Comparison of the effects of calcium antagonists and converting enzyme inhibitors on renal function...
10
Comparison of the Effects of Calcium Antagonists and Converting Enzyme Inhibitors on Renal Function Under Normal and Hypertensive Conditions Juan Carlos Romero, MD, Luis M. Ruilope, MD, Michael D. Bentley, PhD, Mary J. Fiksen-Olsen, BS, Vicente Lahera, PhD, and Maria J. Vidal, MD Calcium antagonists decrease the ability of the kid- ney to autoregulate renal blood flow (RBF) and glo- merular filtration rate (GFR). Therefore, when af- ferent renovascular resistance is elevated, as in es- sential hypertension, there is a resultant increase in RBF and GFR with the administration of calcium antagonists. These agents also induce a marked natriuresis because of direct tubular action through unknown mechanisms. The,natriuresis can be dis- sociated from renal and systemic hemodynamic ac- tions, indicating that the decreased sodium reab- sorption could override other compensatory mecha- nisms explaining the absence of sodium retention during the treatment. The renal effects of converting enzyme inhibi- tors (CEls) can be explained by the reduction of in- trarenal formation in angiotensin II. Because the activation of the renin-angiotensin system is mainly responsible for inducing sodium retention during a decrease in systemic blood pressure, CEls could have a protecting effect without disturbing other homeostatic mechanisms. CEls decrease efferent glomerular resistance, reducing capillary pressure and thereby reducing GFR. This effect is not trans- lated in sodium retention because the reduction of GFR is mild during captopril administration in kid- neys with normal or increased renal perfusion pres- sure. At low renal perfusion pressure, the reduced glomerular afferent vasoconstriction can compro- mise GFR, leading to renal insufficiency. Although these situations are not likely to be encountered during the treatment of uncomplicated essential hy- pertension, in severe hypertension with hypertro- phy of pre-glomerular vessels, glomerular perfusion may decrease. Combination therapy of calcium an- tagonists and CEls has been reported to be an ef- fective treatment of severe hypertension. Currently, little information is available on the manner in which renal function is affected by simultaneous administration of both drugs. (Am J Cardiol 1988;62:596-686) I n recent years, new and potent pharmacologic drugs that can effectively reduce and control hypertension havebeen synthesized and madeavailable to the gen- eral practitioner.ls2 Among thesedrugs, calcium antago- nists and converting enzymeinhibitors (CEIs) have rap- idly gained a significant reputation for their overall effi- cacy in decreasing high blood pressure.2In fact, the pharmacologicactions of thesecompounds are not limit- ed only to a decrease in total peripheral resistance,as occurswith other vasodilators,but they also exhibit rath- er potent renal effects that prevent sodium retention.2 Consequently, the administration of either calcium an- tagonists or CEIs hasbeen suggested to be effectivewhen usedas monotherapyin the treatment of essential hyper- tension3 It is the objective of this review to examine the effects of calcium antagonists and CEIs on renal hemody- namics and on renal tubular excretion when given alone or in combination. We believe that such comparative evaluation of the action of thesedrugs may serveto set a clinical criteria for their appropriate use. Criteria to assess the renal hemodynamics and renal tubular effects of antihyportensive drugs: Guyton et al4 fostered the concept that the developmentof hyperten- sion is critically dependent on the ability of the kidney to excretesodiumat a given perfusion pressure. The charac- teristics of the pressure-natriuresis curve, with respect to changes in renal blood flow (RBF) and glomerular filtra- tion rate (GFR) under normal conditions, are shown in Figure 1. A decrease in renal perfusion pressureto ap- proximately 75 mm Hg evokes a prompt vasodilator au- toregulatory response that preventschanges in RBF and GFR. These autoregulatory characteristics of RBF and GFR are not shared by the excretion of sodium in the urine, which varies in direct proportion to changes in renal perfusionpressure. This relation must beconsidered when examining the renal effects of antihypertensive agents because the natriuretic effects can be offset and evenreversed by the concomitant decrease of blood pres- sure.2 Because of these characteristics, the renal effectsof From the Department of Physiology and Biophysics, Mayo Clinic, Rochester, Minnesota; and the Division of Nephrology, Hospital I” de Octubre, Madrid, Spain. This study was supported by Grant HL-16496 from the National Institutes of Health, Bethesda, Maryland, and the Mayo Foundation, Rochester, Minnesota. Address for reprints: Juan Carlos Romero, MD, Department of Physiology, Mayo Clinic, Rochester, Minnesota 55905. THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5,1988 596
-
Upload
juan-carlos-romero -
Category
Documents
-
view
212 -
download
0
Transcript of Comparison of the effects of calcium antagonists and converting enzyme inhibitors on renal function...

Comparison of the Effects of Calcium Antagonists and Converting Enzyme Inhibitors on Renal Function Under
Normal and Hypertensive Conditions Juan Carlos Romero, MD, Luis M. Ruilope, MD, Michael D. Bentley, PhD, Mary J. Fiksen-Olsen, BS, Vicente Lahera, PhD, and Maria J. Vidal, MD
Calcium antagonists decrease the ability of the kid- ney to autoregulate renal blood flow (RBF) and glo- merular filtration rate (GFR). Therefore, when af- ferent renovascular resistance is elevated, as in es- sential hypertension, there is a resultant increase in RBF and GFR with the administration of calcium antagonists. These agents also induce a marked natriuresis because of direct tubular action through unknown mechanisms. The,natriuresis can be dis- sociated from renal and systemic hemodynamic ac- tions, indicating that the decreased sodium reab- sorption could override other compensatory mecha- nisms explaining the absence of sodium retention during the treatment.
The renal effects of converting enzyme inhibi- tors (CEls) can be explained by the reduction of in- trarenal formation in angiotensin II. Because the activation of the renin-angiotensin system is mainly responsible for inducing sodium retention during a decrease in systemic blood pressure, CEls could have a protecting effect without disturbing other homeostatic mechanisms. CEls decrease efferent glomerular resistance, reducing capillary pressure and thereby reducing GFR. This effect is not trans- lated in sodium retention because the reduction of GFR is mild during captopril administration in kid- neys with normal or increased renal perfusion pres- sure. At low renal perfusion pressure, the reduced glomerular afferent vasoconstriction can compro- mise GFR, leading to renal insufficiency. Although these situations are not likely to be encountered during the treatment of uncomplicated essential hy- pertension, in severe hypertension with hypertro- phy of pre-glomerular vessels, glomerular perfusion may decrease. Combination therapy of calcium an- tagonists and CEls has been reported to be an ef- fective treatment of severe hypertension. Currently, little information is available on the manner in which renal function is affected by simultaneous administration of both drugs.
