Comprehensive assessment study of Blood Transfusion ... · Comprehensive assessment study of Blood...
73
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011 BLOOD SAFETY PROGRAM,DEPARTMENT OF MEDICAL SERVICES, MoH, BHUTAN
Transcript of Comprehensive assessment study of Blood Transfusion ... · Comprehensive assessment study of Blood...

Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
BLOOD SAFETY PROGRAM,DEPARTMENT OF MEDICAL SERVICES, MoH, BHUTAN

Comprehensive Assessment Study of Blood Transfusion Service, Bhutan- 2011
BLOOD SAFETY PROGRAM, DEPARTMENT OF MEDICAL SERVICES, MOH, BHUTAN


1
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
ACKNOWLEDGEMENTS
Blood Safety Program, Ministry of Health, RGoB would like to appreciate the hard work put in by the team members, health officials, laboratory personnel and all those individuals whose behind-the scenes contributions made this assessment study possible with a positive outcome.
Special acknowledgement goes to Dr Nani Nair, WHO Representative, Country office, Bhutan; Dr Neelam Dhingra, Co-ordinator and Dr Amin Noryati, Technical Officer, Blood Safety, WHO/ Geneva for their support and guidance.
The program would like to remember with gratitude Dr Maw-Naing Amaya, Ex-Officiating WHO Representative, Country office, Bhutan.
Special thanks goes to our financial partner OFID-OPEC Fund for International Development for providing the necessary funds for the printing and distribution of this publication.

2
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011

3
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
TABLE OF CONTENTS PAGE NO.
Executive Summary 4
Background 5
Comprehensive assessment study 7
Major findings 9
Summary of findings 29
Recommendations 31
Indicators and targets 33
Team members 34
Map of Bhutan with health facilities 35
Acronyms 36
Annexure list:
Details of blood bank equipment & supplies in western, eastern and central regions Annex 1A,B,C
Donor selection and screening Annex 2
Hb estimation method Annex 3
Details of blood units collected & collection mode Annex 4
Donor deferrals by reasons Annex 5
Number and type of blood units tested ‘Reactive’ to TTIs Annex 6
Fate of ‘Initial Reactive’ units region wise Annex 7
Storage & transport equipment used & temperature control practices Annex 8

4
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
The screening of all donated blood for transfusion transmissible infections before clinical use is a critical function of a blood transfusion service. Therefore establishment of a quality system in the screening process is an effective strategy for the provision of safe blood supply in the country.
WHO/OFID project (2010-2013)In 2010, Bhutan was chosen as one of the four beneficiary countries in the South Asian region to receive a grant from OPEC Fund for International Development (OFID) in partnership with Ministry of Health, Royal Government of Bhutan and WHO. The overall goal of this project is “Prevention of Transfusion-Transmissible HIV/AIDS and hepatitis infections in Bhutan”.
During the three year project implementation period, blood transfusion service (BTS) aims to achieve universal coverage and quality-assured testing of all donated blood through a series of strategies and planned activities that shall strengthen the blood screening process and establish quality systems in blood transfusion chain.
One of the four specific objectives defined to achieve the goal of the project included conduct a comprehensive assessment study of the blood banks which shall reflect the existing constraints, challenges, as well as identify gaps and provide guidance in developing strategies and activities for the project implementation plan.
Though in the past, the national blood bank, JDW, National Referral Hospital, Thimphu has conducted monitoring and supervisory visits of the blood banks in the country, it is for the first time that such a comprehensive assessment has been conducted. Twenty seven hospitals and their respective blood banks have been assessed based on a WHO Framework for Assessment, Monitoring and Evaluation of Blood Transfusion Service (FRAME) tool adapted to meet specific characteristics of the blood service in the country.
Findings of the study highlighted the following constraints and gaps:• Inadequate organization and co-ordination in the national blood supply system.• Lack of secured budget for routine blood transfusion service operations.• Inadequate number of voluntary blood donors due to inadequate general awareness among public on
the importance of voluntary blood donation. • Different levels of blood transfusion service, blood requirements and utilization.• Technical capacity of human resource at blood banks inadequate• Inadequate infrastructure facilities and shortages of testing kits and other critical supplies.• Lack of quality system essentials in blood transfusion service.• Varied blood prescribing practices among the clinicians and ineffective clinical interface.
Achievements and outcomes:• Mapping of the centres and comprehensive assessment by a trained team has been undertaken. • National database of these centres has been created which shall provide baseline information and help
set targets for indicators for future monitoring and evaluation. • The recommendations and suggestions in this report to provide direction in the finalization of action
plan for the project with emphasis on capacity building of personnel, improving laboratory practice and facilities and establishing quality assurance in blood screening and other critical process in blood banks.
• This report shall support and provide insight for the proposal of consolidation of blood transfusion service in the country.
• To benefit in the development of a regulatory framework.
EXECUTIVE SUMMARY

5
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
BACKGROUND
Bhutan is a 46,500 square kilometer country, tucked up in the rugged shoulders of the Eastern Himalayas. With India bordering it in the west, south and east and China (Tibet) in the north, the country is completely landlocked. The terrain starts from the rolling Indian plains to the snow capped, Himalayan mountains of over 24,000 feet above sea level. It is one of the countries with a constitutional democracy instituted just three years ago. Administratively it is divided into twenty districts called ‘Dzongkhags’ with a total population of six hundred and ninety five thousand, eight hundred and twenty two as per the Population and Housing Census of Bhutan (PHCB), 2005.
Health systemModern allopathic system of medicine was formally introduced in Bhutan during the first Five-Year Plan with the initiative of King Jigme Dorji Wangchuck, the third king of Bhutan. Bhutan had trained the first national MBBS doctor by 1954.
At the center, the Department of Health Services was carefully organized and strengthened over the years so as to be able to guide Bhutan’s health development along the right path. Required health programmes were started for prevention, promotion, and control of diseases that were of public health concern. As a signatory to the Alma Ata Declaration in 1978, Bhutan adopted the primary health care approach in its health care delivery system. Today it has one of the best organized primary health care systems in the Region. Even as a late starter in the modern health care system, Bhutan managed to cover over 90% of the population with basic health care service, despite the extremely difficult terrain with scattered and inaccessible population.
The concept of health in Bhutan must be seen in the context of the overall development strategy that defines development as the preservation of spiritual and emotional, as well as economic well being.
The National Health Policy drafted in 2010 relies on the principles of democratization and decentralization of the health service system and development of preventive, curative and promotive components of health care. Of note, it emphasizes on the development of an equitable and acceptable standard of health service system that will reach all segments of the population within the limits of resources, promoting and strengthening inter-sectoral activities and development of appropriate capacity building based on assessed needs.
Among its strategies for ensuring availability of drugs, supplies and equipment, the Ministry of Health has identified developing quality control capability and assuring efficacy and safety of products. The health delivery service is a public service, provided by the Ministry of Health under the Royal Government of Bhutan to the people free of cost that is provision of universal access to needed healthcare through single payer system.
For the purpose of maintaining quality of health care service and protecting the qualified human resource for health, private practice has never been introduced. The health delivery system comprises of 212 health centers of different levels, of which 31 are hospital type, 15 are basic health unit grade-I and 166 basic health unit grade –II, manned by 2155 health professionals including health workers.
Health indicators like the infant mortality, under-five mortality and maternal mortality rates are estimated at 40/1000, 60/1000 and 255/100,000 live births per year respectively (source: Annual Health Bulletin, MoH, 2010)
JDW, NR Hospital in the capital Thimphu serves not only as the apex national hospital but also as the western regional hospital with bed strength of 350 beds providing tertiary health care including intensive care, dialysis, nephrology, cardiology, urology, oncology, and neuro-surgery and neonatology. JDW, NRH

6
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
also provides primary health services to the residents of Thimphu district which has a population of a hundred thousand.
Presently, there are no super-specialized services like cardiac surgeries or transplants within the country for which patients are referred to specialized centers identified in India.
The Eastern Regional Referral Hospital in Mongar with bed strength of 150 provides primary service to Mongar district as well as secondary health care services to a total of eight districts covering a population of two hundred thousand in the region.The Central Regional Referral Hospital in Gelegphug with bed strength of 100 provides primary health care service to the district of Sarpang and secondary health facilities to a total of seven districts in the region.
Each district has one or two district hospitals with bed strength of 20 to 60.A system of referral of patients from district to regional and regional to national level is established for better management of cases needing specialized care.
National Blood Transfusion Service The national blood transfusion service also termed as ‘blood bank service’ is one of the listed programs under the Health Care and Diagnostic Division of Department of Medical Services, Ministry of Health. The transfusion medicine specialist at National Blood Bank, Thimphu and the Diagnostic Service Program Officer are the two focal persons for the planning and co- ordination of all the transfusion related activities at the program level.There is no separate allocation of an annual budget for the NBTS, but the main financial sources are RGoB, WHO and World Bank till date.The national blood policy has been endorsed by MoH in 2007 and the ten-year national blood plan was drafted in 2010 for finalization and adoption. The national standards for BTS have been developed and endorsement by MoH recently in 2012-2013.Regulation of the blood and blood products by the national regulatory body does not exist presently.The blood transfusion service is delivered in the form of hospital based blood banks, which are units of the laboratory service, under direct supervision and responsibility of the hospital administration.Though referred to as blood banks in the country, these twenty seven units perform the functions of a blood centre:- • blood donor recruitment• blood donor selection• blood collection • blood screening for Transfusion Transmitted Infections • provide donor care and counseling • hospital transfusion laboratory• blood storage and blood issue
The head of the national blood bank provides technical expertise and advice on: • Procurement of equipment, reagents and consumables• Human resource development (pre-service and in-service training)• Development of quality systems, national guidelines and standards for BTS.
There are no private or non-government blood banks in the country.Among the many cases of admission to the hospitals are transfusion requiring conditions and diseases such as all types of chronic anemia (especially due to chronic, non-communicable diseases), gynecological and obstetric conditions, malaria, surgeries, and an increasing number of accidents and injuries leading to acute blood loss.

7
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
COMPREHENSIVE ASSESSMENT STUDY
1. OBJECTIVESThe main purpose of the study has been to conduct a situation analysis of the existing blood banks in terms of the managerial and operational capacity to provide adequate, safe and quality blood to meet the demands for clinical blood transfusion.Specifically, the assessment was aimed at profiling:
1. Type of infrastructure and staff dedicated to blood service in all facilities2. The organization and management of blood service at each level3. Build adequate data of baseline indicators for setting future targets
4. METHODOLOGY2.1 Sampling frame and samples27 health facilities were identified for assessment based on one criterion: health facilities involved in delivery of patient care requiring blood transfusions.
2.2 Data Gathering2.2.1 Assessment toolA standard tool for assessment of blood transfusion service developed by the WHO was used as a basis for conducting the evaluation. A technical working group was formed and after a series of consultations among the members, the tool was modified, reviewed, and finally adapted with the inclusion of some questions that aimed at collecting sufficient information and at easing data compilation and analysis from quantitative and qualitative records.
The final assessment tool was prepared in the form of a ‘questionnaire’ form’ which had to be filled by the individual enumerator based on the information provided by the identified health personnel in the respective health facility through an ‘interview process’ and ‘on-site observations’ made during the visit. The term ‘questionnaire’ shall be used henceforth in the subsequent paragraphs of this report.
Provision for additional “comments” at the end of each section was kept to record qualitative remarks to supplement the answers. The assessment team and supervisors were responsible to ensure proper data entry, review available records and attache all supporting documents with the questionnaire.
The questionnaire comprised of a total of seven sections namely:-1. Assessing the health facility2. Assessing the blood bank3. Quality system4. Blood donors and blood collection5. Screening for Transfusion Transmitted Infections 6. Blood group serology and compatibility testing7. Blood storage, transportation & distribution
2.2.2. Team compositionField data collection was done by thirteen health personnel selected by the Department of Medical Services from eleven hospitals. The assessment team consisted of ten laboratory technicians, two laboratory technologists and one program personnel. In addition, the national blood bank in-charge and one personnel from the Epidemiology and Research unit, MoH, also participated in the data compilation, analysis and report preparation.

8
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
2.2.3. Field data collectionThe 13 personnel were divided into 3 teams. Each team composed of 3 to 4 enumerators and 1 supervisor for data collection in one of the three regions namely western, central and eastern region. Each enumerator in the team was assigned to assess two selected blood banks en route for a period of two days per blood bank.
The assessment of the western region commenced on 23rd December 2010.The assessment of the central region commenced on 24th December 2010.And the eastern region assessment began from 27th December 2010.The study was completed in approximately three weeks.The three supervisors conducted verification visits and provided logistical and technical support to the team members and performed direct observation of the facility, conducted structured interviews with the hospital administrators, collected and compiled the completed questionnaire, and other blood transfusion related forms and worksheets.
2.2.4. Pre-assessment briefing workshop of team membersOn 20th and 21st December 2010, the team members underwent a short training on the administration of the adapted WHO assessment tool conducted by a team of resource persons at field training centre, Punakha.The training was intended to brief the participants on:
a. The OFID project, its objectives and goalsb. The objectives, methodology and expected outcome of the comprehensive study c. Agreed operational definitions of all terms and issues addressed in the questionnaire formd. Basic knowledge on blood transfusion safety and current transfusion practices in the country, orient
them on how to administer the assessment tool and ensuring accuracy, relevance and completeness of data using the reference materials and glossary prepared specifically for this study.
2.3 Data entry, compilation and analysisThe data reflects a total of 27 health facilities with their respective 27 blood bank units as all 27 centres were visited and assessed. All 27 filled questionnaire were received from the respective enumerators by the program personnel.The forms were evaluated for completeness and clarity of information gathered by the team. 90 to 95% of the questions had been answered in all the 27 questionnaire. For all quantitative data, the reporting period from 1st January to 31 December 2009 was decided upon. Other qualitative data reported reflects the existing situation in each blood bank.For easy data entry, the qualitative questions were provided with boxes to enumerate the appropriate response.Data was compiled and analyzed using EPI data and SPSS software. The analysed data has been presented in the form of spread sheets, tables and figures. For qualitative data descriptive analysis is applied.
2.4 Limitations2.4.1. Though the WHO assessment tool was evaluated and modified to adapt to the current practices in the blood banks, its simplicity, practicality and clarity of the framed questions was still doubtful being the first time such an assessment was conducted in Bhutan. The tool was not field tested.
2.4.2. Due to the limited categories of technical resource in this field, the team had to be framed with laboratory technicians who had limited experience and confidence in conducting such a study.
2.4.3. Due to the above reason, the study could not include assessment of clinical interface and clinical transfusion aspect, especially on the rational use of blood by doctors, blood utilization and clinical administration of blood.

