Compartment Syndrome 2LT Larson 2LT Loomis 1LT Moravec.
24
Compartment Compartment Syndrome Syndrome 2LT Larson 2LT Larson 2LT Loomis 2LT Loomis 1LT Moravec 1LT Moravec
-
Upload
eileen-grant -
Category
Documents
-
view
230 -
download
0
Transcript of Compartment Syndrome 2LT Larson 2LT Loomis 1LT Moravec.

Compartment SyndromeCompartment Syndrome
2LT Larson2LT Larson
2LT Loomis2LT Loomis
1LT Moravec1LT Moravec
AGENDAAGENDA
Introduction/PurposeIntroduction/Purpose
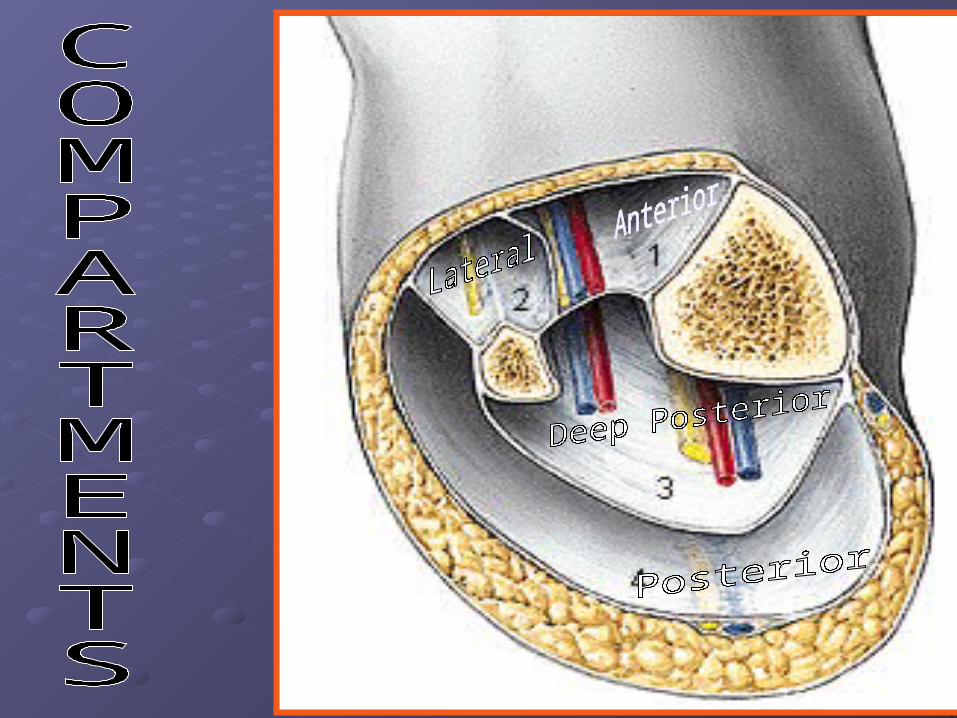
Involved AnatomyInvolved Anatomy
EtiologyEtiology
Clinical Presentation and DxClinical Presentation and Dx
Treatment/InterventionTreatment/Intervention
ConclusionConclusion
INTRODUCTIONINTRODUCTION
Compartment Syndrome can be a life/limb Compartment Syndrome can be a life/limb threatening emergencythreatening emergency
Related to acute trauma or exertion Related to acute trauma or exertion
Affects the muscle tissue, innervation, and Affects the muscle tissue, innervation, and vascularization within a MS compartmentvascularization within a MS compartment
Has also been described in the foot, thigh, Has also been described in the foot, thigh, forearm and gluteal regionsforearm and gluteal regions
Types of CSTypes of CS
Acute Compartment SyndromeAcute Compartment Syndrome
Exertional Compartment SyndromeExertional Compartment Syndrome Acute-one time episodeAcute-one time episode Chronic- with activityChronic- with activity
Under Pressure?Under Pressure?