(Am J Cardiol 1988;62:596-686)
I n recent years, new and potent pharmacologic drugs that can effectively reduce and control hypertension have been synthesized and made available to the gen-
eral practitioner.ls2 Among these drugs, calcium antago- nists and converting enzyme inhibitors (CEIs) have rap- idly gained a significant reputation for their overall effi- cacy in decreasing high blood pressure.2 In fact, the pharmacologic actions of these compounds are not limit- ed only to a decrease in total peripheral resistance, as occurs with other vasodilators, but they also exhibit rath- er potent renal effects that prevent sodium retention.2 Consequently, the administration of either calcium an- tagonists or CEIs has been suggested to be effective when used as monotherapy in the treatment of essential hyper- tension3 It is the objective of this review to examine the effects of calcium antagonists and CEIs on renal hemody- namics and on renal tubular excretion when given alone or in combination. We believe that such comparative evaluation of the action of these drugs may serve to set a clinical criteria for their appropriate use.
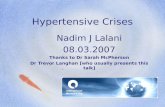
Criteria to assess the renal hemodynamics and renal tubular effects of antihyportensive drugs: Guyton et al4 fostered the concept that the development of hyperten- sion is critically dependent on the ability of the kidney to excrete sodium at a given perfusion pressure. The charac- teristics of the pressure-natriuresis curve, with respect to changes in renal blood flow (RBF) and glomerular filtra- tion rate (GFR) under normal conditions, are shown in Figure 1. A decrease in renal perfusion pressure to ap- proximately 75 mm Hg evokes a prompt vasodilator au- toregulatory response that prevents changes in RBF and GFR. These autoregulatory characteristics of RBF and GFR are not shared by the excretion of sodium in the urine, which varies in direct proportion to changes in renal perfusion pressure. This relation must be considered when examining the renal effects of antihypertensive agents because the natriuretic effects can be offset and even reversed by the concomitant decrease of blood pres- sure.2 Because of these characteristics, the renal effects of
From the Department of Physiology and Biophysics, Mayo Clinic, Rochester, Minnesota; and the Division of Nephrology, Hospital I” de Octubre, Madrid, Spain. This study was supported by Grant HL-16496 from the National Institutes of Health, Bethesda, Maryland, and the Mayo Foundation, Rochester, Minnesota.
Address for reprints: Juan Carlos Romero, MD, Department of Physiology, Mayo Clinic, Rochester, Minnesota 55905.
THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5,1988 596

A SYMPOSIUM: CALCIUM, THE CARDIOVASCULAR SYSTEM AND THE KIDNEY
the drug should be established first by direct infusion into the renal artery in the absence of changes in systemic blood pressure.2-4 Once these effects are established, it should be determined how they are modified when sys- temic pressure is allowed to change.
Effects of calcium antagonists on renal hemodynam- its: In an attempt to comply with the aforementioned criteria, we have compiled experimental studies in which calcium antagonists were injected into the renal artery of normotensive animals, and changes in blood pressure, RBF, GFR, and urinary sodium excretion were simulta- neously recorded (Table I). In 7 observations,5-‘1 the intrarenal administration of calcium antagonists did not affect systemic blood pressure. However, in 2 observa- tions,1°J2 there was a 10 to 20% decrease in blood pres- sure from control levels. This decrease of blood pressure may have resulted from an excess of the drug recirculat- ing from the kidney into the systemic circulation, Table I shows that of the 7 studies in which blood pressure was unchanged, there were 4 that exhibited increments in both RBF and GFR,5-s while in the remaining 3, GFR was unaffected.9-1 l It should be emphasized that in all the studies, there was an increase in urine sodium excretion regardless of changes in GFR. Furthermore, in the 2 studies in which blood pressure was decreased, calcium antagonists induced a clear natriuretic effect without al- tering RBF or GFR.t”,12
r Normal Conditions - 0.5
c
- 04 ‘E s
- f E
- 0.3 -
E - c.3
- 0.1
RPP, mm Hg Pressure natriuresis I
FIGURE 1. Change in renal plasma flow (RPF), glomerular fil- tration rate (GFR) and urinary sodium excretion (UNa) during alterations in renal perfusion pressure (RPP). (Reprinted with permission from Hypertension.52)
Taken together, the studies listed in Table I indicate that the most consistent effect of calcium antagonists is the increased urinary sodium excretion. This effect is most probably due to a direct tubular action since it could be elicited without altering renal hemodynamics. The second conclusion is that when blood pressure remains constant, the natriuretic effects of calcium antagonists are accompanied by renal vasodilatation. In 60% of the cases, this vasodilatation affects the pre-glomerular vas- culature because of the concomitant increase in GFR. Because of the prominence of the natriuretic effect, let us first examine the effects of calcium antagonists on tubu- lar sodium reabsorption and then analyze the renal hemo- dynamic effects.
Effects of calcium antagonists on renal tubular func- tion: The notion that calcium antagonists have a direct renal tubular effect was best demonstrated when blood pressure was reduced (Table I) because in these circum- stances, the natriuresis occurred without changes in RBF or GFR.10m12 Furthermore, it has been shown that acute increase of urinary sodium excretion far outlasts the renal hemodynamic changes.7 However, the mechanisms by which calcium antagonists alter tubular sodium reab- sorption is far from being understood.
Taylor and Windhager13 emphasized that when the intracellular concentration of calcium (Ca2+) is increased in renal tubular epithelium by means of quinidine, calci- um ionophores, or low peritubular sodium concentration, there is a decrease in sodium reabsorption. On the basis of these observations, cytosolic calcium was suggested to be a major factor in regulating the entry of sodium through the apical border of the tubular epithelial cell. In this scheme, an increase in intracellular Ca2+ reduces sodium reabsorption and presumably produces natriuresis. How- ever, this scheme is difficult to reconcile with a precon- ceived notion that calcium antagonists may produce na- triuresis by decreasing the level of cytosolic Ca2+ in tubular epithelial cells. Nevertheless, in micropuncture experiments, MacLaughlin et all4 observed that 10m5M verapamil added to the luminal perfusate of normal Wis- tar rats produced a 36% decrease of sodium reabsorption and that a greater reduction of 61% of sodium reabsorp- tion occurred when verapamil was infused into peritubu- lar capillaries. Similarly, Figueiredo et all5 found a signif-
TABLE I Summarv of Maior Effects of Calcium Blockers on Renal Function When Administered in the Renal Artery
Abe et al5 Nicardipine Roy et al6 Verapamil Bell and Lindner7 Verapamil Yamaguchi et al8 Diltiazem Abe et al9 Verapamil Dietz et allo Verapamil Burke et aill Verapamil Dietz et allo Nifedipine DiBona and Sawinl’ Felodipine
Agent
Decrease in SBP (“h)
Increase in RBF (%)
Increase in GFR (%)
Increase in UNa Above Control (Fold)
NS 29 17 5.9 NS NS NS NS NS NS 20 10
16 42 4.3 11 75 20.0 11 17 2.6 39 NS 4.4 10 NS 5.9 45 NS 3.6 NS NS 2.8 NS NS 2.4
All studies were performed on anesthetized dogs, except for the study by DiSona and Sawin. which was performed on anesthetized rats. GFR = glomerular filtration rate; NS = not significant; RBF = renal blood flow; SBP = systemic blood pressure; UNa = urinary sodium excretion.
