmarks in view (Figure 2.3B). Using this view, we
measured FAC (FAC-3C) and peak GLS for the inferior wall (GLS-3C) using similar methods as
described above. Briefly, FAC-3C (%) = [(EDA3C – ESA3C)/EDA3C] x 100, where EDA3C
and ESA3C are RV areas at end diastole and systole obtained by manually tracing the
endocardial borders (Figure 3.4B). For GLS-3C, the inferior wall’s endocardial border was
manually traced in end-systole from the lateral basal attachment of the tricuspid valve to just
before the pulmonary valve attachment at the infundibulum. The values for all segments were
averaged to obtain an overall GLS-3C for the inferior wall (Figure 3.4C). Similar to GLS-4C,
the image was deemed ‘non-analyzable’ if adequate tracking was not achieved in 10 minutes.
53 | P a g e

The results of RV-4C and RV-3C views were then averaged to calculate global FAC and global
GLS.
Figure 3.4: A. Calculation of longitudinal strain of RV lateral wall (pLS-4C) using speckle tracking echocardiography. The pLS value of each segment (represented graphically by color-coded lines) is averaged to generate an overall pLS-4C. B. Measurement of fractional area change from RV-3C view (FAC-3C). Manual tracing of the endocardial borders was performed to generate respective RV areas at end-diastole (EDA-3C) and end-systole (ESA-3C). FAC-3C was then calculated by formula (EDA-3C – ESA-3C)/EDA-3C). C. Calculation of longitudinal strain of RV inferior wall (pLS-3C) using speckle tracking echocardiography. Figures from Jain et al. J Am Soc Echocardiogr. 2014;27(12):1293-304.
3.5 Left ventricular parameters
LV Dimensions:
LV dimensions were obtained at end-diastole from the apical 4-C view, the LV PLAX view and
the parasternal short axis view taken at the level of papillary muscle. From the apical 4-C view,
mitral valve annulus diameter (MVA) was measured by joining a straight line between the two
leaflet hinge points; the basal diameter (LV B-4C) was measured by drawing a straight line at the
basal segment of the LV cavity, parallel to the MVA to get the maximal distance between LV
free wall and septum; LV length was determined by a straight line joining the midpoint of the
MV annulus and LV apex (Figure 3.5A). Left ventricular end diastolic diameter (LVEDD) was
determined using M-mode of the long and short axis parasternal views. Care was taken to ensure
54 | P a g e

that the line of interrogation was perpendicular to the interventricular septum and ‘cuts’ the LV
cavity at the level of the mitral valve leaflet tips (Figure 3.5B). Finally, left ventricular end
diastolic circumference (LVEDC) was determined in 2D by manually tracing the endocardial
borders of the LV cavity in the short axis parasternal views at the level of the papillary muscles
just below the mitral valve chordae (Figure 3.5C).
Figure 3.5: Measurement of Left Ventricular dimensions using the apical 4C view (A), M-mode of the long axis parasternal view (B), and the short axis parasternal view at the level of the papillary muscles (C). MV: mitral valve; LV: left ventricle; LVEDD: left ventricle end diastolic diameter; LVEDC: left ventricle end diastolic circumference.
LV functional indices:
Shortening fraction (SF): Using the same M mode echocardiography image of the left ventricle
used to measure LVEDD from the LV parasternal long axis view, left ventricular end systolic
diameter (LVESD) was also measured. Shortening fraction was then calculated using the
formula SF(%) = [(LVEDD – LVESD)/LVEDD] x 100 (166).
55 | P a g e

Ejection fraction (EF) using Simpson’s biplane method: From the standard apical 4- and 2-
chamber views of the left ventricle, and using the analysis software’s built-in calculation
package, the endocardial borders of the LV cavity were manually traced at end-diastole and end-
systole to generate respective volumes in millilitres for each view. Biplane EF is then calculated
and provided as a percentage by the software (167).
Mean velocity of circumferential fibre shortening (mVCFc): Mean velocity of circumferential
fibre shortening is considered as a preload independent marker of LV systolic function which is
also adjusted for a given afterload. It is calculated using LV end-diastolic and end-systolic
circumference measured by manually tracing the endocardial borders of the LV cavity at
respective phase in the cardiac cycle in the parasternal short axis view at the level of papillary
muscle. It is then calculated using the formula mVCFc (circumference/sec) = (LVEDC –
LVESC)/LVEDC x ETc); where LVEDC and LVESC are left ventricular circumference in end-
diastole and end-systole respectively and ETc is the LV ejection time corrected for heart rate to
60 beats/seconds by dividing the measured ejection time from the pulse wave Doppler of the LV
outflow by square root of R-R interval measured from the simultaneously recorded
electrocardiographic tracings (168).
Mitral valve inflow was assessed by placing a pulse wave sample gate of 2 mm at the tip of the
mitral valve leaflets during diastole with the Doppler beam parallel to the inflow as visualized
using color Doppler echocardiography. Early (MvE), late (MvA) inflow velocities, their ratio
(MvE:MvA) and VTI were measured as for tricuspid valve inflow. In addition IVRT was
measured as the time lag between cessation of mitral valve inflow and start of flow out of the LV
outflow tract.
56 | P a g e

Myocardial velocities: Similar to the right ventricle, pulsed TDI was obtained by placing a pulse
wave sample gate of 2 mm on the basal segment of the LV free wall just below the lateral mitral
annulus. Peak systolic (s’), early diastolic (e’) and late diastolic (a’) velocities were then
measured. From the Doppler tracings, the time intervals including closing to opening of the
mitral valve (McOt’), IVRT’, duration of systole (systole’= beginning to the end of s’= LVET’)
and diastole (diastole’= beginning of e’ to end of a’) were obtained. As for the right ventricle, e’:
a’, MvE: e’, systole’: diastole’ and MPI’ [= (McOt’-LVET’): LVET’] were calculated. In
addition, s’, a’ and e’ were also measured using pulsed TDI for the interventricular septum by
placing the sample gate at its basal segment.
Speckle Tracking Echocardiography: Longitudinal strain analysis was carried out by obtaining
grey scale images of the left ventricle in three views (the LV apical four- two- and three-chamber
views) at a frame rate of 80 - 100 frames/second. As for the right ventricle, images were
optimized to visualize the myocardial walls and analysis was performed using the 2D STE
software (EchoPAC, version 11, GE Medical Systems). Briefly, the endocardial border was
manually traced at end-systole and the region of interest was narrowed to only include the LV
myocardium. Tracking was automatically performed, and the analysis was accepted after visual
inspection of all the segments and software confirmation of adequate tracking. If tracking was
suboptimal, the endocardial border was retraced. If satisfactory tracking was not accomplished
within 10 min, the non-tracking segments were excluded from analysis. Global peak longitudinal
strain (GLS) was then calculated by averaging all values of the segmental peak longitudinal
strain obtained from the 17 segments in three views (Figure 3.6) (133). Peak strain was defined
as peak value during the entire cardiac cycle as identified by the software (peak G values) (137).
57 | P a g e

For both the left and right ventricle, we chose to measure peak strain instead of end systolic
strain (obtained by manual tracing of each strain curve to the point of aortic valve closure) with
the premise that it would make measurements more user friendly by significantly reducing post
processing time and may minimize inter-rater variability by removing the need for manual
tracing of each strain curve. Further, for a random subset of 100 segments, we recorded and
compared end systolic strain values to the automated peak G values provided by the software and
found them to be not significantly different. The frame rate: heart rate ratio for all STE images
ranged from 0.65 to 0.90.
Figure 3.6: Speckle tracking echocardiography. Strain is measured in the three planes: four chamber, two chamber, and three chamber, and displayed in a bulls eye view with the three individual values and the global average. Figure adapted from Jain et al. J Pediatr. 2016 Nov 28. pii: S0022-3476(16)31231-8. doi: 10.1016/j.jpeds.2016.11.003.
3.6 Hemodynamic measurements
Changes in PVR were estimated by measuring pulmonary artery acceleration time (PAAT)
and pulmonary vascular resistance index (PVRI =RVET: PAAT); both of which have previously
58 | P a g e

been validated in adults and older children and are commonly used parameters in neonatal and
animal studies (169-172). PAAT and RVET were measured from the pulse wave Doppler tracing
of the main pulmonary artery obtained from the parasternal long axis view of the right
ventricular outflow tract with a 2-mm wide Doppler gate placed in the middle of the main
pulmonary artery at the level of the pulmonary valve (Figure 3.7). Further, as a surrogate
qualitative marker of RV systolic pressure, the curvature of the interventricular septum motion at
end-systole was assessed by visual inspection from a 2D parasternal short axis view acquired at
the level of the mitral valve (164). The septal motion was considered as ‘flat’ if there was
complete absence of concavity towards the left ventricle, and as per routine clinical practise, was
taken as an indication for the RV systolic pressure to be between 50% to 100% systemic systolic
pressure. Presence of concavity in the septal motion in end-systole towards the left ventricle
indicated RV systolic pressure to be below 50% systemic systolic pressure, while presence of
concavity towards the right ventricle indicated RV systolic pressure to be above systemic
systolic pressure (102).
59 | P a g e

Figure 3.7: A schematic representation showing measurements of pulmonary artery acceleration time (PAAT) and right ventricular ejection time (RVET) from pulse wave Doppler tracing of the main pulmonary artery obtained at the level of the pulmonary valve. Pulmonary vascular resistance index (PVRI) can then be calculated as shown.
Non-invasive calculation of peak right ventricular systolic pressure (RVSP) were made
whenever feasible, by measuring the peak velocity of tricuspid regurgitant jet using continuous
wave Doppler. The RVSP was then calculated using simplified modified Bernoulli’s equation as
RVSP = 4 x v2 + RAP; where v is the peak velocity of tricuspid regurgitant jet and RAP is right
atrial pressure which in these studies was always assumed to be 5 mmHg (173, 174).
Changes in cardiac outputs were assessed by measuring right ventricular stroke volume
(RVSV) and left ventricular stroke volume (LVSV) respectively using the standard formula [π x
(respective outflow tract diameter/2)2 x velocity time integral] (175). For RVSV, diameter was
measured at the level of pulmonary valve at peak systole from the parasternal long axis view of
the right ventricular outflow tract and VTI was obtained by tracing the pulse wave Doppler trace
obtained at the same level. For LVSV, measurements were performed just proximal to the level
of the aortic valve with diameter being measured from LV PLAX view in 2D image and VTI
60 | P a g e

from the pulse wave Doppler trace obtained from the standard apical-5-chamber view (166, 176).
Stroke volumes were multiplied by the observed heart rate to calculate right ventricular output
(RVO) and left ventricular output (LVO), which were indexed to body weight and expressed as
ml/min/kg. All flow related measurements were measured and averaged over at least 3
consecutive cardiac cycles.
3.7 Assessment of transitional shunts
The shunt at the level of patent ductus arteriosus (PDA) and patent formamen ovale (PFO)
was visualized using 2D and spectral color flow Doppler. When present, the shunt pattern was
characterized using pulse wave Doppler from the standard views - high parasternal view for
PDAs and subcostal view for PFOs. The shunt pattern was classified as shunting from systemic
to pulmonary circulation (i.e. left to right), pulmonary to systemic circulation (i.e. right to left) or
bidirectional. In cases of bidirectional shunts, the duration of right to left shunt was measured
and represented as a percentage of total duration of the cardiac cycle.
3.8 Patient selection and exposure
The inclusion and exclusion criteria as well as experimental exposure related on each study
are outlined in detail in specific Chapters.
3.9 Statistics
All data are presented as frequency (proportion), mean (± standard deviation, SD) or
median (interquartile range, IQR) unless otherwise stated. For chapter 4 and 5, results from D2
scans were compared with D1 using paired student’s t-tests for continuous variables and chi
square test or Fisher’s exact test for categorical variables as appropriate. For chapter 6, data from
4 sequential echocardiograms was analyzed using one way repeat measures ANOVA; while
61 | P a g e

heart function indices only measured on the 1st and 4th scans were compared using paired student
t-test. For chapter 7, comparison of cases with controls was performed using t-test for continuous
variables with parametric distribution or Mann Whitney U test for continuous variables with
non-parametric distribution, and chi square test or Fisher’s exact test for categorical variables as
appropriate. These being observational physiological studies, minimizing type 2 error rate was
considered more important than type 1 error; hence, Bonferroni correction for multiple
comparisons was not used and a p value < 0.05 was considered as significant.
All inter-observer measurement reliabilities were assessed using 20 randomly selected
studies. For intra-observer variability, one investigator performed two off-line analyses 12 weeks
apart to avoid recall bias while inter-observer variability was assessed by a second investigator
who was blinded to the measurements of the first investigator. Inter-observer agreement was
tested using intraclass correlation presented as intraclass correlation coefficient (ICC) and 95%
confidence interval, Bland-Altman (BA) analysis presented as 95% limits of agreement and
coefficient of variation (COV). COV was calculated for each parameter using the formula COV
(expressed as %) = (SD of absolute differences between repeated measurements/ arithmetic mean
of all repeated measurements) x 100. This was done to facilitate a more intuitive comparison
between reproducibility of different parameters. The lower the COV is, the lower the inter-
observer variability. We accepted a p value of < 0.05 as significant. The strength of linear
dependency between indices was examined by estimating Pearson or Spearman’s correlation
coefficient as and when appropriate. Only relationships with p values < 0.05 are shown. SPSS
statistics software version 21 was used to perform the analyses.
Additional study-specific details of statistical methods are provided in individual chapters.
62 | P a g e

Chapter 4: A Comprehensive echocardiographic protocol for assessing
neonatal right ventricular dimensions and function in the transitional Period:
normative data and Z scores*
*Reproduced in compliance with Elsevier’s Author User Rights policy as published in Journal of American Society
of Echocardiography (J Am Soc Echocardiogr. 2014;27(12):1293-304)
63 | P a g e

4.1 Introduction:
Right ventricular dysfunction is a strong predictor of outcomes in many adult and pediatric
diseases (1). It is recognized, in infants with PHT and various congenital heart defects involving
the right ventricle, that an RV functional assessment is an important aspect of care. Despite its
importance, the appraisal of RV function in routine clinical practice has largely remained
qualitative. The American Society of Echocardiography (ASE) has recently published separate
comprehensive guidelines for assessment of the right heart in adults (114), and in children (115).
The applicability of these guidelines to the newborn population is hampered by the limited
availability of normative data and the potential influence of the transitional circulation on these
measurements. Transition from fetal to postnatal life is characterized by major circulatory
changes, which includes a decrease in PVR, an increase in pulmonary blood flow and closure of
fetal shunts - PDA and PFO. Although these changes take place over the first 4-6 weeks after
birth, the most rapid alterations occur within the first few days of life. While research regarding
the use of echocardiography to quantify neonatal RV function is growing, there remains a
paucity of comprehensively acquired data, with even fewer studies looking at the effect of the
transitional circulation during the first 48 hours of age (62, 63, 104, 177). This is crucial as the
majority of critically ill newborns present during this period. Further, the majority of RV
functional parameters established for use in older children and adults are derived almost
exclusively from apical 4C view and hence can be influenced by interventricular septal motion,
which is often restrictive and variable during the first few days of life.
The primary objective of this study was to test the feasibility and reliability of a
comprehensive echocardiographic protocol, including novel indices independent of septal
motion, for quantifying RV dimensions and function in healthy term human neonates. This
64 | P a g e

protocol was used to establish normative data and calculate Z-scores for 2D measurements, TDI
and 2D STE parameters. Finally, we investigated the effect of early transitional changes on these
measurements by comparing results between days 1 and 2 of life. We hypothesized that in
healthy neonates, using a comprehensive approach, it was possible to image the neonatal right
ventricle from multiple views and reliably quantify RV dimensions and function. We further
hypothesized that the novel parameters established for this study would allow quantification of
size and function of the neonatal right ventricle independent of septal motion.
4.2 Additional methods
Inclusion and exclusion criteria: Healthy, term (gestational age 37 to 42 weeks), singleton
newborns with normal birth weight (BW) (between 10th to 90th percentiles for gestational age at
birth), born following an uncomplicated low risk pregnancy were considered eligible for
recruitment. Exclusion criteria were conditions which may alter the transitional circulation
and/or effect neonatal cardiac function during this period and included maternal diseases
(diabetes mellitus; preeclampsia; chorioamnionitis; antenatal diagnosis of placental dysfunction
defined by absent or reversed end-diastolic flow in umbilical arteries on fetal ultrasound; or the
prenatal use of antidepressant medications) and any newborn disease (evidence of a perinatal
depression defined for this study as umbilical cord pH < 7.0 and/or Apgar score of < 5 at 5
minutes of age; the need for active resuscitation at birth; admission to the neonatal intensive care
unit; any congenital malformation; documented episode of neonatal hypoglycemia or clinical
examination suggestive of genetic or cardiovascular abnormalities). We also intended to exclude
neonates with an incidental finding of a congenital heart defect on echocardiograms, except those
with a PFO, small PDA or mild peripheral pulmonary artery stenosis as these are considered
‘normal’ during the transitional period.
65 | P a g e

Exposure: The health records of infants receiving routine postnatal care in the Mother and Baby
Unit at Mount Sinai Hospital were screened and eligible families were approached for consent
within 12 hours of birth. A total of 50 healthy eligible neonates (pre-defined sample size for
convenience) were recruited between December 2011 and September 2012. Each infant
underwent two serial comprehensive evaluations - the first between 12 to 20 hours (D1) and a
second between 30 to 40 hours (D2) of life with a minimum interval of 18 hours between scans.
Each echocardiogram was performed using the study imaging protocol to enable measuring all
functional indices as described above. Blood pressure was recorded using a non-invasive
oscillometric method (DINAMAPR Pro 100, GE healthcare, Tampa, FL).
Additional statistical considerations:
Estimation of reference values and Z-scores: All echocardiographic measurements were assessed
for dependency to BW. Associations with infant length or body surface area were not explored
because of the concerns regarding the accuracy of length measurement in the newborns.
Regression models were empirically tested to optimize the goodness-of-fit between
echocardiographic measurements and BW. Linear (y = ax + b), allometric (y = axb), 2nd order
polynomial (y = ax2 + bx + c), and 3rd order polynomial (y = ax3 + bx2 + cx + d) models were
tested. Selection of the most adequate model for each echocardiographic measurement was based
on goodness-of-fit, on visual inspection of residual values, on fit diagnostic aid plots, and on fit
plots of the residual values over the independent variable by linear regression and polynomial
regression. Mathematical transformation of the dependent variable was only considered if the
distribution of the normalized echocardiographic measurement suggested significant departure
from the normal distribution. Preliminary analysis showed that the variance of the residual values
was not always homogenous across the range of BW (i.e. heteroscedasticity). However, weighted
66 | P a g e

regression approaches yielded clearly over-adjusted results (not shown). Therefore, weighted
regressions were not further explored.
For each echocardiographic measurement, the selected regression model was used to calculate
the predicted mean value according to BW. Residual values (observed measurement minus
predicted mean) were calculated and the SD of the residual values was computed. Z-scores were
then calculated as follows:
Z-Score = (Observed value − Predicted mean) / SD of residual values.
Finally, newly computed Z-scores were tested to ensure that residual association with BW (by
linear regression and polynomial regression) and significant departure from the standard normal
distribution (distribution histograms, box plots, and normal probability plots, and Shapiro-Wilk
Statistic) were not present.
4.3 Results:
Study population:
Fifty neonates (17 male) with a mean gestational age of 39.7 (± 1.2) weeks were included.
Twelve neonates were delivered by caesarian section. The mean cord pH was 7.23 (± 0.07) and
median Apgar score at 5 minutes was 9 (range 8 – 9). Two infants were noted to have premature
atrial contractions during the echocardiogram that were confirmed by a 12-lead
electrocardiogram. The mean time interval between the two scans was 19.9 ± 1.8 hours. Table
4.1 summarizes clinical and echocardiographic characteristics of the included neonates. A small
PDA was present in 44% of subjects on the first day of age which closed spontaneously in the
majority by the second day. An increase in PAAT suggested a decrease in PVR on day 2 vs. day
67 | P a g e

1 of age; which was also consistent with the decreased frequency of flat interventricular septal
motion in systole on day 2.
Table 4.1: Clinical and baseline echocardiographic characteristics during the first two days of life
Characteristic Day 1 Day 2 P
Weight (kg) 3.49 ± 0.44 3.30 ± 0.43 <0.01
Age at scan (hrs) 15 ± 2 35 ± 2 -
Systolic blood pressure (mmHg) 67 ± 8 68 ± 6 0.75
Diastolic blood pressure (mmHg) 39 ± 9 41 ± 7 0.32
Mean blood pressure (mmHg) 48 ± 8 51 ± 8 0.18
Heart rate (beats/min) 118 (108-128) 121 (110-140) 0.18
Patent ductus arteriosus, n (%) 22 (44) 2 (4) <0.001
Patent foramen ovale, n (%) 41 (82) 37 (74) 0.47
Right ventricular ejection time (ms) 216 ± 24 216 ± 23 0.89
Pulmonary artery acceleration time (ms) 49 ± 17 59 ± 15 <0.001
Interventricular septum flat at end systole, n (%) 16 (32) 6 (12) 0.03
Results presented as mean (± SD) or median (IQR).
Feasibility and reliability of RV measurements:
All RV dimensions were measurable from each of the 100 scans analyzed. STE-derived
GLS-4C and GLS-3C measurements were feasible in 94% of the scans. The RV lateral wall
could not be tracked in 2 subjects on D1 and in 4 on D2. The RV inferior wall was traceable in
all but 1 infant on D1 and 5 on D2. At least one wall was analyzable in 98% of scans while a
global GLS calculation was feasible in 90%. Measurements for tricuspid inflow velocities were
not taken in cases of complete fusion of TvE and TvA (10 scans on D1 and 9 on D2). Similarly,
myocardial diastolic velocity measurements were considered non-feasible when e’ and a’ were
indistinguishable (4 cases on D1 and 7 on D2). Remaining functional indices could successfully
be measured from all studies. Majority of parameters demonstrated low intra- and inter-observer
68 | P a g e

measurement variability (Table 4.2). The variability in measuring RV ESA in both views was
relatively higher than end-diastolic area. The biplane-FAC (global-FAC) calculations were less
variable than single-plane FAC-4C and FAC-3C. Tissue Doppler peak velocities were highly
reproducible while MPI’ was more variable.
Table 4.2: Intra- and inter-observer variability of echocardiographic RV measurements
Intra-observer Inter-observer
ICC*
(95% CI)
BA
95% LOA COV (%)
ICC*
(95% CI)
BA
95% LOA COV (%)
RV linear dimensions
B-4C (cm) 0.92 (0.80, 0.97) -0.21, 0.18 5.4 0.86 (0.69, 0.94) -0.26, 0.18 6.4
MC-4C (cm) 0.90 (0.76, 0.96) -0.26, 0.18 6.3 0.83 (0.62, 0.93) -0.21, 0.29 7.0
RVL (cm) 0.89 (0.75, 0.96) -0.25, 0.22 3.8 0.58 (0.21, 0.81) -0.32, 0.49 6.8
B-PLAX (cm) 0.87 (0.71, 0.95) -0.20, 0.22 4.5 0.66 (0.27, 0.86) -0.41, 0.22 6.7
RV cavity areas
EDA-4C (cm2) 0.93 (0.84, 0.97) -0.67, 0.55 6.7 0.86 (0.67, 0.94) -0.76, 0.82 8.7
ESA-4C (cm2) 0.95 (0.89, 0.98) -0.30, 0.35 4.9 0.74 (0.45, 0.89) -0.73, 0.74 10.5
EDA-3C (cm2) 0.87 (0.69, 0.95) -1.07, 1.02 7.8 0.85 (0.67, 0.94) -1.08, 0.85 7.3
ESA-3C (cm2) 0.81 (0.58, 0.92) -0.86, 0.86 10.2 0.80 (0.56, 0.91) -0.97, 0.87 11.0
RV functional indices
FAC-4C 0.82 (0.61, 0.92) -0.09, 0.07 16.7 0.51 (0.09, 0.77) -0.12, 0.13 25.0
FAC-3C 0.67 (0.33, 0.86) -0.10, 0.09 13.9 0.65 (0.29, 0.84) -0.13, 0.12 16.7
Biplane FAC 0.72 (-0.42, 0.88) -0.08, 0.06 13.3 0.76 (0.49, 0.90) -0.06, 0.06 10.0
TAPSE (cm) 0.97 (0.93, 0.99) -0.11, 0.11 3.4 0.52 (0.11, 0.78) -0.16, 0.22 10.9
s’ (cm/s) 0.96 (0.89, 0.98) -0.36, 0.55 3.7 0.94 (0.86, 0.98) -0.53, 0.67 4.9
e’ (cm/s) 0.97 (0.93, 0.99) -0.65, 0.60 3.8 0.52 (0.00, 0.85) -0.99, 0.69 5.0
a’ (cm/s) 0.99 (0.97, 1.00) -0.34, 0.48 2.7 0.77 (0.22, 0.93) -1.20, 0.91 7.0
IVCV’ (cm/s) 0.99 (0.97, 1.00) -0.25, 0.41 3.6 0.98 (0.96, 0.99) -0.48, 0.51 5.2
MPI’ 0.97 (0.92, 0.98) -0.08, 0.06 9.5 0.80 (0.56, 0.92) -0.13, 0.21 20.9
GLS-4C (%) 0.93 (0.78, 0.97) -4.42, 2.37 9.5 0.96 (0.89, 0.98) -3.65, 2.61 9.2
69 | P a g e

GLS-3C (%) 0.77 (0.50, 0.90) -5.11, 5.61 12.5 0.84 (0.63, 0.93) -5.16, 5.10 12.0
Global GLS (%) 0.89 (0.74, 0.96) -3.17, 2.30 7.0 0.87 (0.70, 0.95) -3.28, 2.90 8.0
SD standard deviation; ICC intraclass correlation coefficient; CI confidence interval; BA Bland-Altman; LOA limits of agreement; COV coefficient of variability; 4C apical 4-chamber view; 3C apical 3-chamber view; TVA tricuspid annulus; B/MC basal/mid-cavity diameter; RVL RV length; B-PLAX basal diameter in parasternal long axis view; EDA end diastolic area; ESA end systolic area; FAC fractional area change; TAPSE tricuspid annular plane systolic excursion; s’/e’/a’/IVCV’ peak systolic/early diastolic/late diastolic/isovolumetric contraction tricuspid annular velocities; MPI’ myocardial performance index; GLS peak longitudinal strain of lateral and inferior wall in 4C and 3C respectively; Global FAC = (FAC-4C + FAC-3C)/2; Global GLS = (GLS-4C + GLS-3C)/2; *p<0.05 for all parameters.
Echocardiographic RV dimensions in the transitional period:
Results obtained for RV dimensions parameters for each day are outlined in Table 4.3.
The mean basal antero-inferior diameter (B-PLAX) was larger than the mean B-4C and mean
EDA-3C was larger than the mean EDA-4C (p<0.001). We noted a small but significant increase
in some RV dimensions on D2 (MC-4C, B-PLAX and EDA-4C).
There was a modest but significant association between most RV dimension
measurements and BW; a simple linear regression was sufficient to describe their relationship.
The use of more complex models, e.g. allometric, polynomial, had a tendency to produce
noticeably over-adjusted regression curves. We therefore elected to use a linear model for all RV
dimension measurements. Z-scores can be computed with the beta estimate and the SD of
residual values presented in table 3 using the following equation:
𝑍𝑍 =𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀 𝑀𝑀𝑑𝑑𝑑𝑑𝑀𝑀𝑑𝑑𝑀𝑀𝑑𝑑𝑑𝑑𝑑𝑑 − [𝑑𝑑𝑑𝑑𝑖𝑖𝑀𝑀𝑀𝑀𝑖𝑖𝑀𝑀𝑖𝑖𝑖𝑖 + (𝑏𝑏𝑀𝑀𝑖𝑖𝑀𝑀 𝑀𝑀𝑀𝑀𝑖𝑖𝑑𝑑𝑑𝑑𝑀𝑀𝑖𝑖𝑀𝑀 × 𝐵𝐵𝐵𝐵)]
𝑆𝑆𝑆𝑆 𝑑𝑑𝑜𝑜 𝑀𝑀𝑀𝑀𝑀𝑀𝑑𝑑𝑀𝑀𝑀𝑀𝑀𝑀𝑟𝑟 𝑣𝑣𝑀𝑀𝑟𝑟𝑀𝑀𝑀𝑀𝑀𝑀
Z-scores were adequately distributed with little or no residual association with BW.
70 | P a g e

