
COMPLEX LIVES COMPLEX NEEDS COMPLEX SERVICE SYSTEMS Community worker
Upload
rexnayeeCategory
view
416download
1
Developing a Program to Address Complex Needs in
Older Adults2016 Governor’s Conference on Aging
Kyle R. Allen DO AGSF
VP Clinical Integration
Esther Desimini, RN, MSN, BC, APRN VP Riverside Tappahannock Hospital
Carol Wilson , MHA
Director of Advance Care Planning and Palliative Care Services
Riverside Health System

Takeaways
• Why an innovative model is needed
• Model implementation from a community perspective: Who, What, Where, How
• Keys for success
• Questions and Discussion

BackgroundKyle Allen, D.O.


“The most common chronic condition experienced by adults is multimorbidity, the coexistence of
multiple chronic diseases or conditions.”
Tinetti et al, JAMA, 2012

6
• Poor communication among primary providers, specialists, health and community providers, patients, and families
• Failure to catch problems early • Failure to address psychosocial issues • Lack of coordinated, longitudinal care
management • Ineffective transitional care management
• Insufficient management of multiple medications • Deviations from evidence-based care
Fragmented Care Has Driven High Costs and Resulted in Poor Outcomes
Source: Academy Health 2012

• 2011 RWJF survey of 1,000 primary care physicians
– 85%: Social needs directly contribute to poor health
– 4 out of 5 not confident can meet social needs, hurting their ability to quality care
– 85% of physicians say patients’ social needs are as important to address as their medical conditions
– 95% of physicians serving patients in low income, urban – 76% wish the health system would cover the costs associated with
connecting patients to services that met their social needs
– 1 in 7 prescriptions would be for social needs
– Psychosocial issues treated as physical concerns
Healthcare’s Blind Side

The Modern Death Ritual
• Half of older Americans visited ED in last month of life and 75% did so in their last 6 months of life.
• 70% of people wish to die at home
• Only about 25% reach this goal
• Hospice use is increasing but we are still challenged with length of time under Hospice care
Smith AK et al. Health Affairs 2012;31:1277-85.
8

Characteristics of Complex and Seriously Ill Patients
First, this population is not easily defined and is definitely not defined by prognosis.
▪Functional limitation ▪Dementia ▪Frailty ▪Serious illness(es)
➢Cancer, Severe Heart Conditions, etc. ▪Family and social support needs
9

Reframing Person-Centered Care
From “what is the matter with you”
To “what matters to you”

Eyes on the Top Users
10% of Beneficiaries 57% of Costs
Medicare FFS:

Determinants of Health and Their Contribudon to Premature Death
Health Care 10%
Environmental Exposure 5%
Social Circumstances 15%
Genedc Predisposidon 30%
Behavioral Paeerns 40%
Linkage Across Providers With Connection to Health System and Community Supports and Providers
Source: Schroeder, S. We Can Do Better. N Engl J Med 2007;357 12
• Engage primary care in discharge planning and placement
• Refer patients to system resources and programs
− Intentionally connect patients with appropriate medical homes or disease specific programs for long-term follow-through

Serious or complex illness
Functional impairment
Geriatric Care Palliative CareFoster Independence/control over life Increase quality of life Collaborative Care Model
Reduce suffering Improve quality of life Interdisciplinary Team model
Criteria is not necessarily related to age or diagnosis

Evidence Based Models
• GRACE – Geriatric Resources for Assessment an Care Of The Elderly Project
http://graceteamcare.indiana.edu/case-for-grace.html • Sutter Advanced Illness Management ( AIM) ® $13,000,000 CMS Health Care Innovation Award
http://www.sutterhealth.org/quality/focus/advanced-illness-management.html
• Guided Care http://www.guidedcare.org/
• Independence at Home (IAH) https://www.cms.gov/Medicare/Demonstration-Projects/DemoProjectsEvalRpts/Medicare-Demonstrations-Items/CMS1240082.html
14

Behavioral Health
AdultDay Care
Complex Care Clinic
Home Care, Private Duty & DME
Skilled Nursing Facility/ALF
Patient-Centered Health Care
Neighborhood Palliative Care Clinic/
Hospice
Telemedicine/ Telemonitoring
Geriatric Assessment & Consultation
Area Agencyon Aging & OtherCommunityAgencies
House Calls
A “Health Care Neighborhood” For Those with Advanced and Chronic Illness

Administrator’s PerspectiveEsther Muscari Desimini, RN, MSN, BC, APRN
16

Many reasons….
• Our Mission: Care for Those as You Would Care for Those You Love
• Multiple non-acute care settings in our network and region
• We are the main hospital w/many services in a rural like region
• Hospital and Nursing Home quality is exceptional, recognized nationally for the past three years
• Predominantly older population
• It’s the right thing to do
17