606 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62

THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5,1988 61G
icant decrease of sodium reabsorption in isolated perfused proximal tubules of rabbits when verapamil was added to the bathing solution. The investigators in these stud- ies14J5 concurred that the inhibitory effect of verapamil on the tubular transport of sodium may not be explained by a decrease in cytosolic calcium but by an effect on other transport mechanisms.3
The strong tubular effect of calcium antagonists sug- gests that their natriuretic effect may not be greatly im- paired by a concomitant decrease in total peripheral resis- tance and blood pressure. In order to test this possibility, we conducted a study to measure the urinary sodium excretion in 5 volunteers with essential hypertension and in 5 normotensive volunteers during 5 hours of isotonic saline infusion at the rate of 500 ml/hour. The results were compared with the responses exhibited by both groups submitted to an identical 5 hours of volume expan- sion initiated 1 hour after a single, 20-mg oral dose of nifedipine. Figure 2 shows that with nifedipine, urinary sodium excretion was elevated in both the normotensive and the hypertensive groups. However, nifedipine in- duced an 11.2% decrease in mean systemic blood pressure in hypertensive subjects (from 116 f 6 to 103 f 3 mm Hg), whereas systemic pressure was unchanged in nor- motensive subjects (approximately 81 f 4 mm Hg). These findings indicate that the nifedipine facilitated uri- nary sodium excretion despite the decrease in blood pres- sure exhibited by the hypertensive subjects. The adminis- tration of nifedipine produced a mild elevation in the control levels of plasma renin activity in hypertensive and normotensive subjects that was not statistically signifi- cant (Fig. 3). However, nifedipine did not preclude the suppressive effects of volume expansion on plasma renin activity. Similar considerations are applicable to plasma levels of aldosterone which are shown in Figure 4.
An unanswered question from this experiment is whether urinary sodium excretion would have been corn:
pletely normalized if the blood pressure of the hyperten- sive subjects would have been brought to levels compara- ble to those of the normotensive subjects. Such a possibili- ty is strongly suggested by studies indicating that calcium antagonists do not induce sodium retention in hyperten- sivei6-I9 or in normotensive subjects.17-20
Effects of calcium antagonists on renal hemodynam- its: Loutzenhiser and Epstein21 showed that the efficacy of calcium antagonists to induce vasodilatation is largely determined by the resting vascular tone. Accordingly, the renal vasodilator activity will be considerably diminished when renal perfusion pressure has been previously de- creased because of the ongoing autoregulatory vasodila- tation. This view is supported by several studies5s show- ing that the increments in RBF and GFR evoked by the intrarenal administration of calcium antagonists were abolished by previously decreasing renal perfusion pres- sure to the limit of RBF autoregulation. This concept is shown in Figure 5, which has been reconstructed from experimental data obtained from Navar et a1,22 who showed an abolition of RBF autoregulation after the ad- ministration of calcium antagonists. Similar effects have been reported by other investigators.23,24 It is shown that under normal conditions an increase of renal perfusion pressure from 20 to 8 5 mm Hg is accompanied by propor- tional increments of RBF because the diameter of pre- glomerular vessels remains dilated (Fig. 5, top). From 85 mm Hg, further increments of renal perfusion pressure elicit an autoregulatory vasoconstrictor response in the pre-glomerular vessels in proportion to the increments in blood pressure, thus reducing the arterial diameter. Since the ability of calcium antagonists to induce vasodilatation is determined by the existing degree of vasoconstriction,21 it follows that the administration of this drug will produce a significant vasodilatation only at high levels of renal perfusion pressure (Fig. 5, middle and bottom). In con- trast, RBF will not be altered if calcium antagonists are
Hypertensives
l n With rlifedlpine
0 0 Without nifedipme
Y --
loo L I I I I I J 70 60 90 100 110 120 130
Mean blood pressure, mm Hg
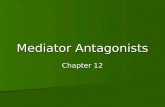
FIGURE 2. Relation of urinary sodium excretion (UNa) and mean blood pressure during volume expansion in 5 normoten- sive and in 5 essential hypertensive subjects during a S-hour infusion of isotonic saline, before (open symbo/s) and after (closed symbok) administration of a single 20-mg oral dose of nifedipine. The symbols represent the average UNa of the sub- jects at each of the l-hour time points during the 5 hours of sodium overload in relation to the arterial pressure (mean & standard error of the mean).
r Normotensives Hypertensives 5
c
l m With nifedipine
4 00 Without nifedipine I
01 ’ ’ ’ ’ I I I I Control 2 4 6 Control 2 4 6
Time, hr
FIGURE 3. Changes in plasma renin activity (PRA) (mean rt standard error of the mean) induced by volume expansion in 5 normotensive and 5 essentiil hypertensive subjects before a I-hour infusion of saline (control), at 2 and 4 hours during the infusion, and 1 hour after (6 hours) the infusion. Open sym bols, before; closed symbols, after administration of nifedi- pine.

A SYMPOSIUM: CALCIUM, THE CARDIOVASCULAR SYSTEM AND THE KIDNEY
Normotensives Hypertensives
14 r I l a With nifedipine
00 Without nifedipine
*L ’ ’ ’ ’ I I I I control 2 4 6 Control 2 4 6
Time, hr
standard error of-the mean) induced by volume expansion in the same subjects during the same conditions as described in Figure 3.
o- 50 100 150 200 250
RPP, mm Hg
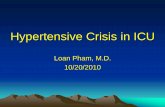
FIGURE 5. Effect of calcium antagonists on renal blood flow (RBF) autoregufation in normotensive and in hypertensive sub- jects. Cylindrical symbols indicate changes in afferent arteri- ole diameter. Top, normal changes in RBF relative to renal perfusion pressure (RPP). Wlthin the range of RBF autoregu- lation, the diameter of the afferent arterioles is progressively reduced with increasing RPP, however, below the limit of au- toregulation, the afferent arterioles are dilated. Middle, ad- ministration of calcium antagonists compromises RBF auto- regulation by shifling the normal curve (broken line) upward (confinuous line). Because the afferent arterioles remain dilat- ed, there is a marked increase in RBF in hypertensives (solid arrow) but oniy a mikt increase of RBF in normotensives (bre ken arrow). Bottom, with a concomitant decrease in systemic blood pressure, RBF in hypertensives is comparable to normo- tensives. RPF = renal plasma flow.
administered in the lower limit or below the range of autoregulation. The lack of RBF autoregulation induced by calcium antagonists may also explain some peculiari- ties relative to the responses of normotensive and hyper- tensive subjects to these drugs. These compounds will elicit a marked increase of RBF in hypertensive subjects, whereas such increments will not be so pronounced in normotensive subjects (Fig. 5, middle).21 If blood pres- sure in the hypertensive patient is concomitantly de- creased by calcium antagonists to levels comparable to those seen in normal subjects, then the effects of incre- ments in RBF are blunted.