9
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
2.4.4. Few questionnaire had some of the questions left unanswered with no reasons mentioned and some were answered incorrectly. The enumerators were also not available during the time of data compilation and analysis to clarify the queries as they had to return to their duty station on completion of their assignments.
2.4.5. The practice of documentation and recording of blood transfusion related activities in Bhutan is still not up to the standard except at few blood centres. There was some degree of variability in response rates to few specific questions making analysis difficult.

10
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
MAJOR FINDINGS
PART 1: ASSESSING THE HEALTH FACILITY
1.1. Twenty seven health facilities including 26 hospitals and 1 basic health unit grade –I were selected for the study and all 27 (100%) were visited and assessment carried out.The hospitals included:
1. National referral hospital 2. Two regional referral hospitals3. Twenty three district level hospitals 4. One basic health unit –I
Table 1: Names of health facilities visited region wise with their respective bed strength and the population coverage
Western region Beds/ population Eastern region Beds/
population Central region Beds/population
JDW,NR Hospital 350/100,000 Eastern RR Hospital, Mongar 150/70,000
Central RR Hospital,
Gelegphug100/ 16,000
Gidakom Hospital 60/5,200 Samdrup Jongkhar Hospital 20/7,700 Trongsa
Hospital 20/3,500
Punakha Hospital 40/19,000 Riserboo Hospital 20/4,000 Dagapela Hospital 20/11,100
Paro Hospital 40/30,000 Tashigang Hospital 50/60,000 Yebilaptsha Hospital 40/2,800
Phuntsholing Hospital 50/20,000 Pema gatshel
Hospital 20/6,000 Sarpang Hospital 10/12,000
Bajothang 10/7,000 Deothang Hospital 50/7,700 Damphu Hospital 20/8,000
Tshimalakha Hospital 20/4,000 TrashiYangtse Hospital 20/18,000 Bumthang
Hospital 40/41,000
Sibsoo Hospital 20/10,000 Lhuntse Hospital 20/14,000Gedu Hospital 20/6,000
Samtse Hospital 60/50,000Gomtu Hospital 20/14,000
Bali BHU-I 10/6,300Total 12 700/2,71,50 Total 8 370/2,0140 Total 7 250/94,400
Total : 27 hospitals
1.2. Each facility was assessed for the level of health care it is providing by an estimation of the categories of doctors and specialists posted, especially those who are involved in prescribing and using blood and blood components for transfusions as part of patient management. Findings show that all the 27 health facilities (100%) had general duty doctors posted whereas specialists like a general surgeons and obstetrician and gynecologist were posted at 7/27 (26 %) centers, anesthesiologists at 6/27 centers (22%), and medical specialist, orthopedician, pediatrician and ENT surgeon were posted at 3 regional hospitals (11%). These are not constant figures as many of the specialists especially in the districts are expatriates from neighboring countries mostly Myanmar.Super specialists were stationed at the national referral hospital only.

11
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Of the 23 district level hospitals, 5 are identified as EMOC centers where emergency obstetric surgeries like caesarian sections, laprotomies are conducted for which support from the blood transfusion service is very essential and 1 DH has been identified as a trauma center also requiring well established blood service.
Figure 1: Percentage of health facilities with different categories of doctors and specialists posted (Total number of health facilities assessed=27)
GDMO, 100%
General Surgeons, 26% Medical Specialist, 11%
Gyn & Obst, 26%
Ortho Surgeon, 11%
Pediatricians, 11%
Anesthesiologist, 22%
ENT Surgeons,
11%
GDMO
General Surgeons
Medical Specialist
Gyn & Obst
Ortho Surgeon
Pediatricians
Anesthesiologist
ENT Surgeons
GDMO, 100%
General Surgeons, 26% Medical Specialist, 11%
Gyn & Obst, 26%
Ortho Surgeon, 11%
Pediatricians, 11%
Anesthesiologist, 22%
ENT Surgeons,
11%
GDMO
General Surgeons
Medical Specialist
Gyn & Obst
Ortho Surgeon
Pediatricians
Anesthesiologist
ENT Surgeons
1.3. The assessment looked into the budgetary support from the hospital annual funds, blood safety program or other sources to conduct awareness and educative activities among general population on importance of blood donation and hold mobile blood drives in the community. The study showed that some support from hospital budget is being provided at NRH, and ERRH whereas CRRH and all the 23DHs do not receive such funds to carry out blood donation related activities.Some funds were made available at regular intervals since 2005 to NRH, both the RRHs and to 5 large DHs namely Paro, Phuntsholing, Samtse, Samdup Jongkhar and Trashigang from the program which received budget allocations from World Bank and WHO to promote blood safety through voluntary non-remunerated blood donations in the country. None of the facilities reported having a financial system in place for the calculation of such recurrent operating costs. The cost for a unit of blood has not been estimated in the country.
1.4. The hospital administration was requested to respond to two commonly observed problems namely:a. Shortage of blood bank reagents and suppliesb. Shortage of blood stocks
Table 2 summarizes the responses of the administrators of which ‘Delay in receiving the supplies at the user end from the procurement division’ was cited by majority as ‘THE’ main cause of shortages of supplies.

12
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Lack of blood storage facilities and voluntary blood donors at the blood centres was felt by many administrators as the major contributing factors to the problem of shortages of blood stocks.
Table 2: Responses of the hospital administratorsProblems faced Reasons cited Solutions/suggestions provided
Shortage of blood bank supplies
Delay in providing supply from DVED-lengthy processLogistical problemsLab techs not trained in inventory and procurement/quantification Supplies inadequateLack of regular monitoring of stocks
Timely supply of reagents from DVEDTo keep buffer stocks of supplies at the regional levelsSOPs to be developed for procurement processTraining of the lab techs in inventory control and their active involvement in the procurement processProcurement of vehicles for timely supplies
Shortage of blood stocks
No blood storage facility No budget for blood donation activitiesLack/small voluntary and regular blood donors
Infrastructure developmentIncrease general awarenessEncourage voluntary donationsAllocation of budget for BTS activitiesAppoint donor recruitersStrengthen the bio-engineering unit for rapid action when equipment breakdown Train the clinicians on appropriate use of blood

13
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 2: ASSESSING THE BLOOD CENTRE All the 27 blood centres were assessed to understand and gather information on:
• functions of each centre • premises and infrastructure, continuous water and electrical supply• human resource provided in terms of number, adequacy, capacity, job responsibilities and training
opportunities• facilities like existing equipment, supplies and reagents
2.1. Types of blood transfusion service All 27 assessed blood banks function as ‘blood centres’, as per the definition of the term ‘blood centre’ and they are all (100%) hospital based.
Table 3: Type and number of blood transfusion centres assessed region wiseRegion NBC & RBC RBC DBC BHU-1 BC Blood Banks Total BCs
Western 1 - 10 1 0 12Central 0 1 6 0 0 7Eastern 0 1 7 0 0 8
Total 1 2 23 1 0 27
2.2. In general, there is a great degree of variability in the basic infrastructure among blood centres. The number of rooms varies from 10 at NBC to nil at a DBC. 4 of 27 (15%) have separate rooms for BTS activities.5 of 27 (19%) share transfusion laboratory related activities with general laboratory. The rest 18 of 27 (66%) share all functions with the general laboratory 12 of 27 (44%) centres responded as having no problem with regular power supply and rest 56% have power cuts with no provision of a generator or alternative power supply.
Table 4: Basic infrastructure at 27 blood centresBlood centres Separate rooms for BTS activity Water supply UPS for critical
equipmentAC facility
WesternJDW,N Hospital Yes yes No YesGidakom No yes No NoPunakha Yes yes No YesParo No yes Yes NoPhuntsholing no, No Yes YesBajothang No No Yes NoTshimalakha Yes yes No NoSibsoo No yes No NoGedu No No Yes NoSamtse No No Yes YesGomtu No yes No YesBali No yes No NoEasternMongar Yes, yes Yes YesSamdrup Jonkha No No No Yes

14
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Reserboo No yes Yes NoTrashigang Yes, except TTI tests &IH tests No Yes NoPema Gatshel Yes, except for TTI yes Yes NoDeothang No yes Yes NoTrashi Yangtse No No Yes NoLhuntse No yes No NoCentralGelephu No No Yes YesTrongsa Yes, except for IIH &TTI tests yes No NoDagana No No No NoYebilaptsa Yes, except for donor interview
&IIHyes No No
Sarpang No No No NoDamphu No No No NoBumthang No yes No No
2.3. Human resource at the blood centresThe NBC, headed by a transfusion medicine specialist functions with staff strength of 10 fulltime dedicated general laboratory technicians and one diploma trained laboratory technician.The 2 RBCs have only 1 fulltime dedicated staff and so emergency BTS activities are carried out by the other laboratory staff on duty.
All the district blood centres use the general pool of medical laboratory technicians for performing the BTS activities including blood donor screening, blood collection, screening for TTIs and immuno-haematological testing.All the laboratory technicians have undergone an in-service training in blood banking and immuno-hematology and 10 blood centres (37%) have one laboratory technician each trained ex-country for a short term in blood banking.Organizational structure indicating authority, responsibility and job descriptions are not developed in a documented format in any of the blood centre. Organogram demonstrating the chain of command is lacking in all the 27 centres.
2.4. Equipment and supplies Almost all equipment, reagents and supplies are centrally purchased and distributed by the Drugs, Vaccine and Equipment Division of Department of Medical Services on an annual indenting basis. Neither the equipment nor any supplies or reagents are available in the local market, though study has shown that there is a practice of making patients purchase TTI test kits in times of no stocks by some hospitals in proximity with India. Quality checks on these kits are not performed by the centres before use.
System of standardised pre-purchase specification and evaluation of all equipment, post purchase validation, and hands-on training of staff on installation is present but responses from almost all centres show that periodic preventive maintenance, after sales service and care, calibration and prompt repair of equipment by the bio-medical engineering unit is inconsistent. Repair or change of spares takes a long time and the technical capacity of the engineers posted at regional units is inadequate. Many non-functioning equipment at times are present without repair for prolonged periods affecting the services of the blood centres.
Adequate awareness and knowledge on the use of developed national guidelines for indenting standard reagents and equipment and on internal quality control of reagents and equipment is lacking among the
15
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
100%
88%
40%
55%
25%
27 centres have equipment for blood donor Hb% estimation, centrifuge, microscope & refrigirator
24 centres have equipment for weighing blood bags
11 centres have di-electric tube sealer
15 centres have special blood bank refrigirator
25 centres have domestic refrigirator
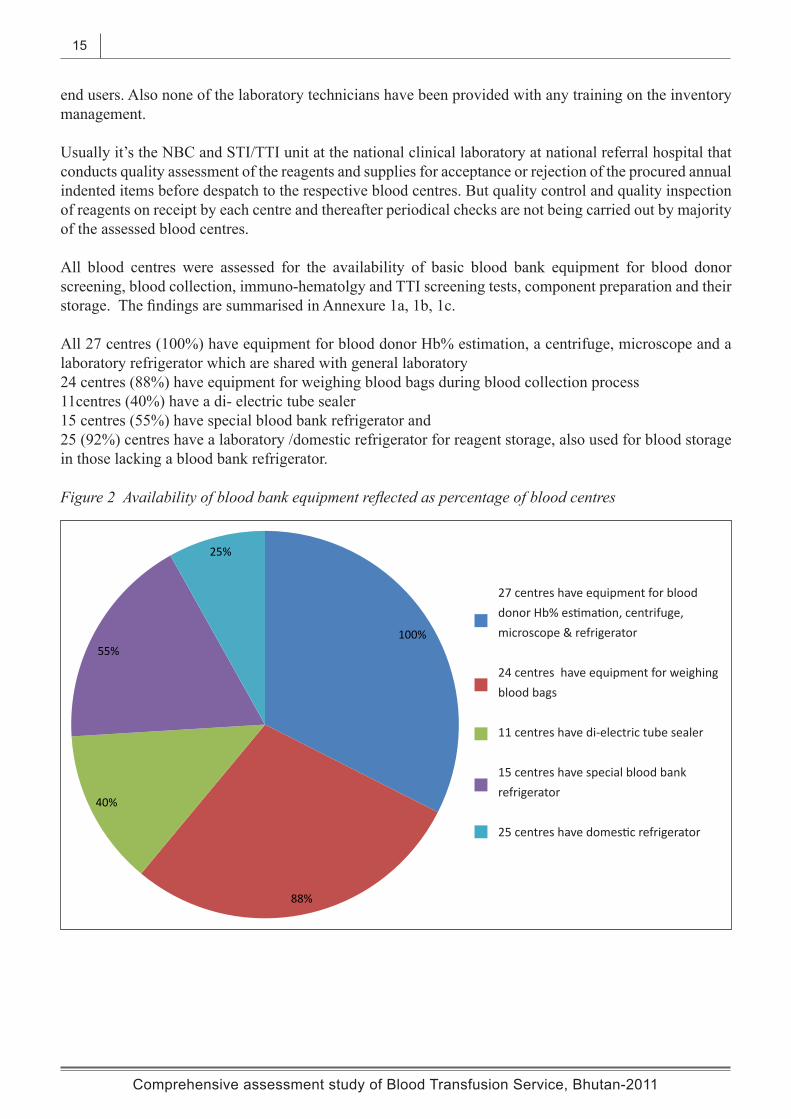
Figure 2 Availability of blood bank equipment reflected as percentage of blood centres
27 centres have equipment for blood donor Hb% estimation, centrifuge, microscope & refrigerator
24 centres have equipment for weighing blood bags
11 centres have di-electric tube sealer
15 centres have special blood bank refrigerator
25 centres have domestic refrigerator
end users. Also none of the laboratory technicians have been provided with any training on the inventory management.
Usually it’s the NBC and STI/TTI unit at the national clinical laboratory at national referral hospital that conducts quality assessment of the reagents and supplies for acceptance or rejection of the procured annual indented items before despatch to the respective blood centres. But quality control and quality inspection of reagents on receipt by each centre and thereafter periodical checks are not being carried out by majority of the assessed blood centres.
All blood centres were assessed for the availability of basic blood bank equipment for blood donor screening, blood collection, immuno-hematolgy and TTI screening tests, component preparation and their storage. The findings are summarised in Annexure 1a, 1b, 1c.
All 27 centres (100%) have equipment for blood donor Hb% estimation, a centrifuge, microscope and a laboratory refrigerator which are shared with general laboratory 24 centres (88%) have equipment for weighing blood bags during blood collection process11centres (40%) have a di- electric tube sealer 15 centres (55%) have special blood bank refrigerator and 25 (92%) centres have a laboratory /domestic refrigerator for reagent storage, also used for blood storage in those lacking a blood bank refrigerator.

