
Complications After Minimally Invasive Total Knee Arthroplasty as Compared With Traditional Incision...
7
Complications After Minimally Invasive Total Knee Arthroplasty as Compared With Traditional Incision Techniques A Meta-Analysis Rajiv Gandhi, MD, MS, FRCSC, * Holly Smith, * Kelly A. Lefaivre, MD, MSc, FRCSC, y J. Rod Davey, MD, FRCSC, * and Nizar N. Mahomed, MD, ScD, FRCSC z§|| b Abstract: The primary objective of our meta-analysis was to compare the incidence of complications between minimally invasive surgery and standard total knee arthroplasty (TKA) approaches. We reviewed randomized controlled trials comparing minimally invasive TKA to standard TKA. After testing for publication bias and heterogeneity, the data were aggregated by random effects modeling. Our primary outcome was the number of complications. Our secondary outcomes were alignment outliers, Knee Society Function scores, and Knee Society Knee scores. The combined odds ratios for complications for the minimally invasive surgery group and alignment outliers were 1.58 (95% confidence interval, 1.01-2.47; P b .05) and 0.79 (95% confidence interval, 0.34-1.82; P = .58), respectively. The standard difference in means for Knee Society scores was no different between groups. Minimally invasive knee surgery should be approached with caution. Keywords: minimally invasive, knee, complications. © 2011 Elsevier Inc. All rights reserved. Minimally invasive knee arthroplasty surgery has experienced a recent surge in popularity, driven by the patient concerns of a faster recovery time and a shorter, more cosmetic scar [1]. After first being successfully applied to unicompartmental knee arthroplasty [2,3], the principles of minimally invasive surgery (MIS) were then expanded to total knee arthroplasty (TKA). The limited incision approaches to TKA include the mini- midvastus [4], the subvastus [5], and mini-arthrotomy techniques [6]. Possible advantages of MIS TKA include less postoperative pain [7], a faster functional recovery [8,9], decreased length of hospital stay [9], and less blood loss [6,10]. The evaluation of any new medical therapy must include a detailed evaluation of both efficacy and safety outcomes. Postoperative complication rates after MIS TKA have been documented in many studies; some have reported more complications in MIS TKA compared with the standard technique, whereas others report fewer or no significant difference. Potential drawbacks of MIS TKA include longer tourniquet times [11-13], poor component placement [11,14] and early implant failure [15]. It is important to note that no published study comparing the MIS technique with the standard technique is adequately powered to report any statistical comparison of complication rates. The literature evaluating the outcomes of MIS TKA consists mainly of nonrandomized prospective and retrospective cohort studies. In many cases, the authors imposed strict eligibility criteria for patients undergoing MIS TKA, limiting the generalizability of their findings. In addition, many of the studies are conducted by individuals who have developed the surgical techniques and must be interpreted with caution. Randomized controlled trials (RCTs) represent the best available data because they limit the potential confounding between treatment groups. We performed a systematic review and meta-analysis of RCTs to compare the complication rates between MIS From the *Division of Orthopaedic Surgery, Department of Surgery, University Health Network, University of Toronto, Toronto, Canada; yDepartment of Orthopaedic Surgery, University of British Columbia, British Columbia, Canada; zDivision of Orthopaedic Surgery, University Health Network, Toronto Western Research Institute, Toronto, Canada; §Division of Health Care and Outcomes Research and Arthritis Community Research and Evaluation Unit, Toronto Western Research Institute, Toronto, Canada; ||Department of Health Policy, Management and Evaluation, University of Toronto, Toronto, Canada; and bDepartment of Surgery, University of Toronto, Toronto, Canada. Submitted July 6, 2009; accepted November 25, 2009. No benefits or funds were received in support of the study. Reprint requests: Rajiv Gandhi, MD, MS, FRCSC, Toronto Western Hospital, University Health Network, 399 Bathurst St, East Wing 1-439, Toronto, Ontario, Canada M5T-2S8. © 2011 Elsevier Inc. All rights reserved. 0883-5403/2601-0005$36.00/0 doi:10.1016/j.arth.2009.11.022 29 The Journal of Arthroplasty Vol. 26 No. 1 2011
-
Upload
rajiv-gandhi -
Category
Documents
-
view
213 -
download
1
Transcript of Complications After Minimally Invasive Total Knee Arthroplasty as Compared With Traditional Incision...

FromUniversityyDepartmBritish CoHealth N§DivisionResearch aCanada;UniversityUniversity
SubmiNo beReprin
Hospital,Toronto,
© 2010883-5doi:10
The Journal of Arthroplasty Vol. 26 No. 1 2011
Complications After Minimally Invasive TotalKnee Arthroplasty as Compared With
Traditional Incision Techniques
A Meta-Analysis
RajivGandhi,MD,MS,FRCSC,*HollySmith,*KellyA.Lefaivre,MD,MSc,FRCSC,yJ. Rod Davey, MD, FRCSC,* and Nizar N.Mahomed, MD, ScD, FRCSCz§||b
Abstract: The primary objective of our meta-analysis was to compare the incidence ofcomplications between minimally invasive surgery and standard total knee arthroplasty (TKA)approaches. We reviewed randomized controlled trials comparing minimally invasive TKA tostandard TKA. After testing for publication bias and heterogeneity, the data were aggregated byrandom effects modeling. Our primary outcome was the number of complications. Our secondaryoutcomes were alignment outliers, Knee Society Function scores, and Knee Society Knee scores.The combined odds ratios for complications for the minimally invasive surgery group andalignment outliers were 1.58 (95% confidence interval, 1.01-2.47; P b .05) and 0.79 (95%confidence interval, 0.34-1.82; P = .58), respectively. The standard difference in means for KneeSociety scores was no different between groups. Minimally invasive knee surgery should beapproached with caution. Keywords: minimally invasive, knee, complications.© 2011 Elsevier Inc. All rights reserved.