Since the autoregulatory vasoconstriction of the pre- glomerular vessels is crucial to maintain GFR,2m4 calcium antagonists will induce changes in GFR similar to those induced on RBF. The blockade of glomerular afferent
0.7
0.5
0.3
0.1
0.7
RPP, mm Hg
FIGURE 6. Effects of cakium antagonists on autoreguiation 01 glomerular filtration rate (GFR) in normotensive and hyperten- sive subjects. Diagram above each curve illustrates diameter of afferent and efferent arterioles and magnitude of GFR. Top, normal changes in GFR with alterations in renal perfu- sion pressure (RPP). With changes of RPP within the range of autoregulation, the diameter of afferent arterioles is reduced and GFR remains constant. With decrements of RPP below the range of autoregulation, even though afferent arterioles are dilated and the efferent arteriole is constricted, GFR is re- duced. Midd/e, administration of calcium antagonists compro- mises GFR autoregulation by shifting the normal curve (br+ ken line) upward (confinuous line). Sime the afferent arte- rioles remain dilated, there is a significant increase in GFR in hypertensives (so/id arrow), which is unlikely to be seen in normotensives (interrupted arrow). Boffom, with a concomi- tant decrease in systemic Mood pressure, GFR in hyperten- sives is comparable to normotensives.
626 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62

vasoconstriction will result in a significant loss of GFR autoregulation (Fig. 6). This concept is supported by the study of Navar et a122 who showed that verapamil pro- duced an almost complete abolition of GFR autoregula- tion. The administration of calcium antagonists in hyper- tensive patients is likely to produce significant increments in GFR that will not be seen in normotensive subjects, whose perfusion pressure is closer to the limit of RBF autoregulation (Fig. 6, middle). However, Figure 6 also shows that if blood pressure in the hypertensives is con- comitantly decreased by calcium antagonists, then GFR will not differ much from the magnitude observed in normotensives.
These concepts can be confirmed by examining the few studies that are available concerning the effect of similar doses of calcium antagonists in hypertensive and
TABLE II Changes in Systemic Blood Pressure (SBP), Renal Blood Flow (RBF), Glomerular Filtration Rate (GFR), and Urinary Sodium Excretion (UNa) Induced by Calcium Antagonists*
Condition SBP RBF
Hypertension - 4% +28% Hypertension -25% N-S” Normotension NS NS
* Data collected from References 16 to 20. NS = not significant.
GFR UNa
+30% +3.43 NS f1.90 NS +2.45
0 50 100 150 200
RPP, mm Hg
c
2.5 ‘E Tn s E
1.5 _
B
0.5 1
250
- 0.7
.E
- 0.5 c 0)
- 5 E
-03 -
:: - c3
-0.1 1
FIGURE 7. Vascular and tubular effects of intrarenally gener- ated angiotensin II (Y symbol) on efferent arterioles and on proximal tubules. Top, changes in vascular tone of afferent and efferent arterioles at perfusion pressures (RPP) of 80, 140 and 190 mm Hg (within the range of autoregulation) and at 40 mm Hg (below the range of autoregulation) are repre- sented by the thickness of the arrow emerging from the glo- merulus, and changes in sodium reabsorption by the proximal tubules are illustrated by the arrows emerging from the tubu- lar lumen. For comparison, the levets of renal plasma flow (RPF), glomendar filtration rate (GFR), and urinary sodium excretion relative to RPP are illustrated in the lower part of the figure.
normotensive subjects (Table II).‘6-20 In normotensives, the oral administration of calcium antagonists does not result in a significant change of systemic blood pressure, RBF or GFR, but produces significant increments of urine sodium excretion because of independent tubular effects.3 In hypertensives, the renal effects are virtually predetermined by the magnitude of the decrease in sys- temic blood pressure. When systemic blood pressure is slightly decreased by 4%, then calcium antagonists are capable of producing significant alterations in RBF, GFR and urinary sodium excretion. In contrast, when systemic blood pressure is decreased by 25%, the adminis- tration of calcium antagonists fails to produce alterations in RBF and GFR. Under these conditions, urinary sodi- um excretion does not achieve the same level as that achieved when blood pressure is minimally altered.
The significance of the therapeutic effects of calcium antagonists on renal hemodynamics have been empha- sized by Hollenberg et alz5 who showed that in two-thirds of patients with essential hypertension, there is an exag- gerated increase in intrarenal vascular resistance. This alteration may constitute the very initial imbalance of Ca2+ metabolism. Such a possibility is strongly supported by the studies of Blackshear et a126 who demonstrated that the first-degree relative of hypertensive patients ex- hibits an enhanced renal vasodilator response to calcium antagonists when compared with relatives of normoten- sive patients. However, the manner in which these alter- ations in renal vascular resistance could impair urinary sodium excretion and influence cardiovascular volume and blood pressure remains to be explained.
~~~~ RPP 401 90 I 140 0 1907
f E 1.5
h 0.5
i RPP, mm Hg
FIGURE 8. Effects of converting enzyme inhibitors on auto- regulatory responses. Top, the afferent arteriole constricts in response to increases in renal perfusion pressure (RPP) but the efferent arteriole remains dilated as a result of converting enzyme inhibitors. The net result of administration of convert- ing enzyme inhibitors (bottom) is an increase in renal plasma flow (RPF) (solid line) at low RPP in comparison to normal RPF (broken line), but little difference at high RPP.
THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5.1988 636

A SYMPOSIUM: CALCIUM, THE CARDIOVASCULAR SYSTEM AND THE KIDNEY
Effects of converting enzyme inhibitors on renal he- chemical characteristics of kininase II.28,29 Kininase II is modynamics and tubular function: CEIs, as implied by mainly responsible for inactivating bradykinin by the their name, are synthetic compounds that inhibit the en- same mechanism that converts angiotensin I into angio- zyme involved in the conversion of angiotensin I into tensin II.28,29 In both circumstances, the enzymes split the angiotensin II.27 CEIs have been shown to share the same last 2 amino acids from the carboxvlic end of the polvnep-
RPP 40; 90 ? 0.7 I-
tides. This means that the effect of CEIs can be account- ed for by the suppression of angiotensin II formation or by a progressive accumulation of bradykinin II, or both.30 The intrarenal effects of endogenous-generated brady- kinin remains poorly defined.31 Consequently, most of the effects produced by CEIs are assumed to be due to the suppression of angiotensin II generation.32 This assump- tion has been adopted in the present review. Consequent- ly, it will be important to first examine the manner in which angiotensin II acts on renal hemodynamics and on renal tubular function, and to then see what effects could be expected by suppressing its formation.
