Complexities and Challenges in Gynaecological · PDF fileComplexities and Challenges in...
23
Complexities and Challenges in Gynaecological Ultrasonography Book 1 Editors Tan Wei Ching Lee Sook Ling Tan Lay Kok
Transcript of Complexities and Challenges in Gynaecological · PDF fileComplexities and Challenges in...
Complexities and Challenges in
Gynaecological Ultrasonography
Book 1
EditorsTan Wei ChingLee Sook Ling
Tan Lay Kok

Published by Red Cells SeriesAn imprint under SingHealth Academy, Singapore Health Services Pte Ltd31 Third Hospital Avenue, #03-03 Bowyer Block C, Singapore 168753
SingHealth Academy Publishing Team:Benny Chung, Alyssa Christudason, Sukhvinder Kaur, Grace Lim, Melissa Ooi, Quek Shin Yi
Copyright © 2011 Singapore Health Services Pte Ltd
All images by Singapore General Hospital.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. Request for permission should be addressed to The Publisher, c/o The Editorial Office, SingHealth Academy, 168 Jalan Bukit Merah, Tower 3 #06-07, Singapore 150168. Tel: (65) 6377-8649, fax: (65) 6377-4262. Email: [email protected].
The publisher makes no representation or warranties with respect to the contents of this book, and specifically disclaims any implied warranties or merchantability or fitness for any particular purpose, and shall in no event be liable for any loss of profit or any other commercial damage, including but not limited to special, incidental, consequential, or other damages.
National Library Board, Singapore Cataloguing-in-Publication DataComplexities and challenges in gynaecological ultrasonography. Book 1 /
editors, Tan Wei Ching, Lee Sook Ling, Tan Lay Kok.– Singapore : Red Cells Series, c2011.
p. cm.ISBN : 978-981-08-9870-0 (pbk.)
1. Generative organs, Female – Ultrasonic imaging – Singapore – Case studies.2. Ultrasonics in obstetrics – Singapore – Case studies.
I. Tan, Wei Ching. II. Lee, Sook Ling. III. Tan, Lay Kok, 1967–
RG107.5.U4618.047543 — dc22 OCN754581805

CoNtENtS
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Foreword . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Leiomyosarcoma Presenting as Post-menopausal Bleeding . . . . . . . . . . . . . . . . . . . . . . 10
Leiomyosarcoma with Multiple Metastases . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Primary Amenorrhea due to Vaginal Atresia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Spontaneous Uterine Rupture Secondary to Recurrent Haematometra from Cervical Stenosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
Dysgerminoma Mimicking the Appearance of Fibromyoma . . . . . . . . . . . . . . . . . . . . . 27
Early Ovarian Carcinoma with Non-specific Ultrasonographic Features . . . . . . . . . . . 31
Adnexal Masses: Pelvic Schwannoma Mimicking an Ovarian Tumour. . . . . . . . . . . . . 38
Adnexal Masses: Synchronous Ovarian and Appendiceal Tumour . . . . . . . . . . . . . . . . 43
Adnexal Masses: Appendiceal Tumours . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
Actinomycosiss Mimicking Pelvic Malignancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
Pelvic Lymphoma Mimicking Pelvic Malignancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Pelvi-abdominal Mass in a Patient Presenting with Pleural Effusion . . . . . . . . . . . . . . 61
Pleural Effusion and Mediastinal Lymphadenopathy Associated with a Pelvic Mass, Ascites and a Raised CA 125 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
Persistent Gestational Trophoblastic Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70
Invasive Hydatidiform Mole in a Perimenopausal Female . . . . . . . . . . . . . . . . . . . . . . . . 74
Caesarean Scar Pregnancy Following Failed Termination of Pregnancy . . . . . . . . . . . 79
Interstitial Ectopic Pregnancy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
Ruptured Cornual Ectopic Pregnancy Presenting as a Hypervascular Uterine Mass . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
Rudimentary Horn Pregnancy in the Early Second Trimester . . . . . . . . . . . . . . . . . . . . . 95
Rudimentary Horn Pregnancy in the First Trimester . . . . . . . . . . . . . . . . . . . . . . . . . . . . 102
Heterotopic Pregnancy Following Ovulation Induction with Gonadotropins . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 108
Abruptio Placenta Resulting in Couvelaire Uterus and Intra-uterine Death . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 113

ABBrEviAtioNS
