
Comparison of Stroke Guidelines: - Karger
32
Europe/Japan Stroke Research Cooperation presents: Comparison of Stroke Guidelines: Similarities and Differences between Japanese and European Recommendations for the Management and Prevention of Acute Ischemic and Hemorrhagic Strokes www.karger.com/ced
Transcript of Comparison of Stroke Guidelines: - Karger

Europe/Japan Stroke Research Cooperation presents:
Comparison of Stroke Guidelines:Similarities and Differences between Japanese and European
Recommendations for the Management and Prevention of Acute Ischemic and Hemorrhagic Strokes
www.karger.com/ced
CED_comp_U1.indd 1 23.05.2013 11:08:21

E-Mail [email protected]
Editorial
Cerebrovasc Dis 2013;35:399–401 DOI: 10.1159/000351406
Comparison of Stroke Guidelines:Similarities and Differences betweenJapanese and European Recommendationsfor the Management and Prevention ofAcute Ischemic and Hemorrhagic Strokes
Michael G. Hennerici a Yukito Shinohara b
a Department of Neurology, UMM, University of Heidelberg, Mannheim , Germany; b Department of Neurology, Federation of National Public Service Personnel Mutual Aid Associations Tachikawa Hospital, Tokyo , Japan
and generally used drug dosages are different in Japan as compared with other American or European countries and vice versa, (2) there may be racial differences, and (3) there have been many publications concerning stroke therapy in Japan, not written in English, which have not been taken into consideration in the development of western stroke GLs. These timely associations and the joint conviction of evidence-based backgrounds for regu-lated treatment on one side and best medical insight into pathomechanisms in the absence of such data challenged an improved mutual cooperation among European and Japanese stroke clinicians.
Since then, the authors of the following articles met re-peatedly and compared the latest versions of the European and Japanese GLs for ischemic and hemorrhagic strokes. From the beginning, we were well aware about the impor-tant differences in structure, style, history and interests that members of the original writing committees in Eu-rope and Japan might have had – as a result, many aspects have only been addressed in one but left out in the other GL, which consequently founded the basis for the com-parison tables and chapters listed in the following two ar-ticles. Aspects of major importance were surprisingly sim-ilar, and hence did not need extensive interpretation even though the classification of evidence levels and recom-
Cerebrovascular Diseases celebrated its 20th anniver-sary in 2010 with a Europe/Japan Stroke symposium in Barcelona, Spain, 20 years after the first European Stroke Conference . The session addressed different aspects of acute stroke management and strategies for stroke pre-vention from two viewpoints with specific traditional and historical backgrounds in modern neurovascular medi-cine, Europe and Japan [1] .
During this meeting, speakers and participants in a large auditorium experienced a surprisingly high coinci-dence of identical or very close proposals and perspec-tives as well as less common but remarkable differences.
Cerebrovascular Diseases had published the 2003 Eu-ropean guidelines (GLs) for the management of ischemic stroke and transient ischemic attacks [2] with an update in 2008 [3] , the European stroke initiative recommenda-tions for the management of ICH in 2006 [4], and very recently, the guidelines for the management of intracra-nial aneurysms and subarachnoid hemorrhage (2013) [5] , based on western evidence. On the other hand, the first English version of Japanese GLs for the management of stroke were published in 2011 [6] , although the first Japanese GLs for the management of stroke appeared in 2004 in Japan [7, 8] . The reasons why Japan made their own GLs are as follows: (1) some of the approved drugs
Received: May 6, 2013 Accepted: May 7, 2013 Published online: May 22, 2013
Prof. Michael G. Hennerici Department of Neurology, UniversitätsMedizin Mannheim University of Heidelberg Theodor-Kutzer-Ufer 1–3, DE–68167 Mannheim (Germany) E-Mail Hennerici @ neuro.ma.uni-heidelberg.de
© 2013 S. Karger AG, Basel1015–9770/13/0355–0399$38.00/0
www.karger.com/ced

Hennerici /ShinoharaCerebrovasc Dis 2013;35:399–401DOI: 10.1159/000351406
400
mendation grades defined by the individual committees differed between both original GLs ( tables 1 , 2 ).
Interestingly, some aspects of ischemic stroke man-agement differed significantly, e.g. the dosage of recom-binant tissue plasminogen activator approved in Japan is lower (0.6 mg/kg) than in Europe (0.9 mg/kg), which de-rived from different customs in cardiovascular treatment prior to the design of acute ischemic stroke trials. Fur-thermore, comedication with neuroprotective agents
(edaravon), intravenous anticoagulant (argatroban) or antiplatelet agents within 1–2 days after stroke onset is recommended in Japan but not in Europe. For cardioem-bolic stroke prevention, a major difference consists in a higher target international normalized ratio (2.0–3.0) in younger subjects versus those >70 years (1.6–2.6), with-out age restrictions in Europe.
Patients with hemorrhagic stroke/intracerebral bleed-ings were treated surgically – in the absence of clear evi-
Table 1a. Classification of evidence levels of stroke (Japan)
Level of evidence
Type of evidence
Ia Meta-analysis (with homogeneity) of RCTsIb At least one RCTIIa At least one well-designed, controlled study but without randomizationIIb At least one well-designed, quasi-experimental studyIII At least one well-designed, nonexperimental descriptive study
(e.g. comparative/correlation/case study)IV Expert committee reports, opinions, and/or experience of respected authorities
This Japanese Guidelines classification was established based on the classification in the National Clinical Guidelines for Stroke (1999) adopted by the UK Royal College of Physicians, with a partial adoption of proposals by the Oxford Center for Evidence-Based Medicine (2001). RCT = Randomized controlled trial.
Table 1b. Classification of evidence levels on stroke (Europe)
Level ofevidence
Classification scheme for a therapeutic intervention
I An adequately powered, prospective, clinical RCT with masked outcome assessment in a representative population or an adequately powered systematic review of prospective, clinical RCTs with masked outcome assessment in representative populations.The following are required:(a)(b) (c)(d)
(e)
randomized concealmentprimary outcome(s) is/are clearly definedexclusion/inclusion criteria are clearly definedadequate accounting for dropouts and crossovers with numbers sufficiently low to have a minimal potential for bias relevant baseline characteristics are presented and substantially equivalent among treatment groups or there is appropriate statistical adjustment for differences
II Prospective matched-group cohort study in a representative population with masked outcome assessment that meets a–e above or RCT in a representative population that lacks one criterion of a–e
III All other controlled trials (including well-defined natural history controls or patients serving as own controls) in a representative population, where outcome assessment is independent of patient treatment
IV Evidence from uncontrolled studies, case series, case reports, or expert opinion
RCT = Randomized controlled trial.

Comparison of Stroke Guidelines Cerebrovasc Dis 2013;35:399–401DOI: 10.1159/000351406
401
dence-based recommendations worldwide – more often depending on the association with hypertension in Japan but not in Europe. Infra- and supratentorial differences were similarly addressed in both regions. However, due to lacking evidence from appropriate trials, patients with large or intraventricular bleedings were only treated if life-saving performance was considered irrespective of neurological outcome – thus treatment of patients in ap-propriate randomized clinical trials is frequently recom-mended in Europe and Japan, but often with different concepts and study designs in participating centers.
We hope that this brief survey – when compared with the lengthy original recommendations – provides a stimu-lating basis for an extended interest among Japanese and European stroke clinicians to learn from their individual experiences and to strengthen efforts for a joint coopera-tion in treating and preventing stroke all around the globe.
The next Europe/Japan Stroke symposium is planned to take place at the European Stroke Conference 2014 in Nice, France
Table 2. Grades of Recommendation
Japanese guidelines European guidelines (ESO)
Grade A: Implementation is highly recommended (based on Ia or at least one datum-rated level Ib).
Level A: Established as useful/predictiveor not useful/predictive for a diagnostic measure or established as effective, ineffective or harmful for a therapeutic intervention; requires at least one convincing class I study or at least two consistent, convincing class II studies.
Grade B: Implementation is recommended (based on at least one datum-rated level II).
Level B: Established as useful/predictiveor not useful/predictive for a diagnostic measure or established as effective, ineffective or harmful for a therapeutic intervention; requires at least one convincing class II study or overwhelming class III evidence.
Grade C1: Implementation can be considered, but it lacks an adequate scientific basis.
Level C: Established as useful/predictiveor not useful/predictive for a diagnostic measure or established as effective, ineffective or harmful for a therapeutic intervention; requires at least two class III studies.
Grade C2: It is not recommendable because of a lack of scientific evidence.
Good Clinical Practice (GCP) points: Recommended best practice based on the experience of the guideline development group. Usually based on class IV evidence indicating large clinical uncertainty, such GCP points can be useful for health workers.
Grade D: Implementation is not recommended.
References
1 Hennerici MG, Minematsu K: Journal anni-versary symposium 2010 dedicated to Europe/Japan stroke research cooperation. Cerebro-vasc Dis 2010; 30: 537–539.
2 European Stroke Initiative Executive Com-mittee, EUSI Writing Committee, Olsen TS, Langhorne P, Diener HC, Hennerici M, Ferro J, Sivenius J, Wahlgren NG, Bath P: Europe-an Stroke Initiative Recommendations for Stroke Management-update 2003. Cerebro-vasc Dis 2003; 16: 311–337.
3 European Stroke Organisation (ESO) Execu-tive Committee: Guidelines for managementof ischaemic stroke and transient ischaemic at-tack 2008. Cerebrovasc Dis 2008; 25: 457–507.
4 Steiner T, Kaste M, Forsting M, Mendelow D, Kwiecinski H, Szikora I, Juvela S, Marchel A, Chapot R, Cognard C, Unterberg A, Hacke W: Recommendations for the management of in-tracranial haemorrhage – part I: spontaneous intracerebral haemorrhage. The European Stroke Initiative Writing Committee and the Writing Committee for the EUSI Executive Committee. Cerebrovasc Dis 2006;22:294–316.
5 Steiner T, Juvela S, Unterberg A, Jung C, Forst-ing M, Rinkel G: European stroke organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage. Cerebrovasc Dis 2013; 35: 93–112.
6 The Joint Committee on Guidelines for the Management of Stroke for the English Ver-sion: Japanese Guidelines for the Manage-ment of Stroke 2009. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S1–S209.
7 Joint Committee on Guidelines for the Man-agement of Stroke, Shinohara Y, et al (eds): Japanese Guidelines for the Management of Stroke 2004 (in Japanese). Tokyo, Kyowa Ki-kaku, 2004, pp 1–233.
8 Shinohara Y, Yamaguchi T: Outline of the Japanese Guidelines for the Management of Stroke 2004 and subsequent revision. Int J Stroke 2008; 3: 55–62.

E-Mail [email protected]
Comparison of the European and Japanese
Guidelines for the Management of Ischemic
Stroke
Rolf Kern a Masao Nagayama b Kazunori Toyoda c Thorsten Steiner d, e
Michael G. Hennerici a Yukito Shinohara f
a Department of Neurology, UMM, University of Heidelberg, Mannheim , Germany; b Departments of Neurology and Rehabilitation, and the Center for Stroke and Neurocritical Care, International University of Health and Welfare Atami Hospital, Atami , and c Department of Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan; d Department of Neurology, Klinikum Frankfurt Höchst, Frankfurt, and e Department of Neurology, University of Heidelberg Hospital, Heidelberg, Germany; f Department of Neurology, Federation of National Public Service Personnel Mutual Aid Associations Tachikawa Hospital, Tokyo , Japan
Guidelines
Cerebrovasc Dis 2013;35:402–418 DOI: 10.1159/000351753
Received: May 6, 2013 Accepted: May 7, 2013 Published online: May 23, 2013
Dr. Rolf KernDepartment of NeurologyUniversitätsMedizin Mannheim, University of HeidelbergTheodor-Kutzer-Ufer 1-3, DE-68167 Mannheim (Germany)E-Mail [email protected]
© 2013 S. Karger AG, Basel1015–9770/13/0355–0402$38.00/0
Since 2011, the authors have met repeatedly and have com-pared the latest versions of published European and Japa-nese GLs for ischemic and hemorrhagic strokes. Many as-pects have only been addressed in one but left out in the other GLs, which consequently founded the basis for the comparison. Classification of evidence levels and recom-mendation grades defined by the individual committees differed between both original GLs. Results: Aspects of ma-jor importance were surprisingly similar and hence did notneed extensive interpretation. Other aspects of ischemic stroke management differed significantly, e.g. the dosage of recombinant tissue plasminogen activator approved in Ja-pan is lower (0.6 mg/kg) than in Europe (0.9 mg/kg), which derived from different practices in cardiovascular treatment prior to the design of acute ischemic stroke RCTs. Further-more, comedication with neuroprotective agents (edara-vone), intravenous anticoagulants (argatroban) or antiplate-let agents within 1–2 days after stroke onset is recommend-ed in Japan but not in Europe. For cardioembolic stroke prevention, a major difference consists in a higher interna-tional normalized ratio target (2.0–3.0) in younger subjects versus in those >70 years (1.6–2.6), without age restrictions
Key Words
Acute stroke treatment · European stroke guidelines · Evidence-based medicine · Ischemia · Japanese stroke guidelines · Randomized clinical trials · Review · Stroke prevention
Abstract
Background: Different aspects of acute stroke management and strategies for stroke prevention derive from two view-points: specific traditional and historical backgrounds and evidence-based medicine from modern randomized con-trolled trials (RCTs), meta-analysis and authorized clinical practice guidelines (GLs). Regarding stroke, GLs have been published by national and international organizations in dif-ferent languages, most frequently in English. Cerebrovascu-lar Diseases published the European GLs for the manage-ment of ischemic stroke and transient ischemic attacks in 2003, with an update in 2008. At about the same time (in 2004), the first Japanese GLs for the management of stroke appeared in Japanese. The first English version of the up-dated Japanese GLs was published only in 2011 and includ-ed differently approved drugs and drug dosages as com-pared with other American or European countries. Methods:
www.karger.com/ced
R.K and M.N. contributed equally to this work.