Minimally invasive knee arthroplasty surgery hasexperienced a recent surge in popularity, driven by thepatient concerns of a faster recovery time and a shorter,more cosmetic scar [1]. After first being successfullyapplied to unicompartmental knee arthroplasty [2,3],the principles of minimally invasive surgery (MIS) werethen expanded to total knee arthroplasty (TKA). Thelimited incision approaches to TKA include the mini-midvastus [4], the subvastus [5], and mini-arthrotomytechniques [6]. Possible advantages of MIS TKA includeless postoperative pain [7], a faster functional recovery
the *Division of Orthopaedic Surgery, Department of Surgery,Health Network, University of Toronto, Toronto, Canada;
ent of Orthopaedic Surgery, University of British Columbia,lumbia, Canada; zDivision of Orthopaedic Surgery, Universityetwork, Toronto Western Research Institute, Toronto, Canada;of Health Care and Outcomes Research and Arthritis Communitynd Evaluation Unit, Toronto Western Research Institute, Toronto,||Department of Health Policy, Management and Evaluation,of Toronto, Toronto, Canada; and bDepartment of Surgery,of Toronto, Toronto, Canada.tted July 6, 2009; accepted November 25, 2009.nefits or funds were received in support of the study.t requests: Rajiv Gandhi, MD, MS, FRCSC, Toronto WesternUniversity Health Network, 399 Bathurst St, EastWing 1-439,Ontario, Canada M5T-2S8.1 Elsevier Inc. All rights reserved.403/2601-0005$36.00/0.1016/j.arth.2009.11.022
29
[8,9], decreased length of hospital stay [9], and lessblood loss [6,10].The evaluation of any new medical therapy must
include a detailed evaluation of both efficacy and safetyoutcomes. Postoperative complication rates after MISTKA have been documented in many studies; some havereported more complications in MIS TKA comparedwith the standard technique, whereas others reportfewer or no significant difference. Potential drawbacks ofMIS TKA include longer tourniquet times [11-13], poorcomponent placement [11,14] and early implant failure[15]. It is important to note that no published studycomparing the MIS technique with the standardtechnique is adequately powered to report any statisticalcomparison of complication rates.The literature evaluating the outcomes of MIS TKA
consists mainly of nonrandomized prospective andretrospective cohort studies. In many cases, the authorsimposed strict eligibility criteria for patients undergoingMIS TKA, limiting the generalizability of their findings. Inaddition,manyof the studies are conducted by individualswho have developed the surgical techniques and must beinterpreted with caution. Randomized controlled trials(RCTs) represent the best available data because they limitthe potential confounding between treatment groups.We performed a systematic review and meta-analysis
of RCTs to compare the complication rates between MIS
30 The Journal of Arthroplasty Vol. 26 No. 1 January 2011
TKA and standard TKA. Our secondary objective was tocompare the outcomes of Knee Society scores (KSS) andoutliers from the acceptable range of alignment for these2 treatment groups.
Materials and MethodsEligibility CriteriaWe included articles relevant to the following: (1)
patients underwent primary TKA; (2) the comparisonwas between minimally invasive TKA and standardTKA; (3) the outcome measures included postoperativecomplications, Knee Society Knee scores, Knee SocietyFunction scores, and alignment outliers; and (4) thestudy was a published or unpublished RCT. Studiesevaluating the intervention of computer navigation–assisted MIS TKA were excluded.
Study IdentificationTwo of the authors (RG and HS) independently
completed a computerized search of the onlinedatabases PubMed MEDLINE and OVID MEDLINE(1950 to May 2009) and EMBASE (1950 to 2009)with the following search terms: (total knee arthroplastyOR total knee replacement OR knee prosthesis) AND(minimally invasive OR mini-incision OR less invasive)AND (postoperative complications OR post-op complicationsOR treatment outcome OR joint instability OR recovery offunction). We also searched the Cochrane Database ofSystematic Reviews, the Cochrane Central Register ofControlled Trials, and www.clinicaltrials.gov. Wesearched the archives of orthopedic meetings forpotential abstracts to minimize publication bias. Wereviewed the American Academy of Orthopedic Sur-geons (2001-2009), Knee Society (2001-2009), Cana-dian Orthopedic Association (2003-2009), and BritishOrthopedic Association (2002-2009) meetings.