3D Three-dimensionalßhCG Beta human chorionic gonadotropinμg/L Microgrammes per litreAFP Alpha feto-proteinCA 125 Cancer antigen 125CA 19-9 Cancer antigen 19-9CEA Carcinoembryonic antigen cm CentimetreCRL Crown rump lengthCRP C-reactive protein CSP Caesarean scar pregnancyCT Computed tomographyDIVC Disseminated intra-vascular coagulationEUA Examination under anaesthesiaFIGO International Federation of Gynecology and Obstetricsg Gramme(s)g/dl Grammes per decilitreGnRH Gonadotropin-releasing hormoneGTD Gestational trophoblastic diseaseGTN Gestation trophoblastic neoplasiaHELLP Haemolysis, elevated liver enzyme levels and low platelet countIUCD Intra-uterine contraceptive devicesIUGS Intra-uterine gestational sacIV Intra-venousLDH Lactate dehydrogenaseLMP Last menstrual periodLSCS Lower segment Caesarean sectionmm MillimetreMRI Magnetic resonance imagingNSAIDs Non-steroidal anti-inflammatory drugsOGD OesophagogastroduodenoscopyPAP Papanicolaou testTHBSO Total hysterectomy and bilateral salpingo-oophorectomyTOP Termination of pregnancyU/L Units per litreU/ml Units per millilitreWHO World Health Organisation
ForEworD
Ultrasound technology (transvaginal and transabdominal) has advanced dramatically and broadened the spectrum of diagnostic imaging in Obstetrics and Gynaecology, making it an important part of the diagnostic algorithm. For example, Colour Doppler ultrasound has enabled enhanced evaluation of gynaecological tumours, and changed the way Obstetrics and Gynaecology is practiced. However, there is a limit to what modern technology can achieve on its own. We still need skills, knowledge of application and interpretation, and clinical wisdom and judgement to allow accurate diagnoses to be made.
The cases in this book illustrate the challenges and complexities faced by the doctors working in the Department of Obstetrics and Gynaecology at the Singapore General Hospital. The authors have compiled 22 cases, highlighting the key aspects of their approach, and the complexities and difficulties faced. The case illustrations are presented in short, readable chapters with clearly articulated learning points on the application of ultrasound technology and clinical judgement in arriving at accurate diagnoses.
I share in the enthusiasm that the authors have shown in writing this book, and hope that readers will find it a useful reference when problems or challenges arise in their daily work in Obstetrics and Gynaecology. I look forward to the publication of future volumes featuring more challenging cases. It will certainly be an invaluable resource of knowledge and information not found in ordinary Obstetrics and Gynaecology textbooks.
Prof Ng Han SeongChairman, Medical Board
Singapore General Hospital

PrEFACE
Ultrasonography is an indispensable diagnostic tool in current obstetric and gynaecological clinical practice, so much so that it has been hailed as the gynaecologist’s stethoscope. There is no shortage of excellent textbooks and treatises on the subject. This book came about because of the numerous complex and challenging gynaecological cases managed in the Department of Obstetrics and Gynaecology, Singapore General Hospital (SGH).
Since 2006, the Department has held a monthly multi-disciplinary meeting, initiated by Professor Ho Tew Hong, involving clinicians and sonographers to present and discuss these cases. What started as a banal continuing educational tool soon led to the realisation that this meeting was a useful and powerful platform to review, audit and above all learn from these cases.
Trainees in particular enjoyed these sessions, and we decided that we should publish our series in a book which would benefit medical practitioners, nurses and sonographers who use ultrasonography on a daily basis. Our intention is not to attempt to replicate a textbook on ultrasound in obstetrics and gynaecology, but rather to create a readable and accessible book focusing on clinical pearls or vignettes gleaned from these meetings. We have selected 22 cases for inclusion in this book, beginning with uterine abnormalities, followed by ovarian pathologies and some ‘infamous mimics’ of adnexal and pelvic masses, finishing with cases on molar pregnancies and uncommon and unusual presentations of ectopic pregnancies. Most of these cases, if not already published, have been accepted for publication in view of their clinical relevance and educational value.
The format we have chosen is deliberately simple and consistent: each case is presented like a case report summarising the clinical presentation and findings, followed by a concise description of the scan images, concluding with the key learning point. Considerable effort has been put into collecting and producing high-quality images for these cases.

The reader can make use of this book in several ways. One would be to read it from cover to cover, correlating the clinical scenario to the scan findings for each case. A more novel method would be to study the scan images first and attempt to arrive at a diagnosis. Through this the reader will realise, like we have, that the use of ultrasound imaging in gynaecology goes well beyond simple picture recognition. An experienced gynaecologist will and should always correlate the scan findings and the clinical scenario, thereby facilitating logical targeted investigations and interventions to optimise patient care.