Table 4.3: Right ventricular dimensions and area measurements during the transitional period
Measurements
Day 1 Day 2
P-value for day 1 vs. day 2
Mean SD Intercept Beta estimate for BW
slope
SD of residual values
Mean SD Intercept* Beta estimate for BW slope*
SD of residual values*
RV linear dimensions
TVA (cm) 1.29 0.15 1.14 0.044 0.151 1.31 0.15 0.54
B-4C (cm) 1.71 0.17 1.20 0.146 0.158 1.74 0.21 0.31
MC-4C (cm) 1.55 0.19 0.86 0.197 0.167 1.71 0.20 1.12 0.168 0.183 <0.01
RVL (cm) 3.06 0.23 2.52 0.154 0.219 3.05 0.23 0.82
B-PLAX (cm) 2.06 0.24 1.89 0.048 0.243 2.24 0.29 1.70 0.153 0.279 <0.01
RV cavity areas
EDA-4C (cm2) 4.11 0.69 1.16 0.841 0.581 4.32 0.64 1.16 0.841 0.581 0.04
ESA-4C (cm2) 3.02 0.57 -0.11 0.893 0.418 3.15 0.54 0.12
EDA-3C (cm2) 6.44 1.18 1.62 1.373 1.014 6.64 0.86 0.29
ESA-3C (cm2) 3.91 0.68 1.58 0.667 0.607 4.10 0.70 0.10
SD standard deviation; BW birth weight; 4C RV-focused apical 4-chamber view; TVA tricuspid valve annulus; B/MC basal/mid-cavity diameter; RVL RV length; B-PLAX basal diameter in parasternal long axis view; EDA end diastolic area; ESA end systolic area. *Only presented if mean values differ significantly from Day 1.
71 | P a g e

Echocardiographic RV functional measurements in the transitional period:
Results obtained for RV functional parameters for each day are outlined in Tables 4.4 and 4.5.
FAC-3C values were higher than FAC-4C on both days (Figure 4.1). The mean difference
between two FAC measurements was 12.2 ± 9.3% on day 1 and 11.9 ± 10.9 on day 2.
Measurement of GLS was similar for both lateral and inferior walls. Apart from a very small but
significant drop in e’, no changes in RV functional parameters were observed between day 1 and
day 2.
Unlike RV dimension measurements, most functional measurements were not
significantly associated with BW, with the exception of FAC. Z-scores for RV functional
measurements which did not show an association with BW, are estimated with the mean and SD
presented in Table 4.5 using the following equation:
𝑍𝑍 =𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀 𝑖𝑖𝑀𝑀𝑀𝑀𝑀𝑀𝑑𝑑𝑀𝑀𝑖𝑖𝑀𝑀𝑀𝑀 − 𝑑𝑑𝑀𝑀𝑀𝑀𝑑𝑑
𝑆𝑆𝑆𝑆
Most RV functional measurements had normal or near normal distribution with the
exception of systole’: diastole’ and MPI’. systole’: diastole’ ratio adopted a log-normal
distribution. Consequently, a log transformation was necessary to obtain a normally distributed
Z-score, which can be estimated with the mean and SD of the log-transformed value in Table 5
using the following equation:
𝑍𝑍 =Ln(𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀𝑀 𝑖𝑖𝑀𝑀𝑀𝑀𝑀𝑀𝑑𝑑𝑀𝑀𝑖𝑖𝑀𝑀𝑀𝑀) −𝑑𝑑𝑀𝑀𝑀𝑀𝑑𝑑
𝑆𝑆𝑆𝑆
MPI’ distribution was very different on D1 compared to D2; such departure from the normal
distribution prevented the computation of a valid Z-score.
72 | P a g e

Table 4.4: Right ventricular fractional area change during transitional period
Measurements
Day 1 Day 2
P-value for day 1 vs. day 2
Mean SD Intercept* Beta estimate for BW slope*
SD of residual values*
Mean SD
FAC-4C (%) 0.26 0.072 0.48 -0.063 0.0667 0.27 0.081 0.68
FAC-3C (%) 0.39 0.068 0.30 0.025 0.0670 0.38 0.058 0.74
Global-FAC (%)
0.33 0.053 0.40 -0.021 0.0520 0.33 0.042 0.89
SD standard deviation; BW birth weight; 4C apical 4-chamber view; 3C apical 3-chamber view; FAC fractional area change; Global FAC=(FAC-4C + FAC-3C)/2. *Only presented for Day 1 as mean values were similar on both days.
Figure 4.1: A box plot graph of fractional area change (FAC) measurements obtained from RV-4C and RV-3C view on day 1 and 2 of age. FAC-3C was significantly greater than FAC-4C on both days.
73 | P a g e

Table 4.5: Right ventricular functional measurements in the transitional period
Measurements
Day 1 Day 2
p value Mean SD Mean SD
Systolic function
TAPSE (cm) 0.92 0.14 0.91 0.13 0.69
s’ (cm/s) 6.55 1.16 6.54 1.09 0.95
IVCV’ (cm/s) 4.88 1.52 4.84 1.39 0.95
GLS-4C (%) 21.17 5.25 21.27 5.35 0.79
GLS-3C (%) 21.38 4.36 20.68 4.12 0.40
Global GLS (%) 21.21 3.93 21.16 4.21 0.72
Diastolic function
TvE (cm/s) 45.60 9.48 44.02 7.96 0.16
TvA (cm/s) 52.09 10.49 53.49 8.64 0.36
TvE: TvA 0.89 0.17 0.83 0.13 0.07
e’ (cm/s) 7.99 1.57 7.33 1.26 <0.01
a’ (cm/s) 8.27 1.57 8.01 1.28 0.45
e’/a’ 0.99 0.23 0.93 0.21 0.09
TvE: e’ 5.85 1.34 6.19 1.36 0.24
IVRT’(ms) 41.38 17.09 43.32 15.55 0.51
Global function
MPI’ 0.42 0.15 0.42 0.12 0.89
systole’: diastole’ 1.08 0.26 1.11 0.31 0.29
Log [systole’: diastole’]
0.05 0.22 0.07 0.25 -
SD standard deviation; 4C apical 4-chamber view; 3C apical 3-chamber view; TAPSE tricuspid annular plane systolic excursion; s’/e’/a’/IVCV’ systolic/early diastolic/late diastolic/isovolumetric contraction tricuspid annular velocities; GLS peak longitudinal strain of lateral and inferior wall in 4C and 3C respectively; TvE: TvA early/late
74 | P a g e

tricuspid inflow velocities; IVRT’ isovolumetric relaxation time; MPI’ myocardial performance index; systole’: diastole’ ratio of duration of systole to diastole; Global GLS = (GLS-4C + GLS-3C)/2.
Systolic functional parameters measured using the RV-4C view demonstrated weak to
modest positive linear correlations (Table 4.6), with the correlation coefficient of 0.45 being the
highest between s’ and GLS-4C. Comparing indices acquired from the RV-3C view with those
measured from the RV-4C view revealed similar results for GLS-3C with GLS-4C (r=0.45,
p<0.001) and GLS-3C with TAPSE (r=0.23, p=0.03). FAC measurements did not correlate
linearly with each other or with any other functional parameters.
Table 4.6: Linear correlations examined for right ventricular functional indices derived from apical 4C view
TAPSE s’ GLS-4C FAC-4C
TAPSE - 0.29 (0.004) 0.29 (0.005) -0.01 (0.88)
s’ - - 0.43 (<0.001) -0.06 (0.53)
GLS-4C - - - 0.07 (0.48)
Data presented as Pearson’s correlation coefficient (p value). RV right ventricle; TAPSE tricuspid annular plane systolic excursion; s’ systolic tricuspid annular velocity; GLS-4C peak longitudinal strain for RV lateral wall; FAC-4C fractional area change in apical 4-C view.
4.4 Discussion:
Clinical significance: In this study we described a comprehensive echocardiographic protocol for
imaging the right ventricle in neonates and established normal values for various RV dimensions
and functional parameters. Preservation of RV function is recognized as a critical prognostic
factor in the management of cardio-pulmonary disorders of adults, in particular PAH (8, 84,
178). Cardio-pulmonary disorders are not uncommon during the newborn period. Acute PHT has
been reported as a primary diagnosis in up to 4% of admissions in tertiary neonatal intensive care
units with a reported mortality ranging from 5-20% (33, 34). Many chronic neonatal respiratory
75 | P a g e

illnesses such as chronic lung disease or congenital diaphragmatic hernia are complicated by
cPHT and high rates of adverse patient outcomes (41, 128, 179). RV function may also be of
critical importance in various congenital heart defects. It is plausible that early recognition of RV
compromise may modify the clinical outcomes for this vulnerable patient population. Clinical
appraisal of RV health in neonates is challenging, as clinical symptoms and signs are non-
specific and investigations such as cardiac catheterization and CMRI are generally not feasible.
2D echocardiography is considered to be the gold standard for the assessment of heart function
in this population, with research emphasis beginning to shift towards RV performance. The
establishment of a comprehensive normative dataset in this study, attained in a systematic
manner, is an important and timely initial step towards examining the relevance of RV
physiology in neonatal disease states.
Although recent reports have highlighted the feasibility of quantifying RV function in
healthy neonates, the majority of these studies used either TAPSE or TDI-derived myocardial
velocities (60, 62, 63, 106, 108, 109, 153, 154). We demonstrate the practicality of employing a
more integrated and comprehensive approach using different 2D echocardiographic views and
emerging techniques for RV assessment in neonates. This approach allowed us to provide
comparative reliability data as well as normative ranges for various measures of RV dimensions
and function. Further, we demonstrated the feasibility of acquiring the RV 3-chamber view and
related novel functional measurements - FAC-3C and GLS-3C.
Rationale for using ‘newer’ indices: The majority of previously established echocardiographic
RV indices for adults have been derived from the RV-4C view, which provides a coronal cut
through the RV. Both 4C-derived FAC and RV linear dimensions are likely to be heavily
influenced by interventricular septal motion, which is often restricted and variable during the
76 | P a g e

early neonatal period (164). TAPSE, TDI-derived tricuspid annular velocities and lateral wall
GLS are measured from the same region of the RV and may not always reflect global RV
performance. Adding additional views may help to overcome some of these limitations. We
hypothesized that, as B-PLAX diameter is independent of septal motion, it may be more
reflective of changes in RV dimensions in newborns. We also observed that FAC values
obtained using RV-3C view were significantly higher than those obtained from 4C view for both
days 1 and 2 of age. As we hypothesized, the RV-3C view may be more reflective of ‘true’ RV
systolic function as it is measured independent of the septum. Another possible explanation
could be that FAC-3C represents systolic function of a different RV region, the RV
infundibulum. The finding that GLS measurements obtained from both RV walls (GLS-4C and
GLS-3C) were not different suggests lack of interference from septal motion to be the primary
reason for higher FAC-3C values. In addition, it was our qualitative experience that the RV
cavity visualized in the RV-3C view had less trabeculations than the RV-4C, which may explain
the superior reliability observed for FAC-3C when compared to FAC-4C in our study. Recent
data have shown that the RV infundibulum is inherently different from the other regions of the
right ventricle (8, 84). Further, we measured and generated normative data for IVCV as it has
recently been described to correlate with invasive measurements of RV contractility in adults
(180). Although it is tempting to hypothesize that use of these indices may provide for a more
global functional appraisal and may facilitate investigations into differential impact of
pathologies and treatments on different regions of the right ventricle, additional testing is
required in a variety of disease populations.
Reproducibility testing: In this study we used three different methods to investigate the
reproducibility of these measurements – intraclass correlation coefficient (ICC), Bland Altman
77 | P a g e

analysis (BA) and coefficient of variability (COV). This was done to ensure a comprehensive
analysis as each method has its strengths and weaknesses. Though ICC is easier to interpret, it
can occasionally be misleading as it compares the variability in repeated measurements with the
overall variability in the study sample. In cases of measurements where the overall variability in
study population is low, ICC may falsely show poor reproducibility and vice versa. This is amply
demonstrated in the results for e’ and MPI’. The ICC for e’, which had low sample variation,
demonstrated poor reproducibility but the reproducibility was excellent when assessed using
COV/BA. On the other hand, MPI’, which varied widely between study patients appeared to
have a good ICC but, showed poor reproducibility on BA/COV. Though calculating limits of
agreement using BA analysis provides the most comprehensive information, its interpretation
and inter parameter comparison is not always intuitive. This is because the results are usually
expressed in units specific to the measurement being evaluated. In contrast, COV allows easy
comparison between different parameters as results are expressed in percentage and are
independent of specific units.
Many previous studies have used pooled images from the right ventricle and the left
ventricle for estimation of inter-observer reliability of certain measurements. This could be
misleading, as the right ventricle, owing to its complex shape and anterior location, is
considerably more challenging to image. The ASE guidelines for targeted neonatal
echocardiography has recommended the use of higher frequency ultrasound transducers (8-12
MHz), to help with the known limitation of inferior near-field resolution of ultrasound, which is
expected to be accentuated in newborns, owing to a thin chest wall (181). Being the most
anterior cardiac structure, this may be especially relevant for imaging the right ventricle. Only
two studies have reported RV-specific measurement reproducibility in neonates (60, 182). The
78 | P a g e

superior reproducibility for myocardial velocities in our study in comparison to Joshi et al (COV
ranging from 2.7-7% vs. 15-24%) could in part be explained by our use of higher resolution
transducers and by the fact that half of the patients in their study were preterms who, as
described earlier, are more difficult to scan. Recently, Levy and coworkers reported a lower
COV than reported in our study for measuring STE-derived RV lateral wall GLS in preterm
infants (COVs of 2.7% and 3.9% vs. 9.5% and 9.2% for intra- and inter-observer respectively)
(60). This may be explained by the rigorous criteria applied in their study for assessment of
image quality, resulting in the exclusion of 16% of scans. We attempted tracking on all acquired
scans and were able to perform GLS-4C measurements in 94% with a COV of <10%. Contrary
to all other parameters investigated, we found that the inter-observer measurement bias was
significant for FAC-4C and MPI’ measurements. This could be due to inherent subjectivity
associated with performing these measurements; specifically, delineating the endocardial borders
in end-systole in a heavily trabeculated neonatal right ventricle and identifying the edges of
tissue Doppler waves. Interestingly, calculation of global-FAC resulted in a noticeable
improvement in inter-observer reproducibility. Conversely, MPI’ measurements showed wide
variation between days with no clear pattern, making calculation of Z-scores impractical and
suggesting against the use of MPI’ for RV assessment in neonates.
Among the indices reported in this study, TVA, trans-tricuspid flow profile, TDI-derived
myocardial velocities and TAPSE, are the only functional indices for which good quality
normative data exists for neonates (62, 63, 130, 183). Our data for these indices were comparable
to previously published results, thus supporting the validity of our study population.
Furthermore, we found that the majority of indices of RV systolic function measured in this
study, demonstrated statistically significant linear correlations. Although these correlations were
79 | P a g e

weak to modest and of uncertain clinical significance, it provided circumstantial evidence
supporting the appropriateness of our methods in eliciting these ‘newer’ indices. Interestingly,
FAC estimated from either views did not correlate with each other or with other indices. This
could suggest the unreliability of FAC measurements, or perhaps, FAC represents a ‘different’
aspect of RV systolic function as FAC is derived from cavity dimensions while all other
parameters are derived from the myocardium. Nonetheless, FAC measurements showed
relatively wide standard deviations and high inter-observer bias, which may limit its clinical
utility in this population.
Deformation measurements: Although they are not inter-changeable, two methods currently exist
for measuring myocardial wall strain. Contrary to previous neonatal studies, we chose not to
utilize TDI-derived strain measurements, but rather employ STE to measure GLS for the RV
walls. Measurements obtained using STE are independent of the angle of the ultrasound beam
and of the shape of the myocardial wall (133). To avoid errors from dividing a short neonatal
myocardial wall into segments, we calculated an overall GLS for the lateral and inferior walls, to
generate a ‘global’ RV-GLS. We chose not to measure strain rate in this study. STE, in contrast
to TDI, uses relatively low frame rates and though this does not significantly influence strain
measurements, because the software determines strain rate by measuring the change in speckle
position frame by frame, this could lead to under sampling and therefore an underestimate of
peak strain rate. This problem is likely to be accentuated in neonates given their higher heart
rates. Further, it’s been shown that while TDI and STE derived longitudinal strain measurements
are comparable in children; the strain rate measurements derived using STE are much lower than
TDI and have poor inter-rater reliability (184). The relative benefits of using STE-derived strain
and strain rate in neonates need further investigation.
80 | P a g e

Effect of postnatal transition: Another consideration while designing this study was to
investigate the effect of physiological circulatory alternations associated with the transition to
postnatal life. This was important for the clinical applicability of our data. Contrary to
expectations, we found no increase in RV GLS from day 1 to day 2 of life, in spite of a reduction
in PVR. There could be several explanations for this finding. First, the decrease in PVR under
physiological conditions may not be large enough to affect STE-derived GLS. Second, the
relatively immature contractile properties of the neonatal myocardium may be less affected by
changes in loading conditions. Lastly, it is plausible that the reduction in preload secondary to
physiological diuresis expected to occur in the first few days of life in healthy neonates negated
the effect of changes in PVR on RV deformational indices. Converse to the effect of changes in
afterload, a drop in preload is expected to lower RV GLS. Indeed, as expected, neonates enrolled
in this study demonstrated weight loss on day 2 of life ranging from 0.6% to 9.3% [mean (±SD)
= 5.6 (± 2.1) %]. We confirm that in healthy neonates, ‘normal’ changes in RV loading
conditions during early postnatal life had no appreciable effect on quantitative echocardiographic
measures of RV function. Mori et al also reported no differences when they compared TDI-
derived myocardial velocities between healthy neonates < 24 hours old (n = 130) with those
between 1-7 days of life (n = 135) (108). We did observe a small increase in some RV
dimensions on day 2 of life. We speculate that this could have been explained by an increase in
left to right shunting of blood across the PFO associated with the reduction in right-sided
pressures on day 2 of life. Although quantitative echocardiographic measurement of shunt
volume was not feasible to test this hypothesis, persistence of a PFO in most infants is highly
suggestive. Nevertheless, as the magnitude of the observed change was small, this finding is
unlikely to be clinically significant.
81 | P a g e

In conclusion, a comprehensive, quantitative RV appraisal using 2D echocardiography is
feasible in neonates and should include measurements of its dimensions and function using
multiple 2D views. We propose that a practical echocardiographic protocol should include
measurement of posterior basal diameter in addition to the conventional apical RV-4C view
derived linear dimensions. Further, RV functional assessment should include parameters which
demonstrated the least inter-observer measurement bias – TAPSE, myocardial velocities, GLS of
the lateral and inferior walls and global GLS. To reduce measurement bias, FAC, when used,
should be measured from both the RV-3C and RV-4C views to generate a global FAC. RV
posterior basal diameter and parameters obtained from RV-3C view, may provide novel indices
for neonatal RV assessment which are independent of septal motion. The normative data
established in this study may provide a reference for future comprehensive investigations into
RV physiology in neonates.
82 | P a g e

Chapter 5: Left ventricular function in healthy term neonates during the
transitional period*
*Reproduced in compliance with Elsevier’s Author User Rights policy as published in the Journal of Pediatrics (J
Pediatr. 2016 Nov 28. pii: S0022-3476(16)31231-8).
83 | P a g e

5.1 Introduction
Impaired LV function is a known association of many disorders of the early neonatal
period, including infants of diabetic mothers, birth asphyxia, PPHN, sepsis, and intrauterine
growth restriction (155, 157, 185-187). Two-dimensional echocardiography is considered the
clinical reference investigation to evaluate LV size and function in neonates. Traditionally, the
most common echocardiographic methods employed to objectively assess LV systolic function
are, M-mode derived shortening fraction (SF) and B-mode derived ejection fraction (EF) using
Simpson’s bi-plane method, both of which are derived from LV cavity dimensions. Although
these methods provide a simple index of LV function and size, their utility in the first few days
of age is hampered by physiological changes in interventricular septal motion and LV geometry
(164). This is due to the progressive increase in SVR, decrease in PVR and decrease in LV
preload with closure of the PDA during this period. Further, SF measures change in LV cavity
dimension at a single point in one plane, which makes it highly operator dependent and not
always reflective of global LV function.
TDI and STE are parameters which assess regional and global LV function by directly
measuring muscle wall characteristics rather than cavity dimensions. TDI is used to measure the
velocity of muscle movement in systole and diastole of the LV free wall and septum, as well as
the timing of cardiac events in a cardiac cycle (188). STE is used to measure LV longitudinal
deformation which is expressed as percentage change in muscle length in systole compared to
end diastole (strain), as well as provide a measure of the speed with which this deformation
occurs (strain rate) (189). Although individual quantitative measure of LV function have been
shown to be feasible in recent neonatal studies (106, 153-155, 157), LV evaluation remains
largely qualitative in neonatal practice. This may reflect a paucity of data regarding normal
84 | P a g e

values and relative measurement reliability of conventional and newer echocardiographic
methods. Further, it is not known whether normal values for these indices change over the first
few days of life (147).
We aimed to characterize LV function with a comprehensive echocardiographic protocol
that incorporates conventional, TDI and STE in order to compare measurement reliability,
establish reference values, and determine their maturational patterns during the early neonatal
transitional period.
5.2 Additional methods
The inclusion and exclusion criteria as well as exposure was similar to that of Chapter 4,
and for ease of reference is reproduced below.
Inclusion and exclusion criteria: Healthy, term (gestational age 37 to 42 weeks), singleton
newborns with normal birth weight (BW) (between 10th to 90th percentiles for gestational age at
birth), born following an uncomplicated low risk pregnancy were considered eligible for
recruitment. Exclusion criteria were conditions which may alter the transitional circulation
and/or effect neonatal cardiac function during this period and included maternal diseases
(diabetes mellitus; preeclampsia; chorioamnionitis; antenatal diagnosis of placental dysfunction
defined by absent or reversed end-diastolic flow in umbilical arteries on fetal ultrasound; or the
prenatal use of antidepressant medications) and any newborn disease (evidence of a perinatal
depression defined for this study as umbilical cord pH < 7.0 and/or Apgar score of < 5 at 5
minutes of age; the need for active resuscitation at birth; admission to the neonatal intensive care
unit; any congenital malformation; documented episode of neonatal hypoglycemia or clinical
examination suggestive of genetic or cardiovascular abnormalities). We also intended to exclude
neonates with an incidental finding of a congenital heart defect on echocardiograms, except those
85 | P a g e

with a PFO, small PDA or mild peripheral pulmonary artery stenosis as these are considered
‘normal’ during the transitional period.
Exposure: The health records of infants receiving routine postnatal care in the Mother and Baby
Unit at Mount Sinai Hospital were screened and eligible families were approached for consent
within 12 hours of birth. A total of 50 healthy eligible neonates (pre-defined sample size for
convenience) were recruited between December 2011 and September 2012. Each infant
underwent two serial comprehensive evaluations - the first between 12 to 20 hours (D1) and a
second between 30 to 40 hours (D2) of life with a minimum interval of 18 hours between scans.
Each echocardiogram was performed using the study imaging protocol to enable measuring all
functional indices as described above. Blood pressure was recorded using a non-invasive
oscillometric method (DINAMAPR Pro 100, GE healthcare, Tampa, FL).
Additional statistical considerations: The strength of linear dependency between infant’s
gestational age at birth and weight on the day of the scan and LV dimensions and functional
indices was examined by estimating Pearson or Spearman correlation coefficients as appropriate.
5.3 Results
The study population’s baseline demographic characteristics were as listed in Chapter 4.
In brief, the study involved 50 healthy term neonates receiving routine postnatal care in the well
Mother and Baby Unit. The mean ± SD gestation and BW was 39.3 ± 1.2 weeks and 3.5 ± 0.44
kg respectively. Sequential scans were performed at 15 ± 2 hours [range 12 – 19] (D1) and 35 ±
2 hours [range 30 – 40] (D2) of age; with a mean time interval of 19.9 ± 1.8 hours. Weight on D2
was significantly lower (3.3 ± 0.4 Kg, p<0.001) with a mean weight loss of 5.6 ± 2.1%. There
was no difference in heart rate [118 (108 – 128) vs. 121 (110 – 140); p=0.20)], systolic blood
86 | P a g e

pressure [(67 ± 8 vs. 68 ± 6); p=0.75] or diastolic blood pressure [(39 ± 9 vs. 41 ± 7); p=0.32]
between two time points. Small restrictive PDAs were present in 22 (44%) of subjects on the
first day of age, remaining patent in only 2 infants (4%) by the second day (p<0.001), while
patent foramen ovale was present in 41 (82%) and 37 (74%) neonates on D1 and D2 respectively
(p=0.47).
LV Dimensions during the Transitional Period
LV dimensions were measurable from all scans (Table 5.1). With the exception of a
slight reduction in LV basal diameter on D2, there was no difference in any of the measurements
between the two time points. A mild to moderate linear correlation was observed between birth
weight and the majority of LV dimensions. There was no difference in dimensions between
males vs. females and scans with PDA open vs. closed (data not shown).
Table 5.1: LV dimensions on days 1 and 2 of age in healthy term neonates
Correlation with weight
Correlation with weight
D2 vs. D1
Variable D1 r p D2 r p p
MV annulus 0.99 ± 0.09 0.29 0.04 0.99 ± 0.08 0.10 0.50 0.73
LV basal diameter 1.91 ± 0.13 0.46 <0.01 1.84 ± 0.14 0.44 <0.01 <0.01
LV length (4C) 3.08 ± 0.26 0.30 0.04 3.07 ± 0.26 0.24 0.10 0.77
Aortic Diameter 0.69 ± 0.06 0.30 0.04 0.69 ± 0.05 0.44 <0.01 0.77
LVEDD (PLAX) 1.79
(1.64 – 1.92)
0.44 <0.01 1.74
(1.65 – 1.87)
0.42 <0.01 0.17
LVEDD (SAX) 1.73 ± 0.23 0.42 <0.01 1.72 ± 0.26 0.49 <0.01 0.91
LVEDC (SAX) 7.61 ± 0.73 0.49 <0.01 7.59±0.67 0.55 <0.01 0.79
Values are presented as mean ± SD or medians (IQR). All units are in centimetres. MV: Mitral Valve; LV: left ventricle; 4C: 4 Chamber; LVEDD: left ventricular end diastolic diameter; PLAX: parasternal long axis view; SAX: parasternal short axis view; LVEDC: left ventricular end diastolic circumference.
LV Function during the Transitional Period
87 | P a g e

All measurements were feasible from each scan except STE in 10% images on D1 (15
out of 150 images; 4 in the four-chamber, 6 in the two chamber and 5 in the three chamber) and
21% images on D2 (32 out of 150 images; 10 in the four-chamber, 9 in the two-chamber and 13
in the three-chamber). With the exception of s’ (Figure 5.1) and mitral valve VTI, all measured
functional indices remained unchanged on D2 (Table 5.2, 5.3). All myocardial velocities were
lower in the septum than respective values for the LV free wall on both days (p < 0.01). There
was no linear correlation between gestation and birth weight with any of the functional
parameters. There was no difference observed between males vs. females, or between scans with
PDA vs. no PDA (data not shown).
Figure 5.1: Peak systolic myocardial velocity in LV free wall and interventricular septum on day 1 and day 2 of life in healthy term neonates.
88 | P a g e

Table 5.2: LV systolic function parameters on days 1 and 2 of age in healthy term neonates
Variable D1 D2 p
Shortening Fraction (%) 39 ± 7 39 ± 8 0.91
mVCF (circ/sec) 1.79 (1.55 – 2.10) 1.89 (1.55 – 2.08) 0.34
Ejection Time (ms) 217 ± 22 212 ± 18 0.15
Systolic Time (ms) 188 (172 – 203) 184 (172 – 195) 0.74
Ejection Fraction (%) – Simpson’s
Two-Chamber 56 ± 9 54 ± 8 0.24
Four Chamber 54 ± 9 53 ± 9 0.38
Biplane 55 ± 7 53 ± 6 0.26
Tissue Doppler s` (cm/s)
Lateral Wall 4.9 ± 0.8 4.6 ± 0.6 <0.01
Septal 3.6 ± 0.6 3.5 ± 0.5 0.04
Peak Longitudinal Strain (%)
Four Chamber - 21.2 ± 2.6 - 21.1 ± 2.2 0.91
Two Chamber - 22.5 ± 2.9 - 22.1 ± 3.0 0.75
Three Chamber - 21.5 ± 2.7 - 20.4 ± 2.5 0.14
Global - 21.7 ± 1.9 - 21.2 ± 1.8 0.23
Peak Longitudinal Strain Rate (1/s)
Four Chamber 2.10 ± 0.44 1.98 ± 0.34 0.15
Two Chamber 2.19 ± 0.39 2.32 ± 0.52 0.09
Three Chamber 2.12 ± 0.43 2.20 ± 0.48 0.53
Global 2.05 (1.90 – 2.28) 2.17 (1.93 – 2.43) 0.27
mVCF: Mean velocity of circumferential fibre shortening; Ejection time was measured using pulsed wave Doppler. Systolic time was measured as the duration of the s` wave using tissue Doppler imaging. Longitudinal strain and strain rate were measured using 2D speckle tracking echocardiography.
Table 5.3: LV diastolic and global function parameters on days 1 and 2 of age in healthy term neonates
Variable D1 D2 p
Pulsed Wave Doppler
Mitral Valve E wave (cm/s) 55.9 ± 8.3 55.7 ± 8.9 0.84
Mitral Valve A wave (cm/s) 50.6 ± 8.2 49.7 ± 9.2 0.45
E:A ratio 1.1 (1.0 – 1.2) 1.1 (0.9 – 1.3) 0.99
Velocity Time Index 9.1 ± 1.5 8.6 ± 1.7 0.02
Isovolumic Relaxation Time (ms) 54 (44 – 68) 55 (46 – 65) 0.77
89 | P a g e