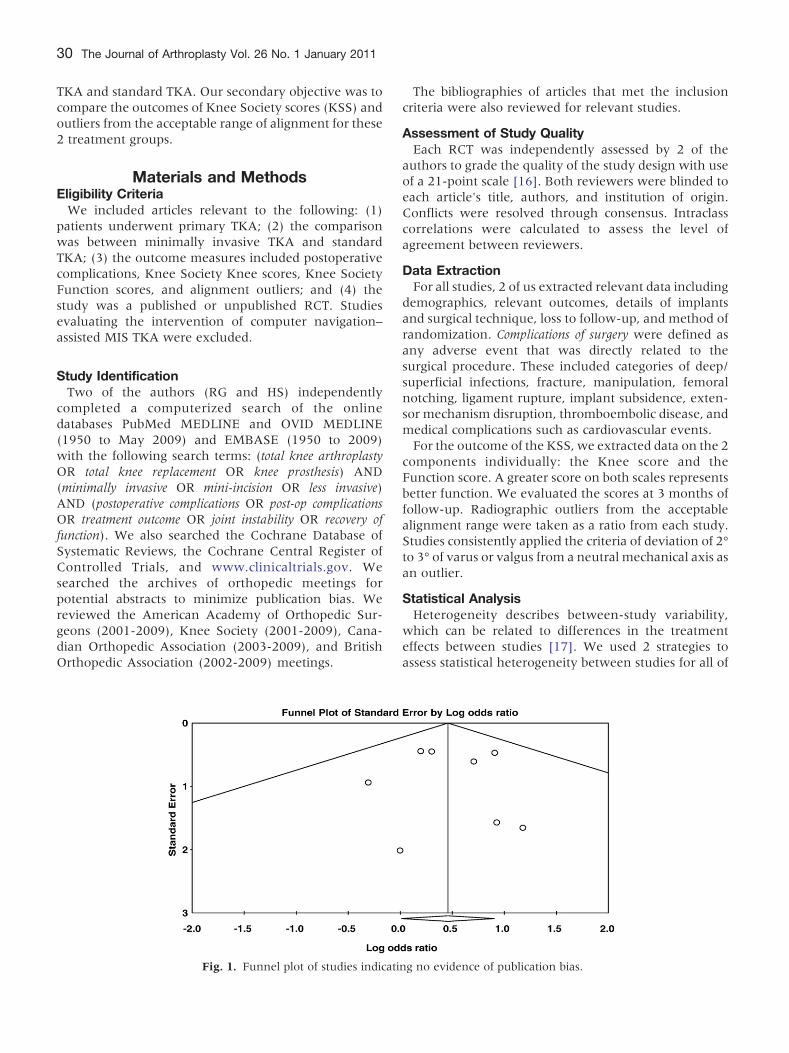
Fig. 1. Funnel plot of studies indicati
The bibliographies of articles that met the inclusioncriteria were also reviewed for relevant studies.
Assessment of Study QualityEach RCT was independently assessed by 2 of the
authors to grade the quality of the study design with useof a 21-point scale [16]. Both reviewers were blinded toeach article's title, authors, and institution of origin.Conflicts were resolved through consensus. Intraclasscorrelations were calculated to assess the level ofagreement between reviewers.
Data ExtractionFor all studies, 2 of us extracted relevant data including
demographics, relevant outcomes, details of implantsand surgical technique, loss to follow-up, and method ofrandomization. Complications of surgery were defined asany adverse event that was directly related to thesurgical procedure. These included categories of deep/superficial infections, fracture, manipulation, femoralnotching, ligament rupture, implant subsidence, exten-sor mechanism disruption, thromboembolic disease, andmedical complications such as cardiovascular events.For the outcome of the KSS, we extracted data on the 2
components individually: the Knee score and theFunction score. A greater score on both scales representsbetter function. We evaluated the scores at 3 months offollow-up. Radiographic outliers from the acceptablealignment range were taken as a ratio from each study.Studies consistently applied the criteria of deviation of 2°to 3° of varus or valgus from a neutral mechanical axis asan outlier.
Statistical AnalysisHeterogeneity describes between-study variability,
which can be related to differences in the treatmenteffects between studies [17]. We used 2 strategies toassess statistical heterogeneity between studies for all of
ng no evidence of publication bias.
Tab
le1.
SummaryDataforRCTsIncluded
inAnalysis
Study
Subjects
MIS
Typ
eMea
nAge
(y)
Male(%
)Mea
nBMI
ImplantTyp
eNo.of
Complications
Mean
Knee
Score
Mea
nFunctionScore
No.of
Outliers
Boergeret
al,2005
M S60
60
MS
69
68
23
25
28
29
LPS
MB&
LPS-flex
13
12
NR
NR
1 0Kim
etal,2007
M S120
120
QS
65.4
65.4
22.5
22.5
28.1
28.1
LPS
16 7
91
92
85
83
NR
Kolisek
etal,2007
M S40
40
MID
67
70
72.5
60
32
30
PS
9 581
77
74
73
0 0Chin
etal,2007
M S60
30
MID
,QS
68.2
63.4
20
10
28.02
29.44
PFC
-FB,LPS
3 2NR
NR
12 3
Tashiroet
al,2007
M S24
25
MID
,QS
76.1
73.9
10 9.5
NR
MB,LPS
-flex&
LPS
1 090
92
92
91
18 14
Karachalioset
al,2008
M S50
50
MID
71.1
70.8
38
30
32
31.5
Gen
esisII
15 13
97
93.8
97
84
3 9Han
etal,2008
M S30
30
MP
66
64
6.7
6.7
26.9
26.4
MB,LPS
-flex
0 0NR
NR
NR
Luringet
al,2008
M S30
30
MP
69
69
NR
31
32
PFC
0 083
86
82
83
5 2Karpman
etal,2008
M S40
19
MID
,QS
73.5
73
37.5
47
29
29
FB,CR
2 0NR
NR
NR
BMIindicates
bodymassindex
;M,minim
ally
inva
sive
;S,stan
dard;
QS,quad
ricepssparing;
MID
,mini-midva
stus;MP,mini-med
ialparap
atellar;MS,mini-subv
astus;FB,fixed
bearing;
MB,
mobile
bearing;
CR,cruciateretaining;
PS,cruciatesubstituting;
PFC
,press-fitcondylar;NR,notreported
.