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
403
in Europe. Conclusion: This brief survey – when compared with the lengthy original recommendations – provides a stimulating basis for an extended interest among Japanese and European stroke clinicians to learn from their individual experiences and to strengthen efforts for joint cooperation in treating and preventing stroke all around the globe.
Copyright © 2013 S. Karger AG, Basel
Reflecting the introduction of evidence-based medi-cine to clinical science, authorized clinical practice guide-lines (GLs) regarding stroke have been published since 1994 by the American Heart Association (AHA), the Roy-al College of Physicians and the European Stroke Organi-zation (ESO), for example. In Japan, evidence-based comprehensive GLs on cerebrovascular diseases were published in 2004 and 2009 from the Japan Stroke Soci-ety, but only in Japanese. In response to the request for the English version, considering the differences in race, stroke types, subtypes and drugs authorized, high mor-bidity and mortality of cerebrovascular disorders in Asian countries, which exceed those of myocardial infarction, and, also, the vast amount of untranslated Japanese lit-erature, the English version of the entire Japanese GLs were first published in 2011 [1–7] . The purpose of this article is to compare the latest versions of the European and Japanese GLs for the management of ischemic stroke.
We compared the GLs, especially Recommendations of ESO GLs 2008 [8] and the 2009 update [9] , with those of the Japanese GLs 2009 (English version in 2011 [1–7] ). We tried to clarify the differences and similarities of both GLs and worked out which recommendations lacked in both GLs. Although Japanese GLs are comprehensive and even include asymptomatic cerebrovascular diseases and specific conditions which cause stroke and rehabilitation, for example, only those GLs relevant to the management of ischemic stroke were extracted from the entire chap-ters. For readers’ convenience, 7 comparison tables were created, which integrate recommendations of both GLs for the management of ischemic stroke. Grades of recom-mendation of both GLs are shown and discussed in the Editorial.
Management of Acute Ischemic Stroke
Referral and Patient Transfer GLs on prehospital care were described only in the Eu-
ropean GLs. In Japan, official GLs on prehospital care
were described in the ‘neuroresuscitation GLs’ (cochaired by Masao Nagayama and Hiroshi Okudera) by the Japan Resuscitation Council [ 10 , English version in prep.]. Although there is little remarkable difference between both GLs, telemedicine was recommended in remote orrural areas in the European GLs (level B). Regarding the prehospital head positioning, Japanese neuroresuscita-tion GLs recommended to avoid the head-up position (class IIb) based on a study indicating that flat positioning improves blood flow velocity in acute ischemic stroke [11] . Regarding the prehospital stroke scale, both GLs did not recommend a specific scale, although Japanese GLs listed the Cincinnati Prehospital Stroke Scale, Los Ange-les Prehospital Stroke Screen, Melbourne Ambulance Stroke Screen and Kurashiki Prehospital Stroke Scale as potential candidates (class IIa).
Emergency Diagnostic Workup GLs on an emergency diagnostic workup were de-
scribed only in the European GLs. In Japan, official GLs on this issue were described in the neuroresuscitation GLs [10] . There is little remarkable difference between both GLs. In the European GLs, the inclusion of diffu-sion-weighted imaging and T2 * -weighted gradient echo sequences was recommended if the required MRI device is available (level A). Japanese neuroresuscitation GLs strengthened the importance of screening acute cardiac diseases and aortic dissection (class I).
Stroke Care Unit and Stroke Unit In the recent Helsingborg Declaration, acute orga-
nized stroke unit (SU) care was described as the backbone of the chain of care for all European stroke victims. In 2013, the ESO Stroke Unit Certification Committee de-fined evidence-based requirements for SU and announced the recommendations to establish a SU and Stroke Center [23] . On the other hand, in Japan, stroke care unit often refers to a ward in which advanced intensive care is pro-vided to acute stroke patients in an unstable condition: in other words an intensive care unit specializing in stroke.
The SU signifies a ward in which a stroke team, which is composed of staff with different types of comedical skills, provides a constant and consistent range of thera-pies, including the treatment of acute phase stroke to re-habilitation; SUs are common in Europe. Both GLs rec-ommended SUs (grade A, level A) for patients with all types of stroke (European GLs) or acute stroke excluding subarachnoid hemorrhage, lacunar infarction, deep coma and poor activities of daily living before onset (Japanese GLs; table 1 ).

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
404
Table 1. General management of acute ischemic stroke
Japanese guidelines European guidelines (ESO)
Stroke care unit and SU
For patients with acute stroke, excluding subarachnoid hemorrhage, lacunar infarction, deep coma and poor activities of daily living before onset, treatment at a SU, which is a ward specializing in stroke and at which medical staff specialized in stroke systematically and prospectively perform intensive treatment and rehabilitation starting from an early stage under monitoring, can reduce the mortality and the duration of hospitalization, increase the rate of discharge for home care and improve the long-term activities of daily living and quality of life (grade A).
(1) It is recommended that all stroke patients should be treated in a SU (class I, level A).(2) It is recommended that healthcare systems ensure that acute stroke patients have access to high technology medical and surgical stroke care when required (class III, level B).
Management fromthe hyperacute to the acute phase of stroke(1) General(2) Respiration
(1) There is no scientific evidence that routine oxygen administration to mild-to-moderate stroke patients without obvious hypoxemia is useful (grade C2). (2) Airway management and artificial respiratory management are desirable for patients with acute-phase stroke in whom a respiratory disorder is likely to cause any disturbance in consciousness (grade C1).
(1) Intermittent monitoring of neurological status, pulse, blood pressure, temperature and oxygen saturation is recommended for 72 h in patients with significant persisting neurological deficits (class IV, GCP).(2) Regular monitoring of fluid balance and electrolytes is recommended in patients with severe stroke or swallowing problems (class IV, GCP).(3) Normal saline (0.9%) is recommended for fluid re place-ment during the first 24 h after stroke (class IV, GCP). (4) It is recommended that oxygen should be administered if the oxygen saturation falls below 95% (class IV, GCP).
(3) Blood pressure (1) The management of hypertension immediately after the onset of stroke can be initiated after a diagnosis of stroke subtype was made, except for the case where hypertensive encephalopathy or subarachnoid hemorrhage is highly suspected. Also, before using hypotensive drugs, it should be ascertained whether increased blood pressure could be due to pain, nausea or a full bladder. In contrast, marked hypotension (shock) should be promptly corrected with infusion and/or hypertensive drugs (grade C1). (2) For acute-phase cerebral infarction, careful antihypertensive therapy is recommendable only when hypertension persists with a systolic blood pressure of >220 mm Hg or a diastolic blood pressure of >120 mm Hg, or concurrent aortic dissection, acute myocardial in-farction, heart failure or renal failure is present (grade C1).
(1) Routine blood pressure lowering is not recommended following acute stroke (class IV, GCP). (2) Cautious blood pressure lowering is recommended in patients with extremely high blood pressure (>220/120 mm Hg) on repeated measurements, or with severe cardiac failure, aortic dissection or hypertensive encephalopathy (class IV, GCP).(3) It is recommended that abrupt blood pressure lowering be avoided (class II, level C).
(4) Glucose control, nutrition
(1) Hyperglycemia or hypoglycemia should be corrected immediately (grade B). (2) Nutrition supplementation to ensure adequate calories and protein intake is recommendable for patients with malnutrition (grade B).
(1) Monitoring serum glucose levels is recommended (class IV, GCP). (2) Treatment of serum glucose levels >180 mg/dl (>10 mmol/l) with insulin titration is recommended (class IV, GCP). (3) It is recommended that severe hypoglycemia [<50 mg/dl (<2.8 mmol/l)] should be treated with intravenous dextrose or infusion of 10 – 20% glucose (class IV, GCP points).(4) Oral dietary supplements are only recommended for nondysphagic stroke patients who are malnourished (class II, level B).(5) Early commencement of nasogastric feeding (within 48 h) is recommended in stroke patients with impaired swallowing (class II, level B).(6) It is recommended that percutaneous enteral gastrostomy feeding should not be considered in stroke patients in the first 2 weeks (class II, level B).
Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
405
Japanese guidelines European guidelines (ESO)
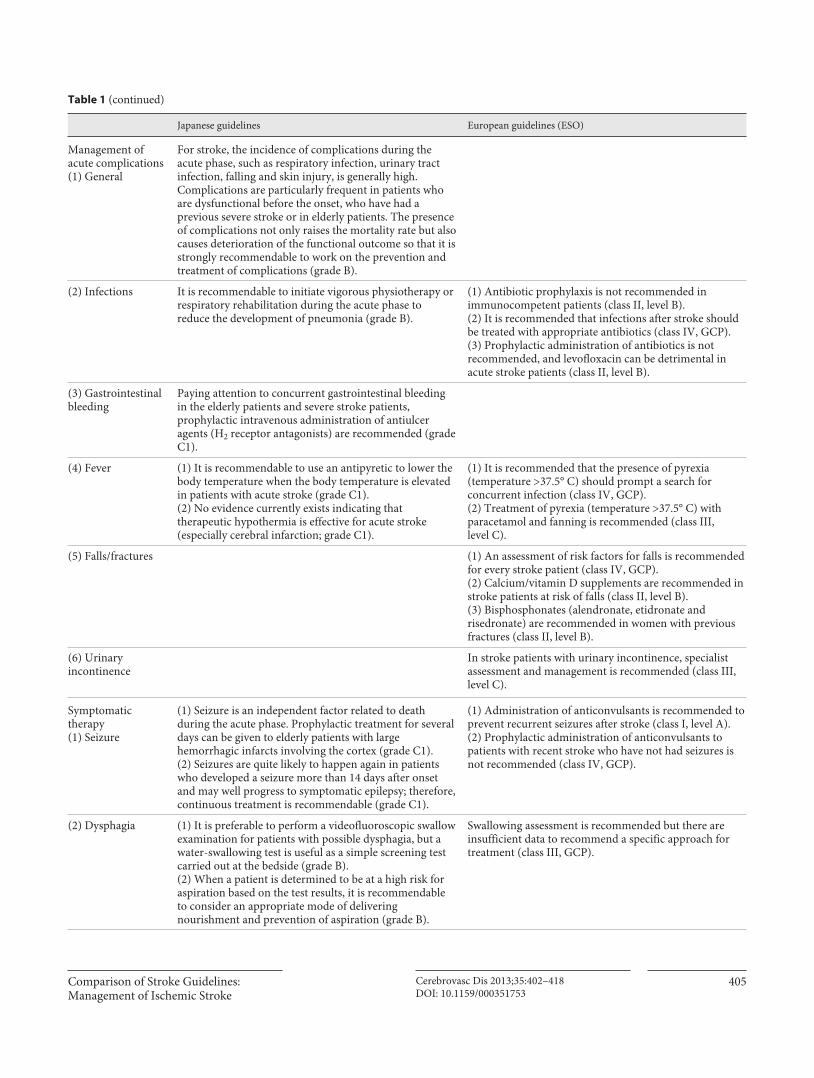
Management ofacute complications(1) General
For stroke, the incidence of complications during the acute phase, such as respiratory infection, urinary tract infection, falling and skin injury, is generally high. Complications are particularly frequent in patients who are dysfunctional before the onset, who have had a previous severe stroke or in elderly patients. The presence of complications not only raises the mortality rate but also causes deterioration of the functional outcome so that it is strongly recommendable to work on the prevention and treatment of complications (grade B).
(2) Infections It is recommendable to initiate vigorous physiotherapy or respiratory rehabilitation during the acute phase to reduce the development of pneumonia (grade B).
(1) Antibiotic prophylaxis is not recommended in immunocompetent patients (class II, level B).(2) It is recommended that infections after stroke should be treated with appropriate antibiotics (class IV, GCP). (3) Prophylactic administration of antibiotics is not recommended, and levofloxacin can be detrimental in acute stroke patients (class II, level B).
(3) Gastrointestinal bleeding
Paying attention to concurrent gastrointestinal bleeding in the elderly patients and severe stroke patients, prophylactic intravenous administration of antiulcer agents (H2 receptor antagonists) are recommended (grade C1).
(4) Fever (1) It is recommendable to use an antipyretic to lower the body temperature when the body temperature is elevated in patients with acute stroke (grade C1). (2) No evidence currently exists indicating that therapeutic hypothermia is effective for acute stroke (especially cerebral infarction; grade C1).
(1) It is recommended that the presence of pyrexia (temperature >37.5° C) should prompt a search for concurrent infection (class IV, GCP).(2) Treatment of pyrexia (temperature >37.5° C) with para cetamol and fanning is recommended (class III, level C).
(5) Falls/fractures (1) An assessment of risk factors for falls is recommended for every stroke patient (class IV, GCP). (2) Calcium/vitamin D supplements are recommended in stroke patients at risk of falls (class II, level B). (3) Bisphosphonates (alendronate, etidronate and risedronate) are recommended in women with previous fractures (class II, level B).
(6) Urinaryincontinence
In stroke patients with urinary incontinence, specialist assessment and management is recommended (class III, level C).
Symptomatictherapy(1) Seizure
(1) Seizure is an independent factor related to death during the acute phase. Prophylactic treatment for several days can be given to elderly patients with large hemorrhagic infarcts involving the cortex (grade C1). (2) Seizures are quite likely to happen again in patients who developed a seizure more than 14 days after onset and may well progress to symptomatic epilepsy; therefore, continuous treatment is recommendable (grade C1).
(1) Administration of anticonvulsants is recommended to prevent recurrent seizures after stroke (class I, level A). (2) Prophylactic administration of anticonvulsants to patients with recent stroke who have not had seizures is not recommended (class IV, GCP).
(2) Dysphagia (1) It is preferable to perform a videofluoroscopic swallow examination for patients with possible dysphagia, but a water-swallowing test is useful as a simple screening test carried out at the bedside (grade B). (2) When a patient is determined to be at a high risk for aspiration based on the test results, it is recommendable to consider an appropriate mode of delivering nourishment and prevention of aspiration (grade B).
Swallowing assessment is recommended but there are insufficient data to recommend a specific approach for treatment (class III, GCP).
Table 1 (continued)

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
406
Management from the Hyperacute to the Acute Phase of Stroke Both European and Japanese GLs recommended the
management of respiration, blood pressure and nutrition ( table 1 ). Although there is little remarkable difference between both GLs, Japanese GLs specified it to the man-agement during the hyperacute phase of stroke before the diagnosis of the stroke subtype, which might be better in terms of actual decision making in clinical practice. Thus, the Japanese GLs recommend that the management of hypertension immediately after the onset of stroke can be initiated after a diagnosis of the stroke subtype is final-ized, except for cases highly suspicious of hypertensive encephalopathy or subarachnoid hemorrhage (grade C1). Both GLs were announced before the publication of the results of SCAST (the Scandinavian Candesartan Acute Stroke Trial) [12] , which does not support blood pressure lowering in the acute phase of stroke associated with raised blood pressure, and the recommendations
were similar in both GLs. Regarding nutritional manage-ment, European GLs were more detailed.
Management of Acute Complications Both European and Japanese GLs described recommen-
dations for complicated infections and fever ( table 1 ). Ad-ditionally, European GLs made recommendations for falls or fractures and urinary incontinence, and Japanese GLs for gastrointestinal bleeding. Both GLs lacked recommen-dations for acute critical complications, e.g. acute respira-tory failure, stunned myocardium, multiple organ failure, and convulsive and nonconvulsive status epilepticus.
Symptomatic Therapy Both European and Japanese GLs described recommen-
dations for seizure and dysphagia. Additionally, Japanese GLs provided recommendations for headache. Both GLs did not recommend specific anticonvulsants for acute or prophylactic treatment, although there is an increasingly
Japanese guidelines European guidelines (ESO)
(3) Headache Headache caused by stroke often disappears in a short period of time, but nonnarcotic analgesics can be used when the headache is severe (grade C1).
(4) Management of brain edema
(1) Intravenous administration of hypertonic glycerol (10%) is recommended for large acute cerebral infarctions accompanying intracranial hypertension such as cardioembolic cerebral infarction and atherothrombotic infarction (grade B; the dosage depends on age and severity, but 10-12 ml/kg should be administered by fractionation over a few doses).(2) The use of mannitol (20%) can be considered in acute ischemic stroke, but no adequate scientific evidence currently exists (grade C1).(3) Corticosteroids are not recommended because of a lack of clear scientific evidence showing their efficacy for acute ischemic stroke (grade C2).
It is recommended that osmotherapy can be used to treat elevated intracranial pressure prior to surgery if this is considered (class III, level C).
(5) Prevention for deep venous thrombosis (DVT) and pulmonary embolism
(1) Subcutaneous injection of heparin or LMW heparin is recommended for the prevention of DVT and pulmonary embolism for patients with acute ischemic stroke with paralysis of the lower extremities. However, because there is a risk of intra- and extracranial hemorrhage, treatment cannot be recommended to be given routinely in patients with acute ischemic stroke (grade C1).(2) Aspirin is not recommended for the prevention of pulmonary embolism in patients with acute ischemic stroke. The effect of dextran on DVT prevention has not been demonstrated (grade C2). There has not yet been sufficient scientific evidence that step-by-step compression stockings or intermittent pneumatic compression is effective for DVT prevention (grade C1).
(1) Early rehydration and graded compression stockings are recommended to reduce the incidence of venous thromboembolism (class IV, GCP).(2) Early mobilization is recommended to prevent complications such as aspiration pneumonia, DVT and pressure ulcers (class IV, GCP).(3) It is recommended that low-dose subcutaneous heparin or LMW heparins should be considered for patients at high risk of DVT or pulmonary embolism (class I, level A).
Table 1 (continued)