From Anatomy we all know the Crural From Anatomy we all know the Crural Fascia is VERY tight and has a limited Fascia is VERY tight and has a limited ability to expand ability to expand
Increased compartmental pressure can Increased compartmental pressure can result in ischemia, neuropraxia and if result in ischemia, neuropraxia and if sustained, tissue NECROSISsustained, tissue NECROSIS
EtiologyEtiology
Acute CS:Acute CS: Direct trauma = Fx or soft-tissue injuryDirect trauma = Fx or soft-tissue injury More common in men (McQueen et al)More common in men (McQueen et al) Initial injury leads to swelling within Initial injury leads to swelling within
compartmentcompartment Muscle damage theorized to increases Muscle damage theorized to increases
osmotic pressure from release of protein-osmotic pressure from release of protein-bound ionsbound ions
EtiologyEtiology
Exertional CS:Exertional CS: Overexertion- Overexertion- Associated with repetitive Associated with repetitive
axial loading (runners and competitive axial loading (runners and competitive skaters)skaters)
Muscle volume can increase up to 20% due to Muscle volume can increase up to 20% due to fiber swelling and blood filling from vigorous fiber swelling and blood filling from vigorous exerciseexercise
EtiologyEtiology
Chronic ECS Chronic ECS (most commonly in Deep (most commonly in Deep
Compartment):Compartment): No anatomical predisposition No anatomical predisposition has been provenhas been provenExcessive compensatory pronation of the Excessive compensatory pronation of the subtalor joint implicatedsubtalor joint implicated During gait this would increase activity of During gait this would increase activity of
deep posterior compartment musclesdeep posterior compartment muscles
Usually bilateral involvement (50%-70%); Usually bilateral involvement (50%-70%); one extremity usually more symptomaticone extremity usually more symptomatic
CLINICAL PRESENTATIONCLINICAL PRESENTATION
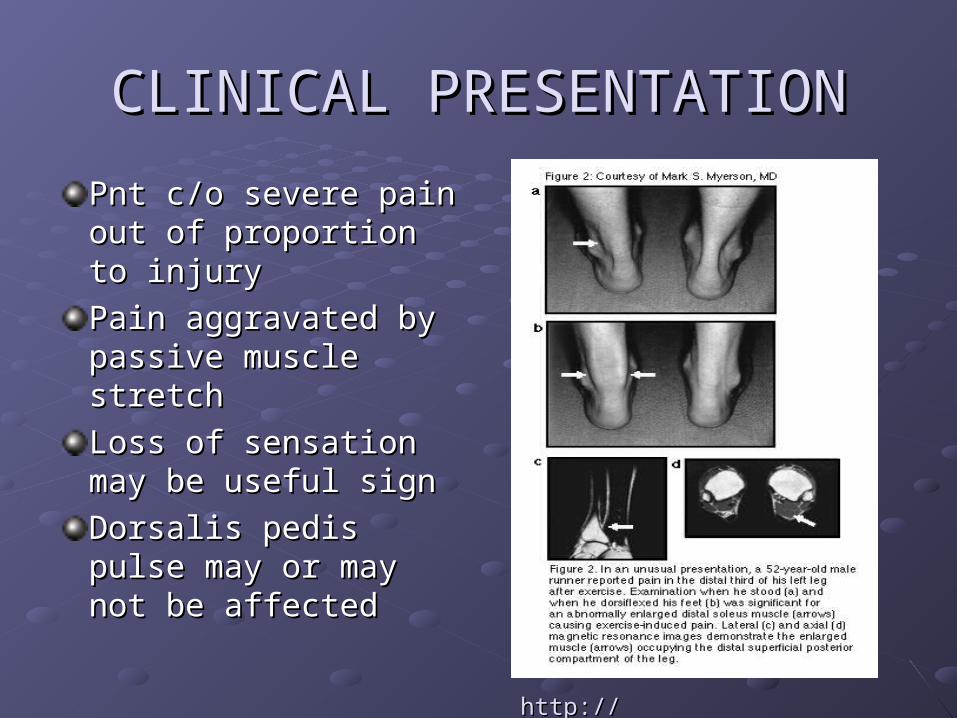
Pnt c/o severe pain out Pnt c/o severe pain out of proportion to injuryof proportion to injury
Pain aggravated by Pain aggravated by passive muscle stretchpassive muscle stretch