16
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
The NBC has facilities for blood component separation into packed red cell, fresh frozen plasma and random donor platelet concentrates and their appropriate storage. Equipment for ELISA testing of blood samples for TTIs is available at STI/TTI unit of national clinical laboratory which performs blood screening.The ERBC has a refrigerated centrifuge but no equipment for storage of blood components like plasma freezer and platelet agitator with incubator.26 (96%) blood centres perform TTI tests on blood donor samples using rapid test kits.Though study shows that regular stock checks are carried out in 20 blood centres, supplies ran out of stock in the last 12 months for a period of 15days to 3 months: - TTI test kits out of stock in18 of 27 centres - Blood bags out of stock in 10 of 27 centres - Blood grouping reagents not available in 2 of 27 centres
Figure 3 No. of blood centres out of supplies in 2008-2009
TTI test kits, 18 centres
Blood bags, 10 centres
ABO reagents, 2 centres

17
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 3: QUALITY SYSTEMThe study attempted to assess the presence of quality system essentials in the blood centres namely:
1. Organizational structure
2. Standards, standard guidelines and SOPs
3. Documentation and record maintenance
4. Assessment: Internal and external, inspection and regulation
5. Training of the staff (this has been covered in Part 2, section 2.3)
3.1. Organizational structure As mentioned earlier the blood centres are a part of the laboratory service based in a hospital setting.Majority of the blood centres have technical man power pool of either two or three general laboratory technicians, one of which is appointed as the in-charge. Hence the management system in a structured manner indicating authority, responsibility and reporting relationship is weak.The department of clinical laboratory at the national hospital of which NBC is a unit is in the process of developing an organogram and writing the job descriptions and responsibilities of all cadres of technical personnel in the laboratory and blood centres like laboratory manager, laboratory supply in charge, teaching in-charge, and quality assurance manager. A committee called the ‘Laboratory Technical Management Committee’ is constituted with specific objectives and terms of reference.
3.2. Standards, standard guidelines and SOPs The availability and use of standard operating procedures for the different activities in a blood centre was assessed. No SOPs are written by individual centres. Response showed that in all the 27 blood centres, generic SOPs which were prepared at national level and distributed are being used. These SOPs include sections for blood donor screening and blood donation, immuno-hematology, blood component preparation, blood storage, transport and issue. National guidelines, strategies algorithms and SOPs on TTI screening are not developed. The STI/TTI unit is in the process of preparing SOPs for testing of blood for infections like HIV, HBV, HCV and syphilis but not in particular for blood screening for TTIs. CME programs are conducted on ‘How to write a SOP’ involving at-least one staff from each laboratory in 2010.A draft document on ‘Standards for blood transfusion service and blood centres’ has been developed by blood safety program for further review, revision and endorsement by Ministry of Health.A manual on ‘Clinical laboratory Standards’ prepared by Quality Assurance and Standardization Division, which provides guidelines and information on tests, equipment and reagents requirements at different levels of laboratories and blood centres in the country is available but the study showed that its use by the blood centre/laboratory during the process of annual procurement and indent is minimal.
3.3. Documentation and record maintenanceAll the 27 blood centres are maintaining manual records in the form of registers, worksheets and forms though not in a systematic manner and the in-charges are responsible for data management. . The maintenance of equipment log books and records of QC tests is lacking in 90% of the centres.The system of submitting six monthly data reports by each centre to NBC is present, but in 2009 only 19 /27centres submitted their reports.3.4. Assessment

18
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Regular internal quality control checks of reagents, equipment and techniques is lacking. Proficiency testing of the technical staff is not conducted and hence level of knowledge and professional skills is not known to provide training opportunities to the needy ones.All 27 blood centres are participating in NEQAS for HIV, HBV and syphilis organised by the Public Health laboratory, Thimphu.8 (30%) of blood centres have participated in NEQAS in BGS in 2009 and 15(56%) are participating in 2011.A system of licensing the blood centres does not exist as all the centres are a unit of government hospitals under MoH and currently no private blood banks operate in the country. The Drug Regulatory Authority of Bhutan has been mandated by RGoB and the Medicine Act of Kingdom of Bhutan 2003 for regulation of all medicinal drugs including blood and blood products in accordance with national blood policy, but due to lack of technical capacity and resources, legislative framework and necessary blood regulatory mechanisms have not been developed.DRA is currently in the initiation process and the ground work has just been started.In 2009 and 2010, a team from NBC had conducted supervisory visits to all the 8 eastern and 7central blood centres using a standard evaluation checklist. Each blood centre and the hospital administration were provided with feedback and recommendations to carry out necessary corrective measures.
PART 4: BLOOD DONOR & BLOOD COLLECTIONDonor education, recruitment, selection and retention practices in the 27 blood centres were assessed, including the availability of trained staff and donor educational materials.
4.1 Donor education and recruitment activities Though 74% have responded as ‘yes’, donor education, recruitment and retention activities carried out are on a very limited scale in these centres.. For standardization purpose all the necessary IEC materials are prepared by the concerned programs in consultation with a division called the Information Communication Bureau (ICB) in the MoH. The blood safety program has developed and distributed two types of donor educational materials (in English and national language) to all the blood centres for such activities. But only nineteen centres (70%) reported using these information pamphlets.There is no designated donor recruitment officer in any of the centre.
4.2. Blood donor selection and screening (Refer to annexure 2) Since there in no doctor available at the blood centres except NBC, the pre-service blood banking curriculum of MLT course includes training of all the laboratory technicians in donor screening, selection, and donor management though only 8 centres (30%) have answered as ‘yes’.All 27 centres (100%) reported availability and use of national selection criteria with 26 (96%) centres following written donor questionnaire form, staff at 25 (92%) interviewing the donors and all 27 (100%) carrying out Hb% estimation and physical checks on blood donors at their centres. 88% centres reported to perform pre-donation counselling.
4.3 Hb% estimation of donors and test methods An indicator of good donor selection practice is the percentage of potential donors for whom the hemoglobin level is determined. All 27 centres (100%) reported to check Hb % during the donor screening process. The use of different methods for Hb% estimation of donors is reflected in Annexure 3.18 centres use only one method whereas 7 centres have the option of using either of two methods and 2 centres have the option of using one of the three methods, dependent on the reagents and consumables availability at that centre.

19
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 4: BLOOD DONOR & BLOOD COLLECTION
Donor education, recruitment, selection and retention practices in the 27 blood centres were assessed, including the availability of trained staff and donor educational materials.
4.1 Donor education and recruitment activities Though 74% have responded as ‘yes’, donor education, recruitment and retention activities carried out are on a very limited scale in these centres.. For standardization purpose all the necessary IEC materials are prepared by the concerned programs in consultation with a division called the Information Communication Bureau (ICB) in the MoH. The blood safety program has developed and distributed two types of donor educational materials (in English and national language) to all the blood centres for such activities. But only nineteen centres (70%) reported using these information pamphlets.There is no designated donor recruitment officer in any of the centre.
4.2. Blood donor selection and screening (Refer to annexure 2) Since there in no doctor available at the blood centres except NBC, the pre-service blood banking curriculum of MLT course includes training of all the laboratory technicians in donor screening, selection, and donor management though only 8 centres (30%) have answered as ‘yes’.All 27 centres (100%) reported availability and use of national selection criteria with 26 (96%) centres following written donor questionnaire form, staff at 25 (92%) interviewing the donors and all 27 (100%) carrying out Hb% estimation and physical checks on blood donors at their centres. 88% centres reported to perform pre-donation counselling.
4.3 Hb% estimation of donors and test methods An indicator of good donor selection practice is the percentage of potential donors for whom the hemoglobin level is determined. All 27 centres (100%) reported to check Hb % during the donor screening process. The use of different methods for Hb% estimation of donors is reflected in Annexure 3.18 centres use only one method whereas 7 centres have the option of using either of two methods and 2 centres have the option of using one of the three methods, dependent on the reagents and consumables availability at that centre.
Figure 4 Equipment used for blood donor Hb% estimation
40%
22%
22%
22%
33%
Photometer
Hemouce method
Hb% color scale
Automatic analyzer
Sahli's method
40%
22%
22%
22%
33%
Photometer
Hemouce method
Hb% color scale
Automatic analyzer
Sahli's method

20
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
4.4 Blood donation system The system of blood unit collection by type of blood donors as per the definition of ‘voluntary’ and’ family/replacement’ was assessed in all 27 centres. During the period from 1st Jan to 13st Dec 2009, a total of 8028 units were collected from 27 blood centres, of which 3686 units (46%) were collected from voluntary blood donors and 4342 units (54%) from replacement donors.None of the 27 centres have 100 % voluntary donation system. 12 centres (44%) reported having some percentage of voluntary blood donation system; the rest 15 centres had only replacement or depository system by family or friends of patients.The percentage of voluntary blood donations in the 12 centres ranged from:
• 5 centres: 25% voluntary donations• 2 centres: up-to 50 % voluntary donations• 5 centres up-to 75 % voluntary donations
Figure 5 Voluntary blood units collected by BCs in western region, 2009 (total western collection=5537, voluntary collection=3036)
0 500 1000 1500 2000 2500 3000
JDW, NRH
Gedakom
Punakha
Paro
P/ling
Bajothang
Tsimalakha
Sibsoo
Gedu
Samtse
Gomtu
Bali
Western region

21
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Figure 6 Voluntary blood units collected by BCs in eastern region, 2009 (total eastern collection=1445, voluntary collection=535 )
Figure 7 Voluntary blood units collected by BCs in central region, 2009་(total central collection=1046 ,voluntary collection=115)
0 50 100 150 200 250 300 350 400 450
Mongar
S/Jonkhar
Reseerbo
Trashigang
Pema Gatshel
Deothang
Trashiyangtse
Lhuntse
Eastern region
0 20 40 60 80 100 120 140
Gelephu
Trongsa
Dagana
Yebilaptsa
Sarpang
Damphu
Bumthang
Central region

22
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Figure 8 Regional variability shown in voluntary blood units collected, 2009
Western region 55%
Eastern region 37%
Central region
8%
Regional variability in voluntary blood donation
The modality of blood collection whether at the blood centre or at mobile blood sites was also studied and reports show that only 5 (19%) centres conducted mobile blood drives of which 4 centres collected 35% of the total voluntary units and 1 centre collected 70 % of the total voluntary units through the mobile drives.
WBDD was observed in 7 centres since 2004.The standard volume collected at all centres using whole blood is 350ml 350 ml, NBC, 2 RBCs and 1 DBC collects 350 and 450 ml volume. For details kindly refer to Annexure 4. 4.5. Donor deferrals776 potential donors were deferred from 21 centres mainly on the basis of five reasons:-
• Hb% < 12 gm%• Medical or surgical conditions• Malaria or travel to malaria regions• High risk behaviour• Miscellaneous
Six centres did not maintain records of donor deferral and 2 centres had no donors deferred in 2009.For details kindly refer to Annexure 5.

23
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Figure 9 Percentage of donors deferred by reasons
Low Hb%, 40%
Medical conditions, 27%
Malaria, 3%
High risk behaviour, 17%
Other, 13%
4.6. Donor retentionThis practice is carried out in 7 centres (25%). Sero-negative donors are counselled and requested to become regular donors for whom donor cards are developed and used. Sometimes these regular donors are called using telephonic services especially in times of shortages.
4.7. Donor notification and counsellingAll donors are provided with an ‘information note’ which contains donation details, post-donation advice and results of TTIs. All are encouraged to collect the TTI results.
There are no confirmatory tests available for Hepatitis B or C. Donors are called, notified and counselled by trained staff at the blood centre or advised to see a doctor in the same health facility. For syphilis, TPHA is done as a confirmatory test and treatment provided by the doctor.
For HIV sero-reactive donors, the staffs direct the donors either to counsellors or trained health personnel in that facility, who then notify, and counsel for a repeat test for which serum samples are sent to reference laboratory in Thimphu for confirmation.
The practice of monitoring the TTI results of especially regular donors is present at some centres as they maintain the records of regular donors in special documents.