Whichever way the book is used, we suggest that it always be kept readily at hand — it will serve as a valuable aide-memoire, a reference for uncommon differentials and a reminder of the value of other imaging modalities and multi-disciplinary input when one encounters seemingly common symptoms that do not obey the usual rules. This is the first volume in what we hope to be a continuing and evolving series. We hope that clinicians, sonographers and all involved in the use of ultrasonography in women’s healthcare will find this book useful in their practice.
Dr tan wei ChingConsultant, Department of Obstetrics and Gynaecology
Lead Consultant, Pre-natal Diagnostic Centre and Early Pregnancy UnitSingapore General Hospital
Ms Lee Sook LingSenior Principal Imaging Technologist, Perinatal Centre
Singapore General Hospital
Dr tan Lay KokSenior Consultant, Department of Obstetrics and Gynaecology
Chief, Section of Maternal Foetal MedicineSingapore General Hospital

CoNtriBUtorS
Chua Hong Liang MBBS, MRCOG, FAMSSenior Consultant, Department of Obstetrics and GynaecologyChief, Section of UrogynaecologySingapore General Hospital
Devendra Kanagalingam MBBS, MRCOGSenior Consultant, Department of Obstetrics and GynaecologyLead Consultant, Labour WardSingapore General Hospital
Ho tew HongMBBS, MMed, FRCOG, FAMSSenior Consultant, Department of Obstetrics and GynaecologyClinical Professor Chief, Gynaecological OncologyKK Women’s and Children’s Hospital
Elisa KohMBBS, MRCOGAssociate Consultant, Department of Obstetrics and GynaecologySingapore General Hospital
Pang Yi Ping, CindyMBBS, MMed, MRCOGAssociate Consultant, Department of Obstetrics and GynaecologySingapore General Hospital
tan Eng LoyMBBS, MMed, MRCOGAssociate Consultant, Department of Obstetrics and GynaecologySingapore General Hospital
tan Hak KoonMBBS, MMed, FRCOG, FAMSHead and Senior Consultant, Department of Obstetrics and GynaecologyClinical Associate ProfessorSingapore General Hospital

tan Lay KokMBBS, MMed, FRCOG, FAMSSenior Consultant, Department of Obstetrics and GynaecologyChief, Section of Maternal Foetal MedicineSingapore General Hospital
tan Poh Kok MBBS, MRCOG Senior Consultant, Department of Obstetrics and GynaecologyLead Consultant, Minimally Invasive SurgerySingapore General Hospital
tay Sun KuieMBBS, MD, FRCOG, FAMS, M App LawSenior Consultant, Department of Obstetrics and GynaecologyClinical Associate ProfessorSingapore General Hospital
tan wei Ching MBBS, MRCOG, FAMSConsultant, Department of Obstetrics and GynaecologyLead Consultant, Pre-natal Diagnostic Centre and Early Pregnancy UnitSingapore General Hospital
Yong tze tein MBBS, MRCOG, FAMSSenior Consultant, Department of Obstetrics and GynaecologySingapore General Hospital
Yu Su LingMBBS, M Med, FRCOG, FAMSSenior Consultant, Department of Obstetrics and GynaecologyChief, Section of Reproductive Medicine and Gynaecology EndocrinologyDirector, Centre of Assisted Reproduction (CARE)Singapore General Hospital

31
early ovarian carcinoma with non-specific ultrasonographic featuresChua Hong Liang, MBBS, MRCOG, FAMS
introductionOvarian cancer is the most frequent cause of death from gynaecological malignancies because of our inability to detect early-stage disease. While ultrasonography is useful for detecting ovarian cancer in asymptomatic women, its usefulness for detecting early-stage epithelial ovarian cancer in women at increased risk is uncertain.
This chapter reports a case of early ovarian carcinoma with non-specific ultrasonographic features.
presentationA 40-year-old married and nulliparous woman presented to the outpatient clinic with a 1-month history of clear vaginal discharge associated with some vague lower abdominal discomfort. She reported no past medical history and normal menstrual cycles.
initial DiagnosisExamination of the breasts, abdomen and pelvis did not reveal any palpable masses. A 2cm endocervical polyp was found upon an examination of the pelvis. It was removed and found to be benign on histological examination.
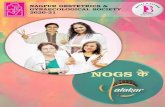
investigation and findingsA pelvic ultrasound showed a 2.5cm lobulated isoechoic mass in the anterior aspect of the right ovary adjacent to a 5 x 2 x 2cm dilated tube (Fig. 1, next page). The left ovary was not seen and a 3 x 2 x 3cm cyst containing two 1.3cm and 1.9cm mid-grey echogenic areas were noted in the left ovarian region (Fig. 2, page 33).

COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
32
Fig. 1: Pelvic ultrasound showing (left) a 2.5cm lobulated isoechoic mass in the anterior aspect of the right ovary, and (right) the 5 x 2 x 2cm dilated right tube
The vaginal discharge was symptomatically treated but did not improve 2 months later. A pelvic ultrasound was repeated and showed a 7 x 5 x 5cm solid mass with irregular contours in the right adnexa (Fig. 3, page 34) adjacent to a 6 x 2cm tubular cystic structure posteriorly, likely to be a hydrosalpinx (Fig. 4, page 34). This time the left ovary was seen and found to contain some fluid and solid areas (Fig. 5, page 34). The ultrasonographic impression was that it could be an endometriotic lesion. The CA 125 level was markedly raised at 2065U/ml.
treatmentThe patient underwent staging laparotomy (THBSO, omentectomy and right pelvic lymph node sampling). Intra-operatively, the right ovary was enlarged with a mixed solid cystic mass of 6cm, adherent to the right pelvic side wall (Fig. 6, page 35). There was a 3cm peritoneal tumour deposit with an enlarged right obturator node. Right hydrosalpinx was noted. The left ovary, uterus, omentum and the intestines were grossly normal.
progressThe patient recovered well post-operatively. Histological assessment confirmed poorly differentiated adenocarcinoma of both ovaries.
outcomeFollowing the surgery, the patient received 6 cycles of chemotherapy. She remained well and disease-free 2 years after the treatment.

33
EARLy OvARIAn CARCInOmA WITH nOn-SpECIFIC ULTRASOnOgRApHIC FEATURES
Fig. 2: Pelvic ultrasound showing (top image) a 3 x 2 x 3cm cyst and (middle image) two mid-grey echoes in the left adnexal region measuring 1.3cm and (bottom image) 1.9cm

COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
34
Fig. 4: Pelvic ultrasound showing a 6 x 2cm tubular cystic structure adjacent to the right ovary, likely to be a hydrosalpinx
Fig. 3: Pelvic ultrasound showing the 7 x 5 x 5cm solid mass with irregular contours in the right adnexa 2 months later
Fig. 5: Pelvic ultrasound showing some fluid and solid areas in the left ovary, likely to be endometriotic in origin

35
EARLy OvARIAn CARCInOmA WITH nOn-SpECIFIC ULTRASOnOgRApHIC FEATURES
Discussion The prognosis for most cases of epithelial ovarian cancer is poor due to delayed diagnosis. However, the prognosis can be favourable if the disease is detected early. Among some of the methods that have been evaluated to predict the risk of malignancy in suspicious ovarian masses are transvaginal ultrasonography and Colour Doppler assessment of blood flow.
Ultrasonomorphologic scoring systems have been developed to aid in the screening for ovarian cancer, with each ultrasonographic parameter of an ovarian tumour being assigned a numerical value. However, the positive predictive value of these scoring systems remains low because of the overlap in appearance of many benign ovarian lesions with malignant disease. In addition, some ovarian malignancies appear as simple cysts on ultrasound without exhibiting a complex morphology, as demonstrated in our case at initial presentation. The recommended cut-off size of uterine adnexal tumours beyond which surgery is likely to detect early cancer is also not well established.
Colour blood-flow imaging can be very helpful in detecting uterine adnexal malignancy because of the presence of neovascularisation in malignant
Fig. 6: Gross specimen of the uterus and right ovary which was enlarged with a mixed solid cystic mass of 6cm
COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
36
tumours. However, the accuracy of the technique is limited due to the significant number of false-positive results. When the presence of septum or papillary projections or solid components in uterine adnexal lesions is detected in greyscale ultrasonography, the presence of Doppler flow within these lesions increases the sensitivity and specificity of ultrasound evaluation of ovarian tumours. Unfortunately, there is no consensus as to which Doppler parameters and cutoff values are the most predictive of malignancy. moreover, vascularity within the papillary projection of a malignant tumour may go undetected when it is very small. Studies have shown considerable overlap of pulsatility index rates between benign and malignant uterine adnexal masses, suggesting that pulsed Doppler ultrasonography is not an independent indicator for malignancy.
Three-dimensional power Doppler ultrasound is increasingly used to evaluate features of tumour vascularity and while its positive predictive value awaits validation, it represents a novel approach for early and accurate detection of ovarian cancer in patients with suspicious findings on standard ultrasound scans.