Loss of sensation may Loss of sensation may be useful signbe useful sign
Dorsalis pedis pulse Dorsalis pedis pulse may or may not be may or may not be affectedaffected
http://www.physsportsmed.comhttp://www.physsportsmed.com
CLINICAL PRESENTATIONCLINICAL PRESENTATION
Leg pain described as a dull ache Leg pain described as a dull ache (localized or diffuse) that begins at a (localized or diffuse) that begins at a predictable time during exercise predictable time during exercise
May also have: May also have: FootdropFootdrop Giving away of the ankleGiving away of the ankle Paraesthesias in the footParaesthesias in the foot Taut, shiny, warm skin that is TTPTaut, shiny, warm skin that is TTP
CLINICAL PRESENTATIONCLINICAL PRESENTATION
Post-exercisePost-exercise Involved compartments are swollen and tenseInvolved compartments are swollen and tense Increased leg girth over involved musclesIncreased leg girth over involved muscles Passive stretching of involved muscles may Passive stretching of involved muscles may
increase painincrease pain Symptoms usually lessen within 30 minSymptoms usually lessen within 30 min

Differential DiagnosisDifferential Diagnosis
Rule out Rule out stress fracturesstress fractures or or periostitisperiostitis Radiographs, bone-scan, bony tendernessRadiographs, bone-scan, bony tenderness
Medial tibial stress syndromeMedial tibial stress syndrome pain and tenderness over soleus bridgepain and tenderness over soleus bridge pain with exercise which can progress to other pain with exercise which can progress to other
activitiesactivities pain increased by hyperpronation of the footpain increased by hyperpronation of the foot
Compression neuropathiesCompression neuropathies-- electromyographyelectromyography
Clinical DiagnosisClinical Diagnosis
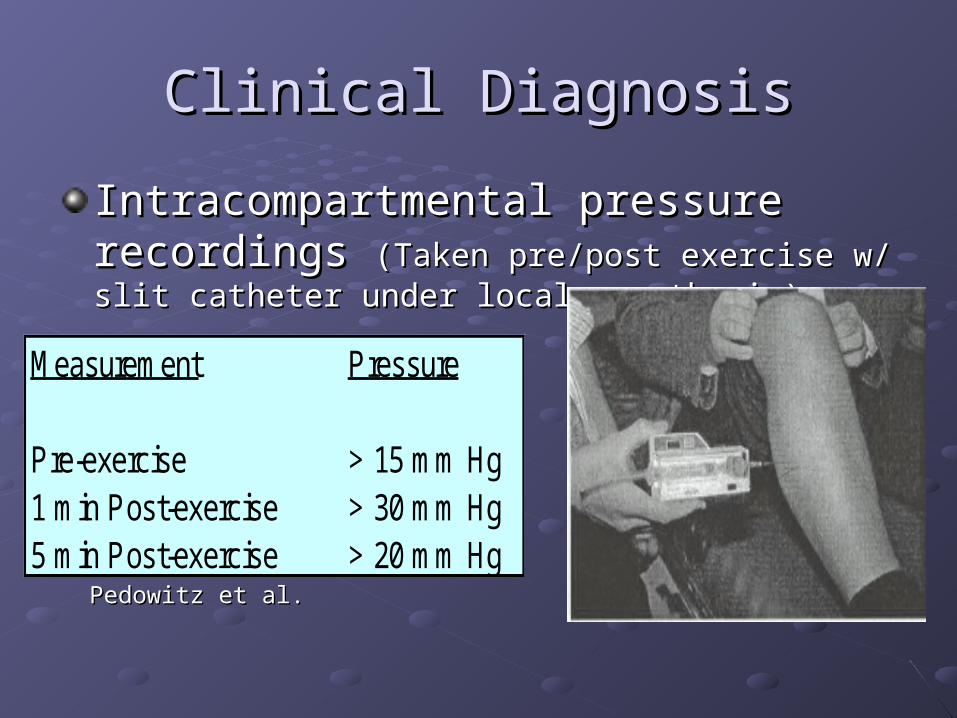
Intracompartmental pressure recordings Intracompartmental pressure recordings (Taken pre/post exercise w/ slit catheter under local (Taken pre/post exercise w/ slit catheter under local anesthesia)anesthesia)
Measurement Pressure
Pre-exercise > 15 mm Hg1 min Post-exercise > 30 mm Hg5 min Post-exercise > 20 mm Hg
Pedowitz et al.Pedowitz et al.