24
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 5: SCREENING OF BLOOD FOR TRANSFUSION TRANSMITTED INFECTIONS
5.1. Infections tested, infection markers and assays usedAll blood centres reported 100 % blood screening for four infections- HIV, Hepatitis B & C and syphilis in the reporting period of 2009. Very negligible number of units is screened for malaria even in the endemic areas due to absence of clear policy guidelines from the ministry.13 centres (48%) perform post –donation screening on blood samples whereas 11 centres (40%) perform pre-donation screening on blood donors and three did not respond to this question. There is no practice of repeating the test on post –donation samples at these centres.The infection markers used are HIV antibody, HBsAg, HCV antibody for HIV, HBV and HCV testing respectively.Other than NBC, all 26 centres (96%) used rapid tests for screening of all 4 markers.NBC used ELISA and rapid assays for blood screening. The report mentions the use of ELISA to screen 72% of the total donations and the rest 28% by rapid tests.
5.2 Percentage of sero-reactive units by type of donations in 2009 (Refer to annexure 6 for details)
Figure 10: Percentage of voluntary blood donations screened ‘sero-reactive’
HIV, 0.05%
HBV, 1%
HCV, 0.05%
Syphillis, 0.50%
Figure 11: Percentage of replacement blood donations screened ‘sero-reactive’
HIV, 0.07%
HBV, 1.06%
HCV, 0.12%
Syphillis, 1.38%

25
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Figure 12: Percentage of total ‘sero-reactive’ blood units
HIV, 0.06%
HBV, 1.03%
HCV, 0.09%
Syphillis, 1%
Regional variability was also observed. Central region reported the highest sero-positivity for three markers namely HIV, HBV and syphilis in comparison to western which reported the least for HIV but highest for HCV. No HCV sero-positive units were detected in eastern and central regions
Figure 13: Regional variability of ‘sero-reactive’ blood units
0.00%
0.50%
1.00%
1.50%
2.00%
HIV HBV HCV Syphils
0.01%
1.03%
0.13%
0.70%
0.14%
1%
0
1.38%
0.19%
1.24%
0%
2%
Western
Eastern
Central
*For details kindly refer to Annexure 6

26
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
5.3. Fate of reactive units (Refer to annexure 7a, 7b, 7c)It has been observed from the reports below that there are no standard guidelines available for blood screening. Algorithms have not been developed for blood screening though the STI/TTI unit at JDW, NRH that performs tests for patients and blood donor samples for HIV, HBV and HCV follow the WHO algorithms for surveillance and /diagnosis of HIV and not for blood screening.
Fate of ‘Initial Reactive’ blood samples:• 23 centres (85%) perform repeat tests on ‘IR’ samples to all four infection markers• 1 centre (3%) performs repeat test on samples ‘IR’ to anti-HIV, HBsAg and RPR • 1 centre (3%) performs repeat test on samples ‘IR’ to anti-HIV and RPR • 2 centres (7%) discard blood units which are ‘IR’ to anti-HIV, HBsAg, and anti–HCV and send
fresh samples of the donor to reference laboratory in Thimphu. RPR reactive samples are repeated at the centre.
Fate of ‘Repeat Reactive’ blood samples• 11 centres (41%) send only anti-HIV ‘RR’ samples to reference laboratory. • 10 centres (37%) send anti-HIV, HBsAg and anti-HCV ‘RR’ samples to reference laboratory • 4 (15%) centres do not send any samples to reference laboratory
Time taken to receive the reports from reference laboratory to the centre is minimum 3 days to a maximum of 30 days at far distanced centres. 4 centres (13%) store frozen samples for look back facility for a period of 30 to 365days due to lack of deep freezers.
27
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 6: BLOOD GROUP SEROLOGY & COMPATIBILITY TESTING
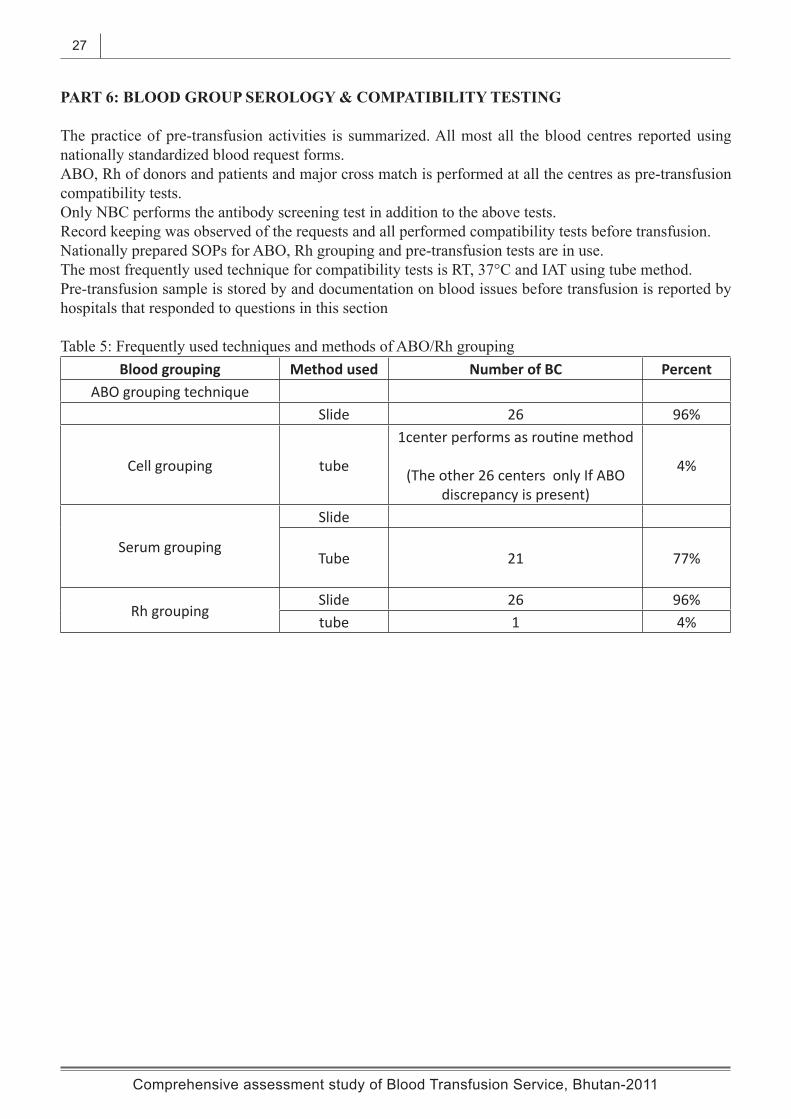
The practice of pre-transfusion activities is summarized. All most all the blood centres reported using nationally standardized blood request forms.ABO, Rh of donors and patients and major cross match is performed at all the centres as pre-transfusion compatibility tests.Only NBC performs the antibody screening test in addition to the above tests.Record keeping was observed of the requests and all performed compatibility tests before transfusion. Nationally prepared SOPs for ABO, Rh grouping and pre-transfusion tests are in use.The most frequently used technique for compatibility tests is RT, 37°C and IAT using tube method.Pre-transfusion sample is stored by and documentation on blood issues before transfusion is reported by hospitals that responded to questions in this section
Table 5: Frequently used techniques and methods of ABO/Rh groupingBlood grouping Method used Number of BC Percent
ABO grouping techniqueSlide 26 96%
Cell grouping tube
1center performs as routine method
(The other 26 centers only If ABO discrepancy is present)
4%
Serum grouping
Slide
Tube 21 77%
Rh groupingSlide 26 96%tube 1 4%

28
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
PART 7: BLOOD STORAGE, TRANSPORTATION, INVENTORY & DISTRIBUTION
7.1 Blood storage equipment (Refer to annexure 8a, 8b, 8c)During the assessment, the blood storage equipment used and the presence or absence of temperature control and monitoring practices were analyzed at all 27 centres region.Blood component facility is available at NBC and ERBC, of which only NBC has equipment for storage of Platelets and frozen plasma.Deep freezers for long-term storage of donor serum samples are not available except at NBC.17 of the 27 centres (59%) have blood bank refrigerators (BBR) for storage of blood and red cells of which 2 centres reported the status of the BBR as non-functioning.The rest 11centres (41%) store blood in domestic/laboratory refrigerators. These centres having no blood bank refrigerator usually follow the practice of storing blood units until blood screening and testing process is completed following which the blood is issued for transfusion.
7.2 Temperature control & monitoring and distribution to clinical areas At the time of visit the enumerators made an observation whether the temperature range of storage equipment used was appropriate to the type of items stored in them and also whether temperature charts were maintained. Temperature monitoring was reported to be done regularly and an updated temperature monitoring charts were seen in 24 /27. Some of the centres reported as storing blood in domestic refrigerators though they were equipped with BBR and these were in functioning status, the reason for this has not been mentioned by the enumerators.Separate storage areas or sections were designated for untested units, ready for distribution and test kits in most of the centres. The most frequently used transport equipment for blood to the clinical areas is vaccine carrier. Assessment showed that there is very little transportation of blood units from one to another centre in 2009.The same vaccine carriers or commercial thermocool or Styrofoam boxes were used for transportation from one centre to other blood centre.

29
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
SUMMARY OF FINDINGS
All the challenges and constraints highlighted during the National Consultative and Planning Meeting of the stake holders in July 2011 were identified during the assessment study and have been summarized below:
1 Blood centers1.1. Each health facility needs blood transfusion set up due to the present day hospital based blood supply system in the country, thus necessitating investment in infrastructure, human resource and critical equipment and supplies, leading to high cost, financial constraints and difficult monitoring.
1.2. Existing variability in the present infrastructure of blood banks in terms of appropriate rooms for BTS related activities and essential backup facilities for critical blood bank equipment.
1.3. Evident human resource constraints. Availability of only one transfusion specialist in the country and almost all the blood banks manned by general laboratory technicians with a certificate training in general medical technology. Other categories of blood bank personnel like donor recruitment staff, phlebotomists or blood bank nurse not available in the country.
1.4. Shortage of basic required equipment in almost 40% of the blood banks and critical supplies like TTI screening reagents and blood bags. The reasons being mainly lengthy, time consuming annual procurement process, inefficiencies in the procurement system, inaccurate quantification during indenting process and lack of up-to-date stock management by the end-user.
1.5. Inadequate support services like biomedical engineering units at all levels. Lack of standards, guidelines and training of the laboratory technicians in inventory and equipment control practices. Difficulties faced in transportation of reagents/equipments/supplies at regular intervals due to long distances and difficult terrain.
2. Health facility2.1. Health facilities not allocating funds in the hospital annual budget to conduct local activities to promote voluntary blood donations, resulting into blood shortages and a system dependent on family /replacement donors, thus compromising blood safety.
2.2. Varying degree of knowledge among doctors on clinical use of blood resulting in varying blood prescribing practices.
2.3. Lack of a hospital transfusion committee in each facility to monitor the blood needs, utilization patterns, adverse transfusion events and enforce adherence to national guidelines on clinical use of blood.
3. Blood donor management 3.1. Inadequate general awareness in the community on the importance of blood donation due to ineffective blood donor education, mobilization and recruitment activities in the country. Voluntary blood donation system indicated at 46% in the country in 2009.
3.2. Blood donor screening and selection activities conducted by laboratory technicians with limited clinical knowledge.
3.3. Blood drives and mobile camps limited to few blood banks.
3.4. Weak and inconsistent practice of donor retention and more reliance on one time donors thereby increasing the donor requirement.

30
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
3.5. No standard guidelines for blood donor notification and counseling.
4. Blood screening process4.1. National policy, policy guidelines, standards algorithms and SOPs for blood screening not available.
4.2. A practice of pre-donation testing of potential blood donors being carried out in district blood banks with the objective of saving on blood bags and discards of tainted blood units.
4.3. Use of rapid assays for TTI testing in majority of centers due to low through-put and inadequate competency of blood bank personnel to perform ELISA testing and lack of system of blood stock inventory maintenance.
4.4 Good laboratory practice of following Standard procedures for ABO, Rh and compatibility testing not followed by many blood banks technicians.
5. Blood inventory, blood storage and monitoring practice5.1. Lack of appropriate blood storage facilities in twelve of the twenty seven centers. Practice of using domestic or laboratory refrigerator for blood storage.Practice of keeping blood stocks and maintaining blood inventory not carried out.
6. Quality systems 6.1. Under developed quality system essentials in the blood transfusion service
6.2. Unclear mandate of the national reference laboratory in relation to:• Evaluation and selection and validation of assay systems and equipment• Confirmatory testing on screen reactive donations for blood donor management• Provision of quality control samples• Organization of external quality assessment schemes
6.3. Weak documentation and data management
6.4. Regulatory mechanism to monitor quality of blood and blood products in the country not established.

31
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
RECOMMENDATIONS
The following interventions have been identified and recommended for implementation in a phased manner1. Short term strategies: some of the priority areas may be incorporated in the OFID strategic plan and activities be conducted in the three year period implementation period to achieve the objectives of the project.
1.1 Human resource development: Ex-country training of more number of laboratory technicians (both short term and long term trainings) on various aspects of blood transfusion.
1.2. Establish quality system1.2.1. Initiate process for organizational structuring, define job descriptions of the laboratory/blood bank personnel and establish the mandate of national clinical laboratory and public health laboratory in the context of blood screening.1.2.2. Develop national standards, strategies, and algorithms for blood screening.1.2.3. Develop SOPs for all blood bank activities1.2.4. Strengthen documentation for better data collection, analysis, use, storage and retrieval at each blood bank
1.3. Improve laboratory practices1.3.1. Use of quality TTI test kits with specificity and sensitivity of >99.5% 1.3.2. Reference laboratory to evaluate and validate TTI test kits, reagents and procured equipment 1.3.3. Ensure proper cold chain of test kits, reagents and blood units during transportation and storage 1.3.4 Training of laboratory technicians and technologists on use of SOPs, algorithms for blood screening1.3.5. Technicians to perform regular, internal quality checks on reagents, equipment and techniques.
1.4. Procurement system1.4.1. Strengthen laboratory procurement system by developing standard protocols for all processes involved during the annual procurement1.4.2. Identify focal persons at DVED and at each blood bank/laboratory for annual procurement process 1.4.3. Train these focal persons on procurement procedures 1.4.4. Improve communication between central procuring agency, individual hospital administration and procurement focal points1.4.5. Explore cost-effective strategies such as WHO bulk procurement schemes for blood screening reagents 1.5. Promotion of voluntary blood donation system 1.5.1. Allocate some percentage from individual hospital budget for conducting blood donation activities like motivation, recruitment of blood donors and holding blood drives.1.5.2. Increase the number of staff at national and two regional blood banks to conduct and support the above activities.1.5.3. Initiate a system of periodic transportation of screened blood units from larger blood bank to nearby smaller blood banks. (This could be taken up as a pilot study at national blood bank).1.5.4. Improve blood donor counseling
• Link the blood donor counselor with HIV/STI counselor• strengthen pre and post donation counseling• Train laboratory personnel in pre and post donation counseling guidelines and SOPs

32
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
1.6. Strengthen laboratory facilities1.6.1. Procurement of basic blood collection, screening, testing and storage equipment.1.6.2. Introduce blood component preparation facilities at central regional blood center1.6.3. Procure transport vans and blood cold chain equipment
1.7. Monitoring and Evaluation1.7.1. Introduce periodic assessment of the blood banks by conducting visits and supportive supervision by teams from national and regional blood banks1.7.2. Participation in EQAS in BGS and TTIs at national and regional level 1.7.3. Develop indicators and targets, to monitor the progress, evaluate the outcomes and plan future activities.
2. Long term strategies: these strategies can be incorporated in the strategic national blood plan and implemented over a period of say fifteen years.
2.1. Human resource development2.1.1. Train atleast two national doctors as transfusion medicine specialists2.1.2. Recruit and train other categories of staff like blood donor recruiters and phlebotomists2.1.3. Introduce a short term (six month) in-country certificate course in ‘blood banking’ for in-service MLTs who can then take charge of the district blood banks.
2. Re-structure the national blood transfusion service 2.1. At the program level, appoint one full time national director of NBTS and a program officer. Allocate a separate budget for the program to conduct all transfusion related activities.2.2. At the service level, create one national and five regional hospital based blood centers in the country headed by specialists and convert all the other blood banks into blood storage and hospital transfusion laboratories.2.3. Develop national standards for future infrastructure development.
3. Regulation of blood service and blood products3.1. DRA to be mandated to develop regulations to monitor the quality of blood and blood products and conduct regular inspections of the centers.3.2. Bhutan Health and Medical Council to oversee the quality of service in terms of
• Human Resource Development • proficiency level of staff, appropriate training needs and continued medical education programs• occupational safety at blood centers in terms of adequate space, hygiene, infectious and bio waste
management and infection control practices.
4. Procurement of mobile blood vans for a comprehensive blood donation process at convenience of the blood donors.