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
407
wide selection of anticonvulsants. Regarding dysphagia, European GLs described that ‘swallowing assessment is rec-ommended but there are insufficient data to recommend a specific approach for treatment (Good Clinical Practice points, GCP)’. On the other hand, Japanese GLs described that ‘it is preferable to perform a videofluoroscopic swallow examination in patients with possible dysphagia, but a wa-ter-swallowing test, which can be carried out at the bedside, may be useful as a simple screening test (grade B)’.
Thrombolytic Therapy (Intravenous Administration) Regarding intravenous administration of a recombi-
nant tissue plasminogen activator (rt-PA; alteplase), both European and Japanese GLs strongly recommended its use with many inclusion and exclusion criteria (grade A, level A; table 2 ). Japanese GLs differed from the European GLs in that: (1) The therapeutic time window was still set at ≤ 3 h after
onset, which was revised to ≤ 4.5 h in 2012 in the re-vised GLs on intravenous rt-PA therapy for acute stroke patients in Japan [13] (grade A). The earlier the administration of rt-PA is, the better the outcome, even within this therapeutic time window (grade A).
(2) The approved dose in Japan is 0.6 mg/kg, because the J-ACT (Japan Alteplase Clinical Trial; a phase III clin-ical study) was performed using a 0.6 mg/kg dose [14] (grade A). In a postmarketing phase-IV trial in Japan (J-ACT II), the rates of recanalization and favorable outcome with 0.6 mg/kg i.v. rt-PA in patients with MR angiography-documented middle cerebral artery oc-clusion were comparable to those previously reported with the 0.9 mg/kg dose [15] .
(3) The Japan Stroke Society has proposed and advised requirements for institutions that may perform intra-venous rt-PA therapy.
(4) Intravenous infusion of low-dose (60,000 U/day) uro-kinase can be considered as treatment for patients with acute cerebral thrombosis (within 5 days) but in the absence of adequate scientific evidence (grade C1). On the other hand, the target population of rt-PA is
gradually expanding. European GLs recommended that intravenous rt-PA may also be administered in selected patients <18 and >80 years of age (level C). Also, in 2013, new GLs of AHA/American Stroke Association recom-mended that rt-PA may be considered in patients with mild stroke deficits, rapidly improving stroke symptoms, major surgery in the prior 3 months and recent myocar-dial infarction [16] (class IIb). In the revised GLs on in-travenous rt-PA therapy for acute stroke patients in Japan [13] , the criteria for target patients were revised and sev-
eral items of contraindication were deleted (e.g. prior ischemic stroke within 1–3 months before onset).
Thrombolytic Therapy (Intra-Arterial Administration) Both GLs recommended intra-arterial thrombolytic
therapy for middle cerebral artery occlusion within 6 h after onset (grade B, level B), but with more specific inclu-sion criteria in Japanese GLs, such as embolic occlusion, moderate or less severe symptoms, no infarct or mild CT findings, and priority of the intravenous rt-PA therapy ( table 2 ). Unlike Japanese GLs, European GLs recom-mended intra-arterial thrombolysis for acute basilar oc-clusion in selected patients (level B) and also intravenous thrombolysis for basilar occlusion as an acceptable alter-native even after 3 h (level B). Because acute basilar occlu-sion is a very life-threatening condition, such recommen-dations would be critically important for physicians.
The revised GLs for appropriate treatment with intra-venous rt-PA therapy in Japan [13] described that intra-arterial local fibrinolytic therapy with urokinase for mid-dle cerebral artery occlusion within 6 h after onset can improve outcome (grade B) based on the results of MELT (Middle Cerebral Artery Embolism Local Fibrinolytic In-tervention Trial) in Japan [17] . Since both GLs were ac-complished before the publication of randomized con-trolled trials (RCTs) on mechanical thrombectomy, no specific recommendations were given for this therapy.
Anticoagulant Therapy in the Acute Stage European GLs clearly described that early administra-
tion of unfractionated heparin, low-molecular-weight (LMW) heparin or heparinoids is not recommended for the treatment of patients with acute ischemic stroke (class I, level A; table 2 ). Japanese GLs described that the use of heparin can be considered for cerebral infarction within 48 h after onset, but adequate scientific evidence is lack-ing (grade C1), and, also, the use of LMW heparin and heparinoid (neither of which are included in the Japanese healthcare insurance) for acute ischemic stroke can be considered, but adequate scientific evidence for either product is lacking (grade C1). These differences in GLs may partially reflect the favorable use of unfractionated heparin in patients with acute cardioembolic and pro-gressing stroke in Japan before.
On the other hand, Japanese GLs recommended arg-atroban, a selective thrombin inhibitor developed in Ja-pan, for cerebral infarction (excluding cardioembolic stroke) within 48 h after onset and with a maximum diam-eter of ≥ 1.5 cm (grade B) based on RCTs in Japan [18–20] .

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
408
Table 2. Pharmacological treatment of acute ischemic stroke
Japanese guidelines European guidelines (ESO)
Thrombolytic therapy(intravenous administration)
(1) The intravenous administration of rt-PA (alteplase) is highly recommended for patients with ischemic stroke who can be treated within 3 h after onset (within 4.5 h in the revised guideline in 2012 [13]) and who are carefully determined to be candidates (grade A). In Japan, healthcare insurance is applicable to the intravenous therapy with alteplase 0.6 mg/kg, and the exclusion criteria for the determination of treatment and criteria for careful administration are defined. In addition, the Japan Stroke Society has proposed and advised requirements for institutions that may perform intravenous rt-PA therapy. (2) Intravenous administration of rt-PAs other than alteplase or desmoteplase (not approved in Japan) is not recommendable be cause it lacks adequate scientific evidence at present (grade C2).(3) Intravenous infusion of low-dose (60,000 U/day) urokinase can be considered as a treatment for patients with acute cerebral thrombosis (within 5 days), but it has no adequate scientific evidence (grade C1).(4) Intravenous antihypertensive therapy is recommendable for patients scheduled to receive thrombolytic therapy when the systolic blood pressure is >185 mm Hg or the diastolic blood pressure is ≥110 mm Hg (grade B).
(1) Intravenous rt-PA (0.9 mg/kg body weight, maximum 90 mg), with 10% of the dose given as a bolus followed by a 60-min infusion, is recommended within 4.5 h of onset of ischemic stroke (class I, level A).(2) The use of multimodal imaging criteria may be useful for patient selection for thrombolysis but is not recommended for routine clinical practice (class III, level C).(3) It is recommended that blood pressures of 185/110 mm Hg or higher is lowered before thrombolysis (class IV, GCP).(4) It is recommended that intravenous rt-PA may be used in patients with seizures at stroke onset, if the neurological deficit is related to acute cerebral ischemia (class IV, GCP).(5) It is recommended that intravenous rt-PA may also be administered in selected patients <18 years and >80 years of age, although this is outside the current European labeling (class III, level C).(6) It is recommended that if thrombolytic therapy is planned or given, aspirin or other antithrombotic therapy should not be initiated within 24 h (class IV, GCP).
Thrombolytic therapy (intraarterialadministration)
(1) For embolic occlusion of the middle cerebral artery with neurological deficits, selective transarterial local thrombolytic therapy is recommended for patients with moderate or less severe symptoms on arrival at the hospital without infarct lesion or with mild finding on CT, and in whom treatment can be started within 6 h after onset (grade B). However, it should be noted that intravenous rt-PA therapy is the first-line treatment for patients to whom drugs can be administered within 3 h after onset.(2) There is no sufficient scientific evidence on local thrombolytic therapy (transarterial) during the acute stage for embolic occlusion in other regions or under other conditions (grade C1).
(1) Intra-arterial treatment of acute middle cerebral artery occlusion within a 6-hour time window is recommended as an option (class II, level B).(2) Intra-arterial thrombolysis is recommended for acute basilar occlusion in selected patients (class III, level B). Intravenous thrombolysis for basilar occlusion is an acceptable alternative even after 3 h (class III, level B).
Anticoagulant therapy in the acute stage
(1) Argatroban, a selective thrombin inhibitor, is recommended for cerebral infarction (excluding cardioembolic stroke) within48 h after onset and with a maximum diameter of ≥1.5 cm (grade B).(2) The use of heparin can be considered for cerebral infarction within 48 h after onset, but adequate scientific evidence is lacking (grade C1).(3) The use of low-molecular-weight heparin and heparinoid(neither of which are included under Japanese healthcareinsurance) for acute ischemic stroke can be considered, butadequate scientific evidence for either product is lacking (grade C1).
Early administration of unfractionated heparin, LMW heparin or heparinoids is not recommended for the treatment of patients with acute ischemic stroke (class I, level A).
Antiplatelet therapyin the acute stage
(1) Intravenous infusion of ozagrel sodium 160 mg/day is recommendable for patients with acute cerebral thrombosis (cerebral infarction excluding cardioembolic stroke) within 5 days after onset (grade B).(2) Oral administration of aspirin 160–300 mg/day is recommendable for patients with acute cerebral infarction (within 48 h; grade A).
(1) It is recommended that aspirin (loading dose 160–325 mg) be given within 48 h after ischemic stroke (class I, level A).(2) The use of other antiplatelet agents (single or combined) is not recommended in the setting of acute ischemic stroke (class III, level C).(3) The administration of glycoprotein IIb-IIIa inhibitors is not recommended (class I, level A).
Neuroprotectiveagents
Edaravone, expected to display a neuroprotective effect, is recommendable for patients with acute cerebral infarction (thrombosis/embolism; grade B).
Currently, there is no recommendation to treat ischemic stroke patients with neuroprotective substances (class I, level A).
Hemodilutiontherapy
(1) Hemodilution therapy with a plasma expander can be considered for the treatment of acute ischemic stroke, but adequate scientific evidence is lacking (grade C1).(2) Hemodilution therapy with extracorporeal circulation can be considered for the treatment of acute ischemic stroke, but no adequate scientific evidence as yet exists (grade C1).
It is recommended that low blood pressure secondary to hypovolemia or associated with neurological deterioration in acute stroke should be treated with volume expanders (class IV, GCP).

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
409
Antiplatelet Therapy in the Acute Stage Both GLs recommended aspirin for patients with acute
cerebral infarction (within 48 h; grade A, level A). Japa-nese GLs recommended intravenous infusion of ozagrel sodium, an intravenous antiplatelet agent developed in Japan, 160 mg/day for patients with acute cerebral throm-bosis (cerebral infarction excluding cardioembolic stroke) within 5 days after onset (grade B) based on an RCT in Japan [21] .
Neuroprotective Agents Although European GLs described no recommenda-
tion for neuroprotective substances (level A), Japanese GLs recommended edaravone, an antioxidant developed in Japan, in patients with acute cerebral thrombosis and embolism (grade B) based on an RCT in Japan [22] .
Management of Brain Edema In Japan, hypertonic glycerol (10%) is the standard
treatment for suspected elevated intracranial pressure rather than mannitol, especially in nonsurgical settings. Recommendation grade was level C on osmotherapy in the European GLs, while it was grade B on hypertonic glycerol (10%) for large acute cerebral infarctions in the
Japanese GLs. Both GLs did not describe any recommen-dations about hypertonic saline treatment.
Hemodilution Therapy Low grade recommendation was made for hemodilu-
tion therapy by both European GLs (GCP) and Japanese GLs (grade C1).
Prevention of Deep Venous Thrombosis and Pulmonary Embolism Regarding pharmacological prevention of deep venous
thrombosis and pulmonary embolism, European GLs strongly recommended low-dose subcutaneous heparin or LMW heparins for patients at high risk of either disease (level A). However, Japanese GLs described that these treatments cannot be recommended to be given routinely to patients with acute ischemic stroke considering the risk of intra- and extracranial hemorrhage (grade C1).
Decompressive Surgery Both GLs recommended decompressive surgery for
hemispheric infarction (grade A, level A) and for large cerebellar infarction (grade C1, level C) which fulfill the conditions ( table 3 ).
Table 3. Surgical and interventional treatment of acute ischemic stroke
Japanese guidelines European guidelines (ESO)
Decompressive surgery
(1) Decompressive craniectomy with a duraplasty within 48 h after onset is recommended for patients1 with a unilateral hemispheric infarction including the territory of the middle cerebral artery (grade A).(2) Conservative treatment is recommended for cerebellar infarction when patients have clear consciousness and no hydrocephalus or brainstem compression is noted on CT imaging (grade C1). In contrast, ventricular drainage is recommended for patients with hydrocephalus seen on CT and moderate disturbance of consciousness such as stupor due to hydrocephalus, but adequate scientific evidence is lacking (grade C1). Decompressive craniectomy is recommended for patients with brainstem compression seen on CT and severe disturbance of consciousness such as coma concomitantly with such CT findings; however,the scientific evidence regarding its efficacy is so far insufficient (grade C1).
(1) Surgical decompressive therapy within 48 h after symptom onset is recommended in patients ≤60 yearsof age with evolving malignant middle cerebral artery infarcts (class I, level A).(2) It is recommended that ventriculostomy or surgical decompression be considered for treatment of large cerebellar infarctions that compress the brainstem (class III, level C).
Hypothermic treatment
(1) Hypothermic treatment can be considered to be instituted as a treatment of acute ischemic stroke, but adequate scientific evidence is as yet unavailable (grade C1).(2) The administration of normothermia therapy using an antipyretic can be considered for acute ischemic stroke, but the scientific evidence is currently inadequate (grade C1).
No recommendation can be given regarding hypothermic therapy in patients withspace-occupying infarctions (class IV, GCP).
1 Specific criteria for eligibility are given in footnotes such as age, severity and duration of the neurological deficits and imaging character-istics.

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
410
Table 4. Management of risk factors for primary prevention of ischemic stroke
Japanese guidelines European guidelines (ESO)
(1) Hypertension (1) Antihypertensive therapy is recommended for hypertensive patients (grade A). (2) Recommended target blood pressure is <140/90 mm Hg for elderly patients, <130/85 mm Hg for young and middle-aged patients, and <130/80 mmHg for patients with concurrent DM or a renal disorder (grade A). (3) As for the selection of antihypertensive drugs, Ca antagonists, diuretics, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are recommended (grade A). In particular, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers are recommended for patients with concurrent DM, chronic kidney disease, paroxysmal AF or heart failure, and evident left ventricular hypertrophy or left atrial enlargement (grade B).
(1) Blood pressure should be checked regularly. It is recommended that high blood pressure should be managed with lifestyle modification and individualized pharmacological therapy (class I, level A) aiming at normal levels of 120/80 mm Hg (class IV, GCP). (2) For prehypertensive (120–139/80–90 mm Hg) patients with congestive heart failure, myocardial infarction, diabetes or chronic renal failure, antihypertensive mediation is indicated (class 1, level A).
(2) Diabetes mellitus
(1) Blood glucose control is recommended for DM patients (grade C1). (2) Strict blood pressure control is advised for type 2 DM patients (grade A). (3) Lipid control with administration of an HMG-CoA reductase inhibitor (statin) is recommended for type 2 DM patients (grade A).
(1) Blood glucose should be checked regularly. It is recommended that diabetes should be managed with lifestyle modification and individualized pharmacological therapy (class IV, level C). (2) In diabetic patients, high blood pressure should be managed intensively (class I, level A) aiming for levels <130/80 mm Hg (class IV, level C). Where possible, treatment should include an angiotensin converting enzyme inhibitor or angiotensin receptor antagonist (class I, level A).
(3) Dyslipidemia Treatment with an HMG-CoA reductase inhibitor (statin) targeting low-density lipoprotein cholesterol is recommended for patients with dyslipidemia (grade A).
Blood cholesterol should be checked regularly. It is recommended that high blood cholesterol [e.g. low-density lipoprotein >150 mg/dl (3.9 mmol/l)] should be managed with lifestyle modification (class IV, level C) and a statin (class I, level A).
(4) Atrialfibrillation
(1) Warfarin is highly recommended for patients with nonvalvular AF (NVAF) with at least 2 of any of the following risk factors: previous ischemic stroke or transient ischemic attack, concurrent congestive heart failure, hypertension, age ≥75 years and DM (grade A). Warfarin is also recommended for NVAF patients with risk factors (grade B). There is no sufficient evidence that aspirin (81–330 mg/day) or warfarin is effective for NVAF patients aged <60 years without risk factors (grade C1). (2) Antiplatelet therapy may be administered to NVAF patients in whom warfarin is contraindicated (grade B). (3) In general, the recommended intensity of warfarin therapy is a PT-INR of 2.0–3.0 (grade A). For elderly (aged ≥70 years) NVAF patients, a PT-INR of 1.6–2.6 is recommended (grade B).
(1) Aspirin may be recommended for patients with NVAF who are <65 years and free of vascular risk factors (class I, level A).(2) Unless contraindicated, either aspirin or an oral anticoagulant (INR 2.0–3.0) is recommended for patients with NVAF who are aged 65–75 years and free of vascular risk factors (class I, level A).(3) Unless contraindicated, an oral anticoagulant (INR 2.0–3.0) is recommended for patients with NVAF aged >75 years, or who are younger but have risk factors such as high blood pressure, left ventricular dysfunction or DM (class I, level A).(4) It is recommended that patients with AF who are unable to receive oral anticoagulants should be offered aspirin (class I, level A).(5) It is recommended that patients with AF who have mechanical prosthetic heart valves should receive long-term anticoagulation with a target INR based on the prosthesis type, but not less than INR 2–3 (class II, level B).
(5) Smoking (1) Smoking is a risk factor for ischemic stroke and subarachnoid hemorrhage. Smoking cessation is recommended for smokers (grade A). (2) Passive smoking may be a risk factor for stroke; thus, passive smoking should be avoided (grade C1). (3) Education for cigarette smoking cessation, nicotine replacement therapy and oral smoking cessation medications are recommendable for smokers (grade B).
It is recommended that cigarette smoking be discouraged(class III, level B).
(6) Alcohol consumption
Heavy drinking should be avoided to prevent stroke (grade A). It is recommended that heavy use of alcohol be discouraged (class III, level B).
(7) Metabolic syndrome
The metabolic syndrome is a risk factor for ischemic stroke. Treatment to reduce body weight to an appropriate level and improve lifestyle with physical exercise and diet as the basis and, when necessary, drug therapy according to each component are recommended (grade B).
Subjects with an elevated body mass index are recommended to follow a weight-reducing diet (class III, level B).