Tissue Doppler - Lateral Wall
e’ (cm/s) 6.7 ± 1.4 6.5 ± 1.2 0.29
a’ (cm/s) 5.5 ± 1.3 5.4 ± 1.3 0.62
e’:a’ 1.3 ± 0.4 1.3 ± 0.4 0.98
Isovolumic Relaxation Time (ms) 53 ± 12 52 ± 10 0.57
Diastolic time (ms) 199 ± 42 195 ± 44 0.66
E:e`ratio 8.7 ± 2.5 8.9 ± 2.8 0.59
Tissue Doppler - Septum
e’ (cm/s) 4.7 ± 1.1 4.8 ± 0.9 0.32
a’ (cm/s) 4.2 ± 0.8 4.4 ± 0.8 0.32
e’:a’ 1.1 (0.9 – 1.3) 1.1 (0.9 – 1.3) 0.85
Longitudinal Strain Rate (1/s)
Two Chamber Early SR 2.92 ± 0.69 2.96 ± 0.63 0.67
Two Chamber Late SR 2.09 ± 0.59 2.22 ±0.60 0.22
Three Chamber Early SR 3.21 ± 0.64 3.06 ± 0.63 0.16
Three Chamber Late SR 2.03 ± 0.66 2.12 ± 0.69 0.70
Four Chamber Early SR 3.12 ± 0.79 3.09 ± 0.53 0.53
Four Chamber Late SR 2.12 ± 0.75 2.14 ± 0.56 0.94
Global Function Parameters
Left ventricular output (mls/min/kg) 128 ± 28 137 ± 28 0.11
Systole: diastole (Pulsed Wave) 0.79 (0.69-0.90) 0.82 (0.70 – 0.98) 0.17
Systole’: diastole’ (Tissue Doppler) 0.98 ± 0.24 0.98 ± 0.19 0.90
Myocardial Performance Index 0.61 (0.53 – 0.70) 0.61 (0.54 – 0.70) 0.80
Measurement Reliability of LV measurements
Overall, all measured indices demonstrated acceptable intra- and inter-observer
measurement reliability (Table 5.4), with longitudinal strain faring better than strain rate (Figure
5.2) as well as conventional measures of FS and EF.
Table 5.4: Intra- and inter-observer variability of left ventricular size and functional measurements
Variable Intra-observer Variability Inter-observer variability ICC*
(95% CI) Mean Bias (95%CI)
COV (%)
ICC* (95% CI)
Mean Bias (95%CI)
COV (%)
90 | P a g e

LV Dimensions MV Annulus 0.97
(0.92 – 0.99) -0.01 (-0.09 – 0.07) 4 0.86
(0.44 – 0.95) -0.05 (-0.18 – 0.09) 7
Basal diameter 0.86 (0.68 – 0.95)
0.01 (-0.16 – 0.18) 5 0.71 (-0.19 – 0.92)
0.14 (-0.10 – 0.38) 7
Length 0.89 (0.73 – 0.96)
0.01 (-0.24 – 0.25) 4 0.88 (0.70 – 0.95)
-0.02 (-0.33 – 0.29) 5
LVEDD 0.97 (0.93 – 0.99)
0.00 (-0.08 – 0.08) 2 0.97 (0.93 – 0.99)
-0.01 (-0.13 – 0.10) 3
Ao diameter 0.93 (0.81 – 0.97)
0.01 (-0.03 – 0.06) 4 0.87 (0.67 – 0.95)
-0.01 (-0.07 – 0.05) 5
LV Functional Indices – Conventional SF 0.92
(0.80 – 0.97) -1 (-8 – 7) 10 0.93
(0.83 – 0.97) 2 (-5 – 8) 9
EF 0.87 (0.67 – 0.95)
-1 (-9 – 7) 6 0.71 (0.24 – 0.89)
4 (-7 – 15) 9
MvE 0.94 (0.84 – 0.98)
-1.41 (-7.24 – 4.43) 6 0.94 (0.82 – 0.98)
2.80 (-3.52 – 9.13) 6
MvA 0.98 (0.96 – 0.99)
-0.80 (-5.36 – 3.76) 5 0.97 (0.92 – 0.99)
1.12 (-4.57 – 6.81) 6
Aortic VTI 0.97 (0.93 – 0.99)
0.02 (-0.71 – 0.75) 4 0.98 (0.92 – 0.99)
0.15 (-0.64 – 0.93) 4
LV Functional Indices – TDI s’ 0.99
(0.97 – 1.00) -0.04 (-0.44 – 0.36) 4 0.99
(0.97 – 1.00) 0.00 (-0.41 – 0.42) 4
e’ 0.94 (0.87 – 0.98)
-0.07 (-0.82 – 0.68) 5 0.92 (0.81 – 0.97)
0.14 (-1.1. – 1.38) 9
a’ 0.97 (0.92 – 0.99)
-0.01 (-0.83 – 0.81) 7 0.98 (0.92 – 0.99)
0.18 (-0.63 – 1.00) 7
IVRT’ 0.94 (0.86 – 0.98)
-0.63 (-6.17 – 4.91) 5 0.95 (0.87 – 0.98)
-0.01 (-5.69 – 5.68) 5
MPI’ 0.95 (0.88 – 0.98)
-0.01 (-0.09 – 0.07) 6 0.89 (0.73 – 0.89)
0.00 (-0.10 – 0.11) 9
Peak longitudinal Strain (GLS) 2 Chamber 0.92
(0.82 – 0.97) 0.05 (-0.20 – 2.30) 7 0.86
(0.66 – 0.94) -0.63 (-3.50 – 2.25) 8
3 Chamber 0.93 (0.84 – 0.97)
0.14 (-2.40 – 2.68) 7 0.90 (0.76 – 0.96)
-0.08 (-3.15 – 2.98) 9
4 Chamber 0.87 (0.71 – 0.94)
-0.06 (-2.95 – 2.84) 8 0.80 (0.54 – 0.92)
0.81 (-2.68 – 4.30) 10
Peak longitudinal Systolic Strain Rate (pLSSR) 2 Chamber 0.81
(0.57 – 0.92) -0.01 (-0.36 – 0.33) 10 0.71
(0.03 – 0.91) -0.19 (-0.51 – 0.14) 9
3 Chamber 0.80 (0.57 – 0.92)
0.04 (-0.38 – 0.46) 13 0.79 (0.54 – 0.91)
-0.02 (-0.47 – 0.43) 14
4 Chamber 0.93 (0.82 – 0.97)
0.00 (-0.27 – 0.28) 8 0.84 (0.65 – 0.94)
0.03 (-0.34 – 0.41) 11
ICC intraclass correlation coefficient; CI confidence interval; BA Bland-Altman; LOA limits of agreement; COV coefficient of variability; 4C apical 4-chamber view; 3C apical 3-chamber view; 2C apical 2-chamber view; * p<0.001 for all ICC;
91 | P a g e

Figure 5.2: Bland Altman plots for inter- and intra-observer measurement variability for mean strain and strain rate measured from left ventricular 4 chamber view in a randomly selected subset of 20 scans. Bias is presented as an absolute difference between two values.
92 | P a g e

5.4 Discussion
In this study, we utilized a comprehensive echocardiographic protocol that included
conventional imaging, TDI, and emerging STE to quantify LV size and function in healthy
newborns during the first two days of age, and provide the first comprehensive set of normal
values for this population and relative measurement reproducibility for these indices. We found
that LV dimensions, but not functional parameters, had a mild to moderate positive linear
correlation with birth weight. Further, we confirmed the validity of our data as normal values in
term neonates after the initial 12 hours of age, by demonstrating no significant change in
association with expected physiological changes in loading conditions between day 1 and day 2
of age.
Although there is an increasing desire to move from a qualitative to quantitative appraisal
of cardiac function, the field of quantitative assessment of LV function in neonates remains
grossly understudied, both for conventional and newer echocardiographic techniques. The
existing data, including inter-rater reliability and normative values, is patchy at best and needs to
be systematically evaluated, especially now that high-resolution ultrasound equipment and newer
imaging modalities are routinely available in NICUs. With the growth of neonatal
echocardiography programs, functional cardiac ultrasound is increasingly being utilized in daily
clinical practice by neonatologists. In this study, we demonstrated that among the tested
variables, measurement bias was least for tissue Doppler derived parameters. STE-derived
longitudinal strain fared slightly better than strain rate and conventional parameters (SF and EF).
This is likely due to the inherent limitation in these measures of the need for the operator to
manually identify and/or trace myocardial borders and that in STE, contrary to TDI, the strain is
directly measured by the software while the strain rate is calculated. In addition, we found that
93 | P a g e

LV related hemodynamic variables commonly employed in targeted neonatal echocardiograms
(mitral valve inflow, aortic diameter, VTI) demonstrated excellent reproducibility. We believe
the results of this study will be particularly valuable to the increasing number of intensivists with
echocardiography skills and will serve to inform day-to-day echocardiographic practices in
NICUs.
This study should be viewed through the prism of introducing a new routine bedside
application to the field of neonatal cardiology. This pilot study in healthy term infants serves as a
derivation cohort that now needs to be followed up with similar comprehensive and systematic
efforts to validate these markers by relating them to patient outcomes in different disease states.
Although it may be premature at this stage to provide categorical recommendations based on a
pre-defined cut-off, it may be feasible to incorporate some, if not all of these parameters, along
with qualitative assessment, for longitudinal monitoring. However, it should be recognized that
similar to other techniques, the measurement bias and clinical utilization of these methods is
likely to vary with image quality and operator experience. The specific threshold of imaging
experience for functional echocardiographic measurements is beyond the scope of this study, but
we recommend that prior to using these techniques in clinical practice, individual practitioners
should, review the emerging image acquisition and data analysis protocols, become aware of the
measurement bias for different indices in their own practice, and discuss the proper ways to
incorporate this knowledge while interpreting results. Overall, we report that the majority of LV
functional indices had acceptable reproducibility with ICC > 0.85, relatively narrow LOA on BA
analysis, and COV < 15%. These results were comparable to those of older children, as well as
that of the right ventricle previously reported by our group in the same population (190, 191).
Future studies should evaluate the role of these techniques, in early identification of pathological
94 | P a g e

deviations to obtain novel insights into the disease mechanism and progression, and to measure
the impact of common therapies, such as inotropes.
Interest in the use of TDI and STE for the assessment of regional and global LV function in
neonates is increasing (192). A recent review of left ventricular systolic strain and strain rate
measurement in infants and children has highlighted the lack of normative data in term neonates,
particularly during the first few days of age (147). Nevertheless, strain measurements have now
been applied to evaluate LV function in few neonatal conditions (150, 151, 157). Smaller studies
have reported that in comparison to healthy controls, LV GLS is lower in term small for
gestational age infants (-15.9% ± 2.1 vs. -21.3% ± 2.8; n=20 in each group) (151), in infants
undergoing total body hypothermia treatment for severe perinatal asphyxia (-11.01% ± 2.48 vs -
21.45% ± 2.74; n=24 in each group) (150), and in infants born after being exposed to pre-
gestational (-10.4 ± 3.2; n=20) and gestational diabetes (-13.1 ± 4.7; n=25) (157). Strain has also
shown to be negatively correlated with serum troponin levels in cases of severe perinatal
asphyxia (r2=0.64) (150). Although these studies highlight the potential utility of STE in
neonates, systematic studies with an a priori aim of establishing a comprehensive normative
dataset in this specific population is a necessary prerequisite to subsequent higher impact studies
in disease states. The control group data of STE-derived LV GLS presented in above studies
(150, 151, 157), as well as TDI-derived strain reported in previous studies which included
neonates on day 1 of age (153, 154), closely match the values obtained in our study.
In this study, we found that the majority of functional parameters when measured after 12
hours of age remained unchanged over the next two days; with the exception of small reductions
in LV lateral wall and septal s`, mitral valve inflow VTI and LV basal diameter. Although it is
not clear whether one or a combination of expected physiological changes associated with
95 | P a g e

postnatal transition were responsible for these changes, these could be explained by a relative
decrease in LV preload on day 2 of age. There are a number of factors which could explain this,
such as an expected increase in left to right shunt across the PFO secondary to decreasing right
sided pressures; the closure of the PDA on day 2 (observed in the majority of neonates), which
though restrictive on day 1, were contributing to LV preload by virtue of the left to right shunt
pattern (observed in 44% of neonates); and normal postnatal diuresis, as evident by the observed
weight loss on day 2. Tissue Doppler systolic velocities have previously been reported to be
influenced by changes in preload (193), while diastolic function assessment using TDI is
considered to be relatively less load dependent, which was also observed in this study (194).
In conclusion, we demonstrated the feasibility and describe the relative reliability and
normal values for LV functional parameters in heathy neonates during the first two days of life.
We also confirm the validity of data generated after 12 hours of age, by confirming the lack of
significant impact of further physiological transitional circulatory changes on these
measurements. We propose that LV function assessment in neonates should be based on a
comprehensive protocol which, in addition to traditionally employed parameters of FS and EF,
should also include TDI, STE derived longitudinal strain and flow derived hemodynamic
variables. Our results suggest that TDI derived myocardial systolic velocity (relatively higher
dependency on preload) and STE derived strain rate (high variability and low reliability), should
be used with caution in neonates during the first few days of age. Clinicians involved in
performing functional echocardiograms in neonates should focus on consolidating their
experience in measuring quantitative indices, be aware of the measurement bias for various
indices in their own practice and carefully consider such bias while interpreting longitudinal
changes over time or response to treatments.
96 | P a g e

Chapter 6: Cardiopulmonary adaptation during the first day of life in
humans*
*Draft of manuscript to be submitted to Circulation.
97 | P a g e

6.1 Introduction
The transition from intrauterine to extrauterine life represents a critical phase of
physiological adaptation, which impacts many organ systems, most notably the heart and the
lungs. The majority of neonates complete this transition without complications; however,
dysregulation of normal postnatal adaptation may lead to acute cardiopulmonary instability
necessitating advanced intensive care support (33). In some situations, death or adverse
neurosensory impairment may ensue (34, 195). The approach to cardiovascular care in these
patients is limited by the lack of reliable or readily available physiologic measures of
cardiopulmonary health and suboptimal thresholds for therapeutic intervention, driven in part by
a paucity of information regarding physiological cardiac adaptation after birth and the interaction
with changes in pulmonary circulation.
Animal experiments have demonstrated a progressive fall in PVR over the first 48-72
hours after birth in response to lung recruitment and increased alveolar oxygen concentration
(196). As PVR falls, the direction of flow across the ductus arteriosus (DA) and foramen ovale
(FO) becomes increasingly left-to-right. This is soon followed by the closure of the DA in most,
ductus venosus in many and lastly FO. These changes and the specific relationship with time
after birth have been poorly documented in human neonates. The impact of the transitional
period on myocardial function and cardiac output is also not well understood.
We have recently published normative data for echocardiography derived indices of RV
and LV ventricular function, pulmonary hemodynamics and shunt characteristics on day one and
two of age for a cohort of 50 healthy term neonates (197, 198). We demonstrated that PVR
reduced over the first two days of age, while cardiac function indices remained unaffected.
However, in those studies we did not evaluate infants within the first 12 hours of life, when the
98 | P a g e

transitional circulatory changes are expected to be highest. The objective of this study was to
delineate, in a time sensitive manner, the natural history of PVR, cardiac output, myocardial
function and transitional shunts over the first 24 hours following birth.
6.2 Additional methods
Inclusion and exclusion criteria: Women with singleton, low risk, uncomplicated pregnancies
who presented at Mount Sinai Hospital during the study period in labor, between 37 and 42
completed weeks of gestation and had no evidence of intra-uterine growth restriction, placental
dysfunction or fetal distress were approached for consent. Our exclusion criteria were based on
the conditions which could potentially impact physiological postnatal adaptation and included
maternal conditions such as diabetes, hypertension, use of antidepressant medications, abnormal
results of the first trimester screen or integrated perinatal screen, any congenital anomaly
identified in the fetus on an anatomy ultrasound, known genetic anomaly, abnormal Doppler
profile in the umbilical artery on the most recent antenatal ultrasound and clinical suspicion of
chorioamnionitis. Further, among recruited neonates, we excluded infants after birth if their
umbilical arterial or venous cord pH was < 7.0, if they had an Apgar score of ≤ 5 at 5 minutes of
age, required any active resuscitation other than drying and stimulation, were noted to have
dysmorphic features or if required admission to the neonatal intensive care unit. In addition, we
excluded any infant with a congenital heart defect on study echocardiogram other than a PDA
and/or PFO.
Exposure: A total of 15 neonates were prospectively recruited and completed the study
procedure. This was a pre-defined sample size of convenience. Expectant parents of prospective
eligible neonates were approached for consent during labour and the consenting process was
completed before delivery. Each recruited neonate underwent four sequential echocardiograms at
99 | P a g e

the following time points: < 0.5 hours, 2 to 3 hours, 7 to 10 hours and 22 to 24 hours of life. For
the first echocardiogram, once consent was obtained, the ultrasound machine was set up inside
the labour room next to the infant warmer. Following delivery and a brief period of skin to skin
care with their mothers, all recruited neonates were brought to the warmer, dried, covered by
warm towels and had neonatal electrocardiograph electrodes applied before undergoing the first
study echocardiogram. This was achieved in all 15 cases at < 30 mins of age. Subsequent scans
were performed at the bedside in the Mother and Baby unit at the pre-specified postnatal age as
above. It was ensured that infants were in a non-agitated quiet state at the time of scans and
simultaneous electrocardiograph recording were also obtained. Each study echocardiogram was
< 20 mins in duration and consisted of recording images in RAW DICOM data format for offline
measurements. All 60 scans performed for this study were digitally stored and analyzed off-line
in a random order. Measures of PVR, ventricular outputs and shunt characteristics were obtained
at each time point. Functional parameters, however, were only obtained at the first and the last
scan. This was done to minimize scanning load on study participants and the specific time points
were chosen based on the rationale that the changes in myocardial loading conditions were
expected to be least at the first and highest at the last scan.
In addition to the measures of PVR mentioned above, for this study we also calculated
PAAT and RVET indexed to the total duration of cardiac cycle, expressed in percentage (PAATi
and RVETi respectively). This was done because PAAT and RVET demonstrated a strong
negative correlation with heart rate, which incidentally changed significantly over the study
period. The following list of echocardiographic indices were employed in this study.
Table 6.1: List of echocardiography derived indices employed in this study
Pulmonary vascular resistance
• Pulmonary artery acceleration time (PAAT) • Pulmonary vascular resistance index (PVRI) = Right ventricular ejection time
100 | P a g e

(RVET)/ PAAT • PAAT indexed to total duration of cardiac cycle and expressed as percentage
(PAATi) Pulmonary blood flow
• Right ventricular stoke volume (RVSV) • Right ventricular output (RVO)
Systemic blood flow
• Left ventricular stoke volume (LVSV) • Left ventricular output (LVO)
Shunts • Patent ductus arteriosus (PDA) • Patent foramen ovale (PFO)
Right ventricular (RV) function
Systolic function • Tricuspid annular plane systolic excursion (TAPSE) • Fractional area change measured from RV-focused apical 4 chamber view (FAC-4C) • Fractional area change measured from RV-focused apical 3 chamber view (FAC-3C) • Tissue Doppler derived peak systolic myocardial velocity measured on RV lateral
wall just below the tricuspid annulus (RV s’) • Peak longitudinal strain measured using speckle tracking echocardiography from the
RV lateral wall (GLS-4C) and inferior wall (GLS-3C) Diastolic function
• Isovolumic relaxation time measured using tissue Doppler imaging (IVRT’) • Ratio of tricuspid valve early (TvE) and late (TvA) inflow velocities
Left ventricular (LV) function
Systolic function • Ejection fraction (EF) measured using Simpson’s biplane method • Tissue Doppler derived peak systolic myocardial velocity measured on LV lateral
wall just below the mitral annulus (LV s’) • Average of the peak longitudinal strain measured using speckle tracking
echocardiography from LV-focused apical 4, 3 and 2 chamber views (LV GLS) Diastolic function
• Isovolumic relaxation time measured using tissue Doppler imaging (IVRT’) • Ratio of mitral valve early (MvE) and late (MvA) inflow velocities
Global heart function (calculated for both ventricles)
• Myocardial performance index measured using tissue Doppler imaging [MPI’ = (IVRT’ + isovolumic contraction time)/duration of systole]
• Ratio of total duration of systole and diastole measured using tissue Doppler imaging (systole’: diastole’)
Measures of cardiac function were measured at 1st scan performed at < 0.5 hours of age and again at 4th scan performed between 22-24 hours of age. Other parameters were measured at each scan time.
Subsequent confirmation of reproducibility of results involved performing a qualitative,
time-specific, post-hoc comparison of parameter values with those obtained in a previous
prospective observational study conducted at our institute (197, 198). It was important to confirm
the representativeness of obtained measures in another larger validation cohort as our primary
derivation cohort consisted of a small number of neonates.
101 | P a g e

Additional statistical considerations: The association between heart rate and indices of PVR was
analyzed using a linear model [outcome= a + b HR +e, where b (estimate) is the coefficient of
HR and the autoregressive covariance (e) structure was used to account for the repeated
measures]. We confirmed the resolution of association with heart rate for PAAT after being
converted to PAATi, as described above (Table 6.2). However, RVETi continued to show
association with heart rate. For validation, values from the D2 scans were compared with D1
scans using paired Student’s t-test or Fisher’s exact tests, as appropriate.
Table 6.2: Association between indexes of PVR and heart rate
Variable Estimate (sdr) p value
PAAT (msec) -0.22 (0.05) <.0001 RVET (msec) -0.993 (0.10) <.0001 PAATi (%) 0.017 (0.11) .105 RVETi (%) 0.08 (0.022) .001 PVRI, mean (SD) -0.0012 (0.005) .820 PAAT pulmonary artery acceleration time; RVET right ventricular ejection time; PAATi and RVETi PAAT and RVET expressed as percentage of total duration of cardiac cycle respectively; PVRI pulmonary vascular resistance index.
6.3 Results
We studied 15 neonates (9 males), born at a mean (SD) gestation and BW of 40 ± 0.8 weeks and
3.5 ± 0.5 Kg respectively. All but three were delivered vaginally. The median (IQR) Apgar score
at 5 minutes of age was 9 (9, 9) and mean cord pH was 7.2 ± 0.1. There were significant changes
observed in the indices of PVR and blood flow during the first 24 hours of life (Table 6.3). Heart
rate was highest at first scan but came down by the time of 2nd scan; then remained unchanged on
subsequent evaluations.
102 | P a g e

Table 6.3: Sequential measurements of echocardiographic indexes of pulmonary vascular resistance and pulmonary and systemic blood flow demonstrating transitional circulatory changes during the first day of life in healthy human neonates
Scan 1 Scan 2 Scan 3 Scan 4 Age (hrs) 0.4 ± 0.1 hrs 2.7 ± 0.2 hrs 8.2 ± 0.6 hrs 22.7 ± 0.7 hrs p PAAT (msec) 33 ± 4 35 ± 4 42 ± 5*¶ 55 ± 7* ¶† <.001 RVET (msec) 166 ± 21 186 ± 21* 208 ± 13* ¶ 216 ± 18* ¶ <.001 PAATi (%) 8.4 ± 1.1 7.4 ± 1.4* 8.1 ± 1.3 10.7 ± 1.4*¶† <.001 PVRI (RVET:PAAT) 5.1 ± .8 5.3 ± .8 5.0 ± .6 4.0 ± .5* ¶† <.001 PA VTI (cms) 8.3 ± 1.4 9.6 ± 2.0* 10.1 ± 1.4* 11.6 ± 1.6 * ¶† <.001 RVSV (mls) 5.3 ± 1.7 6.0 ± 1.7* 6.3 ± 1.4* 7.2 ± 1.3* ¶† <.001
RVSV (mls/Kg) 1.6 ± .6 1.8 ± .6* 1.9 ± .6* 2.1 ± .6* ¶† <.001
RVO (mls/kg/min) 235 ± 87 222 ± 78 218 ± 76 250 ± 78 .043
Ao VTI (cms) 7.5 ± 1.6 9.5 ± 2.2* 10.3 ± 1.9* 10.9 ± 1.7* <.001 LVSV (mls) 3.3 ± .8 3.9 ± 1.1* 4.2 ± .9* 4.2 ± 1.1* <.001 LVSV (mls/Kg) 0.9 ± .2 1.1 ± .2 1.2 ± .2* 1.2 ± .3* <.001 LVO (mls/kg/min) 145 ± 35 138 ± 31 140 ± 34 143 ± 43 NS RVO:LVO 1.7 (1.2, 1.9) 1.7 (1.2, 1.9) 1.5 (1.1, 1.8) 1.7 (1.3, 2.1)† .028 HR (beats/min) 144 (141, 172) 124 (114, 133)* 115 (104, 124)* 113 (107, 129)* <.001
Analysis performed using one way repeat measure ANOVA. Results presented as mean ± SD or median (IQR). * p<.05 vs. baseline, ¶p<.05 vs. 2nd scan, †p<.05 vs. 3rd scan. PAAT pulmonary artery acceleration time; RVET right ventricular ejection time; PAATi and RVETi PAAT and RVET indexed to total duration of cardiac cycle and expressed as percentage respectively; PVRI pulmonary vascular resistance index; RVSV right ventricular stoke volume expressed both in mls as absolute number and mls/kg when index to infant’s body weight; RVO right ventricular output; LVSV left ventricular stoke volume expressed both in mls as absolute number and mls/kg when index to infants body weight; LVO left ventricular output; HR heart rate. NS = p>.10.
103 | P a g e

Indices of PVR: Despite the reduction in heart rate, PAAT remained similar on initial two scans;
subsequently it increased for the rest of the study period. PVRI, however, only demonstrated a
reduction on the last scan. This was in relation to changes in RVET, which continued to increase
over the first 3 scans before stabilizing. PAATi, on the other hand, demonstrated a reduction on
the 2nd scan between 2 to 4 hours of life, before showing a progressive increase for rest of the
study period (Figure 6.1). RVETi also decreased on 2nd scan before returning to baseline values.
Gross sequential changes were also noticeable in the pulmonary artery pulse wave Doppler
contour, with mid or late systolic notching being a frequent finding till 4 hours of life Figure 6.2.
Figure 6.1: Changes in echocardiographic measures of pulmonary vascular resistance (PVR) during the first day of life in healthy human neonates. While PAAT started increasing from 3rd scan onwards (A), PVRI only demonstrated changes on 4th scan (B). This discrepancy was due to a simultaneous increase in RVET during the first 8 hours of age (C). Indexing PAAT to total duration of cardiac cycle (PAATi) made it independent of heart rate and RVET. PAATi showed a reduction at 2nd scan compared to 1st scan, before demonstrating a consistent increase for the rest of the study period. Analysis was performed using one way repeat measure ANOVA. The hollow triangles represent mean values while vertical lines represent 95% confidence intervals observed at each scan. * p<.05 vs. baseline, ¶p<.05 vs. 2nd scan, †p<.05 vs. 3rd scan. PAAT pulmonary artery acceleration time; RVET right ventricular ejection time; PVRI pulmonary vascular resistance index.
104 | P a g e

Figure 6.2: A sequentially obtained pulse wave Doppler trace of the main pulmonary artery from one of the study infants, showing typical changes observed during the first 24 hours of age in healthy neonates following successful postnatal transition. A simultaneous increment in right ventricular ejection time (RVET) resulted in an unchanged pulmonary vascular resistance index (PVRI = RVET/PAAT) on the first three scans. Mid- and/or late-systolic notching was a frequent finding on first two scans.
Indices of cardiac outputs: Overall, changes in indices of cardiac outputs were relatively small
over the study period. Measures of RV stroke volume (PA VTI, RVSV) demonstrated an
increase between 1st and 2nd and again between 3rd and 4th scan, while LV stroke volume
parameters (Ao VTI, LVSV) increased only between 1st and 2nd scan. The right and left
ventricular output per minute and their ratio, however, remained unchanged during the first 24
hours of life.
105 | P a g e