Treating ECSTreating ECS
Conservative at firstConservative at first Cross training with low impact activities Cross training with low impact activities
(swimming, bicycling)(swimming, bicycling) Rest, Ice, Elevation Rest, Ice, Elevation No CompressionNo Compression NSAIDS NSAIDS StretchingStretching Address biomechanical problemsAddress biomechanical problems Gradual return to activityGradual return to activity
Treatment OptionsTreatment Options
If symptoms persist with activity for > 3 to If symptoms persist with activity for > 3 to 6 months6 months
A: Stop prevocational activitiesA: Stop prevocational activities
B: Have Surgery: B: Have Surgery: Fasciotomy of all involved Fasciotomy of all involved compartmentscompartments
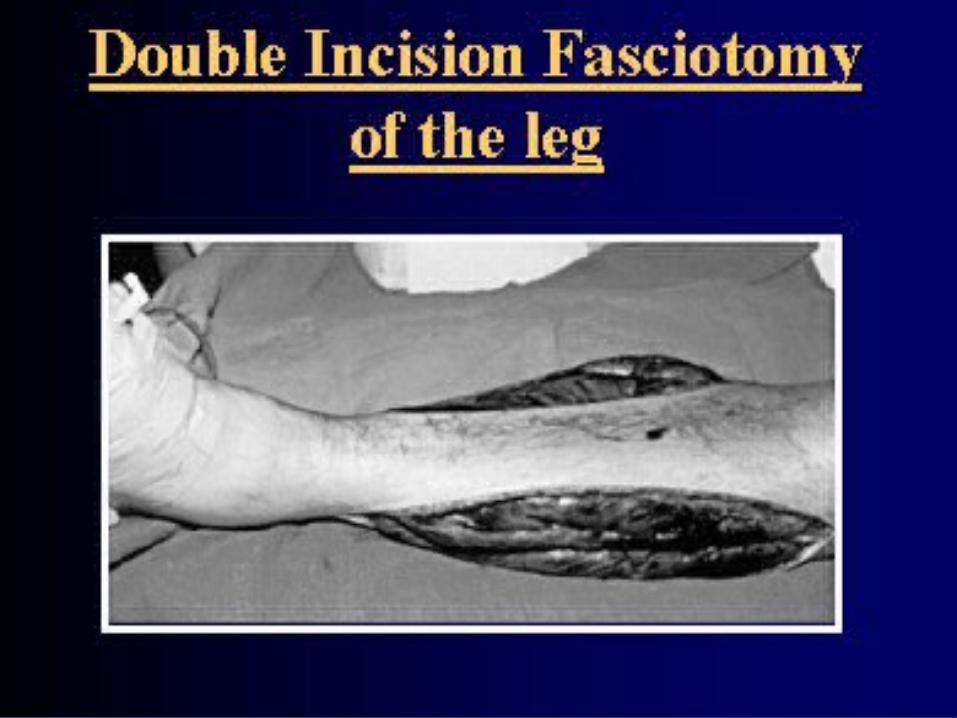
Surgical OutcomeSurgical Outcome
Dependent upon compartment involvement Dependent upon compartment involvement Results of anterior and lateral releases are Results of anterior and lateral releases are
superior to posterior releasesuperior to posterior release Failure of Deep posterior compartment Failure of Deep posterior compartment
release largely due to insufficient release-release largely due to insufficient release-as it is harder to get toas it is harder to get to
Management of fasciotomy wounds is Management of fasciotomy wounds is controversialcontroversial
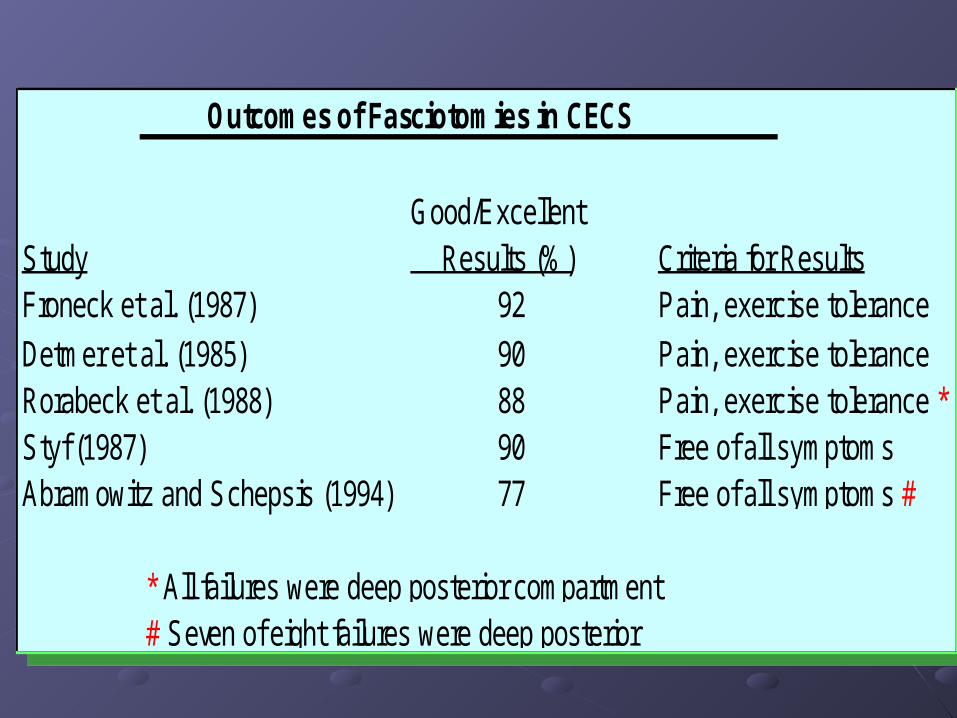
Outcomes of Fasciotomies in CECS
Good/ExcellentStudy Results (%) Criteria for ResultsFroneck et al. (1987) 92 Pain, exercise toleranceDetmer et al. (1985) 90 Pain, exercise toleranceRorabeck et al. (1988) 88 Pain, exercise tolerance *Styf (1987) 90 Free of all symptomsAbramowitz and Schepsis (1994) 77 Free of all symptoms #