33
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
INDICATORS AND TARGETS
Indicator No1: Percentage of blood units collected from voluntary blood donors• Baseline data of 2010: 45 % units collected are from voluntary donors• Target by2013: To increase voluntary blood donations to 75% at the country level
Indicator No2: Number of blood centers in the country performing screening of donated blood units in quality-assured manner. (Donated blood units are considered to be tested in a quality-assured manner if they are tested in centre/laboratory which uses standard operating procedures (SOPs) and participates in an External Quality Assessment scheme (EQA)).
• Baseline data of 2012: One blood center has in-house SOPs developed for TTI testing and is participating in EQAS
• Target by 2013: All blood centers in the country to perform screening of TTIs in a quality-assured manner
Indicator No 3: Prevalence of TTIs in blood donors
• Baseline data of 2009 from 27 blood centers
Prevalence in % Voluntary Replacement TotalHIV 0.05% 0.07% 0.06%HBV 1% 1.06% 1.03%HCV 0.05% 0.12% 0.09%
Syphilis 0.5% 1.38% 1%
• To monitor the prevalence of TTIs in blood donors in 2013 vis a vis baseline of 2009 Indicator No 4: Number of laboratory staff trained on the use of national guidelines and SOPs on screening of blood for TTIs
• Baseline national data: No one trained• Target by 2013: 90 of total 160 number of the laboratory technicians in the country to be trained
@ approximately 30 per year

34
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
TEAM MEMBERS
1. Dr Mahrukh Getshen, National Blood bank In-charge, JDW, NRH, (team leader)
2. Dr B Dhungyel, Pathologist, JDW, NRH (resource person for the training)
3. Mr Namgyal Dorji, Sr. Program Officer, Diagnostic Service Program, Health Care and Diagnostic Division, Department of Medical Services (supervisor for eastern region)
4. Mr Dorji, Head, Pathology Department, JDW, NRH (supervisor for western region)
5. Mr Sonam Wangda, Technologist, JDW, NRH, (supervisor for central region)
6. Ms Damchoe Dema, Medical laboratory technician (enumerator for central region)
7. Mr Rinchen, Medical laboratory technician (enumerator for central region)
8. Ms Phuntsho Wangmo, Medical laboratory technician (enumerator for central region)
9. Mr Gopal Sanyashi, Medical laboratory technician (enumerator for western region)
10. Mr Neten Dukpa, Medical laboratory technician (enumerator for western region)
11. Mr Kezang Wangdi, Medical laboratory technician (enumerator for western region)
12. Ms Thinley Wangmo Medical laboratory technician (enumerator for western region)
13. Mr Tshewang Dorji, Medical laboratory technician (enumerator for eastern region)
14. Ms Pema Choden, Medical laboratory technician (enumerator for eastern region)
15. Ms Tashi Yangzom, Medical Laboratory technician (enumerator for eastern region)
16. Mr Chimmi Dorji, Senior laboratory Officer, Public Health Laboratory, Thimphu
17. Mr Tshering Dorji, Medical Laboratory Technologist, Public Health Laboratory, Thimphu
18. Mr Karma Loday, staff, Epidemiology and Research Unit, Ministry of Health
19. Mr Dopo, Statistical Officer, Ministry of Health
20. Mr Jayendra Sharma, Planning Officer, Policy and Planning Division, Ministry of Health

35
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Map of Bhutan with the existing health facilities, 2009
Source: Ministry of Health, RGoB, Thimphu

36
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
ACRONYMS
AC Air Condition
AIDS Acquired Immunodeficiency Syndrome
BC Blood Centre
BBR Blood Bank Refrigerator
BGS Blood Group Serology
BTS Blood Transfusion Service
CME Continued Medical Education
CRBC Central Regional Blood Centre
CRRH Central Regional Referral Hospital
DBC District Blood Centre
DH District Hospital
DRA Drug Regulatory Authority
ENT Ear, Nose and Throat
ELISA Enzyme Linked Immunoassay
ERBC Eastern Regional Blood Centre
ERRH Eastern Regional Referral Hospital
EMOC Emergency Obstetric Care
FRAME Framework for Assessment, Monitoring and Evaluation of Blood Transfusion Service
GNH Gross National Happiness
GDMO General Duty Medical Officers
HBV Hepatitis B Virus
HBsAg Hepatitis B Surface Antigen
HCV Hepatitis C Virus
HIV Human Immunodeficiency Virus
IC Inventory Control
ICB Information Communication Bureau
IQC Internal Quality Control

37
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
IR Initial Reactive
JDW, NRH Jigme Dorji Wangchuck, National Referral Hospital
MoH Ministry of Health
MLT Medical laboratory technician
NA Not Available
NBTS National Blood Transfusion Service
NBC National Blood Centre
NEQAS National External Quality Assessment Scheme
NF Non-functioning
NR Not Required
NRH National Referral Hospital
OFID OPEC Fund for International Development
PA with PI Platelet Agitator with Platelet Incubator
QC Quality Check
RBC Regional Blood Centre
RGoB Royal Government of Bhutan
RRH Regional Referral Hospital
RR Repeat Reactive
SOP Standard Operative Procedure
STI Sexually Transmitted Infection
TPHA Treponema Pallidum Haemagglutination
TTI Transfusion Transmitted Infection
UPS Uninterrupted Power Supply
WHO World Health Organization
WB World Bank

38
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
IssueEquipment
JDW, NRH
Gida-kom
Puna-kha
Paro P/ling Bajo-thang
Tshima-lakha
Sib-soo
Gedu Sam-tse
Gom-tu
Bali Total
Donor bed 1 1 1 1 1 0 1 1 1 1 1 0 10Donor weighing machine
1 0 1 1 1 1 1 1 0 1 1 0 9
Hb estimation 1 1 1 1 1 1 1 1 1 1 1 1 12BP instrument 1 1 1 1 1 1 1 1 1 1 1 1 12Clinical thermometer 0 1 0 0 0 0 0 0 0 0 0 0 1Blood bag weighing scale
1 0 0 1 1 1 0 1 1 1 1 0 8
Automatic blood collection monitor
1 0 1 1 1 0 1 0 0 1 0 0 6
Electric tube sealer 1 0 1 0 1 0 1 0 0 0 0 0 4Tube stripper 1 0 1 1 1 1 1 1 0 1 1 1 10bench top centrifuge 1 1 1 1 1 1 1 1 1 1 1 1 12Automatic cell washer 1 0 0 0 0 0 0 0 0 0 0 0 1Incubator or water Bath
1 1 1 1 1 1 1 1 1 1 0 0 10
Microscope 1 1 1 1 1 1 1 1 1 1 1 1 12
Refrigerated centrifuge
1 0 0 0 0 0 0 0 0 0 0 0 1
Electronic balance 1 0 0 0 0 0 0 0 0 0 0 0 1Plasma expresser 1 0 0 1 0 0 0 0 0 0 0 0 2Blood bank refrigerator
1 0 1 1 1 0 1 0 1 1 0 0 7
Plasma freezer –300C 1 0 0 0 0 0 0 0 0 0 0 0 1Platelet incubator & shaker
1 0 0 0 0 0 0 0 0 0 0 0 1
Plasma thawer 1 0 0 0 0 0 0 0 0 0 0 0 1ELISA plate washer 0 0 0 0 0 0 0 0 0 0 0 0 0ELISA plate reader 0 0 0 0 0 0 0 0 0 0 0 0 0Lab refrigerator 1 1 1 1 1 1 1 1 1 1 1 1 12Lab thermometer 1 1 0 1 1 0 1 1 0 1 1 0 8Autoclave 1 1 1 0 1 0 0 1 0 1 0 0 6Staff trained on use of equipment
1 1 0 0 1 0 0 1 1 0 0 1 6
Calibration 0 0 0 0 0 0 0 0 0 0 0 0 0Regular maintenance 1 0 0 0 0 0 0 1 1 1 0 0 4Blood bags out of stock in last 12 months
0 1 0 0 0 1 0 1 0 1 0 0 4
TTI test kits out of stock 1 1 0 1 1 1 1 1 1 1 1 0 10Blood Grouping Reagents out of stock
0 0 0 0 0 0 0 1 0 0 1 0 2
System of following standard list
1 1 0 1 0 0 0 0 0 0 0 0 3
System of stock check 1 1 0 1 1 1 1 0 0 0 0 1 7Lab staff trained in IC 0 0 0 0 0 0 0 0 0 0 0 0 0Pts made to buy supplies
0 0 0 0 1 0 0 0 0 0 0 0 1
Annexure 1a: Availability of blood bank equipment & supplies in western region (1=Yes; 0=No)

39
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 1b: Availability of blood bank equipment & supplies in eastern region (1=yes; 0=no)
Issue Equipment Mongar S/Jong Reserboo T/Gang P/Gatshel Deothang T/
Yangtse Lhuntse Total
Donor bed 1 1 1 1 1 0 1 1 7Donor weighing machine 1 1 1 0 0 1 1 1 6Hb estimation 1 1 1 1 1 1 1 1 8BP instrument 1 1 1 1 1 1 1 1 8Clinical thermometer 0 0 0 0 0 0 0 - 0Blood bag weighing scale 1 1 1 1 1 1 1 - 7Automatic blood collection monitor 1 1 0 1 0 0 0 1 4
Electric tube sealer 1 1 0 1 0 0 0 - 3Tube stripper 1 1 1 1 1 1 1 1 8bench top centrifuge 1 1 1 1 1 1 1 - 7Automatic cell washer 1 0 0 0 0 0 0 - 1Incubator or water Bath - 1 1 1 1 1 1 1 8Microscope 1 1 1 1 1 1 1 1 8Refrigerated centrifuge 1 0 0 0 0 0 0 0 1Electronic balance 0 0 0 0 0 0 0 0 0Plasma expresser 1 0 0 0 0 0 0 0 1Blood bank refrigerator 1 1 0 1 0 0 0 1 4Plasma freezer – 300C 0 0 0 0 0 0 0 0 0Platelet incubator & shaker 0 0 0 0 0 0 0 0 0Plasma thawer 0 0 0 0 0 0 0 0 0ELISA plate washer 0 0 0 0 0 0 0 0 0ELISA plate reader 0 0 0 0 0 0 0 0 0Lab refrigerator 0 1 1 1 1 1 1 1 7Lab thermometer 0 1 1 0 1 0 1 0 4Autoclave 0 1 1 0 0 0 0 0 2Staff trained on use of equipment 0 1 0 0 1 0 0 0 2
Calibration 0 0 0 0 0 0 0 0 0Regular maintenance 0 1 0 0 1 0 0 1 2Blood bags out of stock in last 12 months 1 0 1 1 0 1 0 0 4
TTI test kits out of stock in last 12 months 1 0 0 1 1 1 0 0 4
Blood Grouping Reagents out of stock 0 0 0 0 0 0 0 0 0
System of following standard list 0 0 0 0 0 0 0 0 0
System of stock checks 1 0 1 1 1 1 1 1 7Lab staff trained in IC 0 0 0 0 0 0 0 0 0Pts made to buy supplies 0 0 0 0 0 0 0 0 0

40
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 1c: Availability of blood bank equipment & supplies in central region (1=yes; 0=no)
Issue Equipment Gelephu Trongsa Dagana Y/laptsa Sarpang Damphu Bumthang Total
Donor bed 1 1 1 1 1 1 1 7Donor weighing machine 1 0 0 1 1 1 1 5Hb estimation 1 1 1 1 1 1 1 7BP instrument 1 1 0 0 1 1 1 5Clinical thermometer 0 0 0 0 0 1 0 1Blood bag weighing scale 1 0 1 0 1 0 1 4Automatic blood collection monitor 1 1 0 1 0 0 1 4Electric tube sealer 1 1 0 1 0 0 1 4Tube stripper 1 1 1 1 1 1 1 7Bench top centrifuge 1 1 1 1 1 1 1 7Automatic cell washer 1 0 0 0 0 0 0 1Incubator or water Bath 1 1 1 1 1 1 1 7Microscope 1 1 1 1 1 1 1 7Refrigerated centrifuge 0 0 0 0 0 0 0 0Electronic balance 0 0 0 0 0 0 0 0Plasma expresser 0 0 0 0 0 0 0 0Blood bank refrigerator 1 1 0 1 0 1 1 4Plasma freezer –300C 0 0 0 0 0 0 0 0Plasma thawer 0 0 0 0 0 0 0 0ELISA plate washer 0 0 0 0 0 0 0 0ELISA plate reader 0 0 0 0 0 0 0 0Lab refrigerator 1 1 1 1 1 0 1 6Lab thermometer 0 0 0 0 1 1 1 3Autoclave 1 0 0 1 1 0 0 3Staff trained on use of equip 0 1 0 1 1 1 1 5Calibration 0 0 0 0 1 0 0 1Regular meintanance 0 0 0 1 1 0 1 3Blood bags out of stock in last 12 months 0 0 0 0 0 1 1 2
TTI test kits out of stock in last 12 months 0 0 1 0 1 1 1 4
Blood Grouping Reagents out of stock in last 12 months 0 0 0 0 0 0 0 0
System of following standard list 1 0 0 1 1 0 1 4System of stock checks 0 1 1 1 1 1 1 6Lab staff trained in IC 0 0 0 0 0 0 0 0Pts made to buy supplies 0 0 0 0 0 0 0 0