Complications After MIS TKA and Traditional Techniques � Gandhi et al 31
our outcome measures. Firstly, we used the methods ofHedges and Olkin [18]. A P value b .1 was consideredsuggestive of statistical heterogeneity because these testsare traditionally underpowered. Secondly, we calculatedthe I2 statistic that describes the percentage of totalvariation across studies that is attributable to heteroge-neity rather than chance [19]. A value of less than 25% isconsidered low heterogeneity; 50%, moderate hetero-geneity; and 75%, high heterogeneity [19]. Beforeanalyzing the data, we developed hypotheses of potentialsources of heterogeneity including implant manufactur-er, implant type (fixed bearing vs mobile bearing etc),minimally invasive surgical technique, and study quality.To assess for publication bias, the potential for
negative studies to not be published, we constructed afunnel plot for our primary outcome. This plotdemonstrates the relationship between the sample sizeof the studies and the precision in estimating thetreatment effect (Fig. 1). The x-axis represents the logsodds ratio (OR) as a measure of treatment effect,whereas the y-axis represents a measure of study size.Bias can be seen if the plots are asymmetric about thepooled log OR vs a plot resembling an inverted funnel,which represents no bias [20].For both the categorical outcomes of complications
and radiographic outliers, we used the OR as thesummary statistic. This ratio represents the odds ofcomplications in the MIS group over the odds ofcomplications in the standard group. An OR of greaterthan 1 indicates a greater incidence of complications inthe MIS group, and the point estimate of the OR isconsidered statistically significant if the 95% confidenceinterval (CI) does not include the null value 1. For thosestudies that had a zero in a cell for the number ofcomplications in 1 of the 2 groups, we applied the Yatescorrection, as these cells otherwise create problems withcomputing ratio measures and standard errors oftreatment effects. This problem is resolved by addingthe value 0.5 to each cell in the 2 × 2 table for that study[21]. We used the Mantel-Haenszel method to combinethe ORs for the outcomes of interest. For the continuousoutcome of KSS, we pooled data across studies by usingweighted mean differences (and 95% CIs). For thestudies in which the standard error for a mean differencein KSS was not reported, we calculated for the standarderror by converting the P value to a z score and solvingfor the standard error from the formula z = meandifference/standard error.All data were combined with the random effects model
because there was moderate evidence of heterogeneitybetween studies for the outcome of KSS [22]. Therandom effects model is a more conservative approachbecause it assumes that an effect may vary across studiesbecause of differences between studies [22].The analysis was carried out by using Comprehensive
Meta-analysis version 2.0 (Englewood, NJ).
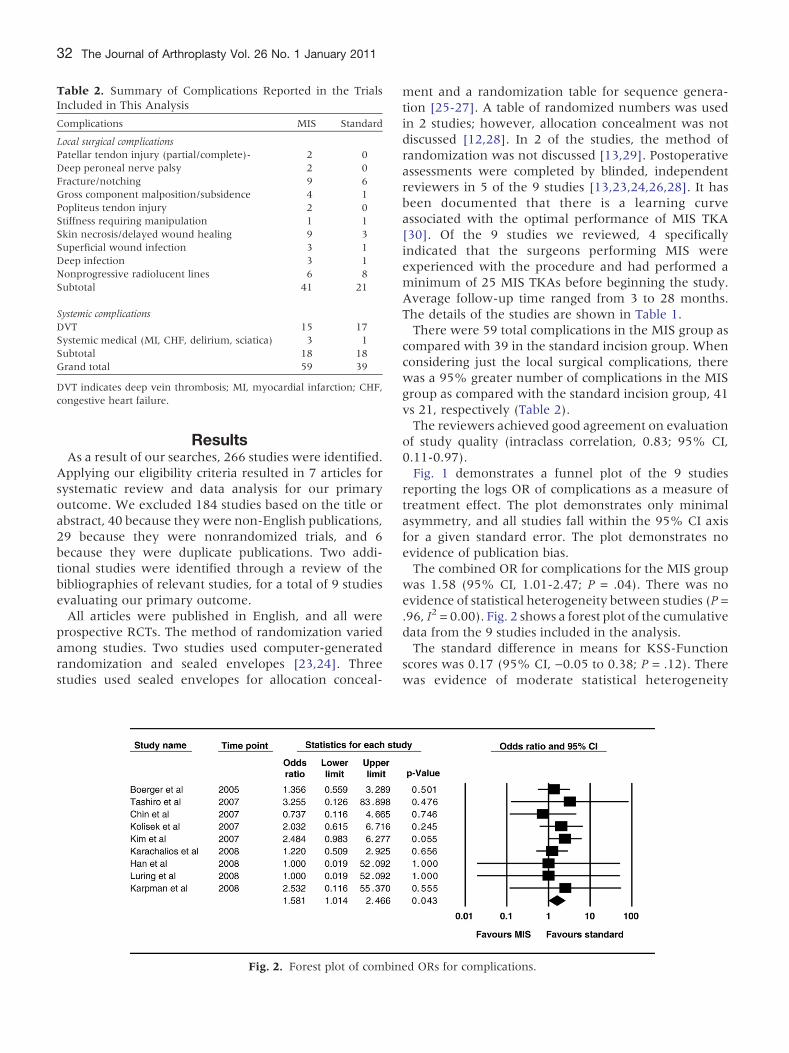
Table 2. Summary of Complications Reported in the TrialsIncluded in This Analysis
Complications MIS Standard
Local surgical complicationsPatellar tendon injury (partial/complete)- 2 0Deep peroneal nerve palsy 2 0Fracture/notching 9 6Gross component malposition/subsidence 4 1Popliteus tendon injury 2 0Stiffness requiring manipulation 1 1Skin necrosis/delayed wound healing 9 3Superficial wound infection 3 1Deep infection 3 1Nonprogressive radiolucent lines 6 8Subtotal 41 21
Systemic complicationsDVT 15 17Systemic medical (MI, CHF, delirium, sciatica) 3 1Subtotal 18 18Grand total 59 39
DVT indicates deep vein thrombosis; MI, myocardial infarction; CHF,congestive heart failure.
32 The Journal of Arthroplasty Vol. 26 No. 1 January 2011
ResultsAs a result of our searches, 266 studies were identified.