* All failures were deep posterior compartment# Seven of eight failures were deep posterior
Outcomes of Fasciotomies in CECS
Good/ExcellentStudy Results (%) Criteria for ResultsFroneck et al. (1987) 92 Pain, exercise toleranceDetmer et al. (1985) 90 Pain, exercise toleranceRorabeck et al. (1988) 88 Pain, exercise tolerance *Styf (1987) 90 Free of all symptomsAbramowitz and Schepsis (1994) 77 Free of all symptoms #
* All failures were deep posterior compartment# Seven of eight failures were deep posterior
PT Intervention Post SurgeryPT Intervention Post Surgery
Immediate Ice and ElevationImmediate Ice and Elevation
Crutches (TTWB) with gradual progression to Crutches (TTWB) with gradual progression to FWB (1 week)FWB (1 week)
Gait training to prevent abnormal movement Gait training to prevent abnormal movement secondary to stiffness and guardingsecondary to stiffness and guarding
ROM exercises to increase circulation:ROM exercises to increase circulation: ankle dorsiflexion, plantar flexion, inversion, ankle dorsiflexion, plantar flexion, inversion,
eversion, alphabet exerciseeversion, alphabet exercise knee flexion/ extension knee flexion/ extension
Rehab ProgressionRehab Progression
Gentle isokineticsGentle isokinetics
Stretching, of involved musclesStretching, of involved muscles
Aerobic training: Limited WB Aerobic training: Limited WB (swimming/cycling)(swimming/cycling)
4 weeks:4 weeks: progression to running and resistive progression to running and resistive
weight training as toleratedweight training as tolerated
2-3 months full return to training2-3 months full return to training
ConclusionConclusionExercise induced ECS is often miss-diagnosed.Exercise induced ECS is often miss-diagnosed.