Natural history of Transitional Shunts (Table 6.4): Transductal shunt was bidirectional in all
patients on the first scan with a maximum duration of right to left shunting being 40% of the total
shunt duration. The proportion of infants with bidirectional shunts, as well as duration of right to
left shunting in bidirectional shunts reduced over the study period. Cessation in transductal flow
was seen in 67% patients by the time of the last scan, with most closing between 7 and 24 hours
of age. The predominant demonstrable flow across the PFO was left to right in most patients at
each time point, the proportion of which increased with time over the study period.
Table 6.4: Natural history and flow characteristics of patent ductus arteriosus (PDA) and patent foramen ovale (PFO) during first day of life in healthy human neonates
Scan 1 Scan 2 Scan 3 Scan 4 Age (hrs) 0.4 ± 0.1 hrs 2.7 ± 0.2 hrs 8.2 ± 0.6 hrs 22.7 ± 0.7 hrs PDA Closed 0 0 3 (20%) 10 (67%) Small restrictive with left to right shunt
0 3 (20%) 7 (47%) 5 (33%)
Bidirectional shunt 15 (100%) 5 (33%) 1 (7%) 0 Growing shunt# 0 7 (47%) 4 (27%) 0 Percentage duration of right to left shunt in bidirectional shunts* [mean(SD; range)]
32 (5; 22-40)% 24 (5; 17-30) % 23% (only one bidirectional
shunt)
-
PFO No flow visualized 5 (33%) 4 (26%) 2 (13%) 2 (13%) Right to left shunt 1 (6%) 0 0 0 Bidirectional shunt 1 (6%) 1 (6%) 1 (6%) 0 Left to right shunt 8 (53%) 10 (67%) 12 (80%) 13 (87%) #Growing shunt was defined as shunt pattern which is almost entirely left to right but had a small right to left component at end-diastole. *= (duration of right to left shunt/total shunt duration) x100. Results presented as number (percentage). No patient had unrestrictive left to right shunt across patent ductus arteriosus. SD standard deviation.
Indices of Myocardial Performance (Table 6.5): In comparison to the 1st scan, significant
increase was observed by the 4th scan time in indices of RV systolic (TAPSE, FAC-4C, GLS-3C)
and global (systole’: diastole’) function; with least overlap seen in values of TAPSE and GLS-3C
between two time points (Figure 6.3). The GLS-3C was lower in comparison to GLS-4C at first
106 | P a g e

scan, but increased to comparable values by end of first day of life (Figure 6.4). There were no
change in indices of LV systolic performance, however, a small but significant rise observed in
diastolic performance (MvE: MvA and systole’: diastole’ ratios).
Table 6.5: Changes in cardiac function in healthy neonates during first the day of life illustrating myocardial adaptation associated with physiological postnatal transition
Scan 1 Scan 4 Mean difference (95% CI)
p
Age 0.4 ± 0.1 hrs 22.7 ± 0.7 hrs - Right Ventricle Systolic function
TAPSE (cm) .72 ± .10 .86 ± .09 - .14 (-.18, -.10) <.001 FAC-4C (%) 18.2 ± 6.8 29.1 ± 14.3 -10.9 (-20.3, -1.5) .027 FAC-3C (%) 33.7 ± 7.9 37.6 ± 5.2 -3.9 (-8.6, .8) .097 RV-s’ (cm/s) 6.7 ± 1.3 6.2 ± .8 .5 (.3, -.03) NS GLS-4C (%) 20.6 ± 3.8 22.7 ± 3.8 -2.0 (-4.4, .4) .089 GLS-3C (%) 17.0 ± 2.5 22.0 ± 2.7 -5.0 (-7.3, -2.6) .001
Diastolic function
IVRT’ (ms) 61 ± 17 51 ± 13 10 (-1, 20) .069 TvE: TvA 1.02 ± 0.54 0.77 ± 0.16 0.26 (-0.12, 0.66) NS
Global function
MPI’ .57 ± .21 .46 ± .16 .12 (-.01, .25) .074 Systole’: diastole’ 1.33 ± .19 1.0 ± .20 .33 (.16, .49) .001
Left Ventricle Systolic function
Ejection fraction (%) 65 ± 7 65 ± 8 -.3 (-4.7, 4.2) NS LV-s’ (cm/s) 5.3 ±1.0 5.2 ± .9 .1 (-.5, 0.7) NS LV-GLS (%) 21.7 ± 2.4 22.1 ± 2.1 -.4 (-2.2, 1.4) NS
Diastolic function
IVRT’ (ms) 48 ± 13 52 ± 7 -4 (-10, 3) NS MvE: MvA .97 ± .25 1.23 ± .30 -.26 (-.48, -.03) .028
Global function
MPI’ .60 ± .16 .61 ± .17 -.01 (-.12, .10) NS Systole’: diastole’ 1.27 ± .22 .97 ± .28 .30 (.13, .46) .002
Analysis performed using paired T-test. Results presented as mean ± SD or median (IQR). (‘) indicates that parameter was measured using tissue Doppler imaging. TAPSE tricuspid annular plane systolic excursion; FAC fractional area change measured from right ventricular (RV) focused apical-4-chamber view (FAC-4C) and RV apical-3-chamber view (FAC-3C); s’ peak systolic myocardial velocity measured from the RV lateral wall just below the tricuspid valve annulus for the right ventricle and from the left ventricular (LV) lateral wall just below the mitral valve annulus for the left ventricle; GLS peak longitudinal strain measured using speckle tracking echocardiography; for the right ventricle GLS was measured from the lateral wall (GLS-4C) and inferior wall (GLS-3C), while for the left ventricle GLS was measured from LV-focused apical 4, 3 and 2 chamber views and then averaged to obtain LV-GLS-global; IVRT’ isovolumic relaxation time; TvE and TvA tricuspid valve early and late inflow velocities respectively; MPI’ myocardial performance index [= (IVRT’ + isovolumic contraction time)/ejection time]; MvE and MvA mitral valve early and late inflow velocities respectively; 95% CI 95% confidence intervals. NS = p>.10.
107 | P a g e

Figure 6.3: Box plot graphs of key echocardiographic measures of right ventricular (RV) systolic function at <0.5 hours and 22-24 hours of life in healthy human neonates following successful postnatal transition. Among the tested variables, TAPSE and GLS-3C demonstrated maximum change between the two time points. Analysis was performed using paired t-test. TAPSE tricuspid annular plane systolic excursion; FAC-4C fractional area change measured from RV focused apical-4-chamber view; GLS peak longitudinal strain measured using speckle tracking echocardiography from the RV lateral wall (GLS-4C) and RV inferior wall (GLS-3C).
108 | P a g e

Figure 6.4: Comparison of peak global longitudinal strain measured using speckle tracking echocardiography from right ventricular lateral wall (GLS-4C) and inferior wall (GLS-3C) at < 0.5 hours and 22-24 hours of age in healthy neonates following uncomplicated postnatal transition. Note that while GLS-4C remained similar at two time points, GLS-3C was significantly lower shortly after birth but increase to values similar to GLS-4C by the end of first day of life.
Validation of measured parameters: The validation cohort consisted of 50 healthy newborns who
underwent sequential echocardiograms at 15 ± 2 and 36 ± 2 hours of age for a previous study.
The mean gestational age and birth weight was 39.3 ± 1.2 weeks and 3.5 ± 0.5 Kg respectively.
Longitudinal changes were observed between two time points in the same parameters as for the
derivation cohort; LVSV and LVO did not change (Table 6.6). Qualitatively, the values obtained
from this historic cohort closely fitted with the trajectory of changes observed in the derivation
cohort in an age-specific manner.
109 | P a g e

Table 6.6: Measurements of echocardiographic indexes of pulmonary hemodymanics, pulmonary and systemic blood flow and characteristics of patent ductus arteriosus (PDA) and patent foramen ovale (PFO) obtained from a cohort of 50 healthy term neonates who underwent serial echocardiograms on day 1 and 2 of age for a previous prospective observational study.
Age 15 ± 2 hrs 35 ± 2 hrs p
PAAT (ms) 50 ± 17 59 ±15 <.001
RVET (ms) 216 ± 24 216 ± 23 NS
PAATi (%) 9.6 ± 2.8 12.0 ± 2.7 <.001
PVRI (RVET:PAAT) 4.8 ± 1.3 3.8 ± .8 <.001
RVSV (mls/kg) 2.1 ± .6 2.5 ± .8 <.001
RVO (ml/kg/min) 246 ± 66 307 ± 90 <.001
LVSV (mls/kg) 1.09 ± .20 1.10 ± .23 NS
LVO (mls/kg/min) 128 ± 28 137 ± 28 NS
HR (beats/min) 119 ± 15 124 ± 17 .042
PDA closed, n(%) 28 (56%) 48 (96%) <.001
PFO closed, n(%) 9 (18%) 13 (26%) NS
All PDAs were small, restrictive and shunting left to right. All PFOs were shunting left to right. PAAT pulmonary artery acceleration time; RVET right ventricular ejection time; PAATi and RVETi PAAT and RVET expressed as percentage of total duration of cardiac cycle respectively; PVRI pulmonary vascular resistance index; RVSV right ventricular stoke volume expressed both in mls as absolute number and mls/kg when index to infants body weight; RVO right ventricular output; LVSV left ventricular stoke volume expressed both in mls as absolute number and mls/kg when index to infants body weight; LVO left ventricular output; HR heart rate. NS = p>.10. Note that the data matched closely with the results generated by the study involving sequential echocardiography assessments during first day of age in a time-specific manner supporting the reproducibility of those observations.
Inter-rater reliability of hemodynamic measures:
The inter- and intra-observer measurement variability for functional variables have been
published by our group (197, 198); measurement variability for hemodynamic indices was
calculated for this study (Table 6.7).
110 | P a g e

Table 6.7: Intra- and inter-observer variability of indices of pulmonary vascular resistance and blood flow
Variable Intra-observer Variability Inter-observer variability ICC
(95% CI) Mean Bias (95%CI) ICC
(95% CI) Mean Bias (95%CI)
PAAT .90 (.76, .96)
.58 (-11.54, 12.70)
.83 (.55, .94)
4.26 (-10.17, 18.69)
RVET .90 (.76, .96)
-1.05 (-23.49, 31.39)
.78 (.51, .91)
7.05 (-27.06, 41.17)
PA diameter
.93 (.83, .97)
.00 (-.17, .17)
.48 (.06, .74)
-.06 (-.28, .17)
PA VTI .99 (.98, .99)
-.03 (-.67, .60)
.98 (.94, .99)
-.11 (-1.13, .91)
Aortic diameter
.93 (.81, .97)
.01 (-.03, .06)
.87 (.67, .95)
-.01 (-.07, .05)
Aortic VTI
.97 (.93, .99)
.02 (-.71, .75)
.98 (.92, .99)
.15 (-.64, .93)
ICC: Intraclass correlation coefficient; CI: confidence interval; Bias calculated using Bland Altman analysis. p value for all ICC < .001.
6.4 Discussion
The postnatal transition represents a time-period during which neonates are exposed to
sudden and complex changes in cardiopulmonary physiology, resulting in increased cardio-
respiratory vulnerability and risk of complications. Echocardiography is now a routinely
employed investigation for diagnostic and monitoring purposes in neonates suffering from
dysregulation of transitional physiology (199); however, the interpretation of various
echocardiographic indices is challenged by a relative paucity of reliable data in a healthy
population during this time period. The clinical care of these sick neonates is further hampered
by a lack of understanding of normal physiological adaptation in the immediate period after
birth. In this prospective, observational, physiologic study of healthy newborns, we sequentially
measured echocardiographic parameters of PVR, myocardial function, cardiac output and fetal
shunts and describe how these change over the first 24 hours of life. We confirmed that the first
day of life is characterized by significant circulatory changes, consistent with the anticipated
111 | P a g e

overall fall in PVR and progressive closure of the DA. In addition, our study has provided
several novel insights in various aspects of transitional physiology in humans as discussed
below.
Indices of Pulmonary Vascular Resistance (PVR): Our results indicate, that in humans, despite a
reduction in the ratio of pulmonary to systemic pressures, as suggested by changes in ductal
shunt pattern, the overall fall in RV afterload may occur at a slower rate until 7-10 hours of life,
after which the rate of fall accelerates. In fact, the net effect of circulatory changes may even be
resulting in a rise in RV afterload over the first 4 hours of life, as suggested by the observed
decrease in PAAT on the second scan after adjustment for heart rate (PAATi). This can be
explained by changes in ductal shunt pattern; specifically, we noted a change from a
bidirectional pattern in all infants at 1st scan, thereby exposing the right ventricle to the
cumulative effect of PVR and SVR, to a predominantly left to right shunt in the majority of
infants on 2nd scan. Previous validation studies for PAAT as a marker for PVR were conducted
in adults and older children (171, 172). Our findings suggest that in newborns, instead of PVR
alone, PAAT may be an estimate of overall RV afterload, which in the presence of an open DA
will also be affected by SVR. We speculate that during early hours of transitional circulation, the
fall in PVR may be negated by the removal of exposure of the right ventricle to systemic
circulation secondary to changes in DA, which may result in a net transient increase in RV
afterload. This, however, will have to be confirmed in future studies as we did not collect
measures of SVR.
Another concern with the use of PAAT in newborns is its strong negative correlation with
heart rate (200), which can impact its clinical utility, particularly for heart rates greater than 100
beats/min (201). Indexing PAAT to cardiac cycle duration resolved this heart rate dependency
112 | P a g e

and appears to make it more sensitive to detect changes in neonatal pulmonary circulation.
PAATi, however, is a novel index and need further validation, ideally by comparison with
invasive definitive investigations; though, in neonates correlation with expected physiology or
clinical outcomes may be more feasible. PVRI, although independent of heart rate, was
insensitive to early pulmonary hemodynamic changes; this was due to concurrent increase in
RVET observed on the first 3 scans in this study. RVETi also decreased significantly on 2nd scan,
however, its interpretation is hampered by a residual association with heart rate despite being
indexed to cardiac cycle duration.
Indices of Myocardial Function: One of the novel and interesting finding of our study was the
presence of relatively lower values for RV systolic (TAPSE, FAC-4C, GLS-3C) and global
(systole’: diastole’) functional parameters during the first 30 minutes of life. All indices
increased significantly by 24 hours of age, reaching values comparable to published data
measured at 12 - 18 and 30 - 40 hours of life (197). While these results may indicate load-
dependency of echocardiographic measures, they may also suggest that it is physiological to
have transiently low RV function during the initial hours after birth. The fact that results
obtained from multiple parameters corroborated and their increase coincided with the
physiological reduction in PVR suggest load dependency of the neonatal right ventricle. This
may relate to the known properties of the immature heart, which significantly differs from adults
by having a lower compliance and higher proportion of non-contractile tissue (202). We
hypothesize that, similar to neonatal left ventricle which has been shown to have an increased
susceptibility to afterload (94), neonatal right ventricle may also be inherently vulnerable to
dysfunction on exposure to persistently high afterload conditions. Our observation of lower
GLS-3C on the first scan which increased to values similar to GLS-4C by 24 hours of age
113 | P a g e

suggest a regional effect of increased afterload on the right ventricle. Whether GLS-3C is more
sensitive to afterload and hence detect changes earlier than GLS-4C in neonates will have to be
examined in future studies. Contrary to RV function, LV functional indices remained relatively
unchanged over the first 24 hours of life, demonstrating values comparable to published data
(198).
Indices of cardiac output: In this study, we found that although stroke volumes for both
ventricles increased between scans one and two, because of higher heart rate immediately after
birth, cardiac outputs per minute remained unchanged. Although sequential evaluations at similar
time points during transition has not been reported before, studies performed at different time
points on the first day of life have documented RVO and LVO in healthy term neonates (203-
208). Few recent studies conducted using modern imaging equipment and similar measurement
technique have reported values comparable to our study (205-207). Noori et al reported RVO
[range 300-340 ml/min/kg] > LVO [range 165-212 ml/min/kg] when measured sequentially at 2,
5 and 10 min of life in 20 term neonates (205). Popat et al reported mean values of RVO 212
ml/min/kg and LVO 190 ml/min/kg at 4 hours of age from 21 term babies (206). A comparative
evaluation of LVO between neonates born by normal vaginal delivery vs caesarian section
performed by Coskun et al showed no difference between the subgroups, with overall mean LVO
of 350 mls/min and 265 mls/min at 1 and 24 hours of age respectively; values indexed to infant’s
weight were not reported (207). Interestingly, similar to our study, previous reports have
consistently found RVO to be greater than LVO on the first day of life. In a fetal
echocardiography study, Mielke et al also reported a median RVO: LVO ratio of 1.4 from 222
normal human fetuses, which was independent of gestational age (25). We found similar RVO:
LVO ratio on first postnatal day, underlining the persistence of RV dominance during this time.
114 | P a g e

Variance between RVO and LVO during the transitional period may be explained by relative
volumes of shunt across the PDA and PFO, neither of which is can be directly quantified by
echocardiography. We hypothesize that the higher RVO: LVO relates to the increased left to
right transatrial shunting, as suggested by earlier closure of PDA but persistence of PFO in the
majority of study infants.
Natural History of Transitional Shunts: In this study, we confirmed the findings of previous
investigators that in healthy term infants, by 24 hours of age, the ductus arteriosus is closed in
the majority of cases and demonstrate restrictive left to right flow pattern shunt in the remaining
before undergoing closure by 40 hours of age (209-212). We, like other recent observations, also
demonstrate a bidirectional ductal shunt in all neonates shortly after birth (205, 213). In addition,
we quantified the percentage bidirectional flow and found it to be ≤ 40% of total shunt duration
in all cases, suggesting pulmonary pressures to be below systemic level by 30 minutes of life
(214). Our results suggest that presence of bidirectional ductal shunt is an unusual occurrence in
healthy neonates after 10-15 hours of age, while PFO shunt may be left to right in the majority
irrespective of age.
Importance of this study: While animal experiments have greatly enhanced our knowledge
regarding the overall transitional physiology (24), data from these may not always be applicable
to humans in the clinical settings due to inter-species variability. For instance, sentinel work by
Rudolph in a canine experimental model showed that birth is followed by a progressive fall in
PVR; however, in the same experiment trajectory of change was reported to be slower in
newborn goats (196). This was in contrast to the experiments in lambs, where PVR changes were
reported to be more dramatic at birth (215). Studies have reported invasive pulmonary artery
pressure measured from healthy human neonates during the initial 72 hours of age (216).
115 | P a g e

Although these studies were of questionable methodology, their results suggested a slower fall in
pulmonary pressures in human neonates, particularly during the initial 10-12 hours of age; this is
in line with our non-invasive assessments. With the availability of high fidelity imaging
equipment, as demonstrated in this study, it may now be feasible to acquire physiological data
directly from humans, which in addition to confirming the expected physiology may also provide
novel, species specific insights, as well as provide clinically applicable control data. For instance
recent studies in human fetuses have shown that in comparison to fetal lambs, human fetuses
shunt less percentage of blood via ductus venosus and have a higher ratio of pulmonary blood
flow to cardiac output (25, 217), thus highlighting the feasibility and importance of acquiring
human data.
In conclusions, Comprehensive neonatal echocardiography may be used to elicit time-specific
cardio-pulmonary adaptive changes associated with postnatal transition in human neonates and
may provide quantitative and pragmatic measures of hemodynamic alterations and cardiac
function. The immediate postnatal period in humans is characterized by significant fall in PVR,
however, the trajectory of fall in net RV afterload may be slower during the initial 10 hours of
life. Cardiac outputs remains stable throughout this period, at least in part, due to compensation
of lower stroke volumes during the initial hours after birth by high heart rate. The first 24 hours
of life is also associated with significant increase in RV performance, which temporarily relate to
fall in PVR and ductal closure patterns; we speculate that these adaptive changes may indicate an
inherent vulnerability of the neonatal right ventricle to high afterload conditions. These data lay
the foundation for future studies of disease states associated with an abnormal transition and may
facilitate the identification of thresholds for therapeutic interventions.
116 | P a g e

Chapter 7: Cardiac Function and Ventricular Interactions in Persistent
Pulmonary Hypertension of the Newborn*
*Draft of manuscript to be submitted to Circulation Imaging
117 | P a g e

7.1 Introduction
Persistent pulmonary hypertension of the newborn is a disorder of postnatal transition,
accounting for a significant proportion of admissions to tertiary NICUs (33, 34). Infants with
PPHN often require advanced and sometimes prolonged cardio-respiratory support and are at
significant risk of mortality and morbidities, which despite widespread use of iNO has remained
unchanged over the past 2 decades (33, 34, 38). Cardiac dysfunction could be a potential
contributor. In older patients with PAH, adaptation of RV function in response to acute or
chronic pressure loading is a major determinant of clinical outcomes (218). Development of RV
dysfunction will result in decreased RVO and unfavourable interventricular interactions with the
left ventricle. A pressure-loaded, dilated right ventricle causes leftward shift of the
interventricular septum; this can result in reduced LV filling, further compromising LVO (37, 99,
185, 219). Whether similar mechanisms are at play in PPHN are unknown.
The neonatal right ventricle may be better poised to compensate for increased RV afterload
related to the physiologic neonatal RV hypertrophy, making unfavourable LV-RV interaction
less likely. On the other hand, however, immaturity of the neonatal myocardium, which is
characterized by high collagen content and lower calcium handling capacity, may make RV
function more load dependent (220). Another factor in PPHN is the presence of right to left
shunting of blood via intra- and extra-cardiac shunts. The persistence of ductus ateriosus may
offload the right ventricle in patients with PPHN but at the expense of pulmonary blood flow,
LV preload and systemic oxygen saturation. A right to left shunt across foramen ovale may
contribute to LV preload and LVO but will result in lower RVO and pulmonary blood flow.
We have recently described normative data for various indices of RV and LV size and
function in a representative cohort of healthy term neonates for the first two days of age by using
118 | P a g e

a comprehensive echocardiographic imaging protocol (197, 198). This protocol is now the
clinical standard in our institution. In the present study, our aim was to identify
echocardiographic parameters of biventricular size, function, and hemodynamics in neonates
presenting with PPHN during the first 3 days of life using the imaging protocol as previously
described (197, 198). We also examined the relationship between key echocardiographic
findings and adverse clinical outcomes. We hypothesized that PPHN would be associated with
RV systolic and diastolic dysfunction.
7.2 Additional methods
This was a retrospective cohort study primarily aimed at describing the echocardiography
correlates and investigate inter-ventricular interaction in neonates with PPHN.
Inclusion and exclusion criteria: This study included infants born at a gestational age ≥ 35
weeks, with a birth weight ≥ 2500 grams and admitted with a diagnosis of PPHN to the NICU of
the Hospital for Sick Children, Toronto, over a 3 year period (2012 to 2015). Eligible infants
were identified by screening the listed diagnoses in the unit’s admission logbook and the
electronic echocardiography database during the study period. The identified infants had to
satisfy the following criteria for inclusion in the study: need for respiratory support with a
fraction of inspired oxygen of ≥ 0.40; confirmed echocardiography diagnosis of PPHN [defined
as presence of bidirectional or right to left shunting across the patent ductus arteriosus (PDA)
and/or patent foramen ovale (PFO), and/or a tricuspid regurgitant (TR) jet with an estimated
right ventricular systolic pressure (RVsP) greater than 1/2 systemic systolic pressure beyond 12
hours of age]; availability of a functional echocardiogram performed using a comprehensive
imaging protocol as previously described above and stored as raw data to allow detailed offline
analysis; absence of congenital heart defect with the exception of a PDA, PFO or small
119 | P a g e

ventricular septal defect; absence of major developmental lung disorders such as congenital
diaphragmatic hernia, large abdominal wall defects, renal defects with oligohydramnios; absence
of known chromosomal anomaly. Clinical data collection: We collected the following clinical
details: gestation, birthweight, cord pH, cardiopulmonary resuscitation (CPR) at birth, 5 minute
Apgar score, use of surfactant, inhaled nitric oxide (iNO) treatment and duration, duration of
invasive ventilation and oxygen therapy, inotrope use, length of hospital stay and need for
extracorporeal membrane oxygenation (ECMO) or death.
Control group: From the echocardiographic data collected on day 1 and 2 of age in 50 well term
neonates for studies described in chapter 4 and chapter 5 (197, 198), the control comparative
group of 50 neonates was constituted by pooling data from 25 day 1 and 25 day 2 scans at
random while including only one scan per infant.
Exposure: Presence of PPHN on a comprehensive echocardiogram during the first 3 days of age.
Additional statistical considerations: Receiver operating curve analysis was performed to
investigate the utility of key echocardiographic indices (p value < 0.1 on univariate analysis) to
predict the composite outcome of death before discharge or need ECMO. Sensitivity, specificity,
positive and negative predictive values were computed where appropriate.
Sample size calculation: The mean ± SD of TAPSE in the control group was used to determine
the sample size for this study. To detect a 10% deference in mean TAPSE among PPHN
neonates, with an alpha of 0.05 and power of 90%, we needed 42 neonates in each group. Hence,
our aim was to include all eligible neonates during the study period based on above mentioned
eligibility criteria with the minimum of 42 PPHN neonates.
120 | P a g e

7.3 Results
Study population
Forty nine infants with PPHN were included in the study. Of these 38 were diagnosed
based on PDA shunt (6 right to left, 32 bidirectional), 5 based on bidirectional PFO shunt and the
remaining 6 using RVSP calculated from tricuspid regurgitant jet; which was overall measurable
in 37 (76%) cases. Cases were compared to 50 healthy controls, none of whom had tricuspid
regurgitation or right to left or bidirectional shunting across the PDA if present (20%). Table 7.1
outlines demographic features and age at scan, which were similar between groups, and clinical
features of interest for the study cohort. Cases demonstrated high RVSP and commonly required
advanced cardio-respiratory therapies including high frequency ventilation, iNO and inotropes.
Table 7.1: Baseline demographics of neonates with PPHN and controls, and clinical outcomes of neonates with
PPHN
PPHN (n= 49 ) Controls (n= 50) p value
Gestation (Weeks) 39.3 ± 1.7 39.7 ± 1.20 .18
Birth Weight (Kg) 3.37 ± 0.56 3.50 ± 0.44 .22
Male gender 25 (51%) 33 (66%) .16
Age at scan (days) 1.7 ± 0.8 1.5 ± 0.5 .22
Heart rate (Beats/min) 131 ± 17 122 ± 17 .02
RVSP (mmHg) 43 [35 – 55] - -
5 Minute Apgar Score 6 [4 – 9] 9 [9 – 9] <.01
CPR at Delivery 12 (25%) 0 (0%) -
Surfactant use 9 (18%) 0 (0%) -
Cord pH 7.11 [6.97 – 7.22] 7.24 [7.17 – 7.27] <.01
121 | P a g e