Serum CA 125 levels have been used in conjunction with ultrasonography to minimise false-positive results although its role as a standalone screening tool remains limited. The combination of serum CA 125 levels and pelvic ultrasound scan seems to improve the sensitivity and specificity of predicting adnexal malignancies in post-menopausal women with an adnexal mass. This is in contrast to the results seen in pre-menopausal women. A positive predictive value of up to 40% can be achieved by combining CA 125 with transvaginal ultrasound results. However, these diagnostic tools appear to have greater sensitivity in detecting ovarian cancer at an advanced stage, as screening tests results remain normal in 3 out of 4 tumours with early-stage disease prior to the diagnosis.
conclusionIf early ovarian malignancy cannot be conclusively excluded, close surveillance of suspicious ovarian lesions with ultrasound together with CA 125 levels may more accurately identify those who will benefit from surgical intervention.
37
EARLy OvARIAn CARCInOmA WITH nOn-SpECIFIC ULTRASOnOgRApHIC FEATURES
learning pointDiagnostic ultrasound examination as an independent modality has limited value for the detection of early-stage epithelial ovarian cancer in asymptomatic women.
Bibliography1. Fishman DA, Cohen L, Blank Sv, Shulman L, Singh D, Bozorgi K, et al. The
role of ultrasound evaluation in the detection of early-stage epithelial ovarian cancer. Am J Obstet gynecol. 2005 Apr;192(4):1214–21; discussion 1221–2.
2. Olivier RI, Lubsen-Brandsma mA, verhoef S, van Beurden m. CA125 and transvaginal ultrasound monitoring in high-risk women cannot prevent the diagnosis of advanced ovarian cancer. gynecol Oncol. 2006 Jan;100(1):20–6.
3. Stirling D, Evans Dg, pichert g, Shenton A, Kirk En, Rimmer S, et al. Screening for familial ovarian cancer: failure of current protocols to detect ovarian cancer at an early stage according to the international Federation of gynecology and obstetrics system. J Clin Oncol. 2005 Aug 20;23(24):5588–96.
4. valentin L, Ameye L, Testa A, Lécuru F, Bernard Jp, paladini D, et al. Ultrasound characteristics of different types of adnexal malignancies. gynecol Oncol. 2006 Jul;102(1):41–8. Epub 2005 Dec 28.
5. varras m. Benefits and limitations of ultrasonographic evaluation of uterine adnexal lesions in early detection of ovarian cancer. Clin Exp Obstet gynecol. 2004;31(2):85–98.
95
RudimentaRy HoRn PRegnancy in tHe eaRly Second tRimeSteRHo Tew Hong, MBBS, MRCOG, FAMS
introductionA unicornuate uterus is a Müllerian anomaly that is caused by the failed development of one of the Müllerian ducts. Most unicornuate uteri have a rudimentary horn, which is non-communicating to the main uterine cavity and connected to the uterus only by fibrous bands. The rudimentary horn may consist of a functional endometrial cavity, or it may be a small solid lump of uterine muscle with no functional endometrium. Pregnancy can occur in the non-communicating rudimentary horn because of transperitoneal migration of sperm through the contralateral tube. Incidence of rudimentary horn pregnancy is reported by Nahum, as well as Urtal and Artal, to be 1 in 100,000 pregnancies or 1 in 5,000–15,000 ectopic pregnancies.
This chapter reports a case of pre-rupture diagnosis and management of rudimentary horn pregnancy in the early second trimester.
PresentationA 26-year-old woman at 15 weeks of her first pregnancy was referred for 2 weeks history of left iliac fossa pain.
initial diagnosisClinical examination confirmed a 15-week-sized mobile uterus.