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
411
Hypothermic TreatmentHypothermic treatment was described in both GLs
with recommendation grade C1 and GCP ( table 3 ). Con-sidering the actual clinical practice, we might need spe-cific GLs for very severe forms of acute ischemic stroke.
Recommendations Mentioned in Only One of the
Guidelines
In addition, the Japanese GLs give statements regard-ing fibrinogen lowering therapy, hyperbaric treatment, emergency carotid endarterectomy/acute revasculariza-tion of the carotid artery, and on the management of spe-cial conditions such as arterial dissection, aortic dissec-tion and cerebral venous occlusion. GLs on the manage-ment of transient ischemic attacks are different regarding their content. The European GLs focus on recommenda-tions on the diagnostic work-up, while mainly the thera-peutic management is described in the Japanese GLs.
Primary Prevention of Ischemic Stroke
Public Awareness and Education The European GLs recommended educational pro-
grams to increase the awareness of stroke at population level and among professionals (level B).
Management of Vascular Risk Factors for Stroke Hy-pertension. Both GLs recommended regular blood pres-sure control and the management of elevated blood pres-sure with lifestyle modification and pharmacotherapy (grade A, level A). Japanese GLs gave more detailed ad-vice for specific drugs to be preferred for hypertensive individuals with and without diabetes mellitus (DM) and chronic kidney disease, for example ( table 4 ). However, both GLs favored the use of an angiotensin-converting enzyme inhibitor or an angiotensin receptor blocker for blood pressure control in patients with DM (grade B, lev-el A), aiming at blood pressure levels <130/80 mm Hg (grade A, level C). Recommendations for target blood pressure were mainly based on GLs from the Japanese Society of Hypertension 2009, European Society of Hy-pertension and European Society of Cardiology 2007 [24, 25].
Diabetes Mellitus. Both GLs recommended regular blood glucose control and management of elevated blood glucose, especially in patients with DM (grade A, level A). Japanese GLs additionally emphasized the importance of lipid control with administration of an HMG-CoA reduc-
tase inhibitor (statin) in patients with type 2 DM accord-ing to a meta-analysis (grade A) [26] .
Dyslipidemia. Both GLs unequivocally recommended lipid control with statins for patients with dyslipidemia (grade A, level A).
Atrial Fibrillation. Both GLs recommended an oral an-ticoagulant for primary prevention of stroke in patients with atrial fibrillation (AF) aged ≥ 75 years and/or the pres-ence of risk factors such as high blood pressure, congestive heart failure or DM (grade A, level A). According to the Japanese GLs, antiplatelet therapy may only be considered for AF patients in whom oral anticoagulants are contrain-dicated (grade B). This recommendation is based on the results of the Japan Atrial Fibrillation Stroke Study [27] . In contrast, European GLs state that ‘aspirin may be recom-mended for patients with non-valvular AF who are young-er than 65 years and free of vascular risk factors’ (class I, level A). According to the results of the Japanese Nonval-vular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study Group and other studies [28–31] , a lower intensity of warfarin therapy with a prothrombin time (PT)-international normalized ratio (INR) of 1.6–2.6 in elderly patients aged ≥ 75 years was recommended in Japan (grade B) instead of the general recommendation of a PT-INR of 2.0–3.0 for patients <75 years and all patients in Europe (grade A, level A). Since both GLs were pub-lished before the RCTs on new oral anticoagulants, no spe-cific recommendations were given for these drugs.
Smoking. Both GLs recommended that cigarette smok-ing should be discouraged or cessation of smoking for smokers (grade A, level B). The Japanese GLs gave more specific recommendations on passive smoking and edu-cation for smoking cessation.
Alcohol Consumption. Both GLs recommended that heavy drinking should be avoided (grade A, level B).
Sleep Apnea Syndrome. For primary prevention, only the Japanese GLs recommended the treatment of the sleep apnea syndrome according to individual clinical conditions (grade C1).
Metabolic Syndrome/Obesity. Both GLs recommended specific measures for weight reduction and improvement in lifestyle (grade B, level B).
Chronic Kidney Disease. The management of chronic kidney disease as a predictor of stroke was discussed in the Japanese GLs only: lifestyle improvement, and blood pressure and blood glucose control were recommended at a high level of evidence.
Unclassified Factors. Some additional statements were made in the European GLs without correspondence in the Japanese GLs: GLs recommended regular physical ac-

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
412
tivity (level B) and ‘healthy’ nutrition (level B), while hor-mone replacement therapy and antioxidant vitamin sup-plements were not recommended (level A).
Antiplatelet Therapy for Primary Prevention/Carotid Stenosis The European GLs gave specific recommendations for
antiplatelet therapy for primary prevention and for the management of asymptomatic carotid stenosis. In brief, the GLs stated that there is no evidence for the use of aspirin (level A) or other antiplatelet agents (GCP) for primary pre-vention of ischemic stroke. Aspirin, however, was recom-mended for patients with asymptomatic carotid stenosis >50% ‘to reduce their risk of vascular events’ (level B), and before and after carotid surgery (level A) [32–34] . Accord-ing to the European GLs, carotid surgery is ‘not recom-mended for asymptomatic individuals with significant ca-rotid stenosis (NASCET 60–99%), except in those at high risk of stroke’ (level C). Carotid angioplasty, with or without stenting, was ‘not recommended for patients with asymp-tomatic carotid stenosis’ (GCP). Sim ilarly, Japanese GLs in-dicated that ‘for asymptomatic severe carotid stenosis, in addition to the best medical treatment including antiplate-let therapy, CEA is only recommended to be performed by appropriate surgeons and at facilities experienced with sur-gery and perioperative management (grade B)’.
Secondary Prevention of Ischemic Stroke
Management of Vascular Risk Factors Hypertension. Similar to primary prevention, both
GLs clearly recommended regular blood pressure control and antihypertensive treatment of elevated blood pres-sure for the prevention of recurrent stroke after the acute phase (grade A, level A; table 5 ).
Diabetes Mellitus. Both GLs recommended regular blood glucose control and management of elevated blood glucose for the prevention of recurrent cerebral infarc-tion (grade C1, GCP). For patients with type 2 DM who do not need insulin, treatment with pioglitazone was rec-ommended after stroke (grade B, level B).
Dyslipidemia. Both GLs strongly recommended high-dose statins in patients with noncardioembolic stroke (grade B, level A). Japanese GLs also recommended the combination of low-dose statins with eicosapentaenoic acid for the prevention of recurrent stroke in patients who are being treated for dyslipidemia (grade B) as such a combination was demonstrated to reduce the risk of re-current stroke in Japanese patients [35] .
Atrial Fibrillation. Both GLs recommended an oral an-ticoagulant for secondary prevention of stroke in patients with AF (grade A, level A) except for those ‘with comor-bid conditions such as falls, poor compliance, uncon-trolled epilepsy, or gastrointestinal bleeding’ (level C, Eu-ropean GLs). A lower intensity of warfarin therapy with a PT-INR of 1.6–2.6 in elderly patients aged ≥ 75 years was recommended in Japan (grade B) instead of the gen-eral recommendation of a PT-INR of 2.0–3.0 for patients <75 years and all patients in Europe (grade A, level A).
Smoking. Both GLs recommended cessation of smok-ing for smokers or that cigarette smoking should be dis-couraged (grade A, level C) although there are no ade-quate data as to whether or not it decreases the recurrence rate (grade C1).
Alcohol Consumption. Both GLs recommended that heavy drinking should be avoided (grade C1, GCP). The Japanese GLs stated that ‘drinking more than a moderate amount of alcohol increases the frequency of cerebral in-farction, but a small amount of drinking decreases the incidence of cerebral infarction’ (grade A) [36] .
Sleep Apnea Syndrome. For secondary prevention, only the European GLs recommended the treatmentof the sleep apnea syndrome with continuous positive air-way pressure breathing, at a low level of evidence (GCP).
Metabolic Syndrome/Obesity. The European GLs rec-ommended a weight-reducing diet for subjects with ele-vated body mass index although there are no specific data in secondary prevention (level C). The Japanese GLs stat-ed that there is ‘a lack of scientific evidence as to whether or not control of the metabolic syndrome is effective for secondary prevention (grade C1).
Antiplatelet Therapy for Secondary Prevention Noncardioembolic Stroke. Antiplatelet therapy for the
prevention of noncardioembolic stroke was recommended in both GLs with a high level of evidence (grade A, level A). In Europe, combination treatment with aspirin and dipyr-idamole [37, 38] or clopidogrel alone [39] , alternatively as-pirin or triflusal [40] alone, were considered first choice; the combination of aspirin and clopidogrel [41] was not recommended (level A). In Japan, aspirin (grade A), clop-idogrel (grade A), cilostazol (grade B) [42–44] or ticlopi-dine (grade B) were considered first choice. The combi-nation therapy with aspirin and dipyridamole was not recommended, partly reflecting the unavailability ofsustained-release dipyridamole in Japan to date ( table 6 ).
Cardioembolic Stroke. Japanese GLs specified that oral anticoagulants represent the first-line treatment for the secondary prevention of cardioembolic stroke (level A)

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
413
while antiplatelet drugs should be administered only if oral anticoagulants are contraindicated.
Anticoagulant Therapy As stated above, both GLs recommended an oral anti-
coagulant for the secondary prevention of stroke in AF patients (grade A, level A), except for those ‘with comor-bid conditions such as falls, poor compliance, uncon-
trolled epilepsy, or gastrointestinal bleeding’ (level C, Eu-ropean GLs; table 6 ). European GLs did not generally rec-ommend anticoagulation after cardioembolic stroke unrelated to AF except for specific conditions (GCP) or a high risk of recurrence (level C). Japanese GLs recom-mended anticoagulation at a PT-INR of 2.0–3.0 for pa-tients with rheumatic heart disease, dilated cardiomyopa-thy and mechanical prosthetic valves (grade A). In addi-
Table 5. Management of risk factors for secondary prevention of ischemic stroke
Japanese guidelines European guidelines (ESO)
(1) Hypertension
Antihypertensive treatment is recommended for prevention of recurrent cerebral infarction. The target blood pressure is defined as <140/90 mm Hg (grade A).
It is recommended that blood pressure be checked regularly. Blood pressure lowering is recommended after the acute phase, including in patients with normal blood pressure (class I, level A).
(2) Diabetes mellitus
(1) Blood glucose control is recommended for prevention of recurrent cerebral infarction (grade C1).(2) The treatment of DM with pioglitazone, a drug improving insulin resistance, is effective for the prevention of recurrent cerebral infarction (grade B).
(1) It is recommended that blood glucose should be checked regularly. It is recommended that diabetes should be managed with lifestyle modification and individualized pharmacological therapy (class IV, GCP).(2) In patients with type 2 diabetes who do not need insulin, treatment with pioglitazone is recommended after stroke (class III, level B).
(3) Dyslipidemia
(1) Dyslipidemia control is recommended for the prevention of recurrent cerebral infarction (grade C1).(2) High-dose statins are effective for the prevention of recurrent cerebral infarction (grade B).(3) Low-dose statins in combination with eicosapentaenoic acid are effective for the prevention of recurrent stroke in patients who are being treated for dyslipidemia (grade B).
(1) Statin therapy is recommended in subjects with noncardioembolic stroke (class I, level A).
(4) Atrialfibrillation
(1) Warfarin is effective for the secondary prevention in cerebral infarction patients with NVAF. In general, it is recommended to control it within the PT-INR range of 2.0–3.0 (grade A).(2) For patients with cerebral infarction or transient ischemic attack aged ≥70 years with NVAF, slightly low doses (PT-INR 1.6–2.6) are recommended (grade B), and it is advised not to exceed a PT-INR of 2.6 to avoid bleeding complications (grade B).
(1) Oral anticoagulation (INR 2.0 – 3.0) is recommended after ischemic stroke associated with AF (class I, level A). (2) Oral anticoagulation is not recommended in patients with comorbid conditions such as falls, poor compliance, uncontrolled epilepsy or gastrointestinal bleeding (class III, level C). Increasing age alone is not a contraindication to oral anticoagulation (class I, level A).
(5) Smoking Smoking cessation decreases the incidence of cerebral infarction (grade A), but there are no adequate data as to whether or not it decreases the recurrence rate (grade C1).
It is recommended that cigarette smoking be discouraged (class III, level C).
(6) Alcohol consumption
Drinking more than a moderate amount of alcohol increases the frequency of cerebral infarction, but a small amount of drinking decreases the incidence of cerebral infarction (grade A). Nonetheless, there is no adequate scientific evidence as to whether or not a small amount of alcohol consumption reduces the recurrence rate (grade C1).
It is recommended that heavy use of alcohol be discouraged (class IV, GCP).
(7) Metabolicsyndrome/obesity
The metabolic syndrome based on visceral obesity is a risk factor for cerebral infarction. However, there is a lack of scientific evidence as to whether or not metabolic syndrome control is effective for secondary prevention (grade C1).
Subjects with an elevated body mass index are recommended to adopt a weight-reducing diet (class IV, level C).