Primary diagnosis
Parenchymal lung disease
(meconium aspiration/ pneumonia)
Idiopathic
Hypoxic ischemic encephalopathy
30 (61%)
13 (27%)
6 (12%)
Total body hypothermia for hypoxic ischemic encephalopathy
19 (39%)
Invasive ventilation 47 (96%)
High frequency ventilation 24 (49%)
iNO Treatment 35 (71%)
Positive response to iNO 27/35 (77%)
Inotrope Use 43 (88%)
ECMO or Death 6 (12%)
iNO Duration (Days)* Ω 2 [1 – 10]
Days of Invasive Ventilation Ω 6 [4 – 10]
Day of Oxygen Use Ω 9 [4 – 16]
Length of Hospital Stay Ω 14 [9 – 21]
Values are presented as mean ± Standard Deviation, median [interquartile range], and count (%). *presented as median [Range]. Ωonly for neonates who survived without ECMO. None of the controls had a significant tricuspid regurgitant jet to measure RVSP. PPHN persistent pulmonary hypertension of the newborn; PAAT pulmonary artery acceleration time; RVET right ventricular ejection time; PVRI Pulmonary vascular resistance index; RVSP Right ventricular peak systolic pressure; CPR cardiopulmonary resuscitation; iNO inhaled nitric oxide; ECMO extracorporeal membrane oxygenation.
Right and Left Ventricular Function and inter-ventricular interactions
In comparison to controls, PPHN neonates demonstrated differences in several indices of
RV and LV function; with more changes seen in RV indices (Table 2 and 3). To evaluate the
confounding effect of a global perinatal ischemic insult, inter-group comparison was also
performed after exclusion of neonates diagnosed with hypoxic ischemic encephalopathy; this did
not alter the results significantly. The right ventricle in PPHN showed a small but significant
increase in linear dimensions (basal diameter in long axis view and distal diameter of the outflow
tract), but RV areas measured in the apical 4-chamber view were not different. RV areas
122 | P a g e

measured from apical 3-chamber view, pulmonary artery diameter as well as LV volume were
lower in PPHN. Both the right and the left ventricle in PPHN neonates demonstrated inferior
systolic, diastolic and global performance in comparison to healthy controls.
Table 7.2: Echocardiographic indices of right ventricular (RV) function in infants with PPHN vs. Controls
Variable A. PPHN (all patients, n= 49 )
B. PPHN (without HIE,
n=30)
C. Controls (n= 50)
p value
A vs. C
p value B vs. C
RV Dimensions Basal Diameter – 4C (cm)
1.75 ± 0.29 1.69 ± 0.28 1.75 ± 0.21 .99 .99
Basal Diameter – Long axis (cm)
2.43 ± 0.28 2.43 ± 0.32 2.14 ± 0.25 <.01 <.01
Outflow Tract – Distal (cm)
1.29 ± 0.22 1.27 ± 0.19 1.03 ± 0.10 <.01 <.01
Pulmonary Artery Diameter (cm)
0.84 ± 0.12 0.82 ± 0.12 0.94 ± 0.09 <.01 <.01
End-Diastolic Area – 4C (cm2)
4.28 ± 1.12 4.09 ± 1.11 4.27 ± 0.69 0.99 0.42
End-Systolic Area – 4C (cm2)
3.40 ± 1.06 3.23 ± 1.11 3.20 ± 0.60 0.25 0.66
End-Diastolic Area – 3C (cm2)
5.46 ± 1.56 5.20 ± 1.27 6.57 ± 1.07 <.01 <.01
End-Systolic Area – 3C (cm2)
3.52 ± 1.08 3.25 ± 0.94 4.07 ± 0.67 .01 <.01
RV-Specific Functional Measurements FAC – 4C (%) 20.80 ± 10.74 19.94 ± 11.40 25.26 ± 6.99 .02 .03 FAC – 3C (%) 35.53 ± 9.30 37.5 ± 9.95 37.90 ±6.48 .21 .87 FAC– Global (%) [=(FAC-4C + FAC-3C)/2]
29.64 ± 7.66 29.81 ± 8.52 31.67 ± 4.62 .18 .35
TAPSE (mm) 6.81 ± 1.92 7.05 ± 1.71 9.25 ± 1.30 <.01 <.01 Tissue Doppler Imaging (TDI) Measurements s’ (cm/s) 5.81 ± 1.68 6.12 ± 1.52 6.62 ± 1.14 .01 .15 e’ (cm/s) 5.71 ± 1.80 6.17 ± 2.02 7.70 ± 1.68 <.01 <.01 a’ (cm/s) 6.44 ± 1.98 6.50 ± 2.17 8.92 ± 2.51 <.01 <.01 Systolic Time (ms) 185 ± 34 182 ± 24 212 ± 25 <.01 <.01
Diastolic Time (ms) 175 ± 42 175 ± 45 203 ± 47 <.01 .01 IVRT (ms) 65 ± 22 58 ± 19 46 ± 12 <.01 <.01 e’: a’ 0.94 ± 0.30 1.00 ± 0.32 0.95 ± 0.24 .83 .52 TvE: e’ 8.51 ± 2.93 7.84 ± 2.47 6.07 ± 1.42 <.01 <.01 Systole’: Diastole’ 1.10 ± .27 1.09 ± 0.25 1.10 ± 0.30 .97 .86 Myocardial Performance Index
0.65 ± 0.37 0.59 ± 0.21 0.41 ± 0.14 <.01 <.01
Pulsed Wave Doppler and Output TvE (cm/s) 46 ± 11 44 ± 10 45 ± 9 .70 .83 TvA (cm/s) 53 ± 12 53 ± 11 55 ± 12 .29 .49 TvE: TvA 0.90 ± 0.27 0.86 ± 0.28 0.85 ± 0.16 .35 .88 PAAT (ms) 36 ± 10 34 ± 8 54 ± 17 <.01 <.01
123 | P a g e

RVET (ms) 175 ± 25 171 ± 17 214 ± 24 <.01 <.01 PVRI (RVET: PAAT) 5.17 ± 1.42 5.20 ± 1.20 4.30 ± 1.00 <.01 <.01 Pulmonary artery VTI cm/s
8.42 ± 2.66 8.11 ± 2.03 11.40 ± 3.00 <.01 <.01
Stroke Volume (ml) 1.46 ± 0.69 1.41 ± 0.59 2.39 ± 0.76 <.01 <.01 Right Ventricular Output (ml/kg/min)
189 ± 87 187 ± 78 291 ± 97 <.01 <.01
Deformation Parameters (STE) GLS – 4C (%) -16.9 ± 5.4 -18.3 ± 5.9 -21.2 ± 5.6 <.01 .04 GLS – 3C (%) -17.7 ± 6.0 -18.8 ± 5.7 -21.8 ± 5.0 <.01 .06 Overall GLS (%) [=(GLS-4C + GLS-3C)/2]
-16.9 ± 5.4 -18.6 ± 5.4 -21.6 ± 4.6 <.01 .04
Data Presented as Mean ± standard Deviation or median (interquartile range). Mean difference (95% confidence interval) only shown for parameters which differed significantly between groups. 4C apical 4-chamber view; 3C apical 3-chamber view; FAC fractional area change; TAPSE tricuspid annular plane systolic excursion; s’/e’/a’/ systolic/early diastolic/late diastolic velocities of basal segment of RV free wall; IVRT Isovolumic relaxation Time; TvE/TvA early/late tricuspid inflow velocities; VTI Velocity Time Index; STE speckle tracking echocardiography; GLS peak global longitudinal strain.
Table 7.3: Echocardiographic indices of left ventricular (LV) function in infants with PPHN vs. Controls Variable A. PPHN
(all patients, n= 49 )
B. PPHN (without HIE,
n=30)
C. Controls (n= 50)
p value
A vs. C
p value
B vs. C LV Dimensions End-Diastolic Diameter (cm)
1.71 ± 0.27 1.73 ± 0.28 1.73 ± 0.24 .73 .97
LV Length – 4C (cm) 3.09 ± 0.34 3.08 ± 0.33 3.09 ± 0.27 .99 .82 End Diastolic Volume – 4C (ml)
4.93 ±1.79 5.15 ±1.79 6.45 ± 1.23 <.01 <.01
Sphericity index (= EDV-4C/Length)
1.57 ± 0.48 1.65 ± 0.47 2.09 ± 0.42 <.01 <.01
LV-Specific Functional Measurements Simpson’s Ejection Fraction – 4C (%)
49 ± 12 51 ± 11 55 ± 9 .01 .10
Simpson’s Ejection Fraction – 2C (%)
49 ± 10 49 ± 12 55 ± 9 <.01 <.04
Simpson’s Ejection Fraction – Biplane (%)
49 ± 7 50 ± 7 55 ± 6 <.01 .01
Shortening Fraction (%) 41 ± 9 41 ± 9 40 ± 8 .49 .46 Tissue Doppler Imaging (TDI) Measurements Lateral Wall s` (cm/s) 5.29 ± 1.62 5.50 ± 1.64 4.79 ± 0.77 .09 .05 e’ (cm/s) 5.23 ± 1.74 5.30 ± 1.65 6.61 ± 1.50 <.01 <.01 a’ (cm/s) 5.67 ± 2.20 5.81 ± 2.39 5.41 ± 1.22 .52 .43 Systolic Time (ms) 162 ± 29 157 ± 22 187 ± 20 <.01 <.01 Diastolic Time (ms) 171 ± 44 174 ± 48 193 ± 35 .01 .09 IVRT’ (ms) 73 ± 23 70 ± 22 52 ± 11 <.01 <.01 e’: a’ 1.02 ± 0.42 1.01 ± 0.35 1.27 ± 0.38 <.01 <.01 MvE: e’ 11.00 ± 5.33 10.52 ± 4.37 9.12 ± 2.98 .06 .83 Systole’: Diastole’ ratio 1.01 ± 0.35 0.96 ± 0.29 1.00 ± 0.21 .82 .65
124 | P a g e

Myocardial Performance Index
0.86 ± 0.38 0.82 ± 0.29 0.61 ± 0.16 <.01 <.01
Septal Wall s` (cm/s) 3.85 ± 1.22 4.09 ± 1.22 3.65 ± 0.55 .35 .09 e’ (cm/s) 4.01 ± 1.34 4.10 ± 1.45 4.81 ± 1.08 <.01 .04 a’ (cm/s) 4.47 ± 1.59 4.52 ± 1.72 4.35 ± 0.94 .67 .65 e’: a’ 0.95 ± 0.32 0.97 ± 0.34 1.14 ± 0.39 .01 .05 Pulsed Wave Doppler and Output MvE (cm/s) 51 ± 15 51 ± 13 57 ± 9 .03 .06 MvA (cm/s) 50 ± 17 51 ± 17 52 ± 9 .62 .73 MvE: MvA 1.08 ± 0.39 1.10 ± 0.45 1.11 ± 0.27 .60 .83 Aortic VTI cm/s 10.5 ± 3.25 10.8 ± 2.65 10.07 ± 1.59 .41 .15 Stroke Volume (ml) 1.03 ± 0.44 1.14 ± 0.46 1.10 ± 0.19 .35 .59 Left Ventricular Output (ml/kg/min)
135 ± 61 153 ± 62 134 ± 26 .92 .12
Deformation Parameters (STE) GLS – 4C (%) -15.6 ± 3.9 -16.5 ± 3.5 -21.1 ± 2.4 <.01 <.01 GLS – 3C (%) -16.7 ± 4.5 -18.3 ± 4.2 -20.8 ± 2.9 <.01 .01 GLS – 2C (%) -16.7 ± 3.1 -17.5 ± 3.2 -22.3 ± 3.3 <.01 <.01 Overall GLS (%) [(GLS-4C + GLS-3C + GLS-2C)/3]
-16.7 ± 3.3 -17.8 ± 3.1 -21.4 ± 2.0 <.01 <.01
Data Presented as Mean ± Standard Deviation. Mean difference (95% confidence interval) only shown for parameters which differed significantly between groups. 4C apical 4-chamber view; 2C apical 2-chamber view; s’/e’/a’/ systolic/early diastolic/late diastolic velocities of basal segment of LV free wall and interventricular septum respectively; IVRT Isovolumic relaxation Time; MvE/MvA early/late mitral inflow velocities; VTI: Velocity Time Index; STE speckle tracking echocardiography; GLS peak global longitudinal strain.
The systolic functional indices which demonstrated least overlap in values between groups
were TAPSE for the right ventricle and GLS for both the right and the left ventricle (Figure 7.1
and 7.2). PPHN neonates also had lower RV stroke volume and output, however, LV output was
not different.
125 | P a g e

Figure 7.1: Box plot graph showing comparison of tricuspid annular plane systolic excursion (TAPSE) between neonates with persistent pulmonary hypertension of newborn (PPHN) and healthy controls.
Figure 7.2: Box plot graphs for overall global peak longitudinal strain for the right and the left ventricle in neonates with persistent pulmonary hypertension of newborn (PPHN) and healthy controls.
126 | P a g e

In neonates with PPHN, moderate but significant inter-ventricular linear correlations
were observed between functional measures of both ventricles; in the whole cohort, as well as
after exclusion of neonates with a diagnosis of HIE (Table 7.4). The strongest correlations were
found between the RV and LV GLS and the RV and LV MPI (Figure 7.3). Functional indices
did not correlate with PAAT or PVRI, while RVSP showed correlation with overall RV-GLS
and FAC-global correlated with the duration of right to left shunt across PDA.
Table 7.4. Pearson’s Product-Moment correlation coefficients for linear correlations between left ventricular (LV) and right ventricular (RV) functional and hemodynamic parameters in patients with PPHN after excluding neonates undergoing total body hypothermia for hypoxic ischemic encephalopathy (n=30)
Septal s’
LV s’
LV-EF
LV-GLS
LV MPI’
LVO LV-IVRT’
SI PVRI RVsP PDA-RL
RVO
RV s’ .49 .44 -.48 .53
FAC-global
.69 .75
TAPSE .68 .62 .45 -.51 .41 .40 .47
RV-GLS .68 .61 .69 .62 .55
RV-MPI’ .62 -.46 .56 -.46 -.58
RVO .45 -.52 .49 -.50 x
RV-IVRT’
.75 -.46 -.49
PDA-RL .79 .48 x
Correlation coefficient (r) are shown if p<0.05. Significant linear correlations were observed between functional and hemodynamic measures of both ventricles. Persistent PPHN pulmonary hypertension of newborn; TAPSE tricuspid annular plane systolic excursion; s’ peak systolic velocity measured at basal segment of RV free wall, LV free wall and interventricular septum respectively; GLS global peak longitudinal strain; FAC fractional area change; IVRT isovolumic relaxation time; MPI myocardial performance index; RVO right ventricular output; LVO left ventricular output; PVRI pulmonary vascular resistance index; RVsP right ventricular peak systolic pressure; PDA R-L duration of right to left shunt across patent ductus arteriosus measured as percentage of total cardiac cycle time; EF ejection fraction (Simpson’s); SI sphericity index (EDV-4C/LV length). There were no significant correlations with pulmonary artery acceleration time or LV end diastolic volume. Note similar analysis when conducted using data from the whole cohort revealed stronger inter-ventricular correlations than above but weaker correlation between functional measures and those indicative of severity of pulmonary pressures (data not shown above).
127 | P a g e

Figure 7.3: Among the inter-ventricular linear correlations observed between various functional indices, the strongest correlation was found between right ventricular (RV) and left ventricular (LV) overall global peak longitudinal strain (GLS) and RV and LV myocardial performance index measured using tissue Doppler imaging (MPI’). Correlation coefficient was calculate using Pearson’s product moment correlation.
Correlation with adverse outcome
Comparison of echocardiographic parameters during the first three days of life revealed
lower TAPSE and RV and LV systolic myocardial velocities for neonates who subsequently died
or needed ECMO compared to those who survived without ECMO, though these differences did
not reach statistical significance (Table 7.5). Of these parameters, lower TAPSE was most
predictive of adverse outcome. A cut off of TAPSE of 6 mm had a sensitivity of 83%, specificity
of 74%, negative predictive value (95% CI) of 97 (86, 99) % and positive predictive value of 42
(25 - 61) % (Figure 7.4).
128 | P a g e

Table 7.5: Comparison of echocardiographic indices between PPHN neonates who subsequently died or needed ECMO vs. those who survived until discharge without ECMO
Variable Death or ECMO (n=6) Survived until discharge (n=43) P Value
FAC-G (%) 22 (13, 29) 19 (12, 31) .94
TAPSE (mm) 5.2 (3.9, 5.7) 7.5 (6.0, 8.4) .05
RV s’ (cm/s) 4.4 (4.0, 5.3) 6.2 (5.0, 6.8) .08
TvE: e’ 10.8 (9.3, 11.2) 8.0 (6.6, 9.9) .28
RV IVRT’ (ms) 55 (51, 73) 64 (51, 80) 1.0
RV MPI’ 0.76 (0.60, 0.87) 0.57 (0.39, 0.70) .11
RV GLS (%) 16 (14, 18) 17 (15, 22) .67
RVO (mL/kg/min) 113 (94, 198) 187 (139, 245) .15
RVSP (mmHg) 33 (30, 45) 47 (37, 55) .17
PAAT (ms) 39 (30, 43) 33 (28, 40) .47
PVRI 4.3 (3.7, 5.6) 5.2 (4.2, 6.4) .33
Sphericity Index 1.7 (1.1, 1.9) 1.5 (1.2, 1.8) .84
LV EDV-4C (mL) 5.5 (2.9, 7.0) 4.7 (3.5, 6.0) .82
Ejection fraction (Simpson’s)
49 (43, 54) 49 (42, 58) .79
LV s’ (cm/s) 4.4 (3.5, 4.5) 5.5 (4.3, 6.3) .06
MvE: e’ 11.7 (10.9, 12.8) 9.5 (7.8, 13.0) .21
LV IVRT’ (ms) 77 (72, 91) 65 (54, 80) .15
LV MPI’ 0.76 (0.70, 0.94) 0.74 (0.62, 0.89) .58
LV GLS (%) 15 (14, 17) 17 (15, 19) .35
LVO (mL/kg/min) 110 (83, 116) 124 (98, 177) .15
All comparisons were made using Mann Whitney U test and results are presented as median (interquartile range). (‘) indicate that measurements were obtained using tissue Doppler imaging. FAC-G global fractional area change; TAPSE tricuspid annular plane systolic excursion; RV right ventricular; LV left ventricular; s’/e’ systolic/early diastolic velocities of basal segment of RV free wall and LV free wall respectively; TvE early tricuspid inflow velocity; MvE early mitral inflow velocity; IVRT’ isovolumic relaxation time; MPI’ myocardial performance index; GLS overall global peak longitudinal strain; RVO right ventricular output; RVSP Right ventricular peak systolic pressure; PAAT pulmonary artery acceleration time; PVRI Pulmonary vascular resistance index; EDV-4C end diastolic volume in apical 4 chamber view; LVO left ventricular output.
129 | P a g e

Figure 7.4: A box plot graph comparing TAPSE for neonates with persistent pulmonary hypertension of newborn (PPHN) who survived until discharge without ECMO (n=43) vs. those who either died or needed ECMO (n=6). A cut off of TAPSE of 6 mm (dotted line) had a negative predictive value (95% CI) of 97 (86, 99)% and positive predictive value of 42 (25 - 61)%.
Influence of Sex
LV functional parameters were lower in females (n=24) in comparison to males (n=25)
[GLS-4C (14.4 ± 3.5 vs. 16.8 ± 4.0%; p = .04); LV-IVRT’ (77 ± 24 vs. 64 ± 18 ms; p = .03); LV
systole’: diastole’ (1.11 ± 0.40 vs. 0.89 ± 0.22; p=.04)]. No other echocardiographic or clinical
differences were observed between males and females; with both groups having a 12% mortality
(n=3 in each group).
130 | P a g e

PDA, total body hypothermia, CPR at birth and iNO treatment
RV and LV functional parameters were lower in patients with a PDA shunting either
bidirectional or right to left (n=38) in comparison to neonates without a PDA (n=10) [median
(IQR) FAC-3C [33 (27, 38) vs 43 (37, 49)%, p<.01]; RV GLS [15 (13, 17) vs. 22 (19, 23)%,
p<.01]; RV systole’: diastole’ [1.02 (0.84, 1.21) vs. 1.25 (1.15, 1.40), p=.03]; LV s’ [4.7 (4.1,
5.9) vs. 6.1 (5.8, 7.0) cm/s, p<.01]; LV systole’: diastole’ [0.92 (0.72, 1.11) vs. 1.24 (1.03, 1.33),
p=.01]; MvE: MvA [1.07 (0.90, 1.23) vs. 0.91 (0.79, 0.96), p=.03]; LVO [114 (91, 163) vs. 170
(127, 210), p=.01]]. Within neonates with PDA, a right to left shunt was associated with lower
values of functional indices than bidirectional shunt (data not shown).
PPHN neonates who were receiving treatment by total body hypothermia (n=19)
demonstrated lower RV systolic [pLS-4C (14.7 ± 3.6% vs. 18.2 ± 5.9%; p=.01)], RV diastolic
[IVRT (78 ± 21 ms vs. 58 ± 19 ms; p<.01)] and LV systolic [GLS (14.9 ± 3.1 vs. 17.8 ± 3.1);
p=.02; LVO (106 ± 48 vs. 153 ± 62 ml/min/kg; p<.01] performance. Additional exposure to CPR
at birth (n=8) vs. hypothermia without needing CPR (n=11) was associated with further
worsening in diastolic performance of both the right ventricle [TvE: e’ (7.1 ± 4.4 vs. 11.3 ± 1.6;
p=.02)] and the left ventricle [IVRT’ (75 ± 19ms vs. 84 ± 33ms; p=.02)]. No differences were
observed in PAAT, PVRI and RVSP in relation to any of the tested variable. Treatment with iNO
or responsiveness to iNO did not correlate with any echocardiographic parameter except a lower
PVRI in PPHN neonates who received iNO (data not shown).
7.4 Discussion
Our study looked at functional parameters for LV and RV function in infants with PPHN.
We confirmed that during the first three days of life, PPHN is associated with multiple adverse
131 | P a g e

alterations in biventricular systolic and diastolic function. TAPSE and longitudinal strain are the
indices of RV systolic function most affected in PPHN, FAC-4C was marginally lower. This is
keeping with the previous report by Zakaria et al, in which 30 neonates with pulmonary
hypertension [median (IQR) age at scan 6 (1-11) days] demonstrated lower TAPSE, but not FAC
(43). Though controls were of more advanced age in this study [age at scan 10 (5, 52) days].
Similar to our study, RV s’ was also found to be low in PPHN, while strain was not measured.
The preservation of FAC in PPHN may reflect the neonatal right ventricle’s effort to preserve its
ejection fraction in the presence of a high afterload, however, it may also indicate a limitation of
our sample size or a high measurement variability associated with FAC calculations, which
requires manually tracing the endocardial borders in a heavily trabeculated neonatal right
ventricle; also previously reported by us (197). Although FAC may be maintained by right
ventricle’s radial or circumferential function as opposed to the longitudinal function detected by
other parameters, this will have to be investigated in future studies. Nevertheless, our findings of
lower RVO in PPHN in spite of preserved FAC and a lack of association between FAC values
and adverse clinical outcomes suggest against utility of FAC in this patient population.
One of the significant finding of this study was the presence of biventricular cardiac
dysfunction in PPHN, with changes seen in systolic and diastolic function of both ventricles. In
addition, use of a comprehensive approach allowed us to investigate and describe the presence of
inter-ventricular correlations between several functional parameters. These findings may be
explained by one or a combination of factors including common underlying etiology responsible
for high pulmonary pressures and cardiac dysfunction, impact of RV dysfunction on the left
ventricle via adverse ventriculo-ventricular interactions and secondary effect of cardiorespiratory
instability and associated treatment strategies on cardiac function such as, hypoxia, acidosis, use
132 | P a g e

of high frequency ventilation and inotropes. Although it was not feasible to delineate individual
contribution of each of these factors, our study provide some important clues. Hypoxic ischemic
encephalopathy and its treatment with hypothermia was an important confounding etiology as
these infants had suffered a significant perinatal global ischemic insult and had a rectal
temperature ranging from 33.5 to 34.5 degrees at the time of the scan. Our results, however,
remained unchanged when analysis was repeated after excluding these neonates, suggesting
cardiac dysfunction in PPHN to be relatively independent of the underlying etiology. Several
mechanisms are known to govern adverse inter-ventricular interactions in pulmonary
hypertension including, shared myocardial fibres between ventricles, dysfunction of the shared
septal wall, lower pulmonary blood flow resulting in low LV filling, transmission of intra-cavity
diastolic pressure via interventricular septum and mechanical effects due to large RV size,
leftward bowing of the interventricular septum and pericardial constraint (14, 73, 75, 84, 221,
222). We did not find significant RV dilatation in neonates with PPHN. This suggests that in
PPHN, early in disease process, adverse inter-ventricular interaction, if at all at play, is not
secondary to mechanical factors or pericardial constraint. Whether adverse inter-ventricular
interactions exists in PPHN and is mediated by other mechanisms, as suggested by our finding of
lower LV volume (indicating reduced LV filling) and septal diastolic dysfunction or whether
cardiac dysfunction is secondary to overall clinical instability frequently seen in this disorder and
not directly related to the high pulmonary pressures, will have to be examined in future studies;
these should ideally be investigated in experimental animal models. Our finding of a relative lack
of association between functional parameters and markers of severity of pulmonary vascular
disease (PAAT, PVRI, RVSP) as well as treatment with iNO points towards latter to be the case.
Our interesting observation of a lack of RV dilatation in PPHN could either be explained by the
133 | P a g e

fact that the observed RV dysfunction in early disease was secondary to factors other than
exposure to high afterload or may relate to the relative immaturity of the neonatal myocardium,
which is known to characterized by a higher proportion of non-compliant tissues such as
collagen (220). Nevertheless, our study demonstrates that PPHN is a global disorder and
highlights the importance of evaluating function for both ventricles irrespective of the underlying
etiology.
Of the studies that have examined the hemodynamics in neonates with PPHN, some have
concluded that low LVO is a common occurrence (37, 99, 219). This is contrary to our finding
and may reflect the fact that previous studies either used older controls or compared their data
with previously published ‘normal’ neonatal reference ranges, which did not account for specific
postnatal age. Our control data was prospectively collected on day 1 and 2 of life. This may also
explain why the LVO values observed in our control cohort were lower than what was
considered as cut off to define abnormal by previous investigators (< 150 mls/min/kg). The
standard validated LVO measurement technique was used in our study, as explicitly described
elsewhere (175, 198). PPHN neonates had lower RVO, which, at least in part, may reflect lower
left to right contribution of the PFO shunt because of the increased right sided pressure in
comparison to controls; all of whom had a left to right shunting PFO. Our results suggests that in
PPHN, PFO shunt along with heart rate may be important factors in maintaining normal range
LVO, which is an indicator of blood flow to pre-ductal organs including brain.
Recent studies have examined the relationship between RV functional indices and outcome
defined as death or need for ECMO in neonates with PPHN (44, 185). Agarwal and colleagues
examined 117 PPHN infants and found RV systole to diastole ratio measured using color flow
Doppler as the best predictor. Malowitz et al reported TAPSE (sensitivity and specificity of 56%
134 | P a g e

and 85% respectively for values < 4 mm) and RV GLS (sensitivity and specificity of 52% and
77% respectively for values ≥ -9%) to be most predictive. We also found TAPSE, albeit a
different cut off (6 mm with sensitivity and specificity of 83% and 74% respectively), but not
strain to be associated with adverse outcome. This difference could reflect differences in study
population as evidenced by a high incidence of adverse outcome in these studies (62% and 30%
respectively) and their inclusion of neonates with congenital diaphragmatic hernia. We chose to
exclude these infants along with other developmental lung disorders as these are inherently
different conditions, which are probably better studied as a separate cohort (45). The 12%
occurrence of death or need for ECMO observed in our study is keeping with the previous
epidemiological reports of neonates with PPHN, suggesting representativeness of our disease
cohort (33, 223). Another difference between our study and the study by Malowitz et al is the
methodology used for measurements. In their study, all measurements were performed offline on
compressed DICOM images (30 frames per second) - TAPSE by measuring the difference in the
distance between tricuspid lateral annulus and transducer interface in diastole and systole and
strain by using Tomtec Velocity Vector Imaging software. In comparison, we measured TAPSE
from M-mode images acquired online at the time of scanning (> 1000 frames per second) and
strain offline on raw data images (100 - 120 frame per second) using a different vendor software
(184). A limitation is that our estimated rate of adverse outcome was based on a small number of
infants and will therefore require confirmation in a larger study.
In this study, we identified previously unknown, risk factors associated with functional
echocardiographic abnormalities within the PPHN cohort. These include female sex, hypoxic
ischemic encephalopathy and therapeutic total body hypothermia, need for CPR at birth, and
presence of a ductal shunt as well as right to left shunt across PDA (clinically can be detected by
135 | P a g e

presence of pre-ductal saturations higher than post-ductal). Given the small sample size in our
study, these results can only be considered as preliminary. Nevertheless, these findings are in
line with that of Malowitz et al, who found a predominant right to left PDA shunt to be
associated with the need for ECMO or death in PPHN.
The current data suggest from a clinical outcome perspective, TAPSE, a simple bedside
measure of RV function, may be a useful parameter for identifying high risk infants with PPHN.
However, this observation is based on small number of retrospective studies and should be
confirmed prospectively in a larger cohort. A major advantage of using multiple indices for
assessment of ventricular function is that it allows for inter-parameter corroboration, as observed
in the primary and secondary analyses of our study; which may lower the risk of being misled by
a random chance finding. This is particularly important in neonates due to non-feasibility of
invasive investigations and a higher chance of multiplying measurement errors due to small
patient size. While we recognize that measuring all indices described in this study would not be
pragmatic in routine day-to-day intensive care practice, we suggest that echocardiographic
evaluation in PPHN should be as comprehensive as feasible and include both RV and LV
function. Special attention should be paid to TAPSE as it may help identifying infants at the
highest risk of adverse outcome.
We also found that even though indices of the severity of pulmonary hemodynamics were
grossly different in PPHN cohort compared to controls, these or iNO treatment did not correlate
with clinical outcomes. This suggest that PPHN may be similar to pulmonary hypertensive
disorders in older patients, where symptomology and clinical outcomes are now known to be
governed less by the severity of disease than by effect of RV function; which in itself is variable
between individuals and is at least partially independent of the measured pulmonary pressures
136 | P a g e

(23, 218). It is plausible that an appropriate evaluation of biventricular function in these high risk
neonates early in the disease course may help delineate underlying pathophysiology and
characterize cardiac dysfunction, and enable titration of therapeutic interventions to individual
patient needs (224). This may well improve patient outcomes, which have otherwise remained
unchanged in spite of the widespread use of pulmonary vasodilator agents. Given the lack of
invasive hemodynamic monitoring in neonates, the non-specific nature of symptoms and
difficulties in eliciting RV specific clinical signs, it is critical for clinicians to have a high index
of suspicion and low threshold for evaluation of RV function in PPHN.
In conclusion, I demonstrate that PPHN is a disorder frequently characterized by global
cardiac dysfunction. In comparison to age appropriate controls, PPHN neonates demonstrate
worsening in several echocardiographic indices of RV and LV systolic and diastolic function
during the first three days of age; which were independent of HIE being the underlying etiology.
TAPSE during the first three days of age identifies neonates at most risk of subsequent adverse
clinical outcome. A pressure loaded neonatal right ventricle during early postnatal life is
characterized by a relative lack of dilatation but demonstrates evidence of significant inter-
ventricular functional correlations.
137 | P a g e