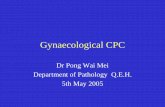
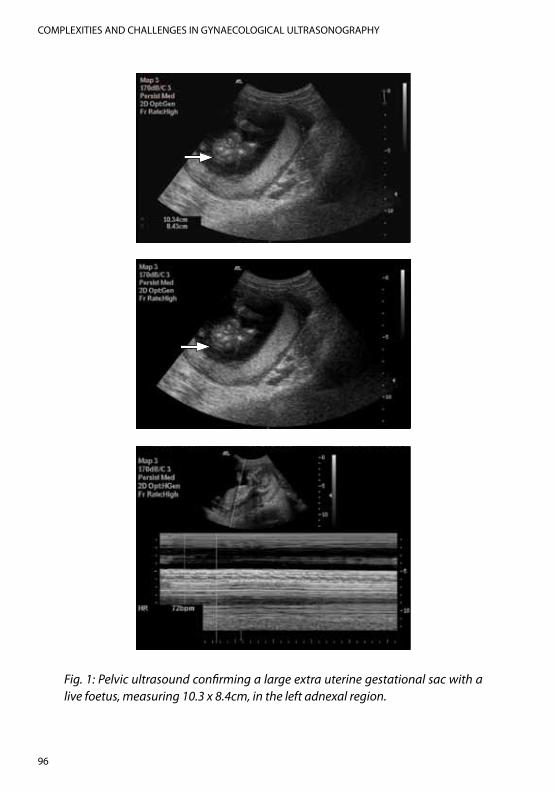
investigation and FindingsPelvic ultrasound confirmed a large extra uterine gestational sac with a live foetus, measuring 10.3 x 8.4cm, in the left adnexal region (Fig. 1, next page). This extrauterine pregnancy was located either in the interstitial part of the left Fallopian tube or in a rudimentary horn of a unicornuate uterus, as the configuration of the endometrial echo within the uterus appeared to be
COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
96
Fig. 1: Pelvic ultrasound confirming a large extra uterine gestational sac with a live foetus, measuring 10.3 x 8.4cm, in the left adnexal region.
97
RUdIMeNTARy HoRN PRegNANCy IN THe eARly SeCoNd TRIMeSTeR
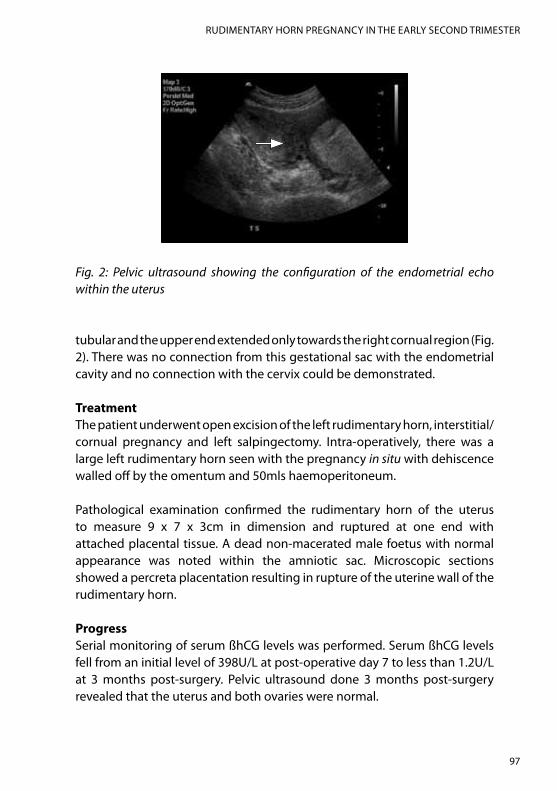
Fig. 2: Pelvic ultrasound showing the configuration of the endometrial echo within the uterus
tubular and the upper end extended only towards the right cornual region (Fig. 2). There was no connection from this gestational sac with the endometrial cavity and no connection with the cervix could be demonstrated.
treatmentThe patient underwent open excision of the left rudimentary horn, interstitial/cornual pregnancy and left salpingectomy. Intra-operatively, there was a large left rudimentary horn seen with the pregnancy in situ with dehiscence walled off by the omentum and 50mls haemoperitoneum.
Pathological examination confirmed the rudimentary horn of the uterus to measure 9 x 7 x 3cm in dimension and ruptured at one end with attached placental tissue. A dead non-macerated male foetus with normal appearance was noted within the amniotic sac. Microscopic sections showed a percreta placentation resulting in rupture of the uterine wall of the rudimentary horn.
ProgressSerial monitoring of serum ßhCg levels was performed. Serum ßhCg levels fell from an initial level of 398U/l at post-operative day 7 to less than 1.2U/l at 3 months post-surgery. Pelvic ultrasound done 3 months post-surgery revealed that the uterus and both ovaries were normal.

COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
98
outcomeThe patient was well at follow-up, with plans for yearly review.
discussion The usual outcome of rudimentary horn pregnancy is rupture in the second trimester in 70% of cases, resulting in life-threatening heavy bleeding. only in rare cases has foetal survival been reported. Pathologic placentation leading to placenta accreta further increases the risk of rupture.
In recent years, there have been increasing reports of pre-rupture diagnosis of rudimentary horn pregnancy made as early as the first trimester.
