
Competencies: an integrated career and competency ... · Competencies: an integrated career and...
20
Competencies: an integrated career and competency framework for information sharing in nursing practice RCN Competencies RCN Competencies
Transcript of Competencies: an integrated career and competency ... · Competencies: an integrated career and...

Competencies:an integrated career and
competency framework for information sharing in nursing practice
RCN CompetenciesRCN Competencies

Contributors
The competency framework was developed by MarinaCopping, Clinical Information Manager, NHS Lothian,on behalf of the Royal College of Nursing (RCN).
It was reviewed by a number of external experts andRCN members and staff.
Note: For ease of reading, ‘patients and/or clients’ arereferred to simply as ‘patients’ in this document.
RCN Legal Disclaimer
This publication contains information, advice and guidance to help members of the RCN. It is intended for use within the UK but readers areadvised that practices may vary in each country and outside the UK.
The information in this booklet has been compiled from professional sources, but its accuracy is not guaranteed. Whilst every effort has beenmade to ensure the RCN provides accurate and expert information and guidance, it is impossible to predict all the circumstances in which itmay be used. Accordingly, the RCN shall not be liable to any person or entity with respect to any loss or damage caused or alleged to be causeddirectly or indirectly by what is contained in or left out of this website information and guidance.
Published by the Royal College of Nursing, 20 Cavendish Square, London, W1G 0RN
© 2006 Royal College of Nursing. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmittedin any form or by any means electronic, mechanical, photocopying, recording or otherwise, without prior permission of the Publishers or alicence permitting restricted copying issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1T 4LP. This publicationmay not be lent, resold, hired out or otherwise disposed of by ways of trade in any form of binding or cover other than that in which it ispublished, without the prior consent of the Publishers.
R O Y A L C O L L E G E O F N U R S I N G
1
Competencies: an integrated career and competency frameworkfor information sharing in nursing practice
1. Introduction 2
– Purpose and scope 2
– Information sharing in context 2
– Legislation, policy and practice 3
2. Sources and related work 4
3. Overview of the framework 5
4. The RCN competency framework for information sharing in nursing practice 6
5. References 15
6. Other resources 16
Appendix 1: Abbreviations and useful definitions 17
Approved until November 2007
Contents

2
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
Introduction
Recent changes in Government policy on the exchange ofhealth information coincide with ongoing plans to makepatients’ health records more easily accessible, usingelectronic means. Easier access to health care data from asingle source shared by everyone could improve thequality and efficiency of care services, reduce the burdenof paperwork and even save lives.
Easy data access, however, also makes patients morevulnerable – which highlights the importance of highprofessional practice standards through a framework forgoverning clinical information. Nurses will easily relate tocore standards in this framework such as confidentiality,security and consent, but debate at a recent RCN congressshowed members’ concerns about nurses’ knowledge andskills in this complex area of practice.
This document has been produced in response to theseconcerns, with the twin aims of improving the profession’sunderstanding of this critical element of practice and ofsupporting action by nurses, managers, educators andothers to work towards improved competence ininformation sharing practice.
Purpose and scope ofthis framework
The development of the competency framework forinformation sharing in nursing practice is based on thefollowing position statement:
✦ to fulfil their professional responsibilities, nurses musthave the knowledge and skills to hold, obtain, share,use and store information about patients (informationmanagement)
✦ nurses must share information about patients withinlegal, professional and common law frameworks,placing the needs and preferences of the patient at thecentre of care
✦ nurses should be confident that patients fullyunderstand their rights and any implications ofinformation sharing, before asking a patient to consentto such sharing (and in most cases before asking themto provide sensitive information).
Information sharing competencies span all areas ofnursing practice and apply also to health care assistants,
nurse researchers and others who may have occasion toshare information about patients. Every effort has beenmade to ensure that the RCN framework is applicableacross all four countries of the UK – legislative andorganisational differences are noted where relevant.
The specific purposes of this competency framework areto:
✦ aid practitioners with professional development,helping them to identify gaps in competence andspecific training needs
✦ provide a basis for assessment of information sharingcompetence
✦ inform the commissioning, development and deliveryof education and training on information managementand information sharing
✦ contribute to developments related to Agenda forChange, Skills for Health and other initiatives, byproviding a professional nursing view of this coreclinical competence.
Information sharing in context
For the purpose of this framework, information sharing isdefined as: “the transfer of information about anindividual verbally, in writing, electronically, as images orvideo from one person/place to another.”
This definition applies to information about staff as well asabout patients, relatives and carers, but while theprinciples set out in the framework apply to all thesegroups, the primary focus here is on patients.
Information sharing is a part of information managementand is central to clinical communication, supporting theprovision of safe, effective and efficient services. It helpsensure continuity, saves time and avoids duplication. Suchbenefits, however, must be balanced against a person’sright to privacy.
In health and social care, most information about anindividual that in any way identifies them is defined assensitive in nature by the Data Protection Act 1998(Parliament, 2000). Before sharing such information, theremust be clear understanding and agreement about who issharing what information, for what specific purpose, andover what time period. The information itself needs to be
1