Chapter 8: Project summary and clinical significance
138 | P a g e

8.1 Project summary and future questions
Right ventricular dysfunction is an established and important predictor of outcomes in
several cardio-respiratory disorders in older patients including congestive heart failure, valvular
heart disease, the post-operative period after cardiac surgery, myocardial infarction and
congenital heart diseases (8, 84). RV dilatation is a predictor of mortality in acute respiratory
distress syndrome (225). Absence of a right ventricle in Fontan’s circulation results in chronic
progressive multi-organ failure secondary to chronic venous congestion (6, 7). It is noteworthy,
however, that patients with Eisenmenger’s syndrome and pulmonary stenosis remain
asymptomatic for decades as the right ventricle adapts to high afterload by undergoing
hypertrophy (86, 87). In no other condition however the relevance of RV function more
appreciated than in PAH. In chronic PAH, irrespective of the underlying etiology and method
used for its assessment (cardiac catherization, MRI, echocardiography), studies have consistently
found indices of RV function to be more predictive of symptoms and clinical outcomes than
indices representing severity of pulmonary vascular disease (15). The ability of the right
ventricle to preserve function varies between patients and disease states and is at least in part is
independent of the degree of pulmonary arterial pressure elevation (13). Significant functional
interactions also exist between the left and right ventricle (221).
Very little is known about heart function in newborn infants in either health or disease
states. The immediate period following birth is unique and is characterized by an increase in
pulmonary blood flow, a rapid (followed by gradual) decrease in PVR and closure of fetal shunts
(196, 215). The specific timing and rate of these events in human neonates are not well known.
The adaptation of an immature heart, in particular the right ventricle, during this phase of
physiological ‘pulmonary hypertension’ has not been studied. This information is clinically
139 | P a g e

important as it enables clinicians to understand the pathophysiological alterations associated with
disease states presenting during this high-risk period. Pulmonary hypertensive disorders are not
infrequent in the setting of the NICU (39). Dysregulation of postnatal transition, primarily failure
of the PVR to decrease to normal levels, results in the well-known syndrome of PPHN, which is
characterized by severe hypoxic respiratory failure secondary to persistence of high RV afterload
after birth (226). Despite the widespread use of iNO, the high rates of mortality and morbidities
associated with this disorder have largely remained unchanged over the last two decades (38). In
addition, underlying RV dysfunction is thought to be an important contributor. Over the last
decade, cPHT has been described in the setting of CNLD (227), a complication affecting more
than half ELBW infants (47). A number of prospective and retrospective studies have now
established that cPHT affects 1 in every 3 cases of CNLD and these patients have a higher rate of
mortality, as well as short term respiratory morbidities (55, 56, 179, 228, 229). Most deaths in
this context occur secondary to RV failure, diagnosis is usually made late in the disease course
and is limited by the use of crude qualitative criteria. It remains unclear how - or if - an immature
right ventricle adapts to a chronic gradual increase in afterload. Further, the significance of RV
function and/or dilation, as well as the use of echocardiographic measures for early identification
of high-risk infants for targeted treatment trials remains unexplored.
One of the primary reasons for these knowledge gaps is the difficulty in clinical assessment
of cardiac health in neonates. The symptoms associated with RV failure are nonspecific and may
overlap with those arising secondary to parenchymal lung disease which is a common occurrence
in these patients. Clinical signs of RV failure, frequently utilized in older patients, are difficult to
elicit in neonates. Definitive investigations like cardiac catheterization and CMRI are generally
not feasible and can only be obtained sporadically, late in the disease course. Echocardiography
140 | P a g e

remains the clinical 'gold standard' investigation to evaluate heart function for these patients, but
until recently evaluation was limited to qualitative assessments. Recent technological
advancements have enabled the development of echocardiography indices for appraisal of RV
size and function in older patients and now in neonates (197, 198). Normative data for TAPSE
and TDI derived myocardial systolic velocity are well established for both term and preterm
neonates (62, 63). There are, however, limited data regarding feasibility, relative reliability and
normal data for many other indices. Our understanding regarding the neonatal right ventricle and
how it responds to acute and/or chronic exposure to increased afterload, as well as its interaction
with the left ventricle remain unknown.
The overall aim for the studies included in this thesis was, to develop tools to help provide
comprehensive, quantitative, reliable, reproducible and pragmatic evaluation of biventricular
cardiac function and pulmonary hemodynamics in newborn infants. We then investigated the
utility of these tools in advancing our knowledge of neonatal cardiopulmonary physiology in
health and disease; specifically, during the immediate postnatal period to describe normal
cardiovascular adaptation in healthy babies and second, in the setting of PPHN, to describe its
value in a disease state. During my clinical fellowship, prior to starting my graduate studies in
the Department of Physiology, I developed a comprehensive echocardiography imaging protocol
specifically for use in neonates, as described in Chapter 2 and Chapter 3. In addition to
incorporating existing functional indices, I developed novel indices from views which may allow
quantification of RV size and function independent of septal motion, an important confounding
variable during the neonatal period. These previously undescribed indices included the linear
dimension of the ‘depth' of the right ventricle (B-PLAX), the area of the posterior RV cavity
(EDA-3C), the functional contribution of the RV infundibulum (FAC-3C) and longitudinal
141 | P a g e

function of its inferior wall (GLS-3C). Subsequently, in the prospective studies described in
Chapter 4 and Chapter 5, I confirmed the feasibility of employing this imaging protocol to
assess RV and LV functional indices during the immediate neonatal period (197, 198). These
studies allowed me to generate relative measurement reliability data for these parameters and
produced a comprehensive set of normal values for the first two days of life in healthy term
neonates. The results obtained from these studies corroborated with previously established data
for TAPSE and TDI, as well as LV longitudinal strain values reported in smaller studies (150,
151); thus supporting the validity of my derivation cohort. In addition, I established the cogency
of these measurements for use in the immediate postnatal period by demonstrating a lack of
appreciable change between the first and second day of life in relation to the anticipated
physiological change in cardiac loading conditions and closure of fetal shunts. The first scan on
day 1 of life, however, in those studies, was performed between 12 to 18 hours of age. Although
this matched the average age at which neonates suffering from disorders of postnatal transition
are commonly evaluated, it was beyond the period when peak changes in loading conditions are
anticipated.
Following this, in another prospective study, described in Chapter 6, I sequentially studied
15 healthy term neonates shortly after birth and ascertained the value of my techniques and
methods by successfully describing detailed cardiopulmonary adaptive changes associated with
birth during the first day of life. Prior to this, our understanding of circulatory changes after birth
was mostly based on animal experiments (24). In this study, I not only confirmed the occurrence
of the expected decrease in PVR and closure of the ductus arteriosus in human neonates but, also
for the first time, provided time-specific, quantitative, physiological circulatory data regarding
postnatal transition in humans. I believe this has a high potential of immediate clinical
142 | P a g e

translation. In this study, I acquired a number of novel facts regarding human transitional
circulation. I demonstrated that in humans, despite the reduction of pulmonary to systemic
pressure ratio, the decrease in pulmonary arterial pressure, after the first 20 minutes of age, may
be slower during the first 10 to 12 hours of life. Further, in spite of major changes in loading
conditions and increase in stroke output, the right and left ventricular outputs remained relatively
stable throughout the first day of life. This was owing to the changes in heart rate and
directionality of shunting across the DA and FO. The ratio of the right and left ventricular output
found in this study closely matched a recent observation using similar methods in normal human
fetuses. This observation is in keeping with the persistence of fetal RV dominance during the
first day of postnatal life. In addition to the alterations in indices of PVR and blood flow, I also
observed significant changes in echocardiographic indices of heart function, particularly the right
ventricle. This data suggested a transient physiological reduction in RV function at < 30 minutes
of age in comparison to measurements performed during the second half of the first day. This has
not been described previously and may suggest a relative vulnerability of the neonatal right
ventricle to high afterload conditions immediately after birth. Finally, I confirmed the
representativeness of these values by performing a time-specific comparison with similar data
obtained prospectively from a previous cohort of healthy neonates included in the studies
described in Chapter 4 and Chapter 5.
To investigate the utility of this protocol in a population of babies with abnormal
cardiopulmonary transition, in Chapter 7, I evaluated a retrospective cohort of neonates with
PPHN who had comprehensive echocardiographic evaluation during the first three days of life.
Use of the imaging protocol developed for this work, allowed me to gain several novel insights
into the pathophysiology associated with this serious disorder of postnatal transition. I observed
143 | P a g e

that unlike older patients, the neonatal right ventricle, early in the disease process, did not show
significant dilatation even in the presence of dysfunction, suggesting a relative absence of
heterotropic adaptive mechanism during early postnatal life. In addition, I found that PPHN is
characterized by global cardiac dysfunction, a finding which persisted in spite of exclusion of
neonates who developed PPHN secondary to a perinatal ischemic insult. This could either
suggest that the underlying mechanisms resulting in dysregulation of postnatal transition or
subsequent clinical instability may affect both ventricles or the presence of inter-ventricular
functional dependence during early postnatal life where the reduction in LV function is a ‘side-
effect’ of RV dysfunction. Additional novel findings of this study included the presence of
significant linear correlations between echocardiographic functional indices of both ventricles
and the identification of risk factors associated with relative adverse cardiac performance within
the PPHN cohort; these have not been previously described and included, female sex, total body
hypothermia in the setting of hypoxic ischemic encephalopathy, the need for CPR at birth and
the presence of a right to left shunt across a PDA and/or PFO. The finding of a lower TAPSE
during the first three days of life being predictive of subsequent adverse outcome of death or
need for ECMO in neonates with PPHN is important. Although this finding was based on a small
patient sample, it corroborates the finding in a recent report by Malowitz et al in which TAPSE,
longitudinal strain and persistent presence of a right to left shunt across PDA was found to be
predictive of adverse clinical outcome in neonates with severe PPHN. The incidence of adverse
outcome was high in this cohort which, unlike my study, included neonates with congenital
diaphragmatic hernia. Small observational studies conducted using TDI derived myocardial
indices in neonates with congenital diaphragmatic hernia have also reported presence of RV
diastolic dysfunction early in the postnatal course to be predictive of subsequent longer duration
144 | P a g e

of need for respiratory support. This supports my observation of the presence of RV dysfunction
and its correlation with adverse clinical outcome in PPHN.
Successful completion of this work has given me the impetus, the necessary reliable
clinical tools and collaborative expertize to continue advancing the knowledge in the ‘untapped’
field of cardiopulmonary physiology in newborn infants. During the conduct of my graduate
studies, I have developed a longitudinal research plan with a clear medium to long term focus on
conducting early interventional randomized control clinical trials, based on carefully described
pathophysiologic mechanisms, targeting RV function in neonatal pulmonary hypertensive
disorders (Figure 8.1). Some of the unanswered questions that I wish to address in my ongoing
and future work and are described in more detailed in Chapter 9 include the following:
• Which of the previously described echocardiographic indices most accurately reflect
RV size and function in neonates with pulmonary hypertension (Validation study)?
• How does a neonatal right ventricle respond to a chronic, but gradually increasing,
exposure to high afterload?
• Can functional indices of RV performance, developed during this work, help early
identification of preterm neonates who subsequently get diagnosed with ‘significant’
chronic pulmonary hypertension?
145 | P a g e

Figure 8.1: A schematic presentation of the long term research strategy developed during the conduct of this thesis, highlighting research questions for my ongoing and future work.
8.2 Clinical relevance
The clinical significance of individual studies have been highlighted in the discussion
section of respective chapters. Overall, the studies conducted as a part of this thesis have a high
potential of early clinical translation. Currently, there are major knowledge gaps in our
understanding of cardiovascular physiology in neonatal disease states and its role as a potential
contributor to the high rate of adverse outcomes observed in certain conditions such as acute or
146 | P a g e

chronic PHT. This may relate in part to a general lack of clinical awareness and in part to
unavailability of reliable measurement tools. As previously discussed, clinical appraisal of heart
function is challenging in neonates, in particular for assessment of RV function.
Echocardiography is commonly used in a qualitative manner, presumably driven by a
technological lag in imaging equipment, but in light of advancements in imaging techniques this
is now changing. High quality imaging equipment suitable for quantitative estimation of
ventricular function in smallest of neonates is now widely available in many NICUs.
Increasingly, many neonatal intensivists are undertaking training in advanced functional
echocardiography and utilizing cardiac imaging in routine clinical practice. For instance, the
majority of Canadian tertiary NICUs now have a program in targeted neonatal echocardiography,
most established in the last 5 to 7 years (230). Similar trends have also been reported from
Australia and New Zealand (231). Neonatologist-performed functional echocardiograms are
commonly followed by changes in clinical management (232, 233). Current utilization of
quantitative echocardiography indices for decision making by neonatologists, however, is based
on normative data which can be described as patchy at best. This may lead to incorrect
assumptions and in appropriate treatment decisions. For instance, LVO < 150 ml/min/kg has
commonly been considered as a cut off threshold to define “critically low LVO” in neonates
(219). This assumption was based on old publications of neonatal ‘normative data’, which did
not account for specific postnatal age. My systematic prospective study, however, showed that
normal neonates when assessed at rest in their natural environment commonly have LVO below
this cut off in the immediate postnatal period. In addition, interpretation of echocardiographic
variables during the immediate postnatal period is marred by a limited understanding of
physiological cardiovascular adaptation and mechanisms of disease. Current approaches to
147 | P a g e

cardiac assessment, definitions of thresholds of concern, standard therapeutic approaches are
often based on dogma and clinical presumptions. There is an urgent need to evolve to a more
thoughtful approach where appropriate diagnostic tools are developed and tested, normality is
understood, pathological deviations from normality are recognized, at risk situations and patients
are timely identified, such that therapies are based on sound physiological principles and their
efficacy can be reliably monitored. High quality, comprehensive and systematic investigations
are critical to advance this field. The studies conducted during the course of my graduate studies
addresses some of these key issues. In the studies conducted, I was able to provide standard
norms for normal heart dimensions that may allow enhanced insight into states of cardiac under-
filling or chamber dilation. Similarly, I describe standard norms of heart function and describe
their interplay with the physiologic modulators of normal postnatal adaptation. These data
provide evidence that suggest that neonatal right ventricle may be vulnerable to dysfunction on
persistent exposure to high afterload. These data may allow for accurate diagnosis of cardiac
dysfunction during this high-risk period. Through my data in the PPHN cohort, I provide a
concrete example of how a pathological state of abnormal transition influences cardiac
performance, which may relate to subsequent adverse clinical outcome. I believe, the knowledge
generated through this body of work will lead to heightened awareness among clinicians
regarding the importance of cardiac function and its assessment in sick neonates, provide tools
and evidence which will inform day-to-day cardiac imaging and its interpretation in the NICUs
and stimulate and guide future efforts to understand cardio-pulmonary pathophysiology and its
clinical relevance in neonatal disease states. All of this may lead to earlier identification and
treatment of at-risk neonates as well as may help plan early targeted interventional clinical trials.
148 | P a g e

Chapter 9: Limitations and future directions
149 | P a g e

9.1 Limitations
There are several limitations of the studies conducted during the course of this work, as
enlisted below:
Chapters 4 and 5:
• Although this study demonstrated the feasibility of reliably quantifying RV and LV size and
function in neonates, which remained largely unaffected by physiological changes in loading
conditions during postnatal transition, I am unable to comment on the impact of unmeasured
but pathological loading conditions on functional parameters.
• I cannot exclude that factors like sex, mode of delivery and the presence of a PDA may have
had a small effect on cardiac performance. I did perform univariate analysis to test these
factors and found no associations, but this study was not designed to detect such relations.
Nevertheless, all PDAs observed in this study were small and hemodynamically
insignificant.
• My finding of linear relationship between BW and RV and LV dimensions can only be
considered applicable to the neonatal period and for appropriately grown neonates (i.e. BW
between 10th to 90th percentile). Future studies should evaluate a wider range of birth
weights (e.g. small or large for gestational age neonates, premature neonates) and age (e.g.
during first year of life), to further explore the extent of this relationship.
• Similarly, though I did not find any relation between gestational age and functional
parameters, this is likely due to the narrow range of gestational age of our study cohort (37
to 42 weeks); hence, the data generated in this study can only be considered relevant to term
150 | P a g e

gestation. Subsequent studies should attempt employing a similar comprehensive imaging
protocol for preterm neonates.
• I did not explore relationship of echocardiographic parameters with body surface area. This
was done to ensure relative accuracy and clinical suitability of the study results. BW is the
most commonly used anthropometric parameter in neonates, while length measurements are
more prone to error, especially in critically ill neonates. Further, the commonly used
formulas for calculating BSA need further validation in neonates (234).
• This study did not investigate the effect of using equipment from different vendors on strain
measurements. The longitudinal strain values reported in this study and may not be
applicable to other vendors (188).
• Although I found similar results on day 1 and 2 of life, due to the timing of scans, I may
have missed the period of peak changes in transitional circulation, which are likely to occur
within the first few hours of age. Nevertheless, the timing of the first scan was based on the
anecdotal experience in sick neonates, where echocardiograms are usually preceded by
medical assessment and stabilization.
• From a normative data point of view, these studies had a relatively small sample size;
however, this still is the largest prospective systematic study in this population with an a
priori aim of establishing normal values.
Chapter 6:
• This observational data is acquired from a small number of neonates and is assumed to be
representative for all populations. There may be sex, racial or other confounders (e.g. mode
of delivery) that we were unable to consider. Nevertheless, although the data acquired in this
study was from a small number of neonates, the fact that it was acquired sequentially and
151 | P a g e

closely fitted with a larger historical cohort in a time sensitive manner indicate the validity
of my findings.
• All measurements reported in this study were derived using echocardiography, which is
subject to operator dependent errors and variability in measurement. Invasive catheterization
or magnetic resonance imaging may provide better estimates of systemic and pulmonary
hemodynamics, myocardial function and the influence of loading conditions, but these are
not feasible in the majority of neonates, particularly in healthy states. Although, there are
limitations, echocardiography represents a feasible and in the hands of expert operators, may
provide reliable measures of changes in hemodynamics and cardiac function.
• The data presented in this study can only be considered applicable to the measurement
techniques used, which have been explicitly described in Chapters 3 (197, 198).
Chapter 7:
• Similar to previous studies in this field, my observations are also limited by being
retrospective in nature, which meant a relatively variable age at scan and potential
confounding effect of pre-scan clinical course and therapeutic interventions including
resuscitation at birth, mode of invasive ventilation, inotropes, therapeutic hypothermia and
iNO. This, however, is also reflective of real life clinical setting where stabilization, medical
interventions and transfer to tertiary centres commonly precede imaging.
• Because of the relatively small sample size, I could not examine the independent effect of
high pulmonary pressure versus potential confounding variables mentioned above on cardiac
dysfunction. For the same reason, the results of the secondary analysis can only be
considered as preliminary. It is likely that this study was under-powered to identify all
potential risk factors associated with cardiac dysfunction in PPHN. This study, however, is
152 | P a g e

the first report of comprehensive cardiac function assessment in this patient population and
provides novel pathophysiological insights as well as identified previously unreported risk
factors.
• Another limitation of this study is the lack of gold standard tests, namely cardiac
catherization and CMRI. It is thus possible that my finding of a lack of RV dilatation in
PPHN may relate to the relative insensitivity of individual echocardiographic measures to
identify changes in RV size. Use of a comprehensive protocol and corroboration of findings
by several parameters, however, makes this as well as being misled by a chance finding less
likely. Nevertheless, future studies should examine the validity of echocardiographic
measures of cardiac size and function in neonates.
• This being a clinical physiological study performed in a vulnerable patient population using
non-invasive tests, is not able to provide confirmation of the suspected underlying
pathophysiology. For instance, I cannot confirm or rule out the presence of inter-ventricular
functional dependence in PPHN or identify the relative contribution of various potential
mechanisms mediating it. This study, however, provides important clues and highlight areas
for future definitive investigations. These in the context of PPHN will have to be explored
using suitable animal models.
• As echocardiography is not a mandatory investigation at the study centre, I cannot rule out a
degree of selection bias in the patient population, which may consist of more severely
affected neonates. Nevertheless, the results of this study support the importance of early
assessment of cardiac function in neonates with PPHN.
9.2 Rationale for future directions and clinical significance
153 | P a g e

As demonstrated in the studies included in this thesis, there are now a number of reliable
surrogate echocardiographic indices of RV size and function which can be applied to the
neonatal population. This is important as echocardiography is the main non-invasive imaging
technique that is routinely available for neonates and is ideally suited for longitudinal
assessments in an acute care setting. Although the concurrent use of several assessment
techniques may be desirable in research, due to time constraints, it is not pragmatic for day-to-
day intensive care clinical practice. The accuracy of individual markers in their representation of
size and function of the neonatal right ventricle is not known, particularly in the presence of high
afterload. Echocardiography measures depend on geometric assumptions, hence their relative
accuracy may vary based on patient population and underlying disorder. It is therefore important
to investigate the validity of these measures by examining their correlation with a gold standard
test. As highlighted before, cardiac catheterization is an invasive procedure, typically not feasible
in neonates due to the high risk of complications; CMRI is a safe and feasible alternative. CMRI-
derived RV volumes and ejection fraction are validated techniques for quantifying RV size and
function respectively. A major advantage of CMRI is that, unlike echocardiography, the
technique of ventricular volumetry does not rely on geometric assumptions as it segments the
chamber volumes throughout the cardiac cycle through a series of contiguous slices aligned
across the short axis of the heart; making this the current non-invasive gold standard for the
assessment of RV size and function. In addition, cine phase contrast CMRI provides a robust
quantification of pulmonary and systemic blood flow (235). CMRI is devoid of exposure to
radiation, it does not require contrast media and has been shown to be feasible in neonates
without the use of sedation (feed and wrap method) (236). CMRI has been demonstrated to be
feasible, safe and has been successfully used to study and validate echocardiographic
154 | P a g e

hemodynamic measures related to the left ventricle and PDA in stable preterm neonates late in
NICU course (236). It is, however, expensive and cumbersome, often requiring out-of-facility
patient transfers and is available only in specialized centers. Nevertheless, CMRI can be
performed in stable and relatively mature infants, making it an ideal method to inform and
improve neonatal echocardiography practices. As a follow up to my previous work, I intend to
undertake a prospective study with the aim of identifying key echocardiography indices for
longitudinal monitoring of RV health in a high-risk population of neonates; specifically, I plan to
evaluate preterm neonates with known cPHT. In this study, I aim to recruit 25 preterm neonates
with moderate-severe CNLD and an echocardiographic diagnosis of cPHT. Each patient will
have a right ventricle-focused echocardiogram (method under investigation) and CMRI (clinical
reference method). Corresponding quantitative indices of RV size, function and blood flow will
be measured for comparison. At the end of the recruitment phase, relationships between
corresponding echocardiographic and CMRI measures will be examined to define the accuracy
and relative reproducibility of echocardiographic measurements. This will be the first study to
appraise the accuracy of echocardiography parameters for RV function in preterm neonates. The
data generated from this study will help to establish a validated and generalizable
echocardiographic surveillance protocol applicable to this patient group. This protocol will
impact clinical care and could benefit future clinical trials. To date, I have secured funding for
this prospective project and will begin recruitment following completion of my graduate studies.
Another objective of my immediate future work, is to investigate the feasibility of earlier
identification of ELBW infants at highest risk of developing cPHT secondary to CNLD. cPHT is
increasingly being recognized as an important determinant of mortality and pre-discharge
respiratory morbidity in ELBW infants. Echocardiography is the clinical ‘gold standard’
155 | P a g e

investigation; however, to date, many of the diagnostic criteria used are crude and inadequate for
early identification in the majority of cases. With technological advancements and the
development of newer imaging modalities, as highlighted by my current and other collaborative
work (64, 66, 193), it is now feasible to serially study quantitative changes in PVR and RV
function in the smallest of neonates, thus providing opportunities for early recognition of disease
(Figure 9.1). In this study, my plan is to recruit a cohort of ELBW infants and serially study
changes in PVR and RV function from the third week of age until 36 weeks of corrected
gestational age, when a diagnosis of CNLD and cPHT is typically made. At the end of the
recruitment phase, I will determine sensitivity and specificity of echocardiographic markers
obtained in the third week of age by comparing infants with versus without cPHT. Early
identification of infants at increased risk of cPHT has direct clinical relevance as it raises the
possibility of disease modification. several potential therapeutic agents such as, inhaled nitric
oxide, milrinone (phosphodiesterase 3 inhibitor), sildenafil (phosphodiesterase 5 inhibitor),
prostacyclin and bosentan (endothelin receptor antagonist) are already available (39); however,
the therapeutic impact of these drugs could be limited unless used early in the disease process,
before a more ‘fixed’ increase in PVR secondary to pulmonary vascular remodeling occurs.
Previous physiological studies have demonstrated a partial vasodilatory effect as a result of these
therapies when used later in established disease, presumably because of pulmonary vascular
remodeling (237-239). This will be the first study examining the predictive value of novel
echocardiographic markers in neonatal cPHT. Early identification is likely to have a significant
impact on preventative or curative treatment strategies. I have already obtained all necessary
approvals for this project and aim to initiate recruitment alongside the previously mentioned
validation study soon after completion of my graduate work.
156 | P a g e

Figure 9.1: One of my immediate future plan is to refine diagnostic criteria for cPHT in preterm neonates with CNLD and identify echocardiographic parameters which best identify at-risk neonates early in disease course.
In addition to earlier recognition of at-risk patients, the use of our comprehensive imaging
protocol in cPHT patients will facilitate longitudinal assessment of the response of the neonatal
right ventricle to chronic increase in afterload and its associated impact on LV performance. Our
study investigating PPHN has demonstrated a relative lack of heterotropic adaptation in the
immediate neonatal period, in keeping with the lack of reference to RV dilatation in previous
studies. Studies of cPHT in preterm neonates, however, have consistently noted the presence of
RV dilatation, indicating a different response in chronic versus acute pressure loading conditions.
Indeed, this has also been our clinical observation (Figure 9.2). One of my goals in this study of
preterm cPHT will be to systematically evaluate neonatal RV physiology in the presence of
chronic pressure loading.
157 | P a g e

Figure 9.2: A parasternal short axis view obtained using 2D echocardiography in a preterm neonate with significant chronic pulmonary hypertension demonstrating severe RV dilatation.
9.3 Final remarks
The importance of incorporating RV function in the study of pulmonary hypertension is
being increasingly recognized as a primary clinical and research target for evaluating the
efficacy of existing therapies and in the development of new ones (1). In spite of commercial
availability and clinical use of a plethora of pulmonary vasodilator therapies, clinical outcomes
of patients with PAH has not shown consistent improvements (23). An overarching focus on
promoting pulmonary vasodilation without considering the impact of employed strategies on
RV functional recovery has been cited by field experts as one of the major reasons behind this
observation. Similarly, the use of pulmonary vasodilators, most notably iNO, have consistently
demonstrated an improvement in acute symptoms of PPHN, but this has not translated into
better survival or long-term clinical outcomes (38, 239). Milrinone, a commonly used inodilator,
158 | P a g e

has recently been shown in a small observational study to improve RV function in term neonates
with PPHN when symptoms were not responsive to standard treatment with inhaled nitric oxide
(224); this improvement was temporarily associated with the resolution of clinical symptoms.
Though pulmonary hypertension in neonates has been a subject of pre-clinical and clinical
research for several decades, the field of RV function is still in its infancy; at least in part due to
the long-standing problem of a relative inability to quantify RV function in small neonatal
hearts. With the current availability of reliable measurement tools, this may now change. The
aim of the studies described herein was to address some of these knowledge gaps and advance
the field of clinical cardiopulmonary physiology in neonates, in particular understanding the role
of the right ventricle in pulmonary hypertensive disorders. My current and future planned work,
as described in the previous section, will provide ideal grounds for realizing my medium to
long-term goal of conducting mechanistic therapeutic trials targeting the specific subgroup of
patients at highest risk of adverse outcomes. This will serve two key purposes – first, avoidance
of exposure to unnecessary pharmacological agents for neonates not at high risk of subsequent
adverse outcome will ensure a favourable risk-benefit profile for therapeutic interventions, as
well as reduce treatment costs. Second, targeting a high-risk group of patients will potentially
lower the required sample size for subsequent clinical trials.
159 | P a g e

Appendix: Additional figures and data
160 | P a g e

Chapter 4
Figure 6.2: Measurement of peak longitudinal strain of RV inferior wall (GLS-3C) using speckle tracking echocardiography from one of the study infants. The endocardial border was manually traced from RV 3-chamber view. The tracking was performed automatically by the software but was visually inspected before accepting results. The pLS values for individual segments (represented graphically by color-coded lines) was averaged to generate an overall pLS-3C.
161 | P a g e

Figure 4.3: Bland-Altman plots showing intra- and inter-observer measurement variability was lower for biplane-fractional area change (global-FAC) in comparison to single-plane measurements acquired from RV apical 4 chamber view (FAC-4C) or from RV apical 3 chamber view (FAC-3C).
162 | P a g e