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
414
tion, Japanese GLs gave specific advice regarding timing of the start of oral anticoagulation after stroke and re-garding interruption of oral anticoagulation for perform-ing medical procedures or surgery based on the GLs of the Japanese Circulation Society [45] .
Cerebral Circulation and Metabolism Enhancers Japanese GLs gave a weak recommendation (grade B)
for the cerebral circulation and metabolism enhancers, such as ibudilast, nicergoline and ifenprodil tartrate to be used ‘only after full consideration of their indications based on the signs and symptoms of each patient’.
Antidepressants Both GLs recommend drug therapy (and interven-
tions without drugs) to improve mood on poststroke de-pressive states (grade A, level A). Japanese GLs specifi-cally mentioned selective serotonin reuptake inhibitors as drugs of choice.
Carotid Endarterectomy Both GLs recommended carotid endarterectomy (CEA)
for patients with symptomatic severe ( ≥ 70%) stenosis of the internal carotid artery (class I, level A), to be performed by the appropriate surgeons and at experienced facilities
Table 6. Pharmacological therapy for secondary prevention of ischemic stroke
Japanese guidelines European guidelines (ESO)
Antiplatelet therapy
(1) Administration of antiplatelet therapy is recommended for the secondary prevention of noncardioembolic stroke (grade A).(2) The most effective antiplatelet therapy (available in Japan) for the secondary prevention of noncardioembolic stroke at present is either aspirin 75 – 150 mg/day clopidogrel 75 mg/day (grade A), cilostazol 200 mg/day, or ticlopidine 200 mg/day (grade B). (3) Antiplatelet therapy is recommended for the secondary prevention of lacunar stroke (grade B), with adequate blood pressure control. (4) For the secondary prevention of cardioembolic stroke, thefirst-line drugs are generally not antiplatelet agents, but the anticoagulant warfarin (grade A). Antiplatelet drugs such as aspirin should be administered only to patients in whom warfarin is contraindicated (grade B).
(1) It is recommended that patients receive antithrombotic therapy (class I, level A).(2) It is recommended that patients not requiring anticoagulation should receive antiplatelet therapy (class I, level A). Where possible, combined aspirin and dipyridamole, or clopidogrel alone, should be given. Alternatively, aspirin alone, or triflusal alone, may be used (class I, level A).(3) The combination of aspirin and clopidogrel is not recommended in patients with recent ischemic stroke, except in patients with specific indications (e.g. unstable angina ornon-Q-wave myocardial infarction or recent stenting); treatment should be given for up to 9 months after the event (class I, level A).(4) It is recommended that patients who have a stroke on antiplatelet therapy should be reevaluated for pathophysiology and risk factors (class IV, GCP).
Anti-coagulant therapy
(1) Warfarin is the first-line medication for secondary prevention of cardioembolic stroke or transient ischemic attack with NVAF, and it is recommended to maintain the PT-INR at 2.0 – 3.0 (grade A). A PT-INR of 1.6–2.6 is recommended for those aged ≥70 years (grade B). Hemorrhagic complications sharply increase with aPT-INR ≥2.6 (grade B).(2) For patients with heart diseases such as rheumatic heart disease and dilated cardiomyopathy, maintenance at a PT-INR of 2.0 – 3.0 is recommended (grade A).(3) For patients with mechanical prosthetic valves, it is recommended to avoid a PT-INR below 2.0 – 3.0 (grade A).(4) Approximate timing of starting warfarin may be within 2 weeks after the onset of cerebral infarction. However, warfarin initiation needs to be delayed in patients with a large infarction, poor blood pressure control and bleeding tendency (grade C1).(5) Aspirin is indicated for patients in whom warfarin iscontra-indicated, but its effect is clearly inferior to that of warfarin (grade B).(6) Oral administration of warfarin is desirably continued whenperforming procedures or minor surgery (such as tooth extraction) during which bleeding can be easily managed. When conducting gastrointestinal endoscopic examination/treatment, warfarin needs to be interrupted for 3 – 4 days. During the interruption of warfarin for 4 – 5 days or less in patients at lower risk of thrombosis orembolism, bridge therapy with heparin, for example, is not usually employed. For patients at higher risk of thrombosis or embolism, drip infusion to avoid dehydration and heparin (bridge therapy) may be employed considering the patient’s condition (grade C1 for these).
(1) Oral anticoagulation (INR 2.0 – 3.0) is recommended after ischemic stroke associated with AF (class I, level A). Oral anticoagulation is not recommended in patients with comorbid conditions such as falls, poor compliance, uncontrolled epilepsy or gastrointestinal bleeding (class III, level C). Increasing age alone is not a contraindication to oral anticoagulation (class I, level A).(2) It is recommended that patients with cardioembolic stroke unrelated to AF should receive anticoagulants (INR 2.0 – 3.0) if the risk of recurrence is high (class III, level C).(3) It is recommended that anticoagulation should not be used after noncardioembolic ischemic stroke, except in some specific situations, such as aortic atheromas, fusiform aneurysms of the basilar artery, cervical artery dissection or patent foramen ovale in the presence of proven deep vein thrombosis or atrial septal aneurysm (class IV, GCP).(4) It is recommended that combined low-dose aspirin and dipyridamole should be given if oral anticoagulation is contraindicated (class IV, GCP).

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
415
( table 7 ). Recommendations were less certain for moder-ate (50–69%) stenosis (grade B, level A). CEA was not rec-ommended for stenosis <50% according to European GLs (level A). However, according to Japanese GLs, CEA could be considered in the presence of vulnerable plaques and/or ulceration at a low level of evidence (grade C1).
Endovascular Therapy Both GLs recommended carotid artery stenting only
under certain conditions (grade B, level A), in particular high-grade stenosis, risk factors for CEA, surgically inac-cessible sites, restenosis after CEA or stenosis following
radiation. Intracranial stenting was not recommended (grade C1, GCP).
Extracranial-Intracranial Bypass Japanese GLs gave a weak recommendation that extra-
cranial-intracranial bypass surgery may be considered with a symptomatic internal carotid artery and middle cerebral artery occlusion/stenosis (grade B). However, this recommendation was made before publication of the COSS (Carotid Occlusion Surgery Study) trial comparing extracranial-intracranial bypass surgery with best medi-cal treatment [46] .
Table 7. Surgical and interventional therapy for secondary prevention of ischemic stroke
Japanese guidelines European guidelines (ESO)
Carotid endarterectomy
(1) For symptomatic severe carotid stenosis (>70%, NASCET method), in addition to the best medical treatment including antiplatelet therapy, CEA is recommende d to be performed by the appropriate surgeons and at facilities experienced in surgery and perioperative management (grade A).(2) For symptomatic moderate carotid stenosis, in addition to the best medical treatment including antiplatelet therapy, CEA is recommended to be performed by the appropriate surgeons and at facilities experienced in surgery and perioperative management (grade B).(3) For asymptomatic severe carotid stenosis, in addition to the best medical treatment including antiplatelet therapy, CEA is recommended to be performed by the appropriate surgeons and at facilities experienced in surgery and perioperative management (grade B).(4) When the vulnerable plaque and/or ulceration is noted in patients with symptomatic mild carotid stenosis or asymptomatic moderate-or-mild stenosis, the indication of CEA could be considered, but the scientific evidence supporting CEA in this case is inadequate (grade C1).
(1) CEA is recommended for patients with 70 – 99% stenosis (class I, level A). CEA should only be performed in centers with a perioperative complication rate (all strokes and death) <6% (class I, level A).(2) It is recommended that CEA be performed as soon as possible after the last ischemic event, ideally within 2 weeks (class II, level B).(3) It is recommended that CEA may be indicated for certain patients with stenosis of 50 – 69%; males with very recent hemispheric symptoms are most likely to benefit (class III,level C). CEA for stenosis of 50 – 69% should only be performed in centers with a perioperative complication rate (all stroke and death) <3% (class I, level A).(4) CEA is not recommended for patients with stenosis <50% (class I, level A).(5) It is recommended that patients remain on antiplatelet therapy both before and after surgery (class I, level A).
Endovascular therapy
(1) Carotid artery stenting is recommended for patients with internal carotid stenosis who have risk factors (grade B).(2) Carotid artery stenting can be considered for patients with internal carotid stenosis who have no risk factor for CEA, but adequate scientific evidence for this approach is lacking (grade C1).(3) There is no adequate scientific evidence for performing angioplasty/stenting for extra-/intracranial artery stenosis excluding the cervical carotid artery (grade C1).
(1) Carotid percutaneous transluminal angioplasty and/or carotid artery stenting is only recommended in selected patients (class I, level A). It should be restricted to the following subgroups of patients with severe symptomatic carotid artery stenosis: those withcontra-indications to CEA, stenosis at a surgically inaccessible site, restenosis after earlier CEA, and stenosis after radiotherapy (class IV, GCP). Patients should receive a combination of clopidogrel and aspirin im mediately before and for at least 1 month after stenting (class IV, GCP).(2) It is recommended that endovascular treatment may becon sidered in patients with symptomatic intracranial stenosis(class IV, GCP).
Endovascular closure of patent foramen ovale
(1) Surgical closure and percutaneous transcatheter closure of the foramen ovale may be considered for the prevention of patent foramen ovale-mediated recurrent paradoxical cerebral embolisms (grade C1).(2) Percutaneous transcatheter occlusion may be considered for the prevention of recurrent paradoxical cerebral embolisms associated with a pulmonary arteriovenous fistula (grade C1).
It is recommended that endovascular closure of a patent foramen ovale may be considered in patients with cryptogenic stroke and high-risk patent foramen ovale (class IV, GCP).

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
416
Endovascular Closure of a Patent Foramen Ovale Both GLs stated that endovascular closure of a patent
foramen ovale can be considered in patients with crypto-genic stroke and either high-risk patent foramen ovale (European GLs, GCP) or recurrent paradoxical cerebral embolism (Japanese GLs, grade C1). It should be noted that the GLs were published before RCTs comparing en-dovascular closure with medical treatment.
Conclusions
This article summarizes similarities and differences between Japanese and European GLs for the management of ischemic stroke published between 2008 and 2011. Al-though there are obvious differences between the GLs re-garding structure, length and categorization of the level of evidence, the vast majority of recommendations is largely similar. However, there are some interesting dif-ferences between the GLs.
For the management of acute ischemic stroke, the most important difference is the dosage of intravenous rt-PA: the approval in Japan envisages a lower dose of 0.6 mg/kg, while in Europe a dose of 0.9 mg/kg is used. The Japanese GLs recommend the selective thrombin inhibi-tor argatroban for noncardioembolic stroke within 48 h after onset. In Europe, early administration of unfrac-tionated heparin, LMW heparin and heparinoids is gen-erally not recommended. During the acute stage, Japa-nese GLs propose intravenous infusion of the antiplatelet agent ozagrel sodium for noncardioembolic stroke, a drug not well known and not approved in Europe. In ad-dition, the Japanese GLs recommend the antioxidant eda-ravone, while in Europe administration of neuroprotec-tive agents are generally not recommended.
For primary and secondary prevention of ischemic stroke, one of the major differences is the dosage of oral anticoagulants for stroke prevention in elderly patients with AF. For patients aged ≥ 75 years, a target PT-INR of 1.6–2.6 is recommended in Japan instead of 2.0–3.0 for younger patients: In Europe, no specific INR adaptation according to age was provided. For treatment of dyslipid-emia in the secondary prevention of stroke, Japanese GLs also allow a combination of eicosapentaenoic acid with low-dose statins as an alternative to the standard treat-ment with high-dose statins. Finally, the drug cilostazol has been investigated extensively and is approved for the secondary prevention of ischemic stroke in Japan as an alternative to aspirin or clopidogrel.
Some new relevant aspects of stroke management have emerged during the last years, such as interventional thrombectomy, intracranial stenting, extra-/intracranial bypass surgery and stroke prevention with new oral anti-coagulants. As the GLs discussed in this article have been announced before publication of trials investigating these treatment strategies, specific recommendations are still lacking. Their inclusion will be a major task for the next upcoming European and Japanese GLs on stroke man-agement.
Acknowledgments
We would like to thank all Members, Staff and the Reviewers of the Joint Committee on Guidelines for the Management of Stroke for the English version, especially Prof. Shotai Kobayashi, the Group Leader of the Chapter ‘Stroke in General’ and Prof. Ka-zuo Minematsu, the Group Leader of the Chapter ‘Cerebral Infarc-tion/TIA’ of the Japanese GLs, and also, Ms. Akiko Tsuchida (Ac-ademic Research Communications, Toyama, Japan) for her pro-fessional assistance in the preparation of the tables.
References
1 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: I. Stroke in gen-eral. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S7–S30.
2 Shinohara Y, Yanagihara T, Abe K, Yoshimine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: II. Cerebral infarction/transient ischemic attack (TIA). J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S31–S73.
3 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: III. Intracerebral hemorrhage. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S74–S99.
4 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: IV. Subarachnoid hemorrhage. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S100–S115.
5 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: V. Asymptomatic cerebrovascular diseases. J Stroke Cerebro-vasc Dis 2011; 20(suppl 1):S116–S128.
6 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: VI. Other types of cerebrovascular disorders. J Stroke Cerebro-vasc Dis 2011; 20(suppl 1):S129–S144.