Studies have suggested several ultrasonographic diagnostic aids that may help in the diagnosis of a rudimentary horn pregnancy. The differential diagnoses of rudimentary horn pregnancy on ultrasonography include: tubal ectopic, cornual ectopic and pregnancy in a bicornuate uterus. distinguishing between these possibilities may be useful because of implications on management.
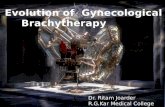
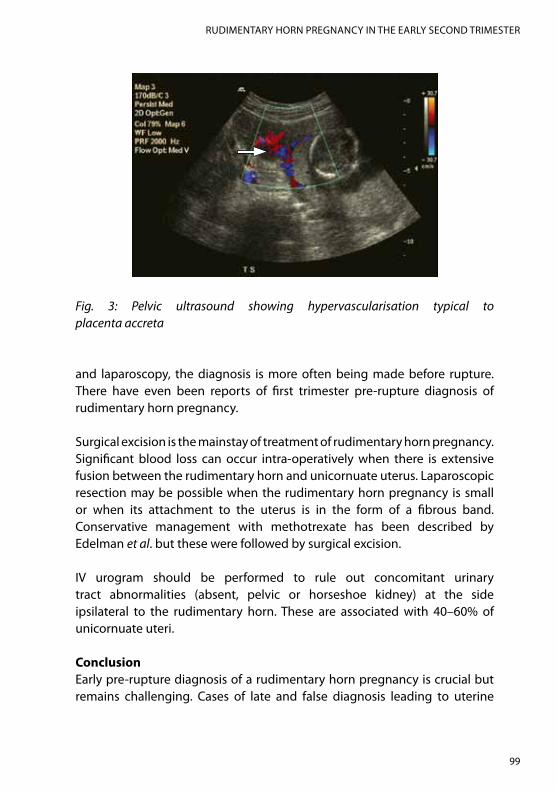
Tsafrir et al. suggested several criteria for ultrasonographic diagnosis of a rudimentary horn pregnancy: (1) pseudo-pattern of an asymmetrical bicornuate uterus: variation in thickness of the myometrium in 2 horns and a marked distance between them favour the diagnosis of a rudimentary horn pregnancy; (2) absent visual continuity between the cervical canal and the lumen of the pregnant horn: ultrasonography of pregnancy in a bicornuate uterus would usually demonstrate continuity between the endometrium lining the gestational sac and the other uterine horn; (3) presence of myometrial tissue surrounding the gestational sac: a tubal pregnancy will not show a ring of myometrium surrounding the gestational sac. Additionally, hypervascularisation typical to placenta accreta may support the diagnosis of rudimentary horn pregnancy (Fig. 3, next page).
other radiologic modalities such as CT scan and MRI have also been shown by ozeren et al. and lawhon et al. to be useful in confirming the diagnosis of rudimentary horn pregnancy. In the past, a majority of cases were diagnosed after rupture of the rudimentary horn. However, with the advent of investigative methods such as ultrasound scan, CT scan, MRI,
99
RUdIMeNTARy HoRN PRegNANCy IN THe eARly SeCoNd TRIMeSTeR
Fig. 3: Pelvic ultrasound showing hypervascularisation typical to placenta accreta
and laparoscopy, the diagnosis is more often being made before rupture. There have even been reports of first trimester pre-rupture diagnosis of rudimentary horn pregnancy.
Surgical excision is the mainstay of treatment of rudimentary horn pregnancy. Significant blood loss can occur intra-operatively when there is extensive fusion between the rudimentary horn and unicornuate uterus. laparoscopic resection may be possible when the rudimentary horn pregnancy is small or when its attachment to the uterus is in the form of a fibrous band. Conservative management with methotrexate has been described by edelman et al. but these were followed by surgical excision.
IV urogram should be performed to rule out concomitant urinary tract abnormalities (absent, pelvic or horseshoe kidney) at the side ipsilateral to the rudimentary horn. These are associated with 40–60% of unicornuate uteri.
conclusionearly pre-rupture diagnosis of a rudimentary horn pregnancy is crucial but remains challenging. Cases of late and false diagnosis leading to uterine

COMPLEXITIES AND CHALLENGES IN GYNAECOLOGICAL ULTRASONOGRAPHY
100
rupture have been reported repeatedly, with some diagnosed only after failed termination of an incorrectly diagnosed intra-uterine pregnancy. In the past, many cases were diagnosed only at laparotomy for acute abdomen in pregnancy.
Pelvic ultrasound remains the main diagnostic tool with other imaging modalities as important adjuncts.
learning PointRudimentary horn pregnancy is a gynaecological emergency which mandates immediate surgical treatment to prevent a potentially fatal rupture.