R O Y A L C O L L E G E O F N U R S I N G
3
complete, accurate and not excessive for the agreedpurpose. Crucially, in most instances, sharing ofinformation should only be done with the explicit consentof the patient.
Legislation, policy and practice
There is now increased focus on information andcommunications technology and on better management ofinformation in general. New legislation has been enactedin the UK similar to laws already in place across Europe,Canada, Australia and New Zealand. The Data ProtectionAct 1998, Human Rights Act 2000, Freedom of InformationAct 2002 and Children Act 2004 are driving changes inpractice and in organisational culture concerninginformation sharing.
New ways of working prompted by recent health policiessuch as patient choice, single assessment and Every ChildMatters (DfES, 2004) have introduced challenges fornursing practice as well as for organisations. Inter-agencyworking is a policy priority as is the breaking down ofbarriers between primary, community and secondaryhealth care. Person-centred care pathways are increasinglycited in service standards and frameworks as the best wayto deliver effective, equitable health care. As these changesare implemented they are further exposing the poorpractice in information sharing which was alreadyhighlighted in reports such as the Laming Inquiry (2002)into the death of Victoria Climbié in England and theKennedy Inquiry (2002) into the death of baby Caleb Nessin Scotland.
At practice level there is greater emphasis on integratedassessments, particularly in services for children and olderpeople. Alongside the development of common assessmentframeworks, protocols are being written to supportinformation sharing between professionals, often focusingon the specifics of the Data Protection Act 1998(Parliament, 2000). However, issues of information sharingin nursing go much wider than this Act. Nurses work withall patient groups including vulnerable adults, childrenand people with mental health problems; these groups arethe subject of additional legislation, knowledge of whichforms part of the competencies required for nursingpractice.
The rapid spread of information and communicationstechnology throughout the UK health sector is alsobringing information sharing issues to the fore. As localservices develop their systems, the interfaces required tosupport communication between providers and locationsbecome even more obvious, as do the challenges to beovercome.

Sources and related work
The RCN competency framework for information sharingin nursing practice is an extension of the RCN corecompetency framework (RCN, 2005) and is linked to theRCN Learning Zone development on information sharing,consent and confidentiality.
Clinical information sharing competencies are groundedmost often in statute, policy guidance and professionalcodes of practice and these are the main sources for thisframework. The framework is based on previous work onhealth information sharing, specifically the NHSInformation Authority project Learning to ManageInformation (NHSIA, 1999) and the NHS Knowledge andSkills Framework (KSF) (DH, 2004). It expands on these bygiving more detail of specific nursing and midwiferyknowledge and practice competency requirements atdifferent career levels.
Links to the competencies defined in the NHS KSF aremade explicit in the competency tables shown in thisdocument. Learning outcomes have been defined whereverpossible using the outcomes defined in the KSF. Whererelevant, references are made in the competency tables tothe appropriate level of KSF core competencies, KSFinformation and knowledge competences (IK) and KSFhealth and wellbeing competencies (HWB). Occasionalreference is made to the Learning to Manage HealthInformation (NHSIA, 1999) document (LTM).
4
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
2
Overview of theframework
Like other RCN competency frameworks, this one reflectsthe belief that cognitive, psychomotor and affectiveattributes define clinical competence for holistic nursingpractice. The framework has four levels (competency) andfourteen domains (activity areas).
Levels of competence
Levels of competence defined in the framework reflect thecareer structure for nursing defined in Making adifference: strengthening the nursing and midwifery andhealth visiting contribution to health and health care (DH,1999) and are cumulative – higher levels of practice buildon earlier competence. Empty cells in the tables indicateno higher (or lower) competency requirement.
Level 1: Health care support workersHealth care assistants (and other nursing support roles)are central to direct patient care. As the KSF makes clear,all members of the health care team must have corecompetencies in communication. Safe, effectivemanagement of information is also a base competency forstaff.
Level 2: Registered practitioner/competent nurse
The competencies specified at this level are the minimumrequired of all nurses and midwives on the Nursing andMidwifery Council (NMC) register. These competenciesare transferable to any setting and are required in all areasof general and specialist practice.
Level 3: Senior registeredpractitioner/experienced nurse
Level 4: Nurse consultant
Domains
1. Effective communication and informationexchange with children, patients, carers.
2. Shared meaning for inter-professionalcommunication.
3. Communication arrangements between differentprofessionals in a team and in related services.
4. Treating patient information with confidentiality,respecting the right to dignity, privacy andintegrity.
5. The role of the Caldicott Guardians in the NHS andtheir specific remit in relation to informationsharing.
6. Core principles of the Data Protection Act 1998.
7. Other relevant legislation – rights, children,vulnerable adults etc.
8. Consent.
9. Nursing codes of conduct and policy/protocols forsharing information.
10. Electronic and paper patient information.
11. Information sharing and record-keeping.
12. Inadvertent sharing and information securityprocesses.
13. Mandatory information sharing.
14. Secondary uses of clinical data and information.
R O Y A L C O L L E G E O F N U R S I N G
5
3

