Complex Study Design - Richmond Pharmacology St… · Complex Study Design . ... • What are the...
25
Dr Ulrike Lorch MD FRCA FFPM Complex Study Design
Transcript of Complex Study Design - Richmond Pharmacology St… · Complex Study Design . ... • What are the...

Dr Ulrike Lorch MD FRCA FFPM
Complex Study Design

Complex Designs
• Adaptive study design• Fusion/Combined/‘Umbrella’ protocols

‘Umbrella’ ProtocolA number of conventional studies are contained in one single study protocol:
Single Ascending Dose Multiple Ascending Dose
Age/Gender comparisons
Intensive cardiacsafety assessments
Food Effect
Ethnic comparisons
Proof of ConceptPatient populationsDrug Drug Interactions
© Ulrike Lorch

One or more decision points are built into the trial design;
The subsequent conduct following that decision point depends on the data observed to that point
‘without undermining the validity and integrity of the trial’
‘Changes are made “by design”, and not on an ad-hoc basis; therefore, adaptation is a design feature aimed to enhance the trial, not a remedy for inadequate planning.’
Paul Gallo et al.: Adaptive Designs in Clinical Drug Development – An Executive Summary of the PhRMA Working Group. Journal of Biopharmaceutical Statistics, 16: 275-283, 2006 http://www.gemini-grp.com/Bayes/PhRMA.pdf
Adaptive study design

The adaptive study design toolkit
Objectives
Adaptive Features
Controls
2
1
3
Decision making based on results as they emerge
© Ulrike Lorch

• What are the benefits of using adaptive protocols?
• Do adaptive and ‘umbrella’ protocols save time?
Potential Benefits

BenefitsBy continuous learning and early decision making
By adjusting the study design taking into account data as it emerges
Research is directed towards
Meaningful assessmentsCollection of relevant data
Research is
SafeCost effectiveEthical

Rationalise and simplify
Additional PK samples
Limited analysis of samples taken
More ECG
Fewer dose levels
Add what is essentialTake away what is not necessary
Analyse data as and when needed
Longer in-house stay
©Dr Ulrike Lorch

Time savings
Saves significant time & cost
Savestime & cost
© Ulrike Lorch

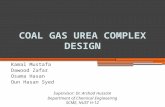
Total Actual Time Savings in 18 of 29 adaptive Studies* which saved time stratified by the type of adaptive features used:
Time Savings
10/14 umbrella studiesSaved on average 77 (21-140) days
8/15 non-umbrella studiesSaved on average 33 (7-63) days
*Lorch U, Berelowitz K, Ozen C, Naseem A, Akuffo E, Taubel J (2012) The practical application of adaptive study design in early phase clinical trials: a retrospective analysis of time savings. Eur. J. Clin. Pharmacol. 68:543–551.
2/14 umbrella studies delayed 21 days against planned schedule due to the need for
substantial amendments (i.e. lack of adaptability)
2/14 umbrella studies completed neutrallycompared to conventional non-adaptive (sequential)
design as adaptive design features were not used
© Ulrike Lorch

How can we write an adaptive study protocol that is sufficiently detailed, clear, systematic whilst allowing for flexibility and evolution?How can the layout facilitate ethical and regulatory review?

Simplicity

The adaptive study design toolkit
Objectives
Adaptive Features
Controls
2
1
3
Decision making based on results as they emerge
© Ulrike Lorch

A set of rules and decision trees rather than detail
Clinical Study Protocol
Study Progression Rules
Toxicity Rules
Adaptive Features Boundaries
Controls
1 23
© Ulrike Lorch

Adaptive Featuresand their Boundaries
Protocol Area Adaptive features Boundaries
Investigational Medicinal Product (IMP) / Dose
Dosing regimensIMP formulation/mode of administration
Starting doseMaximum exposureMaximum dose/exposure incrementsMaximum treatment frequency/duration
Timing / Scheduling OverlapSentinel/Sub-groups
Minimum data requirements for progressionReference to study specific toxicity rules
Study Participants Sample size (cohort size, No. of cohorts)Selection criteria
Minimum/maximum size and No. of cohortsNature, direction and extent of adaptability of selection criteria
Assessments Safety, PK, PD, exploratory samplesand assessments can be adjusted in nature, timing and extent
Minimum data requirements for progressionMaximum extent
Methods/Analysis Methods and or analysis may be optional
Nature, timing, extent and purpose of adaptabilityMinimum data requirements for progression
© Ulrike Lorch