Applying our eligibility criteria resulted in 7 articles forsystematic review and data analysis for our primaryoutcome. We excluded 184 studies based on the title orabstract, 40 because they were non-English publications,29 because they were nonrandomized trials, and 6because they were duplicate publications. Two addi-tional studies were identified through a review of thebibliographies of relevant studies, for a total of 9 studiesevaluating our primary outcome.All articles were published in English, and all were
prospective RCTs. The method of randomization variedamong studies. Two studies used computer-generatedrandomization and sealed envelopes [23,24]. Threestudies used sealed envelopes for allocation conceal-
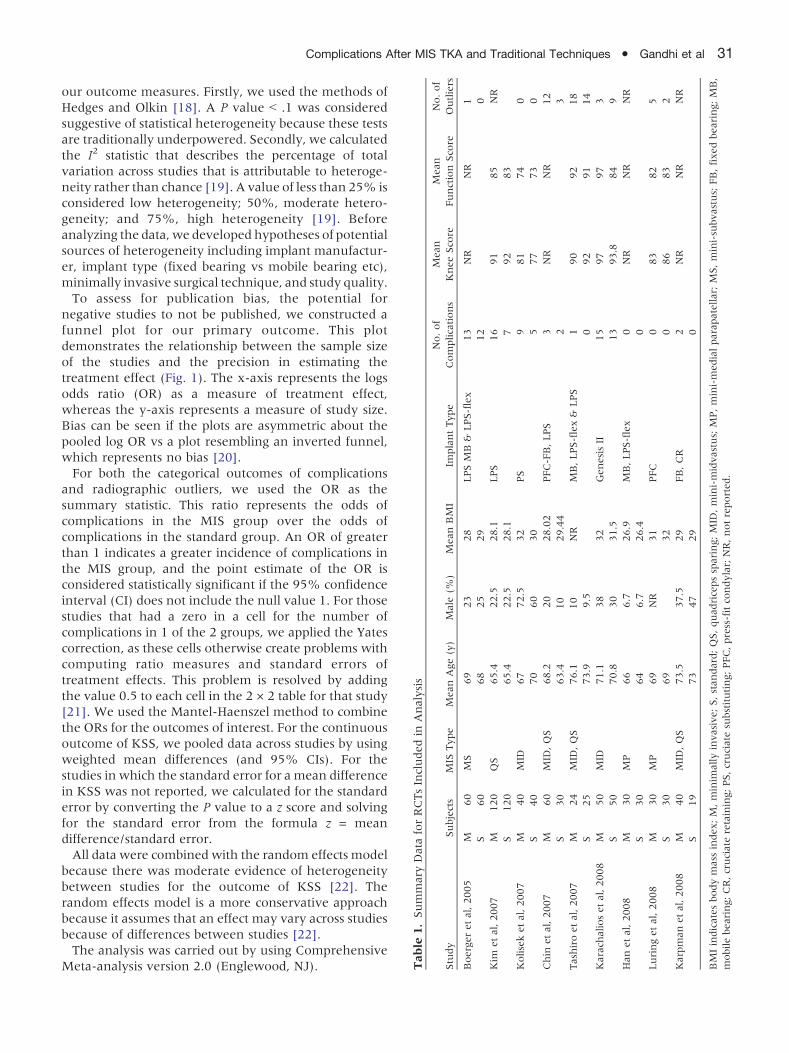
Fig. 2. Forest plot of combin
ment and a randomization table for sequence genera-tion [25-27]. A table of randomized numbers was usedin 2 studies; however, allocation concealment was notdiscussed [12,28]. In 2 of the studies, the method ofrandomization was not discussed [13,29]. Postoperativeassessments were completed by blinded, independentreviewers in 5 of the 9 studies [13,23,24,26,28]. It hasbeen documented that there is a learning curveassociated with the optimal performance of MIS TKA[30]. Of the 9 studies we reviewed, 4 specificallyindicated that the surgeons performing MIS wereexperienced with the procedure and had performed aminimum of 25 MIS TKAs before beginning the study.Average follow-up time ranged from 3 to 28 months.The details of the studies are shown in Table 1.There were 59 total complications in the MIS group as
compared with 39 in the standard incision group. Whenconsidering just the local surgical complications, therewas a 95% greater number of complications in the MISgroup as compared with the standard incision group, 41vs 21, respectively (Table 2).The reviewers achieved good agreement on evaluation
of study quality (intraclass correlation, 0.83; 95% CI,0.11-0.97).Fig. 1 demonstrates a funnel plot of the 9 studies
reporting the logs OR of complications as a measure oftreatment effect. The plot demonstrates only minimalasymmetry, and all studies fall within the 95% CI axisfor a given standard error. The plot demonstrates noevidence of publication bias.The combined OR for complications for the MIS group
was 1.58 (95% CI, 1.01-2.47; P = .04). There was noevidence of statistical heterogeneity between studies (P =.96, I2 = 0.00). Fig. 2 shows a forest plot of the cumulativedata from the 9 studies included in the analysis.The standard difference in means for KSS-Function
scores was 0.17 (95% CI, −0.05 to 0.38; P = .12). Therewas evidence of moderate statistical heterogeneity
ed ORs for complications.