Comparison of Stroke Guidelines: Management of Ischemic Stroke
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
417
7 Shinohara Y, Yanagihara T, Abe K, Yoshimine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Kobayashi S: VII. Rehabilitation. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S145–S180.
8 European Stroke Organisation (ESO) Execu-tive Committee, ESO Writing Committee: Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovasc Dis 2008; 25: 457–507.
9 ESO News: Update Guidelines January 2009. Specific Treatment: Thrombolysis. Cerebro-vasc Dis 2009; 27: 619–620.
10 Neuroresuscitation; in JRC Guidelines 2010 (in Japanese). Tokyo, Japan Resuscitation Council, 2010. http://jrc.umin.ac.jp/pdf/20121022_NR_E.pdf.
11 Wojner-Alexander AW, Garami Z, Cherny-shev OY, Alexandrov AV: Heads down: flat positioning improves blood flow velocity in acute ischemic stroke. Neurology 2005; 64: 1354–1357.
12 Sandset EC, Bath PM, Boysen G, Jatuzis D, Kõrv J, Lüders S, Murray GD, Richter PS, Roine RO, Terént A, Thijs V, Berge E, SCAST Study Group: The angiotensin-receptor blocker can-desartan for treatment of acute stroke (SCAST): a randomised, placebo-controlled, double-blind trial. Lancet 2011; 377: 741–750.
13 Minematsu K, Toyoda K, Hirano T, Kimura K, Kondo R, Mori E, Nakagawara J, Sakai N, Shiokawa Y, Tanahashi N, Yasaka M, Kata-yama Y, Miyamoto S, Ogawa A, Sasaki M, Suga S, Yamaguchi T: Guidelines for intrave-nous application of rt-PA (alteplase), the sec-ond edition, October 2012: a guideline from the Japan Stroke Society. J Stroke Cerebrovasc Dis 2013, in press.
14 Yamaguchi T, Mori E, Minematsu K, Na-kagawara J, Hashi K, Saito I, Shinohara Y, Ja-pan Alteplase Clinical Trial (J-ACT) Group: Alteplase at 0.6 mg/kg for acute ischemic stroke within 3 hours of onset: Japan Al-teplase Clinical Trial (J-ACT). Stroke 2006; 37: 1810–1815.
15 Mori E, Minematsu K, Nakagawara J, Yama-guchi T, Sasaki M, Hirano T, Japan Alteplase Clinical Trial II Group: Effects of 0.6 mg/kg intravenous alteplase on vascular and clinical outcomes in middle cerebral artery occlusion: Japan Alteplase Clinical Trial II (J-ACT II). Stroke 2010; 41: 461–465.
16 Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, Khatri P, Mc-Mullan PW Jr, Qureshi AI, Rosenfield K, Scott PA, Summers DR, Wang DZ, Winter-mark M, Yonas H, American Heart Associa-tion Stroke Council, Council on Cardiovascu-lar Nursing, Council on Peripheral Vascular Disease, Council on Clinical Cardiology: Guidelines for the early management of pa-tients with acute ischemic stroke: a guideline for healthcare professionals from the Ameri-can Heart Association/American Stroke As-sociation. Stroke 2013; 44: 870–947.
17 Ogawa A, Mori E, Minematsu K, Taki W, Takahashi A, Nemoto S, Miyamoto S, Sasaki
M, Inoue T, MELT Japan Study Group: Ran-domized trial of intraarterial infusion of uro-kinase within 6 hours of middle cerebral ar-tery stroke: the middle cerebral artery em-bolism local fibrinolytic intervention trial (MELT) Japan. Stroke 2007; 38: 2633–2639.
18 Tazaki Y, Kobayashi S, Tohgi H, et al: Clinical benefit of an antithrombin agent, MD-805, in acute-phase cerebral thrombosis – a placebo-controlled, multicenter, double-blind, inter-group trial (in Japanese)]. J Clin Exp Med 1992; 161: 887–907.
19 Kobayashi S, Tazaki Y: Effect of the thrombin inhibitor argatroban in acute cerebral throm-bosis. Semin Thromb Hemost 1997; 23: 531–534.
20 Fukuuchi Y, Tohgi H, Shinohara Y, et al: A controlled clinical trial to assess the efficacy and safety of argatroban in treating acute ce-rebral thrombosis in comparison to sodium ozagrel (in Japanese). Neurol Ther 2001; 18: 273–282.
21 Otomo E, Kutuzawa T, Kogure K: Clinical benefit of OKY-046 in acute cerebral throm-bosis – a placebo-controlled, multicenter, double-blind trial (in Japanese). J Clin Ther Med 1991; 7: 353–388.
22 Edaravone Acute Infarction Group: Effect of a novel free radical scavenger, edaravone (MCI-186), on acute brain infarction. Ran-domized, placebo-controlled, double blind study at multicenters. Cerebrovasc Dis 2003; 15: 222–229.
23 Ringelstein EB, Chamorro A, Kaste M, Langhorne P, Leys D, Lyrer P, Thijs V, Thomassen L, Toni D, ESO Stroke Unit Cer-tification Committee: European Stroke Or-ganisation recommendations to establish a stroke unit and stroke center. Stroke 2013; 44: 828–840.
24 Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mit-suyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshi-ma H, Umemura S, Ishimitsu T, Rakugi H, Japanese Society of Hypertension Committee: The Japanese Society of Hypertension Guide-lines for the Management of Hypertension (JSH 2009). Hypertens Res 2009; 32: 3–107, er-ratum p 318.
25 Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Nar-kiewicz K, Ruilope L, Rynkiewicz A, Schmie-der RE, Struijker Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Kjeldsen SE, Erdine S, Narkie-wicz K, Kiowski W, Agabiti-Rosei E, Ambro-sioni E, Cifkova R, Dominiczak A, Fagard R, Heagerty AM, Laurent S, Lindholm LH, Man-cia G, Manolis A, Nilsson PM, Redon J, Schmieder RE, Struijker-Boudier HA, Viigi-
maa M, Filippatos G, Adamopoulos S, Agabi-ti-Rosei E, Ambrosioni E, Bertomeu V, Clem-ent D, Erdine S, Farsang C, Gaita D, Kiowski W, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O’Brien E, Ponikowski P, Redon J, Rus-chitzka F, Tamargo J, van Zwieten P, Viigi-maa M, Waeber B, Williams B, Zamorano JL, Task Force for the Management of Arterial Hypertension of the European Society of Hy-pertension, Task Force for the Management of Arterial Hypertension of the European So-ciety of Cardiology: 2007 Guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hy-pertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–536.
26 Cholesterol Treatment Trialists’ (CTT) Col-laborators, Kearney PM, Blackwell L, Collins R, Keech A, Simes J, Peto R, Armitage J, Baigent C: Efficacy of cholesterol-lowering therapy in 18,686 people with diabetes in 14 randomised trials of statins: a meta-analysis. Lancet 2008; 371: 117–125.
27 Sato H, Ishikawa K, Kitabatake A, et al: Low-dose aspirin for prevention of stroke in low-risk patients with atrial fibrillation: Japan Atrial Fibrillation Stroke Trial. Stroke 2006; 37: 447–451.
28 Yamaguchi T, Japanese Nonvalvular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study Group: Optimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation: a multicenter, prospective, ran-domized trial. Stroke 2000; 31: 817–821.
29 Yasaka M, Minematsu K, Yamaguchi T: Op-timal intensity of international normalized ratio in warfarin therapy for secondary pre-vention of stroke in patients with non-valvu-lar atrial fibrillation. Intern Med 2001; 40: 1183–1188.
30 Stroke Prevention in Atrial Fibrillation Inves-tigators: Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin for high-risk patients with atrial fibrillation: Stroke Prevention in Atrial Fibrillation III ran-domised clinical trial. Lancet 1996; 348: 633–638.
31 Hylek EM, Singer DE: Risk factors for intra-cranial hemorrhage in outpatients taking warfarin. Ann Intern Med 1994; 120: 897–902.
32 Hobson R 2nd, Krupski W, Weiss D: Influ-ence of aspirin in the management of asymp-tomatic carotid artery stenosis. VA Coopera-tive Study Group on Asymptomatic Carotid Stenosis. J Vasc Surg 1993; 17: 257–263.
33 Engelter S, Lyrer P: Antiplatelet therapy for preventing stroke and other vascular events after carotid endarterectomy (review). Co-chrane Database Syst Rev 2003; 3:CD001458.
34 Mayo Asymptomatic Carotid Endarterecto-my Study Group: Results of a randomized controlled trial of carotid endarterectomy for asymptomatic carotid stenosis. Mayo Asymp-tomatic Carotid Endarterectomy Study Group. Mayo Clin Proc 1992; 67: 513–518.

Kern/Nagayama/Toyoda/Steiner/Hennerici/Shinohara
Cerebrovasc Dis 2013;35:402–418DOI: 10.1159/000351753
418
35 Tanaka K, Ishikawa Y, Yokoyama M, Origasa H, Matsuzaki M, Saito Y, et al: Reduction in the recurrence of stroke by eicosapentaenoic acid for hypercholesterolemic patients: sub-analysis of the JELIS trial. Stroke 2008; 39: 2052–2058.
36 Reynolds K, Lewis B, Nolen JD, Kinney GL, Sathya B, He J: Alcohol consumption and risk of stroke: a meta-analysis. JAMA 2003; 289: 579–588.
37 Diener HC, Cunha L, Forbes C, Sivenius J, Smets P, Lowenthal A: European Stroke Pre-vention Study. 2. Dipyridamole and acetylsal-icylic acid in the secondary prevention of stroke. J Neurol Sci 1996; 143: 1–13.
38 Halkes P, van Gijn J, Kappelle L, Koudstaal P, Algra A: Aspirin plus dipyridamole versus as-pirin alone after cerebral ischaemia of arterial origin (ESPRIT): randomised controlled trial. Lancet 2006; 367: 1665–1673.
39 CAPRIE Steering Committee: A randomised, blinded trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996; 348: 1329–1339.
40 Costa J, Ferro JM, Matias-Guiu J, Alvarez-Sabin J, Torres F: Triflusal for preventing se-rious vascular events in people at high risk. Cochrane Database Syst Rev 2005; 3:CD004296.
41 Diener H, Bogousslavsky J, Brass L, Cimmi-niello C, Csiba L, Kaste M, Leys D, Matias-Guiu J, Rupprecht H: Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet 2004; 364: 331–337.
42 Gotoh F, Tohgi H, Hirai S, Terashi A, Fuku-uchi Y, Otomo E, et al: Cilostazol stroke pre-vention study: a placebo-controlled double-blind trial for secondary prevention of cere-bral infarction. J Stroke Cerebrovasc Dis 2000; 9: 147–157.
43 Huang Y, Cheng Y, Wu J, Li Y, Xu E, Hong Z, et al: Cilostazol as an alternative to aspirin after ischaemic stroke: a randomised, double-blind, pilot study. Lancet Neurol 2008; 7: 494–499.
44 Shinohara Y, Katayama Y, Uchiyama S, Ya-maguchi T, Handa S, Matsuoka K, Ohashi Y, Tanahashi N, Yamamoto H, Genka C, Kitaga-wa Y, Kusuoka H, Nishimaru K, Tsushima M, Koretsune Y, Sawada T, Hamada C, CSPS 2 Group: Cilostazol for prevention of second-ary stroke (CSPS 2): an aspirin-controlled, double-blind, randomised noninferiority tri-al. Lancet Neurol 2010; 9: 959–968.
45 Japanese Circulation Society. Circ J 2004; 68(suppl IV):1195–1196.
46 Powers WJ, Clarke WR, Grubb RL Jr, Videen TO, Adams HP Jr, Derdeyn CP, COSS Inves-tigators: Extracranial-intracranial bypass sur-gery for stroke prevention in hemodynamic cerebral ischemia: the Carotid Occlusion Sur-gery Study randomized trial. JAMA 2011; 306: 1983–1992.

E-Mail [email protected]
with regard to ICH are relatively rare both in Japan and Eu-rope. Methods: Since 2011, the authors have met repeat-edly and have compared the latest versions of published European and Japanese GLs for ischemic and hemorrhagic strokes. Many aspects have only been addressed in one but left out in the other GLs, which consequently founded the basis for the comparison. Classification of evidence levels and recommendation grades defined by the individual committees differed between both original GLs. Results: As-pects of major importance were similar and hence did not need extensive interpretation, mostly due to a lack of evi-dence from appropriate RCTs worldwide. The target level to which systolic blood pressure should be lowered is quite high; <170 mm Hg for patients with known hypertension in Europe and <180 mm Hg in Japan. The results of ongoing clinical trials are awaited for the optimal target level and op-timal medications. Concerning ICH associated with oral an-
Key Words
Acute stroke treatment · European stroke guidelines · Evidence-based medicine · Hemorrhage · Japanese stroke guidelines · Randomized clinical trials · Review · Stroke prevention
Abstract
Background: Different aspects of acute stroke manage-ment and strategies for stroke prevention derive from two viewpoints: specific traditional and historical backgrounds and evidence-based medicine from modern randomized controlled trials (RCTs), meta-analysis and authorized clini-cal practice guidelines (GLs). Regarding intracerebral hem-orrhage (ICH), Cerebrovascular Diseases published the 2006 European stroke initiative recommendations for the man-agement of ICH. In 2009, the revised Japanese GLs for the management of stroke, including that of ICH, appeared in Japanese. Whereas GLs for the prevention and treatment of ischemic stroke were presented in detail, recommendations
Guidelines
Cerebrovasc Dis 2013;35:419–429 DOI: 10.1159/000351754
Received: May 6, 2013 Accepted: May 7, 2013 Published online: May 23, 2013
Comparison of the European and Japanese
Guidelines for the Acute Management of
Intracerebral Hemorrhage
Kazunori Toyoda a Thorsten Steiner b, c Corina Epple c Rolf Kern d
Masao Nagayama e Yukito Shinohara f Michael G. Hennerici d
a Department of Cerebrovascular Medicine, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan; b Department of Neurology, Klinikum Frankfurt Höchst, Frankfurt, c Department of Neurology, University of Heidelberg Hospital, Heidelberg, and d Department of Neurology, UMM, University of Heidelberg, Mannheim ,Germany; e Departments of Neurology and Rehabilitation, and the Center for Stroke and Neurocritical Care, International University of Health and Welfare Atami Hospital, Atami , and f Department of Neurology, Federation of National Public Service Personnel Mutual Aid Associations Tachikawa Hospital, Tokyo , Japan
Dr. Kazunori ToyodaDepartment of Cerebrovascular MedicineNational Cerebral and Cardiovascular Center5-7-1 Fujishirodai, Suita, Osaka 565-8565 (Japan)E-Mail [email protected]
© 2013 S. Karger AG, Basel1015–9770/13/0355–0419$38.00/0
www.karger.com/ced
K.T., T.S. and C.E. contributed equally to this work.

Toyoda/Steiner/Epple/Kern/Nagayama/Shinohara/Hennerici
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
420
ticoagulant therapy, both guidelines give similar recom-mendations, namely that anticoagulation should be discon-tinued and the international normalized ratio of prothrombin time should be normalized with prothrombin complex con-centrate or fresh-frozen plasma and additional vitamin K. Patients with ICH were treated surgically, often based on individual decisions – more frequently in Japan, depending on the association with hypertension. Patients with large or intraventricular bleedings were only treated if a life-saving performance was considered, irrespective of the neurologi-cal outcome. Infra- and supratentorial differences weresimilarly addressed in both GLs. Conclusion: This brief sur-vey – when compared with the lengthy original recommen-dations – provides a stimulating basis for an extended inter-est among Japanese and European stroke clinicians to learn from their individual experiences and to strengthen efforts for joint cooperation in treating and preventing stroke all around the globe. Copyright © 2013 S. Karger AG, Basel
Intracerebral hemorrhage (ICH) accounts for 10–17% of all strokes. The incidence of ICH is influenced by racial factors and was found to be higher in Blacks, Hispanics and Asians compared to the white population. In partic-ular, Asian ethnic origin is a possible risk factor for intra-cranial hemorrhage. In 1965, Japan had the highest mor-tality of stroke worldwide with the mortality rate of ICH being quite high among all stroke types. A recent meta-analysis indicates that the incidence of ICH in the gen-eral Asian population was 2-fold higher than that in the white population [1] .
We compared the European Stroke Initiative (EUSI) Recommendations for the management of ICH (2006) [2] and the chapters of ICH in the Japanese guidelines for the management of stroke (2009) [3] . Japanese guidelines are more up to date and thus included trials that were not available when EUSI guidelines were written. In the fol-lowing, we try to present differences and similarities of both guidelines and worked out which recommendations lacked in both guidelines.
Primary Prevention and Treatment of Risk Factors
The EUSI guidelines give no recommendations for primary prevention , but give some evidence concerning different risk factors ( table 1 ). Arterial hypertension is mentioned as the most common risk factor for sponta-
neous ICH. The EUSI Writing Committee describes that the role of hypertension and the beneficial effect of antihypertensive treatment with regard to the risk of ICH were verified in PROGRESS (Perindopril Protec-tion against Recurrent Stroke Study) [4] , which showed that the relative risk of ICH was reduced by 50% in comparison with the placebo-treated group after a 4-year follow-up, but give no recommendation for treatment as primary prevention. In the Japanese guide-lines, hypertension is regarded as the greatest risk factor for ICH and ischemic stroke. There is a positive linear correlation between blood pressure levels and the risk of stroke: the higher the blood pressure, the higher the risk of stroke [5] . Thus, medical antihypertensive treat-ment was strongly recommended as primary preven-tion [6] .
Concerning hypercholesterolemia, the EUSI recom-mendations mention that hypercholesterolemia is associ-ated with a lower risk of ICH, but treatment with statins did not increase the risk of ICH. The risk of hemorrhagic stroke, including ICH, is higher in smokers, but no rec-ommendation of nonsmoking as a primary prevention is verbalized. An increased body mass index, which was found to be correlated with an increase in intraventricular hemorrhage (IVH) volume, or alcohol consumption are also considered risk factors for ICH. The Japanese guide-lines recommend consumption of a moderate amount of vegetables and fruits every day, whereas no dietary advice was found in the EUSI guidelines.
For secondary prevention after ICH, EUSI guidelines give recommendations for lowering blood pressure with a diuretic and angiotensin-converting enzyme inhibitor (level A), excessive alcohol should be discouraged (class IV), persons with elevated body mass index should take a weight-reducing diet (despite lack of evidence) and smok-ers should quit smoking (class IV evidence).
Acute Blood Pressure Management
There is no randomized controlled trial comparing the severity and prognosis of patients with acute hyperten-sion and ICH with/without blood pressure-lowering treat-ment ( table 2 ). Further clinical studies need to be con-ducted in the future to determine the optimal target level to which blood pressure should be lowered from the per-spective of clinical prognosis. The target level in the Japa-nese guidelines is quite high (systolic blood pressure <180 mm Hg) and differs much from the major expert opin-ions in the nationwide survey [7] , where most experts re-