Figure 4.4: Bland-Altman plots showing intra- and inter-observer measurement variability was relatively lower for global peak longitudinal strain (GLS-global) obtained by averaging GLS acquired from RV apical 4 chamber view (GLS-4C) and from RV apical 3 chamber view (GLS-3C) in comparison to its individual components.
163 | P a g e

Figure 4.5: Bland-Altman plots for inter and intra observer measurement variability for myocardial performance index calculated using time periods measured from color flow Doppler (MPI) and tissue Doppler imaging (MPI’). MPI’ was more reproducible than MPI, particularly for the same observer.
164 | P a g e

Figure 4.6: Modest linear correlation observed between RV peak systolic myocardial velocity (s’) measured from TDI and STE-derived peak longitudinal strain of RV lateral wall
Chapter 7
The cardiac functional profile in neonates with PPHN also varied significantly in relation
to the type of shunt pattern at the level of PDA and/or PFO (Table 7.6). A pure right to left shunt
at the level of the PDA (n=6) or PFO (n=7) was associated with inferior cardiac performance. On
the other hand, echocardiograms with a left to right shunt at the level of PFO (n=16) were
characterized by better LV systolic and diastolic indices, even when occurring in association
with a bidirectional or right to left ductal shunt (n=12). Fewer infants with a left to right PFO
shunt needed treatment with inotropes (69% vs. 97%; p=.01). No differences were observed in
PAAT, PVRI and RVSP in relation to shunt patterns.
165 | P a g e

Table 7.6: Alterations in echocardiographic indices in relation to the type of shunt pattern in neonates with persistent pulmonary hypertension of the newborn during first three days of age
PDA shunt right to left (n=6) vs. PDA bidirectional/absent (n=43)
PFO shunt right to left (n=7) vs. PFO left to right/absent or bidirectional (n=42)
PFO shunt left to right (16) vs. right to left/ bidirectional/absent (33)
PFO shunt left to right + PDA shunt right to left/ bidirectional (n=12) vs. others (37)
↓ TAPSE
(4.9 vs. 7.5 mm)
↑ RV MPI
(0.70 vs. 0.56)
↓ RV basal diameter – 4C
(1.62 vs. 1.83 cm)
↑ IVS e’/a’
(1.04 vs. 0.87)
↓ RV s’
(3.9 vs. 6.4 cm/s)
↓ Sphericity index (EDV-4C/LV length)
(1.18 vs. 1.67)
↓ RV End Diastolic Area – 4 Chamber
(3.7 vs. 4.3 cm2)
↑ MvE/MvA
(1.09 vs. 0.94)
↓ RV GLS
(13.7 vs. 18.0 %)
↓ LV EDV-4C
(3.47 vs. 5.5 mls)
↑ LV EF
(Simpson’s biplane)
(55 vs. 46%)
↑ RV IVRT
(93 vs. 60 ms)
↓ LV EF (Simpson’s biplane)
(43 vs. 50%)
↑ MvE/MvA
(1.06 vs. 0.94)
↑ RV MPI
(0.84 vs. 0.56)
↓ LV GLS
(13.6 vs. 17.4)
↓ Sphericity index (EDV-4C/LV length)
(1.03 vs. 1.7)
↓ LV EDV-4C
(3.25 vs. 5.22)
↓ LV EF (Simpson’s biplane)
(42 vs. 50%)
↓ LV s’
(4.1 vs 5.6 cm/s)
↓ LV e’
(2.9 vs. 5.1 cm/s)
↑ LV IVRT
(98 vs. 65 ms)
↓ LVO (102 vs. 141 ml/min/kg)
↓ LV GLS
(12.0 vs. 18.4%)
Interpretation: Relatively lower RV and LV systolic,
Interpretation: Relatively lower RV global function
Interpretation: Interpretation:
166 | P a g e

diastolic and global function. Higher RV diastolic pressure.
and LV systolic function. Higher RV diastolic pressure.
Relatively less RV dilatation and better LV systolic and diastolic performance.
Relatively better septal and LV diastolic performance.
Results are presented as medians and are only listed if p<0.05. All comparisons were made using Mann Whitney U test. There was no infant with a left to right shunting PDA in this cohort. Exclusion of infants with absent PDA (n=10) or absent PFO (n=7) did not change the results (data not shown). Only three neonates had both PDA and PFO shunting right to left. No differences were observed in indices of pulmonary vascular resistance and RV systolic pressure. RV right ventricular; LV left ventricular; IVS interventricular septum; TAPSE tricuspid annular plane systolic excursion; s’/e’/a’/ systolic/early diastolic/late diastolic velocities of basal segment of RV free wall, LV free wall and interventricular septum respectively; GLS global peak longitudinal strain; IVRT isovolumic relaxation time; MPI myocardial performance index; EDV-4C end diastolic volume in apical 4 chamber view; EF ejection fraction; LVO left ventricular output.
167 | P a g e

References
168 | P a g e

1. Voelkel NF, Quaife RA, Leinwand LA, Barst RJ, McGoon MD, Meldrum DR, et al. Right ventricular function and failure: report of a National Heart, Lung, and Blood Institute working group on cellular and molecular mechanisms of right heart failure. Circulation. 2006;114(17):1883-91. 2. Taquini AC, Fermoso JD, Aramendia P. Behavior of the right ventricle following acute constriction of the pulmonary artery. Circ Res. 1960;8:315-8. 3. Fineberg MH, Wiggers CJ. Compensation and failure of the right ventricle. American Heart Journal.11(3):255-63. 4. Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. 1971;26(3):240-8. 5. Kreutzer G, Galindez E, Bono H, De Palma C, Laura JP. An operation for the correction of tricuspid atresia. J Thorac Cardiovasc Surg. 1973;66(4):613-21. 6. de Leval MR. The Fontan circulation: a challenge to William Harvey? Nature clinical practice Cardiovascular medicine. 2005;2(4):202-8. 7. Rychik J. The Relentless Effects of the Fontan Paradox. Seminars in thoracic and cardiovascular surgery Pediatric cardiac surgery annual. 2016;19(1):37-43. 8. Haddad F, Hunt SA, Rosenthal DN, Murphy DJ. Right ventricular function in cardiovascular disease, part I: Anatomy, physiology, aging, and functional assessment of the right ventricle. Circulation. 2008;117(11):1436-48. 9. Nagel E, Stuber M, Hess OM. Importance of the right ventricle in valvular heart disease. Eur Heart J. 1996;17(6):829-36. 10. Baker BJ, Wilen MM, Boyd CM, Dinh H, Franciosa JA. Relation of right ventricular ejection fraction to exercise capacity in chronic left ventricular failure. Am J Cardiol. 1984;54(6):596-9. 11. Engler R, Ray R, Higgins CB, McNally C, Buxton WH, Bhargava V, et al. Clinical assessment and follow-up of functional capacity in patients with chronic congestive cardiomyopathy. Am J Cardiol. 1982;49(8):1832-7. 12. Bleeker GB, Steendijk P, Holman ER, Yu CM, Breithardt OA, Kaandorp TA, et al. Acquired right ventricular dysfunction. Heart. 2006;92 Suppl 1:i14-8. 13. Bogaard HJ, Natarajan R, Henderson SC, Long CS, Kraskauskas D, Smithson L, et al. Chronic pulmonary artery pressure elevation is insufficient to explain right heart failure. Circulation. 2009;120(20):1951-60.
169 | P a g e

14. Naeije R, Manes A. The right ventricle in pulmonary arterial hypertension. European respiratory review : an official journal of the European Respiratory Society. 2014;23(134):476-87. 15. Naeije R. Assessment of right ventricular function in pulmonary hypertension. Current hypertension reports. 2015;17(5):35. 16. Nienaber CA, Spielmann RP, Wasmus G, Montz R, Mathey DG, Bleifeld W. Right ventricular ejection fraction from equilibrium krypton-81m blood pool scans: a noninvasive predictor of pulmonary arterial hypertension. Eur Heart J. 1987;8(3):297-307. 17. Burgess MI, Bright-Thomas RJ, Ray SG. Echocardiographic evaluation of right ventricular function. Eur J Echocardiogr. 2002;3(4):252-62. 18. Champion HC, Michelakis ED, Hassoun PM. Comprehensive invasive and noninvasive approach to the right ventricle-pulmonary circulation unit: state of the art and clinical and research implications. Circulation. 2009;120(11):992-1007. 19. Lankhaar JW, Westerhof N, Faes TJ, Gan CT, Marques KM, Boonstra A, et al. Pulmonary vascular resistance and compliance stay inversely related during treatment of pulmonary hypertension. Eur Heart J. 2008;29(13):1688-95. 20. Ghio S, Schirinzi S, Pica S. Pulmonary arterial compliance: How and why should we measure it? Global cardiology science & practice. 2015;2015(4):58. 21. Hunter KS, Lee PF, Lanning CJ, Ivy DD, Kirby KS, Claussen LR, et al. Pulmonary vascular input impedance is a combined measure of pulmonary vascular resistance and stiffness and predicts clinical outcomes better than pulmonary vascular resistance alone in pediatric patients with pulmonary hypertension. Am Heart J. 2008;155(1):166-74. 22. Voelkel NF, Gomez-Arroyo J, Abbate A, Bogaard HJ. Mechanisms of right heart failure-A work in progress and a plea for failure prevention. Pulmonary circulation. 2013;3(1):137-43. 23. Gurtu V, Michelakis ED. A Paradigm Shift Is Needed in the Field of Pulmonary Arterial Hypertension for Its Entrance Into the Precision Medicine Era. Circ Res. 2016;119(12):1276-9. 24. Rudolph AM. Distribution and regulation of blood flow in the fetal and neonatal lamb. Circ Res. 1985;57(6):811-21. 25. Mielke G, Benda N. Cardiac output and central distribution of blood flow in the human fetus. Circulation. 2001;103(12):1662-8. 26. Rasanen J, Wood DC, Debbs RH, Cohen J, Weiner S, Huhta JC. Reactivity of the human fetal pulmonary circulation to maternal hyperoxygenation increases during the second half of pregnancy: a randomized study. Circulation. 1998;97(3):257-62.
170 | P a g e

27. Gao Y, Raj JU. Regulation of the pulmonary circulation in the fetus and newborn. Physiol Rev. 2010;90(4):1291-335. 28. Fediuk J, Dakshinamurti S. A role for actin polymerization in persistent pulmonary hypertension of the newborn. Canadian journal of physiology and pharmacology. 2015;93(3):185-94. 29. Haworth SG. Pulmonary endothelium in the perinatal period. Pharmacological reports : PR. 2006;58 Suppl:153-64. 30. Hooper SB, Te Pas AB, Lang J, van Vonderen JJ, Roehr CC, Kluckow M, et al. Cardiovascular transition at birth: a physiological sequence. Pediatr Res. 2015;77(5):608-14. 31. Dawes GS. Pulmonary circulation in the foetus and new-born. British medical bulletin. 1966;22(1):61-5. 32. Joyce JJ, Dickson PI, Qi N, Noble JE, Raj JU, Baylen BG. Normal right and left ventricular mass development during early infancy. Am J Cardiol. 2004;93(6):797-801. 33. Walsh-Sukys MC, Tyson JE, Wright LL, Bauer CR, Korones SB, Stevenson DK, et al. Persistent pulmonary hypertension of the newborn in the era before nitric oxide: practice variation and outcomes. Pediatrics. 2000;105(1 Pt 1):14-20. 34. Lipkin PH, Davidson D, Spivak L, Straube R, Rhines J, Chang CT. Neurodevelopmental and medical outcomes of persistent pulmonary hypertension in term newborns treated with nitric oxide. J Pediatr. 2002;140(3):306-10. 35. Eriksen V, Nielsen LH, Klokker M, Greisen G. Follow-up of 5- to 11-year-old children treated for persistent pulmonary hypertension of the newborn. Acta Paediatr. 2009;98(2):304-9. 36. Hosono S, Ohno T, Kimoto H, Shimizu M, Takahashi S, Harada K. Developmental outcomes in persistent pulmonary hypertension treated with nitric oxide therapy. Pediatrics international : official journal of the Japan Pediatric Society. 2009;51(1):79-83. 37. Peterson AL, Deatsman S, Frommelt MA, Mussatto K, Frommelt PC. Correlation of echocardiographic markers and therapy in persistent pulmonary hypertension of the newborn. Pediatr Cardiol. 2009;30(2):160-5. 38. Finer NN, Barrington KJ. Nitric oxide for respiratory failure in infants born at or near term. Cochrane Database Syst Rev. 2006(4):CD000399. 39. Jain A, McNamara PJ. Persistent pulmonary hypertension of the newborn: Advances in diagnosis and treatment. Seminars in fetal & neonatal medicine. 2015;20(4):262-71. 40. Sernich S, Carrasquero N, Lavie CJ, Chambers R, McGettigan M. Noninvasive assessment of the right and left ventricular function in neonates with congenital diaphragmatic
171 | P a g e

hernia with persistent pulmonary hypertension before and after surgical repair. Ochsner J. 2006;6(2):48-53. 41. Patel N, Mills JF, Cheung MM. Assessment of right ventricular function using tissue Doppler imaging in infants with pulmonary hypertension. Neonatology. 2009;96(3):193-9; discussion 200-2. 42. Aggarwal S, Stockman PT, Klein MD, Natarajan G. The right ventricular systolic to diastolic duration ratio: a simple prognostic marker in congenital diaphragmatic hernia? Acta Paediatr. 2011;100(10):1315-8. 43. Zakaria D, Sachdeva R, Gossett JM, Tang X, O'Connor MJ. Tricuspid annular plane systolic excursion is reduced in infants with pulmonary hypertension. Echocardiography. 2015;32(5):834-8. 44. Malowitz JR, Forsha DE, Smith PB, Cotten CM, Barker PC, Tatum GH. Right ventricular echocardiographic indices predict poor outcomes in infants with persistent pulmonary hypertension of the newborn. Eur Heart J Cardiovasc Imaging. 2015;16(11):1224-31. 45. Moenkemeyer F, Patel N. Right ventricular diastolic function measured by tissue Doppler imaging predicts early outcome in congenital diaphragmatic hernia. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2014;15(1):49-55. 46. Jain D, Bancalari E. Bronchopulmonary dysplasia: clinical perspective. Birth defects research Part A, Clinical and molecular teratology. 2014;100(3):134-44. 47. Shah PS, Sankaran K, Aziz K, Allen AC, Seshia M, Ohlsson A, et al. Outcomes of preterm infants <29 weeks gestation over 10-year period in Canada: a cause for concern? J Perinatol. 2012;32(2):132-8. 48. Bhandari V. Postnatal inflammation in the pathogenesis of bronchopulmonary dysplasia. Birth defects research Part A, Clinical and molecular teratology. 2014;100(3):189-201. 49. Bhatt AJ, Pryhuber GS, Huyck H, Watkins RH, Metlay LA, Maniscalco WM. Disrupted pulmonary vasculature and decreased vascular endothelial growth factor, Flt-1, and TIE-2 in human infants dying with bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;164(10 Pt 1):1971-80. 50. Wong PM, Lees AN, Louw J, Lee FY, French N, Gain K, et al. Emphysema in young adult survivors of moderate-to-severe bronchopulmonary dysplasia. The European respiratory journal. 2008;32(2):321-8. 51. Coalson JJ. Pathology of chronic lung disease of early infancy. In: Bland RD, Coalson JJ, eds Chronic lung disease in early infancy New York: Marcel Dekker; 2000:85-124. 2000.
172 | P a g e

52. An HS, Bae EJ, Kim GB, Kwon BS, Beak JS, Kim EK, et al. Pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. Korean circulation journal. 2010;40(3):131-6. 53. Bhat R, Salas AA, Foster C, Carlo WA, Ambalavanan N. Prospective analysis of pulmonary hypertension in extremely low birth weight infants. Pediatrics. 2012;129(3):e682-9. 54. del Cerro MJ, Sabate Rotes A, Carton A, Deiros L, Bret M, Cordeiro M, et al. Pulmonary hypertension in bronchopulmonary dysplasia: clinical findings, cardiovascular anomalies and outcomes. Pediatric pulmonology. 2014;49(1):49-59. 55. Khemani E, McElhinney DB, Rhein L, Andrade O, Lacro RV, Thomas KC, et al. Pulmonary artery hypertension in formerly premature infants with bronchopulmonary dysplasia: clinical features and outcomes in the surfactant era. Pediatrics. 2007;120(6):1260-9. 56. Kim DH, Kim HS, Choi CW, Kim EK, Kim BI, Choi JH. Risk factors for pulmonary artery hypertension in preterm infants with moderate or severe bronchopulmonary dysplasia. Neonatology. 2012;101(1):40-6. 57. Koroglu OA, Yalaz M, Levent E, Akisu M, Kultursay N. Cardiovascular consequences of bronchopulmonary dysplasia in prematurely born preschool children. Neonatology. 2013;104(4):283-9. 58. Slaughter JL, Stenger MR, Reagan PB. Variation in the use of diuretic therapy for infants with bronchopulmonary dysplasia. Pediatrics. 2013;131(4):716-23. 59. Waruingi W, Mhanna MJ. Pulmonary hypertension in extremely low birth weight infants: characteristics and outcomes. World journal of pediatrics : WJP. 2014;10(1):46-52. 60. Levy PT, Holland MR, Sekarski TJ, Hamvas A, Singh GK. Feasibility and reproducibility of systolic right ventricular strain measurement by speckle-tracking echocardiography in premature infants. J Am Soc Echocardiogr. 2013;26(10):1201-13. 61. Levy PT, Dioneda B, Holland MR, Sekarski TJ, Lee CK, Mathur A, et al. Right ventricular function in preterm and term neonates: reference values for right ventricle areas and fractional area of change. J Am Soc Echocardiogr. 2015;28(5):559-69. 62. Koestenberger M, Nagel B, Ravekes W, Urlesberger B, Raith W, Avian A, et al. Systolic right ventricular function in preterm and term neonates: reference values of the tricuspid annular plane systolic excursion (TAPSE) in 258 patients and calculation of Z-score values. Neonatology. 2011;100(1):85-92. 63. Koestenberger M, Nagel B, Ravekes W, Gamillscheg A, Pichler G, Avian A, et al. Right ventricular performance in preterm and term neonates: reference values of the tricuspid annular peak systolic velocity measured by tissue Doppler imaging. Neonatology. 2013;103(4):281-6.
173 | P a g e

64. James AT, Corcoran JD, Jain A, McNamara PJ, Mertens L, Franklin O, et al. Assessment of myocardial performance in preterm infants less than 29 weeks gestation during the transitional period. Early Hum Dev. 2014;90(12):829-35. 65. James AT, Corcoran JD, Franklin O, El-Khuffash AF. Clinical utility of right ventricular fractional area change in preterm infants. Early Hum Dev. 2016;92:19-23. 66. James AT, Corcoran JD, Breatnach CR, Franklin O, Mertens L, El-Khuffash A. Longitudinal Assessment of Left and Right Myocardial Function in Preterm Infants Using Strain and Strain Rate Imaging. Neonatology. 2016;109(1):69-75. 67. Kelly RG, Brown NA, Buckingham ME. The arterial pole of the mouse heart forms from Fgf10-expressing cells in pharyngeal mesoderm. Dev Cell. 2001;1(3):435-40. 68. Mjaatvedt CH, Nakaoka T, Moreno-Rodriguez R, Norris RA, Kern MJ, Eisenberg CA, et al. The outflow tract of the heart is recruited from a novel heart-forming field. Dev Biol. 2001;238(1):97-109. 69. Waldo KL, Kumiski DH, Wallis KT, Stadt HA, Hutson MR, Platt DH, et al. Conotruncal myocardium arises from a secondary heart field. Development. 2001;128(16):3179-88. 70. Meilhac SM, Esner M, Kelly RG, Nicolas JF, Buckingham ME. The clonal origin of myocardial cells in different regions of the embryonic mouse heart. Dev Cell. 2004;6(5):685-98. 71. Meilhac SM, Kelly RG, Rocancourt D, Eloy-Trinquet S, Nicolas JF, Buckingham ME. A retrospective clonal analysis of the myocardium reveals two phases of clonal growth in the developing mouse heart. Development. 2003;130(16):3877-89. 72. Zaffran S, Kelly RG, Meilhac SM, Buckingham ME, Brown NA. Right ventricular myocardium derives from the anterior heart field. Circ Res. 2004;95(3):261-8. 73. Sanchez-Quintana D, Garcia-Martinez V, Climent V, Hurle JM. Morphological changes in the normal pattern of ventricular myoarchitecture in the developing human heart. Anat Rec. 1995;243(4):483-95. 74. Yu W, Li SN, Chan GC, Ha SY, Wong SJ, Cheung YF. Transmural strain and rotation gradient in survivors of childhood cancers. Eur Heart J Cardiovasc Imaging. 2013;14(2):175-82. 75. Smerup M, Nielsen E, Agger P, Frandsen J, Vestergaard-Poulsen P, Andersen J, et al. The three-dimensional arrangement of the myocytes aggregated together within the mammalian ventricular myocardium. Anatomical record. 2009;292(1):1-11. 76. Liebman J. Congenital Malformations of the Heart: Embryology, Anatomy, and Operative Considerations. JAMA: The Journal of the American Medical Association. 1976;236(15):1752.
174 | P a g e

77. Ho SY, Nihoyannopoulos P. Anatomy, echocardiography, and normal right ventricular dimensions. Heart. 2006;92 Suppl 1:i2-13. 78. Geva T, Powell AJ, Crawford EC, Chung T, Colan SD. Evaluation of regional differences in right ventricular systolic function by acoustic quantification echocardiography and cine magnetic resonance imaging. Circulation. 1998;98(4):339-45. 79. Henein MY, Golden Ratio C, Zhao Y, Nicoll R, Sun L, Khir AW, et al. The human heart: application of the golden ratio and angle. International journal of cardiology. 2011;150(3):239-42. 80. Anderson RH, Webb S, Brown NA, Lamers W, Moorman A. Development of the heart: (2) Septation of the atriums and ventricles. Heart. 2003;89(8):949-58. 81. Sarnoff SJ, Mitchell JH, Gilmore JP, Remensnyder JP. Homeometric autoregulation in the heart. Circ Res. 1960;8:1077-91. 82. Forfia PR, Vaidya A, Wiegers SE. Pulmonary heart disease: The heart-lung interaction and its impact on patient phenotypes. Pulmonary circulation. 2013;3(1):5-19. 83. Bartelds B, Borgdorff M, Berger R. Right Ventricular Adaptation in Congenital Heart Diseases. Journal of Cardiovascular Development and Disease. 2014;1(1):83-97. 84. Haddad F, Doyle R, Murphy DJ, Hunt SA. Right ventricular function in cardiovascular disease, part II: pathophysiology, clinical importance, and management of right ventricular failure. Circulation. 2008;117(13):1717-31. 85. van de Veerdonk MC, Kind T, Marcus JT, Mauritz GJ, Heymans MW, Bogaard HJ, et al. Progressive right ventricular dysfunction in patients with pulmonary arterial hypertension responding to therapy. J Am Coll Cardiol. 2011;58(24):2511-9. 86. Jurcut R, Giusca S, Ticulescu R, Popa E, Amzulescu MS, Ghiorghiu I, et al. Different patterns of adaptation of the right ventricle to pressure overload: a comparison between pulmonary hypertension and pulmonary stenosis. J Am Soc Echocardiogr. 2011;24(10):1109-17. 87. Hopkins WE, Waggoner AD. Severe pulmonary hypertension without right ventricular failure: the unique hearts of patients with Eisenmenger syndrome. Am J Cardiol. 2002;89(1):34-8. 88. Guyton AC, Lindsey AW, Gilluly JJ. The limits of right ventricular compensation following acute increase in pulmonary circulatory resistance. Circ Res. 1954;2(4):326-32. 89. Greyson CR. The right ventricle and pulmonary circulation: basic concepts. Rev Esp Cardiol. 2010;63(1):81-95.
175 | P a g e

90. von Anrep G. On the part played by the suprarenals in the normal vascular reactions of the body. The Journal of physiology. 1912;45(5):307-17. 91. Solaro RJ. Mechanisms of the Frank-Starling law of the heart: the beat goes on. Biophys J. 2007;93(12):4095-6. 92. Bristow MR, Zisman LS, Lowes BD, Abraham WT, Badesch DB, Groves BM, et al. The pressure-overloaded right ventricle in pulmonary hypertension. Chest. 1998;114(1 Suppl):101S-6S. 93. Sonnenblick EH. Implications of muscle mechanics in the heart. Fed Proc. 1962;21:975-90. 94. Rowland DG, Gutgesell HP. Noninvasive assessment of myocardial contractility, preload, and afterload in healthy newborn infants. Am J Cardiol. 1995;75(12):818-21. 95. van Loon RL, Roofthooft MT, Delhaas T, van Osch-Gevers M, ten Harkel AD, Strengers JL, et al. Outcome of pediatric patients with pulmonary arterial hypertension in the era of new medical therapies. Am J Cardiol. 2010;106(1):117-24. 96. Tissot C, Beghetti M. Pediatric pulmonary hypertension. In: Humbert M, Lynch JP, eds Pulmonary hypertension New York: Informa Healthcare; 2009:434-454. 2009. 97. Benatar A, Clarke J, Silverman M. Pulmonary hypertension in infants with chronic lung disease: non-invasive evaluation and short term effect of oxygen treatment. Archives of disease in childhood Fetal and neonatal edition. 1995;72(1):F14-9. 98. Valdes-Cruz LM, Dudell GG, Ferrara A. Utility of M-mode echocardiography for early identification of infants with persistent pulmonary hypertension of the newborn. Pediatrics. 1981;68(4):515-25. 99. Evans N, Kluckow M, Currie A. Range of echocardiographic findings in term neonates with high oxygen requirements. Arch Dis Child Fetal Neonatal Ed. 1998;78(2):F105-11. 100. Galie N, Torbicki A, Barst R, Dartevelle P, Haworth S, Higenbottam T, et al. Guidelines on diagnosis and treatment of pulmonary arterial hypertension. The Task Force on Diagnosis and Treatment of Pulmonary Arterial Hypertension of the European Society of Cardiology. Eur Heart J. 2004;25(24):2243-78. 101. Members ATF, Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery J-L, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J. 2009;30(20):2493-537.
176 | P a g e

102. Bossone E, D'Andrea A, D'Alto M, Citro R, Argiento P, Ferrara F, et al. Echocardiography in pulmonary arterial hypertension: from diagnosis to prognosis. J Am Soc Echocardiogr. 2013;26(1):1-14. 103. Dragulescu A, Mertens LL. Developments in echocardiographic techniques for the evaluation of ventricular function in children. Arch Cardiovasc Dis. 2010;103(11-12):603-14. 104. Mertens LL, Friedberg MK. Imaging the right ventricle--current state of the art. Nat Rev Cardiol. 2010;7(10):551-63. 105. Sanchez AA, Levy PT, Sekarski TJ, Hamvas A, Holland MR, Singh GK. Effects of Frame Rate on Two-Dimensional Speckle Tracking-Derived Measurements of Myocardial Deformation in Premature Infants. Echocardiography. 2014. 106. Negrine RJ, Chikermane A, Wright JG, Ewer AK. Assessment of myocardial function in neonates using tissue Doppler imaging. Archives of disease in childhood Fetal and neonatal edition. 2012;97(4):F304-6. 107. Murase M, Ishida A, Morisawa T. Left and right ventricular myocardial performance index (Tei index) in very-low-birth-weight infants. Pediatr Cardiol. 2009;30(7):928-35. 108. Mori K, Nakagawa R, Nii M, Edagawa T, Takehara Y, Inoue M, et al. Pulsed wave Doppler tissue echocardiography assessment of the long axis function of the right and left ventricles during the early neonatal period. Heart. 2004;90(2):175-80. 109. Levy PT, Holland MR, Sekarski TJ, Hamvas A, Singh GK. Feasibility and reproducibility of systolic right ventricular strain measurement by speckle-tracking echocardiography in premature infants. J Am Soc Echocardiogr. 2013;26(10):1201-13. 110. Sheehan F, Redington A. The right ventricle: anatomy, physiology and clinical imaging. Heart. 2008;94(11):1510-5. 111. Damiano RJ, Jr., La Follette P, Jr., Cox JL, Lowe JE, Santamore WP. Significant left ventricular contribution to right ventricular systolic function. Am J Physiol. 1991;261(5 Pt 2):H1514-24. 112. Hoffman D, Sisto D, Frater RW, Nikolic SD. Left-to-right ventricular interaction with a noncontracting right ventricle. J Thorac Cardiovasc Surg. 1994;107(6):1496-502. 113. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39 e14. 114. Rudski LG, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the
177 | P a g e