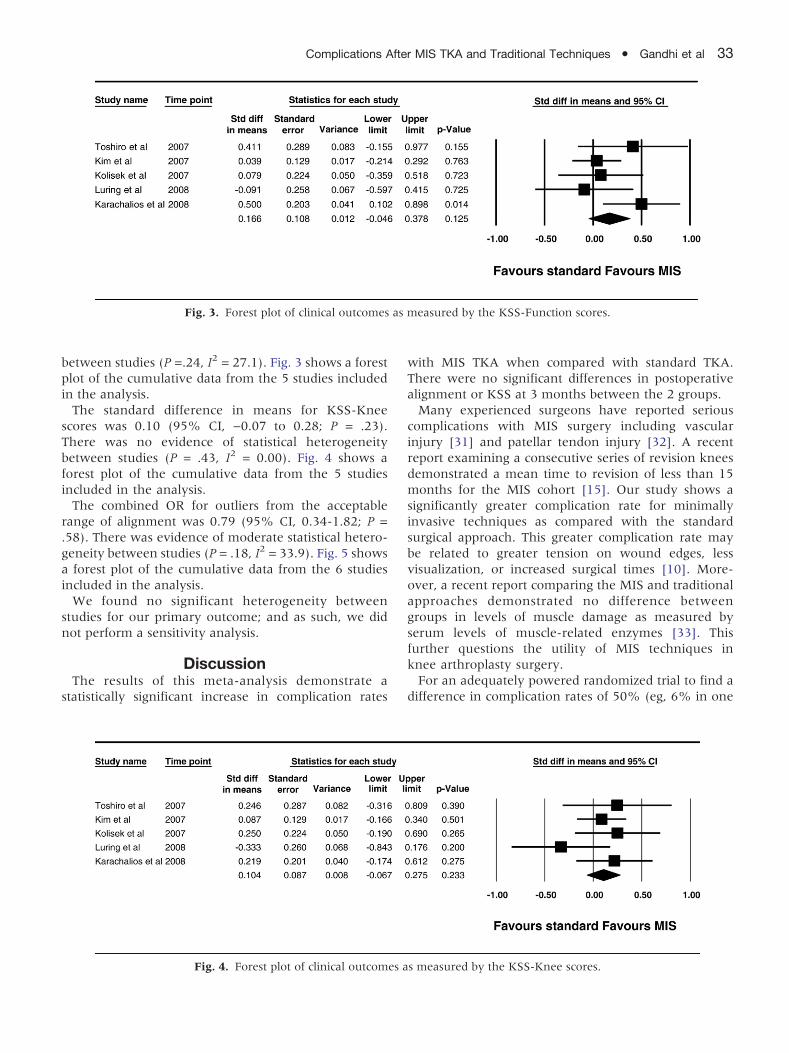
Fig. 3. Forest plot of clinical outcomes as measured by the KSS-Function scores.
Complications After MIS TKA and Traditional Techniques � Gandhi et al 33
between studies (P =.24, I2 = 27.1). Fig. 3 shows a forestplot of the cumulative data from the 5 studies includedin the analysis.The standard difference in means for KSS-Knee
scores was 0.10 (95% CI, −0.07 to 0.28; P = .23).There was no evidence of statistical heterogeneitybetween studies (P = .43, I2 = 0.00). Fig. 4 shows aforest plot of the cumulative data from the 5 studiesincluded in the analysis.The combined OR for outliers from the acceptable
range of alignment was 0.79 (95% CI, 0.34-1.82; P =.58). There was evidence of moderate statistical hetero-geneity between studies (P = .18, I2 = 33.9). Fig. 5 showsa forest plot of the cumulative data from the 6 studiesincluded in the analysis.We found no significant heterogeneity between
studies for our primary outcome; and as such, we didnot perform a sensitivity analysis.
DiscussionThe results of this meta-analysis demonstrate a
statistically significant increase in complication rates
Fig. 4. Forest plot of clinical outcomes a
with MIS TKA when compared with standard TKA.There were no significant differences in postoperativealignment or KSS at 3 months between the 2 groups.Many experienced surgeons have reported serious
complications with MIS surgery including vascularinjury [31] and patellar tendon injury [32]. A recentreport examining a consecutive series of revision kneesdemonstrated a mean time to revision of less than 15months for the MIS cohort [15]. Our study shows asignificantly greater complication rate for minimallyinvasive techniques as compared with the standardsurgical approach. This greater complication rate maybe related to greater tension on wound edges, lessvisualization, or increased surgical times [10]. More-over, a recent report comparing the MIS and traditionalapproaches demonstrated no difference betweengroups in levels of muscle damage as measured byserum levels of muscle-related enzymes [33]. Thisfurther questions the utility of MIS techniques inknee arthroplasty surgery.For an adequately powered randomized trial to find a
difference in complication rates of 50% (eg, 6% in one
s measured by the KSS-Knee scores.
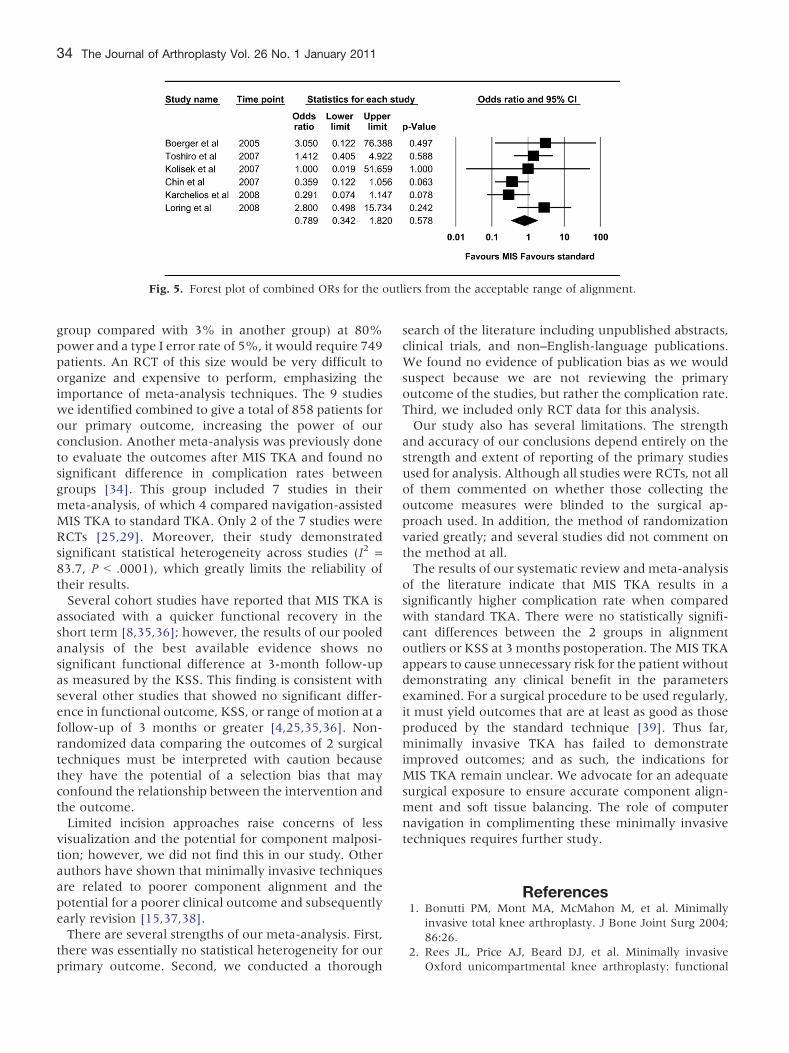
Fig. 5. Forest plot of combined ORs for the outliers from the acceptable range of alignment.