0 50 100 150 200 250
RPP, mm Hg
has been demonstrated both in isolated renal tubule prep- arations and in the in vivo studies.41-44 On the luminal side, angiotensin II is rapidly destroyed by peptidases contained in the brush border.45
Figure 7 shows the regulatory effects of the renin- 3- angiotensin system on GFR and on urinary sodium excre-
tion during changes in renal perfusion pressure. It can be seen that an increase of renal perfusion pressure is accom- panied by a progressive vasoconstriction of glomerular
0 50 100 150 mo 250 afferent arterioles determined by the myogenic responses RPP, mm Hg of autoregulation and is independent of angiotensin II
lntrarenal actions of angiotensin II: It has been shown that the renin release from the kidney is proportional to the decrease in renal perfusion pressure,33 and that these increments of renin release are accompanied by a signifi- cant increase of angiotensin II concentration in the renal interstitium.34,35 In fact, Mendelsohn36 showed that the concentration of angiotensin II in the renal interstitium could achieve several orders of magnitude above that
FIGURE 9. Effect of converting enzyme inhibitors (CEI) on au- found in peripheral plasma. toregulation of glomendar filtration (GFR). Top, the afferent Intrarenal angiotensin II could exert 2 major effects. arteriole constriits in response to increases in renal perfusion pressure (RPP) but the eRerent arteriole remains dilated as a
The first is to produce a selective constriction of the
result of CEI. The net result of CEI administration (iboffom) is efferent glomerular vessels.37,38 This phenomenon has
a decrease in GFR (so/id line) at low RPP but liile difference been shown to occur in the cheek pouch of the hamster at high RPP. 6ecause of the efferent vasodilation, GFR rapidly where the application of angiotensin II to the adventitial decreases when RPP is decreased below the limit of autoregu- sites of glomerular transplanted vessels produce a greater liltlon. vasoconstriction in the efferent than in the afferent arteri-
ole.37 This demonstration is in agreement with the studies of Edwards38 who showed in microperfusion experiments that the efferent arterioles exhibited a higher response to the administration of angiotensin II than the afferent arterioles. The same effect has been demonstrated by Hall et al39,4o in total kidney preparations.
The second major effect of angiotensin II is the stimu- lation of sodium reabsorption by acting directly on the basolateral side of proximal tubule epithelium,41-44 which
nGURE 10. Effect of converting enzyme inhibitors (CEI) on sodium excretion. Top, the afferent arteriole constricts in re- sponse to increases in renal perfusion pressure (RPP) but the efferent arteriole remains dilated as a result of CEI. The net result of CEI administratiin (bottom) is an enhancement of natriuresis (so/id line) at low RPP but littie difference at high RPP. when RPP is decreased below the limit of autoregula- tion, the natriuresis is low because of the compromised glo- merular filtration rate by efferent vasodilatation.
646 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62
‘formation. Such a vasoconstriction is produced by an increase of Ca2+ flux into the smooth muscle of pre- glomerular vasculature, presumably through the activa- tion of stretch-sensitive Ca2+ channels.46 It has been hy- pothesized that Ca2+ flux into the modified smooth mus- cle cells of the juxtaglomerular apparatus is mediated by the same stretch-sensitive Ca2+ channels that are respon- sible for inhibiting renin release.46 This concept is impor-

tam because it explains the relation between the vasocon- strictor response of autoregulation and the decrease of renin release with respect to a given increase of renal perfusion pressure. 46 Because a decrease of renin release is accompanied by an equally proportional decrease in the concentration of angiotensin II in the renal interstitium,47 it follows that the autoregulatory-induced vasoconstrictor responses of afferent vasculature will be balanced by a proportional vasodilatation of efferent vasculature (Fig. 7). The opposite occurs when blood pressure is decreased; in this case, the autoregulatory pre-glomerular vasodila- tation will be accompanied by a proportional enhance- ment of angiotensin generation, which will produce a progressive vasoconstriction of the efferent arterioles (Fig. 7). In this respect, angiotensin plays a major hemo- dynamic role in the maintenance of GFR by adjusting efferent vascular resistance in an inverse proportion to the vascular tone of afferent vasculature.3g,40
When blood pressure is decreased, the enhanced an- giotensin II in the renal interstitium occupies more recep- tors in proximal tubules, favoring the reabsorption of sodium (Fig. 7); the opposite effect occurs when blood pressure is increased. However, it is not known if the reduction in sodium reabsorption that occurs during an increase of renal perfusion pressure is proportional to the reduction in the concentration of angiotensin II in the renal interstitium. Furthermore, the natriuretic response to changes in renal perfusion pressure is not only gov- erned by changes of angiotensin II in renal interstitium but also depends on the formation of prostaglandins from the renal medulla.48-51 The characteristics of this interre- lation have been previously discussed in details2
Renal effect of converting enzyme inhibitors: In con- sidering the aforementioned observations, the results of inhibiting the formation of angiotensin II can now be more clearly understood. As shown in Figure 8, the block- ade of angiotensin II formation at high levels of renal perfusion pressure would not result in an impairment or modification of renal plasma flow because the formation of angiotensin II is negligible and the glomerular efferent vasculature is maximally dilated. In contrast, an en- hancement of RBF could occur when CEI is given at normal or reduced levels of renal perfusion pressure. Un- der these conditions, removal of angiotensin II will result in efferent vasodilatation. However, the increments in RBF may be minimal because RBF is mainly dependent on the afferent vasculature which is unaffected by angio- tensin II. All these changes induced by CEI on RBF have been documented in a study by Navar et a1.22
The inhibition of angiotensin II formation can result in a significant impairment of GFR autoregulation (Fig. 9). At high levels of renal perfusion pressure, the inhibi- tion of angiotensin II formation will not have any effect on GFR since the formation is very low and the efferent arteriole is maximally vasodilated. In contrast, at low levels of renal perfusion pressure, GFR is mainly main- tained by the efferent arteriole constriction induced by angiotensin II. Hence, inhibition of angiotensin II results in a marked reduction of GFR. These effects have been shown by Hall et aP9,4o using total kidney preparation of normotensive animals. Under pathologic circumstances
such as renovascular hypertensions3 and cardiac insuffi- ciency,54 the removal of angiotensin II could produce a total cessation of the filtration process.
Finally, the manner in which CEIs affect pressure natriuresis is illustrated in Figure 10. At high levels of renal perfusion pressure, the administration of CEI will not produce major effects on sodium excretion since at these levels, the stimulatory actions of angiotensin II on proximal sodium reabsorption are minimal. However, as documented by Carmine et aLs5 at low levels of renal perfusion pressure within the range of autoregulation, the administration of CEI produces a marked enhancement of the pressure natriuresis. Although the removal of an- giotensin II at levels of renal perfusion pressure below the autoregulatory limit should result in larger increments of sodium excretion, the effect does not occur because GFR
THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5,1988 65G
Normotensives
0 n With caplopril
0 0 Without captopril
Hypertensives 42--
0 I I I I I I
70 60 90 ICNI 110 120 130
Mean blood pressure, mm Hg
FIGURE 11. Relation of urinary sodium excretion and mean blood pressure during volume expansion in 9 normotensive and 11 hypertensive subjects during a B-hour infusion of iso- tonic saline, before (open symbols) and after (closed symbok) the acute administration of a single 2%mg oral dose of capto- pril. The symbols represent the average urinary sodium excre- tion of the subjects at each of the l-hour time points during the 5 hours of and 1 hour after sodium overload in relation to arterial pressure (mean f standard error of the mean).