R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
4
The RCN competency framework forinformation sharing in nursing practice
1 Effective communication and information exchange with children, patients and carers KSF core dimension 1 – Communication
2. Shared meaning for interprofessional communication (source: LTM)KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 4 Core 1 – level 4 Core 1 – level 4
Checks on clarity of reception andtransmission, and interprets theclinical information duringinterprofessional exchanges
Reviews care for issues of sharedunderstanding
Reviews and develops work onshared definition of care processes
3. A11 Communication arrangements between different professionals in a team and in related services KSF core dimension 1 – Communication
Core 1- level 2 Core 1 – level 3 Core 1 – level 3 Core 1 – level 4
Relates to other members of theteam in a competent manner,demonstrating correct use ofinformation
Relates to other members of theteam and ensures clearcommunication within the team
Acts as a role model and motivatorfor others in interprofessional/interagency care
Facilitates the development of selfawareness in others in the teamthrough reflection
Reflects on own belief and how thiscould influence communication
Is aware of how issues of trust andrespect can affect teamcommunication
Uses reflective practice to exploreperceptions/value/trust of other care team providers,both within/outside the organisation
Facilitates learning opportunitiesfor staff to understand their roles
Able to send and receiveinformation effectively from otherprofessionals in written orelectronic formats within guidelinesof confidentiality and security
Able to send and receive informationeffectively from other professionalsin written or electronic formats
6
Core 1 – level 1 Core 1 – level 3 Core 1 – level 3 Core 1 – level 4
Demonstrates empathy,understanding, respect and honesty
Manages communication with carerand families
Monitors communicationprocesses in the care situation
Reviews and evaluatescommunication issues identified inteam, ward communication andthrough patients' complaints
Demonstrates active listening –check understanding
Coordinates communicationtraining plans
Demonstrates understanding ofnon-verbal communication
Promotes open, two-waycommunication in care processes
Anticipates barrier tocommunication and takes action toimprove communication
Demonstrates active listening

R O Y A L C O L L E G E O F N U R S I N G
7
5. A42 The role of Caldicott Guardians in the NHS and their specific remit in relation to information sharing KSF core dimension 1 – Communication
Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Can identify Caldicott Guardian andunderstand function
Initiates contact with DataProtection Officer /CaldicottGuardian concerning any newinformation flows
Use analytical skills to evaluatenew ways of working to reducerisks to privacy. Seeks CaldicottGuardian to sign off todevelopments
4. A34 Treating patient information with confidentially, respecting the right to privacy, dignity and integrity KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1- level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Understands that the patient has aright to dignity and respect and thatpatient information is ultimately'owned' by the patient
Demonstrates clear understandingof the ethics of care in teammanagement
Leads on ensuring all new staff,including nurses from overseas, aredeveloping a safe culture ofinformation sharing
Is aware of the importance of usingpatient information sources whichare validated by theorganisation/trust
Ensures patient has relevantinformation, presented by meansthat meet the patient's needs (e.g.verbal, written, own language),before seeking consent
Ensures patient information leafletsare available and that staff are awareof their obligation to distribute thesebefore they gain consent
Leads, researches and evaluatesdevelopment and deployment ofinformation resources to meetpatient needs
Demonstrates the importance ofcultural/educational/languageissues in gaining informed consent
Evaluates patient information forsuitability for the patient group
Provides information tools suitablefor individual patients' needs
Ensures staff are aware of differentcommunication strategies/toolsand of how to use tools which areappropriate to patient, eg. written,verbal, pictorial, appropriatelanguage
Is aware of diversity issues ingaining consent
Ensures that the needs of thosewith disabilities e.g. visual, hearingor intellectual impairment, are metin gaining consent
Demonstrates knowledge of suite oftools which can help gain informedconsent
Ensures posters etc are displayedto raise awareness ofconfidentiality rights