Tappahannock and Northern Neck Market Region
18

Riverside Primary Care
Riverside Callao Medical Arts
Riverside Warsaw Medical Arts
Tappahannock Family Practice,
Riverside White Stone Family Practice
Riverside King William Medical Center
Tappahannock Urgent Care

Demographic Overview
20
2013 Population: 63,234 Projected 5 Yr Growth Rate: 3.2% Median Age: 46.6 Median Household Income: $49,648 Per Capita Income: $25,980 Community Health Profile
■The whole market has MUA designation ■Uninsured Estimate of Non Elderly: 16%

Psychographic Overview
• 26% lower middle income African American multigenerational families living in small towns.
• 25% white, middle class families who embrace a rural life of fishing, hunting and family.
• 10% white, fixed income seniors- many retired veterans.
• 9% empty nesting couples & singles with disposable income often spent on travel and outdoor activities.
21

Identified Community Health Concerns
Primary Care
• COPD • Diabetes • Heart Disease & Stroke• Obesity• Mental Health • Substance Abuse
Cause of Death
• Cancer
22

Our Strengths & Challenges
Challenges
• Primarily Medicare Payer (59%)
• Minimal public transportation for services
• Non-existent growth in our community
• We are the largest employer in our region
• Financially healthy, but narrow margins
Strengths
• Low re-admission rates because of collaborations w/community groups & care navigation
• Experienced with comprehensive nurse navigation
• Bay Rivers Telehealth Alliance • Engaged, outstanding, largely
employed physician group
23

Riverside’s Process Carol Wilson, MHA
24

Program Design
• Consultants • Established goals • Conducted Community Needs Assessment
• Population Eligibility Criteria • Investigated evidence based models • Established Scope and Structure
• Assessed Financial Performance • Final Presentation
• Hand-off for Implementation
25

Riverside Leadership Team
• Acute, Outpatient, Home Health, Hospice, Case Management; Clinical and administrative
• High level of commitment
• Biweekly meetings
• Clear roles and authority
26

Adaptability
• Board Certified in Geriatrics and Palliative Care
• Launch of system-wide Care Management initiative
• Adjustments: • Expanded to include palliative care
• Changed patient criteria
• Added complexity to collaborative care delivery
27

28

Ambulatory Geriatric and Palliative Care Consultation • Short,
Moore
RTH Geriatric and Palliative Care Consultation • Desimin
i, Dudley
Orchard Geriatrics and Palliative Care Consultation • Doshier,
Im
Home Health Palliative Care; Hospice • Morgan
, Jims
PCMH Identification and referral • Sibley,
Dameron
House Calls
Northern Neck Steering Committee Desimini, Dudley, Short, Doshier, Boggs, Morgan, Sibley, Allen, Wilson, Russo, Hall,
Fletcher, Miller, Livengood, Williams, Im
Advanced Illness Management (ACP, PC) – Wilson, Cunnington, Im
Geriatrics – Allen, Im
Care Management, Care Transitions – Russo, Hall, Livengood
NICHE – Fletcher, Miller
IT/Telemedicine – Kipp, Hebert, Foss
Quality – Martin, Lim, Comer, Sheikh
Community – As You Wish, EVCTP, LTC Collaborative, CSB, Bay Aging, etc.
Short, Moore, Im
Complex Care Local Governance
Education – Garcia, Hence, Sutton, patient education
Pharmacy - Williams


Outcome MeasuresFinancial Measures
Financial Performance (Consults, staff, overhead)Savings/Efficiency (ED, Unwanted Tx)Downstream revenue (PCP, Hospice)Process MeasuresDocumented Advance Care PlansAcute utilizationEvidence of Advance Care PlanOutcome Measures30 day readmission rate
Mortality: Hospice daysPCP access/utilization
31
Patient Outcomes Quality of Life (SF8/12)
Patient Satisfaction Caregiver Satisfaction + bereaved families
Condition-specific outcomes ** Diabetes control
** Hypertension control **ACOVE indicators
Advance Directive ACP Discussion
Patient Goals identified Patient's goals -degree to which we have met
Where did people die
Resource Utilization
Other ways to capture "avoidance" dollars? ED utilization
30 day readmission rate Home Health Utilization
Hospice Utilization (admissions, LOS)* PCP utilization
Specialty Consult Utilization Palliative Consult Utilization
Hospitalizations in last 6 months of life* Hospital days in last 6 months of life*
Hospital days, terminal hospitalization* ICU admissions in last month of life*
ICU utilization in terminal hospital stay* Chemotherapy in last two weeks of life*
Operations
Number of patients enrolled
** Geriatric assessment ** Discharge clinic
** Palliative consultation (AIM) ** Housecalls
**Comanagement ALOS in the program for each service
Referrals to community resources
Use of decision support tools/risk assessments Documentation timeliness
Referring Physician trends Referring Physician satisfaction
Telemed Utilization Remote Monitoring Referrals from AIM
Assisted Living referrals from AIM DME referrals from AIM
Hospice Referals fromAIM HH Referrals from AIM
Financial Clinic financial performance vs. Budget
Housecalls financial performance vs. Budget Downstream Revenues:
Home health revenue generated and Cont Margin Hospice revenue generated and Cont Margin
Payor mix reports New to Riverside patients
Ancillary charge by practice providers
Challenges
• Leadership changes
• Breaking down silos
• Identifying patients • For referral • For outcome measures
• Developing metrics • Using current systems for health
care of the future
• Outreach • Finding simple language to
present an unfamiliar model
32
Keys to SuccessKyle Allen, D.O.
33