*
0 I I I I I I I I
control 2 4 6 Control 2 4 6
Time, hr
FIGURE 12. Changes in plasma renin activity (mean f stan- dard error of the mean) in 9 normotensfve and 11 hyperten- sive subjects before a S-hour infusion of saline (control), at 2 and 4 hours during the infusion, and 1 hour after (6 hour) the infusion. Open symbols, before; closed symbols, after the ad- ministration of captopril.

A SYMPOSIUM: CALCIUM, THE CARDIOVASCULAR SYSTEM AND THE KIDNEY
has been severely compromised by vasorelaxation of the sodium reabsorption. These speculations are supported efferent arteriole. by the observation that the alterations in renal hemody-
Comparative effects of CEI on renal hemodynamics namics can be corrected by the administration of CEI.60 in normotensive and hypertensive subjects cannot be per- From this consideration, the notion has emerged that for formed in the same manner as that used for calcium non-modulator hypertensives, with the initial disturbance antagonists. There is evidence that in 10 to 20% of the consisting of the lack of regulation of renin release or patients with essential hypertension, the levels of plasma generation of intrarenal angiotensin II, CEI could be the renin activity are increased above normal (high-renin best choice of treatment.60 However, beneficial actions of hypertension), whereas in 20 to 25% of the patients (vol- CEI on renal function can be derived from the effective ume-dependent hypertension), the levels of plasma renin blockade that these drugs exert on angiotensin II forma- activity are decreased. 56 The specific effects of CEI on tion, which increases when systemic blood pressure is renal function in each of these subpopulations have never reduced by vasodilators. This effect would effectively pre- been defined. However, CEI treatment has been prefer- vent sodium retention.2 Another important beneficial ef- entially indicated for the hypertensive patients with high- feet is that CEI can reduce systemic blood pressure and renin levels on the basis of increased sensitivity exhibited urinary sodium excretion with a mild reduction of glo- by this subpopulation to lower systemic blood pressure.57 merular capillary pressure. This decrease of glomerular
Relevant to the issue, Shoback et a15* reported that in capillary pressure, which will not be sufficient to impair a large number of essential hypertensives (40%), there is the process of filtration, has been shown to prevent glo- an inability to decrease the levels of plasma renin activity merular damage.61 during infusions of angiotensin II or during volume ex- In an attempt to see how the kidney with captopril pansion. From this finding, it has been speculated that alters urinary sodium excretion during volume expansion, in these patients (called “non-modulators”), there is an a study was conducted in 11 hypertensive and 9 normo- increased level of intrarenal angiotensin II that may favor tensive subjects in the same manner as that described for
Normotensives St- ,
Hypertensives
0 n With captopril
00 Without capiopril
nifedipine.-Both groups received an isotonic saline infu- sion of 500 ml/hour during 5 hours in the absence of any medication or after the acute administration of a single 25-mg oral dose of captopril.
FIGURE 13. Changes in plasma aldosterone levels (mean f standard error of the mean) in the same subjects during the same conditions described in Figure 12.
2 I I I I I I I I Control 2 4 6 Control 2 4 6
Time, hr
The relation between urinary sodium excretion with respect to the existing mean arterial pressure in the nor- motensive and hyperreactive hypertensive subjects before or during captopril treatment is shown in Figure 11. It can be seen that in the normotensive group, sodium load was accompanied by urinary sodium excretion that aver- aged 253 f 43 @cl/ min at blood pressure levels of 83 f 2 mm Hg. Administration of captopril facilitated urinary sodium excretion, which during a similar sodium load reached an average of 344 f 32 yEq/min without alter- ations in blood pressure (81 f 3 mm Hg). In the hyper- tensive group, sodium load induced a urinary sodium excretion of 342 f 63 yEq/min, at a blood pressure of 116 f 4 mm Hg. The administration of captopril de- creased blood pressure to 106 f 4 mm Hg. At this level,
r . Control n=4
n Nifedipine n=4
0 Nifedipine + CEI n=3 200 -
L Nifedipine + CEI + AIf n=3
g
s - 0 ‘ij -
l X=3.65 f 0.21 ml/min-g
20 40 60 60 100 120 140
RAP mmHg L
666 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62
FIGURE 14. Change in renal blood flow (RBF) in relation to renal perfusion pres- sure during control condition (closed ci~ c/es) and after treatment with nifedipine (closed squares), nifedipine + converting enzyme inhibition (CEI) (open circles), or nifedipine + converting enzyme inhibitors + angiotensin II (All) (c/osed triangles)).

THE AMERICAN JOURNAL OF CARDIOLOGY OCTOBER 5,1988 676
sodium load produced urinary sodium excretion of 247 f 57 pEq/min, which is not significantly lower than the excretory rates seen before captopril and is comparable to the excretory rates in normotensives without captopril, These results indicate that reduction of blood pressure by captopril does not impair urinary sodium excretion. How- ever, the natriuretic effect induced in normotensive and hypertensive subjects appears to be less pronounced than that induced by calcium antagonists (Fig. 2).
Captopril increased the basal level of plasma renin activity (Fig. 12) and reduced plasma aldosterone (Fig. 13) in both normotensive and hypertensive subjects. These initial alterations did not preclude a further sup- pressive action of sodium load on these 2 hormones.
Combined effects of calcium antagonists and con- verting enzyme inhibitors: Since simultaneous adminis- tration of CEIs and calcium antagonists are advocated for the treatment of severe reductions in hypertension,62 it is important to determine the simultaneous effect of both drugs on renal function. Such an attempt has been per- formed in normotensive dogs,22 but no studies in hyper- tensive animals or in normotensive or hypertensive hu- mans have been reported.
From the individual effects of each of these drugs, one could speculate that the suppression of angiotensin II after the administration of calcium antagonists may not produce any significant effect because the vasoconstrictor actions of angiotensin II have already been blocked by preventing the influx of calcium. However, Navar et a122 observed that the administration of calcium antagonists abolished RBF autoregulation (Fig. 14) and that subse- quent inhibition of angiotensin II by CEIs produced a further vasodilatation and a steeper slope in the pressure natriuresis curve. An infusion of angiotensin II reversed the effect of CEI. The investigators interpreted these results to indicate that part of the vasoconstrictor effects induced by angiotensin II are not due to the increase of calcium entry into the smooth muscle but are caused by mobilization of intracellular calcium. This latter effect was then unaffected by calcium antagonists and was re- sponsible for vasodilatation when formation of angioten- sin II was reduced by CEIs. However, such an interpreta- tion could be controversial in the sense that intracellular calcium stores may be rapidly depleted if they are not replenished by influx of extracellular calcium. This obser- vation may also suggest that after calcium-antagonist blockade, the subsequent removal of the constrictor effect of angiotensin II may result in a decrease in filtration if the reduction of intrarenal resistance is from efferent vasodilatation. This appears not to be the case because Navar et a122 showed that the administration of CEI in the presence of calcium blockade produced a significant decrease in blood pressure without significantly affecting RBF or GFR. Urinary sodium excretion was significant- ly decreased, but to a level deemed higher than that seen in untreated control dogs.