Comparison of Stroke Guidelines: Acute Management of Intracerebral Hemorrhage
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
421
garded <140, <150 or <160 mm Hg as a target systolic blood pressure partly based on results of small domestic studies [8, 9] . The EUSI guidelines recommend target lev-els and maximum levels of blood pressure for known and unknown hypertension, and recommend an adaptation
in case of elevated intracranial pressure (ICP). Routine blood pressure lowering is not recommended.
Furthermore, different medications are mentioned in the EUSI guidelines, especially intravenous drugs due to their better controllability. EUSI guidelines recommend
Table 2. Acute blood pressure (BP) management
European guidelines 2006 (EUSI) Japanese guidelines 2009
Known hypertension (HPT)If SBP >180 mm Hg or DBP >105 mm Hg→ BP <170/100 mm Hg or MAP <125 mm Hg (class IV, level C)
maintain SBP <180 mm Hg or MAP <130 mm Hg(grade C1)
Unknown history of HPTIf SBP >160 mm Hg or DBP >95 mm Hg→ BP <150/90 mm Hg or MAP <100 mm Hg (class IV, level C)
when performing surgical treatment:→ more aggressive BP lowering (grade C1)
Decrease pressure not more than 20% of MAP on admission (class IV, level C)When ICP elevated (nitroprusside contraindicated)→ adapt thresholds to cerebral perfusion pressure >70 (class IV, level C)Intravenous drugs recommended for better controllability (GCP) no special hypotensive drug recommended, careful use of
vasodilators (nitrates), because they induce brain HPT (grade C1)
SBP = Systolic blood pressure; DBP = diastolic BP; MAP = mean arterial pressure; HPT = hypertension.
Table 1. Primary prevention and treatment of risk factors
European guidelines 2006 (EUSI) Japanese guidelines 2009
HypertensionAn important role with regard to the risk of ICH.Treatment of hypertension has a beneficial effect (level A).
Treating hypertension is the most vital step to reduce the risk of ICH (grade A).
HypercholesterolemiaAssociated with a lower risk of ICH; however, treatment with statins does not increase the risk of ICH (level B).
It has generally been agreed that its underlying hepatic disease and coexisting hypertension should be treated.Lowering serum cholesterol levels with statins does not increase the incidence of ICH, but some data have implied that intervention for stroke patients may increase the recurrence of ICH (grade B).
Smoking is a risk factor for ICH (level B).People should be encouraged to take a moderate amount of vegetables and fruits every day (grade B).
Alcohol consumptionSeveral studies document an increased risk of ICH in relation to alcohol consumption. Spontaneous ICH can probably also be triggered by binge drinking (level C).
Heavy alcohol consumption leading to abnormal blood γ-GTP levels should be discouraged (grade B).
We recommend the very careful consideration of an appropriate dose of each antithrombotic drug and its dual medications that are required to control concurrent hypertension (grade B).
A variety of illicit drugs are known to cause ICH(amphetamines, cocaine and phenylpropanolamine).

Toyoda/Steiner/Epple/Kern/Nagayama/Shinohara/Hennerici
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
422
a careful use of calcium antagonists because of their rap-id and excessive hypotensive effect. In the Japanese guidelines, the use of calcium antagonists (e.g. nicardip-ine) is contraindicated in patients with hyperacute ICH, because of vasodilating effects and possible antiplatelet actions of calcium antagonists; however, direct evidence for this is lacking. In the above-mentioned nationwide survey, nicardipine was the most popular agent for acute ICH management [7] . In 2011, the Japanese government finally ordered the pharmaceutical makers of nicardi-pine to revise the label. In the new label, description of contraindication for ICH was abolished. In 2012, sev-eral Asian nations similarly revised the label of nicardi-pine.
The EUSI or Japanese guidelines did not consider the results of ATACH (Antihypertensive Treatment of Acute Cerebral Hemorrhage) [10] and INTERACT (In-tensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial) [11] , although the newer American Heart Association/American Stroke Association guide-lines [12] advocate that lowering systolic blood pres-sure to 140 mm Hg is probably safe based on the results of INTERACT [11] . The results of both INTERACT 2 [13] and ATACH II [14] are awaited, and might further answer the question of whether there are other benefits of early systolic blood pressure reduction in patients with ICH, and provide clearer evidence for the target blood pressure and the choice of drugs. However, it seems reasonable to lower blood pressure cautiously appreciating a slight effect of antihypertensives on he-matoma expansion reduction in an overall weak or equivocal context of evidence and considering that au-toregulation is often preserved in the acute phase (as opposed to the postacute phase) of ICH and further-more aggressive lowering of blood pressure theoreti-cally carries the risk of cerebral ischemia in hyperten-sive patients.
Acute Hemostatic Management
EUSI guidelines do not recommend the use of hemo-static agents (as tranexamic acid, e-aminocaproic acid and aprotinin) to control bleeding, because no clinical ef-ficacy has been demonstrated thus far ( table 3 ). Japanese guidelines recommend blood products such as platelets, prothrombin complex concentrate (PCC) or fresh-frozen plasma (FFP) in hypertensive ICH only in case of concur-rent abnormal blood coagulation or platelet counts, though such products have been rarely in clinical use as
hemostatic agents unless patients were anticoagulant us-ers in Japan.
Concerning ICH associated with oral anticoagulant therapy , both guidelines give similar recommendations, whereas Japanese guidelines prefer PCC rather than FFP (although PCC is not covered by the Japanese health in-surance). Current questions arise on feasibility, safety and efficacy of prothrombin-dependent coagulation fac-tors in concentrated PCC versus unconcentrated FFP versus single factors like recombinant coagulation factor VIIa. The current information on these questions is in-consistent, and any conclusion drawn towards the pref-erence of one of these coagulants is premature. Time to reversal of the international normalized ratio (INR) seems to be the most important determinant, and mini-mizing delays in drug administration should have high-est priority, as recommended in both guidelines. Initial dosages of PCC for the reversal are different between both guidelines: 10–30 (or 10–50) U/kg in the EUSI rec-ommendation and 500 U regardless of body weight in the Japanese one.
There is a considerable dilemma concerning when to restart anticoagulant therapy following ICH. The opti-mum timing of the resumption of anticoagulation is a cru-cial issue with conflicting evidence. EUSI recommended to restart not earlier than 10–14 days after the index bleeding but to check indication first. The Japanese guide-lines recommend use of heparin after normalization of INR in patients with an elevated risk for embolism, but do not mention the timing of heparinization. Among the respondents in the nationwide survey, the timing to re-start anticoagulation varied greatly: within 4 days in 7%, 5–7 days in 21%, 8–14 days in 25%, 15–28 days in 28% and 29 days or later in 18% [15] .
The new direct oral anticoagulants (DOAC) as dabiga-tran, rivaroxaban and apixaban seem to be a safer and more convenient replacement for warfarin. Due to fewer drug and food interaction, easier handling and a more favorable risk-benefit profile compared with warfarin,it is conceivable that the number of patients treatedwith DOAC will increase. The optimal management of DOAC-associated ICH is unknown and no specific anti-dote is available. For this reason, physicians are faced with new challenges, especially in emergency situations, and questions arise on how to manage emergency situations like the indication for thrombolysis in acute stroke, and the management of intracranial or gastrointestinal bleed-ings. In the future, guidelines have to give recommenda-tions how to manage DOAC-associated hemorrhages, but data are still limited.

Comparison of Stroke Guidelines: Acute Management of Intracerebral Hemorrhage
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
423
Table 4. Respiratory management
European guidelines 2006 (EUSI) Japanese guidelines 2009
Included in the general management and as part of ICP management (see text).
Airway management and/or artificial respiratory management should be considered when disturbance of consciousness has progressed and a respiratory disorder is present during the acute phase (grade C1). Routine oxygen administration to patients with mild-to-moderate stroke is notrecommended (grade C2).
Hyperbaric oxygen therapy for treatment or determination of surgical indication is not recommended (grade C2).
Table 3. Acute hemostatic management
European guidelines 2006 (EUSI) Japanese guidelines 2009
For non-antithrombotic usersPending further data on efficacy and safety, recombinant factor VIIa should not be used outside of a phase III trial.A phase III trial is needed to confirm the beneficial effect of recombinant factor VIIa in ICH (class IV, level B, obsolete).
Hypertensive ICH + normal coagulation→ Blood products are not recommendable (grade C2).Hypertensive ICH + abnormal platelets or blood coagulation system + bleeding tendency→ consider blood products such as platelets, PCC and FFP (grade C1).There is no adequate scientific evidence to support the use of capillary stabilizers or antiplasmin agents for the treatment of acute ICH (grade C1).
ICH during oral anticoagulant treatment (OAT) such as warfarinINR >1.4 → OAT should be discontinued and the INR should be normalized with PCC or FFP. Intravenous vitamin K should be added (class IV).
Stop warfarin and normalize the prothrombin time (PT) INR to ≤1.35 using vitamin K and blood products as soon as possible (grade B). Use of PCC (not covered by Japanese health insurance) is recommended rather than FFP (grade B). With high risk or recurrent cerebral embolism → activated partial thromboplastin time should be 1.5- to 2-fold higher using heparin after normalizing PT-INR (grade C1).
After ICH, antiplatelet treatment has to be individualized, depending on the presence of ischemic vascular diseases or their perceived risk on the one hand and the anticipated risk of ICH recurrence on the other (class IV).
In patients who develop ICH during thrombolytic therapy, thrombolytic drugs and antithrombotic drugs should be immediately stopped, and it is recommended to correct the low levels of coagulation factors such as fibrinogen and prolonged PT and activated partial thromboplastin time using blood products and protamine (grade C1). Indication for surgical evacuation of the hematoma should be carefully examined while taking account of the functional prognosis after correcting the bleeding tendency (grade C1).
After having rechecked the indication for anticoagulation (following the EUSI recommendations on ischemic stroke), OAT may be continued after 10 – 14 days, depending on the perceived risk of thromboembolic occlusion and ICH recurrence (class IV).

Toyoda/Steiner/Epple/Kern/Nagayama/Shinohara/Hennerici
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
424
Table 5. Management of brain edema and intracranial hypertension
European guidelines 2006 (EUSI) Japanese guidelines 2009
The following measurements might be considered in patients with ICH if ICP increases beyond 20 mm Hg:
(ICP level is not defined)
Body positionElevation of body position with respect to CPP(CPP >60 mm Hg; class IV, level C).
Raising the upper part of the bed to put the body at a 30° angle has been reported to be beneficial for patients with intracranial hypertension (grade C1); however, attention should be given to lowering blood pressure.
Osmotic therapyGlycerol (500 ml 10% per day).Mannitol (100 ml 20%; every 3 – 6 h; serum osmolality <320 mmol/l).Hyper-HAES (NaCl 7.5%, HES 6%, serum sodium <150 mmol/l).THAM buffer (central line because of tissue necrosis) 1 mmol/kg bolus, 0.25 mmol/kg as permanent infusion (pH <7.5 – 7.55;class IV, level C).
Intravenous administration of hypertonic glycerol is recommended for major acute ICH accompanying intracranial hypertension (grade B).There is no specific rationale supporting the idea that mannitol treatment is effective for acute ICH (grade C2), but this treatment can be considered when intracranial pressure progressively increases or clinical findings deteriorate in relation to mass effect (grade C1).
HyperventilationIntermittent hyperventilation (pCO2 level of 30 – 35 mm Hg),most useful in the first hours (class IV, GCP).
In patients using a respirator, a mild hyperventilation(pCO2 adjusted to 30 – 35 mm Hg) is recommended (level IIb).
Analgosedation with barbiturates (pentobarbital or thiopental).
CorticosteroidsAt the current stage, corticosteroids are not recommended(class IV, level C).
There is no concrete scientific evidence demonstrating that corticosteroids are effective in reducing acute ICH (grade C2).
Hematoma evacuation with/without craniectomy.
External ventricular drainage in case of hydrocephalus orclinical deterioration and neuroradiological evidence ofbrainstem compression (GCP).
Table 6. Management of seizures
European guidelines 2006 (EUSI) Japanese guidelines 2009
Early prophylactic treatment of seizures is not recommended for all patients, but may be considered for selected patients with lobar ICH. In all other cases, seizures should only be treated if they occur (level C).
Antiepileptics should be used for seizure attacks in patients with acute stroke. Thereafter, the dosage should be carefully reduced while taking into account the possibility of developing late-onset epilepsy (grade C1).
If seizures occur, a stepwise administration of antiepileptic drugs is generally recommended. Antiepileptic treatment should be continued for 30 days. After this time, treatment should bereduced and eventually discontinued. If seizures reoccur, patients should receive chronic treatment with anticonvulsants (level C).
Seizure occurs frequently in patients with ICH involving the cerebral cortex. In ICH limited to the putamen, thalamus or infratentorium, concurrent seizure is rare. The prophylactic use of antiepileptics is not recommended except for patients who have undergone brain surgery (grade C2).
In ICH patients who developed late-onset seizures (>2 weeks after onset), recurrent seizures often occur; thus, administration of anti-epileptics is advisable (grade C1).

Comparison of Stroke Guidelines: Acute Management of Intracerebral Hemorrhage
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
425
Management of Seizures
In Japanese guidelines, the management of early and late-onset seizures is separately recommended. EUSI guidelines are more detailed and recommend a stepwise treatment with recommendations including drug dosag-es for seizure or status epilepticus treatment ( table 6 ).
Prevention of Deep Venous Thrombosis and
Pulmonary Embolism
Concerning prevention of deep venous thrombosis and pulmonary embolism, both guidelines have similar rec-ommendations ( table 7 ).
Surgical Indication for Acute ICH
Concerning surgical indication for acute ICH , Japa-nese guidelines distinguish between treatment in patients with hypertensive ICH and ICH not associated with hy-pertension. For hypertensive ICH, detailed recommen-dations according to different locations are provided. EUSI guidelines discern only between supratentorial or infratentorial ICH ( tables 8, 9 ). Supratentorial ICH is di-vided into superficial (mostly) lobar and deep (mostly basal ganglion) locations, which mainly goes back to the results of STICH (International Surgical Trial in Intrace-rebral Hemorrhage) [16] . They give no general recom-mendations for surgical treatment. For infratentorial hemorrhages, good results are mentioned for surgical evacuation of cerebellar hematomas, but optimal timing for surgery is not provided. EUSI guidelines do not give recommendations for brain stem hemorrhage, but they
Respiratory Management
There is no special recommendation concerning respiratory management for patients with ICH in the EUSI guidelines ( table 4 ). Oxygenation should be moni-tored continuously; in addition, respiratory care and prophylactic measures concerning aspiration pneumo-nia should be part of the general treatment of all stroke patients, including those with ICH. Japanese guidelines give special recommendations for respiratory manage-ment.
Management of Brain Edema and Intracranial
Hypertension
EUSI guidelines concerning ICP management give more detailed recommendations, especially for drug dosage and an escalation scheme for treatment ( table 5 ). Both guidelines recommend a mild therapeutic hyper-ventilation to achieve arterial pCO 2 levels of 30–35 mm Hg, and both recommend elevation of body position at a 30° angle to decrease ICP. Intravenous administration of hypertonic glycerol is a frequent choice for major acute ICH in Japan. Concerning the application of mannitol, Japanese guidelines recommend the use only in cases of severe mass effect. Barbiturates are not recommended in Japanese guidelines as ultimate treatment option. Both guidelines do not mention hypothermia as therapeutic option to reduce ICP. Japanese guidelines do not recom-mend hypothermia because of lacking evidence (grade C2). Both guidelines recommend lowering of body tem-perature in case of fever, using even methods such as cooling.
Table 7. Prevention of deep venous thrombosis and pulmonary embolism
European guidelines 2006 (EUSI) Japanese guidelines 2009
Compression stockings and intermittent pneumatic compres-sion are recommended for the prevention of thromboembolism in patients with disabling limb weakness from the beginning of treatment (class IV).
When paralysis is noted in patients with acute ICH, deep venous thrombosis and pulmonary embolisms should be preventedusing compression stockings or intermittent pneumaticcompression, or the combination of these (grade B).
Low-dose subcutaneous heparin or low-molecular-weight heparin should be considered after 24 h, especially in patients who are at high risk of thromboembolism (class IV).
Administration of low-dose heparin can be considered for ICH patients with concurrent hemiplegia without rebleeding 3 – 4 days after onset (level IIa).