8
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
6. A44 Core principles of Data Protection Act (DPA) 1998 KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1- level 1 Core 1 – level 1 Core 1 – level 1 Core 1 – level 1
Demonstrates good knowledge ofthe core principles of the DataProtection Act 1998
Has knowledge of informationsecurity policy
Manages risk assessment ofcurrent processes andrecommends and delivers change
Demonstrates knowledge andunderstanding of the role of DataProtection principles in maintainingpatient confidentiality. (Knowledgegained at staff induction.)
Understands legal responsibility oforganisation to ensure that allpatient information managementcomplies with the Data ProtectionAct 1998
Reviews and ensures that staff areaware of duty of confidence asdefined in all staff contracts.Ensures that staff are aware ofdisciplinary procedure in relation toconfidentiality before they signemployment contracts
Understands the constituent partsof confidential and sensitive data
Demonstrates practicalmanagement of the Data ProtectionAct 1998 and defined sensitiveinformation (most NHS data fallswithin this category)
Demonstrates consideration forclarifying purpose of sharing
Demonstrates consideration forclarifying purpose of sharing
Demonstrates consideration forclarifying purpose of sharing
Demonstrates understanding of theimportance of sharing whenappropriate
Demonstrates awareness ofproportionality: information beingshared is proportionate to the need.(Assessed as part of the DataProtection Act 1998 training.)
Demonstrates knowledge of legalconstituent parts of care record e.g.paper notes, images, video clips,electronic records, test results etc
Demonstrates understanding ofdata ownership

R O Y A L C O L L E G E O F N U R S I N G
9
7. A57 Other key legislation – rights, children, vulnerable adults etc KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Demonstrates clear understandingof the link between care and theHuman Rights Act (1998)
Demonstrates clear understandingof the link between care and theHuman Rights Act (1998)
Demonstrates understanding thatthe Children's Act (1989), care ofvulnerable adults, and crime anddisorder legislation differ across theUK
Demonstrates understanding thatthe Children's Act (1989), care ofvulnerable adults, and crime anddisorder legislation differ across theUK
Demonstrates understanding ofrelevant Children's Act in the four UKcountries
Demonstrates understanding ofrelevant Children's Act in the fourUK countries
Demonstrates understanding of Ageof Legal Capacity Act (Scotland)(1991)
Demonstrates understanding ofAge of Legal Capacity Act (Scotland)(1991)
Demonstrates understanding oflegislation related to vulnerableadults
Understands the key principles ofthe Freedom of Information Act(2002)
Understands process flow whenpresented with a freedom ofinformation request
Monitors and manages freedom ofinformation requests to ensure 20day compliance with request
Understand the rights of the unbornchild
Understand what information can beshared about the deceased (HealthRecords Act 1990)
Understands the need to act withsupervision when dealing withpatient information
Understand the legal basis forsharing /obtaining information

10
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
8. Consent KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Demonstrates clear understandingof what constitutes consent
Co-ordinates delivery of informationsharing guidance
Monitors and evaluates currentpractice
Demonstrates understanding of thetypes of consent
Identifies and agrees partnershipswith others
Demonstrates understanding of howlong consent lasts for
Can describe communicationprocess regarding trained staffgaining informed consent
Understands need for consent andrefers on when consent notable/chosen to be given
Demonstrates understanding andimportance of gaining consent, andunderstanding of implicit/explicitconsent issues
Demonstrates clear understandingof the need to obtain patients'consent prior to sharing information
Understands the legal requirementto record patients' views aboutconsent
Understands who can give consentfor sharing for a patient
Understands consent rights ofchildren
Understands who can give consentfor sharing on behalf of a child
Understands the importance andrecording of who has parentalresponsibility for the child
Understands who can give consenton behalf of a vulnerable adult
Provides patients with informationabout consent to share theirinformation
Is able to understand the conceptand practice of informed consent
Is able to carry out 'informedconsent ' with patient
Communicates effectively withpatient and carers, ensuring clarityof transmission of information