41
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 2: Donor selection and screening
Issues Responses No. of blood centers Percent1. Donor related activities carried out
1a: Donor information/education activity carried
Yes 20 74%No 7 26%
1b: Donor educational materials available? No material 8 30%
Locally producedNationally standardized 19 70%
1c: Pre-donation counseling done? Yes 24 88%No 3 12%
2. Availability of specific staff in donor unit
2a. Availability of trained donor recruitment officer
Yes 0 0%No 27 100%
2b. Availability of doctor /trained personnel to manage donor issue
Yes 8 30%No 19 70%
3. Donor selection
3a: Availability and use of national donor selection criteria
No criteria Available & in use 27 100%
4. Tools used for donor selection
4a: Use of a standard donor questionnaire form
Yes 26 96%No 1 4%
4b: Practice of confidential pre-donation counseling and interview
Yes 25 92%No 2 8%
4c: Hb estimation of all potential donors Yes 27 100%
5. WBDD observed in last five years
Yes 11 40%No 16 60%

42
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 3: Hb% determination method (√ =method used)
Blood Centers Hemoglobin Determination Method Western Region Photometer Hemocue Hb colour
scale Automated
AnalyserSahli’s Total methods
JDW, NR Hospital √ √ 2
Gidakom √ 1
Punakha √ 1
Paro √ 1
Phuntsholing √ 1
Bajothang √ √ 2
Tshimalakha √ 1
Sibsoo √ 1
Gedu √ 1
Samtse √ √ 2
Gomtu √ √ 2
Bali √ 1
Eastern RegionMongar √ √ 2
Samdrup Jonkha √ 1
Reseerbo √ 1
Trashigang √ 1
Pema Gatshel √ √ 2
Deothang √ 1
Trashiyangtse √ 1
Lhuntse √ 1
Central RegionGelephu √ √ √ 3
Trongsa √ √ √ 3
Dagana √ 1
Yebilaptsa √ 1
Sarpang √ √ 2
Damphu √ 1
Bumthang √ 1
Total 11 6 6 6 9
√ means method used

43
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 4: Details of blood units collected and mode of collection
Blood centersNumber of collections (in units) % Mode of
collection Vol collected
in ml
Regular donors
Voluntary Family replacement Total %
voluntary Center Mobile yes no
JDW, NRH 2700 888 3588 75 66 34 350/450 YGedakom 43 24 67 64 0 100 350 NPunakha 85 156 241 35 100 350 YParo 33 276 309 10 100 0 350 NPhuntsholing 49 493 542 9 100 0 350 NBajothang 0 89 89 0 0 0 350 NTshimlakha 65 27 92 70 63 37 350 YSibsoo 10 48 58 17 100 0 350 NGedu 0 106 106 0 0 0 350 NSamtse 10 345 355 2 100 0 350 YGomtu 41 11 52 78 100 0 350 YBali 0 38 38 0 0 0 350 NMongar 414 355 769 53 68 32 350/450 YSamdrup Jonkhar 0 50 50 0 0 0 350 NRiserbo 0 48 48 0 0 0 350 NTrashigang 121 189 310 39 30 70 350 YPema Gatshel 0 67 67 0 0 0 350 NDeothang 0 101 101 0 0 0 350 NTrashiyangtse 0 35 35 0 0 0 350 NLhuntse 0 65 65 0 0 0 350 NGelephu 115 479 594 19 100 0 350/450 NTrongsa 0 51 51 0 0 0 350 NDagana 0 23 23 0 0 0 350 NYebilaptsa 0 50 50 0 0 0 350 NSarpang 0 87 87 0 0 0 350 NDamphu 0 65 65 0 0 0 350 NBumthang 0 176 176 0 0 0 350 NTotal 3686 4342 8028 46 927 273

44
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 5: Reasons for deferral of blood donors (NA: data not available)
Blood centersReasons for Deferrals
Low Hb% Medical/Surgical conditions
Malaria, H/o travel High risk Others Total
JDW, NRH 227 167 9 90 79 572Gidakom 0 1 0 0 0 1Punakha 17 4 1 6 0 28Paro 12 14 0 2 13 41Phuntsholing NA NA NA NA NA NABajothang 0 0 0 1 0 1Tshimalakha 0 0 0 1 1 2Sibsoo 4 0 0 0 0 4Gedu NA NA NA NA NA NASamtse 10 3 0 3 3 19Gomtu 3 3 0 0 0 6Bali 8 0 2 0 0 10Mongar 9 12 0 12 0 33Samdrup Jongkhar NA NA NA NA NA NAReserboo 0 1 0 0 0 1Trashigang NA NA NA NA NA NAPema Gatshel NA NA NA NA NA NADeothang NA NA NA NA NA NATrashiyangtse 2 0 0 1 2 5Lhuntse 0 0 0 0 0 0Gelephu 9 6 11 9 2 37Trongsa 0 0 0 0 0 0Dagana 1 0 0 0 0 1Yebilpatsa 0 1 0 3 0 4Sarpang 0 0 0 2 1 3Damphu 7 0 0 4 0 11Bumthang 1 1 0 3 0 5Total 310 213 23 137 101 784

45
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 6: Number & type of blood units tested ‘REACTIVE’ to each TTI in 27 blood centres
Blood centers HIV HBV HCV SyphilisVR VR% RR RR% T% VR VR% RR RR% T% VR VR% RR RR% T% VR VR% RR RR% TR%
JDW (post) 0 0 0 0 0 28 1.03 15 1.7 1.2 2 0.07 4 0.45 0.16 9 0.33 10 1.13 0.53
Gidakom (post) 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Punakha (post) 0 0 0 0 0 1 1.18 3 1.92 1.66 0 0 0 0 0 1 1.18 4 2.56 2.07
Paro (post) 0 0 0 0 0 0 0 3 1.09 0.97 0 0 0 0 0 0 0 0 0 0
Phuntsholing (post)
0 0 0 0 0 0 0 2 0.4 0.37 0 0 0 0 0 0 0 9 1.83 1.66
Bajothang (pre) N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 1 1.11 1.11
Tshimalakha (post)
0 0 0 0 0 0 0 1 3.7 1.08 0 0 0 0 0 0 0 0 0 0
Sibsoo (post) 0 0 0 0 0 1 10 0 0 1.72 0 0 0 0 0 0 0 0 0 0
Gedu N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Samtse (pre) 0 0 1 0.29 0.28 0 0 2 0.58 0.56 0 0 1 0.29 0.28 0 0 2 0.58 0.56
Gomtu (post) 0 0 0 0 0 0 0 1 9 1.92 0 0 0 0 0 0 0 0 0 0
Bali N N 0 0 0 N N 0 0 0 N N 0 0 0
Mongar (post) 1 0.24 0 0 0.13 6 1.45 1 0.28 0.91 0 0 0 0 0 3 0.72 9 0.55 1.56
Samdrup Jonkha (pre)
N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Riserboo (pre) N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Trashigang 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 2 1.65 0 0 0.65
Pemagatshel (pre) N N 1 1.49 1.49 N N 6 8.96 8.96 N N 0 0 0 N N 6 8.96 8.96
Deothang (pre) NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA
Trashiyangtse (pre)
N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Lhuntse (pre) N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Gelelephu (post) 1 0.87 0 0 0.17 1 0.87 6 1.25 1.18 0 0 0 0 0 2 1.74 15 3.13 2.86
Trongsa (pre) N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Dagana (post) N N 0 0 0 N N 0 0 0 N N 0 0 0 N N 0 0 0
Yebilaptsa (post) N N 0 0 0 N N 2 4 4 N N 0 0 0 N N 1 2 2
Sarpang (pre) N N 1 1.1 1.1 N N 1 1.1 1.1 N N 0 0 0 N N 0 0 0
Damphu (post) N N 0 0 0 N N 2 3 3 N N 0 0 0 N N 1 1.54 1.54
Bumthang (pre) N N 0 0 0 N N 1 0.57 0.057 N N 0 0 0 N N 2 1.3 1.3
Total 2 0.05 3 0.07 0.06 37 1 46 1.06 1.03 2 0.05 5 0.12 0.09 17 0.5 60 1.38 1
N = No voluntary donors Voluntary units collected = 3,686 Replacement units collected = 4,342 Total collected = 8,028

46
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 7a: Fate of ‘Initial Reactive’ units in western region
W. Blood centers Quarantined for repeat test Discarded if IR
JDW, ELISAHIV YHBV & HCV YSyp Y
GidakomHIV YHBV & HCV YSyp Y
PunakhaHIV YHBV & HCV YSyp Y
ParoHIV YHBV & HCV YSyp Y
PhuntsholingHIV YHBV & HCV YSyp Y
BajothangHIV YHBV & HCV YSyp Y
TshimalakhaHIV YHBV & HCV YSyp Y
SibsooHIV YHBV & HCV YSyp Y
GeduHIV YHBV & HCV YSyp Y
SamtseHIV YHBV & HCV YSyp Y
GomtuHIV YHBV & HCV YSyp Y
BaliHIV YHBV & HCV YSyp Y
Y= Yes

47
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 7b: Fate of ‘Initial Reactive’ units in eastern region
E. Blood Centres Quarantined for repeat test Discarded if IR
Mongar
HIV YHBV YHCV YSyp Y
S/JonkharHIV YHBV & HCV YSyp Y
Riserboo
HIV YHBV YHCV YSyp Y
TrashigangHIV YHBV & HCV YSyp Y
Pema GatshelHIV YHBV & HCV YSyp Y
DeothangHIV YHBV & HCV YSyp Y
TrashiyangtseHIVHBV & HCVSyp Y
LhuntseHIV YHBV & HCV YSyp Y
Y= Yes

48
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 7c: Fate of ‘Initial Reactive’ units in central region
C. Blood Centres Quarantined for repeat test Discarded if IR
Gelephu
HIV YHBV YHCV YSyp Y
Trongsa
HIV YHBV YHCV YSyp Y
Dagapela
HIV YHBV YHCV YSyp Y
Yebilaptsa
HIV YHBV YHCV YSyp Y
Sarpang
HIV YHBV YHCV YSyp Y
Damphu
HIV YHBV YHCV YSyp Y
Bumthang
HIV YHBV YHCV YSyp Y
Y= Yes

49
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 8a: Storage and transport equipment used and temperature control practices (NR: not required; NF: not functioning)
Blood storage & Equipment
Western blood centersTotal
JDW Gida-kom
Puna-kha Paro P/
ling Bajo T/kha
Sib-soo Gedu Sam-
tse Gomtu Bali
Storage-Blood Bank refrigerator
Yes √ √ √ √ √ NF √ 7, 1 NF
No √ √ √ √ √ 5
Storage-Domestic fridge
Yes √ √ √ √ √ √ 6No
Storage- plasma freezer
Yes √ 1No NR NR NR NR NR NR NR NR NR NR NR
Storage- Deep freezerYes √ 1No √ √ √ √ √ √ √ √ √ √ √ 11
Storage- PA with PIYes √ 1No NR NR NR NR NR NR NR NR NR NR NR
Temperature in range for all eq.
Yes √ √ √ √ √ √ √ √ √ √ 10No √ √ 2
Temperature monitored
Yes √ √ √ √ √ √ √ √ √ √ 10No √ √ 2
Temperature record sheet
Yes √ √ √ √ √ √ √ √ √ √ 10no √ √ 2
Transport equipmentVaccine carrier √ √ √ √ √ √ √ √ √ √ √ √ 12Thermo cool boxes √ √ 2Picnic boxesNone
Blood stocks monitored
Yes √ √ 2No √ √ √ √ √ √ √ √ √ √ 10

50
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 8b: Storage and transport equipment used and temperature control practices (NR: not required; NF: not functioning)
Blood storage equipment
Eastern blood centers TotalMongar S/Jong Re/boo T/gang P/gatsh Deothang T/yantse Lhutse
Storage-Blood Bank refrigerator
Yes √ √ NF √ √ 4, 1NFNo √ √ √ 3
Domestic fridge used for Bld storage
Yes √ √ √ √ √ √ 6No √ √ 2
Storage- plasma freezer
YesNo √ NR NR NR NR NR NR NR 1
Storage- Deep freezer
YesNo √ √ √ √ √ √ √ √ 8
Storage- PA with PIYesNo √ NR NR NR NR NR NR NR 1
Temperature in range for all func eq.
Yes √ √ √ √ √ √ √ 7No √ 1
Temperature monitored
Yes √ √ √ √ √ √ √ 7No √ 1
Temperature record sheet
Yes √ √ √ √ √ √ 6No √ √ 2
Transport equipmentVaccine carrier √ √ √ √ √ √ √ 7Thermo cool boxesPicnic boxes None √ 1
Blood stocks monitored
Yes √ √ √ √ 4No √ √ √ √ 4