34 The Journal of Arthroplasty Vol. 26 No. 1 January 2011
group compared with 3% in another group) at 80%power and a type I error rate of 5%, it would require 749patients. An RCT of this size would be very difficult toorganize and expensive to perform, emphasizing theimportance of meta-analysis techniques. The 9 studieswe identified combined to give a total of 858 patients forour primary outcome, increasing the power of ourconclusion. Another meta-analysis was previously doneto evaluate the outcomes after MIS TKA and found nosignificant difference in complication rates betweengroups [34]. This group included 7 studies in theirmeta-analysis, of which 4 compared navigation-assistedMIS TKA to standard TKA. Only 2 of the 7 studies wereRCTs [25,29]. Moreover, their study demonstratedsignificant statistical heterogeneity across studies (I2 =83.7, P b .0001), which greatly limits the reliability oftheir results.Several cohort studies have reported that MIS TKA is
associated with a quicker functional recovery in theshort term [8,35,36]; however, the results of our pooledanalysis of the best available evidence shows nosignificant functional difference at 3-month follow-upas measured by the KSS. This finding is consistent withseveral other studies that showed no significant differ-ence in functional outcome, KSS, or range of motion at afollow-up of 3 months or greater [4,25,35,36]. Non-randomized data comparing the outcomes of 2 surgicaltechniques must be interpreted with caution becausethey have the potential of a selection bias that mayconfound the relationship between the intervention andthe outcome.Limited incision approaches raise concerns of less
visualization and the potential for component malposi-tion; however, we did not find this in our study. Otherauthors have shown that minimally invasive techniquesare related to poorer component alignment and thepotential for a poorer clinical outcome and subsequentlyearly revision [15,37,38].There are several strengths of our meta-analysis. First,
there was essentially no statistical heterogeneity for ourprimary outcome. Second, we conducted a thorough
search of the literature including unpublished abstracts,clinical trials, and non–English-language publications.We found no evidence of publication bias as we wouldsuspect because we are not reviewing the primaryoutcome of the studies, but rather the complication rate.Third, we included only RCT data for this analysis.Our study also has several limitations. The strength
and accuracy of our conclusions depend entirely on thestrength and extent of reporting of the primary studiesused for analysis. Although all studies were RCTs, not allof them commented on whether those collecting theoutcome measures were blinded to the surgical ap-proach used. In addition, the method of randomizationvaried greatly; and several studies did not comment onthe method at all.The results of our systematic review and meta-analysis
of the literature indicate that MIS TKA results in asignificantly higher complication rate when comparedwith standard TKA. There were no statistically signifi-cant differences between the 2 groups in alignmentoutliers or KSS at 3 months postoperation. The MIS TKAappears to cause unnecessary risk for the patient withoutdemonstrating any clinical benefit in the parametersexamined. For a surgical procedure to be used regularly,it must yield outcomes that are at least as good as thoseproduced by the standard technique [39]. Thus far,minimally invasive TKA has failed to demonstrateimproved outcomes; and as such, the indications forMIS TKA remain unclear. We advocate for an adequatesurgical exposure to ensure accurate component align-ment and soft tissue balancing. The role of computernavigation in complimenting these minimally invasivetechniques requires further study.
References1. Bonutti PM, Mont MA, McMahon M, et al. Minimally
invasive total knee arthroplasty. J Bone Joint Surg 2004;86:26.
2. Rees JL, Price AJ, Beard DJ, et al. Minimally invasiveOxford unicompartmental knee arthroplasty: functional
Complications After MIS TKA and Traditional Techniques � Gandhi et al 35
results at one year and the effect of surgical inexperience.Knee 2004;11:363.
3. Chauhan SK, Norris M, Bonutti P. MIS total kneearthroplasty: minimally invasive surgery or more infor-mation soon. Knee 2006;13:417.
4. Laskin RS, Beksac B, Phongjunakorn A, et al. Minimallyinvasive total knee replacement through a mini-midvastusincision: an outcome study. Clin Orthop Relat Res 2004;428:74.
5. Hoffman AA, Plaster RI, Murdock LE. Subvastus (south-ern) approach for primary total knee arthroplasty. ClinOrthop Relat Res 1991;269:70.
6. Tenholder M, Clarke HD, Scuderi GR. Minimal incisiontotal knee arthroplasty: the early clinical experience. ClinOrthop Relat Res 2005;440:67.
7. Laskin RS. Mini-incision: occasionally desirable, rarelynecessary in opposition. J Arthroplasty 2006;21:19.
8. Haas SB, Cook S, Beksac B. Minimally invasive total kneereplacement through a mini midvastus approach: acomparative study. Clin Orthop Relat Res 2004;428:68.