R O Y A L C O L L E G E O F N U R S I N G
11
9. Nursing Codes of Conduct and policy/protocols for sharing patient information KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Can describe types of patientinformation which is covered by theData Protection Act 1998
Demonstrates a clear understandingof the NMC Guidelines on RecordKeeping 2004
Clearly understands reportingstructure if they feel thatconfidentiality is/has beenbreached
Demonstrates a clear understandingof NMC Code of Conduct 2004
Manages process when there areallegations/incidence ofconfidentiality breaches
Influences policy guidelines ondealing with breaches of securityand confidentiality
Uses tools provided withinstandards set
Follows NMC and local policies incare setting
Reviews quality standards foreffectiveness
Evaluates current practice anddefines improvement plans
Understands and applies theprinciples of effective quality controland validation of information onown practice
10. Electronic and paper patient information KSF core dimension 1 – Communication
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Describes electronic information aspart of care records
Follows NMC guidelines and regardselectronic information as having thesame legal standing as patientpaper record
11. Information sharing and record keeping KSF core dimension 1 – Communication
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Uses the NMC Guidelines on RecordKeeping (2004) in managing records
Develops record managementpractice guidelines
Maintains accurate, complete andtimely records
Audits and evaluates records tosupport multidisciplinary care
Understands the needs under theData Protection Act 1998 for recordsto be complete, accurate and timely
12
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
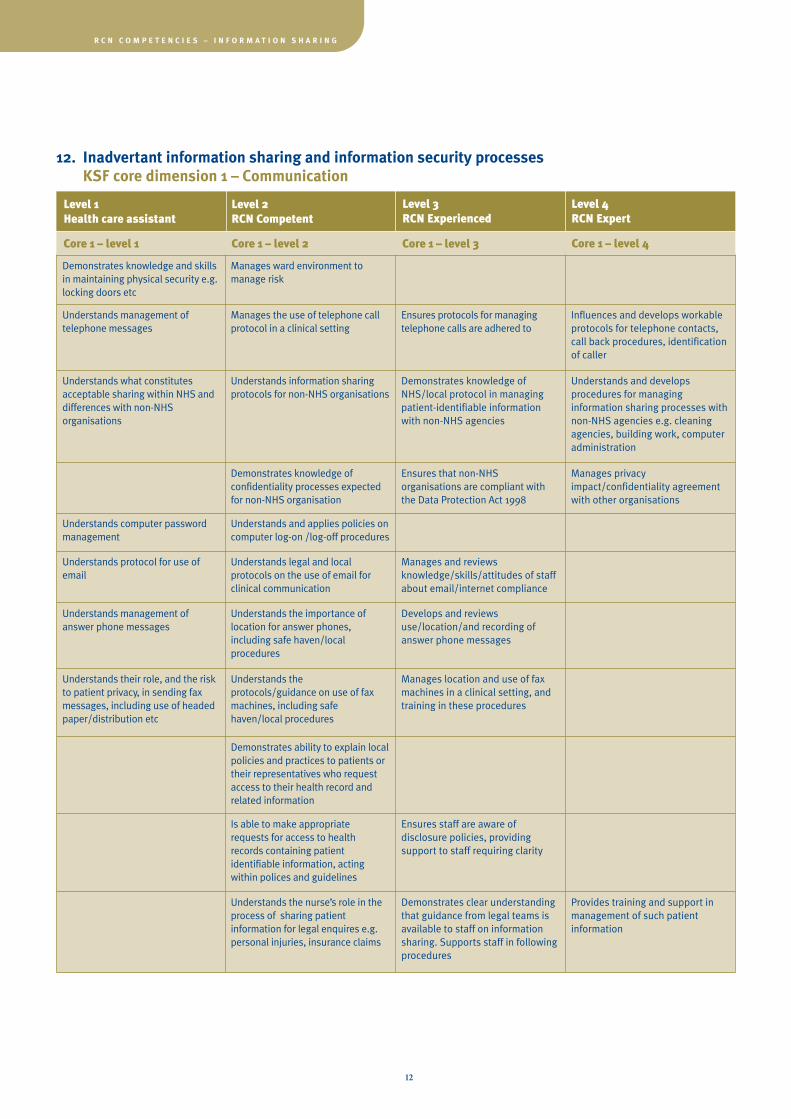
12. Inadvertant information sharing and information security processes KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Demonstrates knowledge and skillsin maintaining physical security e.g.locking doors etc
Manages ward environment tomanage risk
Understands management oftelephone messages
Manages the use of telephone callprotocol in a clinical setting
Ensures protocols for managingtelephone calls are adhered to
Influences and develops workableprotocols for telephone contacts,call back procedures, identificationof caller
Understands what constitutesacceptable sharing within NHS anddifferences with non-NHSorganisations
Understands information sharingprotocols for non-NHS organisations
Demonstrates knowledge ofNHS/local protocol in managingpatient-identifiable informationwith non-NHS agencies
Understands and developsprocedures for managinginformation sharing processes withnon-NHS agencies e.g. cleaningagencies, building work, computeradministration
Demonstrates knowledge ofconfidentiality processes expectedfor non-NHS organisation
Ensures that non-NHSorganisations are compliant withthe Data Protection Act 1998
Manages privacyimpact/confidentiality agreementwith other organisations
Understands computer passwordmanagement
Understands and applies policies oncomputer log-on /log-off procedures
Understands protocol for use ofemail
Understands legal and localprotocols on the use of email forclinical communication
Manages and reviewsknowledge/skills/attitudes of staffabout email/internet compliance
Understands management ofanswer phone messages
Understands the importance oflocation for answer phones,including safe haven/localprocedures
Develops and reviewsuse/location/and recording ofanswer phone messages
Understands their role, and the riskto patient privacy, in sending faxmessages, including use of headedpaper/distribution etc
Understands theprotocols/guidance on use of faxmachines, including safehaven/local procedures
Manages location and use of faxmachines in a clinical setting, andtraining in these procedures
Demonstrates ability to explain localpolicies and practices to patients ortheir representatives who requestaccess to their health record andrelated information
Is able to make appropriaterequests for access to healthrecords containing patientidentifiable information, actingwithin polices and guidelines
Ensures staff are aware ofdisclosure policies, providingsupport to staff requiring clarity
Understands the nurse’s role in theprocess of sharing patientinformation for legal enquires e.g.personal injuries, insurance claims
Demonstrates clear understandingthat guidance from legal teams isavailable to staff on informationsharing. Supports staff in followingprocedures
Provides training and support inmanagement of such patientinformation