51
Comprehensive assessment study of Blood Transfusion Service, Bhutan-2011
Annexure 8b: Storage and transport equipment used and temperature control practices (NR: not required; NF: not functioning)
Blood storage equipmentCentral blood centers
TotalGelephu Trongsa Dagana Yebilaptsa Sarpang Damphu Bumthang
Storage-Blood Bank refrigerator
Yes √ √ √ √ √ 5
No √ √ 2
Storage-Domestic fridgeYes √ √ √ √ 4
No √ √ √ 3
Storage- plasma freezer Yes
No NR NR NR NR NR NR NR
Storage- Deep freezerYesNo √ √ √ √ √ √ √ 7
Storage- PA with PIYes
No NR NR NR NR NR NR NR
Temperature in range for all eq.
Yes √ √ √ √ √ √ √ 7
No
Temperature monitoredYes √ √ √ √ √ √ √ 7
No
Temperature record sheetYes √ √ √ √ √ √ √ 7
No
Transport equipment
Vaccine carrier √ √ √ √ √ 5
Thermo cool boxes
Picnic boxes
None √ √ 2
Blood stocks monitored Yes √ √ 2
No √ √ √ √ √ 5

Comprehensive Assessment of Blood Centers 2010 Page No # 1
ASSESSMENT TOOL FOR THE COMPREHENSIVE STUDY OF THE BLOOD CENTRES IN BHUTAN.
Part 1: ASSESSING THE HEALTH FACILITY
P1.1 Name of the health facility : ……………………………………….P1.2 Official Address of the facility : ………………………………………..P1.3 Number of existing beds : ..............................................................P1.4 Name of the Respondent : ..............................................................P1.5 Designation : ………………………………………..P1.6 E-mail : ………………………………………..P1.7 Telephone (0) and (M) : ………………………………………..P1.8 Fax : ………………………………………..P1.9 Date of Assessment done : ………………………………………..P1.10 The estimated population size served by the facility :………………..( Residential or Census)P1.11 Total number of clinicians-GDMOs : ………………………………………..P1.12 Total number of clinicians,-Specialists : ……………………..............................
Types of specialists to be mentioned:Category Number
P1.13 Is any budget allocated from the annual hospital budget for blood transfusion related activities?
1. Yes2. No
P1.14 Was any budget obtained from the blood safety program in the last five years (2005-2010) to conduct similar activities?
1. Yes2. No
P1.15 If yes, fill up the table below
S/No Activity conducted Year Remarks (if any)
P1.16 Is there any support (financial or in kind) provided directly from any organization/ individual to your blood centre?
1. Yes2. No
P1.17 If yes, fill in the table
Organization or Individual Amount in Nu BTS activity supported

Comprehensive Assessment of Blood Centers 2010 Page No # 2
P1.18 Is your health facility identified as a specialised centre? 1. EMOC centre2. Trauma3. None4. Others (specify):5. .....................
P1.19 Do you receive prior information on the posting of a specialist/GDMO at your facility from the higher authorities?
1. Yes2. No
P1.20 If yes, how early is the information received? ………………days/months/year
Note: It has been found that the shortages or surplus of medicines, reagents and other laboratory supplies is often due to a specialist posted or transferred out from a facility without prior information .
P1.21 Through your experience as an administrator, can you share or provide some additional reasons for the below problems faced in your facility or had faced earlier in another centre? What suggestions or solutions can you give to solve these problems?
Sl. No Problems faced List major reasons Solutions/Suggestions
1 Shortages of laboratory reagent/ supplies
2 Shortages of blood stocks
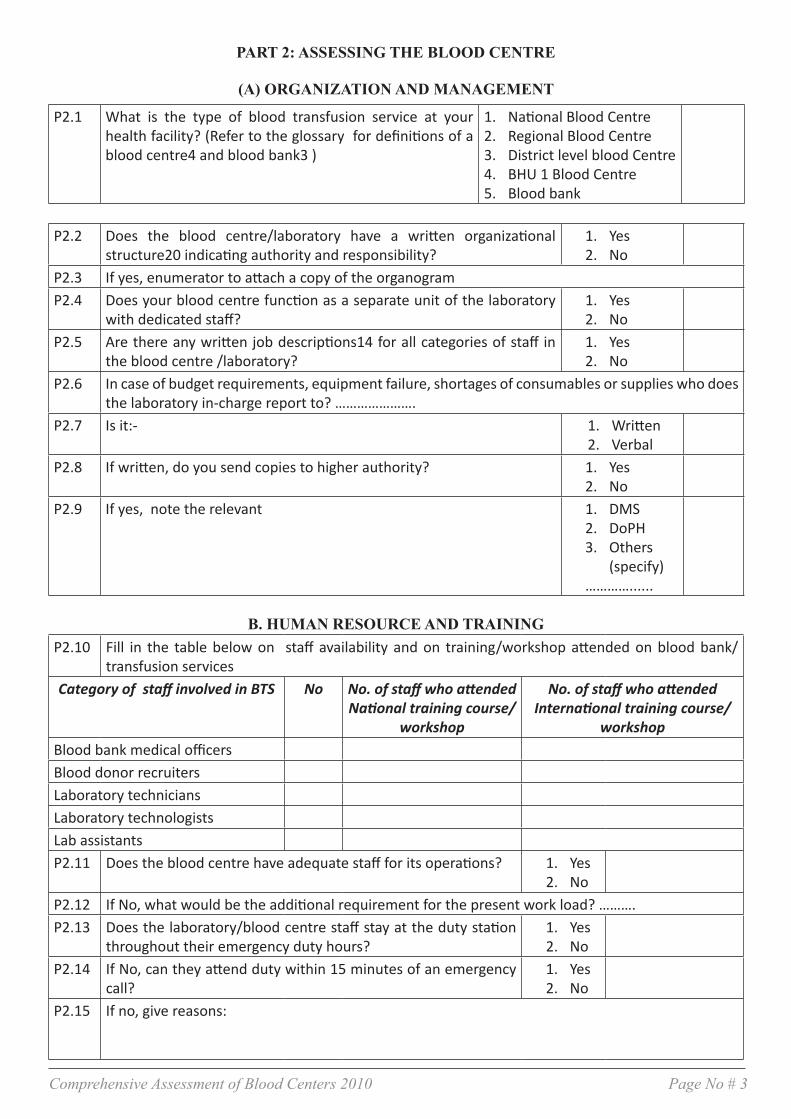
Comprehensive Assessment of Blood Centers 2010 Page No # 3
PART 2: ASSESSING THE BLOOD CENTRE
(A) ORGANIZATION AND MANAGEMENT
P2.1 What is the type of blood transfusion service at your health facility? (Refer to the glossary for definitions of a blood centre4 and blood bank3 )
1. National Blood Centre2. Regional Blood Centre3. District level blood Centre4. BHU 1 Blood Centre5. Blood bank
P2.2 Does the blood centre/laboratory have a written organizational structure20 indicating authority and responsibility?
1. Yes2. No
P2.3 If yes, enumerator to attach a copy of the organogramP2.4 Does your blood centre function as a separate unit of the laboratory
with dedicated staff?1. Yes2. No
P2.5 Are there any written job descriptions14 for all categories of staff in the blood centre /laboratory?
1. Yes2. No
P2.6 In case of budget requirements, equipment failure, shortages of consumables or supplies who does the laboratory in-charge report to? ………………….
P2.7 Is it:- 1. Written2. Verbal
P2.8 If written, do you send copies to higher authority? 1. Yes2. No
P2.9 If yes, note the relevant 1. DMS2. DoPH3. Others
(specify)…………......
B. HUMAN RESOURCE AND TRAININGP2.10 Fill in the table below on staff availability and on training/workshop attended on blood bank/
transfusion services Category of staff involved in BTS No No. of staff who attended
National training course/ workshop
No. of staff who attended International training course/
workshopBlood bank medical officersBlood donor recruitersLaboratory techniciansLaboratory technologistsLab assistantsP2.11 Does the blood centre have adequate staff for its operations? 1. Yes
2. NoP2.12 If No, what would be the additional requirement for the present work load? ……….P2.13 Does the laboratory/blood centre staff stay at the duty station
throughout their emergency duty hours?1. Yes2. No
P2.14 If No, can they attend duty within 15 minutes of an emergency call?
1. Yes2. No
P2.15 If no, give reasons:

Comprehensive Assessment of Blood Centers 2010 Page No # 4
C. EQUIPMENT & SUPPLIES2.16 Please provide information on the availability and functional status of the equipment in your blood
centre/laboratory based on the list below.
Equipment Number available
Number required
Number functioning
Donor beds/couchesDonor weighing machineHaemocue/any other instrument for Haemoglobin Estimation of blood donorsBlood Pressure instrumentClinical ThermometerBlood bag weighing scale (manual or electronic)Automatic blood collection monitor with shakerDielectric Tube sealers Tube stripperLaboratory bench top centrifuge for separation of samples and serological testsAutomatic Cell washerIncubator or water bathRefrigerated centrifuge for blood component preparationElectronic balance for comparing weights of two bags at same timeBlood bank refrigeratorPlasma freezer –300CPlatelet incubator and shakerPlatelet shakerPlasma extractorPlasma thawer
General items Number available
Number required
Number functioning
Binocular microscopeLaboratory/ domestic refrigerator for reagent storage Micro plate shakerELISA plate washerELISA plate readerLaboratory thermometerMicro pipetteStop watch/timer AutoclaveHaematology auto analyzer

Comprehensive Assessment of Blood Centers 2010 Page No # 5
P2.17 Are the staffs at your blood centre trained on calibrating8 equipment? 1. Yes2. No
P2.18 Are the staffs at your blood centre trained on use of equipment? 1. Yes2. No
P2.19 Are the staffs at your blood centre trained to carry out preventive main-tenance as indicated in the equipment’s operational manual?
1. Yes2. No
P2.20 Does your health facility have a Biomedical engineering unit? 1. Yes2. No
P2.21 If no, what is the procedure for equipment repair?……………………….……………………….……………………….................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
P2.22 Is there a system for follow-up on the non functioning equipments sent for repair?
1. Yes2. No
P2.23 If yes, is the follow-up done: 1. Verbal2. Written
P2.24 Is a standard list of blood bank reagents available for annual procure-ment25?
1. Yes2. No
P2.25 If yes, provide the list (enumerator to compare with the standard list of blood bank reagents provided to you and make comments)....................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
P2.26 Who does the quantification of supplies for your blood centre
1. Pharmacy 2. Lab In-charge3. Other (specify)…………………….
P2.27 Is there a system of regular stock checks for all the sup-plies?
1. Yes2. No
P2.28 Is the blood centre/laboratory staffs trained on inventory15 keeping? 1. Yes2. No
P2.29 Has any of the following supplies run out of stock in the last 12 months?
Item Yes No If yes, indicate number approx days or months Action taken
Blood bags
TTI test kits
Blood GroupingReagents
Others (specify)…………………..................................................................................................

Comprehensive Assessment of Blood Centers 2010 Page No # 6
P2.30 Which of the services were affected? 1. Blood donations were stopped2. Routine blood transfusion postponed/
cancelled?3. Routine Surgeries postponed/can-
celled? 4. Emergency services needing blood
transfusion affected5. Other services (specify): ………………
.........................................................P2.31 At the time of shortage/out of stock,
were patients made to buy the test kits/consumables from local market?
1. Yes2. No

Comprehensive Assessment of Blood Centers 2010 Page No # 7
D. PREMISES
P2.32 Does the blood centre have suitable areas /rooms for (Tick the appropriate box): Rooms for Yes NoDonor interview and donor physical examination Blood donation procedure TTI testingBlood processing into componentsImuno-hematology testingBlood storage equipment
2.33 Does the centre/laboratory have:- Yes NoContinuous water supplyUninterrupted power supply(is a back up service available in times of power failure)Air conditioning facility for maintaining room temperature between +20 to +24ºC2.34 Does the centre/laboratory have access to :- Yes No
TelephoneFaxInternet facility

Comprehensive Assessment of Blood Centers 2010 Page No # 8
PART 3: Quality system33
P3.1 Does your blood centre/laboratory have a quality manual32 developed? 1. Yes2. No
P3.2 If yes, produce copy for verification (enumerator to make an observation and comment)………………………………………………………………………………………
P3.3 Does your laboratory/blood centre have a quality manager31? 1. Yes2. No
P3.4 Is inspection (audit1) conducted at your blood centre atleast once in 2 years? 1. Yes2. No
P3.5 Does your centre have Standard Operating Procedures42 (SOPs)? 1. Yes2. No
P3.6 If yes, 1. Internally/In-house developed2. Provided by National blood
bank (central)
Fill up the table below Name of test Developed by: Used/not used
Cent. Int.
Name of test Developed by: Used/not usedCent. Int.
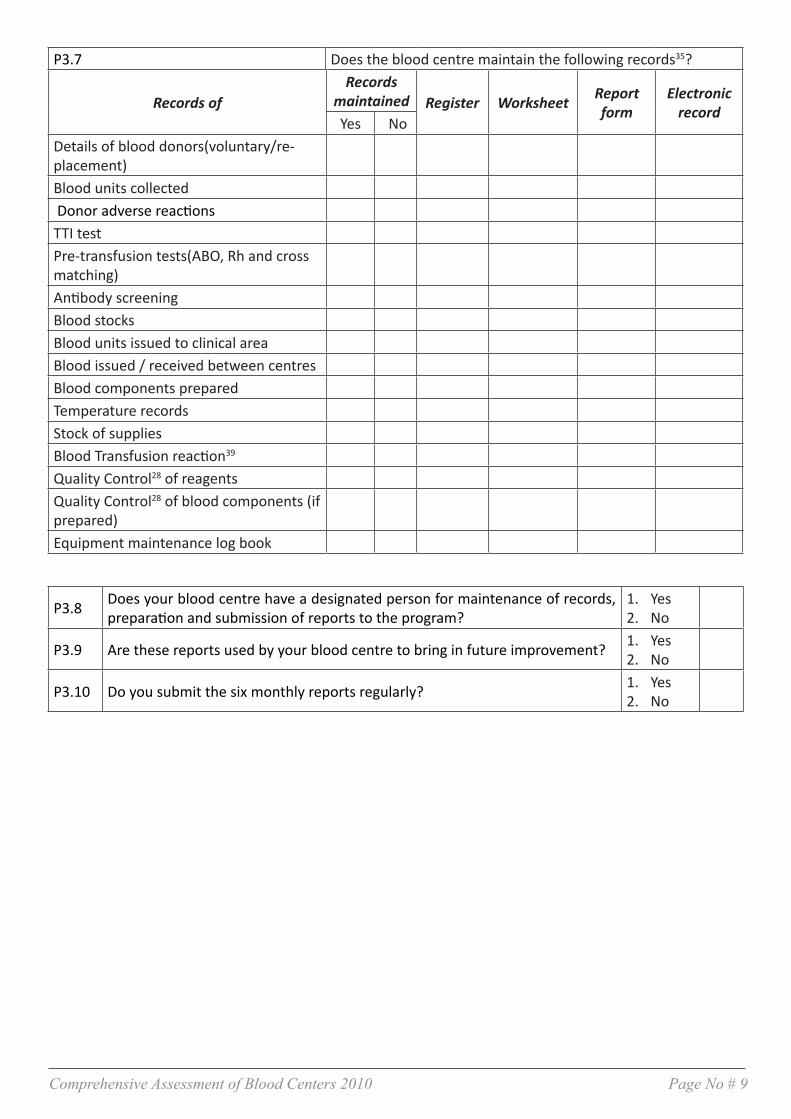
Comprehensive Assessment of Blood Centers 2010 Page No # 9
P3.7 Does the blood centre maintain the following records35?
Records ofRecords
maintained Register Worksheet Report form
Electronic record
Yes NoDetails of blood donors(voluntary/re-placement)Blood units collected Donor adverse reactionsTTI testPre-transfusion tests(ABO, Rh and cross matching)Antibody screeningBlood stocksBlood units issued to clinical areaBlood issued / received between centresBlood components preparedTemperature recordsStock of suppliesBlood Transfusion reaction39
Quality Control28 of reagentsQuality Control28 of blood components (if prepared)Equipment maintenance log book
P3.8 Does your blood centre have a designated person for maintenance of records, preparation and submission of reports to the program?
1. Yes2. No
P3.9 Are these reports used by your blood centre to bring in future improvement? 1. Yes2. No
P3.10 Do you submit the six monthly reports regularly? 1. Yes2. No