Awareness is key due to the dangers of untreated Awareness is key due to the dangers of untreated acuteacute ECS. ECS.
Non-surgical interventions Non-surgical interventions notnot shown to help long shown to help long term.term.
Surgery is intervention for reliably high prognosis.Surgery is intervention for reliably high prognosis.
PT plays important role in Dx and post surgical PT plays important role in Dx and post surgical Tx.Tx.
QUESTIONS?QUESTIONS?
REFERENCESREFERENCES1.1. Tiwari A, Haq AI, Myint F, Hamilton G. Acute compartment syndromes. Tiwari A, Haq AI, Myint F, Hamilton G. Acute compartment syndromes. British Journal of Surgery. British Journal of Surgery. 2002; 89(4): 397-412.2002; 89(4): 397-412.2.2. McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. McQueen MM, Gaston P, Court-Brown CM. Acute compartment syndrome. Who is at risk?[comment]. Who is at risk?[comment]. Journal of Bone & Joint Surgery - British Volume. Journal of Bone & Joint Surgery - British Volume. 2000;82(2):200-203.2000;82(2):200-203.3.3. Pearse MF, Harry L, Nanchahal J. Acute compartment syndrome of the leg: Pearse MF, Harry L, Nanchahal J. Acute compartment syndrome of the leg: fasciotomies must be performed early, but good surgical technique is important. fasciotomies must be performed early, but good surgical technique is important. British Medical Journal. British Medical Journal. 14 September 2002 2002;Volume 325(7364):557-558.14 September 2002 2002;Volume 325(7364):557-558.4.4. Garcia-Mata S, Hidalgo-Ovejero A, Martinez-Grande M. Chronic exertional Garcia-Mata S, Hidalgo-Ovejero A, Martinez-Grande M. Chronic exertional compartment syndrome of the legs in adolescents. compartment syndrome of the legs in adolescents. Journal of Pediatric Orthopedics. Journal of Pediatric Orthopedics. 2001;21(3):328-334.2001;21(3):328-334.5.5. Prentice WE, Voight MI. Prentice WE, Voight MI. Techniques in musculoskeletal rehabilitationTechniques in musculoskeletal rehabilitation . New . New York: McGraw-Hill; 2001.York: McGraw-Hill; 2001.6.6. Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: Ulmer T. The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder? are clinical findings predictive of the disorder? Journal of Orthopaedic Trauma. Journal of Orthopaedic Trauma. 2002;16(8):572-577.2002;16(8):572-577.7.7. Finkelstein JA, Hunter GA, Hu RW. Lower limb compartment syndrome: Finkelstein JA, Hunter GA, Hu RW. Lower limb compartment syndrome: course after delayed fasciotomy. course after delayed fasciotomy. Journal of Trauma-Injury Infection & Critical Care. Journal of Trauma-Injury Infection & Critical Care. 1996;40(3):342-344.1996;40(3):342-344.