9. Schroer WC, Diesfeld PJ, Reedy ME, et al. Mini-subvastusapproach for total knee arthroplasty. J Arthroplasty 2008;23:19.
10. Tria AJ, Coon TM. Minimal incision total knee arthro-plasty: early experience. Clin Orthop Relat Res 2003;416:185.
11. Chen AF, Alan RK, Redziniak DE, et al. Quadricepssparing total knee replacement: the initial experience withresults at two to four years. J Bone Joint Surg [Br] 2006;88-B:48.
12. Han I, Seong SC, Lee S, et al. Simultaneous bilateral MIS-TKA results in faster functional recovery. Clin OrthopRelat Res 2008;466:1449.
13. Boerger TO, Aglietti P, Mondanelli N, et al. Mini-subvastusversus medial parapatellar approach in total knee arthro-plasty. Clin Orthop Relat Res 2005;440:82.
14. Dalury DF, Dennis DA. Mini-incision total knee arthro-plasty can increase the risk of component malalignment.Clin Orthop Relat Res 2005;440:77.
15. Barrack RL, Barnes CL, Burnett SJ, et al. Minimal incisionsurgery as a risk factor for early failure of total kneearthroplasty. J Arthroplasty 2009;24:489.
16. Detsky AS, Naylor CD, O’Rourke K, et al. Incorporatingvariations in the quality of individual randomized trialsinto meta-analysis. J Clin Epidemiol 1992;45:255.
17. Deeks MJ, Altman DG, Bradburn MJ. Statistical methodsfor examining heterogeneity and combining results fromseveral studies in meta-analysis. In: Egger M, Smith GD,Altman DG, editors. Systematic reviews in health care:meta-analysis in context. 2nd ed. BMJ 2001;285.
18. Hedges LV, Olkin I. Statistical methods for meta-analysis.Academic Press 1985;108.
19. Higgins JP, Thompson SG, Deeks JJ, et al. Measuringinconsistency in meta-analyses. BMJ 2003;327:557.
20. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629.
21. Aziz O, Rao C, Panesar SS, et al. Meta-analysis ofminimally invasive internal thoracic artery bypass versuspercutaneous revascularisation for isolated lesions of theleft anterior descending artery. BMJ 2007;334:617.
22. DerSimonian R, Laird N. Meta-analysis in clinical trials.Control Clin Trials 1986;7:177.
23. Karachalios T, Giotikas D, Roidis N, et al. Total kneereplacement performed with either a mini-midvastus or astandard approach: a prospective randomised clinical andradiological trial. J Bone Joint Surg [Br] 2008;90:584.
24. Karpman RR, Smith HL. Comparison of the early results ofminimally invasive vs standard approaches to total kneearthroplasty: a prospective, randomized study. J Arthro-plasty 2009;24:681.
25. Kolisek FR, Bonutti PM, Hozack WJ, et al. Clinicalexperience using a minimally invasive surgical approachfor total knee arthroplasty: early results of a prospectiverandomized study compared to a standard approach. JArthroplasty 2007;22:8.
26. Chin PL, Foo LS, Yang KY, et al. Randomized controlledtrial comparing the radiologic outcomes of conventionaland minimally invasive techniques for total knee arthro-plasty. J Arthroplasty 2007;22:800.
27. Luring C, Beckmann J, Haibock P, et al. Minimal invasiveand computer assisted total knee replacement comparedwith the conventional technique: a prospective, randomisedtrial. Knee Surg Sports Traumatol Arthrosc 2008;16:928.
28. Kim YH, Kim JS, Kim DY. Clinical outcome and rate ofcomplications after primary total knee replacement per-formed with quadriceps-sparing or standard arthrotomy. JBone Joint Surg [Br] 2007;89-B:467.
29. Tashiro Y, Miura H, Matsuda S, et al. Minimally invasiveversus standard approach in total knee arthroplasty. ClinOrthop Relat Res 2007;463:144.
30. King J, Stamper DL, Schaad DC, et al. Minimally invasivetotal knee arthroplasty compared with traditional total kneearthroplasty. Assessment of the learning curve and postop-erative recuperative period. JBone Joint Surg 2007;89:1497.
31. Tria AJ. Advancements in minimally invasive total kneearthroplasty. Orthopedics 2003;26:s859.
32. Aglietti P, Baldini A, Sensi L. Quadriceps-sparing versusmini-subvastus approach in total knee arthroplasty. ClinOrthop Relat Res 2006;452:106.
33. Niki Y, Mochizuki T, Momohara S, et al. Is minimallyinvasive surgery in total knee arthroplasty really mini-mally invasive surgery? J Arthroplasty 2009;24:499.
34. Vavken P, Gruber M, Dorotka R. Outcomes after mini-mally invasive total knee replacement—a meta-analysis. ZOrthop Unfallchir 2008;146:768.
35. McAllister CM, Stepanian JD. The impact of minimallyinvasive surgical techniques on early range of motion afterprimary total knee arthroplasty. J Arthroplasty 2008;23:10.
36. Huang HT, Su JY, Chang JK, et al. The early clinicaloutcome of minimally invasive quadriceps-sparing totalknee arthroplasty: report of a 2-year follow-up. JArthroplasty 2007;22:1007.
37. Dalury DF, Dennis DA. Mini-incision total knee arthro-plasty can increase risk of component malalignment. ClinOrthop Rel Res 2005;440:77.
38. Longstaff LM, Sloan K, Stamp N, et al. Good alignmentafter total knee arthroplasty leads to faster rehabilitationand better function. J Arthroplasty 2009;24:57.
39. Holt G, Wheelan K, Gregori A. The ethical implications ofrecent innovations in total knee arthroplasty. J Bone JointSurg 2006;88:226.


