Comprehensive Assessment of Blood Centers 2010 Page No # 10
PART 4: BLOOD DONORS & BLOOD COLLECTION
P4.1 Is donor information10 /education activity undertaken by your blood centre? 1. Yes2. No
P4.2 Are educational materials available and used for donor information? (These are the IEC materials developed by the National Blood Bank)
1. Yes2. No
P4.3 Is pre-donation counselling23 provided by your blood centre? 1. Yes2. No
Enlist the institutions, government offices, monasteries etc that can be used for donor recruitment activities in your catchment areasSr. No Name
P4.4 Does your blood centre have trained donor recruitment staff? 1. Yes2. No
P4.5 Is there a doctor or trained personnel in your blood centre who can manage issues such as donor health11b and donor safety11c?
1. Yes2. No
P4.6 Was the ‘World Blood Donor Day’ observed by the centre in any of the last 5 years?
1. Yes2. No
P4.7 If yes, which year:
1. 20062. 20073. 20084. 20095. 2010
P4.8 Does your blood centre follow the national donor selection criteria11a and guidelines for the donor suitability?
1. Yes2. No
P4.9 Does your blood centre perform the following to assess donor suitability? Method Yes NoUse of standard donor questionnaire formPre-donation counselling23 & interviewPhysical check like temperature and pulseMeasurement of weight and blood pressureHb% check
P4.10 Is donor confidentiality ensured while assessing donor suitability? 1. Yes
2. NoP4.11 Which of the following methods do you use for donor haemoglobin estimation? Method1.Photometer2.Hemocue3.Hb colour scale 4.Automated Haematology analyser5.Sahli’s method

Comprehensive Assessment of Blood Centers 2010 Page No # 11
P4.12 Indicate the number of whole blood units collected during the reporting period from 1st January to 31st December 2009, by type of donation
Type of donation Number of unitsCentre Mobile
Voluntary Replacement
P4.13 Do you have regular donors38 in your centre? 1. Yes2. No
P4.14 What is the volume of whole blood collected by your centre? 1. 350ml2. 450ml
P4.15 Please indicate the number of pre-donation deferrals against reasons below during the reporting period 1st Jan to 31 Dec.2009
Reasons NumberLow haemoglobinMedical/surgical conditionsHigh-risk behaviourTravel to malaria endemic area or H/o malariaOther non-specific reasons (menstruation ,pregnancy, breast feeding fear of needles, low weight)Total No. of deferralsP4.16 Does your blood centre provide blood units to other centres/blood
bank?1. Yes2. No, If no go to part 5
P4.17 If yes, tabulate below and answer P4.18
Name of blood centre
Regular mode of transportation
(ambulance, private vehicle, bus)
Time taken approx No. of units supplied in 2009
P4.18 What is the number of blood units provided to other centres in 2009?Blood centre/blood
bank Jan
Feb
Mar
Apr
May
June
July
Aug
Sep
Oct
Nov De
c

Comprehensive Assessment of Blood Centers 2010 Page No # 12
PART 5: SCREENING FOR TRANSFUSION TRANSMITTED INFECTIONS (TTIS)
P5.1 Which of the TTIs are tested on the donated blood at your blood cen-tre?
1. HIV 1 & 22. Hepatitis B3. Hepatitis C4. Syphilis5. Malaria
P5.2 Are the screening tests for TTIs done in the: 1.Pre - donation 2.Post - donation
P5.3 Indicate the number of potential blood donors/blood units screened for individual TTI from 1st Jan to 31st Dec. 2009 in the table below
Transfusion Transmitted Infection Number screened HIV 1 & 2Hepatitis BHepatitis CSyphilisMalaria
P5.4 Tick the test method(s) used for screening the blood units for TTIsInfections Rapid test ELISA Chemiluminescence Any other (specify)
HIV 1 & 2Hepatitis BHepatitis CSyphilisMalaria
P5.5 If more than one test method is used in your blood centre during 2009, fill in the table below
Infections The number of donations tested by each of the following methodsRapid Test ELISA Chemiluminescence Any Other, specify
HIV 1 & 2Hepatitis BHepatitis CSyphilisMalaria

Comprehensive Assessment of Blood Centers 2010 Page No # 13
P5.6 If you are doing Pre-donation screening, do you routinely repeat the test us-ing post-donation sample?
1. Yes2. No
P5.7 Is a ‘REPEAT’ test done on all ‘HIV Initial Reactive’17 samples? 1. Yes2. No
P5.8 If yes, provide an algorithm1 if any followed (enumerator to make observation and comment)………………………………………………………………………………………………………………………………………………………………………..If your answer is No what is done to the unit?……………………………………………………………………………………………………………………………………………………………………………………What do you do to the concerned donor?……………………………………………………………………………………………………………………………………………………………………………
P5.9 Is a ‘REPEAT’ test done on all ‘HBV Initial Reactive’17 samples? 1. Yes2. No
P5.10 If yes, provide an algorithm1 if any followed (enumerator to make observation and comment)………………………………………………………………………………………………………………………………………………………………………..If your answer is No what is done to the unit?……………………………………………………………………………………………………………………………………………………………………………………What do you do to the concerned donor?……………………………………………………………………………………………………………………………………………………………………………
P5.11 Is a ‘REPEAT’ test done on all ‘HCV Initial Reactive’17 samples? 1. Yes2. No
P5.12 If yes, provide an algorithm if any followed (enumerator to make observation and comment)………………………………………………………………………………………………………………………………………………………………………..If your answer is No what is done to the unit?……………………………………………………………………………………………………………………………………………………………………………………What do you do to the concerned donor?……………………………………………………………………………………………………………………………………………………………………………
P5.13 For Syphilis, if RPR is reactive do you do TPHA? 1. Yes2. No
P5.14 If yes, provide an algorithm if any followed (enumerator to make observation and comment)………………………………………………………………………………………………………………………………………………………………………..If your answer is No what is done to the unit?……………………………………………………………………………………………………………………………………………………………………………………What do you do to the concerned donor?……………………………………………………………………………………………………………………………………………………………………………

Comprehensive Assessment of Blood Centers 2010 Page No # 14
P5.15 If a ‘REPEAT’ test is performed on all ‘Initial Reactive’17 samples, provide the following details in the table below
TTI marker Screening test reactiveNo. of initial reactive (IR) 17 Number of repeat reactive (RR)37
Anti-HIV 1 & 2 antibodiesHepatitis B surface antigenAnti-Hepatitis C antibodies
P5.16 Are ‘REPEAT REACTIVE’37 samples sent to PHL or Clinical Laboratory, Thimphu for confirmatory tests? For HIV:
1. Yes2. No
P5.17 Are ‘REPEAT REACTIVE’37 samples sent to PHL or Clinical Laboratory, Thimphu for confirmatory tests? For HBV:
1. Yes2. No
P5.18 Are ‘REPEAT REACTIVE’37 samples sent to PHL or Clinical Laboratory, Thimphu for confirmatory tests? For HCV:
1. Yes2. No
P5.19 Does your centre receive the confirmatory test results from the concerned unit?
1. Yes2. No
P5.20 How long does it take to receive the confirmatory test result? ………………..days
P5.21 Does your centre keep records of screening tests performed for TTI marker, by type of donations?
1. Yes2. No
P5.22 If Yes, provide the following details
TTI Marker No. of Voluntary donations found Reactive
No. of Replacement donations found Reactive
Anti-HIV 1 & 2 antibodiesHepatitis B surface antigenAnti-Hepatitis C antibodiesRPRTPHA
P5.23 Is blood ever issued without screening for TTIs? 1. Yes2. No
P5.24 If yes, complete the following table: Reasons for issuance (Tick as appropriate)
Infections Test kits/reagents not available
Emergencytransfusion
Other reason
No. of units issued
HIV 1 & 2 Hepatitis B Hepatitis C Syphilis

Comprehensive Assessment of Blood Centers 2010 Page No # 15
P5.25 In your blood centre, who authorizes issuance for transfusion of unscreened blood?...……………………………………………………………………
P5.26 Does your blood centre store frozen samples of donor plasma/serum? 1. Yes2. No
P5.27 If yes, for how long? …………………………. (days)P5.28 If no, give reasons:
...……………………………………………………………………………………………………………………………………………
P5.29 If yes, are these used for retrospective (look-back) studies? 1. Yes2. No
P5.30 Is Internal Quality Control30 run with each test? 1. Yes2. No
P5.31 For rapid test users, are the results cross-checked by two staff before releasing the result?
1. Yes2. No
P5.32 Does your centre participate in an external quality assessment scheme (EQAS) 13 for TTI testing?
1. Yes2. No
P5.33 If yes, at which level does the centre participate in EQAS13? Fill the table belowLevel1.International2.Regional (WHO SEARO)3.National
P5.34 Are test kits/reagents and samples stored in temperature-monitored environment? Fill in the table below
Items Yes No
Reagents and Test kits
Donor samples
P5.35 Are the reagents and donor samples stored separately? 1. Yes2. No
P5.36 If no, why?
...……………………………………………………………………
………………………………………………………………………

Comprehensive Assessment of Blood Centers 2010 Page No # 16
PART 6: BLOOD GROUP SEROLOGY & COMPATIBILITY TESTING
P6.1 Which of following tests are performed on blood donations for determination of ABO and Rh (D) grouping and what techniques are followed? (tick)
Technique Slide Tube Not doneForward grouping for ABOSerum Grouping for ABORhD Grouping
P6.2 Do you perform red cell antibodies screening test on patient blood samples? 1. Yes2. No
P6.3 Has your centre participated in any external quality assessment scheme (EQAS) 13 for Blood Grouping Serology in the last 5 years?
1. Yes2. No
P6.4 If yes, at which level does the centre participate in EQAS13? Level1.International2.Regional (WHO SEARO)3.NationalP6.5 Does the centre perform compatibility test? 1. Yes
2. NoP6.6 If yes, tabulate the below for the reporting period 1 Jan to 31 Dec 2009:Compatibility test Number of testsPatient’s ABO groupingPatient’s Rh typingCross-matchingAntibody screening test

Comprehensive Assessment of Blood Centers 2010 Page No # 17
PART 7: BLOOD STORAGE, TRANSPORTATION, INVENTORY & DISTRIBUTION
P7.1 Are blood and blood components stored within the pre-defined temperatures as per the SOPs42?
1. Yes2. No
P7.2 Is the temperature of the blood storage equipment monitored in your blood cen-tre?
1. Yes2. No
P7.3 Does your blood centre use domestic refrigerator/freezer for storage of blood or blood components respectively?
1. Yes2. No
P7.4 If yes, complete the table belowEquipment Number of equip-
mentEstimated % of blood and blood components
storedDomestic refrigerator for whole blood/red cell storageDomestic freezer for FFP storage
P7.5 Is the temperature of the above equipment monitored at regular intervals? 1. Yes2. No
P7.6Enumerator to make observation where the blood bags are stored, thermometer position in the refrigerator and comment………………………………………………………………………………
P7.7 Does your blood centre have separate storage areas for following purposes? Storage of Yes NoQuarantine/untested unitsReady for issue units Reactive units for discarding P7.8 How do you transport blood units to the clinical areas? Type of container1. Vaccine carrier 2.Thermocool boxes3.Picnic boxes4.None
P7.9 Do you check the temperature of the random blood unit(s) on receipt from other centre or mobile sites?
1. Yes2. No
P7.10 Is there a mechanism for monitoring stock of blood and blood components? 1. Yes2. No
P7.11 Is the returned blood unit reused? 1. Yes2. No
P7.12 Are any criteria or SOP42 followed to reuse the returned blood? 1. Yes2. No
P7.13 Indicate the number of blood units discarded as per reasons stated below in 2009 reporting period:
Reasons for discard Whole blood and Red cell Platelets FFP/PlasmaTTI Reactive unitsExpired unitsFaulty collectionFaulty storage Any other reason

Comprehensive Assessment of Blood Centers 2010 Page No # 18

Printed @ Lhazeen Printing Press, Changzamtog
1




![Clinical Study Comprehensive Look at Blood Transfusion ... · autologous transfusion[ ]. Using autologous donations for transfusion avoids many of the adverse events associated with](https://static.fdocuments.in/doc/165x107/60c99f0bc8ad33300f37a7c4/clinical-study-comprehensive-look-at-blood-transfusion-autologous-transfusion.jpg)