R O Y A L C O L L E G E O F N U R S I N G
13
13. Mandatory information sharing KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Demonstrates understanding ofdisclosure policy
Demonstrates knowledge andunderstanding of when informationshould be released e.g.prevention/detection of crime
Manages release of patientinformation as part of theprevention and detection of crime
Demonstrates understanding ofprocess for sharing in issues of childprotection
Manages child protection process ina shift work area
Reviews child protection guidanceissued to staff
Is able to access local childprotection protocol
Initiates in child protectioninvestigations
Involved in child protectioninvestigations
Understands that child protectionprotocols provide a local and not anational or UK-wide process
Supports colleagues in childprotection investigation
Ensures child protection guidelinesare available and known to staff
Knows they should contact linemanager with child protectionconcerns
Participates in child protectionprocess
Demonstrates knowledge andunderstanding about wheninformation should be released aspart of a court order
Manages release of patientinformation as part of a court order
Demonstrates knowledge andunderstanding about wheninformation should be released dueto significant public interest (e.g.prevention of serious crime)
Manages process of disclosurewith Caldicott Guardian
Demonstrates awareness ofnotifiable disease process
Demonstrates knowledge andunderstanding about wheninformation should be released forprotection of the public fromserious disease (excluding HIV)
Manages notification withorganisation's medical director
Demonstrates knowledge of nurses'actions in relation to child protection
Manages requests for informationfor prevention or detection ofcrime, under the Data ProtectionAct 1998 or crime and disorderlegislation
Ensures polices are in place tomanage the sharing out ofinformation where consent to usedata has been given
Knows that information must beshared for the purpose of protectionagainst crime and disorder orprotection of state and country

14
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
14. Secondary use of clinical data and information KSF core dimension 1 – Communication
Level 1 Health care assistant
Level 2RCN Competent
Level 3RCN Experienced
Level 4RCN Expert
Core 1 – level 1 Core 1 – level 2 Core 1 – level 3 Core 1 – level 4
Understands the difference betweenaudit and research
Understands the issues of sharingpatient identifiable data in researchand audit – and patients' right torefuse
Understand the issues of sharingpatient identifiable information foreducation, publication andpresentation
Understands the range, purposes,benefits and potential hazards ofaggregating clinical data
Understands the need to obtainpatient consent for use of data inresearch
Understands the NHS guidance onconsent for using anonymisedpatient data
Clearly defines anonymised data
Can identify risks inpseudoanonymisation
Understands the need for CentralOffice for Research EthicsCommittees (COREC) approval forNHS research