American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23(7):685-713; quiz 86-8. 115. Lopez L, Colan SD, Frommelt PC, Ensing GJ, Kendall K, Younoszai AK, et al. Recommendations for quantification methods during the performance of a pediatric echocardiogram: a report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J Am Soc Echocardiogr. 2010;23(5):465-95; quiz 576-7. 116. Levy PT, Machefsky A, Sanchez AA, Patel MD, Rogal S, Fowler S, et al. Reference Ranges of Left Ventricular Strain Measures by Two-Dimensional Speckle-Tracking Echocardiography in Children: A Systematic Review and Meta-Analysis. J Am Soc Echocardiogr. 2016;29(3):209-25 e6. 117. El-Khuffash AF, Jain A, Dragulescu A, McNamara PJ, Mertens L. Acute changes in myocardial systolic function in preterm infants undergoing patent ductus arteriosus ligation: a tissue Doppler and myocardial deformation study. J Am Soc Echocardiogr. 2012;25(10):1058-67. 118. Saleemi MS, Bruton K, El-Khuffash A, Kirkham C, Franklin O, Corcoran JD. Myocardial assessment using tissue doppler imaging in preterm very low-birth weight infants before and after red blood cell transfusion. J Perinatol. 2013;33(9):681-6. 119. Matter M, Abdel-Hady H, Attia G, Hafez M, Seliem W, Al-Arman M. Myocardial performance in asphyxiated full-term infants assessed by Doppler tissue imaging. Pediatr Cardiol. 2010;31(5):634-42. 120. Abdel-Hady HE, Matter MK, El-Arman MM. Myocardial dysfunction in neonatal sepsis: a tissue Doppler imaging study. Pediatric critical care medicine : a journal of the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies. 2012;13(3):318-23. 121. Iwashima S, Sekii K, Ishikawa T, Itou H. Serial change in myocardial tissue Doppler imaging from fetus to neonate. Early Hum Dev. 2013;89(9):687-92. 122. Weidemann F, Eyskens B, Sutherland GR. New ultrasound methods to quantify regional myocardial function in children with heart disease. Pediatr Cardiol. 2002;23(3):292-306. 123. Isaaz K, Thompson A, Ethevenot G, Cloez JL, Brembilla B, Pernot C. Doppler echocardiographic measurement of low velocity motion of the left ventricular posterior wall. Am J Cardiol. 1989;64(1):66-75. 124. Eriksen BH, Nestaas E, Hole T, Liestol K, Stoylen A, Fugelseth D. Longitudinal assessment of atrioventricular annulus excursion by grey-scale m-mode and colour tissue Doppler imaging in premature infants. Early Hum Dev. 2013;89(12):977-82.
178 | P a g e

125. Hiarada K, Orino T, Yasuoka K, Tamura M, Takada G. Tissue doppler imaging of left and right ventricles in normal children. The Tohoku journal of experimental medicine. 2000;191(1):21-9. 126. Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol. 1997;30(6):1527-33. 127. Nestaas E, Stoylen A, Fugelseth D. Myocardial performance assessment in neonates by one-segment strain and strain rate analysis by tissue Doppler - a quality improvement cohort study. BMJ Open. 2012;2(4). 128. Kazanci E, Karagoz T, Tekinalp G, Ozkutlu S, Yurdakok M, Yigit S, et al. Myocardial performance index by tissue Doppler in bronchopulmonary dysplasia survivors. Turk J Pediatr. 2011;53(4):388-96. 129. Gillebert TC, Van de Veire N, De Buyzere ML, De Sutter J. Time intervals and global cardiac function. Use and limitations. Eur Heart J. 2004;25(24):2185-6. 130. Alp H, Karaarslan S, Baysal T, Cimen D, Ors R, Oran B. Normal values of left and right ventricular function measured by M-mode, pulsed doppler and Doppler tissue imaging in healthy term neonates during a 1-year period. Early Hum Dev. 2012;88(11):853-9. 131. Kutty S, Zhou J, Gauvreau K, Trincado C, Powell AJ, Geva T. Regional dysfunction of the right ventricular outflow tract reduces the accuracy of Doppler tissue imaging assessment of global right ventricular systolic function in patients with repaired tetralogy of Fallot. J Am Soc Echocardiogr. 2011;24(6):637-43. 132. Bijnens BH, Cikes M, Claus P, Sutherland GR. Velocity and deformation imaging for the assessment of myocardial dysfunction. Eur J Echocardiogr. 2009;10(2):216-26. 133. Teske AJ, De Boeck BW, Melman PG, Sieswerda GT, Doevendans PA, Cramer MJ. Echocardiographic quantification of myocardial function using tissue deformation imaging, a guide to image acquisition and analysis using tissue Doppler and speckle tracking. Cardiovasc Ultrasound. 2007;5:27. 134. Urheim S, Edvardsen T, Torp H, Angelsen B, Smiseth OA. Myocardial strain by Doppler echocardiography. Validation of a new method to quantify regional myocardial function. Circulation. 2000;102(10):1158-64. 135. Tuzcu V, Bodtke JP, Best TH. Early detection of regional myocardial dysfunction in paced children with congenital complete atrioventricular block. Pacing and clinical electrophysiology : PACE. 2007;30(6):764-71.
179 | P a g e

136. Sutherland GR, Di Salvo G, Claus P, D'Hooge J, Bijnens B. Strain and strain rate imaging: a new clinical approach to quantifying regional myocardial function. J Am Soc Echocardiogr. 2004;17(7):788-802. 137. Voigt JU, Pedrizzetti G, Lysyansky P, Marwick TH, Houle H, Baumann R, et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. J Am Soc Echocardiogr. 2015;28(2):183-93. 138. Weidemann F, Eyskens B, Mertens L, Dommke C, Kowalski M, Simmons L, et al. Quantification of regional right and left ventricular function by ultrasonic strain rate and strain indexes after surgical repair of tetralogy of Fallot. Am J Cardiol. 2002;90(2):133-8. 139. Sachdev A, Villarraga HR, Frantz RP, McGoon MD, Hsiao JF, Maalouf JF, et al. Right ventricular strain for prediction of survival in patients with pulmonary arterial hypertension. Chest. 2011;139(6):1299-309. 140. Puwanant S, Park M, Popovic ZB, Tang WH, Farha S, George D, et al. Ventricular geometry, strain, and rotational mechanics in pulmonary hypertension. Circulation. 2010;121(2):259-66. 141. Pirat B, McCulloch ML, Zoghbi WA. Evaluation of global and regional right ventricular systolic function in patients with pulmonary hypertension using a novel speckle tracking method. Am J Cardiol. 2006;98(5):699-704. 142. Okumura K, Humpl T, Dragulescu A, Mertens L, Friedberg MK. Longitudinal assessment of right ventricular myocardial strain in relation to transplant-free survival in children with idiopathic pulmonary hypertension. J Am Soc Echocardiogr. 2014;27(12):1344-51. 143. Motoki H, Borowski AG, Shrestha K, Hu B, Kusunose K, Troughton RW, et al. Right ventricular global longitudinal strain provides prognostic value incremental to left ventricular ejection fraction in patients with heart failure. J Am Soc Echocardiogr. 2014;27(7):726-32. 144. Haeck ML, Scherptong RW, Marsan NA, Holman ER, Schalij MJ, Bax JJ, et al. Prognostic value of right ventricular longitudinal peak systolic strain in patients with pulmonary hypertension. Circulation Cardiovascular imaging. 2012;5(5):628-36. 145. Burns AT, La Gerche A, D'Hooge J, MacIsaac AI, Prior DL. Left ventricular strain and strain rate: characterization of the effect of load in human subjects. Eur J Echocardiogr. 2010;11(3):283-9. 146. Matsui H, Satomi G, Yasukochi S, Kaneko S, Haseyama K. Evaluation of right ventricular contraction by myocardial strain in children using a two-dimensional tissue tracking method. Pediatr Cardiol. 2008;29(2):377-81.
180 | P a g e

147. Cantinotti M, Kutty S, Giordano R, Assanta N, Murzi B, Crocetti M, et al. Review and status report of pediatric left ventricular systolic strain and strain rate nomograms. Heart failure reviews. 2015;20(5):601-12. 148. Burkett DA, Slorach C, Patel SS, Redington AN, Ivy DD, Mertens L, et al. Left Ventricular Myocardial Function in Children With Pulmonary Hypertension: Relation to Right Ventricular Performance and Hemodynamics. Circulation Cardiovascular imaging. 2015;8(8). 149. Willruth AM, Geipel AK, Fimmers R, Gembruch UG. Assessment of right ventricular global and regional longitudinal peak systolic strain, strain rate and velocity in healthy fetuses and impact of gestational age using a novel speckle/feature-tracking based algorithm. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology. 2011;37(2):143-9. 150. Sehgal A, Wong F, Menahem S. Speckle tracking derived strain in infants with severe perinatal asphyxia: a comparative case control study. Cardiovasc Ultrasound. 2013;11:34. 151. Sehgal A, Doctor T, Menahem S. Cardiac function and arterial indices in infants born small for gestational age: analysis by speckle tracking. Acta Paediatr. 2014;103(2):e49-54. 152. Schubert U, Muller M, Norman M, Abdul-Khaliq H. Transition from fetal to neonatal life: changes in cardiac function assessed by speckle-tracking echocardiography. Early Hum Dev. 2013;89(10):803-8. 153. Pena JL, da Silva MG, Alves JM, Jr., Salemi VM, Mady C, Baltabaeva A, et al. Sequential changes of longitudinal and radial myocardial deformation indices in the healthy neonate heart. J Am Soc Echocardiogr. 2010;23(3):294-300. 154. Nestaas E, Stoylen A, Brunvand L, Fugelseth D. Tissue Doppler derived longitudinal strain and strain rate during the first 3 days of life in healthy term neonates. Pediatr Res. 2009;65(3):357-62. 155. Nestaas E, Skranes JH, Stoylen A, Brunvand L, Fugelseth D. The myocardial function during and after whole-body therapeutic hypothermia for hypoxic-ischemic encephalopathy, a cohort study. Early Hum Dev. 2014;90(5):247-52. 156. El-Khuffash AF, Jain A, Weisz D, Mertens L, McNamara PJ. Assessment and treatment of post patent ductus arteriosus ligation syndrome. J Pediatr. 2014;165(1):46-52 e1. 157. Al-Biltagi M, Tolba OA, Rowisha MA, Mahfouz Ael S, Elewa MA. Speckle tracking and myocardial tissue imaging in infant of diabetic mother with gestational and pregestational diabetes. Pediatr Cardiol. 2015;36(2):445-53. 158. Anavekar NS, Gerson D, Skali H, Kwong RY, Yucel EK, Solomon SD. Two-dimensional assessment of right ventricular function: an echocardiographic-MRI correlative study. Echocardiography. 2007;24(5):452-6.
181 | P a g e

159. Forfia PR, Fisher MR, Mathai SC, Housten-Harris T, Hemnes AR, Borlaug BA, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med. 2006;174(9):1034-41. 160. Kjaergaard J, Petersen CL, Kjaer A, Schaadt BK, Oh JK, Hassager C. Evaluation of right ventricular volume and function by 2D and 3D echocardiography compared to MRI. Eur J Echocardiogr. 2006;7(6):430-8. 161. Ghio S, Klersy C, Magrini G, D'Armini AM, Scelsi L, Raineri C, et al. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. International journal of cardiology. 2010;140(3):272-8. 162. Brierre G, Blot-Souletie N, Degano B, Tetu L, Bongard V, Carrie D. New echocardiographic prognostic factors for mortality in pulmonary arterial hypertension. Eur J Echocardiogr. 2010;11(6):516-22. 163. Giusca S, Dambrauskaite V, Scheurwegs C, D'Hooge J, Claus P, Herbots L, et al. Deformation imaging describes right ventricular function better than longitudinal displacement of the tricuspid ring. Heart. 2010;96(4):281-8. 164. Rein AJ, Sanders SP, Colan SD, Parness IA, Epstein M. Left ventricular mechanics in the normal newborn. Circulation. 1987;76(5):1029-36. 165. Valsangiacomo Buechel ER, Mertens LL. Imaging the right heart: the use of integrated multimodality imaging. Eur Heart J. 2012;33(8):949-60. 166. El-Khuffash AF, McNamara PJ. Neonatologist-performed functional echocardiography in the neonatal intensive care unit. Seminars in fetal & neonatal medicine. 2011;16(1):50-60. 167. Rihal CS, Nishimura RA, Rumberger JA, Tajik AJ. Quantitative echocardiography: a comparison with ultrafast computed tomography in patients with chronic aortic regurgitation. The Journal of heart valve disease. 1994;3(4):417-24. 168. Ruschhaupt DG, Sodt PC, Hutcheon NA, Arcilla RA. Estimation of circumferential fiber shortening velocity by echocardiography. J Am Coll Cardiol. 1983;2(1):77-84. 169. Yared K, Noseworthy P, Weyman AE, McCabe E, Picard MH, Baggish AL. Pulmonary artery acceleration time provides an accurate estimate of systolic pulmonary arterial pressure during transthoracic echocardiography. J Am Soc Echocardiogr. 2011;24(6):687-92. 170. Urboniene D, Haber I, Fang YH, Thenappan T, Archer SL. Validation of high-resolution echocardiography and magnetic resonance imaging vs. high-fidelity catheterization in experimental pulmonary hypertension. Am J Physiol Lung Cell Mol Physiol. 2010;299(3):L401-12.
182 | P a g e

171. Kosturakis D, Goldberg SJ, Allen HD, Loeber C. Doppler echocardiographic prediction of pulmonary arterial hypertension in congenital heart disease. Am J Cardiol. 1984;53(8):1110-5. 172. Levy PT, Patel MD, Groh G, Choudhry S, Murphy J, Holland MR, et al. Pulmonary Artery Acceleration Time Provides a Reliable Estimate of Invasive Pulmonary Hemodynamics in Children. J Am Soc Echocardiogr. 2016;29(11):1056-65. 173. Denton CP, Cailes JB, Phillips GD, Wells AU, Black CM, Bois RM. Comparison of Doppler echocardiography and right heart catheterization to assess pulmonary hypertension in systemic sclerosis. British journal of rheumatology. 1997;36(2):239-43. 174. Currie PJ, Seward JB, Chan KL, Fyfe DA, Hagler DJ, Mair DD, et al. Continuous wave Doppler determination of right ventricular pressure: a simultaneous Doppler-catheterization study in 127 patients. J Am Coll Cardiol. 1985;6(4):750-6. 175. Slama M, Susic D, Varagic J, Ahn J, Frohlich ED. Echocardiographic measurement of cardiac output in rats. Am J Physiol Heart Circ Physiol. 2003;284(2):H691-7. 176. Ficial B, Finnemore AE, Cox DJ, Broadhouse KM, Price AN, Durighel G, et al. Validation study of the accuracy of echocardiographic measurements of systemic blood flow volume in newborn infants. J Am Soc Echocardiogr. 2013;26(12):1365-71. 177. Shiraishi H, Yanagisawa M. Pulsed Doppler echocardiographic evaluation of neonatal circulatory changes. Br Heart J. 1987;57(2):161-7. 178. Warnes CA. Adult congenital heart disease importance of the right ventricle. J Am Coll Cardiol. 2009;54(21):1903-10. 179. Slaughter JL, Pakrashi T, Jones DE, South AP, Shah TA. Echocardiographic detection of pulmonary hypertension in extremely low birth weight infants with bronchopulmonary dysplasia requiring prolonged positive pressure ventilation. J Perinatol. 2011;31(10):635-40. 180. Lindqvist P, Waldenstrom A, Wikstrom G, Kazzam E. The use of isovolumic contraction velocity to determine right ventricular state of contractility and filling pressures A pulsed Doppler tissue imaging study. Eur J Echocardiogr. 2005;6(4):264-70. 181. Mertens L, Seri I, Marek J, Arlettaz R, Barker P, McNamara P, et al. Targeted Neonatal Echocardiography in the Neonatal Intensive Care Unit: practice guidelines and recommendations for training. Writing Group of the American Society of Echocardiography (ASE) in collaboration with the European Association of Echocardiography (EAE) and the Association for European Pediatric Cardiologists (AEPC). J Am Soc Echocardiogr. 2011;24(10):1057-78. 182. Joshi S, Edwards JM, Wilson DG, Wong JK, Kotecha S, Fraser AG. Reproducibility of myocardial velocity and deformation imaging in term and preterm infants. Eur J Echocardiogr. 2010;11(1):44-50.
183 | P a g e

183. Daubeney PE, Blackstone EH, Weintraub RG, Slavik Z, Scanlon J, Webber SA. Relationship of the dimension of cardiac structures to body size: an echocardiographic study in normal infants and children. Cardiol Young. 1999;9(4):402-10. 184. Koopman LP, Slorach C, Hui W, Manlhiot C, McCrindle BW, Friedberg MK, et al. Comparison between different speckle tracking and color tissue Doppler techniques to measure global and regional myocardial deformation in children. J Am Soc Echocardiogr. 2010;23(9):919-28. 185. Aggarwal S, Natarajan G. Echocardiographic correlates of persistent pulmonary hypertension of the newborn. Early Hum Dev. 2015;91(4):285-9. 186. Fouzas S, Karatza AA, Davlouros PA, Chrysis D, Alexopoulos D, Mantagos S, et al. Neonatal cardiac dysfunction in intrauterine growth restriction. Pediatr Res. 2014;75(5):651-7. 187. Tomerak RH, El-Badawy AA, Hussein G, Kamel NR, Razak AR. Echocardiogram done early in neonatal sepsis: what does it add? Journal of investigative medicine : the official publication of the American Federation for Clinical Research. 2012;60(4):680-4. 188. Koopman LP, Slorach C, Manlhiot C, McCrindle BW, Friedberg MK, Mertens L, et al. Myocardial tissue Doppler velocity imaging in children: comparative study between two ultrasound systems. J Am Soc Echocardiogr. 2010;23(9):929-37. 189. Singh GK, Cupps B, Pasque M, Woodard PK, Holland MR, Ludomirsky A. Accuracy and reproducibility of strain by speckle tracking in pediatric subjects with normal heart and single ventricular physiology: a two-dimensional speckle-tracking echocardiography and magnetic resonance imaging correlative study. J Am Soc Echocardiogr. 2010;23(11):1143-52. 190. Forsey J, Friedberg MK, Mertens L. Speckle tracking echocardiography in pediatric and congenital heart disease. Echocardiography. 2013;30(4):447-59. 191. Jain A, Mohamed A, El-Khuffash A, Connelly KA, Dallaire F, Jankov RP, et al. A comprehensive echocardiographic protocol for assessing neonatal right ventricular dimensions and function in the transitional period: normative data and z scores. J Am Soc Echocardiogr. 2014;27(12):1293-304. 192. Breatnach CR, Levy PT, James AT, Franklin O, El-Khuffash A. Novel Echocardiography Methods in the Functional Assessment of the Newborn Heart. Neonatology. 2016;110(4):248-60. 193. El-Khuffash AF, Jain A, Dragulescu A, McNamara PJ, Mertens L. Acute changes in myocardial systolic function in preterm infants undergoing patent ductus arteriosus ligation: a tissue Doppler and myocardial deformation study. J Am Soc Echocardiogr. 2012;25(10):1058-67. 194. Ho CY, Solomon SD. A clinician's guide to tissue Doppler imaging. Circulation. 2006;113(10):e396-8.
184 | P a g e

195. Morel AA, Shreck E, Mally PV, Kim Y, Bailey SM, Wachtel EV. Clinical characteristics and factors associated with term and late preterm infants that do not respond to inhaled nitric oxide (iNO). J Perinat Med. 2016;44(6):663-8. 196. Rudolph AM, Auld PA, Golinko RJ, Paul MH. Pulmonary vascular adjustments in the neonatal period. Pediatrics. 1961;28:28-34. 197. Jain A, Mohamed A, El-Khuffash A, Connelly KA, Dallaire F, Jankov RP, et al. A Comprehensive Echocardiographic Protocol for Assessing Neonatal Right Ventricular Dimensions and Function in the Transitional Period: Normative Data and Z Scores. J Am Soc Echocardiogr. 2014. 198. Jain A, El-Khuffash AF, Kuipers BC, Mohamed A, Connelly KA, McNamara PJ, et al. Left Ventricular Function in Healthy Term Neonates During the Transitional Period. J Pediatr. 2016. 199. Kluckow M, Seri I, Evans N. Functional echocardiography: an emerging clinical tool for the neonatologist. J Pediatr. 2007;150(2):125-30. 200. Serwer GA, Cougle AG, Eckerd JM, Armstrong BE. Factors affecting use of the Doppler-determined time from flow onset to maximal pulmonary artery velocity for measurement of pulmonary artery pressure in children. Am J Cardiol. 1986;58(3):352-6. 201. Chan KL, Currie PJ, Seward JB, Hagler DJ, Mair DD, Tajik AJ. Comparison of three Doppler ultrasound methods in the prediction of pulmonary artery pressure. J Am Coll Cardiol. 1987;9(3):549-54. 202. Friedman WF. The intrinsic physiologic properties of the developing heart. Prog Cardiovasc Dis. 1972;15(1):87-111. 203. Emmanouilides GC, Moss AJ, Monset-Couchard M, Marcano BA, Rzeznic B. Cardiac output in newborn infants. Biology of the neonate. 1970;15(34):186-97. 204. Gessner I, Krovetz LJ, Benson RW, Prystowsky H, Stenger V, Eitzman DV. Hemodynamic adaptations in the newborn infant. Pediatrics. 1965;36(5):752-62. 205. Noori S, Wlodaver A, Gottipati V, McCoy M, Schultz D, Escobedo M. Transitional changes in cardiac and cerebral hemodynamics in term neonates at birth. J Pediatr. 2012;160(6):943-8. 206. Popat H, Kluckow M. Noninvasive assessment of the early transitional circulation in healthy term infants. Neonatology. 2012;101(3):166-71. 207. Coskun S, Yuksel H, Bilgi Y, Lacin S, Tansug N, Onag A. Non-invasive evaluation of the adaptations of cardiac function in the neonatal period: a comparison of healthy infants delivered by vaginal route and caesarean section. Acta medica Okayama. 2001;55(4):213-8.
185 | P a g e

208. Winberg P, Jansson M, Marions L, Lundell BP. Left ventricular output during postnatal circulatory adaptation in healthy infants born at full term. Arch Dis Child. 1989;64(10 Spec No):1374-8. 209. Randala M, Eronen M, Andersson S, Pohjavuori M, Pesonen E. Pulmonary artery pressure in term and preterm neonates. Acta Paediatr. 1996;85(11):1344-7. 210. Hiraishi S, Misawa H, Oguchi K, Kadoi N, Saito K, Fujino N, et al. Two-dimensional Doppler echocardiographic assessment of closure of the ductus arteriosus in normal newborn infants. J Pediatr. 1987;111(5):755-60. 211. Gentile R, Stevenson G, Dooley T, Franklin D, Kawabori I, Pearlman A. Pulsed Doppler echocardiographic determination of time of ductal closure in normal newborn infants. J Pediatr. 1981;98(3):443-8. 212. Reller MD, Ziegler ML, Rice MJ, Solin RC, McDonald RW. Duration of ductal shunting in healthy preterm infants: an echocardiographic color flow Doppler study. J Pediatr. 1988;112(3):441-6. 213. van Vonderen JJ, te Pas AB, Kolster-Bijdevaate C, van Lith JM, Blom NA, Hooper SB, et al. Non-invasive measurements of ductus arteriosus flow directly after birth. Arch Dis Child Fetal Neonatal Ed. 2014;99(5):F408-12. 214. Musewe NN, Poppe D, Smallhorn JF, Hellman J, Whyte H, Smith B, et al. Doppler echocardiographic measurement of pulmonary artery pressure from ductal Doppler velocities in the newborn. J Am Coll Cardiol. 1990;15(2):446-56. 215. Ardran G, Dawes GS, Prichard MM, Reynolds SR, Eyatt DG. The effect of ventilation of the foetal lungs upon the pulmonary circulation. The Journal of physiology. 1952;118(1):12-22. 216. Emmanouilides GC, Moss AJ, Duffie ER, Jr., Adams FH. Pulmonary arterial pressure changes in human newborn infants from birth to 3 days of age. J Pediatr. 1964;65:327-33. 217. Kiserud T. Fetal venous circulation--an update on hemodynamics. J Perinat Med. 2000;28(2):90-6. 218. Hoeper MM, Granton J. Intensive care unit management of patients with severe pulmonary hypertension and right heart failure. Am J Respir Crit Care Med. 2011;184(10):1114-24. 219. Sehgal A, Athikarisamy SE, Adamopoulos M. Global myocardial function is compromised in infants with pulmonary hypertension. Acta Paediatr. 2012;101(4):410-3. 220. Marijianowski MM, van der Loos CM, Mohrschladt MF, Becker AE. The neonatal heart has a relatively high content of total collagen and type I collagen, a condition that may explain the less compliant state. J Am Coll Cardiol. 1994;23(5):1204-8.
186 | P a g e

221. Santamore WP, Dell'Italia LJ. Ventricular interdependence: significant left ventricular contributions to right ventricular systolic function. Prog Cardiovasc Dis. 1998;40(4):289-308. 222. Lindqvist P, Calcutteea A, Henein M. Echocardiography in the assessment of right heart function. Eur J Echocardiogr. 2008;9(2):225-34. 223. Lakshminrusimha S, Keszler M. Persistent Pulmonary Hypertension of the Newborn. Neoreviews. 2015;16(12):e680-e92. 224. James AT, Corcoran JD, McNamara PJ, Franklin O, El-Khuffash AF. The effect of milrinone on right and left ventricular function when used as a rescue therapy for term infants with pulmonary hypertension. Cardiol Young. 2016;26(1):90-9. 225. Lazzeri C, Cianchi G, Bonizzoli M, Batacchi S, Terenzi P, Bernardo P, et al. Right ventricle dilation as a prognostic factor in refractory acute respiratory distress syndrome requiring veno-venous extracorporeal membrane oxygenation. Minerva anestesiologica. 2016;82(10):1043-9. 226. Ostrea EM, Villanueva-Uy ET, Natarajan G, Uy HG. Persistent pulmonary hypertension of the newborn: pathogenesis, etiology, and management. Paediatric drugs. 2006;8(3):179-88. 227. Mourani PM, Abman SH. Pulmonary vascular disease in bronchopulmonary dysplasia: pulmonary hypertension and beyond. Curr Opin Pediatr. 2013;25(3):329-37. 228. Mirza H, Ziegler J, Ford S, Padbury J, Tucker R, Laptook A. Pulmonary hypertension in preterm infants: prevalence and association with bronchopulmonary dysplasia. J Pediatr. 2014;165(5):909-14 e1. 229. Mourani PM, Sontag MK, Younoszai A, Miller JI, Kinsella JP, Baker CD, et al. Early pulmonary vascular disease in preterm infants at risk for bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2015;191(1):87-95. 230. Finan E, Sehgal A, Khuffash AE, McNamara PJ. Targeted neonatal echocardiography services: need for standardized training and quality assurance. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2014;33(10):1833-41. 231. Evans N. Echocardiography on neonatal intensive care units in Australia and New Zealand. Journal of paediatrics and child health. 2000;36(2):169-71. 232. Corredera A, Rodriguez MJ, Arevalo P, Llorente B, Moro M, Arruza L. [Functional echocardiography in neonatal intensive care: 1 year experience in a unit in Spain]. Anales de pediatria. 2014;81(3):167-73. 233. El-Khuffash A, Herbozo C, Jain A, Lapointe A, McNamara PJ. Targeted neonatal echocardiography (TnECHO) service in a Canadian neonatal intensive care unit: a 4-year experience. J Perinatol. 2013;33(9):687-90.
187 | P a g e

234. Ahn Y. Formula and scale for body surface area estimation in high-risk infants. Collegium antropologicum. 2010;34(4):1273-80. 235. Schulz-Menger J, Bluemke DA, Bremerich J, Flamm SD, Fogel MA, Friedrich MG, et al. Standardized image interpretation and post processing in cardiovascular magnetic resonance: Society for Cardiovascular Magnetic Resonance (SCMR) board of trustees task force on standardized post processing. Journal of cardiovascular magnetic resonance : official journal of the Society for Cardiovascular Magnetic Resonance. 2013;15:35. 236. Groves AM, Chiesa G, Durighel G, Goldring ST, Fitzpatrick JA, Uribe S, et al. Functional cardiac MRI in preterm and term newborns. Arch Dis Child Fetal Neonatal Ed. 2011;96(2):F86-91. 237. Mourani PM, Ivy DD, Gao D, Abman SH. Pulmonary vascular effects of inhaled nitric oxide and oxygen tension in bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2004;170(9):1006-13. 238. Banks BA, Seri I, Ischiropoulos H, Merrill J, Rychik J, Ballard RA. Changes in oxygenation with inhaled nitric oxide in severe bronchopulmonary dysplasia. Pediatrics. 1999;103(3):610-8. 239. Baquero H, Soliz A, Neira F, Venegas ME, Sola A. Oral sildenafil in infants with persistent pulmonary hypertension of the newborn: a pilot randomized blinded study. Pediatrics. 2006;117(4):1077-83.
188 | P a g e