Clear Measures
• Pick 3 process
• Pick 3 financial
• Pick 3 outcomes
• For the person who can’t help themselves have 1 bonus metric
• Challenge of data sources and who is “Oz”

Measuring the Value
• The ROI might not be to a single cost center or entity
• The “investment” and “ return” will need to be measured for the whole region
• Reduce ED but increase PCP and Homecare
• Reduce risk for value based purchasing penalties e.g. Medicare Spend per Beneficiary
• Investing for model that might have value that can leverage into enhanced premium payments from MCO , e.g. Managed Long Term Services and Supports MA

CHANGE MANAGEMENT: WHAT EVERY HEALTHCARE LEADER NEEDS TO KNOW HOW TO DO
�36
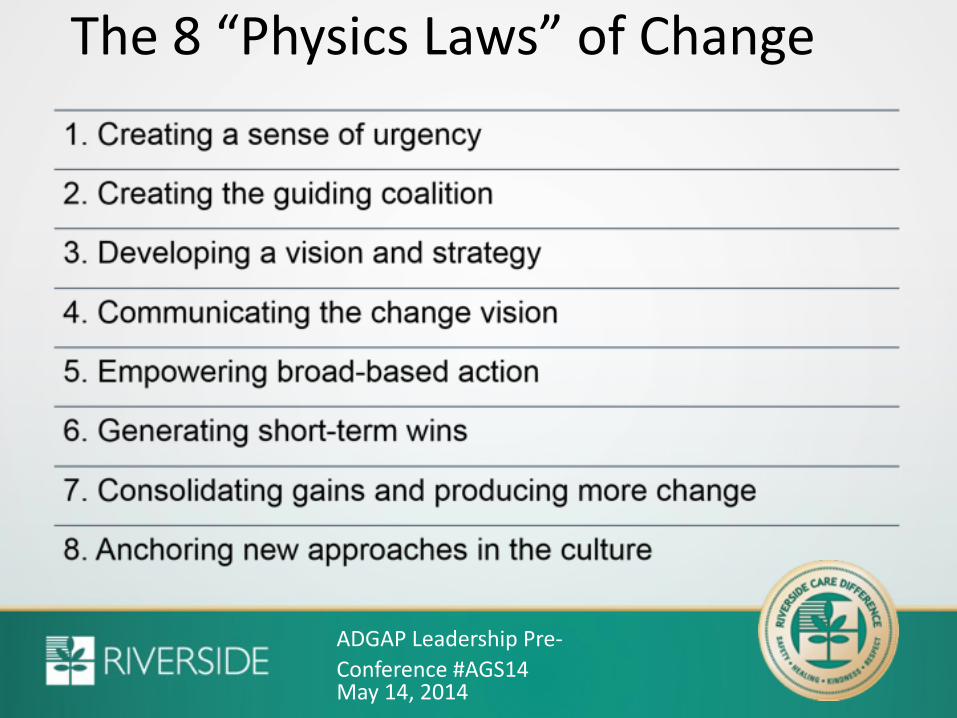
ADGAP Leadership Pre-Conference #AGS14
The 8 “Physics Laws” of Change
May 14, 2014

Share Victory, Share Defeat

Geriatric & Palliative Care Medicine Capability
Success in geriatric and palliative care medicine occurs when:
• Patients don’t get care they don’t want.
• Patients don’t get care which can’t benefit them.
• Patients suffer fewer adverse events.
• Patients experience fewer transitions.
• And cost of marginal care is reduced.

Changing Culture“If you are going to change something you’ve got to live on vision, before you live on reality. You have to be so inspired by the vision, that
you keep telling everybody until it gets in them, and they start living it with you.”
Father President Michael Scanlan, Franciscan University of Steubenville


