Toyoda/Steiner/Epple/Kern/Nagayama/Shinohara/Hennerici
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
426
Table 8. Surgical indication for supratentorial ICH
European guidelines 2006 (EUSI) Japanese guidelines 2009
General recommendation:If ICH <10 ml or mild neurological deficit regardless of the site ifICH → no surgery (grade D).No rationale for recommending evacuation for patients with deep coma (Japan Coma Scale III-300) (grade C2).
No evidence for a general recommendation (class IV, level C).
Putaminal hemorrhage:If ICH is superficial (the clot is subcortical ≤1 cm from the surface and does not reach the deep basal ganglia) orif there is deterioration in consciousness (from GCS level of between 12 and 9 to ≤8) → Consider craniotomy (level C).
–
–
Consider evacuation if hematoma volume >31 ml in patients with moderate neurological findings and evidence of severe mass effect (grade C1).Particularly stereotactic evacuation is recommended for patients with disturbed consciousness (Japan Coma Scale II-20 to 30) (grade B).
Thalamic hemorrhage:No rationale for hematoma evacuation in the acute stage (grade C2). Ventricular drainage can be considered when accompanied with intraventricular hematoma or marked ventricular dilatation (grade C1).
Deep-seated hematomas do not benefit from craniotomy.Stereotactic aspiration may be considered(class IV), especially if mass effect is present.
Lobar (subcortical) hemorrhage:–
–
Consider surgery if hematoma is <1 cm of the surface (grade C1).Craniotomy recommended as surgical procedure (grade C1).
Table 9. Surgical indication for infratentorial ICH
European guidelines 2006 (EUSI) Japanese guidelines 2009
Cerebellar hemorrhageIf cerebellar ICH >2 – 3 cm in diameter, deterioration or brain stem compression and/or hydrocephalus occurs consider surgical evacuation and ventricular drainage as soon as possible (class IV, level C).
Surgery can be considered if cerebellar hemorrhage is >3 cm, if patients deteriorate neurologically, or patients have brain stem compression and hydrocephalus from ventricular obstruction (grade C1).
Intraventricular hemorrhageIntraventricular thrombolysis trials may be considered if an external ventricular drainage becomes necessary (class IV, level C), but not in infants. An intraventricular thrombolysis with urokinase or recombinant tissue plasminogen activator seems to be effective.
Because it is quite likely to be associated with vascular disease it is desirable to perform angiography to detect the bleeding source (grade C1). Ventricular drainage should be considered for acute hydrocephalus (grade C1).
Brainstem hemorrhageNo recommendation. There is no rationale for hematoma evacuation (grade C2).
Ventricular drainage can be considered when most of the hematoma is in the ventricle and the ventricle is highly dilated (grade C1).
In case of hydrocephalusExternal drainage can be ventricular or via the lumbar route if it is a communicating type of hydrocephalus (class IV). Lumbar drainage is definitely contraindicated with all types of obstructive hydrocephalus or if the etiology is in doubt.
Consider external ventricular drainage (grade C1).

Comparison of Stroke Guidelines: Acute Management of Intracerebral Hemorrhage
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
427
are more detailed concerning treatment of hydrocephalus compared with the Japanese guidelines. Both guidelines recommend the use of external ventricular drainage in case of hydrocephalus.
Organized studies on the selection of treatment pro-cedures are rare. Some trials showed a trend in favor of early surgery in supratentorial nonaneurysmal ICH. The international STICH trial was conducted to demonstrate clinical efficacy of surgery in ICH but was not designed to look at the ideal surgical technique. It suggested a small nonsignificant advantage for surgery. A subgroup analysis showed that patients with superficial hemato-mas and without IVH presented a more encouraging pic-ture of surgery [16] . Thus we are still unable to specify potential candidates for the optimum surgical technique in current guidelines. The ongoing STICH II trial [17] investigates the hypothesis that patients with superficial lobar hematomas and no IVH might benefit from early hematoma evacuation (<12 h after randomization) [17] . A previously published meta-analysis of 2,186 cases con-cluded that in particular early surgery (<8 h of ictus) is beneficial [18] .
In Japan, a nationwide survey on 7,010 patients with putaminal hemorrhage was conducted, and mortality and functional prognosis 3 months after its onset were compared in 1990 [19] . The survey indicated that surgical therapy for putaminal hemorrhage was beneficial only when it was performed to save the lives of patients in very poor condition. A randomized comparative trial on ste-reotactic evacuation of putaminal hemorrhage in patients with moderately disturbed consciousness on admission showed a better functional outcome than in those with medical treatment [20] .
It has been shown that patients with smaller hemor-rhage have a better clinical outcome and a lower mortal-ity, which led to the hypothesis that methods of removing ICH in stable patients could result in a lowered risk of mortality and improved outcome [21, 22] . The ongoing MISTIE (Minimally Invasive Surgery plus rt-PA for ICH Evacuation) trial [22] (NCT00224770) has the purpose to determine the efficacy of using a combination of mini-mally invasive surgery and clot lysis with recombinant tissue plasminogen activator to remove ICH using image-based surgery (MRI or CT) to provide catheter access to ICH for the intervention for clot aspiration followed by instillation of up to 9 doses of recombinant tissue plas-minogen activator compared to conventional medical management. The specific objective of MISTIE is to test the efficacy and safety of this intervention and assess its ability to remove blood clots from brain tissue. The treat-
ment of spontaneous supratentorial ICH will remain controversial until a definitive prospective randomized controlled trial shows evidence in favor of a particular treatment. At present, the recommendations for or against surgery are based on conflicting evidence.
Also, for IVH, recommendations are difficult due to the lack of evidence. The EUSI recommend intraventric-ular thrombolysis only within clinical trials, and Japanese recommendations discuss different randomized compar-ative trials on urokinase treatment, concluding that intra-ventricular urokinase is effective at least for life-saving treatment for patients with severe IVH [23] , but give no recommendation for this therapy. It needs to be men-tioned that urokinase might not be available in many countries.
Concerning ICH caused by cerebral arteriovenous malformation, dural arteriovenous fistulas, cavernous angiomas or venous angiomas, Japanese guidelines give very detailed information and recommendations con-cerning risk factors for bleeding, surgery, embolization, stereotactic radiotherapy, epilepsy and pediatric pa-tients. EUSI guidelines give only a short recommenda-tion for ICH caused by arteriovenous malformations. Japanese recommendations also cover ICH due a to brain tumor [‘Surgical treatment is recommended for patients with massive hemorrhage from a brain tumor accompanied by the mass effect (grade C1). Acute dete-rioration of visual acuity and the visual field due to pi-tuitary apoplexy are indications for emergency surgery (grade C1)’].
Recommendations Mentioned Only in One of the
Guidelines
In the EUSI guidelines, recommendation for brain im-aging for ICH diagnosis was described. CT and MRI are equally sensitive, however CT may be faster. ICH in a typ-ical location but at young age or without a history of hy-pertension needs further diagnostic workup, including MR angiography, CT angiography or digital subtraction angiography to investigate the underlying vascular pa-thology. However, Japanese guidelines do not refer to im-aging strategies.
Japanese guidelines give special recommendations concerning upper gastrointestinal bleeding in patients with hypertensive ICH. Special caution should be exer-cised to concurrent gastrointestinal bleeding, and pro-phylactic administration of an antiulcer agent is rec-ommended (C1). EUSI guidelines do not mention upper

Toyoda/Steiner/Epple/Kern/Nagayama/Shinohara/Hennerici
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
428
References
1 van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ: Incidence, case fa-tality, and functional outcome of intracere-bral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 2010; 9: 167–176.
2 Steiner T, Kaste M, Forsting M, Mendelow D, Kwiecinski H, Szikora I, Juvela S, Marchel A, Chapot R, Cognard C, Unterberg A, Hacke W: Recommendations for the management of intracranial haemorrhage – part I: spontane-ous intracerebral haemorrhage. The Europe-an Stroke Initiative Writing Committee and the Writing Committee for the EUSI Execu-tive Committee. Cerebrovasc Dis 2006; 22: 294–316.
3 Shinohara Y, Yanagihara T, Abe K, Yoshi-mine T, Fujinaka T, Chuma T, Ochi F, Nagayama M, Ogawa A, Suzuki N, Katayama Y, Kimura A, Yasui N: III. Intracerebral hemorrhage. J Stroke Cerebrovasc Dis 2011; 20(suppl 1):S74–S99.
4 PROGRESS Collaborative Group: Ran-domised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 in-dividuals with previous stroke or transient ischaemic attack. Lancet 2001; 358: 1033–1041.
5 MacMahon S, Peto R, Cutler J, Collins R, Sor-lie P, Neaton J, Abbott R, Godwin J, Dyer A, Stamler J: Blood pressure, stroke, and coro-nary heart disease. Part 1, Prolonged differ-ences in blood pressure: Prospective observa-tional studies corrected for the regression di-lution bias. Lancet 1990; 335: 765–774.
6 Zhang H, Thijs L, Staessen JA: Blood pressure lowering for primary and secondary preven-tion of stroke. Hypertension 2006; 48: 187–195.
7 Koga M, Toyoda K, Naganuma M, Kario K, Nakagawara J, Furui E, Shiokawa Y, Hasegawa Y, Okuda S, Yamagami H, Kimura K, Okada Y, Minematsu K, Stroke Acute Management with Urgent Risk-Factor Assessment and Im-provement (SAMURAI) Study Investigators: Nationwide survey of antihypertensive treat-ment for acute intracerebral hemorrhage in Japan. Hypertens Res 2009; 32: 759–764.
8 Ohwaki K, Yano E, Nagashima H, Hirata M, Nakagomi T, Tamura A: Blood pressure man-agement in acute intracerebral hemorrhage: relationship between elevated blood pressure and hematoma enlargement. Stroke 2004; 35: 1364–1367.
9 Itabashi R, Toyoda K, Yasaka M, Kuwashiro T, Nakagaki H, Miyashita F, Okada Y, Nari-tomi H, Minematsu K: The impact of hyper-acute blood pressure lowering on the early clinical outcome following intracerebral hem-orrhage. J Hypertens 2008; 26: 2016–2021.
10 Antihypertensive Treatment of Acute Cere-bral Hemorrhage (ATACH) investigators: Antihypertensive treatment of acute cerebral hemorrhage. Crit Care Med 2010; 38: 637–648.
11 Anderson CS, Huang Y, Wang JG, Arima H, Neal B, Peng B, Heeley E, Skulina C, Parsons MW, Kim JS, Tao QL, Li YC, Jiang JD, Tai LW, Zhang JL, Xu E, Cheng Y, Heritier S, Morgenstern LB, Chalmers J, INTERACT In-vestigators: Intensive blood pressure reduc-tion in acute cerebral haemorrhage trial (IN-TERACT): a randomised pilot trial. Lancet Neurol 2008; 7: 391–399.
12 Morgenstern LB, Hemphill JC 3rd, Anderson C, Becker K, Broderick JP, Connolly ES Jr, Greenberg SM, Huang JN, MacDonald RL, Messé SR, Mitchell PH, Selim M, Tamargo RJ, American Heart Association Stroke Council and Council on Cardiovascular Nursing: Guidelines for the management of spontane-ous intracerebral hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Associa-tion. Stroke 2010; 41: 2108–2129.
13 Delcourt C, Huang Y, Wang J, Heeley E, Lind-ley R, Stapf C, Tzourio C, Arima H, Parsons M, Sun J, Neal B, Chalmers J, AndersonC, INTERACT2 Investigators: The second (main) phase of an open, randomised, multi-centre study to investigate the effectiveness of an intensive blood pressure reduction in acute cerebral haemorrhage trial (INTERACT2). Int J Stroke 2010; 5: 110–116.
14 Qureshi AI, Palesch YY: Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH) II: design, methods, and rationale. Neurocrit Care 2011; 15: 559–576.
15 Maeda K, Koga M, Okada Y, Kimura K, Yama-gami H, Okuda S, Hasegawa Y, Shiokawa Y, Furui E, Nakagawara J, Kario K, Nezu T, Minematsu K, Toyoda K, Stroke Acute Man-agement with Urgent Risk-Factor Assessment and Improvement (SAMURAI) Study Investi-gators: Nationwide survey of neuro-special-ists’ opinions on anticoagulant therapy after intracerebral hemorrhage in patients with atrial fibrillation. J Neurol Sci 2012; 312: 82–85.
gastrointestinal bleedings. Furthermore, special recom-mendations for ICH in patients with renal failure are cov-ered only in the Japanese guidelines.
Concerning secondary prevention of depression, Eu-ropean guidelines did not mention this complication, whereas Japanese guidelines recommend the following: Depression frequently occurs after stroke including ICH. It should be assiduously examined for because depression is a factor interfering with cognitive and physical function and activities of daily living (grade B). Drug therapy for a poststroke depressive state is recommended because it is expected to improve depressive symptoms and physical function (grade B).
Both guidelines recommend treatment in specialized care units (in the chapter of Stroke in General in the Jap-anese guidelines). All patients with acute ICH should preferably be treated in stroke units or in intensive care
units if the patient condition requires this, because stroke unit care reduces mortality and increases the likelihood of good functional outcome of stroke in general. Due to a variety of similarities between acute ischemic stroke and ICH, it seems to be plausible that the specialized treat-ment might also be beneficial for patients with ICH (lev-el C). Early mobilization and rehabilitation unless intra-cranial hypertension is present is recommended only in EUSI guidelines (class IV evidence).
Acknowledgments
We would like to thank Drs. Norio Tanahashi (Saitama Medi-cal University International Medical Center) and Masayasu Mat-sumoto (Hiroshima University Graduate School of Biomedical and Health Sciences) for their valuable advice.

Comparison of Stroke Guidelines: Acute Management of Intracerebral Hemorrhage
Cerebrovasc Dis 2013;35:419–429DOI: 10.1159/000351754
429
16 Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, Shaw MD, Barer DH, STICH investigators: Early surgery versus initial conservative treat-ment in patients with spontaneous supraten-torial intracerebral haematomas in the Inter-national Surgical Trial in Intracerebral Haem-orrhage (STICH): a randomised trial. Lancet 2005; 365: 387–397.
17 Mendelow AD, Gregson BA, Mitchell PM, Murray GD, Rowan EN, Gholkar AR, STICH II Investigators: Surgical trial in lobar intrace-rebral haemorrhage (STICH II) protocol. Tri-als 2011; 12: 124.
18 Gregson BA, Broderick JP, Auer LM, Batjer H, Chen XC, Juvela S, Morgenstern LB, Pan-tazis GC, Teernstra OP, Wang WZ, Zuccarel-lo M, Mendelow AD: Individual patient data subgroup metaanalysis of surgery for sponta-neous supratentorial intracerebral hemor-rhage. Stroke 2012; 43: 1496–1504.
19 Kanaya H: Current situations of treatments of hypertensive intracerebral hemorrhage: re-sults of a national survey (in Japanese). Jpn J Stroke 1990; 12: 509–524.
20 Hattori N, Katayama Y, Maya Y, Gatherer A: Impact of stereotactic hematoma evacuation on activities of daily living during the chronic period following spontaneous putaminal hemorrhage: a randomized study. J Neuro-surg 2004; 101: 417–420.
21 Lampl Y, Ronit G, Eshel T: Neurological and functional outcome in patients with supraten-torial hemorrhages. A prospective study. Stroke 1995; 26: 2249–2253.
22 Morgan T, Zuccarello M, Narayan R, Keyl P, Lane K, Hanley D: Preliminary findings ofthe Minimally-Invasive Surgery plus rtPAfor Intracerebral Hemorrhage Evacuation (MISTIE) clinical trial. Acta Neurochir Suppl 2008; 105: 147–151.
23 Andrews CO, Engelhard HH: Fibrinolytic therapy in intraventricular hemorrhage. Ann Pharmacother 2001; 35: 1435–1448.


