The potent vasodilator effects produced by a combi- nation therapy of calcium antagonists and CEI have also been observed in hypertensive patients.62,63 Unfortunate- ly, documentation on the pharmacokinetic effects pro-
duced by the administration of the 2 drugs was not ac- companied by parallel information on the effects of renal function.
Acknowledgment: We thank Paulette Peterson for her assistance in the preparation of the manuscript.
REFERENCES 1. Dollery CT. Hypertension and new antihypertensive drugs: clinical perspec- tives. Fed Proc 1983;42:207-210. 2. Hollenberg NK. The kidney and effective antihypertensive therapy. Am J Cardiol 1985;S6:52H-55H. 3. Romero JC, Raij L, &anger JP, Ruilope LM, Rodicio JL. Multiple effects of calcium entry blockers on renal function in hypertension. Hypertension 1987; 10:140~1s1. 4. Guyton AC, Coleman TG, Cowley AW Jr, Scheel KW, Manning RD Jr, Norman RA Jr. Arterial pressure regulation: overriding dominance of the kid- neys in long-term regulation and in hypertension. Am J Med 1972;52:584-594. 5. Abe Y, Komori T, Miura K, Takada T, Imanishi M, Okahara T, Yamamoto P. Effects of the calcium antagonist nicardipine on renal function and renin release in dogs. J Cardiovasc Pharmacol 1983;5:254-259. 6. Roy MW, Guthrie GP Jr, Holladay FP, Kotchen TA. Effects of verapamil on renin and aldosterone in the dog and rat. Am J Physiol 1983;254:E410-E416. 7. Bell AJ, Lindner A. Effects of uerapamil and nifedipine on renalfunction and hemodynamics in the dog. Renal Physiol 1984;7:329-343. 8. Yamaguchi I, Ikezawa K, Takada T, Kiyomoto A. Studies on a new 1,5- benzothiazepine derivative (CRD-401): VI. Effects on renal bloodflow and renal function. Jpn J Pharmncol 1974;24:511-522. 9. Abe Y, Yukimura T, Iwao H, Mori N, Okahara T, Yamamoto K. Effects of EDTA and uerpamil on renin release in dogs. Jpn J Pharmacol 1983;33:627- 633. 10. Dietz JR, Davis JO, Freeman RH, Villarreal D, Echtenkamp SF. Effects of intrarenal infusion of calcium entry blockers in anesthetized dogs. Hypertension 1983.5.482-488. 11. Burke TJ, Arnold PE, Gordon JA, Bulger RE, Dobyan DC, Schrier RW. Protective effect of intrarenal calcium membrane blockers before or after renal ischemia: functional, morphological, and mitochondriai studies. J Clin Irwest 1984:74:1830-l 841. 12. DiBona GF, Sawin LL. Renal tubular site of action offelodipine. J Pharma- col Exp Ther 1984;228:420-424. 13. Taylor A, Windhager EE. Possible role of cytosolic calcium and Na-Ca exchange in regulation of tranwpithelial sodium transport. Am J Physiol 1979:236:FS05-F512. 14. McLaughlin M, de Mello Aires M, Malnic G. Verapamil effect on renal function of normotensive and hypertensive rats. Renal Physiol1985;8:112-119. 15. Figueiredo JF, Conti GT, Falkenstein D, Sigulem D, Ramos OL. Tetrocaine, procaine and verapamil inhibition offluid absorption in isolated perfused rabbit proximal convoluted tubules. Braz J Med Biol Res 1982;15:259-264. 16. Sakurai T, Kurita T, Nagano S, Sonoda T. Antihypertensive vasodilating and sodium diuretic actions of D-eis isomer of benzothiazepine derivative (CRD- 401). Acta Biol Jpn 1972;18:695-701. 17. Leonetti G, Cuspidi C, Sampieri L, Terzoli L, Zanchetti A. Comparison of cardiovascular, renal, and humoral effects of acute administration of two calci- um channel blockers in normotensive and hypertensive subjects. J Cardiovasc Pharmacol 1982:4:suppl3:319-323. 18. Yokoyama S, Kaburagi T. Clinical effects of intravenous nijedipine on renal
function. J Cardiovasc Pharmacol 1983;5:67-71. 19. Van Schaik BAM, Van Nistelrooy AEJ, Geyskes GG. Antihypertensive and renal effects of nicardipine. Br J Clin Pharmncol 1984;18:57-63. 20. Wallia R, Greenberg A, Puschett JB. Renal hemodynamic and tubular transport effects of nitrendipine. J Lab Clin Med 1985;105:498-503. 21. Loutzenhiser R, Epstein M. Effects of calcium antagonists on renal hemody- namics. Am J Physiol 1985;249:F619-F629. 22. Navar LG, Champion WJ, Thomas CE. Effects of calcium channel blockade on renal vascular resistance responses to changes in perfusion pressure and angiotensin-converting enzyme inhibition in dogs. Circ Res 1986;58:874-881. 23. Ono H, Kokubun H, Hashimoto K. Abolition by calcium antagonists ofthe autoregulation of renal blood jlow. Naunyn Schmiedebergs Arch Pharmacol 1974;285:201&207. 24. Cohen AJ, Fray JCS. Calcium ion dependence of myogenic renal plasma flow autoregulatiom evidence from the isolated perfused rat kidney. J Physiol [Lmd] 1982;330:449-460. 25. Hollenberg NK, Borucki LJ, Adams DF. The renal vasculature in early essential hypertension: evidence for a pathogenic role. Medicine [Baltimore] 1978;57:167-178. 26. Blackshear JL, Garnic D, Williams GH, Harrington DP, Hollenberg NP. Exaggerated renal uasodilator response to calcium entry blockade in&t-degree relatives of essential hypertensive subjects. Hypertension 1987;9:384-389.

A SYMPOSIUM: CALCIUM, THE CARDIOVASCULAR SYSTEM AND THE KIDNEY
27. Ondetti MA, Williams NJ, Sabo EF, Pluscec J, Weaver ER, Kocy 0. Angiotenrin colwerting enzyme inhibitors from the venom of Bothrops jararaca. Isolation, elucidation of structure, and synthesis. Biochemistry 1971;10:4033- 4039.
lar cells, and hypertension: role of physical equilibrium and Ca. Am J Physiol 1986;251:R643-R662. 47. Mendelsohn FA. Angiotensin II: evidence for its role as an intrarenal hor- mone. Kidney Int 1982:22:S78-.%?I.