R O Y A L C O L L E G E O F N U R S I N G
15
Department for Education and Skills (2004) Every childmatters: change for children. Available from:www.everychildmatters.gov.uk/ (accessed 16.06.05)(Internet)
Department of Health, Questions and answers on theHuman Rights Act 1998, London: DH. Available from:www.dh.gov.uk (accessed 31 July 2006). (Internet)
Department of Health (1999) Making a difference:strengthening the nursing, midwifery and health visitingcontribution to health and health care, London: DH.Available from: www.dh.gov.uk (accessed 31 July 2006)(Internet).
Department of Health (2003) Confidentiality: NHS Code ofPractice, London: DH. Available from: www.dh.gov.uk(accessed 31 July 2006) (Internet).
Department of Health (2004) The NHS Knowledge andSkills Framework (NHS KSF) and the development reviewprocess, London: DH. Available from: www.dh.gov.uk(accessed 31 July 2005) (Internet).
Edinburgh and Lothians Child Protection Committee(2003) The report of the death of Caleb Ness, Edinburgh:The City of Edinburgh Council. Available from:www.edinburgh.gov.uk (accessed 31 July 2006) (Internet).
NHS Information Authority (1999) Learning to managehealth information – A theme for clinical education:moving ahead, Birmingham: NHSIA. Available from:www.ic.nhs.uk (Internet).
NHS Scotland (2003) NHS Code of Practice on ProtectingPatient Confidentiality, Edinburgh: Scottish Executive.Available from:http://www.confidentiality.scot.nhs.uk/staffguidance.htm(accessed 31 July 2006) (Internet).
Nursing and Midwifery Council (2004) Code ofProfessional Conduct: standards for conduct, performanceand ethics, London: NMC. Available from www.nmc-uk.org/aDisplayDocument.aspx?DocumentID=201(accessed 31 July 2006) (Internet).
Nursing and Midwifery Council (2005) Guidelines forrecords and record keeping, London: NMC. Available from:www.nmc-uk.org/aFrameDisplay.aspx?DocumentID=609(accessed 31 July 2006) (Internet).
5
References
Parliament (1990) Access to Health Records Act 1990,London: TSO. Available at :www.opsi.gov.uk/acts/acts1990/ukpga_19900023_en_1.htm (accessed 1 December 2006) (Internet).
Parliament (1991) Age of legal capacity (Scotland) Act1991, London: TSO. Available at :www.opsi.gov.uk/acts/acts1991/ukpga_19910050_en_1.htm (accessed 1 December 2006) (Internet).
Parliament (2000) Data Protection Act 1998, London: TSO.Available at: www.ico.gov.uk/eventual.aspx (accessed 31July 2006) (Internet).
Parliament (2000) Freedom of Information Act, London:TSO. Available at: www.foi.nhs.uk/home.html (accessed 31July 2006) (Internet).
Parliament (2000) Human Rights Act 1998: Chapter 42,London: TSO. Available at:www.opsi.gov.uk/ACTS/acts1998/19980042.htm (accessed31 July 2006) (Internet).
Parliament (2004) Children Act 2004, London: TSO.Available at: www.dfes.gov.uk/publications/childrenactreport (accessed 31 July 2006) (Internet).
Royal College of Nursing (2005) RCN core career andcompetency framework. Available at:www.rcn.org.uk/resources/corecompetences/ (accessed 12October 2006)
Secretary of State for Health and Secretary of State for theHome Department (2003) The Victoria Climbié inquiry:report of an inquiry by Lord Laming, London: TSO.