Bibliography1. Cash Rl, Rahmani R, Herer eR. First trimester screening aids in the diagnosis
and management of an ectopic pregnancy in a noncommunicating uterine horn. J Clinical Ultrasound. 2006 Nov–dec;34(9):446–9.
2. daskalakis g, Pilalis A, lykeridou K, Antsaklis A. Rupture of noncommunicating rudimentary uterine horn pregnancy. obstet gynecol. 2002 Nov;100(5 Pt 2):1108–10.
3. edelman AB, Jensen JT, lee dM, Nichols Md. Successful medical abortion of a pregnancy within a noncommunicating rudimentary uterine horn. Am J obstet gynecol. 2003 Sep;189(3):886–7.
4. grimbizis gF, Camus M, Tarlatzis BC, Bontis JN, devroey P. Clinical implications of uterine malformations and hysteroscopic treatment results. Hum Reprod Update. 2001 Mar–Apr;7(2):161–74.
5. Jerbi M, Trimech A, Choukou A, Hidar S, Bibi M, Chaieb A, et al. Rupture of rudimentary horn pregnancy at the 18th week of gestation: a case report. gynecol obstet Fertil. 2005 Jul–Aug;33(7–8):505–7.
6. Kriplani A, Relan S, Mittal S, Buckshee K. Pre-rupture diagnosis and management of rudimentary horn pregnancy in the first trimester. eur J obstet gynecol Reprod Biol. 1995 Feb;58(2):203–5.
7. lawhon BP, Wax JR, dufort RT. Rudimentary uterine horn pregnancy diagnosed with magnetic resonance imaging. obstet gynecol. 1998 May;91(5 Pt 2):869.
8. liatsikos SA, Tsikouras P, Souftas V, Ammari A, Prassopoulos P, Maroulis g, et al. diagnosis and laparoscopic management of a rudimentary uterine horn in a teenage girl, presenting with haematometra and severe
101
RUdIMeNTARy HoRN PRegNANCy IN THe eARly SeCoNd TRIMeSTeR
endometriosis: our experience and review of literature. Minim Invasive Ther Allied Technol. 2010 Aug;19(4):241–7.
9. Markham SM, Waterhouse TB. Structural anomalies of the reproductive tract. Curr opin obstet gynecol. 1992 dec;4(6):867–73.
10. Mavrelos d, Sawyer e, Helmy S, Holland TK, Ben-Nagi J, Jurkovic d. Ultrasound diagnosis of ectopic pregnancy in the non-communicating horn of a unicornuate uterus (cornual pregnancy). Ultrasound obstet gynecol. 2007 oct;30(5):765–70.
11. Nahum gg. Rudimentary uterine horn pregnancy. A case report on surviving twins delivered eight days apart. J Reprod Med. 1997 Aug;42(8):525–532.
12. oral B, güney M, ozsoy M, Sönal S. Placenta accreta associated with a ruptured pregnant rudimentary uterine horn. Case report and review of the literature. Arch gynecol obstet. 2001 May;265(2):100–2.
13. ozeren S, Caliskan e, Corakci A, ozkan S, demirci A. Magnetic resonance imaging and angiography for the prerupture diagnosis of rudimentary uterine horn pregnancy. Acta Radiol. 2004 dec;45(8):878–81.
14. Samuels TA, Awonuga A. Second-trimester rudimentary uterine horn pregnancy: rupture after labor induction with misoprostol. obstet gynecol. 2005 Nov;106(5 Pt 2):1160–2.
15. Taori K, Saha BK, Shah d, Khadaria N, Jadhav V, Jawale R. Sonographic diagnosis of uncomplicated first-trimester pregnancy in the rudimentary horn of a unicornuate uterus. J Clinical Ultrasound. 2008 Jan;36(1):45–7.
16. Tsafrir A, Rojansky N, Sela Hy, gomori JM, Nadjari M. Rudimentary horn pregnancy: first trimester pre-rupture sonographic diagnosis and confirmation by magnetic resonance imaging. J Ultrasound Med. 2005 Feb;24(2):219–23.
17. Ural SH, Artal R. Third-trimester rudimentary horn pregnancy. A case report. J Reprod Med. 1998 oct;43(10):919–921.
18. Zapardiel I, Alvarez P, Perez-Medina T, Bajo-Arenas JM. laparoscopic management of a cavitated noncommunicating rudimentary uterine horn of a unicornuate uterus: a case report. J Med Case Reports. 2010;4:215.