Grade 1 Continue
Grade 2 Non-serious
Expected*
Reversible‡ Frequency†
Not reversible‡ Frequency†
Unexpected*
Reversible‡ Frequency†
Not reversible‡ Frequency†
Grade 3
Non-serious
Expected*
Reversible‡ Frequency† Study suspended
Not reversible‡ Frequency†
Unexpected*
Reversible‡ Frequency†
Not reversible‡ Frequency†
Serious Frequency†
Grade 4-5 Serious Study suspended
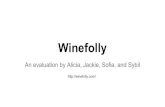
Control MechanismsToxicity Rules
Either one or a combination of the following:
1. Continue2. Explore dosing regimen further3. Suspend further
escalation/exploration4. Explore lower exposure dosing
regimen
Toxicity Study Progression
*As defined in the study protocol‡Within pre-determined observation period † Per system Organ Class© Ulrike Lorch

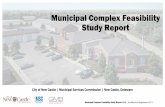
Control MechanismsStudy Progression Rules
= Progression to another study part
Single Dose 4Minimum PK/PD Minimum Safety
Single Dose 3Minimum PK/PD Minimum Safety
Single Dose 2Minimum PK/PD Minimum Safety
Single Dose 1Minimum PK/PD Minimum Safety
Multiple Dose 1Minimum PK/PD Minimum Safety
Patient Dose 1Minimum PK/PD Minimum Safety
Food Effect Dose
Ethnic Comparison Dose 1Minimum PK/PD Minimum Safety
Minimum PK/PD
Minimum Safety
Drug-Drug Interaction
= Exposure/Dose escalation
© Ulrike Lorch

In case of a combined protocol (i.e. the umbrella protocol), do we have to submit the results from the individual parts of the study before we are allowed to move forward to the next part?
How do we deal with adaptive changes? Do they need to be disseminated to REC/MHRA?
Do we need authorizations before proceeding?

*Medicines and Healthcare products Regulatory Agency (MHRA) / National Research Ethics Service (NRES), UK
© Ulrike Lorch

Clinical Study Protocol

Are adaptive studies as safe as non-adaptive studies?How can a REC assess potential risks and their minimization when reviewing an adaptive study?How can Informed Consent for adaptive studies be provided effectively, avoiding amendments?
Ethical Considerations
“Whatever the research context, the interests of participants come first. Their dignity, rights, safety and well-being must be the primary consideration in any research proposal, as well as in REC review. RECs must be assured that there are proportionate safeguards to protect people taking part in research”*
*Governance arrangements for research ethics Committees: a harmonised edition, 9 May 2011, updated April 2012, last accessed 21 July 2014 http://webarchive.nationalarchives.gov.uk/20130107105354/http://dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_133993.pdf,

REC Remit“Although RECs must be assured about the planned ethical conduct and anticipated risks and benefits of any proposed research, they are not responsible for enforcement if the research turns out to be unsafe or is not carried out as agreed. This responsibility rests with the relevant regulators or comparable bodies, as well as with the researchers’ employer and sponsor and with the care organisations where the research takes place […].”
“A REC need not reconsider the quality of the science, as this is the responsibility of the sponsor and will have been subject to review by one or more experts in the field (known as ‘peer review’). The REC will be satisfied with credible assurances that the research has an identified sponsor and that it takes account of appropriate scientific peer review.”
“A REC can expect to rely on established mechanisms for ensuring the proper conduct of the research at individual sites.”
“Where others have a regulatory responsibility, a REC can expect to rely on them to fulfil it. If the law gives another body duties that are normally responsibilities of a REC according to this document, RECs do not duplicate them. For example, the Medicines and Healthcare products Regulatory Agency has the primary legal responsibility for considering the safety of the research it regulates.”
Governance arrangements for research ethics Committees: a harmonised edition, 9 May 2011, updated April 2012, last accessed 21 July 2014 http://webarchive.nationalarchives.gov.uk/20130107105354/http://dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_133993.pdf,

Safety
Toxicity Rules
Adaptive Boundaries
Study Progression Rules
Flexibility to change if safety
requires
Collection of necessary data
only
Avoidance of unnecessary
exposure
ContinuousAssessment
© Ulrike Lorch

Informed Consent
– Divide Informed Consent for ‘umbrella’ studies into relevant distinct parts/forms
– Give headlines of what may change and the boundaries
– Avoid description of technical or scheduling details
– Describe maximum potential risks and inconveniences
© Ulrike Lorch

Thank you