Cabinet Office and Department of Health (2006) Making adifference: safe and secure data sharing between health and adultsocial care staff, London: Better Regulation Executive. Availablefrom: www.cabinetoffice.gov.uk/regulation/ documents/mad/data_sharing.pdf (accessed 31 July2006) (Internet).
Department for Constitutional Affairs (2004) A toolkit for datasharing, London: DCA. Available from:www.dca.gov.uk/foi/sharing/toolkit/index.htm (accessed 31 July2006) (Internet).
Department of Health (2006) The care record guarantee. Availablefrom: www.connectingforhealth.nhs.uk/crdb/docs/crs_guarantee.pdf
NHS Information Standards Board (2005) NHS health record andcommunication practice standards for team-based care, London:NHS. Available from: www.isb.nhs.uk/about-isib/isb-publications/isb-publications#record (accessed 31 July 2006)(Internet).
NHS Scotland data protection and confidentiality website(Scotland): www.show.scot.nhs.uk/confidentiality (accessed 31 July2006) (Internet).
NHS Wales – Informing Health Care website. Available from:www.wales.nhs.uk/sites3/home.cfm?OrgID=365 (accessed 31 July2006) (Internet).
Parliament (1990) Census (confidentiality) Act 1991, London: TSO.Available atwww.opsi.gov.uk/acts/acts1991/ukpga_19910006_en_1.htm(acccessed 1 December 2006) (Internet).
Parliament (1991) The Abortion Regulations 1991, London: TSO.Available at www.opsi.gov.uk/si/si1991.uksi_19910499_en_1.htm(acccessed 1 December 2006) (Internet).
Parliament (2002) The Abortion (Amendment) (England)Regulations 2002, London: TSO. Available atwww.opsi.gov.uk/si/si2002/20020887.htm (acccessed 1 December2006) (Internet).
Scottish Executive (July 2005) How to see your own record: Availablefrom: www.scotconsumer.org.uk/hris/leaflets/other2.htm (accessed 31 July 2006) (Internet).
Department of Health, Social Services and Public Safety (March2005) Northern Ireland Health and Social Care IM&T Strategy.Available from: www.dhsspsni.gov.uk/ict-strategy.pdfChapters 5-6 cover issues of consent and confidentiality.
16
R C N C O M P E T E N C I E S – I N F O R M A T I O N S H A R I N G
6Other resources

Abbreviations used in the frameworkBMA British Medical AssociationDH Department of HealthGMC General Medical CouncilIT Information technology
R O Y A L C O L L E G E O F N U R S I N G
17
Appendix 1:
Abbreviations and useful definitions
Patient identifiableinformation
Information which on its own or in combination can identify an individual. Includes:• patient’s name, address, full post code, date of birth• pictures, photographs, videos, audio-tapes or other images of patients• NHS number and local patient identifiable codes• anything else that may be used to identify a patient directly or indirectly. For example, rare diseases, drugtreatments or statistical analyses which have very small numbers within a small population may allow individualsto be identified.
Anonymisedinformation
Information which does not identify an individual directly, and which cannot reasonably be used to determineidentity. Anonymisation requires the removal of name, address, full post code and any other detail or combinationof details that might support identification.
Pseudonymisation Similar to anonymised information, in that in the possession of the holder it cannot reasonably be used by the holder toidentify an individual. However, in this case the original provider of the information may retain a means of identifyingindividuals. For example, codes or other unique references are often attached to information in place of names, so thatthe data will only be identifiable to those who have access to the key or index of names. Pseudonymisation allowsinformation about the same individual to be linked in a way that true anonymisation does not.
Consent:
1. Explicit or Expressconsent
Articulated patient agreement. The terms ‘explicit’ and ‘express’ are interchangeable. Both mean a clear andvoluntary indication of preference or choice, usually given orally or in writing by a patient and freely given incircumstances where the available options and the consequences have been made clear to that patient.
2. Implied consent Agreement that has been signalled by behaviour of an informed patient.
Disclosure Divulging or provision of access to information.
Health care purposes Activities ‘for health care purposes’ include all activities that directly contribute to the diagnosis, care andtreatment of an individual and to the audit/assurance of the quality of the health care provided. They do notinclude research, teaching, financial audit and other management activities.
Information sharingprotocol
Documented rules and procedures for the disclosure and use of patient information between two or moreorganisations or agencies, which specifically relate to security, confidentiality and data destruction.
Public interest Exceptional circumstances that justify over-ruling the right of an individual to confidentiality, in order to serve abroader societal interest. Decisions about the public interest are complex and must take account of both thepotential harm that disclosure may cause and the interest of society in the continued provision of confidentialhealth services.
Social care Social care is the support provided for vulnerable people, children or adults, including those with disabilities andsensory impairments. It excludes ‘pure’ health care (hospitals) and community care (e.g. district nurses), but mayinclude provision such as respite care. There is no clear demarcation between health and social care. Social carealso covers services provided by others where these are commissioned by councils with social serviceresponsibilities (CSSRs).
Common Law duty ofconfidence
The Common Law duty of confidence arises when a person receives information in circumstances where he or sheknows, or can be taken to know, that the information is to be treated in confidence.
NHS National Health ServiceNMC Nursing and Midwifery CouncilPIAG Patient Information Advisory Group

December 2006
Published by the Royal College of Nursing 20 Cavendish SquareLondon W1G 0RN
020 7409 3333
The RCN represents nurses and nursing,promotes excellence in practice and shapeshealth policies
Publication code 003 082
ISBN 1-904114-28-8
Approved by the RCN Accreditation Unit until November 2007


