28. Yang HYT, Erdos EG, Levin Y. A dipeptide carboxypeptidase that converts 48. Zenser TV, Herman CA, Davis B. Effects of calcium and A23187 on renal angiotensin I and inactivates bradykinin. Biochim Biophys Acta 1970:214:374- inner medullary prostaglandinr E> synthesis. Am J Physiol 1980:238:E371- 376. E376. 29. Yang HYT, Erdos EG, Levin Y. Characterization of a dipeptide hydrolase (kininase II: angiotensin I converting enzyme). J Pharmacoi Exp Ther 1971: 177:291-300.
49. Craven PA, DeRubertis FR. Calcium-dependent stimulation of renal med- ullary prostaglandin synthesis by furosemide. J Pharmacol Exp Ther 1982;222: 306-314.
30. Erdos E. Angiotensin I converting enzyme. Circ Res 1975;36:247-255. 3 1. Scicli AG, Carretero OA. Renal kallikrein system. Kidney Int 1986;29:120- 130. 32. Case DB, Wallace JM, Keim HJ, Weber MA, Sealey JE, Laragh JH. Possible role of renin in hypertension as suggested by renin-sodium profiling and inhibition of converting enzyme. N Engl J Med 1977;296:641-646. 33. Blackshear JL, Spielman WS, Knox FG, Romero JC. Dissociation of renin release and renal uasodilatation by prostaglandin synthesis inhibitors. Am J Physiol 1979;237:F20-F24, 34. Proud D, Nakamura S, Carone FA, Herring PL, Kawamura M, Inagami T, Pisano 53. The kallikrein-kinin and renin-angiotensin system in rat renal lymph. Kidney Int 1986;25:880-885. 35. Bailie MD, Rector FC Jr, Seldin DW. Angiotensin II in arterial and renal venous plasma and renal lymph in the dog. J Clin Invest 1971:50:119-126. 36. Mendelsohn FA. A methodfor measurement of nngiotensin II in tissues and its application to rat kidney. Clin Sri Mel Med 1976;51:11 l-l 25. 37. Navar LG, Gilmore JP, Joyner WL, Steinhausen M, Edwards RM, Casellas D, Carmines PK, Zimmerhackl LB, Yokota SD. Direct assessment of renal microcirculatory dynamics (Symposium Report). Fed Proc 1986;45:2851-2861. 38. Edwards RM. Segmental effects of norepinephrine and angiotensin II on isolated renal microvessels. Am J Physiol 1983;244:F526-F534. 39. Hall JE, Coleman TG, Guyton AC, Balfe JW, Salgado HC. Introrenal role of angiotensin II and [des-Asp’] angiotensin II. Am J Physioi 1979;236A:F252- F259.
59. Craven PA, Studer RK, DeRubertis FR. Renal inner medullary prostaglan- din synthesis. J Clin Invest 1981:68:722-732. 51. Kirschenbaum MA, Lowe AG, Trizna W, Fine LG. Regulation of oasopres- sin action by prostaglandins. Evidence for prostaglandin synthesis in the rabbit cortical collecting tubule. J Clin Itwest 1982;70:1193-1204. 52. Romero JC, Knox FG. Mechanisms underlyingpressure natriuresis. Hyper- tension 1988;11:724-738.
40. Hall JE, Guyton AC, Jackson TE, Coleman TG, Lohmeier TE, Trippodo NC. Control of glomerular filtration rate by renin-angiotensin system. Am J Physiol 1977;233:F366-F372. 41. Harris PJ, Young JA. Dose-dependent stimulation and inhibition of proxi- mal tubular sodium reabsorption by angiotensin II in the rat kidney. Pfugers Arch 1977;367:295-297. 42. Huang WC, Ploth DW, Navar LG. Angiotensin-mediated alterations in nephron function in Goldblatt hypertensive rats. Am J Physiol1982;243:F553- F.560.
53. Johnston CI, Jackson B. Overview: angiotensin converting enzyme inhibition in renovascular hypertension. Kidney Int 1987:31:154-l 56. 54. Dzau VJ. Renin-angiotensin system and renal circulation in clinical conges- tive heart failure. Kidney Int 1987:31:203-209. 55. Carmines PK. Bell PD, Roman RJ, Work J, Navar LG. Prostaglandins in the sodium excretory response to altered renal arterial pressure in dogs. Am J Physiol 1985:248:F8-F14. 56. Brunner HR, Sealey JE, Laragh JH. Renin subgroups in essential hyperten- sion: Further analysis of their pathological and epidemiological characteristics. Circ Res 1973;32-33:wppl:99-I 09. 57. Gavras H, Ribeiro A, Brunner HR, Gavias I. Reciprocal relationships between renin dependency and sodium dependency in essential hypertension. N Engl J Med 1976:295:1278-l 283. 58. Shoback DM, Williams GH, Moore TJ, Dluhy RG, Podolsky S, Hollenberg NK. Defect in the sodium-modulated tissue responsiveness to angiotensin II in essential hypertension. J Clin Invest 1983;72:2115-2124. 59. Hollenberg NK, Moore T, Shoback D, Redgrave J, Rabinowe S, Williams GH. Abnormal renal sodium handling in essential hypertension relation to failure of renal and adrenal modulation of response to angiotensin II. Am J Med 1986;8:412-418.
43. Pelayo JC, Blantz RC. Analysis of renal denervation in the hydropenic rat: Interactions with angiotensin II. Am J Physiol 1984;246:F87-F95. 44. Steiner RW, Tucker BJ, Blantz RC. Glomerular hemodynamics in rats with chronic sodium depletion. Effect of saralasin. J Chin Invest 1979;64:503-512. 45. Schuster VL, Kokko JP, Jacobson HR. Angiotensin II directly stimulates sodium transport in rabbit proximal convoluted tubules. J Clin Invest 1984; 73:507-515. 46. Fray JCS, Lush DJ, Park CS. Interrelationship of bloodflow, juntagiomeru-
60. Hollenberg NK, William GH. Sensitivity to sodium and non-modulation of renal and adrenal responses to angiotensin II: implications for the pathogen&s of essential hypertension. In: Austria E, ed. Pathophysiology of Hypertension Regulatory Mechanism. Amsterdam: Elsevier, 1986:1520-1552. 61. Raij L, Chiou X-C, Owens R, Wrigley B. Therapeutic implications of hypertension-induced glomerular injury: comparison of ennlapril and a combi- nation of hydralazine, reserpine, and hydrochlorothiaride in an experimental model. Am J Med 1985;79:suppl 3C:37-41. 62. White WB, Viadero JJ, Lane TJ, Podesla S. Effects of combination therapy with captopril and nifedipine in severe or resistant hypertension. Clin Pharmacol Ther 1986;39:43-48. 63. Donnelly R, Elliott HL, Meridith PA, Reid JL. An evaluation of thepharma- codynamics and pharmacokinetics of nicardipine combined with enalapril in essential hypertension. J Cardiovasc Pharmacol 1987;10:723-727.
68G THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 62